developing clinical guidelines on promoting oral health health disability ireland.pdf · developing...
TRANSCRIPT
practice & research
developing clinical guidelineson promoting oral health:an action research approachA service providing day and residential care in Ireland has improved the general and
oral health care of people with learning disability. Sheila Doyle and Caroline Dalton report
Over past decades the promotion
of normalisation and socially
inclusive policies has resulted in a
move from institutional care to community
living for people with a learning disability
(Wolfensberger 1972). Service providers seek
to ensure that people experience greater
choice and control in their Mves and are
included Vi/ithin their communities (Jones
1999, Northway etal 2005). According to
the National Intellectual Disability Data-
base 2007. 8.262 individuals (or 32.3 per
cent of people with learning disabilities in
the Republic of Ireland) live in residential
settings, mainly in the community (Kelly ei
al 2007). 'The numbers of people accom-
modated in community group homes and
in residential centres have increased and
decreased respectively, on an almost contin-
uous basis, since data collection commenced
in 1996; Kelly et a/note.
People with a learning disability have the
right to be valued and supported as equal
citizens, including the right to access equi-
table health care. As a result of community
living, such people are accessing main-
stream healthcare services more frequently
1 ¿ LEARNING DISABILITY PRACTICE vol 11 no 2 March 2008

practice & research
(Department of Health and Children 2002).
However, the evolving evidence base suggests
that such individuals experience health
disparities (Mencap 2004). with studies
linking this disparity to a lack of specialist
knowledge and training of community
healthcare vi'orkers on the needs of people
with learning disabilities (Prasher and Janicki
2002). Although these people have the same
rights to equal standards of health care as the
general population, there is evidence that
they generally experience poorer health, and
oral health in particular, have unmet health
needs and have lower uptake of screening
services (Faculty of Dental Surgery 2001).
Importance of oral hygiene
Oral diseases have not always been given as
much priority as other complex medical prob-
lems (Malmstrom et al 2002). Yet the effect
of oral problems on an individual's quality
of life can be profound (Locker 1992). Oral
disease has been linked with other systemic
diseases, including cardiovascular disease,
cerebrovascular disease, diabetes, respiratory
infection, periodontal bone loss and oste-
oporosis (Malmstorm ef ai 2002). Poor oral
health can result in significant pain and an
inability to consume nutritious food, and can
damage a person's self-image and confidence
(National Disability Authority 2005). Good
oral health has many holistic benefits in that
it can improve general health, dignity and
self-esteem, social integration and quality of
life (Fiskeeial2000).
Up to 36 per cent of adults with learning
disability and 80 per cent of adults with
Down syndrome are believed to have
unhealthy teeth and gums (Mencap 2004).
with common oral conditions such as dental
caries and periodontal disease featuring
prominently.
A study can̂ ied out in 27 residential services
in Ireland on the oral health of 281 adults
with leaming disabilities showed the residents
had lower levels of treatment of dental caries
and periodontal diseases in comparison to the
general population (Crowley eta/2003). The
study identified that the residents had more
extractions, fewer restorations, fewer natural
teeth and were less likely to have dentures.
These findings mirror those in a qualitative
study of the oral health of 269 individuals
with leaming disabilities in Northern Ireland
(Department of Health. Social Services and
Public Safety 2005).
A Japanese study of 24 adults with Down
syndrome found that all of them had advanced
periodontal disease. In the worst cases, the
disease had progressed to its maximum, while
the lowest rate was 60 per cent (Yoshihara
et al 2005). The relevance of this finding is
significant for people with Down syndrome
because studies have identified that up to
40 per cent of people with Down syndrome
suffer from congenital heart defects and
immunosuppression (Griffiths 2000). Cardio-
vascular patients are at high risk of developing
bacterial endocarditis during invasive dental
procedures (Stiefil 2002).
'Good oral health has manyholistic benefits in that it
can improve general health,dignity and self-esteem, socialintegration and quality of life'
MethodGiven the importance of oral health care.
the Kerry Parents and Friends Association
undertook an action research approach
to review the oral health of people with
learning disability who make use of their
services in southern Ireland, The associa-
tion is committed to providing a profes-
sionally delivered, quality service to people
with a learning disability and their families,
Avison ei a/ ( 1999) say of action research:
The emphasis is more on what practitioners
do than on what they say they do', and.
according to Coghlan and Brannick (2005).
action research consists of five distinct
areas:
• pre-step: identifying the necessity of
undertaking the research project
diagnosis: identifying the specific issue/
problem involved
planning action: determining the steps
that need to be taken in relation to the
issue/problem
- taking action: implementing the plan
- evaluating action: examining the intended/
unintended outcome of the actions
taken.
Pre-step
Initially, an oral assessment of those using
the service was undertaken by the Health
Service Executive (HSE) dental services
(Southern Region). The HSE is responsible for
providing health and personal social services
for everyone living in the Republic of Ireland.
The dental team examined 68 people with
a learning disability. 18 of whom lived in
homes run by the association. The other 50
were day attendees who lived at home with
their families.
Diagnosis
A total of 38 people needed some form of
treatment after examination. Most of them
could be treated in primary care settings.
with only two assessed as requiring general
anaesthesia for invasive dental treatment.
With more than half of those screened
needing further treatment, staff identified
oral health as an area that needed further
intervention and wanted to promote oral
health. Following this review, the Kerry
Parents and Friends Association decided to
develop clinical guidelines for promoting
oral health.
Planning action
While treatment for most dental diseases is
available, preventive programmes must be
modified according to the needs and abilities
of each individual (Stiefil 2002). Continuous.
systematic and individualised oral care can
inhibit the progression of oral disease (Yoshi-
hara et a/2005).
While it is clear that clinical guidelines
on oral health care should be included in
practice settings, a study in Ireland identified
that only 12 per cent of service areas had
written oral healthcare guidelines in place
(Crowley et at 2003), Despite the importance
vol 11 no 2 March 2008 LEARNING DISABILITY PRACTICE 13
practice & research
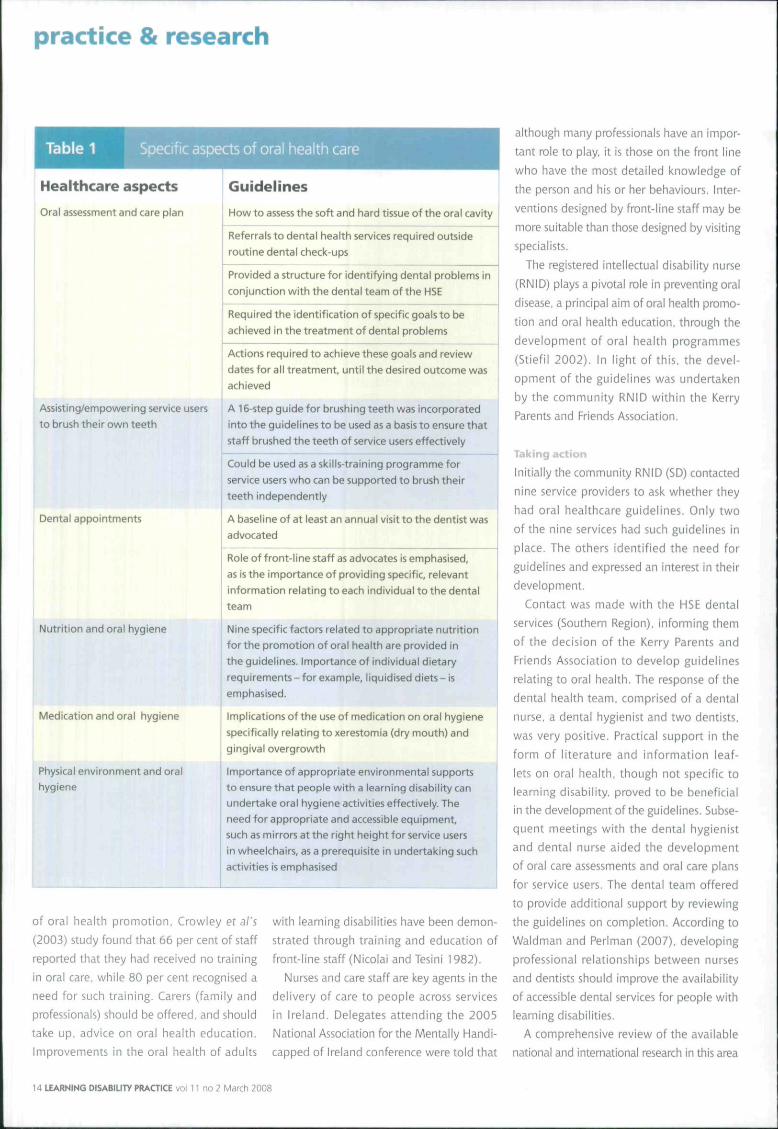
Table 1 ific aspects of oral health care
Healthcare aspects
Oral assessment and care plan
Assisting/empowering service users
to brush their ovun teeth
Dental appointments
Nutrition and oral hygiene
Medication and oral hygiene
Physical environment and oralhygiene
Guidelines
How to assess the soft and hard tissue of the oral cavity
Referrals to dental health services required outside
routine dental check-ups
Provided a structure for identifying dental problems in
conjunction with the dental team of the HSE
Required the identification of specific goals to be
achieved in the treatment of dental problems
Actions required to achieve these goals and review
dates for all treatment, until the desired outcome was
achieved
A 16-step guide for brushing teeth was incorporated
into the guidelines to be used as a basis to ensure that
staff brushed the teeth of service users effectively
Could be used as a skills-training programme for
service users who can be supported to brush their
teeth independently
A baseline of at least an annual visit to the dentist was
advocated
Role of front-line staff as advocates is emphasised,
as is the importance of providing specific, relevant
information relating to each individual to the dental
team
Nine specific factors related to appropriate nutrition
for the promotion of oral health are provided in
the guidelines. Importance of individual dietary
requirements - for example, liquidised diets - is
emphasised.
Implications of the use of medication on oral hygiene
specifically relating to xerestomia (dry mouth) and
gingival overgrowth
Importance of appropriate environmental supports
to ensure that people with a learning disability can
undertake oral hygiene activities effectively. The
need for appropriate and accessible equipment,
such as mirrors at the right height for service users
in wheelchairs, as a prerequisite in undertaking such
activities is emphasised
of oral health promotion. Crowiey et al's
(2003) study found that 66 per cent of staff
reported that they had received no training
in oral care, while 80 per cent recognised a
need for such training. Carers (family and
professionals) should be offered, and should
take up. advice on oral health education.
Improvements in the oral health of aduits
with learning disabilities have been demon-
strated through training and education of
front-line staff (Nicolai and Tesini 1982).
Nurses and care staff are key agents in the
delivery of care to people across services
in Ireland. Delegates attending the 2005
National Association for the Mentally Handi-
capped of Ireland conference were told that
although many professionals have an impor-
tant role to play, it is those on the front line
who have the most detailed knowledge of
the person and his or her behaviours. Inter-
ventions designed by front-line staff may be
more suitable than those designed by visiting
specialists.
The registered intellectual disability nurse
(RNID) plays a pivotal role in preventing oral
disease, a principal aim of oral health promo-
tion and oral health education, through the
development of oral health programmes
(Stiefil 2002). In light of this, the devel-
opment of the guidelines was undertaken
by the community RNID within the Kerry
Parents and Friends Association.
Taking action
Initially the community RNID (SD) contaaed
nine service providers to ask whether they
had oral healthcare guidelines. Only two
of the nine services had such guidelines in
place. The others identified the need for
guidelines and expressed an interest in their
development.
Contact was made with the HSE dental
services (Southern Region), informing them
of the decision of the Kerry Parents and
Friends Association to develop guidelines
relating to oral health. The response of the
dental health team, comprised of a dental
nurse, a dental hygienist and two dentists,
was very positive. Practical support in the
form of literature and information leaf-
lets on oral health, though not specific to
learning disability, proved to be beneficial
in the development of the guidelines. Subse-
quent meetings with the dental hygienist
and dental nurse aided the development
of oral care assessments and oral care plans
for service users. The dental team offered
to provide additional support by reviewing
the guidelines on completion. According to
Waldman and Perlman (2007), developing
professional relationships between nurses
and dentists should improve the availability
of accessible dental services for people with
learning disabilities.
A comprehensive review of the available
national and international research in this area
14 LEARNING DISABILITY PRAaiCE vol 11 no 2 March 2008

practice & research
was also undertaken by the community nurse
(SD) to ensure an evidence-based approach to
the development of the guidelines. Informa-
tion provided by the HSE dental team was
incorporated with research specific to LD in
the development of the guidelines.
The clinical guidelines for the oral health
care of adults with an intellectual disability
were completed last May and focused on the
improvement of oral health care within an
integrated care approach. They were aimed
at all those involved with the health and
welfare of people with a learning disability
and provided information on nine specific
aspects of oral health care (see Table 1 ).
The guidelines offer information on the
care of dentures, oral care of service users
who are edentulous and the oral care of
the unconscious service user. Specific charts
for recording aspects of oral health practice
were also developed, including screening
assessments, oral health care plans and oral
hygiene practices.
Evaluating action
Since the clinical guidelines were completed,
the response has been positive. After they
were endorsed by a management meeting of
the Kerry Parents and Friends Association, a
decision was taken to implement the guide-
lines. Feedback from front-line staff within
the association has also been positive.
Two organisations that were originally
contacted to ascertain whether services
had guidance in place have subsequently
requested a copy of the completed guide-
lines. One of these provided feedback, saying
that the guidelines were practical and easy
to follow. They had been shown to the
dental services for the organisation and it
was recommended that the guidelines be
adopted.
'In identifying best practicein this area, education on oralhealth was considered to bevital for service users, staff
and carers'
Positive feedback from the HSE dental
services indicated that the guidelines will
improve the general and oral health of indi-
viduals attending the service. The dental
team also said that they would like to see
such guidelines developed by all organi-
sations providing services to people with
learning disability.
In identifying best practice in this area.
education on oral health was considered to
be vital for service users, staff and carers.
This has been addressed with the HSE dental
care team, who offered to attend training
sessions to support the use of the clinical
guidelines.
An evaluation of the effect of the guide-
lines and the education of service users, staff
and carers will establish whether the meas-
ures undertaken to promote oral health are
fit for purpose. It is envisaged that such an
evaluation will follow the implementation of
the training programme.
ConclusionThe importance of oral health for people
with a learning disability has been empha-
sised in the literature, as have the health
disparities that can blight lives (Mencap
2004). Learning disability services should
encourage front-line staff to develop knowl-
edge in relation to oral health and offer
guidelines to promote oral health (Crowley
ei al 2003) •
Sheila Doyle RNID, PostgraduateDiploma in Nursing - Multiple andComplex Disabilities, Community Nurse,Kerry Parents and Friends Association
Caroline Dalton RNID, BNS, CertBehaviour Therapy, Lecturer and Courseco-ordinator for the PostgraduateDiploma in Nursing in Multiple andComplex Disabilities (ID), UniversityCollege Cork
References
Avison D, Lau R Myers M, Nielsen PA(1999) Action research. CommumcdííonsoftheACM.42. 1,94-97,
Coghlan D. Brannick T (2005) DoingAction Hesearch In YourOwn Organisation.S,ige Publications, London,
Crowley E, Wheiton H, Murphy Aptat (2003) Oral Health ol Adults with an¡ntellectual Disability in Residential Carein Ireland. Department of Health andChildren, Ireland,
Department of Health and Children{1'002) Proposed Framework for theDevelopment of Clinical Speciäüim andAdvanced Practice in Mental HandicapNursing, Government Publications.Dublin.
Department of Health, Social Servicesand Public Safety (2005) Survey of DentalServices (o People with Learning Disabilitiesin Northern Ireland, www dhsspsni,gov.uk
(Last accessed: 26 February 2008)
Faculty of Dental Surgery (2001 ) OinicalGuidelines & Integrated Care Pathwaysfor the Oral Hea/th Care of People withLeaming Disabilities. Faculty of DentalSurgery, Royal College of Surgeons ofEngland, London,
FiskeJ, GriffithsJ,Jamieson R, MangerD(2000) British Society for Disability andOral Health; guidelines for oral healthcare for long-stay patients and residents,7otjma/ofCerafito/ogy, 17, I. 55-64.
Griffiths J (2000) Guidelines for the OralCare Services for People with Disabilities:Disability and Oral Care. World DentalPress, France, ,
Jones S (1999) Leaming disability!nursing - holistic care at its best. NursingStandard, 13,52,61-63,
Kelly F, Kelly C, Craig S (2007) AnnualReport of the National Intellectual DisabilityDatabase2007, Health Research Board,Dublin.
Locker D (1992) The burden of oraldisorders in populations of older adults,Journa/oí Community Dental Heafth, 9,109-124.
Malmstrom H, Santos-Teachout R. RenY (2002) Dentition and oral health. In;Prasher V Janicki M (Eds) Physical Healthof Adults with Intellectual Disabilities.Blackwell Publishing, Oxford.
Mencap (2004) Treat Me fiigiir! BetterHealthcare for People with LearningDisability. Mencap, London.
National Disability Authority (2005)Oral Health & Disability: The Way Forward.NDA, Dublin, Ireland,
Nicolai A, Tesini D(!982) Improvementsin the oral hygiene of institutionalisedmentally retarded individuals throughtraining of direct care staff, Journa/ ofSpecial Caœ Dentistry. 2. 217-221.
Northway R, Hutchinson C, KingdonA (2005) A Vision for Leamint; DisabilityNursing: A Discussion Document. Learning
Disability Consultant Nurse Network,London,
Prasher V, Janicki M (2002) PhysicalHealth ofAduln with IntellectualDisabilities. Blackwell Publishing,Cornwall,
Stiefil D (2002) Dental cureconsiderations for disabled adults. Journalof Special Care Dentistry. 22. 3, 265-395,
Waldman MB, Perlman SP (2007)Oral health, nurses and patients withdevelopmental disabilities. InternationalJournal of Nursing in Intellectual andDevelopmental Disabilities. 3. 1, 4,
Wolfensberger W (1972) The Principle ofNormjlisation in Human Services, NationalInstitute on Mental Retardation, Toronto.
Yoshihara T Morinushi T Kinjyo S. VämasakiY (2005) Effects of periodic preventativecare on the progression of periodontaldisease in young adiills with Down'ss^ndronieJoumalofOinicJilPeriodontology.32, 6, 556-560.
vol 11 no 2 March 2008 LEARNING DISABILITY PRACTICE 15
