determination of contamination of operation field in head and neck oncological surgery authors:...
TRANSCRIPT

Determination of contamination of operation field in head and neck oncological surgery
Authors: Maciej Mazurek
Filip NowakowskiArtur Włodarczyk
Michał Głuski
Head and Neck Cancer Clinic of Marie Sklodowka Curie Memorial Cancer Centre – InstituteHead: Prof., Andrzej Kawecki Ph.D.
Tutors: Janusz Jaworowski M.D., Maciej Rysz M.D.
Students' Scientific Groupattached toHead and Neck Cancer Clinic

Background:• Surgical resections of head and neck cancer
with one-stage reconstructions are long procedures with high risk of microbial contamination;
• Determination of contaminating factors and efficacy of aseptic procedures is vital for reduction of possible surgical complications.
Aim:
Define possible complications
Determinate contaminating factor
Improvetreatment
Aim of this study is to determinate amount and type of the surgical field contamination factors and to define possible complications that can occur after resection of advanced tumour of head and neck.

Materials and Methods
• Swabs were taken from surgical field and surgical drapes every 2 hours (at 0h, 2h, 4h, 6h);
• Samples were delivered to the laboratory immediately;
• To analize our results we have used Statistica.
• The prospective study, which was approved by Bioethical Committee;
• The study was performed during long time surgical resections with one-stage reconstruction;
Materials and Methods
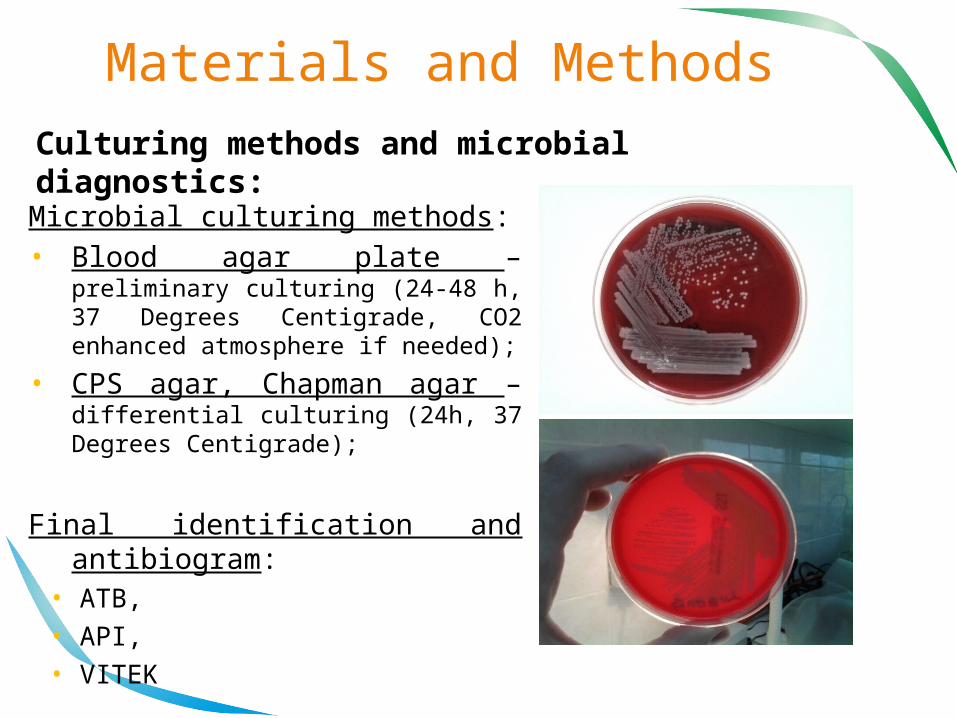
Microbial culturing methods:• Blood agar plate – preliminary
culturing (24-48 h, 37 Degrees Centigrade, CO2 enhanced atmosphere if needed);
• CPS agar, Chapman agar – differential culturing (24h, 37 Degrees Centigrade);
Final identification and antibiogram:
• ATB, • API, • VITEK
Culturing methods and microbial diagnostics:
Results:
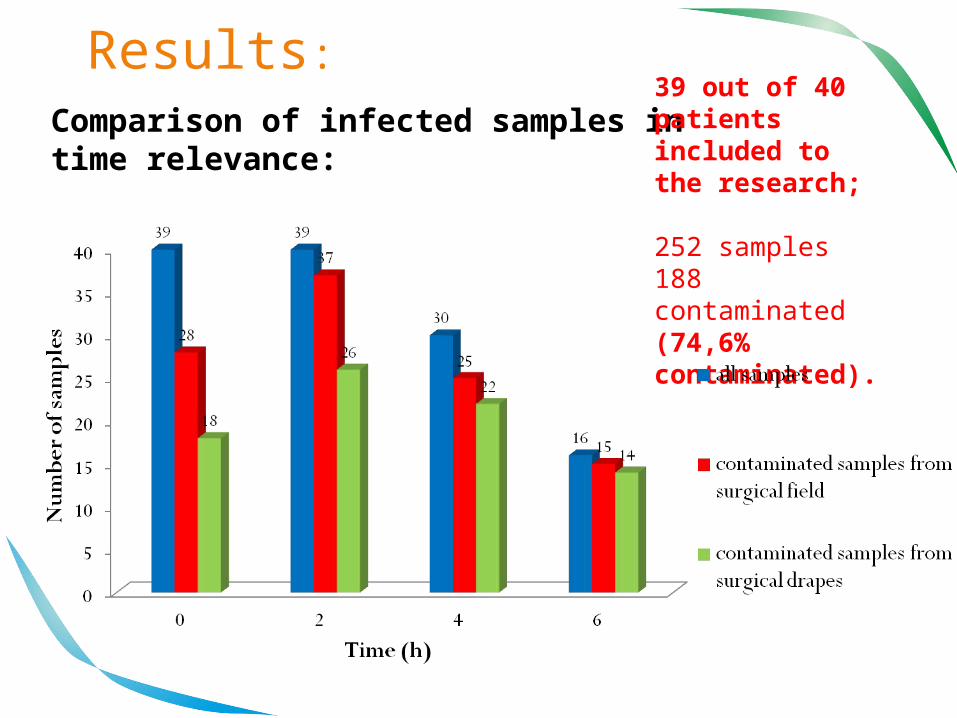
Comparison of infected samples in time relevance:
39 out of 40 patients included to the research;
252 samples188 contaminated(74,6% contaminated).
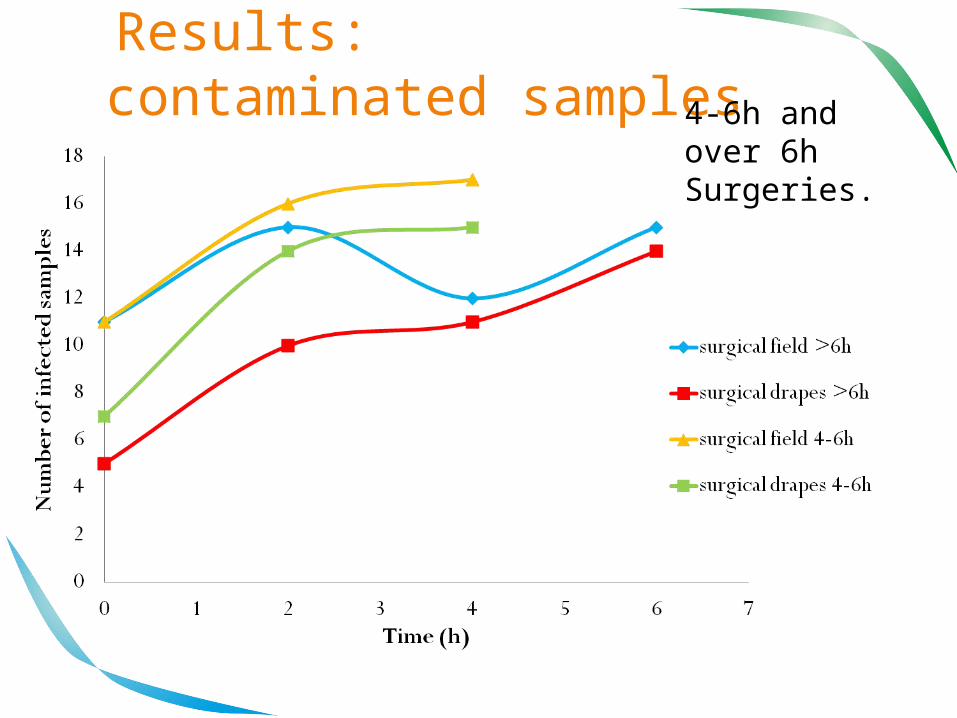
Results: contaminated samples 4-6h and
over 6hSurgeries.
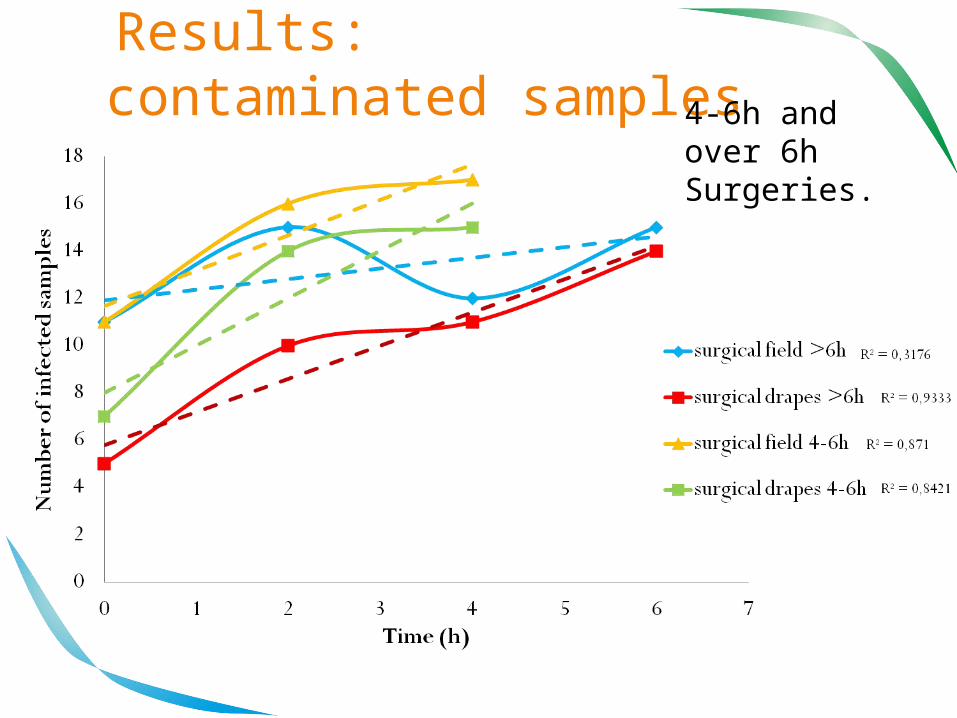
Results: contaminated samples 4-6h and
over 6hSurgeries.

Results: infected samples
Comparison of the most common pathogenes:
One sample could be infectedby more than one pathogeneThese pathogenes were the most popular outcome.

Results: antibiogram
Antibiotic Number of tested samples
Determinated resistancy
Amoxicillin and Clavulanic acid
22 1
Penicillin 11 0
Clindamicin 23 3
Vancomicin 16 0
Ciprofloxacin 20 1
Ceftriaxone 16 2
Tetracycline 19 7
Gentamicin 21 4

Results: complications
Complications after surgeries occured in 8 out of 40 cases (20%).
Conclusions: • The number of infected samples
from surgical field was not constantly increasing in time during surgeries;
• Peak of the contaminations was observed in 2nd hour, in timing of finishing tumour resection;
• Most common pathogenes were: Str. spp, Staph. Coagulasis(-) and Propionibacterium acnes;
• In spite of observing standard asepsis rules contamination of the surgical field occurs frequently.
