designing systems that keep clinicians on the same page
TRANSCRIPT

Joint Commission on Accreditation of Healthcare Organizations. Safety implementing health information and converging technologies. Sentinel Event Alert December 11, 2008. Available at: http//www.jointcommission.org/SentinelEvents/SentinelEventAlert/sea)42.htm, last visited December 23, 2008.
Stead, WW, Lin, HS, editors. Computational technology for effective health care: Immediate steps and strategic directions. Washington, DC: National Academies Press; 2009. Prepublication copy available at http://nlm.nih.gov/pubs/reports/comptech_prepub.pdf. Last visited February 7, 2009.

Paper & automated documentation & communication vary widely (vendor)– focus on DETAILS
– clinicians are not on the same page = errors
– formats change as patients and clinicians move across system
EHRs built to accommodate a single discipline –when care is provided by multidisciplinary teams who have both disciplinary and interdisciplinary responsibilities for care
Little testing done on EHRs to show that features actually work in support of the providers at the point of care
No agreement on how to implement standardized terminologies (SNOMED CT) to create comparability/interoperability

Continuity of information & information format on computer screens are needed to reduce errors at point of care
Focus on ensuring patient’s care team members all understand the big picture of care at the front line across all sites
Standardized language integrated/validated produce comparable data
Provide adequate testing to ensure features of EHRs bring value at the point of care

Plan of care (HANDS)
– (See next 2 screens current/historical)
– Updated at every handoff to include:• all clinical Issues (those identified by all members
of multidisciplinary team-MDs, RNs etc)
• Status of all outcomes of interest
• goals for all outcome ratings at discharge from unit
• Interventions completed in between each handoff


Systems with genuine “full interoperability” can
interact with one another about a specified domain of information because of being interconnected on4 levels:
1.Technical-conveyance of information 2.Semantic-persistence of meaning3.Format- consistency at user-interface4.Process-integration into workflow1
1HL7 EHR Interoperability Work Group. (February 7,2007).Coming to terms: Scoping interoperability for health care

The conveyance of information in a readily usable format. The more alike these factors are across systems the > the TI : – Data elements collected
– Terminologies used to populate the data elements
– Database architecture of relationships among data elements collected
– Software programs used to collect, transmit, display, store, and retrieve data

The persistence of meaning of information. The more alike these factors are across systems the > SI : – Purpose and value of an information set to those
who collect and use it in real time
– Type, consistency, and accuracy of the language/terminologies used to represent meaning and the format of it
– the means used to ensure and validate the reliability of information meaning

User interface (Computer Screen/s) is identical for a particular function (e.g.,Plan of Care) on all EHRs– Functionality offered is the same
– Information is displayed in the same way
– Information is entered in the same way
– Information is retrieved in the same way
– Same Information Is located in the same place
– Same words are used to present information (e.g., standardized terminologiesI

Integration of information into the workflow. The more alike these factors are across systems the > the PI:
– Enforcement of feasible rules governing the what, when, where, and how to document information
– Feasible rules for incorporating information into work flow to ensure appropriate use

An electronically supported approach (10 years of research) for creating & keeping care plans consistent, current, & useful
1. maintains standardization of documentation and communication of the plan of care
2. supports the interdisciplinary team to easily monitor patient problems, interventions, and progress toward outcomes
3. generates valid data for multiple uses, including effectiveness research
4. Interoperable on 4 levels: Technical, Semantic, Format, Process

Contains standardized terms that represent all types of (comprehensive) health care provided by multiple disciplines to children and adults across the continuum; (e.g., ER, ICU, acute, subacute, ambulatory, home care, long term care):– Clinical issues (problems, risk for problems,
prevention)
– Clinical outcome states & ratings
– Goal ratings for clinical outcomes
– Interventions / treatments

Training – demonstrate competency in HANDS Plan of Method (POC)
Document - an admission or update POC on each of clinician’s patients into HANDS (electronic tool )at every formal handoff
Communicate - use POC to structure care conversations at handoffs/interdisciplinary rounds (Use “SHARE” Process)

1. Standardized electronic tool
– ASP (Application Server Provider) deployed
– Can connect to any EHR – HL7 ADT
– Standardized architecture and user interface
– Standardized content (NANDA, NOC, NIC, ICD9)
– Central data repository
2. Standardized POC handoff process
– (SHARE)
3. Standardized training modules

Generate electronic interoperable team & nursing data across organizations (ANA)
Plan of care standard (Joint Commission)
Handoff safety goal (Joint Commission)
“to Implement a standardized approach to hand-off
communications, including an opportunity to ask and
respond to questions (2007).”
MU criteria for care coordination
contains major components of CCR & problem list
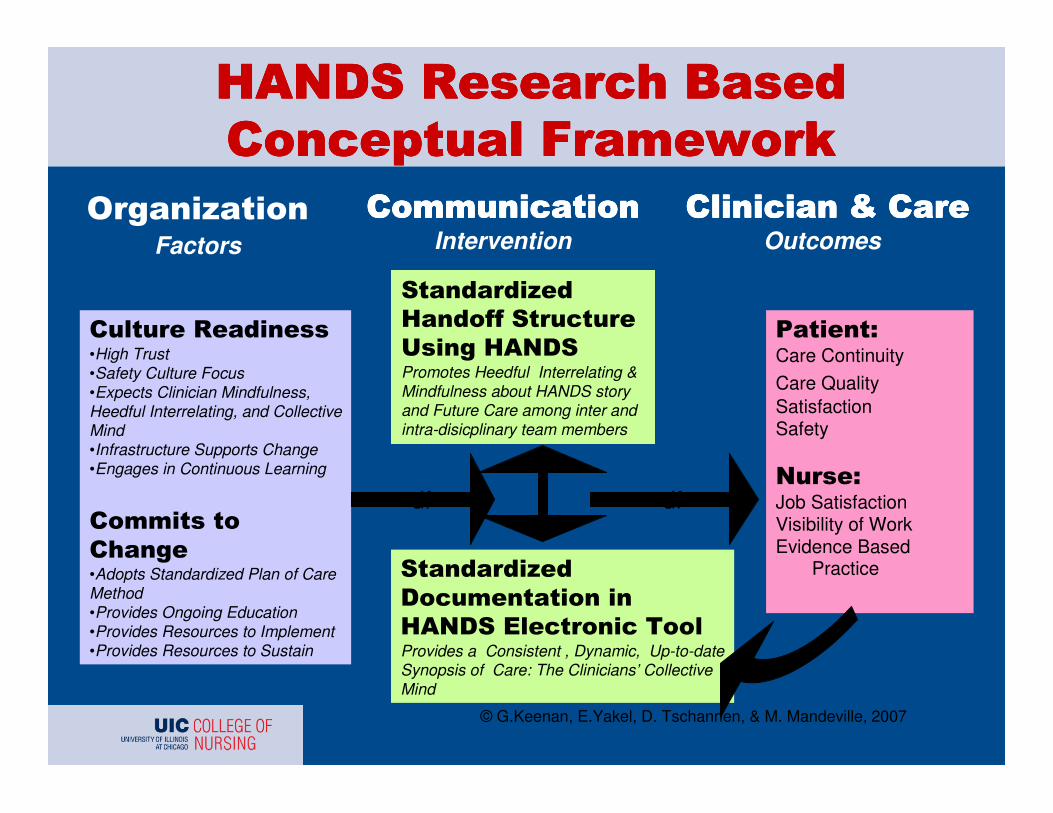
Factors
Intervention
Outcomes
•High Trust •Safety Culture Focus •Expects Clinician Mindfulness, Heedful Interrelating, and Collective Mind•Infrastructure Supports Change•Engages in Continuous Learning
•Adopts Standardized Plan of Care Method •Provides Ongoing Education•Provides Resources to Implement•Provides Resources to Sustain
Promotes Heedful Interrelating & Mindfulness about HANDS story and Future Care among inter and intra-disicplinary team members
Provides a Consistent , Dynamic, Up-to-date Synopsis of Care: The Clinicians’ Collective Mind
Care Continuity
Care QualitySatisfactionSafety
Job SatisfactionVisibility of WorkEvidence Based
Practice
© G.Keenan, E.Yakel, D. Tschannen, & M. Mandeville, 2007
df df

1998 – 2001 PI of subcontract for NINR funded study: “Evaluation of nursing sensitive patient outcomes” – home care/ambulatory/All
1998 – Created HANDS prototype single user application (tested in NINR study)
2002-2003 – Pilot of HANDS on 1 ICU
2004-2005 –Web-based HANDS created
2005-2008 – Multi-site study of HANDS funded by AHRQ: “HIT support for safe nursing care”

When data is interoperable on 4 levels –including at the “user interface” (looks the same e.g., same format, same terminology, same location) on the screens wherever the patient or clinician pull it up then it is reliable and valid and thus 1000s of reports can be generated. The following screens contain examples of reports generated with HANDS data.







Keenan, G, Tschannen, D, & Wesley, M. (2008). Standardized nursing terminologies can transform practice. JONA, 38 (3), 103-106.
Keenan, G., Yakel, E., & Tschannen, D., Mandeville, M. (2008). Documentation and the nurse care planning process. In R. Hughes (Ed) Patient safety and quality: An evidence based handbook for nurses. AHRQ Publication No. 08-0043), Agency for Healthcare Research and Quality, Rockville, MD., Chapter 49, http://www.ahrq.gov/qual/nurseshdbk/docs/KeenanG_DNCPP.pdf
Disclosure:
The HANDS software discussed in this presentation is owned and distributed by HealthTeam IQ, LLC. Dr. Gail Keenan is currently the President and CEO of this company and has a current conflict of interest statement of explanation and management in place with the University of Illinois Chicago.

Support Team
– Christine Anderson, MS, RN,– Elizabeth Brough, PhDc, RN– Brook Ayad, BSN, RN– Sally Decker, PhD, RN– Sharie Falan, MS, RN– Crystal Heath, MS, RN– Mary Killeen, PhD, RN– Deanna Marriott, PhD – Rachelle Ramos, BSN, RN– Santosh Udupi, MS– Julia Stocker, PhD, RN– Kathleen Sutcliffe, PhD, RN– Marcy Treder, BSN
Administrative Team Gail Keenan, PhD, RN, PI Beth Yakel, PhD, Co-PI Mary Mandeville, MBA, Director Dana Tschannen, PhD, RN, Field
Site Director Yvonne Ford, MS, RN Field Site
Director Laura Szalacha, PhD, Statistician
National Advisory Team Catherine Rick, RN, MS Marilyn Chow, RN, DNSc, Connie Delaney, PhD, RN Ada Sue Hinshaw, PhD, RN Joan Shaver, PhD, RN Judy Storfjell, PhD, RN