describe an operation – appendicectomy valerie see 29 th september 2014
TRANSCRIPT

DESCRIBE AN OPERATION – APPENDICECTOMYValerie See
29th September 2014

EMBRYOLOGY AND ANATOMYAppendix

Embryology• 8th week gestation• Narrow diverticulum of the caecal bud• Caecum descends from RUQ to RLQ with development of
lateral wall > medial wall• Appendix base lies at the posteromedial wall of the
caecumLangman’s Medical Embrology 9th Ed.

Anatomy• Blind-ending tube of variable length• True diverticulum of the caecum• Externally: Base identified by convergence of 3 taenia coli
-> longitudinal muscular layer• Surface anatomy: McBurney’s point = 1/3rd along the line
from R) ASIS to umbilicus• Appendix tip – variable
• Retrocaecal (or retrocolic) and intraperitoneal (most common)• Subcaecal, pre-ileal, post-ileal, pelvic• Retroperitoneal

• Mesoappendix – triangular fold of peritoneum• Contains appendicular a.
• Blood supply: appendicular a. – branch of posterior caecal a. – terminal branch of ileocolic a. (corresponding vv.)
• Lymphatic drainage: nodes assoc. with ileocolic a.
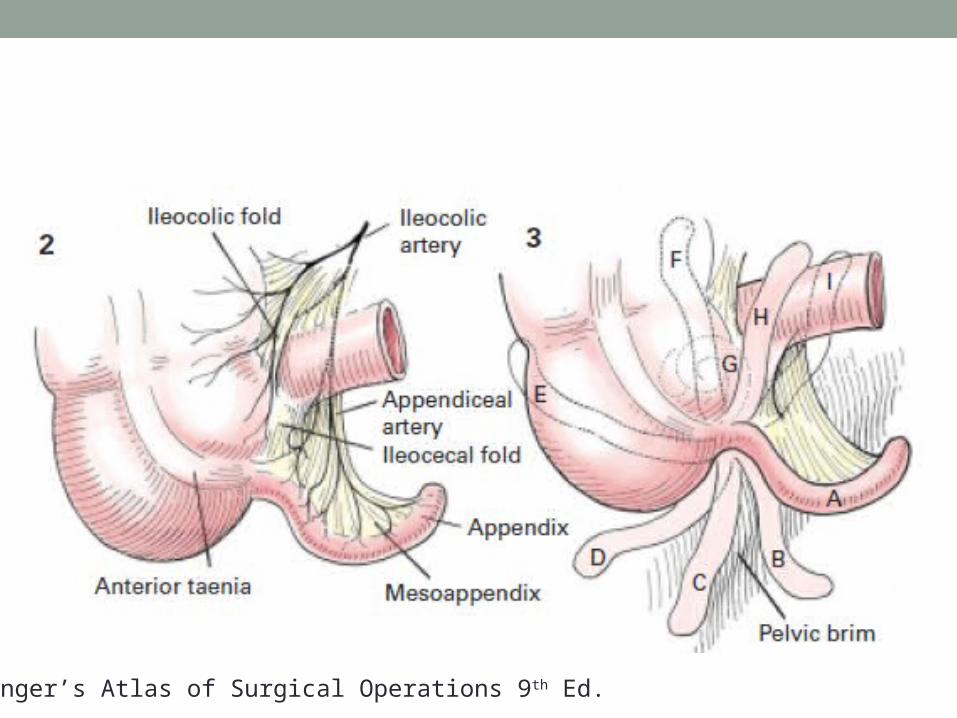
Zollinger’s Atlas of Surgical Operations 9th Ed.

APPENDICECTOMY

Acute Appendicitis• Appendicitis = inflammation of the vermiform appendix• Epidemiology
• Peak incidence between 2nd-3rd decade• Rare in infants
• Lifetime incidence in Male: female = 8.6: 6.7
• Pathogenesis• Aetiology ? Luminal obstruction• ↑ luminal and intramural pressure• Thrombosis and occlusion of small vessels with lymphatic stasis• Localised ischaemia and necrosis• Bacterial overgrowth

Pre-operative Preparation• IV fluids +/- IDC• IV antibiotics – gram negative bacilli and anaerobic cocci• Anti-pyrexials• DVT prophylaxis

LAPAROSCOPIC APPENDICECTOMY
Position and Preparation• Position
• Patient: Supine• Right arm extended• Left arm at patient’s side
• General anaesthesia with endotracheal intubation• Surgeon and assistant: Left side of patient• Equipment
• Laparoscopic tower – fibreoptic light cable, gas tubing – to head of table• Video monitor – across from operating team• Electrocautery and suction irrigator – toward foot of table
• Scrub nurse and Mayo instrument tray – toward foot of table
• Preparation• Empty bladder – Foley catheter• Abdomen is prepared with an appropriate anti-septic solution

Incision• 3 port insertion• Umbilicus (videoscope port)
• Vertical or transverse skin incision just above or below umbilicus• Open Hasson technique
• Pneumoperitoneum established• 2 x 5mm ports under direct vision (+/- infiltration with LA)
• Left lower quadrant• Midline suprapubic
• Patient is re-positioned• Trendelenberg’s position• Rotated right side up
• Diagnostic laparoscopy – 4 quadrant examination

Procedure• Visualisation of the appendix and its mesentry
• Conversion to open if unable to visualise the appendix, mesoappendix and base of the caecum
• Laparoscopic removal of the appendix• Appendix tip grasped with atraumatic forceps and lifted toward
abdominal wall• Window created in mesoappendix – dissecting forceps or
diathermy• Appendicular vessels coagulated or ligated using clip applicator
(endovascular linear stapler)• Appendix base cleared of surrounding tissue• Appendix base divided above absorbable loop ligature or using an
endoscopic cutting linear stapler

Closure• Ports are removed under vision• Abdomen decompressed and Hasson port removed
• Fascial defect closed with figure-of-eight sutures using 0 absorbable sutures
• Skin closed with subcuticular absorbable sutures

OPEN APPENDICECTOMY

Position and Preparation• Position
• Supine• General anaesthesia with endotracheal intubation
• Preparation• Abdomen is prepared with an appropriate anti-septic solution

Incision and Exposure• Tranvserse skin incision at McBurney’s point• External oblique fascia opened along line of fibres• Internal oblique and transversus adominis mm. fibres
identified and split• Peritoneum is grasped and a small incision made


Procedure• Caecum is delivered into the wound• Appendix identified and grasped with a Babcock clamp• Small window created in mesoappendix
• Vessels ligated
• Appendix base crushed with a clamp and ligated using 2-0 absorbable suture -> transected with a scalpel
• Appendiceal stump may be inverted using a purse-string suture

Closure• Peritoneum – 3-0 continuous absorbable suture• Transversus and internal oblique mm. – 2-0 absorbable
sutures• External oblique fascia – continuous 0-0 absorbable
suture• Skin – subcuticular suture or staples


Zollinger’s Atlas of Surgical Operations 9th Ed.