departmental memorandum - nm human … · departmental memorandum mad-mr: 13-07 date: to: ... (mad...
TRANSCRIPT

e-
DErARTMENT
Susana Martinez, Governor Sidonie Squier, Secretary
Julie B. Weinberg, Director
DEPARTMENTAL MEMORANDUM MAD-MR: 13-07 DATE:
TO: 0{ ISD AND MAD STAFF
FROM: t JULIE B. WEINBERG, DIRECTOR. MEDICAL ASSISTANCE DIVISION I~. TED ROTH, DIRECTOR, INCOME SUPPORT DIVISION
THROUGH: ~ ROY BURT, CHIEF, ELIGIBILITY BUREAU
BY: c8. SONY A PIERCE, STAFF MANAGER, ELIGIBILITY BUREAU
SUBJECT: ESTATE RECOVERY FORMS
GENERAL INFORMATION The Human Services Department has contracted with Health Management Systems (HMS) to conduct its Estate Recovery Program. The following forms will be sent out by HMS upon the death of the recipient that has received Long Term Care Medicaid benefits, who meets the Basis for defining the eligible group in Estate Recovery Policy found at NMAC, 8.200.420.13 B. The forms include: The Estate Recovery Brochure (MAD 237), Asset Identification Questionnaire Form (MAD 238), the New Mexico Estate Recovery Notice of Recovery (MAD 239), the New Mexico Estate Recovery Exception Approved (MAD 242), the New Mexico Estate Recovery Request for Update (MAD 243), the New Mexico Estate Recovery Satisfaction of Claim (MAD 244), the New Mexico Estate Recovery Request for Additional Information (MAD 245), the New Mexico Estate Recovery Exception Denied (MAD 246) and the Receipt of Claims Against the Estate (MAD 247) in English and Spanish regarding Estate Recovery.
FILING INSTRUCTIONS Please make the following replacements or additions in the Medical Assistance Forms Manual.
New MAD 237 Form: Estate Recovery Brochure in English dated May 01, 2013 .
Delete MAD 237 Form: Estate Recovery Brochure in English dated November 0 1, 20 I O.
New MAD 237 SP Form: Estate Recovery Brochure ~ Spanish dated May 01 , 2013 .
Delete MAD 237 SP Form: Estate Recovery Brochure in Spanish dated November 01,2010.
New MAD 238 Form: Estate Recovery Asset Identification Questionnaire Form in English dated May 01, 2013 .
Delete MAD 238 Form: Estate Recovery Asset Identification Form in English dated November 01, 2010.
New MAD 238 SP Form: Estate Recovery Asset Identification Questionnaire Form in Spanish dated May 01, 2013 .
Delete MAD 238 SP Form: Estate Recovery Asset Identification Questionnaire Form in Spanish dated November 01 , 2010.
MEDICAL AsSISTANCE DIVISION 1 PO BOX 2348 - SANTA FE, NM 875041 PHONE: (50S) 827-3103 FAX: (50S) 827-3185

New MAD 239 Form: Estate Recovery Notice of Recovery in English dated May 01, 2013.
Delete MAD 239 Form: Estate Recovery Application for Hardship Waiver Form dated November 01,2010.
New MAD 239 SP Form: Estate Recovery Notice of Recovery in Spanish dated May 01,2013.
Delete MAD 239 SP Form: Estate Recovery Application for Hardship Waiver Form in Spanish dated November 01,2010.
New MAD 242 Form: Estate Recovery Exception Approved dated May 01, 2013
New MAD 242 SP Form: Estate Recovery Exception Approved in Spanish dated May 01, 2013
New MAD 243 Form: Estate Recovery Request for Update dated May 01,2013.
New MAD 243 SP Form: Estate Recovery Request for Update in Spanish dated May 01, 2013
New MAD 244 Form: Estate Recovery Satisfaction of Claim dated May 01,2013.
New MAD 244 SP Form: Estate Recovery Satisfaction of Claim in Spanish dated May 01, 2013.
New MAD 245 Form: Estate Recovery Request for Additional Information dated May 01, 2013.
New MAD 245 SP Form: Estate Recovery Request for Additional Information in Spanish dated May 01, 2013.
New MAD 246 Form: Estate Recovery Exception Denied dated May 01, 2013.
New MAD 246 SP Form: Estate Recovery Exception Denied in Spanish dated May 01, 2013.
New MAD 247 Form: Receipt of Claims Against the Estate dated May 01, 2013.
New MAD 247 SP Form: Receipt of Claims Against the Estate in Spanish dated May 01, 2013.
Please address questions concerning this material to Sonya Pierce at [email protected] or at 505-827-7777.
INFORMATION:More information about Estate Recovery can be found on the internet or at a public library. The federal Medicaid Estate Recovery Law can be found at 42 U.S.C. § 1396p (b)(4)(A). Information on the state laws can be found in the New Mexico Statutes: the Medicaid Estate Recovery Law can be found in Chapter 27, Article 2A; and the Uniform Probate Code can be found in Chapter 45.
Federal law requires that the cost of long-term medical care be repaid from the
estates of certain Medicaid recipients.
This law is carried out in New Mexico through the Estate Recovery Program.
TERMS:
Medicaid Claim is a legal notice that the estate of the Medicaid recipient owes a debt to the govern-ment for the amount of money that was spent on behalf of the recipient for long-term medical care.Decedent means the person that died. Estate means the property that is left after someone dies. An estate can include homes, land, money, bank accounts, stocks, dividends, mineral rights, trusts, interests in a law suit, vehicles, boats, household items and any other belongings or property owned by the decedent.Estate Recovery is the process used to repay the government the cost of the long-term medical care from the Medicaid recipient’s estate. Heirs are the living family members (husband/wife, children, parents, brother(s)/sister(s) and/or grandparents) that are placed in line by law to receive the decedent’s property if there is no legal will. Personal Representative is the person that takes the legal action(s) required to hand out the property of the estate.Probate is the court process used to decide what will happen to the property of an estate.
MEDICAL CLAIMS:Upon the death of the Medicaid client, the recipient’s personal representative or heir may contact the HSD Estate Recovery Program to find out how much in Medicaid claimshad been paid out on behalf of the client. When making this request, the representative will need to provide the following information for the recipient: • Name • Social Security Number • Date of birth • Date of deathThe claim information will then be sent to the personal representative or attorney who is handling the affairs of the deceased.
The HSD Estate Recovery Program cannot provide legal advice so you should contact a lawyer if you have any special concerns or questions about Estate Recovery laws.
For more information, contact:
Mail: HMS NM ESTATES PO BOX 167767 IRVING, TX 75016-7767 Phone: 1- 855-212-0144 Fax: 1-855-285-3995 E-Mail: [email protected]
ESTATE RECOVERY PROGRAM
MAD 237 Revised 06/01/13

ESTATE RECOVERY:If you are fifty-five (55) years of age or older when you receive Medicaid services for long-term care, your estate (the property that is left after your death) will be used to pay the State of New Mexico back any money that was spent on your care. These costs can include: nursing home care, in home or community-based services, hospital expenses and prescription drugs.The Human Services Department (HSD) has contracted with Health Management Systems (HMS) to conduct its Estate Recovery Program Operations.
WHY:Federal law requires the State of New Mexico to seek repayment from certain Medicaid recipients because the state receives money from the federal government to help fund its Medicaid program. Since New Mexico also uses state tax dollars for the Medicaid program, state laws must be followed as well. These laws include the Medicaid Estate Recovery Act and the Uniform Probate Code.
WHEN:Estate Recovery only happens after a Medicaid recipient dies. It’s set up this way so that people can get the proper medical care they need without having to take out a loan or sell their belongings to pay for their medical services. Estate Recovery will not apply if the Medicaid client has a surviving spouse, a child that is blind or permanently disabled, or a surviving child that is under twenty-one (21) years old. The New Mexico Human Services Department (HSD) may also reduce or waive the Medicaid claim if a Qualified Hardship is identified. Some examples of Qualified Hardships are listed in this brochure.
HOW:After the client’s death, HSD files a Medicaid claim against the client’s estate for the amount of money that was spent on the recipient’s long-term medical care. If the Estate has a lot of claims filed against it for other debts, taxes or expenses, a court may help to decide which claims will be paid first. Modest funeral expenses and taxes are examples of claims that are usually paid first in New Mexico. The estate is then responsible to repay the debt owed to HSD.
An estate can be used to pay HSD back whether the Medicaid client wrote a will or not and even if the estate does not go through Probate. If there is not enough
money in the estate to cover the Medicaid claim, HSD does not waive its right, as permitted by the Uniform Probate Code, to recover the value of non-probate transfers such as properties transferred on death by deed.
QUALIFIED HARDSHIPS:Some Estates may qualify for relief from Estate Recovery, but only if HSD decides that one or more of the following hardship conditions are met:
• an heir would qualify for public benefits to meet food, clothing and shelter needs; • an heir would not be able to get off of public assistance if the Estate property is used for repayment; • an heir has no source of money other than what the Estate could provide; • the home in the Estate is worth 50% or less than the average price of homes in that county.
Any relief request must be submitted in writing to HSD by the client’s personal representative or heir(s). If HSD denies any part of the request, a Fair Hearing may be requested to review the decision.
No relief will be given if the hardship was caused by the recipient’s (or their representative’s) effort to avoid the legal responsibility to repay Medicaid.
MAD 237 Revised 06/01/13
INFORMACIÓN:Más información sobre Recuperación del Estado se puede encontrar en la Internet o en la biblioteca pública. La ley federal de Medicaid para Recuperación de Estado se puede encontrar en 42 U.S.C. § 1396p (b)(4)(A). Información sobre la leyes del Estado se puede encontrar en los Estatutos de Nuevo México: la ley de Medicaid para Recuperación de Estado se puede encontrar en el capítulo 27, artículo 2A; y Validación Legal del Código de Uniforme se puede encontrar en el capítulo 45.
La ley federal requiere que el costo de asistencia médica de largo plazo este compensado de los estados de ciertos
recipientes de Medicaid.
Esta ley se realiza en Nuevo México a través del Programa de La Recuperación del Estado.
TÉRMINOS:Reclamación de Medicaid es la notificación legal de que el Estado del recipiente de Medicaid tiene una deuda al gobierno por la cantidad de dinero que se gastó en nombre del recipiente por cuidado médico a largo plazo.Fallecido es la persona que ha muerto. Estado corresponde a la propiedad dejada después que alguien muere. Un Estado puede incluir casas, terrenos, dinero, cuentas de banco, acciones, dividendos, derechos de minas, fideicomisos, intereses en un juicio, vehículos, barcos, artefactos para el hogar, y cualquier otra pertenencia o propiedad del fallecido.Recuperación del Estado es el proceso utilizado para reembolsar al gobierno del Estado del recipiente de Medicaid por el costo de cuidados médicos a largo plazo. Herederos son los miembros sobrevivientes de la familia del fallecido (esposo/a, hijos/as, padres, hermanos/as y/o abuelos) que se consideran en línea por la ley para recibir la propiedad del fallecido si no hay testamento legal. Representante Personal es la persona que toma acción(es) legales requeridas para entregar la propiedad del Estado.Legalización de un Testamento es el proceso que la corte utiliza para decidir qué sucederá con la propiedad de un Estado.
DEMANDAS MÉDICAS:Sobre la muerte del cliente de Medicaid, el representante personal o el heredero se puede contactar con el Programa de Recuperación del Estado de HSD para descubrir cuanto son las demandas de Medicaid que se han pagado a nombre del cliente. Al hacer esta petición, el representante necesitara proveer la información siguiente para el recipiente: • Nombre • Número de Seguro Social • Fecha de nacimiento • Fecha de fallecimientoLa información de la demanda entonces será envíada al representante personal o el abo-gado que está manejando los asuntos del fallecido.
El Programa del la Recuperación del Estado de HSD no puede proveer aconsejo legal, así que usted debe contactar con un abogado si usted tiene cualquiera preocupaciones especiales o preguntas sobre leyes de la Recuperación del Estado.
Para más información, contacte:
Por Correo: HMS NM ESTATES PO BOX 167767 IRVING, TX 75016-7767 Por Teléfono: 1- 855-212-0144 Por Fax: 1-855-285-3995 E-Mail: [email protected]
Nuevo México Departamento de
Servicios Humanos
Programa de La Recuperación
del Estado
MADSP 237 Revised 06/01/13
RECUPERACIÓN DEL ESTADO:Si Ud. tiene cincuenta y cinco (55) años de edad o más cuando Ud. recibe servicios de Medicaid para cuidados médicos a largo plazo, su Estado (los bienes que Ud. haya dejado después de su muerte) será utilizado para reembolsar al estado de Nuevo México el dinero que ha gastado en su cuidado médico. Estos costos pueden incluir: cuidado en un hogar de ancianos, servicio en su hogar o servicios de la comunidad, costos de hospital y drogas de prescripción. El Departamento de Servicios Humanos (HSD) tiene un contrato con Health Systems Management (HMS) para llevar a cabo sus operaciones del Programa de Recuperación del Estado.
¿POR QUÉ?La ley federal requiere el estado de Nueve México que persiga el reembolso de ciertos recipientes de Medicaid porque el estado recibe dinero del gobierno federal para ayudar a financiar su programa de Medicaid. Nuevo México también utiliza dinero por impuestos para el programa de Medicaid, y las leyes del estado deben ser cumplidas también. Estas leyes incluyen el Acto de Medicaid para Recuperación de Estado y Validación Legal del Código de Uniforme (Uniform Probate Code).
¿CUÁNDO?La Recuperación de Estado sucede solamente después que el recipiente de Medicaid haya fallecido. Esta fijado de esta manera para que la gente pueda recibir los cuidados médicos que necesiten sin tener que pedir un préstamo o vender sus propiedades para pagar sus servicios médicos.
La Recuperación de Estado no se aplica si el cliente de Medicaid tiene sobreviviente un esposo/a, un hijo/a que es ciego(a) o permanentemente incapacitado, o menor de 21 años. El Departamento de Servicios Humanos (siglas en inglés HSD) también puede reducir o renunciar la reclamación de Medicaid si se identifica una dificultad calificada. Algunos ejemplos de dificultades calificadas se enumeran en este folleto.
¿COMO?Después que el recipiente haya fallecido, HSD presenta un reclamo de Medicaid en contra al Estado por la cantidad de dinero que se pago por el recipiente en cuidado médico a largo plazo. Si el Estado tiene muchas reclamaciones para otras deudas, impuestos o gastos, la corte puede ayudar a decidir cuáles reclamaciones se pagarían primero. Gastos modestos de funerales e impuestos son ejemplos de reclamaciones que se pagarían generalmente primero en Nuevo México. Entonces el Estado está responsable de reembolsar la cantidad debido a HSD.
Un Estado se puede usar para reembolsar a HSD, aunque el recipiente de Medicaid haya o no haya dejado un testamento de última voluntad y aunque el Estado no vaya a legalización de testamento.
Si no hay suficiente dinero en el Estado para cubrir las reclamación de Medicaid, HSD no renuncia el derecho, como lo permite Validación Legal del Código Uniforme, de recuperar el valor de transferencias que son incluidos en el legalización de testamento (tales como transferencia de propiedades después de muerte del difunto por medio de una escritura pública).
DIFICULTADES CALIFICADA: Algunos Estados pueden calificar por alivio de Recuper ación del Estado, pero solamente HSD puede decidir que una o más de las siguientes condiciones de dificultad se cumplen: • Un/a heredero/a califica para beneficios públicos para sus necesidades de alimentos, ropa y lugar para vivir; • Un/a heredero/a no puede dejar asistencia pública si la propiedad del Estado es utilizada para el reembolso; • Un/a heredero/a no tiene ninguna otra fuente de dinero, excepto el que es proporcionado por el Estado; • La casa en el Estado vale 50% o menos que el precio promedio de las casas en ese condado.Cualquier petición de alivio debe ser sometida por escritura a HSD por el Representante Personal o los herederos del cliente. Si HSD niega cualquier parte de la petición, una Audiencia Justa puede ser solicitada para revisar la decisiónNo se dará ningún alivio si la dificultad fue causada por el recipiente (o su representante) en un esfuerzo de evitar la responsabilidad legal de devolver el dinero a Medicaid.
MAD SP 237 Revised 06/01/13

!!! 'iiI )5-
H U MA N iii SERVICES DErARTMENT
MEDICAL ASSISTANCE DIVISION
ESTATE RECOVERY
ASSET IDENTIFICATION
Federal law requires that the cost of long-term medical care be repaid from the estates of certain
Medicaid recipients. This law is carried out through the New Mexico Estate Recovery Program. As a
result, the estate of any New Mexico Medicaid recipient over age 55, who received long-term care,
home and community based services through the Medicaid program is subject to recovery.
Instructions: • Provide all requested information and sign at the end of this form.
• Provide a copy of the deceased member's death certificate. (No exceptions; a copy must
accompany this questionnaire.) Provide copies of all additional documentation identified.
• Provide an address where information may be sent regarding this form.
Asset Identification form and documents can be either mailed to:
Or Faxed to: (855-285-3995)
Or E-mail to:[email protected]
NM Estates Program
P.O. Box 167767
Irving, TX 75016-7767
If you have any questions about how to complete this form, please call toll-free (855) 212-0144
Person Completing this form:
Name: Address:
Telephone: "- -
0 Personal Representative 0 Attorney for Estate Please Check all that apply:
0 Other: c>· J 0
[' r~' ~]"
Has there been (or do you anticipate) any lawsuits filed on behalf of the estate? DYes DNo
If YES provide: Case or File number: Date Filed:
County Court: ~' ''IT'. . .... , . .' ~ ~ ~ ~
Has a petition for probate of the estate been filed? DYes DNo
If YES provide: Case or File number: Date Filed:
MAD 238 Issued 05/01/13
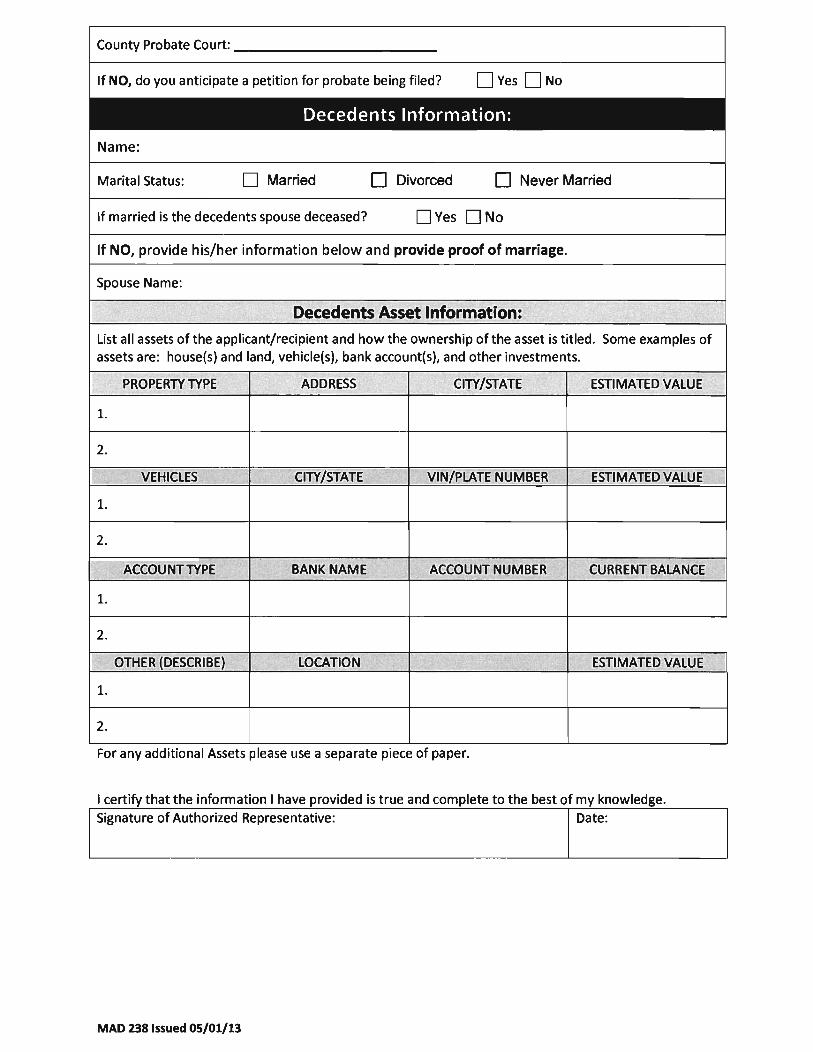
County Probate Court: ___________ _
If NO, do you anticipate a petition for probate being filed? DYes DNo I
Decedents Information:
Name:
Marital Status: D Married D Divorced D Never Married
If married is the decedents spouse deceased? DYes DNo
If NO, provide his/her information below and provide proof of marriage.
Spouse Name:
Decedents Asset Information:
List all assets of the applicant/recipient and how the ownership ofthe asset is titled. Some examples of assets are: house{s) and land, vehicle{s), bank account{s), and other investments.
PROPERlY TYPE ADDRESS CITY/STATE ESTIMATED VALUE
1.
2.
VEHICLES CITY/STATE VIN/PLATE NUMBER ESTIMATED VALUE
l.
2.
ACCOUNT TYPE BANK NAME ACCOUNT NUMBER CURRENT BALANCE
1.
2.
OTHER (DESCRIBE) LOCATION '~ "TT. ESTIMATED VALUE
l.
2.
For any additional Assets please use a separate piece of paper.
I certify that the information I have provided is true and complete to the best of my knowledge.
Signature of Authorized Representative: Date:
MAD 238 Issued 05/01/13

!!t e ( lE-
HUMAN iff SERVICES DEPARTMENT
MEDICAL ASSISTANCE DIVISION
RECUPERACI6N DE PATRIMONIO
IDENTIFICACI6N DE ACTIVOS
La ley federal requiere que el costa de la atenci6n medica a largo plazo se pagarfa con los bienes de
alguno de los beneficiarios de Medicaid. Esta ley se lIeva a cabo a traves del Programa de Recuperaci6n
de New Mexico. Como resultado, el estado de cualquier New Mexico Medicaid receptor mayor de 55
anos, quien recibi6 la atenci6n a largo plazo, el hogar y los servicios basados en la comunidad a traves
del programa Medicaid esta sujeta a la recuperaci6n.
Instrucciones:
• Proporcionar toda la informaci6n solicitada y firmar al final de este formulario.
• Proporcionar una copia del certificado de defunci6n del miembro fallecido. (Sin excepciones, una
copia debe acompanar a este cuestionario.) Proporcione copias de toda la documentaci6n adicional
identificada.
• Proporcionar una direccion donde se puede enviar informacion acerca de este formula rio.
Esta forma y los documentos pueden ser enviados por correo a cualquiera de las tres:
o por fax al: (855-285-3995)
NM Estates Program
P.O. Box 167767
Irving, TX 75016-7767
o por correo electronico a: [email protected]
Si usted tiene alguna pregunta sobre como completar este formulario, por favor lIame al (855) 212-0144
Persona que Completa este Formulario:
Nombre: Direccion:
Telefono:
" ~ -~-
Por favor, marque todas las que o Representante Personal o Abogado de Bienes
correspondan: o Otro: u . ,",
~ .~ cf'"
lHa habido (0 anticipa usted) las demandas presentadas en nombre de los bienes? OSi ONo
En caso afirmativo proporcionar: Caso 0 numero de Fecha de archivos: Radicacion:
Corte del Condado:
'" r " ~
lHa presentado una solicitud de legalizacion de la propiedad? OSiONo
MAD 238 SP Issued 05/01/13
En caso afirmativo proporcionar: Caso 0 numero de archivos:
Corte del Condado de Sucesiones: __________ _
En caso negativo, lse anticipa una presentaci6n de petici6n de legalizaci6n?
Informacion del Difunto:
Nombre:
Fecha de Radicaci6n:
DSi DNo
Estado Civil: D Casado D Divorciado D Nunca se ha casado
lSi esta casado es el c6nyuge del difunto fallecido? DSi DNo
En caso negativo, proporcione su informacion abajo y proporcione la prueba del matrimonio.
Nombre del c6nyuge:
~
Difunto Informaci6n dOe Activos:
lista todos los activos del solicitante/beneficiario y como la propiedad del activo se titula. Algunos ejemplos de activos son: casa(s) y de la tierra, vehiculo(s), cuenta bancaria(s), y otras inversiones.
TIPO DE PROPIEDAD DIRECCI6N CIUDAD/ESTADO VALOR ESTIMADO
1.
2.
VEHfcULOS CIUDAD/ESTADO VIN/MATRfCULA VALOR ESTIMADO
1.
2.
TIPO DE CUENTA NOMBRE DEL BANCO NUMERO DE CUENTA BALANCE ACTUAL
1.
2.
OTRO (DESCRIBIR) .1 UBICACI6N .; ~ !' !. , VALOR ESTIMADO ~.
"
1.
2.
Para cualquier Activos adicionales por favor use una hoja de papel
Certifico que la informaci6n que he proporcionado es verdadera y completa a mi mejor entender.
Firma del Representante Autorizado: Fecha:
MAD 238 SP Issued 05/01/13

!l! -:r ):lt
H U MA N 111 SERVICES D l r " II.. I M £ N T
MEDICAL ASSISTANCE DIVISION
hms
« Contact First Name Last Name» « Org Name» « Contact Address 1» « Contact Address2» « Contact City, State ZIP»
NEW MEXICO ESTATE RECOVERY
NOTICE OF RECOVERY
RE: Estate of « Recipient First Name Last Name» Medicaid ID#: « MID» Date of Death: « DOD»
Dear « Contact First Name Last Name»:
'OR OFJIICIAL USE ONLY
CASE NAME «Recipient First Name Last Name»
MEDICAID 10 NUMBER «MA NUM»
ESTATE CASE 10 NUMBER «CaseID»
NOTICE SENT «Notice Sent Date (Date input box)>>
« DATE»
This letter is to notify you that Health Management Systems (HMS), on behalf of the New Mexico Human Services Department (HSD) intends to seek recovery from the estate of «Recipient First Name Last Name»for the amount of medical assistance paid on behalf of «Recipient First Name Last Name». HSD is the State Agency authorized to provide Medicaid services. HSD contracts with HMS to conduct its Estate Recovery Program. The claim against the estate is «Total Lien» for the period «Service From Date» through «Service To Date».
The Social Security Act (42 V.S.c. 1396p) and State law NMSA § 27-2A-I et seq., require HSD to recover Medicaid expenditures paid by HSD for clients who were 55 years and older and are now deceased. The HSD claim against the estate includes payments for:
• Nursing Facility services, • Home and Community Based services, and • Related hospital and prescription drug services
We have enclosed a copy of the HSD Long Term Care Payment History for the client listing the expenditures subject to recovery.
* «CONTEXT_CD» * *«CASE_ID»* *«DOcTypecode»* «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com

Exceptions
HSD may defer, waive, or reduce its claim against the estate if one of the following exceptions below exists:
• Estate Claim Statutory Exemption • Undue Hardship Waiver • Partial Recovery
If you believe that one of these exceptions may apply, please refer to the Application for that Exception included with this notice. You are additionally directed to inform the heirs that they may also apply for a . Exception. The Application will provide further information on how to request a deferral, waiver, or reduction of the estate claim and the supporting documentation that must be provided. The Application must be received in our office within 30 days from the date of this notice.
Administrative Hearing Rigbts
Rigbt to a bearing: The human services department (HSD) must grant an opportunity for an administrative hearing.
A. When a recipient requests an administrative hearing because he believes that HSD has taken an action erroneously.
B. When services of a medicaid recipient are terminated, modified, reduced, suspended, or denied.
Time limits: A medicaid recipient has 90 days from the date of notice of action to request a fair hearing. To be considered timely, the request must be received by the HSD hearings bureau, the local ISD office, or MAD no later than the close of business on the 90th day. In order to receive continuation of benefits while the hearing process goes forward, the request must be received by HSD (including the HSD hearings bureau, the local ISD office, or the medical assistance division) no later than the close of business on the 13th day. Hearings are conducted and a written decision is issued by the medical assistance division director or designee to the recipient within 90 days from the date that HSD receives the hearing request.
Contact: Human Services Department, Hearings Bureau P.O. Box 2348 Santa Fe, NM 87504 1-800-432-6217
Acknowledgement
Please acknowledge receipt of this letter within 30 days of the date of this notice by completing the enclosed receipt form and returning it to us in the enclosed business reply envelope.
If you have any questions please do not hesitate to call me at the toll free number listed below.
Sincerely, «Electronic Signature» «Caseworker» HMS Caseworker
MAD 239 Issued 05/13 <Project Address» I «Project City. State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com

Enclosures: Receipt form HSD Long Term Care Payment History Applications for Estate Claim Statutory Exemption, Undue Hardship Waiver, or Partial Reduction Copy of the Court Claim Against the Estate (if filed)
MAD 239 Issued 05/13 <Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com

I. Application For Statutory Exemption
Recovery from the a recipient's estate will be made only after the death of the recipient's surviving spouse, if any, and only at a time that the recipient does not have surviving child(ren) who are less than 21 years of age or blind or who meet the social security administration's definition of disability.
HSD will defer its claim against the estate when the HSD client is survived by a surviving spouse, a surviving child under age 21, or a surviving child of any age who is blind or disabled and receives SS! or SSA disability benefits. Ifthe HSD client is survived by any of these individuals, check the appropriate boxes below and attach supporting documentation.
I am attaching documentation which verifies that the HSD client is survived by one of the following individuals (please check all that apply):
o o o
o
o
o
~ --L. ________ ~ _ __"" _____ _L. __ ~ Spouse;
Child under the age of21; or
Child of any age who is blind or disabled and receives Social Security Administration (SSA) disability benefits or Supplemental Security Income (SSI) disability benefits.
AFFIRMATION
I have attached, or have already provided to HMS a copy of the marriage license and a copy of the HSD client's death certificate.
I have attached, or have already provided to HMS a birth certificate or other legal document that verifies the child's age and tlie child's relationship to the HSD client.
I have attached, or have already provided to HMS a birth certificate or other legal document that verifies the child's relationship to the HSD client, and a copy of the child's SSA/SSI disability benefit award letter from the Social Security Administration which verifies the child receives SSA or SSI disability benefits.
By signing below I certify that the information I have provided for an Estate Claim Statutory Exemption is true and correct.
/ / Signature of Authorized Representative (Date)
Telephone Number
Address (Street, City, State, Zip Code)
MAD 239 Issued 05/13 <Project Address» I «Project City. State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com

II. Application for Undue Hardship HSD or its designee may waive recovery because recovery would work an undue hardship on the heirs: The following are deemed to be causes for hardship:
-
-
--
1. Without the receipt of the proceeds of the estate, the heir(s) would become eligible for a needs-based assistance program (such as Medicaid or temporary assistance to needy families (TANF» DYES D NO
2. Without the receipt of the proceeds of the estate, the heir(s) would be put at risk of serious deprivation.
3. Heir(s) would be able to discontinue reliance on a needs-based assistance program (such as Medicaid or temporary assistance to needy families (TANF) if he/she received the inheritance from the estate.
4. The assets subject to recovery are the sole income source for the heir(s).
5. The homestead is worth 50 percent or less than the average (median) price of a home in the county where the home is located based on census data compared to the property tax value of the home.
DYES DNO
DYES DNO
DYES DNO
DYES DNO
If you answered YES to any of these questions, you must provide all of the documents listed below to verify your responses.
D
D
I have enclosed a copy of the County Assessor's Statement or an official document from the New Mexico State Department of Revenue that verifies the HSD client's real property is residential property.
-
I have enclosed a copy of my most recent Federal income tax return and verification of all gross income received by my household ..
You may qualify for an Undue Hardship based on your responses to QJlestions 6 through 9 below.
6. Do you currently reside at the HSD client's residence? DYES DNO
DYES DNO -
--
7. Did you reside at the HSD client's residence at the time of the client's death?
8. Is the HSD client's residence also your primary residence for the 12 months immediately preceding the HSD client's death?
9. Do you own a residence? . " .. ,
DYES DNO
DYES DNO
If you answered YES to Questions 6 through 8, and NO to Question 9, you must provide all ofthe documentation listed below to verify your responses
D
D
D
I have attached verification which establishes that I resided continuously at the residential property for the 12 month period immediately preceding the HSD client's death
I have attached verification which establishes that I resided at the residential property at the time of the HSD client's death, and I have attached verification which establishes that I currently reside at the residential property. Acceptable verification includes utility or other statements, pay stubs, vehicle registration, etc.
MAD 239 Issued 05/13 <Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com
Personal Property Estate Assets Only: I. , r
1. Does the estate contain only Personal Property assets and no residence? DYES DNO 1""-
2. Does your household's gross annual income, which includes new sources of income, exceed the DYES DNO Federal Annual Income Poverty Guidelines?
1.--3. Do you own a home, land, or other real property? , DYES DNO
If you answered YES to Question 1, and NO to Questions 2 and 3, you must provide all of the documentation listed below to support your responses.
D I have attached a copy of my most recent Federal income tax return and verification of my household's gross annual income; including new sources of income my household expects to receive.
AFFIRMATION
0 I have attached, or have already provided to HMS a copy of the Inventory of the HSD client's estate. ~
I have attached, or already provided to HMS a copy of the HSD client's last will to verify that I am an heir to the D HSD client's estate.
-The HSD client died intestate (without a Will). I have attached legal documents to verify that I am a descendant to
0 - the HSD client. If I am not a descendant to the HSD client, I have attached an "Affidavit of Heirship" which verifies that I am a legal heir to the HSD client's estate.
By signing below, I certify that the information I have provided for an Undue Hardship Waiver of Estate Claim is true and correct.
/ / -- ----Signature of Authorized Representative (Date)
Telephone Number
Address (Street, City, State, Zip Code)
MAD 239 Issued 05/13 <Project Address» I «Project City. State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free:-> I www.hms.com
III. Application for Partial Reduction
If you wish to apply for consideration of a Partial Reduction of the Estate Claim, please answer all of the following questions and provide supporting documentation to verify your responses.
1. Will enforcement of the full amount of the HSO claim against the HSD client's estate create DYES DNO a financial hardship to you and your household?
If YES, please explain how enforcement of the full amount of the HSO claim will cause you and your household a fmancial hardship, and provide documentation that supports how your household will experience a fmancial hardship if the full
amount of the HSO claim is enforced. ':'
, . "
" '" ." "
-~. p
2. Will enforcement of the HSO claim against the HSO client's estate create a medical hardship to DYES DNO you and your household?
If YES, please explain how enforcement of the full amount of the HSO claim will cause you or your household a medical hardship and provide documentation that supports how your household will experience a medical hardship if the full
amount of the HSO claim is enforced.
1-
3. What is the total number of persons living in your household (include yourselt)? '" ~
4. Does your household's gross annual income exceed the Federal Income Poverty Guidelines for DYES DNO your household size?
~
S. What is the total fair market value of your household's real and personal property assets, including any " encumbr.ances? $ . Attach verification which verifies the fair market value of all sources of real and
personal property assets that are owned by you and your household.
6. Are there any other creditors who have a claim against the HSO client's estate? DYES DNO
If YES, list the names ofthe creditor(s) and the amount of the creditor's claim.
;: 7. Have any of the creditors that you listed in Question 6 above, foreclosed on the real or personal DYES DNO property in the HSO client's estate?
.-
8. Are there any other factors you would like HSO to take into consideration? If so, please provide an explanation of
the factors you would like considered and attach supporting documentation.
MAD 239 Issued 05113 <Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com

AFFIRMATION
D I have attached, or have already provided to HMS a copy of the Inventory of the HSD client's estate.
D I have attached, or already provided to HMS a copy of the HSD client's last will to verify that I am an heir to the HSD client's estate. The HSD client died intestate (without a Will). I have attached legal documents to verify that I am a descendant to the
D HSD client. IfI am not a descendant to the HSD client, I have attached an "Affidavit of Heirship" which verifies that I am a legal heir to the HSD client's estate.
By signing below I certify that the information I have provided for a Partial Recovery of the Estate Claim is true and correct.
/ / Signature of Authorized Representative (Date)
Telephone Number
Address (Street, City, State, Zip Code)
MAD 239 Issued 05/13 <Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com

ill =- )-:' H UMAN ' SERVICES
D E P ARTMENT MEDICAL ASSISTANCE DIVI SION
hms RECUPERACION DE PATRIMONIO DE NUEVO MEXICO
NOTIFICACION DE RECUPERACION
« Contact First Name Last Name» « Org Name» « Contact Addressl» «Contact Address2» «Contact City, State ZIP»
RE: Patrimonio de « Recipient First Name Last Name» N.o de INDV del miembro: « INDV» Fecha de fallecimiento: « DOD»
Estimado/a «Contact First Name Last Name»:
« DATE»
Esta carta es para notificarle que Health Management Systems (HMS), en nombre del Departamento de Servicios Humanos (HSD) de Nuevo Mexico tiene la intenci6n de recuperar del patrimonio de «Recipient First Name Last Name» los montos por asistencia medica pagados a nombre de «Recipient First Name Last Name». HSD es la Agencia estatal autorizada para proporcionar servicios de Medicaid. HSD contrata a HMS para llevar a cabo su Programa de recuperaci6n de patrimonio. EI reclamo contra el patrimonio es «Total Lien» por el periodo del «Service From Date» hasta el «Service To Date».
La Ley de Seguridad Social (42 U.S.C. 1396p) Y la ley estatal NMSA § 27-2A-I Y subsiguientes requieren que HSD recupere los gastos de Medicaid que HSD pag6 por los clientes que tenian 55 afios 0
mas y ya fallecieron. EI reclamo de HSD contra el patrimonio incluye los pagos para:
• Servicios en un centro de enfermeria, • Servicios basados en el hogar y la comunidad y • Servicios relacionados con los medicamentos con receta medica y servicios de hospital
Hemos adjuntado una copia del Historial de pago de atenci6n a largo plazo de HSD para el cliente, que enumera los gastos sujetos a recuperaci6n.
MAD 239 SP Issued 5/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com

Excepciones
HSD puede aplazar, eximir 0 reducir su reclamo contra el patrimonio si se presenta una de las excepciones que aparecen a continuaci6n:
• Exenci6n legal del reclamo del patrimonio • Exenci6n por dificultad econ6mica • Recuperaci6n parcial
Si cree que puede aplicar una de estas excepciones, consulte la Solicitud para esa excepci6n que se incluye con esta notificaci6n. Adicionalmente se Ie indica que debe informar a los herederos que tambien ellos pueden solicitar una Excepci6n. La Solicitud Ie proporcionara informaci6n adicional sobre c6mo solicitar un aplazarniento, exenci6n 0 reducci6n del reclamo del patrimonio y la documentaci6n de apoyo que debe proporcionar. La Solicitud debe recibirse en nuestra oficina en un plazo de 30 dias a partir de la fecha de esta notificaci6n.
Derechos de audiencia administrativa
Derecho a una audiencia: el Departamento de Servicios Humanos (HSD) debe conceder una oportunidad para una audiencia administrativa segun se describe en esta secci6n y en las siguientes circunstancias. A. Cuando un destinatario solicita una audiencia administrativa porque cree que HSD tom6 una acci6n incorrecta.
B. Cuando se terminan, modifican, reducen, suspenden 0 deniegan los servicios de un destinatario de Medicaid.
Limites de tiempo: un destinatario de Medicaid tiene 90 dias a partir de la fecha de la notificaci6n de acci6n para solicitar una audiencia justa. Para que se considere oportuna, la oficina de audiencias de HSD, la oficina local de ISD 0 MAD debe recibir la solicitud a mas tardar el dia 90, al finalizar el dia laboral. Para continuar recibiendo los beneficios mientras el proceso de audiencia avanza, HSD (incluye la oficina de audiencias de HSD, la oficina local de ISD 0 la division de asistencia medica) debe recibir la solicitud a mas tardar el dia 13, al finalizar el dia laboral. Se llevan a cabo las audiencias y el director de la divisi6n de asistencia medica 0 la persona designada emite al destinatario una decisi6n por escrito, en un periodo de 90 dias, a partir de la fecha en que HSD recibe la solicitud de la audiencia.
Contacto: Human Services Department, Hearings Bureau (Departamento de Servicios Humanos, Oficina de Audiencias) P.O. Box 2348 Santa Fe, NM 87504 1-800-432-6217
Reconocimiento
Debe acusar recibo de esta carta en un periodo de 30 dias a partir de la fecha de esta notificaci6n al completar el formulario de recibo adjunto y devolvernoslo en el sobre de respuesta comercial adjunto.
Si tiene alguna pregunta, no dude en comunicarse conmigo al numero de telefono gratuito que se indica a continuaci6n.
Atentamente,
MAD 239 SP Issued 5/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com
«Electronic Signature» «Caseworker» Especialista de Recuperaci6n
Anexos: Formulario de recibo Historial de pago de atenci6n a largo plazo de HSO Solicitudes para la Exenci6n legal del reclamo del patrimonio, Exenci6n por dificultad econ6mica 0
Reducci6n parcial Copia del Reclamo del tribunal contra el patrimonio (si se presento)
MAD 239 SP Issued 5/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com
I. Solicitud para exencion legal
La recuperaci6n del patrimonio de un beneficiario se llevara a cabo unicamente despues de la muerte del c6nyuge sobreviviente del destinatario, si hay alguno, y solo cuando el destinatario no tenga hijos sobrevivientes que sean menores de 21 afios, que sean ciegos 0 que cumplan con la definici6n de discapacidad de la Administraci6n del Seguro Social.
HSD aplazani su reclamo contra el patrimonio cuando al cliente de HSD Ie sobreviva un c6nyuge, un hijo menor de 21 afios 0 un hijo de cualquier edad que este ciego 0 discapacitado y reciba los beneficios por discapacidad de SSI 0 SSA. Si al cliente de HSD Ie sobrevive cualquiera de estas personas, marque las casillas apropiadas a continuaci6n y adjunte documentaci6n de apoyo.
Estoy adjuntando documentacion que verifica que al cliente de HSD Ie sob revive una de las siguientes personas (mar9ue 10 que corresponda): .-D C6nyuge;
D
D
D
D
D
Hijo menor de 21 afios, 0
Hijo de cualquier edad que es ciego 0 discapacitado y recibe los beneficios por discapacidad de la Administraci6n del Seguro Social (SSA) 0 Seguridad de Ingreso Suplementario (SS1).
AFIRMACION
He adjuntado 0 ya proporcione a HMS una copia de la licencia de matrimonio y una copia del certificado de defunci6n del cliente de HSD. He adjuntado 0 ya proporcione a HMS un certificado de nacimiento u otro documento legal que verifica la edad del menor y el parentesco del menor con el cliente de HSD. He adjuntado 0 ya proporcione a HMS un certificado de nacimiento u otro documento legal que veri fica el parentesco del menor con el cliente de HSD y una copia de la carta de concebimiento de beneficios por discapacidad de SSAISSI del menor por parte de la Administraci6n del Seguro Social, que verifica que el menor recibe beneficiospor discapacidad de SSA 0 SSl.
Al frrmar abajo certifico que la infonnaci6n que proporcione para una Exenci6n legal de reclamo del patrimonio es verdadera y correcta.
/ / Finna del representante autorizado (Fecha)
Numero de telefono
Direcci6n (calle, ciudad, estado, c6digo postal)
MAD 239 SP Issued 5/13 «Project Address» I «Project City. State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com

II. Solicitud or dificultad economica HSD 0 su designado puede renunciar a la recuperacion ya que la recuperacion podria significar una dificultad economica para los herederos. Las siguientes se consideran como causas de la dificultad economica: 1.
2.
3.
4.
5.
Al no recibir de 'los ingresos que corresponden al patrimonio, los herederos serlan elegibles para un programa de asistencia basado en necesidades (como 0 ' 0 Medicaid 0 Asistencia Temporal para Familias Necesitadas (TANF, por sus S1 NO siglas en ingles», Si no reciben los ingresos que corresponden al patrimonio, los herederos D SI D NO podrian estar en riesgo de privaci6n ~ve. Los herederos podrian dejar de depender de un program a de asistencia basado en las necesidades (tal como Medicaid 0 asistencia temporal para 0 si 0 NO familias necesitadas (TANF) si reciben la hetencia del patrimonio. Los activos sujetos a la recuperaci6n son la unica fuente de ingresos para los D si 0 NO herederos. La propiedad vale 50 por ciento 0 menos del precio promedio (medio) de una casa en el condado donde esta ubicada, con base en los datos de censo 0 sf 0 NO com arados con el valor fiscal de la ro iedad.
Si la respuesta es sl a cualquiera de estas preguntas, debe proporcionar todos los documentos que se enumeran abajo para verificar sus respuestas.
o o
He adjuntado una copia de la r>eclaraci6n del asesor del condado 0 un documento oficial del Departamento de Ingresos del estado de Nuevo Mexico que verifica que el bien inmueble del cliente de HSD es propiedad residencial. He adjuntado una copia de mi declaraci6n federal de impuestos sobre la renta mas reciente y verificaci6n de todos los in esos brutos ue recibe mi 0 familiar.
Es posible que califique para una Dificultad economica con base en sus respuestas de las preguntas 6 a 9 a continuacion.
6. "Vive actualmente en la residencia del cliente de HSD? 0 si 0 NO
7. "Vivia en la residencia del cliente de HSD en el momenta su muerte? 0 si 0 NO
8. "La residencia del cliente de HSD era tambien su residencia principal durante 0 si 0 NO los 12 meses inmediatamente anteriores a la muerte del cliente de HSD?
9. "Posee una residencia propia? 0 sf 0 NO
Si las respuestas son sl a las preguntas 6 a 8 y NO a la pregunta 9, debe proporcionar toda la documentacion que se enumera a continuacion para verificar sus respuestas
D
o
o
He adjuntado la verificaci6n que establece que vivi continuamente en la propiedad residencial durante el periodo de 12 meses inmediatamente anteriores a la muerte del cliente de HSD
He adjuntado la verificaci6n que establece que vivi en la propiedad residencial en el momenta de la muerte del cliente de HSD, y
He adjuntado la verificaci6n que establece que actualmente resido en la propiedad residencial. La verificaci6n aceptable incluye facturas de servicios publicos u otros estados de cuenta, recibos de pago, registro de vehiculo, etc.
MAD 239 SP Issued 5/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com

Solo bienes muebles:
1. l.Contiene el patrimonio solo bienes muebles y no residenciales? Dsi DNO .--~.
2. l.Supera el ingreso anual bruto de su grupo familiar, que incluye nuevas fuentes de ingresos, las Directrices federales de pobreza segUn los ingresos Dsi DNO anuales?
3. l.Es propietario de una casa, terreno u otro bien inmueble? Dsi DNO -~
,~
" ,
Si la respuesta es si a la pregunta 1 y NO a las preguntas 2 y 3, debe proporcionar toda la documentacion que se enumera a continuacion para respaldar sus respuestas.
He adjuntado una copia de mi declaraci6n federal de impuesto sobre la renta mas reciente y la verificaci6n del D ingreso anual bruto de mi grupo familiar; incluso las nuevas fuentes de ingreso que mi grupo familiar espera
recibir.
AFIRMACION
D He adjuntado 0 ya he proporcionado a HMS una copia del Inventario del patrimonio del cliente de HSO.
D He adjuntado 0 ya he proporcionado a HMS una copia del testamento del c1iente de HSO para verificar que soy heredero del patrimonio del cliente de HSO.
EI cliente de HSO muri6 intestado (sin testamento). He adjuntado documentos legales para verificar que soy D descendiente del cliente de HSD. Si no soy descendiente del c1iente de HSO, he adjuntado una "Declaraci6n
jurada de derecho a herencia" que verifica que soy heredero legal del patrimonio del cliente de HSD.
AI firmar abajo certifico que la informaci6n que proporcion6 para una Exenci6n por dificultad econ6mica de reclamo del patrimonio es verdadera y correcta.
/ / -- ----Firma del representante autorizado (Fecha)
Numero de tel6fono
Oirecci6n (calle, ciudad, estado, c6digo postal)
MAD 239 SP Issued 5/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com

III. Solicitud para reduccion parcial
Si desea solicitar la consideracion de una Reduccion parcial del reclamo del patrimonio, conteste todas las preguntas siguientes y proporcione documentacion de apoyo para verificar sus respuestas.
1. l,El cumplimiento del total del reclamo de HSO contra el patrimonio del D si D NO cliente de HSD crea una dificultad financiera para usted y su grupo familiar?
Si la respuesta es sf, explique de que manera el cumplimiento con la cantidad total del reclamo de HSO Ie afectani econ6micamente a usted y a su grupo familiar y proporcione documentaci6n que apoye la manera en que su grupo familiar resultarta afectado con dificultades financieras, si se aplica el importe total del reclamo de HSO. __ ~~ __ ~ ____ ~ ________ ~ ________________ ~ ______________ ~~ ___ "
2. l,EI cumplimiento con el reclamo de HSO contra el patrimonio del cliente de D sf D NO HSO crea una dificultad medica para usted y su grupo familiar?
Si la respuesta es st, explique de que manera el cumplimiento con la cantidad total del reclamo de HSD Ie provocara una dificultad medica a usted 0 a su grupo familiar y proporcione documentaci6n que apoye la manera en que su grupo familiar resultaria afectado con dificultades medicas, si se aplica el importe total del reclamo de HSD.
3. l,Cual es el nfunero total de personas que viven en su grupo familiar (incluyendose usted)? ___ --"-__
4. l,Supera el ingreso anual bruto de su grupo familiar las Directrices federales D sf D NO de pobreza seg6n los ingresos para el tamano de su grupo familiar?
5. l,Cual es el valor justo de mercado del total de los activos muebles e inmuebles de su grupo familiar, incluyendo cualquier gravamen? $ . Adjunte verificaci6n que muestre el valor justo de mercado de todas las fuentes de bienes muebles e inmuebles que son su propiedad y la de su grupo familiar.
6. l,Existe algun otro acreedor que tenga un reclamo contra el patrimonio del D sf D NO cliente de HSO?
Si la respuesta es sf, indique los nombres de los acreedores y el monto del reclamo.
7. l,Alguno de los acreedores que indic6 en la Pregunta 6 anterior ejecut6 los bienes muebles 0 inmuebles que son parte del patrimonio del cliente de D sf D NO HSO? .
8. l,Existe alglIn otro factor que Ie gustaria que HSD tomara en consideraci6n? Si es ast, proporcione una explicaci6n sobre los factores que Ie gustaria que se consideraran y adjunte documentaci6n de apoyo. _______ _
MAD 239 SP Issued 5/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com
D
D
D
AFIRMACI6N
He adjuntado 0 ya he proporcionado a HMS una copia del Inventario del patrimonio del cliente de HSD.
He adjuntado 0 ya he proporcionado a HMS una copia del testamento del cliente de HSD para verificar que soy heredero del patrimonio del cliente de HSD.
EI cliente de HSD muri6 intestado (sin testamento). He adjuntado documentos legales para verificar que soy descendiente del cliente de HSD. Si no soy descendiente del cliente de HSD, he adjuntado una "Declaraci6n jurada de derecho a herencia" que verifica que soy heredero legal del patrimonio del cliente de HSD.
Al firmar abajo certifico que la informacion que proporcion6 para un Reclamo de recuperacion parcial del patrimonio es verdadera y correcta.
Firma del representante autorizado
Direcci6n (calle, ciudad, estado, c6digo postal)
MAD 239 SP Issued 5/13
_1_1-(Fecha)
Numero de tel6fono
«Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com

!!! H U MA~m~RVlCES
OErAR T M E N T
MEDICAL ASSISTANCE DIVISION
hms
NEW MEXICO ESTATE RECOVERY
EXCEPTION APPROVED
« Contact First Name Last Name» « Org Name» « Contact Address I» « Contact Address2» « Contact City, State ZIP»
RE: Estate of « Recipient First Name Last Name» Medicaid ID#: « MID» Date of Death: « DOD»
Dear « Contact First Name Last Name» :
' OR OFFICIAL USE OM.
CASE NAME «Recipient First Name Last Name»
MEDICAID ID NUMBER «MA NUM»
ESTATE CASE ID NUMBER «CaseID»
NOTICE SENT «Notice Sent Date (Date input box)>>
« DATE»
Health Management Systems (HMS), on behalf of the New Mexico Human Services Department (HSD), has granted the following exception to the Estate Recovery Program.
Exception Granted
Based on the information provided in your application for exception, the following exception has been granted:
a Estate Claim Statutory Exemption o Case has been deferred from recovery until the statutory exemption no longer applies. o The claim against the estate is in the amount of «Total Lien» for the period «Service
From Date» through «Service To Date».
a Undue Hardship Waiver o Estate recovery has been waived and the case has been closed.
a Partial Recovery
MAD 242 Issued 05/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com

o The claim against the estate has been reduced from « Original Total Lien» to «Compromised Amount». Please contact our office to make payment arrangements.
Administrative Hearing Rights
Right to a hearing: The human services department (HSD) must grant an opportunity for an administrative hearing
A. When a recipient requests an administrative hearing because he believes that HSD has taken an action erroneously.
B. When services of a Medicaid recipient are terminated, modified, reduced, suspended, or denied.
Time limits: A Medicaid recipient has 90 days from the date of notice of action to request a fair hearing. To be considered timely, the request must be received by the HSD hearings bureau, the local ISD office, or MAD no later than the close of business on the 90th day. In order to receive continuation of benefits while the hearing process goes forward, the request must be received by HSD (including the HSD hearings bureau, the local ISD office, or the medical assistance division) no later than the close of business on the 13th day. Hearings are conducted and a written decision is issued by the medical assistance division director or designee to the recipient within 90 days from the date that HSD receives the hearing request.
Contact: Human Services Department, Hearings Bureau P.O. Box 2348 Santa Fe, NM 87504 1-800-432-6217
If you have any questions, please do not hesitate to call me at the toll free number listed below.
Sincerely, «Electronic Signature» «Caseworker» HMS Caseworker
MAD 242 Issued 05/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com
HUMAN I SERVICES DEPARTMENT
MEDICAL ASSISTANCE DIVISION
hms EXCEPCION APROBADA
DE LA RECUPERACION DE PATRIMONIO DE NUEVO MEXICO
« Contact First Name Last Name» « Org Name» «Contact Address I» «Contact Address2» «Contact City, State ZIP»
RE: Patrimonio de « Recipient First Name Last Name» N.o de INDY del miembro: « INDY» Fecha de fallecimiento: « DOD»
Estimado/a «Contact First Name Last Name»:
« DATE»
Health Management Systems, Inc. (HMS), en nombre del Departamento de Servicios Humanos (HSD) de Nuevo Mexico, Ie concedi6 la siguiente excepci6n en el Programa de recuperaci6n de patrimonio.
Excepcion Concedida
Con base en la informaci6n proporcionada en su solicitud de excepci6n, se Ie ha concedido la siguiente excepci6n:
a Exenci6n legal del rec1amo del patrimonio o EI caso de recuperaci6n se aplaz6 hasta que ya no aplique la exenci6n legal. o EI reclamo contra el patrimonio es por la cantidad de «Total Lien» por el periodo del
«Service From Date» hasta el «Service To Date».
a Exenci6n por dificultad econ6mica o Se renunci6 a la recuperaci6n del patrimonio y el caso se cerr6.
a Recuperaci6n parcial o EI reclamo contra el patrimonio se redujo de « Original Total Lien» a «Compromised
Amount». Comuniquese con nuestra oficina para realizar los arreglos de pago.
MAD 242 SP Issued 5/13 «Project Address» I «Project City. State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com

Derechos de audiencia administrativa
Derecho a una audiencia: el HSD debe conceder una oportunidad para una audiencia administrativa.
A. Cuando un destinatario solicita una audiencia administrativa porque cree que HSD tomo una accion incorrecta.
B. Cuando se tenninan, modifican, reducen, suspenden 0 deniegan los servicios de un destinatario de Medicaid.
Limites de tiempo: un destinatario de Medicaid tiene 90 dias a partir de la fecha de la notificacion de accion para solicitar una audiencia justa. Para que se considere oportuna, la oficina de audiencias de HSD, la oficina local de ISD 0 MAD debe recibir la solicitud a mas tardar el dia 90, al finalizar el dia laboral. Para continuar recibiendo los beneficios mientras el proceso de audiencia avanza, HSD (incluye la oficina de audiencias de HSD, la oficina local de ISD 0 la Division de Asistencia Medica) debe recibir la solicitud a mas tardar el dia l3, al finalizar el dia laboral. Se lIevan a cabo las audiencias y el Director de la Division de Asistencia Medica 0 la persona designada emite al destinatario una decision por escrito, en un periodo de 90 dias, a partir de la fecha en que HSD recibe la solicitud de la audiencia.
Contacto: Human Services Department, Hearings Bureau (Departamento de Servicios Humanos, Oficina de Audiencias) P.O. Box 2348 Santa Fe, NM 87504 1-800-432-6217
Si tiene alguna pregunta, no dude en comunicarse conmigo al numero de telefono gratuito que se indica abajo.
Atentamente, «Electronic Signature» «Caseworker» Especialista de Recuperacion
MAD 242 SP Issued 5/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com

=- JJ! ~ H U MA~ iti 5E RvlcES
D EPARTMENT MEDICAL ASSISTANCE DIVISION
hms
« Contact First Name Last Name» « Org Name» « Contact Address 1» « Contact Address2» « Contact City, State ZIP»
NEW MEXICO ESTATE RECOVERY
REQUEST FOR UPDATE
RE: Estate of « Recipient First Name Last Name» Medicaid ID#: « MID» Date of Death: « DOD» Claim against the estate: « Total Lien»
Dear « Contact First Name Last Name» :
FOR OFfICIAL use ONLY
CASE NAME «Recipient First Name Last Name»
MEDICAID 10 NUMBER «MA NUM»
ESTATE CASE 10 NUMBER «CaseID»
NOTICE SENT «Notice Sent Date (Date input box»)
« DATE»
This letter is a request for infonnation regarding the estate of « Recipient First Name Last Name»
Health Management Systems (HMS), on behalf of the New Mexico Human Services Department (HSD) is seeking recovery from the estate of «Recipient First Name Last Name» for the medical assistance paid on behalf of «Recipient First Name Last Name». HSD is the state agency authorized to provide Medicaid services.
Please contact our office at the address or phone listed below with an update as to the status of the estate's real property and/or the probate proceedings.
If you have any questions, please do not hesitate to call me at the toll free number below.
Sincerely, «Electronic Signature» «Caseworker» HMS Caseworker
MAD 243 Issued 05/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com

til ~ A~
H U MA~ lII sE RvlcES D E PARTMENT
MEDICAL ASSISTANCE D IVISION
hms SOLICITUD DE ACTUALIZACION
SOBRE LA RECUPERACION DE PATRIMONIO DE NUEVO MEXICO
« Contact First Name Last Name» « Org Name» « Contact Address1» «Contact Address2» «Contact City, State ZIP»
RE: Patrimonio de « Recipient First Name Last Name» N.o de INDV del miembro: « INDV» Fecha de fallecimiento: « DOD» Reclamo contra el patrimonio: <<Total Lien»
Estimado/a «Contact First Name Last Name» :
« DATE»
Esta carta es una solicitud de informaci6n con relaci6n al patrimonio de «Recipient First Name Last Name»
Health Management Systems, Inc., (HMS), en nombre del Departamento de Servicios Humanos (HSD) de Nuevo Mexico busca recuperar del patrimonio de «Recipient First Name Last Name» por asistencia medica pagados a nombre de «Recipient First Name Last Name». HSD es la agencia estatal autorizada para proporcionar servicios de Medicaid. HSD contrata a HMS para llevar a cabo sus operaciones del Programa de recuperaci6n de patrimonio.
Comuniquese a nuestra oficina en la direcci6n 0 telefono que se indican abajo para una actualizaci6n del estado de los bienes del patrimonio y/o el juicio sucesorio.
Si tiene alguna pregunta, no dude en comunicarse conmigo al numero de telefono gratuito que se indica abajo.
Atentamente, «Electronic Signature» «Caseworker» Especialista de Recuperaci6n
MAD 243 SP Issued 05/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com

ru - -- )-
H U MA~ it1 SERVICES D E PAR T MENT
MEDICAL ASSISTANCE DIVISION
hms
NEW MEXICO ESTATE RECOVERY
SATISFACTION OF CLAIM
« Contact First Name Last Name» « Org Name» « Contact Address I» « Contact Address2» « Contact City, State ZIP»
RE: Estate of « Recipient First Name Last Name» Medicaid ID#: « MID» Date of Death: « DOD» Claim against the estate: <<Total Lien»
Dear « Contact First Name Last Name» :
FOR OFFICIAL USE ONLY
CASE NAME «Recipient First Name Last Name»
MEDICAID ID NUMBER «MA NUM»
ESTATE CASE ID NUMBER «CaseID»
NOTICE SENT «Notice Sent Date (Date input box)>>
« DATE»
Health Management Systems (HMS), on behalf of the New Mexico Human Services Department (HSD) sought recovery from the estate of «Recipient First Name Last Name»for the amount of medical assistance paid on behalf of «Recipient First Name Last Name». HSD is the State Agency authorized to provide Medicaid.
This letter confirms the receipt of «Paid Amount» as satisfaction in full of the claim against the estate of « Recipient First Name Last Name». This case is now closed.
If you have any questions, please do not hesitate to call me at the toll free number below.
Sincerely, «Electronic Signature» «Caseworker» HMS Caseworker
MAD 244 Issued 05/13 «Project Address» I «Project City. State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com

!!! : ~
H U MA~ ifl sERVICES D E PA It TMf NT
MEDICAL ASSISTANC E DIVI SION
hms SATISFACCI6N DEL RECLAMO
DE RECUPERACI6N DE PATRIMONIO DE NUEVO MEXICO
« Contact First Name Last Name» « Org Name» « Contact Address 1» «Contact Address2» «Contact City, State ZIP»
RE: Patrimonio de « Recipient First Name Last Name» N.O de INDV del miembro: « INDV» Fecha de fallecimiento: « DOD» Reclamo contra el patrimonio: <<rotal Lien»
Estimado/a «Contact First Name Last Name» :
« DATE»
Health Management Systems, Inc., (HMS), en nombre del Departamento de Servicios Humanos (HSD) de Nuevo Mexico busca recuperar del patrimonio de « Recipient First Name Last Name» los montos por asistencia medica pagados a nombre de « Recipient First Name Last Name». HSD es la agencia estatal autorizada para proporcionar servicios de Medicaid. HSD contrata a HMS para llevar a cabo sus operaciones del Programa de recuperacion de patrimonio.
Esta carta confirma la recepcion de « Paid Amount» para satisfacer en su totalidad del reclamo contra el patrimonio de «Recipient First Name Last Name» . Este caso esta cerrado.
Si tiene alguna pregunta, no dude en comunicarse conmigo al numero de telefono gratuito que se indica abajo.
Atentamente, «Electronic Signature» «Caseworker» Especialista de Recuperacion
MAD 244 SP Issued 05/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com

.~}!! ~ HUMAN SERVICES
Dl f' ART ME NT MEDICALASSISTAN("E DIVISION
hms « Date»
« Contact Name» « Organization Name» «Organization Address» « Organization City/State/Zip»
RE: Estate of: Date of Death: MERP Case#:
New Mexico Estate Recovery Request for Additional Information
«Recipient Name» «Date of Death» «Case Number»
Dear «Contact First Name Last Name»:
The New Mexico Medicaid Estate Recovery Program requests the following additional documents to aid in the review of statutory and hardship exemptions applicable to the Human Services Department (HSD) Estate Claim regarding «Recipient Name» which may serve to defer or waive said claim.
If there is a Surviving Spouse: o A Death certificate for the deceased HSD client.
o Marriage License for the deceased HSD client.
If there is a surviving Minor ChiidlDisabled Child: o Birth Certificate or any legal document that verifies the child's age and the child's
relationship to the HSD client.
o Current disability benefit award letter for the HSD client's child. (SSIISSA)
If there is a Hardship Applicant: o Hardship applicant's most recent Federal Income tax return.
o 3 months of pay check stubs for the hardship applicant.
o A copy of the hardship applicant's UTILITY BILLS for the 12 months prior to the decedent's death, or BANK STATEMENTS for the 12 months prior to the decedent's death, or PAY RECORDS for the 12 months prior to the decedent's death. The address information on all
MAD 245 Issued 05/13

!It .::( 150
HUMAN iii SERVICES Ol.r~A.r.M(Nr
MEDICAL ASSISTANCE. DIVISION
bills/statements/records must match the HSD client's address.
o County Assessor's Statement or an official document from the New Mexico State Department of Revenue that verifies the HSD client's real property is residential property.
o Verification which establishes that the Hardship applicant resided at the residential property of said HSD client at the time ofHSD client's death.
Other Important Documents: o A copy of the HSD client's bank statement(s) at the time ofhislher death.
o A copy of the HSD client's Will or an Affidavit of Heirship.
o A copy of the HSD client's estate Inventory.
o «Free form» (Such as mortgage paperwork showing property mortgage exceeding market value etc.)
To ensure quickest processing, please fax the requested documentation to (855) 285-3995. Alternatively, the requested documents may be mailed to our address below. Please include a copy of this letter with the requested documents.
Health Management Systems Contractor for HSD
PO Box 167767 Irving, TX 75016-7767
Should you have any questions or concerns, or you have already submitted the requested documentation, please call us toll-free at 855-212-0144.
Sincerely, «Electronic Signature» «Caseworker» MERP Representative
MAD 245 Issued 05/13

m .a;: , 18
HUMAN 1I'f SERVICES Of r ... R T M(N l
MEDICAlASSfSTAN(:E DIVISION
hms «Date»
«Contact Name» «Organization Name» «Organization Address» «Organization City/State/Zip»
Nuevo Mexico Recuperacion de Patrimonio Solicitud de Informacion Adicional
RE: Patrimonio de: Fecha de Fallecimiento: MERP Numero de Caso:
«Recipient Name» «Date of Death» «Case Number»
Estimado/a «Contact First Name Last Name»:
El Programa de Recuperaci6n de Patrimonio de Nuevo Mexico peticiona los siguientes documentos adicionales indicados para ayudar en la revisi6n de las exenciones legales y penalidades aplicables a la Reclamaci6n del los Bienes del Departamento de Servicios Humanos respecto del destinatario «Recipient Name» que puede servir para diferir 0 renunciar a dicha reclamaci6n.
Si bay un conyuge sobreviviente: o Un Certificado de defunci6n del cliente de HSD.
o Licencia de matrimonio para el beneficiario del fallecido miembro de Medicaid.
Si bay un bijo sobreviviente menor de 21 aios Imovilidad reducida: o Certificado de Nacimiento del nino 0 cualquier documento legal que acredite la edad del nino
y la relaci6n del nino al cliente de HSD.
o Carta del premio de beneficio actual de movilidad reducida del hijo del cliente de HSD. (SSJ)
Si bay un Solicitante de Dificultades: o Solicitante de dificultades de la mas reciente declaraci6n federal de impuestos. 0 3 meses de talones de pago de verificaci6n para el solicitante de dificultades.
o Una copia de las facturas del solicitante de dificultad para los 12 meses anteriores al fallecimiento del causante, 0 los extractos bancarios de los 12 meses anteriores al fallecimiento del causante, 0 los registros de pago para los 12 meses anteriores al
MAD 245 SP Issued 05/13

!I! .:;( lS-
H U MAN iii SERVICES OEPARTMENI
MEOICALA$SISTANCE DIVISION
fallecimiento del causante. La infonnaci6n de direcci6n en todas las facturas/declaraciones/registros debe coincidir con la direcci6n del recipiente de HSD.
o Declaraci6n del Asesor del Condado 0 en un documento oficial del Departamento del estado de Nuevo Mexico de ingresos que verifica la propiedad real del recipiente de HSD es propiedad residencial.
o Verificaci6n que establece que el solicitante residi6 por dificultades en la propiedad residencial de dicho recipiente de HSD en el momento del fallecimiento del recipiente de HSD.
Otros Documentos Importantes: o Una copia del extracto bancario del recipiente de HSD en el momento de su fallecimiento.
o Una copia de la Voluntad del recipiente de HSD 0 una Declaraci6n de Herederos.
o Una copia del inventario de bienes del recipiente de HSD.
o «Free fonn» (Tal como hipoteca documentaci6n de la propiedad mostrando que el valor es superior, etc.)
Para asegurar el procesamiento mas nipido, por favor, envie por fax la documentaci6n solicitada a (855) 285-3995. Altemativamente, los documentos solicitados pueden ser enviados por correa a nuestra direcci6n abajo. Por favor, incluya una copia de esta carta con los documentos solicitados.
Health Management Systems Contratista para HSD
PO Box 167767 Irving, TX 75016-7767
Si tiene alguna pregunta 0 duda, 0 ya ha presentado la documentaci6n solicitada, por favor llamenos al nfunero gratuito 855-212-0144.
Sinceramente, «Electronic Signature» «Caseworker» MERP Representante
MAD 245 SP Issued 05/13

_!U _ - -H U MA N Iti SERVICES
DEPARTMENT MEDICAL ASSISTANCE DIVISI ON
hms
NEW MEXICO ESTATE RECOVERY
EXCEPTION DENIED
« Contact First Name Last Name» « Org Name» « Contact Address 1» « Contact Address2» « Contact City, State ZIP»
RE: Estate of « Recipient First Name Last Name» Medicaid ID#: « MID» Date of Death: « DOD»
Dear « Contact First Name Last Name» :
FOR OFfICIAL USE ONI. Y
CASE NAME «Recipient First Name Last Name»
MEDICAID 10 NUMBER «MA NUM»
ESTATE CASE 10 NUMBER «CaseID»
NOTICE SENT «Notice Sent Date (Date input box)>>
« DATE»
Health Management Systems (HMS), on behalf of the New Mexico Human Services Department (HSD), has denied your request for exception.
The claim against the estate is in the amount of «Total Lien» for the period «Service From Date» through «Service To Date».
Please contact our office by phone or at the address listed below to make payment arrangements.
Administrative Hearing Rights
Right to a hearing: The human services department (HSD) must grant an opportunity for an administrative hearing
A. When a Medicaid recipient requests an administrative hearing because he believes that HSD has taken an action erroneously.
B. When services of a Medicaid recipient are terminated, modified, reduced, suspended, or denied.
MAD 246 Issued 05/13 «Project Address» I «Project City. State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com

Time limits: A Medicaid recipient has 90 days from the date of notice of action to request a fair hearing. To be considered timely, the request must be received by the HSD hearings bureau, the local ISD office, or MAD no later than the close of business on the 90th day. In order to receive continuation of benefits while the hearing process goes forward, the request must be received by HSD (including the HSD hearings bureau, the local ISD office, or the medical assistance division) no later than the close of business on the 13th day. Hearings are conducted and a written decision is issued by the medical assistance division director or designee to the recipient within 90 days from the date that HSD receives the hearing request.
Contact: Human Services Department, Hearings Bureau P.O. Box 2348 Santa Fe, NM 87504 1-800-432-6217
If you have any questions please do not hesitate to call me at the toll free number listed below.
Sincerely, «Electronic Signature» «Caseworker» HMS Caseworker
MAD 246 Issued 05/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com

!II =- ,;, H U MA ~ iff sERVICES
DErAIlTMEN T MEDICAL ASSISTANCE D IVI SI ON
hms « Contact First Name Last Name» « Org Name» « Contact Address 1» « Contact Address2» « Contact City, State ZIP»
« DATE»
EXCEPCION DENEGADA
DE LA RECUPERACION DE PATRIMONIO DE NUEVO MEXICO
RE: Patrimonio de « Recipient First Name Last Name» N.o de INDV del miembro: « INDV» Fecha de fallecimiento: « DOD»
Estimado/a «Contact First Name Last Name»:
Health Management Systems, Inc. (HMS), en nombre del Departamento de Servicios Humanos (HSD) de Nuevo Mexico, deneg6 su solicitud de excepci6n.
EI reclamo contra el patrimonio es por la cantidad de «Total Lien» por el periodo del «Service From Date» hasta el «Service To Date».
Comuniquese con nuestra oficina por telefono 0 en la direcci6n que se indica mas adelante para realizar los arreglos de pago.
Derechos de audiencia administrativa
Derecho a una audiencia: el Departamento de Servicios Humanos (HSD) debe conceder una oportunidad para una audiencia administrativa.
A. Cuando un destinatario solicita una audiencia administrativa porque cree que HSD tom6 una acci6n incorrecta.
B. Cuando se terminan, modifican, reducen, suspenden 0 deniegan los servicios de un destinatario de Medicaid.
Limites de tiempo: un destinatario de Medicaid tiene 90 dias a partir de la fecha de la notificaci6n de acci6n para solicitar una audiencia justa. Para que se considere oportuna, la oficina de audiencias de HSD, la oficina local de ISD 0 MAD debe recibir la solicitud a mas tardar el dia 90, al finalizar
MAD 246 SP 05/13 «Project Address» I «Project City. State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com

el dia laboral. Para continuar recibiendo los beneficios mientras el proceso de audiencia avanza, HSD (incluye la oficina de audiencias de HSD, la oficina local de ISD 0 la Division de Asistencia Medica) debe recibir la solicitud a mas tardar el dia 13, al finalizar el dia laboral. Se Bevan a cabo las audiencias y el Director de la Division de Asistencia Medica 0 la persona designada emite al destinatario una decision por escrito, en un periodo de 90 dias, a partir de la fecha en que HSD recibe la solicitud de la audiencia.
Contacto: Human Services Department, Hearings Bureau (Departamento de Servicios Humanos, Oficina de Audiencias) P.O. Box 2348 Santa Fe, NM 87504 1-800-432-6217
Si tiene alguna pregunta, no dude en comunicarse conmigo al numero de telefono gratuito que se indica a continuacion.
Atentamente, «Electronic Signature» «Caseworker» Especialista de Recuperacion
MAD 246 SP 05/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuita «Toll Free» I www.hms.com

dl -==n= H U MA N iii SERVICES
DEPA.RTMlNT MEDICAL ASSISTANCE DI\'1SION
hms
TO: «Contact First Name Last Name»
FROM: Health Management Systems
RE: Estate of «Recipient First Name Last Name»
SUBJECT: Receipt of Claim Against the Estate
«DATE»
Since we do not send our Claim Against the Estate by certified mail, please sign, date and return this Receipt in the provided envelope. Thank you.
RECEIPT
I have received the Claim Against the Estate.
Sign: _________________ _
Date: ____________ _
MAD 247 Issued 05/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I toll free «Toll Free» I www.hms.com
,I, =- '-')--::'
H U MA~ lIf sERVIC ES DEPARTME N r
MEDICAL ASSISTANC E DIVISION
hms
PARA: « Contacto Nombre Apellido»
DE: Health Management Systems
RE: Patrimonio de « Recipient First Name Last Name»
ASUNTO: Recepci6n del Reclamo Contra el Patrimonio
« DATE»
Ya que no enviamos nuestro Reclamo Contra el Patrimonio por correo certificado, por favor firme, feche y devolver este Recibo en el sobre adjunto. Gracias.
RECEPCION
He recibido el Reclamo Contra el Patrimonio
Firma: --------------------------------------Fecha: --------------------------
MAD 247 SP Issued 5/13 «Project Address» I «Project City, State ZIP» I tel «Project Phone» I fax «Project Fax» I tel gratuito «Toll Free» I www.hms.com