department /agency: title: impact assessment of...
TRANSCRIPT

Summary: Intervention & Options
Department /Agency: Title: Impact Assessment of Treatment of Heart Attacks -National GuidanceDepartment of Health
Stage: Implementation Version: 2 Date: 1 October 2008
Related Publications: Treatment of Heart Attack National Guidance. Final Report of the National Infarct Angioplasty Project (NIAP) (DoH, October 2008)
Available to view or download at: http://www.dh.gov.uk
Contact for enquiries: Sue Dodd Telephone: 020 79724825
What is the problem under consideration? Why is government intervention necessary? Thrombolysis is the currently recommended treatment for heart attacks (STEMI) in the National Service Framework for Coronary Heart Disease. More recent evidence suggests that infarct angioplasty for STEMI has significantly better outcomes. A National Infarct Angioplasty Project is now complete and demonstrates that implementation of infarct angioplasty is feasible and cost effective.A three year implementation period has been assumed in costings but it will be for local services to determine their priorities and the pace of change. This guidance provides advice for local service planning.
What are the policy objectives and the intended effects? The main policy objective is to amend the current National Service Framework to reflect best clinical practice and recommend infarct angioplasty as the treatment of choice for people having a heart attack (STEMI). The intended effects are to • reduce mortality from heart attack, • reduce the subsequent numbers of heart attacks suffered by people who have a heart attack. • reduce the subsequent numbers of strokes suffered by people who have a heart attack.
What policy options have been considered? Please justify any preferred option. The purpose of this document is to test the implementation options. There are 2 main options: (i) Status Quo – Do Nothing (ii) Implement Primary Infarct Angioplasty in 3
years The second option of implementing Primary Infarct Angioplasty is the preferred option. Infarct angioplasty has proven benefits and implementation is feasible over the next 3 years. This would achieve these benefits at an early stage.
When will the policy be reviewed to establish the actual costs and benefits and the achievement of the desired effects? The Department will review implementation after 3 years (i.e. in the period after December 2011).
Ministerial Sign-off For final proposal/implementation stage Impact Assessments:
I have read the Impact Assessment and I am satisfied that, given the available evidence, it represents a reasonable view of the likely costs, benefits and impact of the leading options. Signed by the responsible Minister:
Date:
1
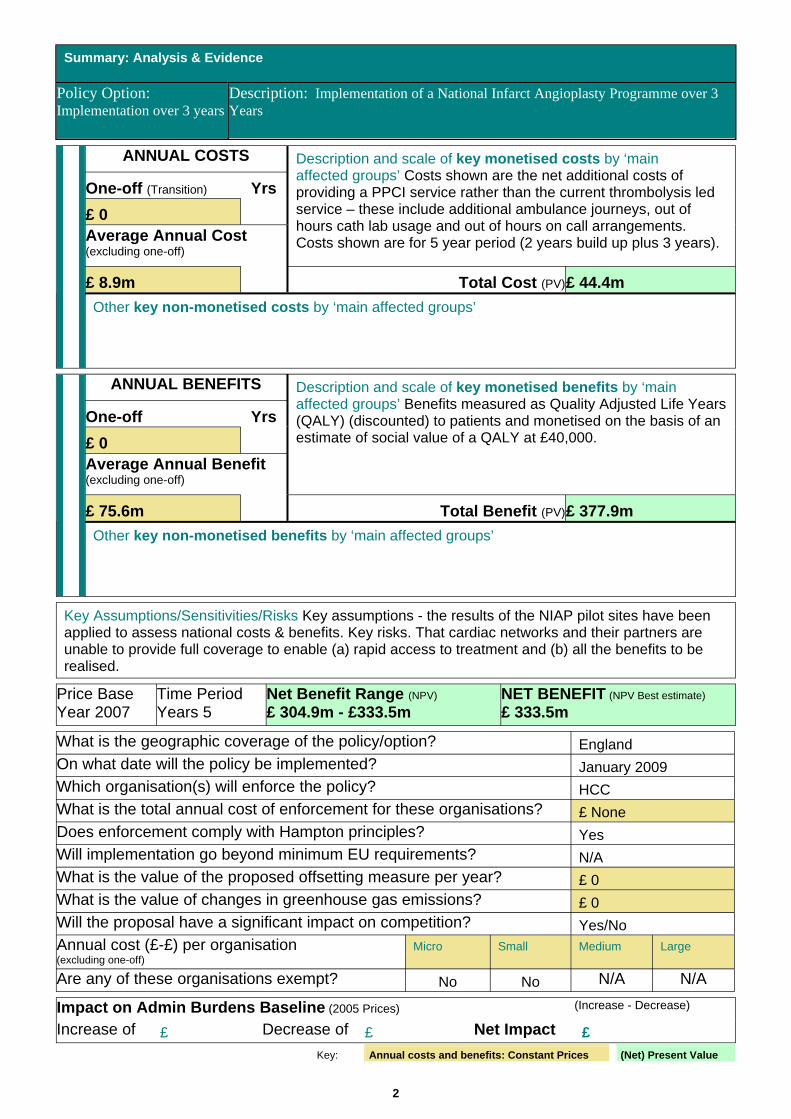
Summary: Analysis & Evidence
Policy Option: Implementation over 3 years
Description: Implementation of a National Infarct Angioplasty Programme over 3 Years
ANNUAL COSTS
One-off (Transition) Yrs £ 0 Average Annual Cost(excluding one-off)
Description and scale of key monetised costs by ‘main affected groups’ Costs shown are the net additional costs of providing a PPCI service rather than the current thrombolysis led service – these include additional ambulance journeys, out of hours cath lab usage and out of hours on call arrangements. Costs shown are for 5 year period (2 years build up plus 3 years).
£ 8.9m Total Cost (PV)£ 44.4mCO
STS
Other key non-monetised costs by ‘main affected groups’
ANNUAL BENEFITS
One-off Yrs £ 0 Average Annual Benefit(excluding one-off)
Description and scale of key monetised benefits by ‘main affected groups’ Benefits measured as Quality Adjusted Life Years (QALY) (discounted) to patients and monetised on the basis of an estimate of social value of a QALY at £40,000.
£ 75.6m Total Benefit (PV)£ 377.9mBEN
EFIT
S
Other key non-monetised benefits by ‘main affected groups’
Key Assumptions/Sensitivities/Risks Key assumptions - the results of the NIAP pilot sites have been applied to assess national costs & benefits. Key risks. That cardiac networks and their partners are unable to provide full coverage to enable (a) rapid access to treatment and (b) all the benefits to be realised.
Price Base Year 2007
Time Period Years 5
Net Benefit Range (NPV)
£ 304.9m - £333.5m NET BENEFIT (NPV Best estimate)
£ 333.5m
What is the geographic coverage of the policy/option? England On what date will the policy be implemented? January 2009 Which organisation(s) will enforce the policy? HCC What is the total annual cost of enforcement for these organisations? £ None Does enforcement comply with Hampton principles? Yes Will implementation go beyond minimum EU requirements? N/A What is the value of the proposed offsetting measure per year? £ 0 What is the value of changes in greenhouse gas emissions? £ 0 Will the proposal have a significant impact on competition? Yes/No Annual cost (£-£) per organisation (excluding one-off)
Micro Small Medium Large
Are any of these organisations exempt? No No N/A N/A
Impact on Admin Burdens Baseline (2005 Prices) (Increase - Decrease)
Increase of £ Decrease of £ Net Impact £ Key: Annual costs and benefits: Constant Prices (Net) Present Value
2

)Evidence Base (for summary sheets
[Use this space (with a recommended maximum of 30 pages) to set out the evidence, analysis and detailed narrative from which you have generated your policy options or proposal. Ensure that the information is organised in such a way as to explain clearly the summary information on the preceding pages of this form.]
Introduction 1. This impact assessment sets out the major costs and benefits that may be associated with
implementing national guidance on the Treatment of Heart Attacks. It describes in detail the problem under consideration and why it is necessary for the Government to intervene. The document describes the policy objectives and their intended effects.
2. Two options have been identified: • Status Quo – Do Nothing • Implement national guidance on Treatment of Heart Attacks.
3. Implementing Treatment of Heart Attacks involves making changes to the care pathway and the treatment given in the immediate care pathway following a heart attack (STEMI). The recommended treatment for all people have a heart attack (STEMI) is infarct angioplasty also known as Primary Angioplasty (PPCI) for people who can receive treatment within 120 minutes of calling for help.
4. This document outlines the costs and benefits associated of providing this treatment routinely and the assumptions which have been made in the calculations. For more detailed discussion of how the treatment of heart attacks and the results of national pilot studies please see the document Treatment of Heart Attack – National Guidance. Final report of the National Infarct Angioplasty Project1.
5. The costs and benefits of implementing infarct angioplasty or PPCI at the pilot sites have been evaluated independently by the School of Health and Related Research (ScHARR) and the Institute of Work Psychology at the University of Sheffield. Their formal report on the NIAP project provides the data on which this impact assessment is based2.
6. The treatment recommended for Heart Attacks was referred to and the pilot work commended in the Next Stage Review of the NHS (Darzi) 3 which was the subject of formal consultation between July, 2007 and October, 2007. The final report “High quality care for all: NHS Next Stage Review Final Report” (CM 7432, June 2008) 4 responds to this consultation and is available on the DH website.
3

What is the problem under consideration? What is a heart attack?
7. A heart attack is said to have occurred when the myocardium (heart muscle) is damaged as a result of impaired blood supply. This is known as a myocardial infarction. The amount of damage is greatest when the blood supply to part of the heart is cut off altogether as a result of thrombus (blood clot formation) within one of the coronary arteries ( blood vessels) supplying that area of the heart. Under these circumstances the electrocardiogram (ECG) recorded after the onset of occlusion will usually show an abnormality termed ‘ST elevation’, and patients suffering this condition are said to have sustained ‘ST elevation myocardial infarction’, abbreviated to STEMI. This guidance covers the management STEMI. Non ST elevation myocardial infarction or NSTEMI is the subject of separate NICE guideline.
What are the different treatments for heart attack?
8. Because the mechanism underlying occlusion of the coronary artery is the formation of thrombus (blood clot), attention was first directed towards various drugs, which have the ability to dissolve clot, termed thrombolytic agents. In the late 1980s and through the 1990s these agents became widely prescribed, mainly by hospital staff once the patient had been admitted to hospital. Not surprisingly these agents increase the risk of bleeding and have also been shown to cause some strokes. However, this risk is outweighed by the benefits of improved survival following the heart attack. Some patients are unsuitable for thrombolysis, for instance, because they are at higher risk of bleeding, and even among those who are suitable in approximately 20% to 30% of cases the artery fails to reopen following the treatment.
9. Following the publication of numerous trials it was shown that the outcome for patients with STEMI was closely related to the length of time that the coronary artery was occluded, and the completeness of restoration of blood flow achieved with treatment; the longer the duration of occlusion, or the more incomplete the restoration of blood flow, the greater the damage to the heart muscle and the worse the patient’s outcome. This prompted the investigation of two alternative treatment options. The first involved the use of thrombolytic agents, but given before the patient arrives in hospital, known as pre-hospital thrombolysis (PHT), with the drug usually administered by trained paramedics. This results in earlier administration of the agents and better outcome for patients. The second involved a more mechanical approach to the problem. By inserting a catheter (tube) into the body, via a peripheral artery in the groin or wrist, a balloon catheter is passed down the coronary artery and the occlusion unblocked, usually with the additional insertion of a stent (a cylindrical metallic mesh) to hold the affected area open. This technique is termed primary angioplasty, or to give it its full name primary percutaneous coronary intervention (PPCI).
What impact do heart attacks have nationally?
10. Ischaemic Heart Disease is the single largest cause of death in England with 77,000 deaths in 2006 (17% of the total)., This is despite the fact that deaths from heart disease have reduced substantially since the publication of the National Service Framework for Coronary Heart Disease1 and are ahead of national targets. Ischaemic Heart Disease deaths under the age of 75 years accounted for 260,000 years of life lost.
11. In 2007, just under 63,400 people in England were recorded on the national heart attack database (MINAP) and of these 25,600 were STEMI and 37,800 were non-STEMI.
4

Why is government intervention necessary? Previous Government Action
12. At the time of publication of the National Service Framework (NSF) for Coronary Heart Disease in March 2000 5, the number of patients in whom PPCI had been tried was relatively small and so the clinical and financial consequences were not certain enough to commend it as a routine method for treating heart attack (STEMI). Chapter three of the NSF therefore concentrates on a thrombolytic treatment strategy for heart attack and, to secure an improvement in patient outcomes, sets out a standard that people thought to be suffering from heart attack should be assessed professionally and given thrombolysis within 60 minutes of them calling for professional help. Progress towards this standard was supported by investment in the roll out of pre hospital thrombolysis (PHT). Provision of thrombolysis in Accident and Emergency Departments led to significant improvement in times to treatment in the first few years after the NSF. More gradual progress has been achieved since then with the increase in PHT. Progress has been closely monitored by the Department of Health and driven by performance indicators set by the Healthcare Commission. In 2007/8, 71% of people 6 who received thrombolysis for heart attack did so within 60 minutes in England compared to 24% at the time of publication of the NSF. In 2007 25% of STEMI patients had PPCI.
13. The use of PPCI for heart attack has however continued to develop in England. The first limited services started to be offered in a small number of cardiac centres by about 2002. In June 2003 the Prime Minister’s Delivery Unit conducted a review of national policy for treatment of heart attack 7. In the light of the experience from these centres and the expanding evidence from clinical trials, the Prime Minister’s Delivery Unit recommended that the Department of Health developed a clear policy for expanding PPCI and drew conclusions on the advisability and feasibility of a national rollout of this service. NIAP was set up to inform this policy with £1 million provided to develop a dataset and to support data collection and analysis at a number of pilot sites. PPCI services have continued to expand during NIAP.
The Need for Improvement
14. The interim report from NIAP 8 produced some promising results from the pilot studies and these have been confirmed in the final evaluation report which is being published shortly. Infarct angioplasty improves patient outcomes provided treatment is delivered within 120 minutes of call for help (Call to Balloon Time or CBT) and at a cost which is considerably lower than the benefits delivered.
15. The Darzi review pointed to this work as being an important example of the benefits which could be achieved for patients by organising services on the basis of more specialised centres of excellence.
16. Also in December 2006, Professor Boyle produced Mending Hearts and Brains 9, a report that made the clinical case for reconfiguration in terms of delivering better urgent case for heart attack (and ‘brain attack’). This stressed the need for heart attack and stroke services to be delivered by personnel with an appropriate level of experience and training in settings with sophisticated diagnostic and monitoring facilities on a 24 hours a day, seven days a week, immediate-access basis.
17. To deliver the full benefits available to patients having heart attacks, it is recommended that infarct angioplasty (PPCI) is implemented across the country.
Policy objectives and intended effects 18. When implemented, this national guidance on the treatment of heart attacks is intended to provide :
• High quality state of the art treatment for all patients available within 120 minutes of calling for help, available 24 hours a day, seven days a week.
5

• Better outcomes in terms of reduced mortality associated with having a heart attack. • Better outcomes in terms of a reduced number of people suffering a further heart attack or a
stroke after a first heart attack. • Advice, guidance and support for commissioners, cardiac networks and Strategic Health
Authorities in the planning, development and monitoring of services • Information for patients’ and their families’ about treatment following a heart attack by
providing standards expected from “heart attack centres”.
19. The guidance will not act as a detailed clinical guideline.
20. The strategy applies to heart attack treatment in England only.
Policy options 21. The final NIAP report identifies two options:
• Status Quo – Do Nothing • Implement Infarct Angioplasty for people having a Heart Attack (STEMI) within 3 years
22. The first option of doing nothing and maintaining the status quo is not a sustainable course of action. Infarct angioplasty is a proven treatment with better outcomes than current treatment of thrombolysis plus angiography (known to be 60% of those having thrombolysis currently) plus PCI or CABG for around 50% of these in the following year 2. Infarct angioplasty is already available to around 25% of people having a heart attack – at the pilot sites and in other hospitals where clinical enthusiasm has led to early partial implementation.
23. The second option of implementing infarct angioplasty (PPCI) for people having a heart attack (STEMI) is for commissioners and cardiac networks – working with their partners/component organisations – to agree and implement new patterns of care which will enable as many people as possible to receive treatment within 120 minutes Call to Balloon (CTB) time. This approach will maximise the potential benefits from PPCI. The final report from NIAP includes guidance on the key factors for commissioners and cardiac networks to consider when they are developing their plans. It is vital in this process that all partners are involved. The ambulance service in each area has a critical part to play in enabling patients to arrive within the requisite time. Local plans and policies developed need to be agreed between acute and ambulance Trusts and commissioners working together in cardiac networks. While the NIAP report provides guidance on the basis of the pilot sites, this is not prescriptive and recognises that local areas will develop their services in line with local circumstances, infrastructure and capability.
24. It is recognised that for a small part of the country it is likely – at least over the first 3 years – that services which are close enough to local populations to meet the 120 minutes CTB time will not be able to be developed. A preliminary estimate suggests that this may equate to just over 1.3 million people (2.6% of the population). For these people it is recommended that they receive thrombolysis, followed by subsequent angiography so that a decision can be made about whether a PCI or CABG is required. There may also be people who live within range of a PPCI centre – but unforeseen circumstances prevent them from reaching that centre in time for PPCI. Recommended treatment for those people is also thrombolysis, followed by subsequent angiography so that a decision can be made about whether a PCI or CABG is required.
Detailed Consideration of Options
25. Part of the NIAP was an independent evaluation of the costs and assessed benefits of implementing PPCI for heart attack (STEMI) at the pilot sites. This evaluation is available as a separate report 2
and is the major source of information for this impact assessment. The evaluation used data from the
6

pilot sites but also applied results from the York model 10 which assessed the change in outcomes which resulted from different periods of delay from initial onset of a heart attack to firstly thrombolysis and subsequent treatment (if any) and secondly primary PCI. A key finding in this York model was that the benefits of PPCI were greatest up to an hour beyond the time when people would have received thrombolysis. While outcomes continue to be superior for PPCI as opposed to thrombolysis beyond that time, they diminish. Thrombolysis is recommended within 60 minutes of a call for help and therefore the guidance is that PPCI should be delivered within 120 minutes of the call for help.
. Summary and Assumptions
26. Two possibilities were considered in terms of the numbers of heart attacks (STEMI) that would need treatment in the future, the first based on reductions of 1.5% per year over the 5 years - requiring 13,454 PPCIs in year 3, the second based on stable STEMI numbers – requiring 14,293 PPCIs in year 3. The reducing STEMI numbers scenario is considered to be the most likely over the coming 5 years and this is the basis of the costs and benefits included in this summary.
27. The average annual cost over the 5 years assessed, is £114.4m (NPV).
28. The average annual saving to the NHS is £105.5m (NPV).
29. The net average annual cost to the NHS over the 5 years is estimated at £8.9m (NPV).
30. Prevention of Deaths - Each year at full implementation, approximately 237 deaths from heart attack will be prevented.
31. Prevention of Subsequent Heart Attack – Each year there will be 630 fewer subsequent heart attacks.
32. Prevention of Subsequent Strokes – Each year there will be 261 fewer strokes.
33. The estimated average QALY gain per annum associated with these benefits over the first 5 years, assuming a value per QALY of £40,000, is £75.6m (NPV).
34. The net benefit (NPV) over the 5 years is estimated to be £333.5m.
35. Two scenarios for implementation were considered, the first do nothing and the second to proceed to full implementation over a period of 3 years. The benefits of infarct angioplasty for heart attack (STEMI), which is recognised as being superior to current treatment, can only be realised on an equitable basis with full implementation.
Costs and Savings/Benefits of Proposals 36. All costs and benefits presented here are for England only, and all sums are at 2007/8 prices
discounted at 3.5% per annum in line with HMT Green Book 11.
Total costs 37. Calculation of the total annual cost at full implementation, assumes that 97.4% of the eligible
population can be covered by a PPCI service and that 95% of this eligible population receive PPCI. These costs are based on an estimated increase of 13,454 receiving infarct angioplasty in year 3 with reducing STEMI numbers of 1.5% per annum.
38. The increase in cost to the NHS arises from introducing PPCI at selected sites across the country – identified by commissioners and cardiac networks. This increase in cost is estimated to be £145.7m (NPV) in the first full year (year 3) for reducing STEMI numbers. These sites will all be
7

undertaking PCI already and therefore the change in practice will not require changes in physical infrastructure.
Total savings 39. The savings to the NHS will come from discontinuing current treatment i.e. thrombolysis, followed
by angiography for around 60% and PCI or CABG for around 50% of those within a year 2. The savings in the first full year (Year 3) are estimated to be £134.4m (NPV) with reducing STEMI numbers.
Total Net Costs 40. The following table shows the net cost at 2007/8 price base and the net cost (NPV) which has been
calculated by multiplying the additional cost (2007/8 price base) of PPCI by the number of people who will receive PPC, discounted at 3.5% pear year (in line with HMT Green Book). This is shown for reducing STEMI numbers.
Year 1 Year 2 Year 3 Year 4 Year 5 Total £m £m £m £m £m £m
Reducing STEMI Net Cost at 2007/8 Price Base
4.2 8.2 12.1 11.9 11.7 48.1 Net Cost (NPV) Discounted at 3.5% per annum, 4.2 7.9 11.3 10.8 10.2 44.4
Benefits and Monetarised QALY gains 41. The benefits are the improved outcomes which will arise from heart attack (STEMI) patients
receiving PPCI rather than current treatment. These benefits are in
• Reduced mortality at 1 month • Reduced mortality at 6 months • A reduction in subsequent coronary events for those that survive their heart attack at 6 months • A reduction in strokes for those that survive their heart attack at 6 months.
42. The table below shows the estimated total monetarised (NPV) QALY gain attached to the improved outcomes specified above over the 5 year period ; as well as the total monetised benefit of the QALY gain with use of a social value of £40,000 (with a QALY discount at 1.5%). For more details on the QALY estimates and sensitivity analysis around the cost per QALY of this treatment for heart attack (STEMI) guidance, see Annex B.
Year 1 Year 2 Year 3 Year 4 Year 5 Total Reducing STEMI QALY Gain (a)
846 1,642 2,390 2,319 2,251 9,448 Value of Gain (£m) – PV (b)
33.8 65.7 95.6 92.8 90.0 377.9
(a) QALY gain discounted at 1.5% per year.
Sensitivity Analysis
43. Sensitivity analysis has been undertaken in assessing the impact the QALY benefit of changes in STEMI. The likely scenario is a reduction of 1.5% per annum and stable STEMI and a reduction of 3% per annum have been calculated.
8

Year 1 Year 2 Year 3 Year 4 Year 5 Total Average Gain p.a
Reducing STEMI - 3% per annum 819 1,563 2,238 2,137 2,040 8,797 1,759 Reducing STEMI - 1.5% per annum 846 1,642 2,390 2,319 2,251 9,448 1,890 Stable STEMI 872 1,718 2,539 2,501 2,464 10,094 2,019 Variance from Likely Reduction of 1.5% Reducing STEMI - 3% per annum (27) (79) (151) (182) (211) (650) (130) Stable STEMI 26 76 149 182 214 647 129
If STEMIs reduced by 3% per annum rather than 1.5% per annum – there would be 650 (7%) fewer QALYs over the 5 year period, an average of 130 (7%) fewer QALYs per annum. If STEMIs remained stable there would be 647 (7%) more QALYs over the 5 year period an average of 129 (7%) more QALYs per year. If costs remained constant then the cost per QALY (discounted) would be in the range £4,769 for the stable STEMI scenario to £5,472 for the 3% reduction scenario. Both of these still represent good value relative to the estimate of the social value of a QALY of £40,000.
Transitional Costs
Potential transitional costs may arise in relation to project management, training and consultation with partners and the public. In some places these may be covered as routine management and training costs and in others additional costs may be incurred. For example in the North East cardiac Network they estimate the costs of additional training will be in the region of £11,000. Transitional costs have not been included in this assessment, because of uncertainty about how they will be handled locally.
Risks
44. The main risks are that cardiac networks and their partners are unable to provide full coverage to enable rapid access to treatment and all the benefits to be realised and that organisations which cease receiving heart attacks will not be able to make savings involved in the current pattern of thrombolysis led treatment.
45. Cardiac Networks Unable to Provide Full Coverage. The impact of this will be that fewer people having a heart attack will switch to PPCI. This will reduce the savings required and the net cost and reduce the benefits in QALYs, reduced deaths and reduced subsequent heart attacks and strokes. However, the cost per QALY gained for the population receiving PPCI should remain much the same.
46. Organisations Ceasing to Receive Heart Attacks Unable to Make Savings. The potential impact of this is that either implementation goes ahead and the overall costs are higher or that in some parts of the country less than full coverage is achieved. The factors which mitigate against this risk are
• Already 25% of people with STEMI are receiving PPCI and this has been achieved without major apparent financial problems.
• In those places that undertake PPCI their saving is a combination of changes in their system of care and ceasing to use thrombolytic agents and their increase in costs are primarily for staff on call out of hours and additional cath lab operating for acute trusts and longer and more ambulance journeys for ambulance trusts.
• The modelled phasing of implementation over 3 years means that organisations have time to produce workable solutions – this may be easier in some places than others. The change in reciurrent revenue cost, saving and net cost is incremental over the 3 years (at 2007/8 price base) is shown in the following table – for stable STEMI numbers and reducing STEMI numbers.
9

STEMIs Reduce by 1.5% per year Recurrent Revenue - £m (2007/9 Price Base) Year 1 Year 2 Year 3 After 3 Years
Total Cost - Current Strategy 49.5 48.0 46.5 144.0 Total Savings - PPCI Strategy 53.6 52.0 50.4 156.1 Total Net Cost 4.2 4.0 3.9 12.1
Recurrent Revenue - £m (2007/8 Price Base) Stable STEMI Numbers Year 1 Year 2 Year 3 After 3 Years Total Cost - Current Strategy 51.0 51.0 51.0 152.9 Total Savings - PPCI Strategy 55.3 55.3 55.3 165.8 Total Net Cost 4.3 4.3 4.3 12.9
• The North East Cardiac Network has already reviewed the cost and savings impact on a Trust by Trust basis of implementing PPCI using two centres. It has concluded that the overall package is workable for the partner organisations.
Key data sources Table 1 – Summary of key data sources
Data source Use Background National Infarct Angioplasty Project (NIAP) Interim Report (DoH. February 2008) 8
Evidence on pilot sites and patients treated and factors involved in providing a service.
The NIAP was established to examine different models of implementing PPCI. The interim report analyses data from the patients’ hospital admission and includes observations from the pilot sites that may be useful to those planning to introduce PPCI.
National Infarct Final evidence from Final report on the NIAP project which Angioplasty Project the pilot sites of the provides guidance on the implementation (NIAP) Final Report (DoH. October 2008) 1
total patients treated, the service
of PPCI across throughout those parts of England where 120 minute Call to
models developed Balloon time can be achieved.. and the outcomes.
Evaluation of the Assessment of costs Formal evaluation report commissioned National Infarct and benefits of as part of NAIP to independently assess Angioplasty Project (August 2008) 2
implementing infarct angioplasty.
the implications. Costs and benefits of infarct angioplasty.
Asseburg C, Bravo Provides the This publication provided the vital Vergel Y, Palmer S, detailed assessment assessment of the outcomes and was Fenwick E, de Belder M, of the outcomes used in the SCHARR/IWP report to Abrams K and Sculpher associated with undertake the cost benefit and QALY M. Assessing the PPCI and assessment. effectiveness of primary thrombolysis in angioplasty compared to relation to time thrombolysis and its delays. relationship to time delay: a Bayesian evidence synthesis. Heart 2007;93:1244-5010.
Myocardial Ischaemia Records the number MINAP is a national database of all National Audit project of heart attacks and people in England (and some other parts
10

(MINAP) the number of STEMIs in
of the UK) who have a heart attack, the nature of their heart attack and the
England. treatment/ investigation they receive. British Cardiovascular Intervention Society Audit Database
Provides estimates of numbers of Primary PCIs undertaken in 2007
The United Kingdom national PCI Audit Data have been collected by BCIS since 1991. Audit data is presented at their annual conference and results are viewable at http://www.bcis.org.uk/resources/audit
National Infarct Angioplasty Project (NIAP) Interim Report
47. The interim report was published in February 2008 8. The National Infarct Angioplasty Project (NIAP) is an observational study set up by the Department of Health in collaboration with the British Cardiovascular Society and British Cardiovascular Intervention Society to test the feasibility of developing primary angioplasty services as the initial treatment for heart attack across England. Data from seven pilots (ten centres) were collected from April 2005 to March 2006. Patients recruited to the study in that year were then followed up for a further year to March 2007.
48. This interim report details the study design, pilots and findings from the hospital admission data and the emerging findings from analysis of the first year of data collected by the project’s seven pilot sites from April 2005 to March 2006. The findings in this report were intended to inform commissioners and cardiac networks in their discussions on reconfiguration of acute services and to feed into work on the NHS Next Stage Review.
49. Of those patients having reperfusion treatment for heart attack, 25% now receive primary angioplasty in this country who would have previously been treated with thrombolytic drugs. There is consensus that this provides superior outcomes if delivered quickly. This report suggested that primary angioplasty will be most effective (and cost-effective) if delivered within 120 to 150 minutes of the patient’s call for help (‘call-to-balloon’ time). (N.B. Since then this has been reduced to 120 minutes in line with wider European assessments).
50. The aims of the NIAP were to address the logistical difficulties in providing primary angioplasty services, highlighting the challenges for different geographical settings, and to assess the workforce implications, patients’ experiences and costs. Included in this interim report were some of the general observations made by the pilot sites in relation to the challenges they faced in developing their primary angioplasty services during the patient recruitment period from April 2005 to March 2006. These comments fall under the broad headings of communication, protocols, audit, workforce and funding.
51. The key findings from the NIAP interim report are:
• The development of PPCI services is feasible in a variety of geographical settings • Establishing a PPCI service requires a multidisciplinary approach and good communication between all stakeholders. • Acceptable call-to-balloon times are achievable by direct, or indirect admission to the primary angioplasty centre but the ideal is undoubtedly direct admission to the catheter laboratory at the primary angioplasty centre.
National Infarct Angioplasty Project (NIAP) Final Report
52. The final report from NIAP is in the form of guidance to the NHS 1. It examines the results of the National Infarct Angioplasty Project (NIAP) and, based on these findings and review of recent clinical trial evidence, advises on best practice for the treatment of heart attack. This advice supersedes that given on treatment of heart attacks in Chapter Three of the National Service
11

Framework for Coronary Heart Disease 5 , published in March 2000. The National Institute for Health and Clinical Excellence (NICE) is currently preparing a guideline on the management of unstable angina and non - ST elevation myocardial infarction (nSTEMI), which will update the remainder of Chapter Three. This is due for completion in December 2009.
53. How is a STEMI Treated? Because the mechanism underlying occlusion of the coronary artery is the formation of thrombus (blood clot) attention was first directed towards various drugs, which have the ability to dissolve clot, termed thrombolytic agents. In the late 1980s and through the 1990s these agents became widely prescribed, mainly by hospital staff once the patient had been admitted to hospital. Not surprisingly these agents increase the risk of bleeding and have also been shown to cause some strokes. However, this risk is outweighed by the benefits of improved survival following the heart attack. Some patients are unsuitable for thrombolysis, for instance, because they are at higher risk of bleeding, and in those who are suitable in approximately 20% to 30% of cases the artery fails to reopen following the treatment.
54. Following the publication of numerous trials, it was shown that the outcome for patients with STEMI was closely related to the length of time that the coronary artery was occluded, and the completeness of restoration of blood flow achieved with treatment. The longer the duration of occlusion, or the more incomplete the restoration of blood flow, the greater the damage to the heart muscle and the worse the patient’s outcome. This prompted the investigation of two alternative treatment options. The first involved the use of thrombolytic agents, but given before the patient arrives in hospital, known as pre-hospital thrombolysis ( PHT), with the drug usually administered by trained paramedics. This results in earlier administration of the agents and better outcome for patients. The second involved a more mechanical approach to the problem. By inserting a catheter (tube) into the body, via a peripheral artery in the groin or wrist, a balloon catheter is passed down the coronary artery and the occlusion unblocked, usually with the additional insertion of a stent (a cylindrical metallic mesh) to hold the affected area open. This technique is termed primary angioplasty, or to give it its full name primary percutaneous coronary intervention (PPCI).
55. PHT and PPCI – A Summary of the Conclusions of the Evidence to Date. Broadly speaking, whilst PHT has the advantage that it can be administered earlier than PPCI, the latter results in more reliable opening of the artery and with a lower risk of stroke and of the artery re-blocking over the next few hours or days. Also, as mentioned above, not all patients are suitable for thrombolysis and for those who are treated in this way some of the occluded arteries fail to reopen. Some of those whose arteries fail to open following thrombolysis may subsequently be treated by angioplasty, which in this setting (following thrombolysis) is termed rescue PCI. Logistically it is more difficult to undertake PPCI than deliver thrombolysis because it requires in-hospital treatment with the use of technically specialised equipment (a cardiac catheter laboratory) and highly trained staff. It is worth noting that even when thrombolysis is successful coronary reperfusion may take 30 to 90 minutes to occur after the administration of the thrombolytic agent. Many international trials have been undertaken comparing thrombolytic agents with PPCI, with the main conclusions being as follows.
56. First, PPCI reduces mortality, and improves longer term outcome compared to thrombolysis when both treatments can be undertaken within a similar time frame.
57. Second, the advantage of PPCI over thrombolysis decreases with increasing delay in undertaking the procedure. Whilst much debate still surrounds this issue it is suggested that the benefit of PPCI may be lost, or considerably reduced, if it takes more than 90 minutes longer to undertake the procedure than it would to administer a thrombolytic drug.
58. Third, more patients are potentially suitable for PPCI than thrombolysis, and PPCI is associated with fewer strokes and recurrent heart attacks during the hospital admission.
59. Fourth, the greatest delay in providing effective treatment is often the time taken for patients to recognise that they have a problem and calling for help.
12

60. The Need for Specialist Centres. As evidence of the longer-term benefits of PPCI has been steadily growing, Professor Boyle, National Director for Heart Disease and Stroke set out the clinical case for developing these services in his paper Mending Hearts and Brains 9 published in December 2006. He acknowledged however that not every hospital would be able to provide this service as it requires a cardiac catheter laboratory and highly trained staff to be available 24 hours a day and seven days a week (24/7). PPCI has therefore been identified as one of those services more appropriately provided in a specialist centre.
61. Professor Lord Darzi ‘s NHS Next Stage Review Final Report High Quality Care For All 4
published in June 2008 refers to the need to improve access to the most clinically and cost effective treatments as one way of improving service quality. The Strategic Health Authority visions for the 21st century NHS on which Lord Darzi based his final report, set out the arguments for creating specialised centres for heart attack in order to deliver better outcomes and a world-class service. NIAP has examined service delivery in detail in some existing specialised centres and the report sets out these findings.
Evaluation of the National Infarct Angioplasty Project
62. The School of Health and Related Research (ScHARR) and the Institute of Work Psychology (IWP) at the University of Sheffield were commissioned by the National Institute for Health Research NHS Service and Delivery Organisation R & D Programme to undertake an independent evaluation of the pilot sites. The evaluation was to determine the feasibility and acceptability to patients and carers of angioplasty for treatment of STEMI, to evaluate the different ways services could be organised, to investigate the organisational barriers to implementing these services and associated workforce issues and, finally, to estimate the cost effectiveness of these services in practice.
63. Findings from the evaluation report have been taken into account in the advice given in the guidance in the final report and provide the data for this impact assessment. The evaluation report is being published on the National Institute for Health Research’s Service and Delivery Organisation R & D programme website http://www.sdo.nihr.ac.uk/ on 20 October 2008 2.
64. The main findings from the evaluation were as follows.
• The NIAP hospitals varied in size, configuration, infrastructure, referral routes and activity levels.
• The NIAP hospitals treated 2072 patients (71% male, age range 24 to 104) over the evaluation year, 70% admitted directly to a primary PCI hospital and 30% transferred from a non-PCI hospital.
• Median call-to-balloon times were 87 minutes for direct to catheter laboratory, 132 minutes via coronary care, 140 minutes via the emergency department, and 161 minutes for transfers from a non-PCI hospital.
• Establishing the full 24-hour primary PCI service from the start appeared to work better than incremental expansion.
• Staff needed to work in a flexible, multi-skilled manner across traditional task boundaries.
• On-going training was required to retain experienced team members.
• Failure to harmonise staff pay and conditions before commencing the service meant inequity of reward and rest after out-of-hours working.
• Primary PCI required simple direct access for patients and good teamworking across professional boundaries.
13

• Building and maintaining relationships with key stakeholders was critical to service development and sustainability.
• Regular audit of the heart attack pathway identified blockages limiting the capacity of the system.
• Development of primary PCI may have been associated with knock-on effects upon elective services and particularly upon rehabilitation.
• Patients and carers reported high overall levels of satisfaction with NIAP and control care (patients 78% v 71% excellent (p=0.074), carers 63% v 55% (p=0.049)).
• Patients at NIAP sites reported higher levels of satisfaction than control sites with the time waited and the efficiency of treatment (80% v 67% excellent (p<0.001) and 83% v 74% (p=0.009)).
• Satisfaction with information given on how to manage the condition in future was lower in NIAP than control sites (38% v 46% excellent (p=0.049)).
• The mean cost of the treatment episode was £3,509 for thrombolysis at control sites, £4,361 for thrombolysis at NIAP sites, and £5,176 for PPCI at NIAP sites.
• Primary PCI-based care was more expensive than thrombolysis-based care but at £4520 per quality-adjusted life year gained would be considered cost-effective.
• Direct access to the primary PCI hospital catheter laboratory was most likely to be cost-effective, whereas thrombolysis-based care was dominant when analysis was limited to those transferred from a non-PCI centre.
Assessing the effectiveness of primary angioplasty compared to thrombolysis and its relationship to time delay. Bravo Vergel et al (the York Model) 10
65. In terms of clinical effectiveness, a recent UK study by Bravo Vergel et al 10. (referred to in the evaluation report as the York model) compared primary PCI to thrombolysis, based on synthesis of clinical trials to estimate short term event rates which were then extrapolated over the longer term to estimate costs and benefits.
66. The conclusion of Bravo Vergel et al was “The benefit of primary angioplasty, over thrombolysis, depends on the former’s additional time delay. For delays between 30 and 90 minutes, angioplasty is superior, on average, for 1-month fatal and non-fatal outcomes. Thrombolysis may be the preferred option in terms of 6-month mortality only for delays at around 90 minutes and beyond but there is considerable uncertainty for longer time delays.”
67. The York model provided a model of the potential cost-effectiveness of PCI based upon data from randomised trials. The NIAP evaluation provided an opportunity to populate this model with real-life data from a representative sample of UK NHS acute hospitals. In doing this the evaluation report needed to develop specific aspects of the model so that it more accurately reflected routine access to the primary PCI hospital catheter laboratory.
68. Bravo Vergel et al summarise the estimated absolute probabilities of the occurrence of death and subsequent events 1 month or 6 months after angioplasty or thrombolytic therapy (mean and 95% CrI), together with the odds ratios (95% CrI) comparing primary angioplasty and thrombolysis and probabilities that angioplasty is superior. The results are for the average observed ‘angioplastyrelated time delay’ (i.e. 54.3 minutes).
14

Myocardial Ischaemia National Audit project (MINAP)
69. MINAP was established in 1999, in response to the national service framework (NSF) for coronary heart disease, to examine the quality of management of heart attacks in hospitals in England and Wales.
70. The project uses a highly secure electronic system of data entry, transmission and analysis developed by the Central Cardiac Audit Database (CCAD). This system uses encryption of patient identifiers to allow secure transfer of data between hospitals and central servers and allows linkage with the Office of National Statistics for tracking of mortality.
71. Initially the project focused on the hospital management of heart attack (STEMI). However the dataset has been expanded to cover other acute coronary syndromes (ACS) and the introduction of pre-hospital thrombolysis and primary percutaneous intervention. All hospitals in England and Wales that admit patients with acute coronary syndromes contribute data.
British Cardiovascular Intervention Society Audit Database
72. Data were provided from the audit database to check the number of heart attacks reported through MINAP and obtain an up-to-date assessment of the number of PPCIs undertaken in England in 2007.
Key assumptions
73. The analysis was based on presentation of heart attacks to providers in England only. It therefore excludes English residents who may attend hospitals elsewhere when they have a heart attack.
74. The number of STEMI heart attacks was obtained from the MINAP database for 2007. It is estimated that MINAP underreports heart attacks by around 5% and the MINAP figure has been increased by 5% of the reported numbers.
75. The number of people currently receiving Primary PCI, either at NIAP sites are in other places opportunistically, was taken from the BCIS audit database in order to calculate the net potential increase in people who would become eligible for PPCI.
15

76. Eligible population for PPCI – it was assumed that 97.6% of the population would live in areas which could be served by high quality PPCI centres and that 2.6% would be unable to access a PPCI service.
77. Of the eligible population, 95% of people presenting with heart attack (STEMI) would be given PPCI and that 5% would be contraindicated.
78. It was assumed that no additional cath lab capacity would be required across the country to implement PPCI.
79. The SCHARR/IWP report 2 identified the average cost of current treatment (in non-PPCI sites) and the average cost of offering a PPCI service at the NIAP sites. These average costs were built up from a detailed assessment of unit costs. It is assumed that these average costs can be applied across the country in making this national NHS assessment of costs and benefits.
80. The average costs included unit costs for Drug Eluting Stents (DES) of just under £640 and for bare metal stents £220 (a difference of £420). A recent NICE report 12 issued guidance which defines more precisely the circumstances in which DES should be used and that the additional cost of DES over bare metal stents in £300 or less. Given that DES are used in both current treatment (for PCI post thrombolysis) and in PPCI this change is not considered material.
81. The difference in outcomes between people receiving thrombolysis and people in the NIAP PPCI group will apply to all cases of heart attack (STEMI) with full implementation of infarct angioplasty. This is a conservative assumption because some of the people in the NIAP PPCI group had lengthy time delays. This was partly because of the learning curve that organisations were moving through as they implemented PPCI. Longer time delays were more marked if people came via or past another hospital and came to the service via the Emergency Department rather than direct to the Cath Lab. The guidance stresses the importance of devising services which are able to meet the required times, with suggestions about how this can be best achieved. The outcome benefits of actual implementation may well be better than those summarised in this Impact Assessment.
16

Treatment for Heart Attack – Current Provision, Stakeholders & Future Numbers Current Service Arrangements & Key Stakeholders
82. The recommended treatment for heart attacks included within the NSF for CHD 5 was thrombolysis. In most parts of the country this is still the first line treatment provided. People with heart attacks are taken by ambulance, or turn up unaided or with relatives/friends to acute hospitals throughout the country. If they come by ambulance, those with STEMIs may receive pre-hospital thrombolysis, if not they are likely to receive thrombolysis when they reach hospital. People having thrombolysis may proceed to have an angiogram and/or a PCI or a CABG following assessment and investigation.
83. The results of the evaluation and the national guidance indicate that the preferred pattern in future is for people having heart attacks (STEMI) to be taken the centres which have sufficient cases on a 24 hour a day/7 day a week basis to provide a high quality PPCI service.
84. This in turn means that the number of hospitals to which people are taken, or recommended to go to, when they have a heart attack will reduce across the country. The precise configuration will be determined by the key stakeholders in each cardiac network. They will work together to review the numbers of expected cases, transport times and local infrastructure to arrive at a solution which delivers PPCI within the recommended timescales and delivers the improved outcomes indicated by the evidence base.
85. The key stakeholders are therefore • people suffering a heart attack, • ambulance services (including air ambulances – voluntary sector but subcontracted by an ambulance service), • Acute trusts, • Primary Care Trusts (PCTs) as commissioners; and • Strategic Health Authorities (SHAs). • Other stakeholders include the British Cardiovascular Society (BCS), the British Cardiovascular Intervention Society, the National Institute for Health and Clinical Excellence (NICE) and the British Heart Foundation (public education).
Stakeholders for whom there is a financial impact
86. The following sub-set of stakeholders will experience a financial impact in the implementation of this guidance.
87. PCTs as commissioners who will need to specify their service requirements and change their commissioning arrangements and financial flows to match the new model of service.
88. Ambulance Services – there will be longer journeys for some patients and more transfers. These will have a marginal cost impact as they already have crew and ambulances but may need some additions for backfilling. There will be a reduction in use of thrombolysis in most areas. The impact of training and retraining is likely to be marginal as they already provide training, but the content may need to be changed and more crew may need training. Telemetry is additional but not essential and the DH has already put funding in for this as part of the pre-hospital thrombolysis programme.
89. Acute trusts without cath labs. There will be a small saving from not doing thrombolysis but increases in training and retraining. These Trusts will also cease to admit people with heart attacks (STEMI) but may admit the same people post PPCI if patients are transferred back to their local area.
17

90. Acute trusts with day time service. It is recommended that centres offering PPCI do so on a 24 hour basis but in some places service models may be adopted where a day time PPCI service is operated. Facilities and staff are already there and undertaking elective work for STEMI and NSTEMI heart attacks. There may be less elective STEMI PCI. Any spare cath lab capacity will be available for the increasing volumes of electrophysiology/arrhythmia work.
91. Acute trusts with 24/7 PPCI services – it is assumed that no new cath lab facilities will be required. However, the impact is in increased costs for out of hours work, for running facilities more intensively and for the drugs and cath lab consumables required for undertaking PPCI. All of these items are factored into the cost assessment made by the SCHARR/IWP evaluation 2 and the costs associated with providing a PPCI service.
Number of People Having Heart Attacks & Potentially Eligible for PPCI
92. The MINAP database received details of 60,391 heart attacks in 2007, of which 24,350 were STEMIs. This is estimated to be 5% less than the actual total, so for this assessment the numbers were uplifted to 63,411 heart attacks of which 25,568 were estimated to be STEMIs. It is estimated that 78% of these had reperfusion therapy (either thrombolysis or PPCI).
93. The total number of people in England potentially eligible for PPCI was derived by assuming that all of those currently receiving reperfusion would be eligible plus a further 7.5% of the total who are not suitable for thrombolysis but would be suitable for PPCI. This total number eligible for PPCI is 20,801. In 2007, the BCIS database received details of 4,784 people having a PPCI and it has therefore been assumed that a further 16,017 would have been potentially eligible for PPCI (20,801 less 4,784) in 2007.
94. Heart attacks (STEMI) have been reducing as a percentage of total heart attacks – the reduction is thought to have equated to 1-2% per year. For sensitivity testing, the impact the 16,071 above has been reduced by 1.5% per year over the 5 years which have been assessed to identify the impact if this reduction continues into the future.
95. The distance which people with a heart attack (STEMI) have to travel to receive PPCI is crucial to the delivery of better outcomes. If travel times are too long the benefits will not be delivered and there are parts of England which will potentially not be able to receive PPCI because they will be too far from high quality centres. An initial assessment has therefore been made of those parts of the country which may not be able to access PPCI in the first 3-5 years of implementation. This suggests that there may be 2.6% of the England population and 3.8% of the heart attack STEMI cases which will continue to receive thrombolysis followed by angiography and PCI or CABG. These areas are summarised in the following table.
SHA AREA/TRUST Population at Risk South West North Devon 79,000
West Dorset & Dorset County 67,000 West Midlands Shropshire 85,000
Herefordshire 68,000 East Midlands Lincolnshire 280,000 Yorkshire & Humber Scarborough plus 120,000 North West Cumbria 300,000
Morecambe Bay 330,000 Total 1,329,000
England Total Population 50,500,000 % Outside PPCI range 2.6%
18

96. The impact of this reduction is to reduce the number of heart attacks (STEMI) which would be eligible to receive PPCI to 15,045 heart attacks.
97. In addition, not all people who arrive at a hospital with a heart attack (STEMI) will be suitable for PPCI and as a result it has been assumed that 5% (752) of the 15,045 will receive other care and treatment, leaving 14,293 eligible and suitable for PPCI.
98. The projected numbers of cases eligible and suitable for PPCI are shown in the following table on two bases, the first at stable numbers of STEMIs and the second with a 1.5% reduction per year. It is also assumed that full implementation will require 3 years and that around one third of eligible and suitable heart attacks (STEMI) will receive PPCI in year 1 (2009), two thirds in year 2 (2010) and all of them in year 3 (2011).
Year STEMI Reduces 1.5% year on year Stable Numbers of STEMI Total
STEMI (1) STEMI Receiving
PPCI Total
STEMI (1) STEMI Receiving
PPCI Year 1 – 2009 13,867 4,866 14,293 4,764 Year 2 – 2010 13,659 9,245 14,293 9,528 Year 3 – 2011 13,454 13,454 14,293 14,293 Year 4 - 2012 13,252 13,252 14,293 14,293 Year 5 - 2013 13,054 13,054 14,293 14,293
Total (Over 5 Years) 67,287 53,871 71,465 57,171
19

Assessment of Costs & Benefits Costs of Providing PPCI Services
99. The SCHARR/IWP evaluation report 2 included an economic assessment of the PPCI services provided by the NIAP sites, compared with control sites offering predominantly thrombolysis led services. Full details are available in their report.
100. Costings were undertaken of the immediate treatment received by people having a heart attack (STEMI) and all treatments received over a period of 6 months following the heart attack. This enabled the two options to be costed more appropriately because many people who start off by having thrombolysis eventually receive PCI or CABG on an elective basis.
101. The factors which were taken into account in costing the services were as follows:
• All Drugs used people having PPCI and Thrombolysis • Tests and Interventions • Hospital stays • Ambulance Journeys • Staff Costs per Minute • Cath Lab Operating Costs per Minute • PPCI Consumables
102. A full list of the unit costings within each of these categories is included in Annex 2. The mean costs and 95% confidence limits for the full costs of treatment (rather than just the initial intervention) are shown in the following table.
Control NIAP
Costs 10,700
[8010, 16,100]
11,600
[8810, 17,200]
QALYs 6.40
[5.82, 6.96]
6.58
[6.01, 7.15]
Diff costs 829
[130, 1440]
These mean costs of £11,600 per person treated for systems offering PPCI and £10,700 per person treated for systems continuing with the current services have been used to calculate the savings and costs and the resulting net increase in expenditure. This net increase is £900 per case.
Costs and Savings/Benefits of Proposals 103. All costs and benefits presented here are for England only, and costs and savings are at 2007/8
prices discounted at 3.5% per annum in line with HMT Green Book.
Total costs 104. Calculation of the total annual cost at full implementation, assumes that 97.4% of the eligible
population can be covered by a PPCI service and that 95% of this eligible population receive PPCI. These costs are based on an estimated increase of 13,454 receiving infarct angioplasty in year 3 with reducing STEMI numbers and 14,293 people with heart attacks (STEMI) receiving infarct angioplasty per year with stable STEMI numbers.
105. The increase in cost to the NHS arises from introducing PPCI at selected sites across the country – identified by commissioners and cardiac networks. This increase in cost is estimated to be £145.7m (NPV) in the first full year (year 3) for reducing STEMI numbers and £154.8m (NPV) for stable
20

STEMI numbers. These sites will all be undertaking PCI already and therefore the change in practice will not require changes in physical infrastructure.
Total savings 106. The savings to the NHS will come from discontinuing current treatment i.e. thrombolysis, followed
by angiography for around 60% and PCI or CABG for some of those at a later data. The savings in the first full year (Year 3) are estimated to be £134.4m (NPV) with reducing STEMI numbers and £142.8m (NPV) with stable STEMI numbers.
Total Net Costs 107. The following table shows the increase in costs, savings and the net cost at 2007/8 price base and at
NPV (discounted by 3.5% in line with HMT Green Book) which has been calculated by multiplying the additional cost (2007/8 price base) of PPCI by the number of people who will receive PPPC. This is shown for the reducing STEMI and stable STEMI numbers.
Year 1 Year 2 Year 3 Year 4 Year 5 Total £m £m £m £m £m £m
Reducing STEMI
Full Cost at 2007/8 Price Base 53.6 105.6 156.1 153.7 151.4 620.5
Full Savings at 2007/8 Proce Base 49.5 97.4 144.0 141.8 139.7 572.3
Net Cost at 2007/8 Price Base 4.2 8.2 12.1 11.9 11.7 48.1
Full Cost – NPV 53.6 102.1 145.7 138.7 132.0 572.0
Full Savings – NPV 49.5 94.1 134.4 127.9 121.7 527.6
Net Cost – NPV 4.2 7.9 11.3 10.8 10.2 44.4 Stable STEMI
Full Cost at 2007/8 Price Base 55.3 110.5 165.8 165.8 165.8 663.2
Full Savings at 2007/8 Proce Base 51.0 102.0 152.9 152.9 152.9 611.7
Net Cost at 2007/8 Price Base 4.3 8.6 12.9 12.9 12.9 51.5
Full Cost – NPV 55.3 106.8 154.8 149.5 144.5 610.9
Full Savings – NPV 51.0 98.5 142.8 137.9 133.3 563.5
Net Cost – NPV 4.3 8.3 12.0 11.6 11.2 47.4
108. Overall the net cost of implementing this guidance is £12.1 (at 2007/8 price base) if there is a year on year reduction of 1.5% in heart attack (STEMI) numbers and £12.9 million (at 2007/8 price base) in the first year of full coverage (2011) if heart attack (STEMI) numbers remain stable.
Improved Outcomes from Providing PPCI Services
109. The main areas in which outcomes is better with PPCI compared with thrombolysis are in relation to reduced deaths at 1 month and 6 months, reduced reinfarctions at 6 months for people who have
21

already had a heart attack and reduced strokes at 6 months for people who have already had a heart attack.
110. The differences in rates calculated and reported in the SCHARR/IWP evaluation report are shown in the following table.
Probabilities of Short Term nd Points 95%
Confidence 95% CI 95% CI Mean Intervals Low High
STEMI Patients Treated Thrombolysis
7.59% [0.0743, 7.43% 7.76% Dead 1 month 0.0776]
8.95% [0.0757, 7.57% 13.10% Dead 6 months 0.131]
7.62% [0.0662, 6.62% 10.70% MI 6 months 0.107]
2.67% [0.0112, 1.12% 6.72% Stroke 6 months 0.0672]
NIAPP PCI 5.92% [0.0381, 3.81% 8.70%
Dead 1 month 0.0870] 7.19% [0.0432, 4.32% 12.10%
Dead 6 months 0.121] 2.94% [0.0155, 1.55% 5.55%
MI 6 months 0.0555] 0.73% [0.0023, 0.23% 1.87%
Stroke 6 months 0.0187]
111. The outcomes are consistently better for the NIAP PPCI group than for those having thrombolysis, with one exception which is the 95% upper confidence limit for the probability of death within one month.
112. These differences in outcomes post intervention have been used to assess the differences in the number of people with poorer outcomes which would follow from the introduction of PPCI treatment, compared with a thrombolysis based service. The assessments for the stable STEMI numbers and reducing STEMI numbers are shown in the following table.
Difference in Outcomes between NIAP PPCI & Thrombolysis – Probabilities of death, subsequent heart attack and subsequent stroke in Year 3
Stable Numbers of STEMI STEMI Reduces 1.5% year on year
Mean 95% CI Mean 95% CI 95% CI Probability 95% CI Low High Probability Low High
Died within 1 month 239 517 -134 225 487 -126 Died within 6 months 252 465 143 237 437 135 Heart Attack 6 months 669 725 736 630 682 693 Stroke 6 months 278 127 693 261 120 653
For the first full year of operation (Year 3 undiscounted) compared with current treatment, PPCI would be expected to result in
• 239 fewer deaths within 1 month for stable STEMI numbers and 225 fewer deaths with reducing numbers of STEMIs. • 252 fewer deaths within 6 months for stable STEMI numbers and 237 fewer for reducing numbers of STEMIs • 669 fewer subsequent heart attacks for stable STEMI numbers and 630 fewer for reducing numbers of STEMIs
22

• 278 fewer subsequent strokes for stable STEMI numbers and 261 fewer for reducing numbers of STEMIs.
113. The SCHARR/IWP evaluation 2 calculated the quality adjusted life years (QALY) gained using probabilities of the outcomes reported above – based on the characteristics and experience of the NIAP PCI group compared with those having thrombolysis. They also calculated the ICER. The results for both QALY gain (discounted) and ICER are shown in the following table.
Lower Confidence Upper Confidence Mean Limit (95%) Limit (95%)
Diff QALYs 0.183 -0.0764 0.415
ICER 4520
114. The SCHARR/IWP evaluation 2 calculates the probability that treatment with PCI based care, as used in the NIAP hospitals, would be cost effective across a range of values that a decision maker might be willing to pay for an additional QALY. At a willingness to pay (WTP) of £20k per QALY, the probability that NIAP would be cost effective is approximately 0.9.
115. The difference in QALYs between the NIAP PCI group compared with those having thrombolysis was used to calculate the total QALY gain and the cost per QALY. The following table shows the QALY gain in year 3 at full implementation for stable STEMI numbers and STEMIs reducing by 1.5% per year.
116. In the third (full) year of implementation the QALY gain (discounted) with reducing numbers of STEMI is 2,390 and with stable numbers of STEMI is 2,539.
117. For the mean QALY gain, the cost per QALY gained is calculated as £5,067 (discounted). This compares very favourably with the social value of £40,000 used by the Department of Health.
23

Specific Impact Tests: Checklist
Use the table below to demonstrate how broadly you have considered the potential impacts of your policy options.
Ensure that the results of any tests that impact on the cost-benefit analysis are contained within the main evidence base; other results may be annexed.
Type of testing undertaken Results in Evidence Base?
Results annexed?
Competition Assessment No Yes Small Firms Impact Test No Yes Legal Aid No Yes Sustainable Development No Yes Carbon Assessment No Yes Other Environment No Yes Health Impact Assessment Yes No Race Equality No Yes Disability Equality No Yes Gender Equality No Yes Human Rights No Yes Rural Proofing No Yes
Annexes
Annex 1: Specific Impact Tests
Competition Assessment
118. The heart attack (STEMI) treatment guidance will not have any major impact on competition.
Small Firms Impact Test
119. The heart attack (STEMI) treatment guidance will not have a major impact on small firms. There may be two marginal effects. The first because people who work for small firms have heart attacks like everyone else. This new guidance will reduce the time lost off work from ill health and the loss of employees due to death by a small amount. The second because a reduction in the number of people who have a stroke subsequent to their heart attack may reduce the number of people requiring nursing home care in the future.
Legal Aid 120. The heart attack (STEMI) treatment guidance will not have any impact on Legal Aid
Sustainable Development
24

121. The heart attack (STEMI) treatment guidance takes account of and supports the five principles of sustainable development: o Living within environmental limits; o Ensuring a strong, healthy and just society; o Achieving a sustainable economy; o Promoting good governance; and o Using sound science responsibly.
Carbon Assessment and Other Environment
122. The heart attack (STEMI) treatment guidance will have a low impact on carbon and other environmental considerations. The Treasury Green book notes that in cases where quantification is impractical, a qualitative assessment of the policy is appropriate. The heart attack treatment guidance includes recommendations for specialist PPCI centres and as a result a proportion of patients may travel further for the most appropriate treatment. The increased distance of ambulance travel is offset by the substantial outcome benefits for heart attack patients who are treated in specialist centres.
Health Impact Test
123. The sole purpose of the heart attack (STEMI) treatment guidance is to improve outcomes. This is reflected throughout the main body of the Impact Assessment. The heart attack treatment guidance will help reduce health inequalities by recommending standard evidence based treatment for all patients having a heart attack (STEMI).
Single Equality Impact Assessment
124. This document is accompanied by a Single Equality Impact Assessment which examines the impact of the guidance on race, disability, gender and human rights.
Rural Proofing
125. The heart attack treatment guidance recognises the importance of developing high quality heart attack (STEMI) treatment that can be accessed by as many individuals as possible, including those in rural areas. It is designed to offer guidance for local commissioners and providers to develop services that meet local needs.
126. However, a critical factor in the guidance is the time taken between a call for help and treatment being given. This is recommended to be within 120 minutes. In some parts of the country this may not be feasible because of the distance from sparser populations and high quality centres which can deliver this treatment.
127. An initial assessment has been made of the areas where delivering the service may be difficult due to the distances to be travelled. The areas where this may be difficult are shown in the following table.
25

SHA Trust Population South West North Devon - Part 79,000
Dorset - Part 67,200 West Midlands Herefordshire - Part 67,600
Shropshire - Part 85,000 East Midlands Lincolnshire - Part 282,000 Yorkshire & Humber Scarborough & Eastern Yorkshire - Part 122,400 North West North Cumbria 301,000
Morecambe Bay & surrounding area 333,000 Total 1,337,200
This combined population across the country of just over 1.3 million represents 2.6% of the population. Despite this assessment local commissioners and cardiac networks are recommended to identify solutions to enable these populations to access PPCI. If this is not possible they will be treated with thrombolysis plus angiography for some and PCI or CABG for some at a later date.
Impact on the Admin Burdens Baseline
128. This strategy will not have any impact on administrative or regulatory burden. Coronary Heart Disease services already feature in the Healthcare Commission’s inspections and there are no explicit plans to change this as a result of this guidance. MINAP collects data on all heart attacks and the treatment that is given and BCIS audit collects data on all angioplasties. These data collections will continue and will be a source of routinely collected data to assist with the evaluation of the implementation of the guidance in 3 years time.
Annex 2: Unit Costs Used for Costing
Unit Costs for Assessing Current Service Model and PPCI Model
129. The evaluation report assembled unit costs for the different service elements associated with the current model of service and the NIAP PPCI sites. These are set out in the SCHARR/IWP evaluation report 2 and are reproduced in the following table.
Name Cost Notes Source
Drugs
Thrombolytic drug Streptokinase 81.18 1.5 million-unit vial = £81.18 Myocardial infarction, initiated within 6–12 hours, 10 mg by intravenous injection, followed by intravenous infusion of 50 mg over 60 minutes, then 4 infusions each of 10 mg over 30 minutes (total dose 100 mg over 3 hours; max. 1.5 mg/kg in patients
BNF (2007)
Actilyse (Alteplase rtPA) 735
less than 65 kg). Assume 1x10mg vial (£135), 2x50mg vials (£300 each) Injection , powder for reconstitution, reteplase 10 units/vial, net price pack of 2 vials (with 2 prefilled syringes of diluent and transfer device) = £666.11. Dose is 10 units over not more than 2 minutes,
BNF (2007)
Rapilysin (Reteplase RPA)
Metalyse (tenecteplase TNK)
666.11
612.5
followed after 30 minutes by a further 10 units net price 40-mg (8000-unit) vial = £612.50; 50-mg (10 000-unit) vial = £612.50
BNF (2007)
BNF (2007)
26

Non proprietary heparin, 24 hours, 1ml amp (£0.36) followed by 24 hours at 18 units per kg/hr = 5ml
Unfractionated heparin 4.04 vial (£.68) BNF (2007) Low molecular weight Assume Clexane, 8000 unit syringe heparin 21.6 (£5.40) for 75kg, for days (4 doses) BNF (2007)
Thienopyridine platelet inhibitor clopidogrel 35.31 Plavis, 75mg x 28 tab pck BNF (2007)
initial 250 micrograms per kg (=18.75 milligrams) then 125 nanograms/kg/minute for 12 hrs (=6.75 milligrams): total 25.5
abciximab milligrams. Vial is 10 milligrams so 3 IV 2b/3a Agent (ReoPro®) 781.2 vials needed. BNF (2007)
Angiotensin II Blocker Losartan, cozaar, 50mg - 28 tabs = (ARB) losartan (COZAAR). 18.09 £18.09 BNF (2007)
net price 250mg vial =£310, initially by intravenous injection, 750 micrograms/kg then by intravenous infusion 1.75 mg/kg/hour for up to 4 hours after procedure. We assume 2 hours infusion, 75kg weight and vials split between initial injection and
Bivalirudin Angiox 620 subsequent infusion BNF (2007)
Tests NHS reference costs 2006/7 TDADS
Exercise Test 59 DA15 NHS reference costs 2006/7 TDADS
Echocardiography 58 DA02 NHS reference costs 2005/6 TRADIO RBJ1 (£303) inflated by 3% based on
Radionuclide Study 312.09 price index (Curtis 2007) NHS reference costs 2005/6 TRADIO RBF2 (£251) inflated by 3% based
Angiography 258.53 on price index (Curtis 2007) NHS reference costs 2006/7 TEI, EA14Z, Coronary Artery Bypass Graft
CABG 7976 (First Time) NHS reference costs 2006/7 TEI, EA32Z, Percutaneous Coronary Intervention (0-2 stents) and
PCI 2534 Catheterisation
Hospital stay NHS reference costs 2006/7,'XC06ZTHE, 'Intensive Therapy Unit / Intensive Care Unit:1
Day on ITU 990 Organs Supported, TCCSAL NHS reference costs 2006/7, CC7,
Day on CCU 450 Coronary Care Unit, TCORCU NHS reference costs 2006/7, 'XC06ZHDU, 'High Dependancy
Day on HDU 657 Unit:1 Organs Supported, TCCSAL NHS reference costs 2006/7 in Curtis
Day on Acute Ward 223 (2007) NHS reference costs 2006/7, 'LC02A, 'Haemodialysis/Filtration 19 years and over, TRENAL (NOTE: we assume this cost is added to a stay
Day on dialysis 381 on a general ward)
Ambulance journeys NHS reference costs 2006/7 TUPAR(EM), Emergency
Paramedic emergency transfer 247 Transfers/Urgents, PSETU
Staff costs per minute
Curtis 2007, per minute, patient related excluding qualifications,
Cardiologist in hours 2.53 medical consultant
out of hours 2.53
27
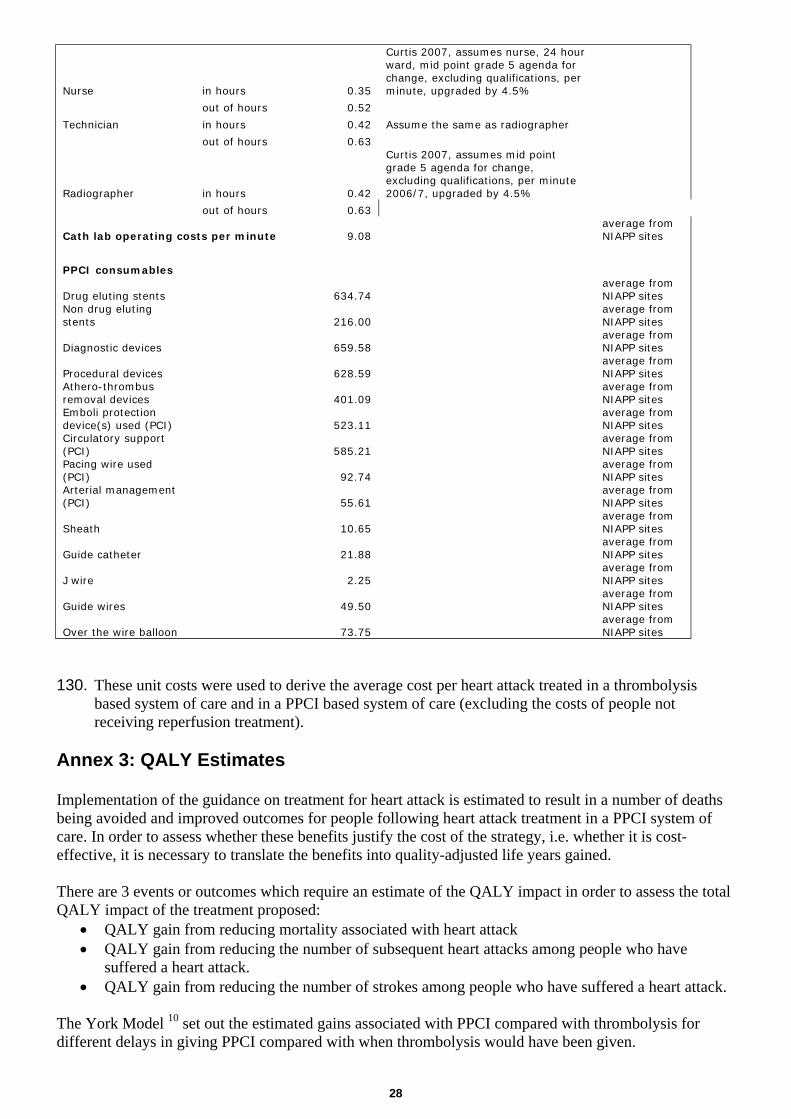
Curtis 2007, assumes nurse, 24 hour ward, mid point grade 5 agenda for change, excluding qualifications, per
Nurse in hours 0.35 minute, upgraded by 4.5%
out of hours 0.52
Technician in hours 0.42 Assume the same as radiographer
out of hours 0.63 Curtis 2007, assumes mid point grade 5 agenda for change, excluding qualifications, per minute
Radiographer in hours 0.42 2006/7, upgraded by 4.5%
out of hours 0.63 average from
Cath lab operating costs per minute 9.08 NIAPP sites
PPCI consumables average from
Drug eluting stents 634.74 NIAPP sites Non drug eluting average from stents 216.00 NIAPP sites
average from Diagnostic devices 659.58 NIAPP sites
average from Procedural devices 628.59 NIAPP sites Athero-thrombus average from removal devices 401.09 NIAPP sites Emboli protection average from device(s) used (PCI) 523.11 NIAPP sites Circulatory support average from (PCI) 585.21 NIAPP sites Pacing wire used average from (PCI) 92.74 NIAPP sites Arterial management average from (PCI) 55.61 NIAPP sites
average from Sheath 10.65 NIAPP sites
average from Guide catheter 21.88 NIAPP sites
average from J wire 2.25 NIAPP sites
average from Guide wires 49.50 NIAPP sites
average from Over the wire balloon 73.75 NIAPP sites
130. These unit costs were used to derive the average cost per heart attack treated in a thrombolysis based system of care and in a PPCI based system of care (excluding the costs of people not receiving reperfusion treatment).
Annex 3: QALY Estimates
Implementation of the guidance on treatment for heart attack is estimated to result in a number of deaths being avoided and improved outcomes for people following heart attack treatment in a PPCI system of care. In order to assess whether these benefits justify the cost of the strategy, i.e. whether it is cost-effective, it is necessary to translate the benefits into quality-adjusted life years gained.
There are 3 events or outcomes which require an estimate of the QALY impact in order to assess the total QALY impact of the treatment proposed:
• QALY gain from reducing mortality associated with heart attack • QALY gain from reducing the number of subsequent heart attacks among people who have
suffered a heart attack. • QALY gain from reducing the number of strokes among people who have suffered a heart attack.
The York Model 10 set out the estimated gains associated with PPCI compared with thrombolysis for different delays in giving PPCI compared with when thrombolysis would have been given.
28

The results from the York model 10 were applied to the NIAP site data and the following table summarises the estimated differences in outcome comparing the probabilities of short term end points for people receiving thrombolysis, people having PPCI in the control group and people having PPCI in the NIAP group. The following table summarises the probabilities.
Probabilities of short-term endpoints, means and 95%-CI – Base case
Dead (1 month) Dead (6 months) MI (6 months) Stroke (6 months) Thrombolysis 0.0759
[0.0743, 0.0776] 0.0895
[0.0757, 0.131] 0.0762
[0.0662, 0.107] 0.0267
[0.0112, 0.0672] Control PPCI 0.0510
[0.0338, 0.0725] 0.0619
[0.0385, 0.101] 0.0276
[0.0156, 0.0495] 0.0069
[0.0022, 0.0178] NIAPP PCI 0.0592
[0.0381, 0.0870] 0.0719
[0.0432, 0.121] 0.0294
[0.0155, 0.0555] 0.00727
[0.0023, 0.0187]
These differences are factored into the QALY estimates undertaken by SCHARR/IWP based on the York Model populated with data from the NIAP sites.
Discounting
A discounting rate of 1.5% was applied, which is standard DH practice for QALY gains.
References
1 Treatment of Heart Attack – National Guidance. Final report of the National Infarct Angioplasty Project (NIAP) (Department of Health. October 2008).
2 Evaluation of the National Infarct Angioplasty Project. Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation R&D (NCCSDO)R. SCHARR/IWP (October 2008).
3 Our NHS Our Future: NHS next stage review. Interim Report (Department of Health. October 2007).
4 High quality care for all: NHS Next Stage Review Final Report (CM 7432, June 2008) 5 The National Service Framework for Coronary Heart Disease (Department of Health. March
2000). 6 Myocardial Ischaemia National Audit Project (MINAP). 7 Department of Health. Review of Early Thrombolysis (June 2003). 8 National Infarct Angioplasty Project (NIAP) Interim Report (Department of Health. February
2008) 9 Mending hearts and brains – clinical case for change: Report by Professor Roger Boyle,
National Director for heart disease and stroke (Department of Health. December 2006). 10 Asseburg C, Bravo Vergel Y, Palmer S, Fenwick E, de Belder M, Abrams K and Sculpher M.
Assessing the effectiveness of primary angioplasty compared to thrombolysis and its relationship to time delay: a Bayesian evidence synthesis. Heart 2007;93:1244-50.
11 HM Treasury. The Green Book. Appraisal and Evaluation in Central Government. 12 2008/009 NICE appraisal of drug eluting stents for the treatment of coronary artery disease.
(NICE, February 2008).
29