dental implants in irradiated versus nonirradiated ... · dental implants in irradiated versus...
TRANSCRIPT

CLINICAL REVIEW David W. Eisele, MD, Section Editor
Dental implants in irradiated versus nonirradiated patients: A meta-analysis
Bruno Ramos Chrcanovic, DDS, MSc,1* Tomas Albrektsson, MD, PhD,1,2 Ann Wennerberg, DDS, PhD1
1Department of Prosthodontics, Faculty of Odontology, Malm€o University, Malm€o, Sweden, 2Department of Biomaterials, G€oteborg University, G€oteborg, Sweden.
Accepted 17 September 2014
Published online 16 June 2015 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/hed.23875
ABSTRACT: The purpose of the present meta-analysis was to test thenull hypothesis of no difference in dental implant failure rates, postopera-tive infection, and marginal bone loss for patients being rehabilitated bydental implants and being previously irradiated in the head and neckregion versus nonirradiated patients against the alternative hypothesis of adifference. The study suggests that irradiation negatively affects the sur-vival of implants, as well as the difference in implant location (maxilla vsmandible), but there is no statistically significant difference in survivalwhen implants are inserted before or after 12 months after radiotherapy.
The study failed to support the effectiveness of hyperbaric oxygen therapyin irradiated patients. It was observed that there was a tendency of lowersurvival rates of implants inserted in the patients submitted to higher irra-diation doses. The results should be interpreted with caution because ofthe presence of uncontrolled confounding factors in the included studies.VC 2015 Wiley Periodicals, Inc. Head Neck 38: 448–481, 2016
KEY WORDS: dental implants, radiotherapy, infection, marginal boneloss, meta-analysis
INTRODUCTIONIn an attempt to decrease implant failure rates, moreattention is being placed on understanding the etiologicand risk factors that lead to the failure of dentalimplants.1 The question of whether or not patients irradi-ated in the head and neck region are more at risk of los-ing dental implants has been receiving increasingattention in the last years, as implants have been increas-ingly used in patients with oral cancer.
Radiotherapy is largely used for the treatment of headand neck cancer, as primary therapy, adjuvant to surgery,as well as in conjunction with concurrent chemotherapy, oras palliative treatment for late stage and untreatable headand neck malignancies. Although the radiotherapy canincrease cure rates, the irradiated patient is susceptible tosecondary effects and a series of potential orofacial compli-cations. Radiotherapy may result in progressive fibrosis ofblood vessels and soft tissues, in xerostomia, in osteoradio-necrosis, and in reduction of bone-healing capacity, amongothers.2–4 Because of the cumulative effects of radiation onbone vascularity, the regenerative capacity of these tissuesis limited, and this may have a deleterious impact on subse-quent implant osseointegration.5
The ability to anticipate outcomes is an essential partof risk management in an implant practice. Recognizing
conditions that place the patient at a higher risk of failurewill allow the surgeon to make informed decisions andrefine the treatment plan to optimize the outcomes.1 Theuse of implant therapy in special populations requiresconsideration of potential benefits to be gained from thetherapy. To better appreciate this potential, we conducteda systematic review and meta-analysis to compare the sur-vival rate of dental implants, postoperative infection, andmarginal bone loss of dental implants inserted in irradi-ated and nonirradiated patients.
MATERIALS AND METHODSThis study followed the Preferred Reporting Items for
Systematic reviews and Meta-Analyses (PRISMA) state-ment guidelines.6 A review protocol does not exist.
Objective
The purpose of the present review was to test the nullhypothesis of no difference in the implant failure rates,postoperative infection, and marginal bone loss forpatients being rehabilitated by dental implants and beingirradiated or previously irradiated in the head and neckregion versus nonirradiated patients against the alternativehypothesis of a difference.
Search strategies
An electronic search without time or language restric-tions was undertaken in April 2014 in the following data-bases: PubMed, Web of Science, and the Cochrane OralHealth Group Trials Register. The following terms wereused in the search strategy on PubMed: ((dental implant[Text word]) AND irradiated [Text word]); (dental implant[Text word]) AND radiotherapy [Text word]); (dental
*Corresponding author: Bruno R. Chrcanovic, Department of Prosthodontics,Faculty of Odontology, Malm€o University, Carl Gustafs v€ag 34, SE-205 06,Malm€o, Sweden. E-mail: [email protected];[email protected]
Contract grant sponsor: CNPq, Conselho Nacional de DesenvolvimentoCient�ıfico e Tecnol�ogico – Brazil.
448 HEAD & NECK—DOI 10.1002/HED MARCH 2016

implant [Text word]) AND radiation [Text word]); (dentalimplant [Text word]) AND radiation therapy [Text word])).
The following terms were used in the search strategyon Web of Science, in all databases: ((dental implant[Topic]) AND irradiated [Topic]); (dental implant[Topic]) AND radiotherapy [Topic]); (dental implant[Topic]) AND radiation [Topic]); (dental implant [Topic])AND radiation therapy [Topic])).
The following terms were used in the search strategy onthe Cochrane Oral Health Group Trials Register: ((dentalimplant OR dental implant failure OR dental implant sur-vival OR dental implant success AND (irradiated OR radio-therapy OR radiation OR radiation therapy)).
A manual search of dental implants-related journals,including British Journal of Oral and Maxillofacial Sur-gery, Clinical Implant Dentistry and Related Research,Clinical Oral Implants Research, European Journal ofOral Implantology, Head & Neck, Implant Dentistry,International Journal of Oral and Maxillofacial Implants,International Journal of Oral and Maxillofacial Surgery,International Journal of Periodontics and RestorativeDentistry, International Journal of Prosthodontics, Jour-nal of Clinical Periodontology, Journal of DentalResearch, Journal of Oral Implantology, Journal of OralRehabilitation, Journal of Craniofacial Surgery, Journalof Cranio-Maxillofacial Surgery, Journal of Maxillofacialand Oral Surgery, Journal of Oral and Maxillofacial Sur-gery, Journal of Oral Rehabilitation, Journal of Perio-dontology, Oral Oncology, and Oral Surgery OralMedicine Oral Pathology Oral Radiology and Endodon-tology, was also performed.
The reference list of the identified studies and the rele-vant reviews on the subject were also scanned for possi-ble additional studies. Moreover, online databasesproviding information about clinical trials in progresswere checked (clinicaltrials.gov; www.centerwatch.com/clinicaltrials; www.clinicalconnection.com).
Inclusion and exclusion criteria
Eligibility criteria included clinical human studies,either randomized or not, comparing implant failure, post-operative infection, and/or marginal bone loss in patientsirradiated for head and neck cancers versus nonirradiatedpatients. For this review, implant failure represents thecomplete loss of the implant. Implants that were placedand could not be used because of positional problems (theso-called “sleepers”) were here not considered as failures.Exclusion criteria were case reports, technical reports,animal studies, in vitro studies, and review articles.
Study selection
The titles and abstracts of all reports identified through theelectronic searches were read independently by the 3 authors.For studies appearing to meet the inclusion criteria, or forwhich there were insufficient data in the title and abstract tomake a clear decision, the full report was obtained. Disagree-ments were resolved by discussion among the authors.
Quality assessment
The quality assessment was performed by using the rec-ommended approach for assessing risk of bias in studies
included in Cochrane reviews.7 The classification of therisk of bias potential for each study was based on the 4following criteria: sequence generation (random selectionin the population), allocation concealment (steps must betaken to secure strict implementation of the schedule ofrandom assignments by preventing foreknowledge of theforthcoming allocations), incomplete outcome data (clearexplanation of withdrawals and exclusions), and blinding(measures to blind study participants and personnel fromknowledge of which intervention a participant received).The incomplete outcome data will also be consideredaddressed when there are no withdrawals and/or exclu-sions. A study that included all the criteria mentionedabove was classified as having a low risk of bias, a studythat did not include one of these criteria was classified ashaving a moderate risk of bias. When 2 or more criteriawere missing, the study was considered to have a highrisk of bias.
Data extraction and meta-analysis
From the studies included in the final analysis, the fol-lowing data were extracted (when available): year of pub-lication, study design, unicenter or multicenter study,number of patients, patients’ age, follow-up, days of anti-biotic prophylaxis, mouth rinse, implant healing period,failed and placed implants, postoperative infection, mar-ginal bone loss, implant surface modification, radiother-apy, timespan between irradiation and implant surgery,hyperbaric oxygen therapy (HBO), type of prostheticrehabilitation, jaws receiving implants (maxilla and/ormandible), grafting procedures, observed occurrences ofdeath during the follow-up period, presence of smokersand/or alcohol drinkers among the patients, and adjunc-tive chemotherapy. Contact with authors for possiblemissing data was performed.
Implant failure and postoperative infection were thedichotomous outcome measures evaluated. Weightedmean differences were used to construct forest plots ofmarginal bone loss, a continuous outcome. The statisticalunit for “implant failure” and “marginal bone loss” wasthe implant, and for “postoperative infection” was thepatient. Whenever outcomes of interest were not clearlystated, the data were not used for analysis. The I2 statisticwas used to express the percentage of the total variationacross studies because of heterogeneity, with 25% corre-sponding to low heterogeneity, 50% to moderate, and75% to high. The inverse variance method was used forrandom-effects or fixed-effects model. Where statisticallysignificant (p < .10) heterogeneity was detected, arandom-effects model was used to assess the significanceof treatment effects. Where no statistically significant het-erogeneity was found, analysis was performed using afixed-effects model.8 The estimates of relative effect fordichotomous outcomes were expressed in risk ratio (RR)and in mean difference in millimeters for continuous out-comes, both with a 95% confidence interval (CI). Only ifthere were studies with similar comparisons reporting thesame outcome measures was meta-analysis to beattempted. In the case where no events (or all events)were observed in both groups, the study provided noinformation about relative probability of the event andwas automatically omitted from the meta-analysis. In this
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 449

(these) case(s), the term “not estimable” is shown underthe column of RR of the forest plot table. The softwareused here automatically checks for problematic zerocounts, and adds a fixed value of 0.5 to all cells of studyresults tables where the problems occur.
A funnel plot (plot of effect size vs SE) will be drawn.Asymmetry of the funnel plot may indicate publicationbias and other biases related to sample size, although theasymmetry may also represent a true relationship betweentrial size and effect size.
The data were analyzed using the statistical software ReviewManager (version 5.2.11, The Nordic Cochrane Centre, TheCochrane Collaboration, Copenhagen, Denmark, 2014).
RESULTS
Literature search
The study selection process is summarized in Figure 1.The search strategy resulted in 1683 articles. Four combi-nations of terms were used for PubMed and Web of Sci-ence, which resulted in a number of 686 duplicates. The3 reviewers independently screened the abstracts for thosearticles related to the focus question. The initial screeningof titles and abstracts resulted in 78 full-text articles; 919were excluded for not being related to the topic. The full-text reports of the remaining 78 articles led to the exclu-sion of 24 because they did not meet the inclusion criteria
(9 did not state the number of implants per group, 6 eval-uated implants only in irradiated mandibles, 3 evaluatedimplants for craniofacial prostheses, 2 were earlierfollow-ups of the same study, 2 were the same study pub-lished in another journal, 1 did not insert implants in irra-diated bone, and 1 article was not evaluating implantfailures). Additional hand-searching of the reference listsof selected studies did not yield additional articles. Thus,a total of 54 publications were included in the review.
Description of the studies
Detailed data of the 54 included studies are listed inTables 1 and 2. Ten controlled clinical trials9–18 and 44retrospective studies5,19–61 were included in the meta-analysis. When the e-mail of one or more authors of thearticles was found, questions were sent to request infor-mation about missing data. Authors of 3 studies59–61
replied with the requested information.Seventeen studies5,10,11,16,19,21,25,26,30,32,33,39,42,53,58,60,61 had
a maximum follow-up from 5 to 9 years, whereas 18studies13,23,24,27,36–38,41,43–46,50,51,54–56,59 had a maximumfollow-up of at least 10 years. From the studies with availabledata of patients’ range age, 10 studies12,25,36,38,44–46,50,53,59
included non-adult patients. Eight studies5,19,21,23,29,43,52,57 didnot inform of the patients’ age. Only 6 studies22,24,28,47,48,59
provided information about postoperative infection, with 35
FIGURE 1. Study screening process.
CHRCANOVIC ET AL.
450 HEAD & NECK—DOI 10.1002/HED MARCH 2016

TABLE1.
Detaileddataoftheincluded
studies–part1
Authors
Published
Studydesign
No.ofpatients
(no.perg
roup)
Patients’age
range,y(%)
Follow-up
visits(ra
nge)
Days
ofantibiotics/
mouthrin
seNo
.offailed/
placed
implants
Implantfailure
rate(%)
pvalue
Postoperative
infection
pvalue
Albrektsson
etal19
1988
RA(multicenter)
1641
(NM)
NM3–8y
NM3/49
(G1)
6.12
(G1)
NMNM
NM270/7996
(G2)
3.38
(G2)
3/16
(GRM
x)18.75(GRM
x)0/33
(GRM
d)0(GRM
d)218/3089
(Gn-RM
x)7.06
(Gn-RM
x)52/4907(Gn-RM
d)1.06
(Gn-RM
d)
Sclaroffetal20
1994
RA(unicenter)
22(15,G1
;7,
G2)
23–79(58.7)
3y2mo
NM0/80
(G1)
0(G1)
NMNM
NM2/34
(G2)
5.9(G2)
Franz� en
etal21
1995
RA(unicenter)
5(3,G<50
Gy;
2,G�50
Gy)
NM3–6y
10/NM
0/13
(G<50
Gy)
0(G<50
Gy)
NMNM
NM1/7(G�50
Gy)
14.29(G�50
Gy)
Aldegheri
etal22
1996
RA(unicenter)
7(1,G
Mx;6,
GMd)
44–66(55)
Mean2.7y(1–4)
NM0/6(GRM
x)0(GRM
x)NM
0(GRM
x)NM
0/13
(GRM
d)0(GRM
d)1(GRM
d)
Eckertetal23
1996
RA(unicenter)
20(6,G
Mx;18,
GMd)*
NM12
yNM
8/22
(GRM
x)36.36(GRM
x)NM
NMNM
1/89
(GRM
d)1.12
(GRM
d)
Weischer
etal9
1996
CCT(unicenter)
27(13,G1
;14,
G2)
44–70(56,G1
)26
mo
10/NM
4/57
(G1)
7.02
(G1)
NMNM
NM42–70(57,G2
)3/48
(G2)
6.25
(G2)
Alietal24
1997
RA(unicenter)
10(3,G
Mx;7,
GMd)
39–82(62.6)
Mean33
mo
(11–64)
5/NM
6/10
(GRM
x)60
(GRM
x)NM
0(GRM
x)NM
0/32
(GRM
d)0(GRM
d)1(GRM
d)
Chan
etal25
1997
RA(unicenter)
17(5,G
1;12,
G2)
11–78(55)
Mean32
mo
(6–84)
NM4/23
(G1)
17.39(G1)
NMNM
NM0/46
(G2)
0(G2)
Esserand
Wagner26
1997
RA(unicenter)
78(64,G1
;14,
G2;6,G
Mx;72,
GMd)
37–79(55-58,
G1)
5y
NM39/249
(65,G1
)†15.66(G1)
NMNM
NM
48–58(54,G2
)7/71
(5,G
2)†
9.86
(G2)
6/28
(13,GR
Mx)
†21.43(GRM
x)40/292
(57,GM
d)†
13.70(GMd)
33/221
(GRM
d)14.93(GRM
d)7/71
(Gn-RM
d)9.86
(Gn-RM
d)
Jisander
etal10
1997
CCT(unicenter)
17(NM)
47–78(67)
Mean21
mo
(1–62)
10/NM
3/38
(GRM
x)7.89
(GRM
x)NM
NMNM
2/65
(GRM
d)3.08
(GRM
d)
Kelleretal27
1997
RA(unicenter)
19(8,G
RBG;
11,
GRNB
)24–84(60)
10y
NM1/26
(GRB
G)3.85
(GRB
G)NM
NMNM
0/72
(GRN
B)0(GRN
B)
Markeretal28
1997
RA(unicenter)
12(6,G
1;6,G2
)42–81(71)
Mean14
mo
(7–47)
7/14
0/19
(G1)
0(G1)
NM0(G1)
NM0/19
(G2)
0(G2)
0(G2)
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 451

TABLE1.
Cont
inue
d
Authors
Published
Studydesign
No.ofpatients
(no.perg
roup)
Patients’age
range,y(%)
Follow-up
visits(ra
nge)
Days
ofantibiotics/
mouthrin
seNo
.offailed/
placed
implants
Implantfailure
rate(%)
pvalue
Postoperative
infection
pvalue
McGhee
etal29
1997
RA(unicenter)
6(5,G
1;1,G2
)NM
3y
NM2/21
(G1)
9.52
(G1)
NMNM
NM0/5(G2)
0(G2)
0/9(GRB
G)0(GRB
G)2/12
(GRN
B)16.67(GRN
B)0/5(Gn-RG
B)0(Gn-RG
B)
Niimietal30
1997
RA(multicenter)
24(9,G
Mx;16,
GMd;7,GH
BO;
18,G
n-HB
O)
NM(64.8)
2–73
mo
NM9/39
(GRM
x)23.08(GRM
x)NM
NMNM
3/71
(GRM
d)4.23
(GRM
d)4/31
(GHB
O)12.90(GHB
O)8/79
(Gn-HB
O)10.13(Gn-HB
O)7/67
(G�45
Gy)
10.45(G�45
Gy)
5/51
(G>45
Gy)
9.80
(G>45
Gy)
Roum
anas
etal31
1997
RA(unicenter)
20(11,G1
;9,
G2)
25–78
1–49
mo
NM0/45
(G1)
0(G1)
NMNM
NM1/35
(G2)
2.9(G2)
0/39
(GRB
G)0(GRB
G)1/32
(Gn-RB
G)3.1(Gn-RB
G)0/5(GRN
B)0(GRN
B)0/4(Gn-RN
B)0(Gn-RN
B)
Andersson
etal32
1998
RA(unicenter)
15(*)
62–74(68)
5y
10/NM
0/12
(GRM
x)0(GRM
x)NM
NMNM
2/78
(GRM
d)2.56
(GRM
d)
Brogniez
etal33
1998
RA(NM)
19(NM)
37–74(53)
Mean38
mo
(6–68)
NM0/3(2,G
RMx)
†0(GRM
x)NM
NMNM
2/50
(13,GR
Md)
†4(GRM
d)
Iharaetal34
1998
RA(multicenter)
18(10,G1
;8,
G2;4,G
HBO;
6,Gn-HBO
)
22–82(64.2)
Mean27.6mo
NM6/39
(G1)
15.38(G1)
>.05
(GHB
O)NM
NM9/35
(G2)
25.71(G2)
3/19
(GHB
O)15.79(GHB
O)3/20
(Gn-HB
O)15
(Gn-HB
O)
Esseretal35
1999
RA(unicenter)
62(34,G1
;28,
G2)
40–76(54.7,G1
)Mean58.2mo
NM9/148(G1)
6.08
(G1)
>.05
NMNM
44–77(55.3,G2
)3/128(G2)
2.34
(G2)
Fosteretal36
1999
RA(unicenter)
22(3,G
1;19,
G2)
12–82(49)
11y
NM0/15
(GRG
B)0(GRG
B)NM
NMNM
7/89
(Gn-RG
B)7.87
(Gn-RG
B)
Granstr€ om
etal37
1999
RA(unicenter)
78(52,G1
;26,
G2;20,GH
BO;
32,G
n-HB
O)‡
23–94(64.9)
0.1–15.1y
NM87/246
(G1)
35.37(G1)
NMNM
NM12/89(G2)
13.48(G2)
8/99
(GHB
O)‡
8.08
(GHB
O)79/147
(Gn-HB
O)53.74(Gn-HB
O)
Kelleretal38
1999
RA(unicenter)
54(2,G
1;52,
G2)
15–73(48)
12y
NM0/11
(G1)
0(G1)
NMNM
NM33/237
(G2)
13.92(G2)
CHRCANOVIC ET AL.
452 HEAD & NECK—DOI 10.1002/HED MARCH 2016

TABLE1.
Cont
inue
d
Authors
Published
Studydesign
No.ofpatients
(no.perg
roup)
Patients’age
range,y(%)
Follow-up
visits(ra
nge)
Days
ofantibiotics/
mouthrin
seNo
.offailed/
placed
implants
Implantfailure
rate(%)
pvalue
Postoperative
infection
pvalue
Mericske–Stern
etal11
1999
CCT(unicenter)
17(11,G1
;6,
G2)
38–81(58)
Mean37
mo
(12–84)
NM8/33
(G1)
24.24(G1)
NMNM
NM0/20
(G2)
0(G2)
0/12
(GMx)
0(GMx)
8/41
(GMd)
19.51(GMd)
Weischerand
Mohr39
1999
RA(unicenter)
40(18,G1
;22,
G2)
43–75(55)
Mean37
mo
(6–117)
NM10/83(G1)
12.05(G1)
>.05
NMNM
5/92
(G2)
5.43
(G2)
Werkm
eister
etal40
1999
RA(unicenter)
29(12,G1
;17,
G2)
35–79(55)
3y
NM8/30
(G1)
26.67(G1)
<.05
(G1–G2
)NM
NM19/79(G2)
24.05(G2)
14/45(Gn-RB
G)31.11(Gn-
RBG)
8/30
(GRN
B)26.67(GRN
B)5/34
(Gn-RN
B)14.71(Gn-
RNB)
5/16
(G>54
Gy)
31.25(G>54
Gy)
3/14
(G<54
Gy)
21.43(G<54
Gy)
Gotoetal41
2002
RA(unicenter)
36(23,GR
BG;
13,G
RNB)
20–83(52.9)
Mean1881
d(72–3901)
NM11/92(G1)
11.96(G1)
NMNM
NM4/88
(G2)
4.55
(G2)
11/52(GMx)
21.15(GMx)
4/128(GMd)
3.13
(GMd)
4/68
(GRB
G)5.88
(GRB
G)11/112
(GRN
B)9.82
(GRN
B)
vanSteen-
berghe
etal12
2002
CCT(unicenter)
234(NM)
15–80(50)
3y
NM2/33
(G1)
6.06
(G1)
<.01
NMNM
25/1230(G2)
2.03
(G2)
Vischetal13
2002
CCT(unicenter)
130(30,
Gy<50
Gy;100,
G�50
Gy)
34–87(62)
Upto14
y(every12
mo)
“Prescribed”
33/108
(GRM
x)28.70(GRM
x).001
(GMx-GM
d)NM
NM
31/338
(GRM
d)9.76
(GRM
d).05(G
50Gy)
19/207
(G<50
Gy)9.18
(G<50
Gy)
>.05
(G12)
45/239
(G�50
Gy)18.83(G�50
Gy)
29/175
(G<12)
16.57(G<12)
35/271
(G�12)
12.92(G�12)
Caoand
Weischer42
2003
RA(unicenter)
27(12,G1
;15,
G2)
45–79(NM)
5y
NM18/53(G1)
33.96(G1)
<.01
NMNM
11/78(G2)
14.10(G2)
Granstr€ om43
2003
RA(unicenter)
45(30,GH
BO;
15,G
n-HB
O;25,
GRMx;20,
GRMd)
NMMean9.8y
(2.2–22)
NM5/133(GHB
O)3.8(GHB
O)NM
NMNM
17/73(Gn-HB
O)23.3(Gn-HB
O)14/109
(GRM
x)12.8(GRM
x)8/97
(GRM
d)8.2(GRM
d)0/40
(GRB
G)0(GRB
G)2/14
(GRN
B)14.3(GRN
B)
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 453
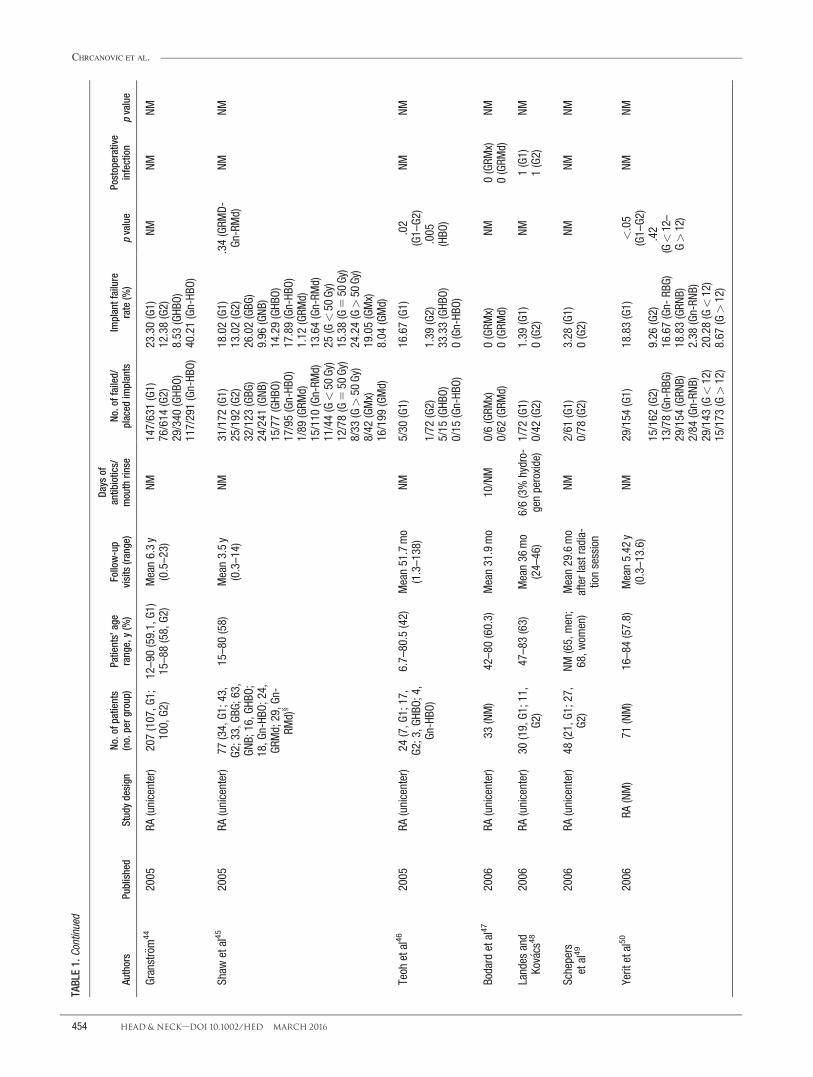
TABLE1.
Cont
inue
d
Authors
Published
Studydesign
No.ofpatients
(no.perg
roup)
Patients’age
range,y(%)
Follow-up
visits(ra
nge)
Days
ofantibiotics/
mouthrin
seNo
.offailed/
placed
implants
Implantfailure
rate(%)
pvalue
Postoperative
infection
pvalue
Granstr€ om44
2005
RA(unicenter)
207(107,G
1;100,G2
)12–90(59.1,G1
)Mean6.3y
(0.5–23)
NM147/631(G1)
23.30(G1)
NMNM
NM15–88(58,G2
)76/614
(G2)
12.38(G2)
29/340
(GHB
O)8.53
(GHB
O)117/291(Gn-HB
O)40.21(Gn-HB
O)
Shaw
etal45
2005
RA(unicenter)
77(34,G1
;43,
G2;33,GB
G;63,
GNB;16,G
HBO;
18,G
n-HB
O;24,
GRMd;29,G
n-RM
d)§
15–80(58)
Mean3.5y
(0.3–14)
NM31/172
(G1)
18.02(G1)
.34(GRM
D-Gn-RMd)
NMNM
25/192
(G2)
13.02(G2)
32/123
(GBG
)26.02(GBG
)24/241
(GNB
)9.96
(GNB
)15/77(GHB
O)14.29(GHB
O)17/95(Gn-HB
O)17.89(Gn-HB
O)1/89
(GRM
d)1.12
(GRM
d)15/110
(Gn-RM
d)13.64(Gn-RM
d)11/44(G<50
Gy)
25(G<50
Gy)
12/78(G
550
Gy)
15.38(G
550
Gy)
8/33
(G>50
Gy)
24.24(G>50
Gy)
8/42
(GMx)
19.05(GMx)
16/199
(GMd)
8.04
(GMd)
Teoh
etal46
2005
RA(unicenter)
24(7,G
1;17,
G2;3,G
HBO;
4,Gn-HBO
)
6.7–80.5(42)
Mean51.7mo
(1.3–138)
NM5/30
(G1)
16.67(G1)
.02
(G1–G2
)NM
NM
1/72
(G2)
1.39
(G2)
.005
(HBO
)5/15
(GHB
O)33.33(GHB
O)0/15
(Gn-HB
O)0(Gn-HB
O)
Bodard
etal47
2006
RA(unicenter)
33(NM)
42–80(60.3)
Mean31.9mo
10/NM
0/6(GRM
x)0(GRM
x)NM
0(GRM
x)NM
0/62
(GRM
d)0(GRM
d)0(GRM
d)
Landes
and
Kov� acs
482006
RA(unicenter)
30(19,G1
;11,
G2)
47–83(63)
Mean36
mo
(24–46)
6/6(3%
hydro-
genperoxide)
1/72
(G1)
1.39
(G1)
NM1(G1)
NM0/42
(G2)
0(G2)
1(G2)
Schepers
etal49
2006
RA(unicenter)
48(21,G1
;27,
G2)
NM(65,men;
68,w
omen)
Mean29.6mo
afterlastradia-
tionsession
NM2/61
(G1)
3.28
(G1)
NMNM
NM0/78
(G2)
0(G2)
Yeritetal50
2006
RA(NM)
71(NM)
16–84(57.8)
Mean5.42
y(0.3–13.6)
NM29/154
(G1)
18.83(G1)
<.05
(G1–G2
)NM
NM
15/162
(G2)
9.26
(G2)
.42
(G<12–
G>12)
13/78(Gn-RB
G)16.67(Gn-
RBG)
29/154
(GRN
B)18.83(GRN
B)2/84
(Gn-RN
B)2.38
(Gn-RN
B)29/143
(G<12)
20.28(G<12)
15/173
(G>12)
8.67
(G>12)
CHRCANOVIC ET AL.
454 HEAD & NECK—DOI 10.1002/HED MARCH 2016

TABLE1.
Cont
inue
d
Authors
Published
Studydesign
No.ofpatients
(no.perg
roup)
Patients’age
range,y(%)
Follow-up
visits(ra
nge)
Days
ofantibiotics/
mouthrin
seNo
.offailed/
placed
implants
Implantfailure
rate(%)
pvalue
Postoperative
infection
pvalue
Nelson
etal51
2007
RA(unicenter)
93(29,G1
;64,
G2)
26–89(59)
Mean10.1y
(5–161
mo)
4/NM
7/124(G1)
5.65
(G1)
.08
NMNM
4/311(G2)
1.29
(G2)
Schoen
etal14
2007
CCT(unicenter)
26(13,GH
BO;
13,G
n-HB
O)47–77(60.1)
1yafterplace-
mentofthe
prostheses
14/NM
8/54
(GHB
O)14.81(GHB
O)NM
NMNM
3/49
(Gn-HB
O)6.12
(Gn-HB
O)
Alsaadietal52
2008
RA(unicenter)
412(2,G
1;410,
G2)
NMUp
to2yafter
abutment
connection
NM3/15
(G1)
20(G1)
.003
NMNM
98/1499(G2)
6.54
(G2)
Schoen
etal15
2008
CCT(unicenter)35
(50k)(19,G
1;16,G
2)41–81(61.5)
1yafterplace-
mentofthe
prostheses
NM2/76
(G1)
2.63
(G1)
NMNM
NM2/64
(G2)
3.13
(G2)
Cuesta–G
iletal53
2009
RA(unicenter)
111(79,G1
;32,
G2)
13–79(52)
6mo–9y
NM75/395
(G1)
18.99(G1)
NMNM
NM6/311(G2)
1.93
(G2)
(GBG
-GNB
)
Kleinetal54
2009
RA(unicenter)
43(27,G1
;16,
G2;13,
G<50
Gy;14,
G�50
Gy)
NM(58.4)
12y
NM13/116
(G1)
11.21(G1)
NMNM
NM12/74(G2)
16.22(G2)
4/55
(G<50
Gy)
7.27
(G<50
Gy)
9/61
(G�50
Gy)
14.75(G�50
Gy)
Korfage
etal16
2010
CCT(unicenter)
50(31,G1
,19,
G2)
41–81(61.5)
6wk,1and5y
NM13/123
(G1)
10.57(G1)
<.05
NMNM
1/72
(G2)
1.39
(G2)
Salinas
etal5
2010
RA(unicenter)
44(26,G1
;18,
G2)
NMMean41
mo
(4–108)
NM23/90(G1)
25.56(G1)
.57
(G1–G2
)NM
NM
8/116(G2)
6.90
(G2)
.27
(GBG
-GN
B)14/51(GRB
G)27.45(GBG
)9/39
(GRN
B)23.08(GNB
)6/63
(Gn-RB
G)9.52
(Gn-RB
G)2/53
(Gn-RN
B)3.77
(Gn-RN
B)
Barrow
man
etal55
2011
RA(unicenter)
31(NM)
20–76(50.7)
15y
NM5/48
(G1)
10.42(G1)
NMNM
NM0/67
(G2)
0(G2)
0/35
(GMx)
0(GMx)
5/80
(GMd)
6.25
(GMd)
0/9(Gn-RN
B-Mx)
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 455

TABLE1.
Cont
inue
d
Authors
Published
Studydesign
No.ofpatients
(no.perg
roup)
Patients’age
range,y(%)
Follow-up
visits(ra
nge)
Days
ofantibiotics/
mouthrin
seNo
.offailed/
placed
implants
Implantfailure
rate(%)
pvalue
Postoperative
infection
pvalue
Buddula
etal56
2011
RA(unicenter)
48(NM)
NM(60.2)
12y
NM20/62(GRM
x)32.36(GRM
x)NM
NMNM
13/209
(GRM
d)6.22
(GRM
d)8/59
(GRB
G)13.56(GRB
G)25/212
(GRN
B)11.79(GRN
B)
Heberer
etal17
2011
CCT(unicenter)
20(NM)
NM(61.1)
Mean14.4mo
(12–26)
4/NM
0/55
(GRM
x)0(GRM
x)NM
NMNM
2/42
(GRM
d)¶
4.76
(GRM
d)
Sammartino
etal18
2011
(CCT)
(multicenter)
69(9,G
Mx;60,
GMd;49,
G<50
Gy;20,
G�50
Gy)
28–63(55.8)
Atleast3
yNM
18/42(GRM
x)42.86(GRM
x)<.05
(GMx-GM
d)NM
NM
2/130(GRM
d)1.54
(GRM
d)<.05(G
50Gy)
7/111(G<50
Gy)
6.31
(G<50
Gy)
13/61(G�50
Gy)
21.31(G�50
Gy)
12/127
(G<12)
9.45
(G<12)
8/61
(G�12)
13.11(G�12)
Fenlon
etal57
2012
RA(multicenter)
41(12,G1
;29,
G2)
NM3y
NM15/35(G1)
42.86(G1)
NMNM
NM3/110(G2)
2.73
(G2)
Linsen
etal59
2012
RA(unicenter)
66(NM)
6–82
(55.7)
Mean48
mo
(12–140)
NM8/127(G1)
6.30
(G1)
NM18
(G1)
NM6/135(G2)
4.44
(G2)
13(G2)
1/49
(GMx)
2.04
(GMx)
13/213
(GMd)
6.10
(GMd)
1/17
(GRM
x)**
5.88
(GRM
x)7/110(GRM
d)**
6.36
(GRM
d)0/32
(Gn-RM
x)**
0(Gn-RM
x)6/103(Gn-RM
d)**
5.83
(Gn-RM
d)8/79
(GBG
)10.13(GBG
)6/183(GNB
)3.28
(GNB
)
Manchade
laPlataetal60
2012
RA(unicenter)
50(30,G1
;20,
G2)
40-74(55.5,G1
)Mean45
mo
(range6-96)
NM22/225
(G1)
9.78
(G1)
.063
(G1–G2
)NM
NM18-80(56.2,G2
)6/130(G2)**
4.62
(G2)
7/94
(GRM
x)**
7.45
(GRM
x)15/131
(GRM
d)**
11.45(GRM
d)
Katsoulis
etal61
2013
RA(unicenter)
28(46†
†)(20,
G1;26,G2
)NM
(57.7)
2–5y
NM14/62(G1)
22.58(G1)
NMNM
NM4/42
(G2)
9.52
(G2)
4/24
(GMx)**
16.67(GMx)
10/80(GMd)**
12.5(GMd)
6/20
(GRB
G)30
(GRB
G)8/42
(GRN
B)19.05(GRN
B)2/26
(Gn-RB
G)7.69
(Gn-RB
G)2/16
(Gn-RN
B)12.5(Gn-RN
B)
CHRCANOVIC ET AL.
456 HEAD & NECK—DOI 10.1002/HED MARCH 2016
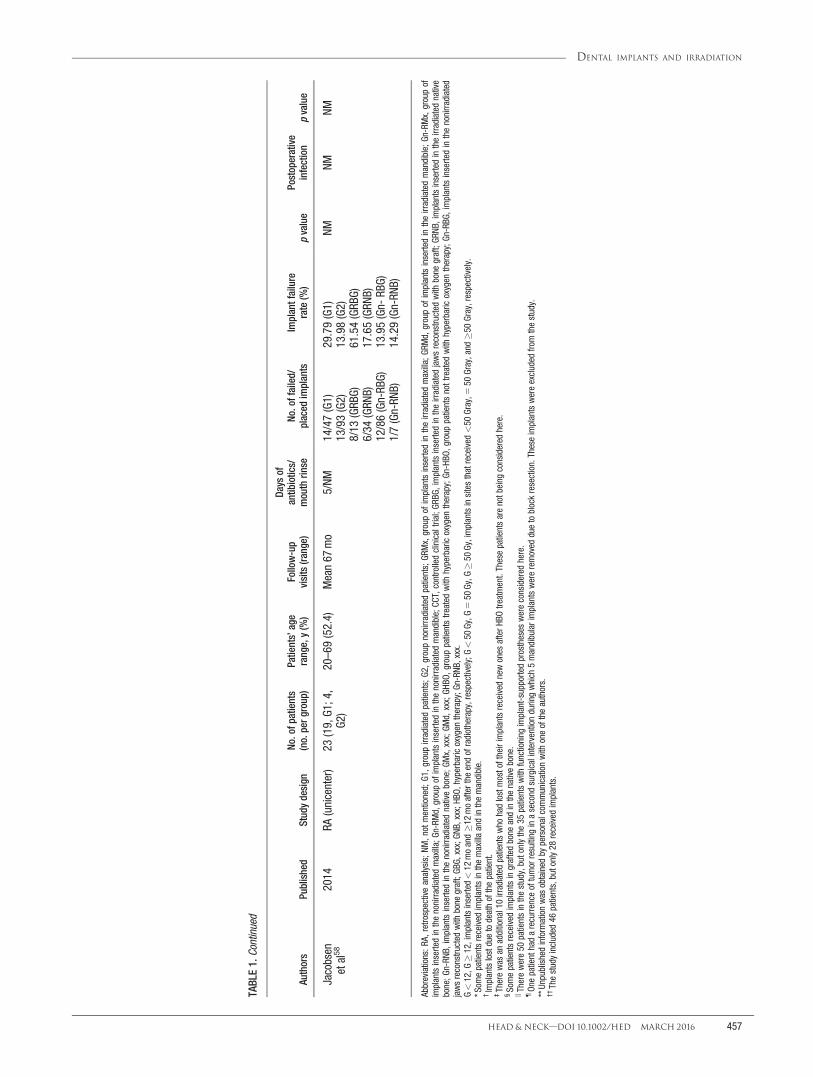
TABLE1.
Cont
inue
d
Authors
Published
Studydesign
No.ofpatients
(no.perg
roup)
Patients’age
range,y(%)
Follow-up
visits(ra
nge)
Days
ofantibiotics/
mouthrin
seNo
.offailed/
placed
implants
Implantfailure
rate(%)
pvalue
Postoperative
infection
pvalue
Jacobsen
etal58
2014
RA(unicenter)
23(19,G1
;4,
G2)
20–69(52.4)
Mean67
mo
5/NM
14/47(G1)
29.79(G1)
NMNM
NM13/93(G2)
13.98(G2)
8/13
(GRB
G)61.54(GRB
G)6/34
(GRN
B)17.65(GRN
B)12/86(Gn-RB
G)13.95(Gn-
RBG)
1/7(Gn-RN
B)14.29(Gn-RN
B)
Abbreviations:R
A,retrospectiveanalysis;N
M,n
otmentioned;
G1,g
roup
irradiatedpatients;G2
,group
nonirradiatedpatients;GR
Mx,groupofimplantsinsertedintheirradiatedmaxilla;GR
Md,groupofimplantsinsertedintheirradiatedmandible;Gn-RMx,groupof
implantsinsertedinthenonirradiatedmaxilla;Gn-RMd,groupofimplantsinsertedinthenonirradiatedmandible;CC
T,controlledclinicaltrial;G
RBG,
implantsinsertedintheirradiatedjawsreconstructed
with
bone
graft;GR
NB,implantsinsertedintheirradiatednative
bone;G
n-RN
B,implantsinsertedinthenonirradiatednativebone;G
Mx,xxx;GM
d,xxx;GH
BO,group
patientstreated
with
hyperbaricoxygen
therapy;Gn-HBO
,group
patientsnottreated
with
hyperbaricoxygen
therapy;Gn-RBG
,implantsinsertedinthenonirradiated
jawsreconstructed
with
bone
graft;GB
G,xxx;GN
B,xxx;HB
O,hyperbaricoxygen
therapy;Gn-RNB
,xxx.
G<12,G�12,implantsinserted<12
moand�12
moafterthe
endofradiotherapy,respectively;G<50
Gy,G
550
Gy,G�50
Gy,implantsinsitesthatreceived<50
Gray,5
50Gray,and�50
Gray,respectively.
*Som
epatientsreceived
implantsinthemaxillaandinthemandible.
†Implantslostduetodeathofthepatient.
‡Therewas
anadditional10irradiatedpatientswho
hadlostmostoftheirimplantsreceived
newones
afterH
BOtreatment.Thesepatientsarenotbeing
considered
here.
§Somepatientsreceived
implantsingraftedbone
andinthenativebone.
kTherewere50
patientsinthestudy,butonlythe35
patientswith
functioning
implant-supportedprostheses
wereconsidered
here.
¶On
epatienthadarecurrence
oftumorresulting
inasecond
surgicalinterventionduringwhich
5mandibularimplantswereremoved
duetoblockresection.Theseimplantswereexcluded
fromthestudy.
**Unpublishedinform
ationwas
obtained
bypersonalcommunicationwith
oneoftheauthors.
††Thestudyincluded
46patients,butonly28
received
implants.
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 457

TABLE2.
Detaileddataoftheincluded
studies–part2
Authors
Published
Healingperiod/
loading
Mean
6SD
ofmarginalbone
loss,m
mImplantsurface
modification(brand)
Radiotherapy
Hyperbaric
oxygen
therapy
Type
ofprosthetic
rehabilitation/jaws
receivingimplants
Studyenvironm
ent,
chem
otherapy,cases
ofdeath,
bone
graft,
smokers,alcohol
abuse,observations
Albrektsson
etal19
1988
NMNM
Turned
(Brånemark,
Nobelpharm
a,G€ oteborg,
Sweden)
NMNM
NM/maxillaandmandible
–
Sclaroffetal20
1994
7mo
NMTurned
(Brånemark,
Nobelpharm
a,G€ oteborg,
Sweden;n
536),acid-
etched
(Osseotite(3i/
ImplantInnovations,
Palm
BeachGardens,
FL;n
578)
Generally
30treatmentsof
200rads
pertreatment,
radiotherapy.Implants
wereplaced
from4–
6wkbeforeradiotherapy
(exceptin2patients).
NPFixed,overdenture/
mandible
4patientsdied
duringthe
follow-up,graft(iliac
crest,
fibulaflap)
Franz� enetal21
1995
31= 2-6mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
25–64Gy.Implantswere
placed
2yafter
radiotherapy.
NPFixed/mandible
2sm
okers,2diabetics,
adjunctivechem
otherapy
in1patient,graftNM
Aldegheri
etal22
1996
4–10
mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
50–70Gy.Implantswere
placed
from5–96
mo
afterradiotherapy(mean
44).
NPOverdenture/maxillaand
mandible
Adjunctivechem
otherapy
in3
patients,graft(iliac
crest)
Eckertetal23
1996
NMNM
NM2005–6480cGy.
NPFixed,overdenture,
obturator/m
axillaand
mandible
GraftN
M
Weischeretal9
1996
6mo(G1)
NMTurned
(Brånemark,Nobel
BiocareAB,G
€ oteborg,
Sweden;n
535),TPS
(IMZ,Friadent,
Mannheim,G
ermany;
n5
32),sandblasted
andacid-etched(Frialit-2
system
,FriatecAG
,Mannheim,G
ermany;
n5
38)
Dose
ranged
between36
and75
Gy(average
42.5),fractions
of5
dosesof2Gy/wkor4
dosesof2.5Gy/wk.
Implantswereplaced
from13–72moafter
radiotherapy.
NPFixed,overdenture/
mandible
Adjunctivechem
otherapy
in7
patientsofG1
,bonegrafts
in15
patients(7inG1
,8in
G2)
3–6mo(G2)
Alietal24
1997
6–12
mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
2500–5750cGy
NPFixed,overdenture/maxilla
andmandible
GraftN
M
Chan
etal25
1997
4–6mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden),TPS(IM
Z,FriatecAG
,Mannheim,
Germ
any)
60Gy
NPFixed,overdenture/maxilla
andmandible
1patientdied
duringthe
follow-up,graftN
M
CHRCANOVIC ET AL.
458 HEAD & NECK—DOI 10.1002/HED MARCH 2016

TABLE2.
Cont
inue
d
Authors
Published
Healingperiod/
loading
Mean
6SD
ofmarginalbone
loss,m
mImplantsurface
modification(brand)
Radiotherapy
Hyperbaric
oxygen
therapy
Type
ofprosthetic
rehabilitation/jaws
receivingimplants
Studyenvironm
ent,
chem
otherapy,cases
ofdeath,
bone
graft,
smokers,alcohol
abuse,observations
Esserand
Wagner26
1997
Usually
6mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden;n
5178),TPS
(IMZ,InterporeInt.,
Irvine,CA
;n5
71)
Totaldoseof36
Gyin
conventional
fractionation,anditwas
restrictedtopatients
who
hadatumorsize
of>3cm
ormanifested
cervicalmetastases.
Intervalbetweentheend
ofradiotherapy
and
implantplacementw
asatleast9
mo.
NPFixed,overdenture/maxilla
andmandible
17patientsdied
duringthe
follow-up,grafts(1
bicorticaliliaccrest,3
spongiosachips)
Jisanderetal10
1997
Mean6mo
(range3–11)
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden;n
598),
titanium-blasted
(Astra,
Astra
Tech
AB,M
€ olndal,
Sweden;n
55)
>50
Gy(8
patients),<
50Gy
(9patients),implantswere
placed
intheirradiated
jawsaftera
periodof
18–228
mo(mean
88mo).
7patients
Fixed(n
522)/m
axillaand
mandible
Fixedprostheses,6
patients
died
duringthefollow-up,
graftsNM
Kelleretal27
1997
3–7mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
Mean5600
cGy(range,
2755–7000).Implants
insertedinamedian
periodof72
mo(range,
16–168)after
irradiation.
NPFixed,overdenture/
mandible
2patientsdied
duringthe
follow-up(10implants),
graft(iliac
crest,fibula,
scapula)
Markeretal28
1997
NMNM
TPS(Bonefit,ITI,
Waldenburg,
Switzerland)
40–50Gy,5
fractions
of2Gy
perw
k.Implants
wereplaced
inthe
irradiatedjawsaftera
periodof8–32
mo
(mean,23).
NMOverdenture/maxillaand
mandible
4patientsdied
duringthe
follow-up,graft(iliac
crest,
rib)
McGheeetal29
1997
4–8mo
NMHA
-coated(Steri-Oss
DentalImplants,Los
Angeles,CA
)
>50
Gydelivered
overa
6–8wkperiod.Implants
placed
3–22
moafter
theinitialresection/
reconstruction.
NPOverdenture/mandible
University,graft(fibula)
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 459

TABLE2.
Cont
inue
d
Authors
Published
Healingperiod/
loading
Mean
6SD
ofmarginalbone
loss,m
mImplantsurface
modification(brand)
Radiotherapy
Hyperbaric
oxygen
therapy
Type
ofprosthetic
rehabilitation/jaws
receivingimplants
Studyenvironm
ent,
chem
otherapy,cases
ofdeath,
bone
graft,
smokers,alcohol
abuse,observations
Niimietal30
1997
4–“�
13”mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
Theintervalbetween
implantsurgeryand
radiotherapy
ranged
from1–240mo.
7patients(20“dives”
beforeand10
“dives”
afterimplantplacement,
with
2.4absolute
atmosphericpressure
for9
0min)
Fixed(64implants–2
lost),overdentures
(46
implants–10
lost)/m
ax-
illaandmandible
University,nobone
grafts
Roum
anas
etal31
1997
6mo
NMTurned
(Brånemark,
Nobelpharm
a,G€ oteborg,
Sweden)
9patientsreceived
pre-
implantradiotherapy
and2patientspost-
implantradiotherapy.
NMFixed,overdenture/
mandible
2patientsdied
duringthe
follow-up(4implants),graft
(fibula)
Andersson
etal32
1998
6mo(maxilla)
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
44Gy
(n53),50Gy
(n5
7),60Gy
(n51),
68Gy
(n5
4).Implant
placem
entm
ean
22.1mo(range,8–
65mo)after
radiotherapy.
NPFixed/maxillaandmandibleUniversity,adjunctive
chem
otherapy
in1patient,
3patientsdied
duringthe
follow-up(15implants),
graftN
M
3–6mo
(mandible)
Brogniez
etal33
1998
5–8mo
NMHA
-coated(NM;n
542)
Averagedose
57Gy
(range,40–74).The
minimum
waitingperiod
betweencompletionof
irradiationandthe
placem
entofimplants
was
5mo(range,5–
192,mean,17).
NPFixed,overdenture/maxilla
andmandible
6patientsdied
duringthe
follow-up(15implants),
someimplantsplaced
inbone
grafts,buttheexact
numbernotinform
ed
“uncoated”
(NM;
n5
11)
Iharaetal34
1998
Mean9.1mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
Mean62.3Gy
(radiotherapy
before
implantplacement;
meanperiodbefore
implantplacement:
77.3mo),m
ean79.8Gy
(radiotherapy
both
beforeandafterimplant
placem
ent;meanperiod
betweenradiotherapy
andplacem
entw
as6.5mobeforeand
13moafterplacement),
60.8Gy
(radiotherapy
afterimplantplacement;
radiotherapy
1moafter).
4patients
Overdenture/maxilla
Chem
otherapy
in7patientsof
G1and1patientofG2
CHRCANOVIC ET AL.
460 HEAD & NECK—DOI 10.1002/HED MARCH 2016

TABLE2.
Cont
inue
d
Authors
Published
Healingperiod/
loading
Mean
6SD
ofmarginalbone
loss,m
mImplantsurface
modification(brand)
Radiotherapy
Hyperbaric
oxygen
therapy
Type
ofprosthetic
rehabilitation/jaws
receivingimplants
Studyenvironm
ent,
chem
otherapy,cases
ofdeath,
bone
graft,
smokers,alcohol
abuse,observations
Esseretal35
1999
5mo(range,
4–8)
NMTurned
(Brånemark,Nobel
Biocare,G€ oteborg,
Sweden)
60Gy.M
eaninterval
betweenimplantsurgery
andradiotherapy:
23.1mo(range,10–
101).
NPFixed,overdenture/
mandible
38sm
okers(20,G1
:18,G2
),17
patients(13G1
,4G2
)died
duringthefollow-up
(56implantsG1
,19
implantsG2
)
Fosteretal36
1999
NMNM
NMNM
NMNM
/mandible
University,allpatients
receivinggrafts(iliaccrest,
fibula)
Granstr€ om
etal37
1999
NMNM
Turned
(Brånemark,Nobel
Biocare,G€ oteborg,
Sweden)
Mean57.7Gy
(range,25–
145)
20tim
esbeforesurgery
and10
times
postoperatively.Pure
oxygen
delivered
at250
kPa,for9
0min
NM/maxillaandmandible
University,14patientsdied
duringthefollow-up,only
implantsexposedand
loaded
andinnativebone
Kelleretal38
1999
4–6mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
55–61Gy
NPFixed,overdenture/maxillaGraft(iliac
crest-
allpatients)
Mericske-Stern
etal11
1999
3–16
mo
NMTPS(ITI,Waldenburg,
Switzerland)
50–74Gy.7
implants
placed
after
radiotherapy,17before
radiotherapy,9
implants
placed
after
osteoradionecrosis.
2patients
Fixed,overdenture/maxilla
andmandible
University,11sm
okers,8
drinking
alcohol,graft(9
patients–fibula,scapula,
iliac
crest),5patientsdied
duringthefollow-up
Weischerand
Mohr39
1999
Mean5.5mo
(range,3–10,
G1)
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden;n
553),
sandblastedandacid-
etched
(Frialit-2
system
,FriatecAG
,Mannheim,
Germ
any;
n5
80;
Ankylos,Dentsply-Fria-
dent,M
annheim,
Germ
any;
n5
6),TPS
(IMZcylinder,Friatec,
Mannheim,G
ermany;
n5
36)
36–72Gy.M
eaninterval
fromtheendof
irradiationtoimplant
placem
ent:48
mo
(range,13–189).
NPFixed,overdenture/maxilla
andmandible
University,graft(iliaccrest)
Mean
3.2mo
(range,3–6,
G2)
Werkm
eister
etal40
1999
NMNM
NMMean54
Gy(range,42–
64).Implantsplaced
atleast24moafter
irradiation.
NPNM
/mandible
University,graft(iliaccrest)
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 461

TABLE2.
Cont
inue
d
Authors
Published
Healingperiod/
loading
Mean
6SD
ofmarginalbone
loss,m
mImplantsurface
modification(brand)
Radiotherapy
Hyperbaric
oxygen
therapy
Type
ofprosthetic
rehabilitation/jaws
receivingimplants
Studyenvironm
ent,
chem
otherapy,cases
ofdeath,
bone
graft,
smokers,alcohol
abuse,observations
Gotoetal41
2002
NMNM
NMNM
NMNM
/maxillaandmandible
University,graft(21patients-
19inmandible,2in
maxilla)
vanSteen-
berghe
etal12
2002
6mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
NMNP
NM/maxillaandmandible
University,adjunctive
chem
otherapy
was
perform
edinsome
patients,butthe
exact
numberw
asnotinformed,
graftN
M
Vischetal13
2002
Atleast6
mo
NMHA
-coated(Dyna,Dyna
DentalEngineeringBV,
Bergen
opZoom
,Netherlands;
n5
390;
Screw-Vent,Zimmer
Dental,C
arlsbad,CA
;n
556)
2–6MV,externalbeam
s,daily
fractions:2
Gray,5
fractions/wk.The
intervalbetweenimplant
surgeryand
radiotherapy
ranged
from6moto22
y.
NPNM
/maxillaandmandible
University,implantsinserted
withoutperiodontal
infection,2-stageprotocol,
50patients(38%
)died
duringthefollow-up.Thirty-
fiveimplants(8%)w
ere
insertedintojawstreated
with
bone
resections
(partialm
axillectomyand
partialorsegm
ental
mandibulectom
y).The
survivaloftheseimplants
was
significantly(p
5.04)
worse
comparedwith
that
ofimplantsinjawswithout
thesesurgicaltreatments
(61%
and83%,
respectively).
Caoand
Weischer42
2003
5–8mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden),sandblasted
andacid-etched(Frialit-
2system
,FriatecAG
,Mannheim,G
ermany)
From
36–76Gy
(Co/MeV
photons,4–5fractions
of2–2.5Gy
perw
eek).
Implants6moafter
radiotherapy.
NPOverdentures
(n5
21),
fixed
fulldentures
(n5
3),implant-sup-
portedfixed
bridge
(n5
1)/maxilla
Adjunctivechem
otherapy
in4
patients,sinusfloor
elevationwith
aniliac
bone
graftin4patients,7
implantinthezygomatic
region
Granstr€ om43
2003
NMNM
NM48–120
GyPerform
edin30
patients
NM/maxillaandmandible
Graft
CHRCANOVIC ET AL.
462 HEAD & NECK—DOI 10.1002/HED MARCH 2016

TABLE2.
Cont
inue
d
Authors
Published
Healingperiod/
loading
Mean
6SD
ofmarginalbone
loss,m
mImplantsurface
modification(brand)
Radiotherapy
Hyperbaric
oxygen
therapy
Type
ofprosthetic
rehabilitation/jaws
receivingimplants
Studyenvironm
ent,
chem
otherapy,cases
ofdeath,
bone
graft,
smokers,alcohol
abuse,observations
Granstr€ om44
2005
NMNM
Turned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
21–120
Gy.528
implants
installedinan
irradiation
field,58implants
exposedtoradiotherapy
afterinstallation,and14
implantsinstalledinan
irradiationfieldand
wereadditionally
exposedtoradiotherapy
afterinstallation.
Perform
ed(protocolnot
inform
ed)
Fixed,overdenture/maxilla
andmandible
University,42patientsdied
duringthefollow-up(36G1
,6G2
),55
smokersinG1
,adjunctivechem
otherapy
in29
patients(177
implants),
nografts,implantsinthe
craniomaxillofacialarea
Shaw
etal45
2005
3–6mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)?(Im
tec,Imtec
Corporation,Ardm
ore,
OK),(Brånemark
1Imtec;
n5
35),
sandblastedandacid-
etched
(Frialit-2
system
,FriatecAG
,Mannheim,
Germ
any;
n5
196),TPS
(IMZ,InterporeInt.,
Irvine,CA
;n5
155)
40–66Gy.Implant
placem
entscheduled
approximately1yafter
surgeryor1yafter
completionof
postoperative
radiotherapy.
24patients,20
dives(2.4
atmfor9
0min)before
insertion
and10
dives
afterinsertion
Fixed,overdenture/maxilla
andmandible
University,grafts
(iliaccrest,
fibula,radius),1patient
died
duringthefollow-up
Teoh
etal46
2005
Atleast6
mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden),acid-etched
(Osseotite3i/Im
plant
Innovations,PalmBeach
Gardens,FL)
60–79Gy,given
overa6–
8wkperiod,6patients
received
radiotherapy
beforeimplant
placem
entand
1patient
hadradiotherapy
after
dentalimplantswere
placed.
3patients,20
sessions
at2.4atmbeforeimplant
placem
entand
another
10sessions
afterward
Fixed,overdenture/
mandible
Hospital,graft(fibulafree-
flap),submergedimplants,
2patientsdied
duringthe
follow-up,adjunctive
chem
otherapy
in6patients
Bodard
etal47
2006
7mo
NMSandblasted(Ciny,Serf
Dedienne
sant
� e,Lyon,
France;n
562),turned
(BrånemarkMKIII,Nobel
BiocareAB
,G€ oteborg,
Sweden;n
54),
sandblastedandacid-
etched
(Ankylos,
Dentsply-Friadent,
Mannheim,G
ermany;
n5
2)
Averagedose
ofradiotherapy
was
60.5Gy
(range,40–
100).The
delaybetween
radiotherapy
and
implantationwas
54mo
(range,4–120).
NPFixed,overdenture/maxilla
andmandible
Adjunctivechem
otherapy
in7
patients,graftN
M
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 463

TABLE2.
Cont
inue
d
Authors
Published
Healingperiod/
loading
Mean
6SD
ofmarginalbone
loss,m
mImplantsurface
modification(brand)
Radiotherapy
Hyperbaric
oxygen
therapy
Type
ofprosthetic
rehabilitation/jaws
receivingimplants
Studyenvironm
ent,
chem
otherapy,cases
ofdeath,
bone
graft,
smokers,alcohol
abuse,observations
Landes
and
Kov� acs
482006
Average25
d1y,1
60.8
(G1)
Sandblastedandacid-
etched
(SLA,
Straum
ann,Walderburg,
Switzerland;n
599),
TPS(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden;n
515)
57Gy,atsingledosesof
1.9Gy.The
average
timeperiod(range)
betweentumortherapy
andimplantplacement
was
16.5(3–55)mo,21
(4–55)mobetween
irradiationandimplant
insertion
and8(3–20)
mobetweenoperation
andimplantinsertionin
nonirradiatedpatients.
NMOverdenture(telescoped)/
mandible(interforaminal
only)
University,adjunctive
chem
otherapy
in13
patientsofG1
,90%
ofthe
patientsedentulous,non-
subm
ergedimplants,3
died
nottum
or-related,2
diabetics,no
bone
grafts
0.4
60.5
(G2)
2y, 1.4
60.9
(G1)
0.4
60.5
(G2)
Schepers
etal49
2006
Mean9mo
(G1)
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
60–68Gy
asaboostdose
ontheprimarytumor
site(within6wkof
ablationofthetumor)
and10–68Gy
onthe
symphysealarea,
implantswereplaced
duringtumorresection.
NPNM
/mandibular
(interforaminal)
University,nobone
grafts,7
patientsdied
duringthe
follow-up(22implants),34
implantswerenotusedfor
retentionofadental
prosthesis(15G1
,19G2
)
Mean
4.7mo(G2)
Yeritetal50
2006
Atleast6
mo
NMTPS(IM
Z,Friadent,
Mannheim,G
ermany;
n5
282),sandblasted
andacid-etched(Frialit-
2,Friadent,M
annheim,
Germ
any;
n5
26),
sandblastedandacid-
etched
(Xive,Friadent,
Mannheim,G
ermany;
n5
8).
Daily
fractions
of2Gy
givenon
25d(totaldose
of50
Gy).About4–8
wk
afterirradiation27show
[zaq
no="AQ2
"]?>
respective
surgeryofthecancer
was
perform
edtogether
primaryreconstruction
ofthemouthflooror
mandibulard
efectw
ithamicrovascularflap.
Implantinsertionwas
applied1.41
y(mean)
afterthe
reconstructive
surgery.
NPOverdenture/mandible
Chem
otherapy
perform
edin
allpatients,38
patients
died
duringthefollow-up
CHRCANOVIC ET AL.
464 HEAD & NECK—DOI 10.1002/HED MARCH 2016
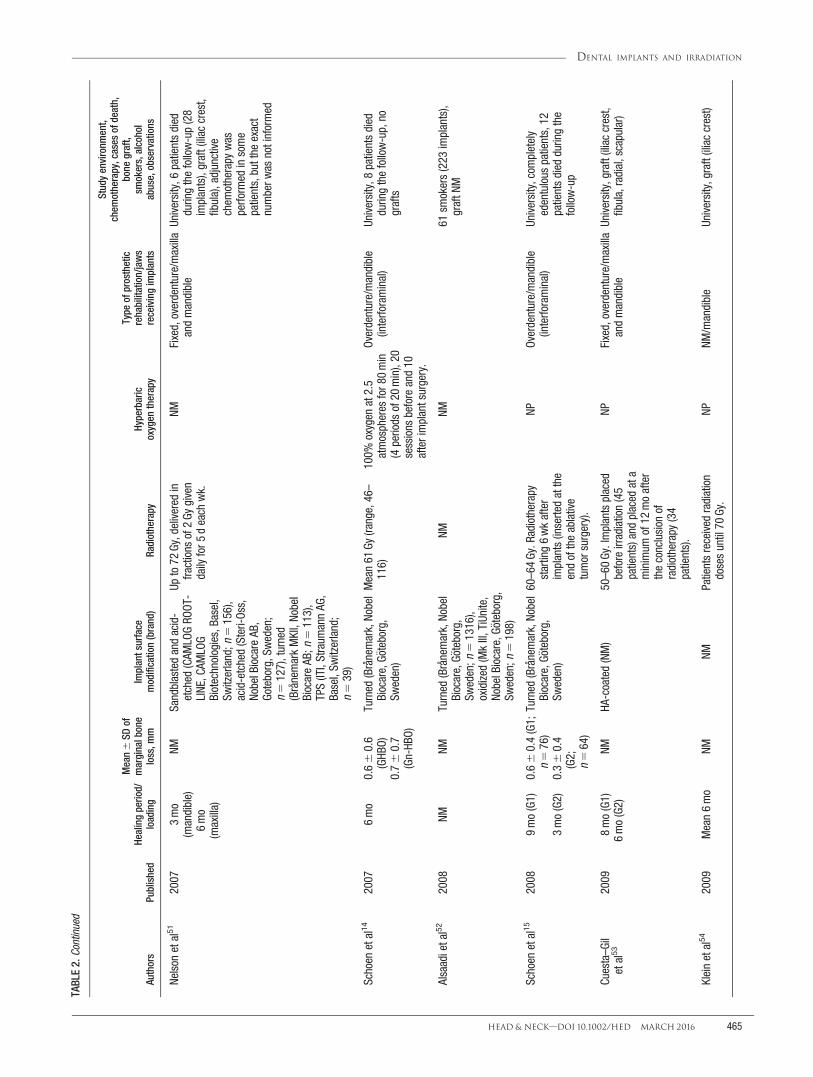
TABLE2.
Cont
inue
d
Authors
Published
Healingperiod/
loading
Mean
6SD
ofmarginalbone
loss,m
mImplantsurface
modification(brand)
Radiotherapy
Hyperbaric
oxygen
therapy
Type
ofprosthetic
rehabilitation/jaws
receivingimplants
Studyenvironm
ent,
chem
otherapy,cases
ofdeath,
bone
graft,
smokers,alcohol
abuse,observations
Nelson
etal51
2007
3mo
(mandible)
NMSandblastedandacid-
etched
(CAM
LOGRO
OT-
LINE
,CAM
LOG
Biotechnologies,Basel,
Switzerland;n
5156),
acid-etched(Steri-Oss,
NobelBiocareAB
,Goteborg,Sweden;
n5
127),turned
(BrånemarkMKII,Nobel
BiocareAB
;n5
113),
TPS(ITI,Straum
annAG
,Basel,Sw
itzerland;
n5
39)
Upto72
Gy,delivered
infractions
of2Gy
given
daily
for5
deach
wk.
NMFixed,overdenture/maxilla
andmandible
University,6
patientsdied
duringthefollow-up(28
implants),graft(iliac
crest,
fibula),adjunctive
chem
otherapy
was
perform
edinsome
patients,butthe
exact
numberw
asnotinformed
6mo
(maxilla)
Schoen
etal14
2007
6mo
0.6
60.6
(GHB
O)Turned
(Brånemark,Nobel
Biocare,G€ oteborg,
Sweden)
Mean61
Gy(range,46–
116)
100%
oxygen
at2.5
atmospheres
for8
0min
(4periods
of20
min),20
sessions
beforeand10
afterimplantsurgery.
Overdenture/mandible
(interforaminal)
University,8
patientsdied
duringthefollow-up,no
grafts
0.7
60.7
(Gn-HB
O)
Alsaadietal52
2008
NMNM
Turned
(Brånemark,Nobel
Biocare,G€ oteborg,
Sweden;n
51316),
oxidized
(MkIII,TiUnite,
NobelBiocare,G
€ oteborg,
Sweden;n
5198)
NMNM
61sm
okers(223
implants),
graftN
M
Schoen
etal15
2008
9mo(G1)
0.6
60.4(G1;
n5
76)
Turned
(Brånemark,Nobel
Biocare,G€ oteborg,
Sweden)
60–64Gy.R
adiotherapy
starting6wkafter
implants(insertedatthe
endoftheablative
tumorsurgery).
NPOverdenture/mandible
(interforaminal)
University,com
pletely
edentulous
patients,12
patientsdied
duringthe
follow-up
3mo(G2)
0.3
60.4
(G2;
n5
64)
Cuesta–G
iletal53
2009
8mo(G1)
NMHA
-coated(NM)
50–60Gy.Implantsplaced
beforeirradiation(45
patients)andplaced
ata
minimum
of12
moafter
theconclusion
ofradiotherapy
(34
patients).
NPFixed,overdenture/maxilla
andmandible
University,graft(iliaccrest,
fibula,radial,scapular)
6mo(G2)
Kleinetal54
2009
Mean6mo
NMNM
Patientsreceived
radiation
dosesuntil70
Gy.
NPNM
/mandible
University,graft(iliaccrest)
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 465

TABLE2.
Cont
inue
d
Authors
Published
Healingperiod/
loading
Mean
6SD
ofmarginalbone
loss,m
mImplantsurface
modification(brand)
Radiotherapy
Hyperbaric
oxygen
therapy
Type
ofprosthetic
rehabilitation/jaws
receivingimplants
Studyenvironm
ent,
chem
otherapy,cases
ofdeath,
bone
graft,
smokers,alcohol
abuse,observations
Korfage
etal16
2010
9mo(G1)
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
Dose>40
Gy,starting
within6wkafter
surgery.
NPOverdenture/mandible
University,com
pletely
edentulous
patients,grafts
NM,implantsinstalled
duringablativetumor
surgery,2-stageprotocol,
12and26
patientsdead
after1
and5y,
respectively.
3mo(G2)
Salinas
etal5
2010
Atleast6
mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
>6000
cGytothe
mandibleafterthe
fibula
flapbutbeforeimplant
placem
ent.Four
patients
received
theradiation
treatmentsafterimplant
placem
ent,and
thereforeadjunctiveHB
Owas
notusedinthese
patients.
20dives(100%
oxygen,
2.4atmospheres
absolutepressure,
90min)beforeand10
divesafterthe
placem
entofdental
implants
Fixed/mandible
University,graft(fibulaflaps),
adjunctivechem
otherapy
in11
patients,23
smokers,
19patientswith
alcohol
abuse
Barrow
man
etal55
2011
NMNM
Turned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden)
NM12
patients.20
treatments
beforeplacem
entof
dentalimplantsand10
treatmentssubsequently
at2–2.5ATAfor6
0min
Fixed,overdenture/maxilla
andmandible
Hospital,graft(iliac
crest,
fibula),submerged
implants,5
patientsdied
duringthefollow-up
Buddulaetal56
2011
NMNM
NMMean60.7Gy
(range,
50.2–67.5).The
mean
timeintervalbetween
radiationandfirst
implantplacementw
as3.4y.
57patients(14GB
G,43
GNB)
NM/maxillaandmandible
Privateclinic,graft(iliaccrest,
scapula,femur)
Hebereretal17
2011
Mean10.2wk
(maxilla)and
6.9wk
(mandible)
Provided
infor-
mationcon-
cerningSLA
vsmodSLA
inthemax-
illaand
mandible
Sandblastedandacid-
etched
(SLA,
Straum
ann,Walderburg,
Switzerland)
Radiotherapy
upto72
Gy,
delivered
infractions
of2Gy
givendaily
for5
deach
wkover6wk.
Implantplacementw
asperform
edaftera
minimum
of6moafter
theradiationtherapy.
NPFixed,overdenture/maxilla
andmandible
University,chemotherapy
perform
edinallpatients,no
smokers
CHRCANOVIC ET AL.
466 HEAD & NECK—DOI 10.1002/HED MARCH 2016

TABLE2.
Cont
inue
d
Authors
Published
Healingperiod/
loading
Mean
6SD
ofmarginalbone
loss,m
mImplantsurface
modification(brand)
Radiotherapy
Hyperbaric
oxygen
therapy
Type
ofprosthetic
rehabilitation/jaws
receivingimplants
Studyenvironm
ent,
chem
otherapy,cases
ofdeath,
bone
graft,
smokers,alcohol
abuse,observations
Sammartino
etal18
2011
6mo
(mandible)
NMMostfrequently
used:
“standardsolid-screw
implantw
ithmicrostructured
surface”
Dose
classifiedas<50
Gyand>50
Gy.The
mean
timebetweenthelast
irradiationandimplant
placem
entw
as9.4mo.
NPFixed,overdenture/maxilla
andmandible
University,nobone
grafts,no
smokers,no
diabetics
8mo
(maxilla)
Fenlon
etal57
2012
6mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden),titanium-
blasted(Astra,Astra
Tech
AB,M
€ olndal,
Sweden),porous-
beaded
(Endopore,
Sybron,O
range,CA
)
66Gy
NPFixed/maxillaandmandiblePublichospitals,145
implants
placed
in47
vascularized
grafts,56implantsplaced
inresidualbone
Linsen
etal59
2012
3–8mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden;n
5258),
titaniumoxideionized
(Straum
ann,Freiburg,
Germ
any;
n5
4)
Postoperativeradiation
therapywas
delivered
beforeimplant
placem
entto34
patientsindaily
fractions
of2Gy.The
targetvolumewas
treated
toatotaldoseof
36Gy
in26
patientsand
atotaldoseof60
Gyin
8patients.Thetim
eintervalbetweenradical
oralcancersurgery,
radiationtherapyand
implantplacement,
respectively,ranged
from6–126mo.
NPFixed,overdenture/maxilla
andmandible
University,submerged
implants,4
patientsdied
duringthefollow-up(16
implants),adjunctive
chem
otherapy
in59
implants,graft(79
implants)
Manchade
laPlataetal60
2012
3–6mo
NMReabsorbableBlastM
edia
(MGOsseous-Mozograu,
Valladolid,Spain)
50–70Gy.The
mean
periodfromtheendof
radiotherapy
toimplant
placem
entw
as33.4
618.1mo(range,
12–96).
In4patientswho
developed
osteoradionecrosis
Fixed,overdenture/maxilla
andmandible
University,6
patientswere
smokersanddrinkers,
adjunctivechem
otherapy
in4patients(39implants),
graft(iliac
crest,calvaria,
40implants)
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 467

TABLE2.
Cont
inue
d
Authors
Published
Healingperiod/
loading
Mean
6SD
ofmarginalbone
loss,m
mImplantsurface
modification(brand)
Radiotherapy
Hyperbaric
oxygen
therapy
Type
ofprosthetic
rehabilitation/jaws
receivingimplants
Studyenvironm
ent,
chem
otherapy,cases
ofdeath,
bone
graft,
smokers,alcohol
abuse,observations
Katsoulis
etal61
2013
NMNM
NM56–81Gy
NMFixed,overdenture/maxilla
andmandible
University,25patientswere
smokersand/ordrinkers,
adjunctivechem
otherapy
in13
patients(allinG1
),13
patientsdied
duringthe
follow-up
Jacobsen
etal58
2014
6mo
NMTurned
(Brånemark,Nobel
BiocareAB
,G€ oteborg,
Sweden),oxidized
(TiUnite,N
obelBiocare
AB,G
€ oteborg,Sw
eden),
sandblasted,acid-
etched,and
chem
ically
treated
(Neoss,N
eoss,
Cologne,Germ
any)
63Gy
(range,50–73).O
naverage,thedental
implantswereinserted
17mo(range,4–48
mo)
afterreconstruction,but
beforetheirradiation
NPFixed/mandible
University,5
patientsdied
duringthefollow-up(13
implants),78%
smokers,
52%
drankalcohol
regularly,graft(fibulaflap)
Abbreviations:N
M,notmentioned;NP
,notperform
ed;cGY,xxx;G
1,groupirradiatedpatients;G2
,group
nonirradiatedpatients;HA
,XXX;TPS,titanium
plasma-sprayed;GH
BO,group
patientstreated
with
hyperbaricoxygen
therapy;Gn-HBO
,group
patientsnottreated
with
hyperbaricoxygen
therapy;HB
O,hyperbaricoxygen
therapy;GB
G,XXX;GN
B,XXX;SLA,XXX;modSLA,xxx.
CHRCANOVIC ET AL.
468 HEAD & NECK—DOI 10.1002/HED MARCH 2016

occurrences in a total of 158 patients receiving 543 implants.Three22,24,47 of the 6 studies compared postoperative infectionbetween implants inserted in irradiated maxillae and irradiatedmandibles, and the other 3 studies28,48,59 between implantsinserted in irradiated and nonirradiated patients. Only 4 stud-ies14,15,17,48 provided information about marginal bone loss.Thirteen studies19,23,28,36,37,40,41,43,44,52,55,56,61 did not informof the healing period of the implants before loading.
Twenty-seven studies10,11,13–16,20,25–28,31–33,35,37,44–46,48–51,55,58,59,61
informed of the death occurrences among the patients during thefollow-up. Eighteen studies5,9,12,17,21,22,32,34,42,44,46–48,50,51,59–61 hadpatients who were also submitted to adjunctive chemo-therapy. In 2 studies,17,50 all patients were submitted tochemotherapy. Part of the patients in 9 stud-ies5,11,21,35,44,52,58,60,61 were smokers, and 2 studiesexcluded smokers.17,18 It was informed in 5 stud-ies5,11,58,60,61 that some of the patients were frequent con-sumers of alcoholic beverages.
Patients were submitted to bone grafting procedures in29 studies.5,9,11,20,22,26–29,31,33,36,38–43,45,50,51,53,55–61 Fourstudies18,37,48,49 evaluated implants in native bone only.Eighteen studies5,9,14–16,20,21,29,31,35,36,38,40,48–50,54,58 eval-uated implants inserted in the mandible only, of which 4studies14,15,48,49 assessed the implants in the inter-foraminal region only, and 3 studies34,38,42 only in themaxilla. HBO was performed in patients of14 studies.5,10,11,14,30,34,37,43–46,55,56,60
The most commonly used implants used was the turnedBranemark (Nobel Biocare AB, G€oteborg, Sweden), in 35 stud-ies,5,9,10,12,14–16,19–22,24–27,30–32,34,35,37–39,42,44–47,49,51,52,55,57–59 butnot exclusively in 12 studies.9,10,20,25,26,39,42,45–47,51,52 Eight stud-ies23,36,40,41,43,54,56,61 did not inform of what kind of implantswas used. Sixteen studies5,12,13,16,18,34,35,39,40,42,45,46,50–52,60
informed whether there was a statistically significant differenceor not between the implant failure rates between the procedures,whereas 1 study28 showed no implant failures. Thirteen stud-ies9,10,13,14,17,21,24,28,32,47,48,51,58 provided information about theuse of prophylactic antibiotics, and only 3 studies13,28,48 aboutmouth rinse by the patients.
The comparisons concerning the outcome “implantfailure” are summarized in Table 3.
Quality assessment
Each trial was assessed for risk of bias, and the scoresare summarized in Table 4. All studies were judged to beat high risk of bias.
Meta-analysis
A summary of the meta-analyses comparisons concern-ing implant failures is presented in Table 3. The forestplots are presented in Figures 2–11.
Six studies22,24,28,47,48,59 provided information aboutpostoperative infection. A fixed-effects model was used,because of lack of statistically significant heterogeneityeither when comparing implants inserted in irradiatedversus in nonirradiated patients (p 5 .52; I2 5 0%;Figure 12) or when comparing implants inserted in irra-diated maxilla versus in irradiated mandible (p 5 .86;I2 5 0%; Figure 13). The results showed that therewas no statistically significant difference in the 2 com-parisons (RR 5 1.40; 95% CI 5 0.73–2.68; p 5 .31
and RR 5 0.81; 95% CI 5 0.09–7.27; p 5 .85,respectively).
Only 2 studies15,48 provided information about the mar-ginal bone loss with SD, necessary for the calculation ofcomparisons in continuous outcomes, comparing implantsinserted in irradiated versus in nonirradiated patients.There was statistically significant difference (mean differ-ence 5 0.62; 95% CI 5 0.21–1.03; p 5 .003; heterogene-ity: I2 5 92%; p < .00001, random-effects model; Figure14) between the groups concerning the marginal boneloss, favoring nonirradiated patients. One study14 pro-vided information comparing marginal bone loss inimplants inserted in irradiated patients being submittedversus not submitted to HBO. A meta-analysis for thiscomparison was not performed.
Publication bias
The funnel plot did not show asymmetry when thestudies reporting the outcome “implant failure” in thecomparison between irradiated and nonirradiated patientswas analyzed, indicating possible absence of publicationbias (see Figure 15).
DISCUSSIONOne relevant question in the present study is whether
the lack of a difference between irradiated and nonirradi-ated patients in some studies concerning implant failurerates is a real finding or is due to the lack of statisticalpower, given the small number of patients and/orimplants per group. However, a statistically and clinicallysignificant difference favoring the nonirradiated patientswas found after the meta-analyses, stressing the impor-tance of meta-analyses to increase sample size of individ-ual trials to reach more precise estimates of the effects ofinterventions. The significantly higher failure rates in irra-diated compared to nonirradiated patients might be causedby the long-term effects of reduced vascularization com-promising the implantation site.50 In general, radiationtherapy has 2 antagonistic effects with regard to recoveryof irradiated tissue: a short-term positive cellular effectresulting in the improvement of reduced bone-healingcapacity,62 and a long-term negative effect resulting inpermanent damage of osteoprogenitor cells63 and a grad-ual, progressive endarteritis obliterans, with thrombosis ofsmall blood vessels, fibrosis of the periosteum andmucosa, and damage to osteocytes, osteoblasts, and fibro-blasts.64 Moreover, irradiation of tissues that contain inte-grated implants increases the risk of soft tissuedehiscences around the implants, and osteoradionecrosismay lead to loss of the implants.65 This failure differenceafter radiation therapy was observed in several studiesincluded here, although the radiation dosage and observa-tion period varied in the majority of these cases.
Another aspect to consider is the use of HBO. There isno strict consensus about the use of adjunctive HBO ther-apy, but many studies stressed the advantages of HBOtreatment for wound healing in the irradiated soft andhard tissue.50 As a result, some authors use HBO as anadditive therapy when implant therapy in irradiated boneis planned. It is stated in the literature that HBO resultsin an increased oxygen tension in the irradiated ischemic
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 469

TABLE3.
Summaryofthecomparisonsconcerning
implantfailures
No.ofimplantsfailed/placed
(%)
Risk
ratio
(95%
CI)
pvalue
Heterogeneity
No.ofstudies
Forestplot–figurenumber
Irradiated
Nonirradiated
2.18
(1.71–2.79)
<.00001
I25
52%,p
5.0002,
random
-effectsmodel
37,5,9,11,12,15,16,19,20,25,26,28,29,31,34,35,37–42,44–46,48–55,57–61
2640/3914
(16.35)
684/14514(4.71)
Irradiated
1HB
OIrradiatedwithoutH
BO0.61
(0.27–1.39)
.24
I25
86%,p<.00001,
random
-effectsmodel
814,30,34,37,43–46
377/768
(10.02)
244/769(31.73)
Irradiatedmaxilla
Irradiatedmandible
3.16
(1.76–5.68)
.0001
I25
70%,p<.0001,
random
-effectsmodel
1710,13,17–19,22–24,26,30,32,33,43,47,56,59,60
4128/667(19.19)
121/1771
(6.83)
Irradiatedmaxilla
Nonirradiatedmaxilla
2.85
(1.07–7.57)
.04
I25
0%,p
5.67,
fixed-effectsmodel
219,59
54/33
(12.12)
218/3121
(6.98)
Irradiatedmandible
Nonirradiatedmandible
0.80
(0.27–2.34)
.68
I25
58%,p
5.07,
random
-effectsmodel
419,26,45,59
641/453
(9.05)
80/5191(1.54)
Irradiatedgrafted
Irradiatednativebone
1.35
(0.93–1.94)
.44
I25
48%,p
5.06,
random
-effectsmodel
95,27,29,31,41,43,56,58,61
741/325
(12.61)
63/542
(11.62)
Irradiatedgrafted
Nonirradiatedgrafted
3.31
(2.02–5.41)
<.00001
I25
27%,p
5.24,
fixed-effectsmodel
65,29,31,36,58,61
828/147
(19.05)
28/301
(9.30)
Irradiatednativebone
Nonirradiatednativebone
2.74
(1.49–5.04)
.001
I25
24%,p
5.26,
fixed-effectsmodel
65,31,40,50,58,61
960/304
(19.74)
12/198
(6.06)
Higherirradiationdose
Lowerirradiationdose
1.64
(0.98–2.75)
.06
I25
47%,p
5.08,
random
-effectsmodel
713,18,21,30,40,45,54
1098/542
(18.08)
51/515
(9.90)
<12
mo
>12
mo
1.37
(0.76–2.45)
.29
I25
64%,p
5.06,
random
-effectsmodel
313,18,50
1170/445
(15.73)
58/505
(11.49)
Abbreviations:95%
CI,95%
confidenceinterval;<
12mo,>12
mo,implantsinserted<12
moand>12
moafterthe
endofradiotherapy,respectively.
CHRCANOVIC ET AL.
470 HEAD & NECK—DOI 10.1002/HED MARCH 2016

bone and provokes capillary neoangiogenesis63 and boneformation.66 The exact correlation between HBO doseand duration of antifibrotic response is not yet settled. Ithas been convincingly demonstrated that such treatmentdramatically decreases the risk of trauma-induced osteora-dionecrosis by promoting vascular proliferation, collagen
synthesis, bone remodeling activities, and healing of bonewounds in irradiated tissues.67 Moreover, HBO therapyincreases the amount of force necessary to unscrew inte-grated titanium implants in irradiated bone,68 which sug-gests that promoted integration has occurred. Larsenet al66 showed a difference of 13.9% in mean percent of
TABLE 4. Results of quality assessment
Authors PublishedSequence generation
(randomized?)Allocation
concealmentIncomplete outcomedata addressed Blinding
Estimated potentialrisk of bias
Albrektsson et al19 1988 No Inadequate Yes No HighSclaroff et al20 1994 No Inadequate No No HighFranz�en et al21 1995 No Inadequate No No HighAldegheri et al22 1996 No Inadequate No No HighEckert et al23 1996 No Inadequate No No HighWeischer et al9 1996 No Inadequate No No HighAli et al24 1997 No Inadequate No No HighChan et al25 1997 No Inadequate Yes No HighEsser and Wagner26 1997 No Inadequate Yes No HighJisander et al10 1997 No Inadequate Yes No HighKeller et al27 1997 No Inadequate Yes No HighMarker et al28 1997 No Inadequate Yes No HighMcGhee et al29 1997 No Inadequate No No HighNiimi et al30 1997 No Inadequate No No HighRoumanas et al31 1997 No Inadequate Yes No HighAndersson et al32 1998 No Inadequate Yes No HighBrogniez et al33 1998 No Inadequate Yes No HighIhara et al34 1998 No Inadequate No No HighEsser et al35 1999 No Inadequate Yes No HighFoster et al36 1999 No Inadequate No No HighGranstr€om et al37 1999 No Inadequate Yes No HighKeller et al38 1999 No Inadequate No No HighMericske-Stern et al11 1999 No Inadequate Yes No HighWeischer and Mohr39 1999 No Inadequate No No HighWerkmeister et al40 1999 No Inadequate No No HighGoto et al41 2002 No Inadequate No No Highvan Steenberghe et al12 2002 No Inadequate No No HighVisch et al13 2002 No Inadequate Yes No HighCao and Weischer42 2003 No Inadequate Yes No HighGranstr€om43 2003 No Inadequate No No HighGranstr€om44 2005 No Inadequate Yes No HighShaw et al45 2005 No Inadequate Yes No HighTeoh et al46 2005 No Inadequate Yes No HighBodard et al47 2006 No Inadequate No No HighLandes and Kov�acs48 2006 No Inadequate No No HighSchepers et al49 2006 No Inadequate Yes No HighYerit et al50 2006 No Inadequate No No HighNelson et al51 2007 No Inadequate Yes No HighSchoen et al14 2007 No Inadequate Yes No HighAlsaadi et al52 2008 No Inadequate No No HighSchoen et al15 2008 No Inadequate Yes No HighCuesta–Gil et al53 2009 No Inadequate No No HighKlein et al54 2009 No Inadequate Yes No HighKorfage et al16 2010 No Inadequate Yes No HighSalinas et al5 2010 No Inadequate No No HighBarrowman et al55 2011 No Inadequate Yes No HighBuddula et al56 2011 No Inadequate No No HighHeberer et al17 2011 No Inadequate No No HighSammartino et al18 2011 No Inadequate Yes No HighFenlon et al57 2012 No Inadequate No No HighLinsen et al59 2012 No Inadequate Yes No HighMancha de la Plata et al60 2012 No Inadequate Yes No HighKatsoulis et al61 2013 No Inadequate Yes No HighJacobsen et al58 2014 No Inadequate Yes No High
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 471

integration after 4 months in irradiated versus nonirradi-ated animals. This difference dropped to 6.38% when ani-mals received HBO before and after implantation. Thedifference was shown to be significant, although withoutestablishing whether this reduction is of significance inrelation to implant support. As long as the direct bone-implant interface is sufficiently large to support the supra-structure, it can be argued that additional support to theimplant surface is unnecessary, particularly in light ofpatient inconvenience and the cost of HBO treatment.32
Moreover, results from animal experiments may onlypartly be extrapolated to clinically relevant conditions forendosseous implants in irradiated bone. Apart from con-siderable methodological limitations in the simulation ofthe therapeutic reality and temporal restrictions, eventsduring the follow-up (induction of neoplasms, loss ofimplants, osteoradionecrosis, etc), differences related tocell cycles, structural peculiarities of the bone matrix, theperiosteal situation, and the enzyme system of the specieshave to be taken into account.69 It is no less impor-tant to mention that several studies included
here9,10,14,15,17,19,21,23,26–28,30–33,35,47–49,51,59,60 demon-strated a high survival rate for the implants placed in irra-diated jaws without the use of adjunctive HBO therapy. Itmight have been expected that there was a significantlyhigher failure for patients submitted to HBO, becausemost of the patients selected for HBO could have been ata higher risk for osteoradionecrosis because of a higherirradiation dose, and consequently at a higher risk ofimplant loss. For example, the difference in implant sur-vival between the HBO and non-HBO treated patientsobserved in the study of Schoen et al14 was remarkable,but was mainly caused by 1 HBO-treated patient whodeveloped osteoradionecrosis and subsequently lost all 4implants. However, the present meta-analysis found nostatistically significant difference when comparingimplant failures in irradiated patients receiving or notHBO, which is most likely the result of the small samplesize in many studies and selection bias. There are still norandomized, controlled, double-blind studies conducted toprove that HBO really has a significant osseointegrationstimulating effect in irradiated patients. However, there
FIGURE 2. Forest plot for the event “implant failure” in the comparison between irradiated versus nonirradiated patients. [Color figure can beviewed in the online issue, which is available at wileyonlinelibrary.com.]
CHRCANOVIC ET AL.
472 HEAD & NECK—DOI 10.1002/HED MARCH 2016

are certain technical difficulties related to designing sucha study, such as blinding a chamber treatment and thedesign of the placebo treatment.37
The timespan between the irradiation and the implantsurgery may influence the survival of the dental implants,but recommendations for an optimal time interval areinconsistent. Dental implants can be inserted during theablative surgery or after completed radiotherapy. Whenthe implants are inserted during the ablative surgical ses-sion, a large part of the integration will occur in theperiod between surgery and radiotherapy (ie, within 4–6weeks).70 However, a clear majority of studies herereviewed report on implants installed after radiotherapy.The advantage of placement after radiotherapy is that theanatomic situation, residual function, and prognosis canbe taken into account in the decision of whether to useimplants. Moreover, tumor recurrence has been reported
to occur most often between 8 and 12 months after sur-gery, according to 1 study,71 or within 2 years accordingto another one,21 thus, oral rehabilitation may be delayeduntil this period of highest risk has passed. The disadvant-age is that patients are often psychologically and physi-cally weakened by the therapy, resulting in postponementor even cancellation of prosthetic rehabilitation.72 More-over, after radiotherapy, the vascularization and regenera-tive ability of the irradiated tissues can be decreased,which may lessen the prospect of successful osseointegra-tion of the dental implants.11 The subject is controversial.King et al73 indicated that blood vessels that weredestroyed radiologically show partial recovery after 3 to 6months. W€achter and Stoll74 conducted histomorphomet-ric studies, the results of which state that implantationcan be performed, at the earliest, 12 to 18 months afterthe conclusion of irradiation. Jacobsson62 reported an
FIGURE 3. Forest plot for the event “implant failure” in the comparison between irradiated patients receiving versus not receiving hyperbaricoxygen (HBO). [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
FIGURE 4. Forest plot for the event “implant failure” in the comparison between irradiated maxilla versus irradiated mandible. [Color figure can beviewed in the online issue, which is available at wileyonlinelibrary.com.]
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 473

improvement in the bone healing capacity by a factor ofalmost 2.5 during a 12-month period after irradiation.According to the author, functional self-regeneration ofthe damaged tissue would provide sufficient implant heal-ing and osseointegration capacities of the bone 1 yearafter radiation therapy. On the other side, Marx and John-son63 stated that after 6 months, fibrosis is expected tostart in the irradiated tissues as a result of reduced cellreproducibility and progressive ischemia. This processwill increase with time, especially when curative doses ofradiotherapy have been given. The present meta-analysisfound no statistically significant difference when failureof implants was compared for the implants installedbefore and after a period of 12 months from the radio-therapy, and this is most likely the fact that only 3 stud-ies13,18,50 performed this comparison. Two other studiesdid not report a defined time point to make the compari-son, but did not find any influence of time of implanta-tion on the implant failure rates.10,48
Concerning the radiation dose, the implants insertedinto locations irradiated with �50 Gray (Gy) in 4 stud-ies13,18,21,54 had a lower survival rate than implants inlocations that are irradiated with <50 Gy. The same hap-pened in another study,40 but comparing different dosethresholds (>54 vs <54 Gy). Generally, high radiationdoses >50 Gy have been reported to result in chroniccomplications like radioxerostomia and impaired woundhealing.75 Also, irradiation doses above 65 Gy may sig-nificantly increase the risk of development of osteoradio-necrosis,76 which may also be a reason for implantfailures. Moreover, it was shown that there is a distinctdose-dependent relationship between the duration andextent of irradiation and the resulting reduced osteogene-
sis.77 Bone healing was delayed at lower doses of radia-tion with the formation of more impaired fibrous tissueand nonlamellar bone, and bone healing was severely dis-turbed at radiation doses used to treat head and neck can-cer.78 However, the present meta-analysis was not able tofind a significantly higher risk of losing an implant inpatients receiving higher doses of radiotherapy. Onceagain, this result may have been influenced by the limitednumber of studies performing this comparison. The com-parable survival rates of both groups in the study of Niimiet al30 and even a higher survival rate of implants insertedinto locations of higher doses in the study of Shaw et al45
might be caused by the effects of reduced vascularizationthat compromises both irradiated and nonirradiatedlocations.63
Another circumstance that may increase implant failureis the anatomy of the implantation site. Oral anatomymay change after ablative surgery and eventually afterreconstruction by grafts and flaps, and the resultingdefects and bulky areas or the presence of insufficientsoft tissues for coverage may compromise prosthetic reha-bilitation.41,79 One could speculate that the bony sectionof the graft may have been nonvital from the time ofplacement or that placement of implants in the graftedblock of bone may have compromised the vitality of theblock.57 Some studies on this topic address the increasedimplant loss in augmented bone to the reduced primarystability of dental implants because of impaired mechani-cal bone quality as well as to increased bone resorptionkinetics.80–82 The lower survival of implants in thegrafted bone may be the result of differences in bonequality, bone volume, and revascularization comparedwith the original residual bone. There is also a difference
FIGURE 5. Forest plot for the event “implant failure” in the comparison between irradiated versus nonirradiated maxilla. [Color figure can beviewed in the online issue, which is available at wileyonlinelibrary.com.]
FIGURE 6. Forest plot for the event “implant failure” in the comparison between irradiated versus nonirradiated mandible. [Color figure can beviewed in the online issue, which is available at wileyonlinelibrary.com.]
CHRCANOVIC ET AL.
474 HEAD & NECK—DOI 10.1002/HED MARCH 2016

when it comes to the graft type. Vascularized bone flapsmaintain their viability even after prolonged periods ofischemia provided that the medullary nutrient blood sup-ply is later restored.83 This is unlike nonvascularizedbone grafts, where implant placement must await alengthy delay to allow for “creeping substitution”84 tooccur. Even with all these disadvantages, the presentstudy found no statistically significant difference concern-ing failures of dental implants when inserted in irradiatedgrafted bone or in irradiated native bone. This could berelated to the assumption that the clinical courses ofimplants may not be affected by the presence of graftedbone once the graft has succeeded,41 even if this is diffi-cult to ascertain, as not every study included in the pres-ent review provided detailed information about graftingprocedures. On the other side, when the failure rates werecompared in irradiated versus nonirradiated patients, therewas a statistically significant difference for implantsinserted in grafted bone and in native bone. Once again,when the term “irradiation” is inserted into the equation,there are significant differences.
Concerning the different jaws, it was observed in 1study13 that the most dominant variable influencingimplant survival in irradiated bone is the implant’s loca-
tion in the maxilla or mandible. The side effects ofradiotherapy seem to be more serious in the mandiblethan in the maxilla because of the inferior blood supplyof the former bone.10 However, according to the resultsof the present meta-analysis, it seems that implant fail-ure in the maxilla follows a similar course in irradiatedand nonirradiated patients. The results comparingimplant failures in irradiated and nonirradiated max-illa19,59 and in irradiated and nonirradiated mandi-ble19,26,45,59 must be interpreted with caution because ofthe limited number of studies reporting this information(2 and 4, respectively). It is also important to considerwhether all implants had been inserted in the field ofirradiation, even though this information was rarely pro-vided by the included studies. In the case of the mandi-ble, for example, the external beam radiation therapy fororal malignancies does not always include the wholemandible and, hence, implants inserted anterior to themental foramina might be inserted in a field of lowerradiation dose. This will naturally affect the outcome forthe implants.37
When it comes to postoperative infection, soft tissuemay be affected by irradiation, and the causes might bethe postoperative and postirradiation xerostomia, different
FIGURE 7. Forest plot for the event “implant failure” in the comparison between irradiated grafted bone versus irradiated native bone. [Color figurecan be viewed in the online issue, which is available at wileyonlinelibrary.com.]
FIGURE 8. Forest plot for the event “implant failure” in the comparison between irradiated versus nonirradiated grafted bone. [Color figure can beviewed in the online issue, which is available at wileyonlinelibrary.com.]
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 475

saliva quantity and quality, and altered microflora as wellas the presence of scar tissues after reconstruction and theloss of attached and keratinized gingiva adjacent to theimplants.48,50 It may be suggested that stable soft tissueconditions are crucial for the possibility to perform oralhygiene and can influence the clinical performance of theimplants in irradiated patients.17 This could influence theincidence of peri-implantitis and consequently the mar-ginal bone loss. The present meta-analysis showed thatthere was a statistically significant difference between the
irradiated versus nonirradiated patients concerning themarginal bone loss, favoring nonirradiated patients. How-ever, this result must be interpreted with caution becauseof the limited number of studies that evaluated the condi-tion. The same can be said about the meta-analysis resultsfor the outcome postoperative infection.
The studies included here have a considerable numberof confounding factors, and most of the studies, if not all,did not inform how many implants were inserted and sur-vived/lost in several different conditions.
FIGURE 9. Forest plot for the event “implant failure” in the comparison between irradiated versus nonirradiated native bone. [Color figure can beviewed in the online issue, which is available at wileyonlinelibrary.com.]
FIGURE 10. Forest plot for the event “implant failure” in the comparison between higher versus lower irradiation dose. [Color figure can be viewedin the online issue, which is available at wileyonlinelibrary.com.]
CHRCANOVIC ET AL.
476 HEAD & NECK—DOI 10.1002/HED MARCH 2016

First, bone resections may result in unfavorable pros-thetic circumstances by producing bulky and soft areas.In these situations, (removable) prosthetic appliances areoften complicated and may cause overloading of theimplants.79 This negative influence may be responsiblefor lower survival rate of implants inserted into jawstreated with bone resections, compared with that ofimplants inserted into jaws that did not undergo bonesurgery.13
Second, the percentage of patients who had receivedpostoperative radiotherapy may have decreased over timeamong the survivors, as it was observed in many studies,which could have contributed to the relatively low failurerate of implants in irradiated bone. Those patientsselected to be submitted to radiotherapy may be thepatients with cancers of the worst prognosis.
Third, in the analysis of implant survival, it is impor-tant to ascertain whether the implants that were placedand considered osseointegrated were, in fact, used for thefinal implant-supported prosthesis.85 A longer follow-upperiod can lead to an increase in the failure rate, espe-cially if it extended beyond functional loading, may leadto an increase in the failure rate, because other prostheticfactors can influence implant failure from that pointonward. This might have led to an underestimation ofactual failures in some studies. However, it is hard todefine what would be considered a short follow-up periodto evaluate implant failures when comparing thesetechniques.
Fourth, most patients with oral cancer have a history ofpoor oral hygiene, smoking, and drinking.29 The local
environment is less favorable to dental implants than inhealthy subjects. Saliva quantity and quality as well asoral microflora change considerably after salivary glandresection. Landes and Kov�acs48 observed that plaque andperi-implant bleeding index remained typically high com-pared with noncancer patients. Oral hygiene and compli-ance were limited, although patients received individualoral hygiene instructions. On the other hand, a rapid pla-que accumulation and bleeding tendency was concomitantwith postoperative and postirradiation xerostomia, alteredmicroflora, saliva quantity and quality, smoking, anddrinking. Irradiation leaves a less viable bone that isprone to infection; furthermore, oral xerostomia postradio-therapy complicates the situation.40
Fifth, as oral cancer represents around 3% of the totalcancer incidence,86 most of the studies were not able tocreate a homogenous collective for more factors, such asoral squamous cell carcinoma, edentulousness, or severelyreduced tooth number. By breaking down the study byeach variable, the authors of the studies may have hadserious doubts regarding the clinical value in a study thatis not totally homogenous in tumor staging, precise doseof irradiation, etc. It can be said that in order to have suf-ficient group sizes and a clinically relevant conclusion,groups in the studies were therefore not supposedly bro-ken down further. Homogenous or matched collectiveshave a somewhat higher significance but they tend to beinhibited by small case numbers.48
Sixth, it is known that the surface properties of dentalimplants, such as topography and chemistry, are relevantfor the osseointegration process influencing ionic
FIGURE 11. Forest plot for the event “implant failure” in the comparison between insertion of implants within 12 months after radiotherapy versusafter 12 months after radiotherapy. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
FIGURE 12. Forest plot for the event “postoperative infection” in the comparison between irradiated versus nonirradiated patients. [Color figurecan be viewed in the online issue, which is available at wileyonlinelibrary.com.]
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 477
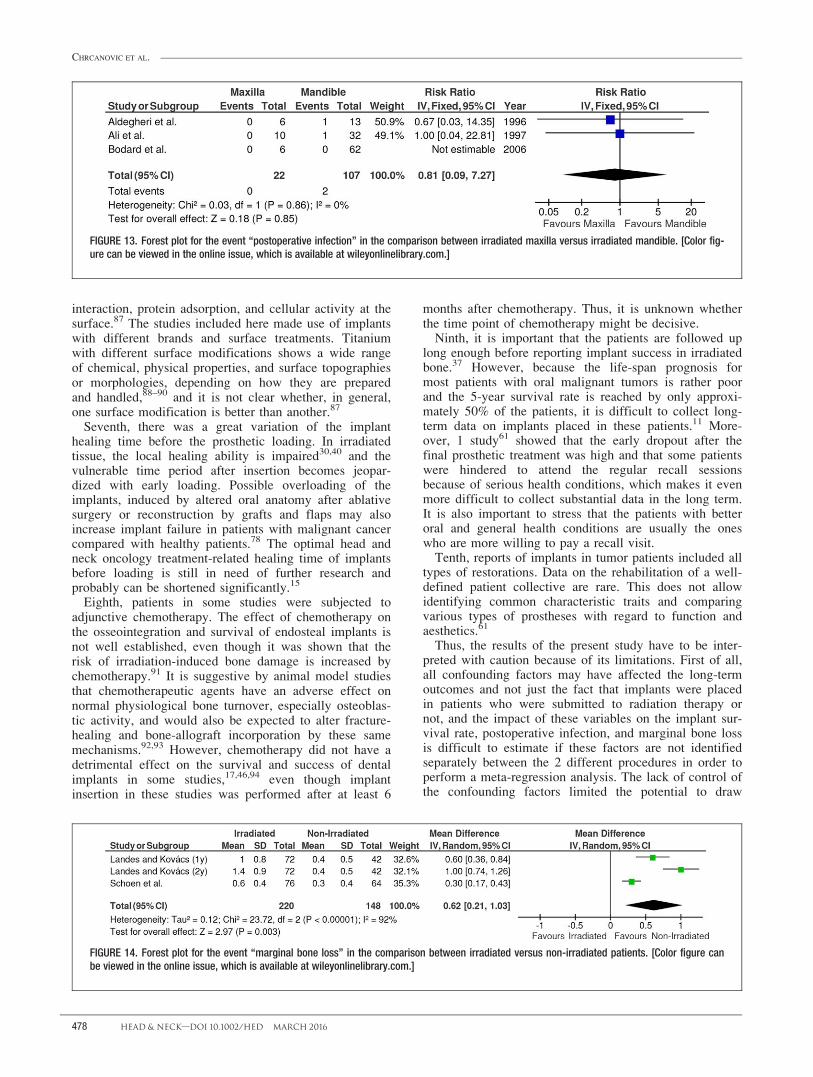
interaction, protein adsorption, and cellular activity at thesurface.87 The studies included here made use of implantswith different brands and surface treatments. Titaniumwith different surface modifications shows a wide rangeof chemical, physical properties, and surface topographiesor morphologies, depending on how they are preparedand handled,88–90 and it is not clear whether, in general,one surface modification is better than another.87
Seventh, there was a great variation of the implanthealing time before the prosthetic loading. In irradiatedtissue, the local healing ability is impaired30,40 and thevulnerable time period after insertion becomes jeopar-dized with early loading. Possible overloading of theimplants, induced by altered oral anatomy after ablativesurgery or reconstruction by grafts and flaps may alsoincrease implant failure in patients with malignant cancercompared with healthy patients.78 The optimal head andneck oncology treatment-related healing time of implantsbefore loading is still in need of further research andprobably can be shortened significantly.15
Eighth, patients in some studies were subjected toadjunctive chemotherapy. The effect of chemotherapy onthe osseointegration and survival of endosteal implants isnot well established, even though it was shown that therisk of irradiation-induced bone damage is increased bychemotherapy.91 It is suggestive by animal model studiesthat chemotherapeutic agents have an adverse effect onnormal physiological bone turnover, especially osteoblas-tic activity, and would also be expected to alter fracture-healing and bone-allograft incorporation by these samemechanisms.92,93 However, chemotherapy did not have adetrimental effect on the survival and success of dentalimplants in some studies,17,46,94 even though implantinsertion in these studies was performed after at least 6
months after chemotherapy. Thus, it is unknown whetherthe time point of chemotherapy might be decisive.
Ninth, it is important that the patients are followed uplong enough before reporting implant success in irradiatedbone.37 However, because the life-span prognosis formost patients with oral malignant tumors is rather poorand the 5-year survival rate is reached by only approxi-mately 50% of the patients, it is difficult to collect long-term data on implants placed in these patients.11 More-over, 1 study61 showed that the early dropout after thefinal prosthetic treatment was high and that some patientswere hindered to attend the regular recall sessionsbecause of serious health conditions, which makes it evenmore difficult to collect substantial data in the long term.It is also important to stress that the patients with betteroral and general health conditions are usually the oneswho are more willing to pay a recall visit.
Tenth, reports of implants in tumor patients included alltypes of restorations. Data on the rehabilitation of a well-defined patient collective are rare. This does not allowidentifying common characteristic traits and comparingvarious types of prostheses with regard to function andaesthetics.61
Thus, the results of the present study have to be inter-preted with caution because of its limitations. First of all,all confounding factors may have affected the long-termoutcomes and not just the fact that implants were placedin patients who were submitted to radiation therapy ornot, and the impact of these variables on the implant sur-vival rate, postoperative infection, and marginal bone lossis difficult to estimate if these factors are not identifiedseparately between the 2 different procedures in order toperform a meta-regression analysis. The lack of control ofthe confounding factors limited the potential to draw
FIGURE 13. Forest plot for the event “postoperative infection” in the comparison between irradiated maxilla versus irradiated mandible. [Color fig-ure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
FIGURE 14. Forest plot for the event “marginal bone loss” in the comparison between irradiated versus non-irradiated patients. [Color figure canbe viewed in the online issue, which is available at wileyonlinelibrary.com.]
CHRCANOVIC ET AL.
478 HEAD & NECK—DOI 10.1002/HED MARCH 2016

robust conclusions. Second, most of the included studieshad a retrospective design, and the nature of a retrospec-tive study inherently results in flaws. These problemswere manifested by the gaps in information and incom-plete records. Furthermore, all data rely on the accuracyof the original examination and documentation. Itemsmay have been excluded in the initial examination or notrecorded in the medical chart.95–97 Third, much of theresearch in the field is limited by small cohort size andshort follow-up periods.
The failure of dental implants in irradiated patients istherefore subjected to many considerations and predict-ability is dependent upon issues like the use of HBO andchemotherapy, the timing of the implant placement inrelation to radiation therapy, the radiation dosage, theinsertion of implants in native of grafted bone, selectionof anatomic site, the patients’ oral hygiene conditions andhabits (smoking, drinking), the implant surface treatment,the prosthetic loading conditions, the type of prostheticrestoration, the period of follow-up, and risk ofosteoradionecrosis.
CONCLUSIONThe results of the present review should be interpreted
with caution because of the presence of uncontrolled con-founding factors in the included studies, none of themrandomized. Within the limitations of the existing investi-gations, the present study suggests that irradiation nega-tively affects the survival rates of dental implants, as wellas the difference in the implant location (ie, maxilla ormandible). The study has failed to support the effective-ness of HBO therapy in irradiated patients requiring den-tal implants. It also suggests that there is no statisticallysignificant difference in survival when implants areinserted before or after 12 months after the radiotherapy.It was observed that there was a tendency to a lower sur-vival rate of implants inserted in the patients submitted tohigher irradiation doses.
AcknowledgmentsThe authors thank Dr. Christian Walter, Dr. V�eroniqueBrogniez, and Dr. Jean-Louis Blanc for having sent us
their articles, and Dr. Sabine Linsen, Dr. Regina Mer-icske–Stern, and Dr. Mar�ıa Mancha de la Plata, who pro-vided us with some missing information about theirstudies.
REFERENCES1. Chrcanovic BR, Albrektsson T, Wennerberg A. Reasons for failures of oral
implants. J Oral Rehabil 2014;41:443–476.2. Vissink A, Burlage FR, Spijkervet FK, Jansma J, Coppes RP. Prevention
and treatment of the consequences of head and neck radiotherapy. Crit RevOral Biol Med 2003;14:213–225.
3. Chrcanovic BR, Reher P, Sousa AA, Harris M. Osteoradionecrosis of thejaws–a current overview–part 1: physiopathology and risk and predisposingfactors. Oral Maxillofac Surg 2010;14:3–16.
4. Chrcanovic BR, Reher P, Sousa AA, Harris M. Osteoradionecrosis of thejaws–a current overview–part 2: dental management and therapeuticoptions for treatment. Oral Maxillofac Surg 2010;14:81–95.
5. Salinas TJ, Desa VP, Katsnelson A, Miloro M. Clinical evaluation ofimplants in radiated fibula flaps. J Oral Maxillofac Surg 2010;68:524–529.
6. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferredreporting items for systematic reviews and meta-analyses: the PRISMAstatement. Int J Surg 2010;8:336–341.
7. Higgins JPT, Green S, Cochrane Collaboration. Cochrane handbook forsystematic reviews of interventions. Chichester, England; Hoboken, NJ:Wiley–Blackwell; 2008. p 649.
8. Egger MS, Smith GD. Principles of and procedures for systematic reviews.In: Egger MS, Smith GD, Altman DG, editors. Systematic Reviews inHealth Care: Meta-analysis in Context. London, UK: BMJ Books; 2003. pp23–42.
9. Weischer T, Schettler D, Mohr C. Concept of surgical and implant-supported prostheses in the rehabilitation of patients with oral cancer. Int JOral Maxillofac Implants 1996;11:775–781.
10. Jisander S, Grenthe B, Alberius P. Dental implant survival in the irradiatedjaw: a preliminary report. Int J Oral Maxillofac Implants 1997;12:643–648.
11. Mericske–Stern R, Perren R, Raveh J. Life table analysis and clinical eval-uation of oral implants supporting prostheses after resection of malignanttumors. Int J Oral Maxillofac Implants 1999;14:673–680.
12. van Steenberghe D, Jacobs R, Desnyder M, Maffei G, Quirynen M. The rel-ative impact of local and endogenous patient-related factors on implantfailure up to the abutment stage. Clin Oral Implants Res 2002;13:617–622.
13. Visch LL, van Waas MA, Schmitz PI, Levendag PC. A clinical evaluationof implants in irradiated oral cancer patients. J Dent Res 2002;81:856–859.
14. Schoen PJ, Raghoebar GM, Bouma J, et al. Rehabilitation of oral func-tion in head and neck cancer patients after radiotherapy with implant-retained dentures: effects of hyperbaric oxygen therapy. Oral Oncol2007;43:379–388.
15. Schoen PJ, Raghoebar GM, Bouma J, et al. Prosthodontic rehabilitation oforal function in head-neck cancer patients with dental implants placedsimultaneously during ablative tumour surgery: an assessment of treatmentoutcomes and quality of life. Int J Oral Maxillofac Surg 2008;37:8–16.
16. Korfage A, Schoen PJ, Raghoebar GM, Roodenburg JL, Vissink A,Reintsema H. Benefits of dental implants installed during ablative tumoursurgery in oral cancer patients: a prospective 5-year clinical trial. Clin OralImplants Res 2010;21:971–979.
17. Heberer S, Kilic S, Hossamo J, Raguse JD, Nelson K. Rehabilitation ofirradiated patients with modified and conventional sandblasted acid-etchedimplants: preliminary results of a split-mouth study. Clin Oral ImplantsRes 2011;22:546–551.
18. Sammartino G, Marenzi G, Cioffi I, Tet�e S, Mortellaro C. Implant therapyin irradiated patients. J Craniofac Surg 2011;22:443–445.
19. Albrektsson T, Dahl E, Enbom L, et al. Osseointegrated oral implants. ASwedish multicenter study of 8139 consecutively inserted Nobelpharmaimplants. J Periodontol 1988;59:287–296.
20. Sclaroff A, Haughey B, Gay WD, Paniello R. Immediate mandibular recon-struction and placement of dental implants. At the time of ablative surgery.Oral Surg Oral Med Oral Pathol 1994;78:711–717.
21. Franz�en L, Rosenquist JB, Rosenquist KI, Gustafsson I. Oral implant reha-bilitation of patients with oral malignancies treated with radiotherapy andsurgery without adjunctive hyperbaric oxygen. Int J Oral MaxillofacImplants 1995;10:183–187.
22. Aldegheri A, Beloni D, Blanc JL, Kaplanski P, Legre R, Zanaret M. Dentalrehabilitation using osseointegrated implants: treatment of oro-maxillo-facial cancer. A preliminary study of 7 cases [in French]. Rev StomatolChir Maxillofac 1996;97:108–116.
23. Eckert SE, Desjardins RP, Keller EE, Tolman DE. Endosseous implants inan irradiated tissue bed. J Prosthet Dent 1996;76:45–49.
24. Ali A, Patton DW, el-Sharkawi AM, Davies J. Implant rehabilitation ofirradiated jaws: a preliminary report. Int J Oral Maxillofac Implants 1997;12:523–526.
25. Chan MF, Hayter JP, Cawood JI, Howell RA. Oral rehabilitation withimplant-retained prostheses following ablative surgery and reconstructionwith free flaps. Int J Oral Maxillofac Implants 1997;12:820–827.
FIGURE 15. Funnel plot for the studies reporting the outcomeevent “implant failure.” [Color figure can be viewed in the onlineissue, which is available at wileyonlinelibrary.com.]
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 479

26. Esser E, Wagner W. Dental implants following radical oral cancer surgeryand adjuvant radiotherapy. Int J Oral Maxillofac Implants 1997;12:552–557.
27. Keller EE, Tolman DE, Zuck SL, Eckert SE. Mandibular endosseousimplants and autogenous bone grafting in irradiated tissue: a 10-year retro-spective study. Int J Oral Maxillofac Implants 1997;12:800–813.
28. Marker P, Siemssen SJ, Bastholt L. Osseointegrated implants for prostheticrehabilitation after treatment of cancer of the oral cavity. Acta Oncol 1997;36:37–40.
29. McGhee MA, Stern SJ, Callan D, Shewmake K, Smith T. Osseointegratedimplants in the head and neck cancer patient. Head Neck 1997;19:659–665.
30. Niimi A, Fujimoto T, Nosaka Y, Ueda M. A Japanese multicenter study ofosseointegrated implants placed in irradiated tissues: a preliminary report.Int J Oral Maxillofac Implants 1997;12:259–264.
31. Roumanas ED, Markowitz BL, Lorant JA, Calcaterra TC, Jones NF,Beumer J III. Reconstructed mandibular defects: fibula free flaps andosseointegrated implants. Plast Reconstr Surg 1997;99:356–365.
32. Andersson G, Andreasson L, Bjelkengren G. Oral implant rehabilitation inirradiated patients without adjunctive hyperbaric oxygen. Int J Oral Maxil-lofac Implants 1998;13:647–654.
33. Brogniez V, Lejuste P, Pecheur A, Reychler H. Dental prosthetic recon-struction of osseointegrated implants placed in irradiated bone. Int J OralMaxillofac Implants 1998;13:506–512.
34. Ihara K, Goto M, Miyahara A, Toyota J, Katsuki T. Multicenter experiencewith maxillary prostheses supported by Branemark implants: a clinicalreport. Int J Oral Maxillofac Implants 1998;13:531–538.
35. Esser E, Neukirchen S, Wagner W. Comparative studies of Branemarkimplants in the irradiated and not irradiated mandible [in German]. MundKiefer Gesichtschir 1999;3 Suppl 1:S125–S129.
36. Foster RD, Anthony JP, Sharma A, Pogrel MA. Vascularized bone flapsversus nonvascularized bone grafts for mandibular reconstruction: an out-come analysis of primary bony union and endosseous implant success.Head Neck 1999;21:66–71.
37. Granstr€om G, Tjellstr€om A, Branemark PI. Osseointegrated implants inirradiated bone: a case-controlled study using adjunctive hyperbaric oxygentherapy. J Oral Maxillofac Surg 1999;57:493–499.
38. Keller EE, Tolman DE, Eckert SE. Maxillary antral-nasal inlay autogenousbone graft reconstruction of compromised maxilla: a 12-year retrospectivestudy. Int J Oral Maxillofac Implants 1999;14:707–721.
39. Weischer T, Mohr C. Ten-year experience in oral implant rehabilitation ofcancer patients: treatment concept and proposed criteria for success. Int JOral Maxillofac Implants 1999;14:521–528.
40. Werkmeister R, Szulczewski D, Walteros–Benz P, Joos U. Rehabilitationwith dental implants of oral cancer patients. J Craniomaxillofac Surg 1999;27:38–41.
41. Goto M, Jin–Nouchi S, Ihara K, Katsuki T. Longitudinal follow-up ofosseointegrated implants in patients with resected jaws. Int J Oral Maxillo-fac Implants 2002;17:225–230.
42. Cao Y, Weischer T. Comparison of maxillary implant-supported prosthesisin irradiated and non-irradiated patients. J Huazhong Univ Sci TechnologMed Sci 2003;23:209–212.
43. Granstr€om G. Radiotherapy, osseointegration and hyperbaric oxygen ther-apy. Periodontol 2000 2003;33:145–162.
44. Granstr€om G. Osseointegration in irradiated cancer patients: an analysiswith respect to implant failures. J Oral Maxillofac Surg 2005;63:579–585.
45. Shaw RJ, Sutton AF, Cawood JI, et al. Oral rehabilitation after treatmentfor head and neck malignancy. Head Neck 2005;27:459–470.
46. Teoh KH, Huryn JM, Patel S, et al. Implant prosthodontic rehabilitation offibula free-flap reconstructed mandibles: a Memorial Sloan–Kettering Can-cer Center review of prognostic factors and implant outcomes. Int J OralMaxillofac Implants 2005;20:738–746.
47. Bodard AG, Gourmet R, Lucas R, Bonnet E, Breton P. Dental implants inirradiated areas: a series of 33 patients [in French]. Rev Stomatol Chir Max-illofac 2006;107:137–142; discussion 143–144.
48. Landes CA, Kov�acs AF. Comparison of early telescope loading of non-submerged ITI implants in irradiated and non-irradiated oral cancerpatients. Clin Oral Implants Res 2006;17:367–374.
49. Schepers RH, Slagter AP, Kaanders JH, van den Hoogen FJ, Merkx MA.Effect of postoperative radiotherapy on the functional result of implantsplaced during ablative surgery for oral cancer. Int J Oral Maxillofac Surg2006;35:803–808.
50. Yerit KC, Posch M, Seemann M, et al. Implant survival in mandibles ofirradiated oral cancer patients. Clin Oral Implants Res 2006;17:337–344.
51. Nelson K, Heberer S, Glatzer C. Survival analysis and clinical evaluationof implant-retained prostheses in oral cancer resection patients over a meanfollow-up period of 10 years. J Prosthet Dent 2007;98:405–410.
52. Alsaadi G, Quirynen M, Kom�arek A, van Steenberghe D. Impact of localand systemic factors on the incidence of late oral implant loss. Clin OralImplants Res 2008;19:670–676.
53. Cuesta–Gil M, Ochandiano Caicoya S, Riba–Garc�ıa F, Duarte Ruiz B,Navarro Cu�ellar C, Navarro Vila C. Oral rehabilitation with osseointe-grated implants in oncologic patients. J Oral Maxillofac Surg 2009;67:2485–2496.
54. Klein MO, Gr€otz KA, Walter C, Wegener J, Wagner W, Al-Nawas B.Functional rehabilitation of mandibular continuity defects using autologous
bone and dental implants – prognostic value of bone origin, radiation ther-apy and implant dimensions. Eur Surg Res 2009;43:269–275.
55. Barrowman RA, Wilson PR, Wiesenfeld D. Oral rehabilitation with dentalimplants after cancer treatment. Aust Dent J 2011;56:160–165.
56. Buddula A, Assad DA, Salinas TJ, Garces YI. Survival of dental implantsin native and grafted bone in irradiated head and neck cancer patients: a ret-rospective analysis. Indian J Dent Res 2011;22:644–648.
57. Fenlon MR, Lyons A, Farrell S, Bavisha K, Banerjee A, Palmer RM. Fac-tors affecting survival and usefulness of implants placed in vascularizedfree composite grafts used in post-head and neck cancer reconstruction.Clin Implant Dent Relat Res 2012;14:266–272.
58. Jacobsen C, Kruse A, L€ubbers HT, et al. Is mandibular reconstruction usingvascularized fibula flaps and dental implants a reasonable treatment? ClinImplant Dent Relat Res 2014;16:419–428.
59. Linsen SS, Martini M, Stark H. Long-term results of endosteal implantsfollowing radical oral cancer surgery with and without adjuvant radiationtherapy. Clin Implant Dent Relat Res 2012;14:250–258.
60. Mancha de la Plata M, G�ıas LN, D�ıez PM, et al. Osseointegrated implantrehabilitation of irradiated oral cancer patients. J Oral Maxillofac Surg2012;70:1052–1063.
61. Katsoulis J, Fierz J, Iizuka T, Mericske–Stern R. Prosthetic rehabilitation,implant survival and quality of life 2 to 5 years after resection of oraltumors. Clin Implant Dent Relat Res 2013;15:64–72.
62. Jacobsson M. On bone behaviour after irradiation. PhD thesis. G€oteborg,Sweden: University of G€oteborg; 1985.
63. Marx RE, Johnson RP. Studies in the radiobiology of osteoradionecrosisand their clinical significance. Oral Surg Oral Med Oral Pathol 1987;64:379–390.
64. Scully C, Epstein JB. Oral health care for the cancer patient. Eur J CancerB Oral Oncol 1996;32B:281–292.
65. Granstr€om G, Tjellstr€om A, Albrektsson T. Postimplantation irradiation forhead and neck cancer treatment. Int J Oral Maxillofac Implants 1993;8:495–501.
66. Larsen PE, Stronczek MJ, Beck FM, Rohrer M. Osteointegration ofimplants in radiated bone with and without adjunctive hyperbaric oxygen.J Oral Maxillofac Surg 1993;51:280–287.
67. Marx RE, Ames JR. The use of hyperbaric oxygen therapy in bony recon-struction of the irradiated and tissue-deficient patient. J Oral MaxillofacSurg 1982;40:412–420.
68. Johnsson K, Hansson A, Granstr€om G, Jacobsson M, Turesson I. Theeffects of hyperbaric oxygenation on bone-titanium implant interfacestrength with and without preceding irradiation. Int J Oral MaxillofacImplants 1993;8:415–419.
69. Granstr€om G, Jacobsson M, Tjellstr€om A. Titanium implants in irradiatedtissue: benefits from hyperbaric oxygen. Int J Oral Maxillofac Implants1992;7:15–25.
70. Schoen PJ, Reintsema H, Raghoebar GM, Vissink A, Roodenburg JL. Theuse of implant retained mandibular prostheses in the oral rehabilitation ofhead and neck cancer patients. A review and rationale for treatment plan-ning. Oral Oncol 2004;40:862–871.
71. Haas I, Hauser U, Ganzer U. The dilemma of follow-up in head and neckcancer patients. Eur Arch Otorhinolaryngol 2001;258:177–183.
72. Kwakman JM, Freihofer HP, van Waas MA. Osseointegrated oral implantsin head and neck cancer patients. Laryngoscope 1997;107:519–522.
73. King MA, Casarett GW, Weber DA. A study of irradiated bone: I. histopa-thologic and physiologic changes. J Nucl Med 1979;20:1142–1149.
74. W€achter RS, Stoll P. Possibilities and limits of endosseous implants in theoral rehabilitation of cancer patients after radiation [in German]. Zeitschriftf€ur Zahn€arztliche Implantologie 1994;10:171–176.
75. Cooper JS, Fu K, Marks J, Silverman S. Late effects of radiation therapy inthe head and neck region. Int J Radiat Oncol Biol Phys 1995;31:1141–1164.
76. Nguyen TD, Panis X, Froissart D, Legros M, Coninx P, Loirette M. Analy-sis of late complications after rapid hyperfractionated radiotherapy inadvanced head and neck cancers. Int J Radiat Oncol Biol Phys 1988;14:23–25.
77. Jacobsson M, Kalebo P, Albrektsson T, Turesson I. Provoked repetitivehealing of mature bone tissue following irradiation. A quantitative investi-gation. Acta Radiol Oncol 1986;25:57–62.
78. Jacobsson M, Tjellstr€om A, Thomsen P, Albrektsson T, Turesson I. Inte-gration of titanium implants in irradiated bone. Histologic and clinicalstudy. Ann Otol Rhinol Laryngol 1988;97:337–340.
79. Nishimura RD, Roumanas E, Beumer J, 3rd, Moy PK, Shimizu KT. Resto-ration of irradiated patients using osseointegrated implants: current per-spectives. J Prosthet Dent 1998;79:641–647.
80. Shirota T, Ohno K, Michi K, Tachikawa T. An experimental study of heal-ing around hydroxylapatite implants installed with autogenous iliac bonegrafts for jaw reconstruction. J Oral Maxillofac Surg 1991;49:1310–1315.
81. Pogrel MA, Podlesh S, Anthony JP, Alexander J. A comparison of vascu-larized and nonvascularized bone grafts for reconstruction of mandibularcontinuity defects. J Oral Maxillofac Surg 1997;55:1200–1206.
82. Umstadt HE, V€ollinger J, M€uller HH, Austermann KH. Implants in avascu-lar iliac crest bone transplants. Prospective study of 176 implants [in Ger-man]. Mund Kiefer Gesichtschir 1999;3 Suppl 1:S93–S98.
CHRCANOVIC ET AL.
480 HEAD & NECK—DOI 10.1002/HED MARCH 2016

83. Berggren A, Weiland AJ, Dorfman H. The effect of prolonged ischemiatime on osteocyte and osteoblast survival in composite bone grafts revascu-larized by microvascular anastomoses. Plast Reconstr Surg 1982;69:290–298.
84. Albrektsson T. Repair of bone grafts. A vital microscopic and histologicalinvestigation in the rabbit. Scand J Plast Reconstr Surg 1980;14:1–12.
85. Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term effi-cacy of currently used dental implants: a review and proposed criteria ofsuccess. Int J Oral Maxillofac Implants 1986;1:11–25.
86. Shah JP, Patel SG, American Cancer Society. Cancer of the head and neck.Hamilton: BC Decker; 2001.
87. Wennerberg A, Albrektsson T. On implant surfaces: a review of currentknowledge and opinions. Int J Oral Maxillofac Implants 2010;25:63–74.
88. Chrcanovic BR, Pedrosa AR, Martins MD. Chemical and topographic anal-ysis of treated surfaces of five different commercial dental titaniumimplants. Mater Res 2012;15:372–382.
89. Chrcanovic BR, Leao NLC, Martins MD. Influence of different acid etch-ings on the superficial characteristics of Ti sandblasted with Al2O3. MaterRes 2013;16:1006–1014.
90. Chrcanovic BR, Martins MD. Study of the influence of acid etching treat-ments on the superficial characteristics of Ti. Mater Res 2014;17:373–380.
91. Marx RE. Osteoradionecrosis: a new concept of its pathophysiology.J Oral Maxillofac Surg 1983;41:283–288.
92. Friedlaender GE, Tross RB, Doganis AC, Kirkwood JM, Baron R. Effectsof chemotherapeutic agents on bone. I. Short-term methotrexate and doxor-ubicin (adriamycin) treatment in a rat model. J Bone Joint Surg Am 1984;66:602–607.
93. Young DR, Virolainen P, Inoue N, Frassica FJ, Chao EY. The short-termeffects of cisplatin chemotherapy on bone turnover. J Bone Miner Res1997;12:1874–1882.
94. Kov�acs AF. Influence of chemotherapy on endosteal implant survival andsuccess in oral cancer patients. Int J Oral Maxillofac Surg 2001;30:144–147.
95. Chrcanovic BR, Abreu MH, Freire–Maia B, Souza LN. Facial fractures inchildren and adolescents: a retrospective study of 3 years in a hospital inBelo Horizonte, Brazil. Dent Traumatol 2010;26:262–270.
96. Chrcanovic BR, Souza LN, Freire–Maia B, Abreu MH. Facial fractures inthe elderly: a retrospective study in a hospital in Belo Horizonte, Brazil.J Trauma 2010;69:E73–E78.
97. Chrcanovic BR, Abreu MH, Freire–Maia B, Souza LN. 1,454 mandibularfractures: a 3-year study in a hospital in Belo Horizonte, Brazil.J Craniomaxillofac Surg 2012;40:116–123.
DENTAL IMPLANTS AND IRRADIATION
HEAD & NECK—DOI 10.1002/HED MARCH 2016 481