dental ceramics.. old and new
TRANSCRIPT



There was always an intimate relation between metal and ceramic
material, Will this relationship will continue in the future?
Ceramics is a term refer to any product made from a nonmetallic inorganic material usually processed by firing at a high temperature.
Porcelain is s more restrictive term and refers to a specific compositional range of ceramic material originally made by mixing Kaolin ( hydrated aluminosilicate), quartz ( silica ), and feldspars (potassium and sodium aluminosilicates), and firing at high temperature.
All-ceramic inlays, onlays, veneers, and crowns can provide some
of the most esthetically A pleasing restorations currently available.
They can be made to match natural tooth structure accurately in
terms of color, surface texture, and translucency. Well-made all
ceramic restorations can be virtually indistinguishable from
unrestored natural teeth.
More recently, improved materials and techniques have been
introduced in an attempt to overcome disadvantages inherent in
that traditional method. These improvements, particularly the use
of higher strength ceramics and adhesives for bonding the ceramic
restoration to tooth structure.
Ceramic objects have been fabricated for thousands of years through
the attempts of Egyptian and Chinese.
More than two hundred years later was the first attempt to use
ceramics for making denture teeth was by Alexis Duchateau in 1774.
1887 C. H. Land made the first ceramic crowns and inlays with a
platinum foil matrix technique and was granted a patent. At that time
feldspathic porcelain used in the fabrication.
The popularity of ceramic restorations declined with the introduction of
acrylic resin in the 1940s and continued to be low until the
disadvantages of resin veneering materials (increased wear, high
permeability leading to discoloration and leakage) were realized.
In 1962 Weinstein and Weinstein patented a leucite-containing
porcelain frit for use in metalceramic restorations.
In 1965 McLean and Hughes advocated using aluminous porcelain,
which is composed of aluminum oxide (alumina) crystals dispersed in
a glassy matrix which is called ‘ High Strength Ceramics ‘

The chief disadvantage of the early restorations was their low
strength, which limited their use to low stress situations, such as those
encountered by anterior teeth. Even so, fracture was a fairly common
occurrence, which prompted the development of higher strength
materials.
These developments have included modifications to the microstructure
of the ceramic material during the manufacturing process, and the
development of different techniques to fabricate the product.

In spite of their excellent esthetic qualities and outstanding
biocompatibility, dental ceramics, like all ceramic materials, are brittle.
They are susceptible to fracture at the time of placement and during
function. Brittle materials such as ceramics contain at least two types
of flaws: fabrication defects and surface cracks, from which fracture
can initiate.

Fabrication Defects
Fabrication defects are created during processing and consist of :
o voids or inclusions generated during sintering. Condensation of a
ceramic slurry by hand before sintering may introduce porosity.
Sintering under vacuum reduces the porosity in dental ceramics
from 5.6 to 0.56 volume percent.
o Also, microcracks develop within the ceramic upon cooling in
leucite-containing ceramics and are caused by thermal contraction
mismatch between the crystals and the glassy matrix.
Surface Cracks
Surface cracks are induced by machining or grinding. The average
natural flaw size varies from 20 to 50 µm. Usually, fracture of the
ceramic material takes place from the most severe flaw.


The principle of toughening by crystalline reinforcement is to increase
the resistance of the ceramic to crack propagation by introducing a
dispersed crystalline phase with high toughness.
Crystals can acts as crack deflector when their coefficient of thermal
expansion is greater than that of the surrounding glassy matrix,
placing them under a tangential compressive stresses after the
ceramic has been cooled to room temperature.
Transformation toughening is obtained, for example, in ceramics
containing partially stabilized tetragonal zirconia.
Zirconia (ZrO2) exists under several crystallographic forms. Zirconia
is monoclinic at room temperature and tetragonal between about
1170° C and 2370° C. The transformation between tetragonal and
monoclinic zirconia is accompanied by an increase in volume. The
tetragonal form can be retained at room temperature by addition of
various oxides such as yttrium oxide ( Y2O3) or cerium oxide (CeO2).

Stress can trigger the transformation from tetragonal (3Y-TZP) to
monoclinic zirconia, thereby leading to strengthening as a result of an
increase in grain volume in the vicinity of the crack tip.

chemical strengthening relies on the replacement of small ions with larger ions by diffusion from a molten salt bath in which the ceramic or glass is immersed.
the exchange leads to the creation of a compressive layer at the surface of the ceramic.‘ Finally, any applied load must first overcome this built-in compression layer before the surface can be placed into tension; this results in an increase in fracture resistance.

• Tempering is obtained by using rapid but controlled cooling.
• This also create a compressive stress layer at the surface of a glass
or a ceramics.
• Although widely used in the glass industry, neither of these two
techniques is used for dental ceramics.

The principle is the formation of a low-
expansion surface layer formed at a high
temperature. Upon cooling, the low-
expansion glaze places the surface of the
ceramic in compression and reduces the
depth and width of surface flaws
standard technique, also called self-
glazing, does not significantly improve the
flexural strength of feldspathic dental
porcelains. However, a low-expansion
glass called glaze can also be applied at
the surface of the ceramic.


Alumina-Based Ceramic
Alumina-Based Ceramic was first introduced
to dentistry by McLean and Hughes in 1965.
Alumina-Based Ceramic is composed of
aluminum oxide (alumina) crystals dispersed
in a glassy matrix.
The technique involved the use of an opaque inner core containing 50% by weight alumina
for high strength. This core was veneered by
a combination of esthetic body and enamel
porcelains with 15% and 5% crystalline
alumina, respectively
The flexure strength approximately twice that
of feldspathic porcelains (139 to 145 MPa).
Leucite-Reinforced Ceramic
Leucite-reinforced ceramics containing up to 45% by volume tetragonal leucite the greater leucite content leads to higher flexural strength (104 MPa) and compressive strength.
Because the crystals contract more than the surrounding glassy matrix, this results in the development of tangential compressive stresses in the glass around the leucite crystals. These stresses can act as crack deflectors and contribute to increased resistance of the ceramic to crack propagation

Heat-pressed ceramics have been popular in restorative dentistry since
the early 1990s. The restorations are waxed, invested, and pressed in a
manner somewhat similar to that for gold casting.

Leucite-Based Ceramic
• First-generation heat-pressed ceramics contain leucite (KAlSi2O6 or K2O • Al2O3 •
4SiO2) as a reinforcing phase, in amounts varying from 35% to 55% by volume.
• Heat-pressing temperatures )1150° and 1180° C).
• The crystal size varies from 1 to 5 µm.
• The amount of porosity is 9 vol%.
• The flexural strength of these ceramics (120 MPa).
Two techniques are available
A staining technique (surface stain only) and a layering technique involving the application of veneering ceramic.
Disadvantages
• The initial high cost of the equipment.
• The relatively low strength.

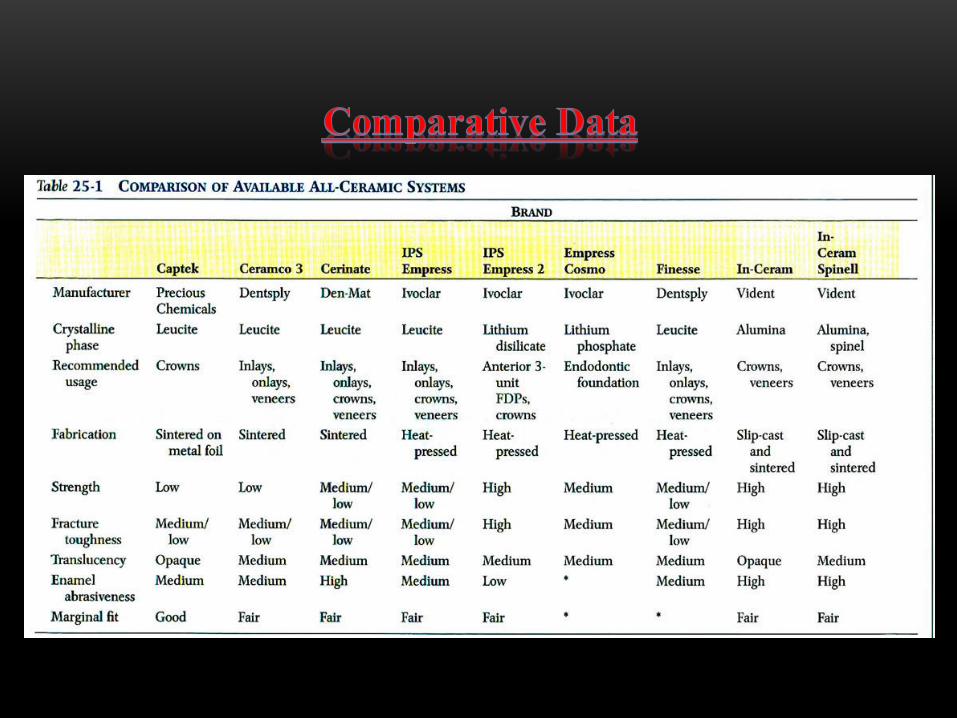
materials for heat-pressing are
IPS Empress, Optimal Pressable Ceramic, and two lower fusing
materials, Cerpress and Finesses

Lithium Disilicate–Based Materials
• The second generation of heat-pressed ceramics contain lithium disilicate (Li2Si2O5) as a major crystalline Phase.
• Heat-pressing temperatures (890° to 920° C).
• The final microstructure consists of about 65% by volume of highly interlocking prismatic lithium disilicate crystals.
• The amount of porosity is 1 vol%.
the main advantage is their enhanced flexural strength (300 MPa) and fracture toughness (2.9 MPa • m0.5).
Applications --------- < Anterior fixed partial prostheses.
• IPS Empress 2 is an example for lithium disilicate, IPA Empress Cosmo is an example for lithium phosphate.


• Slip-casting was introduced in dentistry in the1990s
• The first step of the process involves the condensation of a porcelain
aqueous slurry slip on a refractory die.
• The porosity of the refractory die helps condensation by absorbing the
water from the slip by capillary action
• The restoration is incrementally built up, shaped, and finally sintered
at high temperature on the refractory die.
Alumina and Spinel-Based Slip-Cast Ceramics
It consists of 68 vol% alumina, 27 vol% glass, and 5 vol% Porosity
The flexural strength is around 600 MPa
Spinel-based slip-cast ceramics are more translucent, because the spinel phase
allows better sintering, but the flexural strength is slightly lower (378 MPa) than
that of the alumina-based system.
In Ceram, In Ceram Spinell, In Ceram Cosmo is an example
Application : short-span anterior fixed partial prostheses

Zirconia-Toughened Alumina Slip-Cast Ceramics
• It consists of 34 vol% alumina, 33 vol% zirconia stabilized with 12 mol% ceria
(12Ce-TZP), 23 vol% glassy phase, and 8 vol% residual porosity
• The combination of alumina and zirconia allows two types of strengthening Mechanisms
• The flexural strength : 630 Mpa
Advantage --------- < high strength
Disadvantages --------- <high opacity (with the exception of the spinel-based
materials)

• The evolution of computer-aided
design/computer-aided
manufacturer (or computer-
assisted machining) (CAD/CAM)
systems for the production of
machined inlays, onlays, veneers,
and crowns led to the development
of a new generation of ceramics
that are machinable.

Hard Machining
• Machinable ceramics can be milled to form inlays, onlays, veneers, and
crowns using CAD/ CAM technology to produce restorations in one office
visit.
• After the tooth is prepared, the preparation is optically scanned and the
image is computerized. The restoration is designed with the aid of a
computer, as shown in. The restoration is then machined from ceramic
blocks by a computer-controlled milling machine. The milling process takes
only a few minutes.
• Feldspar, leucite, and lithium disilicate–based ceramic blocks are available in
the market


Soft Machining Followed by Sintering
The CAD/CAM and copy-milling systems can also be used to machine
presintered alumina, spinel, or zirconia-toughened-alumina blocks.
Advantages : The blocks are easy to mill, which leads to substantial
savings in time and tool wear
grain size of 0.2 to 0.7 μm
sintering temperature 1350° to 1550° C
durations from 2 to 6 hours
flexural strength (900-1500 MPa)
fracture toughness (greater than 5 MPa • m0.5)


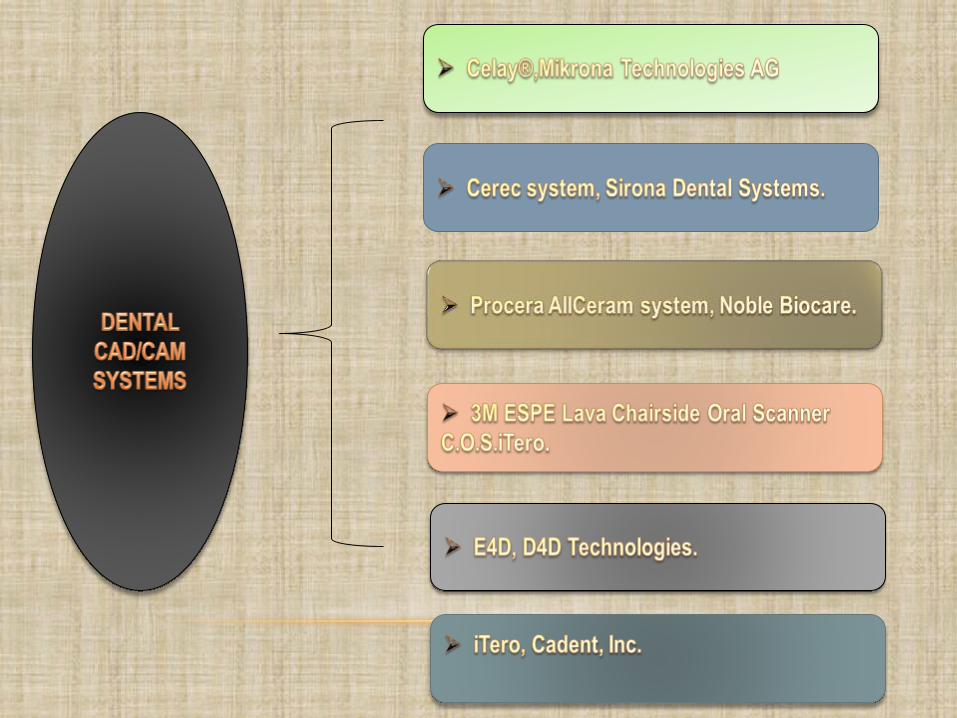

Dental CAD/CAM systems consist of three components:
1. A scanner or digitizing instrument that transforms physical
geometry into digital data.
2. Software that processes the scanned data an creates images of
the digitized object. Some systems then enable restorations to be
designed for the digitized object.
3. Fabrication technology that transforms the digital data of the
restoration into a physical product. Different systems place the
fabrication technology in the dental office, dental laboratory, or
centralized facility.
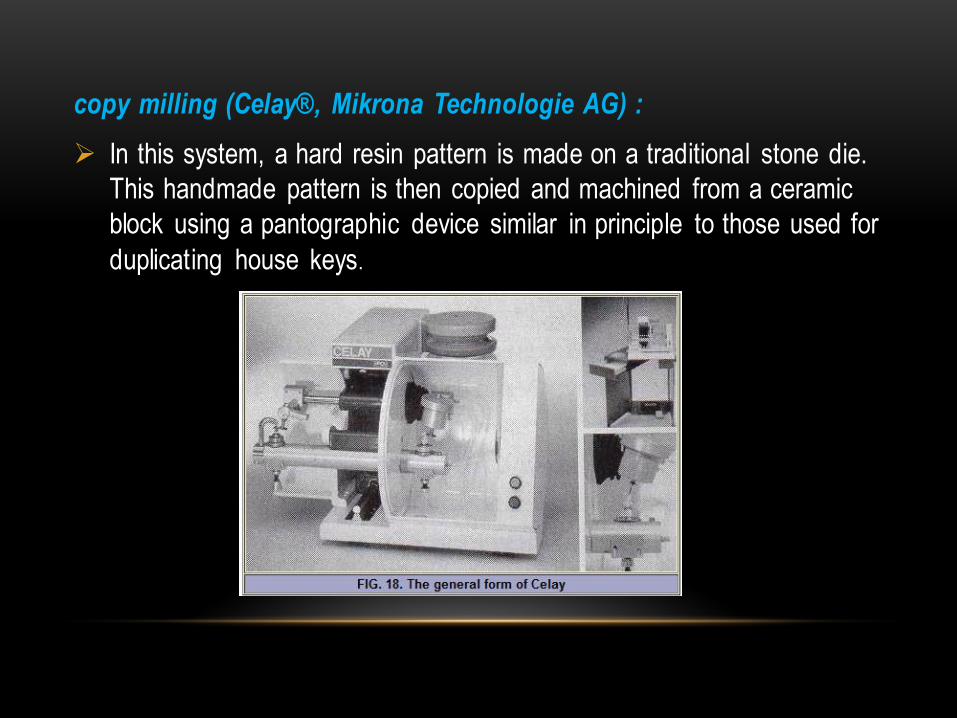
copy milling (Celay®, Mikrona Technologie AG) :
In this system, a hard resin pattern is made on a traditional stone die.
This handmade pattern is then copied and machined from a ceramic
block using a pantographic device similar in principle to those used for
duplicating house keys.

Cerec system
• The Cerec system has been marketed
since the 1980s, with the improved
Cerec 2 system introduced in the mid-
1990s and the Cerec 3 in 2000.
• Several materials can be used with this
system: VITA Mark II, ProCad s and In-
Ceram Alumina and Spinell.
• VITA Mark II contains feldspar, ProCad is a leucite-containing ceramic
• Weaknesses of the earlier Cerec
system include the poor marginal fit of the restorations and the lack of
sophistication in the machining of the
occlusal surface, but these weakness
have overcomed in Cerec 3.
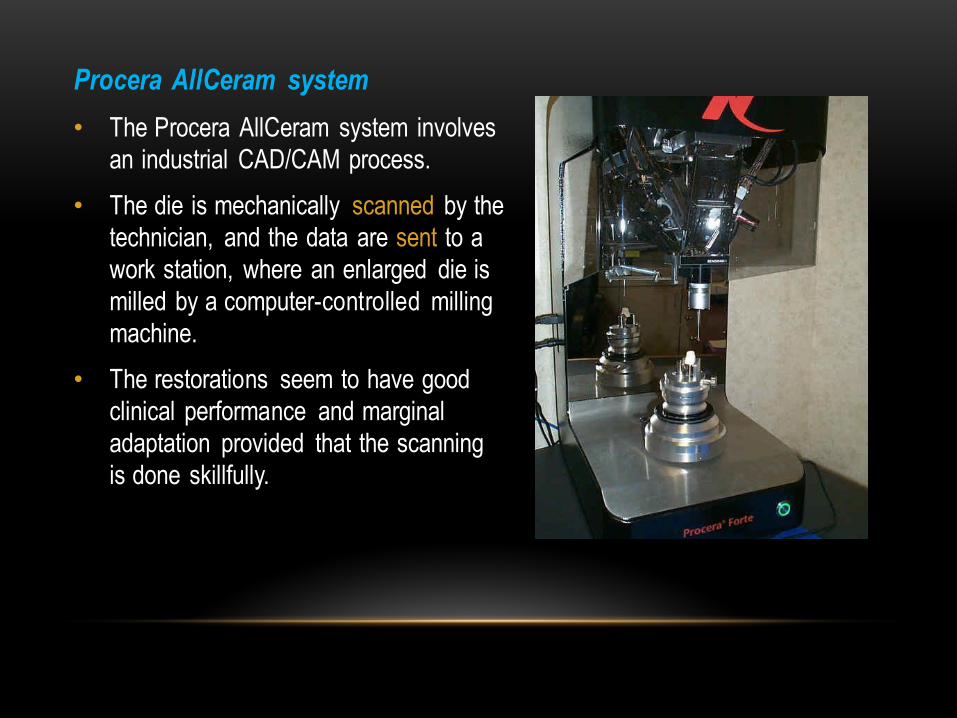
Procera AllCeram system
• The Procera AllCeram system involves
an industrial CAD/CAM process.
• The die is mechanically scanned by the
technician, and the data are sent to a
work station, where an enlarged die is
milled by a computer-controlled milling
machine.
• The restorations seem to have good
clinical performance and marginal
adaptation provided that the scanning
is done skillfully.

In a 10-year study of 308 ceramic restorations placed in 74 patients between 1991 and
1994, the restoration survival rate was 94.7% after 5 years and 85.7% after 10 years,
which is comparable to the survival rates of cast gold restorations.
A systematic review of studies that reported on single-tooth restorations fabricated with
CAD/CAM technology from 1985 to 2007 revealed a failure rate of 1.75% per year,
calculated per 100 restoration years from a total of 1957 restorations and a mean
exposure time of 7.9 years. The review estimated a total 5-year survival rate of 91.6%.
the unique mechanical properties of 3Y-TZP, making possible the realization of both single
and multiunit anterior and posterior restorations.

PORCELAIN LABIAL VENEER
Porcelain labial veneers can be fabricated by means of a refractory die
technique, as well as on a platinum matrix and with heat-pressed-ceramics.
'Porcelain labial veneers can also be made with the machinable systems.
Lumineers®, is one brand of porcelain veneer. These veneers are made out
of porcelain named Cerinate®. And because Cerinate® is exceptionally
strong, Lumineers® veneers can be made to extremely thin tolerances (on
the same order as the thickness of a contact lens).

Den-Mat Corporation (the manufacturer) promotes placement using a
protocol that involves no drilling, no shoots dental aesthatic.
The thickness of a Lumineer® veneer can be as little as 0.2 to 0.3
millimeters
The most ideal candidates for having Lumineers® veneers placed using
a "no drilling" technique are typically those people whose teeth are ...
o already relatively straight in alignment.
o and only require a slight color or other cosmetic change.
o Additional beneficial conditions include teeth that are relatively
small, lingually inclined or have spaces between them.

INLAYS AND ONLAYS
Refractory Dies Ceramic restorations are normally made through the
use of the heat-pressed systems, but some technicians prefer a
refractory Marginal adaptation can be excellent, depending more on
the technician's skill than on the ceramic material used.

ALL-CERAMIC PARTIAL FIXED DENTAL PROSTHESES
All-ceramic FDPs have a checkered history. Their construction was
attempted with aluminous porcelain by connecting alumina cores with
pure alumina rods. These restorations were usually unsuccessful:
either they fractured or the restorations encroached excessively into
the embrasures, resulting in hygiene deficiencies.

ALL-CERAMIC FOUNDATION RESTORATIONS
All-ceramic materials have been used as foundation restorations for
endodontically treated teeth to overcome esthetic problems
associated with metal post and core systems. The post is made of
zirconia, chosen for its excellent strength, and depending on the
system, the core material can be composite resin or a pressable
ceramic.
