denervazione-deafferentazione · drg, their connectivity with the spinal cord, and the ability of...
TRANSCRIPT

Denervazione-deafferentazione

The terms “denervation” and “deafferentation” are
frequently confused and misused; they do not mean the
same thing.
2
Devor, M. (2006). Response of nerves to injury in relation to neuropathic pain. Chapter 58. In S. L. McMahon & M. Koltzenburg (Eds.), Wall and Melzack’s textbook of pain (5th ed., pp. 905–927). London: Churchill Livingstone.

Denervation in the present context refers to severing sensory axons that
innervate the limb. Sensory endings rapidly degenerate in the process of
anterograde (Wallerian) degeneration. However, sensory cell bodies in the
DRG, their connectivity with the spinal cord, and the ability of (ectopically
generated) afferent impulses to reach the CNS are largely preserved.
3

Deafferentation refers to blocking the arrival of afferent impulses into the
CNS by severing dorsal roots (Dorsal Rhizotomy). The sensory neurons in the
dorsal root ganglion (DRG) mostly survive, as do sensory endings in the skin.
The limb is not denervated. It is very likely that pain due to denervation and
deafferentation results from different mechanisms (Devor 2006).

5
Pain and autotomy after nerve injury is probably due to
abnormal spontaneous afferent discharge generated
ectopically at the nerve injury site, and in axotomized DRG
neurons. There might also be a contribution by residual intact
neurons that continue to innervate adjacent skin. The ectopic
firing plays two roles. First, it constitutes a primary
nociceptive afferent signal. Second, it probably triggers
central sensitization in the spinal cord dorsal horn, and
perhaps also in the brain. The sensitized CNS amplifies and
augments pain sensation due to the spontaneous afferent
discharge. It also renders light tactile input from residual
neighboring afferents painful, yielding tactile allodynia in the
skin bordering on the denervated zone (Defrin et al. 1996;
Devor 2006).

6
Pain and autotomy after deafferentation must be due to
another mechanism as dorsal rhizotomy does not trigger
massive ectopia in axotomized afferents, and even if it did, the
impulses would have no access to the CNS. Pain following
rhizotomy is, therefore, presumed to be due to impulses that
originate within the deafferented CNS itself. Deafferentation
triggers many structural and neurochemical changes in the CNS,
and abnormal bursting discharges have been recorded in
deafferented spinal dorsal horn in animals and in humans. The
possibility that deafferentation pain is indeed due to this activity
is supported by the observation that surgical destruction of the
abnormal dorsal horn tissue by DREZotomy often relieves this
type of pain (Rossitch et al. 1993; Guenot et al. 2002). ???????????????????

Denervazione
7
Dolore neuropatico periferico Spontaneo ed evocato
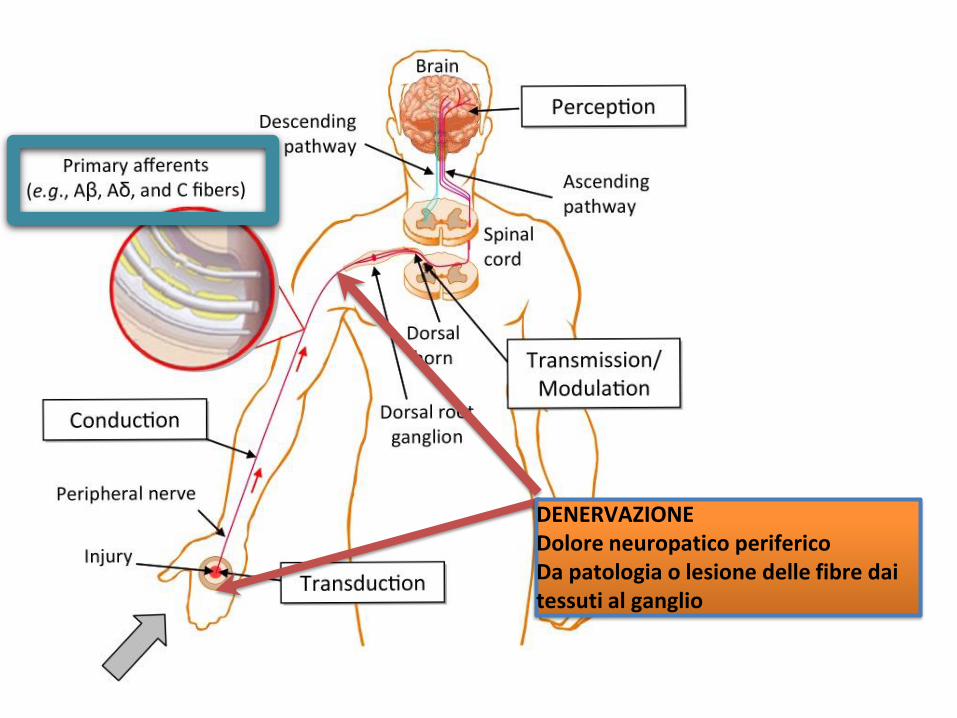
DENERVAZIONE Dolore neuropatico periferico Da patologia o lesione delle fibre dai tessuti al ganglio

La deafferentazione termo-nocicettiva e il dolore neuropatico
centrale “da deafferentazione”
9
Dolore spontaneo
Buonocore
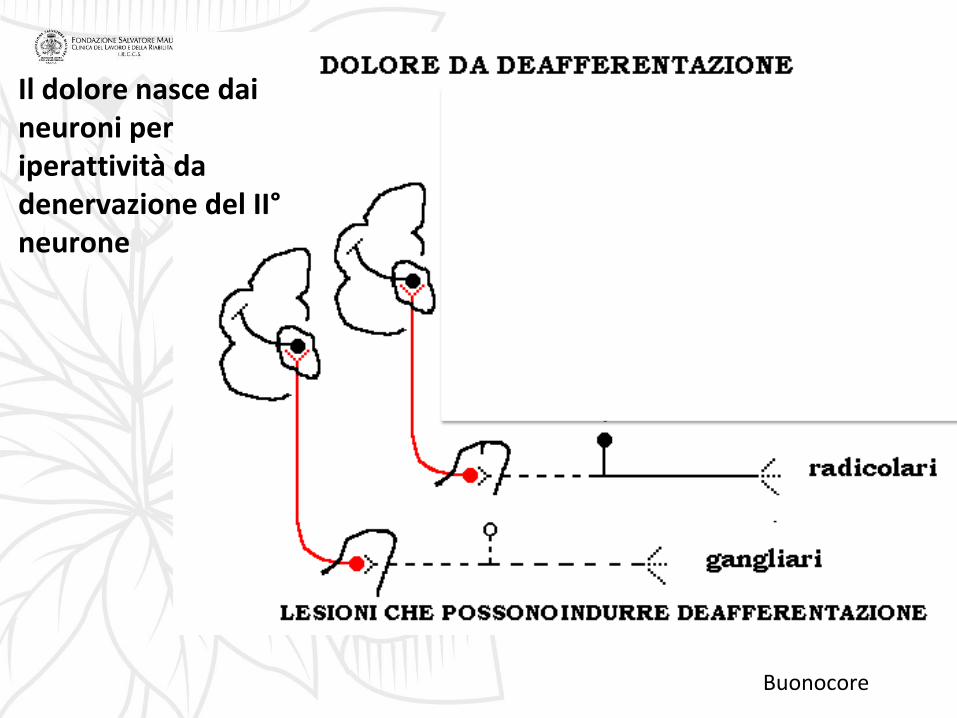
Il dolore nasce dai neuroni per iperattività da denervazione del II° neurone

Deafferentazione del II° neurone per lesione del I° neurone sensitivo
fibre termo-dolorifiche Adelta e C

Buonocore

Avulsione del plesso brachiale


Sensory loss in avulsion of
C5-T1. C4
innervates the skin of the
outer aspect of the shoulder;
T2 innervates the skin of the
inner aspect of the arm
15
Dolore spontaneo (mai evocato) all’avambraccio e alla mano sia in forma di bruciore che di morsa in una zona completamente addormentata (anestesia dolorosa)

Buonocore
Deafferentazione del III° neurone

Buonocore
LESIONI MIDOLLARI
PERDITA DELLE SENSIBILITA’ TERMO-DOLORIFICHE E TATTILI PROPRIOCETTIVE

PERDITA DELLE SENSIBILITA’ TERMO-DOLORIFICA

DEAFFERENTAZIONE CORTICALE

Central post stroke pain

21
Deafferentation Pain
Central Pain
Central Neuropathic
Pain
Anesthesia dolorosa
Thalamic pain

Central pain Dolore che origina nel SNC
22
Central neuropathic pain Dolore ectopico che origina per lesione della via
somatosensoriale centrale
Deafferentation pain Dolore che origina per interruzione della via
termo-nocicettiva tra i neuroni

Considerazioni finali
IL DOLORE IN MOLTE FORME CLINICHE E’ UN DOLORE DA DEAFFERENTAZIONE

I LIVELLI DI DEAFFERENTAZIONE LNGO LA VIA TERMO-NOCICETTIVA

• IL DOLORE DA DEAFFERENTAZIONE E’ SEMPRE SPONTANEO
• SI PRESENTA IN AREE DI ASSENZA DI SENSIBILITA’ TATTILE – DOLORIFICA
• L’ESTENSIONE DELL’AREA E’ MINORE RISPETTO ALL’AREA DI DANNO NEUROLOGICO
• IL DOLORE E’ SEMPRE PROFONDO A VOLTE DESCRITTO COME BRUCIORE E A VOLTE COME MORSA, COSTRIZIONE O ESPLOSIONE
• SCOMPARE CON IL SONNO E SI RIDUCE SENSIBILMENTE IN MOMENTI DI DISTRAZIONE
• AUMENTA CON L’EMOZIONE E GLI EVENTI NEGATIVI
• NON SI ACCOMPAGNA MAI AD ALLODINIA E A IPERALGESIA