dementia and speech abnormalities
TRANSCRIPT

Salim AL-Huseini81575
Dementia and speech
abnormalities SULTANTE OF
OMAN

Case 1
• A 79-year-old man is admitted to the hospital for an elective total knee replacement. He lives by himself and performs all of his activities of daily living. His medical history includes degenerative joint disease, coronary heart disease, and hypertension. He has no history of psychiatric problems or alcohol and drug history.

• In the evening, several hours after an uneventful surgical procedure, the patient becomes diaphoretic and tachypnic. He is alert, but also agitated and confused, and cannot give full attention to the hospital staff and their questions. He does remember his name, but does not believe that he is in a hospital.

Choose the most likely diagnosis
1. Amnesic Disorder2. Delirium3. Dementia4. Multi-infarct dementia

• For the past 10 years the memory of a 74-year-old woman has progressively declined. Lately, she has caused several small kitchen fires by forgetting to turn off the stove, she cannot remember how to cook her favorite recipes, and she becomes disoriented and confused at night. She identifies an increasing number of objects as “that thing” because she cannot recall the correct name. Her muscle strength and balance are intact
Case 2

Choose the most likely diagnosis.
a. Huntington’s disease b. Multi-infarct dementia c. Creutzfeldt-Jakob disease d. Alzheimer’s disease e. Wilson’s disease

case 3
• A 70-year-old male with a dementing disorder dies in a car accident. During the previous five years, his personality had dramatically changed and he caused much embarrassment to his family due to his intrusive and inappropriate behavior. Pathological examination of his brain shows fronto-temporal atrophy, gliosis of the frontal lobes’ white matter, characteristic intracellular inclusions, and swollen neurons. Amyloid plaques and neurofibrillary tangles are absent

Choose the correct diagnosis:
a. Alzheimer’s disease b. Pick’s disease c. Creutzfeldt-Jakob disease d. B12 deficiency dementia e. HIV dementia

Case 4 • 65-year-old woman with a history of MI, hypertension, and
asthma presents with new onset of hallucinations. She can no longer sleep at night because she sees small children and cats in her apartment. She thinks she must be going crazy and is too frightened to explain the symptoms to her husband. She has no prior psychiatric history. Her vital signs are blood pressure supine 115/80 mm Hg and standing 90/60 mm Hg. Physical examination reveals an alert, oriented elderly woman with a slight resting tremor and mild rigidity in her upper and lower extremities, but no cog wheeling. Mini-mental status examination reveals deficits in long-term recall.

Choose the most likely diagnosis.
a. Huntington’s disease b. Parkinson disease c. Creutzfeldt-Jakob disease d. Alzheimer’s disease e. Lewy body dementia

Case 5
• A 78-year-old man comes to the physician for evaluation after falling five times in 2 months. An x-ray skeletal survey reveals no fractures, but the patient admits to worsening urinary incontinence over the previous 4 months. His wife states that his memory and concentration have deteriorated recently.

Choose the most likely diagnosis.
a. Huntington’s disease b. Multi-infarct dementia c. Normal pressure hydrocephalus d. Alzheimer’s disease e. Lewy body dementia

A 72-year-old married man is brought for evaluation to a primary care physician by his wife. His wife is very concerned about her husband’s decline in memory, as well as his development of stuttering speech and a slow gait over the past two to three years.
She reports that he now requires assistance with bathing and grooming, and that he has been reporting seeing children hiding in their bedroom closet. He often refuses to go to bed at night until he removes all of the clothing from the closet in order to “find the children.” He has no prior history of any medical problems and takes no medications.
Case 6

On physical examination : muscle rigidity, with a slow, shuffling gait but no tremor. The patient appears very confused, and his score on a Mini-Mental State Exam is 15/30
Investigations: a complete blood count, chemistry panel, thyroid
profile, syphilis serology, and vitamin B12 and folate levels are all within normal limits.
MRI was ordered (reveals generalized atrophy with no sign of acute infarction).

The patient’s wife calls on the day of the scheduled MRI, stating that her husband had become aggressive while she was trying to dress him..
The physician prescribes risperidone 1 mg twice per day to control his aggression. The patient then develops profound rigidity, with difficulty swallowing and drooling.

What is the most likely diagnosis?
a. Huntington’s disease b. Multi-infarct dementia c. Parkinson disease d. Alzheimer’s disease e. Lewy body dementia

A 78 years old female is brought to the clinic by her daughter . The daughter tells you that her mother is
having difficulty with her memory.
2 years ago & since that time she has deteriorated in a slow steady manner . However she is not totally incapacitated.
She is able to perform some of the activities of daily living : dressing & bathing .When she cooks ,she often leaves burners on & when she drives the car she often gets lost.
Case

What are the points that make the diagnosis of dementia most likely in this case???
The daughter states that her mother’s memory and confusion have been getting worse Her personality has changed ,her kind &caring mother now displays periods of both agitation and aggressionNo history of trauma not alcoholic PMH : unremarkable FH: unremarkable Examinations : unremarkable

Definition
- Progressive deterioration of intellectual function with preservation of consciousness.
-Most important risk factor is increasing age
5% of population over the age 65 years 20% of population over the age 80 years
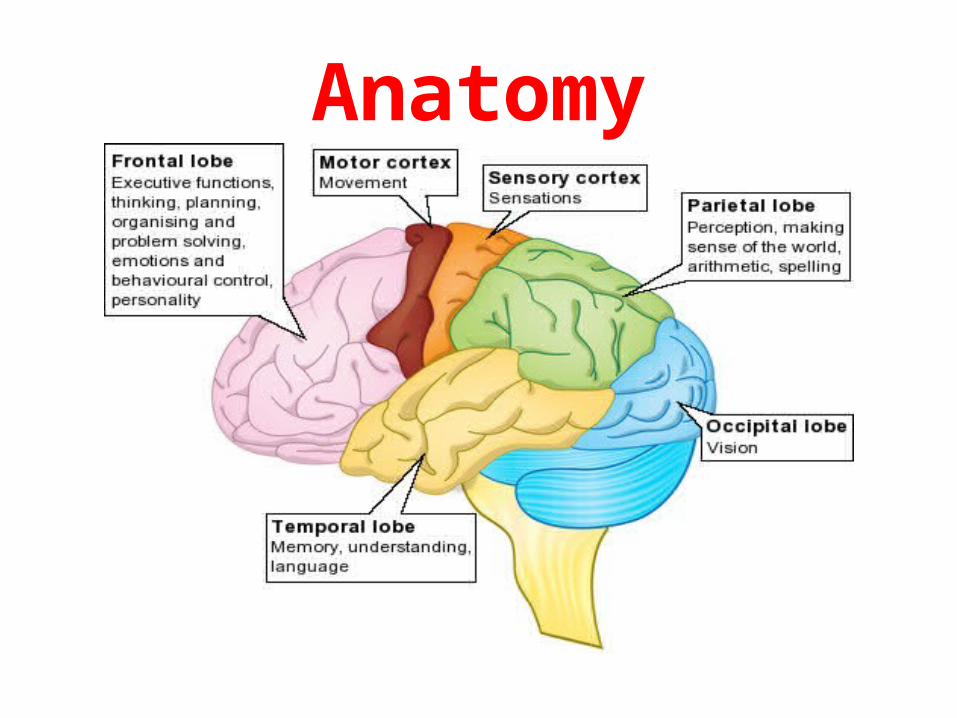
Anatomy

Delirium vs. Dementia Variable Delirium Dementia
Level of attention Impaired (fluctuated) Usually, alert
Onset acute Gradual
Course Fluctuating from hour to hour ( sun downing)
Progressive deterioration
consciousness Clouded Intact
Hallucinations Present In advanced case
Prognosis Reversible Largely irreversible , but up to15% due to treatable causes and are reversible

• Poor memory ( more for recent)• Impaired attention
• Aphasia, apraxia• Disoriented
Cognition
• Odd and disorganized• Restless, wondering
• Self neglect
Behaviour
• Anxiety• DepressionMood
Clinical features

• Slow• delusionsThinking
• illusion• hallusination
Perception
•impairedInsight



Frequency of common causes of dementia
Alzheimer s disease 50-60%Vascular disease 15-20%Mixed dementia 10-20%Other <10% like lewy-body dementia, pick s disease,
alcohol related,vitm B12...
aafp.org

assessmentAims:*identify rare treatable conditions that may present as dementia*diagnose any condition that may exacerbate dementia (..eg.. Delirium, infection)* Obtain the information needed to plan continuing care.
Assessment of functional capacity in dementia pt:
*Continence*Dressing*Self-care*Cooking ability and nutrition*Shopping/ housework*Degree of orientation at home*Social contact*Safety in the home

• Patient history:Interview the patient and their family members
about nature of onset, specific deficits, physical symptoms, and comorbid conditions
Review medications, as well as family and social history
assessment

• Examination:
General appearance.Speech, mood, thinking, behavior.aphasia, apraxia, agnosia and executive functioning. Mini mental state examination.Neurological examination.Systemic examination.
assessment

Mini Mental State Examination
Maximum score Score
5 ___
5 ___
3
___
5 ____
3
____
Orientation 1. What is the (year) (season) (date) (day) (month)?2. Where are we: (state) (county) (town or city) (hospital)
(floor)? Registration 3. Name three common objects (e.g., "apple," "table,"
"penny"): Take one second to say each. Then ask the patient to repeat all three after you have said them. Give one point for each correct answer. Then repeat them until he or she learns all three. Count trials and record. Trials: ___
Attention and calculation 4. Spell "world" backwards. The score is the number of
letters in correct order.(D___L___R___O___W___)
Recall5. Ask for the three objects repeated above. Give one point
for each correct answer.(Note: recall cannot be tested if all three objects were not remembered during registration.)

Mini Mental State Examination- cont
Maximum score Score
2 ___
1 ___
3
___
1
___ 1
___ 1
___
Total score: 30
___
Language 6. Name a "pencil" and "watch." 7. Repeat the following: "No ifs, ands
or buts." 8. Follow a three-stage command: "Take a paper in your right hand, fold
it in half and put it on the floor.“9. “CLOSE YOUR EYES”. 10. Write a sentence. 11. Copy the following design:
Scores of 24 or higher are generally
considered normal.

Blood test •FBC, ESR, CRP•T4 and TSH•urea and
creatinine•glucose•B12 and folate
•syphilis
serology•HIV •caeruloplasmi
n
other
•cerebrospinal fluid
examination•electroenceph
alography (EEG)
Imaging
•MRI•CT•SPECT
investigation

Management:
Treat any treatable physical disordersTreat the cause of superimposed deliriumTreat even minor medical problemsInvolve and support relativesArrange help for carersMedications for night and daytime restlessnessIf home care fails, arrange hospital care

Drug treatment*Restlessness: sedative ..eg thioridazine, promazine*Paranoid delusions: antipsychotic*Depressive symptoms: antidepressent*Alzheimer's disease: cholinesrerase inhibitors..eg donepezil, rivastigmine


Alzheimer’s diseas
e
• most common type of dementia.• The prevalence increase with age .
RF• FH• down syndrome• Head injury
Cause • Accumulation B amyloidal peptide cause
progressive neural damage increase number of senile plaques reduced cerebral production of acetylcholine synthesis
Alzheimer's disease

Pathophysiology
• Genetic factors• Pathogenesis: Gross pathology : o diffuse atrophy especially frontal and
temporal and parietal lobes\ Dilation of ventricles

Con/ Pathogenesis
• Microscopic pathology: Senile plaques, amyloid angiopathy Neurofibrillary tanglesBiochemical pathology: 50-90% reduction in
action of choline acetyltransferase


CF • slowly progressive memory loss of
insidious onset in a fully conscious patient
• slowly progressive behavioral changes
CF• Aphasia • Apraxia • Agnosia
• Disturbance of executive functions
Treatment • cholinesterase inhibitors,(donepezil,
rivastigmine, and galantamine are currently approved
• Antiglutamatergic (memantine)
Alzheimer's disease
VD • 2nd most common cause of dementia.
Pathology
• Multiple infarcts of varying size• The brain is atrophic , ventricular
dilatation
Clinical features
• Stepwise progression • Episodes of confusion
• Seizure• Neurological signs
Vascular dementia

Diagnostic criteria
for Vascular
dementia:
• Vascular risk factors such as hypertension, coronary
disease, and diabetes mellitus
• Specific evidence of :• strokes and transient -
ischemic attacks • Neuroimaging evidence of
strokes • Psychiatric disturbances (eg,
emotional lability, depression, apathy)

LBD • characterized by dementia and Parkinson’s disease .
• More rapid than in Alzheimer's disease
Pathology • Lewy bodies (pale halo-like intracellular, eosinophilic inclusions. )
CF • Initially ,visual hallucination predominant .• Fluctuating cognitive loss
• sings of parkinsonism• Sensitive to side effects of neuroleptic drugs
Lewy body disease

• hydrocephalus that occurs in adults, usually older
adults.•It is tried of: dementia,
ataxia, incontinence
cause•The drainage of CSF is
blocked gradually, and the excess fluid builds up
slowly.
treatment
•Shunt surgery is the most common treatment for the
symptoms of normal pressure hydrocephalus.

Fronto-temporal Dementia
FTD• A rare, progressive form of dementia characterized by
core symptoms of:• disinhibtion, emotional lability, apathy and or
detachment• (PICK’S DISEASE)
Diagnosis
• front temporal atrophy in MRI or CT.• Cytoplasmic inclusion bodies (Picks
bodies)


Conclusion • Dementia is common and its different from cognitive decline
due to normal aging process
• The most common type of dementia is AD followed by VD
• Early detection of AD plays a significant role in better prognosis • VD can be prevented by controlling the risk factors
• There are several treatable forms of dementia like in: hypothyroidism, nutritional deficiencies, NPH

Speech Abnormalities

MCQ1
• One of the most common features of neurological disorders are Language deficits and are collectively known as
• a) Dysphasias• b) Alogias • c) Anomias• d) Aphasias

MCQ2
• When an individual displays a deficit in the comprehension of speech involving difficulties in recognising spoken words and converting thoughts into words is known as
• a) Wernicke's aphasia • b) Broca's aphasia • c) Beidecker's aphasia • d) Warnick's aphasia

MCQ3
• If an individual has an inability to initiate speech or respond to speech with anything other than simple words is known as
• a) Nonfluent aphasia • b) Fluent aphasia • c) Disruptive aphasia • d) Anomic aphasia

What is Aphasia• Aphasia is an impairment of language.
(speak , understand ,fluency ,reading and writing)
• Most of the lesion that cause aphasia involve dominant hemisphere. (95% of R handed people, the L cerebral hemisphere is dominant.


PROCESS OF SPEECH
TYPES OF SPEECH DISORDERS
HEARING
UNDERSTANDING
THOUGHT &WORD PROCESSING
VOICE PRODUCTION
ARTICULATION
DEAFNESS
APHASIA
APHASIA
DYSPHONIA
DYSARTHRIA

Etiology• stroke (most common cause )• injury to the brain • tumors in the brain• Alzheimer's disease

Type of aphasia
– Broca’s anterior aphasia (expressive)– Wernicke’s posterior aphasia (receptive)– Conduction aphasia– Nominal aphasia– Global aphasia

Boca's Area or Brodmann areas 44 & 45
• Its The motor speech area• posterior inferior frontal gyrus • formation of words • connections with the adjacent primary motor
areas - the muscles of the larynx, mouth, tongue,
soft palate, and the respiratory muscles • controls the output of spoken language.

Broca’s aphasia
• Expressive, no fluent aphasia • comprehension is intact .• Effortful speech and slow .• Often associated with a right side
hemiparesis.

Wernicke's area or Brodmann's area 22
• sensory speech area • superior temporal gyrus with extensions around the posterior end of the lateral sulcus into the parietal region. • It receives fibers (visual cortex and auditory
cortex in the superior temporal gyrus). • It permits understanding written and spoken
language

Wernicke’s Dysphasia
• Receptive ,fluent aphasia .• Impaired comprehension of writing or
spoken language. • intact speech ,but not make much sense .-Phonemic problem e.g. flush for brush

Conduction Aphasia
• Communication between Broca’s and Wernicke’s area is impaired
• Repetition is impaired • Comprehension and fluency are less affected

Nominal aphasia
• Naming of objects is impaired, but other aspects of speech are intact
• Lesion is usually in the posterior dominant temporoparietal area


DYSARTHRIA
• Acquired speech disorder caused by impaired control of muscle responsible for speech
• Caused by weakness, paralysis, or incoordnation of the speech muscle.
• The language content is normal .

Causes
• Stroke • Nerve – muscle diseases eg ( Myasthenia gravis )• Muscle disease eg ( myopathy )• Progressive neurological disease - Parkinson's - Huntington's

Types • Spastic ; UMN damage, bilateral • Flaccid ; LMN damage • Ataxic ; cerebellar damage• Hypokinetic; extrapyramidal - Parkinson's disease • Hyperkinetic; extrapyramidal - Huntington's disease • Mixed ; multiple motor system affected

Spastic dysarthria
• Common type of dysarthria • Caused by bilateral damage to UMN • Causes - stroke - ALS ( amyotrophic lateral sclerosis) - MS• Neurological symptoms - weakness, reduced ROM, decrease fine motor
control

Flaccid dysarthria
• Caused by impairment of LMNs in cranial nerve and spinal nerve
• Weakness in speech or respiratory musculature• Vital CNs to speech production - trigeminal , facial , glossopharyngeal, vagus ,
accessory and hypoglossal • Relevant SNs - cervical and thoracic

Ataxic dysarthria
• Damage to cerebellum • Primarily affect articulation and prosody• Cuases - Degenerative disease - Stroke - Toxic condition * lead , mercury, alcoholism , cyanide - tumors, infection

Hypokinetic dysarthria• Associated with basal ganglion pathology • The only dysarthria that may have increased speech rate • Causes - Parkinson's disease - traumatic head injury * punch drunk encephalopathy - toxic metal poisoning -stroke • Neurological symptoms - increased muscle tone , decreased range and frequency of
movement

Hyperkinetic dysarthria
• Dysfunction to basal ganglia• Produce involuntary movements that interfere
with normal speech production • Causes - chorea - tardive dyskinesia - dystonia

DYSPHONIA
• Is due to defect in the production of soundCAUSES1) Laryngeal diseases-eg;laryngitis2) Vocal cord lesions3) Xth cranial nerve palsy4) psychogenic

Evaluation
• Assess comprehension: – Ask the patient to carry out one, two or several steps of
command– E.g. Stand up, jump and close the door
• Assess repetition: – Ask the patient to repeat a sentence
• Assess naming: – Ask the patient to name common and uncommon things
• Assess reading and writing: – Usually affected in dysphasia

Evaluation
• Dysarthria and dysphonia– Listen to spontaneous speech, note VOLUME,
RHYTHM and CLARITY– Ask the patient to repeat phrases like ‘yellow
lorry’ to test lingual sounds and ‘baby hippopotamus’ to test labial sounds and some tongue twisters
– Ask the patient to count till 30 to assess muscle fatigue
– Ask the patient to cough and say ‘Aaah’

Evaluation
• Dysphasias– During spontaneous speech, listen to FLUENCY and
APPROPRIEATNESS of content, particularly for par aphasias and neologisms
– Ask the patient to name common objects – Give the patient a 3-stage command– Ask the patient to repeat simple sentences– Ask the patient to read a paragraph– Ask the patient to write a sentence and examine the
handwriting

Management
• Most patients recover spontaneously or improve within the first month
• Speech therapy can be helpful, but unlikely to be of benefit after the first few months

• Pharmacological treatment for aphasia following stroke (Review)
• Speech and language therapy for aphasia following stroke (Review)

Resources
• Macleod’s clinical examination• Davidson’s principles and practice of medicine• Oxford handbook of clinical medicine• Step up to medicine