deliverable 6.4: report on learning session ii · 2018-01-24 · report on learning session ii wp...
TRANSCRIPT
This publication arises from the ACT@Scale (Advancing Care Coordination and Telehealth deployment at Scale) Programme which has received funding from the European Union, in the framework of the Health Programme under grant agreement 709770. The ACT@Scale programme is fully aligned with the European Innovation Partnership in Active and Healthy Ageing objectives to deploy integrated care for chronically ill patients.
Deliverable 6.4:
Report on learning session II
WP 6: Service Selection
ACT@Scale Advancing Care Coordination
and Telehealth @ Scale
D 6.4: Report on learning session II
Public Page 2 of 89 V 1.0/ 21 Dicember 2017
Document Information
PROJECT ACRONYM: ACT@Scale CONTRACT NUMBER: 709770 DISSEMINATION LEVEL: Confidential / Public / Restricted NATURE OF DOCUMENT: Report
TITLE OF DOCUMENT: Report on learning session II REFERENCE NUMBER: D6.4 WORKPACKAGE: WP6 VERSION: V1.0 EXPECTED DELIVERY DATE: M20 DATE: 21 December 2017 AUTHORS:
Kronikgune Danika Schepis [email protected] Ane Fullaondo [email protected] Esteban de Manuel [email protected]
EDITOR: Danika Schepis, Kronikgune, [email protected]
Short description of the Deliverable: With the support of the Evaluation Engine: • Follow up the implementation process performed by each region and the PDSA cycles • Extract main lessons learned in the implementation process • Promote the transferability of knowledge throughout the process

D 6.4: Report on learning session II
Public Page 3 of 89 V 1.0/ 21 Dicember 2017
REVISION HISTORY
REVISION
DATE COMMENTS AUTHOR (NAME AND ORGANISATION)
V0.0 14/07/2017 Deliverable structure Danika Schepis, Kronikgune
V0.1 12/09/2017 Scheme correction, subject development, programs contribution
Danika Schepis and Ane Fullaondo, Kronikgune, WP5 partners, Cataluña
V o.2 25/09/2017 PLAN and DO template from Cataluña
Danika Schepis and Ane Fullaondo, Kronikgune, partners, Cataluña
V 0.3 02/10/2017 KPI analysis Danika Schepis and Ane Fullaondo, Kronikgune
V 0.4 05/10/2017 Change in structure Danika Schepis, Ane Fullaondo and Esteban de Manuel, Kronikgune
V 0.5 25/10/2017 PDSA analysis Danika Schepis, Ane Fullaondo and Esteban de Manuel, Kronikgune
V 0.6 20/11/2017 Study phase analysis Danika Schepis, Ane Fullaondo and Irati Erreguerena, Kronikgune
V 0.7 12/12/2017 Study phase analysis by AISBE and Aquas
Danika Schepis and Ane Fullaondo, Kronikgune; Joseph Roca, AISBE, Nuria Rodriguez, Aquas
V 1.0 21/12/2017 Final revision and editiong Danika Schepis and Ane Fullaondo, Kronikgune
Disclaimer
The content of this report represents the views of the author only and is his/her sole responsibility; it cannot be considered to reflect the views of the European Commission and/or the Consumers, Health, Agriculture and Food Executive Agency or any other body of the European Union. The European Commission and the Agency do not accept any responsibility for use that may be made of the information it contains.

D 6.4: Report on learning session II
Public Page 4 of 89 V 1.0/ 21 Dicember 2017
Background Deliverable 6.4 Advancing Care Coordination & TeleHealth (ACT) project goal is to identify, transfer and scale up existing and operational Care Coordination and Telehealth good practices with the target of reaching a total of 75,000 care recipients across regions and programmes in multiple European countries.
ACT@Scale taps into experiences from successful real life deployment projects in five European regions by using indicators to assess real world services and linking drivers and outcomes. The project activities are built around key methods and aspects needed in order to reach the project goal. At the same time, the activities reflect the areas that need to be addressed in an upscaling process. These areas include and cover: Stakeholder and change management, Service selection, Sustainability and business models, Citizen empowerment.
Work Package on Service Selection (WP6) aim is to achieve an appropriate level of distribution of health and care resources defined by the dynamic needs of the patients and populations addressed, enhancing risk prediction in the clinical scenario.
WP6 has committed to produce at least a deliverable at the end of each phase of the project, as described in the table below:
Table 1 ACT@Scale project Phases and WP6 deliverables
Baseline phase
Learning cycle phase Coaching phase Dissemination phase
M0-6 M7-18 M19-30 M31-36 D6.1 Service selection methodology report
D 6.2 Report on learning session I D 6.3 Report on learning cycle
D6.4 Report on learning session II D6.5 Report on coaching cycle
D 6.6 Final report on service selection
Deliverable 6.4 encompasses the work done during months 7 to 18 in WP5: the learning cycle and introduces the next phase with the first learning session M19. It compiles a comprehensive overview of the PDSA process of the ACT@Scale programmes selecting service selection as key driver for scaling-up, which were:
1. Multimorbid population integrated intervention (MM) -Basque Country 2. Telemonitoring services for congestive heart failure (CHF)-Basque Country 3. Support of Complex case managment (AISBE-CCP) -Catalonia 4. Integrated care for subacute and frail older adults , Parc Sanitari Per Virgili (FOA-
PSPV) -Catalonia 5. Collaborative self-management services to promote healthy life style: physical
activity (AISBE-PA) -Catalonia 6. Diabetes monitoring program -Northern Ireland
D 6.4: Report on learning session II
Public Page 5 of 89 V 1.0/ 21 Dicember 2017
Executive Summary
The aim of ACT@Scale is to scale up good practices within a given region by implementing collaborative approaches. ACT@Scale methodology, based on Plan-Do-Study-Act (PDSA) cycles, applies multi-organizational structured collaborative quality improvement procedures and adapts them to scale up integrated care experiences.
This deliverable documents the information gathered during the first PDSA cycle in those programs that have selected the service selection driver. This information is organized and follows the structure below:
Road maps description: similarities and diversities between programs Analysis of PDSA cycle in the programs that have selected Service
Selection Evaluation and future implementacions
From the roadmaps analysis, it is clear which areas each program has to improved. All programs that selected service selection as a driver have identified the underuse of stratification tools and methods as area of improvement. More over, the two programs from Basque Country described the need to work on care fragmentation detected in their system. The first PDSA cycle has allowed programs to make significant progress in the interventions outlined, most of them have reported an implementation progress of 25-50%. They all have deeply described improvements and difficulties in the planned interventions. None of the programs has dismissed any of the planned actions, meaning that the initial interests and priorities still remain. Some programs has noted the need for new interventions that might be taken into account during the second PDSA cycle.
D 6.4: Report on learning session II
Public Page 6 of 89 V 1.0/ 21 Dicember 2017
Content Document Information ............................................................................................................2
Executive Summary .................................................................................................................. 5
1. Collaborative methodology in ACT@Scale ......................................................................... 9
2. Service Selection programs ................................................................................................. 9
3. Roadmaps ........................................................................................................................... 10
3.1 Improvement areas ........................................................................................................ 11
3.2 Objectives ...................................................................................................................... 13
3.3 Interventions ................................................................................................................. 15
4 PLAN phase ......................................................................................................................... 17
4.1 Introduction ................................................................................................................... 17
4.2. Multimorbid population integrated intervention - Basque Country ........................ 17
4.2.2 Roles ....................................................................................................................... 17
4.2.2 Carer's plan review ................................................................................................ 18
4.2.3 Reconciliation of the care plan .............................................................................. 19
3.2.4 Training on stratification ....................................................................................... 19
4.3 Telemonitoring services for Congestive Heart Failure (CHF)- Basque Country ...... 22
4.3.1 Patient Identification ............................................................................................. 22
4.3.2 Care Plan ............................................................................................................... 22
4.3.3 Monitoring services ................................................................................................ 23
4.3.4 Data collected ......................................................................................................... 23
4.4 Support of Complex case Managment (AIBSE-CCP)- Catalonia ...............................25
4.4.1 Changes ..................................................................................................................25
4.4.2 Data collected ....................................................................................................... 27
4.5 Integrate Care for Subacute and frail Older Adults (PSPV) - Catalonia .................... 29
4.5.1 Changes.................................................................................................................. 29
4.5.2 Data collected ........................................................................................................ 30
4.6 Collaborative Self-Management services to promote healthy life style: Physical Activity (AIBSE-PA) - Catalonia ........................................................................................ 31
4.6.1 Changes .................................................................................................................. 31
4.6.2 Data collected ........................................................................................................ 33

D 6.4: Report on learning session II
Public Page 7 of 89 V 1.0/ 21 Dicember 2017
5. DO phase ............................................................................................................................ 34
5.1 Introduction ................................................................................................................... 34
5.2 Multimorbid population integrated intervention -Basque Country ........................... 34
5.2.1 Roles ........................................................................................................................ 34
5.2.2. Carer's plan review ............................................................................................... 35
5.2.3 Reconciliation of the care plan .............................................................................. 37
5.2.4 Training on stratification ....................................................................................... 38
5.3 Telemonitoring services for Congestive Heart Failure (CHF) - Basque Country....... 41
5.3.1 Patient Identification .............................................................................................. 41
5.3.2 Care Plan ................................................................................................................ 42
5.3.3 Monitoring services ................................................................................................ 43
5.4 Support of Complex case Management (AIBSE-CCP) – Catalonia ........................ 45
5.5 Integrated care for subacute and frail older adults (PSPV) - Catalonia.................... 48
5.6 Collaborative Self-Management services to promote heathly life style: Physical Activity (AIBSE-PA) – Catalonia ................................................................................... 50
5.7 Summary ....................................................................................................................... 53
6. STUDY phase ..................................................................................................................... 54
6.1 Introduction ................................................................................................................. 54
6.2 Impact on service selection ......................................................................................... 56
6.3 Multimorbid population integrated intervention - Basque Country .......................... 57
6.4 Telemonitoring services for congestive heart failure (CHF)-Basque Country.......... 61
6.5 Support of Complex case managment (AISBE-CCP) – Catalonia ............................. 65
6.7 Integrated care for subacute and frail older adults , Parc Sanitari Per Virgil (PSPV) - Catalonia ............................................................................................................................ 70
6.5 Collaborative self-management services to promote healthy life style: physical activity (AISBE-PA) – Catalonia ........................................................................................ 73
6.6. Global analysis ............................................................................................................ 78
7. ACT phase ........................................................................................................................... 81
7.1 ACT phase Reporting .................................................................................................... 81
7.2 Multimorbid population integrated intervention -Basque Country .......................... 82
7.3 Telemonitoring services for congestive heart failure (CHF)-Basque Country .......... 83
7.4 Support of Complex case managment (AISBE-CCP) –Catalonia .............................. 84

D 6.4: Report on learning session II
Public Page 8 of 89 V 1.0/ 21 Dicember 2017
7.5 Integrated care for subacute and frail older adults , Parc Sanitari Per Virgil (PSPV) -Catalonia ............................................................................................................................ 85
7.6 Collaborative self-management services to promote healthy life style: physical activity (AISBE-PA) –Catalonia ........................................................................................ 86

D 6.4: Report on learning session II
Public Page 9 of 89 V 1.0/ 21 Dicember 2017
1. Collaborative methodology in ACT@Scale
The aim of ACT@Scale is to scale up good practices within a given region by implementing collaborative approaches. ACT@Scale methodology is based on Plan-Do-Study-Act (PDSA) cycles, as described in D 6.1. This methodology helps to apply multi-organizational structured collaborative quality improvement procedures and to adapt them to scale up integrated care experiences.
The different phases of the collaborative methodology of ACT@Scale are:
1. Baseline phase 2. Learning cycle 3. Coaching cycle 4. Dissemination phase
In D 5.2 ,6.2, 7.2 and 8.2 deliverables each program have described the information collected in the baseline phase.
2. Service Selection programs
The programs that have selected ”Service Selection” as a driver are:
7. Multimorbid population integrated intervention (MM) -Basque Country 8. Telemonitoring services for congestive heart failure (CHF)-Basque Country 9. Support of Complex case managment (AISBE-CCP) -Catalonia 10. Integrated care for subacute and frail older adults , Parc Sanitari Per Virgili (FOA-
PSPV) -Catalonia 11. Collaborative self-management services to promote healthy life style: physical
activity (AISBE-PA) -Catalonia 12. Diabetes monitoring program -Northern Ireland
Five out of 6 programs that had selected service selection driver continue in the project. The Diabetes Telehealth program from Northern Ireland has withdrawn from ACT@Scale project. This program has provided considerable support and reassurance
D 6.4: Report on learning session II
Public Page 10 of 89 V 1.0/ 21 Dicember 2017
to many individuals, their families and cares over the past six years. However, the contract for the existing service has come to an end. In the context of a challenging financial climate, and taking account of an evaluation of the service, it has been agreed that the current Telehealth service will be phased out.
3. Roadmaps
During the baseline phase , each multidisciplinary team analysed the baseline status of each program (D6.2). Improvement areas were detected, objetives agreed and specific actions to be implemented defined. Based on this information, each program generated a roadmap that has guided the learning sessions and action periods of the PDSA cycles.
Roadmaps of the programs working specifically in service selection driver were compared, in order to extract commonalities, differences and insights. This exercise, which was carried out during the 3rd General Asembly in Groningen, allowed to share challenges and different approaches between programs.
In the following tables (pag 10-15), the improvement areas, objectives and interventions planned for service selection driver are presented. Commonalities, differences and insights between programs are described.
Tables abbreviation list: BAS: Basque Country MM: Mutimorbid integrated patients program CHF: Telemonitoring of CHF patients program CAT: Catalonia CCP: Complex case management program PA: Physical activity program

D 6.4: Report on learning session II
Public Page 11 of 89 V 1.0/ 21 Dicember 2017
3.1 Improvement areas
Improvement areas
1: Care fragmentation
Care plans created by different professionals are not shared and patient´s view is not included. Monitoring services are not adapted to patients´ and caregivers´ capacities and disease´s phase.
Multiple disease-based care plans. Detected discontinuity due to poor coherence in services, fragmented care, gap between social and health care. Not all stakeholders involved/have access to the plan. Unclear definition of roles.
Multimorbid integration
Telemonitoring CHF
BAS:
Gaps in coordination between different care levels in patients´ care plan definition.
MM Care fragmentation at all levels. CHF: Poor information sharing between stakeholders.
description commonalities insights differences
MM Relevant care fragmentation.
VS
CHF: Importance of patients’ perspective.

D 6.4: Report on learning session II
Public Page 12 of 89 V 1.0/ 21 Dicember 2017
Telemonitoring CHF
Improvement areas
1: Underuse of stratification tools and methods
Poor clinical risk assessment - Arbitrary criteria - Only clinical criteria - Not considering population based stratification patients & dynamic changes Need refinement of some integrated care services: information exchange and patient empowerment.
Clinical variables and social aspects are not considered in the stratification. Output of the stratification is not updated as frequent as needed. Lack of clinical view in the stratification of patients. Non-dynamic stratification which does not respond to changing needs. Poor professionals´ credibility on the tool.
Multimorbid integration
BAS & CAT:
Link population based strategy with clinical risk assessment.
Clinicians perceive population based strategy non-matching current clinical status (they do not see the benefit).
BAS: No social support data yet. No education on stratification Updates: 1 year
VS
CAT: Updates: 6 months
description commonalities insights differences
BAS: Clinicians need data on daily basis.
Clinicians need better understanding on how to use population- based strategy.
CAT: Better criteria to indetify patients at risk
Complex case management
Physical activity
Better identification of risk patients in early readmission and difficult care transition.
Frail older adults

D 6.4: Report on learning session II
Public Page 13 of 89 V 1.0/ 21 Dicember 2017
3.2 Objectives
Objectives
1: Care fragmentation
Ensure the existence of an updated personalized care plan agreed by all stakeholders. Make the care plan visible to all stakeholders. Provide monitoring service adapted to patient capacities and disease phase.
Create a reconciled care plan agreed by all stakeholders. Assess patient on health, social and mental status, share information with all stakeholders.
Multimorbid integration
Telemonitoring CHF
BAS:
Need for shared and reconciled care plan.
MM: Similar roles in all organizations but disctinct actors performing the activities. CHF: Personalized monitoring interventions included in the care plans.
description commonalities insights differences
MM: Monitoring service adapted to patients health.
VS CHF: Shared care plan among all stakeholders.
Have personalized care plans and align resources and capacity
Align the resources and capacity of each organization with the corporative model to be deployed.

D 6.4: Report on learning session II
Public Page 14 of 89 V 1.0/ 21 Dicember 2017
Telemonitoring CHF
Include dynamic predictive risk. Evaluate transitional & long term community care model. (Re)define, implement, evaluate program: transitional care services, workflows, collaborative platform. Link tertiary care to primary care (vertical).
Consider more clinical variables and social features into the stratification and align the patients changing characteristics with stratification output. Population-based stratification: - Consider the clinical perspective of healthcare professionals -Specify the criteria - Improve professionals understanding
Multimorbid Integration
BAS & CAT: Giving more info to professionals. Right selection of patients.
BAS: Offer more tools to professionals to increase their knowledge on stratification VS CAT: Integrations. Catalonia is more focused on vertical and horizontal integration.
description commonalities insights differences
Empower professionals to use the stratification systems.
Complex case management
Physical activity
Frail older adults
Identify risk patients in early readmission and difficult care transition. Validated model to identify risk factors. Find predictors factors for readmission. Horizontal integration within community.
Objectives
1: Care fragmentation
Apply stratification to provide right service to patient (and caregivers)
Include dynamic predictive risk. Refine & expand program for regional scalability: community based services, collaborative platform for interoperability, assess convergence, implement and evaluate (regional roadmap).

D 6.4: Report on learning session II
Public Page 15 of 89 V 1.0/ 21 Dicember 2017
3.3 Interventions
Interventions
1: Care fragmentation
Resources (tools, guidelines and training) available for personalized care plans for all stakeholders.
Agree on inclusion criteria for monitoring service that fit better with patient/caregivers disease phase and capacities.
Regular review of care plan and adapt it to patient’s changing needs. Plan available in Electronic Health Records for all care professionals on 24x7 basis.
Multimorbid integration
Telemonitoring CHF
BAS: Regular update in terms of service and resources available to personalized care plan
MM: Definition of roles involved in the pathway. CHF: Definition of inclusion criteria for monitoring service.
description commonalities insights differences
MM: Clear structure of integrated care pathway.
VS CHF: Tools for better personalize care plans.
Develop care plans and defined roles and procedures
Describe the roles (social and health care) required in the integrated care pathway for multimorbid patients and define the specific actors who will perform these roles in each organization.

D 6.4: Report on learning session II
Public Page 16 of 89 V 1.0/ 21 Dicember 2017
Telemonitoring CHF
Implement the Complex case program (CCP) protocol: Community-based management of CCP. Integrated care for patients under long-term oxygen therapy. Adoption of information and communication technologies. Adaptive case management tools. Deployment of program.
Prepare, plan and provide training sessions for professionals to explain the theoretical basis of the stratification, its methodology and its application in the Basque Health System.
Multimorbid Integration
CAT: Enhanced clinical risk assessment and stratification
MM: Universal training for all professionals CHF: Integration patient´s health info into EHR CCP: Implementation of CCP protocol PA: New stratification approach
description commonalities insights differences
MM: provide training sessions on theoretical basis of the stratification CHF: Telemonitoring data accessible on the EHR CCP: Structured service workflow definition using a collaborative & adaptive case management (ACM) approach PA: Include study based evaluation to predict risk factors
Complex case management
Interventions
2: Underuse of stratification tools and methods
Improve current stratification approach and Evaluate revised stratification
New stratification approach: Pre-habilitation programme for high risk candidates to major surgery. Clinically stable chronic patients in Primary Care.
Integrate patient´s health info in the Electronic Health Record. Run the stratification´s update in a 6-month basis.
Evaluation: dynamic predictive risk, models for enhanced transitional & long term community based management, population based health risk, assessment & stratification, health care value generation services.
Evaluation: dynamic predictive risk, population based health risk, risk assessment & stratification, supporting ICT tools, assessment strategies, healthcare value generation services
Physical activity
D 6.4: Report on learning session II
Public Page 17 of 89 V 1.0/ 21 Dicember 2017
Based on the results of the baseline analysis above represented, each program identified improvement actions to be implemented that are subject of the learning cycle.
In the following sections the work performed by programs durig the PDSA steps is documented.
4 PLAN phase
4.1 Introduction PLAN phase is the first step of the learning cycle and aims to plan the actions and develop a framework to test the change. The timeframe for this phase was from October 2016 to December 2016. During this phase at least one multidisciplinary team meeting per program was organized to outline the implementation of improvement changes.
Description of PLAN phase for each service selection program is described below.
4.2. Multimorbid population integrated intervention - Basque Country
4.2.2 Roles
D 6.4: Report on learning session II
Public Page 18 of 89 V 1.0/ 21 Dicember 2017
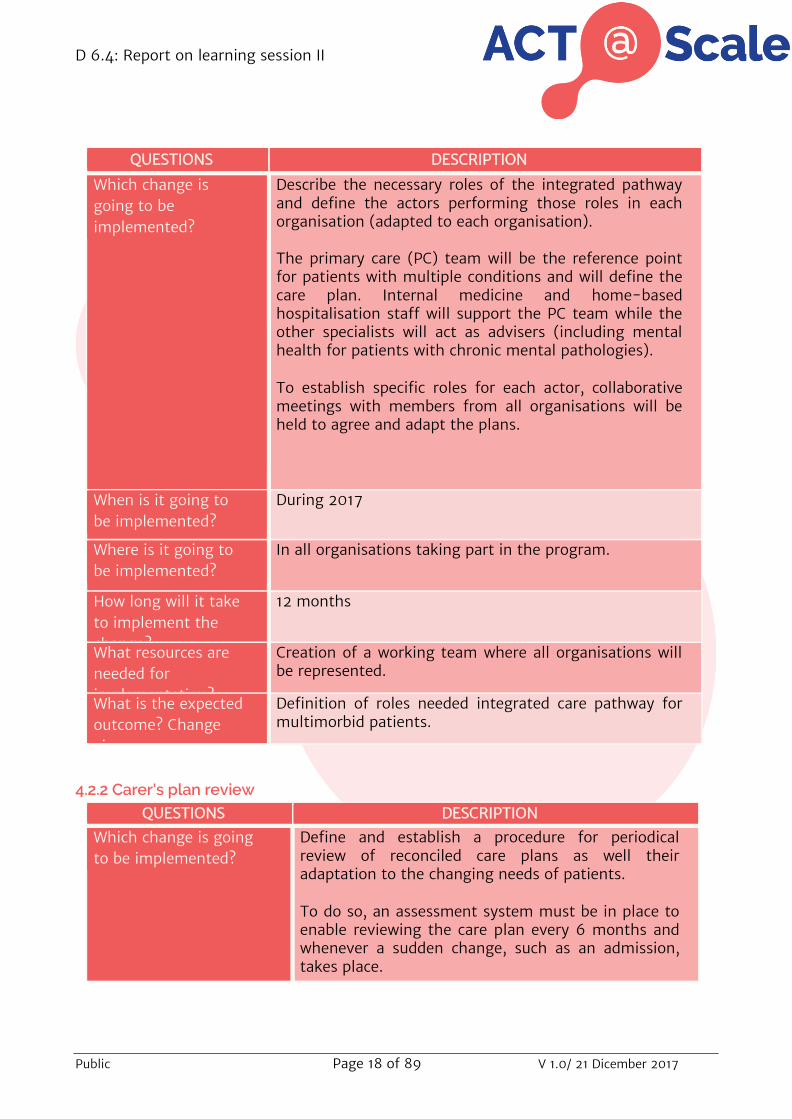
QUESTIONS DESCRIPTION
Which change is going to be implemented?
Describe the necessary roles of the integrated pathway and define the actors performing those roles in each organisation (adapted to each organisation).
The primary care (PC) team will be the reference point for patients with multiple conditions and will define the care plan. Internal medicine and home-based hospitalisation staff will support the PC team while the other specialists will act as advisers (including mental health for patients with chronic mental pathologies).
To establish specific roles for each actor, collaborative meetings with members from all organisations will be held to agree and adapt the plans.
When is it going to be implemented?
During 2017
Where is it going to be implemented?
In all organisations taking part in the program.
How long will it take to implement the change?
12 months
What resources are needed for implementation?
Creation of a working team where all organisations will be represented.
What is the expected outcome? Change aims
Definition of roles needed integrated care pathway for multimorbid patients.
4.2.2 Carer's plan review QUESTIONS DESCRIPTION
Which change is going to be implemented?
Define and establish a procedure for periodical review of reconciled care plans as well their adaptation to the changing needs of patients.
To do so, an assessment system must be in place to enable reviewing the care plan every 6 months and whenever a sudden change, such as an admission, takes place.

D 6.4: Report on learning session II
Public Page 19 of 89 V 1.0/ 21 Dicember 2017
When is it going to be implemented?
During 2017
Where is it going to be implemented?
In all organisations taking part in the program.
How long will it take to implement the change?
12 months
What resources are needed for implementation?
Creation of a working team including actors from both care levels as well as social workers.
What is the expected outcome? Change aims
Define a review procedure of care plans for patients with multiple comorbidities to address their changing needs.
4.2.3 Reconciliation of the care plan
QUESTIONS DESCRIPTION
Which change is going to be implemented?
Ensure the reconciled personalised care plan is available in the electronic health records for all professionals 24/7.
When is it going to be implemented?
During 2017
Where is it going to be implemented?
In all Osakidetza organisations.
How long will it take to implement the change?
12 months
What resources are needed for implementation?
Osakidetza's Central Services, along with the IT and clinical advisory teams will define and produce the tool to reconcile and personalise care plans.
What is the expected outcome? Change aims
Access to the reconciled personalised care plan from the electronic health record.
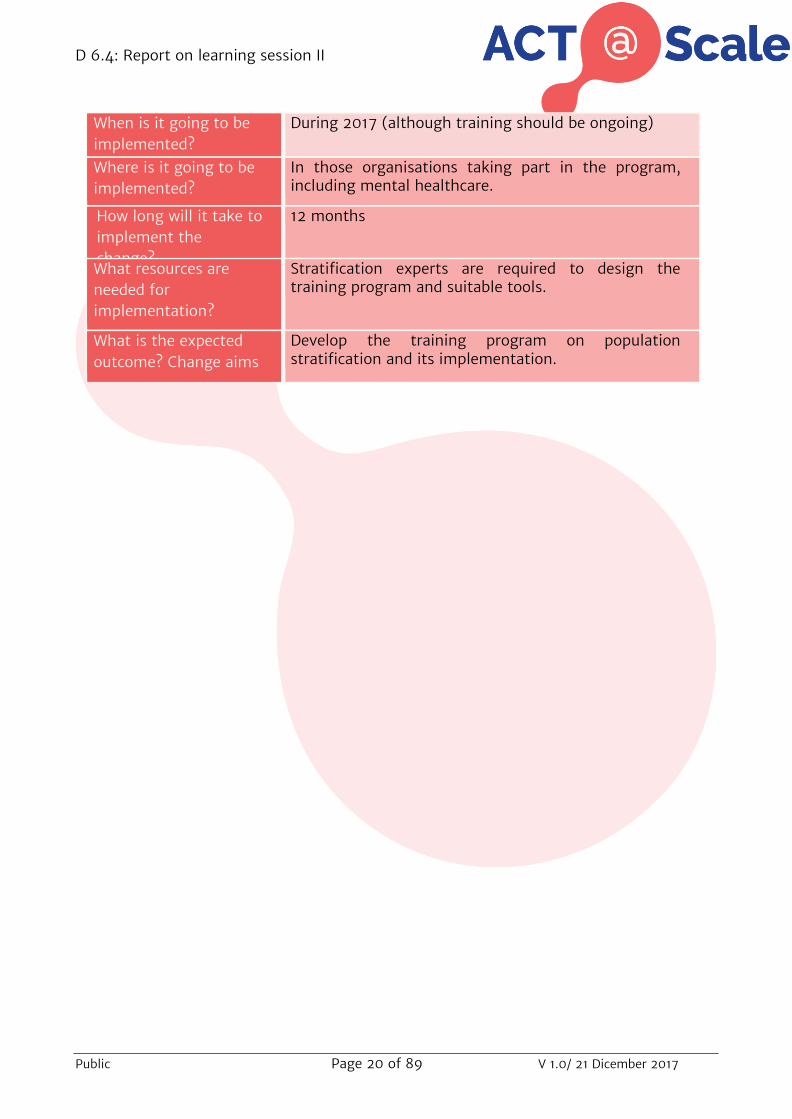
3.2.4 Training on stratification
QUESTIONS DESCRIPTION
Which change is going to be implemented?
Prepare, plan and provide training sessions (online and face-to-face) for professionals to explain the theory supporting population stratification, its methodology and application in Osakidetza.
To do so, training contents must be defined.
D 6.4: Report on learning session II
Public Page 20 of 89 V 1.0/ 21 Dicember 2017
When is it going to be implemented?
During 2017 (although training should be ongoing)
Where is it going to be implemented?
In those organisations taking part in the program, including mental healthcare.
How long will it take to implement the change?
12 months
What resources are needed for implementation?
Stratification experts are required to design the training program and suitable tools.
What is the expected outcome? Change aims
Develop the training program on population stratification and its implementation.

D 6.4: Report on learning session II
Public Page 21 of 89 V 1.0/ 21 Dicember 2017
4.2.5 Data collected QUESTIONS DESCRIPTION
What data do we need to collect?
-Gender
-No of comorbidities
-Mortality
-No of hospital admissions
-Days of hospitalization
-No of readmissions within 30 days
-No Contact with GP
-No of contacts with specialists
-No ofcontacts with specialist nurses
-No of emergency department visits
Who will collect the data?
GPs
Primary Care nyrsing
Internists
Hopsital nursing
eHealth centre nursing
When will the data be collected?
Real time data collection
How will the data be collected?
Data is registered and visualized in the Electronic Health record. The Osakidetza Business Intelligence engine extracts the data for further analysis

D 6.4: Report on learning session II
Public Page 22 of 89 V 1.0/ 21 Dicember 2017
4.3 Telemonitoring services for Congestive Heart Failure (CHF)- Basque Country
4.3.1 Patient Identification
QUESTIONS DESCRIPTION
Which change is going to be implemented?
Establish criteria to identify unstable patients who may benefit from intensive care.
When is it going to be implemented?
During the first half of 2017.
Where is it going to be implemented?
It will be implemented in organisations where the program is being deployed (ICO Bilbao Basurto).
How long will it take to implement the change?
The change will require at least 6 months.
What resources are needed for implementation?
A team made up of healthcare professionals (cardiologists, nursing, primary care, central healthcare directorate, eHealth centre) of participating organisations will assess the criteria.
What is the expected outcome? Change aims
The definition of criteria differentiating patients who may benefit more from telemonitoring will enable the program to achieve better health results and increase user satisfaction.
4.3.2 Care Plan QUESTIONS DESCRIPTION
Which change is going to be implemented?
Provide the necessary resources (technological tools, clinic guidelines, training) and create reconciled and personalised care plans (including patient and carer viewpoints) accessible for all professionals.
When is it going to be implemented?
Although work to achieve this change will begin at the start of 2017, due to the complexity of this activity, implementation may be delayed until the end of the same year.
Where is it going to be implemented?
In participating ICOs (Bilbao Basurto).
How long will it take to implement the change?
Change implementation may be extended to the end of 2017.
What resources are needed for implementation?
Teams made up of healthcare professionals along with IT technicians, shall work together to make reconciled plans accessible from medical records.

D 6.4: Report on learning session II
Public Page 23 of 89 V 1.0/ 21 Dicember 2017
What is the expected outcome? Change aims
Care plans are expected to be agreed by all professionals who treat telemonitoring patients and be available from medical records.
4.3.3 Monitoring services
QUESTIONS DESCRIPTION
Which change is going to be implemented?
Define and agree the criteria to provide patients with the monitoring service (telemonitoring, Personal Health Folder, follow-up by phone) most suitable for their skills and illness stage.
When is it going to be implemented?
During the first half of 2017.
Where is it going to be implemented?
In ICO Bilbao Basurto, which is the organisations currently deploying the program.
How long will it take to implement the change?
The first six months in 2017.
What resources are needed for implementation?
The team of health professionals, ehealtyh Centre, managers and Central Healthcare Directorate will work together to establish the criteria and portfolio of monitoring services.
What is the expected outcome? Change aims
The types of monitoring are expected to be provided according to patient´s profiles.
4.3.4 Data collected
QUESTIONS DESCRIPTION
What data do we need to collect?
-Gender
-Bpdy Mass Index (Kg/m2 )
-Systolic blood pressure (mmHg)
-Diastolic blood pressure (mmHg)
-No of comorbidities
-Mortality
-No of hospital admissions
-Days of hospitatlization
-No of readmissions within 30 days
D 6.4: Report on learning session II
Public Page 24 of 89 V 1.0/ 21 Dicember 2017
-No of contacts with GP
-No of contacts with specialists
-No of contacts with specialist nurses
-No of emergency department visits
Who will collect the data?
GPs
Primary Care nurses
eHealth centre
Cardiologists
Hospital nurses
When will the data be collected?
Real time data collection
How will the data be collected?
Data is registered and visualized in the Electronic Health Record. The Osakidetza Business Intelligence engine extracts the data for further analysis

D 6.4: Report on learning session II
Public Page 25 of 89 V 1.0/ 21 Dicember 2017
4.4 Support of Complex case Managment (AIBSE-CCP)- Catalonia
4.4.1 Changes QUESTIONS DESCRIPTION
Which change is going to be implemented?
The interventions/changes to be carried out have to be defined: develop specific ideas for changes that lead to scaling up within the selected drivers in each good practice; agree on interventions; and document the “change package”. They will be further refined once the first PDSA cycle starts.
Specific interventions for large scale deployment of all the concepts indicated above are described in the core manuscript and on-line supplementary material recently submitted to npj Primary Care Respiratory Medicine under the title Regional Implementation of Community-based Collaborative Management of Complex Chronic Patients.
When is it going to be implemented?
From December 16’ to may 17’
Where is it going to be implemented?
Support of Complex Case Management Program
How long will it take to implement the change?
6 MONTHS
What resources are needed for implementation?
Care professionals (general practitioners, nurses, and social workers), specialists (doctors, allied health professionals), technologists, patients and caregivers.

D 6.4: Report on learning session II
Public Page 26 of 89 V 1.0/ 21 Dicember 2017
What is the expected outcome? Change aims
1. Enhanced clinical risk assessment and stratification
-Evaluation of the potential of the population-based health risk assessment tool in Catalunya (GMA, Adjusted Morbidity Groups) to enhance clinical risk prediction.
-Generation and evaluation of dynamic risk predictive modelling for stratification of patients included in the home hospitalization program.
-Generation and evaluation dynamic risk predictive modelling for enhanced transitional care and long-term community-based management of chronic patients.
2. Service refinement
-To expand and refine the current home-hospitalization program assessing its potential for regional scalability at health system level.
-To design enhanced transitional care services bridging hospital and community.
-Further refine current long-term community-based management of complex chronic patients (CCP) to overcome current limitations for generalization reported in Hernandez C et al (NPJ Prim Care Respir Med. 2015 Apr 9;25:15022).
3. Structured service workflow definition using a collaborative & adaptive case management (ACM) approach
-To define workflows for the above services following a collaborative & adaptive case management approach, as reporter in Cano I et al. J Biomed Inform. 2015 Jun;55:11-22 further elaborated below.
4. Development and implementation of an open ACM platform aligned with the regional interoperability program (IS3).
-To develop and validate an open collaborative & ACM platform on top of existing health information systems (SAP and eCAP) and aligned with the current regional interoperability logistics.

D 6.4: Report on learning session II
Public Page 27 of 89 V 1.0/ 21 Dicember 2017
-To elaborate a roadmap assessing convergence of current ICT-supported integrated care initiatives into the collaborative ACM platform alluded to above.
5. Transformation of the current personal health folder (La Meva Salut®)into a collaborative tool supporting patient self-management integrated with the regional interoperability program (IS3).
-Implementation and evaluation of the enhanced version of La Meva Salut® as tool fostering: i) collaboration between patient and professionals; ii) empowering for self-management; and, iii) materializing the concept of Digital Health Framework reported in Cano I et al J Transl Med. 2014 Nov 28;12 Suppl 2:S10. doi: 10.1186/1479-5876-12-S2-S10.
4.4.2 Data collected QUESTIONS DESCRIPTION
What data do we need to collect?
Assessment:
1. Characteristics of the target population;
2. Intermediate outcomes indicating adequacy of utilization;
3. Process indicators life styles and empowerment;
4. Structured indicators: integrated care (11 indicators suggested by AQuAS)
Multi-criteria Decision Analysis:
1.Changes in the process of care delivery;
2. Changes in patient lifestyle;
3. Changes in Biomedical, Physiological and Health Outcomes;
4. Changes in Health-related quality of life;
5. Changes in final health outcomes, assessing related costs
D 6.4: Report on learning session II
Public Page 28 of 89 V 1.0/ 21 Dicember 2017
Who will collect the data?
Methodological Staff
Technology experts
When will the data be collected?
From February to April
How will the data be collected?
Information System

D 6.4: Report on learning session II
Public Page 29 of 89 V 1.0/ 21 Dicember 2017
4.5 Integrate Care for Subacute and frail Older Adults (PSPV) - Catalonia
4.5.1 Changes
QUESTIONS DESCRIPTION
Which change is going to be implemented?
Stratification of patients at higher risk of early readmission. To improve the stratification, we will evaluate risk factors for early readmission such as; comorbidity, number of prescription drugs and social risk. We will test existing tools (for instance Identification of Seniors At Risk (ISAR) tool, the MultiPrognostic Index (MPI) tool, the LACE score if feasible etc), and create a new tool if necessary.
When is it going to be implemented?
From December 16’ to April 17’
Where is it going to be implemented?
Integrated Care for sub acute and frail older adults
How long will it take to implement the change?
5 MONTHS
What resources are needed for implementation?
-Experts: attending physician in the resource, and researcher on transitions of care
-Core team:
- Decision makers
- Project Manager and representative (being a single institution this is the person)
- Implementers: physician, nursing team, Physical therapist, Social Worker, and Transitional coachers
It Will be carried out by a “transition coach”, which will be a nurse with 40-50 hours training, and who will work in collaboration with the physicians, social workers and physical therapists.

D 6.4: Report on learning session II
Public Page 30 of 89 V 1.0/ 21 Dicember 2017
What is the expected outcome? Change aims
To implement a validated model to identify risk factors of early readmission, after testing different existing indicators.
In parallel, we will develop an original proposal to study predictors of readmissions, and a new tool, based on the available data of the patients in the unit
4.5.2 Data collected
QUESTIONS DESCRIPTION
What data do we need to collect?
-Readmission rate and in the first 7, 30 and 90 days post-discharge.
-Days spent at home in the first 30 and 90 days.
-Transition to a long-term care facility or nursing home, in the following 3 to 6 months.
-Physical function at 30 days post-discharge.
-Adherence to medication and physical activity (process indicators).
-Evaluation of patient experience through questionnaires and individualized interviews, taking into account patients goals.
-Costs of the intervention and cost-effectiveness, compared to standard care.
Who will collect the data?
Nursing Program Team
Physician Program Team
Physical therapist Team
Social Worker Team
Methodological Staff
When will the data be collected?
From February to April
How will the data be collected?
Information System
D 6.4: Report on learning session II
Public Page 31 of 89 V 1.0/ 21 Dicember 2017
4.6 Collaborative Self-Management services to promote healthy life style: Physical Activity (AIBSE-PA) - Catalonia
4.6.1 Changes QUESTIONS DESCRIPTION
Which change is going to be implemented?
The protocol uses a population-health approach to addresses the four aims: Firstly, implementation of collaborative self-management services designed to promote PA in three study groups representative of different layers of the population-based risk stratification pyramid[21], namely: (i) Prehabilitation for high risk candidates to major surgery; (ii) Community-based rehabilitation for clinical stable chronic patients with moderate to severe disease; and, (iii) Promotion of physical activity and healthy lifestyles for citizens at risk and patients with mild disease. The second aim is adaptation and assessment of information and communication technologies (ICT) as supporting tools for both patients and professionals. Thirdly, the program evaluates the impact of each PA in terms of cost-effectiveness. Finally, the current study will generate a roadmap for regional adoption of the PA services.
When is it going to be implemented?
From december 16’ to may 17’
Where is it going to be implemented?
Collaborative self-management services to promote physical activity
How long will it take to implement the change?
6 MONTHS
What resources are needed for implementation?
Collaborative self-management services promoting physical activity across health-care tiers. Deployment of three use cases in one of the healthcare sectors of the city of Barcelona will target cardiovascular disorders (CVD), chronic obstructive
D 6.4: Report on learning session II
Public Page 32 of 89 V 1.0/ 21 Dicember 2017
pulmonary disease (COPD) and type 2 diabetes mellitus (T2DM). A patient-centered approach will be adopted. ICT stands for information and communication technologies.
What is the expected outcome?
Change aims
1. Enhanced clinical risk assessment and stratification
-Evaluation of the potential of the population-based health risk assessment tool in Catalunya (GMA, Adjusted Morbidity Groups) to enhance clinical risk prediction.
-Generation and evaluation of dynamic risk predictive modeling for stratification of patients included in the pre-habilitation program.
2. Service refinement
-To expand and refine the current pre-habilitation program assessing its potential for regional scalability at health system level.
-To launch community-based services to promote physical activity in chronic patients.
3. Structured service workflow definition using a collaborative & adaptive case management (ACM) approach
-To define workflows for the above services following a collaborative & adaptive case management approach, as reporter in Cano I et al. J Biomed Inform. 2015 Jun;55:11-22.
4. Development and implementation of an open ACM platform aligned with the regional interoperability program (IS3).
-To develop and validate an open collaborative & ACM platform on top of existing health information systems (SAP and eCAP) and aligned with the current regional interoperability logistics.
-To elaborate a roadmap assessing convergence of current ICT-supported integrated care initiatives into the collaborative ACM platform alluded to above.
5. Transformation of the current personal health folder (La Meva Salut®)into a collaborative tool supporting patient self-management integrated with the regional
D 6.4: Report on learning session II
Public Page 33 of 89 V 1.0/ 21 Dicember 2017
interoperability program (IS3).
-Implementation and evaluation of the enhanced version of La Meva Salut® as tool fostering: i) collaboration between patient and professionals; ii) empowering for self-management; and, iii) materializing the concept of Digital Health Framework reported in Cano I et al J Transl Med. 2014 Nov 28;12 Suppl 2:S10. doi: 10.1186/1479-5876-12-S2-S10
4.6.2 Data collected
QUESTIONS DESCRIPTION
What data do we need to collect?
The PA program assessment will include: (i) Evaluation of the rollout of each of the three implementation studies (Sections 1S to 3S); and, (ii) Long-term assessment of the entire program beyond the two-year lifespan of the protocol.
Who will collect the data?
Methodological Staff
Technology experts
When will the data be collected?
From February to April
How will the data be collected?
Information System
D 6.4: Report on learning session II
Public Page 34 of 89 V 1.0/ 21 Dicember 2017
5. DO phase 5.1 Introduction DO phase is the second step of the learning cycle in which the planned actions are tested and observations are documented. The timeframe for this phase was from January 2017 to June 2017. During this phase each program has organized meetings with the multidisciplinary teams according to their availability and the needs detected form the implementation point of view. The process of change implementation fro each program is described below.
5.2 Multimorbid population integrated intervention -Basque Country
5.2.1 Roles
QUESTIONS DESCRIPTION
Were the changes implemented?
Explain how and describe if any problems or unexpected finding appeared /arose
The necessary roles of the integrated pathway have been described. The actors performing those roles in each organisation (adapted to each organisation) have been defined.In detail: The primary care team (GP, GP practice nurses and case managers) is the reference for patients with multiple comorbidities and is responsible for the care plan monitoring. Internal medicine, hospital nursing and home-based hospitalisation staff are in charge of patient´s monitoring during the hospitalization and are in close contact with the PC team at hospital discharge.
Was the implementation done according to the scheduled time?
Explain how and describe if any problems or unexpected finding appeared /arose
According to “PLAN”: during 2017
Was the implementation area respected?
Explain how and
Yes, in all organisations taking part in the program (12 Integrated Care Organizations- ICOs).

D 6.4: Report on learning session II
Public Page 35 of 89 V 1.0/ 21 Dicember 2017
describe if any problems or unexpected finding appeared /arose
How long did the change take to implement?
Explain how and describe if any problems or unexpected finding appeared /arose
According to “PLAN”: 12 months
Were the resources implemented accordingly with need?
Explain how and describe if any problems or unexpected finding appeared /arose
A working team, where all organisations are represented, has been created.
Were the objectives of the changes respected?
Explain how and describe if any problems or unexpected finding appeared /arose
Yes, the team has agreed on the definition of roles needed in the provision of care for multimorbid patients
0-25% 25-50% 50-75% 75-100%
Implementation progress
x
5.2.2. Carer's plan review
QUESTIONS DESCRIPTION
Were the changes implemented?
Explain how and describe if any problems
The procedure for periodical review of reconciled care plans as well their adaptation to the changing needs of patients is being defined. The content of the care plan and the actors who access to it have been agreed. Now, the working group is focused on the

D 6.4: Report on learning session II
Public Page 36 of 89 V 1.0/ 21 Dicember 2017
or unexpected finding appeared /arose
semi-automatic development of the personalized care plan based on clinical guidelines and professionals´ criteria.
Was the implementation done according to the scheduled time?
Explain how and describe if any problems or unexpected finding appeared /arose
During 2017 the content of the care plans have been defined. During the 2018 the development of the platforms to create personalized care plans will be finished.
Was the implementation area respected?
Explain how and describe if any problems or unexpected finding appeared /arose
The platform, which enables the creation and monitoring of personalized care plans for multimorbid patients, will be implementated and piloted in 4 out of the 12 organizations involved in the program.
How long did the change take to implement?
Explain how and describe if any problems or unexpected finding appeared /arose
It will required 18 months, 6 months more than expected.
Were the resources implemented accordingly with need?
Explain how and describe if any problems or unexpected finding appeared /arose
Creation of a working team including healthcareactors from both care levels who are responsible for multimorbid patients and It technicians as well.
Were the objectives of the changes respected?
Explain how and describe if any problems or unexpected finding
The content of the care plans and who has access to it have been established. However, the procedure for periodical review is not defined yet. We expect to have the protocol agreed by mid 2018.

D 6.4: Report on learning session II
Public Page 37 of 89 V 1.0/ 21 Dicember 2017
appeared /arose
0-25% 25-50% 50-75% 75-100%
Implementation progress
x
5.2.3 Reconciliation of the care plan QUESTIONS DESCRIPTION
Were the changes implemented?
Explain how and describe if any problems or unexpected finding appeared /arose
The content of the care plan has been defined. Additionally, the algorithms based on the clinical guidelines that enable the reconciliation of multiple care plans have been created. Now, the working team is estableshing the platform which will allow the semi-automatic development of personalized care plans and will make them available though the Electronic Health Record.
Was the implementation done according to the scheduled time?
Explain how and describe if any problems or unexpected finding appeared /arose
During 2017 the content of the care plans have been defined. During the 2018 the development of the platforms to create personalized care plans will be finished.
Was the implementation area respected?
Explain how and describe if any problems or unexpected finding appeared /arose
The platform, which enables the creation and monitoring of personalized care plans for multimorbid patients, will be implementated and piloted in 4 out of the 12 organizations involved in the program.
How long did the It will required 18 months, 6 months more than

D 6.4: Report on learning session II
Public Page 38 of 89 V 1.0/ 21 Dicember 2017
change take to implement?
Explain how and describe if any problems or unexpected finding appeared /arose
expected.
Were the resources implemented accordingly with need?
Explain how and describe if any problems or unexpected finding appeared /arose
Osakidetza's Central Services, the IT department and clinical advisory teams are responsible for the definition, productions and piloting of the platform for reconciled and personalised care plans for multimorbid patients.
Were the objectives of the changes respected?
Explain how and describe if any problems or unexpected finding appeared /arose
The objetive is still the initial one, access to the reconciled and personalised care plan by professionals though the Electronic Health Record.
0-25% 25-50% 50-75% 75-100%
Implementation progress
x
5.2.4 Training on stratification QUESTIONS DESCRIPTION
Were the changes implemented? Explain how and describe if any problems or unexpected finding appeared /arose
Existing materials for the training on population based stratification (theory, methodology and application) have been reviewed. It has been agreed that new content will be added to update and complement the sessions. In next months the training course will be finalized and provided to professionals, probably only online (Osakidetza´s training platform).
D 6.4: Report on learning session II
Public Page 39 of 89 V 1.0/ 21 Dicember 2017
Was the implementation done according to the scheduled time?
Explain how and describe if any problems or unexpected finding appeared /arose
The training course will be available for professionals for mid 2018.
Was the implementation area respected?
Explain how and describe if any problems or unexpected finding appeared /arose
The training will be availbale for all professionals of Osakdietza.
How long did the change take to implement?
Explain how and describe if any problems or unexpected finding appeared /arose
The implementation of the change will require 18 months, 6 month more than planned.
Were the resources implemented accordingly with need?
Explain how and describe if any problems or unexpected finding appeared /arose
Stratification experts and staff from the Osakidetza Training Department required for the design the training program are on board.
Were the objectives of the changes respected?
Explain how and describe if any problems or unexpected finding appeared /arose
The objective is fully respected: develop and implement the training program on population based stratification
0-25% 25-50% 50-75% 75-100%
Implementation progress
x
D 6.4: Report on learning session II
Public Page 40 of 89 V 1.0/ 21 Dicember 2017
D 6.4: Report on learning session II
Public Page 41 of 89 V 1.0/ 21 Dicember 2017
5.3 Telemonitoring services for Congestive Heart Failure (CHF) - Basque Country
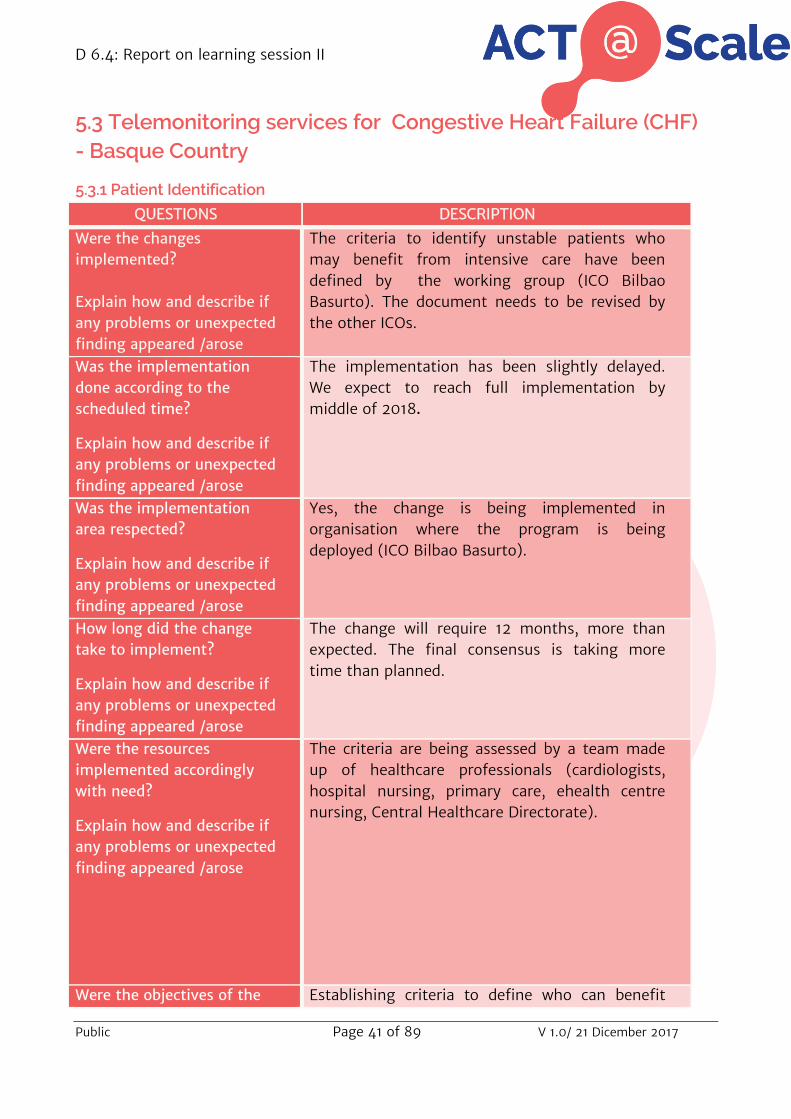
5.3.1 Patient Identification
QUESTIONS DESCRIPTION
Were the changes implemented? Explain how and describe if any problems or unexpected finding appeared /arose
The criteria to identify unstable patients who may benefit from intensive care have been defined by the working group (ICO Bilbao Basurto). The document needs to be revised by the other ICOs.
Was the implementation done according to the scheduled time?
Explain how and describe if any problems or unexpected finding appeared /arose
The implementation has been slightly delayed. We expect to reach full implementation by middle of 2018.
Was the implementation area respected?
Explain how and describe if any problems or unexpected finding appeared /arose
Yes, the change is being implemented in organisation where the program is being deployed (ICO Bilbao Basurto).
How long did the change take to implement?
Explain how and describe if any problems or unexpected finding appeared /arose
The change will require 12 months, more than expected. The final consensus is taking more time than planned.
Were the resources implemented accordingly with need?
Explain how and describe if any problems or unexpected finding appeared /arose
The criteria are being assessed by a team made up of healthcare professionals (cardiologists, hospital nursing, primary care, ehealth centre nursing, Central Healthcare Directorate).
Were the objectives of the Establishing criteria to define who can benefit

D 6.4: Report on learning session II
Public Page 42 of 89 V 1.0/ 21 Dicember 2017
changes respected?
Explain how and describe if any problems or unexpected finding appeared /arose
more from Tele CHF might result in better health outcomes and increased user´s satisfaction .
0-25% 25-50% 50-75% 75-100%
Implementation progress
x
5.3.2 Care Plan QUESTIONS DESCRIPTION
Were the changes implemented? Explain how and describe if any problems or unexpected finding appeared /arose
The Tele CHF program is being created in a specific section of the Electronic Health Record, the so-called Program Management System which is based on procedures and clinical guidelines. The program will include the activities to be perfomed by specific actors when caring of remotely CHF patients. This program, accessible by all professionals, has been successfully piloted; however the full implementation is still pending.
Was the implementation done according to the scheduled time?
Explain how and describe if any problems or unexpected finding appeared /arose
Due to the complexity of the development of the Program Management System and the program istself, the implementation has been delayed.
Was the implementation area respected?
Explain how and describe if any problems or unexpected finding appeared /arose
In the organizations where the Tele CHF is being deployed (ICO Bilbao Basurto).
How long did the change take to implement?
Explain how and
The implementation is expected to be finalized by mid 2018.

D 6.4: Report on learning session II
Public Page 43 of 89 V 1.0/ 21 Dicember 2017
describe if any problems or unexpected finding appeared /arose
Were the resources implemented accordingly with need?
Explain how and describe if any problems or unexpected finding appeared /arose
Teams, made up of healthcare professionals along with IT technicians, are working together to make the Tele CHF program available via the Electronic Health Record.
Were the objectives of the changes respected?
Explain how and describe if any problems or unexpected finding appeared /arose
The Tele CHF program will be agreed by all professionals responsible for patients with CHF and will be available through the Electronic Health Record.
0-25% 25-50% 50-75% 75-100%
Implementation progress
x
5.3.3 Monitoring services QUESTIONS DESCRIPTION
Where the changes implemented? Explain how and describe if any problems or unexpected finding appeared /arose
The criteria defining which monitoring service are the most appropriate ones for each patient have beenestablished. The monitoring service portfolio includes telemonitoring, Personal Health Folder and follow-up by phone. The document needs to be revised by the other ICOs.
Was the implementation done according to the scheduled time?
Explain how and describe if any problems or unexpected finding appeared /arose
The change will be fully implemented by middle of 2018.

D 6.4: Report on learning session II
Public Page 44 of 89 V 1.0/ 21 Dicember 2017
Was the implementation area respected?
Explain how and describe if any problems or unexpected finding appeared /arose
Yes, in the organization where the TeleCHF is being deployed (ICO Bilbao-Basurto)
How long did the change take to implement?
Explain how and describe if any problems or unexpected finding appeared /arose
In ICO Bilabao-Basurto the implementation will be finalized by end 2017, 6 months more than planned.
Were the resources implemented accordingly with need?
Explain how and describe if any problems or unexpected finding appeared /arose
Teams, made up of healthcare professionals and Central Healthcare Directorate representatives, are working together to define the criteria.
Were the objectives of the changes respected?
Explain how and describe if any problems or unexpected finding appeared /arose
Provision of the most appropriate monitoring service according to patient´s profile.
0-25% 25-50% 50-75% 75-100%
Implementation progress
x

D 6.4: Report on learning session II
Public Page 45 of 89 V 1.0/ 21 Dicember 2017
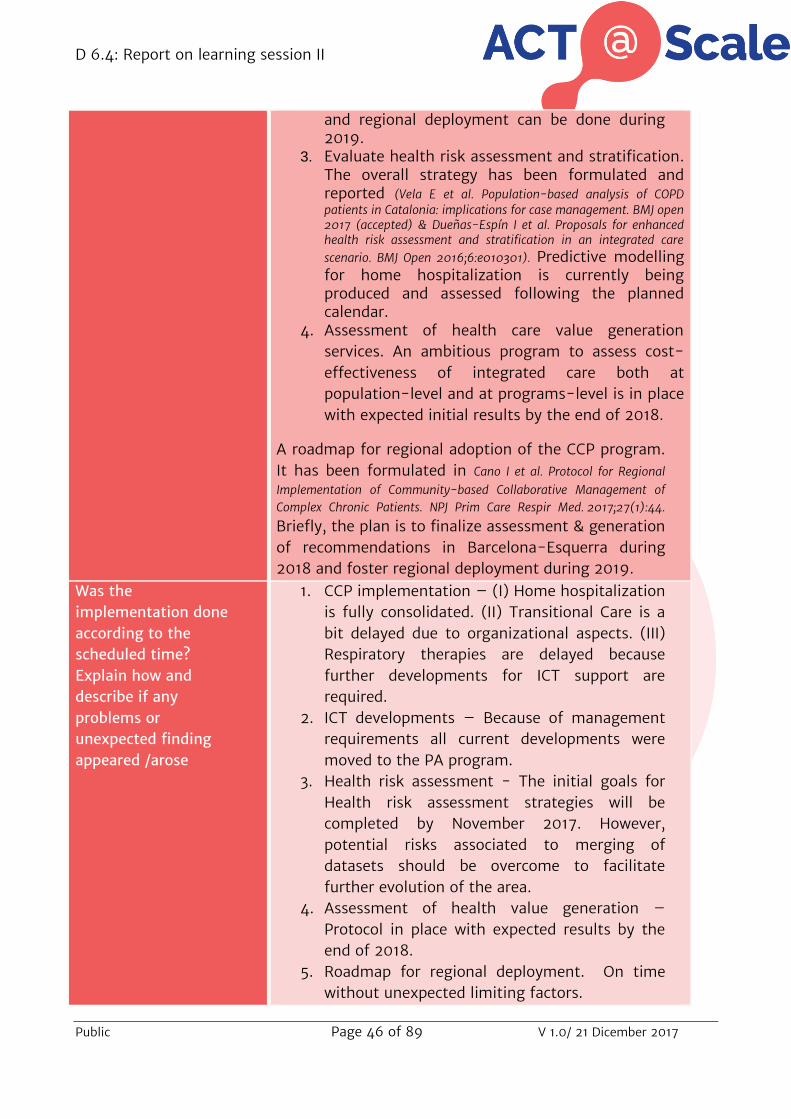
5.4 Support of Complex case Management (AIBSE-CCP) – Catalonia
QUESTIONS DESCRIPTION Where the changes implemented? Explain how and describe if any problems or unexpected finding appeared /arose
1. Implement the CCP protocol: The characteristics and implementation strategies are described in detail in Cano I et al. Protocol for Regional Implementation of Community-based Collaborative Management of Complex Chronic Patients. NPJ Prim Care Respir Med. 2017;27(1):44. Briefly, (I) Home hospitalization has been consolidated and expanded (from 12 beds per day to 36 beds per day, as initially planned. (II) Redesign of the transitional care program addressing home-based patients requiring specialized care is being conducted through two parallel strategies: (i) the ongoing reform of specialized care in the community; and, (ii) an observational study assessing characteristics and requirements of candidates to transitional care to be completed by Fall 2018. Finally, (III) the Long-term oxygen therapy (LTOT) clinic has been implemented within the Pneumology Department during 2017, as part of the reform of specialized care in the community. But, a new integrated care program on respiratory therapies encompassing: (i) LTOT; (ii) Sleep problems; and, (iii) Home ventilation should be designed on Spring 2018 to assess its potential implementation during 2019. This program on respiratory therapies is conceived as a use case to assess the potential of collaborative work across healthcare tiers.
2. Adoption of information and communication technologies. Two main actions are being addressed: (i) Transformation of the current regional personal health folder (La Meva Salut) into a self-management system (SMS); and, (ii) Development of a smart adaptive case management (SACM) platform build-up on top of current Health Information System. Because of organizational issues, the two ICT interventions have been moved to the Physical Activity program (PA). The calendar is to achieve implementation and assessment within PA during 2018 such that generalization to CCP
D 6.4: Report on learning session II
Public Page 46 of 89 V 1.0/ 21 Dicember 2017
and regional deployment can be done during 2019.
3. Evaluate health risk assessment and stratification. The overall strategy has been formulated and reported (Vela E et al. Population-based analysis of COPD patients in Catalonia: implications for case management. BMJ open 2017 (accepted) & Dueñas-Espín I et al. Proposals for enhanced health risk assessment and stratification in an integrated care scenario. BMJ Open 2016;6:e010301). Predictive modelling for home hospitalization is currently being produced and assessed following the planned calendar.
4. Assessment of health care value generation services. An ambitious program to assess cost-effectiveness of integrated care both at population-level and at programs-level is in place with expected initial results by the end of 2018.
A roadmap for regional adoption of the CCP program. It has been formulated in Cano I et al. Protocol for Regional Implementation of Community-based Collaborative Management of Complex Chronic Patients. NPJ Prim Care Respir Med. 2017;27(1):44.
Briefly, the plan is to finalize assessment & generation of recommendations in Barcelona-Esquerra during 2018 and foster regional deployment during 2019.
Was the implementation done according to the scheduled time? Explain how and describe if any problems or unexpected finding appeared /arose
1. CCP implementation – (I) Home hospitalization is fully consolidated. (II) Transitional Care is a bit delayed due to organizational aspects. (III) Respiratory therapies are delayed because further developments for ICT support are required.
2. ICT developments – Because of management requirements all current developments were moved to the PA program.
3. Health risk assessment - The initial goals for Health risk assessment strategies will be completed by November 2017. However, potential risks associated to merging of datasets should be overcome to facilitate further evolution of the area.
4. Assessment of health value generation – Protocol in place with expected results by the end of 2018.
5. Roadmap for regional deployment. On time without unexpected limiting factors.

D 6.4: Report on learning session II
Public Page 47 of 89 V 1.0/ 21 Dicember 2017
Was the implementation area respected? Explain how and describe if any problems or unexpected finding appeared /arose
Yes Solving organizational aspects was initially slow. But all aspects were fully solved by Spring 2017. Previously forecasted limiting factors have been
How long did the change take to implement? Explain how and describe if any problems or unexpected finding appeared /arose
Solving organizational aspects took > 6 months Main issue were redistribution of personal, acceptance of the new organigram. No unexpected issues
Were the resources implemented accordingly with need? Explain how and describe if any problems or unexpected finding appeared /arose
Yes, the issue has been solved through negotiations with the public payer - Catsalut
Were the objectives of the changes respected? Explain how and describe if any problems or unexpected finding appeared /arose
Yes, fully respected
0-25% 25-50% 50-75% 75-100%
Implementation progress
x

D 6.4: Report on learning session II
Public Page 48 of 89 V 1.0/ 21 Dicember 2017
5.5 Integrated care for subacute and frail older adults (PSPV) - Catalonia
QUESTIONS DESCRIPTION
Where the changes implemented? Explain how and describe if any problems or unexpected finding appeared /arose
No, we are still in process, in order to identify the patients we are collecting data that will help us identify the patients at risk, this will be a retrospective measurement to be use in patient selection next year according to the results.
Was the implementation done according to the scheduled time? Explain how and describe if any problems or unexpected finding appeared /arose
No, we are in process, collecting data and defining indicators like: 1.Readmission Rate; 2.Days spent at home; 3. Transition to a long-term care facility or nursing home; 4.Cost intervention and cost effectiveness
Was the implementation area respected? Explain how and describe if any problems or unexpected finding appeared /arose
Yes. The implementation is related to identify the risk patients in early readmission and difficult care transition
How long did the change take to implement? Explain how and describe if any problems or unexpected finding appeared /arose
At the moment we are still working on it, data collection up to date by now
Were the resources implemented accordingly with need? Explain how and describe if any problems or unexpected finding appeared /arose
Yes.
D 6.4: Report on learning session II
Public Page 49 of 89 V 1.0/ 21 Dicember 2017
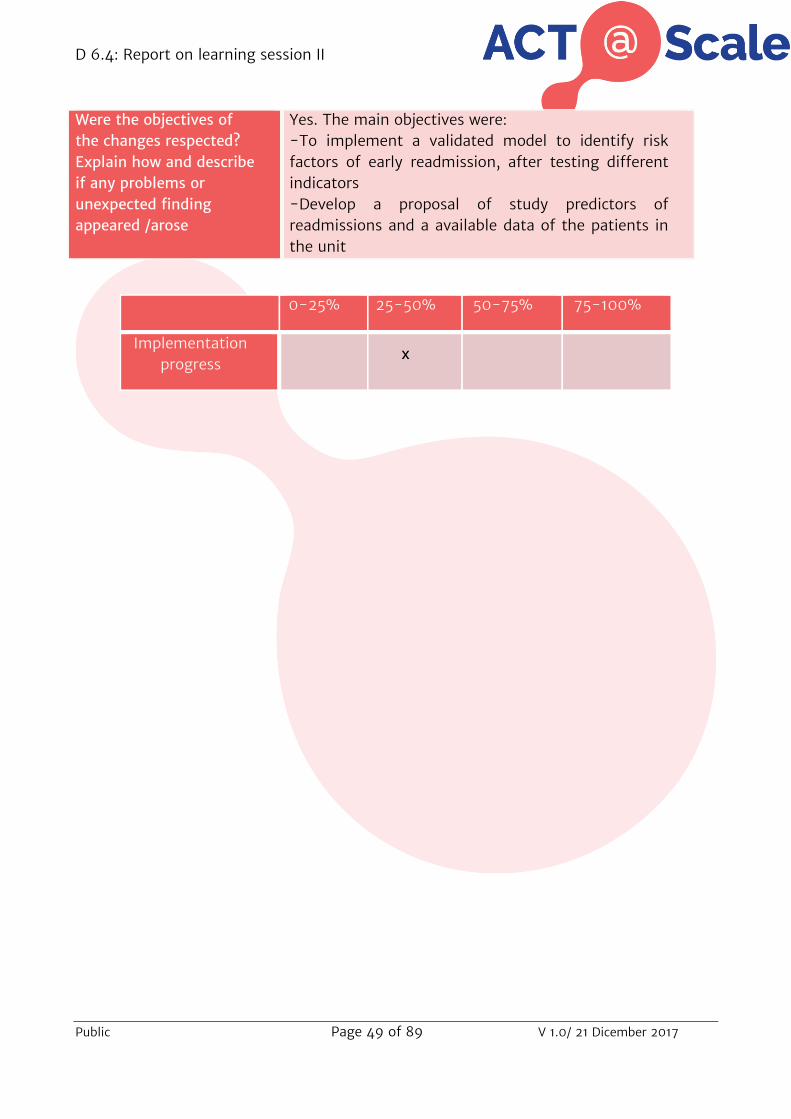
Were the objectives of the changes respected? Explain how and describe if any problems or unexpected finding appeared /arose
Yes. The main objectives were: -To implement a validated model to identify risk factors of early readmission, after testing different indicators -Develop a proposal of study predictors of readmissions and a available data of the patients in the unit
0-25% 25-50% 50-75% 75-100%
Implementation progress
x

D 6.4: Report on learning session II
Public Page 50 of 89 V 1.0/ 21 Dicember 2017
5.6 Collaborative Self-Management services to promote heathly life style: Physical Activity (AIBSE-PA) – Catalonia
QUESTIONS DESCRIPTION Where the changes implemented? Explain how and describe if any problems or unexpected finding appeared /arose
Yes, all changes have been implemented. But, pace of implementation and priorities/strategies have been adapted, as summarized below: 1. The prehabilitation program has been deployed as
planned and it is currently a main stream program in Barcelona-Esquerra and it will likely become a general program in Catalonia
2. The program on rehabilitation of chronic patients has been kept at pilot level because of limitations due to three main factors: i) organizational changes; ii) ICT developments, and, iii) business model issues
3. The program addressed to promotion of physical activity in citizens at risk and mild chronic patients is also kept at pilot level due to identical reasons.
Was the implementation done according to the scheduled time? Explain how and describe if any problems or unexpected finding appeared /arose
Yes for the prehabilitation program. Deployment of the other two programs has been delayed, as explained above. We learnt that we should first achieve full maturity in the prehabilitation program because it contains all the elements needed for the other two programs, as well as for extension of the concept to other healthy lifestyle programs addressing nutrition, addictions and more. Main steps achieved are: a) Demonstration of efficacy of the prehabilitation
program through a RCT (Barberan A et al. Personalised Prehabilitation in High-risk Patients Undergoing Elective Major Abdominal Surgery: A Randomized Blinded Controlled Trial. Ann Surg. 2017 May 9. doi: 10.109) and effectiveness of the program after its generalization as mainstream service at Hospital Clinic. Cost-effectiveness is currently under analysis. The details of the entire plan to be implemented,

D 6.4: Report on learning session II
Public Page 51 of 89 V 1.0/ 21 Dicember 2017
including the three programs alluded to above, are described in the PhD thesis - Deployment of novel integrated care services to promote healthy life styles: physical activity as a use case by Anael Barberan Garcia – to be defended on 20th September 2017.
b) Creation of the preHabilitation Unit at Hospital Clinic presented to the media on March 2017
c) Plan of three workshops (late Sept and Oct 2017) aiming at refining the service design through design thinking strategies. The workshops are jointly promoted by the Health Technology cluster and BCN Design Centre with three main purposes: i) Define regional extension of the program addressing perisurgical care in general; ii) Generalization of the program to the other two initiatives (rehab of chronic patients and citizens at risk); and, iii) Identification of business models to provide sustainability to the entire ACT@Scale initiative.
d) Development of an ICT platform integrated with current healthcare providers to support the service. It is based, in part, in the transformation of the personal health folder into a self-management tool.
e) Redesign of the entire rehabilitation program in the Hospital as well as the role of service providers in the area of Barcelona-Esquerra.
Was the implementation area respected? Explain how and describe if any problems or unexpected finding appeared /arose
The five points (from a) to e) described above summarize the changes introduced as well as the current action plan. In terms of timing, we believe that by mid 2018 all the above aspects will be completed such that the full program should be in place by the end of that year
How long did the change take to implement? Explain how and describe if any problems or unexpected finding appeared /arose
The diagnosis of the need for adapting the deployment plan was done during the first trimester of 2017. The redesign process as well as progressive implementation of the new strategy is being done in a stepwise manner in order to have full implementation of the five items by the end of the current year (2017) and final deployment in one year

D 6.4: Report on learning session II
Public Page 52 of 89 V 1.0/ 21 Dicember 2017
time (end of 2018) Enhanced risk assessment strategies will be implemented during 2018 after proper evaluation of the strategies implemented for complex chronic patients si completed.
Were the resources implemented accordingly with need? Explain how and describe if any problems or unexpected finding appeared /arose
So far, yes. Deployment of the full program (2018) will require additional resources that are currently being explored.
Were the objectives of the changes respected? Explain how and describe if any problems or unexpected finding appeared /arose
Basically yes. The changes in the implementation strategies have been introduced in order to enhance efficiencies and achieve long-term sustainability of the setting
0-25% 25-50% 50-75% 75-100%
Implementation progress
x

D 6.4: Report on learning session II
Public Page 53 of 89 V 1.0/ 21 Dicember 2017
5.7 Summary
Program Intervention Implementation
progress
Multimorbid population integrated intervention
Clear definition of care pathways and roles
75-100%
Care Plan revision 25-50%
Reconciliation of care plans 25-50%
Staff training on stratification tools
25-50%
Telemonitoring services for CHF
Establish criteria to identify candidate patients for telemonitoring
50-75%
Personalized and reconciled care plan
50-75%
Monitoring services according to patient´s profile and needs
50-75%
Support of Complex case management
Service refinement 50-75%
Service and structure workflow 0-25%
Development and implementation of an open adoptive care managment
0-25%
Transformation personal health folder
0-25%
Risk stratification 25-50%
Integrated care for subacute and frail older
adults
Risk assessment Study predicting factor for readmission
25-50%
Service refinement 25-50%
Service and structure workflow 25-50%
Development and implementation of an open adoptive care managment (ACM)
25-50%
Collaborative self-management services to
promote healthy life style: physical activity
Identification of risk factors 25-50%
Study predicting factor for readmission
25-50%

D 6.4: Report on learning session II
Public Page 54 of 89 V 1.0/ 21 Dicember 2017
6. STUDY phase 6.1 Introduction STUDY phase is the third step of the learning cycle. The timeframe for this phase was from June 2017 to September 2017. During this phase each program has organized at least one meeting with the multidisciplinary team to analyse the impact of the changes implemented so far.
Service selection work package defined a set of indicators to track the three domains of the driver: 1) identification and selection of patients; 2) services responding to patient’s needs; and 3) on-boarding the required professionals and services.
Briefly, the indicators are classified into two groups:
Service Selection general indicators (mapping indicators): describe the service selection key elements at population and individual levels. Overall, 31 indicators have been defined.
Service Selection key progress indicators (KPIs): aim to monitor changes through the implementation process and scaling-up on service selection. The 21 ordinal indicators of all the Service Selection general indicators are considered KPIs.
All indicators are described in D6.1.
KPIs are tracked annually across programs which work specifically on service selection driver. Program Managers, who have a deep and extensive knowledge of the programs, had completed two rounds of service selection questionnaire: firstly at baseline (July 2016) and secondly at the end of the STUDY phase (September 2017).
As mentioned in D6.3, among the KPIs, two types can be distinguished according to the elements of the service selection approach studied:
1. Qualitative Indicators: investigate strategy components such as approach, tools and participants involvement, defined as “scope and ambition”.
2. Quantitative Indicators: investigate strategy deployment, utilization and changes such us coverage, frequency of usage and professional numbers, defined as “utilization and coverage”.

D 6.4: Report on learning session II
Public Page 55 of 89 V 1.0/ 21 Dicember 2017
List of KPIs:
Qualitative indicators
Existence of formal risk stratification approach
Patients´identification and selection criteria
Risk stratification access and changes by professionals
Variables taken into account to assess patient's needs
Interventions according to levels of risks
Presence of individualized care plan
Variables taken into account to match specific interventions with patient's needs
Service types that can be activated
Criteria for service dynamic adaptation
Degree of adaptive case management
Level of patient/caregiver involvement in the care plan
Degree of healthcare tiers accessibility to patients care plan
Quantitative indicators
Deployment of risk stratification approach
Re-stratification frequency
Target population included in the program
Frequency of interventions´ revisions to match patient’s needs
Staff evaluation of awareness and actions
Staff trained in identification, evaluation and selection of case
Staff trained in care plan formulation, evaluation, follow-up and adaptation
Training frequency in identification, evaluation and selection of case
Training frequency in care plan formulation, evaluation, follow-up and adaptation
The evolution of the Key Progress Indicators from 2016 to 2017 per program are presented in D6.3. In addition to the description of the progress of both single and composite indicators shown in the deliverable aforementioned, the potential relationship between changes implemented and the score of specific indicators is depicted in the following section.
D 6.4: Report on learning session II
Public Page 56 of 89 V 1.0/ 21 Dicember 2017
6.2 Impact on service selection In order to assess the impact of the improvement changes implemented on the dimensions investigated in service selection driver, the relationship between the information collated in both PLAN and DO phases (sections 4 and 5 of this document) and Program Manager´s survey results (reported in D6.3) is introduced below.

D 6.4: Report on learning session II
Public Page 57 of 89 V 1.0/ 21 Dicember 2017
6.3 Multimorbid population integrated intervention - Basque Country
PLAN DO
(implementation progress)
KPI Results
2016 2017
Describe actors and roles of the integrated care pathway
Roles and actors described and defined (75-100%)
Deployment of risk stratification approach 3 4
Risk stratification access and changes by professionals 3 4
Interventions according to level of risks 3 1
Service type that can be activated 3 4
Define procedure to periodically review care plan and adapt it to patient’s needs
The care plan will be periodically reviewed and adapted to patient’s needs (25-50%)
Variables taken into account to assess patient’s need 1 4 Variables taken into account to match specific intervention with patient’s need
3 4
Frequency of interventions´ revisions to match patient’s needs
2 2
Criteria for service dynamic adaptation 1 1
Degree of adaptive case management 2 2
Ensure the personalised care plan is available in the electronic health records for all professionals 24/7
Content of care plan and accessibility have been set. (25-50%)
Presence of individualized care plan 2 4 Level of patients/caregivers involvement in the care plan 2 4
Degree of healthcare tiers accessibility to patient´s care plan
4 3
Staff evaluation of awareness and actions 1 3 Staff trained in identification, evaluation and selection of case
0 2
Staff trained in care plan formulation, evaluation follow-up and adaptation 0 2
Training frequency in identification, evaluation and selection of case 0 2
Training frequency in care plan formulation, evaluation, follow-up and adaptation
0 1
Table 1

D 6.4: Report on learning session II
Public Page 58 of 89 V 1.0/ 21 Dicember 2017
There are few key performance indicators to which no improvement changes are associated.
KPI Results 2016 2017
Existence of formal risk stratification approach 4 4
Patient´s identification and selection criteria 4 4
Re-stratification approach 1 1
Target population included in the program 4 4
Table 2

D 6.4: Report on learning session II
Public Page 59 of 89 V 1.0/ 21 Dicember 2017
During this first PDSA cycle, the multimorbid patients´ program focused specifically on three interventions:
1. Describe the roles (social and health care) required in the integrated care pathway for multimorbid patients and define the specific actors who will performed these roles in each organization (tailoring of the program)
2. Define and set up a procedure to regularly review the reconciled care plan and adapt it to the patient´s changing needs
3. Make the reconciled and personalized care plans accessible in the Electronic Health Record for all healthcare professionals in a 24x7 basis
According to the results shown on table 1, it can be noted that most indicators have improved.
As a consequence of the final consensus on the roles of the actors involved in the integrated care pathway for multimorbid patients, the risk stratification approach is fully implemented. Initially the multimorbid patients were identified by the stratification tool as target for the program; however, professionals did not include all patients systematically. Now, healthcare professinals have the specific instruction to provide the service to all multimorbid patients marked by the population-based stratification. The new roles allow professionals to modify the multimorbid patient pool based on their clinical judgement as well.
The content of the individualized care plan for multimorbid patients and the accesibility criteria for professionals is already defined. Additionally, how the patient´s assessments and self-management goals will be jointly agreed by healthcare professionals and patients is already drawn. This progress is reflected in the enhanced scores of “Presence of individualized care plan” and “Level of patients/caregivers involvement in the care plan”.
In the future, the personalized care plans for each multimorbid patient will be available in the Electronic Health Record. These plans will be regularly reviewed to ensure that they are adapted to patient´s changing needs. Yet, the current version of the care plan is not automatically updated. Therefore, the indicators related to adaptive case management remain within a range.
By planning and designing the individualized care plans, need for professionals´ training on case selection and care plan formulation has arise. Non-structured training has been provided to some extent but specific actions are required to schedule formal education programs. In line with this, indicators on training show a slight increase.
The vast majority of those indicators that remain constant do not have an improvement action associated, such as the re-stratification frequency and the criteria used to targeting patient with the stratification tool. In fact, these two actions are led

D 6.4: Report on learning session II
Public Page 60 of 89 V 1.0/ 21 Dicember 2017
by the Basque Department of Health, which is not formally included in the project. Thus, having influence in these indicators is beyond our range.

D 6.4: Report on learning session II
Public Page 61 of 89 V 1.0/ 21 Dicember 2017
6.4 Telemonitoring services for congestive heart failure (CHF)-Basque Country
PLAN DO
(implementation progress)
KPI Results
2016 2017
Establish criteria to identify unstable patients
First draft of criteria has been approved (50-75%)
Existence of formal risk stratification approach 2 2
Deployment of risk stratification approach 4 4
Patient´s identification and selection criteria 2 2
Risk stratification access and changes by professionals 3 4
Re-stratification frequency 1 4
Target population included in the program 1 3
Create personalised care plans
Program management system has been piloted and it is accessible to all professionals (50-75%)
Presence of individualised care plan 2 4
Frequency of interventions´ revisions to match patient’s needs
4 4
Criteria for service dynamic adaptation 1 1
Degree of adaptive case management 2 2
Level of patients/caregivers involvement in care plan 2 2
Degree of healthcare tiers accessibility to patients care plan 3 3
Define the criteria to provide patients with the right monitoring service
Criteria defined. Implementation in progress (50-75%)
Variables taken into account to assess patient’s needs 4 4
Interventions according to level of risks 3 3
Variables taken into account to match specific interventions with patient’s needs
4 4
Service type that can be activated 3 4 Table 3

D 6.4: Report on learning session II
Public Page 62 of 89 V 1.0/ 21 Dicember 2017
There are some key performance indicators to which no improvement changes are associated.
KPI Results 2016 2017
Staff evaluation of awareness and actions 1 1
Staff trained in identification, evaluation and selection of case - -
Staff trained in care plan formulation, evaluation, follow-up and adaptation - -
Training frequency in identification, evaluation and selection of case - -
Training frequency in care plan formulation, evaluation, follow-up and adaptation - -
Table 4

D 6.4: Report on learning session II
Public Page 63 of 89 V 1.0/ 21 Dicember 2017
The areas in which the program has been working on during this fisrt PDSA cycle are:
1. Define criteria to identify unstable patients who may benefit from intensive care 2. Make available the resources required (technological tools, clinical guidelines,
training) and create personalized care plans (including patient´s and caregiver´s perspectives) available for all stakeholders
3. Define and agree on the criteria to provide patient and/or caregivers with the monitoring service (telemonitoring, Personal Health Folder, phone-based follow-up) which best fits his/her capacities and disease phase
Target population of the telemonitoring program is identified and selected by an individual stratification approach using rules-based thresholds of certain parameters (diagnosis of CHF and at least one hospital admission in the previous 6 months). Although these inclusion criteria have been used to some extent, clinicians felt the urgency to establish more detailed guidelines to detect unstable patients who may benefit more from the telemonitoring.
During 2017, the multidisciplinary team have drafted the new inclusion criteria for patients candidate to receive telemonitoring services. Today, healthcare professionals are able to re-assess and re-consider whether patients can be included in the program by modifying the risk stratification results based on their clinical judgement (see improved score of “Re-stratification frequency”). The proportion of target population included in the telemonitoring program has significantly increased, partially as a consequence of this better definition of the inclusion criteria.
The further implementation and scaling up of the telemonitoring program mainly depends on the availability of the Program Management System, which allows the creation of individualized care plans. During 2017 the Program Management System has been successfully piloted using the telemonitoring program as use case. As a result, the individualized care plan is in place (“Presence of individualised care plan” scores 4), however, further development is required to ensure that the care plan is adapted to patient´s fluctuating needs. Today the degree of adaptive case management, which is entirely based on clinical criteria, only permits to plan future events and guide the type of interventions offered to telemonitoring patients. Reason why, the indicator “Degree of adaptive case management” remains steady. During the next PDSA cycle, the program will focused its efforts on enhancing the functionalities of the Program Management System, hence the care plan will be constantly updated according to patient´s needs. This improved version of the individualized care plan is expected to include not only the results of patient´s assessments but also self-management goals. All healthcare professionals from primary care and hospital can access the individualized care plan since the Program Management System is already embedded in the Electronic Health Record.

D 6.4: Report on learning session II
Public Page 64 of 89 V 1.0/ 21 Dicember 2017
By defining the criteria to provide patients with the most suitable monitoring service according to their skills and illness stage, the program expects to align the interventions offered with patient´s risk. This improvement change has not been fully achieved, so “Interventions according to level of risk” indicator shows no change.
It is noteworthy the need to provide professionals with training on: (i) case selection and evaluation and (ii) care plan formulation, follow-up and adaptation. Although there are not specific improvement changes focused on these issues, the multidisciplinary team might reflect on the possibility of including them in the second PDSA cycle.

D 6.4: Report on learning session II
Public Page 65 of 89 V 1.0/ 21 Dicember 2017
6.5 Support of Complex case managment (AISBE-CCP) – Catalonia
PLAN DO
(implementation progress)
KPI Results
2016 2017
Enhance clinical risk assessment and stratification
Use of population-based into clinics. Elaboration of predictive modelling (25-50%)
Existence of formal risk stratification approach 2 3
Deployment of risk stratification approach 1 2
Patient’s identification and selection criteria 2 2
Re-stratification frequency 2 3
Variables taken into account to assess patient’s needs
3 4
Interventions according to levels of risk 1 2
Frequency of intervention revisions to match patient needs 3 4
Service refinement Accessility-
Scalability-Metrics (25-50%)
Identified population included, ratio 2 3
Presence of individualized care plan 3 4
Variables taken into account to match specific intervention with patient needs 3 4
Service types that can be activated 2 3
Level of patient/caregiver involvement 2 3
Degree of Health Care tiers access to care plan 2 3
Staff evaluation of awareness and actions 1 3
Structured service workflow definition using a collaborative &
Introduction of a collaborative ACM approach for all
Criteria for service dynamic adaptation 1 3

D 6.4: Report on learning session II
Public Page 66 of 89 V 1.0/ 21 Dicember 2017
adaptive case management (ACM) approach
services (25-50%)
Degree of adaptive case management 1 3
Development and implementation of an open ACM platform aligned with the regional interoperability program (IS3)
ICT developments moved to PA program for strategic reasons (0-25%)
None NA NA
Transformation of the current personal healkth forlder (la Meva Salut ®) into a collaborative tool supporting patient self-managment integrated with the regional interoperability program (IS3)
ICT developments moved to PA program for strategic reasons (0-25%)
None NA NA
Table 5
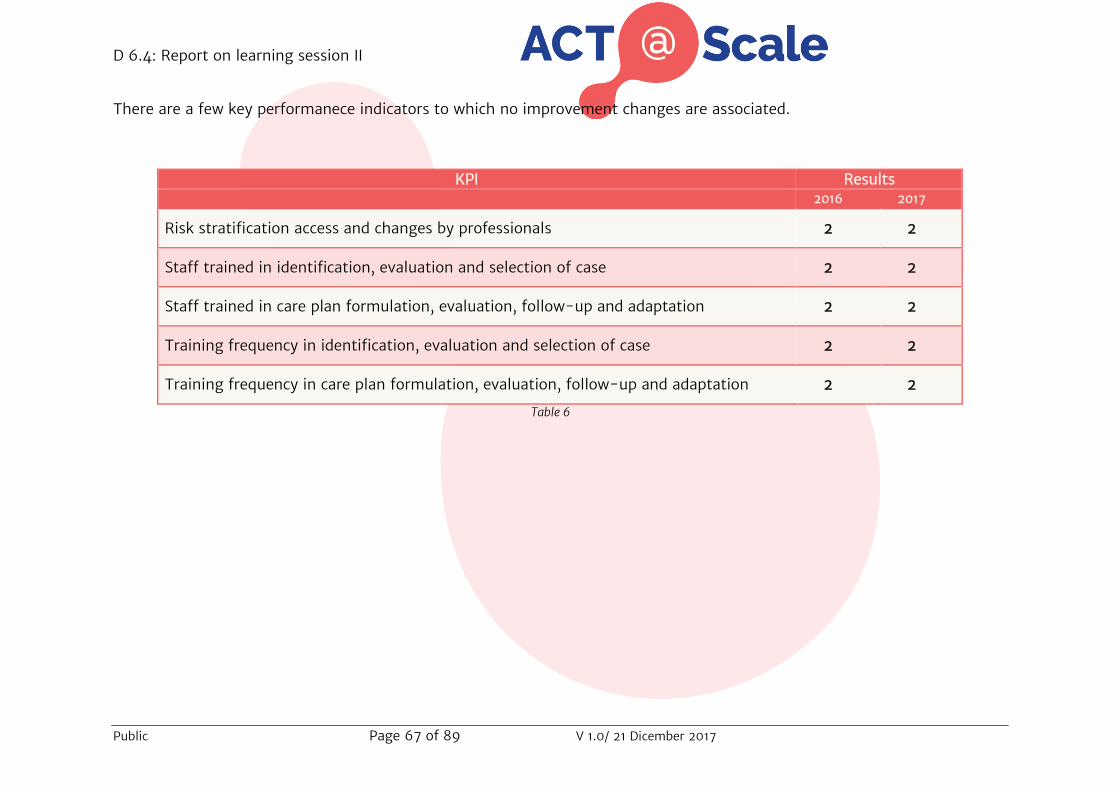
D 6.4: Report on learning session II
Public Page 67 of 89 V 1.0/ 21 Dicember 2017
There are a few key performanece indicators to which no improvement changes are associated.
KPI Results 2016 2017
Risk stratification access and changes by professionals 2 2
Staff trained in identification, evaluation and selection of case 2 2
Staff trained in care plan formulation, evaluation, follow-up and adaptation 2 2
Training frequency in identification, evaluation and selection of case 2 2
Training frequency in care plan formulation, evaluation, follow-up and adaptation 2 2
Table 6

D 6.4: Report on learning session II
Public Page 68 of 89 V 1.0/ 21 Dicember 2017
The program’s interventions to be carried out within service selection were:
1. The implementation of three integrated care interventions for enhanced community-based management of Complex Chronic Patients (CCP) using a collaborative adaptive case management (ACM) approach: i) Consolidation of the Home hospitalization service; ii) Refinement of transitional care services aiming at improving the interplay between specialized care and community-based care; and, iii) Integrated care for patients under respiratory therapies involving: a) long-term oxygen therapy (LTOT); b) Sleep disorders; and, c) Home ventilation
2. The adoption of information and communication technologies (ICT) build-up on top of existing health information systems with two main aims: i) Adaptation of the regional personal health folder (La Meva Salut) to a self-management system (SMS)and, ii) Develop a Smart adaptive case management platform (SACM) to supporting ACM.
3. The evaluation of the impact of enhanced clinical health risk assessment and stratification based on the (Vela E et al. Population-based analysis of COPD patients in Catalonia: implications for case management. BMJ open 2017 (accepted) & Dueñas-Espín I et al. Proposals for enhanced health risk assessment and stratification in an integrated care scenario. BMJ Open 2016;6:e010301).
4. The assessment of healthcare value generation of the services, both during the deployment phase and after regional scale-up of the novel services;
5. The study will generate a roadmap for regional adoption of the CCP program that will be based on the plans described in detail in Cano I et al. Protocol for Regional Implementation of Community-based Collaborative Management of Complex Chronic Patients. NPJ Prim Care Respir Med. 2017;27(1):44.
That five improvement areas have been carefully planned and the bulk of work is quite advanced such that a reasonable estimate is that achievements of the program are within the range 50-75%, despite specific KPIs are behind the overall achievement score. Briefly, we estimate that 75% of the goals will be accomplished by the end of 2018 and full implementation in AISBE, as well as regional implementation of specific areas of the program will be achived during 2019.
The major issues that the program encountered have been: i)Acceptancy of the new organization and new structure; ii) ICT developments; and, iii) Access to different datasets for health risk assessment purposes; iv) Redistribution of responsibilities and resources; and, v) Access to new resources needed for accomplishment of the program.
One major change in the initial program has been that ICT developments associated to: i) Transformation of the regional personal health folder (La Meva Salut) into a self-management system (SMS), as well as ii) Development of the SACM (Smart collaborative Adaptive Case Management) have been moved from the current CCP

D 6.4: Report on learning session II
Public Page 69 of 89 V 1.0/ 21 Dicember 2017
program to the Physical Activity (PA). The reason for the change being that currently the CCP program is mostly based on home hospitalization activities supported by mobile applications of the Hospital health information providing full coverage of the basic needs. Clearly, it is most convenient to develop novel ICT tools as part of the PA program to subsequently transfer them to the CCP program, as planned during the second semester of 2018.
Moreover, we would like to stress that an analysis of the KPI grading reported in D6.3, displayed significant problems due to different factors. Among them: i) Lack of responses to some items in the first evaluation (2016); ii) Poor activation of patients’ questionnaires; and, iii) Inconsistent responses for the evolution of some KPIs between 2016 and 2017 due to suboptimal responses. We strongly suggest to use that grading of KPIs reported in the current CCP table which reflects the consensus scoring of the relevant staff of the program both for 2016 and 2017.

D 6.4: Report on learning session II
Public Page 70 of 89 V 1.0/ 21 Dicember 2017
6.7 Integrated care for subacute and frail older adults , Parc Sanitari Per Virgili (PSPV) - Catalonia
PLAN DO (implementation progress KPI Results 2016 2017
Identification of risk factors
Collecting data and identifying patients in risk Retrospective data collection (Implementation Progress: 25-50%) -
Existence of formal risk stratification approach 2 4
Deployment of risk stratification approach
2 2
Identified population included 2 1 Re-stratification frequency 1 4 Patients´ identification and selection criteria
4 1
Study predicting factor for
readmission
Redefining indicators: (1)readmission rate, (2)days spent at home, (3)transition to a long term care at nursing home,(4)Cost intervention and cost effectiveness compared to a standard care (Implementation Progress 25-50%)
Interventions according to levels of risks
1 3
Frequency of intervention revisions to match patients needs 4 3
Variables taken into account to assess patient's needs 4 4
Criteria for service dynamic adaptation
4 1
Staff evaluation of awareness and actions
4 2
Table 7
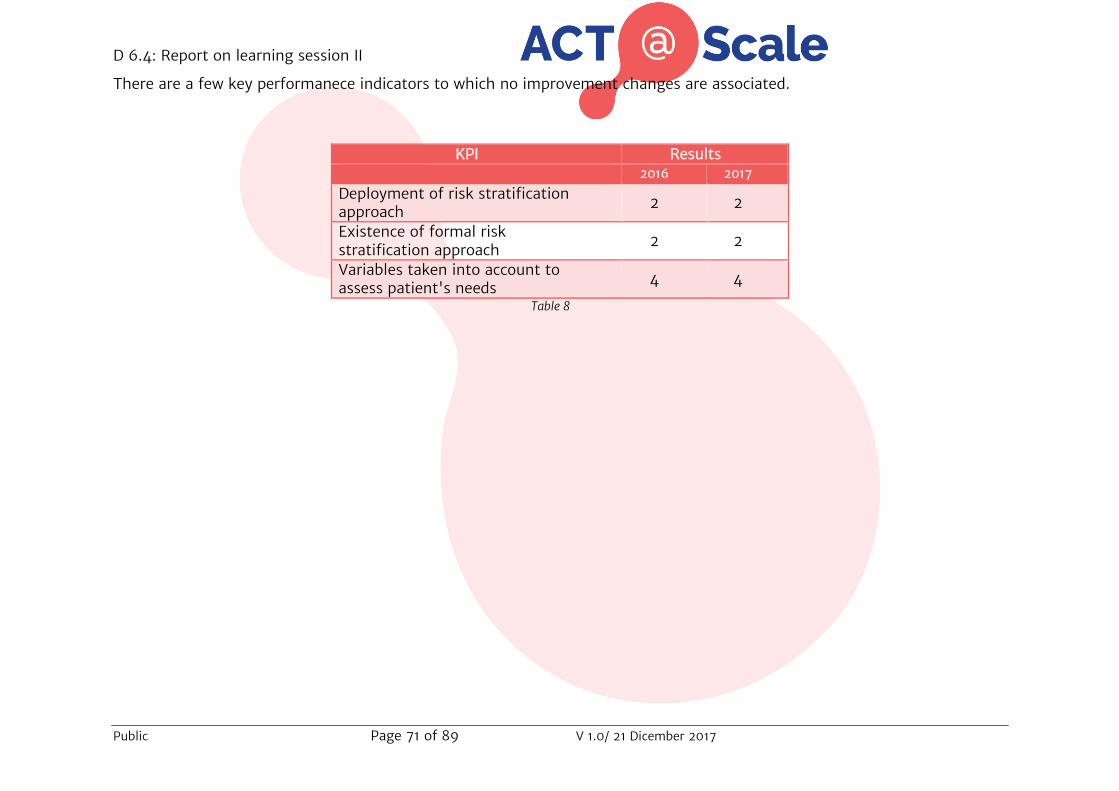
D 6.4: Report on learning session II
Public Page 71 of 89 V 1.0/ 21 Dicember 2017
There are a few key performanece indicators to which no improvement changes are associated.
KPI Results 2016 2017
Deployment of risk stratification approach
2 2
Existence of formal risk stratification approach
2 2
Variables taken into account to assess patient's needs 4 4
Table 8

D 6.4: Report on learning session II
Public Page 72 of 89 V 1.0/ 21 Dicember 2017
Discussion
The aims set by this program were:
1. Stratification of patients at higher risk of early readmission. To improve the stratification, they will evaluate risk factors for early readmission such as: comorbidity, number of prescription drugs and social risk. The idea is to test existing tools (for instance Identification of Seniors At Risk (ISAR) tool, the MultiPrognostic Index (MPI) tool, the LACE score if feasible etc.), and create a new tool if necessary.
2. In parallel, to Study of predicting factors for readmission, based on the available data of the patients in the unit.
In this first year of implementation, the program has reported problems related to patient selection criteria and definition of risk because of the increasing healthcare burden and other issues. The process has been more time consuming than expected and at the moment they are still working on it and during next year the implementation it will be expected
The very same issues appear in the Program Manager Survey results (D6.3). In the two analysed areas (Fig 1 and 2) the program doesn´t show any appreciable improvement (4% in utilization and coverage and -8% in scope and ambition, giving a total of -3% implementation score)
It is remarkable that in case of Re-stratification process, during 2016 the program developed the process once a year and during 2017 the evaluation was continuous; and the implementation process in re-stratification process has improved from 1 to 4.
Also, regarding the Interventions according to risks levels, the program has improved. In 2016 the program was the same for population regardless of risk scores, in 2017 the program has defined specific workflows for different group risks. This has supposed that the implementation process has improved from 1 to 3. It is remarkable that the variables related to assess patients’ needs, the program has not improved because in 2016 was at the top of score, and during 2017 this score has been maintained too.
In general, the program has a good level of maturity (from 2.8 to 2.9) even though it doesn´t show, in general, a great level of implementation during the last year. By defining the basics for patient selection criteria and risk stratification, many of the services that the program planned to implement, will be achieved.

D 6.4: Report on learning session II
Public Page 73 of 89 V 1.0/ 21 Dicember 2017
6.5 Collaborative self-management services to promote healthy life style: physical activity (AISBE-PA) – Catalonia
PLAN DO
(implementation progress)
KPI Results
2016 2017
Enhance clinical risk assessment and stratification
Use of population-based into clinics Elaboration of predictive modelling (25-50%)
Existence of formal risk stratification approach 2 3
Deployment of risk stratification approach 2 3
Patient’s identification and selection criteria 2 3
Re-stratification frequency 3 4
Variables taken into account to assess patient’s needs
3 4
Interventions according to levels of risk 3 4
Frequency of intervention revisions to match patient needs 3 4
Service refinement Accessility-Scalability-Metrics (25-50%)
Identified population included, ratio 1 3
Presence of individualized care plan 2 4
Variables taken into account to match specific intervention with patient needs
2 4
Service types that can be activated 2 3
Level of patient/caregiver involvement 2 3
Degree of Health Care tiers access to care plan 2 3
Staff evaluation of awareness and actions 1 2
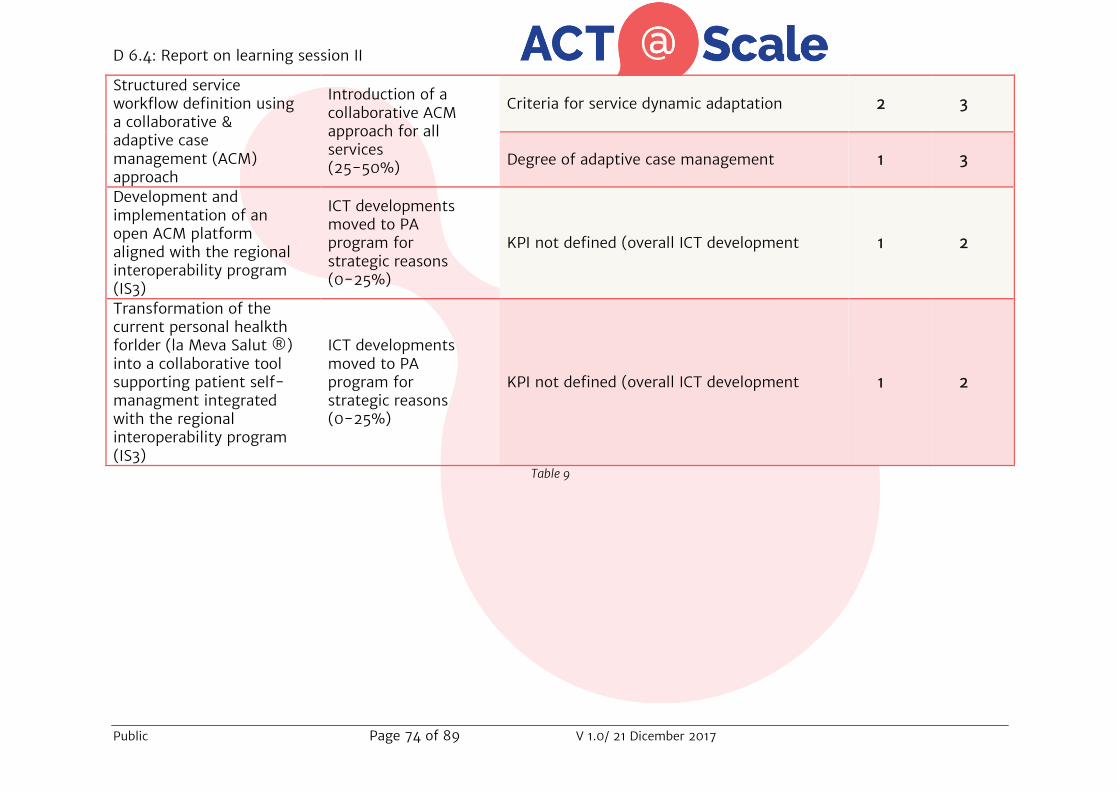
D 6.4: Report on learning session II
Public Page 74 of 89 V 1.0/ 21 Dicember 2017
Structured service workflow definition using a collaborative & adaptive case management (ACM) approach
Introduction of a collaborative ACM approach for all services (25-50%)
Criteria for service dynamic adaptation 2 3
Degree of adaptive case management 1 3
Development and implementation of an open ACM platform aligned with the regional interoperability program (IS3)
ICT developments moved to PA program for strategic reasons (0-25%)
KPI not defined (overall ICT development 1 2
Transformation of the current personal healkth forlder (la Meva Salut ®) into a collaborative tool supporting patient self-managment integrated with the regional interoperability program (IS3)
ICT developments moved to PA program for strategic reasons (0-25%)
KPI not defined (overall ICT development 1 2
Table 9

D 6.4: Report on learning session II
Public Page 75 of 89 V 1.0/ 21 Dicember 2017
There are a few key performanece indicators to which no improvement changes are associated.
KPI Results 2016 2017
Risk stratification access and changes by professionals 2 2
Staff trained in identification, evaluation and selection of case 2 2
Staff trained in care plan formulation, evaluation, follow-up and adaptation 2 2
Training frequency in identification, evaluation and selection of case 2 2
Training frequency in care plan formulation, evaluation, follow-up and adaptation 2 2
Table 10
D 6.4: Report on learning session II
Public Page 76 of 89 V 1.0/ 21 Dicember 2017
The physical activity (PA) program aims to achieve large-scale deployment of the aspects described below:
1. Implementation of collaborative self-management services designed to promote physical activity (PA) in three study groups representative of different layers of the population-based risk stratification pyramid[21], namely: (i) Prehabilitation for high risk candidates to major surgery; (ii) Community-based rehabilitation for clinical stable chronic patients with moderate to severe disease; and, (iii) Promotion of physical activity and healthy lifestyles for citizens at risk and patients with mild disease.
2. Development and assessment of information and communication technologies (ICT) as supporting tools for both patients and professionals. The two ICT-supporting tools to be developed are: i) SMS (self-management system); and, ii) SACM (smart adaptive case management) already described in the CCP program and also in Cano I et al. Protocol for Regional Implementation of Community-based Collaborative Management of Complex Chronic Patients. NPJ Prim Care Respir Med. 2017;27(1):44.
3. Evaluation of the impact of each PA in terms of cost-effectiveness. The current study will generate a roadmap for regional adoption of the PA services
The program has very successfully covered the first type of service Prehabilitation for high risk candidates to major surgery) in terms of implementation, service workflow refinement, factors determining transferability and business models ensuring adoption. Current activities regarding this service are: i) Development and evaluation of ICT supporting tools alluded to above; ii) Generalization of the service beyond major abdominal surgery; and, iii) Evolution of the service toward perisurgical care involving health risk assessment and stratification. All these aspects are currently being worked out and it is our expectation to fulfill all these goals within 2018. Morever, 2018 will be a key year to apply the lessons learnt in the Prehabilitation service to the other two services following the plan described in Barberan-Garcia A et al. Protocol for regional implementation of collaborative self-management services to promote physical activity. BMC Health Services, 2017(submitted).
Main goals for 2018 are: i) Assessment of current developments of the perisurgical care program; ii) Plan regional deployment of the perisurgical care program; and, iii) Initiate the two other PA services: a) Community-based rehabilitation for clinical stable chronic patients with moderate to severe disease; and, b) Promotion of physical activity and healthy lifestyles for citizens at risk and patients with mild disease. During 2019, it is planned the regional deployment of the perisurgical care services; and, ii) Implementation of the other two services in AISBE.
As already mentioned in the discussion of the CCP program, we would like to stress that an analysis of the KPI grading reported in D6.3 displayed significant problems due to different factors. Among them: i) Lack of responses to some items in the first
D 6.4: Report on learning session II
Public Page 77 of 89 V 1.0/ 21 Dicember 2017
evaluation (2016); ii) Poor activation of patients’ questionnaires; and, iii) Inconsistent responses for the evolution of some KPIs between 2016 and 2017 due to suboptimal responses. We strongly suggest to use that grading of KPIs reported in the current PA table which reflects the consensus scoring of the relevant staff of the program both for 2016 and 2017.
D 6.4: Report on learning session II
Public Page 78 of 89 V 1.0/ 21 Dicember 2017
6.6. Global analysis The specific objective of Service Selection is to achieve an appropriate level of distribution of health and care resources defined by the dynamic needs of the patients and populations addressed, enhancing risk prediction in the clinical scenario. To follow this process, KPIs track all service selection elements, both population- and individual- based, such as coverage description, identification and selection of patients, services responding to patient’s needs and on-boarding the required professionals and services.
As described above and elsewhere (section 6 and D6.3), two different areas have been analysed: service selection strategy components and deployment.
When strictly analysing the numerical results, qualitative indicators, which define the “Scope and ambition” area, show comparable results when looking at data from 2016 and 2017 (fig 1). All programs have a starting point of at least 2.5 out of 4, being 2.8 the average score. In 2017 we observed a slight increase in the implementation process.
For instance, in the Basque Country’s programs, professionals have extended access and possibility to make changes in the risk stratification output, which allow including professionals´ experience based criteria into the stratification tool. Basque programs also reported a change in the presence of an individualized care plan even though its semi-automatic execution is still on-going.
Catalonia’s programs have worked in different aspects of the strategy components. The complex case management program has included new variables into the stratification approach to match patient’s needs, such as patient´s functional health status, pain, social/emotional support, activity of daily living, frailty, cognitive status, etc. Moreover, the multidisciplinary team has developed and adopted a predictive model that establishes a relationship between sets of variables to predict future outcomes. They also have worked on creating an individualized care plan. These last two points have been accomplished also by the Physical Activity program.
As reported in this deliverable, all programs are actively involved in the implementation phase but we might need to wait for a longer timeframe than just one year to detect the expected results.

D 6.4: Report on learning session II
Public Page 79 of 89 V 1.0/ 21 Dicember 2017
Figure 1: Service Selection Qualitative Indicators average results per indicated program
The quantitative indicators, which define the “Utilization and coverage” area, display bigger variation when comparing data from 2016 and 2017. To be noted, in a 1 to 4 scale, all programs scored at least 1 in 2016, with an average score of 1.47. The progress of this specific area is lower than “Scope and ambition” in 2016. By observing the global analysis (fig 2), it is visible that the improvement is more salient in the programs that had a lower score in 2016.
For example, the multimorbid integration program has established the basis for a formal training on stratification to healthcare professionals, which results in improvement of indicators related to staff evaluation. This enhancement allows the Multimorbid integration program to present the highest score (from 1.2 to 2.3; see D6.3).
On the other side, Frail Adult program, even though it has notably improved in risk stratification frequency and training frequency in identification, evaluation and selection of case (section 6.7 and D6.3), by being the most implemented at base line (2.8), does not appear to have notable changes over the last year (2.9).
0
1
2
3
4Telehealth CHF
Multimorbidpatients
Phisical ActivityFrail Adult
Complex case
Scope and ambition
2017
2016

D 6.4: Report on learning session II
Public Page 80 of 89 V 1.0/ 21 Dicember 2017
Figure 2: Service Selection Quantitative Indicators average results per indicated program
Taken together, the results indicate that the “scope and ambition” area focused on strategy components such as approach, tools and participants´ involvement are taken into account shows a lower degree of evolution (average values calculated among all programs: the average from 2016 is 2.82; the average from 2017 is 2.92; total evolution rate: 3.5%).
The area describing strategy deployment, utilization and changes such as coverage, frequency and professional numbers, points out the most prominent progress when comparing data from 2016 and 2017 (average values calculated among all programs: the average from 2016 is 1.47; the average from 2017 is 1.93; total evolution rate: 31.5%).
It has to be noted though, that the scope/ambition and utilization/coverage areas have a very different starting point in 2016, being 2.82 and 1.47 out of 4, respectively. This means that “scope and ambition” area starts with an evolution rate that is already the 70% of the total, while “utilization and coverage” area starts with an evolution rate that is 37.5% of the total. In this scenario, it is more likely that, after the first PDSA cycle, we will be able to appreciate changes in the second area but not in the first.
The aim within ACT@Scale project for service selection driver is to reach an overall evolution score across programs, from baseline to final measures, of 20%. Based on the baseline questionnaire in 2016 and the KPIs data collected in 2017, we can conclude that until now the overall progress in service selection driver is set at 17.5% (average value between “scope and ambition” and “utilization and coverage” evolution rate). The tendency is appropriate, so the expected global outcome seems to be achievable.
0
1
2
3
4
TelehealthCHF
Multimorbidpatients
PhisicalActivity
Frail Adult
Complexcase
Ulitization and coverage
2017
2016
D 6.4: Report on learning session II
Public Page 81 of 89 V 1.0/ 21 Dicember 2017
7. ACT phase ACT phase is the fourth step of the learning cycle. The timeframe for this phase is from October 2017 till December 2017. During this phase each program will organized at least one meeting with the multidisciplinary team to refine changes and determine future plans, based on the results of the STUDY phase. Here the decisions made during the ACT phase are reported by program.
7.1 ACT phase Reporting The tables below present the analysis of each program status. Each program completed the table identifying the improvement actions, describing its status (option) and adding related comments. Options:
(i) Adopt: the desired change is achieved. Once improvement is affirmed, determine when the successful change can be reproduced on a larger scale.
(ii) Adapt: revise the change process. Return to Plan, Do, Study, Act. Repeat the test using a different method or by gathering different pre and post data. Consider if circumstances changed or if the test fell short of the desired change outcome.
(iii) Abandon: the change exacerbated the old problem or created a new harmful problem. Return to the Plan phase. Delve into understanding the problem to see if additional underlying causes can be uncovered. Critically revise other potential solutions. Once a new plan is developed, complete the Do, Study, Act phases again.

D 6.4: Report on learning session II
Public Page 82 of 89 V 1.0/ 21 Dicember 2017
7.2 Multimorbid population integrated intervention -Basque Country
Improvement actions Option
(Adopt, adapt or abandon
Comments
Clear definition of care pathways and roles
Adopt
The roles of the actors involved in the integrated care pathway for multimorbid patients has been defined and agreed by all organizations. The organizations are ready to adopt the defined care pathways.
Creation of personalized care plans
Adapt
The content and accessibility criteria of the personalized care plan have been defined. During the 2nd PDSA cycle the technological tool to create and execute semi-automatically the personalized care plan will be built.
Staff training on stratification tools
Adapt
The content of the training courses has been drafted. During the 2nd PDSA cycle the sessions of the online training program will be develop and provided to professionals.

D 6.4: Report on learning session II
Public Page 83 of 89 V 1.0/ 21 Dicember 2017
7.3 Telemonitoring services for congestive heart failure (CHF)-Basque Country
Improvement actions Option
(Adopt, adapt or abandon
Comments
Criteris to identify unstable patients and to provide patient and/or caregivers with the most suitable monitoring service
Adopt
Criteria have been established and adopted. They are currently used in the daily routine.
Creation of personalized care plans
Adapt
The content and accessibility criteria of the personalized care plan have been defined. During the 2nd PDSA cycle the Program Management System functionalities will be enhanced. By this mean, the care plan will be constantly updated according to patient´s needs.
Staff training on 1. Case selection and
evaluation and 2. Care plan formulation,
follow-up and adaptation.
Adapt
The need for training courses has been underlined during the KPIs result analysis. During the 2nd PDSA cycle the possibility of providing training to healthcare professionals will be tackled and analysed. Its implementation will be considered.

D 6.4: Report on learning session II
Public Page 84 of 89 V 1.0/ 21 Dicember 2017
7.4 Support of Complex case managment (AISBE-CCP) –Catalonia
Improvement actions Option (Adopt, adapt or abandon
Comments
Service refinement Adopt
The services have been identified and refined. Full implementation is predicted to be completed by end of 2018
Service and structure flow Adapt
The work flow structure has been delayed due to refinement in system implementation. This item will be carried out properly during 2018 and 2019
Development and implementation of an open adoptive care managment
Adapt
The system has been developed but implementation is delayed This intervencion will be carried out properly during 2018 and 2019
Transformation personal health folder
Adapt
This intervencion is dependent on the previous one. Once the ACM is up and running the personal health forlder will be too.
Risk stratification Adapt
The Risk stratification have been defined. Full implementation is predicted to be completed by end of 2018

D 6.4: Report on learning session II
Public Page 85 of 89 V 1.0/ 21 Dicember 2017
7.5 Integrated care for subacute and frail older adults , Parc Sanitari Per Virgili (PSPV) -Catalonia
Improvement actions Option
(Adopt, adapt or abandon
Comments
To implement a validated model to identify the risk factors of an early readmission, after testing some indicators
Adapt
In process:
-Defining indicators:
*Readmission Rate
*Days spent at home
*Transition to a long-term care facility or nursing home
*Cost intervention and cost effectiveness
-During the next 2nd PDSA cycle:
*Define the data collection
*implementation in early readmission and difficult care transition in risk patients
To develop an original proposal to study predictors of readmissions and a new tool, based on the available data for the patients
Adapt
In process:
-Collecting data to identify risk patients
-During the next 2nd PDSA cycle:
* A retrospective measurement will be developed next year
*A evaluating process it will be implemented

D 6.4: Report on learning session II
Public Page 86 of 89 V 1.0/ 21 Dicember 2017
7.6 Collaborative self-management services to promote healthy life style: physical activity (AISBE-PA) –Catalonia
Improvement actions Option
(Adopt, adapt or abandon
Comments
Identification of risk factors Adapt
The program has identified risk factors. Now it will focus on development and evaluation of ICT supporting tools
Study predicting factor for readmission
Adapt
The program has studied predicting factor for readmission. The main focus for 2018-2019 will be :a) Community-based rehabilitation for clinical stable chronic patients with moderate to severe disease; and, b) Promotion of physical activity and healthy lifestyles for citizens at risk and patients with mild disease
D 6.4: Report on learning session II
Public Page 87 of 89 V 1.0/ 21 Dicember 2017
8. Conclusion
In this deliverable all areas of implementation in which each program has devoted its time and effort are detailed. There have been programs mainly focused on the integration of the health care provision (i.e. Complex Case Management program) and others especially concentrated on set criteria to select the right patient target group (i.e. Telemonitoring of CHF and Frail Adults programs). All similarities and differences of the five programs that selected Service selection as driver, have been described.
In the “DO” templates all programs reported around 50% of the implementation process completed. Based on these results, it can be noted that the programs are on the right path to accomplished with the planned interventions.
The fisrt PDSA cycle has been completed and all programs have reported rigorously the actions performed in each step. During the STUDY phase, the programs have identified some of the topics in which they have encountered more difficulties and others to which they will direct their efforts for the coming PDSA cycle. Together with the results derived from the PM surveys, each program has been able to determine which intervention needed to be sharpened. To be noted, none of the programs identifyed interventions that need to be abandoned.
In Service Selection, three are the main domains:
1. Description, identification and selection of patients 2. Services responding to patients needs 3. On-boarding the required professionals and services
The central hypothesis is that health risk prediction and stratification optimizes the definition of well-structured programs and adaptive case management. In this scenario, WP6 aimed to promote the implementation of both population-based and individual risk assessment in order to respond to dynamic needs of a large number of patients.
Description, identification and selection of patients
In a population approach, Service Selection drives the identification of population risk strata through risk stratification, and the allocation of structured health programs targeted to a specific population group according to their risk strata. At individual clinical level, Service Selection aims to provide an adaptive personalized case management. It defines individualized care plans for patients with different individual risks and care needs, under the umbrella of the above mentioned structured health programs.
Population-based risk assessment may identify patients that either are not on the radar of service providers or/and presently unmet needs. This approach facilitates health service planning, which enables large-scale deployment of integrated care services for a

D 6.4: Report on learning session II
Public Page 88 of 89 V 1.0/ 21 Dicember 2017
target population. Of relevance, programs that had population based approach in 2016, have added individual approach to their stratification method, using both simultaneously. Eventhough the stratification method is not fully developed in all programs, when it is used is accessible to health professional for suggestions or change.
Regarding the stratification , none of the programs considered changing the existing update timing There seems to be a consensus that, at this stage, the frequency is well set in each context.
In the same line, each program uses different inclusion and exclusion criteria. The number of variables assessed in the case evaluation helps the development of individualized care plans. Case evaluation should assess all relevant variables to ensure that services respond to patients needs. Accordingly, in 2017 all programs used multiple variables for case evaluation and patient’s needs, including diagnosis, disease severity, patient clinical level and othesr (family support, social surrounding, etc).
Services responding to patients needs
In this dimension Service Selection aims to have a well distributed services accordign to patients´ needs. The perfect scenario would be to have individualized care plans that changes according to patient´s evolution (aging, disease status, patient conditions ect). All programs declare to have organized care, including coordination between primary and specialist care, however the level of service adaptation to patients´ condition and needs is not sufficiently evolved. Although some of them state that patient´s self-assessment results are introduced in care plan design, the definition of the care plan is mostly based on clinical criteria. Therefore we still need to explore whether the use of a more structured method, like rules-based thresholds and predictive tools, would generate benefit and added value in terms of health related outcomes and, health service´s planning and efficiency.
It is worth highlighting that all programs have a wide range of interventions to be delivered depending on the patient’s needs. These interventions cannot be generalized, as they vary significantly according to the health area covered and context in which they operate.
On-boarding the required professionals and services
The coordination and integration of professionals and services has a high impact not only on patients´ health outcomes but also on health care system´s effectiveness and efficiency. Type of professionals and services involved differ between programs. Generally, all programs agree on the need of improving coordination and communication between care level (primary and secondary care) and between professionals (doctors, nurses, IT staff ect).

D 6.4: Report on learning session II
Public Page 89 of 89 V 1.0/ 21 Dicember 2017
Regarding the level of awareness about service selection components (case identification, case evaluation, case selection and, care plan formulation and follow-up) amongst the staff, there is a clear lack of specific actions in most programs. In fact, they have implemented concrete interventions to regularly evaluate staff´s awareness and to act upon findings.
Programs that assessed to some extent the awareness reported the existence of training in case identification, case evaluation, and case selection, and in care plan formulation, evaluation, follow-up and adaptation as well. The training frequency varies between programs, leaving space to improvement. Assuming that the healthcare professionals can influence in the quality and effectiveness of the care provision, it is essential to increase their skills to better management of patients.