deliverable 6.1: service selection methodology report · 2016-10-13 · service selection...
TRANSCRIPT

This publication arises from the ACT@Scale (Advancing Care Coordination and Telehealth deployment at Scale) Programme which has received funding from the European Union, in the framework of the Health Programme under grant agreement 709770. The ACT@Scale programme is fully aligned with the European Innovation Partnership in Active and Healthy Ageing objectives to deploy integrated care for chronically ill patients.
Deliverable 6.1: Service Selection Methodology Report
WP 6: Service Selection
ACT@Scale Advancing Care Coordination and
Telehealth @ Scale

D 6.1: Service Selection Methodology Report
Public Page 2 of 88 V3.0 / 27 September 2016
Document Information PROJECT ACRONYM: ACT@Scale CONTRACT NUMBER: 709770 DISSEMINATION LEVEL: Public NATURE OF DOCUMENT: Report TITLE OF DOCUMENT: Service Selection Methodology Report REFERENCE NUMBER: D6.1 WORKPACKAGE: WP6 VERSION: 3.0 EXPECTED DELIVERY DATE: M5 30/09/2016 DATE: 27 September 2016 AUTHORS:
Esteban de Manuel, Kronikgune [email protected] Anna Giné March, Kronikgune [email protected]
EDITOR: Esteban de Manuel, Kronikgune [email protected] Anna Giné March, Kronikgune [email protected]
Short description of the Deliverable: Description of methods used to identify service selection key elements REVISION HISTORY
REVISION
DATE COMMENTS AUTHOR (NAME AND ORGANISATION)
V0.1 07/07/2016 Document outline Anna Giné March Kronikgune
V0.2 11/07/2016 Document outline reviewed
Ane Fullaondo Kronikgune
V0.3 22/07/2016 Introduction, Section 1 and programs 1 and 2.
Anna Giné March – Basque Country Kronikgune
V0.4 28/07/2016 Program 3, 4, 7, 8, 9, 10 and 14), and section 2.3.
Anna Giné March Kronikgune Montse Moharra - Catalunya

D 6.1: Service Selection Methodology Report
Public Page 3 of 88 V3.0 / 27 September 2016
Emilie Nielsen – RSD Maarten Lahr – Groningen
V1.0 30/08/2016 Program 11, 12 and 13.
Anna Giné March Kronikgune Claire Büchner – NIRE
V1.1 01/09/2016 Document reviewed Esteban de Manuel Anna Giné March Kronikgune
V1.2 05/09/2016 Section 2.1 Esteban de Manuel Catalina Martinez Anna Giné March Kronikgune
V1.3
07/09/2016 Section 2.2. Esteban de Manuel Anna Giné March Kronikgune
V2.0 09/09/2016 Executive Summary Conclusions
Esteban de Manuel Anna Giné March Kronikgune
V3.0 27/03/2016 Program 5, 6 included and section 2.1. re-done. Document reviewed
Josep Roca – Catalunya Esteban de Manuel Anna Giné March Kronikgune

D 6.1: Service Selection Methodology Report
Public Page 4 of 88 V3.0 / 27 September 2016
Executive Summary Aims and objectives Service selection has two approaches. In a population approach, Service Selection drives the identification of population risk strata through risk stratification, and the allocation of structured health programs targeted to a specific population group according to their risk strata. At individual clinical level, Service Selection aims to an adaptive personalized case management. It defines individualized care plans for patients with different individual risks and care needs, under the umbrella of the above mentioned structured health programs, The specific objective of Work Package on Service Selection (WP6) is to achieve an appropriate level of distribution of health and care resources defined by the dynamic needs of the patients and populations addressed, enhancing risk prediction in the clinical scenario. This D.6.1 Service Selection Methodology Report is a description of methods used to identify service selection key elements to gather baseline information of Service Selection. Methods The Service Selection mapping presented in this document is based on a questionnaire sent to all programmes. The questionnaire gathers baseline information on service Selection (Service Selection mapping indicators). Indicators are based on key informants’ knowledge, so most of them have a qualitative basis. They are formulated as questions with a closed range of responses. Each question is an indicator. There is one questionnaire per program. Service Selection indicators will track all service selection elements, population and individual, reaching description, identification and selection of patients, services responding to patient’s needs and on-boarding the required professionals and services. An analysis at program level and at project level was performed. Programs from five regions are described: North of the Netherlands, region of South Denmark, Catalonia, the Basque Country, and Northern Ireland. Results A total of 14 questionnaires were received from 14 programme managers of 5 regions participating in the project (Basque Country; Catalonia; Groningen; Northern Ireland and South Denmark). Results in service selection were analysed by program and overall project level.

D 6.1: Service Selection Methodology Report
Public Page 5 of 88 V3.0 / 27 September 2016
Conclusions In order to facilitate the decision making for collaborative methodologies and ACT@Scale learning phase, guideline questions where extract from the results to help programs to identify their service selection strengths and weaknesses. Description, identification and selection of patients
• Can a service selection population approach improve the description, identification and selection of patients on those programs with just an individual assessment?
• Would the re-stratification period have any influence on the outcomes of the program? Would it be desirable to invest on more frequent re-stratification? Is there any characteristic that would help us to do so?
• Case evaluation assesses all variables that are needed for an integrated care plan formulation?
Services responding to patients needs
• Would a more formal method to assess patients’ changing needs facilitate service dynamic adaptation?
• To what extend a risk stratification approach will facilitate the adaptive care plans management?
• Would programs that not consider patient involvement in the care plan benefit to do so?
On-boarding the required professionals and services
• Would programs benefit of a formal strategy to involve the required professionals and services in the scaling-up scenario?
• Does the professionals’ awareness (in case identification, case evaluation, and case selection, and service dynamic adaptation) facilitate program scaling-up?
• Would program benefit of involving health professionals in formal change mechanisms?

D 6.1: Service Selection Methodology Report
Public Page 6 of 88 V3.0 / 27 September 2016
Content Document Information ........................................................................................................... 2
Executive Summary ................................................................................................................. 4
List of abbreviations ................................................................................................................ 8
Glossary ................................................................................................................................... 9
Introduction ............................................................................................................................ 10
1. Service Selection approach .................................................................................................. 11
1.1. Service Selection outcomes ...................................................................................... 12
1.2. Service selection and scaling-up ................................................................................. 13
1.3. Service selection indicators .......................................................................................... 14
Data collection methodology .......................................................................................... 15
Service Selection mapping indicators ............................................................................. 18
Service Selection key progress indicators ...................................................................... 29
2. Service Selection Mapping ................................................................................................ 30
2.1. ACT@Scale overall Service Selection Mapping .......................................................... 30
Description, identification and selection of patients .................................................... 30
Services responding to patients needs .......................................................................... 40
On-boarding the required professionals and services .................................................. 49
2.2 Service Selection Mapping by programs ...................................................................... 55
Multimorbid Population Integrated Intervention ........................................................... 55
Telemonitoring services for Congestive Heart Failure ...................................................57
Healthcare support programmes for nursing homes .................................................... 59
The Chronic Patient Programme – Badalona Serveis Assistencials .............................. 61
Support of complex case management ‐ AISBE ............................................................ 63
Collaborative self‐management services promoting healthy lifestyles: physical activity - AISBE ........................................................................................................................... 65
Integrated care for subacute and frail older adults PSPV ............................................. 67
Asthma / COPD Telehealth service ................................................................................ 69
Embrace – Connecting health and community services ............................................... 71
Heart Failure Programme ................................................................................................ 73
COPD telemonitoring services ........................................................................................75
Diabetes telemonitoring services ................................................................................... 77

D 6.1: Service Selection Methodology Report
Public Page 7 of 88 V3.0 / 27 September 2016
Weight management telemonitoring services .............................................................. 79
Centre for Telepsychiatry ................................................................................................ 81
3. Conclusions ........................................................................................................................ 82
Annex ..................................................................................................................................... 88

D 6.1: Service Selection Methodology Report
Public Page 8 of 88 V3.0 / 27 September 2016
List of abbreviations ACG Adjusted clinical groups AS Appraisal standard CREG Chronic related groups CRG Clinical risk groups D6.1 Deliverable 6.1 GMA Morbidity-adjusted groups RS Risk stratification WP Work package

D 6.1: Service Selection Methodology Report
Public Page 9 of 88 V3.0 / 27 September 2016
Glossary Risk stratification: Risk stratification is defined as a systematic process to target, identify and select patients who are at risk of poorer health outcomes, and who are expected to benefit most from a particular intervention or suite of interventions. Programs: Programs/interventions/services are defined as actions taken to maximize the prospects of achieving the patient’s or providers’ goals of care, including the removal of barriers to success. Care plan: A formal plan, resulting from a needs assessment, detailing a Care Recipient’s treatment, services and support and frequency which may or may not be shared with the Care Recipient Integrated Care Plan: A Care Recipient, Care Plan providing comprehensive information on the on-going and future care services, treatment and support from all organisations and Caregivers, which may or may not be shared with the Care Recipient.

D 6.1: Service Selection Methodology Report
Public Page 10 of 88 V3.0 / 27 September 2016
Introduction Advancing Care Coordination & TeleHealth (ACT) project goal is to identify, transfer and scale up existing and operational Care Coordination and Telehealth good practices with the target of reaching a total of 75,000 care recipients across regions and programmes in multiple European countries. ACT@Scale taps into experiences from successful real life deployment projects in five European regions by using indicators to assess real world services and linking drivers and outcomes. The project activities are built around key methods and aspects needed in order to reach the project goal. At the same time, the activities reflect the areas that need to be addressed in an upscaling process. These areas include and cover:
• Stakeholder and change management • Service selection • Sustainability and business models • Citizen empowerment
Work Package on Service Selection (WP6) aim is to achieve an appropriate level of distribution of health and care resources defined by the dynamic needs of the patients and populations addressed, enhancing risk prediction in the clinical scenario. This deliverable will scope best practices in each of the partner regions and programs from a study of existing documentation as well as collating information from partners.

D 6.1: Service Selection Methodology Report
Public Page 11 of 88 V3.0 / 27 September 2016
1. Service Selection approach Service Selection aims to achieve an appropriate level of distribution of health and care resources defined by the dynamic needs of the patients and populations addressed, enhancing risk prediction in the clinical scenario. Service selection has two approaches:
• In a population approach, Service Selection drives the identification of population risk strata through risk stratification, and the allocation of structured health programs targeted to a specific population group according to their risk strata.
• At individual clinical level, Service Selection aims to an adaptive personalized case management. It defines individualized care plans for patients with different individual risks and care needs, under the umbrella of the above mentioned structured health programs.
Image 1. Service Selection approach
Population Service
Selection
Patient Service Selection
Individual care plan
Individual clinical risk assesment
Target Population Program
Population risk
stratification

D 6.1: Service Selection Methodology Report
Public Page 12 of 88 V3.0 / 27 September 2016
1.1. Service Selection outcomes Service Selection outcomes are:
1) Description, identification and selection of patients Identification of potential candidates (case identification); inclusion into the program (case selection) and assessment of clinical requirements (case evaluation).
Identification of patients can be done by population-based health risk assessment or by individual patient identification or by a mixed method. Selection of patients can be the result of the population based identification or be the result of a specific clinical assessment.
2) Services responding to patients needs
Services responding to needs can be designed at Population Program or individual care plan levels. Services responding to patients needs is based on case evaluation, follow-up and dynamic adaptation according to the evolution of the patient.
3) On-boarding the required professionals and services Collaboration among professionals, healthcare levels and integration between healthcare and social support services for dynamic allocation of the patient in his/her optimal healthcare level.

D 6.1: Service Selection Methodology Report
Public Page 13 of 88 V3.0 / 27 September 2016
1.2. Service selection and scaling-up There is consensus on the role of population-based health risk assessment as relevant driver for large-scale deployment of integrated care services. Individual risk assessment can help to define the personalized health care that a particular patient needs, his or her individualized care plan. The central hypothesis is that health risk prediction and stratification optimizes the definition of well-structured programs and adaptive case management. It should help overcome current limitations for efficient healthcare planning and patient management, such as silos, gaps, overlaps and repetitions of care provision, both at meso (organizational) and micro (clinical) levels. Service selection is a relevant driver for large scale deployment of integrated care. Accordingly, WP6 aims to drive to adopt the highly-transferable clinical risk assessment and stratification approach, in order to respond to dynamic needs of a large number of patients and large populations, but also at individual clinical level. Both are related.

D 6.1: Service Selection Methodology Report
Public Page 14 of 88 V3.0 / 27 September 2016
1.3. Service selection indicators Service Selection has two different kinds of indicators:
• Service Selection general indicators aim to identify which are the key elements of service selection, at population and individual levels. They describe, mapping the service selection within the 14 good practices on CC&TH identified in ACT@Scale.
• Service Selection key progress indicators (KPIs) aim to monitor changes through the implementation process and scaling-up on service selection. KPIs are a subgroup of the Service Selection general indicators.
Image 2. Service selction indicators
Service Selection indicators will track all service selection elements, population and individual, reaching description, identification and selection of patients, services responding to patient’s needs and on-boarding the required professionals and services.
Service Selection Key elements
(General Indicators)
Service Selection Progress Indicators
(Key Progress Indicators)

D 6.1: Service Selection Methodology Report
Public Page 15 of 88 V3.0 / 27 September 2016
Data collection methodology Project managers of each of the 14 good practices on CC&TH identified in ACT@Scale were asked to fill proposed questionnaires per programme. All 14 programs completed send the questionnaire completed. Short Name Description Target Group
Basque Country
1 Multimorbid Integration
Multimorbid Population Integrated Intervention Programme
Complex multimorbid patients
2 CHF telemonitoring
Telemonitoring services for Congestive Heart Failure
Heart failure patients
Catalonia
3 Nursing homes Healthcare support programmes for nursing homes
Elderly living in institutionalised homes
4 Chronic Care The Chronic Patient Programme – Badalona Serveis Assistencialis
Complex chronic and frail patients
5 Complex case management
Support for complex case management AISBE
Complex patients that require linking tertiary care with the community
6 Physical activity Services promoting healthy lifestyles: physical activity - AISBE
Chronic patients in need of physical activity
7 Frail older adults Integrated care for subacute and frail older adults PSPV
Frail elderly patients
Netherlands
8 Asthma/COPD Asthma / COPD Telehealth service
Patients suffering from asthma and / or COPD
9 Embrace Embrace – Connecting health and community services
Patients suffering from asthma and/or COPD

D 6.1: Service Selection Methodology Report
Public Page 16 of 88 V3.0 / 27 September 2016
10 Effective Cardio Heart Failure Program Complex heart failure patients
Northern Ireland
11 COPD Telemonitoring
COPD telemonitoring services People with COPD
12 Diabetes telemonitoring
Diabetes telemonitoring services People with diabetes
13 Weigh Management Telemonitoring
Weight management telemonitoring services
Woman with BMI over 39
South Denmark
14 Telepsychiatry Center for Telepsychiatry Citizens eligible for telepsychiatric treatment
Table 1: ACT@Scales programmes on CC&TH
The questionnaire aim to gather service selection indicators:
• Service Selection Key elements (mapping indicators) are depicted once and presented as a mapping exercise in the section 2 of this deliverable. The main target is to gather baseline information of Service Selection, both at population and individual level.
• Service Selection Progress Indicators (key progress indicators) will be
tracked annually on project’s month 7th, 19th and 31th. ACT@SCALE Description of Action establishes that overall scores of service selection KPIs across programmes improved by 20% between baseline and final measures.

D 6.1: Service Selection Methodology Report
Public Page 17 of 88 V3.0 / 27 September 2016
Indicators are based on key informants’ knowledge, so most of them have a qualitative basis. They are formulated as questions with a closed range of responses. Each question is an indicator. There is one questionnaire per program. There are three types of variables:
• Nominal variables are represented by letters. Example: Profile of Professionals engaged in Program/service selection (tick all that apply):
a) Primary Care Clinicians b) Community Nurses c) Specialist/Consultants d) Hospital Nurses e) Social workers f) Managers
• Ordinal variables are represented by numbers. Example: If there is a risk stratification approach, to which extent is used to formal targeting, identification and selection of patients in real practice?
1) It is defined but not used (not yet implemented) 2) Used to some extent (lowly implemented) 3) Used extensively (highly implemented) 4) Always used (fully implemented)
• Descriptive variables are represented by free text boxes. Example:
Please indicate program’s inclusion criteria
Inclusion criteria:

D 6.1: Service Selection Methodology Report
Public Page 18 of 88 V3.0 / 27 September 2016
Service Selection mapping indicators DESCRIPTION, IDENTIFICATION AND SELECTION OF PATIENTS
INDICATOR 1: EXISTENCE OF A FORMAL RISK STRATIFICATION APPROACH USED TO IDENTIFY AND SELECT OF PATIENTS
Description: Is there a formal risk stratification approach used to identify and select of patients*?
1) No 2) Individual level 3) Population level 4) Both, individual and population level
*Formal risk stratification approach is understood as a systematic process to target, identify and select patients who are at risk and who are expected to benefit most from a particular intervention or suite of interventions.
INDICATOR 2: LEVEL/S USED TO IDENTIFY, AND SELECT PATIENTS.
Description: Please indicate which level/s is used to identify, and select patients (tick as many as appropriate.
Case Identification of potential candidates
Case selection Inclusion into the program
Case evaluation Characterization and assessment of clinical requirements
Individual clinical assessment
Population risk stratification
INDICATOR 3: DEPLOYMENT OF THE RISK STRATIFICATION APPROACH
Description: What degree of deployment has the risk stratification approach?

D 6.1: Service Selection Methodology Report
Public Page 19 of 88 V3.0 / 27 September 2016
1) It is defined but not used (not yet implemented) 2) Used to some extent (lowly implemented) 3) Used extensively (highly implemented) 4) Always used (fully implemented)
INDICATOR 4: PATIENTS´ IDENTIFICATION AND SELECTION CRITERIA
Description: If there is a risk stratification approach used to formal targeting, identification and selection of patients, on which criteria is based?
1) Clinical criteria: Based on the clinician training, knowledge, instinct and experience.
2) Descriptive method: rules-based thresholds for certain parameters or pre-established decision criteria that describe a high-risk patient (> 65 years, COPD, one previous admission).
3) Predictive tool: It is based on predictive models that seek to establish relationships between sets of variables to predict future outcomes, events or healthcare expenditure, using statistical and machine learning methods.
4) Mixed method: 3 and 1 INDICATOR 5: POPULATION RISK STRATIFICATION TOOL USED
Description: If there is a Population Risk Stratification tool used (answer 3 or 4 in the previous question), which is it?
a) Adjusted Clinical Groups Predictive Model (ACG-PM) b) Clinical Risk Groups (CRG) c) Diagnosis-related Groups (DRG) d) Diagnostic Cost Groups/Hierarchical Condition Categories
(DCG-HCC) e) A proprietary model, namely: ___________________ f) None of the above. g) Other: _________________________
INDICATOR 6. ACCESS AND CHANGES TO RISK STRATIFICATION INFORMATION RESULTS BY HEALTHCARE PROFESSIONALS
Description: If there is a Risk Stratification tool used, how stratification information results can be accessed and modified by healthcare professionals?

D 6.1: Service Selection Methodology Report
Public Page 20 of 88 V3.0 / 27 September 2016
1) Healthcare professionals are informed of the final list of their
stratified patients 2) Healthcare professionals can identify individual stratified
patients on their health records. 3) Healthcare professionals can identify individual stratified
patients on their health records and suggest changes. 4) Healthcare professionals can identify individual stratified
patients on their health records and can edit and modify the stratified patients.
INDICATOR 7. RISK STRATIFICATION RE-STRATIFICATION FREQUENCY
Description: If there is a Risk Stratification tool used, which is the re-stratification frequency?
1) >12 months 2) 1to 12 months 3) <1 month 4) Ongoing (continuous)
INDICATOR 8. CASE SELECTION. PROGRAM SELECTION INCLUSION AND EXCLUSION CRITERIA
Description: Please indicate program selection inclusion and exclusion criteria (case selection)(max. 100 words)
INDICATOR 9. INCLUSION INTO THE PROGRAM (CASE SELECTION): RATIO OF IDENTIFIED POPULATION FINALLY INCLUDED IN THE PROGRAM.
Description: Inclusion into the program (case selection): Ratio of identified population finally included in the program.
1) <25% 2) 25-50% 3) 51-75% 4) >75%
INDICATOR 10. CASE EVALUATION: VARIABLES TAKEN INTO ACCOUNT TO ASSESS SPECIFIC PATIENT´S NEEDS

D 6.1: Service Selection Methodology Report
Public Page 21 of 88 V3.0 / 27 September 2016
Description: Which variables does it take into account to assess specific patient´s needs (case evaluation)?
1) Diagnosis 2) Diagnosis + severity 3) Diagnosis + severity + patient-level clinical requirements 4) Diagnosis + severity + patient-level clinical requirements +
specific characteristics (functional health status, pain, social/emotional support, activities of daily living, frailty, cognitive status and others)
SERVICES RESPONDING TO PATIENTS NEEDS INDICATOR 11. INTERVENTIONS ACCORDING TO LEVELS OF RISKS IN THE TARGET POPULATION GROUP
Description: Does the Program define different interventions according to different levels of risks in the target Population Group?
1) No, the program is the same for population regardless of the risk scores.
2) Different care levels intervene depending of the group risk 3) plus Specific workflows are defined for different groups’ risk
INDICATOR 12. PRESENCE OF AN INDIVIDUALIZED PATIENT CARE PLAN
Description: Is there an Individualized Patient Care Plan?
1) No, the program is the same for all patients regardless of their conditions.
2) It may be some specific clinical decisions according to patient´s evolution but not a formal care plan.
3) There is an individualized care plan but it does not change according to the evolution of the patient.
4) There is an individualized care plan that dynamically changes according to the evolution of the patient.
INDICATOR 13. VARIABLES TAKEN INTO ACCOUNT TO MATCH SPECIFIC INTERVENTIONS TO THE PATIENT´S NEEDS

D 6.1: Service Selection Methodology Report
Public Page 22 of 88 V3.0 / 27 September 2016
Description: If there is a care plan (answers 2, 3 and 4 in previous question), which variables does it take into account to match specific interventions to the patient´s needs?
1) Diagnosis 2) Diagnosis + severity 3) Diagnosis + severity + patient-level clinical requirements 4) Diagnosis + severity + patient-level clinical requirements +
specific characteristics (functional health status, pain, social/emotional support, activities of daily living, frailty, cognitive status and others)
INDICATOR 14. INTEGRATED CARE PLAN MATURITY: SERVICE TYPES THAT CAN BE ACTIVATED.
Description: If there is a care plan, please select which specific service type can be activated (integrated care plan maturity):
1) Usual care reactive to patient demand, including full range of patient care options that a clinician could choose to provide or offer to meet an individual patient’s needs, such as medication reviews, referral to specialist, social care, rehabilitation and community nursing services (episode centered)
2) Organized care: includes (1), ensuring coordination over time between primary and specialist care, for diagnostics and for social support, as well as ensuring timely review (Process).
3) Proactive plan care, includes (2) with based on risk stratification patient selection, according to patient-level clinical requirements, including Care management if required, self-management programs and follow-up (Care plan)
4) Proactive shared care planning –includes (3) with goals agreed with patient and stakeholders involved, ensuring a patient-centered care plan, including changes when required (Personalized care plan)
INDICATOR 15. SERVICE DYNAMIC ADAPTATION: FREQUENCY OF PLANNED INTERVENTIONS REVISIONS TO MATCH PATIENT CHANGING NEEDS
Description: If there is a care plan, which is frequency of the planned interventions revisions to match patient changing needs (service dynamic adaptation)?

D 6.1: Service Selection Methodology Report
Public Page 23 of 88 V3.0 / 27 September 2016
1) >12 months 2) 1to 12 months 3) <1 month 4) Ongoing (continuous)
INDICATOR 16. CRITERIA FOR SERVICE DYNAMIC ADAPTATION
Description: If there is risk stratification approach used in service dynamic adaptation, on which criteria is based?
1) Clinical criteria: Based on the clinician training, knowledge,
instinct and experience. 2) Descriptive method: rules-based thresholds for certain
parameters or pre-established decision criteria that describe a high-risk patient (> 65 years, COPD, one previous admission).
3) Predictive tool: It is based on predictive models that seek to establish relationships between sets of variables to predict future outcomes, events or healthcare expenditure, using statistical and machine learning methods.
4) Mixed method: 3 and 1
INDICATOR 17. DEGREE OF ADAPTIVE CASE MANAGEMENT
Description: If there is a risk stratification approach in service dynamic adaptation, which is the adaptive case management it allows?
1) Just predict future events. 2) Besides (1) guides the type of interventions offered to the
patient. 3) Besides (2), define the intensity of intervention offered to the
patient. 4) Besides (3), establish an individualized care plan.
INDICATOR 18. SCOPE OF THE ADAPTIVE CARE plan
Description: The adaptive care plan includes (tick all that applies):
a) Patient care well-defined Goals b) Pharmacological interventions c) Immunization

D 6.1: Service Selection Methodology Report
Public Page 24 of 88 V3.0 / 27 September 2016
d) Nursing care e) Rehabilitation activities f) Medical Devices and appliances g) Referral to specialist(s) h) Surgical procedures i) Health Promotion activities (exercise, nutrition, other
habits…) j) Health coaching –health literacy, patient activation,
adherence to care plans, and self-management skill building. k) Social care l) Community resources m) Clinical assessments and metrics (physical exams, Lab Tests,
diagnostic procedures) n) Planned encounters and follow up o) Logistic support p) Others:________________________________
_________ INDICATOR 19. ELEMENTS AND ACTIVATION OF THE ADAPTIVE CARE PLAN
Description: Please explain what does the adaptive care plan consist of? Which elements are incorporated? When are those activated? (max. 100 words)
INDICATOR 20. LEVEL OF PATIENT / CAREGIVER INVOLVEMENT IN THE CARE PLAN.
Description: Level of patient / caregiver involvement in the care plan.
1) Does not include results of patient assessments 2) Includes results of patients assessments, but not self-
management goals 3) Includes results of patient´s assessments and self-management
goals agreed by healthcare professionals and patient. 4) Includes results of patient´s assessments, self-management goals
agreed by healthcare professionals and patient, and patient follow-up
INDICATOR 21. ICTS SUPPORT IN CARE PLAN EXECUTION, FOLLOW-UP AND EVENT HANDLING.

D 6.1: Service Selection Methodology Report
Public Page 25 of 88 V3.0 / 27 September 2016
Description: If there is ICTs support in care plan execution, follow-up and event handling, please tick all that apply:
a) It fosters patient empowerment and self-management b) It facilitates remote supervision/monitoring c) It supports health professionals in decision making process d) It facilitates collaboration among professionals across healthcare
levels e) It facilitates collaboration among healthcare and social-care
ON-BOARDING THE REQUIRED PROFESSIONALS AND SERVICES
INDICATOR 22. DEGREE OF HEALTHCARE TIERS ACCESSIBILITY TO THE PATIENT CARE PLAN
Description: Degree of healthcare tiers accessibility to the patient care plan?
1) Primary Care Clinician or nurse or specialist 2) Primary Care Clinician + nurse 3) Multi-level clinicians (Primary Care and hospital) 4) Multi-level clinicians + social and other resources
INDICATOR 23. PROFILE/S OF PROFESSIONALS INVOLVED IN THE IDENTIFICATION OF POTENTIAL CANDIDATES (CASE IDENTIFICATION), INCLUSION INTO THE PROGRAM (CASE SELECTION) AND ASSESSMENT OF CLINICAL REQUIREMENTS (CASE EVALUATION)
Description: Which is the profile/s of the professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation)? (Tick all that apply):
a) Primary Care Clinicians b) Community Nurses c) Specialist/Consultants d) Hospital Nurses e) Social workers f) Managers g) Other: _____________

D 6.1: Service Selection Methodology Report
Public Page 26 of 88 V3.0 / 27 September 2016
INDICATOR 24. PROFILE/S OF THE PROFESSIONALS INVOLVED IN CARE PLAN FORMULATION, EVALUATION, FOLLOW-UP AND ADAPTATION
Description: Which is the profile/s of the professionals involved in care plan formulation, evaluation, follow-up and adaptation? (tick all that apply):
a) Primary Care Clinicians b) Community Nurses c) Specialist/Consultants d) Hospital Nurses e) Social workers f) Managers g) Other: _____________
INDICATOR 25. NUMBER OF HEALTHCARE PROFESSIONALS INVOLVED IN THE PROGRAM.
Description: Please specify the number of healthcare professionals involved in the program:
• Primary Care Clinicians: ___________ • Community Nurses: _______________ • Specialist/Consultants: ____________ • Hospital Nurses: ___________________ • Social workers: ___________________ • Managers: _______________________ • Other: ___________________________
INDICATOR 26. EVALUATION OF AWARENESS AND ACTIONS AMONGST STAFF.
Description: Awareness amongst staff evaluated regularly and findings acted upon appropriately
1) Never evaluated 2) Evaluated but no action taken 3) Evaluated and findings acted upon sporadically 4) Evaluated regularly and findings acted upon appropriately

D 6.1: Service Selection Methodology Report
Public Page 27 of 88 V3.0 / 27 September 2016
INDICATOR 27. PROPORTION OF HEALTHCARE PROFESSIONALS INVOLVED THAT HAS BEEN FORMALLY TRAINED IN CASE IDENTIFICATION, CASE EVALUATION, AND CASE SELECTION
Description: Proportion of healthcare professionals involved that has been formally trained in case identification, case evaluation, and case selection?
1) <25% 2) 25-50% 3) 51-75% 4) >75%
INDICATOR 28. PROPORTION OF HEALTHCARE PROFESSIONALS INVOLVED THAT HAS BEEN FORMALLY TRAINED IN CARE PLAN FORMULATION, EVALUATION, FOLLOW-UP AND ADAPTATION
Description: Proportion of healthcare professionals involved that has been formally trained in care plan formulation, evaluation, follow-up and adaptation?
1) <25% 2) 25-50% 3) 51-75% 4) >75%
INDICATOR 29. FREQUENCY OF THE TRAINING IN CASE IDENTIFICATION, CASE EVALUATION, AND CASE SELECTION
Description: Which is frequency of the training in case identification, case evaluation, and case selection?
1) >12 months 2) 1to 12 months 3) <1 month 4) Ongoing (continuous)
INDICATOR 30. FREQUENCY OF THE TRAINING IN CARE PLAN FORMULATION, EVALUATION, FOLLOW-UP AND ADAPTATION
Description: Which is frequency of the training in care plan formulation, evaluation, follow-up and adaptation?

D 6.1: Service Selection Methodology Report
Public Page 28 of 88 V3.0 / 27 September 2016
1) >12 months 2) 1to 12 months 3) <1 month 4) Ongoing (continuous)
INDICATOR 31. HEALTHCARE PROFESSIONALS INFLUENCE THE PROCESS OF CHANGE
Description: Healthcare professionals influence the process of change (tick all that apply):
a) Can modify the selected stratified patients b) Can choose a wide range of patient care options to meet
patients’ needs c) There are formal participation mechanisms to develop or
change the intervention/program d) They are involved in training or supporting their
colleagues e) There is a strategy to share good practices or outcomes. f) They are involved in the design and implementation of
PDSA cycles as active.

D 6.1: Service Selection Methodology Report
Public Page 29 of 88 V3.0 / 27 September 2016
Service Selection key progress indicators Description, identification and selection of patients
1. Existence of formal risk stratification approach used to formal targeting, identification and selection of patients
2. Extent is used to formal targeting, identification and selection of patients in real practice
3. Criteria to formal targeting, identification and selection of patients
4. Degree of access and modification by healthcare professionals
5. Ratio of identified population finally included in the program
Services responding to patients needs 6. Existence of individualized Patient Care Plan
7. Variables taken into account to match specific interventions to the patient´s needs
8. Integrated care plan maturity: specific service that can be activated
9. Service dynamic adaptation: frequency of the planned interventions revisions to match patient changing needs
10. Adaptive case management capacity
11. Adaptive care plan scope
12. Patient/caregiver involvement in the care plan
On-boarding the required professionals and services 13. Healthcare tiers accessibility to health plan
14. Number of healthcare professionals involved in the program
15. Evaluation of awareness amongst staff
16. Proportion of healthcare professionals involved trained in case identification, case evaluation, and case selection
17. Proportion of healthcare professionals involved trained in care plan formulation, evaluation, follow-up and adaptation
18. Healthcare professionals influence the process of change

D 6.1: Service Selection Methodology Report
Public Page 30 of 88 V3.0 / 27 September 2016
2. Service Selection Mapping
2.1. ACT@Scale overall Service Selection Mapping
Description, identification and selection of patients First indicator is whether a formal risk stratification approach is used to identify and select patients. From 14 programs analysed, 8 use just and individual stratification approach, including the 3 Northern Ireland’ programs which approach is not formal. Two programmes use just a population approach, and four of them use a mixed approach that includes individual and population level.
1) No 2) Individual level
3) Population level
4) Both, individual and population level
CHF TELEMONITORING MULTIMORBID INTEGRATION
NURSING HOMES
CHRONIC CARE COMPLEX CASE MANAGEMENT
PHISICAL ACTIVITY
FRAIL OLDER ADULTS
ASTHMA/COPD
EMBRACE
EFFECTIVE CARDIO COPD TELEMONITORING DIABETES TELEMONITORING WEIGH MANAGEMENT TELEMONITORING
MENTAL HEALTH Table 2. Indicator 1: Existence of a formal risk stratification approach used to identify and select of patients

D 6.1: Service Selection Methodology Report
Public Page 31 of 88 V3.0 / 27 September 2016
Individual clinical assessment is used for case identification of potential candidates, case selection and inclusion in the program and case evaluation, characterizing and assessing clinical requirements.
Case Identification of potential candidates
Case selection Inclusion into the program
Case evaluation Characterization and assessment of clinical requirements
CHF TELEMONITORING
Individual clinical assessment Population risk stratification
MULTIMORBID INTEGRATION
Individual clinical assessment Population risk stratification
NURSING HOMES
Individual clinical assessment Population risk stratification
CHRONIC CARE
Individual clinical assessment Population risk stratification
COMPLEX CASE MANAGEMENT
Individual clinical assessment Population risk stratification
PHISICAL ACTIVITY
Individual clinical assessment Population risk stratification
FRAIL OLDER ADULTS
Individual clinical assessment Population risk stratification
ASTHMA/COPD
Individual clinical assessment Population risk stratification
EMBRACE
Individual clinical assessment Population risk stratification
EFFECTIVE CARDIO
Individual clinical assessment Population risk stratification
COPD TELEMONITORING
Individual clinical assessment Population risk stratification

D 6.1: Service Selection Methodology Report
Public Page 32 of 88 V3.0 / 27 September 2016
DIABETES TELEMONITORING
Individual clinical assessment Population risk stratification
WEIGH MANAGEMENT TELEMONITORING
Individual clinical assessment
Population risk stratification
MENTAL HEALTH
Individual clinical assessment Population risk stratification
Table 3. Indicator 2: Level/s used to identify, and select patients.
D 6.1: Service Selection Methodology Report
Public Page 33 of 88 V3.0 / 27 September 2016
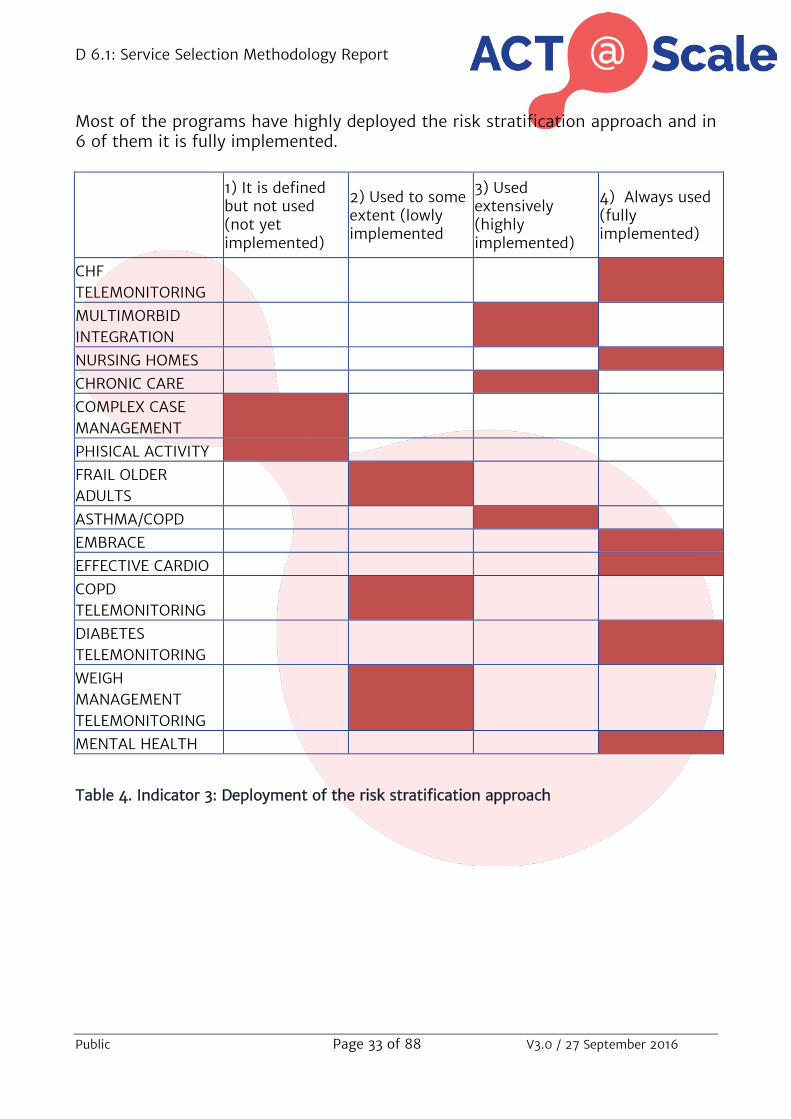
Most of the programs have highly deployed the risk stratification approach and in 6 of them it is fully implemented.
1) It is defined but not used (not yet implemented)
2) Used to some extent (lowly implemented
3) Used extensively (highly implemented)
4) Always used (fully implemented)
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER
ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH
MANAGEMENT TELEMONITORING
MENTAL HEALTH
Table 4. Indicator 3: Deployment of the risk stratification approach

D 6.1: Service Selection Methodology Report
Public Page 34 of 88 V3.0 / 27 September 2016
The criteria used in the risk stratification approach to target, identify and select patients in 2 programs, in 6 it is based of the programs just in rules-based thresholds using certain parameters or pre-established decision criteria. However 6 of them also used predictive tools, which are based on predictive models that seek to establish relationships between sets of variables to predict future outcomes, events or healthcare resources use.
1) Clinical criteria 2) Descriptive method 3) Predictive tool 4) Mixed method
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL
ACTIVITY FRAIL OLDER
ADULTS ASTHMA/COPD EMBRACE EFFECTIVE
CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH
MANAGEMENT TELEMONITORING
MENTAL HEALTH
Table 5. Indicator 4: Patients´ identification and selection criteria
Most programs utilize well-known predictive tools, some of them are of free access, and others are proprietary models.

D 6.1: Service Selection Methodology Report
Public Page 35 of 88 V3.0 / 27 September 2016
Risk Stratification information is accessible to the health professionals. However this information is display in different ways and the ability to modify is not uniform across the programs. In programs, the professionals only get the final list of the stratified patients. In other two, they can identify them in their health records. In one program, they identify individual stratified patients and suggest changes in the risk strata of the patient. And finally, in three of them, they can either edit and modify the stratified patients, and change the strata.
1) Healthcare professionals are informed of the final list of their stratified patients
2) Healthcare professionals can identify individual stratified patients on their health records.
3) Healthcare professionals can identify individual stratified patients on their health records and suggest changes.
4) Healthcare professionals can identify individual stratified patients on their health records and can edit and modify the stratified patients.
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH MANAGEMENT
TELEMONITORING MENTAL HEALTH
Table 6: Indicator 6. Access and changes to Risk Stratification information results by healthcare professionals
D 6.1: Service Selection Methodology Report
Public Page 36 of 88 V3.0 / 27 September 2016
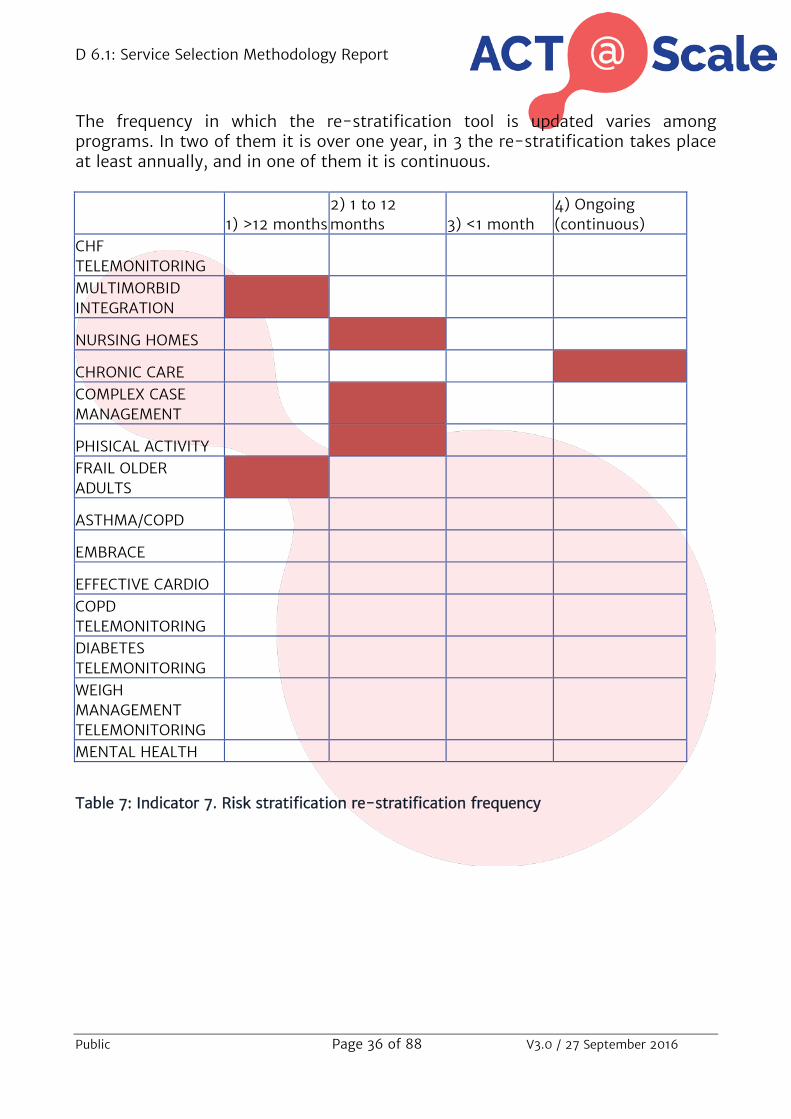
The frequency in which the re-stratification tool is updated varies among programs. In two of them it is over one year, in 3 the re-stratification takes place at least annually, and in one of them it is continuous.
1) >12 months
2) 1 to 12 months 3) <1 month
4) Ongoing (continuous)
CHF TELEMONITORING MULTIMORBID INTEGRATION NURSING HOMES CHRONIC CARE COMPLEX CASE MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD TELEMONITORING DIABETES TELEMONITORING WEIGH MANAGEMENT TELEMONITORING MENTAL HEALTH
Table 7: Indicator 7. Risk stratification re-stratification frequency
D 6.1: Service Selection Methodology Report
Public Page 37 of 88 V3.0 / 27 September 2016
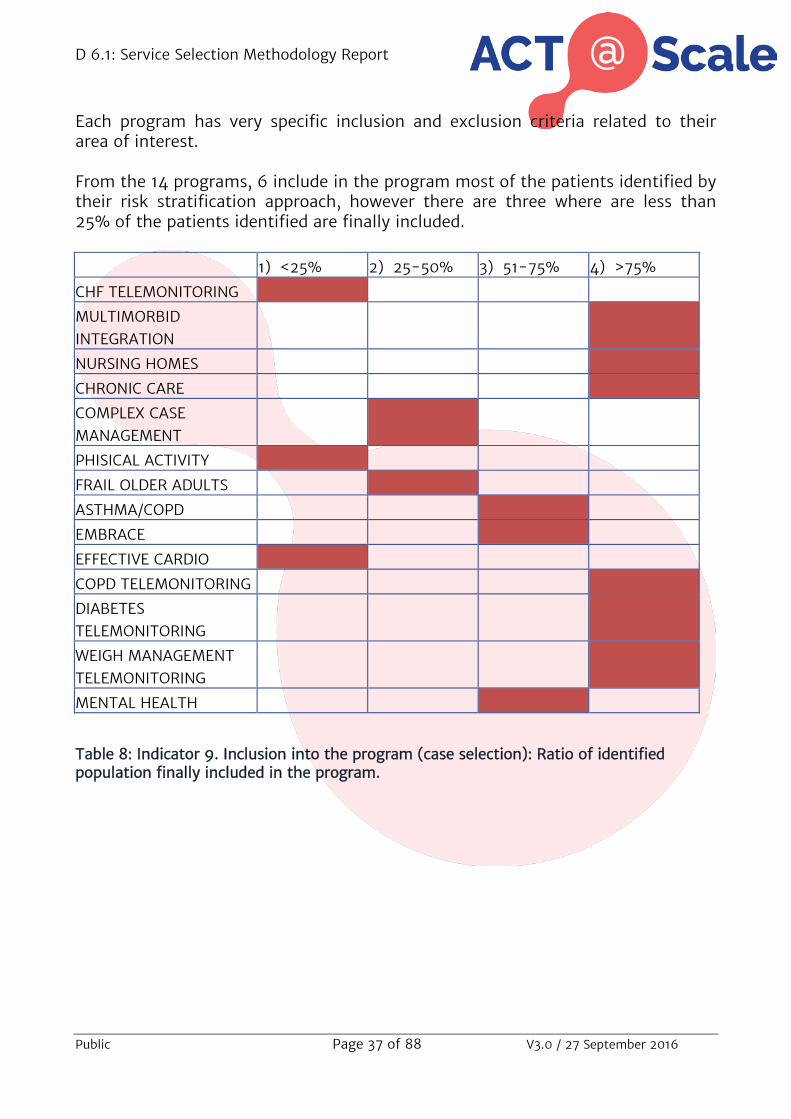
Each program has very specific inclusion and exclusion criteria related to their area of interest. From the 14 programs, 6 include in the program most of the patients identified by their risk stratification approach, however there are three where are less than 25% of the patients identified are finally included.
1) <25% 2) 25-50% 3) 51-75% 4) >75%
CHF TELEMONITORING MULTIMORBID
INTEGRATION NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD TELEMONITORING DIABETES
TELEMONITORING WEIGH MANAGEMENT
TELEMONITORING MENTAL HEALTH
Table 8: Indicator 9. Inclusion into the program (case selection): Ratio of identified population finally included in the program.

D 6.1: Service Selection Methodology Report
Public Page 38 of 88 V3.0 / 27 September 2016
Most programs have a broad range of criteria taken into account to assess the specific patient’s needs, including diagnosis, severity, patient-level clinical requirements and some specific characteristics related with each program, as functional health status, pain, social and emotional support that they have, the activities of daily living they are able to perform, and so on.
1) Diagnosis 2) Diagnosis + severity
3) Diagnosis + severity + patient-level clinical requirements
4) Diagnosis + severity + patient-level clinical requirements + specific characteristics (functional health status, pain, social/emotional support, activities of daily living, frailty, cognitive status and others)
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH
MANAGEMENT TELEMONITORING
MENTAL HEALTH
Table 9: Indicator 10. Case evaluation: Variables taken into account to assess specific patient´s needs

D 6.1: Service Selection Methodology Report
Public Page 39 of 88 V3.0 / 27 September 2016
Most programs are organized according to the risks scores. In three of them, there is no differences regardless the risk scores but most of them include different levels of care according to the group’s risk.
a. No, the program is the same for population regardless of the risk scores.
b. Different care levels intervene depending of the group risk
c. 2) plus Specific workflows are defined for different groups´s risk
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER
ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH
MANAGEMENT TELEMONITORING
MENTAL HEALTH
Table 10: Indicator 11. Interventions according to levels of risks in the target Population Group

D 6.1: Service Selection Methodology Report
Public Page 40 of 88 V3.0 / 27 September 2016
Services responding to patients needs Most programs have an individualized care plan that changes dynamically according to the evolution of the patient’s need, although three of them are not formalized.
1) No, the program is the same for all patients regardless of their conditions.
2) It may be some specific clinical decisions according to patient´s evolution but not a formal care plan.
3) There is an individualized care plan but it does not change according to the evolution of the patient.
4) There is an individualized care plan that dynamically changes according to the evolution of the patient
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL
ACTIVITY FRAIL OLDER
ADULTS ASTHMA/COPD EMBRACE EFFECTIVE
CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH
MANAGEMENT TELEMONITORING
MENTAL HEALTH
Table 11: Indicator 12. Presence of an individualized Patient Care Plan

D 6.1: Service Selection Methodology Report
Public Page 41 of 88 V3.0 / 27 September 2016
If there is a care plan, it usually takes into account all variables that gather in patients’ assessment, such as diagnosis, severity, patient-level clinical requirements and specific characteristics
1) Diagnosis
2) Diagnosis + severity
3) Diagnosis + severity + patient-level clinical requirements
4) Diagnosis + severity + patient-level clinical requirements + specific characteristics (functional health status, pain, social/emotional support, activities of daily living, frailty, cognitive status and others)
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL
ACTIVITY FRAIL OLDER
ADULTS ASTHMA/COPD EMBRACE EFFECTIVE
CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH
MANAGEMENT TELEMONITORING
MENTAL HEALTH
Table 12: Indicator 13. Variables taken into account to match specific interventions to the patient´s needs

D 6.1: Service Selection Methodology Report
Public Page 42 of 88 V3.0 / 27 September 2016
Most of the programs referred they have a proactive shared planning, with goals agreed with patient and stakeholders involved. The objectives of the care plan are set according to the patient clinical requirements and include services such as care management, self-management programs or follow-up.
1) Usual care reactive to patient demand, including full range of patient care options
2) Organized care: includes (1), ensuring coordination over time between primary and specialist care
3) Proactive plan care, includes (2) with based on risk stratification patient selection, and care management
4) Proactive shared care planning –includes (3) with patient-centered care plan, including changes when required
CHF TELEMONITORING MULTIMORBID INTEGRATION NURSING HOMES CHRONIC CARE COMPLEX CASE MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD TELEMONITORING DIABETES TELEMONITORING WEIGH MANAGEMENT TELEMONITORING MENTAL HEALTH
Table 13. Indicator 14. Integrated care plan maturity: Service types that can be activated.

D 6.1: Service Selection Methodology Report
Public Page 43 of 88 V3.0 / 27 September 2016
Programs review their plan’s interventions continuously.
1) >12 months 2) 1 to 12 months 3) <1 month 4) Ongoing
(continuous) CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH
MANAGEMENT TELEMONITORING
MENTAL HEALTH
Table 14: Indicator 15. Service dynamic adaptation: Frequency of planned interventions revisions to match patient changing needs

D 6.1: Service Selection Methodology Report
Public Page 44 of 88 V3.0 / 27 September 2016
The adaptation of the care plans are base only in clinical criteria, that means in clinicians’ training, knowledge, instinct and experience.
1) Clinical criteria 2) Descriptive method 3) Predictive tool 4) Mixed method:
3 and 1 CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL
ACTIVITY FRAIL OLDER
ADULTS ASTHMA/COPD EMBRACE EFFECTIVE
CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH
MANAGEMENT TELEMONITORING
MENTAL HEALTH
Table 15: Indicator 16. Criteria for service dynamic adaptation

D 6.1: Service Selection Methodology Report
Public Page 45 of 88 V3.0 / 27 September 2016
The risk score guides the type of intervention offered to the patient in four programs. In another four it also modifies the formal individualized care plan.
1) Just predict future events
2) Besides (1) guides the type of interventions offered to the patient.
3) Besides (2), define the intensity of intervention offered to the patient.
4) Besides (3), establish an individualized care plan.
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER
ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH
MANAGEMENT TELEMONITORING
MENTAL HEALTH
Table 16: Indicator 17. Degree of adaptive case management

D 6.1: Service Selection Methodology Report
Public Page 46 of 88 V3.0 / 27 September 2016
The adaptive care plans include in most programs a wide range of services that can be activated. No all of them have well-defined goals but all of them include different interventions according to the characteristics of the program.
Table 17: Indicator 18. Scope of the adaptive care plan
a) P
atie
nt c
are
wel
l-de
fine
d G
oals
b) P
harm
acol
ogic
al
inte
rven
tion
s c)
Im
mun
izat
ion
d) N
ursi
ng c
are
e) R
ehab
ilita
tion
act
ivit
ies
f) M
edic
al D
evic
es a
nd
appl
ianc
es
g) R
efer
ral t
o sp
ecia
list(
s)
h) S
urgi
cal p
roce
dure
s i)
Hea
lth
Prom
otio
n ac
tivi
ties
j) H
ealt
h co
achi
ng –
heal
th
liter
acy,
pat
ient
act
ivat
ion
k) S
ocia
l car
e l)
Com
mun
ity
reso
urce
s m
) C
linic
al a
sses
smen
ts a
nd
met
rics
(
n) P
lann
ed e
ncou
nter
s an
d fo
llow
up
o) L
ogis
tic
supp
ort
p) O
ther
s:
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER
ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH
MANAGEMENT TELEMONITORING
MENTAL HEALTH

D 6.1: Service Selection Methodology Report
Public Page 47 of 88 V3.0 / 27 September 2016
The level of involvement of patients and/or caregivers in the care plan is different depending on the program. Half of the programs declare that they include the results of patient´s assessments, self-management goals, and patient follow-up in their care plan.
1) Does not include results of patient assessments
2) Includes results of patients assessments, but not self-management goals
3) Includes results of patient´s assessments and self-management goals agreed by healthcare professionals and patient.
4) Includes results of patient´s assessments, self-management goals agreed by healthcare professionals and patient, and patient follow-up
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL
ACTIVITY FRAIL OLDER
ADULTS ASTHMA/COPD EMBRACE EFFECTIVE
CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH
MANAGEMENT TELEMONITORING
MENTAL HEALTH
Table 18: Indicator 20. Level of patient / caregiver involvement in the care plan.
D 6.1: Service Selection Methodology Report
Public Page 48 of 88 V3.0 / 27 September 2016
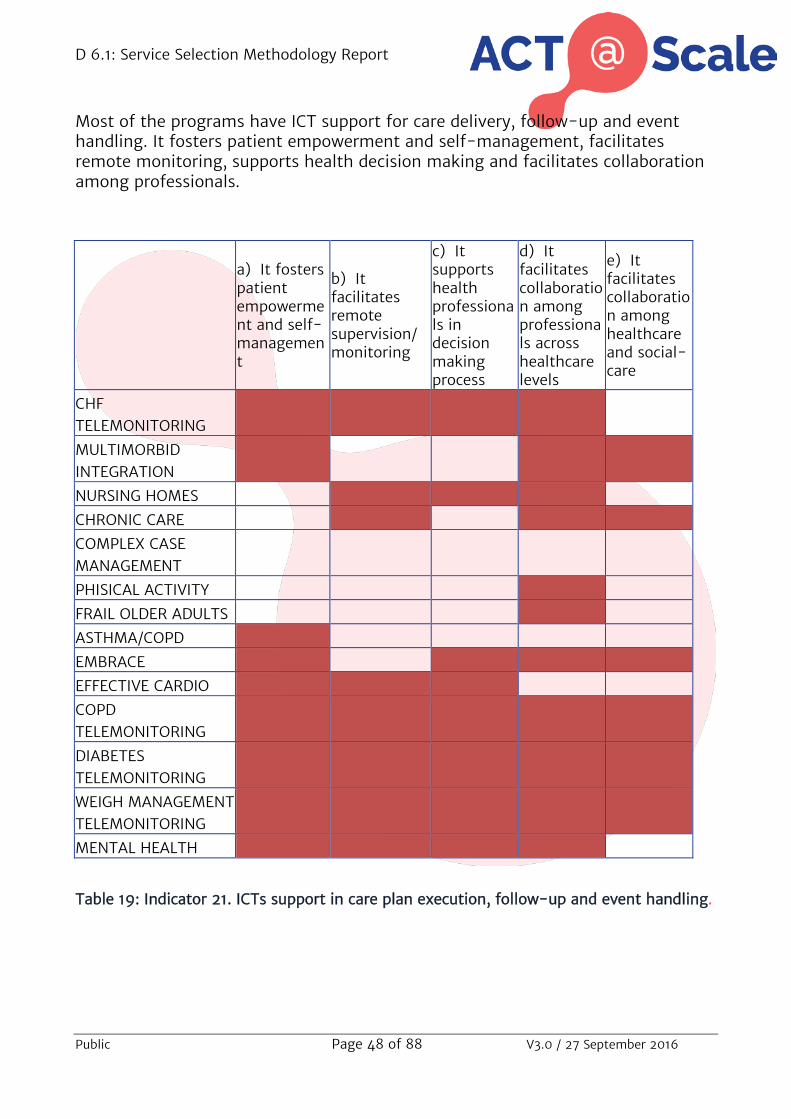
Most of the programs have ICT support for care delivery, follow-up and event handling. It fosters patient empowerment and self-management, facilitates remote monitoring, supports health decision making and facilitates collaboration among professionals.
a) It fosters patient empowerment and self-management
b) It facilitates remote supervision/monitoring
c) It supports health professionals in decision making process
d) It facilitates collaboration among professionals across healthcare levels
e) It facilitates collaboration among healthcare and social-care
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH MANAGEMENT
TELEMONITORING MENTAL HEALTH
Table 19: Indicator 21. ICTs support in care plan execution, follow-up and event handling.

D 6.1: Service Selection Methodology Report
Public Page 49 of 88 V3.0 / 27 September 2016
On-boarding the required professionals and services Patients care plans are accessible to all health care professionals in most programs. In three of them they are also accessible to social and other organizations professionals.
1) Primary Care Clinician or nurse or specialist
2) Primary Care Clinician + nurse
3) Multi-level clinicians (Primary Care and hospital)
4) Multi-level clinicians + social and other resources
CHF TELEMONITORING MULTIMORBID INTEGRATION NURSING HOMES CHRONIC CARE COMPLEX CASE MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD TELEMONITORING DIABETES TELEMONITORING WEIGH MANAGEMENT TELEMONITORING MENTAL HEALTH
Table 20: Indicator 22. Degree of healthcare tiers accessibility to the patient care plan

D 6.1: Service Selection Methodology Report
Public Page 50 of 88 V3.0 / 27 September 2016
The range of profesionals involved in the identification of potential candidates to be included in the program is wide. It depents on the program that we deal with. In most of them primary care clinicians and community nurses are involved, in some of them specialis, hiospital nurses or even social workers can participate.
a) P
rim
ary
Car
e C
linic
ians
b) C
omm
unit
y N
urse
s
c) S
peci
alis
t/
Con
sult
ants
d) H
ospi
tal
Nur
ses
e) S
ocia
l wor
kers
f) M
anag
ers
g) O
ther
:
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL
ACTIVITY FRAIL OLDER
ADULTS ASTHMA/COPD EMBRACE EFFECTIVE
CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH
MANAGEMENT TELEMONITORING
MENTAL HEALTH
Table 21: Indicator 23. Profile/s of professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation)
D 6.1: Service Selection Methodology Report
Public Page 51 of 88 V3.0 / 27 September 2016
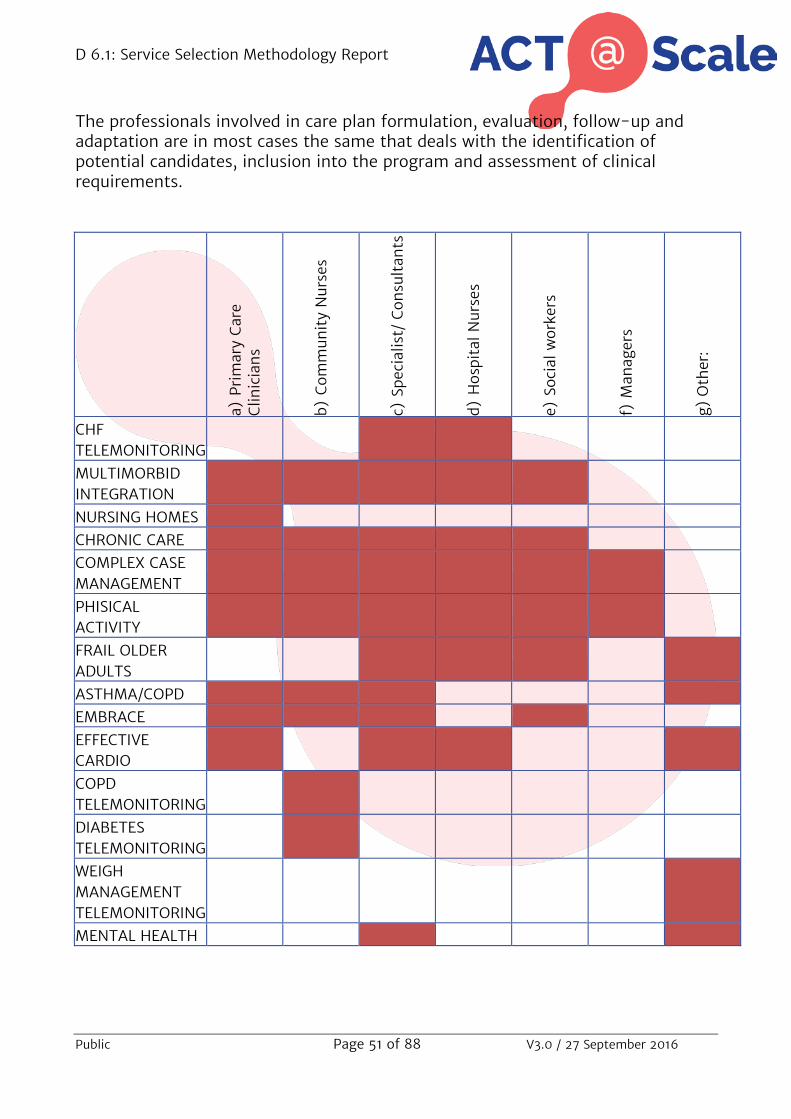
The professionals involved in care plan formulation, evaluation, follow-up and adaptation are in most cases the same that deals with the identification of potential candidates, inclusion into the program and assessment of clinical requirements.
a) Pr
imar
y C
are
Clin
icia
ns
b) C
omm
unit
y N
urse
s
c) Sp
ecia
list/
Con
sult
ants
d) H
ospi
tal N
urse
s
e) S
ocia
l wor
kers
f) M
anag
ers
g) O
ther
:
CHF TELEMONITORING MULTIMORBID INTEGRATION NURSING HOMES CHRONIC CARE COMPLEX CASE MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD TELEMONITORING DIABETES TELEMONITORING WEIGH MANAGEMENT TELEMONITORING MENTAL HEALTH

D 6.1: Service Selection Methodology Report
Public Page 52 of 88 V3.0 / 27 September 2016
Table 22: Indicator 24. Profile/s of the professionals involved in care plan formulation, evaluation, follow-up and adaptation
The number of health care profesionals involed on different programs varies depending of the type of program and degree of deployment.
Prim
ary
Car
e C
linic
ians
Com
mun
ity
Nur
ses
Spec
ialis
t/
Con
sult
ants
Hos
pita
l Nur
ses
Soci
al w
orke
rs
Man
ager
s
Oth
er
CHF TELEMONITORING 2-3 3 4 2 MULTIMORBID INTEGRATION 150 150 3 3 0 2 1 NURSING HOMES CHRONIC CARE 7 7 12 5 18 13 COMPLEX CASE MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER ADULTS 3 3 1 2 ASTHMA/COPD 500-700 30 10-20 4 23 EMBRACE 40 20-30 10-15 20-30 EFFECTIVE CARDIO 10-15 1-2 1-3 COPD TELEMONITORING 55 DIABETES TELEMONITORING 35 WEIGH MANAGEMENT TELEMONITORING 25 MENTAL HEALTH 25 2
Table 23: Indicator 25. Number of healthcare professionals involved in the program.
D 6.1: Service Selection Methodology Report
Public Page 53 of 88 V3.0 / 27 September 2016
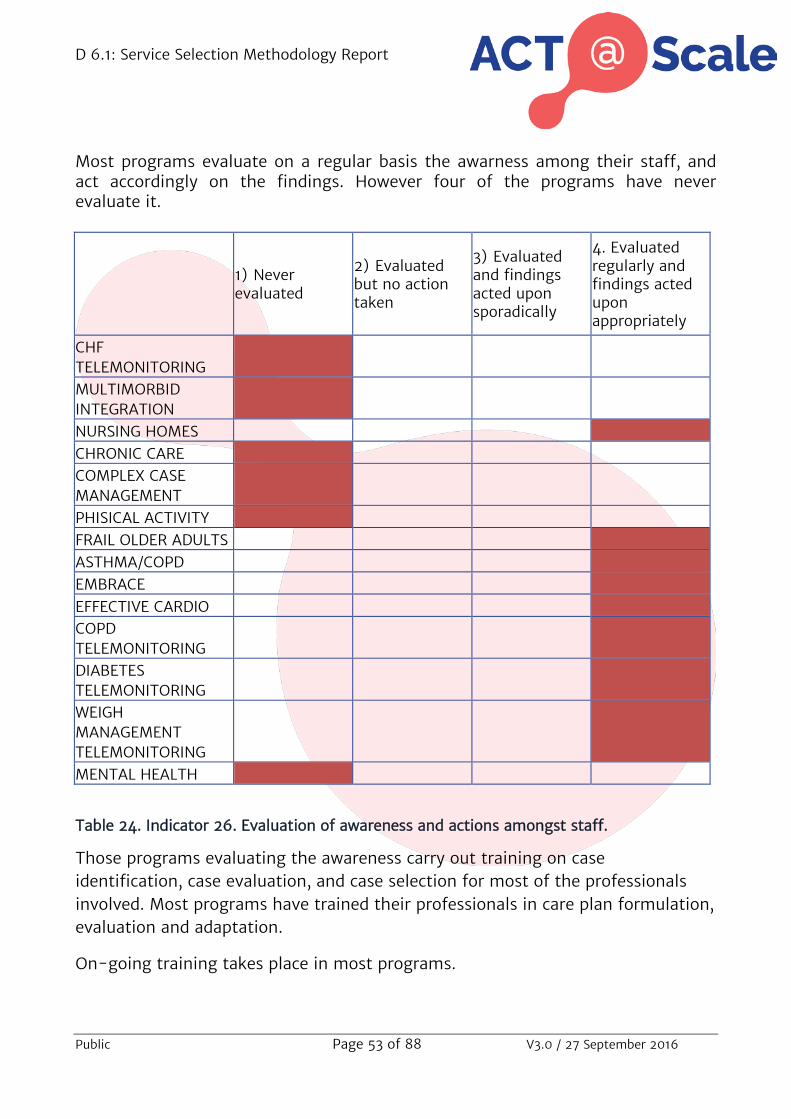
Most programs evaluate on a regular basis the awarness among their staff, and act accordingly on the findings. However four of the programs have never evaluate it.
1) Never evaluated
2) Evaluated but no action taken
3) Evaluated and findings acted upon sporadically
4. Evaluated regularly and findings acted upon appropriately
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL ACTIVITY FRAIL OLDER ADULTS ASTHMA/COPD EMBRACE EFFECTIVE CARDIO COPD
TELEMONITORING DIABETES
TELEMONITORING WEIGH
MANAGEMENT TELEMONITORING
MENTAL HEALTH
Table 24. Indicator 26. Evaluation of awareness and actions amongst staff.
Those programs evaluating the awareness carry out training on case identification, case evaluation, and case selection for most of the professionals involved. Most programs have trained their professionals in care plan formulation, evaluation and adaptation.
On-going training takes place in most programs.

D 6.1: Service Selection Methodology Report
Public Page 54 of 88 V3.0 / 27 September 2016
Heath care professionals can influence what happens in care deployment. They decide on the care services that patients get, and they are involved in training process and share good practices and outcomes amongst them. Although they are no participating so much in the formal change mechanisms in the programs, as for example de PDSA cycles that can be organized.
a) Can modify the selected stratified patients
b) Can choose a wide range of patient care options
c) There are formal participation mechanisms
d) They are involved in training
e) There is a strategy to share good practices
f) They are involved in the design and implementation
CHF TELEMONITORING
MULTIMORBID INTEGRATION
NURSING HOMES
CHRONIC CARE COMPLEX CASE
MANAGEMENT PHISICAL
ACTIVITY FRAIL OLDER
ADULTS ASTHMA/COPD EMBRACE EFFECTIVE
CARDIO COPD
TELEMONITORING
DIABETES TELEMONITORING
WEIGH MANAGEMENT TELEMONITORING
MENTAL HEALTH

D 6.1: Service Selection Methodology Report
Public Page 55 of 88 V3.0 / 27 September 2016
Table 25. Indicator 31. Healthcare professionals influence the process of change
2.2 Service Selection Mapping by programs
Multimorbid Population Integrated Intervention Description, identification and selection of patients The Population Integrated Intervention Program has a formal risk stratification approach used to identify and select patient, at individual and population level. It is highly implemented. Clinical criteria and predictive tool are used to formally target, identify and select patients. The Population Risk Stratification tool used is the Adjusted Clinical Groups Predictive Model (ACG-PM). Healthcare professionals can identify individual stratified patients on their health records and suggest changes. The re-stratification frequency is over 12 months. Inclusion criteria consider demographic data and at least two chronic diseases included in the Charlson Comorbidity Index. Subjects who have either been registered with an active cancer diagnosis under treatment, have undergone an organ transplant, or are undergoing dialysis prior to enrolment or are candidates for palliative care are excluded. Most of the patients identified are finally included in the program. Services responding to patients needs The Program defines different interventions according to different levels of risks. Different care levels intervene depending of the group risk, and specific workflows are defined for different groups´ risk. There is not a formal individualized Patient Care Plan. There may be some specific clinical decisions according to patient´s evolution but not a formal care plan. Diagnosis, severity and patient-level clinical are taken into account to match specific interventions to the patient´s needs. Proactive care is based on risk stratification, according to patient- clinical requirements. It includes care management self-management programs and follow-up. The frequency of the planned interventions´ revisions to match patient changing needs (service dynamic adaptation) is between 1 to 12 months. Clinical criteria are used in service dynamic adaptation, based on clinician training, knowledge, instinct and experience. This adaptive care plan includes pharmacological interventions, immunization, nursing carer, rehabilitation activities, medical devices and appliances, referral to specialist, surgical procedures, health promotion activities, health coaching, social care, clinical assessments and metrics and planned encounters and follow up. The care plan includes results of patient´s assessments and self-management goals agreed by healthcare professionals and patients.

D 6.1: Service Selection Methodology Report
Public Page 56 of 88 V3.0 / 27 September 2016
There is ICT support for care plan delivery, follow-up and event handling. It fosters patient empowerment and self-management and facilitates collaboration among professionals across healthcare levels and among healthcare and social-care. On-boarding the required professionals and services The patient care plan is accessible to Primary Care, Hospital, Social and other professionals. The profile of the professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation) are mainly Primary Care Clinicians. The professionals involved in care plan formulation, evaluation, follow-up and adaptation are primary care clinicians, community nurses, specialist, hospital nurses and social workers. Awareness amongst staff has not yet been evaluated. Healthcare professionals influence the process of change as they can modify the selected stratified patients and can choose a wide range of patient care options to meet patients’ needs.

D 6.1: Service Selection Methodology Report
Public Page 57 of 88 V3.0 / 27 September 2016
Telemonitoring services for Congestive Heart Failure Description, identification and selection of patients Telemonitoring services for Congestive Heart Failure have a formal risk stratification approach used to identify and select patients at individual level. This risk stratification approach is fully implemented. A descriptive method is used to formal target, identify and select a patient. It is based on rules-based thresholds for certain parameters or pre-established decision criteria that describe a high-risk patient. There is no Population Risk Stratification tool used, only Yale Index (individual clinical assessment). Inclusion criteria include diagnosis, clinical assessment and previous use of resources. Life expectancy, less than 12 months, is an exclusion criterion. Less than 25% of the identified population is finally included in the program. Case evaluation to assess specific patient´s needs takes into account diagnosis, severity, patient-level clinical requirements and some specific characteristics. Services responding to patients needs The Program does not define different interventions according to different levels of risks in the target Population Group. There may be some specific clinical decisions according to patient´s evolution but not a formal care plan. Diagnosis, severity, patient-level clinical requirements, specific characteristics are taken into account to match specific interventions to patient´s needs. The care plan includes usual care, reactive to patient demand. It includes the full range of patient care options that a clinician can provide or offer to meet an individual patient’s needs, such as medication reviews, referral to specialist, social care, rehabilitation and community nursing services (episode centred). There is a continuous planning of interventions revisions to match patient changing needs (service dynamic adaptation). Clinical criteria are used in service dynamic adaptation, based on the clinician training, knowledge, instinct and experience. It guides the type of interventions offered to the patient. The adaptive care plan includes pharmacological interventions taking into account results of patient’s assessments, but not self-management goals. There is ICT support for care plan delivery, follow-up and event handling. It fosters patient empowerment and self-management, facilitates remote supervision, supports health professionals in decision making process and facilitates collaboration among professionals across healthcare levels. On-boarding the required professionals and services The patient care plan is accessible to Primary Care and Hospital professionals. The professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation) are cardiologists and specialized nurses.

D 6.1: Service Selection Methodology Report
Public Page 58 of 88 V3.0 / 27 September 2016
The same professionals are involved in care plan formulation, evaluation, follow-up and adaptation. The number of healthcare professionals involved in the program are 150 Primary Care Clinicians, 3 Cardiologists, 3 hospital Nurses, 2 managers and one data manager. The awareness amongst staff has not yet been evaluated. Healthcare professionals influence the process of change as they can choose a wide range of patient care options to meet patients’ needs and are involved in training or supporting their colleagues.

D 6.1: Service Selection Methodology Report
Public Page 59 of 88 V3.0 / 27 September 2016
Healthcare support programmes for nursing homes Description, identification and selection of patients The healthcare support program for nursing homes has a formal risk stratification approach used to identify and select patients, at individual and population level. It is fully implemented. Clinical criteria and predictive tool are used to formal target, identify and select patients. The Population Risk Stratification tool used is Morbidity Adjusted Groups (GMA). Healthcare professionals are informed of the final list of their stratified patients. The re-stratification frequency is between 1 to 12 months. All people who live in a nursing home are identified. Most of the identified patients are finally included in the program. Diagnosis and severity are taken into account to assess specific patient´s needs (case evaluation. Services responding to patients needs The Program does not define different interventions according to different levels of risks in the target Population Group. There is an individualized care plan that dynamically changes according to the evolution of the individual patient. Diagnosis, severity, patient-level clinical requirements and specific characteristics are taken into account to match specific interventions to the patient´s needs. There is a proactive shared care planning based on risk stratification patient selection, according to patient-level clinical requirements. It includes care management (if required), self-management programs and follow-up, with goals agreed with patient and stakeholders involved. It ensures a patient-centred care plan, including changes when required (Personalized care plan). The revisions to match patient changing needs (service dynamic adaptation) are continuous. Service dynamic adaptation uses a descriptive method based on rules-based thresholds for certain parameters or pre-established decision criteria that describe a high-risk patient. The adaptive care plan includes patient care well-defined goals, pharmacological interventions, immunization, nursing care, rehabilitation activities, medical devices and appliances, referral to specialists, surgical procedures, health promotion activities, health coaching –health literacy, social care, community resources, clinical assessments and metrics, planned encounters and follow up and logistic support. It includes results of patient´s assessments but not self-management goals. There is ICT support for care plan delivery, follow-up and event handling. It facilitates remote supervision, supports health professionals in decision making process and facilitates collaboration among professionals across healthcare levels. On-boarding the required professionals and services

D 6.1: Service Selection Methodology Report
Public Page 60 of 88 V3.0 / 27 September 2016
The patient care plan is accessible to Primary Care and Hospital professionals. The profile of the professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation) are Primary Care Clinicians and social workers. The professionals involved in care plan formulation, evaluation, follow-up and adaptation are Primary Care clinicians. Awareness amongst staff is evaluated regularly and findings acted upon appropriately. Most of the healthcare professionals involved have been formally trained in case identification, case evaluation, and case selection, care plan formulation, evaluation, follow-up and adaptation. Training is continuous. Healthcare professionals influence the process of change as they can choose a wide range of patient care options to meet patients’ needs, are involved in training or supporting their colleagues. There is a strategy to share good practices or outcomes.

D 6.1: Service Selection Methodology Report
Public Page 61 of 88 V3.0 / 27 September 2016
The Chronic Patient Programme – Badalona Serveis Assistencials Description, identification and selection of patients A formal risk stratification approach is used to identify and select patients, taking into account individual and population levels. It is used extensively. Risk stratification approach is used to formal target, identify and select patients. It is based in clinical criteria and a predictive tool that seeks to establish relationships between sets of variables to predict future outcomes, events or healthcare expenditure, using statistical and machine learning methods. The population risk stratification tool used is a proprietary model, a mixed method between ACG and CRG plus other self-designed criteria. Healthcare professionals can identify individual stratified patients on their health records. The re-stratification frequency is continuous. The program selection inclusion criteria include demographical, clinical, social and resources used criteria. Oncologic patients are excluded. Most identify patient are finally included in the program. Specific patient’ needs evaluation includes diagnosis, severity, patient-level clinical requirements and specific characteristics (functional health status, pain, social/emotional support, activities of daily living, frailty, cognitive status and others). Services responding to patients needs Different care levels intervene depending of the group risk, no specific workflows are defined for different risk groups. There is an individualized care plan that dynamically changes according to the evolution of the patient. The care plan takes into account diagnosis, severity, patient-level clinical requirements and specific characteristics. There is proactive shared care plan includes goals agreed with patient and stakeholders involved, and a patient-centred care plan, that changes when required (Personalized care plan). This care plan is reviewed continuously to match patient’s need. The service dynamic adaptation is based on the clinician training, knowledge, instinct and experience. The adaptive care plan includes nursing care, rehabilitation activities social care, community resources, clinical assessments and metrics, planned encounters and follow up and logistic support. It does not include patient’s self-assessment. There is ICT support in care plan delivery, follow-up and event handling, remote supervision, collaboration among professionals across healthcare levels and collaboration among healthcare and social-care. On-boarding the required professionals and services The patient care plan is accessible to Primary Care, hospital, social and other resources professionals. The professionals involved in the identification of potential candidates (case identification), inclusion into the program (case

D 6.1: Service Selection Methodology Report
Public Page 62 of 88 V3.0 / 27 September 2016
selection) and assessment of clinical requirements (case evaluation)are Primary Care Clinicians, Community Nurses, Specialist, Hospital Nurses and Social workers. The professionals involved in care plan formulation, evaluation, follow-up and adaptation are Primary Care Clinicians, Community Nurses, Specialist, Hospital Nurses, Physiotherapist and Geriatrician. There are 7 Primary Care Clinicians, 7 Community Nurses, 12 Specialist, 5 Hospital Nurses, 18 Social workers, 4 Physiotherapist, and 9 Geriatrician involved. The awareness amongst staff has not been evaluated. Healthcare professionals influence the process of change. They can choose a wide range of patient care options to meet patients’ needs, there are formal participation mechanisms to develop or change the intervention. They are involved in training or supporting their colleagues. There is a strategy to share good practices or outcomes.

D 6.1: Service Selection Methodology Report
Public Page 63 of 88 V3.0 / 27 September 2016
Support of complex case management ‐ AISBE Description, identification and selection of patients Support of complex case management program has a formal risk stratification approach used to identify and select of patients, at individual and population level. The risk stratification approach is defined but not yet extensively used. Descriptive methods and predictive tool is used to target, identify and select patients. The Population Risk Stratification tool used GMA (Adjusted Morbidity Groups), which has a 6 month re-stratification frequency. Healthcare professionals can identify individual stratified patients on their health records. The variables does it take into account to assess specific patient´s needs (case evaluation) are diagnosis, severity and patient-level clinical requirements. This program defines different interventions according to different levels of patient’s risk, and specific workflows are defined. Services responding to patients needs There is an individualized care plan that dynamically changes according to the evolution of the patient. The variables that it takes into account to match specific interventions to the patient´s needs are diagnosis, severity, patient-level clinical requirements and specific patient’ characteristics. The care plan ensures coordination over time between primary and specialist care, for diagnostics and for social support, as well as ensuring timely review. It is continuously reviewed to match patient changing needs (service dynamic adaptation). Service dynamic adaptation is based on rules-based thresholds for certain parameters or pre-established decision criteria that describe a high-risk patient. It allows predicting future events. The adaptive care plan includes patient care well-defined goals, pharmacological interventions, immunization, nursing care, rehabilitation activities, medical devices and appliances, referral to specialist, surgical procedures, health promotion activities, health coaching, social care, community resources, clinical assessments and metrics, planned encounters and follow up and logistic support. It also includes results of patient´s assessments and self-management goals agreed by healthcare professionals and patient. ICTs support in care plan execution, follow-up and event handling, facilitating collaboration among professionals across healthcare levels. On-boarding the required professionals and services

D 6.1: Service Selection Methodology Report
Public Page 64 of 88 V3.0 / 27 September 2016
The patient care plan is accessible to Primary Care and hospital professionals. The professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation) are Primary Care Clinicians, Community Nurses, Specialist, Hospital Nurses, Social workers and Managers. The same professionals are involved in care plan formulation, evaluation, follow-up and adaptation. The awareness amongst staff has not yet been evaluated. Healthcare professionals influence the process of change. They can modify the selected stratified patients and can choose a wide range of patient care options to meet patients’ needs. They are formal participation mechanisms to develop or change the intervention. They are involved in training or supporting their colleagues and there is a strategy to share good practices or outcomes. Finally, they are involved in the design and implementation of PDSA cycles as active.

D 6.1: Service Selection Methodology Report
Public Page 65 of 88 V3.0 / 27 September 2016
Collaborative self‐management services promoting healthy lifestyles: physical activity - AISBE Description, identification and selection of patients Collaborative self‐management services promoting healthy lifestyles program has a formal risk stratification approach used to identify and select of patients, at individual and population level. The risk stratification approach is defined but not yet extensively used. Descriptive methods and predictive tool is used to target, identify and select patients. The Population Risk Stratification tool used GMA (Adjusted Morbidity Groups), which has a 6 month re-stratification frequency. Healthcare professionals can identify individual stratified patients on their health records. The variables does it take into account to assess specific patient´s needs (case evaluation) are diagnosis, severity, patient-level clinical requirements and specific characteristics. This program defines different interventions according to different levels of patient’s risk, and specific workflows are defined. Services responding to patients needs There is an individualized care plan that dynamically changes according to the evolution of the patient. The variables that it takes into account to match specific interventions to the patient´s needs are diagnosis, severity, patient-level clinical requirements and specific patient’ characteristics. The care plan ensures coordination over time between primary and specialist care, for diagnostics and for social support, as well as ensuring timely review. It is continuously reviewed to match patient changing needs (service dynamic adaptation). Service dynamic adaptation is based on rules-based thresholds for certain parameters or pre-established decision criteria that describe a high-risk patient. It allows predicting future events. The adaptive care plan includes patient care well-defined goals, pharmacological interventions, immunization, nursing care, rehabilitation activities, medical devices and appliances, referral to specialist, surgical procedures, health promotion activities, health coaching, social care, community resources, clinical assessments and metrics, planned encounters and follow up and logistic support. It also includes results of patient´s assessments and self-management goals agreed by healthcare professionals and patient. ICTs support in care plan execution, follow-up and event handling, facilitating collaboration among professionals across healthcare levels. On-boarding the required professionals and services

D 6.1: Service Selection Methodology Report
Public Page 66 of 88 V3.0 / 27 September 2016
The patient care plan is accessible to Primary Care, hospital professionals and physiotherapists. The professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation) are Primary Care Clinicians, Community Nurses, Specialist, Hospital Nurses, Social workers and Managers. The same professionals are involved in care plan formulation, evaluation, follow-up and adaptation. The awareness amongst staff has not yet been evaluated. Healthcare professionals influence the process of change. They can modify the selected stratified patients and can choose a wide range of patient care options to meet patients’ needs. They are formal participation mechanisms to develop or change the intervention. They are involved in training or supporting their colleagues and there is a strategy to share good practices or outcomes. Finally, they are involved in the design and implementation of PDSA cycles as active.

D 6.1: Service Selection Methodology Report
Public Page 67 of 88 V3.0 / 27 September 2016
Integrated care for subacute and frail older adults PSPV Description, identification and selection of patients Integrated care for subacute and frail older adults program has a formal risk stratification approach used to identify and select of patients at individual level. A mixed method is used to formal target, identify and select patients. It is based on clinical criteria and predictive tool. The Risk Stratification tool used is the Identification of Seniors at Risk (ISAR) screening tool, used at individual level. Healthcare professionals are informed of the final list of their stratified patients. The re-stratification frequency is over 12 months. Inclusion criteria include clinical criteria and ISAR screening tool. Clinical criteria are medical/hemodynamic stability, clear diagnosis at the basis of the crisis, flared-up medical disease or superimposed disease on a complex clinical situation, requiring intensive treatment and monitoring, potentially able to be discharged home in 10 days. Exclusion criteria include instability, unclear diagnosis, and expectation of longer stays. Between 25 to 50% of the identified patients are finally included in the program. Diagnosis and severity are variables taken into account to assess specific patient´s needs (case evaluation). Services responding to patients needs The Program does not define different interventions according to different levels of risks in the target Population Group. There is an individualized care plan that dynamically changes according to the evolution of the patient. Diagnosis, severity, patient-level clinical requirements and specific characteristics are the variables taken into account to match specific interventions to the patient´s needs. There is a proactive shared care planning based on risk stratification patient selection, according to patient-level clinical requirements, including Care management if required, self-management programs and follow-up, with goals agreed with patient and stakeholders involved, ensuring a patient-centred care plan, including changes when required (Personalized care plan). There is a continuous process of revisions to match patient changing needs (service dynamic adaptation) based on clinical criteria and predictive tool. It allows predicting future events, to guide the type of interventions offered to the patient, to define the intensity of intervention offered to the patient and to establish an individualized care plan. The adaptive care plan includes pharmacological interventions, nursing care, rehabilitation activities, health promotion activities, social care, community resources, clinical assessments and metrics and logistic support. It includes results of patient´s self-assessments, goals agreed by healthcare professionals and patient, and patient follow-up. There is ICT support in care plan delivery, follow-up and event handling. It facilitates remote supervision/monitoring, supports health professionals in

D 6.1: Service Selection Methodology Report
Public Page 68 of 88 V3.0 / 27 September 2016
decision making process and facilitates collaboration among professionals across healthcare levels. On-boarding the required professionals and services Primary Care and hospital professionals have access to patient care plan. The professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation) are Primary Care Clinicians and specialist. The professionals involved in care plan formulation, evaluation, follow-up and adaptation are specialist, hospital nurses, social workers, physical therapists and pharmacist. The number of professionals involved in the program are 3 speccialist, 3, hospital nurses, 1 social worker 1 pharmacist and 1 PT. Awareness amongst staff is evaluated regularly and findings acted upon appropriately. Between 51 to 75% of healthcare professionals involved have been formally trained in case identification, case evaluation and case selection. Most of healthcare professionals were involved in care plan formulation, evaluation, follow-up and adaptation that have been formally trained. The frequency of the training in case identification, case evaluation, and case selection is over 12 month. There is a continuous training in care plan formulation, evaluation, follow-up and adaptation. Healthcare professionals influence the process of change as there is a strategy to share good practices or outcomes.
D 6.1: Service Selection Methodology Report
Public Page 69 of 88 V3.0 / 27 September 2016
Asthma / COPD Telehealth service Description, identification and selection of patients Asthma / COPD Telehealth program has a formal risk stratification approach used to identify and select of patients, at individual level. The risk stratification approach is highly implemented. Healthcare professionals can identify individual stratified patients on their health records and can edit and modify the stratified patients. The re-stratification frequency is between 1 to 12 months. Inclusion criteria comprise patients suspected COPD, ACOS or having pulmonary symptoms of unknown origin. Between 51-75% of identified patients are finally included in the program. Diagnosis, severity, patient-level clinical requirements and specific characteristics are taken into account to assess specific patient´s needs. Services responding to patients needs The Program defines different interventions according to different levels of risks in the target Population Group. Different care levels intervene depending of the group risk. There is an individualized care plan that dynamically changes according to the evolution of the patient. It takes into account diagnosis, severity, patient-level clinical requirements and specific characteristics to match specific interventions to the patient´s needs. It is a proactive plan care, that includes full range of patient care options that a clinician could provide or offer to meet an individual patient’s needs. They include medication reviews, referral to specialist, social care, rehabilitation and community nursing services. It ensures coordination over time between primary and specialist care, for diagnostics and for social support, as well as ensuring timely review. It is based on risk stratification patient selection, according to the patient´s clinical requirements, including Care management, self-management programs and follow-up. The frequency of the planned interventions revisions to match patient changing needs (service dynamic adaptation) is between 1 to 12 months. The risk approach used in service dynamic adaptation is only based on the clinician training, knowledge, instinct and experience. It allows predicting future events, to guide the type of interventions offered to the patient, to define the intensity of intervention offered to the patient and to establish an individualized care plan. The adaptive care plan includes patient care well-defined goals, pharmacological intervention, rehabilitation activities, referral to specialist, Health Promotion activities, health coaching, clinical assessments and metrics, planned encounters and follow up. It also includes results of patients’ assessments, but not self-management goals. There is ICT support in care plan delivery, follow-up and event handling. It fosters patient empowerment and self-management (in further development), facilitates
D 6.1: Service Selection Methodology Report
Public Page 70 of 88 V3.0 / 27 September 2016
remote monitoring, supports health professionals in decision making process and facilitates collaboration among professionals across healthcare levels. On-boarding the required professionals and services Primary Care and hospital professionals have access to the patient care plan. The profile of the professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation) and in care plan formulation, evaluation and follow-up are Primary Care Clinicians, Community Nurses, Specialist, Managers and Laboratory technicians. Overall, 500-700 Primary Care Clinicians, 30 Community Nurses, 10-20 Specialist, 4 Managers and 23 Laboratory Technicians are involved in the program. Awareness amongst staff is evaluated regularly and findings acted upon appropriately. Most of the healthcare professionals involved has been formally trained in case identification, case evaluation, and case selection and trained in care plan formulation, evaluation, follow-up and adaptation. Training takes place once or more every year. Healthcare professionals influence the process of change. They are involved in the design and implementation of PDSA cycles.

D 6.1: Service Selection Methodology Report
Public Page 71 of 88 V3.0 / 27 September 2016
Embrace – Connecting health and community services Description, identification and selection of patients The Embrace program has a formal risk stratification approach used to identify and select of patients at individual and population level. This risk stratification approach is fully implemented, and annually assessed. A descriptive method is used to formal targeting, identification and selection of patient is based on rules-based thresholds for certain parameters or pre-established decision criteria that describe a high-risk patient. The Population Risk Stratification tool used is the Intermed-SA-E and the Groningen Frailty Indicator (GFI). Healthcare professionals can identify individual stratified patients on their health records and can edit and modify the stratified patients. The re-stratification frequency is between 1 to 12 months. Inclusion criteria comprises elderly over 75, living at home or in an elderly home. Patients with long-term stay in nursing home, receiving an alternative type of integrated care are excluded. Between 51 to 75% of patients identified are finally included in the program. Diagnosis, severity, patient-level clinical requirements and specific characteristics are it taken into account to assess specific patient´s needs (case evaluation). Services responding to patients needs Different care levels intervene depending of the group risk. There is an individualized care plan that dynamically changes according to the evolution of the patient. Diagnosis, severity, patient-level clinical requirements and specific characteristics are taken into account to match specific interventions to the patient´s needs. Proactive shared care planning is based on risk stratification patient selection, according to patient-level clinical requirements. It includes Care management if required, self-management programs and follow-up, with goals agreed with patient and stakeholders involved, ensuring a patient-centred care plan, including changes when required (Personalized care plan). The frequency of the planned interventions revisions to match patient changing needs is between 1 to 12 months. Service dynamic adaptation is based on predictive models that seek to establish relationships between sets of variables to predict future outcomes, events or healthcare expenditure, using statistical and machine learning methods. It predicts future events, guides the type of interventions offered to the patient, define the intensity of intervention offered and establish an individualized care plan. This care care plan includes patient care well-defined goals, pharmacological interventions, nursing care, rehabilitation activities, medical Devices and appliances, referral to specialist, health Promotion activities, health, social care, community resources, clinical assessments and metrics, planned encounters and follow up and logistic support. It includes results of patient´s assessments, self-

D 6.1: Service Selection Methodology Report
Public Page 72 of 88 V3.0 / 27 September 2016
management goals agreed by healthcare professionals and patient, and patient follow-up. There is ICT support in care plan delivery, follow-up and event handling. It fosters patient empowerment and self-management, supports health professionals in decision making process, facilitates collaboration among professionals across healthcare levels and facilitates collaboration among healthcare and social-care. On-boarding the required professionals and services Primary Care, Hospital and social professionals have access to the patient care plan. The professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation) are Primary Care Clinicians, Community Nurses, Specialist and Social workers. The same professionals are involved in care plan formulation, evaluation, follow-up and adaptation. Overall, the number of healthcare professionals involved in the program is 40 Primary Care Clinicians, 20-30 Community Nurses, 10-15 Specialists and 20-30 social workers. Awareness amongst staff is evaluated regularly and findings acted upon appropriately. Most of the healthcare professionals involved have been formally trained in case identification, case evaluation, and case selection and in care plan formulation, evaluation, follow-up and adaptation. Training is continuous. Healthcare professionals influence the process of change. They can modify the selected stratified patients; can choose a wide range of patient care options to meet patients’ needs. They are involved in training or supporting their colleagues. There is a strategy to share good practices or outcomes and they are involved in the design and implementation of PDSA cycles.

D 6.1: Service Selection Methodology Report
Public Page 73 of 88 V3.0 / 27 September 2016
Heart Failure Programme Description, identification and selection of patients The Congestive heart failure (CHF) program has a formal risk stratification approach used to identify and select of patients, at individual level. It is fully implemented. A descriptive method is used to formal target, identify and select patients, based on rules-based thresholds for certain parameters or pre-established decision criteria that define high-risk patients. There is no Population Risk Stratification tool, only NYHA classification is used (individual clinical assessment). Healthcare professionals can identify stratified patients on their health records. They can edit and modify the stratified patients. Inclusion criteria comprises patients who were in New York Heart Association (NYHA) class II–IV, were in a stable condition, had good command of the Dutch language, in possession of a television set. Patients who were unable to provide informed consent were excluded from the study are excluded. Less that <25% of the identified patients are finally included in the program. Diagnosis, severity, patient-level clinical requirements, specific characteristics are variables taken into account to assess specific patient´s needs. Services responding to patients needs Different care levels intervene depending of the group risk. There is an individualized care plan that dynamically changes according to the evolution of the patient. Diagnosis, severity, patient-level clinical requirements, and specific characteristics are the variables taken into account to match specific interventions to the patient´s needs. There is a proactive shared care planning based on risk stratification patient selection, according to patient-level clinical requirements, including care management if required, self-management programs and follow-up. There are goals agreed with patient and stakeholders involved, ensuring a patient-centred care plan, including changes when required (Personalized care plan). Planned interventions revisions to match patient changing needs are continuous. The service dynamic adaptation uses a descriptive method based on rules-based thresholds for certain parameters or pre-established decision criteria that describe a high-risk patient. It predicts future events, guides the type of interventions offered to the patient, define the intensity of intervention offered and establish an individualized care plan. The adaptive care plan includes patient care well-defined goals, pharmacological interventions, nursing care, rehabilitation activities, medical devices and appliances, referral to specialist, surgical procedure, health Promotion activities, health coaching, social care, community resources, clinical assessments and metrics and planned encounters and follow up. It also sncludes results of patient´s self-assessments, goals agreed by healthcare professionals and patient, and patient follow-up.

D 6.1: Service Selection Methodology Report
Public Page 74 of 88 V3.0 / 27 September 2016
There is ICT support in care plan delivery, follow-up and event handling as it fosters patient empowerment and self-management. It facilitates remote supervision/monitoring and supports health professionals in decision making process. On-boarding the required professionals and services Primary Care and hospital professionals have access to the patient care plan. The professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation)are Primary Care Clinicians, Community Nurses, Specialist and Hospital Nurses. These same professionals plus Researchers are involved in care plan formulation, evaluation, follow-up and adaptation. Overall, the number of healthcare professionals involved in the program is 10-15 Primary Care Clinicians, 1-2 specialist, 1-3 Hospital Nurses. Awareness amongst staff is evaluated regularly and findings acted upon appropriately. Most of the professionals involved have been formally trained in case identification, case evaluation, and case selection and in care plan formulation, evaluation, follow-up and adaptation. Both trainings are continuous. Healthcare professionals influence the process of change as they are involved in the design and implementation of PDSA cycles.

D 6.1: Service Selection Methodology Report
Public Page 75 of 88 V3.0 / 27 September 2016
COPD telemonitoring services Description, identification and selection of patients COPD telemonitoring program has a formal risk stratification approach used to identify and select of patients but an individual clinical assessment that is defined but not extensively used. Targeting, identification and selection of patients are based on clinician training, knowledge, instinct and experience. For COPD programs there are no inclusion/exclusion criteria. Each professional decides in partnership with patient and carer if it is suitable. Most of the patients identified are finally included in the program. The variables that are taken into account to assess specific patient´s needs (case evaluation) are diagnosis, severity, patient-level clinical requirements and specific characteristics. Individual professional will assess patient holistically as to their suitability for telemonitoring. This relates to cognitive and functional status; family support; and ability to install equipment in patient’s home (need telephone line). Services responding to patients needs The Program defines different interventions according to different levels of risks in the target Population Group. Different care levels intervene depending of the group risk. There is an individualized care plan that dynamically changes according to the evolution of the patient. The variables that are taken into account to match specific interventions to the patient´s needs are diagnosis, severity, patient-level clinical requirements and specific characteristics. There is a proactive shared care plan that includes goals agreed with patient and stakeholders involved, ensuring a patient-centred care plan, including changes when required. It is continuously reviewed to match patient changing needs (service dynamic adaptation), based on clinical criteria, that guides the type of interventions offered to the patient. The adaptive care plan includes patient care well-defined Goals, nursing care and rehabilitation activities. It also includes results of patient´s assessments, self-management goals agreed by healthcare professionals and patient, and patient follow-up. There is ICT support in care plan delivery, follow-up and event handling as fosters patient empowerment and self-management, facilitates remote supervision, supports health professionals in decision making process, and facilitates collaboration among professionals across healthcare levels and between healthcare and social-care. On-boarding the required professionals and services Primary Care and hospital professionals have accessibility to the patient care plan. Specialist nurses in respiratory diseases are the professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case

D 6.1: Service Selection Methodology Report
Public Page 76 of 88 V3.0 / 27 September 2016
evaluation, and in care plan formulation, evaluation, follow-up and adaptation. Overall, 55 community Nurses are involved in the program. Awareness amongst staff is evaluated regularly and findings acted upon appropriately. Most of the healthcare professionals involved have been formally trained in case identification, case evaluation, and case selection and in care plan formulation, evaluation, follow-up and adaptation. Both trainings are continuous. Healthcare professionals influence the process of change. They can choose a wide range of patient care options to meet patients’ needs. They are involved in training or supporting their colleagues, there is a strategy to share good practices or outcomes and there are formal participation mechanisms to develop or change the intervention.

D 6.1: Service Selection Methodology Report
Public Page 77 of 88 V3.0 / 27 September 2016
Diabetes telemonitoring services Description, identification and selection of patients Diabetes telemonitoring program has no formal risk stratification approach to identify and select of patients. A risk stratification approach is defined but not implemented. Individual patients are identified and selected based on clinician training, knowledge, instinct and experience. There are no explicit inclusion/exclusion criteria. The professional decides in partnership with patient and carer if it is suitable. Most of the patients identified are finally included in the program. The variables take into account to assess specific patient´s needs (case evaluation) are diagnosis, severity, patient-level clinical requirements and specific characteristics. Services responding to patients needs The Program defines different interventions according to different levels of risks. There is an individualized care plan that dynamically changes according to the evolution of the patient. The variables take into account to match specific interventions to the patient´s needs are diagnosis, severity, patient-level clinical requirements and specific characteristics. There is a proactive shared care plan that includes goals agreed with patient and stakeholders involved, ensuring a patient-centered care plan, including changes when required. Is is continuously reviewed to match patient changing needs (service dynamic adaptation), based on clinical criteria, that guides the type of interventions offered to the patient. The adaptive care plan includes patient care well-defined Goals, nursing care and rehabilitation activities. It also includes results of patient´s assessments, self-management goals agreed by healthcare professionals and patient, and patient follow-up. There is ICT support in care plan delivery, follow-up and event handling as fosters patient empowerment and self-management. It facilitates remote supervision, supports health professionals in decision making process, and facilitates collaboration among professionals across healthcare levels and between healthcare and social-care. On-boarding the required professionals and services Primary Care and hospital professionals have accessibility to the patient care plan. Specialist nurses for diabetes are the professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation, and in care plan formulation, evaluation, follow-up and adaptation. Overall, 35 community Nurses are involved in the program. Awareness amongst staff is evaluated regularly and findings acted upon appropriately. Most of the healthcare professionals involved that has been formally trained in case identification, case evaluation, and case selection and in

D 6.1: Service Selection Methodology Report
Public Page 78 of 88 V3.0 / 27 September 2016
care plan formulation, evaluation, follow-up and adaptation. Both trainings are continuous. Healthcare professionals influence the process of change. They can choose a wide range of patient care options to meet patients’ needs, are involved in training or supporting their colleagues, there is a strategy to share good practices or outcomes and there are formal participation mechanisms to develop or change the intervention.

D 6.1: Service Selection Methodology Report
Public Page 79 of 88 V3.0 / 27 September 2016
Weight management telemonitoring services Description, identification and selection of patients This program has no formal stratification tool. To target, identify and select patients, an individual clinical assessment is used. There are well-defined clinical criteria that uses rules-based thresholds for certain parameters or pre-established decision criteria that describe a high-risk patient. It is not fully implemented yet. Most of the patients identified are finally included in the program. Patient needs evaluation take into account diagnosis, severity and patient-level clinical requirements. Services responding to patients needs Different care levels intervene depending of the group risk. There are no specific workflows defined for different risk groups. There is an individualized care plan that dynamically changes according to the evolution of the patient. The care plan takes into account diagnosis, severity, patient-level clinical requirements and specific characteristics (weigh monitoring). This care plan is reviewed continuously to match patient’s need, based on clinical criteria. It guides the type of interventions offered to the patient. The adaptive care plan includes patient care well-defined goals, health promotion activities, includes results of patient´s assessments, self-management goals agreed by healthcare professionals and patient, and patient follow-up. There is ICT support in care plan delivery, follow-up and event handling. It facilitates patient empowerment and self-management, remote supervision, supports health professionals in decision making process, collaboration among professionals across healthcare levels and social-care. On-boarding the required professionals and services The patient care plan is accessible to Primary Care and hospital. Midwives and dietician for WTHP are the professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation). They are also the ones involved in care plan formulation, evaluation, follow-up and adaptation. The professionals involved in the program are 20 midwives and 5 dieticians healthcare professionals involved in the program. The awareness of staff is evaluated regularly and actions are taken properly upon findings. Most of the professionals involved have been trained in case identification, case evaluation, and case selection and in care plan formulation, evaluation, follow-up and adaptation. Those trainings are continuous. Healthcare professionals influence the process of change as they can choose a wide range of patient care options to meet patients’ needs. There are formal participation mechanisms to develop or change the intervention. They are

D 6.1: Service Selection Methodology Report
Public Page 80 of 88 V3.0 / 27 September 2016
involved in training or supporting their colleagues and there is a strategy to share good practices or outcomes.

D 6.1: Service Selection Methodology Report
Public Page 81 of 88 V3.0 / 27 September 2016
Centre for Telepsychiatry Description, identification and selection of patients Centre for Telepsychiatry Program has no risk stratification approach used to identify and select of patients. There is a self-referral system where patients refer themselves to telepsychiatric services. No formal targeting, identification and selection of patient clinical criteria is used. Inclusion criteria comprise age over 18 years old and DSM-IV diagnostic criteria. Only minimally or moderately depressed enter the service. To assess specific patient´s needs (case evaluation) the MINI International Neuropsychiatric 5.0 interview is used. Services responding to patients needs The telepsychiatric service follows guidelines, individualised for each patient, according to the professionals’ monitoring and contact with the patients. There are specific clinical decisions according to patient´s evolution but not a formal care plan. Diagnosis and severity are taken into account to match specific interventions to the patient´s needs. To match patient changing needs, service dynamic adaptation is continuous. It is based on the clinician training, knowledge, instinct and experience to predict future events. The adaptive care plans includes planned encounters and follow up. There is ICT support in care delivery, follow-up and event handling. It fosters patient empowerment and self-management, facilitates remote supervision, supports health professionals in decision making process and facilitates collaboration among professionals across healthcare levels. On-boarding the required professionals and services Primary Care Clinician or nurse or specialist can have access to the patient care plan. The professionals involved in the identification of potential candidates (case identification), inclusion into the program (case selection) and assessment of clinical requirements (case evaluation) are psychologist or psychiatrist. The same professionals are involved in care plan formulation, evaluation, follow-up and adaptation. Awareness amongst staff has not been evaluated. Healthcare professionals influence the process of change. There is a strategy to share good practices or outcomes.

D 6.1: Service Selection Methodology Report
Public Page 82 of 88 V3.0 / 27 September 2016
3. Conclusions Description, identification and selection of patients In a population approach, Service Selection drives the identification of population risk strata through risk stratification, and the allocation of structured health programs targeted to a specific population group according to their risk strata. At individual clinical level, Service Selection aims to an adaptive personalized case management. It defines individualized care plans for patients with different individual risks and care needs, under the umbrella of the above mentioned structured health programs.
The question is whether having a population approach will benefit those programs with just an individual assessment. Population-based health risk assessment may be able to identify patients that are not in the radar of heath care organizations, so is potentially a facilitator of large-scale deployment of integrated care services. In the programs that are currently using risk-stratification tools, other questions may arise. Those the re-stratification period have any influence on the outcomes

D 6.1: Service Selection Methodology Report
Public Page 83 of 88 V3.0 / 27 September 2016
of the program? Would it be desirable to invest on more frequent re-stratification? Is there any characteristic that would help us to do so? The proportion of patients included on the program among those identified it depends on the population targeted on the operational process and the service selection approach. Inclusion and exclusion criteria respond to clinical situation that the program deals with. They cannot be generalized and depend on the scientific evidence. The number of variables assessed on the case evaluation will help later on in the development of an individualized integrated care plan for patients. Case evaluation should assess all relevant variables to ensure that services respond to patients needs in an integrated way.
• Can a service selection population approach improve the description, identification and selection of patients on those programs with just an individual assessment?
• Would the re-stratification period have any influence on the outcomes of the program? Would it be desirable to invest on more frequent re-stratification? Is there any characteristic that would help us to do so?
• Case evaluation assesses all variables that are needed for an integrated care plan formulation?

D 6.1: Service Selection Methodology Report
Public Page 84 of 88 V3.0 / 27 September 2016
Services responding to patients needs Most programs declare to have individualized care plans that changes according to the evolution to the patient, what is something highly desirable. All programs declare to have organized care, including coordination between primary and specialist care. Most of them declare to have goals agreed with patients and all stakeholders, and a share individualized care plan that are changed when required. Programs adapt dynamically their services to tie patient’s needs, for that a formal risk assessment is done with a variable periodicity. Most of the programs declare to adapt their intervention to match patient changing needs in a regular basis, which seems quite sensitive.
There is not a formal method for adaptation of the care plans to the patients’ needs. In most of them, these changes are based just on clinical criteria, based on their own knowledge and experience. However some of the programs use more formal methods, like rules-based thresholds, predictive tools, o a mix of them to do these changes. Would programs benefit for a more formal approach? All programs have a wide range of interventions that are defined according to the patient’s needs. Programs’ interventions cannot be generalized, as they depend on the heath area that they cover. Insolvent of the patient in the care plan is considered in most programs, including patient’ self-assessment and agreed goals. Programs may benefit of a higher patient involvement level.

D 6.1: Service Selection Methodology Report
Public Page 85 of 88 V3.0 / 27 September 2016
ICT support is generally established in most programs, supporting patient empowerment, monitoring and facilitating health professionals’ decision making coordination. Coordination between health and social professionals, when it happens, it is also facilitated by ICT.
• Would a more formal method to assess patients’ changing needs facilitate service dynamic adaptation?
• To what extend a risk stratification approach will facilitate the adaptive care plans management?
• Would programs that not consider patient involvement in the care plan benefit to do so?

D 6.1: Service Selection Methodology Report
Public Page 86 of 88 V3.0 / 27 September 2016
On-boarding the required professionals and services The professionals and services involved vary between programs. All professionals and services involved should have accessibility to the patient care plan.
It should be asses what will be the increase of professionals if the programs will be up-scaled to wider populations. Awareness evaluations seem to be issue in program development; in fact most of the programs evaluate it and act upon findings. The benefits to do so should be considered by those programs that do not do it. Programs that declare to assess awareness, declare to carry out training in in case identification, case evaluation, and case selection, but also in care plan formulation, evaluation, follow-up and adaptation. The question is whether those that do not asses awareness will do these trainings too, and what will be the benefit to do so. On-going training takes place in most programs. Heath care professionals can influence what happens in care deployment. They decide on the care services that patients get, and they are involved in training process and share good practices and outcomes amongst them. Although they are no participating so much in the formal change mechanisms in the programs, as for example de PDSA cycles that can be organized.
• Would programs benefit of a formal strategy to involve the required professionals and services in the scaling-up scenario?
D 6.1: Service Selection Methodology Report
Public Page 87 of 88 V3.0 / 27 September 2016
• Does the professionals’ awareness (in case identification, case evaluation, and case selection, and service dynamic adaptation) facilitate program scaling-up?
• Would program benefit of involving health professionals in formal change mechanisms?

D 6.1: Service Selection Methodology Report
Public Page 88 of 88 V3.0 / 27 September 2016
Annex