definitions -...
TRANSCRIPT

1
CELLULAR ADAPTATIONS OF GROWTH &
DIFFERENTIATION
• Departemen Patologi Anatomi FakultasKedokteran Universitas Sumatera Utara Medan
Definitions
• Pathology is a dicipline bridging clinical
practice & basic sience
• To render diagnosis & guide therapy
• Identity changes in :
– Gross
– Morphology (microscopy) appearance of cell
tissues

2
The scientific focus of pathology is :
Etiology
• On the cause of disease
Pathogenesis
• Mechanisme of its development & the pathways by which morphologic changes
occur
Normal Homeostasis
If cell adjusting structure & function
to accommodate changing demands &
extracellular stresses
3
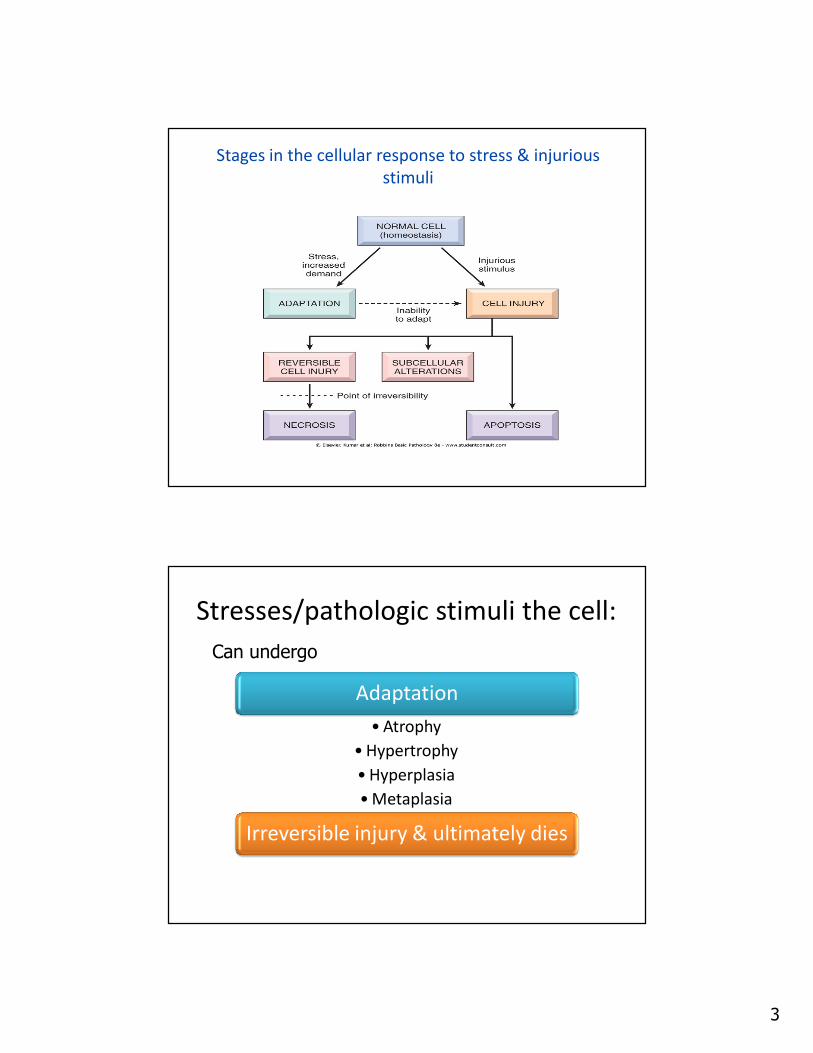
Stages in the cellular response to stress & injurious
stimuli
Stresses/pathologic stimuli the cell:
Adaptation
• Atrophy
• Hypertrophy
• Hyperplasia
• Metaplasia
Irreversible injury & ultimately dies
Can undergo

4
Perubahan sel & jaringan :
Agenesis
Aplasia
Hypoplasia
Atrophy
Hypertrophy
Hyperplasia
Metaplasia
Dysplasia
Anaplasia
Granuloma
• Complete absent of an
organ
• E.g. :
– Renal agenesis
– Ovarial agenesis
– Tubal agenesis, etc.
Agenesis Aplasia
• Anlarge is present but
never develops
• E.g. :
– Lung aplasia with tissue
containing rudimentary
duct & connective tissue

5
• Anlarge develoved incompletly but the tissue
histhologicaly normal
• Ex. : microcephaly
Hypoplasia
• Decrease in the:
– Size
– Function of a cell
• But not dead
Atrophy

6
Causes of atrophy :
1. ↓ functional demand (immobilitation in fracture, prolonged
bed rest)
2. Inadequate supply O2 (ischemia)
3. Insufficient nutrients (starvation, inadequate nutrition,
chronic disease)
4. Interrruption of trophic signals transmitted by chemical
mediators (endocrine system/Neuromusculator transmission)
e.g. : thyroid, adrenal cortex, ovarium, testis.
5. Persistent cell injury by chronic inflamation
e.g. : chronic gastritis, prolonged pressure
6. Aging : brain, heart (Senile Atrophy)
Atrophy The adjacent image is a section of heart muscle (myocardium). The spaces between muscle fibers are not present in normal myocardium. The muscle fibers are thinner than normal creating spaces between them, a finding suggesting atrophy.

7
The mechanism of atrophy :
• ↓ synthesis
• ↑ catabolism
• Influenced by a number of hormones
e.g. :
• Insulin
• Tyroid stimulating hormon
• Glucocorticoids
• ↑ in the size of cell accompanied by augmented functional capacity
• Hypertrophy is a response to trophic signals
• Commonly a normal procesess
Hypertrophy

8
… hypertrophy
Physiological (hormonal) hypertrophy
• in puberty
• ↑ production of sex hormon
• Hypertrophy breast tissue
• Abnormal hormon production in cancer
↑ Functional demands
• Exercise
• Pathological conditions (myocardial cell)
• Kidney hypertrophy on surgical removed
Hypertrophy Here is another section of myocardium in an area adjacent to a healed myocardial infarct ("heart attack"). Since cardiac muscle cannot regenerate, fibrous connective tissue fills in the defect. Nearby viable muscle cells increase in size to compensate for cells that died. In this section enlarged nuclei indicate that the cells have undergone hypertrophy (increase in volume of cells).
Hypertrophy At higher magnification, the enlargment of cardiac muscle cells and nuclei is apparent. Since cardiac muscle cells cannot divide, they adapt by increasing their size (hypertropy).

9
Hyperplasia
↑ the number of cells in an organ / tissue
1. Physiologic hyperplasia
– Hormonal hyperplasia
– Compensatory hyperplasia
2. Pathologic hyperplasia
– Excessive hormonal / growth factor stimulation
e.g. : Endometrial hyperplasia
Hyperplasia can be :

10
1. Hormonal stimulation• ↑ Estrogen endometrium (hyperplasia)
• Gynecomastia
2. Increased functional demand- secondary polycytemia- lymphocyte hyperplasia
3. Persistent Cell Injury- chronic inflammation in the skin and
the epi –thelium of viscera
- hyperplasia of the bladder epithelium
Metaplasia
Reversible change in which 1 adult cell type is replace by another
adult cell type (convertion of 1 differentiated cell type of
another)
Metaplasia is usually reversible if the stimulus is
removed
• Squamous metaplasia of the bronchial epithelium to tobacco
• Lower oesophagus by reflux acidic gastric
• Endocervical metaplasia
Most common is the replacment of a glandular epithelium by a squamous cell.

11
Metaplasia of normal columnar (left) to squamous epithelium
(right) in a bronchus, shown (A) schematically and (B)
histologically
Cellular alteration in the size, shape & organization of the cellular component of a tissue
1. Variation in the size & shape of cells
2. Enlargment, irregularity & hyperchromatism of the
nuclei
3. Disorderly arrangement of the cells within the
epithelium
Dysplasia
The most common in the cervix & bronchus

12
Dysplasia included in the morphological classification of the
stage if intraepithelial neoplasia
Dysplasia is a preneoplastic lession in the sense
that it is a necessary stage in the multistep cellular
evolution to cancer.
• Normal cell � primitive cell
• E.g. : Malignant cell
– Carcinoma
– Sarcoma
– Adenocarcinoma
– Lymphoma
– Etc.
Anaplasia

13
2 principal pattern of cell death :
• Commonly : coagulative necrosis
• Cellular swelling
• Protein denaturation
• Organellar breakdown
• Cell rupture
NECROSIS
• Regulated event
• Programmed deathAPOPTOSIS

14
Term Definition
Necrosis Antemortem pathologic cell death
Apoptosis Antemortem programmed cell death
Autolysis Postmortem cell death
CAUSES OF CELL INJURY
Hypoxia
Physical Agent
Chemical and drugs
Microbiology Agents
Immunologic Reaction
Genetic Defects
Nutritional Inbalance
Aging

15
• Anemia
• Ischemia
• Intoxication CO2
• Aerobic oxidative
respiration
• Mechanical trauma
• Extreme temprature :
heat, cold
• Radiation: X-ray, sun light
• Electric shock
• Athmosphere pressure
Hypoxia Physical Agent
… CAUSES OF CELL INJURY
• Sufficiently concentrated :
– Glucose
– Salt
– O2
• Air pollutants
• Insecticides
• Asbestosis
• Ethanol
• Cellular metabolism (i.e.
waste products)
• Tape worms
• Rickettsia
• Virus
• Bacteria
• Fungi
… CAUSES OF CELL INJURY
Chemical agent & drugs Microbiology Agents

16
… CAUSES OF CELL INJURY
• Anaphylactic reaction
• Autoimmune diseases
Immunologic Reaction
Genetic Defects
• Congenital malformation
• Sickle cell anemia
• G-6-PD
Nutritional Imbalance
• Protein calori insufficiency
• Vitamins defficiency
• Diabetes
Aging

17
Cellular
response to
injurious
stimuli
depends on :
• Injury type
• Duration
• Severity
Current
Status :
• Nutritional
• Hormonal
• Adaptibilityof the cell
Intercellular
systems :
• Cell membrane integrity
• Aerobic respiration
• Protein synthesis
• Integrity genetic apparatus
O2 & oxygen
derived free
radicals :
• Ischemic
• Hypoxic injury
Mechanism of Cell Injury
The ultrastructural features of these stages of cell injury.
Normal cell & changes in reversible & irreversible cell injury
(necrosis)

18
• Reduced of :– Oxidative
phosphorylation in
mitochondria
– Activity Na Pump
• Cellular swelling
• Loss of microvilli� Glycogen depleted
� ↓ protein synthesis
� Formation of cell surface
blebs
• Severe vacuolization of
the mitochondria
• Damage of :
– Mitochondrial matrix
– Plasma membrane
• Swelling of lysosomes
• Accumulation of
amorphous calcium
• Rich dentities in
mitochondrial matrix
Reversible injury Irreversible injury

19

20
Figure 1-6.
Cellular features of
necrosis (left) &
apoptosis (right)
1. Reversible acute cell injury
2. Necrosis (cell death after irreversible injury)
3. Apoptosis (cell death by suicide)
4. Subcellular alteration as a respond to chronic
or persistent injury stimuli
5. Intracellular accumulations of a number of
substance
Forms & Morphology of Cell Injury

21
Sublethal Damage
1. Recoverable (but � necrosis is not)
2. Ultrastructural damage mitochondria
3. Swelling of cellular organelles ( hydrophic deg.)
4. Fatty change is impairment of metabolism
Morphologic changes that follow cell death in living tissue
1. Intense eosinophilia of the dead cell is due to loss of RNA & coagulation of protein
2. Nuclei undergo: 1. Pyknosis
2. Karyorhexis
3. Karyolysis
� Leaving a shrunken cell devoid of nucleus
1. Protein may be liberated from the dead cell
Necrosis

22
The morphologic appearance of necrosis isthe result of two essentially processes :
1. Enzymatic digestion of the cell2. Denaturation of protein
Autolysis : is a cell death by hydroliticenzymes.
Heterolysis : cell death by the lysosomes of invading inflammatory cells.
Nuclear Changes: This nucleus is faded -- karyolysis.
Karyolytic nuclei suggest that cells have died (undergone necrosis).

23
Nuclear Changes: Pyknosis While cytoplasmic changes associated with cell death are not specific, nuclear changes are. The large arrow indicates a normal-appearing nucleus while the smaller arrow indicates a nucleus that is small and dark -- features of "pyknosis." Pyknotic nuclei suggest that cells have died (are undergoing necrosis).
Fragmented nuclei suggest that cells have died. Karyorrhexis is the term used for this circumstance. The nucleus indicated by the large arrow may be undergoing karyorrhexis. The smaller arrow indicates a fragmented nucleus: it could be karyorrhexis or a mitotic figure (a cell undergoing mitosis).

24
Types of Necrosis
Depends on :
1. Cells compotitions
2. Speed of necrosis
3. Type of injuries

25
• Implies preservation of basic structural outline of the coagulated cell / tissue for a span of days.
• The structural protein and the enzymatic protein thus blocking cellular proteolysis
• Coagulation necrosis is cahareteristic of hypoxic death of cells in all tissue except the brainE.g. : Myocardial Infarction (occlusion of arterial supply )
Coagulative Necrosis
• Liquefactive/Colliquativa Necrosis• Dead tissue that appears semi liquid as a result of dissolution of tissue by the action of hydrolytic enzymes
• E.g.: cerebral infarction, necrosis caused by bacterial inf.
• Caseous Necrosis• Dead cell form an amorphous proteinaceaus mass, no original architecture can be seen histologically(soft & white resembling cream cheese)
• Most often in fact of tuberculous infection with central necrosis

26
• Gumatous Necrosis
• Dead tissue, it is firm & rubbery like caseous necrosis in the
spirochetal infection syphilis.
• Hemorrhagic Necrosis
• Dead tissue suffused with extravasated red cell, when cell
death is due to blockage
• Fat Necrosis
• Not really necrosis.
• Focal areas of fat destruction tipically occuring following
pancreatic injury /after trauma to fat for (ex. in the breast)
• Describes foci of hard yellow material seen in dead adipose
tissue
• Fibrinoid Necrosis
• Fibrin deposited in damage necrotic vessel
walls in hypertension and vasculitis
• Gangrene
• Extensive tissue necrosis ; is complicated to
a variable degree by secondary bacterial
infection

27
APOPTOSIS• Responsible for the programmed cell death in several
important physiology processes
• Including :
– During embryogenesis (in implantation, organogenesis, &
developmental involution)
– Hormon dependent physiologic involution (endometrium,
lactating, prostate after castration)
– Cell deletion in proliferating population (intestinal crypt
epithelium / cell dead in tumor)
– Deletion of autoreactive T cell in the thymus,
cell death of cytokine starved lymphocytes
CLINICAL EFFECTS OF NECROSIS
• Abnormal function
– Kidney : renal failure
– Cortex in brain : muscle paralysis
– Heart : heart failure
– Lung : hemoptysis
– Bacterial infection : gangrene

28
• Realease of contens of necrotic cells
– Liver : elevation SGOT
– Heart : creatine kinase
• Systemic effects
– Fever
– Inflamatoar Reaction
• Local effects
– Hemorrhage
– Ulceration
Apoptosis of epidermal cells in an immune-
mediated reaction
A. Apoptotic cells are visible in the
epidermis with eosinophilic cytoplasm
and small, dense nuclei.
B. High power of apoptotic cell in liver in
immune-mediated hepatic cell injury.
(Courtesy of Dr. Scott Granter, Brigham and Women's Hospital, Boston, AM.) (Courtesy of Dr. Dhanpat Jain, Yale University, New Haven, CT.)

29
CELLULAR ADAPTATIONS OF GROWTH ANDDIFFENTIATION
Environment adaptation of the cell1. Physiologic Adaptation
- Hormones- Endogenous chemical mediators
2. Pathologic Adaptation- Induction of new protein synthesis by target cell
Cell Injury :• Death of cells ( permanent organ injury )• Sublethal injury ( adaptation )
Granuloma
• Special type of chronic inflamation in tissue
reaction.
• Cause :
infection : TBC fungal syphilis,
etc
non-
infection :sarcoidosis
Crohn’s
disease

30
NECROBIOSIS
• Gradual cell damage
• Progressive
• Singly or small group cells.
• Reversible (+/-)
• Example : hepar cell � deg.
cell death � healing � fibrosis.
Alterations in structure and function that may
lead to cell death, or at least diminished capacity
of the cell to respond an injury
CELLULAR AGING
• Reduced cell in :
– Pleomorphic vacuolated mitochondria
– Repair of chromosomal damage

31
… CELLULAR AGING
Morphologic alteration in :
• Pleomorphic vacuolated mitochondria
• ↓ endoplasmic reticulum
• Disorted Golgi Apparatus
• Accumutaion of lipofuscin pigment
Cellular senescence is multifactorial :
1. The cumulative effects of extrinsic influences:
free radical damage
2. Intrinsic molecular program of cellular aging
cell have a finite life span

32
DEGENERATION
Cloudy swelling
Fatty change
Hydropic Atropy
Hyaline Mucoid AmyloidCalcifica-
tion
Ballooning degeneration

33
Hydropic change of gestational mole
Fatty Change At higher magnification the intracytoplasmic fat droplets are clearly evident.

34
Hyaline Droplet Degeneration Sometimes protein droplets appear within the cy_toplasm of sick cells. These droplets appear homogeneous, glassy, bead-like structures -- an apearance known as "hyaline.”
THANK YOU
SELAMAT BELAJAR
O1

Slide 68
O1 Owner, 11/20/2009