deferasirox for the treatment of iron overload in non-transfusion-dependent thalassemia
TRANSCRIPT
Deferasirox for the treatmentof iron overload innon-transfusion-dependentthalassemiaExpert Rev. Hematol. Early online, 1–15 (2013)
Ali T Taher*1,Sally Temraz1 andM DomenicaCappellini2
1Department of Internal Medicine,
American University of Beirut, Riad El
Solh 1107 2020, Beirut, Lebanon2Universita di Milano, Ca Granda
Foundation IRCCS, Milan, Italy
*Author for correspondence:
Tel.: +9611350000
Fax: +9611370814
Non-transfusion-dependent thalassemia (NTDT) defines a group of patients who do notrequire regular transfusions for survival, but are at significant risk of iron accumulation fromunderlying disease-related mechanisms distinct from transfusional iron overload. Managementof iron overload in NTDT has received little attention compared with that of b-thalassemiamajor, despite evidence of significant iron-induced complications with advancing age. Theefficacy and safety of the iron chelator deferasirox in NTDT has been evaluated in two pilotstudies and the first prospective, randomized, placebo-controlled study (THALASSA) of anychelator in NTDT. Treatment with deferasirox for up to 2 years yielded a sustained reductionin iron burden, with a clinically manageable safety profile. Following these trial data,deferasirox is the first iron chelator approved for use in NTDT patients, and with NTDTguidelines now available, physicians are better equipped to achieve effective monitoring andmanagement of iron burden in NTDT.
KEYWORDS: deferasirox • iron chelation • iron overload • thalassemia
The a- and b-thalassemias are a group ofinherited hematological disorders character-
ized by the common underlying molecular
etiology of defective hemoglobin (Hb) a- orb-globin chain synthesis [1–4]. The conse-
quent imbalance in the normal globin chain
composition of the Hb tetramer molecule
impairs erythropoiesis and leads to anemia.
Varying degrees of dysfunction in globin
chain production (absence or reduced
synthesis) give rise to thalassemia pheno-
types with marked differences in symptom
severity and treatment requirements, from
clinically asymptomatic carriers (thalassemia
trait) to severely anemic and red blood cell
transfusion-dependent clinical presentations
(b-thalassemia major) [1–4].Non-transfusion-dependent thalassemia
(NTDT) falls between the phenotypes of tha-
lassemia trait and b-thalassemia major, and
encompasses thalassemia patients who do not
require regular transfusions for survival but
may require transfusions for situations such as
infection, pregnancy or surgery [5–7]. From a
worldwide perspective, the primary forms ofNTDT include HbH disease, HbE/b-thalasse-mia and b-thalassemia intermedia (b-TI) [6].
These disorders demonstrate a significant pres-
ence in regions spanning the Mediterranean,
Middle East, sub-Saharan Africa and Central
and South East Asia [2,6,8].HbS/b-thalassemia, one of the two addi-
tional NTDT syndromes, can be found mainly
in the sub-Saharan, Middle East, Mediterra-
nean and Indian regions. The second addi-
tional NTDT syndrome, HbC/b-thalassemia,
is restricted mainly to sub-Saharan and North
African regions [6].While the predominance of NTDT in low-
or middle-income countries is recognized,
more developed regions, such as North
Europe and the USA, have recently seen an
increasing prevalence of these conditions as a
result of population migration [2,6,9]. With
greater understanding of the disease and
improved public health, it is likely that the
awareness and hence incidence of NTDT will
increase [6,10,11].
Drug Profile
www.expert-reviews.com 10.1586/17474086.2013.827411 � 2013 Informa UK Ltd ISSN 1747-4086 1

Non-transfusion-dependent thalassemias are associated with awide-ranging clinical picture whereby patients experience symp-toms across a broad spectrum of severity [2,4,10,12–16]. This isexemplified by observations in patients with b-TI and HbE/b-thalassemia who, at one end of the disease spectrum, may dis-play a mild clinical presentation (with normal growth status),and at the other, a more severe phenotype marked by early-onset anemia and related symptoms (such as retardation ofgrowth and development and skeletal deformities) that couldultimately dictate a regular transfusion requirement [16,17]. Thepresence of genetic modifiers also contributes to the varied clin-ical description of NTDT disorders. The non-deletional formof HbH disease, for example, is associated with earlier manifes-tation of symptoms, greater anemia severity and a higher likeli-hood of transfusion requirement than deletional HbH disease(harbors one or more deletions of a-globin genes) [18].
Although NTDTs may display a milder and less clinicallydiscernible phenotype than b-thalassemia major in somepatients, this does not obviate the risk of progressively seriouscomplications with age. In fact, NTDT patients are vulnerableto a host of complications that are as significant as those seenin b-thalassemia major but nonetheless somewhat diverse fromthe latter group of patients [19,20]. Such complications inNTDT include extramedullary hematopoiesis, thromboembolicevents, pulmonary hypertension, leg ulcers, renal complications,endocrine disease and skeletal deformities and an increased riskof hepatocellular carcinoma [17,20–22].
General consensus of opinion supports chronic anemia andexcess iron loading as a primary pathophysiological cause ofclinical complications in NTDT [14,17,21,23,24]. The mechanismby which iron accumulates in NTDT differs from thatobserved in patients with b-thalassemia major [21,25], whosemain source of iron load derives from transfusion therapy.Instead, iron overload in NTDT is primarily attributed toincreased gastrointestinal iron absorption secondary to ineffec-tive erythropoiesis and chronic anemia (FIGURE 2).
In NTDT, excess iron accumulates mainly in the liver and to alesser extent in the heart, which may explain the propensity for alower occurrence of myocardial siderosis in patients withb-TI than in their b-thalassemia major counterparts [26]. However,untreated older NTDT patients remain at risk of iron-related cardiac abnormalities [27–29], potentially through exposureof cardiac tissue to non-transferrin-bound iron, as opposed to sig-nificant iron accumulation within cardiac cells [26,30]. The proposedrelationship between iron overload and clinical complications inNTDT is also borne out by studies that reveal an increased risk ofvascular, endocrine and bone disease with elevations in liver ironconcentration (LIC) over 5 mg Fe/g dry weight (dw) [24,31] and aclear association between increased risk of morbidity and serumferritin (SF) levels beyond 300 ng/ml [32]. Moreover, evidencedrawn from b-TI patients suggests a pattern of increasing compli-cations with advancing age and a coincident progressive accumula-tion of iron over time [33]. It is clear then that early monitoring andintervention are key to preventing the development of iron-induced complications in NTDT patients [21].
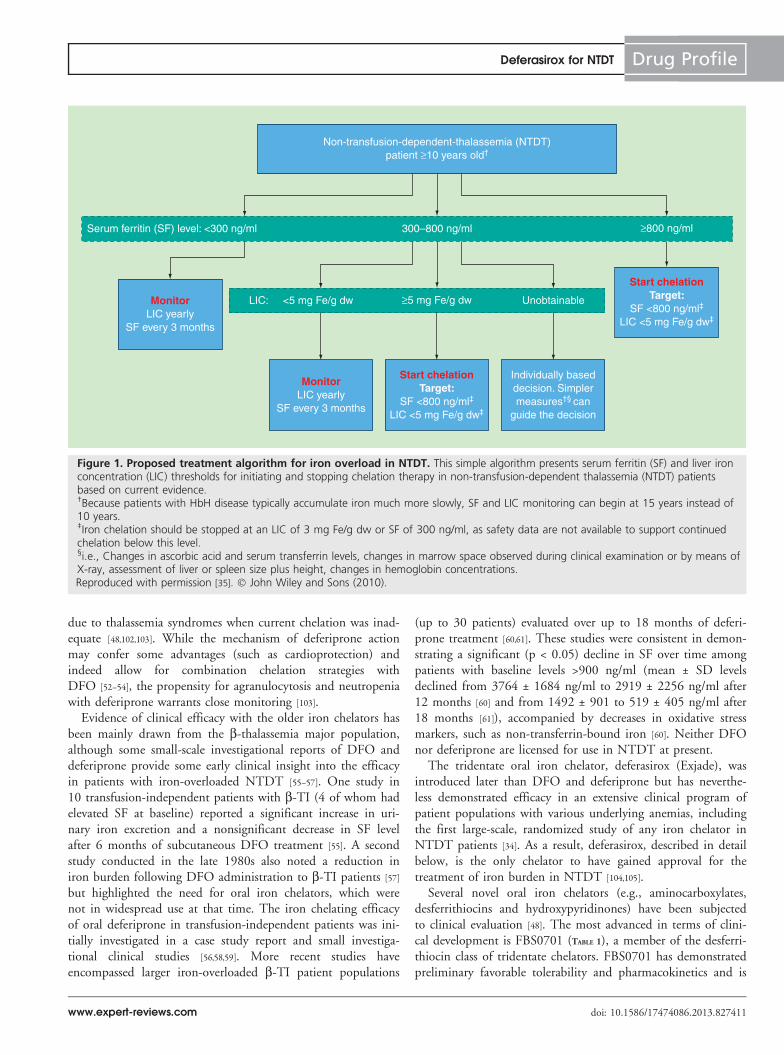
Current status of chelation treatment in NTDTThe management of iron overload in NTDT patients has mer-ited little attention until recently, with few studies on ironoverload and chelation in this group of patients. However,greater awareness of the disease process alongside emerging datafrom NTDT patients is facilitating the development of treat-ment pathways solely aligned to the NTDT patient population.Of note, recent evidence, including published data from arandomized clinical trial of iron chelation in NTDTpatients [34], has formed the basis of a novel decision-making algorithm to aid monitoring of iron burden and initia-tion of chelation therapy in NTDT patients in clinical practice(FIGURE 1) (see Expert commentary) [34,35].
The algorithm advocates monitoring of SF and LIC on amonthly and annual basis, respectively, beginning when thepatient is 10 years old, to prevent iron accumulation to poten-tially toxic levels [35]. Serum ferritin is a widely utilized, afford-able and convenient surrogate marker of total body iron [21,36].However, unlike b-thalassemia major, measurement of SF mayunderestimate the level of iron load in NTDT patients. Studieshave consistently demonstrated significantly lower SF concen-trations among patients with b-TI than with b-thalassemia major, even though LIC was comparable betweenthe two groups [37–39]. Despite this, a significant positive corre-lation has been shown to exist between SF and LIC across themain NTDT subtypes [12,38–40]. The recently developed treat-ment algorithm for iron overload in NTDT seeks to minimizethe potential for underestimation with SF by incorporatingadditional direct LIC measurements, determined throughbiopsy or a noninvasive method (such as MRI), at levels of SFbetween 300 and 800 ng/ml [35,40]. MRI is broadly consideredthe preferred method for LIC assessment as it is noninvasivewith accurate, reproducible results [41]. MRI assessment techni-ques include longitudinal (T1) and transverse (T2) tissue relax-ation times and signal intensity ratios [42–44]. The most widelyaccepted methodologies are T2* (which uses a gradient-echo sequence) [45] and R2 (=1/T2; which uses a spin-echo sequence) [43,46]. The FerriScan method for R2 hasreceived approval from the European Medicines Agency andthe US FDA.
Iron chelators bind with high affinity to iron to form a non-toxic complex that is subsequently excreted from the body.A number of iron chelators are available for the treatment ofiron overload in thalassemia patients (TABLE 1) [23,47,48]. Deferox-amine (DFO; Desferal) is a hexadentate chelator widely usedsince 1962 for reduction of iron overload in patients withtransfusion-dependent anemias [48,101]. The limitations imposedby the need for frequent and prolonged subcutaneous DFOadministration negatively impact patient compliance, with con-sequent elevated risk of iron-induced complications andincreased societal costs [49–51]. The oral iron chelator deferi-prone (Ferriprox) was first licensed in Europe in 1999 for thetreatment of iron overload in thalassemia major when DFOwas contraindicated or inadequate; it was also approved in theUSA in 2011 for the treatment of transfusional iron overload
Drug Profile Taher, Temraz & Cappellini
doi: 10.1586/17474086.2013.827411 Expert Rev. Hematol.
due to thalassemia syndromes when current chelation was inad-equate [48,102,103]. While the mechanism of deferiprone actionmay confer some advantages (such as cardioprotection) andindeed allow for combination chelation strategies withDFO [52–54], the propensity for agranulocytosis and neutropeniawith deferiprone warrants close monitoring [103].
Evidence of clinical efficacy with the older iron chelators hasbeen mainly drawn from the b-thalassemia major population,although some small-scale investigational reports of DFO anddeferiprone provide some early clinical insight into the efficacyin patients with iron-overloaded NTDT [55–57]. One study in10 transfusion-independent patients with b-TI (4 of whom hadelevated SF at baseline) reported a significant increase in uri-nary iron excretion and a nonsignificant decrease in SF levelafter 6 months of subcutaneous DFO treatment [55]. A secondstudy conducted in the late 1980s also noted a reduction iniron burden following DFO administration to b-TI patients [57]
but highlighted the need for oral iron chelators, which werenot in widespread use at that time. The iron chelating efficacyof oral deferiprone in transfusion-independent patients was ini-tially investigated in a case study report and small investiga-tional clinical studies [56,58,59]. More recent studies haveencompassed larger iron-overloaded b-TI patient populations
(up to 30 patients) evaluated over up to 18 months of deferi-prone treatment [60,61]. These studies were consistent in demon-strating a significant (p < 0.05) decline in SF over time amongpatients with baseline levels >900 ng/ml (mean ± SD levelsdeclined from 3764 ± 1684 ng/ml to 2919 ± 2256 ng/ml after12 months [60] and from 1492 ± 901 to 519 ± 405 ng/ml after18 months [61]), accompanied by decreases in oxidative stressmarkers, such as non-transferrin-bound iron [60]. Neither DFOnor deferiprone are licensed for use in NTDT at present.
The tridentate oral iron chelator, deferasirox (Exjade), wasintroduced later than DFO and deferiprone but has neverthe-less demonstrated efficacy in an extensive clinical program ofpatient populations with various underlying anemias, includingthe first large-scale, randomized study of any iron chelator inNTDT patients [34]. As a result, deferasirox, described in detailbelow, is the only chelator to have gained approval for thetreatment of iron burden in NTDT [104,105].
Several novel oral iron chelators (e.g., aminocarboxylates,desferrithiocins and hydroxypyridinones) have been subjectedto clinical evaluation [48]. The most advanced in terms of clini-cal development is FBS0701 (TABLE 1), a member of the desferri-thiocin class of tridentate chelators. FBS0701 has demonstratedpreliminary favorable tolerability and pharmacokinetics and is
Non-transfusion-dependent-thalassemia (NTDT)patient ≥10 years old†
Serum ferritin (SF) level: <300 ng/ml
LIC: <5 mg Fe/g dw Unobtainable≥5 mg Fe/g dwMonitorLIC yearly
SF every 3 months
MonitorLIC yearly
SF every 3 months
Start chelationTarget:
SF <800 ng/ml‡
LIC <5 mg Fe/g dw‡
Start chelationTarget:
SF <800 ng/ml‡
LIC <5 mg Fe/g dw‡
Individually baseddecision. Simplermeasures†§ can
guide the decision
300–800 ng/ml ≥800 ng/ml
Figure 1. Proposed treatment algorithm for iron overload in NTDT. This simple algorithm presents serum ferritin (SF) and liver ironconcentration (LIC) thresholds for initiating and stopping chelation therapy in non-transfusion-dependent thalassemia (NTDT) patientsbased on current evidence.†Because patients with HbH disease typically accumulate iron much more slowly, SF and LIC monitoring can begin at 15 years instead of10 years.‡Iron chelation should be stopped at an LIC of 3 mg Fe/g dw or SF of 300 ng/ml, as safety data are not available to support continuedchelation below this level.§i.e., Changes in ascorbic acid and serum transferrin levels, changes in marrow space observed during clinical examination or by means ofX-ray, assessment of liver or spleen size plus height, changes in hemoglobin concentrations.Reproduced with permission [35]. � John Wiley and Sons (2010).
Deferasirox for NTDT Drug Profile
www.expert-reviews.com doi: 10.1586/17474086.2013.827411

currently undergoing testing in Phase II clinical trials of patientswith transfusional iron overload [48,62–64]. At doses of up to50 mg/kg/day, FBS0701 was generally well tolerated and allowedsome patients to achieve a reduction in LIC (mean ± SD changefrom baseline to week 72 of -0.69 ± 4.98 mg Fe/g dw), indicat-ing that further dose-escalation studies should be conducted todetermine a dose at which all patients achieve a substantialreduction [65].
Deferasirox: an introductionDeferasirox was the first oral iron chelator to be licensed in theUSA for the treatment of chronic iron overload in patients withtransfusion-dependent anemias. Recently, deferasirox receivedapproval in the USA for use in NTDT patients ‡10 years of agewith an LIC ‡5 mg Fe/g dw and SF >300 ng/ml. In Europe, itis approved for use in NTDT patients with LIC ‡5 mg Fe/g dwor SF levels consistently over 800 ng/ml with inadequateresponse or a contraindication to DFO [104,105].
In NTDT patients, initiation of deferasirox is recommendedat a starting dose of 10 mg/kg/day, which may be increased toa maximum of 20 mg/kg/day after 4 weeks if the baseline LICexceeds 15 mg Fe/g dw or if LIC is >7 mg Fe/g dw after6 months. Deferasirox should be taken, dispersed in water,orange or apple juice, on an empty stomach at least 30 minbefore food. For patients receiving deferasirox, monitoring ofSF and LIC is required at monthly and 6-monthly intervals,respectively, and interruption of treatment is recommended ifSF levels decline below 300 ng/ml or if LIC drops below 3 mgFe/g dw [104]. Continuous monitoring of iron burden is neces-sary even after interruption of iron chelation to determine iflevels have risen sufficiently to restart chelation therapy.
Deferasirox offers the convenience of oral, once-daily dosingover the three-times daily dosing of deferiprone and subcutane-ous administration required for DFO which, in the absence ofunmanageable adverse events, may increase compliance inmany patients. Cost considerations could limit its widespreadavailability in regions with limited resources, although studiestaking into consideration the patient’s quality of life havedemonstrated the cost–effectiveness of deferasirox [66–68]. Othercharacteristics of deferasirox, such as the ability to access intra-cellular iron (including cardiac cells) and a long half-life, mayalso prove to be of benefit in the treatment of iron overload(for review see [69]).
Chemistry
Deferasirox is identified chemically as 4-[3,5-bis(2-hydroxy-phenyl)-1H-1,2,4-triazol-1-yl]-benzoic acid (TABLE 1), and ishighly lipophilic. Deferasirox is a tridentate ligand (molecu-lar weight 373 g/mol) that binds iron in a 2:1 ratio. Defera-sirox demonstrates an affinity and specificity for iron that isgreater than that for copper and zinc, thus reducing the like-lihood of exhaustion of these trace elements [70,104]. How-ever, variable decreases in serum concentrations of copperand zinc have been noted, the significance of which remainsunclear [104].
Pharmacodynamics
The pharmacodynamic effects of deferasirox have been observedin an iron balance metabolic study [104]. Deferasirox, at dosesof 10, 20 and 40 mg/kg/day, induces a mean net iron excretion(0.119, 0.329 and 0.445 mg Fe/kg body weight per day,respectively), which is within the clinically relevant range (0.1–0.5 mg/kg/day).
Pharmacokinetics & metabolism
The pharmacokinetics of deferasirox have been investigated inpreclinical and clinical studies [71–73,104]. After oral administra-tion, deferasirox is rapidly absorbed with a median time tomaximum plasma concentration of approximately 1.5–4 h andis distributed throughout the body with volume of distributionat steady state of 14.37 ± 2.69 L [104]. Peak concentration(Cmax) and area under the plasma concentration–time curve ofdeferasirox have been shown to increase approximately dose-proportionally after single-dose and under steady-state condi-tions [104] but deferasirox does not accumulate with multipledosing [72]. With once-daily administration, plasma levels ofdeferasirox are maintained within the therapeutic range over24 h (mean elimination half-life of 7–11 h) [72,104].
Deferasirox is approximately 99% protein-bound in vivo, vir-tually exclusively to serum albumin [104]. The metabolism andelimination processes of deferasirox in the liver and gut areschematically depicted in FIGURE 3. Deferasirox is mainly metabo-lized through glucuronidation to the metabolites M3 (acyl glu-curonide) and M6 (2-O-glucuronide) [73]. Following deferasiroxadministration, excretion of the agent and its metabolites ispredominantly fecal (84%), with renal excretion accounting forjust 8% of the administered dose [73,104].
The potential exists for drug interactions with defera-sirox [74,104]. Importantly, deferasirox should not be administeredwith aluminium-containing antacid preparations [104]. The agentmay induce cytochrome P450 (CYP) 3A4 and inhibit CYP1A2resulting in a decrease or increase in the relevant substrate, respec-tively. Therefore, deferasirox should be closely monitored forreduced effectiveness during coadministration with medicationsmetabolized by CYP3A4 (e.g., midazolam, cyclosporine, simvas-tatin) and CYP1A2 substrates with a narrow therapeutic index,such as theophylline, should be avoided during deferasiroxadministration. Additionally, lower dosing of repaglinide andpaclitaxel (metabolized by CYP2C8) should be considered if theagent is used concomitantly with deferasirox; close monitoring ofblood glucose levels is also required. Concomitant use withpotent UDP-glucuronosyltransferase inducers and bile acidsequestrants may lead to a decrease in deferasirox efficacy [104].
Clinical efficacy
To date, two small studies and one larger randomized trialhave evaluated the efficacy of deferasirox for the treatment ofiron overload in NTDT patients (TABLE 2) [34,75,76]. The studiesadopted a similar dosing design to earlier studies in patientswith transfusional iron overload, whereby dose adjustment ofdeferasirox was determined according to efficacy and safety
Drug Profile Taher, Temraz & Cappellini
doi: 10.1586/17474086.2013.827411 Expert Rev. Hematol.

Table
1.Overview
ofironch
elators
forthetreatm
entofironoverload.
Characteristic
Deferoxamine
Deferiprone
Deferasirox
FBS0701†
Chelatorproperty
Hexadentate
Bidentate
Tridentate
Tridentate
Molecularmass
(g/m
ol)
657
139
373
400
Chemicalstructure
N OH
OH
NH
N
N OH
H2N
OH
NO
O
O
O
NO
OH
CH
3
CH
3
OH
N
NN
OH
O
OH
O O
O
O
OH
N
S
O
OH
Administereddose
(mg/kg/day)
20–40(children)
40–50(adults)
75–99
20–40
Investigational3–32
Route
ofadministration
Subcutaneous/iv
8–24h;
5–7days/week
Oral
Three-tim
esdaily
Oral
Once-daily
Oral
Once-daily
Pharm
acokinetics
and
pharm
acodynamics
Half-life
Route
ofexcretion
20–30min.
Urinary
andfecal
2–3h
Urinary
7–11h
Fecal
~19h
Biliary
†Curren
tlyundergoingPhase
IItestingin
patients
withtransfusionalironoverload
.iv:Intraven
ous.
Data
takenfrom
[23,63,101–104].
Deferasirox for NTDT Drug Profile
www.expert-reviews.com doi: 10.1586/17474086.2013.827411

trends (for review see Galanello 2012 [69]). Patients with renal orhepatic impairment were generally excluded from the threestudies. All studies evaluated changes in iron burden as pri-mary and secondary end points according to measurement ofSF and LIC (as determined by MRI). Both the Voskaridouand Ladis studies also assessed cardiac iron concentration, asassessed by cardiac T2* [75,76].
Voskaridou et al. (2010) conducted an open-label, prospec-tive, single-center trial of deferasirox in iron-overloaded patientswith b-TI [76]. Adults (mean age of 41 years) who had receivedsporadic transfusions (�20 units) and had confirmed iron over-load (SF levels ‡1,000 ng/ml, liver MRI T2* <25 ms or
cardiac T2* <28 ms) at baseline were eligible to enter thestudy. In these 11 patients, deferasirox was administered at astarting dose of 10 or 20 mg/kg/day according to baseline ironburden, with subsequent dose adjustments (by increments of5 mg/kg/day every 3 months) according to SF trends, adverseevents (AEs) and laboratory parameters. Eight of the 11 patients(73%) who completed deferasirox therapy had previously beentreated, but were poorly compliant, with DFO. After 12 monthsof treatment, significant improvement was observed in the pri-mary end point of change, mean liver MRI T2*, from 3.4 to4.4 ms in 9 of 10 patients (p = 0.02) (TABLE 2). Notably, meancardiac T2* and left ventricular ejection fraction were
Iron
RESmacrophages:
release of recycled iron
Ineffective erythropoiesis
HIFsGDF 15
Hepcidin
Kidney
Erythropoietin
Liver
LIC
SF
Chronic anemia Hypoxia
Duodenum
Ferroportin
Duodenal iron absorption
Figure 2. Metabolism of iron in non-transfusion-dependent thalassemia. Ineffective erythropoiesis and chronic anemia/hypoxia leadto increased growth and differentiation factor 15 (GDF 15) and altered expression of HIFs. As a consequence, hepcidin is suppressed, andiron absorption from the gut as well as release of recycled iron from the reticuloendothelial system is increased. In turn, there is a deple-tion of macrophage iron, accompanied by relatively low levels of SF, and preferential portal and hepatocyte iron loading, which results inan elevation of liver iron concentration.HIF: Hypoxia-inducible transcription factor; SF: Serum ferritin.Adapted from [17,23].
Drug Profile Taher, Temraz & Cappellini
doi: 10.1586/17474086.2013.827411 Expert Rev. Hematol.

Table
2.Overview
ofkeyclinicalefficacy
andsafety
resu
ltsfordeferasiroxin
studiesofpatients
withNTDT.
Study
(year)
Study
design
Patients
(age,years)
Treatm
ent
regim
en
Keyefficacy
resu
lts
Keysafety
resu
lts
Ref.
Voskaridou
etal.(2010)
Prospective,
single-arm
,
1year,
open
-labeltrial
11b-TI
patien
ts
(28–53)
Deferasirox
(startingdose
10or20mg/kg/day)
After12months,significant
improvemen
tfrom
baselinein:
LiverMRIT2
*:baseline3.4–4
.4ms
(p=0.02;n=9);meanSF:
baseline
2030–1165ng/m
l
(-865ng/m
l;p=0.02;n=9).
Mild
AEsin
tenpatients
(nausea,
n=8;diarrhea,n=2)within
first
month
oftreatm
ent.
Nosignifican
tchangesin
meanserum
creatinine,
cystatinCor24-h
proteinuria.
Decreasein
liver
transaminasesat12
months(ALT:from
63.5
to36.5
U/L;
AST:from
64.8
to42.5
U/L).
[76]
Ladisetal.
(2010)
Prospective,
single-arm
,
1year,
open
-labeltrial
11b-TI
patien
ts
(24–40)
Deferasirox(starting
dose
10or
20mg/kg/day)
Significantdecrease
in:meanLIC:
baseline16.1;12months10.9,24
months4.8
mgFe/g
dw;p=0.005for
both;meanSF:
baseline1083;12
months566,24months365ng/m
l;
p=0.005forboth.
Patients
withLIC<3mgFe/g
dw:
five
(45%
).
AEsin
twopatients
(mild
diarrhea,
dizziness
andmalaise)
resolvedwith
treatm
entandwithoutdeferasirox
interruption.
Stable
creatininelevelsover1year
(baseline60.1;1year61.0
mmol/l)
elevatedcreatinineat
2years
(69.8
mmol/l;p=0.005).Noabnorm
al
creatinineclearance
orcreatininelevels
>ULN
.
Decreasein
liver
transaminasesat1
and2years
(AST:baseline42.8
U/L;
1year
30.8
U/L;2year25.9
U/L.ALT:
baseline50.5
U/L;1year29.9
U/L;
2year
20.0
U/L).
[75]
Taheretal.
(2012)
(THALA
SSA)
Prospective,
randomized,
double-blind,
placebo-controlled,
1year
trial
166NTDT
patien
ts
(10–69)
Deferasirox(starting
dose
5or10mg/kg/day)
ormatchingplacebo
After12months,significant
improvemen
tin:LICvs
placebo†:
-2.33±0.7
mgFe/g
dw
(startingdose
5mg/kg/day)and-4.18±
0.69mgFe/g
dw
(startingdose
10mg/kg/day),p�
0.001forboth.
SFvs
placebo†:-235ng/m
l(starting
dose
5mg/kg/day)
and–3
37ng/m
l
(startingdose
10mg/kg/day),
p<0.001forboth.
Incidence
ofoverallAEsnotrelatedto
studydrug:76.4
and78.2%
deferasiroxstartingdose
5or
10mg/kg/dayand80.4%
placebo.
Treatm
ent-relatedAEsin
40(24.1%
)
patients;nausea(6.6%
),rash
(4.8%)
anddiarrhea(3.6%)were
most
commonoverall.
Four(deferasirox-treated)patients
reportedsixtreatm
ent-relatedserious
AEs(abdominalpain,pyrexia,
hepatotoxicity
[notconfirm
edbya
central
laboratory],cellulitis,pruritus
andrash
(n=1each).
Serum
creatinineincreases>33%
above
baselineand>ULN
at‡2
consecutive
visits:three(5.5%
)
deferasirox-treatedpatients.
[34]
†Least-squaresmean.
AE:Adverseevents;ALT:Alanineaminotransferase;AST:Aspartate
aminotran
sferase;NTDT:Non-transfusion-dep
endentthalassemia;SF:
Serum
ferritin;ULN
:Upperlim
itofnorm
al.
Deferasirox for NTDT Drug Profile
www.expert-reviews.com doi: 10.1586/17474086.2013.827411

maintained at normal levels from baseline through 12 monthsof deferasirox treatment.
The preliminary findings reported by Voskaridou et al.(2010) were replicated in a second study, which investigatedthe effectiveness of deferasirox in 11 patients with b-TI [75,76].Transfusion-independent (<20 packed red blood cells in theirlifetime) adult patients with variable genotypes and iron over-load (SF levels ‡500 ng/ml and LIC ‡2 mg Fe/g dw) wereenrolled in the 24-month study and received deferasirox at10 or 20 mg/kg/day. Over the course of the study, dose adjust-ments were permitted at the end of each year and treatmentwas discontinued when SF levels declined below 250 ng/ml orbelow an LIC of 2 mg Fe/g dw. Of the six males and fivefemales who entered (64% were chelation-naıve), one patientwithdrew after 6 months of treatment as a result of noncompli-ance, and a second patient completed only 12 months of treat-ment after achieving the target iron levels described above. Inthe remaining patients, there were significant improvements iniron burden, evident in mean reductions in SF and LIC, withfive patients achieving LIC <3 mg Fe/g dw (TABLE 2). Treatmentefficacy was not adversely influenced by genetic factors poten-tially associated with iron accumulation such as thalassemia orHFE (hereditary hemochromatosis) genotype. Mean cardiacT2* and left ventricular ejection fraction values were withinnormal ranges at baseline and after 24 months of treatment inthis small group of NTDT patients.
THALASSA (assessment of Exjade in NTDT), a random-ized, double-blind, placebo-controlled, Phase II trial, is themost recent and largest study of deferasirox in NTDT patients(b-TI, a-thalassemia and HbE/b-thalassemia) [34]. In THA-LASSA, iron-overloaded (LIC ‡5 mg Fe/g dw and SF>300 ng/ml) patients who had not received transfusions in theprevious 6 months were randomized to deferasirox startingdoses of 5 or 10 mg/kg/day or matching placebo. In total,148 of 166 (89.2%) patients aged 10 years or older (mean age32 years) completed 1 year of treatment. Almost half (48.4%)of treated patients exhibited predefined LIC thresholds (>7 mgFe/g dw and LIC reduction <15% from baseline) that resultedin an increase of their deferasirox dose at 24 weeks, suggestingthe importance of dose adjustments to achieve therapeutic tar-gets. After 1 year, mean LIC and SF levels significantlyimproved from baseline in the deferasirox 5 and 10 mg/kg/daystarting dose cohorts compared with their placebo counterparts(p � 0.001) (TABLE 2) [34]. A significant dose-associatedeffect was noted for the least-squares mean absolutedecrease in LIC, whereby deferasirox at a starting dose of10 mg/kg/day reduced values by a significantly greater magni-tude than 5 mg/kg/day (a decrease of 3.80 from a baseline of14.6 mg Fe/g dw vs 1.95 mg Fe/g dw from a baseline of13.1 mg Fe/g dw; p = 0.009). Overall, 13 (23.6%) of patientsachieved LIC <5 mg Fe/g dw in the 10 mg/kg/day deferasiroxstarting dose group compared with eight (14.5%) who receivedthe starting dose of 5 mg/kg/day. In a subanalysis of NTDTsubgroups, it was shown that the efficacy response was consis-tent across NTDT subgroups, age groups (< and ‡18 years),T
able
2.Overview
ofkeyclinicalefficacy
andsafety
resu
ltsfordeferasiroxin
studiesofpatients
withNTDT(cont.).
Study
(year)
Study
design
Patients
(age,years)
Treatm
ent
regim
en
Keyefficacy
resu
lts
Keysafety
resu
lts
Ref.
Taheretal.
(THALA
SSA)
1-year
open
-lab
el
extensionof
THALA
SSA
133NTDT
patien
ts
Deferasirox(starting
dose
5or10mg/kg/day)
withdose
escalation
upto
20mg/kg/day
Patients
receivingdeferasiroxin
the
core
plusextension(n
=110):Mean
absolute
changein
LIC:–7.14mgFe/g
dw;Medianchangein
SF:
–450ng/m
l.
Patients
withLIC<3mgFe/g
dw:18
(16.4%).
Patients
receivingdeferasiroxin
the
extensionhavingcrossedoverfrom
placeboin
thecore
(n=56):Patients
withLIC<3mgFe/g
dw:6(10.7%).
Most
commonAEsregardless
ofstudy
drugrelationship:Deferasiroxcore
plus
extensiongroup(n
=110):upper
respiratory
tract
infection(20.9%
),
pyrexia(17.3%
),diarrhea(13.6%),
headacheandnau
sea(both
12.7%),
upperab
dominalpain,anemia
and
gastroenteritis(11.8%
).
Serum
creatinineincreases>33%
above
baselineandab
ove
ULN
at‡2
consecutive
visits:five
(4.5%)patients
inthecore
plusextensiongroup.
ALT
increase
>5xULN
and>2�
baseline:onepatientin
thecore
plus
extensiongroup.
[78]
†Least-squaresmean.
AE:Adverseevents;ALT:Alanineam
inotransferase;AST:Aspartate
aminotran
sferase;NTDT:Non-transfusion-dependen
tthalassemia;SF:
Serum
ferritin;ULN
:Upperlim
itofnorm
al.
Drug Profile Taher, Temraz & Cappellini
doi: 10.1586/17474086.2013.827411 Expert Rev. Hematol.

gender, race, baseline LIC and SF levels and splenectomystatus [77].
Using receiver operating characteristic testing, a subanalysiswas conducted to determine whether SF levels can beemployed to predict clinically relevant LIC thresholds inNTDT patients [40]. Results from 282 screened patientsshowed that those with SF >800 ng/ml had a high probability(91.7%) of LIC ‡5 mg Fe/g dw (threshold for dose initiationin the THALASSA study) while SF >2,000 ng/ml was highlypredictive (92.9%) of LIC ‡7 mg Fe/g dw (threshold fordose increase in the THALASSA study). Thus, SF may be auseful guide to initiate and adjust chelation therapy inNTDT patients.
Results are also recently available from an extension of THA-LASSA, which evaluated the continued (up to 2 years) efficacyand safety of deferasirox in patients receiving deferasirox in thecore study in addition to patients receiving placebo whoswitched to deferasirox [78]. Overall, 133 of 148 NTDTpatients who completed the core study enrolled in the 1-yearextension phase, including 48 patients who crossed over fromplacebo to deferasirox treatment. The majority of patients (n =130) completed extended treatment with deferasirox at a meanactual dose of 9.8 ± 3.6 mg/kg/day (patients treated with
deferasirox in the core and extension phases). Dosing in theextension phase was relatively higher in patients who crossedover from placebo, at 13.7 ± 4.6 mg/kg/day. Results showedthat LIC and SF continued to decrease in the extension period(TABLE 2). Among the 110 patients who received deferasiroxthroughout the core and extension study (up to 2 years oftreatment), a mean absolute decrease in LIC of 7.14 mg Fe/gdw from baseline was observed (FIGURE 4) [79] and was accompa-nied by a median decrease in SF of 450 ng/ml.
Although not covered in detail here, it is noteworthy thatdeferasirox has also been investigated in 31 double heterozygousHb S/b-thalassemia patients, showing again an effective man-agement of iron burden [80].
Two preliminary studies [75,76] and the pivotal THA-LASSA study [34] were unequivocal in demonstrating amarked reduction in iron burden with up to 2 years ofdeferasirox treatment in NTDT patients. Efficacy wasachieved at generally lower deferasirox doses (starting doses5 and 10 mg/kg/day, escalating to up to 20 mg/kg/day) thanreported in studies of patients with transfusional iron over-load (>30 mg/kg/day) [81], although the need for monitoringand dose adjustment remains as important to achievetherapeutic goals.
Deferasirox
DeferasiroxFe-complex
conjugated metabolites
BileMrp2
FeII
Deferasirox
UGT
GlucuronidesM3, M6
UGT
CYP2D6
M4 M1
Hydroxylatedmetabolites
CYP1A
Liver
Gluc.
Mrp3?
Blood Kidney Urine
ST
Sulf.M7
Fe-[deferasirox]2
Portal blood
Deferasiroxfree hydroxy metabolites
Feces
Gut
Figure 3. Proposed scheme for the disposition of deferasirox in humans after peroral administration. The figure shows the pro-posed metabolism and elimination processes for deferasirox in the liver and the gut. P450-catalyzed metabolism of deferasirox appears oflittle importance as 6% was recovered as M1 and M7 and 2% as M4. Renal excretion accounts for 8% of the dose mainly in the form ofM6. The anion transporter Mrp2 appears to be involved in the hepatobiliary elimination of deferasirox and M3. The basolateral Mrp3 is alikely candidate for eliminating some deferasirox metabolites into the sinusoidal blood followed by final excretion from the kidney.Adapted with permission from [73]. � 1998–2010, Drug Metabolism and Disposition by American Society for Pharmacology andExperimental Therapeutics.
Deferasirox for NTDT Drug Profile
www.expert-reviews.com doi: 10.1586/17474086.2013.827411

Safety & tolerability
Observed AEs in studies of NTDT patients were mild andconsistent with the documented safety profile of deferasirox(TABLE 2) [82]. There were no fatalities reported during defera-sirox treatment in the THALASSA study or the two prelimi-nary studies.
The design of the largest study (THALASSA) was based onclinical experience gained with DFO, specifically application oflower doses when body iron levels are low in order to minimizeAEs [34]. Indeed, deferasirox was generally well tolerated atadministered doses that were considerably lower than previouslyused for transfusion-dependent patients with b-thalassemia.Moreover, AEs were manageable among the NTDT popula-tion, including those patients who achieved the stopping targetof LIC below 3 mg Fe/g dw [83]. The incidence of overall AEsunrelated to study drug in the 1-year THALASSA study wasgenerally comparable between deferasirox 5 or 10 mg/kg/dayand placebo [34]. Adverse events potentially related to defera-sirox were mainly gastrointestinal in nature and occurred at asimilar frequency to the placebo group. Notably, treatment-related AEs were reported in THALASSA at a frequencythat was approximately half of that observed in a 1-year studyof patients with transfusion-dependent anemias (24.2 vs50.3%) [84]. Gastrointestinal events of nausea (6.6%) and diar-rhea (3.6%) encompassed the majority of treatment-related AEs
in 166 patients who received deferasirox in the THALASSAstudy and were similarly reported in the two earlier pilot stud-ies of NTDT patients [34,75,76]. Most AEs did not necessitatediscontinuation of treatment, instead resolving spontaneouslyor with drug interruption or adjustment. The safety profile ofdeferasirox in the 1-year THALASSA study was maintainedwhen the treatment duration was extended over a second year(TABLE 2) [79].
In the core 1-year THALASSA study, three (5.5%) patientsexperienced two consecutive serum creatinine increases >33%above baseline and above the upper limit of normal (ULN),one of which resolved without treatment discontinuation; tworesolved on treatment interruption. Furthermore, no progressiveincreases in serum creatinine, creatinine clearance, alanine ami-notransferase (ALT) or aspartate aminotransferase (AST) werenoted. In patients treated for up to 2 years, five (4.5%) patientsoverall experienced two consecutive serum creatinine increases>33% above baseline and above the ULN and one patient hadALT >5 � ULN and 2 � baseline [84].
There were no reports of serum creatinine increases abovethe ULN in the Voskaridou et al. and Ladis et al. stud-ies [75,76], although in the Ladis et al. study mean creatininelevels were elevated at the end of 2 years of treatment afterbeing stable during the first year (TABLE 2). Both Ladis et al.and Voskaridou et al. reported a decrease in liver enzymes(ALT and AST) over time (TABLE 2), which may be indicativeof a corresponding improvement in liver function followingthe reduction in iron burden achieved with deferasiroxtreatment [75,76].
Specific post-marketing safety data are not yet availablefor NTDT patients treated with deferasirox given the recentindication in these patients. It should be noted that cases ofacute renal and hepatic failure, some of which were fatalparticularly in patients with comorbidities and those whoare in the advanced stages of their hematologic disorder,have been observed in transfusion-dependent disease. Gas-trointestinal hemorrhage may also be fatal, especially in eld-erly patients who have advanced hematologic malignanciesand/or low platelet counts (for full details see US label [104]).Close monitoring is recommended, including laboratorytests of renal and hepatic function, for all patients treatedwith deferasirox [104].
ConclusionsIron overload management in NTDT patients has notreceived the attention given to that of b-thalassemia majorpatients; however, recent studies in NTDT patients clearlydemonstrate the association of high iron burden with seriouscomplications, indicating the importance of iron manage-ment in patients other than those who are transfusion-dependent. Recent iron chelation studies, including aprospective, placebo-controlled trial, a new indication fordeferasirox in NTDT and recently available clinical guide-lines pave the way for improvement in management of ironburden in these patients.
–10
Patients, n
Placebo/deferasiroxany dose
Deferasiroxany dose
Baseline 6
110
55
94
Core study Extension study
51
93
51
82
47
84
46
Deferasirox any dosePlacebo/deferasirox any dose
12
Placebo/deferasirox:median = 14.0 mg/kg/day
Deferasirox extension:median dose = 10.8 mg/kg/day
Deferasirox (core + extension):median dose = 9.5 mg/kg/day
Time (months)
18 24
–8
–6
–4
Mea
n a
bso
lute
ch
ang
e in
LIC
(mg
Fe/
g d
w) –2
0
2
Figure 4. Absolute change in LIC with deferasirox in NTDTpatients.This research was originally published in [79]. � The AmericanSociety of Hematology.
Drug Profile Taher, Temraz & Cappellini
doi: 10.1586/17474086.2013.827411 Expert Rev. Hematol.

Three studies, including the THALASSA study, have clearlyshown that deferasirox, at doses up to 20 mg/kg/day, achieveseffective control of iron levels in NTDT over 2 years. Theobserved safety and tolerability profile of deferasirox in NTDTpatients from these studies was consistent with reports in otherestablished patient populations.
With the necessary monitoring of iron burden in NTDTpatients along with the timely initiation, monitoring and doseadjustment of deferasirox treatment, patients should be able toachieve effective control of their iron burden reducing their riskof iron-associated complications.
Expert commentaryGiven the evidence of increased morbidity with escalating ironburden in non-transfusion-dependent thalassemia (NTDT)patients, the importance of controlling iron burden has cometo the forefront. Many of the lessons we have learned fromcontrolling iron in transfusion-dependent thalassemias can helpinform practice here. Over time, NTDT patients can indeedachieve similar levels of iron overload, due to increased intesti-nal absorption, to those in transfusion-dependent thalassemias.The need to monitor iron burden is, of course, pertinent toboth non-transfusion and transfusion-dependent thalassemias,to allow the initiation of chelation therapy when appropriate(FIGURE 1) as well as timely dose adjustments to meet therapeuticgoals. Of particular note in NTDT is the underestimation ofiron load by serum ferritin (SF) assessments. Iron assessmentby MRI is the preferred assessment for NTDT patients butwill not be accessible to all patients; hence, SF can still be usedwith caution.
Thus, in NTDT patients, the algorithm shown in FIGURE 1
recommends initiation of iron chelation therapy with SF con-centrations exceeding 800 ng/ml or liver iron concentration(LIC) ‡5 mg Fe/g dw. Where SF is between 300 and 800 ng/mL, the treatment decision may depend upon LIC or otherfactors. Continuous monitoring of SF and LIC is required todetermine treatment progress and the need for interruption ofchelation therapy should SF levels reach the target of below300 ng/ml or LIC reaches levels below 3 mg Fe/g dw(FIGURE 1) [35,40].
The availability of recent trial data of deferasirox treat-ment for up to 2 years and the US FDA and Europeanapproval of the use of deferasirox in NTDT patients havepaved the way for more effective control of iron burden inNTDT patients.
Five-year viewRecent experiences and data from the THALASSA trial havebeen employed to help update guidelines for the treatment ofNTDT patients, which have recently been published by theThalassemia International Federation [106]. Implementation ofthese new guidelines will not only raise awareness of the needto treat iron overload in these patients but will importantlyoffer guidance on how to do so. New trials with deferasirox in
NTDT are ongoing, for example NCT01709838, which is aPhase IV multicenter study. Further data from such trials willinform appropriate dosing strategies for deferasirox, withrespect to appropriate starting doses, the need to dose adjustand the need to interrupt chelation if treatment goals arereached. Lifelong treatment with iron chelation may not benecessary in NTDT patients, but the need to monitor ironburden continues throughout life. Of particular interest overthe long term will be determination of the impact of effectiveiron chelation on complications in NTDT patients. Emergenceof long-term data with iron chelation, as well as additionalinvestigative treatments for NTDT patients, such as fetalhemoglobin inducers, will no doubt be critical in improvingthe lives of NTDT patients.
Information resources1. For healthcare professionals outside the USA, the following
website details background on thalassemias (sponsored byNovartis): www.ironhealthalliance.com/disease-states/thalasse-mia.jsp.
2. For an overview of NTDT see Blood Reviews; 26S (2012).3. For a comprehensive review of iron chelation therapy in
NTDT see Taher AT et al. Treating iron overload inpatients with non-transfusion-dependent thalassemia. Am. J.Hematol. http://onlinelibrary.wiley.com/doi/10.1002/ajh.23405/abstract
4. For prescribing information see www.pharma.us.novartis.com/cs/; www.pharma.us.novartis.com/product/pi/pdf/exjade.pdf and www.medicines.org.uk/emc/medicine/18805 (pleasealso consult your own country regulations).
5. Musallam KM et al. Elevated liver iron concentration isa marker of increased morbidity in patients with betathalassemia intermedia. Haematologica 96, 1605–1612(2011).
6. Taher AT et al. Deferasirox reduces iron overload signifi-cantly in non-transfusion-dependent thalassemia: 1-yearresults from a prospective, randomized, double-blind,placebo-controlled study. Blood 120(5), 970–977 (2012).
Financial & competing interests disclosure
AT Taher received research funding and honoraria from Novartis
Pharmaceuticals. MD Cappellini reports participating in a Novartis
Pharmaceuticals speaker’s bureau and receiving honoraria from Novar-
tis and Genzyme. The authors are fully responsible for the content and
editorial decisions for this manuscript. The authors have no other rele-
vant affiliations or financial involvement with any organization or
entity with a financial interest in or financial conflict with the subject
matter or materials discussed in the manuscript apart from those
disclosed.
Financial support for medical editorial assistance was provided by
Novartis Pharmaceuticals. The authors thank Michelle Utton-Mishra,
Mudskipper Business Ltd, for medical editorial assistance with this
manuscript.
Deferasirox for NTDT Drug Profile
www.expert-reviews.com doi: 10.1586/17474086.2013.827411

Key issues
• Deferasirox (Exjade) is a once-daily tridentate chelator with proven efficacy in the treatment of transfusional iron overload.
• The efficacy and safety of deferasirox in non-transfusion-dependent thalassemia (NTDT) patients has been established in pilot studies,
and subsequently in the first large prospective study of an iron chelator in the NTDT population, the THALASSA study.
• Across studies spanning up to 2 years of treatment, deferasirox was associated with a significant reduction in iron burden in NTDT
patients, as measured by liver iron concentration and serum ferritin.
• The safety profile of deferasirox in NTDT is generally consistent with previous reports, with manageable gastrointestinal events
comprising the majority of treatment-related adverse events.
• Regular monitoring and clinical management, including laboratory tests of renal and hepatic function, is required for all patients
undergoing treatment with deferasirox.
• Deferasirox is the first iron chelator to gain approval for the treatment of iron overload in NTDT patients.
• Data from the THALASSA study support current prescribing recommendations for deferasirox and have served as a fundamental basis
for the development of guidelines on chelation therapy in NTDT patients.
References
Papers of special note have been highlighted as:
• of interest
•• of considerable interest
1 Cao A, Galanello R. Beta-thalassemia.
Genet. Med. 12, 61–76 (2010).
2 Harteveld CL, Higgs DR.
Alpha-thalassaemia. Orphanet. J. Rare. Dis.5, 13 (2010).
3 Muncie HL Jr, Campbell J. Alpha and beta
thalassemia. Am Fam Physician.80, 339–344 (2009).
4 Vichinsky E. Advances in the treatment of
alpha-thalassemia. Blood Rev. 26 (Suppl. 1),
S31–S34 (2012).
5 Galanello R. Recent advances in the
molecular understanding of
non-transfusion-dependent thalassemia.
Blood Rev. 26 (Suppl. 1), S7–S11 (2012).
6 Weatherall DJ. The definition and
epidemiology of non-transfusion-dependent
thalassemia. Blood Rev. 26 (Suppl. 1),
S3–S6 (2012).
7 Camaschella C, Cappellini MD.
Thalassemia intermedia. Haematologica80, 58–68 (1995).
8 Colah R, Gorakshakar A, Nadkarni A.
Global burden, distribution and prevention
of beta-thalassemias and hemoglobin E
disorders. Expert Rev. Hematol.3, 103–117 (2010).
9 Michlitsch J, Azimi M, Hoppe C et al.Newborn screening for hemoglobinopathies
in California. Pediatr. Blood Cancer52, 486–490 (2009).
10 Vichinsky E. Hemoglobin E syndromes.
Hematology Am. Soc. Hematol. Educ.Program 79–83 (2007).
11 Vichinsky EP. Changing patterns of
thalassemia worldwide. Ann. N. Y. Acad.Sci. 1054, 18–24 (2005).
12 Lal A, Goldrich ML, Haines DA et al.Heterogeneity of hemoglobin H disease in
childhood. N. Engl. J. Med.364, 710–718 (2011).
13 Laosombat V, Viprakasit V,
Chotsampancharoen T et al. Clinicalfeatures and molecular analysis in Thai
patients with HbH disease. Ann. Hematol.88, 1185–1192 (2009).
14 Musallam KM, Taher AT, Rachmilewitz EA.
b-thalassemia intermedia: A clinical
perspective. Cold Spring Harb. Perspect.Med. 2, a013482 (2012).
15 Weatherall DJ, Clegg JB. Inheritedhaemoglobin disorders: an increasing globalhealth problem. Bull World Health Organ.79, 704–712 (2001).
16 Galanello R, Origa R. Beta-thalassemia.Orphanet. J. Rare. Dis. 5, 11 (2010).
17 Taher AT, Musallam KM, Cappellini MD,
Weatherall DJ. Optimal management of
b-thalassaemia intermedia. Br. J. Haematol.152, 512–523 (2011).
18 Chen FE, Ooi C, Ha SY et al. Genetic andclinical features of hemoglobin H disease in
Chinese patients. N. Engl. J. Med.343, 544–550 (2000).
19 Taher A, Isma’eel H, Cappellini MD.
Thalassemia intermedia: revisited.
Blood Cells Mol. Dis. 37, 12–20 (2006).
20 Taher AT, Musallam KM, Karimi M et al.Overview on practices in thalassemia
intermedia management aiming for lowering
complication rates across a region of
endemicity: the OPTIMAL CARE study.
Blood 115, 1886–1892 (2010).
21 Musallam KM, Cappellini MD, Wood JC,
Taher AT. Iron overload in
non-transfusion-dependent thalassemia:
a clinical perspective. Blood Rev.26 (Suppl. 1), S16–S19 (2012).
22 Mallat NS, Mallat SG, Musallam KM, and
Taher AT. Potential mechanisms for renal
damage in beta-thalassemia. J. Nephrol. doi:10.5301/jn.5000253 (2013) (Epub ahead of
print).
23 Taher A, Hershko C, Cappellini MD. Iron
overload in thalassaemia intermedia:
reassessment of iron chelation strategies.
Br. J. Haematol. 147, 634–640 (2009).
24 Musallam KM, Cappellini M.D., Wood JC
et al. Elevated liver iron concentration is a
marker of increased morbidity in patients
with b-thalassemia intermedia.
Haematologica 96, 1605–1612 (2011).
•• This study provides fundamental evidence
demonstrating the correlation between
elevated liver iron burden and increased
vascular, endocrine and bone disease, and a
relationship with advancing age.
25 Rivella S. The role of ineffective
erythropoiesis in non-transfusion-dependent
thalassemia. Blood Rev. 26 (Suppl. 1),
S12–S15 (2012).
26 Taher AT, Musallam KM, Wood JC,
Cappellini MD. Magnetic resonance
evaluation of hepatic and myocardial iron
deposition in transfusion-independent
thalassemia intermedia compared to
regularly transfused thalassemia major
patients. Am. J. Hematol. 85,288–290 (2010).
27 Au WY, Lam WW, Chu WW et al.Organ-specific hemosiderosis and functional
correlation in Chinese patients with
thalassemia intermedia and hemoglobin H
disease. Ann. Hematol. 88, 947–950 (2009).
28 Voskaridou E, Douskou M, Terpos E et al.Magnetic resonance imaging in the
Drug Profile Taher, Temraz & Cappellini
doi: 10.1586/17474086.2013.827411 Expert Rev. Hematol.

evaluation of iron overload in patients with
beta thalassaemia and sickle cell disease.
Br. J. Haematol. 126, 736–742 (2004).
29 Lombardo T, Tamburino C, Bartoloni G
et al. Cardiac iron overload in thalassemic
patients: an endomyocardial biopsy study.
Ann. Hematol. 71, 135–141 (1995).
30 Glickstein H, El BR, Link G et al. Actionof chelators in iron-loaded cardiac cells:
accessibility to intracellular labile iron and
functional consequences. Blood 108,
3195–3203 (2006).
31 Musallam KM, Cappellini MD, Taher AT.
Evaluation of the 5 mg/g liver iron
concentration threshold and its association
with vascular and endocrine/bone morbidity
in b-thalassemia intermedia. Blood120(21), abstract 1024 (2012).
32 Musallam KM, Cappellini MD, Daar S
et al. Serum ferritin levels and morbidity in
b-thalassemia intermedia: A 10-year cohort
study. Blood 120(21), abstract 1021 (2012).
33 Taher AT, Musallam KM, El-Beshlawy A
et al. Age-related complications in
treatment-naive patients with thalassaemia
intermedia. Br. J. Haematol.150, 486–489 (2010).
34 Taher AT, Porter J, Viprakasit V et al.Deferasirox significantly reduces iron
overload in non-transfusion-dependent
thalassemia: 1-year results from a
prospective, randomized, double-blind,
placebo-controlled study. Blood 120,
970–977 (2012).
•• The first large prospective study of an iron
chelator in the non-transfusion-dependent
thalassemia (NTDT) population, which has
also served as a basis for the development
of a novel treatment algorithm for iron
chelation therapy in NTDT.
35 Taher AT, Viprakasit V, Musallam KM,
Cappellini MD. Treating iron overload in
patients with non-transfusion-dependent
thalassemia. Am. J. Hematol. 88,409–415 (2013).
36 Fischer R, Harmatz PR. Non-invasive
assessment of tissue iron overload.
Hematology Am. Soc. Hematol. Educ.Program 215–221 (2009).
37 Origa R, Galanello R, Ganz T et al. Liveriron concentrations and urinary hepcidin in
b-thalassemia. Haematologica 92,
583–588 (2007).
38 Pakbaz Z, Fischer R, Fung E et al. Serumferritin underestimates liver iron
concentration in transfusion independent
thalassemia patients as compared to
regularly transfused thalassemia and sickle
cell patients. Pediatr. Blood Cancer49, 329–332 (2007).
39 Taher A, El Rassi F, Isma’eel H et al.Correlation of liver iron concentration
determined by R2 magnetic resonance
imaging with serum ferritin in patients with
thalassemia intermedia. Haematologica93, 1584–1586 (2008).
40 Taher AT, Porter JB, Viprakasit V et al.Estimation of liver iron concentration by
serum ferritin measurement in
non-transfusion-dependent thalassemia
patients: Analysis from the 1-year
THALASSA study. Haematologica97 (Suppl. 1), abstract 0927 (2012).
41 Wood JC. Magnetic resonance imaging
measurement of iron overload.
Curr. Opin. Hematol. 14, 183–190 (2007).
42 Gandon Y, Olivie D, Guyader D et al.Non-invasive assessment of hepatic iron
stores by MRI. Lancet 363,357–362 (2004).
43 St Pierre TG, Clark PR, Chua-anusorn W
et al. Noninvasive measurement and
imaging of liver iron concentrations using
proton magnetic resonance. Blood105, 855–861 (2005).
44 Hankins JS, McCarville MB, Loeffler RB
et al. R2* magnetic resonance imaging of
the liver in patients with iron overload.
Blood 113, 4853–4855 (2009).
45 Garbowski MW, Carpenter J-P, Smith G,
Pennell DJ, and Porter JB. Calibration of
improved T2* method for the estimation of
liver iron concentration in transfusional iron
overload. Blood 114(22), abstract 2004
(2009).
46 St Pierre TG, El-Beshlawy A, Elalfy MS
et al. Multicenter validation of spin-density
projection-assisted R2-MRI for the
non-invasive measurement of liver iron
concentration. Blood 116(21),
abstract 2053 (2010).
47 Heli H, Mirtorabi S, Karimian K. Advances
in iron chelation: an update. Expert Opin.Ther. Pat. 21, 819–856 (2011).
48 Ma Y, Zhou T, Kong X, Hider RC.
Chelating agents for the treatment of
systemic iron overload. Curr. Med. Chem.19, 2816–2827 (2012).
49 Delea TE, Sofrygin O, Thomas SK et al.Cost effectiveness of once-daily oral
chelation therapy with deferasirox versus
infusional deferoxamine in
transfusion-dependent thalassaemia patients.
US healthcare system perspective.
Pharmacoeconomics 25, 329–342 (2007).
50 Delea TE, Edelsberg J, Sofrygin O et al.Consequences and costs of noncompliance
with iron chelation therapy in patients with
transfusion-dependent thalassemia:
a literature review. Transfusion 47,
1919–1929 (2007).
51 Cappellini MD, Pattoneri P. Oral iron
chelators. Annu. Rev. Med. 60,25–38 (2009).
52 Huang YC, Chang JS, Wu KH, Peng CT.
Regression of myocardial dysfunction after
switching from desferrioxamine to
deferiprone therapy in beta-thalassemia
major patients. Hemoglobin 30,
229–238 (2006).
53 Kolnagou A, Economides C, Eracleous E,
Kontoghiorghes GJ. Long term comparative
studies in thalassemia patients treated with
deferoxamine or a deferoxamine/deferiprone
combination. Identification of effective
chelation therapy protocols. Hemoglobin32, 41–47 (2008).
54 Peng CT, Tsai CH, Wu KH. Effects of
chelation therapy on cardiac function
improvement in thalassemia patients:
literature review and the Taiwanese
experience. Hemoglobin 32, 49–62 (2008).
55 Cossu P, Toccafondi C, Vardeu F et al.Iron overload and desferrioxamine chelation
therapy in beta-thalassemia intermedia.
Eur. J. Pediatr. 137, 267–271 (1981).
56 Olivieri NF, Koren G, Matsui D et al.Reduction of tissue iron stores and
normalization of serum ferritin during
treatment with the oral iron chelator L1 in
thalassemia intermedia. Blood 79,
2741–2748 (1992).
57 Pippard MJ, Weatherall DJ. Iron balance
and the management of iron overload in
b-thalassemia intermedia. Birth Defects Orig.Artic. Ser. 23, 29–33 (1988).
58 Pootrakul P, Sirankapracha P, Sankote J
et al. Clinical trial of deferiprone ironchelation therapy in beta-thalassaemia/
haemoglobin E patients in Thailand.
Br. J. Haematol. 122, 305–310 (2003).
59 Rombos Y, Tzanetea R, Konstantopoulos K
et al. Chelation therapy in patients with
thalassemia using the orally active iron
chelator deferiprone (L1). Haematologica85, 115–117 (2000).
60 Akrawinthawong K, Chaowalit N,
Chatuparisuth T, Siritanaratkul N.
Effectiveness of deferiprone in
transfusion-independent beta-thalassemia/
HbE patients. Hematology 16,113–122 (2011).
Deferasirox for NTDT Drug Profile
www.expert-reviews.com doi: 10.1586/17474086.2013.827411

61 Chan JC, Chim C-S, Ooi CG et al. Use of
the oral chelator deferiprone in the
treatment of iron overload in patients with
Hb H disease. Br. J Haematol. 133,198–205 (2006).
62 Neufeld EJ, Galanello R, Viprakasit V et al.A phase 2 study of the safety, tolerability,
and pharmacodynamics of FBS0701, a
novel oral iron chelator, in transfusional
iron overload. Blood 119, 3263–3268
(2012).
63 Rienhoff HY, Jr., Viprakasit V, Tay L et al.A phase 1 dose-escalation study: safety,
tolerability, and pharmacokinetics of
FBS0701, a novel oral iron chelator for the
treatment of transfusional iron overload.
Haematologica 96, 521–525 (2011).
64 Galanello R, Aydinok Y, Piga A et al.A 48 week phase 2 study of the safety,
tolerability and efficacy of FBS0701, a novel
iron chelator for treatment of transfusional
iron overload. Haematologica97 (Suppl. 1), abstract 0606 (2012).
65 Aydinok Y, Galanello R, Viprakasit V et al.The safety, tolerability and efficacy of fbs0701,
an iron chelator in clinical development for
transfusional iron overload: data from
72 weeks of treatment.Haematologica98 (Suppl. 1), abstract S1175 (2013).
66 El Ouagari K, Migliaccio-Walle K, Lau H,
Bozkaya D. Cost-effectiveness of deferasirox
in lower-risk myelodysplastic syndrome
(MDS) in Canada (abstract 343). Leuk Res.35, S137-S138 (2011).
67 Calabro A, Delea TE, Sofrygin O et al.Cost-effectiveness of once-daily oral
chelation therapy with deferasirox versus
infusional deferoxamine in transfusion-
dependent thalassemic patients: a Brazilian
perspective. Haematologica 91(Suppl. 1),
abstract 804 (2006).
68 Delea TE, Thomas SK, Baladi J, Phatak PD.
Cost-effectiveness analysis of oral iron
chelation therapy with deferasirox (Exjade,
ICL670) versus infusional chelation therapy
with deferoxamine in patients with
transfusion-dependent myelodysplastic
syndrome. Blood 106(11), abstract 5585
(2005).
69 Galanello R, Campus S, Origa R.
Deferasirox : pharmacokinetics and clinical
experience. Expert Opin. Drug Metab.Toxicol. 8, 123–134 (2012).
70 Steinhauser S, Heinz U, Bartholoma M
et al. Complex formation of ICL670 and
related ligands with FeIII and FeII. Eur. J.Inorg. Chem. 21, 4177–4192 (2004).
71 Bruin GJ, Faller T, Wiegand H et al.Pharmacokinetics, distribution, metabolism
and excretion of deferasirox and its iron
complex in rats. Drug Metab. Dispos.36, 2523–2538 (2008).
72 Piga A, Galanello R, Forni GL et al.Randomized phase II trial of deferasirox
(Exjade, ICL670), a once-daily,
orally-administered iron chelator, in
comparison to deferoxamine in thalassemia
patients with transfusional iron overload.
Haematologica 91, 873–880 (2006).
73 Waldmeier F, Bruin GJ, Glaenzel U et al.Pharmacokinetics, metabolism, and
disposition of deferasirox in beta-thalassemic
patients with transfusion-dependent iron
overload who are at pharmacokinetic steady
state. Drug Metab. Dispos. 38, 808–816(2010).
74 Skerjanec A, Wang J, Maren K, Rojkjaer L.
Investigation of the pharmacokinetic
interactions of deferasirox, a once-daily oral
iron chelator, with midazolam, rifampin,
and repaglinide in healthy volunteers.
J. Clin. Pharmacol. 50, 205–213(2010).
75 Ladis V, Berdousi H, Gotsis E, and
Kattamis A. Deferasirox administration for
the treatment of non-transfusional iron
overload in patients with thalassaemia
intermedia. Br. J. Haematol. 151,504–508 (2010).
• One of the two pilot studies supporting
the efficacy and safety of deferasirox in
NTDT patients.
76 Voskaridou E, Plata E, Douskou M et al.Treatment with deferasirox (Exjade)
effectively decreases iron burden in patients
with thalassaemia intermedia: results of a
pilot study. Br. J. Haematol. 148, 332–334(2010).
• One of the two pilot studies supporting
the efficacy and safety of deferasirox in
NTDT patients.
77 Taher AT, Porter JB, Viprakasit V et al.Reduction in liver iron concentration is
consistent across subgroups of
non-transfusion-dependent thalassemia
patients treated with deferasirox: Results
from the 1-year THALASSA study.
Haematologica 97 (Suppl. 1),
abstract 0924 (2012).
78 Taher AT, Porter JB, Viprakasit V et al.Deferasirox effectively reduces iron overload
in non-transfusion-dependent thalassemia
(NTDT) patients: 1-year extension results
from the THALASSA study. Ann. Hematoldoi:10.1007/s00277-013-1808-z (2013)
(Epub ahead of print).
79 Taher AT, Porter JB, Viprakasit V et al.Deferasirox continues to reduce iron
overload in non-transfusion-dependent
thalassemia: A one-year, open-label
extension to a one-year, randomized,
double-blind, placebo-controlled study
(THALASSA). Blood 120(21), abstract
3258 (2012).
•• Provides extension data (a total of 2 years)
highlighting the continued reduction of
liver iron burden with deferasirox
treatment in patients with NTDT enrolled
in the THALASSA study.
80 Voskaridou E, Plata E, Douskou M et al.Deferasirox effectively decreases iron burden
in patients with double heterozygous HbS/
beta-thalassemia. Ann. Hematol.90, 11–15 (2011).
81 Taher A, Cappellini MD, Vichinsky E et al.Efficacy and safety of deferasirox doses of
>30 mg/kg per d in patients with
transfusion-dependent anaemia and iron
overload. Br. J. Haematol. 147, 752–759(2009).
82 Vichinsky E. Clinical application of
deferasirox: Practical patient management.
Am. J. Hematol. 83, 398–402 (2008).
83 Taher A, Porter J, Viprakasit V et al.The safety profile of deferasirox remains
consistent as non-transfusion-dependent
thalassemia patients approach the
target liver iron concentration of
<3 mg Fe/g dw for interrupting chelation.
Haematologica. 98 (Suppl. 1),
abstract P391 (2013).
84 Cappellini MD, Porter JB, El-Beshlawy A
et al. Tailoring iron chelation by iron intake
and serum ferritin trends: the prospective
multicenter EPIC study of deferasirox in
1744 patients with various
transfusion-dependent anemias.
Haematologica 95, 557–566 (2010).
Websites
101 Desferal (deferoxamine) Basic Prescribing
Information (2010).
www.pharma.us.novartis.com/product/pi/
pdf/desferal.pdf
102 Apotex. Ferriprox summary of product
characteristics (2011).
www.emea.europa.eu/docs/en_GB/
document_library/EPAR_-
_Product_Information/human/000236/
WC500022050.pdf
103 Apotex. Ferriprox prescribing information
(2011).
Drug Profile Taher, Temraz & Cappellini
doi: 10.1586/17474086.2013.827411 Expert Rev. Hematol.

www.ferriprox.com/us/pdf/ferriprox_full_pi.
104 Novartis Pharmaceuticals. EXJADE
(deferasirox) US Prescribing Information
(2013).
www.pharma.us.novartis.com/product/pi/
pdf/exjade.pdf
105 Novartis Pharmaceuticals UK Ltd. Summary
of Product Characteristics - EXJADE
125 mg, 250mg, 500mg dispersible tablets
(2013).
www.medicines.org.uk/emc/medicine/
18805/SPC/
106 Thalassemia International Federation.
Guidelines for the management of non
transfusion dependent thalassaemia (NTDT)
(2013).
www.thalassaemia.org.cy/wordpress/wp-
content/uploads/2013/05/NTDT-
BOOKLET-FINAL-PDF.pdf
Deferasirox for NTDT Drug Profile
www.expert-reviews.com doi: 10.1586/17474086.2013.827411