declaration of originality - epubs.surrey.ac.ukepubs.surrey.ac.uk/850426/1/tosan edematie phd thesis...
TRANSCRIPT

Readiness for Innovation in Public Healthcare Service Delivery
Organisations in the UK
By
Tosan Tracey Edematie
Submitted for the Degree of Doctor of Philosophy
Surrey Business School
Faculty of Healthcare Management and Policy
University of Surrey
Supervisors:
Dr Theopisti Chrysanthaki
Prof Jane Hendy
©Tosan Tracey Edematie 2019

Declaration of originality
This thesis and the work to which it refers are the results of my own efforts.
Any ideas, data, images or text resulting from the work of others (whether
published or unpublished) are fully identified as such within the work and
attributed to their originator in the text, bibliography or in footnotes. This thesis
has not been submitted in whole or in part for any other academic degree or
professional qualification. I agree that the University has the right to submit
my work to the plagiarism detection service TurnitinUK for originality checks.
Whether or not drafts have been so-assessed, the University reserves the
right to require an electronic version of the final document (as submitted) for
assessment as above.
Signature: Tosan. T. Edematie
Date: 25.01.2019

AbstractPurpose – Despite the fact that research in readiness is growing, there are gaps in the context of enacting readiness within healthcare. Adopting the complex adaptive systems theory, this thesis aimed to extend the theoretical understanding of the concept of organisational readiness for innovation in the context of healthcare. It examined the meanings and the processes involved in achieving and maintaining a state of readiness for innovation in the UK public healthcare services sector from the perspective of its senior leaders.
Methodological approach – The thesis included three studies. First, a narrative systematic review was conducted across different bibliographic databases to explore the associated meanings and factors influencing organisational readiness for innovation. The search revealed that there were different meanings and processes associated with the development, implementation and sustainability of the construct. These included the stage vs. the process-based debate, the various disagreements amongst theorists on the multifaceted nature of the construct and its impact (i.e. behavioral, psychological and structural), and its relation to organisational change. This led to the adoption of a qualitative research method to further investigate the topic in the context of UK public healthcare services. Twenty semi-structured individual interviews in total were conducted. The data were collected in two phases. The first phase consisted of a total of ten senior managers working in NHS organisations. This first phase investigated from an internal point of view how organisational readiness for innovation was successfully managed within the National Health Service (NHS) – it explored meanings, discrepancies between organisational change management and innovation, and identified contextual (pre) conditions and processes of how leadership may influence readiness for innovation, its enactment and sustainability. In the second phase, a total of ten semi-structured personal interviews were conducted with senior management representatives from the Academic Health Science Networks groups. This second phase provided information on the perspective and role of an external facilitator’s organisation in supporting and sustaining an innovation ‘ready’ culture in the NHS. Conducting the study in two phases allowed the researcher to see the level and reasons for alignment in the senior management’s views from different organisational perspectives – internal and external.
Summary of results – A significant distinction was found in the senior managers’ opinion regarding the definition of innovation and organisational change. Successful innovation management was described as a much more complex and intricate process than organisational change management. Readiness was perceived as an iterative process of interaction between different stakeholders, their new ideas and the environment to enable innovation development and service improvement. Participants acknowledged that readiness for innovation was driven by collective engagement and intrinsic motivation from members of the NHS organisation. The findings presented, among others, some unique key contextual factors enabling organisational readiness for innovation which include: free spaces, communities of practice, and five types of leadership style: systems leadership, collective leadership, distributed leadership, lateral leadership, and transformational leadership.
Conclusions – The study generated new understanding about the theoretical distinction of innovation from organisational change. It provided new rationale about the meaning of organisational readiness for innovation based on views from those managing the process internally and externally in the NHS. The study recommended a conceptual framework enabling scholars, practitioners, senior managers, and policy makers to understand the actions required in order to prepare the NHS for the long-term success, adaptability, and the sustainability of organisational innovations in healthcare services.
AcknowledgementsFirst, I am grateful to the Almighty God for granting me my heart desire to
embark on this research project and showing me his endless love and grace
throughout the duration of the PhD study. I am also grateful to my
supervisors, Dr Theopisti Chrysanthaki for her extensive support and
direction, and Prof Jane Hendy for giving me the constant guidance and
constructive criticism. I thank them very much for their effort that has enabled
the completion of my PhD. Also, I would like to thank the Senior
Administrative Officer for Research Degrees, Karen Short, for her motivation
and support through my PhD study.
I am grateful to the senior managers at the Academic Health Science
Networks for their help and time. I also thank the senior managers at the
Clinical Commissioning Group in southeast England, the NHS Trust in east
London, and the NHS regulatory body in south London. Without their
participation, it would have been difficult to achieve the outcome of this
research.
I am also indebted to my family, my friends Aizehi, Ugochi, Seyi, my colleague
Nouf, and my editor Dr Cherrell who rendered remarkable services in a short
space of time. Without their encouragement, support, and understanding, the
PhD would have been quite difficult to complete. Lastly, thank you to the team
at the Library and Learning Support that provide solutions to technical
problems to improve learning experiences.

Table of Contents
DECLARATION OF ORIGINALITY........................................................................................... II
ABSTRACT...................................................................................................................................... III
ACKNOWLEDGEMENTS............................................................................................................ IV
CHAPTER 1....................................................................................................................................... 11.1 INTRODUCTION.........................................................................................................................................11.2 RESEARCH GAP.......................................................................................................................................51.3 RESEARCH QUESTIONS AND OBJECTIVES.....................................................................................81.4 METHODOLOGY.....................................................................................................................................101.5 THEORETICAL CONCERNS: A NEW FRAMEWORK OF INNOVATION READINESS.............111.6 CONTRIBUTION OF RESEARCH........................................................................................................121.7 OVERVIEW OF THE THESIS................................................................................................................12
CHAPTER 2..................................................................................................................................... 15
AN OVERVIEW OF THE INNOVATION MANAGEMENT LITERATURE....................152.1 INTRODUCTION.......................................................................................................................................152.2 DIFFERENTIATING BETWEEN INNOVATION AND ORGANISATIONAL CHANGE...................172.3 TYPOLOGIES OF INNOVATION...........................................................................................................192.4 THE INNOVATION THEORIES.............................................................................................................22
2.4.1 Schumpeter’s Economic Theory........................................................................................222.4.2 Rogers’ diffusion theory of Innovation.............................................................................24
2.5 INNOVATION PROCESS MODELS....................................................................................................282.5.1 Linear models of innovations................................................................................................312.5.2 Non-linear models of innovations......................................................................................33
2.6 INNOVATION NEEDS IN THE NHS...................................................................................................352.7 FACTORS THAT LIMIT SUCCESSFUL INNOVATION MANAGEMENT IN THE PUBLIC HEALTHCARE SECTOR UK.........................................................................................................................392.8 ORGANISATIONAL READINESS – A PRECEDENT FOR SUCCESSFUL INNOVATION ADOPTION.........................................................................................................................................................452.9 CHAPTER SUMMARY............................................................................................................................48
CHAPTER 3..................................................................................................................................... 49
A SYSTEMATIC REVIEW ON THE ASSOCIATED MEANINGS AND FACTORS INFLUENCING ORGANISATIONAL READINESS FOR INNOVATION......................49
3.1 INTRODUCTION.......................................................................................................................................493.2 THE SYSTEMATIC LITERATURE REVIEW METHOD.....................................................................51
3.2.1 Planning phase............................................................................................................................. 513.2.2 Search phase................................................................................................................................ 52Inclusion criteria........................................................................................................................................ 57Exclusion criteria...................................................................................................................................... 583.2.3 Storing the results....................................................................................................................... 593.2.4 Study selection and screening phase..............................................................................593.2.5 Data appraisal and synthesis phase................................................................................613.2.6 Study limitations........................................................................................................................... 61
3.3 RESULTS..................................................................................................................................................693.3.1 Background theory underlying organisational readiness.....................................693.3.2 Readiness is a change message.......................................................................................713.3.3 Readiness is perceived capability.....................................................................................763.3.4 Readiness is commitment to change...............................................................................783.3.5 Readiness is organisational fit.............................................................................................823.3.6 Readiness as stages of change.........................................................................................84

3.3.7 Readiness is a process-based synthesis......................................................................853.4 DISCUSSION............................................................................................................................................863.5 CHAPTER SUMMARY............................................................................................................................89
CHAPTER 4..................................................................................................................................... 91
EPISTEMOLOGICAL AND METHODOLOGICAL FRAMEWORK................................914.1 INTRODUCTION.......................................................................................................................................914.2 THE RESEARCHER’S EPISTEMOLOGICAL POSITION..................................................................914.3 THE RESEARCH DESIGN.....................................................................................................................954.4 QUALITATIVE DATA COLLECTION.....................................................................................................97
4.4.1 The sampling strategy..........................................................................................................994.4.2 Participants recruitment.................................................................................................... 101
4.5 THE ANALYTIC PROCESS.............................................................................................................1034.6 DEMONSTRATING RIGOR.............................................................................................................108
4.6.1 Credibility................................................................................................................................... 1084.6.2 Transferability......................................................................................................................... 109
4.7 ETHICAL CONSIDERATIONS............................................................................................................1104.7.1 Voluntary participation and Informed consent.....................................................1104.7.2 Confidentiality and anonymity.......................................................................................1104.7.3 Safety of participants and researcher.......................................................................111
4.8 CHAPTER SUMMARY.........................................................................................................................111
CHAPTER 5.................................................................................................................................. 112
EXPLORING THE CONCEPTUALISATION OF ORGANISATIONAL READINESS FOR INNOVATION IN THE PUBLIC HEALTHCARE SERVICES DELIVERY SECTOR: THE INNER CONTEXT.........................................................................................112
5.1 STUDY AIMS.........................................................................................................................................1125.2 METHOD................................................................................................................................................ 117
5.2.1 Participants.................................................................................................................................. 1175.2.2 The interview schedule......................................................................................................... 1175.2.3 Data collection process......................................................................................................... 122
5.3 REFLECTIONS OF THE RESEARCHER ON INTERVIEW PROCESS.......................................1225.4 PERSONAL REFLEXIVITY..................................................................................................................1235.5 RESULTS...............................................................................................................................................124
5.5.1 Different or same concepts? Accounting for differences in the management of innovation and organisational change..................................................1245.5.2 Defining organisational readiness for innovation in a public healthcare context......................................................................................................................................................... 1315.5.3 Enablers of organisational innovation state of readiness..................................137
5.6 DISCUSSION.........................................................................................................................................1535.7 CHAPTER SUMMARY...............................................................................................................................169
CHAPTER 6.................................................................................................................................. 171
EXPLORING THE ENABLING FACTORS AND PROCESSES UNDERLYING AN INNOVATION READINESS STATE OF BEING: THE OUTER CONTEXT..............171
6.1 STUDY AIMS.........................................................................................................................................1716.2 METHOD................................................................................................................................................ 175
6.2.1 Participants.................................................................................................................................. 1756.2.2 The interview schedule....................................................................................................... 1756.2.3 Data collection process......................................................................................................... 179
6.3 REFLECTIONS OF THE RESEARCHER ON THE INTERVIEW PROCESS..............................1796.4 RESULTS...............................................................................................................................................1806.4.1 ENHANCING AND ENABLING PROCESSES FOR AN INNOVATION DRIVEN CULTURE180
6.4.2 Leadership, what about it? And its role in enabling a culture of innovation......................................................................................................................................................................... 1996.4.3 Catalysing readiness: what can we learn from innovators?............................207
6.5 DISCUSSION.........................................................................................................................................2126.6 CHAPTER SUMMARY.........................................................................................................................223
CHAPTER 7.................................................................................................................................. 224
DISCUSSION AND CONCLUSION.......................................................................................2247. 1 GENERAL OVERVIEW.......................................................................................................................2247.2 CRITICAL SUMMARY OF STUDIES.................................................................................................2247.3 BRINGING IT ALL TOGETHER: KEY FINDINGS TO THE RESEARCH QUESTIONS...........2257.4 THE STRENGTHS AND LIMITATIONS OF THE RESEARCH AND FUTURE DIRECTIONS. 2337.5 CONCLUSION.......................................................................................................................................235
APPENDICES.............................................................................................................................. 236
REFERENCES............................................................................................................................. 281

List of Figures
Figure 2. 1: Model of Disruptive Innovation.......................................................................21Figure 2. 2: Schumpeterian four-phase cycle...................................................................23Figure 2. 3: Innovation adoption curve based on the diffusion of innovation theory......................................................................................................................................................27Figure 2. 4: The innovation process model........................................................................28Figure 2. 5: Basic linear model of innovation....................................................................31Figure 2. 6: First generation ‘technology push’ model of innovation....................31Figure 2. 7: Second-generation market pull model of innovation...........................32Figure 2. 8: The innovation pathway.....................................................................................38Figure 2. 9: Stages of organisational change.................................................46
Figure 3. 1: Systems thinking framework for analysing adoption and diffusion of innovation in healthcare system.........................................................................................50Figure 3. 2: Extract of final search string.............................................................................55Figure 3. 3: Search limiter based on major subject heading during data search................................................................................................................................................................... 56Figure 3. 4: Search and selection scheme.........................................................................60Figure 3. 5: Lewin’s processes of planned change.......................................................70
Figure 5. 1: The NHS – how providers are regulated................................................116
Figure 7. 1: A framework for developing and enacting a state of organisational readiness for innovation in public healthcare services organisation...................................................................................................................................... 232

List of Tables
Table 3. 1: Narrative overviews used as key sources in this review....................62
Table 5. 1: Research questions, aims and exempla interview questions...............115Table 5. 2: Demographic characteristics of participants..........................................118Table 5. 3: Themes and sub-themes on the differences in the management of innovation and organisational change...............................................................................125Table 5. 4: Themes and sub-themes on the meanings of organisational readiness for innovation.............................................................................................................133Table 5. 5: Themes and subthemes on the enablers of organisational innovation state of readiness..................................................................................................139
Table 6. 1: Research study questions, aims and exempla interview questions................................................................................................................................................................. 174Table 6. 2: Demographic characteristics of participants..........................................176Table 6. 3: Themes and sub-themes on enhancers and enabling processes for an innovation driven culture..............................................................................................182Table 6. 4: Themes and sub-themes on leadership and its role in enabling innovation culture.......................................................................................................................... 201Table 6. 5: Themes and sub-themes on the lessons NHS can learn from other industry............................................................................................................................................... 208

List of Appendices
Appendix A: Systematic review search strings.............................................................236Appendix B: Interview guide for NHS study....................................................................244Appendix C: Interview guide for AHSN study................................................................245Appendix D: Participant information sheet......................................................................247Appendix E: Introductory brief email...................................................................................249Appendix F: Favourable Ethical Opinion..........................................................................250Appendix G: Consent form.......................................................................................................252Appendix H: Risk assessment form....................................................................................253Appendix I: One complete transcript from the NHS dataset..................................254Appendix J: One complete transcript from the AHSN dataset..............................264

Chapter 11.1 Introduction
“We need new ways of thinking and of working in order to accommodate
the complexity of the challenge for health system innovation and change”
(Herbert and Best, 2011, p. 31)
The United Kingdom’s healthcare industry is portrayed in many different ways,
but arguably it is among the best in the world. The World Health Organisation
ranked the UK as the eighteenth best in the world out of 191 countries. This
places it in the top ten per cent (World Health Organisation, 2000). Healthcare
in the UK is provided by public health services, that is, the National Health
Service (NHS) that provides free care to patients at the point of use. The NHS
is the major provider of healthcare services in England. It administers free
healthcare to everyone in need of it at the point of delivery and is the world’s
largest integrated national health system and the largest public sector
provider of healthcare (Williams et al., 2008; Barlow, 2011; Department of
Health, 2011a). The UK private healthcare sector, in comparison to the public
sector, is focused on profit-making and some aspects are self-financed while
others may be covered by medical insurances. In addition to this, the NHS
contracts private providers to reduce the waiting lists in order to ensure that
patients are seen as quickly as possible (Doyle and Bull, 2000; Pym, 2018).
In recent times (2018), the NHS Trust has been in the news for poor patient
quality care as seen in the case of Rosie Dawson. It was reported that she
arrived at Torbay General Accident and Emergency Department following a
gynaecological problem which left her bleeding and in severe pain. As the
hours went by, and with the staff struggling to find free beds, Rosie was
examined on a trolley in front of other patients in the corridor (BBC News,
2018). Furthermore, there have been other reports of thousands of people
being left stuck in ambulances waiting for Accident and Emergency staff to
find free beds. Patients were reportedly being treated or ‘dying prematurely’
on hospital corridors, despite the best efforts of the healthcare staff (Triggle,

2018). These events are among some of the predicaments the National
Health Service (NHS) Trust has faced in recent times. Overwhelmed with the
increasing demands, there is a desperate search for solutions that can
respond to these needs by providing quality care at a reduced cost. It has
been suggested that the adoption of ‘innovation’ presents a significant
opportunity to assist the public healthcare services delivery sector to do this
(Barlow and Burn, 2008; Christensen, Groosman and Hwang, 2009; Weberg,
2009; D’Alfonso et al., 2016; Collins, 2018).
Innovation in healthcare means several different things ranging from new
surgical products and medical practices, patient education tools and protocols
(i.e. objects), new management structures or financial schemes to newly
proposed service delivery models that can all lead to significant changes to
the organisation and for the wider society (West and Farr, 1990; Damanpour,
1991; Greenhalgh et al., 2005; Weberg, 2009; Dixon-Woods et al., 2011).
England is recognised as a world leader in healthcare innovations
(Department of Health, 2011a) with some of its native groundbreaking medical
innovations including the first kidney transplant, development of computed
tomography scans and magnetic resonance imaging scanners, the
contraceptive pill, antibiotics, vaccines, in-vitro fertilisation, and the DNA
double helix (Department of Health, 2011a). In addition, there are the new
drug combinations to reduce low-density lipoprotein cholesterol by as much
as 75 per cent; a hybrid insulin delivery system that acts as an artificial
pancreas to manage diabetes; neuromodulation systems implant to treat
sleep apnea; and scalp cooling systems to reduce hair loss from
chemotherapy treatments (Cleveland Clinic Innovations, 2017).
To understand innovation, there is the important need to conceptualise it as a
multi-phase process which involves the successful initiation, adoption,
implementation, and dissemination of an idea into widespread use across the
whole service (West and Farr, 1990; Damanpour and Wischnevsky, 2006;
Department of Health, 2011a). Sometimes, the challenge is at the adoption
and implementation phases. Adoption is defined as when an individual
member of an organisation or any other decision-making unit decides to

engage in the process of putting an idea into practice (Rogers, 2003;
Department of Health, 2011a). It entails a mental process based on a
reflective evaluation of the proposed idea(s) from a wide range of
perspectives (technical, financial and strategic). Together, all these will
influence the decision to accept or reject the innovation as the desired
solution. This decision often occurs at the individual level (Rogers, 2003), but
also takes place at the top management level as their perspective on the
innovation will influence their willingness to allocate resources for its adoption.
The implementation phase consists of a series of actions and events that aim
to modify the innovation to prepare the organisation for trying it out and for its
continual use. This requires the collective commitment of the members of an
organisation to habitually and routinely use it in their work (Klein and Sorra,
1996; Weiner, Lewis and Linnan, 2009; Shea at al., 2014). Weakness or
failure in either the adoption or the implementation phase can hamper the
success of any innovation as shown by Collins (2018) in his review of how to
speed up the adoption of service innovations in the NHS. The review
highlighted instances of the slow adoption of innovation across the system. In
many cases, this failure to adopt and implement such features could also be a
result of the lack of funds to introduce innovation into the system since the
NHS delegated only 0.1 per cent of available resources to the adoption and
dissemination of innovation (Collins, 2018). Other contributory factors include
the roll-out time, the need for additional resources and training, a resistance to
change, reluctance to pursue innovations outside the organisation’s core
responsibilities, and a display of an egoistic behaviour amongst clinical staff.
These have all been known as some of the primary reasons why the rate of
innovation adoption is slow in the public healthcare service delivery
organisations (Greenhalgh et al., 2005; MacMahon, MacCurtain and
O’Sullivan, 2010; Collins, 2018). It is within this context that the study of
organisational readiness for innovation is emerging in healthcare service
research.
Organisational readiness is a complex, multi-dimensional and multi-faceted
construct for which different conceptualisations have been proposed
(Armenakis, Harris and Mossholder, 1993; Weiner, 2009; Rafferty, Jimmieson
and Armenakis, 2012; Attieh et al., 2013; Holt and Vardaman, 2013).
Organisational readiness has been identified as the vital ‘antecedent’ that
influences the behaviour and attitude of an individual towards a proposed
change endeavour (Armenakis, Harris and Mossholder, p. 681). Several case
studies have raised the significance of readiness in innovation adoption (i.e.,
acceptance) and implementation (i.e., use). The UK government sponsored
the Whole Systems Demonstrator Programme which is the world’s largest
randomised control trial of telehealth and telecare and the benefits from it
were clear, as the trial revealed that telehealthcare is associated with lower
mortality and reduced emergency admission rates (Steventon et al., 2012).
However, other results from the trial demonstrated that telehealthcare was not
cost effective (Henderson et al., 2013), nor did it appear to alter patients’ state
of well-being (Steventon et al., 2013). The demonstrator programme led to the
strengthening of existing communication links between health and social care,
but overall, it was not a whole system change. Both the systems and the staff
were not ‘ready’ for a truly integrated service and for new ways in which
services were delivered (Hendy et al., 2012). The potential of telehealthcare
innovation may be mixed, but the failure concerning service integration across
NHS health and social care has been linked to a ‘lack of organisational
readiness’ (Hendy et al., 2012). Here, Hendy et al. (2012, p. 5) stated
readiness as the “extent to which the participating sites involved were
prepared to participate and succeed in the innovation endeavour.”
Another study conducted in a primary healthcare organisation in South Africa,
showed assessing organisational readiness for change towards adopting
health innovations, such as mental health services, is necessary to facilitate
the successful implementation of new services into practice (Brooke-Sumner
et al., 2018). This is because assessing contextually appropriate measures of
organisational readiness helped to reveal potential implementation barriers
(e.g., low staff motivation, lack of time and resources, and low staff perception
for the need of change) and provided the opportunity to close any gaps prior
to resources mobilisation for the proposed new service. Here, organisational
readiness for change is regarded as a shared psychological state which is
contingent on organisational members’ determination to change (i.e.,

commitment) and their belief in the capability to implement change (i.e.,
efficacy) (Weiner, 2009).
1.2 Research gap
There is particular interest in conceptualising and measuring readiness for
innovation in health service delivery organisations (Greenhalgh et al., 2004;
Oostendorp et al., 2015; Sheard, Jackson and Lawton, 2017). There has also
been work on the development of tools to assess an organisation’s readiness
to adopt innovations in the healthcare sector through the use of Likert-type
scale, in which responses are scored against theoretically-derived factors.
The Texas Christian Union Organisational Readiness for Change (TCU-ORC)
is one of the most common measures adopted in healthcare (Simspon and
Dansereau, 2007). Unfortunately, reviews have revealed that some of the
available organisational readiness instruments exhibit weakness in the validity
of their scales (Holt et al., 2007; Weiner, Amick and Lee, 2008). Though a few
studies exist that have attempted to validate existing measuring scales of
readiness (Snyder-Halper, 2002; Khan et al., 2014; Shea et al., 2014), the
field of system readiness research is relatively minute in health services
research (Greenhalgh et al., 2004; Oliveira et al., 2017). This is combined with
two main issues which this thesis seeks to provide clarify:
First, researchers in the field of healthcare conducting organisational
readiness research have done so independently, assessing specific types of
change, particularly in information technological, whilst using different
theoretical perspectives. This has led to proliferation of the term and
conceptual ambiguity on the meaning of organisational readiness (Weiner,
Amick and Lee, 2008). More specifically there has been failure to distinguish
organisational readiness for change literature from that of readiness for
innovation, and in accepting theories of change to be used interchangeably in
management of readiness for innovation processes. It is worth mentioning
that planning for change, and planning for innovation are two completely
different processes (Zaltman, Duncan and Holbek, 1973; King and Anderson,
2002; Van de Van et al., 2008; Vincent, 2013). Organisational change is an
approach to moving individuals, organisational members, and teams from a

current state to a desired/known one. Managers tend to facilitate the process
of change by applying the principles underlying several change management
tools. Such framework includes Kotter’s (1996) eight-step model which is one
of the most popular approaches for leading change. This model advises
managers to create a sense of urgency for the proposed change, empower
teams, create a vision for the change, and, once change is enacted, highlight
the change benefits in order to maintain the momentum. McKinsey’s 7-S
model is another powerful framework which looks at the seven crucial
elements that enhance organisations success – strategy, structure, systems,
shared values, styles, staff and skills. The model is about analysing all of the
7-S, making sure each element supports the other, thereby, giving
management knowledge on what change needs to be implemented in order to
make a business change endeavour viable. These change management tools
are beneficial as they offer a simple sequence of stages organisational
managers can follow to implement successful change and improve the
outcomes of the change programs. On the other hand, innovation
management is about managing processes of product, programs, and
services in an organisation, moving from the status quo to the unknown, as
the desired outcome is oftentimes unpredictable (Rogers, 2003; Barlow, 2011;
Department of Health, 2011a; Van de Ven, 2017; Collins, 2018). Although a
change management framework may increase the odds of steering the
innovation process from development to implementation, managers have no
control over the obstacles that may be encountered along the way (Van de
Ven, 2017). Studies so far have failed to take into account the heterogeneity
of the processes involved and that innovation management is relatively more
complex to enact because a simple organisational change does not have the
same impact as innovation.
Second, there is an inconsistent notion regarding the approach for theorising
readiness during the management of an intended organisational innovation.
The existing conflict is between stage-based and process-based
conceptualisation. A stage-based approach declares that readiness is
pertinent to a particular state during the process of enacting an organisational
change. For instance, Armenakis, Harris and Mossholder’s (1993) three-stage

model presents readiness as the first stage before the initial adoption and
implementation. In contrast, a process-based conceptualisation posits that
readiness is a continuous assessment throughout a given change
intervention, rather than at one-point in time (Stevens, 2013). The conceptual
dissimilarity in operationalising the construct of readiness makes it difficult for
organisational managers to understand the engagement and assessment of
readiness during a change program. It has been argued that a process-based
rationalisation offers a more potent and holistic theory for exploiting the
sequence and movement of change events rather than that of a stage-based
conceptualisation (Pettigrew, 1997; Hernaus, 2008; Stevens, 2013). The
complexity due to the structure, and internal politics of today’s healthcare
service organisations requires a flexible approach to coping with the changing
demands of its environment. Understanding the problems of health systems
requires taking into account the behaviour of the system over time rather than
researching the process and impact based on ‘static snapshots’ (Senge,
2006). Thus, a process-based approach presents an appropriate way to
overcome corresponding problems while providing a timely feedback as
assessment is carried out continuously. Such an approach enables the
researchers to capture the changes in the relationship between the processes
and the outcomes over time (Pettigrew, 1997; Rubin, Pronovost and Diette,
2001). On the other hand, a stage-based approach does not capture the
influence of readiness over time in a given context, and fails to appreciate that
the impact of readiness might differ at subsequent points in time (Hernaus,
2008; Stevens, 2013).
The need to focus on a process-based view of organisational readiness has
been recognised, yet research on this is limited and largely focused on
examining the iterative nature of readiness at an individual level. The
individual level of readiness is an important motivational factor for successful
implementation of change as it encompasses the individuals’ beliefs and
motivation towards change (Christl et al., 2009). However, assessing
readiness at the organisational level is crucial for ensuring the success of
improvement programmes because implementation is not something that can
be achieved in isolation. It requires collective decision-making and a

commitment to continuous application without which implementation could fail
(Van de Ven et al., 2008; Weiner, 2009; Burnett et al., 2010). Apart from this,
designing and evaluating innovations for enhancing health systems require
those involved to “stand back from a fixation with the individual components”
and take the whole system into consideration in order to strengthen the
innovations (Adam and de Savigny, 2012, p. iv1). In the absence of a
theoretical elucidation on these issues, there will be the continued inability to
validate the measures of readiness and to promote cumulative understanding.
Gaps in this information make it difficult for the public healthcare sector to
arrive at an appreciation of the importance of organisational readiness for
successful innovation management. It, therefore, seems logical to first
consider the meaning of readiness and how it has been conceptualised in
research on organisations. This would include a consideration of factors that
might influence an organisation and its members’ decision to become
informed and engaged, and the approach healthcare managers can
effectively adopt in order to be ready prior to, during and after the innovation
process.
1.3 Research questions and objectives
In keeping with a process-based view, the overall purpose of this thesis is to
explore senior management’s perspective and their significant role in
developing and articulating persuasive arguments in effecting readiness for
innovation in the public healthcare sector. This thesis will seek to provide
conceptual clarity on the meaning of readiness for innovation and to explain
the processes that may enable or inhibit healthcare leaders in facilitating and
increasing readiness in their organisations. It will examine how individuals -
internal and external NHS senior managers of the public healthcare services
sector - make sense of the innovation process; why readiness is significant to
the process of innovation management; and how these individuals perceive
and enact readiness in context (Eby et al., 2000). This group of stakeholders
was chosen because of their role in the decision-making processes that lead
to transformational change. They also tend to engage largely in sense-making
activities and employ strategies to guide members of their organisations as

well as to foster their commitment to and support for the organisation’s
innovative goals (Damanpour, 1991; Jung, Chow and Wu, 2003; Robinson
and Goudy, 2009; Avery and Bergsteiner, 2011; Kyratsis, Ahmad and
Holmes, 2012; Jyoti and Dev, 2015). Most organisations have what is called
an authority based innovation decision-making approach (Rogers, 2003). This
means that decisions about whether or not an organisation adopts an
innovation rests within this authority. Research has shown that organisational
leaders play an instrumental role in developing and sustaining the climate for
change and innovation (Kimberly and Evanisko, 1981; Meyer and Goes,
1988; Damanpour, 1991; Damanpour and Schneider, 2006). Given the above
aim, this thesis seeks to answer a number of research questions which are
formulated as follows:
1. How is innovation to be distinguished from organisational change
and why?
2. What is organisational readiness for innovation and why does it
matter?
3. What are the key barriers and facilitators of readiness for
innovation in healthcare service organisations (NHS)?
In keeping with these research questions, these are the study objectives:
1. To conduct a systematic review of the literature on the
conceptualisation of “organisational readiness for innovation” in
healthcare services over the past decade, and to identify the gap
in research.
2. To explore senior managers’ construction of the meaning of
readiness.

3. To identify the barriers and facilitators (i.e. agents, routines,
practices, structures) that provide the time and context for the
development of an organisational ‘ready’ culture.
4. To develop a framework that managers in public healthcare
service organisations can apply towards developing and enacting
a state of readiness.
1.4 Methodology
To conduct the research and investigate the research questions stated above,
a narrative systematic literature review and qualitative approach using
individual semi-structured interviews was employed. These methods were
purposively chosen to elucidate particular aspects of the research questions.
In a field such as healthcare where researchers, policy makers and healthcare
providers are inundated with an abundance of information, a systematic
review of the literature is necessary to effectively identify the existing
knowledge and to supply critical data to provide a rationale for decision-
making (Mulrow, 1994). The systematic review provides an explicit method for
obtaining answers to some aspect of the research questions, thereby,
enabling accurate and reliable conclusions for further investigation, using
qualitative approach (Gopalakrishnan and Ganeshkumar, 2013). Also, the use
of qualitative research is particularly appropriate for generating and
developing theoretical knowledge within complex and multi-faceted contexts
and this can also help to provide a better understanding of the contexts as
well as the events within the contexts or the experiences (Britten et al., 1995;
Sofaer, 1999; Braun and Clarke, 2013). This combined approach allows for
triangulation in regards to the empirical evidence and should contribute to a
deeper and more nuanced understanding of the topic.
1.5 Theoretical concerns: A new framework of innovation readiness
The discussion of the theoretical concerns of this thesis together with the
review of the literature on innovation management and readiness and the
context under study (public healthcare service organisations) led to the
adoption of the complex adaptive systems theory as the main theoretical
framework for this thesis. Nesse et al. (2010) argue that healthcare systems
frequently fail to innovate as they do not yet recognise the implications of
complexity thinking in managing system implementations. Complex adaptive
systems thinking provides an approach to problem solving as it appreciates
the complex nature of systems as being continuously changing, governed by
history and feedback and where the role and influence of agents and context
are critical. In addition, new policies and actions of different agents often
generate counterintuitive and unpredictable consequences, in some cases,
long after polices have been implemented (Checkland, 1999; The Health
Foundation, 2010; Adam and de Savigny, 2012). Complex adaptive systems
thinking has been applied in healthcare to help explain the characteristics of
leadership that will result in better performance (Weberg, 2012). It has been
also used to provide an additional way to consider the organisational and
behavioural changes required to accelerate innovation (Eby et al., 2000; Plsek
and Wilson, 2001; Atun et al., 2009; Datte and Barlow, 2010; McDaniel,
Driebe and Lanham, 2013). The use of complex adaptive system theory in
healthcare research and for policy design has stimulated much interest.
However, its application has been criticised given the dearth of empirical
research available to allow for comparative evidence (Datte and Barlow, 2010;
The Health Foundation, 2010; Atun, 2012). Therefore, the thesis will explore
how systems thinking can be used to effectively increase innovation,
particularly because it unveils the elements of success and failure in
implementing and sustaining readiness in the healthcare context.

1.6 Contribution of research
The core contribution of this research is to deepen the theoretical
understandings on the conceptualisation and practices of readiness in the
public healthcare services sector. This is based on the managerial
perspectives of how several conditions and factors could be used to influence
public healthcare systems to move to a state of innovation readiness. The
research also sets out to propose a new theoretical framework, based on the
managerial insights as well as the principles of complex adaptive systems, to
inform healthcare systems on how to be innovation ready and for managerial
practicality. The thesis further makes policy recommendations and also offers
suggestions for future research in this largely unexplored field.
1.7 Overview of the thesis
Chapter Two
Following this introductory chapter, Chapter 2 reviews and analyses the
literature on innovation management with the goal of exploring the topic to
gain a broad overview on the theories of innovation management, and the
factors identified as being influential in enabling the development of a
successful culture of innovation in the public healthcare sector, specifically in
the National Health Service (NHS) England.
Chapter Three
Chapter 3 presents a systematic literature review that synthesises and
critically appraises the current literature and theoretical debates surrounding
the concept of organisational readiness for innovation. This was done in order
to specifically address the following question: How is organisational readiness
for innovation conceptualised? The aim of the review was to investigate the
meaning of organisational readiness for innovation, and how the determinants
for its implementation have been theorised and researched empirically. The
review also discusses the principles of the complex adaptive systems theory
as a framework to underpin the present research in the exploration of the
concept under study.
Chapter Four
The aim of the fourth chapter is to discuss and justify the researcher’s
epistemological stance, and the implications of using qualitative research
methodologies within the thesis. This is followed by a more detailed
consideration of the research methodologies involved and the criteria used to
assess rigour, particularly in regard to the qualitative approach used.
Chapter Five
The main aim of this chapter is to explore the senior managers’ perspectives
on the meaning of organisational readiness in order to gain an understanding
of its significance and establish if differences exist between the management
of innovation and organisational change. Data from interviews with the ten top
managers were analysed using the thematic analysis principles as explained
in Chapter Four. The findings from the data are presented in this chapter.
Chapter Six
Chapter 6 discusses the second and last empirical study of the thesis which
used an exploratory qualitative interview methodology approach to investigate
ten senior managers’ view from an external organisation. This was done to
gain an external perspective on the enablers and enabling processes towards
enacting an innovative organisational culture. The study also investigated the
role of leadership in influencing readiness. The findings are presented in this
chapter along with the researcher’s personal reflections during the interview
process.
Chapter Seven
In Chapter 7 the main findings of the systematic review and the empirical
studies presented in this thesis are drawn together and discussed in relation
to the extent to which the main aims of the thesis have been achieved. The
wider theoretical and practical implications arising from the main findings are
also explored and the implications of the results are considered in relation to
some of the main theories of innovation management and organisational

readiness. The chapter concludes by reflecting on the methodological
challenges, the strengths and limitations of the research and with
recommendations for further research being made.

Chapter 2
An overview of the innovation management literature
2.1 Introduction
In a modern and fast-paced environment characterised by hyper-competition
and an uncertain economic climate, innovation provides a competitive
advantage and is essential for an organisation’s success, economic growth,
and survival (D’Aveni, 1994; Hage, 1999; Johannessen, Olsen and Lumpkin,
2001). Organisations need to constantly innovate to generate new business
advantages (Tushman and O’Reilly, 1996; Dess and Picken, 2000) and
acquire capabilities that will guarantee success in the dynamic business
environment (Teece, Pisano and Shuen, 1997; Eisenhardt and Martin, 2000).
Innovation is a fundamental element of today’s world (Schumpeter, 1934;
Drucker, 1985) and is usually adopted to generate and maintain a sustainable
competitive advantage (Johannessen, Olsen and Lumpkin, 2001) which
brings benefits to individuals and society. In the commercial sector, innovation
is a key element of success for increasing market share and organisational
productivity (Fonseca, 2002; Tidd and Bessant, 2013). Recent successful
innovations include the market for automobiles, improved technological
devices (mobile phones, video conferencing), mobile banking, enhanced
safety in automobiles using airbags, and more environmentally friendly
techniques (electric vehicle adoption) (European Commission, 1995; Shaikh
and Karjaluoto, 2015; Wesseling et al., 2015; Nagy, Schuessler and
Dubinsky, 2016).
When it comes to the public healthcare service delivery organisations,
politicians, taxpayers, patients and regulators are asking for improved results
including: quicker access, earlier diagnosis, and greater sensitivity to cultural
diversity and health disparities (Plsek, 2014a). The challenges the public
healthcare sector face today call for more than simple incremental
improvements; it requires new approaches and new thinking – which is

innovation. This is so because business as usual cannot deliver the results
needed (Edwards, 2014) and history has shown that organisations that fail to
innovate will suffer. There is evidence that organisations within the public
healthcare sector are capable of innovative thinking as seen by the
introduction of the electronic outpatient system called e-RS which is expected
to reduce the number of missed appointments in the UK by half and save the
NHS at least £50 million (Armstrong, 2018a; Armstrong 2018b). This kind of
thinking has also provided digital solutions such as the wearable sensors
which enable automated observations, consequently providing better long-
term condition management for patient both in the hospital and at home.
These are some of the successful NHS innovative projects in recent times
that have delivered many benefits, such as, saving the clinicians’ time, better
patient outcomes, better access to services, and reduced waiting times.
Nevertheless, the consensus is that barriers remain in successful innovation
management across the NHS which makes it less successful than it should be
(Barlow, 2011; Department of Health, 2011a; Gifford et al., 2012). The
adoption and the spread of innovation is particularly challenging in the NHS
based on evidence showing the slow rate of the uptake and spread of
innovations (Collins, 2018).
The aim of this chapter is to give an overview of the innovation management
literature. First, the significant differences between innovation and
organisational change management are explained. The terms innovation and
organisational change have become management buzzwords in the twenty
first century (King and Anderson, 2002; Weberg, 2009; Kotsemir, Arboskin
and Meissner, 2013), with managers and academia using these terms
interchangeably. Politicians and business gurus have significantly stressed
the need for industry to respond to competition by becoming more innovative
with many step-by-step models offering a guide on how to enact such
changes successfully. Despite the familiarity of both terms, it has proved
problematic in providing clarity and precision in defining them (King and
Anderson, 2002). This chapter describes theoretical differences and critically
discusses the many meanings of innovation. Subsequently, the chapter
discusses various theories of innovation in order to give an understanding of

how innovation is seen. Types of innovation and their characteristics are
considered critically. The economic theory, the diffusion theory, and the linear
theory of innovation in healthcare which have gained recognition in
management discipline are scrutinised to give an understanding on how
innovation is conceptually developed, occurs and is evolving within the
healthcare context. The major issues hindering successful organisational
innovation in the healthcare sector will also be highlighted, particularly those
pertinent to the UK’s National Health Institute (NHS). The chapter concludes
with the importance of organisational readiness in aiding the public healthcare
sector in a better delivery of innovations.
2.2 Differentiating between innovation and organisational change
The main definitional issue which has engaged academic writers is how to
distinguish between innovation and organisational change. The conflation of
these two distinct terms has merely served to muddy the waters (King and
Anderson, 2002, p. 2). The distinction between organisational change and
innovation is relevant to this study because as the two terms are sometimes
used interchangeably, clarification of the difference is important in order to
focus on innovation management.
First, Zaltman, Duncan and Holbek (1973) defined innovation as any idea,
practice, or tangible thing perceived as new to the adopter (e.g., an individual,
whole organisation, work team or group). A new idea may be the starting point
of an innovation, but cannot be called an innovation until its successful
adoption – i.e., the implementation or use of the new ideas (Zaltman, Ducan
and Holbek, 1973; Damanpour and Evan, 1984). Organisational change is
the alteration in the structure and functioning of a social system. Whether this
is perceived as innovative or novel is not relevant (Zaltman, Duncan and
Holbek, 1973) and whether this change requires adoption or acceptance
amongst organisational members might also be irrelevant. Using this
rationale, Zaltman, Duncan and Holbek (1973, p. 10) cite that “all innovations
imply change, but not all change involves innovation since not everything an

organisation adopts is perceived as new.” King and Anderson (2002, p. 2-3)
explain that innovation must be “new to the social setting within which it is
introduced, although not necessarily new to the person(s) introducing it.”
Second, an innovation must be intentional, coordinated and planned (West
and Farr, 1990; Greenhalgh et al., 2004). For example, a factory reducing its
staff or hiring new staff to minimise costs or optimise efficiency would not be
considered as an innovative change. However, if the factory adopts an
innovative model (e.g., a new project management approach) to train and
upgrade staff skills to enhance performance, this can be described as
innovative because it meets the criteria of novelty and coordinated actions.
Another example is the approach taken by successful business innovators
such as Amazon, Dell, Southwest Airlines and Apple. These companies did
not invent selling books, computer manufacturing, the provision of flight
services or phone manufacturing. Instead, they adopted new business models
in their market and secured impressive growth rates and performed better
than their competitors (Markides, 2006; Massa and Tucci, 2013).
A third distinction is developed from management philosophy. Management
scientists and organisational sociologists have described organisational
change management as a framework for managing the processes and plans
of a proposed change. The concept of change management dates to early
works like Kurt Lewin’s three-step change model (Lewin, 1951) that
recommends a management tool to facilitate the process of change
implementation within the context of organisational change. The knowledge
that innovation will follow strategy has been a prominent concept in innovation
strategy theory. Change management can be a component of innovation, but
they are not always the same thing. Van de Ven et al. (2008) provide
reasonable evidence to show that innovation management is not as simple as
organisational change management because innovation is complex with
uncertainties, setbacks and shocks along the way. Thus, while a static model
is rational and goal-oriented, it does not specify how to incorporate the
individual’s dynamism into organisational analysis. Therefore, as Van de Ven

(1986) proposed, innovation is the outcome of relationships as people have to
be engaged with each other over time to bring it about.
While innovation, by general definition is the implementation of distinctive new
ideas, this thesis is clear in defining it in healthcare services as “ a novel set of
behavious, routines, and ways of working that are directed at improving health
outcomes, administrative efficiency, cost effectiveness, or users’ experience
and that are implemented by planned and coordinated actions” (Greenhalgh
et al., 2004, p. 582).
2.3 Typologies of innovation
The classification of innovation can be attributed to Joseph Schumpeter’s
study of innovation economics (Schumpeter, 1934) where he defined
innovation in terms of novelty, that is, “a new product or a new quality of a
product; a new production method; a new market; a new supply source; or a
new organisational structure” (Schumpeter, 1934, p. 66). Most researchers
into technology and economics have focused on studying product and
process typologies as these seem to be the most popular areas. Product
innovations refer to new products introduced into relevant markets by an
organisation to fulfil the physical and non-physical needs of external
consumers or clients (Damanpour and Gopalakrishnan, 2001). Process
innovations are the introduction of new production methods, management
approaches and technology to a firm’s operations that can be used to improve
management processes to enable the creation of a product or delivery of a
service (Utterback and Abernathy, 1975; Damanpour and Aravind, 2006).
Innovation is also classified based on the magnitude or the degree to which
the innovation is ‘incremental’ or ‘radical’ (Wolfe, 1994; Gopalakrishnan and
Damanpour, 1997; Varkey, Horne and Bennet, 2008; Menguc, Auh and
Yannopoulos, 2013; Norman and Verganti, 2014). It can be a continuous or
discontinuous type of innovation; it can either advance but preserve the status
quo or upset the current conditions (Tushman and Anderson, 1986; Bessant,
2005; Moore, 2005). It can be incremental by involving minor changes in the
individual elements of the innovation or radical by involving significant

changes in the overall structure of the innovation (Henderson and Clark,
1990). Zaltman, Duncan and Holbek (1973) described radical innovation as
the degree to which an innovation differs from the existing alternative. Radical
innovations, to some extent, are disruptive of the existing systems and
change the status quo by creating brand new innovations that deliver a large
increase in value to stakeholders who can implement and adapt successfully
to the innovation. However, radically new technology is not disruptive
innovation. Radical innovations are often sporadic and discontinuous
compared to incremental innovations which are adaptive, linear and
continuous (Varkey, Horne and Bennet, 2008; Damanpour and Aravind,
2012). Incremental innovation may likely impact the organisation only, while
more radical innovation will be associated with the market and even the
industry (Crossan and Apaydin, 2010).
There are two types of innovation in healthcare: sustaining innovation and
disruptive innovation. Sustaining innovation, whether through dramatic,
incremental or radical breakthrough, makes a good product better. This type
of innovation can be often technologically challenging to apply, but matters
little as organisations are interested in profit-making and maintaining their
place in the established market (see Figure 2.1). Disruptive innovation has
been argued as the future for healthcare. There have been misconceptions
that disruptive innovations refer to radically new technologies. Clayton
Christensen, the founder of disruptive theory, has provided conceptual clarity
on the meaning of disruptive innovation. Christensen, Grossman and Hwang
(2009) defined disruption as an innovation that converts complex, intuitive
processes into simpler, less costly, and accessible innovations. On the other
hand, technical radical innovations may or may not be disruptive because the
purpose of most technologies is to provide greater values to their existing
mainstream customers, and, therefore, sustain the functions of the current
system. Airplanes that fly faster, mobile phone batteries that last longer, or
computers that process faster are all examples of sustaining innovations
(Christensen, Grossman and Hwang, 2009).
Figure 2. 1: Model of Disruptive Innovation
Source: Christensen, Grossman and Hwang (2009)
Christensen, Grossman and Hwang (2009) states that only disruptive
innovations possess the following three characteristics: (1) it simplifies
problems that previously required unstructured processes of intuitive
experimentation to resolve; (2) it is affordable and accessible; and (3) it
creates an economically coherent value network. An example of a disruptive
innovation is Apple Music which disrupts the marketplace by providing a
simplification of music production and mini computers. Other examples
include Internet and mobile banking, the uptake of distance learning in
advanced education, and booking patient appointments through mobile
application. A well-known example of disruptive technology in healthcare is
cardiac angioplasty. Before the early 1980s, patients with coronary artery
disease were treated with by-pass surgery which was complex and expensive
and required highly skilled medical teams and longer stays in the hospital for
recovery. The disruptive innovation led to a simpler angioplasty enabling less
experienced practitioners to treat more patients in lower cost settings
(Christensen, Bohmer and Kenagy, 2000). Disruptive innovation not only has

great potential for the healthcare sector, but also poses a challenge. This is
because it may disrupt professional practices and processes (e.g., patient
referral system); upset the conventional way of thinking; and even undermine
professional status and power (Plsek, 2014b). He, however, suggests that the
leaders of healthcare organisations should seek to think strategically in
dealing with the challenge of disruptive innovations by allowing other
industries to pioneer the innovation and then to be responsive by adapting it
quickly. They should also adopt a first mover strategy of recognising, initiating,
and disseminating disruptive innovations as business opportunities.
All these innovation typologies are useful for understanding the various kinds
of innovations that can occur in the healthcare sector. This helps to broaden
the general conception of innovation in this sector beyond product and
process innovation.
2.4 The innovation theories
Innovation management scholars have proposed several theories to help
researchers understand human psychology and behaviours, interpersonal
relationships within organisations, and their associations with individual and
collective performance (Naqshbandi, Singh and Ma, 2016). In this thesis, two
of the most frequently mentioned theory in non-healthcare and healthcare
services research are discussed, namely, economic theory (Schumpeter,
1934), and Rogers’ diffusion theory of innovation (Rogers, 2003). The
intention of this section is not debate which theory is better than the other, but
rather, the goal is to describe the development of theories underlying the
process of innovation management.
2.4.1 Schumpeter’s Economic Theory
Joseph Schumpeter’s gave one of the most influential treatises of innovation
as a theory in his model of economic development (Schumpeter, 1934;
Schumpeter, 1942). There are two stages to Schumpeter’s model where the
first stage of the model is known as ‘circular flow.’ Schumpeter’s posits that
during the first stage, an economy is in a stationary equilibrium which is
characterised by no profits, no interest rates or savings, unemployment, and
the same products in circulation. This circular flow is broken by innovation.
The second phase follows through reactions to the original impact of
innovation. Schumpeter viewed innovation as the revolutionary change which
promotes economic development by moving the economy from a stationary
state to a dynamic one. This economic development consists of new
combinations of ideas and continual improvements in existing products which
results in innovation. Schumpeter explained that the business cycle of an
economy follows a cyclic process, with ups and downs in the level of activity,
a period during which trade expands then slows down and expands again. For
instance, the second stage of the model is divided into four phases: Prosperity
(expansion or boom or upswing of the economy due to the impact of
innovation); Recession (from prosperity to recession due to decline in demand
and investment which result to a rise in unemployment); Depression
(downswing of the economy due to deflation produces increase in investment,
gradual increase in employment and recovery in production); and Recovery
(from depression to prosperity) (see Figure 2.2).
Figure 2. 2: Schumpeterian four-phase cycle
Source: Simmie (2014) Own illustration, based on Schumpeter (1939)
Another common theme in Schumpeter’s work was the relationship between
innovation and entrepreneurship for economic growth. Schumpeter (1934)
explains that innovations are fundamental to economic growth and the central
innovator is the entrepreneur because he/she appropriates existing resources

for new uses and creates brand new opportunities for investment and
economic growth. New ideas are incapable of reaching execution without
being taken up by entrepreneurs and implemented through their influence
(Schumpeter, 1934). Schumpeter (1934) also considered creative destruction
as a characteristic of innovation as the latter revolutionises the economic
structure by terminating the old structure and creating a new one. In the
absence of this, continuous imitation would be the norm (Schumpeter, 1942).
Based on Schumpeter’s work, innovation is a primary generator of growth
which involves doing things in a new way. However, the disruption brought
about by innovation can lead to the growth, adaptation or liquidation of
industries. In summary, Schumpeter stresses that innovation is the creative
destruction that develops the economy with the entrepreneur having the
important role as the creator of change (Schumpeter, 1934; Schumpeter,
1939; Schumpeter, 1942).
2.4.2 Rogers’ diffusion theory of Innovation
The theory of diffusion is one of the oldest social science theories. Diffusion of
innovation seeks to explain how, why, and at what rate ideas and technology
perceived as new spread across a social system (Strang and Soule, 1998;
Rogers, 2003). Rogers (2003) developed one of the better-known theoretical
approaches to the diffusion of innovation. Rogers (2003) argues that diffusion
is the process through which information about an innovation is shared
through communication channels over time in a social system (Rogers, 2003).
In healthcare, this theory is useful for determining the adoption of a new
clinical behaviour by the clinical team or the healthcare system and in
deciding which component will require extra effort if diffusion is to occur
(Sanson-Fisher, 2004). According to Rogers (2003), there are five
characteristics of a new clinical innovation that will partly promote behavioural
change amongst health professionals and determine the rate of adoption and
diffusion. Greenhalgh et al. (2005) in a systematic review on the diffusion of
innovations in health service organisations also identified other characteristics
of innovations, but these are not as common as the ones Rogers listed.
Rogers (2003) explained that innovation characteristics explain the 48 to 87

per cent disagreement in the rate of adoptions. The five elements include:
relative advantage, compatibility, complexity, observability and trialability.
o Relative Advantage. Innovations that exhibit beneficial qualities that
are apparent to proposed adopters are adopted and implemented more
successfully. Relative advantage is a prerequisite for adoption because
individuals will not embrace an innovation they do not consider to be useful
(Dirksen, Ament and Go, 1996; Meyer, Johnson and Ethington, 1997;
Carlfjord et al., 2010). However, a relative advantage does not always
guarantee an increased rate of adoption (Denis et al., 2002; Grimshaw et al.,
2004), as some innovations undergo a lengthy period of contestation and
discussion amongst potential adopters, despite the evidence of their
effectiveness (Greenhalgh et al., 2004). The perceived degree to which an
innovation is useful raises debate as ‘individual behaviour’ plays a key role
(Rogers, 2003).
o Compatibility. Rogers (2003) argues that for diffusion to occur rapidly,
an innovation must be compatible with the values of members of the
organisation. When the targeted individuals find the innovation to be very
compatible with their important values, they are more likely to make a
consistent and committed use of the innovation. There will be few objections
because the employees perceive that the innovation bolsters their existing
values (Klein and Sorra, 1996). On the other hand, if it is perceived as not
being aligned with their values and beliefs, members of the organisation may
ignore it completely or it will diffuse very slowly (Meyer and Goes, 1988;
Rogers, 2003; Greenhalgh et al., 2004; Ferlie et al., 2005; Feldstein and
Glasgow, 2008; Fennell and Warnecke, 2013).
o Complexity. Complexity is referred to as the capability to perceive and
process different ideas, events and assess or analyse them correctly to draw
deductions and make decisions (Tabak and Barr, 1999). The more
complicated the proposed innovation, the slower the rate of diffusion because
simple innovations spread faster than complicated ones (Denis et al., 2002;
Rogers, 2003; Fleuren, Wiefferink and Paulussen, 2004). Individuals with high
cognitive complexity analyse situations better than others and are more

capable of reaching creative and novel solutions (Vance, Zell and Groves,
2008). Thus, they would support innovation adoption because they
understand aspects of the innovation that might seem very complex and
misleadingly disadvantageous to others.
o Observability. Observability is the degree to which the usage and
positive impact of an innovation are ‘visible’ to intended users (Meyer and
Goes, 1988; Denis et al., 2002; Rogers, 2003). Visibility reduces uncertainty
and encourages discussion amongst colleagues. In surgery, the visible
benefits of a technological innovation stimulates quicker uptake, as no one
wants to be left out (Denis et al., 2002; Sanson-Fisher, 2004).
o Trialability. This is described as the ability to pilot an innovation on a
limited basis without making a huge commitment (Ostlund, 1974; Rogers,
2003). Innovations that can be tested on a small scale tend to be adopted
more easily because experimentation reduces risk and makes the benefits
widely known (Rogers, 2003; Fleuren, Wiefferink and Paulussen, 2004).
However, a balance needs to exist between trials that show the positive
benefits of an innovation and the excessive repetition of these trials (Barlow
and Burn, 2008). The reasons for this are clear as too many trials can lead to
the misuse of organisational resources and can suppress the market for
innovation as manufacturers face demand for repeated trials from different
sources that wish to test to find out whether a product fits within their context.
Rogers (2003) further proposed a model of variation in adoption behaviours
by classifying the adopters into categories on a continuum of communication.
These categories are: innovators, early adopters, early majority, late majority
and laggards (see Figure 2.3). These adopters can be further classified into
two main groups: earlier adopters and later adopters. Earlier adopters are
innovators, early adopters, and early majority, while later adopters are late
majority and laggards. Berwick (2003) applied Rogers’ theory to a healthcare
context to understand how members of healthcare organisations contribute to
the diffusion of innovation through their organisation and across other
organisations in the healthcare sector. This application helps to define where

to focus efforts to enable faster diffusion of innovation in healthcare
organisations.
Figure 2. 3: Innovation adoption curve based on the diffusion of innovation theory
Source: Rogers (2003)
According to Rogers, every group plays a role in ensuring the spread of
innovations while the innovators refine interesting ideas into more tangible
products, services or processes. The early adopters discover innovators and
test their innovations while the early majority networks with the early adopters
to learn more details about the innovation and to determine underlying risks
and benefits. The late majority monitors the environment and the laggards
have custody of the past (Rogers, 2003). The early adopters are socially well-
connected, readily embrace opportunities for innovation, test several
innovations and give feedback. They are the most crucial to the spread of
innovation because of their risk appetite, propensity to experiment, leadership
roles and their well-connected social networks. In healthcare settings, these
early adopters are most likely to be selected as leaders of clinical associations
and will often be approached by pharmaceutical companies or medical
technology firms. The early majority learn about innovations from social
interactions with early adopters. Therefore, organisations that encourage
these kinds of social networking will experience faster diffusion rates

compared to organisations that have a culture of isolation and seclusion
(Berwick, 2003). This implies that successful diffusion depends more on how
an organisation handles and maximises the relationships between its
innovators and early adopters, and the collaboration between early adopters
and the early majority than with any other groups.
Criticism of Rogers’ diffusion model has to do with its implications of pro-
innovation bias and individual blame bias. Pro-innovation bias is the implicit
assumption that the adoption of an innovation is universally positive, meaning
that it is more cost-effective, constructive or able to solve problems (Van de
Ven, 1986). Rogers (2003) asserts that the outcomes of innovation
consequences are often over-hyped and that the effectiveness of an idea can
only be determined after implementation (cf. Van de Ven, 1986). For example,
a new clinical guideline classified as an innovation by some practitioners may
be perceived as a nuisance to nurses when introduced into patient wards
(Greenhalgh et al., 2005). The individual-blame bias is finding fault with
individuals for their non-adoption of an innovation. Rogers (2003) stresses the
importance of recognising these biases and to realise that all innovations are
not necessarily beneficial and that reasons for the non-adoption of innovations
must be viewed beyond individualistic reasons (Rogers, 2003).
2.5 Innovation Process Models
Many researchers, including Van de Ven (1986) and Schroeder et al. (1989),
have argued that the innovation process stage models are not entirely
representative of its intrinsic complexity. However, stage process models help
in understanding the structural and social conditions for innovation (Kanter,
1985). This thesis takes the stages of the innovation process to be invention,
development, adoption, implementation and diffusion (Utterback, 1971;
Varkey, Horne and Bennet, 2008; Department of Health, 2011a) (see Figure 2.4).
Figure 2. 4: The innovation process model

Source: Varkey, Horne and Bennet (2008) and Department of Health (2011a)
Invention is the use of available market and technical information to develop a
pioneer solution that solves problems (Schmookler, 1966; Fagerberg, 2004).
This phase is dominated by idea generation and opportunity recognition. The
former occurs through observation, studies, and research surveys which
result in the production of a proposal (Utterback, 1971; Varkey, Horne and
Bennet, 2008). Generated ideas are streamlined to produce the best ones
(O’Connor and Brown, 2003). Opportunity recognition determines the ideas
that have good business feasibility and best value by a thorough evaluation of
the strategic fit of the idea with the organisation's objectives and the
availability of resources to actualise, develop and market the proposed
innovation (Van de Ven, 1986; Kanter, 1988; Varkey, Horne and Bennet,
2008).
In the development stage of the innovation process, the best ideas from the
invention stage undergo design, prototyping and pilot testing (Kanter, 1998;
Varkey, Horne and Bennet, 2008; Department of Health, 2011a). After
designing, the first actualisation is achieved by prototyping. Prototypes are
mock representations of the functionality of an innovation that enable effective
realisation of the idea (Kanter, 1988). Pilot testing of the innovation
determines the utility of the innovation (Varkey, Horne and Bennet, 2008).
Adoption and implementation are overlapping stages in the process of
innovation management (Rogers, 2003). Innovation adoption refers to the
series of processes that an organisation undergoes before the decision to use
an innovation (Rogers, 2003; Barlow, 2011). Adoption has been developed
conceptually as a multi-stage event but, operationally, it occurs as a single

stage (Pierce and Delbecq, 1977; King, 1990). Adoption consists of the
initiation, decision and the confirmation stages (Zaltman, Duncan and Holbek,
1973; Rogers, 2003) which represent the pre-adoption, decision and the post-
adoption activities (Pierce and Delbecq, 1977; Rogers, 2003; Jasperson,
Carter and Zmud, 2005). The initiation stage involves becoming aware of
existing innovations, evaluating them for their suitability and proposing them
for adoption by persuasion and communication (Meyer and Goes, 1988;
Rogers, 2003). In the decision stage, innovation aspects are assessed by
decision-makers to determine if the innovation meets technical, financial and
strategic objectives. Ultimately, a decision to accept or reject the innovation is
made (Meyer and Goes, 1988). Lastly, confirmation involves the adaptation of
the innovation and trials and preparation for its proper use in the organisation,
(Duncan, 1976; Meyer and Goes, 1988; Rogers, 2003).
Innovation implementation occurs simultaneously as well as after the
innovation adoption. Therefore, phases of adoption and implementation can
be coincidental. Innovation implementation is the process of getting
organisational members to use an innovation committedly, consistently and
appropriately in a maximum capacity. It is the transitional phase between the
decision to adopt and the routine use of the innovation (Meyer and Goes,
1988; Klein and Sorra, 1996; Greenhalgh et al., 2005). Implementation is
important because organisations can adopt innovations and fail in
implementing them. Sometimes, when an innovation does not achieve the
intended benefits, it is not due to the ineffectiveness of the innovation, but
because of the failure of the implementation stage (Klein and Sorra, 1996;
Klein and Knight, 2005).
Diffusion is the last stage of the innovation process. It is the systematic uptake
of an innovation into widespread use across the whole service (Department of
Health, 2011a). It involves any activities carried out to accelerate the adoption
of the new practices across many organisations, and ultimately throughout an
entire healthcare organisation (Plsek, 2003). Greenhalgh at al. (2005) classify
diffusion into pure diffusion and active diffusion. Pure diffusion is the spread of
innovations in an informal, unintended and localised way that is mainly

propagated by peers. Active diffusion is dissemination which is more
intentional, formal, centralised and propagated through vertical hierarchies.
Although mass media and other communication channels create cognisance
of an innovation, social networks, which are the friendships and support
between members of a social system, are the main means of diffusion of
innovation (Greenhalgh et al., 2005).
2.5.1 Linear models of innovations
In the linear model, innovation begins with basic research, followed by applied
research and development and ends with production and diffusion (Godin,
2006, p. 33). This model assumes a simple sequential process as shown in
Figure 2.5.
Figure 2. 5: Basic linear model of innovation
Source: Godin (2006)
This model has been developed in three steps. The first step connects applied
research to basic research, the second adds experimental development, and
the third, production and diffusion (Godin, 2006). This model was developed
when pure science was the ideal and researchers began investigating a
causal link between basic and applied research. Rothwell (1994) expanded
upon the evolution of innovation models using the concept of five generations
of innovation processes. The first and second-generation models are linear
models, the third-generation model is a transitional one and the fourth and
fifth-generation models are non-linear models. The first-generation innovation
model was centered on ‘technology push’ as the main impetus for innovation.
Here, innovation was driven by research with minimal market influence. The
technology-push model as shown in (Figure 2.6)
Figure 2. 6: First generation ‘technology push’ model of innovation

Source: Godin (2006)
Here, there is a linear development from scientific research through
technological development to the marketplace. The second generation
‘market pull’ model of innovation was characterised by market demand being
a source of new ideas for research and development and influencing
innovation. The ‘market pull’ model is seen in Figure 2.7.
Figure 2. 7: Second-generation market pull model of innovation
Source: Godin (2006)
These linear models endured criticisms due to their simplicity and the
omission of feedback loops between the stages of the innovation process.
Mowery and Rosenberg (1979) argued that the interaction between science,
technology and marketplace demand was poorly represented in these
models. They did not consider other environmental inputs and had little
systematic evidence for verification (Forrest, 1991). Hobday (2005) also
warned that they ignored the effect of external factors and underplayed the
role of human decision-making and the complexity of processes within each
stage. Organisations frequently adopt simplistic models to improve innovation
processes. An example is the Cooper Stage-Gate innovation model where an
evaluation gate follows each stage of activity (Cooper, Edgett and
Kleinschmidt, 2002). In attaining successful innovation management, a linear
model provides an easy guide for each stage of action (Cooper, Edgett and
Kleinschmidt, 2002; Tidd and Bessant, 2013).

The traditional models of healthcare are almost entirely linear and
transactional in that they move from innovation supplier to buyer to patient
(Bierbaum, 2015). These prevailing linear approaches in healthcare give a
poor representation of the real situation because they ignore the effects of
certain policies, the network of relationships, feedback mechanisms and other
non-linearities present in the system (Sengupta and Abdel-Hamid, 1993). This
approach is considered as being too simplistic for complex systems like
healthcare and often leads to unanticipated consequences and policy
resistance (Sterman 2000; Plsek, 2003). However, some researchers have
contended that despite unfavourable criticisms, the inherent simplicity of the
linear model is the reason for its longevity because of its usefulness in the
analysis of innovation decisions, providing an easy guide for each stage of
action (Hobday, 2005; Godin, 2006; Kotsemir, Abroskin and Meissner, 2013;
Tidd and Bessant, 2013).
2.5.2 Non-linear models of innovations
Rothwell’s generation ‘coupling model of innovation’ combines the
technological push and the focus on market demand approaches. This model,
although largely sequential, has feedback loops that promote integration at
the R&D and market interphase (Rothwell, 1994; Corre and Mischke, 2005;
Hobday, 2005). This third-generational model was a transition towards
integrative non-linear models. Criticisms of this model are that it is very
simplistic and does not consider the influence of environmental factors.
However, it is a more representative model of the innovation process than the
preceding ones (Rothwell and Dodgson, 1991; Rothwell, 1994).
The fourth-generation and fifth-generation models are non-linear innovation
models. These were formed due to innovation models shifting from sequential
to more integrated processes (Hobday, 2005; Galanakis, 2006). Recent
thinking explains that innovation management follows a dynamic approach
which consists of a cycle of divergent and convergent repeatable activities
and interactions which occur within different organisational levels and
externally (Van de Ven et al., 2008). The continuous feedback loops present
in these models represent an integration of internal and external resources

and reciprocal relationships between stakeholders in the innovation process
(Rothwell, 1994; Galanakis, 2006). These models capture the high level of
cross-functional integration within departments in organisations such as R&D
and manufacturing, and the external collaborations such as strategic
partnerships with external stakeholders (Rothwell and Dodgson, 1991;
Hobday, 2005).
Some of these non-linear innovation models are the cyclic model of Gomory
(1989), the neural network model of Ziman (1991), the Funnel model of
Wheelwright and Clark (1992), the innovation journey by Van De Ven et al.
(2008) among many others. Another non-linear model is the Chain-Linked
model (Kline-Rosenberg model) which proposes that innovation occurs due to
the interplay of technological knowledge and market opportunities. Several
innovation pathways and feedback mechanisms give this model its non-
linearity (Kline, 1985; Kline and Rosenberg, 1986; Kline, 1991). Kline's model
incorporates two kinds of intercommunications in the innovation process. The
first interplay highlights the processes within a given organisation. The
awareness of a new market opportunity is followed by analytic design,
development, production, distribution and marketing. The second
intercommunication denotes the relationships between the organisation and
its wider science and the technology network with a focus on a stored
scientific and technical knowledge base.
This non-linear model differs from linear models as it stresses the importance
of knowledge, process research and invention in the innovation process. Kline
(1985) attributes the primary source of innovation to cumulated human
knowledge and argues that harnessing available knowledge and improving
existing knowledge are the two important parts in achieving innovation. This
model argues that invention or analytic design is the first step in the
innovation process, not research (Kline, 1985; Kline and Rosenberg, 1986) in
contrast with other linear models that underplay the role of the invention stage
by omitting it or proffering research as the starting point of innovation. Kline
(1985) argues that when a problem is encountered, available knowledge is
first recalled and research only occurs when available knowledge is

inadequate. The model also focuses on systems and process research which
the linear model neglected. Kline (1985) asserts that systems and process
research is important for the reliable performance of products.
Lastly, this model shows the variety of sources of innovation which include
existing or new knowledge, scientific and technical discoveries, market needs
and information from the consumer. This nullifies the argument of the relative
importance of technology versus the importance of market needs purported
by second-generation innovation models (Push vs. Pull). Also, the presence
of feedback loops in this model negates the question of cause and effect. This
is because in circular processes, causes become effects after some time and
every effect becomes a cause in due time as well.
2.6 Innovation Needs in the NHS
The NHS is the major provider of healthcare services in England. It
administers free healthcare to everyone in need of it at the point of delivery
and is the world’s largest integrated national health system and largest public-
sector provider of healthcare (Williams et al., 2008; Barlow, 2011; Department
of Health, 2011a). Innovation in the NHS is important in the transformation of
patient outcomes because of the effect of new medicines, technologies and
processes. Since its establishment in 1948, the NHS has a track record of
cutting-edge innovations. The development of MRI and CT scan technologies,
in-vitro fertilisation, genetic fingerprinting, the portable defibrillator, the
disposable syringe and the contraceptive pill were all pioneered in the UK
(Department of Health, 2011a).
Although innovation is a solution to many problems in healthcare, it is very
costly because, unlike other sectors where innovation reduces costs, in
healthcare, it increases costs as it leads to an increase in demand for better
treatment and more people being treated (Cutler, 1995; Cutler and McClellan
2001). Cutler and McClellan (2001) term this phenomenon as the ‘treatment
expanse effect’. Increased costs and spending is driven by changes in
demography, a growing number of people with long-term conditions and the
changing patterns of public demands fuelled by advances in knowledge,

science and technology (Department of Health, 2011a; Department of Health,
2011b). A significant portion of the public spending budget is spent on health.
In 2016, £140bn was spent on health which was almost 30 per cent of the
entire public spending budget. At this rate of spending, with increasing
demands and costs, NHS England, Monitor and independent analysts have
calculated a funding gap of £30 billion by the year 2020 due to disparity
between available resources and growing healthcare demands (Roberts,
Marshall and Charlesworth, 2012; NHS England, 2014). The increase in
demand for quality healthcare and the funding pressures in the NHS require
drastic changes to achieve effective and sustainable solutions.
However, systematic adoption and diffusion of innovations in the form of
drugs, diagnostic methods, medical interventions and managerial practices
have been quite slow. Several challenges in the care delivery pathways make
it imperative for the spread and uptake of innovation to be quicker. The
number of elderly people is projected to rise with about 2.8 million people over
65 years old representing a 25 per cent increase needing nursing and social
care between 2015 and 2025. Elderly care is more expensive than care for
other age-groups. This increase will escalate the cost of the resources
required to pay for their treatment (Caley and Sidhu, 2010; Guzman-Castillo
et al., 2017). Since 2004, the number of visits to the Accidents and
Emergency (A&E) units have substantially increased, rising from 16.5 million
in 2003/04 to 22.9 million in 2015/16 - a surge of more than 39 per cent (The
King’s Fund, 2017a). This rise has led to longer waiting times. Baker (2017)
reports that emergency admissions have risen faster than population
increase. There were 69.0 emergency admissions per 1,000 population in
2011/12 compared to 77.1 per 1, 000 people in 2016/17 which signifies a 12
per cent faster admission rate than the population. There was a 3 per cent
increase in emergency admissions in 2017/18, compared to 2016/17 (The
King’s Fund, 2017a). These rising admission rates have increased bed-
occupancy rates up to 87.1 per cent as of September 2017 leading to chronic
bed shortages across the country (NHS England, 2017a).

Apart from this, waiting times and lists for treatments by consultants (referred
by GPs) are growing rapidly. The amount of people waiting for elective
treatment has increased by 25 per cent in the last three years with the number
at 4.1 million at the end of August 2017 (Baker, 2017; The King’s Fund,
2017b). All these challenges are aggravated during winter due to pressures
such as A&E closures and diverts which cause an increase in the amount of
older people and those who need hospital beds (NHS England, 2017a; The
King’s Fund, 2017b). Combined with these challenges, there is a change in
the population’s expectation of the NHS to include vaccination, mental health
and social care, antenatal and maternity services and the provision of
medicines in addition to treating diseases (NHS Office of London Clinical
Commissioning Groups, 2017).
Innovation in the NHS could help to combat these challenges and increase
productivity, efficiency and the effectiveness of the NHS to considerably
improve patient safety and care quality outcomes in the tough financial
climate (Marjanovic et al., 2017). It will also foster economic growth in the
science, technology and engineering industries that develop products and
technology for the NHS which is a major investor and wealth creator in the UK
(Department of Health, 2011a). Thus, healthcare delivery systems need to
continuously innovate to provide cost-effective ways of healthcare delivery
that will revamp the care system, sustain a pioneering health service and
meet the challenges of an ageing population by using new combinations of
technology, infrastructure, services and organisations (Darzi, 2008; Barlow,
2011).
However, the process of successful innovation management is notoriously
difficult in large disaggregated organisations such as the NHS (Department of
Health, 2011a; Deparment of Health, 2011b). The unpredictability of
constituent parts of the system and the many interdependencies between
them (Dattee and Barlow, 2010) exacerbated by chaotic communication lines
and ambiguous responsibility circles foster power tussles and cultural silos
that make innovation difficult to adopt, implement and diffuse (Barlow and
Burn, 2008; Barlow, 2011) (see Figure 2.8).

Figure 2. 8: The innovation pathway
Source: Barlow and Burn (2008)
The dissemination of innovation across a social complex system like the NHS
follows a slow initial phase where innovators and early adopters embrace an
innovation, followed by a surge in uptake by the early majority and late
majority groups when the innovation benefits are obvious (Rogers, 2003;
Barlow and Burn, 2008). Williams et al. (2008, p. 25) labelled the gap in
uptake between the ‘early adopter and the early majority as the ‘valley of
death chasm’ (as seen in Figure 2.3). This chasm refers to the profound
differences in attitude towards the adoption of innovation between these two
groups. The implication of this chasm is a variable time lag between when

early adopters and the early majority adopt an innovation as the time it takes
the chasm to be bridged which corresponds positively to the speed of the
innovation uptake. The conservative views of most clinicians and healthcare
delivery providers in the early and late majority groups may arise from the
highly segmented structure of the health industry, the role of small and
medium enterprises as technology sources for innovation, and the cultural
gap between the NHS and industry (Williams et al., 2008).
2.7 Factors that limit successful innovation management in the public healthcare sector UK
In addition to the chasm, the literature has identified several other factors that
limit successful innovation adoption across the NHS. These include the
following:
o Complexity of the healthcare system. Healthcare organisations are
often described as complex systems (Plsek, 2003; Rowlands, Sims and Kerry,
2005; Dattee and Barlow, 2010) and successful innovation management is
especially difficult in large disaggregated organisations like the NHS
(Department of Health, 2011a, Department of Health, 2011b). Compared to
public health organisations like the NHS where innovations are planned within
an enormous and highly complex structure, the organisational structure in
private industry is less fragmented and so allows flexibility for innovation.
Decision-making in private industries is much faster due to the lack of multiple
structural layers, shorter chains of commands and less complex structures. It
is not uncommon to see private organisations with budgets for innovation and
the freedom to experiment with innovations of various kinds (Miles, 2004; Tan,
2004; Cankar and Petkovsek, 2013).
o Prevalence of linear models in healthcare. The traditional business
models of healthcare have been almost entirely linear and transactional with
a top-down approach to innovation that is motivated by supply (Castle-
Clarke, Edwards and Buckingham, 2017). NHS organisations attempt to
handle obstacles in isolated ways instead of dealing with them systemically.
To innovate consistently, especially in a complex organisation, a systemic

approach is needed to tackle all barriers that limit innovation uptake (Loewe
and Dominiquini, 2006; Bierbaum, 2015). In the NHS, different performance
targets and budgets for various services encourage emphasis on the
functioning of individual parts instead of a focus on the entire operation.
Consequently, patients and clinicians as well as equipment and services
move through the system in isolated segments with separate targets. Delays
in a segment may not affect the targets of individual segments but will have
an adverse effect on the entire system and lead to the patient not receiving
the entire benefit of care that was intended (Plsek and Wilson, 2001).
Most organisations in the private industry use open innovation models which
allow them to assimilate external expertise into innovative processes to
effectively reduce costs, manage risk and offer better products and services
(Granstrand, 2011). The influx and efflux of knowledge helps increase
innovation and expands the markets for external innovation use (Chesbrough
2006). This is done through strategic bartering of information with suppliers,
clients, research centers, universities and other relevant bodies outside the
organisation in order to combine valued resources that can benefit the
organisation's innovative process (Brant and Lohse, 2014). This model of
innovation is more systemic and integrative because it forces all parts of a
system to collaborate and ensures more connectivity between isolated parts.
Some companies adopt a controlled approach to open innovation by being
strategic about utilising open innovation by adopting closed and open
innovation methods to protect proprietary information and maintain
competitive advantage. Apple uses a linear and closed innovation model for
its core hardware, but leverages this out by incorporating open models in the
development of some software elements (Linden, Kraemer and Dedrick,
2009; Lippoldt and Stryszowski 2009; Williamson and De Meyer, 2012). New
Zealand uses a framework called Integrated Performance and Incentive
Framework (IPIF) to measure performance of the entire system holistically,
rather than measuring separate elements to foster integration and ensure the
needs of local communities are met (Ashton, 2015).
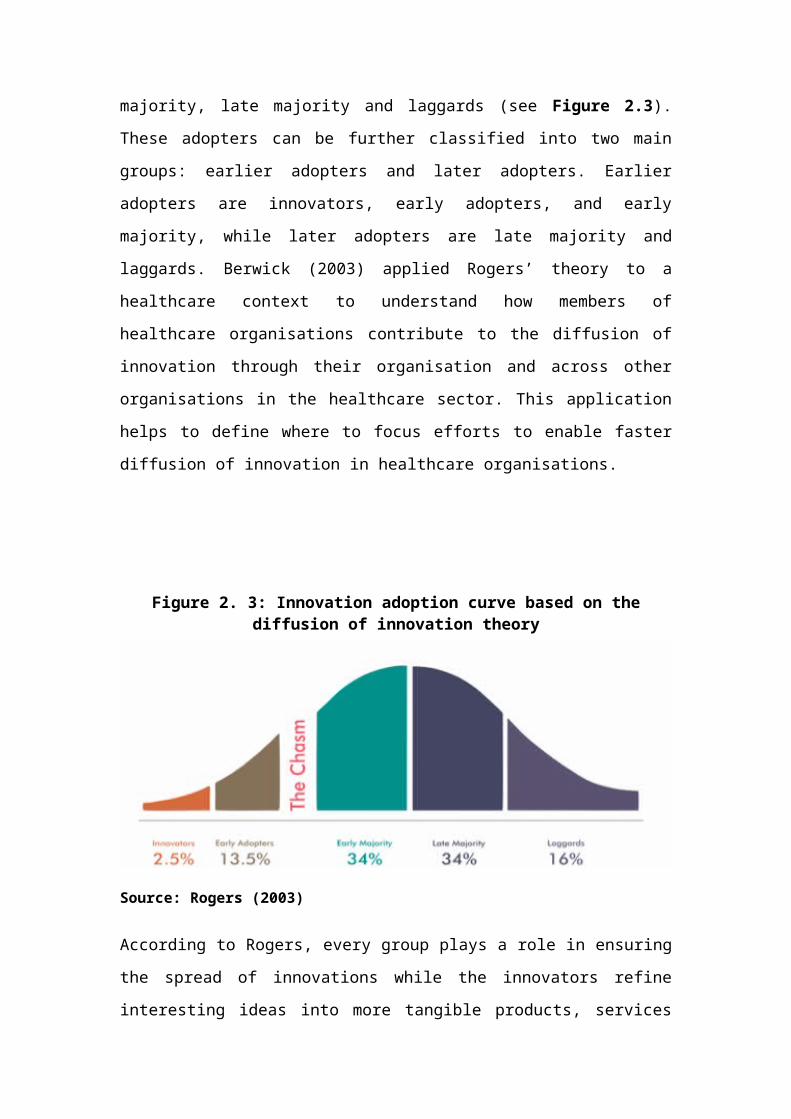
o Organisational culture and values. The right culture fostering
innovation and innovative behaviours within the NHS is lacking. Take for
instance, the fact that identifying problems and finding solutions are rarely
built into staff day-to-day job descriptions in the NHS, including those of the
hospital clinicians. This is further aggravated by a lack of clarity about the
extent to which chief executives are involved in the innovation process
(Castle-Clarke, Edwards and Buckingham, 2017). If, chief executives are
excluded from the innovation process, innovation is unlikely to occur. This
lack of an innovation culture in day-to-day processes may be due to risk
aversion and conservatism prevalent in an industry that comes with many
weighty consequences for missteps by unsuccessful innovators. (Loewe and
Dominiquini, 2006). The constant change and re-organisation in the NHS also
exacerbate this by causing ‘innovation fatigue’ (Barlow and Burn, 2008;
Barlow, 2011). All these barriers make the creation of a culture that supports
innovation very challenging.
o Communications and social networks. In the NHS, social networks
often have isolated communities of interest that comply with unwritten rules.
This networking structure has the tendency to make effective collaboration
and knowledge transfer across established organisational groups difficult
(Barlow and Burn, 2008). For example, doctors have informal, egalitarian and
horizontal networks that are effective at spreading peer influence. In contrast,
nurses have formal, hierarchical and vertical networks that are effective at
sending, receiving and diffusing systematic information between diverse
groups and passing on decisions from a higher authority (West et al., 1999;
Barlow and Burn, 2008; Ferlie et al., 2010). These differences in
communication methods can make collaborative efforts from functioning
multidisciplinary communities of practice difficult to coordinate (Ferlie et al.,
2005; Barlow and Burn, 2008; Barlow, 2011).
While the NHS has been strongly advocating for evidence-based medicine
and explicit, expert knowledge in clinical practice, the private sector is more
focused on the need for tacit knowledge to achieve desired outcomes (Bate
and Robert, 2002, p. 22). Horizontal networks that cut across hierarchies in

the NHS need to be created to foster a community of diverse professionals
that come together to learn best practice and share ideas. Knowledge transfer
is a concept that underlies this approach (Bate and Robert, 2002) because
individual knowledge if unshared, is unknown and should be shared so other
people can gain from it (Quintas, 2002). More focus needs to be put on the
building of an integrated social and community process in the public sector
(Bate and Robert, 2002).
Private sector companies have understood the value of tacit knowledge
transfer (Grant, 2001; Hauschild, Licht and Sterin, 2001) and there is a huge
emphasis on knowledge in the private sector with firms prioritising the
procurement and exploitation of their employees' knowledge (Bate and
Robert, 2002). Tacit knowledge is the conceptual understandings of
individuals combined with practical expertise (Kogut and Zander, 1992;
Nonaka, 1994). A survey reported that 89 per cent of 100 European business
leaders considered knowledge to be the key to business power (Murray and
Myers, 1997). Organisations in the private sector have knowledge transfer
initiatives such as Ernst and Young's sharing knowledge and best practice
program and Dow Chemical's project to leverage on intellectual capital.
o Leadership. Due to the strict national guidelines and targets that guide
Trusts managers’ decision-making and action in the NHS, enabling
environments that encourage innovation from staff at all levels are
uncommon. This is because managers in the NHS are appraised by how well
they deliver on defined projects and adhere to existing budgets, and not by
how innovative they are (LIF and Vasco Advisers, 2013). Effective leadership
to promote innovation entails recognising the benefits and challenges
associated with innovation, providing support for clinical and non-clinical staff,
and promoting learning through trial and error without the fear of penal
measures for failure, all of which is difficult in the NHS because of the
erroneous belief that innovation is a luxury and this results in staff being
completely focus on the day to day tasks (Barlow, 2011; The King’s Fund,
2018). Leaders in the NHS may need to be incentivised like their peers in the
private sector so that they are motivated to innovate and apply strategic

planning in the management of the many professionals performing highly
specialised roles. Most of the times, leaders in the public sector are driven by
the moral and ethical responsibility to provide public service and they are
usually in a highly pressured environment with the expectation of delivering
outcomes within strict budgetary guidelines, all for which they receive
inadequate rewards for good performances (Fiddis, 2016).
o Financial rewards and incentives. Creating a culture of rewards and
balancing incentives to accelerate the adoption and diffusion of innovation in
the NHS has proved to be challenging (Department of Health, 2011a). A
performance-based reward system is needed to create an organisational
culture that supports continuous innovations (Lau and Ngo, 2004; Camelo-
Ordaz, Fernández-Alles and Valle-Cabrera, 2008; Tidd and Bessant, 2013).
Staff are appraised by how well they adhere to the budget, follow guidelines
or perform tasks outlined by NICE directives and government targets and so
this leaves little motivation to do things differently (Barlow and Burn, 2008;
Barlow, 2011).
The NHS uses the tariff system which has set prices and rules for NHS
providers as a method of reimbursement for innovative solutions. Here, NHS
providers are paid yearly based on the median cost of about fifty procedures
called health resource groups which are based on national benchmarks and
may not necessarily be reflective of the population. This method of payment
may not be beneficial to some trusts that produce high efficiency innovations,
as they may receive less because the system does not subsidise the cost of
expensive innovation (Barlow and Burn, 2008; NHS Improvement, 2016).
Countries like Germany promote innovation using structured financial
incentives and reimbursements and this has proved to be successful in
achieving desired healthcare outcomes (LIF and Vasco Advisers, 2013).
Although the NHS has tried to incentivise innovation with the inauguration of
several Innovation Challenge Prizes with lucrative cash payments (NHS
Improvement, 2016) and the Pay for Performance (P4P) System (Abduljawad
and Al-Assaf, 2011) to motivate staff, innovation initiation and uptake remain
slow (Barlow and Burn, 2008; Barlow, 2011). Rewards or incentives can be
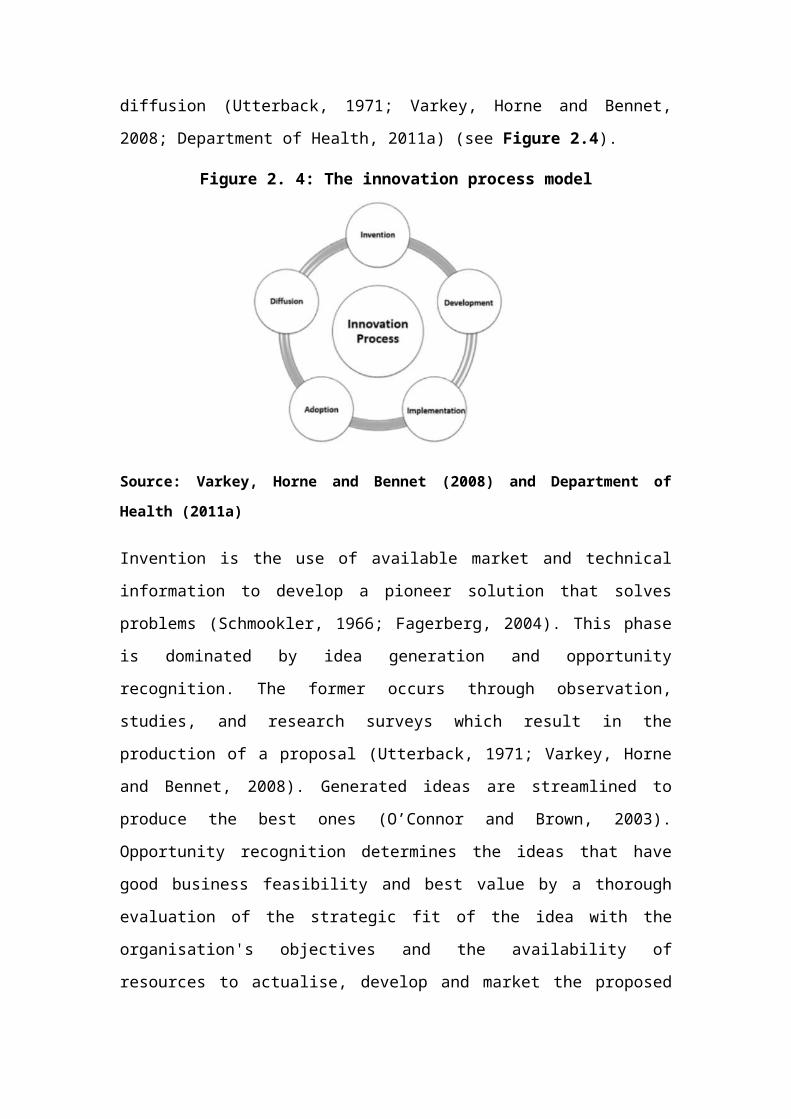
extrinsic or intrinsic where the former refers to all monetary incentives and the
latter to the employees’ need to feel capable and relevant and have some
autonomy in the workplace (Frey and Osterloh, 2001; Claire, 2013). Both can
be deployed as ways to effectively motivate staff to make innovation a part of
their daily activities.
In the private sector, organisations reward employees with monetary and non-
monetary incentives which include: P4P, money, gift cards, experience
rewards, training, plaques, thank you letters and certificates of recognition.
Air Liquide has an annual ceremony where it honours its best inventors in
addition to giving them monetary rewards. ConocoPhilips also has a Viable
Cash Incentives Program (VCIP) where employees receive cash payments
based on the performance of individual business units and the entire company
(Abduljawad and Al-Assaf, 2011; Claire, 2013).
Fottler (1981) highlighted that the rigid hierarchy of decision-making in public
health sector organisations heightens this lack of an effective reward system.
For example, if an innovation initiative is not introduced by top management in
the NHS, its financial and management burden is less likely to be rewarded
for success (Barlow and Burn, 2008).
o Political influences. There tends to be an irresistible tendency for
politicians to be leading the NHS, despite their apparent commitment to
devolution (Ham, 2014). This political influence results in frequent changes in
policy and places constant pressure on managers to achieve quick results in
short time frames (Bozeman, 1987; Boyne, 2002). This makes NHS Trusts
leaders focus on short-term views that limits the adoption of innovation. It also
poses difficulty and fear for leaders to plan, partly due to radical policy shifts
and uncertainties about the future (Barlow and Burn, 2008). Innovations that
cause drastic changes in service delivery also may create public concern
which could make politicians anxious owing to the political nature of
healthcare (Barlow and Burn, 2008). Ham (2014) urges the government to
clearly define the politicians’ roles by developing an accountability map where
the implications for parliamentary supervision are set out. In comparison to
the UK where much accountability rests with NHS England, Sweden has a
very decentralised healthcare system, where county councils are accountable
for the provision of healthcare and have sovereignty as to how their
operations are run. This method reduces interference from the national level,
and so individual councils can make informed decisions based on the
healthcare needs of their respective localities (Triggle, 2005).
o Poor collaboration with private sector. Rising healthcare demands
and limited resources are putting the NHS under pressure with some of these
demands becoming more difficult to meet (Doyle and Bull, 2000). The private
sector should be encouraged to support the NHS to reduce some of the load it
carries. This can be accomplished by the existing public and private health
systems cooperating to serve the public better. Cooperative approaches can
help to achieve better healthcare outcomes, reduce costs and, thereby,
ensure a healthier population. A good example of a thriving public and private
sector partnerships is the Manises partnership in Valencia, Spain, where
innovative integrated care delivery has resulted in a surpassing of set targets,
increased interventions in prevention and diagnosis and per capita funding
being 25 per cent lower than that of the public health systems (Madan and
Sanches, 2013).
o Disproportionate focus on innovation research and development.
The NHS puts more effort and investment in research and development
instead of adoption and implementation which makes investments more
biased towards research and development. NHS England (2017a) reports that
the NHS spent about £1.2 billion on research and development in 2014-2015.
However, spending to facilitate adoption and diffusion of developed
innovations in the NHS through the AHSNs was £50 million from 2013 to 2018
which is less than 0.1 per cent of available resources. Innovative companies
in the private sector like Apple, GE Healthcare, and Johnson & Johnson
spend up to 25 per cent of available resources on promoting and spreading
innovation rather than on its development stage (Castle-Clarke, Edwards and
Buckingham, 2017; The King’s Fund, 2018).

2.8 Organisational readiness – a precedent for successful innovation adoption
Organisational members can resist innovation and even if this occurs, it can
be difficult to make it last. Therefore, it is important to understand the
innovation management process in order to manage it effectively and gain
support from organisational members at each stage. Management
researchers have conducted extensive work on how to influence successful
organisational change and what strategies organisational leaders may adopt
in the course of innovation management. A useful way to gain a better
understanding of this process is to adopt Kotter’s (1996) eight-step change
model. Kotter (1996) believes that organisational change can be managed
using an eight-stage approach and identified important factors such as: 1)
creating a sense of urgency, 2) establishing and empowering strong teams, 3)
creating, 4) communicating the vision, 5) taking actions to minimise any
obstacles, 6) creating and rewarding of short-term goals to increase
commitment, 7) highlighting change benefits in order to maintain the
momentum, and 8) anchoring the changes. However, it has been contended
that the difficulty and increasing failure to successfully implement change
programmes within an organisation results from change leadership oversight
in providing effective ‘readiness’ process before attempting to initiate change
(Armenakis and Harris, 2002; Williams, 2011; Rees, 2014). In another attempt
to offer advice for effectively implementing organisational change, Armenakis
and Harris (2009) describe the process of inaugurating organisational change
unfolds as a three stage-model, which is seen in Figure 2.9 below.
Figure 2. 9: Stages of organisational change
Source: Armenakis and Harris (2009)
In the typical sequence of traffic light colour phases, a flashing red light
represents readiness (as seen in Figure 2.9) and creates a warning/alert, for
individuals to stop, identify and anticipate what is ahead. This is a potential
hazardous event or indicates a lane to switch onto before the amber light
comes on to aid cautious driving. Lewin’s (1951) explains that successful
organisational change goes through a series of changes, namely, readiness,
adoption and institutionalisation to help organisational members’ job
performance. During readiness, which is the first stage, the message of why
change is needed should be communicated to the organisational members,
with individual apprehensions and uncertainties identified and managed.
Organisational readiness has been regarded as the enabling factors that
influence innovation processes and determine implementation success
(Lehman, Greener and Simpson, 2002; Holt et al., 2010; Gifford, 2012; Rees,
2014). An empirical study which assessed the impact of lean thinking across
three emergency departments in New Zealand revealed hospitals that
integrated and considered readiness factors (i.e., team involvement and
infrastructure, leadership involvement and support, and shared strategy) into
its planning and operational processes experienced effective implementation
for quality improvement scheme (Rees, 2014). Another empirical study
corroborated that developing a measure of organisational readiness is critical
to change success, because it help promotes engagement between clinicians

and patients, which is critical to the quality used to manage and facilitate a
healthcare organisation and its clinical team’s willingness and ability to
effectively interact and involve its patients in its organisational design and
governance. This is critical to the quality and efficiency of healthcare delivery
(Oostendorp et al., 2015). A number of studies have identified the importance
of measuring factors related to organisational readiness for the planning and
implementation of eHealth in healthcare institutions, in order to reduce the risk
of failure (Jennett, Gagnon and Brandstadt, 2005; Touré, Poissant and
Swaine, 2012; Saleh et al., 2016).
The context facing the healthcare services delivery sector within NHS
England is very obvious and challenging. Politicians communicate their
frustration by commissioning a new report every other couple of years,
decrying about the slow pace of change, and emphasising the potential
benefits of innovation (Collins, 2018). With healthcare delivery targets missed
and increasingly demand on NHS England, different actions and measure
have been developed to achieve changes, yet failure rates are still reported
(Castle-Clarke, Edwards and Buckingham, 2017). According to Todnem
(2005, p. 6) to “implement and manage innovation without being ready is
debatably like a baby trying to walk before being able to crawl: possible for
some, impossible for most.” The latter part indicates that failure is the ultimate
outcome of organisations that fail to prepare, prior to the fulfilment of a critical
task. NHS organisations require an understanding of what the conditions are
to readiness, and how to enact and sustain it.
2.9 Chapter summary
The purpose of this chapter was to explore how the concept of innovation
management has been developed and has evolved. The chapter introduces
the reader to the distinction between innovation and organisational change
and explained that innovation is characterised by a number of unique features
that make it distinct from organisational change – namely novelty, productivity,
intentionality, and complexity. Then, the various types of innovation were
discussed and the various theories and models of innovation examined. The
chapter showed that the uniqueness of innovation, alongside the context in

which the public healthcare sector exists – specifically the NHS imposes a
number of challenges on endeavours which makes it more difficult to adopt
and spread. The chapter discussed that the concept of organisational
readiness is a central component for successful innovation management in
the public healthcare sector. Therefore, in the next chapter, the concept of
readiness for innovation is explored. The aim is to increase understanding in
this area, by exploring the meanings and the conditions for enabling an
organisation’s readiness to innovate.

Chapter 3
A systematic review on the associated meanings and factors influencing organisational readiness for
innovation
3.1 Introduction
Readiness is pertinent to the study of organisational innovation because it has
important implications for increasing the delivery of quality service
improvements to healthcare on an increased scale. As it has been highlighted
in Chapter 2, organisational readiness is a socially constructed phenomenon
(Armenakis, Harris and Mossholder, 1993; Bouckenooghe, Devos and van
den Broeck, 2009; Rafferty, Jimmieson and Armenakis, 2012) while it’s
meaning has been conceptualised differently by management researchers.
Therefore, this chapter synopsises an extensive literature review addressing
the research question - how is organisational readiness for innovation
conceptualised? The chapter considers both content (definition and
operationalisation of organisational readiness) and process (reviewing the
literature in a systematic and reproducible way). The chapter discusses (1)
the meanings of organisational readiness for innovation and explores the
similarities and differences between the various meanings stated in the
literature, and (2) the factors enabling readiness for successful innovation
management. The chapter discusses a clear knowledge gap where further
research should be directed, and presents a transferable and vigorous
methodology that was undertaken and ultimately led to the identification of the
research questions that this study seeks to answer.
Organisational readiness for innovation is a behavioural, and systems
manifestation of the connection to, identification with, and involvement in
innovation management process. Several theories have provided insight into
readiness for change and the dynamics involved in readiness interpolations

(i.e., Armenakis et al. change message theory, Rogers theory of diffusion, and
organisational fit theory). In an attempt to extend our theoretical
understanding and move research forward, it was decided to take a
completely different approach to further explore the model that defines
innovation as a continuous evolution. To this end, complex adaptive systems
thinking provided a theoretical framework for this study. Systems thinking “is a
conceptual framework, a body of knowledge and tools that has been
developed over the past fifty years, to make full patterns clearer, and to help
us see how to change effectively” (Senge, 2006, p. 7). The fundamental
rationale for choosing this approach is that it best helps us in understanding
how the difficult and intransigent problem within the public healthcare system
arises, and to provide some leverage and insight into what is done wrongly,
and what can be done better to enhance readiness for innovation (Senge,
2006). The conceptual framework builds on five propositions which affects
adoption, and diffusion of innovations within health systems – i.e. the
characteristics of the problem, the nature of the perceived attributes of the
innovation, the perceptions and positions of multiple actors within and external
to the system, the health system characteristics (organisations’ financial state,
regulatory changes, relational changes), and the broad context (Atun, 2012)
(see Figure 3.1).
Figure 3. 1: Systems thinking framework for analysing adoption and diffusion of innovation in healthcare system

Source: Atun (2012)
Building on these considerations, this study examines what factors might
shape public healthcare organisations’ readiness for innovation. There is also
a question of how the interactions and interdependencies across the varying
elements may shape the creation and sustainability of organisational
readiness for innovation.
This chapter will first explain the systematic review method describing how the
literature search was conducted, the basis of the search strings used, the
search strategy, the inclusion and exclusion criteria and the definitions that
guided the review. Then, it discusses the findings and their implications,
thereby, highlighting a number of issues central to organisational readiness in
the literature on innovation. This ultimately led to the identification of the
research questions that this thesis seeks to answer.
3.2 The systematic literature review method
Greenhalgh et al. (2005, p. 1) defined a systematic literature review as one
“undertaken according to an explicit, rigorous and reproducible methodology.”
Systematic reviews differ from traditional narrative reviews by embracing a
scientific, replicable and transparent approach (Cook, Mulrow and Haynes,
1997). It minimises researcher bias and error through using rigorous search
methods for published and unpublished sources while allowing the application
of strict inclusion criteria to address a specific research question (Cook,
Mulrow and Haynes, 1997; Tranfield, Denyer and Smart 2003; Aveyard, 2010;
Mallett et al., 2012). Though the search process of a systematic review is
tedious and time-consuming, the results can strengthen the link between
research evidence and optimal healthcare (Cook, Mulrow and Haynes, 1997;
Aveyard, 2010).
Given the breadth of the research question, the review was conducted over
three months. The next few sections describe the review process.

3.2.1 Planning phase
To ensure precision and the alignment of the search terms with the topic, the
following relevant terms are defined. Innovation in service delivery and
organisations mean “a novel set of behaviours, routines, and ways of working
that are directed at improving health outcomes, administrative efficiency, cost
effectiveness, or users’ experience, and that are implemented by planned and
coordinated actions” (Greenhalgh et al., 2004, p. 582). Readiness refers to
the organisational members and the organisation’s ability to successfully
implement an innovation initiative (Holt et al., 2010). Health services delivery
organisations deal with the “diagnosis and treatment of diseases or the
promotion, maintenance and restoration of health” (World Health
Organisation, 2014).
During the planning phase, the primary researcher worked alongside a review
specialist in order to improve and ratify the review design. Four database trials
were conducted with the literature review specialist present. The purposes of
the sessions were to:
(1) Identify the gaps on innovation readiness.
(2) Identify the existing literature on innovation readiness.
(3) Ascertain the appropriate key words and search terms.
(4) Formulate, fine-tune and proof-check that the search terms and key
words were appropriate for the database.
(5) Review the questions and identify appropriate articles.
The steps were iteratively developed to ensure that the systematic review
search was rigorous, replicable and reliable.
3.2.2 Search phase
On completion of the planning phase, the primary researcher embarked on
the search phase. An initial broad search was conducted which covered
business, management, nursing and allied fields, biomedicine and
behavioural sciences. The Cochrane Library was considered in the initial

stage of the review; however, during the planning phase it became apparent
that the Cochrane database library did not match the needs of this review.
This was because the research question was management-based while the
Cochrane Library only provided information on clinically-based interventions.
The search included the use of four electronic bibliographic databases,
namely:
Medline (EBSCO), which was chosen because it is a key database for
health issues. In addition, the search words developed in the Medline
database were transferable across other EBSCO databases. This
facilitated the fine-tuning of the search string list (see Appendix A) and
highlighted the irrelevant search strings which simplified the search
when using the other databases.
CINAHL was chosen to provide access to relevant information on
readiness for innovation in the nursing sector.
Business Source Complete was selected to attain a broad scope of
search results that consisted of business, finance, and management
journals.
PsychInfo was chosen to provide information on organisational
readiness amongst individuals as the psychological aspect of
readiness was dominant within its literature.
These four bibliographic databases were chosen as being sufficient to provide
the required breadth of relevant information without excessive duplication.
With the assistance of a literature review specialist, a list of search strings
was formulated and modified to suit the index terms of the chosen databases.
The search strings were not limited to the abstracts and titles only as this
excluded an enormous number of articles. Instead, combinations of keywords
and MESH headings were used.
The search strings formulated were comprised of the following terms:
organisation, organisational innovation, inventions, entrepreneurship,
innovation management, innovation readiness, service innovation, system
innovation, change, organisational change, readiness for change,

determinants of innovation, change management, determinants of change,
readiness, health service delivery, delivery of health care, management and
determinant. The box outlined in (Figure 3.2) shows how the keywords were
combined. The search results generated from the four databases were refined
by skimming through the subject headings in order to distinguish the
relevance to the review question, and thereafter only relevant publications
were included. To keep the review manageable some inclusion and exclusion
criteria were defined (see Figure 3.3).

Figure 3. 2: Extract of final search string
((MH “innovate*”) OR (AB “innovate*” OR TI “innovate”) OR (“invent*”) OR
(AB ”invent*” OR TI “invent*”) OR (MH “Inventions”) OR (MH “Entrepreneurship”) OR (MH “Organizational
Innovation”) OR (AB Organi♯ational Innovation OR TI Organizational Innovation”)
OR
(“ system innovation$”) OR (“service innovation$”) OR (“innovation readiness”) OR (“readiness for innovation”)
OR (“innovation management”) OR (“managing innovation”)
AND
(“change”) OR (“organi♯ational change”) OR (“change readiness”) OR (“readiness for change”) OR
(“determinant£ of change”) OR (“change manage*”)
AND
(“readiness”) OR (“prepar*”) OR (“adopt*”) OR (“indicat*”) OR (“assess*”)

Figure 3. 3: Search limiter based on major subject heading during data search

Inclusion criteria
The search strategy was designed to focus on all sectors in order to obtain a
heterogeneous span of the literature. The original inclusion criteria were:
(1) Studies that reported the impact of readiness on increasing innovation
uptake and sustainability.
(2) Studies that included the terms ‘organisational innovation’, ‘change’ and
‘readiness’ in their titles.
(N.B. although the review is on readiness for organisational innovation, it
was necessary to extend the search to cover studies on organisational
change as both concepts are often conflated within the literature and
organisational change is broadly covered).
(3) English and non-English publications.
As the review extended, it was apparent that the search had yielded
thousands of journal articles which provided only a minimal contribution to the
research question. It was, therefore, decided to narrow the inclusion criteria to
the following:
(1) Only articles in English in order to avoid translation issues.
(2) Articles published within the last decade, i.e. from January 2004 to 2014.
This time frame was chosen because innovation within healthcare is
relatively new and therefore recent publications would contain references
to the earlier work.
(3) Scholarly peer-reviewed articles only. However, in the Medline and
CINAHL databases peer-reviewed articles limited the search results, with
relevant publications unobtainable. It was consequently decided to review
both peer and non-peer review articles from Medline and CINAHL. While
for the Business Source Complete and PsychInfo databases, only peer-
reviewed articles were selected in order to restrict the number of articles
identified during the search.
(4) The search concluded with journals that specified:
A theoretical concept, model of innovation or change readiness
and

Identified methods to measure organisational readiness.
(5) Relevant websites such as that of the National Institute for Health.
Exclusion criteria
The range of study types excluded were:
(1) Articles out of the review context. For example, articles that focused on
change agents, technological competencies, leadership succession,
cultural change, and readiness in education (as shown in Figure 3.3).
(2) Publications without any references.
(3) Magazines, editorials and commentaries as these lacked a theoretical
basis and detailed information.
In addition to the electronic-database searches, non-electronic sources were
also manually searched, and these included:
Text books: 18 books were selected for review and chosen based upon
their titles which included words such as ‘innovation’, ‘readiness’,
‘innovation management’, or ‘diffusion of innovation’.
Google Scholar: Keywords such as ‘innovation readiness’ and
‘innovation’ were used to interrogate Google Scholar search and this
produced a total of 20,600 articles.
SAGE journals: Linking of words such as ‘readiness for innovation’,
was employed when searching the SAGE journals and this produced a
total of 4,441 articles with 20 selected for further review.
Other information sources searched which were not databases
included: Institute for Health Care Improvement, NESTA, and Future
Health Systems-Innovation for equity. However, the search results from
these sources were eliminated as the information was not particularly
relevant to the review.

3.2.3 Storing the results
The search results were exported into Endnote x7. At this stage, the
duplication of articles was identified and the existing search results were
screened against the inclusion criteria. Studies that did not meet the eligibility
criteria were excluded using the justification described above. Excluded data
were transferred into several group headings within Endnote x7 in order to
gain access and show evidence of the search results. To produce a
reproducible and transparent procedure, all the searches were recorded and
the results tabulated (see Appendix A).
3.2.4 Study selection and screening phase
A total of 18,033 articles were identified through electronic searching. After
eliminations on the basis of the title, and the inclusion and exclusion criteria,
416 articles were retained. From these, 29 articles were identified for review
as they met the inclusion criteria. During the review of these 29 articles, a
snowballing process occurred and a further 79 articles were selected. In
addition, articles were manually searched and a total of 50 more publications
were chosen. The articles selected from the snowballing process and the
manual search did not have to meet the inclusion and exclusion criteria.
Instead, they were selected based on:
(1) Relevancy contribution to the review questions;
(2) Contribution to the fundamental foundation for the review; and
(3) Provision of a basic understanding of organisational readiness for
innovation and/or change.
In total, 157 journal articles were selected and put forward for the final review.
After the final screening using the inclusion and exclusion criteria, 20 articles
were selected for appraisal. During the final appraisal, 18 articles (see Figure 3.4) were selected and these formed the basis of the review discussion and
the subsequent recommendation.

Figure 3. 4: Search and selection scheme

3.2.5 Data appraisal and synthesis phase
In maintaining rigour, the selected articles were appraised based on their
validity and relevance to the review question using a generic critical appraisal
tool composed by Woolliams et al. (2009) and the Critical Appraisal Skills
Programme (CASP) appraisal tool that can be found at the CASP website
(www.phru.nhs.uk/casp/casp.htm). The appraisal tools assist in critically
appraising the value of the literature by following the evaluation checklists.
The findings of the primary studies were then grouped together in a table
using a narrative summary (see Table 3.1). The narrative summary technique
was chosen over other forms of data synthesis as it enables a discussion of
the evidence in a descriptive manner which can lead to higher levels of
abstraction (Dixon-Woods et al., 2005). The primary studies were grouped
under seven sub-categories: name of author and year, construct name, article
type, study design, conceptual definition, operationalisation of the construct,
and the scope of the study. The use of sub-categories provided a clear
explanation of the study findings and helped in the critical evaluation of the
specific review question.
3.2.6 Study limitations
This review has some limitations, as for two of the databases searched, only
peer-reviewed publications were selected. Although the reason for this was
explained in the systematic review method phase, publication bias may have
still occurred. Relevant subjects on the conceptualisation readiness may have
been found within grey literature. Limited empirical evidence may also have
been identified as a result of the specified criterion to include only publications
with readiness for ‘organisational change’ or ‘innovation’ in the title. In
addition, specified search limiters were employed to only include publications
with theories, models, frameworks or measurement criteria. However, the
review discussion is based on recent publications by prominent scholars and
experts in the management field.

Table 3. 1: Narrative overviews used as key sources in this review
Author (Year) Construct Name Article Type Study Design
Conceptual Definition Stage Construct Applies
Scope of the study
(Armenakis, Harris and Mossholder, 1993)
Readiness for change
Conceptual - Readiness is the degree to which organisational members believe a change is needed and the organisational capacity to successfully implement those changes.
Implementation The authors emphasise the significance of building readiness within the context facing an organisation. Discussing various strategies useful for communicating readiness.
(Snyder-Halpern, 1998)
Readiness for nursing research programme
Empirical Survey Not defined Continuous Process
Describes the importance of innovation readiness in health services organisations and examines how readiness can be measured.
(Eby et al., 2000) Organisational readiness for change
Empirical Survey Readiness is the ‘cognitive precursor to the behaviours of either resistance to, or support for, a change effort’ (p.420).
Continuous process
Discusses the factors that drive readiness for organisational change.
(Snyder-Halpern, 2001)
Organisational readiness for innovation
Empirical Survey Innovation readiness is the “level of fit between an innovation and an organisation” (p.180).
Continuous Process
Develops indicators for assessing information technology innovation in health

Table 3. 1 continued: Narrative overviews used as key sources in this reviewAuthor (Year) Construct Name Article Type Study
DesignConceptual Definition Stage Construct
AppliesScope of the study
services organisations.
(Lehman, Greener and Simpson, 2002)
Organisational readiness for change
Empirical Survey Not defined. Not specified Focuses primarily on four domains of organisational readiness that include: motivational readiness, institutional resources, staff attributes and organisational climate.
(Snyder-Halpern, 2002)
Organisational innovation readiness
Empirical Survey Innovation readiness is the “level of fit between an innovation and an organisation” (p.180).
Continuous Process
Validates innovation readiness scales developed in phase two study as above.
(Weeks et al., 2004)
Organisational readiness for change
Empirical Survey Readiness ‘is the degree to which an individual sales manager’s (1) beliefs, attitudes, and intentions regarding the context to which change is needed, and (2) perceptions of the organisation’s ability to deal with change under dynamic business conditions’ (p.9).
Implementation Measures the impact of organisational readiness on individual job performances. Also, the impact of the fear of change on readiness.
Table 3. 1 continued: Narrative overviews used as key sources in this reviewAuthor (Year) Construct Name Article Type Study
DesignConceptual Definition Stage Construct
AppliesScope of the study
(Snyder and Fields, 2006)
Organisational innovation readiness
Empirical Survey Innovation readiness is the “level of fit between an innovation and an organisation” (p.180).
Continuous process
Validates the reliability and validity of the psychometric findings across the two previous studies.
(Holt et al., 2007) Readiness for organisational change
Empirical Mixed-methodology
Readiness ‘is a comprehensive attitude that is influenced by content, process, context, and individuals; it reflects the extent to which an individual or individuals are cognitively and emotionally inclined to accept, embrace, and adopt a particularly plan to purposefully alter the status quo’ (p.235)
Not specified Develops a conceptual framework to guide a comprehensive readiness measure, based on a wealth of primary studies.
(Weiner, Amick and Lee, 2008)
Organisational readiness for change
Conceptual - Readiness is a ‘two-dimensional construct that refers to organisational members’ motivation and capability to implement intentional organisation change’ (p.424).
Implementation Reviews a large, fragmented body of work on readiness for organisational change, including its definition and measurement.

Table 3. 1 continued: Narrative overviews used as key sources in this reviewAuthor (Year) Construct Name Article Type Study
DesignConceptual Definition Stage Construct
AppliesScope of the study
(Weiner, 2009) Organisational readiness for change
Conceptual - Readiness refers to ‘organisational members’ change commitment and change efficacy to implement organisational change’ (p.68).
Implementation Organisational change proposes a theory of readiness that considers both its determinants and outcomes.
(Holt et al., 2010) Readiness for change
Conceptual - Readiness is the ‘degree to which those involved are individually and collectively primed, motivated, and technically capable of executing the change…By initial readiness we mean the degree to which those involved are individually and collective primed, motivated, and technically capable of executing the change.’ This includes ‘psychological factors that reflect the extent to which individuals hold key beliefs regarding
Implementation Argues that readiness for change consists of structural and psychological factors that have an influence at the individual level and organisational level.

Table 3. 1 continued: Narrative overviews used as key sources in this reviewAuthor (Year) Construct Name Article Type Study
DesignConceptual Definition Stage Construct
AppliesScope of the study
the change, recognise that a problem needs to be addressed, and agree with the changes that individuals and the organisation must take….It also includes the structural factors that reflect the circumstances under which change is occurring and the extent to which these circumstances enhance or inhibit the implementation of a change’ (p.50).
(Rafferty, Jimmieson and Armenakis, 2012)
A multilevel review of change readiness
- Readiness is influenced by an individual’s beliefs and an individual’s affective emotional responses to a specific change event.
Not specified The authors emphasise the importance of ‘affect’ as a component of readiness and advise that readiness should be considered at multiple levels, i.e. individual, work group and organisational levels.

Table 3. 1 continued: Narrative overviews used as key sources in this reviewAuthor (Year) Construct Name Article Type Study
DesignConceptual Definition Stage Construct
AppliesScope of the study
(Attieh et al., 2013)
Organisational readiness
Conceptual - Innovation readiness ‘is the willingness and ability to adopt or implement an innovation in the workplace’ (p. 6).
Adoption or Implementation
Reviews the literature on readiness for change in healthcare and provides a framework for readiness.
(Holt and Vardaman, 2013)
Readiness for change
Conceptual - Readiness is the ‘degree to which those involved are collectively primed, motivated and technically capable of executing the change’ (p.9)
Preparation Provides a case for an expanded conceptualisation of readiness that incorporates ‘awareness’- i.e. mindfulness, of the change agents part about how a change is unfolding in order to alter routine behaviours of individuals and support a proposed change.
(Stevens, 2013) Process-Based approach of conceptualising change readiness
Conceptual - Readiness is a ‘continuous function of an individual’s cognitive and affective evaluations (themselves influenced by a host of internal and external factors) of
Continuous Process
Provides a framework for synthesising readiness as process-based at an individual level of analysis.

Table 3. 1 continued: Narrative overviews used as key sources in this reviewAuthor (Year) Construct Name Article Type Study
DesignConceptual Definition Stage Construct
AppliesScope of the study
a set conditions and the way in which those evaluations are then tied to change-relevant responses that are positive and proactive in nature’ (p.345).
(Khan et al., 2014)
Support tool for organisational readiness for change.
Conceptual - Readiness is the ‘degreeto which organisational members are both psychologically and behaviourally prepared to implement change’ (p. 2).
Implementation Proposes a tool to aid innovation implementation decision-making.
(Shea at al., 2014)
Organisational readiness for implementing change
Empirical Mixed- methodology
Organisational readiness ‘refers to the extent to which organisational members are psychologically and behaviourally prepared to implement organisational change’ (p.3)
Implementation Demonstrates validity and reliability of the psychometric properties of readiness identified in Weiner’s theory.
3.3 Results
This section discusses the findings of the studies and their implications for
further research. In total, seven of the eighteen articles (39%) were published
before 2004 and the remaining eleven (61%) were published within the last 10
years. Although the review inclusion criteria stated that only articles published
within the last ten years should be included, seven studies outside this time
frame were included as they contained relevant information. Of the selected
articles, nine (50%) offered conceptual discussions on organisational
readiness and the remaining nine (50%) were empirical based research. In
total, nine (56%) studies were conducted within health services research and
nine (44%) focused on general organisations and management.
Organisational readiness has been portrayed differently across the literature.
The next section provides the contextual knowledge underpinning the
construct ‘readiness’. This section presents the findings underpinning the
construct readiness from across the literature reviewed, organised broadly
around different theories. The section aims to answer the review questions by
discussing critically the meanings of readiness and the conditions underlying
its measurement.
3.3.1 Background theory underlying organisational readiness
Lewin (1939) explained that human behaviour, that is, personality, thoughts,
feelings, attitudes, motivation, and ideologies, stems from small or large
changes and forces within people’s environment or social field. In the field
theory, Lewin (1947) explained a social field is the totality of coexisting
realities such as groups, sub groups, culture, social facts, barriers, outlets of
communication and systems, which are considered as mutually
interdependent. Lewin (1947) believed a social field is in a continuous state of
adaptation, and that ‘social change’ and ‘social stability’ are relative concepts
as individual or group behaviours are simply without change, the only
difference being the type and degree of change. For instance, the mere
constancy of productivity amongst a work team in a factory does not ascertain
stability, in spite of change. Neither does change prove little resistance. Only
70

by relating the degree of constancy to the strength of forces acting on the
deviation or adherence from the present state of circumstances can the
resistance or stability of the group’s behaviour be fully understood and change
can be planned (Lewin, 1947). Lewin coined this term ‘quasi-stationary
equilibrium’ to explain that whilst individual behaviour is a product of the
pattern and rhythm of the social group to which they belong, behaviour tends
to fluctuate, owing to the changes of the forces and events that impinge on
the group. Based on force field theory, Lewin explained that changing an
individual’s or a group’s behaviour requires an understanding of the nature of
the forces - restraining or driving - acting to maintain the existing status quo or
the present situation (Lewin, 1947). The driving forces that make individuals
attracted to change, such as ambition and goals needs, must be strengthened
whilst the restraining forces that prevent people from accepting change are
weakened or reduced.
Lewin (1947) later integrated the force field theory with a three-stage theory of
change to explain how to unfreeze the existing equilibrium, moving it towards
a desired change and then freezing the change at the desired level in order
for the constancy of the new behaviour and a new equilibrium or quasi
equilibrium is, thus, formed (Lewin, 1947). Lewin’s model of behavioural
change establishes a theoretical foundation upon which understanding
readiness for organisational change is formed solidly, particularly Lewin’s
three-step model of change.
Figure 3. 5: Lewin’s processes of planned change
Source: Armenakis and Bedeian (1999)
71

The concept of unfreezing is that of destabilising the equilibrium by interfering
with the forces and conditions that maintain the behaviour and processes of a
group in its present form in order to break the old habit (Lewin, 1947). Building
on Lewin’s idea, Schein (1999) comments that individuals must go through
three processes during unfreezing for readiness to change to be generated.
An individual must first feel dissatisfied about the outcome of social events
and this ‘disconfirmation’ arouses the driving force with which the individual
strives to achieve the goals required to fulfill a need. This will then enable
individuals to have a perception of “psychological safety” which is a collective
or self-feeling where individuals feel safe to embark on a task without the fear
of being reprimanded if error occurs (Baer and Frese, 2003, Schein, 1999).
Studies have shown a relationship between psychological safety and team
learning (Edmondson, 1999) which in turn is associated with higher team
creativity (West and Farr, 1990), job performance and job involvement (Brown
and Leigh, 1996). Lewin’s theories of behaviour provide the basis for
analysing, understanding, and reinforcing change at the individual, group, and
organisational level. The effect of Lewin’s theorising about the principles
underlying the social-psychological world laid a foundation for change
management researchers to begin to develop their own theories of
organisational readiness. The section below includes some of the various
conceptualisations of organisational readiness identified within the literature.
3.3.2 Readiness is a change message
Building further on Lewin’s premises, specifically the ‘unfreezing’ concept,
Armenakis, Harris and Mossholder (1993) referred to readiness as the
‘cognitive antecedent’ that stimulates organisational members’ willingness to
accept or reject a proposed organisational change. ‘Cognitive’ here refers to
“the beliefs, attitudes, intentions of organisational members regarding the
need for and capability of implementing organisational change” (Armenakis
and Fredenberger, 1997, p. 144). Armenakis et al. (1993; 1997) considered
readiness to be a catalyst that aids the successful implementation of
organisational change because when organisational readiness is high,
organisational members are more interested in the change, exercise greater
72

effort during the change process and will exhibit greater persistence in the
face of obstacles or setbacks (Weiner, Amick and Lee, 2008, p. 382).
Rafferty, Jimmieson and Armenakis (2012) pointed out that whilst Armenakis,
Harris and Mossholder’s (1993) definition of readiness remains highly
accepted for explaining behavioural intentions, it fails to acknowledge the
affective component of change readiness. Affect considers the different
emotions such as ‘sadness, happiness, disgust, joy, and excitement’ that may
influence the individual’s readiness towards any change initiative (Rafferty,
Jimmieson and Armenakis, 2012). Direct evidence supports this opinion as,
for example, Weeks et al. (2004) found that organisational managers who
were more fearful of change were also more sensitive about their
organisation’s readiness for change. Thus, we see that an individual’s affect
has an impact on the cognitive appraisal concerning his or her perception
about their organisations’ readiness to change (Antonacopoulou and Gabriel,
2001; Baer and Frese, 2003; Choi et al., 2011; Huy, 2011; Rafferty,
Jimmieson and Armenakis, 2012; Ashkanasy, Humphrey and Huy, 2017).
Applying both the principles of Kurt Lewin’s (1947) seminal work and
Bandura’s (1986) social learning theory, Armenakis, Harris and Feild (1999)
proposed a five-message component model for institutionalising
organisational change. The model aims to guide change agents to understand
how individuals define and represent a proposed change and then go on to
cope with it. Research has shown that organisational change must be first
enacted at the individual level (Walinga, 2008). Armenakis, Harris and Feild
(1999) proposed that an individual’s readiness evolved through a series of
stages beginning with the “change message” used by change agents for
conveying a need for change. For individuals to be able to construct a
reasoned perception and emotional information towards a proposed change
endeavour, a change message must be developed and be a composite of the
following five elements which are:
o Discrepancy. Defined as the “difference between the current state
and the ideal situation” (Self and Schraeder, 2009, p. 172), discrepancy
reinforces the need for change. When organisational members are unable to
73

identify a compelling difference between the present state and the desired
one, there would be no drive towards achieving it (Armenakis, Harris and
Mossholder, 1993; Armenakis, Harris and Feild, 1999). A classic example is
Coch and French’s (1948) experiment on reducing resistance amongst
organisational members working at a plant factory that produced pajamas.
The study consisted of four experimental groups with varying degrees of
participation and showed that group participation in planning the changes and
management communicating the need for change greatly modified group
resistance to change. Another example is Prochaska and DiClemente (1983)
trans-theoretical model which suggests how persons thinking about changing
their smoking behavior would use sources of information related to the pros
and cons. Discrepancy is a critical element of the change management
process as it shapes an individual’s mind-set and movement towards change.
In line with the knowledge acquisition perspective, as individuals recognise
the differences between new and existing information, there is a shift in their
current mental model and this triggers a willingness to engage in the process
of change readiness (Rusly, Sun and Corner, 2015).
o Appropriateness. The second message component of the change
message described by Armenakis et al. (1993; 1999) is the degree of
‘appropriateness.’ When targeted, organisational change members consider
that the new strategy and its complementing structure being introduced are
needed (i.e., discrepancy) and then the next issue of appropriateness is being
questioned. This takes the form of the question: “Is the specific change being
introduced appropriate?” Cole, Harris and Bernerth (2006) described an
organisation in which individuals who had a strong satisfaction with
appropriateness showed higher job satisfactions and lower turnover
intentions, even when the vision for change was unclear. Thus, management
must demonstrate that the proposed change initiative is most appropriate for
the organisation, otherwise, organisational members will show resistance
(Self and Schraeder, 2009).
o Principal support. The third component of a change message is
known as the principal or leader support. This component answers the
74

question, “Who supports the change?” According to Armenakis, Harris and
Feild (1999, p. 103) principal support was necessary to provide information
and convince organisational members that the formal and informal leaders
were committed to a successful implementation … of the change.” When a
change idea is proposed, organisational members will look out for
management support, especially if there is a past history of failure or
abandoned projects (Armenakis and Harris, 2000; Self and Schraeder, 2009).
Given the higher level of organisational cynicism impacting on change
outcomes, it is management’s responsibility to convey their long-term
commitment to an action that is anticipated to be useful (Wisdom et al., 2014;
Aarons et al., 2016). Management do, in fact, have to communicate their
commitment across three different variables – time, energy, and resources –
which are necessary to drive planned change through to successful
implementation (Kilmann, 1984; Armenakis and Harris, 2002; Lehman,
Greener and Simpson, 2002; Weiner, 2009). A perception of principal support
conveys a message to organisational members that management is ready to
commit beyond the quick fix or a short-term approach taken to solve problems
(Kilmann, 1984). Several management researchers have stressed that the
absence of managerial support could cause organisational members not to
commit themselves to utilising an innovation because they perceive it as
simply being a fad (Klein and Knight, 2005; Birken et al., 2015; Shipton et al.,
2016).
o Efficacy. The fourth message component proposed by Armenakis,
Harris and Feild (1999) relates to efficacy. This is one’s perceived capability of
achieving one’s tasks (Bandura, 1989). Armenakis, Harris and Feild (1999)
described efficacy as answering the question: “Can I/we successfully
implement the change?” If organisational members do not perceive they have
the capability of completing a task successfully, then their level of readiness
becomes compromised. People with higher levels of self-efficacy are more
proactive and creative in problem-solving (Tabak and Barr, 1996; Gong,
Huang and Farh, 2009; Richter et al., 2012). Therefore, organisational
members with this quality would be more supportive of innovation because
they would feel competent enough to handle the challenges associated with it.
75

o Personal valence. The fifth component of the change message is
known as personal valence. Bernerth et al. (2007) explained that
organisational members can believe a change is needed, that top
management would support it, and that the organisation has the capability to
implement the change. However, if they perceive the proposed change does
not add some kind of significant benefit at a personal level or that the change
has a degree of potential harm, they are more likely to be unresponsive and
unwilling to embrace the change effort (Armenakis and Harris, 2002; Weeks
et al., 2004; Bernerth et al., 2007; Vakola, 2014). Rogers (2003) argues that
for diffusion to occur rapidly, an innovation must be compatible with the values
of members of the organisation. When the targeted individuals find the
innovation to be very compatible with their important values, they are more
likely to make a consistent and committed use of the innovation. There will be
few objections because the employees perceive that the innovation bolsters
their existing values (Klein and Sorra, 1996; Σπανός and Spanos, 2009). On
the other hand, if it is perceived as not being aligned with their values and
beliefs, the staff may ignore it completely or it will diffuse across the
organisation very slowly (Meyer and Goes, 1988; Rogers, 2003; Greenhalgh
et al., 2004; Ferlie et al, 2005; Feldstein and Glasgow, 2008; Fennell and
Warnecke, 2013). By leadership clarifying the personal valence to
organisational members, they address the question: “What is in it for me?”
Armenakis and Harris (2002) explained that in the readiness speech, the
intrinsic and extrinsic valence should be emphasised which can include
employment stability and flexibility and the organisational members’ progress
and development.
Armenakis, Harris and Mossholder (1993) explained that change agents must
take into account that influence strategies (such as persuasive
communication, active participation), as well as the contextual factors and
interpersonal dynamics are what determines the effectiveness of an individual
readiness to change. However, in a socially constructed organisation,
organisational members may share a separately schemata or interpretative
scheme different from those of the change agents (Bartunek, Balogun and
Do, 2011). Thus, it has been advised that the change message is maintained
76

throughout the duration of the change process (Armenakis, Harris and
Mossholder, 1993; Todnem, 2005). The implication of the five-change model
is that readiness is the outcome of a change process (mental state or
cognitive antecedent to change supportive or resistance behaviour), and can
also be the social cognitive process through which the mental state is
achieved (Stevens, 2013). However, in the case of the aforementioned, it
raises conceptual ambiguity, as readiness is conceivable as one of different
components (e.g., intentions, attitudes, and beliefs).
3.3.3 Readiness is perceived capability
‘Readiness’ is defined as an individual and an organisation’s capability to
change (Lehman, Greener and Simpson, 2002; Weiner, Amick and Lee, 2008;
Weiner, 2009). Weiner (2009) defined readiness as the degree to which
organisational members share a sense of collective efficacy to deliver change.
Self-efficacy is one of the several cognitive processes frequently considered
in the determination of an individual’s behaviour towards readiness (Gist and
Mitchell, 1992; Armenakis and Harris, 2002).
Formerly, self-efficacy was defined as the individual’s belief in their ability to
execute a specifc undertaking (Bandura, 1977). More recently, the definition
has expanded to include a range of other elements. Self-efficacy is defined as
the collective’s “beliefs in their capabilities to mobilise the motivation, cognitive
resources and courses of action needed to exercise control over task
demands” (Bandura 1990, p. 316). Hence, self-efficacy is not concerned with
“the skills a person has, but what they can do with those skills, applying it in
an effectual way to produce change” (Weiner, Amick and Lee, 2008, p. 425).
People feel, think and behave according to their perceived potential
effectiveness at any given moment and about any given situation or object. An
individual will process available information and assess the adequacy of their
resources in order to cope. A person with a highly developed sense of self-
efficacy will be motivated to undertake a difficult task, persist in the face of
obstacles and be committed to completing the course of action. This is in
comparison to an individual with a low level of self-efficacy who will view
77
problems or tasks as formidable and so is likely to slacken off or give up
(Maddux and Lewis, 1995). A review of the literature pointed out that self-
efficacy and intrinsic interest in tasks can be positively and adversely affected
as certain conditions existing prior to the change can and do influence the
individual’s interpretation of organisational innovation. These are discussed
under the following subheadings:
Personal characteristics that affect individuals’ response to innovation
Every decision-maker or individual involved in the adoption process brings a
unique perspective in the process and so the final decision is subject to
individual behavioural influences and the perceptions of the people involved.
The characteristics that influence such behaviours include:
o Risk propensity. Innovation, especially the radical type, involves a
high-level of risk and uncertainty. Risk propensity is the susceptibility to take
risk and tolerate and learn from failure (Sitkin and Pablo, 1992). This quality is
correlated to individuals' risk tolerance, opposition to change and acceptance
for ambiguity (Baird and Thomas, 1985). Decision-makers with high risk
tolerance, high tolerance for ambiguity and low opposition to change will tend
to take more risks, be more flexible and therefore support the decision to
adopt an innovation (Saleh and Wang, 1993; Σπανός and Spanos, 2009;
García-Granero et al., 2015).
o Cognitive complexity. Cognitive complexity is referred to as the
capability to perceive and process different ideas, events and assess or
analyse them correctly to draw deductions and make decisions (Tabak and
Barr, 1996). The more complicated the proposed innovation, the slower the
rate of diffusion because simple innovations spread faster than complicated
ones (Meyer and Goes, 1988; Denis et al., 2002; Rogers, 2003; Greenhalgh
et al., 2004). Individuals with high cognitive complexity analyse situations
better than others and are more capable of reaching creative and novel
solutions. Thus, they would support innovation adoption because they
understand aspects of the innovation that might seem very complex and
misleadingly disadvantageous to others.
78

o Demographic characteristics of the decision-makers. Other
characteristics including age, education and past experiences affect
innovation adoption as shown by the literature (Goll and Rasheed, 2005;
Damanpour and Schneider, 2006; Wang et al., 2016). Younger managers
may be more open to new ideas due to their more recent education that is in
keeping with more recent occurrences. Thus, they are willing to take more
risks compared to older managers who are more committed to existing
conditions and are less willing to change. Similarly, higher formal education
may increase the receptivity to new ideas and improve cognitive complexity
and self-efficacy (Huber, Ragin and Stephens, 1993; Wang et al., 2016). Past
experiences with innovation also positively affect innovation (Tabak and Barr,
1996; Amabile and Pratt, 2016; Lee, Hallak and Sardeshmukh, 2016)
because this fosters more self-efficacy, optimism, positivity and confidence
about the prospective innovation.
3.3.4 Readiness is commitment to change
Weiner (2009) defined readiness as organisational members ‘shared
commitment’ to deliver change. Commitment is explicitly one of the most
salient factors for successful innovation implementation and has been
positively linked to improvement performance (Klein and Sorra, 1996;
Rafferty, Jimmieson and Armenakis, 2012; Sol, Beers and Wals, 2013; Shea
at al., 2014; McDonald, 2015). Commitment is defined as a ‘force (mind-set)
that binds organisational members to a course of action deemed necessary
for the successful implementation of a change initiative’ (Herscovitch and
Meyer, 2002, p. 475). It has also been defined as an individual’s sense of
psychological and emotional attachment and loyalty to the organisation
(O'Reilly and Chatman, 1986; Meyer and Allen, 1991). This commitment
generates a mind-set that drives an individual to engage in activities
necessary for the successful implementation of a proposed task (Herscovitch
and Meyer, 2002). Meyer and Allen (1991) explained that individuals are
sometimes compelled to show commitment because of the consequences -
good or bad – that may arise from adopting change. For instance, fear of
being unemployed, losing a prospective position, and even a feeling of guilt
79

due to the organisation’s financial investment in the individual’s training and
development (Meyer and Allen, 1991).
The commitment component of readiness differs from Lewin (1947) and
Armenakis and Harris (2002), and their three-stage model for enhancing
commitment to organisational change. In the model proposed by Armenakis
and Harris (2002), institutionalisation of change occurs through a process of
first creating readiness which then contributes to the organisational members’
decision to adopt the innovation. This leads to a commitment to change and
later, institutionalisation. This process of commitment is referred to as the
freezing stage. In contrast, the level of commitment described by Herscovitch
and Meyer (2002) and Weiner (2009) appears to be wider in scope and does
not refer to any particular stage of the organisational change process.
However, the conceptualisation of readiness as a change message or a level
of commitment is seen as a cognitive precursor to change supportive
behaviours (Stevens, 2013). The literature identified some contextual factors
that impact the commitment level towards innovation, these include: positive
climate for innovation, continuous culture for innovation, team reflexivity, and
absorptive capacity.
o Organisational climate. Gaddis et al. (2003, p. 253) described
organisational climate as the “shared normative expectations regarding social
interactions and other work behaviours.” Organisational members’ perception
of the climate determines their day-to-day models and rules as to what kind of
behaviour is acceptable, supported and rewarded. Further, it influences how
they manage difficulty in abstruse situations and it also influences how they
respond to pressure to increase productivity within resource constraints
(Gaddis et al., 2003; Weeks et al., 2004). Douglas et al. (2017) believe that in
comparison to organisational culture, climate is more tangible and more
attention should be paid to it since it can influence the organisational
members’ belief about their organisation’s values or culture. A number of
studies have identified the fundamentals of climate that support innovation-
driven behaviours. The literature on innovation suggests that it is more likely
to occur within organisations or groups that reward and recognise innovative
80

behaviours (Klein and Sorra, 1996; Luecke and Katz, 2003; Kanter, 2013;
Tidd and Bessant, 2013). Such organisations stimulate a culture that readily
assimilates and implements new knowledge (Schneider, Brief and Guzzo,
1996; French et al., 2009; Holt et al., 2010; Schein, 2010). An effective
implementation climate is usually characterised by mutual trust and respect,
with organisational members having a positive perception of psychological
safety and openness to share and discuss their opinions. This also includes
the leaders’ willingness to consider suggestions for new approaches to the
situation (Schneider, Brief and Guzzo, 1996; Gaddis et al., 2003; Tidd and
Bessant, 2013). A climate that provides a level of autonomy for organisational
members to manage their own workspace and which permits the use of
discretion and initiative by them is also positively associated with adoption
(Mumford and Gustafson, 1988; Rafferty, Ball and Aiken, 2001; Englehardt
and Simmons, 2002; Kramer and Schmalenberg, 2003; Apker, Ford and Fox,
2003; Mazzei, Flynn and Haynie, 2016).
o Organisational culture. Organisational culture concerns the tightly
rooted beliefs, values and shared norms which reside within the deeper level
of the organisational member’s psyche (Schneider, Brief and Guzzo, 1996).
Given that these beliefs and values are deep-rooted and intangible, it makes
culture quite difficult to change (Schneider, Brief and Guzzo, 1996; Douglas et
al., 2017). Research has shown that an emphasis on continuous improvement
is a prerequisite for any organisational culture intending to drive innovation
(Garcia-Sabater, Marin-Garcia and Perello-Marin, 2012; Assarlind and
Aaboen, 2014). For example, Todnem’s (2005) study representing viewpoints
of middle managers in the top 100 visitor attractions in the United Kingdom
reported that all of the participants were in support of an organisational culture
and structure that facilitated a continuous management of change and a high
level of readiness and possessed the ability to implement change as required.
Ninety-six per cent advocated the need to facilitate a continuous readiness for
change through a constant change message rather than one on the
implementation and management of a particular change endeavour. Seventy-
four per cent perceived continuous change as impractical due to resource
restraints and high levels of stress resulting from an increased workload.
81

Vakola (2014) shared that organisational members who are confident of their
capability to change are able to deal with stressful incidents, and in turn
produce high readiness. Thus, in order to develop a continuous culture,
leadership need to focus on several things, including: the re-shaping of the
capacity for innovation through ongoing training to maintain the organisational
members’ competence; resource allocation; the integration of innovation into
the curricula; and a constant communication about innovation benefits during
the adoption stage (Frambach and Schillewaert, 2002; Greenhalgh et al.,
2004; Mitchell et al., 2010).
o Collective reflexivity. West (1996) defined team reflexivity as
organisational members’ ability to “collectively reflect upon the teams goals,
strategies, and processes and the wider organisations and environments, and
adapt them accordingly” (as seen in West, 2002, p. 376). The emphasis on
team reflexivity is based on the notion that the environment is constantly
evolving and there is need for continuous reflection and learning so an
organisation can plan and adapt accordingly (Tjosvold, Tang and West, 2004;
West 2002; Hoegl and Parboteeah, 2006; Schulz, Kajamaa and Kerosuo,
2015; Schmutz and Eppich, 2017). Past research has found that team
reflexivity is positively related to team effectiveness and innovation (Hoegl and
Parboteeah, 2006; Schippers, West and Dawson, 2015), and an early
adoption of innovations based on best practice guidelines (Dubé and
Ducharme, 2014). West (2002) explained that a high level of reflexivity
creates an intangible readiness for, and guides organisational members’
responsiveness towards pertinent openings for actions and processes to
implement innovation. A reflexive environment will help foster a proper
identification of the problematic issues, an efficient use of time and the
resources needed to produce solutions. Thus, organisational members are
more prepared and willing to embrace the need for change.
o Absorptive capacity. Absorptive capacity is an organisation’s ability to
identify new external knowledge and to assimilate, transform, and apply it
within an organisational context (Cohen and Levinthal, 1990; Zahra and
George, 2002). This has positive implications for pre-adoption and adoption
82

(Cohen and Levinthal, 1990; Zahra and George, 2002; Lane, Koka and
Pathak, 2002; Williams, 2011). For example, healthcare organisations with
mechanisms in place for managing the use of knowledge and those which
have the knowledge and skills tend to respond to the evidence about the need
to innovate quicker (Harvey, Jas and Walshe, 2014).
3.3.5 Readiness is organisational fit
This definition of readiness is grounded in the research into information
technology systems. The successful implementation of large-scale health
information technology systems is costly to implement as well as difficult to
operate with failure rates of 30 per cent or greater (Southon, Sauer and
Dampney, 1997; Kellermann and Jones, 2013; Almajali, Masa’deh and
Tarhini, 2016). In an uncertain climate, readiness helps to augment certainty
and minimise wrong assessment regarding the potential for a successful
innovation programme (Snyder-Halpern, 1998). Snyder-Halpern (1998; 2001)
stated that readiness can help minimise the potential risks associated with
innovation activities and increase the chances of a more successful
information technology systems outcome. Similar to Armenakis, Harris and
Mossholder (1993) view of continuous readiness for any large-scale change
programme, Snyder-Halpern (1998) identified readiness as the most crucial
stage during the innovation management process because it acts as a
predecessor to successful innovation adoption, implementation, and diffusion.
In defining readiness, Snyder-Halpern (2001) referred to it as the degree of
‘fit’ between new information technology systems and the organisation’s
internal characteristics and external dynamics.
The concept of fit has been well-established in the literature on information
systems. A popular organisational information technology fit framework is the
MIT’90s developed by Scott Morton (1991). The framework depicts a series of
relationship between five constructs – strategy, structure, information
technology, management process, and roles and skills. Based on this
framework, high performance is sustained when there is a tight fit across the
aforementioned elements (Southon, Sauer and Dampney, 1997). Snyder-
Halpern provided a model that can aid healthcare change leaders in their
83

decision-making processes during the implementation of an information
technological system. The term ‘fit’ is key in the model because of the notion
that health information technology implementation necessitates the
consideration of a range of technical, social and organisational determinants
to ensure the usefulness of the technological innovation for both the clinicians
and the organisational processes (Snyder-Halpern, 1998; Snyder and Fields
2006; Cresswell and Sheikh, 2013). Based on the fit theory, organisational
validity is actually established if there is a fit or congruence between an
information system and its organisational context (Markus and Robey, 1983;
Livari, 1992; Martin et al., 2008).
Most of the past studies on information technology have adopted the diffusion
of innovation theory (Rogers, 2003) to explain the attributes that influence
information systems adoption from the consumer’s perspective. Among the
commonly examined characteristics that promote the adoption of the
technology are: relative advantage, compatibility, and trialability. Although the
findings are transferrable to information systems innovations for users
acceptance, Southon, Sauer and Dampney (1997) argued that the diffusion of
innovation theory remains only applicable at the level of the individual user
and does not provide information about other attributes that may influence
diffusion and technology transfer (Southon, Sauer and Dampney, 1997).
Theories about information technology have indicated that high organisational
readiness is an individual factor and does not necessarily lead to better
integration because other contextual factors play a role in determining the
success of any particular innovation. Drawing insights from organisational fit
theory, the following section discusses the factors that interact to influence the
success of the adoption and implementation of innovation.
o Availability of resources. Lacovou, Benbasat and Dexter (1995)
defined organisational readiness as the level of financial resources and
availability of resources in terms of the time to explore new ideas prior to
adoption, technical support as well as the human and material resources
required to execute the innovation effort. The availability of resources was
considered to be vital “because some firms, especially those smaller in size,
84

tend to lack the resources necessary for investment in information
technological’’ (Lacovou, Benbasat and Dexter, 1995, p. 469). Empirical
evidence has emphasised that increased investment in financial and human
resources would help to enhance the exchange of health information across
settings and systems between nursing homes and a wide variety of
stakeholders, including nurses, physicians and pharmacists (Rantz et al.,
2010; Alexander et al., 2015; Alexander et al., 2016).
o Process integration. Snyder Halpern (2001) defined the process
dimension of readiness as the degree of fit between the prospective
innovation characteristics and existing organisational processes. Process
readiness answers the question: Which process needs to be changed or
modified? (Alexander et al., 2016, p. 6). Prior to implementation, conducting
process readiness necessitates assessment of the existing organisational
workflow to identify need, and then harmonising proposed innovation with the
current processes. Tailoring the current processes with proposed innovation is
essential because every organisation has a different degree of readiness to
adopt a new technology (Lacovou, Benbasat and Dexter, 1995; Alexander et
al., 2016).
3.3.6 Readiness as stages of change
Conceptualising readiness as a stage is another common approach deeply
rooted in the trans-theoretical model of change (Prochaska and DiClemente,
1983). This model is an integrative theory of therapy that evaluates an
individual’s readiness to adopt a healthy behaviour. Based on the model, an
individual trying to change moves through a series of stages that include pre-
contemplation where the individual at this stage is unaware of the need to
change his or her behaviour. Thus, he is characterised as uninterested or
unready for help. At the contemplation stage, the individual becomes
conscious of the pros and cons of changing and begin to weigh up the
decision to change. The person then enters the preparation stage, starts to
get ready, and takes gradual steps towards change. The action at the next
stage entails overt modification, for example, lifestyle changes. Finally, he or
85

she arrives at the maintenance stage where the person is able to sustain their
progress and works towards preventing a relapse. The trans-theoretical model
of change bears similarity with Armenakis, Harris and Mossholder’s (1993)
idea of creating a message. However, the trans-theoretical informs the need
for reinforcement management (i.e., finding rewards for new ways of working
in order to prevent individuals from reverting back to the former behaviour),
which was not explicit in the change model (Prochaska, Prochaska and
Levesque, 2001). In comparison to Lewin’s three-step change model, the
trans-theoretical model fails to indicate the exact stage where readiness is
applicable. Other change management researchers imply readiness is
applicable before the implementation of the innovation and immediately after
the adoption phase (Eby et al., 2000; Snyder-Halpern, 2001; Weiner, Amick
and Lee, 2008; Khan et al., 2014; Shea et al., 2014). Holt et al. (2007) and
Attieh et al. (2013) suggest that readiness applies during the adoption or
implementation phase.
3.3.7 Readiness is a process-based synthesis
Stevens (2013, p. 13) defined readiness as a “continuous function of an
individual’s cognitive evaluations influenced by a host of internal and external
contextual factors.” According to Stevens (2013), an individual’s readiness is
influenced by the changes in their organisational context (e.g., competition,
political influence, availability of resources and management support, and
concurrent change) over time. Stevens (2013) view deviates from the
traditional stage-based synthesis (Holt et al., 2010; Choi and Ruona, 2011)
that suggests initial readiness is a sufficient catalyst to subsequent phases of
the change process or the precursor to it (Armenakis, Harris and Mossholder,
1993). Stevens (2013) emphasised that readiness must be maintained
throughout the course of an innovation programme because individuals’ tend
to re-assess and re-consider various events and organisational context to
determine their future behaviour, intention, and attitude. A process-based
synthesis has advantage over the stage-based view as it serves as a
framework within which to integrate other models of readiness at different
points in time and when required (Jones, Jimmieson and Griffiths, 2005;
86

Todnem, 2005). Thus, the concept of readiness plays a significant role from
the development to implementation of an innovation which enables an
organisation to assess potential risks and exercise sound decision-making
(Snyder-Halpern, 1998). The main idea underlying readiness as a continuous
function is that the conditions and scenarios influencing an individual’s
evaluations are not static and predisposed to change at any point in time.
Unlike the stage-based conceptualisation that focuses on the elements that
influence an individual’s belief about readiness (Rafferty, Jimmieson and
Armenakis, 2012), the continuous-based idea states that such particularity
and distinction with regard to readiness is only relevant to a specific set of
conditions (Stevens, 2013).
3.4 Discussion
The review presented in this chapter aimed to consider the current literature
regarding the definition, operationalisation and the factors enabling readiness
for successful innovation management. The researcher reviewed studies
published between 2010 and 2014, out of which 18 met the criteria of studies
of organisational approach to readiness. To identify all the relevant studies, a
structured and systematic approach to data gathering and synthesis was
followed. To achieve the research objectives, 416 publications were reviewed
from which 18 studies were selected for final appraisal. It can be concluded
that the literature lacks rigor and homogeneity and overall is of poor quality.
This is due to small sample sizes, mixed conceptualisations of readiness, and
a lack of differentiation between readiness for innovation and organisational
change. The review highlights that there is limited knowledge concerning the
conceptualisation of organisational readiness.
Firstly, existing definitions of readiness lack a level of criticalness, depth, and
consistency. An absolute number of terms have been used to convey the
meaning of readiness (e.g., commitment, fit, capacity, and attitudes towards
change) and different theoretical models have been proposed. Despite the
richness of theories and models on organisational readiness, there still exist
conceptual incongruences on the meaning. The foundation of the readiness
literature is formed on Lewin’s three-step model for planned change. The
87

simplicity of the model makes it easy to follow, offering a step-by-step
guidance on how to implement change successfully (Cummings and Worley,
2009). Styhre (2002) argues that Lewin’s three-step model offers an over-
simplistic approach to managing organisational change as it assumes an
organisation is in a static state. It fails to recognise that the state of the
environment during freezing is not essentially as it was during unfreezing
(Styhre, 2002). The model also suggests a linear assumption of organisational
change, where the first stage proceeds to the subsequent stage and so forth
(Styhre, 2002). Van de Ven et al. (2008) has made it explicit that innovation
does not follow a simple linear sequence, but rather emerges through
dynamic non-linear and complex process which makes it difficult to predict.
Lewin’s three-step model serves as a powerful representation of change, but
remains a weak model for understanding the principles of organisational
readiness for innovation (Styhre, 2002). Armenakis, Harris and Feild (1997)
five-message model has gained wide acceptance in organisational change
readiness literature. Armenakis et al’s (2007) five-message model, it makes
three valuable contributions. Firstly, it can be used to identify individuals’
belief associated with any particular change. Secondly, it can be used to
complement a different change instrument that is considered useful for
developing organisational change. Thirdly, unlike unfreezing, the change
message can be conducted at any point in time during development, adoption
and implementation. The model has raised academic interest in the studies of
the effect of cognitive and affective processes on individual behaviours
towards organisational change (Seo, Bartunek and Barrett, 2010; Rafferty,
Jimmieson and Armenakis, 2012). However, despite the existing conclusion
about the message model, Blackman, O’Flynn and Ugyel (2013) mentioned
that the application of its approach has reported no improvement in the
success of change. Further readiness conceptualisations that offer an
understanding of factors that influence readiness fall into two broad
categories, the first of which is the characteristics and behaviours of
individuals within the organisation. Here, the literature focused on variables
such as risk propensity, education level, level of awareness, and past
experiences. These factors were related to the reason why an individual
resists change. The second has to do with the effect of how the
88
characteristics of the organisation influence the organisational members'
readiness towards the execution of a course of action. Variables identified
include reward for innovativeness, collective thinking, and the organisation’s
external environment. Problems in conceptualisation of the factors enabling
readiness are due to the lack of clarity about how some of such factors can be
enacted within the organisational context to produce readiness success.
Secondly, theoretical disputes exist within the literature, which has to do with
whether readiness should be treated as a stage-based or a process-based
approach during the implementation of a specific intervention. Most change
management authors have adopted a stage-based perspective for
considering readiness during the organisational change processes. Stage-
based assumptions have focused on the linearity of a system, that is, how
independent components predict the future behaviour of agents in their
commitment to the adoption of an innovation. Understanding readiness in this
way is to take a reductionist and deterministic stance as it treats the factors
that influence innovation in isolation without acknowledging how the different
components interact to create a state of readiness. It also implies that the
future state of a system could be fully predicted, ignoring the impact and role
of interacting agents that co-evolve within the context and produce
organisational and emergent properties (Dooley, 1997; McDaniel, Driebe,
and Lanham, 2013). In contrast, the process-based conceptualisation of
readiness reflects a non-linear view, showing that readiness is never-ending
during the process of managing a specific intervention. This process-based
view enhances an organisation’s level of future anticipation which enables it to
be better prepared for future uncertainties. It also facilitates the way in which
an organisation’s managers think about alternate techniques to improve
success during the innovation process. Such a process-based
conceptualisation of organisational readiness is in line with Van de Ven et al’s
(2008) complexity thinking which portrays innovation as a complex and non-
linear process which requires managers learning the right way to mange in
chaos. This should point out the need to think beyond the stage vs. process
conceptualisation of readiness. Instead, if it is agreed that innovation is a
process, then organisational readiness for innovation should be managed
89
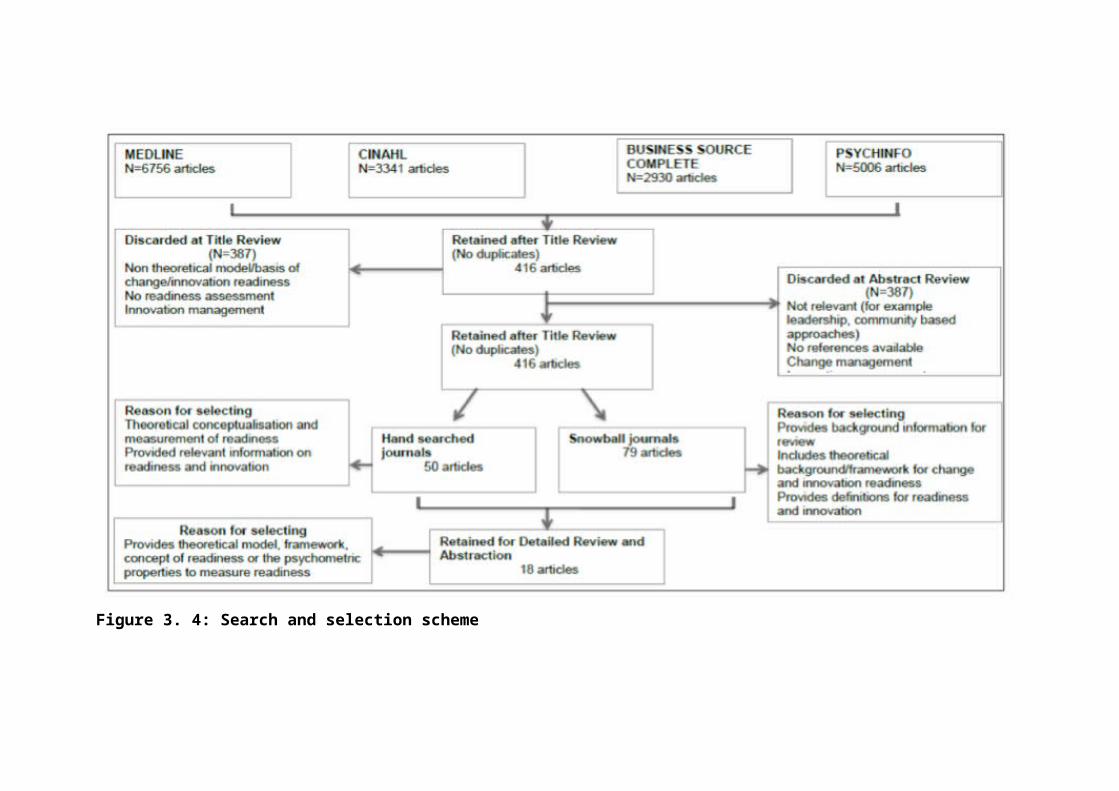
within this context. Though the findings of the review highlighted several
enablers and determinants of readiness, what it failed to establish was how
these factors are enacted within the organisational context to produce
readiness.
Innovation management theorists have called for a move away from this
mechanistic approach of cause and effect to a more non-linear focus of
integrating interdependencies. Recent applications of the complex adaptive
system thinking makes it necessary to consider organisational readiness for
innovation as an evolutionary process and a continuous movement that
emerges as agents communicate their individual capabilities through
interactions with each other over time (Marion and Uhl-Bien, 2002; Senge,
2006). The complex adaptive system theory does not disregard the
management practices rooted in the mechanistic approach, rather it provides
a new lens through which to consider readiness effectively, especially for
organisations established in unstable and uncertain environments (Dooley,
1997; Stacey, 2011). It, therefore, calls for the consideration of a more holistic
perspective that takes cognisance of the interactions within a system, how this
impacts on the systems’ behaviour and how the future can be predicted
(Dooley, 1997; Marion and Uhl-Bien, 2001; Senge, 2006).
3.5 Chapter summary
This chapter aimed to provide an in-depth analysis on the concepts of
organisational readiness for innovation – its meaning and the factors
influencing successful innovation management. This process has helped the
researcher to expand their understanding of the readiness theory, recognise
the gap in research and identify the relevant research questions. The
construct of ‘readiness’ is discussed in the literature as pivotal in influencing
innovative behaviours and improving the success rate for organisational
innovation outcomes. However, the use and application of different theoretical
perspectives by management researchers has created conceptual ambiguity
on the meaning of readiness. In addition, there is a paucity of literature in
healthcare on the ways in which readiness impacts the innovation
management process, and how it may affect or be affected by the
90
interrelationship across the interacting contextual elements. In moving this
field of knowledge forward, the present research will seek to provide clarity on
the following issues. The first has to do with how innovation differs from
organisational change as this will change management’s perspective in
treating innovation management as mere change. The second relates to
exploring what the meaning of organisational readiness for innovation is, and
its relevance in managing organisational innovation. The third is how
readiness can be enabled and sustained in complex organisational settings
such as the public healthcare sector. The chapter concluded with the notion
that organisational readiness for innovation could be better understood
through the lens of complex adaptive systems theory to improve our
understanding on how patterns and contextual condition change over time to
influence successful innovation management. In the following chapter, the
methodological and epistemological approaches adopted to investigate this
research are discussed.
91
Chapter 4
Epistemological and methodological framework
4.1 Introduction
The research design, the definitions of the concepts and the type of evidence
collected were all influenced by the researcher’s epistemological position.
Therefore, it is useful to make this explicit. This chapter sets out to explain the
philosophical framework within which the study was undertaken. Saunders,
Lewis and Thornhill (2012) research ‘onion’ served as a guide to the
researcher in determining the stages through which the research must pass
when formulating an effective methodology. The benefit of the research onion
is that it creates a sequence of stages through which different methods of
data collection can be understood and the study methodological steps can be
described. Thus, the first section concentrates on the research questions
being addressed and how the researcher’s epistemological position informed
and influenced the choice and development of the research strategy. This is
followed by a more detailed discussion of the research methodologies
adopted, that is, the research strategy, the data collection method with the
time horizon for data collection, and the criteria used to assess rigour
particularly in relation to the qualitative approach used.
4.2 The researcher’s epistemological position
As stated earlier, the aim of the research is to provide conceptual clarity on
the meaning of organisational readiness for innovation and the factors that
might influence an organisation’s decision-making when contemplating the
possibility of enacting readiness. This is necessary in order to provide a
descriptive account and lay the groundwork for future research. In
approaching this task, the researcher adopted an exploratory socially
construction approach. The social constructionist philosophy approach is
92

particularly useful in capturing complex and dynamic social phenomena that
are content, context and time dependent and answers the research questions.
Research philosophy represents a worldview that defines the entire
framework of beliefs, values and methods within which the research takes
place, the researcher's place in it, and the range of possible relationships to
that world and its parts (Guba and Lincoln, 1994; Joubish et al., 2011). The
research philosophy paradigm framework is made up of ontology,
epistemology and methodology assumptions (Guba and Lincoln, 1994;
Saunders, Lewis and Thornhill, 2012). These assumptions are deeply
connected to each other as the outlook of ontology (reality) affects the
epistemology (knowledge) which has an effect on the view of human nature,
and ultimately, the methodology applied in the study (Holden and Lynch,
2004).
Creswell (2013) asserts that research philosophy influences the practice of
research. It is a strong deciding factor in the development and refinement of
research methods and the strategy to be employed and their suitability to
research needs. This chosen strategy may be dependent on the context of the
study and the nature of the research questions being asked (Crossan, 2003;
Holden and Lynch, 2004; Saunders, Lewis and Thornhill, 2012). The
researcher’s experience, understanding of philosophy and personal beliefs
may also have an effect on the method adopted (Denzin and Lincoln, 1998;
Creswell, 2013). Holden and Lynch (2004) explain that another advantage of
having knowledge and a good understanding of research philosophy is the
person’s ability to identify the appropriateness and limitations of particular
approaches at an early stage, thus preventing inappropriate use while
maximising the use of available resources and enhancing confidence in the
research results.
The ultimate veracity of any research philosophy cannot be established
because it is the tacit set of basic beliefs that the researchers have been able
to devise, considering the way they have chosen to respond to the
ontological, epistemological and methodological questions. Therefore, they
cannot be proven in a conventional or explicit way and have to be accepted
93

based on certain principles (Guba and Lincoln, 1994; Easterby-Smith, Thorpe
and Jackson, 2015).
A constructionist philosophy was adopted in this study. Constructionism is
closely related to an interpretivist paradigm and is a naturalistic approach to
research (Rubin and Rubin, 2011; Saunders, Lewis and Thornhill, 2012). This
philosophy asserts that reality is socially constructed and knowledge occurs
as a result of our social practices and institutions or the interactions between
social groups. This construction of reality is an active process and individuals
acting together in large and small groups, influenced by history, culture, and
other broad factors, construct the world in which they engage (Young and
Collin, 2004; Rubin and Rubin, 2011; Saunders, Lewis and Thornhill, 2012).
Social actors have various interpretations of the situations they are placed in
because individuals will use their view of the world and interaction with their
environment to observe and understand situations, and then draw
interpretations from them. These interpretations influence their actions and
their social interaction with others. This means that knowledge is supported by
social processes and that knowledge and social action go together (Gasper,
1999; Young and Collin, 2004; Saunders, Lewis and Thornhill, 2012).
Therefore, knowledge and reality are social products that are incapable of
being understood independently of the social actors that construct and make
sense of that reality (Chen, Shek and Bu, 2011).
This implies that knowledge of the world cannot be determined directly, but by
the construction imposed on it by the mind, social interactions, culture, history
and ideology, so there is no absolute knowledge or truth, but interpreted
meanings and different knowledges and truths (Chen, Shek and Bu, 2011;
Rubin and Rubin, 2011). Furthermore, knowledge prevails not because of the
dependence on the authenticity of the viewpoint that is being examined, but
on the changes in social actions like negotiations, communication and conflict
(Gergen, 1985; Gergen, 1987).
The constructionist philosophy assumes relativist ontology, a subjectivist
epistemology, and a naturalistic and qualitative set of methodological
94

procedures. That is, it assumes that there are multiple realities where the
knower and the respondents create understanding together and this occurs in
the natural world and not in an experimental or controlled setting (Guba and
Lincoln, 1994; Denzin and Lincoln, 1998; Chen, Shek and Bu, 2011).
Ontologically, constructionism assumes a relativist stance. This means that
there are diverse interpretations of reality and the only accessible things are
our different representations of the world and none of them is truer than the
other. An objective reality is not possible for human beings because of the
intentionality of perception and the subjective interpretations of humans (Guba
and Lincoln, 1994; Chen, Shek and Bu, 2011). Therefore, there are multiple
and equally meaningful realities that depend on the individual’s constructions
because reality is constructed by social, cultural and historical factors, rather
than being a stable and constant single truth. So, meanings are formed,
transferred, used, and negotiated, and, hence, those interpretations of reality
may shift over time as circumstances and constituents change (Orlikowski
and Baroudi, 1991; Guba and Lincoln, 1994; Chen, Shek and Bu, 2011).
The constructionist philosophy is premised on the subjectivist epistemological
belief. This focuses on the social interactions between the researcher and the
research subjects and assumes that discoveries are made and revised as the
study proceeds (Guba and Lincoln, 1994; Chen, Shek and Bu, 2011;
Saunders, Lewis and Thornhill, 2012). According to Boland (1979), this
means that individuals behave towards things on the basis of the meanings
that things have for them, and that these meanings arise due to social
interactions and are developed and modified through an interpretive process.
Therefore, social process is not captured and understood by hypothetical
deductions, but involves getting inside the world of those generating it, and
understanding “how practices and meanings are formed and informed by the
language shared by people working towards a shared goal” (Orlikowski and
Baroudi, 1991, p. 14).
The methodological approaches, which are most appropriate for the
constructionist research philosophy are naturalistic inquiry and qualitative
research methods (Burrell and Morgan, 1979; Rubin and Rubin, 2011).
95

Creswell (2013) explains further that the researcher uses a narrative design
and open-ended interviewing to collect data to further the research objectives
and avoids imposing external categories on a phenomenon. The criteria for
this philosophy to be successfully adopted are trustworthiness, soundness,
credibility, transferability, readiness, accountability and confirmability. It is also
characterised by a standpoint theory, interpretive records and ethnographic
descriptions (Denzin and Lincoln, 1998; Chen, Shek and Bu, 2011).
During the research process, the researcher adopts an attitude of reflexivity
and avoids measuring and identifying findings with a well-defined set of
constructs, but strives to obtain constructs from the field by a thorough
examination and exposure to the phenomenon of interest (Orlikowski and
Baroudi, 1991; Chen, Shek and Bu, 2011). This means that the researcher
gains new knowledge about the world of the participant without bias,
predilection or a fixed mind-set.
The contribution of constructionism towards this research is that it exposes
the connections which underlie the different parts of social reality by
examining the social rules and meanings that make social practices possible.
Therefore, social relations and the interactive nature of human behaviour that
revolve around shared meanings, interpretations and construction of a cultural
and social reality are observed and analysed (Gibbons, 1987; Orlikowski and
Baroudi, 1991).
4.3 The research design
Qualitative and quantitative methods are used in data collection – depending
on the analytical situation and the nature of the research question (Britten et
al., 1995; Mays and Pope, 1995; Lee, Mitchell and Sablynski, 1999; Corbin
and Strauss, 2008; Saunders, Lewis and Thornhill, 2012). In approaching a
misconstrued research area, the researcher was faced with where to begin,
and how to develop understanding in a way that is rigorous and credible. In
addressing this problem, it was decided that a qualitative approach would be
most useful in facilitating a more elaborate understanding of the responses of
individuals to the notion of organisational readiness for innovation.
96

The qualitative research method is typically effective in answering research
questions such as: “What is X?” “How does X occur?” “How does X vary in
different circumstances and why?” This is in contrast to “How many Xs are
there?” as the qualitative method does not generally seek to enumerate (Pope
and Mays, 1995, p. 43). The qualitative research method is well suited for
exploratory purposes, that is, when an existing theory is underdeveloped,
poorly understood or ill-defined (Britten et al., 1995). In such instances,
quantitative research is hampered because a hypothesis cannot be passably
constructed in advance (Britten et al., 1995). Qualitative research methods
are needed in order to identify what are the issues, to give interpretations of
meanings, and to generate rich and detailed descriptions of the subject area
(Braun and Clarke, 2013). These characteristics make the qualitative research
methodology well suited for this research.
Broadly defined, qualitative research is any kind of research that uses words
as numbers in comparison to quantitative research that uses number as data
(Braun and Clarke, 2013). The goal of qualitative research is to develop
concepts which help in the understanding of social phenomenon in natural
settings rather than in experimental or controlled settings, and to interpret the
subjective meanings, views and experiences of the individuals and groups
involved (Britten et al., 1995; Mays and Pope, 1995; Pope, van Royen and
Baker, 2002). Typically, qualitative research focuses on understanding the
opinions of those being researched rather than the researcher’s opinions
(Britten et al., 1995). It captures the complexity and contradictions that
characterise the real world, yet allows the researcher to make sense of the
patterns of meanings (Braun and Clarke, 2013). Qualitative research
approaches provide an exploratory and flexible way for data gathering that
allows the researcher to gain a deeper understanding of a particular issue
which cannot be obtained using quantitative research (Braun and Clarke,
2013). The use of qualitative research methods tends to augment the
researcher’s peripheral vision which is central at the preliminary stage of
investigation, and thus, helps to move inquiry toward narrower and definite
questions (Sofaer, 1999).
97

Qualitative research is increasingly common in health services research
(Shortell, 1999; Sofaer, 1999; Mays and Pope, 2000). There is a claim that
health services researchers tend to borrow theories from other disciplines and
have done little to develop their own comprehensive and independent theories
(Sofaer, 1999). This has resulted in the challenge of trying to apply evidence-
based medicine in everyday clinical practice (Shortell, 1999). Given the
complexity of healthcare systems, it cannot be solely understood by simply
monitoring quantitative measures and indicators. Understanding the
perspectives of multiple stakeholders and their experiences is crucial to
understanding the complex and dynamic nature of healthcare systems and
ways to improve whole-systems change (Sofaer, 1999). Qualitative research
offers a number of ways for identifying barriers to improving performances by
explaining why performance does or does not occur (Pope, van Royen and
Baker, 2002). The use of such methods could lead to a better understanding
of how to improve organisational innovation performances (Pope, van Royen
and Baker, 2002). A qualitative research design is, therefore, most suitable
for answering the research questions of this thesis.
4.4 Qualitative data collection
The choice of a data collection method is usually determined by the research
questions, the objectives and the design (Saunders, Lewis and Thornhill,
2012). For this study, the face-to-face, semi-structured interview was the
preferred choice for data collection. This method was chosen for its
appropriateness for the research questions, the analytical situation and the
overall design (Lee, Mitchell and Sablynski, 1999). The use of interviews
enabled the researcher to get closer to the interviewees’ perspective and
capture rich descriptions of phenomenon from their point of view, therefore,
gaining access to aspects of information that would not be accessible with
other methods of data collection (Britten et al., 1995; DiCicco‐Bloom and
Crabtree, 2006; Rowley, 2012a; Saunders, Lewis and Thornhill, 2012). This
research is an exploratory study where the use of ‘prompts’ and ‘probes’ to
expand on participants’ responses was of great importance and so semi-
98

structured interview was the choice for data collection (Qu and Dumay, 2011;
Saunders, Lewis and Thornhill, 2012; Braun and Clarke, 2013).
Semi-structured interviewing is the most common type of interview in
qualitative research and is usually the choice for data collection when the
researcher’s intention is to gather retrospective and real-time reports by
people experiencing the phenomenon of theoretical interest (DiCicco‐Bloom
and Crabtree, 2006; Rowley, 2012a; Gioia, Corley and Hamilton, 2013). With
semi-structured interviewing, the interviewer develops an interview schedule
or guide (see Appendices B & C) that outlines a list of well-phrased and
carefully selected questions to be delivered in a set order. Still, it permits the
flexibility to deviate from a set of questions in order to delve more deeply into
pertinent viewpoints and issues that were not anticipated by the interviewer at
the outset of the research (Britten et al., 1995; Pope, van Royen and Baker,
2002; DiCicco‐Bloom and Crabtree, 2006; Rowley, 2012a; Saunders, Lewis
and Thornhill, 2012). Similarly, the interviewer may decide to exclude or add
some questions to a particular interview, depending on the context of that
specific interview. The order of questions in a semi-structured interview may
also vary, depending on the flow of the conversation (Saunders, Lewis and
Thornhill, 2012).
Moreover, semi-structured interviews provide the researcher with the
opportunity to probe answers where it is necessary for the interviewees to
explain or elaborate on their responses. It also becomes a relevant choice of
data collection if an epistemological approach is being taken where
understanding meanings and the phenomena of the participants are of
importance (Saunders, Lewis and Thornhill, 2012). The use of a qualitative
method enables open-ended questions which often result in a level of
disclosure that would be unusual in a structured interview (Britten., 1995;
Saunders, Lewis and Thornhill, 2012). Open-ended questions are preferred
as they encourage participants to provide in-depth and detailed responses
and to discuss what is important to them (Braun and Clarke, 2013).
As earlier stated, the goal of a qualitative interview is to capture the array and
diversity of participants’ responses in their own words (Saunders, Lewis and
99

Thornhill, 2012; Braun and Clarke, 2013). Therefore, the interviews for this
study were audio-recorded with the interviewees’ permission. Potential
participants were presented with the participant information sheet (see
Appendix D) before consenting to take part in the study. This was important
so they would understand that their interview would be audio-recorded (Braun
and Clarke, 2013). The use of audio-recording played an active role during
data gathering as it allowed the researcher to focus on the topic of discussion,
to listen more and have greater control in terms of directing the questions
(Kvale and Brinkmann, 2009; Saunders, Lewis and Thornhill, 2012). Making
audio-recordings also made it easier for the researcher to become familiar
with the data and engage more deeply with its context (Bryman, 2012).
Another benefit of the audio-records was that it allowed verification of the
findings by using extracts from interviews and it enabled coherence in writing
up the result (Saunders, Lewis and Thornhill, 2012).
4.4.1 The sampling strategy
As this study aimed to explore the opinions and insights of managerial
leadership on the conceptualisation of organisational readiness for innovation,
the following two major stakeholder groups were selected:
Chief Executive Officers and
Managing Directors (Members of the board – e.g., General Managers,
Directors, Non-executive director, and Chairman),
These groups were selected because of their role in leading health
improvement in their organisations and the wider society. They were chosen
to represent a diverse range of managerial views on leading and managing
organisational innovation. The choice was supported by the literature which
recognises that leadership is a sense-making process that requires leaders to
make meaning from retrospective and ongoing events in order to lead (Pye,
2005). This approach allowed the researcher to probe further below the
surface of the topic in order to gain deeper insights and richer information.
The choice of non-probability sampling was justified given that this study
sought to explore the meanings and enactment of readiness from the
100

perspective of the healthcare stakeholders and not to measure outcomes or
gain a statistical generation of data (Saunders, Lewis and Thornhill, 2012).
Apart from this, qualitative research is time-consuming and expensive, and it
is not practicable to use probability sampling (Mays and Pope, 1995). The
studies conducted within this thesis used the non-probability purposive
sampling strategy. In qualitative studies, the typical approach to sampling is
purposive with the objective of generating insightful and comprehensive
knowledge (Pope, van Royen and Baker, 2002; Braun and Clarke, 2013). One
objective of purposive sampling is that it allows the researcher to be
intentional during the recruitment phase, selecting key persons based on their
unique characteristics and ability to provide rich and detailed information on
the subject being explored (Mays and Pope, 1995; Pope, van Royen and
Baker, 2002; DiCicco-Bloom and Cranbtree, 2006; Saunders, Lewis and
Thornhill, 2012; Braun and Clarke, 2013).
As this is a qualitative research, the sample data did not seek to obtain
statistical representativeness of all the cases from which the samples were
selected; rather, it sought to pursure the theoretical lines of enquiry
(Saunders, Lewis and Thornhill, 2012). The empirical studies within this
thesis, therefore, focused on a relatively small number of participants selected
for a specific purpose in order to obtain an information-rich case study in
which the research questions were explored in depth in order to gain
theoretical insights.
Typically, qualitative research focuses less on sample size in comparison to
quantitative studies. Instead, the focus is on sampling adequacy – which
means the sample must be suitable, comprising of participants who have the
expertise on the subject being explored. This ensures optimum quality of the
data and minimum dross (Morse et al., 2002). Qualitative researchers advise
continuous sampling and data analysis until no new categories or themes
appear and all ideas in the theory are well developed. This is otherwise known
as theoretical saturation (Lee, Mitchell and Sablynski, 1999; Morse et al.,
2002; DiCicco-Bloom and Crabtree, 2006; Saunders, Lewis and Thornhill,
2012). At this point, “ideas emerging from the data are re-confirmed in new
101

data, giving rise to new ideas that must be validated in previously collected
data” (Morse et al., 2002, p. 18). However, Guest, Bunce and Johnson (2006)
provide some guidelines on the minimum non-probability sample size,
explaining that twelve in-depth interviews should suffice within a fairly
homogenous group. In contrast, they note that twelve interviews are unlikely
to be enough to reach data saturation in a heterogenous group. Given this
factor, twenty interviews were undertaken and considered appropriate.
4.4.2 Participants recruitment
Involving stakeholders at the managerial level was a key tenet of this study.
Interviews were conducted with 20 participants in total. The participants were
recruited through networking and the snowballing process (Saunders, Lewis
and Thornhill, 2012). Three out of the twenty participants were strongly
recommended by the researcher’s supervisors. These three participants were
then asked to recommend other colleagues and associates. The remaining
fifteen participants were identified by the researcher after reading their profiles
on the organisation’s portal. This was done to ensure that the ‘ideal’ research
candidates were targeted, that is, persons who were innovative with highly
developed expertise in leadership and who showed continuous improvement
in their leadership approach.
The rationale for the choice of the organisations from which participants were
recruited was influenced by commendation, organisation’s function, and
location. The names of the organisation were not specified in order to
maintain anonymity and confidentiality. Instead, the name of the organisation
was represented by its region of location. In the first set of data collection,
participants consisted of ten individuals from three different organisations
namely: a Clinical Commissioning Group (CCG) in southeast of England; an
NHS Trust in east London; and an NHS body responsible for regulating
aspects of care in south London. The recruitment for two of the participants
was based on supervisor’s recommendation. These participants were senior
managers in a CCG in south east of England, and an NHS Trust in east
London respectively. This led the researcher to seek to recruit other
individuals from within the specific CCG and NHS Trust. In total one
102

participant was recruited from the CCG, and five participants from the NHS
Trust (see Table 5.2 in Chapter Five). To gain distinct perspectives and
contribute uniqueness to the quality of data, the researcher decided to
approach another organisation that formed part of the NHS. The rationale for
the choice of this organisation was due to their role in helping to deliver NHS
England’s priorities for sustainable improvement (see Chapter Five for its
unique characteristic). From this organisation four participants were recruited.
This makes the total of ten participants for the first set of empirical study (as
seen in Chapter Five).
The rationale for the selection of the organisations from which to recruit
participants was also influenced by their location. The researcher worked from
London and Surrey, thus, it was sensible to select organisations within close
proximity in order to minimise the cost incurred from long-distance journey
and to control, to a certain degree, the amount of travel time to the
participants’ organisations. Thus, to achieve the overall aim for the second
phase of the research, the researcher sought for individuals within the
Academic Health Science Networks (AHSNs). This consisted of three AHSNs
organisations in total – two were based in London, and one based in the south
east of England. Notwithstanding, it was important that each of the
organisations from which participants were recruited brought unique and
distinctive capabilities to the wider collaboration in public healthcare sector,
and, through partnership, they were making an impact on the wider population
(see Chapter 5 and Chapter 6 respectively for characteristics of the
organisations from which participants were recruited).
On identification of a suitable participant, a brief email about the study was
sent them (see Appendix E). Respondents who wished to participate were
then presented with a participant information sheet which consisted of the
details of the research project, namely, its purpose, the degree of
participation required, information on data protection, confidentiality and
anonymity, data storage and dissemination, and contact details for futher
information and how to file a complaint (if necessary). After this, a date, time
and location for intereviews were agreed upon. Recruitment of participants
103

within this study was an arduous process. This was as a result of the
cancellation of appointments upon short-notice and the long-distance to be
travelled to reach the participants’ location. In addition, there was the
extremely difficult task of having to constantly request and remind personal
assistants and secretaries to set up the research appointment and look for
alternate dates due to the participant’s busy diary. Finally, recruitment lasted
longer than originally expected. Approximately 12 months were spent in
completing the interviewing process.
4.5 The analytic process
The purpose of qualitative analysis is to gain a deeper understanding of the
gathered data by looking beneath the surface of the data with the aim of trying
to understand the meaning of the accounts given during the interview and to
provide a conceptual explanation and some sort of theoretical implication
(Braun and Clarke, 2013). There are many different methods of qualitative
analysis, but some are more commonly adopted in health services research.
In this study, a thematic analysis approach was adopted as it is possibly one
of the most widely used qualitative methods of data analysis, yet it has
received less support than other traditional methods of analysis.
Researchers (Attride-Stirling, 2001; Dixon-Woods et al., 2005) argued that
thematic analysis suffers from a paucity of methodological direction and clarity
of process. However, Braun and Clarke (2006) have decided that thematic
analysis is a specific method. Within this study, comparative thematic analysis
is applied. Thematic analysis entails the identification of themes and a
rigorous coding process that aims to capture data according to the themes
that are discussed, rather than essentially trying to develop a novel theory to
describe the findings (Ryan and Bernad, 2000). One of the advantages of
thematic analysis is its theoretical flexibility which enables researchers to use
different information types in a systematic manner, thus, making it useful for
synthesising data from different sources (Boyatzis, 1998).
Within this study, thematic analysis was favoured because it is less
dependent on theoretical saturation and more on data availability (Cho and
104
Lee, 2014). Consequently, the anticipation of the length of the research period
becomes less challenging. Additionally, thematic analysis does not require the
meticulous theoretical expertise of grounded theory which makes it more
accessible and not grounded in any pre-existing theoretical framework.
Therefore, thematic analysis can be used to do different things within any
epistemological position (Boyatzis, 1998; Braun and Clarke, 2006). For
example, within this thesis, thematic analysis is used as a constructionist
method to “explore the ways in which meanings, realities, events, experiences
and so on are the effects of a range of discourses operating within a social
context” (Braun and Clarke, 2006, p. 81). This, in turn, also explores the way
the broader social context impinges on those meanings to sustain
organisational readiness for innovation. Thematic analysis can be defined as
the search for common themes that emerge across a dataset in relation to the
research question(s), allowing a level of patterned meaning within the dataset
(Daly, Kellehear and Gliksman, 1997; Braun and Clarke, 2006; Braun and
Clarke, 2013). The emerging themes then become the categories for analysis
(Fereday and Muir-Cochrane, 2006).
The process of thematic analysis within this study began with the researcher
becoming familiar with the dataset through careful line-by-line analysis and re-
analysis and writing down the initial concepts (Rice and Ezzy, 1999; Braun
and Clarke, 2006). This initial stage of data familiarisation was vital as it
enabled the researcher to become immersed in the data, identify patterns,
comprehend meanings in their entirety, and get an overview of the likely depth
and breadth of the information (Aronson, 1995; Pope and Mays, 1995; Braun
and Clarke, 2006; Bradley, Curry and Devers, 2007). During this step, the
researcher manually created memos and noted recurring themes within the
data as well as personal thoughts about what was going on in the text. Memo
writing is a key tool used for identifying and building core relationships across
datasets (Strauss and Corbin, 1990) as it helps the researcher to refine and
keep track of ideas and important discussions and issues that may emerge
during data collection (Bowen, 2008; Cho and Lee, 2014).
The next stage was that of coding which involves identifying and highlighting
105

key concepts that illustrate the concept studied (Ryan and Bernard 2000;
Braun and Clarke, 2006; Fereday and Muir-Cochrane, 2006; Bradley, Curry
and Devers, 2007). It provided the researcher with a formal system for
organising data and for identifying and documenting links within and between
views discussed in the data (Bradley, Curry and Devers, 2007). Codes are
tags ascribed to the data set to help catalogue the key concepts described
while preserving the contexts in which these concepts are described (Miles
and Huberman, 1994).
Coding can be done in an inductive (bottom-up approach and data driven) or
deductive (theoretical thematic analysis) manner (Braun and Clarke, 2006;
Bradley, Curry and Devers, 2007). In this research, data analysis was
conducted in an inductive way, using the constant comparative method of
grounded theory (Glaser and Strauss, 1967; Strauss and Corbin, 1990). The
process of coding began with ‘open coding’ also known as ‘first-order
analysis’, and this was done manually. Manual analysis was chosen because
it compels the researcher to focus on depth and meaning and involves the
researcher more personally with the data, unlike what happens when software
programmes are used (John and Johnson, 2000; Kodish and Gittelsohn,
2011). The researcher worked through the dataset systematically, using
highlighters to indicate potential patterns, identify thought-provoking aspects,
and to write notes on the texts. During the inductive coding, efforts were made
not to force a pre-concerived idea on the interpretation of the data (Bradley,
Curry and Devers, 2007). However, in this first-order analysis, the researcher
adhered faithfully to the interviewee terms (see Table 5.3). At this stage, the
task became overwhelming due to many categories exploding at the front end
of this study.
The researcher then began to seek for similarities and differences among the
many categories similar to Glaser and Strauss’s constant comparison method
(Gioia, Corley and Hamilton, 2013). Constant comparison was done within a
single interview, followed by between interview transcripts, until no new
categories were identiifed (Pope and Mays, 1995; Bradley, Curry and Devers,
2007; Bowen, 2008). As segments of texts were compared and contrasted,
106

Corbin and Strauss (2008) questioning criteria were used to help the
researcher to uncover relationships among categories by answering these
questions “What are the characteristics of the code? Under what conditions
are these codes used? How is the code similar to or different from preceding
code?” This questioning technique enabled the researcher to essentially
generate linkages that went from analysis to interpretation (Scott, 2004). The
researcher scrutinised and compared data with data and these with codes in
order to organise and identify concepts that did not seem to cluster together.
This back and forth interplay was constantly done with the data until all
relevants concepts were identified and coded (Bowen, 2008). A common
criticism with coding is the loss of context, hence, the researcher took care to
code interviews extracts inclusively, which means to keep out little of the
relevant surrounding data (Braun and Clarke, 2006). The process of constant
comparison also included a continuous search for negative cases or
discomforming views (Ryan and Bernard, 2000; Morse et al., 2002; Bradley,
Curry and Devers, 2007; Bowen, 2008; Corbin and Strauss, 2008). Negative
cases can disconfirm parts of a model or indicate that new connections need
to be made. The search for negative cases cannot be ignored as they help the
researcher to re-conceptualise the themes and categories (Ely et al., 1991;
Gioia, Corley and Hamilton, 2013).
On the development and collation of the first-order concepts, the researcher
began to search for themes across the datasets. This phase is the second
level of coding and analysis known as thematic coding or second-order theme
which involves the sorting of the potential codes into potential themes and
collating the coded data extracts within the identified themes. The researcher
began to analyse the codes and considered how each code may be combined
to form a theme. Once a theme was developed and theoertical saturation was
reached, the researcher further distilled the emerging second-order themes
into second-order “aggregate dimensions.” According to Gioia, Corley and
Hamilton (2013), developing first-order and second-order themes and second-
order aggregate dimensions are necessary in order to build a data structure.
Using a data structure is a pivotal step which allows the researcher to
organise the data into a sensible visual aid and provide a graphical
107

demonstration of how the raw data was processed to form themes (Gioia,
Corley and Hamilton, 2013). They further explained that the use of a data
sturcture compels a researcher to step up in “thinking about the data
theoretically, and not just methodologically” (p.21). A data structure is
generally used to demonstrate an overall conceptualisation of the data
pattens and the nature of the interconnections between them (Ryan and
Bernard, 2000; Attride-Stirling, 2001; Scott, 2004; Braun and Clarke, 2006).
Data structure maps also provide an effective way for researcher to “fragment
texts and finding within it explicit rationalisations and their implicit signification”
(Attride-Stirling, 2001, p. 388). Since coding was an on-going process, the
data structure was considered each time to ensure that it reflected the
meanings evident in the data set as a whole. Most importantly, the data
structure served only as a tool and not the analysis itself (see Table 5.3).
As the process of coding continued, the researcher reviewed the themes
developed. The researcher read and re-read all the collated extracts/code for
the themes to consider if they appeared to form a coherent pattern. At this
stage, some themes needed to be collapsed into a single one while others
that did not fit were either re-analysed or discarded. In addition, the validity of
individual themes was considered in relation to the data set and any additional
data within the themes that had been missed out was coded. At the end of
this phase, the researcher had developed different themes and showed how
they all fit together on the thematic map. One criticism of thematic analysis is
that the generating of themes can go on ‘ad infinitum,’ hence the researcher
stopped the process of coding and developing themes when refining and re-
coding only served to make the coding frame more nuanced (Braun and
Clarke, 2006).
On developing a satisfactory thematic structure of concepts, themes were
defined and refined (Braun and Clarke, 2006). The themes were then
compared in relation to the research questions to ensure there was no
overlap. Each theme was also considered in relation to itself and to other
themes in order to identify if a theme should contain a sub-theme. A narrative
discussion of the analysis finding was then written as seen in the subsequent
108

chapters.
4.6 Demonstrating rigor
The trustworthiness of qualitative studies has generally been debated,
perhaps, because their concept of reliability and validity is difficult to judge in
the same way as its quantitative counterpart (Morse et al., 2002; Pope, van
Royen and Baker, 2002; Shenton, 2004). It has been argued that because the
nature and purpose of qualitative and quantitative research are different, it is
inaccurate to apply the same measures of merit (Krefting, 1991). For instance,
external validity, which is a key criterion in quantitative study and produces
generalisation from research sample to the population (Saunders, Lewis and
Thornhill, 2012), is not relevant in qualitative studies (Krefting, 1991). This is
so because the main purpose of qualitative study is often to generate
hypotheses for further investigation rather than to test them (Britten et al.,
1995; Mays and Pope, 1995; Saunders, Lewis and Thornhill, 2012). To
evaluate this study, the trustworthiness of the data was established based
upon Denzin and Lincoln’s (1998) trustworthiness criteria that include
credibility and transferability.
4.6.1 Credibility
Credibility is defined as the degree to which data and findings from data
analysis are believable (Ritchie and Lewis, 2003). It is equivalent to that of
internal validity used by quantitative researchers in seeking to ensure that
their study measure is actually what is intended, in other words, the reality
(Shenton, 2004). From the qualitative researcher’s perspective, a study is
credible if the descriptions or meanings shared are ‘congruent with the reality’
(Sandelowski, 1986). From a social constructivist perspective, the reality is
co-created and cannot be compared to an objective reality. However, the
selection of participants from two different organisations led to a diversification
of views which is necessary to provide a view of reality (Denzin, 1970). This
also helped to minimise any biases that might have been introduced by
participants in one particular location. Credibility was also increased in this
study through peer debriefing which involved holding group discussions with
109

independent colleagues who had experience in the use of qualitative methods
(Erlandson, 1993; Creswell, 1998; Merriam and Tisdell, 2015). The use of
data structure in the analyses also increased the credibility of the study (Gioia,
Corley and Hamilton, 2013).
Additionally, as already mentioned in the previous section, deviant and
disconfirming cases were continuously searched for, examined and explained
in order to increase data reliability and validity and to confirm credibility
(Britten et al., 1995; Mays and Pope, 1995; Creswell, 1998). Credibility was
also enhanced through the critical assessment of the participants’ verbatim
accounts with the researcher paying attention to key non-verbal cues
sometimes displayed and the statements made (Ely et al., 1991; Krefting,
1991).
4.6.2 Transferability
Transferability is concerned with the extent to which the findings of a study is
generalisable or applicable to different contexts (Merriam, 1998). In
quantitative research, the findings can be generalised to a wider population. In
contrast, the subjectivity and small number of sample sizes in qualitative study
presents a challenge with generalisation (Shenton, 2004). To improve the
transferability of results, authors recommend the need for researchers to
communicate the boundaries of the study and to describe its context (Mays
and Pope, 1995; Shenton, 2004). This helps to illustrate how the study
contributes to and fits in with other empirical works and contexts. Therefore,
within this study, a full and clear account of the data collection methods
employed and of the analysis were provided, including, the number of
organisations taking part in the study and where they were based; the number
of participants involved in the study and the criteria for inclusion was made
clear; and the number and length of time of data collection was reported. This
method was systematic and consistently followed which allows others to judge
the evidence and interpretations presented. A clear account of the method
provided within this chapter also allows for other researchers to judge the
transferability of findings within their local contexts (Pope, van Royen and
Baker, 2002).
110

4.7 Ethical considerations
Saunders, Lewis and Thornhill (2012) refer to ethics as the standards of
behaviour that guide research conduct in relation to the rights of the
participants. A number of ethical issues was considered in relation to
choosing and formulating the research questions, data collection, storing and
analysing the data and writing up and reporting the findings. At the start of the
study, ethical clearance was obtained from the University of Surrey. The
University of Surrey Ethics Committee gave a favourable opinion for the
research with reference number (see Appendix F). The preliminary study
also received favourable ethical consideration from the Research and
Development Department of the NHS Trust in East London. On obtaining
ethical approval, the factors below were considered.
4.7.1 Voluntary participation and Informed consent
Obtaining informed consent is obligatory for all research that involves
recognisable subjects (Richards and Schwartz, 2002). Prior to the interview,
participants were sent the details of the study being conducted including the
study purpose and nature, duration of the interview, contact details for
supervisors and head of school, potential risks and benefits of their
participation. The participants were also informed about the researcher’s right
to publishing the data and possible access to the data analysis. Additionally,
participants were informed that their participation was voluntary and they had
the right to withdraw their data at any stage. Apart from this, participants were
asked to sign a consent form before the interview proceeded (see Appendix G).
4.7.2 Confidentiality and anonymity
Confidentiality and anonymity are central issues for all researchers (Britten et
al., 1995; Kvale and Brinkmann, 2009; Bryman, 2012; Bazeley, 2013). To
ensure confidentiality in this study, only the researcher handled the raw data.
In ensuring anonymity, participants’ names and organisations were assigned
a code during data transcription and analysis.
111

4.7.3 Safety of participants and researcher
This study guaranteed social responsibility and obligations to participants. In
minimising potential risks to participants, study risk assessment was
discussed with the health and safety officer within the Department of
Healthcare Management and Policy at the University of Surrey. The outcome
of the conducted risk assessment showed that the study would not cause
distress of any kind to participants. In ensuring the researcher’s safety, the
safety guidelines issued by the University of Surrey and participants’
organisations were followed – as shown in the risk assessment form (see
Appendix G).
4.8 Chapter summary
This chapter provided a comprehensive description of the research design,
context and methodology. The rationale for adopting a constructionism
research philosophy and the use of qualitative research paradigm were
explained in detail. The following were also clearly explained: the data
collection method, sampling strategy, method of data analysis, and the
rationale for selection of organisations to recruit participants along with the
process taken to recruit study participants. Finally, the procedures taken to
guarantee rigour as well as the ethical considerations concerning the study
were explained. In the subsequent chapter, the findings of this study are
presented and discussed.
112

Chapter 5
Exploring the conceptualisation of organisational readiness for innovation in the public healthcare
services delivery sector: The inner context
5.1 Study Aims
Healthcare leaders increasingly realise the potential benefits and the role of
readiness for change in building a culture of innovation in healthcare
communities (Konu and Viitanen, 2008; Robert et al., 2009; Glifford et al.,
2012; Weberg, 2012; Ham, 2014). The evidence from the systematic review
suggests that the construct of organisational readiness for innovation still
requires extensive research to fully comprehend its associated meanings,
operationalisation and enactment. Readiness is often described as a
psychological construct experienced at both the individual and the
organisational levels, but there is a lack of consistency and even controversy
regarding its conceptualisation and impact (Weiner, Amick and Lee, 2008;
Rafferty, Jimmieson and Armenakis, 2012). In line with a stage-based
approach, organisational readiness is considered a one off event change that
needs to be assessed before the implementation of an innovation commences
because it has a great impact on and determines the effectiveness of the
outcome (Prochaska et al., 2001; Weiner, Amick and Lee, 2008; Holt and
Vardaman, 2013; Shea et al., 2014).
On the contrary, other change and innovation management scholars reinforce
the idea of adopting a more process-based analysis of the concept of
readiness and they also emphasise the need for a continuous evaluation of its
state during the innovation management process (Jones, Jimmieson and
Griffiths, 2005; Todnem, 2005; Williams, 2011; Stevens, 2013). The literature
presently lacks an agreed definition of the concept as well as a detailed step-
by-step guide on how one can manage, develop, and maintain a state of
innovation readiness within healthcare service organisations (Greenhalgh et
113

al., 2005). This first empirical study aims to provide conceptual clarity on the
meaning of organisational readiness for innovation, and to identify and
describe some of the existing factors that enhance as well as inhibit its
emergence and sustainability over time.
The literature review revealed that the organisational innovation process is
comprised of a series of stages influenced by a range of contextual conditions
(Rogers, 2003; Greenhalgh et al., 2004; Wisdom et al., 2014; Amabile and
Pratt, 2016). However, innovation management is a complex process which
makes it difficult to apply the principles of simple mechanistic tools used for
organisational change management (Van de Ven et al., 2008). It is necessary
to identify the significant differences between managing organisational
readiness for innovation and that of organisational change in order to
understand how best to develop, create and sustain an innovative culture.
This will be partly achieved by revealing the similar and different
conceptualisation of innovation management and organisational change
based on the views of a number of key stakeholders on the meaning of both
constructs within the healthcare service delivery organisations.
To investigate the overall research question, opinions from managerial
leadership within the Clinical Commissioning Group, NHS Trust, and an NHS
Regulatory body were obtained. These three organisations were chosen in an
attempt to gain an overall perspective at the organisational level for managing
innovation within the NHS. Although the scope of responsibility differs across
mandate (see Figure 5.1), they each have a core function to support the
wider NHS to make transformational improvement through the implementation
of innovations. How they implement these changes is based on their contexts
and needs.
Focusing on the NHS leaders’ perspective, the purpose of the study is
threefold: firstly, to provide conceptual clarity on the meaning of innovation
and, identifying how innovation management is different from organisational
change. Secondly, it examines how different stakeholder groups within the
NHS define organisational readiness for innovation in the NHS context.
Thirdly, it seeks to identify factors that influence the process and outcomes of
114

organisational readiness for innovation and to understand how they influence
it and why (See Table 5.1 for research questions and example of interview
questions).
115
Table 5. 1: Research questions, aims and exempla interview questions
Research questions Study aims Example of interview questions
1. How do the senior managers in the NHS distinguish innovation from organisational change and why?
To provide conceptual clarity on the meaning of innovation, identifying how innovation management is different from organisational change.
What are the most significant differences between managing innovation and other forms of organisational change?
2. How do the senior managers in the NHS define organisational readiness for innovation and why does this matter in the NHS context?
To examine how different stakeholder groups define organisational readiness for innovation within the context under study (National healthcare services sector).
What does organisational readiness for innovation mean?
3. What are the perceived barriers of organisational readiness for innovation in public healthcare service organisations and how can it be overcome (facilitators)?
To identify factors that influences the process and outcomes of organisational readiness for innovation and understand how they influence it and why.
What factors may affect successful innovation management?
116

Figure 5. 1: The NHS – how providers are regulated
Source: The King’s Fund (2016)
The study was conducted across two geographical locations in the UK which
include: Guildford, a town in Surrey, and London, the capital of England. It
was carried out at three sites: a Clinical Commissioning Group in south east
of England, an NHS Trust in east London, and one of the NHS organisation
responsible for regulating aspects of care in south London. See below a
description of each organisation:
1. Clinical Commissioning Group
Commissioning is the planning and monitoring of healthcare services that
meet the population’s needs by prioritising health outcomes, procuring
products and services, and managing service providers (Powell, 2017).
Clinical Commissioning Groups (CCGs) are membership bodies made up of
GP practices that commission routine services for their local populations.
These services include urgent and emergency care services, community
health services, and maternity and mental health services (Department of
Health, 2013, NHS England, 2014; Powell, 2017).
2. NHS Trust
NHS services are delivered by organisations called providers. NHS Trusts
and foundation trusts are inclusive and responsible for delivering primary care
services. These include general practice, dentistry, optometry and pharmacy
117

services, acute care services, ambulance services, mental care services and
community health services (NHS England, 2014).
3. NHS regulatory body for quality improving – safeguarding people’s interest
This organisation is responsible for promoting improvement across the NHS
by building capability, capacity, and improving knowledge and skills. They are
also in charge of regulating the performance management and governance of
NHS Trusts and foundation trusts (The King’s Fund, 2016).
5.2 Method
5.2.1 Participants
Each participant belonged to the top hierarchy of their organisation based on
the premise that the main research question was to determine managerial
perspectives. The data in this specific study was collected from ten
participants in total - nine male and one female (9:1). The ratio of men to
women in the sample size was unintentional and was based on the
accessibility of the respondents. To preserve anonymity and confidentiality,
participants’ names were coded using terms such as chief executive and
managing directors, respectively (see Table 5.2 for demographic
characteristics of study participants).
5.2.2 The interview schedule
The interview schedule was used as a guide to ask purposeful questions. The
aim of the interview was to explore organisational readiness for the successful
management of innovation in the healthcare services sector. Due to the fact
that a semi-structured interview was used, it allowed for exclusion of some
questions in particular contexts. In this study, participants were asked the
same questions to aid comparison across the data sets and interesting
concepts were further explored using probes.
118

Table 5. 2: Demographic characteristics of participants
Participant number
Stakeholder group Type of Organisation Gender Years of service in the NHS
Rationale for choosig participant
001 Chief Executive Officer Clinical Commisionning Group
♂ 29 This participant is responsible for the CCG leadership, budgets and developing care pathways to support hospitals. With over 20 years of experience in the NHS, the participant has an in depth knowledge in improving organisational development and operations across an entire organisation.
003 Chief Executive Officer NHS Trust ♂ 30 An expert in managing large and complex healthcare environments, leading organisational turnaround and structural strategic change.
006 Chief Executive Officer NHS Trust ♂ 16 Having worked across a range of strategic and operational roles in the NHS, the participant has expertise in leading change and performance management across healthcare.
119

Table 5. 2 continued: Demographic characterisitcs of participants
Participant number
Stakeholder group Type of Organisation Location Years of service in the NHS
Rationale for choosig participant
002 Managing Director NHS Trust ♂ 7 Named in Health Service Journal as one of the top 50 innovators in healthcare. Participant has experience across research and development, service redesign, leadership, innovation and business transformation. Participant holds the role of Director of Information within an NHS Trust
009 Medical Director NHS Trust ♂ 18 With experience in delivering leadership, transforming services, building leadership and improvement and co-author of over twenty peer-reviewed papers in medical and social sciences, participant is highly proficient in innovation management.
10 Managing Director NHS Trust ♂ 20 With a strong background in strategic development, the participant is the Director of Planning and Governance in an NHS Trust.
120
Table 5. 2 continued: Demographic characterisitcs of participants
Participant number
Stakeholder group Type of Organisation Gender Years working in the NHS
Rationale for choosig participant
004 Managing Director NHS Regulatory body ♀ 15 Participant has diverse experience working at national and international levels supporting challenged Trusts, designing and delivering improvement programmes.
005 Managing Director NHS Regulatory body ♂ 11 A lead directorate in establishing Academic Health Science Networks (AHSN), participant is involved in working to create a continuous culture of innovation and improvement in patient services.
007 Managing Director NHS Regulatory body ♂ 10 With over 11 years experience in urgent and emergency care, primary and secondary care and private healthcare organisations, participant works at a national level providing bespoke solutions to NHS organisations.
008 Managing Director NHS Regulatory body ♂ 6 Participant is experienced in strategic management and supporting transformational change across healthcare trusts.
121

Generally, the interview’s (INV) length was approximately 30 minutes to one
hour and varied across each interview. For instance, INV 001 length was 48
min; INV 002 was 52 min, INV 003 was 35 min; INV 004 was 54; INV 005 was
min 60 min; INV 006 was 30 min; INV 007 was 38 min; INV 008 was 60 min;
INV 009 was 25 min; and INV 10 was 60 min. The length of interview did not
influence the quality of data gathered. In fact, the participant shared thought-
provoking views and provided noteworthy instances regarding the questions
under study, and in cases were participants pre-informed the researcher
about limited time, they ended up talking for more than half an hour. The time
during the day when interviews took place varied and most interviews were
conducted in the morning and early afternoon, either at the participant’s
organisation or at a café. This happened for all, except INV 003 whose
interview was conducted in the late afternoon precisely at 5 p.m.due to when
the participant was available and the travel time needed for the researcher to
arrive at the scheduled location.
The researcher started by asking participants about their current role and how
it related to innovation management. The aim was to gain an overview of how
innovation influenced their decision-making process and organisational
expectations. This question generated rich information as participants became
fully involved in the interview, giving real-world scenarios and explaining how
innovation helped to resolve it. They also revealed some of the complexities
underlying the management of innovation. An example is having to forgo
opportunities in order to introduce an innovation into the clinical process or the
length of time for the benefits to become apparent. Participants were then
asked to elaborate on the uniqueness of the innovation and other forms of
organisational change. Based on their responses, if innovation was seen as
being different, participants were then asked to discuss the salient conditions
for the success of innovation. The findings indicated that readiness was
associated with innovation through leadership creating the culture that
enabled organisational members space to be free. The next question
considered what it meant to be ready. Participants were then asked to discuss
the factors they considered relevant to readiness in order to elicit more
information about the enabling processes related to successful innovation.
122

Finally, the last question of the interview was aimed at determining if there
were significant differences in managing organisational readiness in the NHS
and other industries. This was done in order to arrive at conclusions and
make recommendations.
5.2.3 Data collection process
The interviews were conducted face-to-face and lasted between 30 minutes to
one hour and they took place in the participants’ workplace or sometimes in a
cafe. On the day of the interview, both researcher and interviewee signed an
informed consent form confirming anonymity and confidentiality.
At the end of each interview session, a synopsis was completed almost
immediately. This synopsis included a section on general feelings about the
interview, themes identified, and any observation that affected the
interviewee’s response. The use of interview synopses in this study helped to
stimulate deeper thinking on the part of the researcher regarding the research
questions. It also confirmed early identification of recurrent themes, and
enabled early identification of variances across data sets (Saunders, Lewis
and Thornhill, 2012). A copy of the interview synopsis was attached to each
transcript to aid with data analysis. The researcher transcribed the audio-
recordings (see Appendix I for one complete transcripts). Particular care was
taken to produce an orthographic record for all transcripts focusing on
transcribing spoken words and other sounds in the recorded data (Braun and
Clarke, 2013).
5.3 Reflections of the researcher on interview process
To provide an on-going developmental dialogue, many memos were kept. The
use of memos allowed the researcher to maintain control over the experience
as it helped in the making of useful comments raised before and after the
interviews, and in identifying problems and ways to minimise them. One of the
problems identified was the power dynamism between the researcher and the
participants. Given that the researcher was a student with no prior experience
in the field, there was a sense of the participants possessing a greater power,
123

sometimes leading to an indirect power struggle, in a few cases. This was
seen, for example, with the participants being reluctant to delve deeper when
a point was raised, or when the nature of the participant’s response restrained
the researcher from asking further about a question. Taking this matter into
consideration, in the interviews that followed, the researcher made use of
many more probing techniques to encourage more discussion by the
participants.
Each interview started with the participants being asked to define innovation
and to elaborate on how innovation differed from other forms of organisational
change. Using this line of questioning helped to resolve the agenda setting
power to which senior managers are accustomed to making them feel that
they must control the direction of the interview. Adopting this approach to
questioning not only put forward the concept about organisational innovation,
but also shifted the participants’ focus from themselves as managers.
5.4 Personal reflexivity
Reflexivity is an ongoing mutual shaping between researcher and research
(Attia and Edge, 2017). There is a need for qualitative researchers’ to be
reflexive in their research approach in order to ensure that their “findings is
not simply a result of their own perspective” (Evans et al., 2018. p, 3). It is
worth noting that some facets of the researchers identity will influence the
types of questions asked, the participant’s reply to these questions, and the
analysis of findings. The researcher motivation for embarking on this research
project is entrenched in her experience and background in the pharmaceutical
industry. The researcher was intrigued about the process of managing
healthcare innovation, how it starts and how it differs between the private
industry and the public sector. This was the starting point, to look at how the
NHS acts and reacts in the business world and in particular, around
innovation management. The researcher had little prior knowledge on the
subject of enquiry and on NHS context. Throughout the period of her studies
the researcher kept an interview diary to note down her feelings, assumptions,
and interpretations of context. These deliberations enabled the researcher to
reflect on her preconceived ideas on the topic gained from the literature
124

review, and where possible and applicable, provide important insights to the
ongoing interviews. The researcher worked closely with her supervisors to
make explicit her feelings, and beliefs in order to better understand the
participants’ perspectives. To achieve inter-coder reliability, her supervisors
also analysed a subsample of the interviews, and then jointly the elicited
themes were discussed – which has increased rigour and provided the
researcher with more confidence in the analysis.
5.5 Results
The results from the analysis revealed many themes which were later divided
into three main master themes, each exploring one of the four pre-stated
objectives. Within each theme, a number of sub-themes were identified which
will be discussed in detail below. It should be noted that although the master
themes are presented separately, they are interrelated. Extracts are included
to support each of the four themes presented here. They are:
1. Different or same concepts? Accounting for differences in the
management of innovation and organisational change
2. Defining organisational readiness for innovation in a healthcare context
3. Enablers of organisational innovation state of readiness
5.5.1 Different or same concepts? Accounting for differences in the management of innovation and organisational change
Under this first broad theme, participants discussed their views on how the
concepts of innovation and organisational change differed in terms of a fixed
or iterative process, and their impact and level of complexity. Their responses
were grouped in subthemes each representing a key dimension as follows.
1. Process vs. Impact
2. Degree of complexity, structure and impact
(see Table 5.3 below for a breakdown of the 1st order concepts, 2nd order
themes and aggregate dimensions).
125
Table 5. 3: Themes and sub-themes on the differences in the management of innovation and organisational change 1st Order Concepts 2nd Order Themes Aggregate Dimensions
“Innovation is an attitude towards continuous improvement” (003/44)
“Change is just shuffling the decks of card” (007/86)
“Innovation people have to have motivation” (007/87)
“Organisational change is more of a management thing” (10/181)
“Innovation must give an additional benefit” (001/66)
“The two go hand in hand” (001/179)
Continuous Process/ Fixed but Open minded Attitude
Vs.
Outcome
Process
Vs.
Outcome
“Innovation is some sort of nebulous thing” (001/108)
“Organisational change is quite straightforward” (002/143)
With innovation there is no structure involved (007/101)
“Organisational change is straightforward” (002/143)
“No one has ever invented an organisational change I can call innovative” (005/209)
“Organisational change does not affect the outside world” (005/198)
Complex
Vs.
Impact
Degree of Complexity, Structure and Impact
126

1. Process Vs. Outcome
For this first theme, participants made a clear temporal and procedural
distinction between the concepts of innovation and organisational change. For
some of the participants, the notion of innovation is an “iterative” phenomenon
that evolves over time. Participants continued to describe innovation as
behavioural, being radically open-minded to new ideas, accepting that things
change and with one being ready to adapt accordingly.
Innovation is very much an iterative process, just constantly changing in a business environment.
(Managing Director – NHS Regulatory body, *007/91-92)*Indicates that text is taken from interview 7, line 91-92
I don't regard innovation as a process. I think innovation is something you are always constantly looking at, new ideas, new ways of working and keeping your mind open and your organisation's mind open and encouraging all my staff who are designing and are working with colleagues and the provider.
(Chief Executive Officer – CCG, 001/56-59)
In keeping with the same line of thinking, there was a general consensus
amongst participants that innovation was an organisation’s philosophy and
mind-set in the way that they functioned, and by this they continuously sought
new solutions from the outside which they could apply to fit and improve the
existing context. Examples of this were new drug treatments or new
technologies adopted to deliver better care. To further support the
interpretation that innovation is behavioural, participants in the study
explained using examples to show that innovation requires a mental push for
organisational members to think and act in a different way.
Innovation is also about the way in which I characterise as other people's ideas are made to work better in an environment where there's that sort of continuous improvement attitude. Or it could be the way you encourage staff to just focus on continuously improving what they are doing. So, there's the diffusion of evaluating good practice, but actually, the real focus we are trying to adopt here is where staff is encouraged to just continuously improve on what they do and that's part of innovation as well.
(Chief Executive Officer – NHS Trust, 003/43-49)
I think it is different from organisational change. Organisational change can just happen because it has to happen. You need to save money,
127

therefore restructure, do this, do that do that. Is that innovation? No, it is just shuffling the deck of cards that you got. Innovation, people have to have motivation…. I think that they are pretty much poles apart.
(Managing Director – NHS Regulatory body, 007/83-91)
On the contrary, participants explained that organisational change was not
iterative. Organisational change was described as intermittent, a
management-based approach that is essentially egocentric in that it focuses
inwardly on the organisation and improvement of its performance, efficiencies
and cost reduction endeavours. Organisational change was essentially not
open for discussion or modification as management required change and it
must be accomplished, unlike innovation that stressed leadership
continuously and encouraged organisational members to be responsive in
their stance and expectations.
Do I think innovation is different from organisational change? I think it is different from organisational change. Organisational change can just happen because it has to happen. You need to save money, therefore restructure, do this, do that do that. Is that innovation? No, it is just shuffling the deck of cards that you got.
(Managing Director – NHS Regulatory body, 007/83-86)
I think innovation is not organisational change, whether it answers your question or not. Innovation in more ways is driven by the doctors and nurses and organisational change is sometimes seen as a bit of a management thing.
(Managing Director – NHS Trust, 10/178-181
This is not to conclude that innovation cannot drive efficiency. A participant
strongly pointed out that innovation must be perceived as new and present
additional benefits to those implementing the service before it would be fully
adopted. This means that an innovation, for the greater part, has to surpass
the performance of what already exists, even as implied by the following
participant:
.... And not just thinking that innovation is always good. No, it's not. It's actually evaluating and thinking through all these new ways of looking at the literature and so much of what we do is scientifically based where you are looking at the literature and research and always looking at new ways of thinking in what we all 'Lean Ways of Working'. Are these conferring an additional benefit for the time you are going to
128

invest in innovation? Or new ways of doing things that would be at least as good as the current way of operating.
(Chief Executive Officer – CCG, 001/61-68)
In some ways, innovation precedes the implementation of organisational
change as it is first proposed and organisational change is initiated as a result
and this is managed by the implementing organisation. A participant explained
that innovation necessitates organisational change in the way it operates in
order to put the new idea into effect. Unlike organisational change, the
ramifications of innovation are that the system processes might need to be
altered to ensure successful implementation.
Well, often the two are hand in hand. Because to reach innovation, you often need to change the way your organisation behaves. I am a commissioner so if I'm innovating or putting forward, I have a service specification that I'm asking my providers of care to implement. So actually, the innovation that I'm going to expect to be delivered will happen in the providers that I am commissioning to deliver this new pathway of care. So for me, the organisational change isn't about me.
(Chief Executive Officer – CCG, 001/178-179)
2. Degree of complexity, structure and impact
With this second theme, participants made a clear differentiation between the
concept of innovation and organisational change based on the degree of
‘complexity,’ ‘structure’ and ‘impact.’
First, the participants explained that innovation was not prescriptive and
needed to be amorphous to enable people to think outside of the box. One
participant talked about innovation in terms of it being a challenge because
some people thrived on being creative, while others found it much harder. The
level of difficulty was aptly described by one of our participants: “If you want to
know how difficult it is to change, try wearing your watch on the other wrist”
(005/329). Putting the watch on another wrist is difficult to do because it is
doing something new, hence, the difficulty. Innovation means things are being
done in a different way which usually takes time as it is not easy to change a
routine. Irrespective of the participants’ level and active involvement in the
process, it was argued that convincing people to change is difficult.
Furthermore, because innovation is amorphous, it makes it difficult to directly
manage directly. Organisational change, on the other hand, is described as
129

clearly prescriptive, with step-by-step guidance that management provides in
order to meets its objectives. This can be seen by what two participants said:
I think it is more complex managing innovation that other forms of change. I think it is because it's a bit more amorphous; it's a bit more difficult to describe. If we go for organisational change and let's say we reduce all the hospital sites from one to three and people start running shops and all that, those are quite simple things to define and I can tell people to do things differently. You used to work in Canterbury; you now work in Ashford, that's organisational change, that's quite straightforward. I think with innovation, I am saying to you innovate, come up with a new idea and they would look at me, some people will look at me and say I don't know. But other people will fly…I think it is harder. And some people respond to being managed to innovate and some people really don't like it. A lot of people look at me and say I don't want to do a new job, I don't want to innovate…So I think it's harder.
(Managing Director – NHS Trust, 002/138-154)
I think innovation is a complex process. I think that even if it's a simple idea, how you bring that simple idea into everyday process in a trust is a difficult thing; it's not easily obvious. So even whenever there are simple things, as simple as the Elbows' and Gel outside every ward but it was ages before everybody used the gel and went into the ward. They had signs up, you can't come in unless you got, but actually it took ages, it doesn't spread quickly even if you have got champions inside organisations, it just doesn't.
(Managing Director – NHS Trust, 005/277-284)
Following the same line of thought, the uncertainty surrounding the concept of
innovation was described by most participants as ‘nebulous’, although it was a
situation that provided them with a sense of freedom to manage
organisational capabilities. This point is quite interesting because it showed
that innovation was not just for the rank and file employees, but also for
organisational managers and that it gave them the freedom and space within
which to manoeuvre. This flexibility would seem to distinguish innovation from
other forms of organisational change as it is portrayed as less restricted and
structured. Consider the following response by one of the participants:
Innovation is some sort of nebulous thing..… My own organisation is the CCG. There are 211 of us across England and how we do it and introduce new things will be very different to the other 211. There will be some similarities but it's about organisational form. Also, what is an organisation? There are the laws and governance that are set out and
130

common or the expectations that are common amongst all 211 people. I sign my CCG contract and the expectations is that I will live within the standing financial instructions of the NHS and I have a duty as a chief officer to be accountable to the Secretary of State for Health for delivering against this mandate. That's fine. But then within that, that's the commonality. But then how I do that is up to me as long as I stay within my statutory limits and don't become ultra vires against those. So.... All of those things are in the NHS constitution that I have to deliver as part of my annual contract with the NHS and if I don't, I will be sacked. So but within that, how you do it is often left to you I've got a lot of freedom in terms of managing how I do things locally and I call that innovation.
(Chief Executive Officer – CCG, 001/109-133)
Interestingly, another participant disagreed with the idea that managing
innovation is more complex than other forms of organisational change. The
participant explained that innovation was only complex if structures and
constraints were built around it. For example, if organisational members
perceive that innovation could not be delivered within the set time frame, then
the need to accept the idea would instinctively be minimised. However, if they
perceive that they have sufficient resources, such as time, flexibility,
knowledge and information, the tendency to accept innovation and deliver it
would be greatly enhanced. Organisational change, on the other hand, was
described as simpler and more direct because it had a set format which made
it easier to implement, and it did not need a new way of working.
So, innovation is not organisational change. I think that they are pretty much poles apart. One is very much structured; innovation is very much an iterative process, just constantly changing in the business environment. I don't think innovation more complex. I think it's complex if you want to make it complex or you want to put a structure around it. ………. I think the problem is, if you tried to constrain innovation. You won’t innovate because you are kind of going, “Okay, you can innovate, but you have only got a week to do this process”, and so you are going to cut corners, you're going to find a quick way to get from A to B…. We need you to come and say, “Take your time, don't worry about it, go and speak to these people and do whatever, put the research in. I don't think innovation is complex at all, given the right resources, where there is time, money, and space whatever.
(Managing Director – NHS Regulatory body, 007/90-107)
If we go for organisational change and, let's say, we reduce all the hospital sites from one to three and people start running shops and all that, those are quite simple things to define and I can tell people to do
131

things differently. You used to work in Canterbury; you now work in Ashford, that's organisational change, that's quite straightforward. I think with innovation, I am saying to you innovate, come up with a new idea and they would look at me, some people will look at me and say,” I don't know.”
(Managing Director – NHS Trust, 002/139-145)
Further insights into the difference between innovation and organisational
change were discussed regarding the degree of the impact that occurred
when either took place. Participants stated that innovation disrupts the
systems at a “whole care level” and impacts how services are delivered
across the various avenues of care as well as how the public receives care.
On the other hand, organisational change was described as being disruptive
at an “individual level” where the changes impact only those within the
system, and not the external environment. Participants further argued that the
degree of impact from an innovation was often times higher than that from an
organisational change.
Yeah, there is a difference between innovation and organisational change because I think that organisational change is very rarely thought of, it is disruptive at an individual level, but organisational change is not disruptive at a whole system care level, so we are going through a change at the moment which for individuals in new organisations is quite disruptive. It's not really disrupting the service that we are providing to the outside world though. So that is organisational change. Yeah, that's organisational change. So I think that the NHS goes on, patients still get seen, doctors still turn up and patients get better or not, as the case may be, but whether the organisational change around that has much impact on it, I don't really think it does because it's about a culture. The NHS is about the culture of caring and people care no matter what the organisation structure is doing around them… So, I think they are two different things. I don't think that anybody has ever invented an organisational change that I would call innovative. They might produce organisational changes, which they think is going to help innovation.
(Managing Director – NHS Regulatory body, 005/150-209)
5.5.2 Defining organisational readiness for innovation in a public healthcare context
With this second broad theme, participants discussed their views on how they
perceived the meaning of organisational readiness for innovation under the
following headings:
132

1. Interactive dynamism
2. A movement
Their responses were grouped into sub-themes with each representing a key
dimension and can be seen in Table 5.4 below where there is a breakdown of
the 1st order concepts, 2nd order themes and aggregate dimensions.
133

Table 5. 4: Themes and sub-themes on the meanings of organisational readiness for innovation 1st Order Concepts 2nd Order Themes Aggregate Dimensions
“Keeping up good practice and bringing it back” (008/149)
“Just being open to new ideas” (001/289) Relations and Openness
Interactive Dynamism “Not thinking of the emperor’s new
clothes” (001/293) “Be self reflective to always look into…”
(001/288)
Critical thinking
“Is having a group of people who want to move it on to the next level” (002/304)
“Staff see it as their responsibility to continuously improve” (003/149)
“Top team that champions and supports” (004/282)
ChampionsVs.
Top team championingA movement
“They have an outward facing chunk” (005/360)
“It is the flexibility to free up space “(007/183)
Special agents/EdgeVs.
Flexibility
134

1. Organisational readiness is an interactive dynamism
Firstly, participants described readiness as the responsiveness to new ideas
by organisational members who interact and engage, over time, in relation to
others inside and outside their environment. This definition focuses on two
basic dynamics – people and openness, and critical thinking. Thus, there is
the human side to organisational readiness because people need to be open
by paying attention to new ideas; and to seek for opportunities to improve and
learn. For example, a participant pointed out that organisational members
must engage with external networks to develop a shared understanding of
good practice and then bring back the new knowledge to the organisation.
Participants further highlighted that during interactions, the level of willingness
to consider and attempt new things was what organisational readiness is
about.
I think it means I keep coming back to this, the extent to which staff sees it as their responsibility to continuously improve and if you got a staff base where people take that view, I think anything's possible. Where you have got a staff group who, particularly your clinical team and your senior staff, are isolated from other networks and other organisations, so if they don't want to go and see what their neighbouring hospital is doing well or if they are not engaged in going to conferences and keeping up good practice and bringing it back, then that's one failing.
(Chief Executive Officer – NHS Trust, 003/149-156)
Okay, what it means to me is it in the context you have given in terms of continual innovation? Is the NHS responsive to innovative ideas from inside and outside that will improve things for patients and those delivering care.
(Managing Director – NHS Regulatory body, 008/465-469)
It means it's ready for change. It's constantly looking to change. Be open, self reflective, to always look into, just being open to new techniques and new things. Not being closed and conservative.
(Chief Executive Officer – CCG, 001/288-290)
Participants further expressed readiness as a process that required a certain
level of self-reflection and control as not all ideas may add value and are
suitable for introducing change in healthcare context. This degree of
reflectivity is dependent on an individual’s interpretation of the impact this
change might have on patients’ information.
135

It means it's ready for change. It's constantly looking to change. Be open, self reflective, to always look into, just being open to new techniques and new things. Not being closed and conservative. Although, it is often in the patient's best interest if you are conservative. It's not always that everything new is wonderful and hey diddle diddle. It's not. It's not being swayed and thinking of the emperor's new clothes, no not really.
(Chief Executive Officer – CCG, 001/288-293)
2. Organisational readiness is a movement
Secondly, participants described organisational readiness as a movement
that involved a group of people that wanted to see the organisation moving in
the direction of having continuous innovations. These groups of people
consist of two types – the champions and those on the outward edge.
Champions are those groups of people within their workplace that move the
services far beyond their job description and requirements. They motivate
others, try-out new practices, and disseminate new ideas into their work place
to challenge the status quo. Champions see it as a core responsibility to
continuously seek workplace improvement, and they do it willingly. The
participants explained that champions are motivated to innovate, not out of
selfish-interest or extrinsic rewards, but because of the sense of pleasure,
satisfaction and accomplishment they derived from it. For example, by sharing
a personal experience, a participant within the study justified his drive towards
continuous innovations as one born, not out of expectations from the board,
but rather from an aspiration for his trusts to be recognised as one of the best
in the country in information.
I think that readiness is about having a group of people who want to move it to the next level. And it doesn't have to be everyone, but the people who are like that are open to it. So no one asked me to do anything I do, no one asked me for an information strategy, but I do what I do because I want our hospital to be, if not the best, but at least within the five trusts in the country in information. But nobody asked me to do it, nobody set me that target, but I came and said if we are going to do it, let's be the best in the country.
(Managing Director – NHS Trust, 002/303-309)
To me, that means that there are a majority of people within the organisation who see improvement as a core part of the job and something that they get enjoyment and passion from…. and the
136

organisation consists of more people who challenge the status quo, rather than be comfortable with the status quo.
(Chief Executive Office – NHS Trust, 006/159-165)
I think it means, I keep coming back to this, the extent at which staff see it as their responsibility to continuously improve and if you got a staff base where people take that view, I think anything's possible.
(Chief Executive Officer – NHS Trust, 003/149-151)
Along with this, participants explained that organisational readiness was when
leaders enable a working environment that gives champions the “space” to
take risks and consider things in a new way. These findings showed the
importance of leadership support as a prerequisite for readiness as it, more or
less, determines the degree to which the champions can move, improve and
increase their innovative capabilities. A participant explained that
organisational readiness was about the leadership’s willingness and
commitment to motivate their team to push the boundaries and be challenged
to do more.
I suppose that readiness is leadership have got the flexibility to free up space.
(Managing Director – NHS Regulatory body, 007/183-184)
So, if they are ready for innovation, you have got a top team that really champions and supports it. You have got a top team that rewards that kind of behaviour. You have a top team that tolerates the risks associated with doing things differently. They put some resources behind it, they skill people up, they actually stretch people. If somebody says " I think we can probably shave off a couple of months waiting time for this if we did things differently", you might have the top team say "Let's not make it a couple of months, let's make it a couple of years" or "Double it!" or whatever might be relevant for them; really push them to go a bit farther.
(Managing Director – NHS Regulatory body, 004/281-333)
Participants further described an organisation that is ready for innovation as
one with an outward facing chunk called the “edge.” This outward looking
edge is described as a group of special agents assigned on a unique mission
to leverage external resources and to identify ideas that can bring about
significant and sustainable returns. Consequently, these people will seek to
implement these ideas by helping to adapt them for use through the
interpretation and translation of the ideas into action. Unlike champions, this
137

group of people are specifically employed to help the organisation achieve
innovation and tap into the opportunities of the future. To successfully develop
such a model, the participants explained the need for the outward edge to
remain isolated from the rest of the organisation. Accordingly, effective
readiness for innovation requires a level of flexibility to influence the
approaching development of events. Participants also explained that
readiness for innovation also requires leadership’s capacity to remain open
and flexible, releasing space and suspending control, whenever possible, to
allow people belonging to the outward edge to determine how to engage in
the processes for continuous innovations until a more comprehensive view of
the event emerged.
Well, I think that it means that it is open to ideas but I think it also means that it has a way of testing ideas and bringing them into being. So, we have a team in our organisation called the Horizons Team and its job is to find new ideas from other industries, it could be somewhere else in the world and bring them back and adapt them for use. And so that's all they do, and when that idea is taken on board by somebody else in the same organisation, then they leave it and go and do that again. And that is quite challenging for the rest of the organisation because that part of the organisation, they have got a director and I don't really treat them like a director and that upsets the other directors because they are treated specially but I am saying yeah they are and that's because we need them to be treated like that, because if they are not, if we bring them in and wrap all this governance stuff around them and we have lots of control, then they wouldn't be able to do what they are doing… Organisations that are going to be innovative need an outward facing chunk of the organisation, which is the edge, and is to be able to bring new stuff into the inward phase.
(Managing Director – NHS Regulatory body, 005/299-318)
I suppose that they have got the flexibility to free up space.(Managing Director – NHS Regulatory body, 007/183)
5.5.3 Enablers of organisational innovation state of readiness
Under this third broad theme, participants discussed several strategies that
could be adopted to achieve a state of readiness. In describing these
enablers, participants highlighted problems pertinent to the NHS that hindered
the development of a state of readiness to innovate. Their responses were
grouped in sub-themes each representing a key dimension:
138

1. Free spaces
2. Interactive relationship
3. Stability
4. Attracting the right people with the right fit.
5. Anticipation for Future Events (see Table 5.5 for a breakdown of the 1st
order concepts, 2nd order themes and aggregate dimensions)
139

Table 5. 5: Themes and subthemes on the enablers of organisational innovation state of readiness 1st Order Concepts 2nd Order Themes Aggregate Dimensions
“Create a space” (002/132) “Give people freedom” (007/466) Freedom
Free spaces “Find them, put them in positions of
authority” (006/186) “Protect them from professional jealousy”
(002/158)Identify & Protect
“Congratulate and NOT blame”(008/292) “Create like a dragons’ den” (003/26) Incentivise “You need be able to sail the ship”
(002/323) “Don't ruin the size” (002/347)
Sustain
“If you don't involve your end users you can just forget about it” (007/205)
You risk clinical workforce being conservative if you do not engage them (009/54)
“Diversity of thoughts over diversity of people” (004/422)
“Encourage competition… must be based on trusts” (004/420)
People matter/Diversity of thoughtsVs.
TrustInteractive relationships & partnership
“They have really long standing leadership” (005/306)
“A shift creates room for improvement” (004/370)“Establish one method for continuous improvement” (009/202)
Stable leadershipVs.
Shift, andOne method
Stability
140

Table 5. 5 continued: Themes and subthemes on the enablers of organisational innovation state of readiness1st Order Concepts 2nd Order Themes Aggregate Dimensions
Recruit only people that “fit” (006/254). “You don't want all to be innovators”
(10/297)
FitVs.
Right balance
Attracting the right people with the right fit “Create a religion” (002/213) “Create a branding and marketing fizz”
(002/482)Branding
A ‘critical mass’ with the same thinking (004/542)
“A legislation to integrate it into undergraduate curriculum” (004/534)
The legislation
“Public healthcare sector is dealing with the here and now” (008/660)
“Non-healthcare sector is dealing with next year” (008/660)
Looking ahead Anticipation for Future Events
141

1. Free spaces
Majority of the participants agreed that one of the main impediments to
innovation readiness within the NHS was the lack of space for staff to spend
time in innovative thinking. NHS staff was in a constant fire-fighting state,
moving from one agenda to the next to keep the wheels turning. It could be
argued fairly that people needed to get off the treadmill and spend more time
innovating, but the demands keep increasing with people getting older and
living longer. The NHS was clearly overburdened with the staff experiencing
burn-out from working such long hours, in addition to there being a lack of
encouragement to share their ideas.
One of the key problems we have in the NHS today is the lack of space to think and, therefore, then to do. So, my clinical workforce, clinicians are working at a hundred miles an hour. Some of them are working ungodly hours just to keep the service delivered. So, where is the space even if they wanted to think and to innovate because they are just keeping the wheel turning?
(Medical Director – NHS Trust, 009/250-254)
In an acute organisation, they are fire fighting all the time. There's always something to do. So they actually can’t say: “Every Friday for the next two months I'm not going to do any work, I am going to just stay at home and I am going to do something completely different. It's rare to find an organisation that would go down that route and say “Do you know what? You can do that.”
(Managing Director – NHS Regulatory body, 007/117-120)
But the difficulty is that the people at the front end are either so busy that they don’t have the time or have the conversations to share their ideas or they are not well connected enough or they feel that they don't have the influence to share their ideas.
(Managing Director – NHS Regulatory body, 008/99-101)
Given the fact that innovation requires managerial freedom to facilitate
readiness, the participants argued that free spaces should be established.
Therefore, this section discusses how to best develop, manage and sustain
free spaces under several sub-themes including, namely, freedom, identity
and protect, incentivise, and sustain.
To begin with, the participants described space as an informal network where
people can benefit from innovative freedom and the opportunity to
experiment. This freedom means the ability to make collective decisions
142
without intrusion from management; to express new ideas and to acquire new
knowledge and to engage with people and ideas within or outside the
organisation. Such spaces can also be strategically configured to create
innovation. One of the directors participating in the study gave the following
example of this. He described how a typical day at Google would involve 70
per cent of the employees’ time being spent on a matter relating to searching
since Google’s primary occupation was that of a searching company. A further
20 per cent would be spent on things related to searching, such as Gmail and
Google Maps; and then, 10 per cent on engagement in anything innovative
and creative. He regarded Google as a company that was ready for
innovation and, thus, made provision for innovation for its employees. In
creating free spaces, time outside of business-as-usual should be prioritised
to allow members of an organisation to engage in processes that could
stimulate innovation. A participant argued that one of the advantages of free
spaces was that it saves time, thus, turnaround happens quicker.
They are given freedom. Individuals and teams are given freedom on teams to decide and come up with new ways of practice.
(Chief Executive Officer – CCG, 001/261-262)
So when I do innovation, it wasn't my idea to build that app, it was my idea to create a space where people might come in and do interesting things. So, none of these innovations are mine, but I just created the context for innovation, if you like, the context for benefits. But I didn't do any of the innovations. I guess I wrote the strategy and I tried to set the culture, but I didn't do any innovation. I just created the space where innovation would happen.
(Managing Director – NHS Trust, 002/129-135)
It is also about giving people an opportunity to innovate as well. Giving people the freedom and a bit more chances to experiment a bit more with their time, to have the ability to kind of be able to go out and speak to a person, go out and learn different things.
(Managing Director – NHS Regulatory body, 007/466-470)
Monthly, we had an update meeting to find out what was going on, whether there was what we could do as a senior leadership team to help them unblock problems or something. But basically, we stayed out of the way and I think that's been really successful because they managed to bring their timeline forward by about three or four months to do a sort of alpha and beta testing process before they went live which they hadn't planned in properly so we were able to help them with that.
143

(Managing Director – NHS Regulatory body, 005/299-234)
Secondly, participants described another way to create space was by
identifying the people who want to innovate, upskill them to expand their
capabilities, and grant them access to authority, as well as protect them.
According to the participants, Trusts were exposed to some amount of
pressure politically which generated defensive behaviours making people less
tolerance of risk-taking. It, therefore, became the responsibility of leaders to
protect the free spaces from certain individuals, especially long-serving
leaders that had become complacent with the existing ways of working. Such
people were seen as posing a threat to innovators, especially young persons
just beginning their careers.
In any organisation, there will always be people who are wanting to change and innovate and you have to find them, you have to put them in positions of authority, look after them, develop them, help them grow and develop them and they become the leaders of the organisation because not always are there people who are in management positions the people who are the innovators.
(Chief Executive Officer – NHS Trust, 006/185-189)
And actually, if you teach people the right tools, the creativity tools, if you put an innovation process in place within an organisation and if you have got the right kind of culture, then you are going to have innovation in your organisation… people require additional skills in order to come up with that innovation in the first place. They need the skill set to run an innovation process. Idea generation, divergence, convergence, prototyping, have they got those kind of skills?
(Managing Director – NHS Regulatory body, 004/64-243)
I have to create the space for innovation, I have to protect them as well…The difficulty as you go along, sometimes there is professional jealousy, that's quite a big issue…and a lot of people don't like to be criticised so they just go back and fall into the routine of doing the things they are supposed to do.
(Managing Director – NHS Regulatory body, 002/199-207)
Thirdly, participants discussed the need to incentivise free spaces. The use of
incentives was described as making the culture of an organisation a more
favourable place to work, and a driver of innovative behaviour. Participants
further highlighted that incentives can occur in various forms as “not everyone
is incentivised directly by fame, money or power” (002/435). People like to be
celebrated and recognised for their contribution and attempt at innovation,
144
even if they sometimes fail. Incentives can also be given in the form of
contribution towards personal development and career advancement, such as
sponsorship for pursuing advanced studies. In addition, a participant revealed
an interesting approach to incentivise people which is to give them the
opportunity to present their ideas and upon acceptance, reward them with
funds for their implementation.
So incentivising people, I think it is key. I think celebrating success ... but also you know giving them sponsorship and support which is also pretty key. The other factor is that the NHS, for too long has been quite intolerant of people going off and trying things and failing. I think there's something about congratulating people for trying as opposed to blaming and sanctioning them for failing. Does that make sense?
(Chief Executive Officer - NHS Trust, 003/285-293)
The other thing that is interesting is creating the grounds and culture and setting for innovation… and I am creating links with universities and sponsoring people to go on masters degree.
(Managing Director – NHS Trust, 002/113-118)
We are about to start a process of sort of a new ideas incubator, which is where people come forward, a bit like a Dragons’ Den type of environment where people can step forward with their new ideas that might need some priming and money to really consider which would be the best ideas to support, that require funding.
(Chief Executive Officer – NHS Trust, 003/25-28)
Finally, one participant in the study pointed out that innovation spaces should
be of the right size. Qualifying his comment based on a personal experience,
he gave an example about an informal network he established which
collapsed due to reasons including, polyphony and inadequate rewards and
incentives. The director explained that as the numbers of people increased, it
became difficult to innovate.
…And once it got quite big, a hundred to a hundred and fifty people, it lost that and so it developed growing pains and just couldn't innovate because it became a big ship and you couldn't kind of turn. But when it was twenty to fifty people, it was really innovative because there was something in the air ‘let's just do’, we can do anything, that kind of thing. And there were incentives and rewards to work around that because we were quite small…. So there's something about being the right size to innovate and it's interesting, the thing I'm involved in now, there's half a dozen of us so it's really innovative because it's new and
145

we can build stuff like every day. But if it was a success and that turned into twenty, thirty, forty, fifty people, that innovation might slow down and the challenge will be how you incubate an area where they can't keep innovating. … The big companies, the Apples, the Googles, I think when they acquire companies, I think they leave them at arm's length so they still are small enough to innovate so I think it's something about when you find that time and space when people innovate, you need to try and not ruin it by making it too big almost.
(Managing Director – NHS Trust, 002/320-346)
2. Interactive relationships and partnership
A participant argued that the NHS England was tribal with an hierarchy which
acted as a barrier to knowledge exchange opportunities. The participant
claimed that even as a senior leader, it remained difficult for him to secure
access to the National Lead. He had to go through four or five people before
speaking to the Lead and, most likely, he would not be able to share the idea.
The participant explained that the system was inflexible.
I still think that the NHS is very tribal, in terms of your consultant groups, your clinicians, your commissioners, your nurses, your managers, it was interesting, my six months at IQ, the commissioners were seen as the enemy and that's not healthy. So in terms of hierarchy, particularly with IQ being hosted by NHS England, it's probably never been more evident to me. There's not so much hierarchy with the IQ, there is certainly a lot of hierarchy in NHS England.
(Managing Director – NHS Regulatory body, 008/799-804)
A participant used the organism metaphor in explaining the importance of
relationships to foster readiness for innovation within healthcare
organisations. The organism metaphor recognises that healthcare is a
turbulent and ever-changing environment. Motivating people to engage with
innovation in such an environment requires interactions with one another and
the forming of strong, long lasting relationships to achieve complex tasks.
An organisation isn't a static being, it's an organic organism really and people matter. Relationships, relationships, relationships, you can build all the bloody structures you want but it's all about making sure that the procedures are there that help people think and make it happen and who they engage with and how they deliver on what the expectations are is the crucial thing.
(Chief Executive Officer – CCG, 001/257-260)
146

Participants argued that different kinds of relationships that existed with a
number of stakeholders groups across the system are relevant to promote
and establish a state of readiness. For example, this could be seen with
regard to the patients’ group. Participants discussed how this group of
stakeholders were often over-looked as their views were not taken into
consideration during the innovation management process. Participants made
it clear that without the patients’ active involvement, the adoption of the
innovation might not take place.
I think organisational readiness needs to be promoted at a very senior level so that the message goes down consistently that we welcome innovation and we particularly welcome innovation from patients, because they are often overlooked because they experience the service on a daily basis, and I don’t think we tap enough from patients in terms of “What have your experiences told you might help us? Why do we do that differently”, we tend to look within the service all the time for the ideas, or we look across the sea, to what the States are doing or to what Norway is doing or Sweden in terms of their healthcare.
(Managing Director – NHS Regulatory body, 008/398-404)
With readiness the thing is tapping into the patients' and the wider population's interests and appetite in understanding what we are trying to do and listening generally to their feedback. What is it that the patients and public are saying to us about our services? And if they are not up to it, getting them to change and we need a strong sell about what we are about.
(Chief Executive Officer – CCG, 001/457-459)
If you don't involve your end customer, you can just forget it because they won’t use it, because it won’t be implemented successfully because you would think it is actually the best thing in the world and be really really proud of it and then you go and push it out to somebody, they just kind of go: “No, I'm not happy with that at all.”
(Managing Director – NHS Regulatory body, 007/205-209)
Participants also commented on the need for better and stronger relationships
with the clinical workforce to make them ready to innovate. Generally, clinical
staff tend to be conservative towards innovation, but their competitive nature
and their source of influence, usually from senior staff, could affect their
attitudes towards innovation.
The difficult bit is in the clinical work force we risk being very conservative. So you would have to be really compelling in your argument for change for them to want to change and to actually
147

contribute to be part of the change ….. But actually, what I have to do to make that work is to engage the clinical workforce to think in a way that I think in one sense about innovation and systems.
(Medical Director – NHS Trust, 009/46-55)
There are some people who would take some time to get involved and engaged. I think that what you tend to do is use the tipping point, so you get enough people as part of their peers who are interested, think it's the right thing to do, lots of clinical staff are competitive so they won't want to be left behind and sometimes it's also about understanding who they listen to...who their influences are, sometimes because of a long standing work relationship, when they work with consultants for a long time, they know consultants from when they are juniors, they'd often listen to the senior nurses if you get the senior nurses on board.
(Chief Executive Officer – NHS Trust, 006/132-142)
The participants also talked about partnership and the perception that
continuous improvement within the NHS required the involvement of more
than one organisation. Participants contended that collaborative efforts across
AHSNs, local authority, social service, and other NHS partner organisations
would foster better solutions to identify how local needs could be better
delivered. Working together in partnership leverages the diversity, expertise,
and collaborative relationships, and also, importantly, it creates trusts and
encourages healthy competition.
I would form really a good partnership with my local AHSN and I would find out what the hell they are doing and also, I would find out what they are doing with other AHSNs.
(Managing Director – NHS Regulatory body, 005/427)
And so, if this competition between organisations is not good trust, if there is blame between organisations, then that's not going to have good trust within it. If people don't value the diversity of thought, not the diversity of people but that diverse range of thinking. So, you know recognising the fact that actually a scientist, a English student, a history student, all those different kinds of backgrounds, they contribute a whole range of different perspectives, and you are likely to come up with a much better solution. So that kind of thought, diversity. If that's tolerated or if it's not tolerated. How can local authority possibly know how to deliver our services better, if that only local authority were the NHS? You can see all kinds of ramifications playing out.
(Managing Director – NHS Regulatory body, 004/420-430)
148

3. Stability
Many of the participants criticised the constant re-organisations and
restructuring, and considered these as part of the problem to risk aversion in
the NHS. Frequent changes in political mandates, and even the strategic
move in 2013 that replaced Strategic Health Authorities (SHA) with CCGs,
had caused relationships to break down.
The other big element in the NHS is the constant reorganisations. Top down and bottom up. The trouble is that the NHS is owned by, because it's so political, each Secretary of State of Health for whatever political view often wants to come in and change the health service.
(Chief Executive Officer – CCG, 001/434-437)
So, the NHS has gone through a massive restructuring in health and social care from around two and a half years ago. And I don't think parts of it have recovered, it's not stable enough yet. There was a lot of skill sets and relationships that were there that have been broken by the restructuring. And it means that because you haven't gotten those relationships and people aren't familiar with the structures, I think everything is much slower.
(Managing Director – NHS Regulatory body, 004/305-310)
Participants discussed how enabling readiness requires stability in good
leadership and methodology. Participants shared the view that stable
organisations, especially those with stable leadership, are effective in
fostering internal innovations and embracing a culture of improvement.
Specifically, a participant argued that hospitals that had succeeded in
achieving innovations across the country were known to “have a stable
leadership team for over five years” (10/288). Interestingly, another participant
stated that a change in leadership presents a real window to adopt innovative
approaches, especially for poorly performing Trusts because a new top team
can set a new tone and provide a clear strategy for how innovative vision
needs to be articulated.
Some trusts do because they create that pressure over a period of time but they are nearly always ones with long standing leaderships so they are not the ones that have got a new chief executive in two years. It is places like UCLH and Suffolk Royal and Sheffield where they have had really really long standing stable leadership and they have managed to create the space for internal innovation and improvement in a way that other organisations just look at and they can't believe that they can do that.
149

(Managing Director – NHS Regulatory body, 005/302-308)
So, there's a trust that I worked for in the North East where innovation was absolutely what they did. What led it to that? Good leadership from the chief executive chair, stable executive team.
(Chief Executive Officer – NHS Trust, 006/169-171)
So, I think that if an organisation has been really struggling and its top team gets shifted out, there can be a bit of a hiatus and things are a little bit more turbulent. But it means that things aren't set in stone if we start doing things differently.
(Managing Director – NHS Regulatory body, 004/369-371)
However, participants maintained that a single method for continuous
improvement that was clear, tested and approved to deliver innovations would
reduce the loss of valuable time and momentum formed from building
relationships, especially when a new leader came in. According to a
participant in the study, evidence in the social sciences is clear about what
success methodology looked like; and successful hospitals in the world have
delivered a learning platform that Denning advocated. The participant shared
that he only adopted the work of Denning to lead change in his hospital, and
that he avoided strategies that did not use this approach.
It is very easy though, to how you improve your readiness. You improve your readiness by having a clear methodology for improvement. So what happens in healthcare is that there are many different ways of apparently improving systems. That is madness. That is why staff gets confused, doctors get confused. Here is the latest…. I'm going to use a term I think it is right. Bullshit Bingo for management. Bullshit Bingo language is the latest exciting toy that we can bring and you pay for as a consultancy firm and I would help you solve what's ongoing in your organisation. Of course, all that has done is distract and distract because there are different ways of doing. Successful healthcare organisations which have been privileged to explore the world have achieved their really rock star status by a number of key things – constancy of good leadership, clinician engagement, establishing a mechanism of constant learning to achieve outstanding care. But they have established it by using one method of continuous improvement, one method.
(Medical Director – NHS Trust, 009/190-202)
4. Attracting the right people with the right fit
Participants stated that recruitment is essential in driving an organisation’s
success. While there was greater demand, the participants maintained that
150

the NHS needs an objective recruitment strategy that removes people who
are not innovative and employs those who fit in with the organisation’s value
and belief system. For example, if continuous improvement and patient focus
are the core values at Salford Royal NHS Foundation Trust, then the human
resource management’s drive should be to recruit persons who could optimise
care and be flexible.
I think having, organisations having much clearer compact or covenants with their staff about what really is expected and they give and they get. But I actually think that the workforce market needs to change, because whilst there is greater demand than there is supply, it is much more difficult to encourage that sort of approach. You have to be able to turn people down. You have to be able to say, "Nope, you are not going to fit because you don't share the same values and approach so we are not going to appoint you.
(Chief Executive Officer – NHS Trusts, 006/248-255)
Well, sounds obvious but a lack of people that are going to drive. It has a recruitment policy that doesn't recruit innovative people so you can probably start to design recruitment strategies that take out people.
(Managing Director – NHS Trust, 002/457-458)
On the contrary, another participant in the study expressed the view that all
organisational members do not need to be innovative. The participants
explained that the key element was to have the right balance, in that all
should not be innovators, but essentially they should have the skillsets for
effective innovation management.
If you have got the recruitment right, because you have to go and get good people, so it that sort of thing of you do not pick a specialty, you don’t want them all to be innovators… You need a clinical team, that real skill set and then within that team to have the right balance of people. You can tell they are driven; they want to go and change things.
(Managing Director – NHS Trust, 10/296-302)
Another participant explained that if the NHS was to gain a significant
competitive advantage, it must employ effective recruitment strategies to
attract pioneering and dynamic people through reinvention of its brand by
developing exciting positions and departments.
I think you can do a lot with recruitment. I think recruitment is quite interesting and is something you can change and I think sometimes
151

you can set the sort of thing that when you build it they will come. So I'm going to launch a National Centre for Health Informatics. I don't even know what means and neither do you. But I will appetise it and see what will happen and people will look towards it. It's whatever you want it to be, that kind of thing. Sometimes you have to create some branding and a bit of marketing fizz to see what happens, you know.
(Managing Director – NHS Trust, 002/473-484)
A director among the interviewees suggested an attention-grabbing scheme
for creating a more innovation ready NHS. According to the participant, the
legislation should enforce innovation training development modules to be
integrated in the undergraduate medical programme, specifically for those
individuals intending to work in the public healthcare service sector. This
would help create a critical mass of people who understand the expectations,
share a common language, and possess the skill-sets that would contribute
towards bringing change to the NHS.
Wouldn’t it be great? So what if we said, this kind of skilling up and training up which would probably take two to three days. If that was included in every undergraduate's program, wouldn't that be fantastic? So all of the people employed in the NHS as part of their undergraduate development, if they got skilled up in this kind of stuff, wouldn't it be great? Cause that means, the doctors, the nurses, the managers will all have a common language and a theory… So getting that Critical Mass, so maybe the legislation should be that everybody who is a university student who may work in the health service has part of that basic training.
(Managing Director – NHS Regulatory body, 004/533-539)
5. Anticipation for future events
For this theme, participants described a condition for enabling readiness
based on principles applied in other industries. The public healthcare sector,
by its nature, has a different perspective on readiness for innovation. The
unique job of the NHS, (namely, social care, mental health and local
services), is to constantly deliver the kind of services where children have to
be protected, mental health patients have to be kept safe and hospitals need
to ensure that patients get better and go home. These are the realities and so,
whatever change accompanies innovations for greater efficiency must be
‘safe’ because the consequences for failure are severe because human life is
at risk. However, another participant argued that this notion was a ‘red
152

herring’ or a logical fallacy that allowed the public healthcare sector to avoid
taking risks.
I don't think they are that different. I think people use them to say it would be difficult to in the NHS cause there are patients involved and I think that's a red herring most of the time.
(Managing Director – NHS Trust, 002/520-522)
In other industries, innovation is readily sought after in order to keep up with
the changing external environment and the market trends in order to stay
ahead of the competition. The private sector “lives” by its readiness or “dies”
for not being innovative. The culture in the private sector is far more ruthless
as innovation has a direct impact on profitmaking. Often times, the old way of
doing things is inadequate to meet new demands, and innovation is pursued
in response to the need. Within this context, other industries tend to use
forecasting as a special analytical tool, it also considers business from the
perspective of innovation, and use this to inform the the decision-making
processes, with strong emphasis on the next big idea. Participants also
underscored a fundamental difference in attitude towards readiness in the
other types of industries when compared to the healthcare sector, and this is
the former being driven by the need to survive. They believed that this
accounted for the major difference between the private and public sectors in
their motivation and expectations to adopt innovation.
So, in the private sector, you live or die by your readiness for innovation. It is a fact, isn’t it? Kodak is the best example. Kodak is one of the best examples; they died because they were not ready for innovation, so they are dead. Fuji which is film based, actually saw the horizon, set its readiness and is now a great success. So in the private sector, you live or die by your readiness. The public sector by their nature, have to steadily keep delivering services, whereas, non-healthcare organisations can risk being innovative and live and die by it.
(Medical Director – NHS Trust, 009/173-178)
I think in the private sector in particular, where frankly the culture is far more ruthless in terms of if you are not delivering profit, because it is a very money oriented, if you are not delivering profit, and you are just doing the same old, same old and your margins are coming down all the time, then the private sector is under pressure to innovate. So the leaders of the private sector, they, and from my experience from the ones that I have engaged with, welcome absolutely largely innovators
153

because they can come up with the next idea. So to me, that's the, it probably comes from the focus on the NHS is very much about the here and now. We have got so much pressure to deliver now, and actually our waiting list is going up and up and up, and we need to cut our waiting list back so we are dealing with the here and now. The private sector, they are dealing with next year already and I think that's to me the biggest difference.
(Managing Director – NHS Regulatory body, 008/645-661)
I don't know whether it's healthcare versus non-healthcare or whether it's public sector versus private sector, I don't know. I don't think that there should be any difference. I think that the tools and techniques and approach in healthcare and non-healthcare, in private sector and public sector are fundamentally the same. So, the creativity thinking, the processes, the culture stuff are fundamentally the same, whether it's IBM or Google or things like that. They are all fundamentally the same. Whether people feel empowered to do it, I think might differ.
(Managing Director – NHS Regulatory body, 004/445-462)
5.6 Discussion
The empirical study within this chapter set out to determine managerial
leadership’s perceptions of organisational readiness for innovation. The
findings in this study were based on ten qualitative interviews from individuals
within three NHS organisations: a CCG; an NHS Trust; and one of the NHS
regulatory bodies. The study had three main objectives. The first was to clarify
the understanding of innovation management by further investigating whether
there was a difference between organisational innovation and organisational
change. The second was to explore the meaning of organisational readiness,
clarifying issues raised in the systematic review of a stage-based and a
process-based approach to conducting readiness, and by investigating
whether organisational readiness would have any impact on successful
innovation management. The third aimed to corroborate findings from the
systematic review study by again demonstrating a number of contextual
factors that influence readiness and by identifying other conditions necessary
for the enactment of organisational readiness for innovation. Within the
discussion section, certain commentaries cited by the participants are
paraphrased to strengthen a given point.
154

In exploring the first objective, it was observed that the participants’ perceived
innovation and organisational change as two different phenomenon. The first
theme to emerge was the participants’ perceptions about innovation as a
process that is on-going and continuous. They agree with the prevalent view
within the literature that innovation is a stage-based sequence that involves
creativity, adoption, implementation and diffusion (Rogers, 2003; Department
of Health, 2011a). However, the attitude of members of an organisation
towards continuous improvement, openness and self-reflectivity was deemed
as a strong determinant for the degree of innovation in the public healthcare
sector (Damanpour, 1991; Schippers, West and Dawson, 2015). Innovation
was also described as a process that is not static, but in continuous motion
(Drucker, 1985; Van de Van et al., 2008; Camisón and Villar-López, 2014).
The outcomes of the process consisted of what is defined as organisational
change. Organisational change deals with restructuring and reorganising of
an organisation’s current way of working in order to improve its performances
in the form of cost savings, and increasing productivities or improvements
(Vincent, 2013). However, participants explained that such change does not
need to be innovative; it is about doing what makes an organisation run more
effectively to deliver the needs of the local community. The view is consistent
with Zaltman, Duncan and Holbek (1973) contention that while all innovations
imply change, not all change involves innovation since not everything an
organisation adopts is perceived as new. Innovation, as agreed on among the
participants, is an idea that is far more than something new. The innovation
should add value to healthcare services by improving financial savings and
quality and by providing better outcomes for patients (Rogers, 2003;
Greenhalgh et al., 2004; Weberg, 2009). As Schumpeters’ (1934) describes,
innovation is the driving force of organisational change. Schumpeters’ view of
innovation is relevant to the present healthcare system as he regards it as a
major influence for economic growth.
Innovation was further differentiated from organisational change in terms of
the degree of complexity, structure and impact. Plsek (2008) and Van de Ven
(2017) have discussed in depth the intricacy of implementing new ideas and
how the innovation process follows a non-linear cycle which is uncontrollable
155

and unpredictable. However, the findings further revealed that innovation is
difficult to define and remains an amorphous phenomenon – requiring
creativity, flexibility, autonomy and empowerment as well as control and
efficiency in real decision-making processes (Khazanchi, Lewis and Boyer,
2007). For example, Van de Ven (1986) explained that despite the promised
potential of innovation, the psychological limitations of human beings to pay
attention to new ideas and high predisposition to focus on existing
organisational norms and values often poses a challenge to managing the
intricacy of the innovation process. In terms of the findings, a participant
stated, “I think with innovation, I am saying to you innovate, come up with a
new idea and they would look at me, some people will look at me and say I
don't know. I try and say you need to expand, why don't you do a prop and
deliver and she just doesn't do it to the point where you think what do I do with
you, do I get out of the way or do I just let you carry on what you are doing.”
Surprisingly, the innovation management literature has received little
attention on better understanding of the processes of novelty-seeking and
novelty-finding. Understanding why people behave the way they do and how
to best deal with them in a workplace environment require neuropsychological
and cognitive neuroscience insights (Schweizer, 2006). It is well established
that novelty-seeking behaviour in individuals is attributed to personality traits
such as self-confidence, risk-taking, independence, and judgmental autonomy
(Schweizer, 2006; Eisele, 2017), along with cues from the social environment
(Woodman, Sawyer and Griffin, 1993; Zhang and Bartol, 2010; Amabile and
Pratt, 2016). Flexibility and autonomy have been suggested to stimulate
creativity and trigger innovation-oriented behaviour principal to enhance
performance and service-user orientation (Khazanchi, Lewis and Boyer, 2007;
Anand et al., 2012; Wynen et al., 2014; Keohane, 2018). As part of one chief
executive officer’s response, he has greater freedom to explore new ideas,
select across the widest range of evidence-based interventions, and to
introduce innovations into CCGs. This view the participant labelled as
innovation – a greater freedom given to an accountable individual to deliver
against organisational mandate in a way they see fit and most effective
(Keohane, 2018). For example, multi-site case studies (Verzulli, Jacobs and
156

Goddard, 2011; Allen et al., 2012), carried out on a series of interviews with
senior managers and clinicians to investigate the impact of governance on
autonomy in public hospitals in England. The findings showed that the NHS
foundation trusts exhibited ability to make longer-term strategic business-like
plans and devised an efficient approach due to having greater flexibility and
control over financial, management and organisational decision-making.
However, increased autonomy had no significant impact on improved
performance in the public sector due to weak incentives to make use of
autonomy, the existing systems of accountability, political directives, and the
governance constraints.
From the findings also emerged a second theme which can be considered as
relatively new within the body of literature on innovation management. Of the
ten participants, one mentioned that organisational change was about
individual units working to trigger innovations, whilst innovation disrupts the
whole system care level. This proposition exhibits properties of complex
adaptive systems which is supported by research. In analysis of the UK’s
Whole Systems Demonstrator telehealthcare programme by Hendy et al.
(2012), it was observed that the lack of nuanced understandings of integrated
whole systems approach among staff and managers significantly increased
fragmentation and discontinuities of remote care across the system, that is,
healthcare and social care. This finding implies greater system integration is a
powerful driver to significantly increase implementation of complex innovation.
A study by Masri, Wood-Harper and Kawalek (2017) into electronic patient
records implementation and knowledge transfer practice in the BP Trust, UK,
further indicates that in order to ease the implementation process, a systems
thinking approach encourages the view of knowledge as a product of
interaction between agents within a social system. When the networking
across social systems is improved, the level of the innovation is higher (Adam
and de Savigny, 2012; Atun, 2012; Masri, Wood-Harper and Kawalek, 2017).
The AHSNs are a perfectly good example of a comprehensive system
approach for achieving results through innovation because they are about
working collaboratively and building partnership across organisational
boundaries, including the NHS, academia and industry. The whole concept is
157

that new ideas would be assimilated quickly into use in the NHS and this, in
turn, would help the NHS with innovation. The NHS in recent times have
engaged in many discussions about the relevance of systems thinking in
order to achieve better outcomes. The participants explained how innovation
has much impact at a whole system care level in comparison to organisational
change where the impact is at the level of the individuals within the
organisation. Consider an example in practice where a healthcare manager,
intending to improve the appointments booking process, may introduce
flexible appointment times in order to improve ways of working within the
Health Centre. Based on the findings, organisational change will necessitate
involving only the other people who work in the healthcare centre, such as the
receptionist, individual patients, doctors, and nurses. On the other hand, the
Health Centre Manager might consider the wider system opportunity and the
added public value to be obtained through having an integrated system.
Exploring this initiative will mean involving a wider scope of people who can
help improve health, such as those within the healthcare centre,
physiotherapy unit, occupational therapy unit, social workers, and counsellors.
Thus, it creates a wider-systems impact that is felt across varying patients
group, carers, family, and across the sub-systems within a system (NHS
Education for Scotland, 2018). This situation is more likely to be complex, but
organisational change is more likely to be the result of the former – which is
involving only the people working within the healthcare center for a specific
change. Thus, innovation is the processes that generate and reinforce whole-
systems level impact.
In investigating the second objective, the findings support the many existing
definitions of readiness, including the attitude-based approach which shows a
willingness and openness to consider new perspective responsiveness. There
is also the intention-based approach that reflects the top team commitment to
support innovation. The process-based approach which necessitates team
reflectivity and continuous evaluation to be able to deal with change under
dynamic conditions. It was observed that participants characterised
organisational readiness for innovation as the relational dynamics highly
facilitated by organisational ways of thinking, acting and organising.
158
Participants discussed readiness concerning the perceptions and positions of
collective actors. These include members of an organisation (physicians,
nurses, professions allied health professionals), mangers, senior leaders and
how these actors individually and collectively determine the responsiveness of
the adoption system to novel interventions, and influence the differential
stages in the innovation process (Atun et al., 2009). For example, the findings
expanded the locus of the meaning of organisational readiness revealing new
aspects which include the idea of champions and the external edge, also
referred to as boundary spanners. These two new categories of innovators
require further discussion as the findings show that champions are
distinguishable from external boundary spanners. Champions have been
referred to as individuals who “identify with the idea as their own and with its
promotion as a cause to a degree that goes far beyond the requirements of
their job (Schon, 1963, p. 84).” Champions voluntarily push innovation ideas
as part of their day-to-day working practices and are found across all levels.
For example, they are among the top management who actively encourage
staff to engage with colleagues within and across organisations and
encourage staff to constantly seek for new ideas. They also are willing to
tolerate risks by providing resources that will allow staff to fix problems
identified within the system and by continuously matching organisational
resources and capabilities with the opportunities in the internal and external
environment (Carmeli, Gelbard and Gefen, 2010; Collins, 2018; Zhang et al.,
2018). Then there are the physicians, clinicians, and nurses who build
relationships, interconnections and interdependencies across organisational
structures in order to identify innovative ideas from inside and outside that will
improve things for patients and those delivering care. It was not clear from the
findings how the role of champions evolved over the course of organisational
innovation, but the results of an empirical study by Hendy and Barlow (2012)
showed that the role of champions is detrimental in the implementation stage
of innovation management, especially if they are required to move outside an
organisational context. Although more research is clearly needed to explain
the conditions that govern the success of champions and how to sustain their
behaviour, the findings suggested that the concept of entrepreneurial spaces
159

might stimulate champion behaviours (see discussion of space in the later
part of this section).
On the other hand, boundary spanners are a dedicated cadre of people
purposely selected and assigned within an organisation to seek new improved
working practices in order to manage complex problems and adapt them for
use (Cohen and Levinthal, 1990; Ansett, 2005; Tidd and Bessant, 2013). One
of participants within the regulatory body made a revealing description of
readiness for innovation as the absorptive capacity for new knowledge within
public healthcare service delivery organisations. In augmenting absorptive
capacity, two of the participants within the regulatory body further described
readiness as senior leadership flexibility and engagement in creating more
active and established innovation roles that support and empower specific
group of people/team who will act as a practical interface between the
organisation and the wider context. This designated group of people or
boundary spanners will work autonomously and holistically for the purpose of
generating awareness of different interventions available, knowledge
translation and implementation (Gilburt, 2016). The deliberate creation of
boundary spanner roles has been explored in the UK CLAHRC-NDL’s
(Collaboration for Leadership in Applied Health Research and Care,
Nottinghamshire, Derbyshire and Lincolnshire) initiative in its adoption of the
model of diffusion fellows (Rowley, 2012b). Diffusion Fellows comprised of
NHS leaders seconded from the local healthcare economy one day a week to
act as champions for change, translating knowledge from academics into their
work practice. Evidence from the case studies showed that boundary
spanners help to bridge the research to practice gap and the communities of
practice and to underpin and sustain improvements in healthcare (Rowley et
al., 2012). Studies have shown that individuals who are successful at
engaging in activities that span organisational boundaries tend to have a
strong awareness of agency, a proclivity towards innovation and risk, and
personality traits that enable their activities (Williams and Sullivan, 2009;
Williams, 2013; Evans and Scarbrough, 2014). While the rewards of boundary
spanners and champions are evident, some of the participants identified the
risk of isolation and the lack of security in these roles (Scott, 2011). For
160

example, one participant cited “Some people look at me and think flash show
off, why is he out there speaking at this conference; I don't think I like him.”
Thus, it is important that leadership intending to develop and enact
organisational readiness through boundary-spanning interventions must
incorporate structural features to support diverse groups in translational
activities, and confidence in working across organisations (Scott, 2011; Evans
and Scarbrough, 2014). The findings suggested extensive interaction,
learning by individual and collective reflectivity, and experimenting as
fundamental facets of the readiness for innovation process in complex
adaptive systems such as healthcare. The above explanations serve to
illustrate that the meaning of organisational readiness for innovation is both
conceptual, describing the behaviour of an innovation readiness culture, and
operational where strategies are employed to ensure the organisation’s vision
and identity are successfully managed.
In exploring the third objective, participants described several contextual
factors influencing the development and enactment of organisational
readiness for innovation, and in their explanation some limitations were
mentioned. One of the main barrier participants revealed to organisational
readiness for innovation is the overstretched and escalating work pressures
on NHS staff. Staff cannot find time to consider new ways of doing things
because they are working under so much pressure and are finding it difficult
to cope (Cordery, 2017). A recent survey conducted across 134 NHS general
acute trusts in England revealed strong correlations between an overstretched
workforce and the poor quality of inpatient care. The results of the survey
further show that poor staff well-being was generally associated with high
absences and low retention rate, and that this is predicted to worsen given the
potential impact of Brexit (Sizmur et al., 2018). While the lack of time poses a
constraint, participants further commented on the status hierarchy existing in
the NHS which makes it difficult for people to communicate across
professional boundaries. In addition to this was the risk associated with
human life that undoubtedly creates uncertainty in the minds and attitudes of
people towards risk aversion and innovation. According to the participants,
this lack of empowerment and of the right connection and influence for the
161

people at the front-line robs them of their new ideas and enthusiasm, and also
results in pockets of innovation going on locally and in isolation. Within the
context of this study, participants first described a new and attention-grabbing
concept referred to as ‘free spaces’ as a coping strategy for balancing
workload, psychological effect and innovation outcomes.
The construct of free spaces began in the movements for democratic change
in America. For example, the African-America churches that led the civil rights
movement in the 1950s and 1960s promoted collective action that prohibited
discrimination and ended segregation. Free spaces are seen in the today’s
media where the press challenges the diversity of thoughts, and using
feedback, it sends innovators into a perpetual cycle of questioning,
observation and experimentation. Thus, it keeps the society in a “beta state of
perpetual equilibrium-disequilibrium, between harmony and turbulence,
always looking for something new, some fresh solutions to vexing old
problems” (Batra, 2014, p. 56). Evans and Boyte (1986) and Fantasia and
Hirsch (1995) defined free spaces as “social settings that are insulated from
the control of the elites in a social system and therefore invite the voluntary
participation of the subordinated and ready them for collective action” (as
seen in Rao and Dutta, 2012, p. 626). Participants within this study described
free spaces as an environment in which frontline staff are encouraged to
make bold speeches, are left alone to engage in conversations about the
problem at hand, and conduct endless experimentation leading to potential
solutions, and also come up with associative future possibilities (Batra, 2014).
This proposition is supported by research. An empirical study conducted
across two Belgian acute care university hospitals showed that nurse
managers who engaged nurses by “getting them to express their opinions or
to speak up through talk or reflection with colleagues or the nurse manager; to
grumble and complain and to laugh and weep” create a more balanced and
supportive psychological work environment that impacts innovations and
improve patients’ care and well-being positively (Van Bogaert et al., 2017, p.
9). The participants explained that autonomy within spaces helps to create a
culture of differing thinking, nonconformity, resistance to peer pressures, and
foster interaction and collaboration (Kellogg, 2009; Lichtenstein et al., 2006;
162

Oksanen and Ståhle, 2013; Batra, 2014). While free spaces might exclude the
control of dictatorship, participants also commented on the positive effect of
leader inclusiveness by saying that the “words and actions exhibited by
leaders that invite and appreciate others’ contribution” build psychological
safety and promoted innovation efforts in healthcare teams (Nembhard and
Edmondson, 2006, p. 941). For example, leaders can help to nurture and
sustain free spaces by congratulating and not sanctioning people whether an
attempt fail or succeed; and by providing constructive feedback/criticism along
with nurturing spaces through resources allocation (i.e., training), and formal
appraisals (Hughes, 2010; Jacobs et al., 2015; Tappen et al., 2017).
Interestingly, the participants suggested a theme which is gaining recognition
within the NHS context in recent times and is new in the body of innovation
management literature for healthcare services research. This theme is known
as ‘Dragon’s Den.’
The changing and difficult financial state of the NHS often poses a barrier for
staff with a new idea and seeking for funding to support innovation and new
ways of working (Mazhindu and Gregory, 2015). Unfortunately, most of these
new ideas sit under the radar of chief executives, and as a result promising
ideas and innovations can easily be overlooked and abandoned (NHS
Confederation, 2015). One method offering to become accepted as a means
of allocating funds, encouraging staff engagement, embracing and supporting
creativity, and developing innovation for research is Dragons’ Den (Duffin,
2011; Faragher and Williams, 2014). The Dragons’ Den, which resembles the
popular BBC television series, has been adapted in many sectors for years as
a drive for stimulating innovation, creative thinking and assessing innovations.
For example, the organisation responsible for London Transportation known
as Transport for London (TFL) introduced the Dragons’ Den scheme to
promote better services (Transport for London, 2018). A number of
universities in the UK have also adopted the Dragons’ Den style to award
funding to students for innovative projects (Kingston University London, 2016;
University of Southampton, 2018; Durham University Business School 2019).
The Dragons’ Den approach gives innovators the opportunity to propose their
ideas in front of key NHS decision-makers, such as CCG’s management
163
executive team, governing body members and other key stakeholders from
the healthcare community, also known as the ‘Dragons’ in order to win
funding for projects to improve services (Duffin, 2011). Unlike the television
series, the Dragons do not demand a percentage of the innovator’s profit in
exchange for financial support and mentorship. Instead organisations offer an
evaluation of the innovation in an NHS environment, which following a
streamlined process may result to procurement and possible commissioning.
Two of the well recognised NHS organisations that have successfully adopted
the Dragons’ Den style initiative and are pioneers in using this technique to
find new and cutting edge ideas are: Salford Clinical Commissioning Group
and NHS Oldham Clinical Commissioning Group (NHS Confederation, 2015).
Both Trusts have reported outstanding ideas in terms of the number of
innovations it has brought forward and from among which they have short-
listed the ideas that gained the Dragons’ vote in their corresponding Dragons.
The trusts have also funded the evaluation of their innovations in the relevant
healthcare environments. The Dragons’ Den initiative style in healthcare is
opening up a world of opportunities for both healthcare and the NHS
marketplace. For small or medium sized organisations that usually find it
difficult to get their foot into the doorway, this initiative has provided the
opportunity to compete for a funded evaluation of their innovations in the
healthcare setting. The initiative is engaging and helping to set a benchmark
for best practice, and create an innovative spirit among NHS staff (NHS
Confederation, 2015).
Participants further broadened our knowledge on the contextual elements for
driving and maintaining an organisational state of readiness culture. They
talked about the recruitment challenges faced across the NHS and how hiring
the right individuals with the right skills and abilities play an essential part for
enabling a continuous innovation culture. According to one of the participants’
“you have to be able to turn people down that do not fit the same values .” The
findings showed that readiness thus requires an NHS that moves away from
its traditional model to a mandate that is daring and innovative, supporting
new ways of working through recruiting innovative people (Northern Devon
Healthcare NHS Trust, 2015). However, the findings postulate the need to
164

promote diversity in skillset and opinions in order to achieve the right balance
in the workforce. This view is congruent with the literature as empirical studies
exploring knowledge translation between diverse and homogenous groups
have revealed that the project teams encompassing multiple disciplines had
different types of knowledge to continually draw on insights and that they also
demonstrated flexibility in how their roles were enacted (Evans and
Scarbrough, 2014). This finding is further supported in complex adaptive
systems thinking which postulates that self-emergent higher-order learning
and behaviour that leads to innovation and organisational adaptability are
triggered through interactions amongst diverse agents within spaces
(Anderson, Issel and McDaniel, 2003; Englehardt and Simmons, 2002;
Lichtenstein et al., 2006). Contingent upon this, one of the participants
explained that ‘branding’ could be used to strengthen effective recruitment
strategy in the NHS. Understanding why there is a need for branding in
positioning the public healthcare sector for innovation is remarkably new and
distinct from the existing organisational readiness literature. Branding is
“beyond a name or a slogan, it is the summation of all of the benefits that
uniquely relate to a brand organisation – in this case the public healthcare
system” (Gapp and Merrilees, 2006, p. 173). The participant explained how
externalising the NHS brand can serve as an effective marketing and
communication tool to support potential employees in seeing how working
with the NHS can benefit them (Gapp and Merrilees, 2006). According to the
participant, branding helps to “attract really strong graduates and make them
aware that good things happen here.” Thus, it influences the perception
external stakeholder groups hold of the organisation’s brand (Punjaisri and
Wilson, 2007). To implement successful brand building, the participant
suggested engaging with academic institutions such as universities as a key
instrument. In fact, Northern Devon Healthcare NHS Trust have employed this
innovative strategy in dealing with challenges encountered in recruiting certain
staff groups, such as registered nurses, medical staff, and support workers.
The Trusts partners with local universities and has successfully established a
care academy with local colleges to support the inclusion of internships and
apprentices. This was done to further increase its presence in the labour
market and to promote careers within the NHS and to inspire college and
165

university graduates to consider healthcare as a career option, thus engaging
with the potential younger workforce and ensuring a prospect workforce
pipeline (Northern Devon Healthcare NHS Trust, 2015).
The findings further increased the awareness of the need for internal
marketing as a management strategy in creating organisational readiness for
innovation. The approach of internal marketing is based on employees being
treated as internal customers who must be just as aggressively persuaded
about the organisation’s goals as the external customers (Varey and Lewis,
1999). It is the process of promoting and communicating the brand internally
to the employees (Gapp and Merrilees, 2006). As Kotler (2000, p. 22)
suggests, “internal marketing must precede external marketing. It makes no
sense to promote excellent service before the organisation’s staff is ready to
provide it.” Though the findings did not give explicit detail on how to internalise
the branding movement, this topic has been covered in the literature and will
be considered in minute detail for the purpose of providing recommendations
for moving the NHS towards a state of readiness for innovation. The concept
of internal marketing is that employees must be trained and motivated to
recognise the needs of the customer (Varey and Lewis, 1999). For example,
Apple has a unique organisational culture that accentuates innovation,
consequently, their process of recruiting new people is highly selective and
extremely thorough when they provide training. Apple recognises that the
most effective approach to promoting the image of their brand is for every
employee, particularly the ones who serve in the shop floor, to perfectly and
positively epitomise that image as a whole. Everybody who has been to an
Apple store knows that employees who attend to customers are willing and
prepared to provide answer to an endless number of questions. In the same
manner, the NHS can train its staff to project the vision and goals for
accelerating innovation in new ways of delivering care. Within the study, the
participants’ advised senior managers to provide incentives for their
employees in order to engender their commitment and build brand-supporting
behaviour (Punjaisri and Wilson, 2007). Comment from one participant in
particular suggests the adoption of non-financial incentives such as employer-
sponsored degrees to fund employee-students who wish to secure higher
166

learning (i.e., master-degree level courses). The findings strongly suggest that
the public healthcare sector will need to invest in resources to communicate
its brand externally and make its present employees brand oriented. Thus,
more attention should be given to addressing the environment in which NHS
staff and leaders operate to help ensure its jobs are attractive in future.
The findings also shared new insight that might challenge traditional
curriculum approaches in educating undergraduate medical and nursing
professionals. A forward-thinking attitude with a focus on the integration of
innovation core skills into medical and nursing school programmes should
increase the potential for a sustainable innovation ready culture. The findings
established that such an approach would produce a cultural mind-set for
students to see innovation as part of the NHS core values. This should
produce a sense of readiness and a new type of skilled medical graduates,
prepared and able to deal with the challenges of a rapidly changing health
sector as well as to find new ways to meet the increasing needs of future’s
patients (University of Surrey, 2018). A good example of this is the way that
the University of Surrey medical school has designed an innovative
curriculum, integrating digital and communication health technology, and
organisational leadership. The aim of this is to enable medical students from
the first day of their foundation programme to be aware of the implications of
technology in delivering better patient care, and to produce graduates who are
able to drive change, lead multidisciplinary teams, and organise the delivery
of healthcare using big data and the latest technology (University of Surrey,
2018).
The frequent reorganisation of the provider and the commissioning landscape
was said to pose a problem for achieving systems change. Participants
highlighted the fact that the high turnover in the NHS is a problem that needed
to be addressed, and they went on to prescribe longer leadership tenures and
consistent innovation approaches as an enabler for greater commitment
towards innovation among the staff base (Baker, 2011; Ham, 2014;
Anandaciua, Ward and Randhawa, 2018). Participants expressed the view
that high performing trusts that show the value of leadership continuity and
167

stability, the employees tend to experience a clear vision and goals for
improvement. Participants gave examples of trusts such as the University
College, London and Suffolk Hospital which have succeeded in driving
continuous innovation through stable leadership.
The findings additionally suggest that ‘future anticipation’ is a condition for
enabling readiness based on principles applied in the non-healthcare
innovative sector. Participants pointed to the private sector and how it stays
innovative by engaging with pioneers to obtain forecasts for future directions.
The literature labelled such tactics as forecasting strategy which is a
“surviving behaviour” that allows organisations to leverage their established
links to gain important information to help them stay abreast of the latest
trends and to reduce leadership uncertainity about the legitimacy of new
technologies (Goes and Park, 1997). This proposition shares several
characteristics with open-innovation literature as authors in this field suggest
that the greater innovation potential coming out from relationship
management is the results of the opportunity to leverage knowledge
resources in their process (Bullinger et al., 2012; Reinhardt, Bullinger and
Gurtner, 2014; Tani, Papaluca and Sasso, 2018).
The findings further identified no real significant differences in the skill set for
and the approach reuired for managing organisational readiness in public
healthcare, versus private healthcare sector and other industries. The
difference is that the latter are more open to innovation because of the context
of their operation where there is constant competition between companies.
Innovation in the healthcare sector, especially because it is public, encounters
complications due to the interdependencies across systems and subsystems,
and a lack of clarity on innovation procesees (Barlow, 2011).
Participants explained the role of effective partnerships in driving an
innvoation readiness culture. Based on systems thinking theory, innovation
spans across different sub-systems within a whole system and it is their
interaction that creates a response that leads to adaptive outcomes. Systems
thinking has made us aware that the connection between people in a system
is facilitated by the quality of their relationship and the effectiveness of the
168

communication and processes integrated to plan and coordinate the
distibuted responsibilities the individuals undertake collectively (Lichtenstein
et al., 2006; Dattee and Barlow, 2010; Atun, 2012). Similarly, participants
expressed the view that if the NHS is to engage in successful organisational
readiness for innovation, then good relationships are important. According to
a participants, “an organisation is an organic organism and people matter.”
This metaphor moves away from the goal-oriented social entities view to a
holistic approach in order to determine and identify the interacting processes
that need internal balance as well as in relation to the external environment
(Marion and Uhl-Bien, 2001). Even as organisms are made up of interrelated
parts and organs, so organisations are made up of interrelated sub-systems
that rely on each other to adapt to environmental circumstances, maintain the
functionality of the system and ensure its evolution, sustainment and
improvement. Participants emphasised the point that implementing successful
organisational readiness for innovation relies on a combination of
interferences and interventions working together holistically across all
healthcare settings (Joseph-Williams et al., 2017). First is the quality of
relationships across patient group and the wider population to help them
understand their experience, the difficulty they face in accessing the service,
what needs to be change, and how to go about making these improvements.
This proposition is in line with Rogers (2003) diffusion of innovation theory
which suggests that an innovation that does not meet end-users needs is
likely to be rejected, no matter the intended benefits. The determination to put
patients at the centre of the NHS has been unanimously accepted in the
aftermath of the Robert Francis’s report on the failings at the Mid Staffordshire
(Flott et al., 2017). The need for a coordinated approach and a concerted
effort for gathering data on patient experience at clinical, organisational, and
policy levels, and advise for its use in an effective way to stimulate
improvements has been explored in the literature (Reeves, West and Barron,
2013; Coulter et al., 2014; Flott et al., 2017). The responsiveness of health
providers and healthcare systems to patient’s experience is crucial to all users
of healthcare as this will provoke pioneering approaches to quality
improvement (Flott et al., 2017). The next set of stakeholders group
successful readiness relies upon is the clinical workforce. The findings
169

highlighted that the effectiveness of communication with the clinical workforce
can help to change their attitudes and assumptions by engaging them in
genuine discussions and shared reflection that can help build trust and
facilitate more collective creativity (Josephs-Williams et al., 2017). Finally, the
findings underlined the importance of building partnership with the AHSN to
explore the possibilities and the know-how on making improvements.
5.7 Chapter summary
The aim of this research was to differentiate between innovation and
organisational change, and to uncover representations and the facilitators
instrumental to the conceptualisation and deliberations about readiness by
describing the concepts that shape an organisation’s innovation state of
readiness in the public healthcare sector. The first main point is that
innovation is different from organisational change. The participants were clear
in distinguishing innovation from organisational change based on these four
premises: goodness, dynamism, positivity, and newness. New ideas were
articulated as a by-product of constant engagement and interaction with
people and their organisation. Readiness was conceptualised as the overall
physical and mental state of being, the ubiquitous culture of the organisation
and its operating climate. Many of the studies on organisational readiness
have weaknesses when applied to culture. Although there are many works
about the cultural-related elements, the connection among the interrelations of
the components of organisational readiness is still absent as well as knowing
how to help sustain the momentum of readiness among healthcare services
providers, their service users and care givers. If organisational readiness for
innovation is to be considered as a cultural phenomenon, then there is the
need to take a whole systems and constructionist approach to ascertain
clearly the kinds of variables that will lend themselves to specific
measurement and hypotheses testing. The findings showed readiness needs
to be conceptualised as an on-going process directed at innovations, learning,
relationship, abilities and adaptabilities. The participants’ discussions were
centred on three key dimensions: iteration, space and its impact on the
organisational behaviour towards readiness, and the responsibility of
170

leadership in enabling the space. The follow-up study will now consider the
processes for enabling iteration of readiness within interactive spaces, and
the role of leadership as the context changes over time. In doing this, there is
no better organisation to seek such evidence than the Academic Health
Science Networks. The study will have a primary agenda to encourage
innovation adoption in the NHS by enabling and driving spaces for knowledge
sharing and mobilisation. The study will have a different perspective – by this
external viewpoint, which will contribute new knowledge on a continuous
process-based perspective of organisational readiness for innovation.
171
Chapter 6
Exploring the enabling factors and processes underlying an innovation readiness state of being:
The outer context
6.1 Study Aims
The empirical study conducted in Chapter Five by the researcher made use of
a qualitative methodology to explore how different stakeholder groups (chief
executive officers and directors) in the NHS involved in the management and
facilitation of the innovation implementation process perceived the construct
of organisational readiness for innovation, the meanings associated with
readiness, and the factors that both hinder and enable readiness.
The findings from this study showed that organisational readiness for
innovation in the inner organisational context is best conceptualised as
multifaceted with interactions and a sustained phenomenon through a series
of iterative nonlinear processes which enable an organisation to be able to
self-adapt continuously to changes in practices. Organisational innovation is
slightly more complex than managing organisational change because the
former requires professional association, collaboration and knowledge
creation. Apart from this, innovation requires a wide range of additional
adaptations in order to address the complexities that might arise. For
example, if a political or regulatory directive changes, an organisation must
shift its model to adapt it. The findings from the previous study indicated that
space, described as an environment, was an important condition for readiness
for innovation. In addition, another recurrent theme was the significant role of
top leadership in enabling the context in which organisational members
interacted.
In light of these findings, a further qualitative study was carried out to explore
the views of stakeholders working in an organisation that plays an important
role in the spread and adoption of innovation and to relate the findings to NHS
172

staff, health and social care professionals, businesses and other
organisations who are also looking for improved ways to working. The study
aimed to bolster credibility by providing a thorough validation of the narrative
accounts and to highlight differences in perspectives across stakeholders and
across organisational innovation contexts, both (inner and vs. outer. context).
Validation is useful to inform the development of a framework to conceptualise
and enact organisational readiness for innovation in health services delivery
organisations (Attieh et al., 2013).
Research has shown that knowledge gained from an external standpoint is
extremely relevant when trying to develop organisational strategy to enhance
the creation and adoption of innovative solutions (Bailey, 2010). Accordingly,
this study explored the perspectives of the senior managers from an
innovation facilitator, namely, the Academic Healthcare Science Networks
(AHSNs). AHSNs were established in 2013 to help spread innovation rapidly
and on a large scale in order to improve healthcare services and generate
economic growth (The AHSN Network, 2017). The AHSN is the first port of
call for people who are attempting to do innovation across the pipeline in NHS
England. Acting as catalysts, AHSNs support innovation in healthcare by
helping to spread best practices and by creating an infrastructure and the right
conditions to enable the adoption and diffusion of innovation across health
and social care economies with a clear focus on improving patient outcomes
(Hose, 2016). There are 15 regional AHSNs across England and each
network differs in its structure and operational approach based on their local
health and social challenges and priorities. The AHSNs are:
East Midlands
Eastern
Health Innovation Manchester
Health Innovation Network
Imperial College Health Partners
Kent, Surry and Sussex
North East and North Cumbria
Innovation Agency: Academic Health Science Network for Cumbria
Oxford
173

South West
University College London Partners
Wessex
West Midlands
West of England
Yorkshire & Humber
In the present study, representatives were interviewed from three different
AHSN organisations. Two of the organisations were based in London and one
in south east of England. The three networks were selected for easy
accessibility as the researcher resided in London. In addition, each of the
networks brought unique and distinctive capabilities to the wider collaboration,
and through partnership they were making an impact on the wider population.
To achieve the study aim, the perspective of senior managers within these
three AHSNs was sought by means of qualitative interviews. The research
questions explored were as follow (see Table 6.1).
174

Table 6. 1: Research study questions, aims and exempla interview questions
Research questions Study aims Exempla interview questions
1. Which factors AHSN senior managers perceive as enablers of an innovative organisational culture, and how do they influence readiness?
To identify the interactive conditions that foster an innovative and a productive future, and understand how to create the time and space, and spawn innovative self-organising behaviour among staff.
How can a culture of innovative champions be created within the NHS?
2. How do AHSN senior managers describe the role of leadership in creating a continuous state of readiness?
To explore how leadership creates the conditions in which continuous readiness is produced.
What is the role of leadership in increasing capacity and attitudes towards innovation amongst staff?
3. How can the NHS learn from other sectors?
To ascertain strategies and recommendations in moving the NHS innovation landscape forward.
What can the NHS learn from organisations that have succeeded in creating a culture of innovation readiness?
175

6.2 Method
6.2.1 Participants
Each participant belonged to the management hierarchy of their organisation
and they were purposively selected in order to fulfill the main objective of the
research which was to explore the perspective of the managers in their
capacity as leaders. Ten participants in total formed the sample size in this
particular study. The ten participants comprised of six males and four females
(6:4), and this was not deliberate, but rather subjected to their interest in
participating in the study. The participants were deemed to possess the
knowledge and expertise required to explore the perimeters of this research
(see Table 6.2 for rationale for choosing the participants). The participants’
remained anonymous in order to comply with the confidentiality agreement
stated on the consent form. Instead of their names, the participants were
represented using only codes such as chairman, improvement manager, and
directors (see Table 6.2 for the demographic background of the participants).
6.2.2 The interview schedule
The interview schedule acted as a guide for answering the study questions.
The aim of the interview was to examine the enabling processes towards the
development of a continuous innovation culture. Generally, the length of the
interview was approximately 21 minutes to over an hour and varied across
each interview. For instance INV 11 length was 39 min; INV 12 was 1 hr. 45
sec, INV 13 was 1 hr. 12 minutes; INV 14 was 54; INV 15 min was 43 min;
INV 16 was 38 min; INV 17 was 26 min; INV 18 was 45 min; INV 19 was 39
min; and INV 20 was 21 min. The duration of an interview impacted on the
quality of data gathered. Interviews that lasted for less than 30 minutes lacked
the depth of knowledge compared with the others that lasted over 30 minutes.
However, the researcher had no control over the situation as, for instance, in
cases INV 17 and INV 20, the participants had prior engagements and were
constrained by time. The time during the day when interviews took place
varied and most interviews were conducted in the morning or early afternoon.
176

Table 6. 2: Demographic characteristics of participants
Participant number
Stakeholder group Type of Organisation Gender Years working in the AHSN
Rationale for choosig participant
11 Chairman Academic Health Science Network
♂ 5 With over 25 years of business experience working at board level for blue-chip organisations, participant is in charge of fostering adoption and enhancing the greater spread of innovation across affiliated networks.
12 Improvement Manager Academic Health Science Network
♀ 4 With a strong track record for leading multidisciplinary teams in change improvement programmes across public and private sectors, participant is responsible for building quality and service improvement for patients, carers, and the public.
13 Director of Innovation and Reasearch
Academic Health Science Network
♂ 4 This participant has 17 years in general management role within the NHS, alongside an expert in managing and improving services, and leading organisation. Participant is presently in charge of engaging with industry and improving engagement between industry. Also directly in charge of applying a process that was developed in his AHSNS to other AHSNs.
177
Table 6. 2 continued: Demographic characteristics of participants
Participant number
Stakeholder group Type of Organisation Gender Years working in the AHSN
Rationale for choosig participant
14 Clinical Director Academic Health Science Network
♂ 1 Participant is presently the only clinician across the fifteen AHSNs that leads patient safety collaborative program.
15 General Manager Academic Health Science Network
♂ 5 Responsible for providing support and improvement in performance, and aid to accelerate the spread of best practices and innovation.
16 Medical and Divisional Director
Academic Health Science Network
♂ 1 With over 30 years experience working as a physcian and consultant cardiologist in the NHS, participant has sat on National Guideline Committee, the Education Committee of Royal College of Physicians, and National Association of Clinical Tutors. Having long standing experience and strong expertise in the field of clinical and managerial care, participant is knowledgeable about directing staff, coordinating change and leading organisational readiness.
17 Director of Commercial Development
Academic Health Science Network
♀ 4 With academic expertise and commercial background, participant is in charge of devising ways in which innovation can be
178
converted into practice.
179
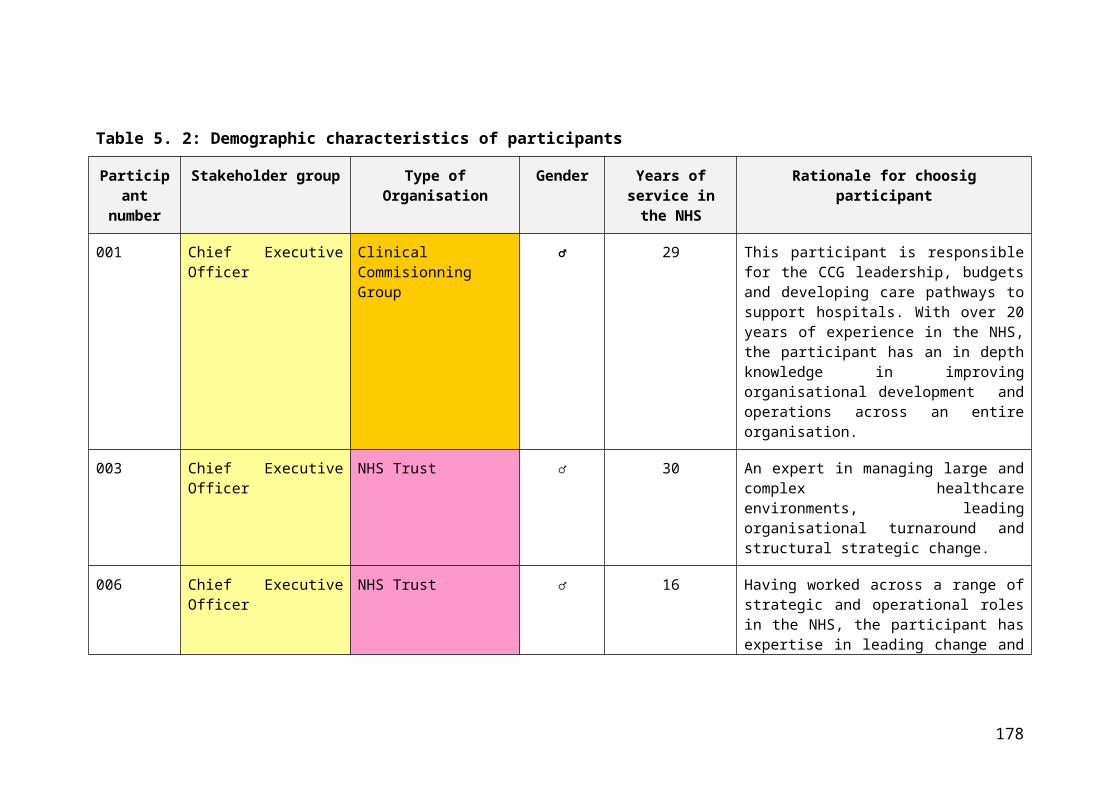
Table 6. 2 continued: Demographic characteristics of participants
Participant number
Stakeholder group Type of Organisation Gender Years working in the AHSN
Rationale for choosig participant
18 Director of Capability Development
Academic Health Science Network
♀ 5 Participant has diverse experience working in operations within acute trusts, and is presently in charge of leading improvement and leadership, helping organisations to have a shift in mind-set to support improvement.
19 Direction of Innovation and Implementation
Academic Health Science Network
♀ 5 A lead director in providing support across the organisation, building partnerships to increase the pace of innovation diffusion through pull and peer-to-peer horizontal approaches.
20 Medical Director Academic Health Science Network
♂ 5 With an expertise in academia and business development, respondent is in charge of overall business strategy setting, business and commercial development and intellectual leadership by working with a variety of partners at a national and international level.
180

181

The interview started by asking participants to elaborate on how their role
within the Academic Health Science Network had evolved over time. The
findings from the previous empirical study in Chapter Five indicated that time
and space were associated with innovation. Therefore, the researcher
decided to include this question in order to obtain more information on the
relationship between time, space and a culture of continuous innovation. This
question was also used as a probe for identifying other conditions that
influenced innovation. The question about what factors enable innovation
activities was included to examine the practices and structures in place that
provided time for the development of an innovation culture. If not already
mentioned by the participants, the role of leadership in increasing the capacity
for innovation was asked. The final question about the lessons that could be
learnt from external innovators was considered in order to try and identify
effective principles and practices used to facilitate innovation.
6.2.3 Data collection process
The interviews were conducted face-to-face and were expected to last
between 30 minutes to one hour as stated in the information sheet that
provided brief and clear information about the specifics of the study. In some
situations, the interview extended beyond an hour as participants became
engrossed in the conversation. On the day of the interview, participants
signed a form affirming their consent to participant and be audio-recorded
during the interview. At the end of the interview, participants were thanked
and asked if they had any questions pertaining to study. Some participants
also identified other persons within the Academic Health Science Networks
who could be interviewed. The researcher wrote a synopsis of each interview
almost immediately afterwards and the interview was transcribed and then
analysed using the analytic process stated in Chapter 4 (see Appendix J for
one complete transcribed interview).
6.3 Reflections of the researcher on the interview process
Following the previous study on the NHS, the researcher had a better
understanding and prior knowledge of the different actions to take in reducing
182
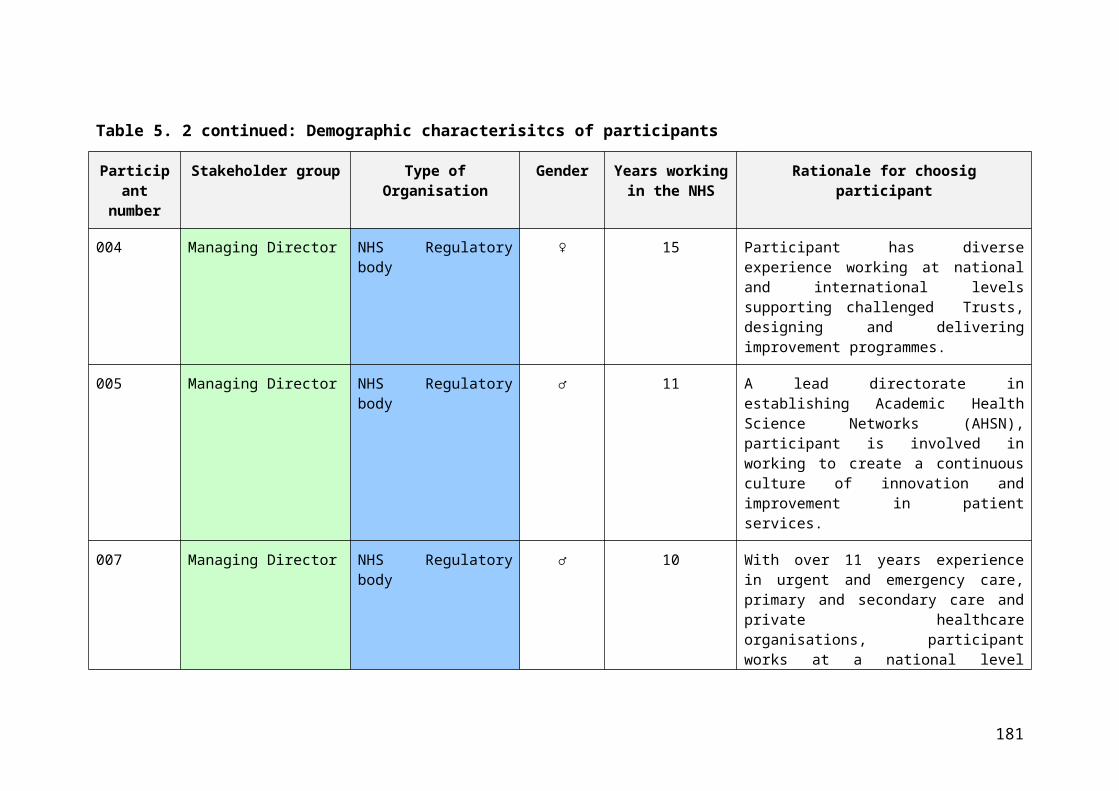
the effect of power dynamism between participants and researcher. One of
unavoidable challenges was the issue of noise whenever the interviews were
conducted in a café. The sounds from the people and the coffee machine at
times interrupted the flow of information. The participants had to listen
carefully to be sure of what was being said and during the transcription of the
interviews, the recording had to be played repeatedly to extract the correct
information.
6.4 Results
The results from the analysis generated many themes which were later
divided into three main master themes related to all the three previously
stated aims. Within each theme, a number of sub-themes were identified
which will be discussed in detail below. It should be noted that although the
master themes are presented separately, they are interrelated. Excerpts from
the interviews are included to support each theme presented. The three
themes were:
1. Enhancing and enabling processes for an innovation driven culture
2. Leadership, what about it? And its role in enabling a culture of
innovation
3. Catalysing readiness - what can we learn from the innovators?
6.4.1 Enhancing and enabling processes for an innovation driven culture
Under this first broad theme, the participants discussed their perspectives on
how to enable a culture for continuous service improvement and innovation
readiness. This section consists of seven sub-themes, namely:
1. Perpetual movement in context
2. Time and Space
3. Leadership buy-in
4. Systems thinking
5. Communities of practice
6. Partnership working and relationships
183

7. Mandated learning
(see Table 6.3 for a breakdown of the 1st order concepts, 2nd order themes
and aggregate dimensions).
184
Table 6. 3: Themes and sub-themes on enhancers and enabling processes for an innovation driven culture 1st Order Concepts 2nd Order Themes Aggregate Dimensions
“Go around in cycle trying to revevaluate what you need to be doing” (14/203)
“Humble enough to recognise the need for improvement, and ambitious enough to address that need for improvement” (15/159)
Constant (Re) Evaluation for Proactive Response Perpetual movement in context
“Prioritise its time for its staff” (15/162) “Create a safe space for failure” (14/290)
Time and Space for Sucess and Failure Time and Space
“It starts from the top and takes years” (18/203)
“It starts at the top” (20/100) “Concerted effort to shift the culture”
(18/203)
No Quick FixVs
Concerted Effort
Leadership-buy in
“Measure as you go along” (14/369) “Reward and recognise” (19/103) “It is actually worse to give someone false
expectations” (17/251)
Managing Performance and Expectations
“We need those that are passionate” (16/587)
“Out with the dead wood & in with new blood” (12/394)
“Can everyone play a different role” (13/507)
Champions&
Role Diversity
185

Table 6. 3 continued: Themes and sub-themes on enhancers and enabling processes for an innovation driven culture1st Order Concepts 2nd Order Themes Aggregate Dimensions
“These things are happening but we need to be transparent” (17/266)
“What problem are we trying to solve” (20/176)
Transparency & Problem Understanding Systems Thinking
“You become more of a community” (14/243)
“You work for rather than you work with” (14/20)
United Will
Communities of Practice “Support the grassroot sort of proposal”
(14/256) “Can be devolved or centralised” (20/132)
Devolved SystemVs
Fit for Context “A neutral voice enables” (18/138) “Competition drives performance” (13/98)
CompetitionVs.
CollaborationPartnership Working & Relationships
“Redeploy and retrain” (15/212) “Have a bit of time in a different industry”
(18/442) “Integreate into undergraduate cirriculum”
(15/249)
Continuous Workforce Development Mandated Learning
186

1. Perpetual movement in context
An innovative organisation, according to the participants, was one that
constantly needed to experiment and keep up with the changing demands in
order to stay ahead. This process required a systematic and constant (re)
evaluation of organisational objectives. Organisational members must pay
attention to the internal capabilities and the external organisational needs and
demands for improvement with feedback from the environment to serve as an
impetus. In addition, a proactive and timely identification of the need to
change was an essential first step towards continuous improvement.
So I think it needs to be, if I was visualising my ideal organisation or a system, it would need to be very responsive. And I think that that's responsive in two ways. That's responsive to what's going on around it or the need to the organisation itself. So these things are never static. You are always permanently going around in a cycle trying to re-evaluate what you need to be doing.
(Clinical Director, 14/234-238)
So one that is humble enough to recognise the need for improvement, and ambitious enough to address that need for improvement… and open-minded enough to look outside of its own organisation for solutions.
(General Manager, 15/158-160)
However, one of our participants argued whether an organisation’s culture
that embraced innovation depended also on contextual factors, such as
financial and human resources. He qualified his comment using an example
of how he had helped Hospital X improve quality care and deliver faster
services through upscaling. However, when there was a slight squeeze on
finances, a manager ordered that the skill mix be reduced. In this example,
limited resource prevented the mobilisation of structural capacity (material
resources) and social cognitive resources (readiness and potential
commitment) to facilitate innovative action. Therefore, context plays a critical
role in shaping organisational capacity and its ability to respond to calls for
continuous innovation.
We have to differentiate between context and content…. So this is a policy issue of, we want to support innovation and we talk about giving people time and space and supporting an innovative culture, and yet,
187

our performance management process is still around organisational efficiency and outcomes. So it is not down to the individual organisation to be innovative. And they, because of the context, might simply squash the innovative opportunity, if you have no cash, or the way that your organisation is managing cash, you will remove the, I forgot what the term that Trish uses, slack resources, if you remove all of the slack resources you haven't got it. …. It's a combination of context and capability or content.
(General Manager, 13/378-415)
2. Time and Space
Some participants expressed the view that the lack of space and time for
people to be innovative in their approach made it difficult for them to
understand the issues their organisation faced and to create solutions on how
to deal with the problems encountered. Generally, time appeared to be the
biggest barrier at the moment for staff working in the NHS to engage in
continuous improvement initiatives. Participants also felt that innovation was
generally not something that was considered as very important in the NHS.
Participants were concerned that issues, such as increased pressure to
deliver their operational job, and an insufficient number of staff reduced the
time to think about how the work needed to be done.
Time is the key bit. So if you look at the industry’s approach to innovation, it is very much creating time and space for people to have an opportunity to step back and question or be questioned about the way that they are working on how it could be better. We just don't have that time built into the way that we work so we are always working at such an incredible pace.
(Clinical Director, 14/313-317)
And having the time to actually put your head above that and think about doing things in different ways is difficult unless you are directly told that you need to do it or it is in eighteen weeks that you need to implement or the 4 hour wait in A&E and things which make you realise you have to go do, you have to think about things in different ways. But I think time is the biggest issue because everybody is so stretched. I think the fact that innovation is generally not something that is being always prioritised.
(Director of Innovation and Implementation, 19/117-122)
I think having the space, people are so flat out and staffing is so difficult that quite often people try and dedicate time to stuff, but can't.
(Director of Capability Development, 18/254-255)
188
One of the surprising findings from the study was that low productivity, a high
rate of absentee and sick leave, failed recruitment, and low retention of
employees were all indicative of the organisational culture and seemed to be
associated with the lack of time and space dedicated to innovate. On the
other hand, when workspace culture was created, organisational members
began to feel valued and there was a potential for an increase in net
productivity.
We just don't have that time built into the way that we work so we are always working at such an incredible pace. But there is an opportunity that, and in some ways the cycle can be broken by improving the environment in which we work and the way in which we work because a lot of our sicknesses, both real time sickness and retention of people within and recruitment into working environments is a relatively useful thermometer of what the culture and organisation is like…. So if you are failing to recruit people or keep people in roles or you have a relatively high rate of, you know, either short term or long-term sickness in the organisation that tends to be a marker of poor culture. And ironically, there's reasonably good evidence I've seen that shows that by improving the workspace culture and the value of the organisation for their workers, you bring all of those measures into an improved arena and actually your net productivity will go up. But what we don't tend to do, we don't tend to invest in our work, you know, in our colleagues so they don't feel valued, they just feel harassed.
(Medical and Divisional Director, 14/319-330)
However, when it was impossible to tackle the work place demands, the
participants felt that the leaders should create a sense of space and set
expectations for their team or organisation. In one participant’s own words, “…
good leadership creates that bubble that allows people to flex, within reason”
(14/629). The approach required was that of prioritising innovation as part of
the way of working and managing it within a kind of strategic environment.
The result would be a sense of real time experimentation, such as testing if
the proposed innovation was applicable and useful and then finding new ways
of doing things and championing these. In addition, the other approach was to
get people to experiment in real time. Part of allotting time was to create
opportunities within the week where doctors or nurses who were not in clinics
or doing rounds on the wards had time and space allotted for thinking about
innovation.
189

You know, can you find time to sit and innovate and think? Well, you should be able to and again, even in the middle of the winter, the space allocated within a consultant’s timetable, in particular, and the registrar's timetable, and the junior doctors, there should be space allocated.
(Medical Director and Divisional Director, 16/273-275)
Participants also talked about allowing people to understand that it was alright
to fail. A participant expressed how a fear of failure crippled many individuals
from being innovative. The participant’s observation was that given the
psychological and organisation’s considerations, negative meaning is
attached to failure and this discourages members of the organisation from
pursuing experimentation and embracing failure. In fact, whenever failure
occurs, it should be seen as an essential part of the innovation process and
needs to be embraced as a learning opportunity.
I think our fear of failure in the NHS is so high and there is just absolutely no flexibility with that. I think that is where things cripple a lot of individuals.
(Director of Commercial Development, 17/346-348)
You are getting people to do these stuff in real time so you are really actually starting to try things out. There's a sense that you know you can do it and fail and that's okay. Failing is kind of useful… One of the things I really tried to create at BSUH, and I think it is really important, is to create a safe space for failure; it's a really difficult thing to do….
(Clinical Director, 14/412-590)
I think a lot of things don't get implemented mostly because no one wants to make that decision, they don't want to be wrong. And I think there just needs to be more of a safe place for people to try ideas.
(Director of Innovation and Implementation, 19/193-195)
There is the need to create an environment that provides the opportunity to
learn from failure as this can produce effective new solutions. There must be
some rigor built into the systems and processes in order to increase the
identification of failure and to reduce its avoidance. Participants stated that an
innovative culture that promotes failure identification should have a system
that supports organisational members and which did not only aim to reveal
their errors immediately, but also provided opportunities for them to share
information on what led to that error. A participant referred to David
190

Brailsford’s strategy of one per cent performance improvements which led
Britain to win Olympic gold in cycling in 2002. The approach was simple and
consisted of recording every decision made, whether a change in diet or the
type of massage gel used on the athlete, and its good or bad effects. Then, he
used all the information to develop a winning strategy. By doing this, the
difference between performances was measured and so it was easy to
identify the factors contributing to improvements and adjust accordingly.
An improver, once they start being given permission, such as, “This is your environment, if you think there is something that needs changing, you have the permission to change it as long as you are able to show what you have done and how you have done it”..…So, actually if we get things wrong two or three times, but we can show how we got it wrong, then technically, we should be able to change it next time so that we don't make the same mistake each time. But most times, we don't measure as we go, so we have no way of picking up what's changed. You know, you are not going to get it right the first time… The David Brailsford approach, the guy who ran the cycling team, the British cycling team, his approach was not a seismic change; it was made by little one per cent adjustments. And then you show the benefits of those one per cent adjustments, and as you go you build up to something that becomes really important.
(Medical and Divisional Director, 14/363-378)
The creation of a space poses difficulty because it allows for greater flexibility,
and the possibility of failure. For these reasons, some organisations or
persons can avoid taking the appropriate course of action related to the
execution of a task. On the other hand, establishing clearly defined
parameters of the space creates a sense of expectation and accountability for
innovation.
If you have made a mistake, then it's something you need to be able to feel comfortable admitting that you have made a mistake and be supported … And equally, the organisation needs to understand that it's not always a singular problem that has happened and look behind that. But equally, that person needs to show some accountability … and you should understand what is the expectation … and there is an expectation that you should report it … I think it is really important to create a safe space for failure; it is a really difficult thing to do well. But good leadership creates that bubble that allows people to flex, within reason. There has got to be some rigour but actually built into that as well, you know, I've got an idea about where I want to get to, but really what I need from you is an understanding of how we are going to get
191

there and that navigation process, you are in control. So if you want to go all the way over there to come all the way back, there’s a good reason and there is some value in it, that's fine. But we still need to get there and we probably need to get there by next year. So the quickest route is this way but it might not be the right way because you know what the problem is between here and there better than I do. So you create that space for people to be innovative in approach and understanding and skilled. So by the time they get to the destination, they understand the issues, the problems they have found, they own the solutions and that’s part of that sustainability, it is that they have solved the problem, and there is a huge ambition in gaining it.
(Clinical Director, 14/276-643)
I don’t think it’s just the space. I think it is having clarity on what the priority is and innovation being part of that. I am being clear on what, where innovation is going to help with the numerous things that need to happen.
(Director of Innovation and Implementation, 19/183-184)
3. Leadership buy-in
Another essential enabling condition for building and sustaining an innovative
culture is the need for innovation efforts to begin from the top. A participant in
the study argued that many Trusts struggle to implement innovation because
the leadership finds it difficult to define innovation. This leads to a lack of a
defined innovation strategy and no definite innovation framework. This
enabler highlighted the fact that the senior leaders of an organisation must
make strategic decisions that emphasise innovation as a priority and adopt a
buy-in approach. This should be based on a set of strategies to disseminate
the vision and build commitment towards continuous innovation improvement.
To effectively use this model, the participant argued that leaders must move
from “quick fix” thinking to one of a concerted effort in order to stimulate the
continuous adoption of the innovation. The participant argued that capabilities
must be built into systems so that people understand the reason why they
need to change what they were doing, perceive that they have the ability to
change, and be able to identify the benefits of innovation.
Well, all our evidence stresses that innovation starts at the top. So if the CEO of an organisation and the executive team have no sophisticated understanding of what innovation means beyond R and D, very little happens. And what you get is a lot of frustration at the frontline and a lot of sort of ad hoc innovation and a lot of duplication, frankly, because the organisation is not just geared up to have a
192

meaningful innovation ecosystem. So what we are aiming for is effectively something where the executive has a very clear vision of what innovation does for the organisation, accepts that innovation doesn't necessarily mean R and D, but it means ruthless stealing of stuff that's already out there.
(Managing Director, 20/99-108)
So the organisations I know that have more of the culture of innovation improvement start from the top and it includes the board, including the non-execs have made a strategic and, consequently, concerted effort to shift the culture of the organisation and that has taken years so this is not a quick fix.
(Director of Capability Development, 18/202-205)
According to a participant, the complex nature of the NHS makes it difficult to
manage the process of innovation because of the many Trusts that work
independently and do things differently. This results in fragmentation, lack of
clarity in the evaluation of the performance of the innovators, and with
innovations considered as advantageous, even when they were not, being
accepted by some Trusts. The participant called on leaders to respond to this
problem by applying intelligence and critical awareness when evaluating
ideas, and by rewarding individuals for performance rather than the opposite.
The participant stressed the need for leaders to effectively manage the
performance of innovators by the implementation of an open performance
appraisal which would allow critical feedback. This should be provided to
innovators in order to further improve the situation. Under such
circumstances, if the feedback was fair, innovators would be motivated to
keep on being innovative. It was also considered important that organisational
members understand the leaders’ expectations and have enough support to
meet them.
We are not great at necessarily managing expectations of innovators. So they need to understand that the pathway, well for starters, it is not really defined, it's not defined because we are talking about an organisation that spans the whole of the UK and even though it is a unified health care system, it's not really…. So our expectation about innovators and them doing great and wonderful things and us being able to push their innovations through the NHS, it needs to be managed a bit better than that. Because we don't want people that have great ideas to not have great ideas and to stop having great ideas, but we need to let them know that when we come back and say, “This is not a good idea and this is not going to work,” that we are
193

not and killing them as in someone with a creative spirit, we want to foster that, but it needs to be managed. We are not great at necessarily managing expectations of innovators. And I've seen far too many ideas that aren't great ideas be carried on just a little bit too far because nobody wants to say that's it bad. Nobody wants to upset anyone and it's actually worst to give someone false expectations as opposed to telling them straight up that it's not something that can be supported. So I think we need to manage expectations and be slightly more critical than what we currently are.
(Director of Commercial Development, 17/249-253)
Engaging champions was perceived as another way of actively enabling
continuous innovation. According to the participants, champions are described
as individuals and teams that are relatively young, and most importantly, they
are good at their jobs and passionate about seeking out new and improved
ways of working and facilitating readiness.
So for me, innovation champions should be in an organisation, individuals and teams that are continuously looking to improve the organisation and ready for change.
(Head of Innovation and Research, 16/587-588)
So, as an organisation they are open to innovation, they have that culture of innovation. I think they have quite a young and dynamic group of clinicians, they have always pushed the boundaries, so they are ready to take on innovation.
(Improvement Manager, 12/262-264)
However, it is the leader’s responsibility to identify champions and engage
them so they are better able to identify and tailor solutions for dealing with
problems. In one example, a participant explained how patient flows and
hospital management respond to the pressures in the Accident and
Emergency department by introducing champions and, thereby, developing
resilience in the work place.
Cause innovation really in health service is not, this is not kind of a real invention, although that happens. It is about innovative, finding an innovative technology and adapting it and making it operationally kind of work properly. So, I think probably rather than the lone kind of pioneers, we need to think about how we can put teams together who can effectively turn that kind of stuff into, if it's a trial, then into operational use.
(Chairman, 11/213-217)
194

In another conversation, a participant mentioned the role recruitment plays in
building creativity and innovation in an organisation. The participant argued
that leaders must recruit the right people into an organisation and keep the
wrong ones out. Doing this would re-vitalise the work environment and bring
in new ideas that could enhance responsiveness to risk-taking. In addition,
there is the need to build innovation into job specifications so people are
aware of the expectations.
Identifying champions has to come from the chief executive and the executive team, if they want to… you know, in terms of the people, it is the investment in the people in that group of, it's getting rid of that dead wood in the organisation, those that don't want to change… Those who are able to take risks and try something. So where you recruit new blood into the organisation, so you look for those. Whether it's part of their recruitment campaign but actually looking for innovation as built into job plans or job descriptions, so in a way you are building health care innovators.
(Improvement Manager, 12/394-400)
However, another participant was not in agreement with the idea that
including innovativeness into job descriptions would necessarily improve
innovation in the work place.
So basically clinicians are asked to do something innovative in the few hours that they have left. That’s not, you know, that's not the kind of ecosystem that we are talking about. We are talking about something that's much more deliberate and we like the kind of concept of Chief Imitation Officers rather than Chief Innovation Officers. Though we don't think that specific innovation roles in organisations are necessarily the answer.
(Managing Director, 20/124-129)
A nearly similar point of view was expressed by another participant who said
that a team also needed to be balanced with a variety of personality types.
While champions were necessary for reinforcing new thinking, he stated that
“it is not everyone’s job to be innovative, we would fall apart if everyone was
creative” (13/506). Creating work group diversity has a direct effect on group
performance as the same participant shared an account on how a
performance test conducted within St Guy’s and Thomas hospital revealed
that because the work team consisted of individuals with the same personality
type, this led to poorer outcomes, as opposed to a group with greater
195

diversity. Therefore, the participant suggested that a culture of innovation did
not mean that everyone had to be looking for new ways of working;
sometimes it was important to have good workers who followed instructions.
It is good for the organisation and for the patients who we are there to serve for us to be a good follower, although we don't want slavish followers. We want people who will follow intelligently and are also encouraged to say, "That doesn't work" or, “here is why it doesn't work. May be if we did this.” So everyone can play a different role in the innovation process… So have we got the mix, the factors in the team right? Or have we got a team full of the same people and do we encourage lots of the same people in our career structure towards creating the same people and not creating a balance that is necessary…
(Head of Innovation and Research, 13/502-565)
4. Systems thinking
A number of participants conveyed their frustration about the lack of systems
thinking across NHS England which has led to several issues. Among them
was an overall lack of interconnectedness that limited organisational
members’ cognitive and information processing capability to identify the
problems innovation was designed to address. The other was a system failing
to provide accurate representations of innovations in terms of what was
presently being worked on, who was working on it, and what needed to be
done. The participants recommended that the application of a systems
thinking approach would create a network wide feedback loop between sub-
systems and enable a more complete understanding of the problems before
trying to resolve them. They also believed that being able to understand the
system would generally help leaders to better recognise the boundaries of a
problem and so make more informed decisions. Although not stating it so
explicitly, another participant mentioned that the application of systems
thinking would be useful for data analysis and in helping to articulate issues. It
is clear that the complex problems developed within the system could not be
solved by simple solutions because this requires a properly integrated and
long-term approach in order for it to be innovative. Nevertheless, systems
thinking reinforces the need for collaboration and collective thinking which
usually gives rise to new ideas.
196

I think the AHSNs have done quite a good job at this and obviously there is still a lot of work to be done. But as I said, there are fifteen commercial directors and there are improvement directors and there are people that meet on a monthly basis to try to say, “This is something great that is happening in North London, maybe it would work really well in Sheffield, let's have that conversation.” These things are happening, but we need to be able to make it again slightly more transparent because we don't need a hundred and fifty apps to tell us how many staff we count. And if you are a clinician in a trust and you think this is a great idea and you are being supported and told it is, you are actually wasting your time because no one is going to buy that app. First of all, because there are a hundred and three other ones and what is it actually solving and if the answer is nothing? Since it's not a clinical need, it will be very difficult to find a budget for that. So we need to be a bit clearer as to what the actual problems are and how we are going to solve them.
(Director of Commercial Development, 17/260-275)
But in brief, we think that there is an overemphasis on the supplier set of innovations so most of the conversations about innovations start with solutions, gadgets, nice stuff; they rarely start with a careful understanding of what the problem is that we are trying to solve. So there's an inability to even describe the problem, believe it or not. Yes, we know we are having a new crisis, but what exactly is it? What are the underlying drivers? There is no systems thinking so there is a level of sophistication both in terms of data analysis and kind of problem understanding that's just not there.
(Managing Director, 20/174-181)
5. Communities of practice
A participant pointed out that enacting readiness entailed understanding an
organisation as a community. This view suggests that to innovate, a leader
must first engage with his organisation, gathering information on the problems
and possible solutions, and then create the space which enables
organisational members to be part of the innovation process. To express the
communities of practice view, the participant shared a scenario at his Trust
where two junior doctors voluntarily created and managed the ideas within a
space with organisational leadership providing the support to bolster the
determination and enthusiasm of staff who were engaged in the space. This
shows that enabling communities of practice helps to create an inner
responsiveness and commitment as well as encourage organisational
197
members to take ownership of their environment. According to the participant,
an organisation becomes more of a community when its organisational
members start adopting the view of, “I work for or with rather than I work at an
organisation… ” (14/241).
So we set up a thing called an innovation forum which was relatively low level. It was run by two of our junior doctors; it was set up by them and run by them, but supported by the trust. And anyone in the organisation, whether you were a porter or a student or whatever, you could submit a proposal for a change process, which it wasn't like we are going to solve the IT problems of the NHS, it would be, you know, we see a problem where there is a localised issue …and we want to try and fix it by doing this. And then they would bring that to the forum, they would present it to the group, people would ask them a few questions and, if we liked it, they would go off and do it and then come back and show what they had done … The organisation supports them to fix the problem or gives them the permission to just go ahead and fix it. And within that will be a way of enhancing and gathering information around innovation. A lot of time we think we know what the problems are in the organisation by looking from above down into it, whereas, in fact, what we need to do is get down in the organisation and look around you and start getting to the bottom of what the problems are. And asking those people how they fix it. So it's supporting the grassroots sort of proposal … So you know it's, we are trying to be that sort of space that people want to come and inhabit to do that work jointly. I think the sexier word people are using a lot more now in a some ways is about communities in practice so that's a lot of what we are doing in many ways within the AHSN. We help develop those communities in practice.
(Clinical Director, 14/238-610)
However, a slight conflict of viewpoints was also observed in the analysis of
the responses. Another participant explained how mechanisms were different
across organisations and that one model did not fit all types of environments.
This participant suggested that the ‘right model’ for each context was the way
to go as some systems were more effective under a “devolved” structure,
whereas, others succeeded better when decision-making rested with the
senior management at the centre of the business.
So some organisations have very devolved innovation structures, like Procter and Gamble, some have very centralised ones like J and J. You know, what we do is expose our partners to the different models and the variety of models and have them decide what their intention is and find the right model for their circumstances.
198

(Managing Director, 20/132-135)
6. Partnership working and relationships
Participants discussed how healthcare has a political perspective which
stresses greater competition in order to “drive up performance.” However, for
participants, such competition thwarts concerted effort and reduces the
transfer of knowledge across the system. It is interesting how the Trusts
compete with one another and so fail to appreciate the value of partnership
that would be of greater assistance in the introduction of systems thinking to
identify problems and develop solutions.
So it is not in the interest of everyone to be sharing information on how they do well. And so you have a competitive market and that means there is difference and government likes the idea of having competition to drive up performance but doesn't like to admit that there is a downside which is information or knowledge gets stuck and it is not easily moved.
(Head of Innovation and Research, 13/94-98)
And I think the one thing that we try and do is, we try to work together. Obviously, we work in partnership, we work for our partners. Each NHS trust like I said, they are their own individual institution, they really and truly as much as they don't want to admit it, they do compete with the people down the road, it’s you know, that's just the way it is.
(Director of Commercial Development, 17/353-356)
The participants discussed how partners working and developing relationships
were crucial to increase the spread of innovation. For example, without
developing partnerships and relationships with industries and people, it would
be impossible for AHSNs to lead and support innovation across their
networks. AHSNs can bring different professionals into closer collaboration
because of their established relationships. Working as partners allows
organisational members to work across the usual perimeters and,
occasionally, it may involve people from different sectors within the same
organisation working collaboratively to develop solutions to an organisational
issue. For example, professionals in healthcare and social care can work
together to support the sector in delivering better integrated care and support.
The participants also stated that partnerships also provide access to diverse
199

skill sets as “…one organisation would not be able to solve the problem on its
own” (19/268).
I think that one of the things that UCL Partners prides itself on is partnership working…. our whole being is about developing partnerships with people. So it's a really important thing for us because actually without the partnerships and without the relationships you can't do very much cause it's about trust, isn't it? And sometimes it's about being a neutral voice to enable two or three of four or five organisations come together
(Director of Capability Development, 18/132-138)
So collectively the AHSNs, I think have become clearer on their role within their local geographies in providing support around turning innovation into practice… and have had and have built relationships with the NHS and industry which helps to bring kind of NHS academics and entrepreneurs together more effectively. I think it's just sort of… we have had greater clarity and focus and success since it first started and have also increasingly worked collectively in sort of subgroups across the country.
(Director of Innovation and Implementation, 19/29-35)
So internationally, we are part of something called Health Excel, which is the global network of digitally minded companies and providers, and BCs to work on innovation challenges…We have local relationships and partnerships.
(Managing Director, 20/61-66)
Efforts to promote an innovation culture also require collective working with
the public to understand their needs and dissatisfaction and possible ways
towards improvement.
And I think half the time people don't necessarily want the very best, but they want to be treated well, they want access, they want you know, I don’t think we have a mature enough relationship with our users.
(Director of Capability Development, 18/523-525)
7. Mandated Learning
There was general consensus among the participants that the current cohort
of professionals is not equipped to think in an innovative way. For example,
doctors and nurses who gained their medical degrees in the past few decades
were unlikely to have received modular training on how to write business
cases or how to engage with evaluation tools during the innovation process.
200

The participants explained that to develop a culture that was more enabling of
a different way of working, people need to be taught and different training
programmes need to be developed to bridge this learning gap. Along with this
kind of thinking, the participants also suggested that the relevant knowledge
and skills about how to operate in an ever changing environment should be
taught at the undergraduate level of the medical curriculum so that everyone
speaks the same language and understands the rules of the culture.
So, I think that there is a role for continuous workforce development. I think that there are innovation skills, and awareness and open-mindedness that can be taught and should be taught. And for the current cohort of professionals who didn't have these innovation skills and modules in their nursing degrees or medical degrees, there is modular learning that could take place. But the real answer is in building innovation skills and capabilities in the undergraduate curriculum in the way that Surrey University proposes that its medical school does.
(Managing Director, 15/243-249)
You would need to have a quality improvement process and programme embedded so it's training up clinicians. So your traditional doctor and nurse in their training don't learn about business. They don't necessarily learn about marketing, they don't learn about the product life cycle, and identifying, listening to customers’ needs, getting evaluations. They might be good at research and doing studying and pulling evidence together, so there are similarities. But when you have a product or a process, there's something, there's a process that you can go through and it's knowing how you can get your way to support that and I think if the culture has set out right at the beginning quite loud and clear, we are supportive of innovation
(Improvement Manager, 12/279-288)
A participant talked about the skills gap among the leaders that could affect
the future of the NHS. They opined that many potential leaders lacked the
behaviour and skillset necessary for successful organisational innovation. He
drew attention to the seemingly logical movement from his position of being a
Chief Operating Officer to that of a Chief Executive, and the system’s failure
to realise that each role required a different skillset. Although chief operating
officers were usually good at management, they might lack the ability to think
and act strategically. The participant also shared a personal experience of the
difficulty he faced in transition from being in Operations at a Trust to a Senior
201

Director at an NHS regulatory organisation. To address the skills gap, the
participant had to get further training, thus, reinforcing the need for it. It was
little wonder that he recommended a development programme which allows
leaders to exchange organisations for a short time to acquire some of the
needed skills. An example of this could be two chief operating officers, one in
a poorer organisation and the other in a better organisation, switching
positions for a few months. The objective would be for each officer to learn
about a possible different approach and model for service improvement. Even
if an operating officer from a “shiny beast” organisation switched to a poor and
failing one, rich learning could take and lead to a more innovative response to
problem-solving. Such approach could stimulate revolutionary and innovative
ideas as staff work with different people and in a different environment. The
participant also reiterated that such an exchange was not about turning the
NHS into a business, as such, but rather it was a way to improve the sharing
of knowledge.
I think it would probably be better for them to go on a development programme. So probably if you are deemed as having talent in the NHS and let's say, you are a future executive, you actually going to work in a totally different environment for even a month will do you more good than being on a NHS development programme, I think……because you know being a chief executive is not the same as being a chief operating officer, it's not the same as being a medical director; it's not the same as being a finance director, so there's a skilling challenge. And also, another challenge I think is not only is it you know all the skill set, it's what often happens, and you know this is perfectly, I’d do it, you’d do it, it's a natural thing, but you take your skill set with you and then you lean to that skill set because it's comfortable. And then you have chief executives that are trying to micromanage the hospital, behaving like chief operating officer. Well, that's crap and it's not going to help. So, you know, it's fascinating from a leadership point of view.
(Director of Capability Development, 18/410-472)
6.4.2 Leadership, what about it? And its role in enabling a culture of innovation
It was seen earlier that without the right leadership, it was impossible to create
an environment of innovation and improvement within the NHS. This section
discusses the themes and sub-themes participants identified as underlying
202
the roles of leadership in enabling a state of readiness. This discussion is
based on the following three themes:
1. Psychological Commitment, and Attitudinal Loyalty
2. Rethinking followership and influence
3. Adapting to the situation
(see Table 6.4 for a breakdown of the 1st order concepts, 2nd order themes
and aggregate dimensions).
203

Table 6. 4: Themes and sub-themes on leadership and its role in enabling innovation culture 1st Order Concepts 2nd Order Themes Aggregate Dimensions
“Identify your successor and then you start to develop your successor” (14/512)
“Develop new cohorts of people” (14/488) “You need to rotate people” (14/485)
Mentor & DevelopVs.
Rotate
Psychological Commitment, and Attitudinal Loyalty
“Shift from leadership to followership” (14/416)
“Promote a person and not the thing” (14/415)
“If you took away leadership it would emerge” (13/698)
Lead from behind
Rethinking followership and influence
“Leaders modelling that in themselves” (19/161)
“Its kind of role-modelled at the top” (20/244)
Model it!
“Tell people what to do” (13/459) “Enables space and time” (11/266) “Capable to adapt to the sitaution”
(13/462)
Command and ControlVs.
EnablingVs.
Adaptive
Adapting to the situation
204

1. Psychological Commitment and Attitudinal Loyalty
It was generally agreed among participants that creating a culture of
innovation and building that capability within its processes necessitates
deliberate determination from the leadership. Specifically, participants
stressed that leadership, psychological commitment and attitudinal loyalty
were major considerations in the organisational members’ behavioural loyalty
towards innovations. The participant described psychological commitment on
the part of the leaders as the state of mind they have about making the
environment conducive for innovation. It was more or less, the leaders’
determination to see innovation happen at all costs.
It's not a quick fix. It's a long haul …kind of a mental investment. So for a board, it's likely to take some finance, but it's also going to take resource from a creating space from the people that are involved day to day. And it's that commitment from the executive team to enable staff to do that and so there's lots of discussion, sure you have seen this…
(Director of Capability Development, 18/222-226)
Attitudinal loyalty is a mental commitment to a team and a consequence of
leadership’s mentorship and the development of team members. Effective and
successful leaders usually invest in their teams by employing various
strategies for developing and mentoring prospective successors. The
participants explained that many leaders impeded their own growth by not
helping members of their team to grow. Leaders have to train successors so
that a fully equipped team can support a coordinated and coherent move of
the organisation towards innovation and risk taking. Therefore, leaders should
be training people in their team to push themselves to improve their work and
the leaders should allow them to manage the unanticipated independently. By
doing this, they build a sustainable culture of innovation, and there should be
at least one person ready to step into a leader’s position, if the opportunity
arose. Apart from this, developing new cohorts of people would help to deal
with the present issue of leadership and the capability gap in the NHS.
So I think there is probably a few things in there for me. One of them is about resilience, so that's resilience of the people who are in the leadership positions. You know this work is really tiring and it's lonely.
205
You spend a lot of time in organisations very much on the edge of what everyone thinks is okay. So if you sit in the status quo where everything doesn't change and shift, it's quite *inaudible* Nothing ever changes, everything is as it were. Whereas if you are primarily in a space where everything is moving and changing and evolving, it's quite tiring to constantly be checking where you are. So there's an element of making sure that you are supporting the people who are doing that work actively. And that might be making sure that there is enough of them, and also the people, that there is an active succession planning. Because I think people, when they are in leadership positions, should only be in them for short periods of time because they become quite exhausted and their ability to be effective reduces downwards quite quickly. So, you need to rotate people through who take on roles, so you are permanently developing new cohorts of people. And the other elements of the sustainability of it is that as you start to find people who are doing this work, you are developing them and then they start to move into leadership positions themselves. So it doesn't mean that you finish your leadership position, you are tossed on the scrap heap; it means that you come back through and you then take on different roles.
(Clinical Director, 14/472-491)
It is clearly acknowledged from the above excerpt that leaders should not stay
in the same position for too long as it gets hackneyed and they lose their
edge. It became obvious over the course of the analysis of the information
collected from the participants that constantly changing leadership can impact
negatively on the organisational members’ readiness for innovation. The
general participant recommendation was for the NHS to renew leadership
through an ordered “rotation.” Ideally, one participant explained what should
happen was that when people assumed a leadership position that lasted for
three years. At the eighteen-month mark, they need to identify a successor
and start to develop that person. After this, the leader should leave the
position by switching roles for six months during which he supports his
successor. This strategy should move the organisation towards collective
leadership which should help to distribute the burden of management
amongst organisational members and give someone that may be more
capable an opportunity to engage in the organisation in new ways.
2. Rethinking followership and influence
Traditionally, leaders tend to “lead from in front,” however, to create an
environment where organisational members become innovative necessitates
206

a shift in this model of leadership. It is said that the shepherd ensures the
flock keeps together by using the staff to nudge and stir them to action if the
flock drifts too far or runs into danger. Leaders are expected to do the same
and the participants argued that a “shift from leadership to followership” was
sometimes necessary to develop creativity and maintain the drive and
commitment to continuously improve. They were quick to point out that
assuming a position of a follower did not mean giving up leadership
responsibilities, but rather it was “leading from behind”. It meant stepping
back when a person brought forth an idea and so the leader would be creating
the space for that individual to go to the front and lead only when there is
need. A participant made an interesting remark pertinent to this idea by
saying: “If you took away leadership, leadership would emerge because by
supporting people, you become the leader” (13/697).
In the process of helping others and enabling them to function, the leader
would still be seen as such, even if people did not call him that. The above
quote furthermore signified that leadership could arise from anyone within the
organisation, and leadership was, in fact, a matter of influence, as will be
explained shortly.
So, it's that shift from leadership to followership, so you see something that is really really good. What you do is that you promote that person rather than promote the thing. So… the difference is sometimes leaders will take an idea and make it their own and lead with it. And that's great for the leader, but it might dog down the quality of what’s going on, it actually might work against you and create a bit of a vacuum because people are thinking, “Well, every time we come up with something, he or she runs off with it.” Whereas if you were the person who is standing behind them and saying, “This is something we all need to do,” then you as the leader with the network, everyone is going, "Oh, Tony thinks that's really good, I'm going to go and have a look at that." And then that gives those people, puts those people, in a better space. So I think the key is that innovation champions are often the ones that lead well, lead from behind, they don't lead from in front.
(Clinical Director, 14/450-461)
According to a participant, “…it is the influence that is leadership” (13/703).
The interview responses outlined that in order to motivate people to innovate,
it requires the influence of the leaders based on their responsibility to set
207
standards for their employees’ behaviour and by being the kind of individuals
others would want to emulate. For example, if leaders want to see the rest of
the organisation responsive to an idea, then they need to learn to look beyond
their organisation for solutions, and sometimes be dissatisfied with the status
quo. By so doing, a standard would be set as to what was suitable or not and
room would then be created for possible innovation. Previously, it was
mentioned that innovation is often seen as a kind of additional work or even a
distraction from the core business. In addition, there is the fact that people
cannot be forced to innovate. Therefore, it was argued that the leaders had
the responsibility to motivate staff to become innovative by setting clear
expectations and, as one participants stated, by “presenting themselves
above the parapet and be the vocal minority that is the leading edge of
advocating and delivering change” (15/258).
You need to have leaders modelling that in themselves and having them show leadership and adopting new ways of working rather than focusing on the kind of business as usual of the here and now. In general, I suppose, a bit more courageous leadership, and that’s people being able to see that actually leaders are working in different ways, taking some more risks in a managed way, and therefore it creates an environment where others feel it is more acceptable for them to do likewise. I think it is providing clarity on what is okay and what isn’t okay, so people don’t overstep the boundaries, but there’s no kind of focus or innovative effort because there isn’t a lot of time in the system.
(Director of Innovation and Implementation, 19/192-199)
3. Adapting to the situation
Under this theme, participants’ explained that good leadership established the
environment for innovation by balancing their power between knowing when
to take control and when to step back and support others. One participant put
it this way:
There are times when good leadership might be simply telling people what to do and what you need is speed of response… So, context is going to describe that good leader will potentially need to be capable of adapting to the situation.
(Head of Innovation and Research, 13/459-463)
208

However, the command and control kind of approach was seen as restrictive
and rigid, with many claiming that it did not work. According to another
participant, “shouting at people louder or being more fierce or fearful with
people was useful for driving up research agenda in the early days, but it will
never work now” (13/431). The participants went on to explain that command
and control might work in a commercial situation where you have to follow
instructions or risk getting sacked, but it was not an effective approach for
managing the processes of innovation in the public healthcare delivery sector.
Furthermore, this type of control worked when the focus was on
organisational efficiency, but with the new bid to accelerate useful health
innovation within the NHS, leaders must now create a workplace culture that
supports innovative behavior. Participants argued that out of necessity,
leadership will have to shift their attitude towards risk-taking to “facilitation and
enabling” for innovation to take place. Facilitation entails the creation of an
environment which is more enabling of different ways of thinking in order to
produce a sense of expectation from organisational members. A good way
you do this is by creating space to innovate, getting people to experiment in
real time, pointing people in the right direction and providing links for
innovators to help get their ideas off the ground. As enablers, leaders also
need to develop strategies and allocate resources to promote innovation. This
is what one participant said:
Leader has to be appropriate for the context. So are the leaders that we have developed over the last twenty-five years who have been told that the only thing that matters is organisational efficiency. Are they ever going to be the right people to now lead and sustain the transformation plan? Well, they cannot do command and control but they have to do facilitation and it should be for the detriment of some organisations, and for benefit of the population, not for the benefit of the organisation to the detriment of the patient.
(Head of Innovation and Research, 13/462-471)
And the third bit for leadership is the kind of enabling support. So whether it's time or people or it's physical space or it is links to universities. Part of that enabling bit is also managing stakeholders, which is that you just need to give us some space to do this because we are trying to change what we do.
(Chairman, 11/266-284)
209
I call on the leaders in the patch to recognise that the system is broken and our current standards of service delivery are sub-standard and insufficient and to recognise the place for continuous improvement and disruptive innovation, and addressing that and encourage them to use what's in their power to set strategy and allocate resources to ensure the implementation of the strategy to get on and do that and sustain innovation. Because without leadership, none of this would happen.
(General Manager, 15/236-241)
6.4.3 Catalysing readiness: what can we learn from innovators?
This last section focuses on the lessons NHS Trusts can learn from regional
and international organisations that have succeeded in creating a culture of
innovation readiness. The findings were grouped under three main themes:
1. Bottom-up solutions
2. Business-like thinking
3. Long-term incentive programmes
(see Table 6.5 for a breakdown of the 1st order concepts, 2nd order themes
and aggregate dimensions).
210

Table 6. 5: Themes and sub-themes on the lessons NHS can learn from other industry 1st Order Concepts 2nd Order Themes Aggregate Dimensions
‘Let people create their own solutions’ (11/343)
“Collective thinking as a way of driving for solutions” (14/585)
Collective thinking Bottom-up solutions
“Make it business-like that is the way good businesses work” (14/681)
‘I would like to see them flexible and responsive to the needs’ (15/294)
“You have to offset the expense” (14/666)
ReflexivenessVs.
Value-based decisionBusiness-like thinking
“The next minute they are gone and somebody else’s vision comes in” (18/583)
“You cannot do innovation in annual budget contracts” (20/188)
Commitment and Regulating contracts Long-term incentives
211

1. Bottom-up solutions
The NHS can learn from other cultures that enable their organisational members to
think and act like entrepreneurs to achieve outstanding success. A participant
argued that big industry partners such as Microsoft, Oracle, Google and international
health organisations, such as Kaiser Permanente, all maintain a state of readiness
as part of an open culture. This culture encourages problem-solving to come from
among the grassroots through the creation of space for people to be innovative. Both
the element of an open culture and the creation of space tends to accelerate what
participants referred to as “distributed decision-making and a collective thinking
process” which triggers the sharing of ideas among organisational members to
manage activity and adapt to new and changing contexts. This notion of bottom-up
solutions is best built on relationships and trust so that knowledge is shared freely,
and this creates a degree of ownership that leads to continuous sustainable
improvements in the system.
You have to have people creating their own solutions, rather than everyone sitting in a white hall passing it down, it doesn't bloody well work. So is there a lot of prioritisation and a lot of development and adaptation locally? More of that happens in people sharing so we are still not having people sharing, people sharing best practices. I think that what you get, we can also learn that, if in organisations, you have got this kind of distributed decision-making and support coming forward, that changes are more sustainable and you get that greater sense of ownership.
(Chairman, 11/349-355)
So actually let us use the collective thinking as a way of driving either where we should be looking for solutions or what those solutions are. And there is kind of an expectation that most of what we would be doing would come from the wider thinking rather than just, you know, the leaders or the leadership. And there's almost like an expectation that you would be part of the solution, not we will tell you what the solution is. So you create that space for people to be innovative in approach and understanding and skilled.
(Clinical Director, 14/584-589)
What relationship do we actually have between the clinical staff and the management is really interesting because if you compare that to other industries, there is something fundamentally broken, right? And it's a very odd relationship. So, yeah I'm not surprised that this staff doesn't have time.
(Managing Director, 20/260-266)
2. Business-like thinking
212
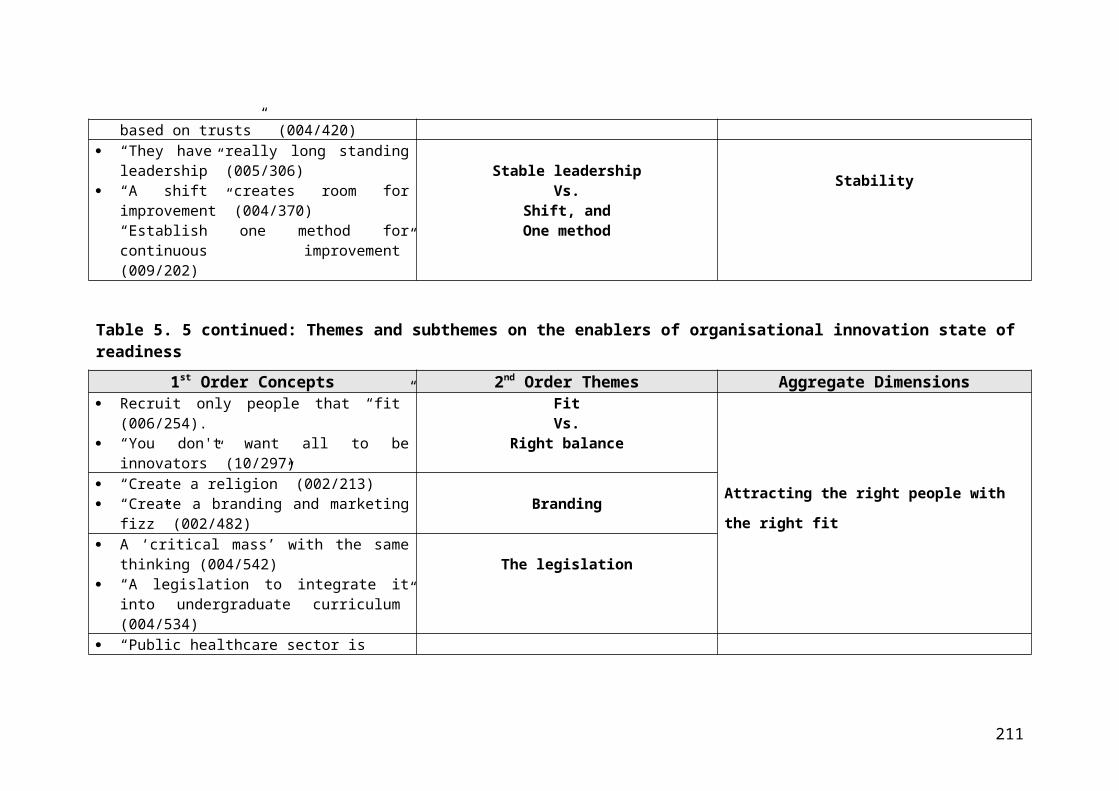
Participants highlighted that innovative industries operate an effective businesslike
thinking model. Such thinking comes from knowledge of what the customer or public
needs. Making the NHS more businesslike in the right areas would have implications
for the organisational members to be more innovative and more aware of
innovations. This might require the NHS to better serve the needs of the patients by
providing good quality and safe care in a timely fashion, and to deal with patients
equitably irrespective of their gender and ethnicity. Participants explained that the
difficulty with being businesslike sometimes was that although the quality of service
was achieved, costs might increase. Thus, learning to make real value-based
decisions is crucial, and the values need to be aligned with the organisation’s goals
and objectives.
Well, everything we do is done with members, NHS member organisations, but I suppose that the thing I would like to see rub off on the membership is the sort of flexibility and responsiveness of our small sectional enterprise member based network. So of course to survive as a member based organisation, you need to be flexible and responsive to the members, but I think the same applies at a different level to the NHS members.
(General Manager, 15/287-291)
But I think really, really engaged businesses have that responsiveness, that reflexiveness in the way that they work because they are aware that the market is always shifting and so they need to be able to be adaptive… Most of the organisations are way too big even on their own to be adaptive. So I turn it like an oil tanker... So making them more businesslike puts them in charge a little bit more so it's about thinking about or who's our end, who is our customer and our customers are our patients and they want us to be adaptive and responsive to what they need and what they need is high quality, safe, effective, timely and equitable healthcare. That's what they want. That's the end product, and actually, yeah making it more businesslike is really important. So if it's making it about the right things so sometimes when businesses fail, they worry about the money rather than the quality. If you make it all about quality, savings come, but the quality is also about not having any waste. You know, so actually everything you are doing is not the best thing, which might be slightly more expensive but you have offset the expense because the quality is greater, so therefore the level of harm is lower and so therefore the expense the harm incurs is reduced. It makes perfect sense.
(Clinical Director, 14/608-667)
3. Long-term incentive
Innovation was perceived as a long-term development. To achieve it in the future of
an organisation requires a long-term mental and physical investment. One of the
213

major barriers to this was identified by participants as the high turnover rate within
the leadership reduces organisational members’ commitment levels. To create the
desirable stability, the participant proposed that the executive teams within the
organisations should commit to long-term tenures. One of our participants shared a
good example of how a chief executive at a university hospital in Birmingham
persuaded her executive team to commit themselves to fulfilling the organisation’s
vision for a period of time. This required them to agree not to leave and they all
signed up for it. Although it was not legally binding, they stayed and the strategy
helped the hospital to become one of the best organisations in the country. Apart
from this, the participants suggested that incentives could also play a significant role
in supporting long-term commitment.
So a really good example of this is the UHB, the University Hospitals Birmingham and I can't remember what the time period was, but the chief executive said that she wanted a commitment from all of her executive team for a period of time, … Now, this wouldn’t be a legally binding thing because you can't do that …This happened because there's so much turnover that even if somebody has got a great vision, the next minute they are gone and somebody else's vision comes in … And I also think that there needs to be an incentive. So I think that people need to sign up for the long term and I think that the boards need to encourage them to do this…
(Director of Capability Development, 18/574-586)
Innovation was also perceived to be a continuous process with the benefits often
delivered over time. This makes short to medium-term expectations bound to fail
since innovation does not happen overnight. As one of the participants argued that
the present budget practices and polices impeded the development of innovation
readiness. He said: “…the NHS has annual business cycles and annual budgets and
everything that does not deliver within the year is not considered as essential unless
it's a Foundation Trust” (20/144). The willingness of politicians to commit to a long-
term contract is crucial if they want to see innovative options explored. The findings
revealed that commitments to a long-term contract would foster leadership
commitment and deliver lasting solutions.
There is something about the kind of short budget cycles, which I already alluded to. You cannot do innovation in annual budget cycles, you just can't. So it would help if there were longer term contracts, you know, which we have seen in other countries where because you have like five to ten year
214

contracts, you can actually do meaningful things within that. So that's an issue.
(Managing Director, 20/186-191)
6.5 Discussion
The empirical study within this chapter set out to explore managerial leadership’s
perceptions on the enabling factors and processes underlying organisational
readiness for innovation from an external perspective. The findings were based on
ten qualitative interviews from individuals across three distinct AHSNs based in
London and south east of England. The study had three main objectives. The first
was to determine the enhancing and enabling processes that led to iteration of
readiness of innovation. The second aim was to further increase an understanding
on the role of leadership, their effect and practices in the response to developing a
culture of innovation. The third aim was to determine the processes utilised by other
innovative organisations in enabling a state of readiness. Within this discussion
section, certain commentaries cited by the participants are paraphrased to
strengthen a given point.
Participants first of all described an organisational culture that is innovative means.
An innovation driven public healthcare sector was portrayed as an environment were
members of the organisation are committed to a constant re-evaluation of its existing
state against new effective interventions, and to be responsive enough to meets its
members changing needs through the adoption of these innovations. This concept of
a perpetual state of movement shared similarity with the views of the NHS senior
managers from the previous study in Chapter Five. Building on responsiveness and
the consistency of re-evaluation of existing and newer practices, the findings offered
the concept of reflexivity to successfully cope with, manage and change in response
to new events. Thus, the senior managers’ viewpoint is affirming some of the
contextual elements discussed in the literature review as integral to successful
innovation. These include openness and reflexivity. It was apparent from the
participants’ comments that being reflexive is much more than simply being
reflective. The latter deals with “thinking about something after the event, whereas
the etymological origin of the former concept means to bend back upon oneself”
(Marshall, Fraser and Baker, 2010, p. 21). According to West (2002), reflexivity
215

consists of three elements – reflection (i.e., attention, awareness, monitoring and
evaluation of the entity of reflection), planning, and adaptation. However, the findings
revealed one new technique that promotes reflexivity in everyday clinical practice.
The technique was described as critical to enhancing the safety of everyday activity;
and driving collective reflectivity on the knowledge and questions that clinicians have
about the need for continuous improvements. The practice participants discussed for
strengthening NHS workforce capacity for reflexivity is an interesting feature known
as ‘communities of practice,’ a relatively new term, even though the phenomenon
has existed for a very long time.
The concept of communities of practice shares similarity with the idea of free spaces
described by the senior managers within the NHS from the previous dataset in
Chapter Five. While the concept of space is birthed from the social movement
theory, communities of practice arose from Lave and Wenger (1991) situated
learning concept – that a new community member learn and absorb knowledge by
immersion in the community. Wenger (1999) has then significantly expanded on the
concept. Communities of practice is defined as a “group of people who share a
common concern, set of problems, or a passion about a topic, and who deepen their
knowledge and expertise in this area as they interact with each other on a
continuous basis” (Wenger, McDermott, and Snyder, 2002, p. 4). In healthcare it is
defined as “self-organising and self-governing groups of people who share a passion
for their field and strive, through collaboration, to become better practitioners”
(Health Innovation Network, 2016, p. 14). The nature of communities of practice is
that membership is optional and voluntary, which means the individuals do not
necessarily work in the same organisation every day, or are from the same
professional/social sphere, but they voluntarily meet because they find value in their
interactions. The concept is observable across different spheres of life. For example,
the soccer mums and dads who use game times to share insights about the elusive
art of parenting. There are also artists who congregate in open spaces to deliberate
the values a new music style. This also includes frontline managers supervising
engineering operations who get the opportunity to commiserate and to learn about
new market trends and anticipated shifts (Wenger, McDermott and Snyder, 2002).
AHSNs are a practical example of organisations that have been purposively created
to act as communities of practice. With a systematic structure in place, AHSNs
216

provide greater specialisation and collaboration by interweaving the whole system of
independent business units, trusts, academics, and industry. In addition to this, they
help to facilitate access to cutting edge knowledge which they deploy, leverage in
practice, and spread across the NHS. Communities of practice in health and social
care do exist, but can remain largely invisible within the hospital.
Contributions from the findings advise NHS trust leaders to deliberately cultivate a
mechanism that would bring people together in a strategic way in order to develop
best practice, implement new knowledge, or shape existing knowledge so that
people can perform their day-to-day jobs more effectively (Le May, 2009).
Externally, NHS trusts must increasingly partner with other organisations and build
relationships across other industries and network platforms such as the AHSNs.
Internally, participants advised that cultivating communities of practice required
leaders to permit designated time and day for deliberation over existing issues,
brainstorming engagement towards problem-solving, and for sharing information and
insights on how to best implement the knowledge collated to suit the needs and
context of practice (Drath, 2001; Lichtenstein et al., 2006; Le May, 2009). According
to one of the participants, a high engagement of employees with creativity improves
staff health, reduces sickness, absences and turnovers, and improves productivity.
This proposition has been supported in an NHS survey where the findings revealed
that a high level of engagement is associated with lower rates of absenteeism, with
an increase of one standard deviation of engagement equating to an average of
£150,000 from lower staff absence (West and Dawson, 2012). Thus, it can be
concluded that communities of practices give their members a sense of being
valued, respected and supported (West and Dawson, 2012).
Wenger, McDermott and Snyder (2002) make us to understand that because
communities of practice are voluntary and organic, what makes them successful
over time is their ability to evoke enough enthusiasm, significance, and value to
attract and engage members. The participants acknowledged this view and, thus,
stress the importance for hospital executive teams to actively recruit new individuals
to the organisation’s core to bring fresh vitality, grow and keep the continuity of
established communities of practice. However, this does not mean just any kind of
individuals, but those who can be flexible, dynamic and can take a more active role
217
in engaging and interacting with people and ideas over time (Conner, 1998; Wenger,
McDermott and Snyder, 2002; Martins and Terblanche, 2003; Nemeth et al., 2008;
Lencioni, 2012). However, a participant added that a good measure of diversity is
necessary and must be properly managed in order to promote a more interesting
relationship among members and to encourage richer learning and creativity. This
point is of much interest as it looks beyond the heterogeneity of skills or background,
or the commonality in a community. Instead, it stresses the point that different
personality qualities like self-awareness, resilience, and confidence are the
foundation of how people behave, and is a central part of determining the
effectiveness of interaction within communities of practice. Leaders need to be
aware of the strengths and limitations in these areas and appreciate the value of
individual personality traits in juxtaposition with skills and aptitudes during
recruitment.
In the second objective, participants discussed the role and responses of
organisational leadership in enhancing an innovation driven environment. It was
apparent that without the right leadership, it would be difficult to create the
environment for innovation and improvement among the employees of the NHS. The
complexity of the NHS along with its hierarchical structure keeps the question of
leadership style open (Masri, Wood-Harper and Kawalek, 2017). From the findings, it
was observed that there was not one specific style or approach to leadership fit for
the public healthcare sector, but rather that organisational leaders needed to be
dynamic and able to adapt by recognising what type of behaviour that is useful and
appropriate at different points in time and in different situations. Drawing on the
interviews with the senior managers from the AHSNs, this thesis offers two main
approaches to leading complex adaptive organisations, such as the NHS, towards
organisational readiness. First, there is the need for “systems leadership,” labelled
as a “new, new leadership” by Marion and Uhl-Bien (2002, p. 1). From the findings, it
was observed that three other forms of leadership behaviour emerged, namely,
“collective leadership,” “distributed leadership,” and “lateral leadership.’’ The second
is “transformational leadership” labelled as “new leadership” by Bryman (1996).
The discussion will first focus on systems leadership. There was a general
consensus amongst those interviewed that more effort needed to be made towards
218

developing system leaders. For example, one of the participants stressed the
importance of the systems leadership view by saying: “The wicked problems in
healthcare, the systems problems, they are not organisational, they are also
organisational problems but we have very good organisation leaders.” A systems
thinking perspective reveals that an organisational problem would require a deeper
understanding of the whole and would take into account the behaviour of the system
over time, rather than a “snap-shot” view (Senge, 2006, p. 65). In the same line of
thinking, systems leadership is defined as “a collective form of leadership – a
concerted effort of many people working together at different places in the system
and at different levels” (NHS Education for Scotland, 2018, p. 4). In this way, system
leaders develop and foster collective leadership which “means everyone taking
responsibility for the success of the organisation as a whole – not just for their own
job or area” (West et al., 2014, p. 4). West at al. (2014) in the Kings Fund espoused
the importance of developing collective leadership for overcoming the challenges
that the NHS now faces. For sustainable organisational readiness for innovation,
West et al. (2014) advise that public healthcare organisations should foster collective
leadership mind-sets through developing the capability of the collective at all levels
of the system, rather than following the traditional approach of leadership that
focuses on developing individual capability (Marion and Uhl-Bien, 2002).
The systems leadership framework moves away from command and control
orientation and instead encourages a participatory form of working (Regine and
Lewin, 2000; Stacey, Griffin and Shaw, 2000; Streatfield, 2001). The momentum for
control lies within interactive bonding across interdependent individuals in a system
(Marion and Uhl-Bien, 2002) while the labelled leader in the system behaves in a
less hierarchical way than leaders traditionally behave (James, 2011). Apart from
this, systems leadership sees control as bottom-up rather than top-down and at the
control of the leader as transformational leadership perspective suggests (Marion
and Uhl-Bien, 2002). For example, the findings showed participants making it clear
that in sustaining healthy communities of practice, leadership does not depend on
one person, but rather internal leadership emerges depending on the needs and
expertise. In other words, systems leadership creates “distributed leadership.”
Distributed leadership is a new architecture for leadership, providing a shift from the
sole, individual role to the collective social process emerging through interactions
219
across all organisational levels (Lichtenstein et al., 2006; Bolden, 2011, Currie and
Lockett, 2011). Harris (2008) and James (2011) explain the term ‘distributed’ meant
individuals take the lead at various times and the power shifts as different individuals
emerged to be leading. In organisational dynamics, Barry (1991) used the term “boss
less team” or a “self-managed teams” to describe distributed leadership. Barry’s
work suggests distributed leadership is a “collection of roles and behaviours that can
be split apart, shared, rotated and used sequentially or concomitantly” (Barry, 1991,
p. 34). This basically implies that at different points in time, people with and without
formal leadership positions can exist in a team, with each person undertaking a
complementary leadership role (Barry, 1991, p. 34).
James (2011) expressed the view that distributed leadership is integral to the
practices of NHS organisations. He stated that “the NHS needs people to think of
themselvesas leaders not because they are personally exceptional, senior or
inspirational to others, but because they can see what needs doing and can work
with others to do it” (James, 2011, p. 18). The findings by Fitzgerald et al. (2013)
showed that a multi-tiered distributed leadership pattern among senior manager,
middle manager and staff is an effectual enabler of service improvements across
public sector organisations, like healthcare. However, there are claims that the act of
distributing decision-making among organisational members is not always good
leadership. Empirical evidence shows a link between distributed leadership and
reduced team effectiveness and increased conflicts (Heinicke and Bales, 1953;
Storey and Holti, 2013). In summation, a systems views of leadership is relevant to
the NHS as senior healthcare managers alone cannot lead organisational readiness
for innovation, front line staff need to be involved in leadership roles. But, what does
system leadership entail?
The findings showed that systems leaders encourage collective leadership cultures
by creating the conditions under which teams can flourish. For example, they
promote dialogue for discussion and debate, i.e., free space and time for people to
meet and explore different points of views which can produce learning, new
solutions, new thinking, and new possibilities to make improvement (Marion and Uhl-
Bien, 2001; Lichtenstein et al., 2006; Uhl-Bien, Marion and McKelvey; 2007; NHS
Education for Scotland, 2018). They help encourage flexibility while holding people
220

accountable for their outcomes (NHS Education for Scotland, 2018). This idea bears
similarity with an earlier view a senior manager within the NHS set of data shared.
According to the CCG chief executive officer, innovation is his freedom to manage
his job delivering against the objectives in line with the organisational members
needs – which are local CCGs - and within that freedom, he is accountable to the
Secretary of State. Similarly, the findings within the AHSNs study enlightened us that
in sustaining the momentum of communities of practice, organisational leaders in
their authority needed to provide resources to facilitate innovative opportunities that
may arise within interactive spaces. Along with establishing review processes and
developing well-structured appraisals of performance to monitor and address poor
performances, there is the need to give helpful feedback to innovators in order to
promote fairness, transparency, and accountability. It is fair to say that such a
rigorous process does not take away from the autonomy within free space or
attempts to control what is happening. The findings showed that this was necessary
to review the success and/or failure of uniquely funded projects, to provide shared
learning, and also to recognise new knowledge contribution in order to distribute
rewards and recognitions for achievement or innovation attempts (Wenger,
McDermott and Snyder, 2002; West et al., 2014). For example, at DaimlerChrysler,
when staff complained that the performance system was unfair, the leadership of the
company put together a team consisting of six engineering managers to review the
results of the engineering TechClubs and they provided feedback and guidance to
individuals on a number of completed projects (Wenger, McDermott and Snyder,
2002). Besides, healthcare professionals need to be accountable for using their time
most effectively, including opting out of or attending meetings according to
organisational needs. Consequently, systems leaders will need to strike a balance
between governance and flexibility to enable innovation and creativity (NHS
Education for Scotland, 2018).
Interestingly, as systems leaders encourage flexibility, the findings showed that
‘lateral leadership’ is promoted. Lateral leadership “is an individual’s personal
initiatives to engage with people outside the normal sphere of influence” (NHS
Education for Scotland, 2018, p. 22). Participants advocated that organisational
members needed to spend time networking and engaging with the wider problem in
open space. Systems type of leadership recognises and promotes the importance of
221

collaboration and effective working across organisational boundaries between
primary and acute trust and between health and social services (Storey and Holti,
2013). The systems leadership perspective, therefore, postulates that leadership in
public healthcare sector should leverage open innovation (as discussed in Chapter
Two) to devise, develop, and disseminate novel solutions in healthcare (Bullinger et
al., 2012; Tani, Papaluca and Sasso, 2018).
The second style of leadership apparent from the findings for enabling the processes
of readiness for innovation is transformational leadership. The concept of
transformational leadership is attributed to Burns’ (1978) seminal work. According to
Bass (1999, p. 11) transformational leadership “refers to the leader moving the
follower beyond immediate self-interests through the following four approaches.
First, there is ‘idealised influence’ when the leader sets an example for the followers
to follower. Second, is ‘inspirational motivation’ leadership which envisages the
vision for a desirable future, and communicates how it can be reached. The third is
‘intellectual stimulation’ when the leader encourages their followers to think in
creative and innovative ways. The fourth, ‘individualised consideration’, is displayed
when the leader pays attention to the followers, offers support and coaches them.
The transformational leaders delegate assignments as opportunities for growth.
Wong, Cummings and Ducharme (2013) in their systematic review of the literature
identified transformational leadership as one of the most prominent leadership
theories guiding healthcare leadership research. As the public healthcare faces
economic meltdown, stressful work environments, anticipated shortfall of medical
staff, the view has been expressed that a relational leadership style where followers
have trust for their leaders and are motivated to go above and beyond their role is
required (Wong, Cummings and Ducharme, 2013).
The findings showed that transformational leadership practices are positively related
to increased staff expertise, risk-taking, and reduced staff turn-over (Gumusluoglu
and Ilsev, 2009; Brown et al., 2013; Wong, Cummings and Ducharme, 2013;
Gyensare et al., 2016; Vitale, 2018). This is in contrast to systems leadership that
sees control as bottom-up and embedded within the dynamics of the system.
Transformational leadership implants top-down expectation with leader-centered
activity (Marion and Uhl-Bien, 2002). For example, a systems leader creates a
222

space, then pushes the organisation to the edge of chaos through overburdening the
staff with unmanageable demands, and then having them to discover for themselves
a new way of working together which helps them to learn how to self-organise
around the most difficult problems (Regine and Lewin, 2000; Marion and Uhl-Bien,
2001). In contrast, the transformational leader identifies the vision for a space and
rather than staying out of it, the leader makes use of a participative behavioural
approach to drive intellectual stimulation behaviour among staff or takes a directive
approach to control the interactive dynamics that lead to creativity (Bass, 1999). In
the above example, systems leadership let people create their own solutions, using
collective thinking as a way of driving for solutions. Transformational leaders,
through emphasis on motivating and inspiring behavior, mobilise their followers
behind their vision. In other words, systems leadership ‘leads from behind,’ while
transformational leaders ‘leads from in front.’ While both models of leadership
address the processes for creating transformation to stimulate organisational
innovation and performances from very different perspectives, it is difficult to
conclude which approach best fits the management of innovation in the public
healthcare sector. The general consensus from the interviews was that the style of
leadership needed to be based on the given context. Thus, healthcare leaders must
be attentive to the needs of their organisation, the organisational members, and the
service-users as well as being responsive and flexible enough to make the
necessary adjustments. These could involve the setting of new strategies and
adopting a new vision including a move towards innovation and being committed to
taking risks, and providing resources.
Based on the information collected, the participants revealed that approaches
fostering systems thinking are predominantly useful in creating an innovation driven
culture. It was observed that focusing on diversity and creating that inclusive culture
through systems leadership can produce innovative outcomes. Additionally,
participants conveyed the idea that systems thinking approaches are extremely
useful when introducing an innovation into health systems in order to create a culture
of transparency across the entire public health care system. In the same vein, some
participants mentioned that readiness for innovation is impeded due to a lack of
understanding and emphasis on the true nature of the problem. In light of this, a
participant argued that there is an overemphasis on the supplier set of innovations
223

with most of the discussions about innovations starting with solutions. The Innovation
and Technology Tariff, though useful, has helped to reduce some of the barriers
clinicians and innovators experience in promoting the uptake and spread of low-cost
innovations. However, it does not offer a solution in moving the NHS away from a
supply-driven approach or to solving the tension between a policy move towards
accountable care systems and to small-to-medium sized enterprises (SMEs) bidding
for NHS contracts (Castle-Clarke, Edwards and Buckingham, 2017). Nevertheless, it
is believed that partnerships and relationships between NHS organisations and
AHSNs will lead to the development of a better capacity and improved skills to
systematically define problems and scout for solutions. On a related note, a
participant said: “There's an inability to even describe the problem, believe it or not.
Yes we know we are having a new crisis, but what exactly is, what are the underlying
drivers? There is no systems thinking so there is a level of sophistication both in
terms of data analysis and kind of problem understanding that's just not there. So we
spend an increasing amount of our time helping our partners to understand the
problems of the place.”
The NHS innovation space is clearly complex and the change that is needed to
enable readiness is a culture change, which requires the entire system, both locally
and regionally, working together in identifying the most pressing issues and findings
solutions for these problems. This idea is also consistent with Kilmann’s (1984)
discussion of how important it is for leaders not to gravitate towards using a singular
approach that offers fragmented pieces and treats problems in isolation by ignoring
how the contextual interactions occurring across the system contribute to finding
innovative solutions. This approach can be seen in a situation where, for example,
staff working in a hospital complain about a lack of direction and the top team puts a
new system into place without trying to find out how the interrelated sub-units and
other elements of the organisation contribute to solving the problem. This is what
Kilmann aptly describes as a quick-fix. The findings demonstrated that quick fixes
only offered a temporary response and failed to address the long-termed underlying
causes of the problems (Kilmann, 1984). This suggests the need of the management
to apply the concept of systems thinking which posits that changes in behaviour over
time are not static, and changes in one part of the system can lead to counterintuitive
consequence in another part, therefore, an integrated working effort is important
224

(Dattee and Barlow, 2010; Barlow, 2011). The results also suggests that the
application of systems thinking would enable an organisation to be better equipped
to anticipate events and to be prepared for any emerging challenges (The Health
Foundations, 2010; Atun, 2012; Lipsitz, 2012). The participants’ views on systems
thinking showed that they believed it could contribute to a better capture of feedback
data, improve data analysis, and lead to a more effective handling of problems. The
application of this approach would also be expected to help leaders learn more about
the management of complex systems (Fraser and Greenhalgh, 2001; Wilson, Holt
and Greenhalgh, 2001; Morgan 2006; Dattee and Barlow; 2010; Lipsitz, 2012). On
this basis, the findings indicated that an organisational culture that is innovative was
not a quick fix, and many healthcare innovations were not managed successfully
because leaders were applying linear and reductionist approaches (Marion and Uhl-
Bien, 2001).
For the third objective, participants revealed specific variables the public healthcare
sector can learn from the private healthcare and non-healthcare sectors. Among
these were the bottom-up approach and reflexivity which have already been
discussed. Along with this, the participants discussed the construct ‘long-term’ as a
key characteristic for sustainability of a continuous innovation ready environment.
One of the problems raised across both datasets is the high vacancy rates and the
short tenures among the leaders of the NHS innovative driven culture. In 2014,
research conducted by the King’s Fund revealed a third of NHS providers had at
least one-board position level not permanently filled. This was due to the ‘blame
culture’ in the NHS and the unrealistic expectations of what can be achieved in short
timeframes (Janjua, 2014). The University Hospitals Birmingham was described by
one of the participant, as an example of a Trust that has benefited from
organisational and leadership stability. The participant described how the Trust chief
executive explained that the stability of leadership was essential for the success of
her organisation as it allowed her senior team to plan and grow through a collective
leadership strategy. The findings suggest that long tenure does provide greater
strategic coherence, focus and flexibility – especially in the public sector where it
might be difficult to predict what the future will bring (Timmins, 2013; Manso, 2017;
Anandaciva et al., 2018).
225

6.6 Chapter summary
This chapter has presented the sub-themes under three major themes: enhancing ad
enabling processes for an innovation driven culture, leadership, what about it? And
its role in enabling a culture of innovation, and catalysing readiness – can we learn
from the innovators. The chapter established several conditions that are relevant in
enabling a culture of innovation. From these conditions, the most prominent one
seemed to be that of creating a sense of community as people are more inclined to
take ownership as a step towards institutionalising a state of readiness. It was
discovered that an innovative culture was perceived as an inclusive one where
everyone, including leaders, organisational members, service users, politicians, and
partners has a role to play.
In addition, it is apparent that the role of leadership in achieving innovation is
undisputable. The participants’ views demonstrated that a single leadership style,
especially a command and control one, is not adequate for innovation in a complex
environment. Rather, organisational leaders must learn to be flexible, capable of
adapting to the changing environment and to understand what an organisation
needed in different situations. Leaders were perceived as being like shepherds that
ensured that the flock kept together as they used their power and authority to gently
encourage and move organisational members forward when they seemed to have
lost their motivation, strayed from the vision, or ran into danger.
The chapter also presented potentially applicable lessons the NHS can learn and
institute from other sectors. This includes the need for NHS Trusts to build a capacity
for learning and adaptation in terms of adopting a flexible, bottom-up approach. In
addition, is the need for a reflexive business model and a better understanding of its
user needs.
In the following chapter, the results of the both empirical studies are reviewed and
the general conclusions and implications drawn.
226
Chapter 7
Discussion and Conclusion
7. 1 General overview
The current thesis sets out to extend the theoretical understanding of the concept of
organisational readiness for innovation. It also examines the meanings, factors and
the processes involved in achieving and maintaining a state of readiness for
innovation in the public healthcare services sector from the perspective of the senior
leaders. The research consisted of a narrative literature review to explore how the
concept of innovation management has been developed and has evolved; a
systematic review to provide an in-depth analysis of the literature; and a discussion
on the conceptualisation of the construct of readiness. In addition, there was a
qualitative set of interviews conducted with a sample of NHS and AHSNs senior
managers to address the relevant conceptual questions. The present chapter aims to
review the findings discussed from the previous chapters and synthesise them to
provide answers to the research questions presented in the introduction of the
thesis. The objective of this chapter is to provide a theoretical discussion and also to
put theory into practice. Therefore, it concludes with a proposed integrated
framework that extends the principles of the complex adaptive systems theory to
include the concept of the organisational state of readiness as well as to provide a
guide on how to implement it in practice. The conceptual, methodological and
practice-based implications and the strengths and limitations of the research are also
discussed.
7.2 Critical summary of studies
The literature review helped in understanding innovation within the context of
healthcare and the issues unique to this environment. Innovation was described as
new and beneficial programmes or systems that enhance healthcare services and
can reduce cost. However, theories of diffusion (Schumpeters, 1934; Rogers, 2003;
Godin, 2003; Greenhalgh et al., 2005) and non-linearity (Van de Van et al., 2008)
227

helped to bring to light the complex process concerning the management of
innovation in public healthcare organisations. In the midst of these complexities, a
small number of health and social care researchers (Greenhalgh et al., 2004;
Weiner, 2009; Hendy et al., 2012) identified readiness as the prerequisite for the
success of innovation. The concept of readiness led to the consideration of how it
was generally conceptualised in the innovation management literature. Therefore, to
obtain a comprehensive understanding of this phenomenon, a systematic review of
the literature was undertaken. This allowed for a thorough focus on the research
questions, especially given the fact that readiness was used interchangeably to also
mean preparedness.
The findings from the literature on readiness revealed that there were many different
concepts regarding the term. These included the stage vs. the process-based
debate, the various disagreements among theorists based on their construct of
readiness and the fact that it includes behavioural, psychological and structural
aspects. This was further complicated by the small sample sizes upon which some of
these conclusions were based and, in some cases, the limited empirical evidence on
how to measure readiness. In addition, there was a limited amount of studies on
readiness in the innovation management literature in comparison to those on
organisational change. Based on the findings from the literature review, it was very
clear that organisational change was different from innovation. This made it difficult
to accept the principles of the change models used in conceptualising readiness for
innovation. These were the issues that led to the research questions explored within
this thesis.
7.3 Bringing it all together: Key findings to the research questions
The significant findings discussed are based on those from the systematic review
and the shared understandings from stakeholders from the internal NHS and those
from the external AHSNs in the two empirical studies. Interestingly, both groups of
senior managers had a shared understanding of how readiness was conceptualised
and discussed a list of actions required for making it successful from both an inner
and an outer perspective.
228

The first research question explored was: How is innovation to be distinguished from organisational change and why? This area received less attention in the
literature so it lacked empirical evidence to demonstrate any differences in the
principles for the management of innovation. However, the empirical findings
revealed that innovation is distinguishable from organisational change which
supported key aspects the literature. It reinforced Zaltman, Duncan and Holbek’s
(1973) perspective on the distinction between both in that innovation is something
new that requires acceptance and implies change, while change does not pre-
suppose innovation. Unlike change management, which is intermittent and led by
organisational leadership (Lewin, 1951; Kotter, 1995; Vincent, 2013), innovation was
described by the senior managers as continuous in nature and embedded within an
organisation’s culture as well as their staff attitudes and mindsets (Rogers, 2003;
Schweizer, 2006; Van de Van et al., 2008; Camisón and Villar-López; 2014). Thus,
innovation requires a degree of collective reflexiveness, flexibility and autonomy to
stimulate and drive positive outcomes (Khazanchi, Lewis and Boyer, 2007; Anand et
al., 2012; Wynen et al., 2014; Keohane, 2018). Furthermore, the participants
expressed the belief that some degree of readiness might be required when
implementing organisational change brought about by managerial decisions.
However, it was absolutely essential when dealing with the change that came with
innovation.
The findings further concurred with the literature that the process of innovation
management goes through a linear sequence of invention, adoption and
implementation and diffusion (Rogers, 2003; Greenhalgh et al., 2005; Department of
Health, 2011a). However, the process leading to successful adoption and
implementation was described as complex, with many uncertainties, setbacks and
shocks along the way (Plsek, 2003; Weberg, 2012; Van de Ven, 2017) and the
complexity of the public healthcare sector made innovation a much slower and more
complicated process (Plsek, 2003; Barlow, 2011; Atun, 2012). Innovation
management is not a simple topic; in fact, this concept was often linked to different
concepts of the complex adaptive systems theory. In comparison to organisational
change, the concept of innovation was described as necessitating a whole-systems
effort which sees interdependencies across the wider system within the public
healthcare sector. The findings present the complex adaptive systems thinking
229
concept as relevant in order to better understand the relationship between the
behaviour of each agent, the collective, and what drives the effect of the
interconnected dynamics (The Health Foundation, 2010; Lipsitz, 2012; Tani,
Papaluca and Sasso, 2018).
The second question explored was: What is organisational readiness for innovation and why does it matter? One of the main objectives of this question
was to address the conceptual ambivalence that was apparent in the literature
relating to whether or not organisational readiness should be described as a stage or
a process. The findings were in line with the school of thought that proffered a
process-based conceptualisation of readiness throughout the lifecycle of an existing
project (Armenakis, Harris and Mossholder, 1993; Jones, Jimmieson and Griffiths,
2005; Todnem, 2005; Stevens, 2013). In much the same vein, the theory that Van de
Ven (2017) proposed was that innovation is a journey that started at development
and ended in its implementation or termination. However, the participants’
interpretation of readiness was not in line with this concept as Van de Ven (2017)
viewed innovation in the same way as an organisational change process which has a
clear beginning and end.
Organisational readiness was described as on-going, irrespective of an innovation
implementation. A useful analogy for organisational readiness for innovation in public
healthcare service organisations is the operation of a mechanical watch. This
mechanism works by ‘continuous movement’ which generates kinetic energy to keep
the wheel turning to display accurate time. In this analogy, the watch is the public
healthcare organisation with readiness as the kinetic energy that propels the
movement of the wheel. The wheel refers to the interacting agents, their properties
and the contextual elements, while innovation is the result of the motion of the
wheels that leads to the display of accurate time. A watch needs continuous kinetic
energy to function effectively. This continuous motion makes the wheel to move and
sustains this movement until accurate time is shown. In the case when there is an
absence of kinetic energy, the wheels will not move, time will not be displayed, and
the watch will not function at optimal capacity. In public healthcare, readiness set
and keep the organisation in a state of movement, it has to be on-going, without
which the force required to drive the system towards generating system-wide
230

promising realisation, capabilities, innovation, and adaptive outcomes is nonexistent.
Participants’ process-based conceptualisation of readiness depicts the construct as
the outcome of the endless interactions of multiple stakeholders. These will either
shape an innovation to enable alignment with the health systems function or keep
the organisation in a state of being ready to adopt an innovation. Thus it increases its
absorptive capacity, and enhances its adaptive capacity to enable it to deal with the
changing public healthcare environment. This proposition should replace the
traditional linear view of readiness in the literature that is based on the stages of
change model that describes the operationalisation of readiness at a particular point
in time during the innovation management process. In this respect, the findings
reinforce the need for the leaders of public healthcare organisations to move away
from cause-and effect thinking and be open in considering the principles of complex
adaptive system by fostering relationships and creating conditions so the system can
evolve and produce innovative outcomes (The Health Foundation, 2010; Lipsitz,
2012; Pype et al., 2017).
The third question was: What are the key barriers and facilitators of readiness for innovation management in healthcare service organisations (NHS)? The
findings confirmed that organisational readiness is a multifaceted and
multidimensional construct (Weiner, 2009; Attieh et al., 2013; Shea et al., 2014).
Many of the readiness enhancers and enabling processes described by both groups
of participants as being relevant in the context of healthcare were also identified in
the literature.
At an individual level, some of the key characteristics that were identified as
influencing employees’ behavior towards innovation readiness included a vision for
innovation; self-perception of the usefulness for innovation in solving an existing
problem, the capacity to successfully implement innovation, the right connection and
influence for people at the front-line; and time for experimenting (Rogers, 2003;
Greenhalgh et al., 2005; Atun, 2012; Long, Cunningham and Braithwaite, 2013;
Wisdom et al., 2014).
At the team and organisational levels, the level of collective reflexiveness,
empowerment towards decision-making and risk-taking, diversity of thoughts and
agile thinking, and boundary spanners in collaborative networks were seen as
231

contributory to catalysing a culture of innovation readiness (Marshall, Fraser and
Baker, 2010; Griffiths et al., 2012; Long, Cunningham and Braithwaite, 2013;
Wisdom et al., 2014). The findings also revealed some new and unique enhancers
and enabling processes facilitating readiness that were not apparent in the review of
the literature on organisational readiness. Two of such factors were the concept of
‘free spaces’ and ‘communities of practice.’ Both concepts comprise of diverse
individuals across external networks and staff from NHS organisations who
voluntarily come together, engage in knowledge sharing, and generate responses to
both internal and external pressures (Marion and Uhl-Bien, 2001; Lichtenstein et al.,
2006; Lencioni, 2012). Through this kind of networking, a different approach to
problem-solving has emerge instead of the isolated one usually pursued by
individual Trusts which is a common practice based on traditional thinking. This new
way of acting moves the public healthcare sector towards a systems thinking
perspective. Participants further added that the free spaces developed internally
within Trusts required a measure of performance by the leadership. This predicates
the need for monitoring on the notion that individuals and teams are not isolated, and
for increasing staff accountability for decision-making and time management. Other
newly identified enabling processes to foster an readiness capacity at an
organisational level included the establishment of a strong organisational brand
identity to attract pioneers and the need to deal with the staffing crisis presently in
the NHS that limits staff from engaging in creativity and processes that stimulates
innovation (Gapp and Merrilees, 2006; Punjaisri and Wilson, 2007; Northern Devon
Healthcare NHS Trust, 2015). There was also the need for long-term leadership
tenure to help move Trusts from a blame culture to a learning one (Janjua, 2014;
Manso, 2017; Anandaciva et al., 2018).
The participants further discussed specific leadership behaviours necessary for
enabling and enacting readiness for innovation in public healthcare organisations.
These behaviours were ascribed to the individual leaders as well as groups and the
organisation itself. The possession of these characteristics was seen as helping to
increase the capacity of the system to achieve its goal and produce new outcomes
(Lichtenstein and Plowman, 2009). The findings revealed that a mixed method
leadership approach that is increasingly adaptive, flexible and engaging is required
for driving the NHS towards a state of readiness for innovation. This includes a
232

systems style of leadership were leaders foster the conditions where people at all
levels can work cogently according to their potential (Lichtenstein et al., 2006; The
Health Foundation, 2010; NHS Education for Scotland, 2018). This happens by the
adoption of a distributed and collective leadership style which occurs among the
teams and in the context of the organisation (Harris, 2008; Currie and Lockett, 2011;
James, 2011). Transformational leadership which involves leaders building strong
and trust-based relationships with their staff and motivating people to buy into their
vision for innovation is also a requisite (Jung, Chow and Wu, 2003; Doody and
Doody, 2012; Jyoti and Dev, 2015).
A theoretical framework was developed based on the senior managers experiences
in passive knowledge obtained from the commonalities in the interview datesets
acquired from both groups of stakeholders interviewed. The framework is an outline
guide for the managerial application of the complexity theory in moving an
organisation towards a state of readiness. The information within the framework is in
no particular order and is better shown as a bulleted list. It is beyond the scope of
this thesis to test the validity of the framework, however, it provides a starting point
for future research. The theoretical framework (see Figure 7.1) proposed that the
creation and maintenance of organisational readiness for innovation in public
healthcare will be influenced by four ingredients: space, communities of practice,
leadership engagement and practice, and policy and advocacy. Research reveals
that innovation is increasingly collaborative, involving the interaction of multiple
stakeholders during the process. The existence of free spaces means that staff
become more open, comfortable, and make a concerted effort towards continuous
improvement. This translates into a highly responsive and flexible physical
environment that allows NHS staff in a range of group interactions and alignments to
discuss a problem and decide on solutions that work within the given context.
Communities of practice most importantly underpin open innovation and partnership
– a movement where diverse unconnected individuals come together and form a
group as a means of sharing both tacit and highly complex information and to
explore ways of working, learning and finding solutions to existing problems.
Communities of practice bring about change through collaborative, sharable spaces,
and they are presently growing in numbers to help meet the enormous challenges in
the NHS (Greenhalgh, 2011; Health Innovation Network, 2016). A range of
233

stakeholders, especially Trust leaders, within the adoption system has a role to play
in influencing readiness across an entire system. The findings showed their role vary
from enabling resources, exerting influence, executing policy, and integrating the
processes necessary to stimulate innovation readiness behaviour to increase
positive outcomes. Lastly, policymakers and advocacy play a unique role in
influencing the general context within which the pubic healthcare sector exists. They
do this through increasing the funding for innovation across hospitals and by
legislating for innovation thinking to be integrated in the medical and nursing
undergraduate curriculum.
As seen in (Figure 7.1), the framework shows that readiness is not the responsibility
of any single individual. This was borne out when the participants discussed how to
enact readiness as it was not discussed from a single perspective, but rather from a
multiple one. This took into consideration the role of the individual employee, the
collective team, the organisation at large, leadership and policy. The framework
shows an overview of the interplay that extends across the different levels of the
various stakeholders involved in the management of the innovation process. The
enabling processes at each level created other adaptive outcomes as well as
sustainable improvements, faster solutions and shared practice. Although it is not
explicit within the framework how policy might interact directly with an individual or
the team, it would seem that the exchange of knowledge within interactive spaces
reduces the power barrier and encourages freedom. The framework shows that
readiness at one agent level is not sufficient to generate the impetus required to
drive a readiness for innovation in the healthcare systems. Contrariwise, it indicates
that the result of the interacting agents working together enables the system to
sustain and deliver the right level of readiness for innovation in healthcare.
234

Figure 7. 1: A framework for developing and enacting a state of organisational readiness for innovation in public healthcare services organisation
235

7.4 The strengths and limitations of the research and future directions
This thesis has provided conceptual clarity by extending the literature (Weiner, 2009;
Attieh et al., 2013; Stevens, 2013) on organisational readiness for innovation and
doing the same for the theoretical and practical knowledge on the topic. The
proposed theoretical framework for managing readiness in the public healthcare
services organisation in the UK is a unique contribution with transferable findings for
local Trusts and practitioners. This section further stipulates the main strengths and
limitations of the present research.
The first significance of the research is that it is one of few that have considered the
construct of readiness through the lens of the complex adaptive systems theory. The
application of the complexity theory regarding healthcare is nascent, but has been
recently attracting much interest about how it can be used to solve healthcare
problems. Therefore, the findings from this thesis can inform healthcare
professionals on the theory and practice of innovation readiness. There is also the
novelty of the view that readiness is iterative and does not, or better, should not,
cease at the end of an innovation. The findings confirm that the application of
complex adaptive system principles should enable public healthcare systems to
learn how they should respond to changes, accordingly.
The second outcome from this study is that the findings provide an overview on how
complexity thinking can affect the practice of leadership in order to move healthcare
into a state of readiness for innovation. The findings support the complexity theory
regarding leadership which seems better suited for the constantly evolving
knowledge-based economy that exists in healthcare today. The findings expand the
scope of leadership beyond the mere level of commitment as shown in the readiness
literature. They further indicate the key characteristics and behavioural traits of a
leader in managing readiness within a complex system. However, unlike other
traditional views of leadership, the systems leadership theory does not have many
real world examples in healthcare which makes it difficult to apply in practice.
236

The purpose of this thesis was to explain how a complex organisation such as NHS
England could create and maintain a state of readiness for innovation in order to
make it adaptive and effective in coping with the complexities of the innovation
management process. The interviews were a useful tool in generating in-depth
information on the personal accounts of senior leaders and their experiences of how
readiness could be defined, facilitated and enacted. Instead of relying on just the
leaders’ perspective, the inclusion of other stakeholder groups, such as the clinical
staff (implementers) and other members of the organisation, will enrich further
understanding about sharedness of those definitions and of the key perceived
factors that can support the state of readiness.
Reflecting upon the limitations of this research, some points should be considered.
The organisations from which participants were recruited were based in London and
south east of England which made the findings, to some extent, context specific.
This study was also limited by its qualitative nature and so generalisations could not
be made. Therefore, it is being recommended that further research be conducted on
the subject from a longitudinal, multi-organisational and multi-site approach using
comparative methods to try and explain the determinants and processes of
readiness for innovation.
The research raised some issues regarding the use of an integrative framework in
the study of organisational readiness for innovation. It is important to point out that
the lack of empirical evidence about the usefulness of an approach that applied the
complex adaptive systems theory “does not indicate a lack of effect, or that theories
or interventions are ineffective, as there may be a few studies of good quality
available from which to draw conclusions” (The Health Foundation, 2010, p. 5).
Instead, it provides an opportunity for future research to establish the validity of the
theoretical framework for understanding the mechanism that influences the self-
organising characteristics of public healthcare services organisation, that is, the
perpetual movement that makes the complex system adapt and evolve.
There is definitely a place for the use of complex adaptive system theory in
understanding public healthcare systems. However, if the theory is to be turned into
practice and applied by managers and practitioners, it requires more research on
how to put the concepts into practice. The terminology also needs to be simplified.
237

The proposed theoretical framework provides an interesting and useful starting point
for developing and sustaining innovation readiness in an organisation. It is beyond
the scope of this thesis to test the feasibility, acceptability and effectiveness of such
a framework in managing the readiness for innovation process. Therefore, it is being
proposed that the following questions should be addressed in future studies: How
feasible and applicable is the framework for being ready to innovate? What is the
optimal level of the enablers when moving toward a state of readiness? How can the
strength and weakness of the enablers be determined? How does complex adaptive
system evolve over time to maintain readiness? What are the specific characteristics
of public healthcare services organisations that are in a continuous state of
readiness?
7.5 Conclusion
In closing this discussion, the aim was to shed the light on some of the key factors,
for example communities of practice, free spaces, systems leadership, collective
leadership, distributed leadership, and transformational leadership that would make
healthcare services organisations innovation ready. Developments in organisational
readiness for innovation have focused mainly on a micro-level analysis on the role of
individual contextual factors in influencing behaviours towards innovation adoption.
Within this context, the findings from this thesis allowed a consideration of how
readiness may evolve over time, what the conditions might be, the momentum and
the approach required to keep an organisation in a perpetual state of readiness.
Consequently, these results have implications for policy initiatives and the decision-
making carried out by the organisational leaders in the healthcare system.
238

AppendicesAppendix A: Systematic review search strings
Medline (EBSCO) search strategy
Syntax guide/-index term (MeSH) heading)$- adds no or more characters#- to cover z or sexp- explode: includes narrower terms to the index term being exploded?- adds no or one character*- explore different definition
String number
Search strings Results
A 1 KW "innovat*" 107,7422 AB "innovat*" OR TI "innovat*" 62,4473 KW "invent*" OR TI "invent*" 56,1584 "invent*" 76,6595 MH "Inventions" 2146 MH "Entrepreneurship 1,8507 MH "Organizational Innovation" 20,4508 AB Organizational Innovation OR TI Organi#ational Innovation 199
9 Organizational Innovation 8,546
B 10 KW "System innovation$" 2811 KW "Service innovation$" 6512 KW "Innovation readiness" 613 KW "readiness for innovation" 414 KW "Innovation management" 5315 KW "managing innovation" 13
C1 16 KW "change" 746,234C2 17 KW "organi#ational change" 1,193
18 KW "change readiness" 8719 KW "readiness for change" 98120 KW "determinant# of change" 155
21 KW "change readiness scale" 122 KW "change manage*" 695
D 23 KW "readiness" 8,63924 KW "system readiness" 1225 KW "prepar*" 735,88626 KW "adopt*" 148,703
E 27 KW "performance" 586,79928 KW "indicat*" 2,321,03029 KW "scale" 393,98530 KW "assess*" 1,979,270String number
Search strings Results
31 KW "measure*" 2,249,77532 KW "evalu*" 2,402,91833 KW "apprais*" 33,232
F 34 (MH "Delivery of Health Care") 63,36335 KW "Health service delivery" 947
G1 36 KW "Organi#ation" 608,660G2 37 KW "determinant#" 164,534G3 38 KW "management" 842,739
239
String number
Search strings Results
A 39 S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9 185,343
B 40 S10 OR S11 OR S12 OR S13 OR S14 OR S15 165
C1 41 S16 745,234C2 42 S17 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 2,982
D 43 S23 OR S24 OR S25 OR S26 884,946E 44 S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 7,106,257
F 43 S34 OR S35 64,113G1 46 S36 608,660G2 47 S37 164,534G3 48 S38 842, 739
49 S39 OR S40 185,34350 S41 AND S49 17,64051 S42 AND S49 98552 S43 AND S49 878353 S44 AND S49 100,53754 S45 AND S49 3,08255 S46 AND S49 31,71256 S47 AND S49 1,77957 S48 AND S49 22,50958 S23 AND S49 50659 S24 AND S49 4 (irrelevant)60 S25 AND S49 6,667(irrelevant)61 S26 AND S49 5682 (irrelevant)62 S27 AND S49 10.233(irrelevant)63 S28 AND S49 23,373(irrelevant)64 S29 AND S49 25,193(irrelevant)65 S30 AND S49 46,272(irrelevant)66 S31 AND S49 37,699(irrelevant)67 S32 AND S49 35,803(irrelevant)68 S33 AND S49 (1392)69 S49 OR S50 OR S51 OR S52 OR S53 OR S54 OR S55 OR S56 OR
S57 OR S58 OR S59 OR S60 OR S61 OR S62 OR S63 OR S64 OR S65 OR S66 OR S67
185,343
String number
Search strings Results
70 Limiters - Date of Publication: 20040101-20141231; English LanguageNarrow by SubjectMajor: - delivery of health careNarrow by SubjectMajor: - diffusion of innovationNarrow by SubjectMajor: - organizational innovationSearch modes - Boolean/Phrase
N=6756Articles selected- 243
240

CINAHL search strategy
String number
Search strings Results
A 1 KW"innovat*" 23,8732 KW "invent*" 17,4553 MH "Entrepreneurship 1,8814 MH "Organizational Innovation" 76
B 5 KW "System innovation$" 156 KW "Service innovation$" 427 KW "Innovation readiness" 38 KW "readiness for innovation" 39 KW "Innovation management" 510 KW "managing innovation" 10
C1 11 KW "change" 95,213C2 12 KW "organi#ational change" 7,294
13 KW "change readiness" 3514 KW "readiness for change" 46615 KW "determinant# of change" 3616 KW "change manage*" 695
D 17 KW "readiness" 3,51018 KW "system readiness" 219 KW "prepar*" 44,54020 KW "adopt*" 22,360
E 21 KW "performance" 76,66822 KW "indicat*" 148,44623 KW "scale" 76,52424 KW "assess*" 370,04925 KW "measure*" 285,74026 KW "evalu*" 399,22127 KW "apprais*" 11,212
F 28 KW "Health service delivery" 375
G 29 KW "Organi#ation" 36,347G2 30 KW "determinant#" 14,184
String number
Search strings Results
G3 31 KW "management" 212,423
A 32 S1 OR S2 OR S3 OR S4 42,835B 33 S5 OR S6 OR S7 OR S8 OR S9 OR S10 76
C1 34 S11 95,218C2 35 S12 OR S13 OR S14 OR S15 OR S16 12,094D 36 S17 OR S18 OR S19 OR S20 68,980E 37 S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 837,781F 38 S28 375G1 39 S29 36,347G2 40 S30 14,184G3 41 S31 212,423
42 S32 OR S33 43,12243 S34 AND S42 3,98344 S35 AND S42 1,01345 S36 AND S42 3,02246 S37 AND S42 23,63447 S38 AND S42 3548 S39 AND S42 1,27249 S40 AND S42 35750 S41 AND S42 570051 S17 AND S42 20652 S18 AND S42 1
241

String number
Search strings Results
53 S19 AND S42 1,34454 S20 AND S42 1,58055 S21 AND S42 224356 S22 AND S42 507657 S23 AND S42 652558 S24 AND S42 11,75459 S25 AND S42 10,15660 S26 AND S42 11,75461 S27 AND S42 57062 S42 OR S43 OR S44 OR S45 OR S46 OR S47 OR S48 OR S49 OR S50
OR S51 OR S52 OR S53 OR S54 OR S55 OR S56 OR S57 OR S58 OR S59 OR S60 OR S61
42,835
63 imiters - Published Date: 20040101-20141231Narrow by SubjectMajor: - research, nursingNarrow by SubjectMajor: - health care deliveryNarrow by SubjectMajor: - instrument validationNarrow by SubjectMajor: - diffusion of innovationSearch modes - Boolean/Phrase
3341n=31
242

Business Source Complete search strategy
String number
Search strings Results
A 1 "innovat*" 291,9252 "invent*" 98,1803 MH "Inventions" 4,8444 MH "Entrepreneurship 27,7365 MH "Organizational Innovation" 1046 KW “Organi#ational Innovation” 12,981
B 7 KW "System innovation$" 928 KW "Service innovation$" 6319 KW "Innovation readiness" 610 KW "readiness for innovation" 711 KW "Innovation management" 8,02212 KW"managing innovation" 277
C1 13 KW “change” 443,061C2 14 KW "organi#ational change" 24,221
15 KW "change readiness" 5416 KW "readiness for change" 16917 KW "determinant# of change" 3918 KW "change manage*" 6050
D 19 KW "readiness" 15,07120 KW "system readiness" 2621 KW "prepar*" 352,68322 KW "adopt*" 169,052
E 23 KW "performance" 733,97124 KW "indicat*" 336,08325 KW "scale" 97,79326 KW "assess*" 296,83527 KW "measure*" 503,20528 KW "evalu*" 600,61729 KW "apprais*" 85,476
F 30 MH "Delivery of Health Care") 76631 KW "Health service delivery" 120
G1 32 KW "Organi#ation" 565,747)G2 33 KW "determinant#" 33,895G3 34 "management" 2,390,142
A 35 S1 OR S2 OR S3 OR S4 OR S5 OR S6 405.234B 36 S7 OR S8 OR S9 OR S10 OR S11 OR S12 8,872C1 37 S13C2 38 S14 OR S15 OR S16 OR S17 OR S18 27,787D 39 S19 OR S20 OR S21 OR S22 526,438E 40 S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 2,131,501
F 41 S30 OR S31 889G1 42 S32 566,384G2 43 S33 33,928G3 44 S34 2,392,234
45 S35 OR S36 405,23446 S37 AND S45 128,05547 S38 AND S45 21,19748 S39 AND S45 31,60549 S40 AND S45 84,33250 S41 AND S45 11751 S42 AND S45 44,15452 S43 AND S45 286953 S44 AND S45 136,60954 S19 AND S45 80955 S20 AND S45 2 (irrv)
243

String number
Search strings Results
56 S21 AND S45 13,44957 S22 AND S45 18,27458 S23 AND S45 31,55059 S24 AND S45 15,88260 S25 AND S45 7,83061 S26 AND S45 16,23362 S27 AND S45 22,15763 S28 AND S45 20,25364 S29 AND S45 3,09465 S45 OR S46 OR S47 OR S48 OR S49 OR S50 OR S51 OR S52 OR
S53 OR S54 OR S55 OR S56 OR S57 OR S58 OR S59 OR S60 OR S61 OR S62 OR S63 OR S64
405,234
66 Limiters - Scholarly (Peer Reviewed) Journals; Published Date: 20040101-20141231Narrow by Subject: - medical innovationsNarrow by Subject: - literature reviewsNarrow by Subject: - sustainabilityNarrow by Subject: - evaluationNarrow by Subject: - creative ability in technologyNarrow by Subject: - creative abilitySearch modes - Boolean/Phrase
2930n=96
244

Psycho Info search strategy
String number
Search strings Results
A 1 KW"innovat*" 44,4212 AB "innovat*" OR TI "innovat*" 35,0953 KW"invent*" OR TI "invent*" 86,4464 KW"invent*" 107,2395 MM "Innovation" 4,2436 MM "Creativity" 15,207
B 7 KW "System innovation$" 138 KW "Service innovation$" 1439 KW "Innovation readiness" 410 KW "readiness for innovation" 511 KW "Innovation management" 59312 KW "managing innovation" 58
C1 13 KW "change" 226,493
C2 14 MM "Organizational Change" 6,90915 MM "Change Strategies" 6516 KW "organi#ational change" 9,40817 MM "Readiness to Change" 56818 KW "determinant# of change" 6019 KW "change readiness scale" 120 KW "change manage*" 192121 KW "change management" 1846
D 22 KW "readiness" 12,04223 KW "system readiness" 224 KW "prepar*" 64,36625 KW "adopt*" 57,718
E 26 KW "performance" 286,92727 KW "indicat*" 476,82628 KW "scale" 221,54229 KW "assess*" 535,55230 KW "measure*" 586,96031 KW "evalu*" 404,52832 KW "apprais*" 22,600
F 33 "MM "Health Care Delivery" 12,71334 KW "Health service delivery" 986
G1 35 DE "Organizations" 16,77036 KW "Organi#ation" 121,529
G2 37 KW "determinant#" 37,785
G3 38 KW "management" 231,361A 39 S1 OR S2 OR S3 OR S4 OR S5 OR S6 162,788B 40 S7 OR S10 OR S11 OR S12 801C1 41 S13 226,493
C2 42 S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 10,470
D 43 S22 OR S23 OR S24 OR S25 130,900
E 44 S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 1,601,938
F 45 S33 OR S34 13,197G1 46 S35 OR S36 130,677
47 S39 OR S40 162,78848 S41 AND S47 12,61749 S42 AND S47 1,21450 S43 AND S47 7,607
245

String number
Search strings Results
51 S44 AND S47 112,78552 S45 AND S47 72853 S46 AND S47 685354 S37 AND S47 1,65355 S38 AND S47 15,69156 S22 AND S47 69457 S23 AND S47 410,57258 S24 AND S47 2,69159 S25 AND S47 4,45360 S26 AND S47 12,83461 S27 AND S47 29,15462 S28 AND S47 41,36863 S29 AND S47 46,41764 S30 AND S47 59,78465 S31 AND S47 27,39866 S32 AND S47 1,63067 S47 AND S48 AND S49 AND S50 AND S51 AND S52 AND S53 AND
S54 AND S55 AND S56 AND S57 AND S58 AND S59 AND S60 AND S61 AND S62 AND S63 AND S64 AND S65 AND S66
407,572N=46
246

Appendix B: Interview guide for NHS study
1. Firstly, can you tell me a bit about yourself and how you came into your current role?
2. Can you tell me within your current role, any work you do relating to innovation management?
Prompt: Can you tell me a bit more about the process of managing innovation?
3. Talking about innovation management, can you tell me what is your understanding of innovation?
Prompt: In your opinion is there any difference between organisational change and innovation?
4. Can you tell me what are the difference, between innovation management and other types of change?
Prompt: Is it any more complex managing innovation than organisational change?
5. Can you tell me what you think is important in terms of successful innovation management?
Prompt: Can you tell me about a recent success or failure? Prompt: What factors do you think were salient to the success or failure and why?
6. When I say the organisation is ready for innovation - what does this mean to you?
Prompt: Have you got any idea from past experiences?
7. Can you tell me experiences you have of organisations that are innovation ready?
Prompt: What made them ready? Prompt: For you how do ready organisations differ from those that lack readiness?
8. If you are put in charge of getting an organisation ready for innovation, what are the key things you would get the organisation to do?
Prompt: What do you consider are the most important things that facilitate successful readiness for innovation and why?
9. What factors do you suggest hinder successful organisational readiness?
Prompt: What implications do external relationships with stakeholders have on readiness?
10. How do you think innovation readiness in healthcare might be different from other sectors?
Prompt: What are the differences if any, in managing innovation in healthcare sector and other sectors?
11. How important is innovation and innovation readiness to the UK NHS?
Prompt: What possible advantages could continuous readiness for innovation have for the future of the NHS?
Prompt: Do you think innovation ready Trusts will have the potential to do more with less and still raise quality of care?
12. Lastly, What can we do to improve the NHS innovation landscape?
Closing comment- is there anything you would like to add?
Thank you very much for your time. Please do you have any questions for me? Is there anyone that would be important to speak to?
247

Appendix C: Interview guide for AHSN study
1. Can you please tell me a bit about yourself and how you came into your current role?
Prompt: What would you say is your main priority presently?
Prompt: How has this role evolved over time?
Prompt: How do you see your role evolving in the future?
2. Can you tell me what the main responsibility of the AHSN is?
Prompt: How has the role of AHSN evolved in terms of working directly with the NHS?
Prompt: How has the role of AHSN evolved in terms of working directly with private industry?
Prompt: How has the role of AHSN evolved in terms of working directly with wider external network?
3. How effective would you say the AHSN works with other innovation vehicles?
For example, I know there is no CLAHRC in this region, but other vehicles such as SEC Strategic Clinical Networks, and the Clinical Senate?
Prompt: How does the AHSN work with the wider NHS innovation landscape?
Prompt: What is the overlap between the AHSN and these other innovation vehicles, in terms of the boundary?
4. What would you say are the key elements that make the different innovation vehicles successful?
Prompt: How do these innovation vehicles measure with regard to the elements mentioned?
Prompt: How do you think the AHSN fits this bill?
Now I would like to ask you specifically about staffs working within the NHS Trusts. One of the things I am interested in my research, is how more time and space can be embedded in NHS staffs day-to-day work for innovative activities.
5. So Guy, in your opinion how would you describe an organisational innovative culture?
Prompt: What are the most important elements in terms of creating this culture?
Prompt: What skills are most critical in this kind of organisation for innovative activities to be embedded in staff’s daily routine?
6. In the current economic climate, do you think staffs working in local NHS Trust have the capacity and time to be innovative?
Prompt: What factors would you say limit staffs innovation capabilities?
Prompt: What factors would you suggest enable staffs innovative capabilities?
Prompt: How do you think the issue of ‘time’ impact on NHS staffs’ innovation capabilities?7. What kind of organisational structure is needed to create this culture of individuals championing innovation?
Prompt: How does the structure of the organisation work in terms of scaling up?
Prompt: What is the salient role of NHS staffs in ensuring effective delivery of an innovative culture?
Prompt: How does the role of NHS staffs evolve in such an innovative culture?
248

8. What is the role of a leader in creating this culture for innovation?
Prompt: What role does the leadership of an organisation play in enhancing innovative capability amongst staffs?
Prompt: How do you suggest the leadership in an innovative organisational culture evolve over time?
9. How does the AHSN play a role in improving effective leadership, culture and collective innovative capability within the NHS?
Prompt: What specific actions do the AHSN take to encourage and stimulate an innovative culture within the NHS?
Prompt: What specific actions can the AHSN take to make the NHS innovation ready by 2020?
10. What can the NHS learn from organisations that have succeeded in creating this culture of innovation?
Prompt: What can the NHS learn from national and international innovative organisations in order to accelerate pace and scale of innovation?
Prompt: What can the NHS learn specifically from the AHSN way of working?
Prompt: If the NHS finally gets it right creating this everyday culture of innovativeness, how would you suggest it sustains it?
Closing comment- do you have any further comments about accelerating the adoption and spread of innovation in healthcare?
Is there anyone that would be important to speak to?
249

Appendix D: Participant information sheet
IntroductionMy name is Tosan Edematie and I am a PhD student at the University of Surrey. I would like to invite you to take part in a semi structured face-to-face interview, as part of my doctoral research project. Before you decide whether to participate it is important you understand why the research is being done. Please take time to read the following information carefully.
What is the purpose of this study?This study seeks to assess what is organisational readiness and explore how readiness is useful for the successful management of innovation.
Why have I been invited to take part in this study?To gain greater understanding of innovation management processes within service delivery organisations the study will conduct semi-structured interviews. This involves the selection of senior staff from healthcare, academia and policy making.
Do I have to take part?No, you do not have to participate. A decision not to participate would not have any impact on your employment status. If you decide to participate your employer will not be aware of your participation, and will not be aware of your responses. You can also withdraw at any time without giving a reason. However, any data submitted up to the point of withdrawal from the study will be used, subject to participant’s agreement.
What will my taking part in this study require?You will be asked to attend a face-to-face interview. The interview will take place at a mutually agreed location and will last no longer than 45 minutes. The interview will be audio recorded, subject to your approval. If you would prefer not to be audio recorded, hand written notes will be used.
What will I have to do?If you would like to take part please send a confirmation email to [email protected] stating of your interest to participate. Please state your contact details and most convenient time to reach you. Then I will contact you in order to arrange for an interview appointment and location.
What are the possible disadvantages of taking part?There are no potential risks involved in your participation.
What are the possible benefits of taking part?It is unlikely that you will benefit directly. But, you have the option of being informed on the overall results of the study. You can contact the researcher- Tosan Edematie: [email protected], six months after the day of interview.
What happens when the research study stops?All data is stored on a secured university server. The research data will be stored securely for at least 10years in line with University of Surrey policy. The results of the study might be published in a scientific journal or presented at a conference. Overall summary of the findings will be available upon request.
What if there is a problem?Any complaint or concern about any aspect of the way you have been dealt with during the course of the study will be addressed. You can contact the Head of Surrey Business School- Professor Andy Adcroft: [email protected]
Will my taking part in the study be kept confidential?Yes. All of the information you give will be anonymized so that those reading reports from the
250

Appendix:
Introductory brief email
Dear…
Supervisors. Dr. Jane Hendy Work number: 0148368743 Email: [email protected] The Department of Health Care Management & PolicyUniversity of Guildford, Surrey GU2 7XH UKSurrey.
Dr Theopisti ChrysanthakiWork number: 01483682511Email: [email protected]
Who is organising and funding the research?The researcher
Who has reviewed the project?The study has been reviewed and received a Favourable Ethical Opinion (FEO) from the University of Surrey Ethics Committee.
Thank you for taking the time to read this Information Sheet.
251
My name is Tosan Edematie and I am a PhD Student at the University of Surrey, placed within the Department of Healthcare Management & Policy at Surrey Business School. I am looking to interview key members of healthcare, policy makers, commissioners and academia in order to gain new insights on how innovation processes can be successfully managed and to provide research on how the NHS can become more innovation ready. You have been identified as someone who can provide a useful perspective on the management and readiness of organisational innovation and therefore we would like to invite you to take part in a short interview. The aim of the interview is to generate knowledge on how health service delivery organisations can be better prepared for innovation. Your participation is essential in developing an in-depth understanding of the key issues and factors. The interviews will last no longer than 45 minutes and will take place at a suitable location and time that is convenient. The information obtained from the interviews will be treated as confidential and will be anonymised. I am aware that you have a very busy schedule but I would be really grateful if you could advise me of your availability – any amount of time you have will be fine. Many thanks for your consideration, Kind regards,Tosan
PhD Research StudentMiss Tosan EdematieThe Department of Health Care Management & PolicyUniversity of Surrey,Guildford, Surrey GU2 7XHUnited KingdomEmail: [email protected] SupervisorsDr. Jane Hendy Dr Theopisti ChrysanthakiEmail: [email protected]; [email protected],k
252

Appendix F: Favourable Ethical Opinion
253

Favourable Ethical Opinion (continues)
254

Appendix G: Consent form
Please complete the whole of this sheet after the Participant information sheet
Initial Please circle one
1. I the undersigned voluntarily agree to take part in this study on organisational readiness for innovation in healthcare service delivery organisations.
YES/NO
2. I have read and understood the Participant Information Sheet provided. I have been given a full explanation of the nature, purpose and likely duration of the study. I have been given the opportunity to ask questions on all aspects of the study and have understood the advice and information given as a result.
YES/NO
3. I understand the interview will be audio recorded and I agree to comply with this.
YES/NO
4. As outlined in the information sheet, I consent to my data being used for this study. I understand that all information collected is held and processed in the strictest confidence, and in accordance with the Data Protection Act (1998).
YES/NO
5. I understand that I am free to withdraw from the interview at any time without needing to justify my decision and without prejudice.
YES/NO
6. I have been given adequate time to consider my participation and agree to comply with instructions.
YES/NO
7. I understand that I am free to withdraw from the study at any time, without needing to justify my decision and without prejudice. However, any data submitted up to the point of withdrawal from the study would be used.
YES/NO
8. I confirm that I have read and understood the above and freely consent to participate.
YES/NO
Name of Participant (BLOCK CAPITALS)……………………………………
Signed....................................................
Date……………………………………..
I have explained the study and the above participant has given their full consent to participant in this research study.
Name of researcher (BLOCK CAPITALS)……..............................................
Signed....................................................
Date……………………………………..
255

Appendix H: Risk assessment form
Consideration Person at Risk
Scale of Risk
Existing Protocols
Additional Mechanisms
Digital audio recording device
Participant and Researcher
Low Back up device immediately after interview.Check device battery capacity prior to interview.Use both device and phone to record.
Ensure at all time that device is turned on during the interview.
Deletion of data from audio recording device
Participant and Researcher
Low Data will be copied onto USB flash drive prior to deletion of data
All back up copies will be saved on to secure university server
Loss of data Researcher High Data will be backed-up onto USB flash drive and server university server
Storage of Data Participant and Researcher
Low Data will be backed-up onto USB flash drive
Anonymity of data collected
Participant Medium All data will be securely storedCodes will be used to anonymize participant
Publication of research finings
Participant Low All data will be anonymized
Protection of confidentiality
Participant Medium Make assurance of confidentiality via consent form
Reaching target number of participants
Researcher Low Seek for larger number of participants that are holders of knowledge in the research fieldSeek potential participants within supervisors contact
Time scale for research
Researcher Low Schedule interview dates in advanceSpecify timeline for interview to be stated and completed
256
257

Appendix I: One complete transcript from the NHS datasetSo, firstly can you tell me a bit about yourself and how you came into your current position?Yeah, so my name is Chris Green and [background noise] Care Intensive Support Team in NHS England. So
career history, I've always been interested in numbers, that’s fairly boring. But what I have done is that I started
off as an accountant, a trainee accountant and qualified and then kind of wanted to move into a different field and
moved away from where I was working and found myself in the NHS. I started off in primary care and it's been
around GP practice but then I wanted to spread my wings so I moved out into private healthcare so I started out
working for a group called BBP in Natfield and places like that and then started to go into acute care.
So I was working for hospitals and key trusts for about eight years as Analytical lead for Urgent and Emergency
Care. And for about two years, I have been doing consultancy work for NHS England around mostly care and
analytics and looking at different organisations, processes and procedures around treating patients in emergency
care settings.
Okay.And so my role now is to look at different organisations that the team go into and look at it from a data
perspective. So we have clinicians, we have operational managers at the senior level, director level, and now I go
in there and I have a look at data, to have a look to see whether I can spot anything that we should be identifying
or tackling before we actually go in there.
So it's a very interesting role, it's a new role. I'm the first person to have this role so it's giving me a lot of room to
just think about whether we are doing things right. Not just going from one thing to the next to the next, that's the
one thing that I found, you were just firefighting all the time and moving and moving. You were learning but I don't
think it was at the pace I probably wanted to learn and this new role allows me to have the time and flexibility to
be able to spread my wings and do my own research.
Okay, fantastic. So is it all about numbers?It is but it’s all about how you apply those numbers as well. So we can have a look at one metric, and say: “This
is going up, this is going down and this has significant variation.” But why is it going up and down?
[Background noise]
We are going to say: “So it's doing this because of this and should it continue, should it not?” So you are taking
data in action, so you are taking a number and you are saying: “What about this? Why is it that it can do this?”
And we dig into it more.
So we can go into an organisation and we can speak to the people delivering this care to the patients, and we
can say “Why is it that this happened, for example, these patients that are admitted on a Saturday have a longer
length of stay? What is it that you are doing different on a Saturday that you are not doing on any other day of the
week?” So it's really kind of moving that from a number and putting it into something which is practical and
applicable to an organisation.
Okay, fantastic. So do you do anything relating to innovation management in your current role?Yeah we do. And I think over the kind of three or four years, I have tried to spend some of my time on things
which are kind of roughly related to my job. And I think Mark would probably allude it to the Google triangle, so
you kind of got 70 percent of my day job is doing what I actually have to do. 20 percent is doing stuff that is kind
of related to my job and 10 percent is doing stuff who knows what might happen.
But I do spend about 20 percent of my time which is around stuff that is vaguely related to my job. It's really really
important because you don't know how you will pick something up. So I spend, the thing with my current job is
258

that I get opportunities to network with an awful lot of different people from different backgrounds and areas of
expertise. And so what we would do is I will go and spend time with them and say right, "What is it that you do,
how do you do it? what's the methodology, what's the research behind it?” and then, I might take a section of
something that somebody is looking at in A and E and then take another section that somebody is looking at in
acute care
Yeah yeah yeah yeah And I will piece those bits together to say this is what we should do more of. And right we should completely
change the way we are looking at something. So innovation is absolutely key at the moment and that is the thing
that I did not have before this contract, time to be able to do as much as I wanted to. Yes, we did it and I won
awards for that. But in my current role, I have got the flexibility to say “This whole day, this whole week, I want to
look at something completely different, a completely different area because it might work out”. This flexibility is
not being afraid to fail at something, because sometimes it may not work out but if you have kind of gone down
the hole and received a methodology that you have actually come up with in the past.
So it is actually a deliberate thing you do?Yeah.
So do you do this at an organisational level or just at an individual level?No. So the whole team is about 12,13 people in the team and the whole point of the team is that we learn from
each other and we share better practices and we hear about good practices and also we are constantly looking
for ‘Why do you do it in a different way?, do you have more people? Do you structure in a different way?”, so that
is constant innovation and is always about “Well, we heard this from a different country, and can we apply that
here in the NHS in England?”, and so yes we can treat new neurological patients in a different way because of
the way that they do it in Scandinavia that is completely different. That prevents people from coming into
admissions and it doesn't clog up the system and so on and so forth. So it is completely based on innovation,
learning from others and sharing best practices.
Okay, fantastic. So talking about innovation management, what is your understanding of innovation? Do you think that it's different from organisational change, other forms of organisational change?That's a good question. Do I think innovation is different from organisational change? I think it is different from
organisational change. Organisational change can just happen because it has to happen. You need to save
money, therefore restructure, do this, do that do that. Is that innovation? No, it is just shuffling the deck of cards
that you got. Innovation, people have to have motivation. They have to be motivated to go through a process of
innovation. They have to kind of go “We want to make a difference, we want to make a difference in XYZ” and so
therefore, how can they look at a particular area to learn from it. So, innovation is not organisational change. I
think that they are pretty much poles apart. One is very much structured; innovation is very much an iterative
process, just constantly changing in a business environment.
Okay. That's interesting. So, do you think, is any more complex managing innovation? From your perspective, it seems more complex. What's the process of complexity? What does it entail?I don't think it's more complex. I think it's complex if you want to make it complex or you want to put a structure
around it. But innovation works better, if you just kind of say to somebody, if I go to my boss and I say: “I got an
idea, my idea is going to be that I am going to reinvent the wheel, it is going to be revolutionary”, and if that
person has the confidence to let me go off and do it and be like “Go on then, you go off and do it”, there is
nothing complex about that. There is no structure involved. I think the problem is, if you tried to constrain
259

innovation. You won’t innovate because you are kind of going “Okay, you can innovate, but you have only got a
week to do this process”, and so you are going to cut corners, you're going to find a quick way to get to A and B.
We need you to come and say “Take your time, don't worry about it, go and speak to these people and do
whatever, put the research in”. I don't think innovation is complex at all, given the right resources, where there is
time, money, space whatever……
Even within…would you say the same thing even within acute trusts?Yeah, I would. But the problem is that they do not have the space, they don't have that time to kind of go: “You
know what? Do not worry about this week. Go off and do that thing you have always wanted to do. Don’t worry
about this week” because there is always something to do. I am not saying there isn’t in my job because my
boss would [laughs] but I have the ability to say: “Okay, I don’t need to do that today, so today I can focus on
something that is really important and meet with you or that person”.
In an acute organisation, they are firefighting all the time.
Yeah, yeah, yeah, yeah.There's always something to do. So they actually can’t say: “Every Friday for the next two months I'm not going to
do any work, I am going to just stay at home and I am going to do something completely different. It's rare to find
an organisation that would go down that route and say “Do you know what? You can do that”. Whether they
should or shouldn't is another question altogether.
Exactly! Because how do you know people are actually been productive? Yeah, yeah. You have to have the confidence in that person, even if you were to go and say: “Write a one page
summary of what your proposal is, what your research project is, what you are hoping to innovate, pitch to your
boss, and then if your boss says yes then right the next four Fridays you can say “I'm not going to be at work.
Even if I’ll be at work by wouldn't be doing any standard work, I'll be doing something slightly different””. So, as
long as it has structure in place, I don't think innovation is complex at all. But there are a lot of problems.
But you said a while ago that there should be no structure so……It's like any process, it can be as complicated as you want, and it should have the right level of complexity and it
should have the right level of structure. So, if it needs to have…..I’m sorry; I suppose that I didn’t explain that. It
shouldn't be overly complicated, it shouldn't have too much structure, it should be as complex as it needs to be,
and it should have as much structure as it needs to be.
So, if it needs ti be that you have every Friday off, then you do that. If it needs to be within a certain timeframe
then it needs to be within that. What it can't be is that it can't be dictated to. Innovation can't be dictated, you can
say: “Right, you are going to come up with something brand new in a week’s time.” That won’t just happen.
Yeah.So, it's as complex and as structured as it needs to be, no more.
Okay. So can you tell me what you think is important in terms of successful innovation management? Do you have any example of a recent success or failure and what was salient to the success or failure of it?So, different products that I've created have taken something that is very very bulk standard in terms of what we
are presenting, in terms of information, and we have transformed the way the organisation had used that
information, like “Right, what is it we are doing different right now that we were not doing last week, last month,
last year”.
And so, I don't think there's any key measurement.
260

YeahI think the only thing I would say is that I always spend time with the people that the innovation was designed to
help. So, innovation was not necessarily designed to help me, it was designed to help other people. So, I spend a
lot of time with my end users, with my customers to kind of say: “What is it then is going to help you? Right from
the start, my innovation is that I'm going to do this” “Absolutely that is a great idea; you should really focus on
that”. Go away, pitch it to the boss and say: “I'm going to be working on this” and he says “Fine, that’s great. You
go off and do that”, and then meeting every now and then with my end customers, and kind of going: “Okay, this
is the first step, I've done this bit”. “Right, that's really good, yes, no”. So, absolutely involving your end users or
customers throughout your innovation is a key measurement of success. I have not really seen anything that has
like a yes, no, as in it is quantitative. But you can kind of say: “Right, are they really happy with it? Are they using
it?” Absolutely, they have done. There are other things I've always developed. If you don't involve your end
customer, you can just forget it because they won’t use it, because it won’t be implemented successfully because
you would think it is actually the best thing in the world and be really really proud of it and then you go and push
it out to somebody, they just kind of go: “No, I'm not happy with that at all.”
True, true. So, from your success criteria, you're quite happy because you've done it. And you've created some technical
masterpiece which is great. However, if no one uses it, what's the point? You have wasted your time and their
time.
Okay. So when I say organisation is ready for innovation, what does that mean to you?I'll take it that they have kind of got the flexibility that they want to do something different or they need to do
something different. I suppose it is the identification that they know that they need to do something different. If
you didn't know that, then why would you innovate? You just think you are the best. I don't know, that's quite a
tricky one there.
Do you have any idea from like past experiences?Sorry, please can you repeat the question?
When I say the organisation is ready to innovate, what does this mean to you?I suppose that they have got the flexibility to free up space and they have got the capability to say: "You can go
off and do something”. I don't think it is any more complex than that. Really, I don't think it's, I see your point
about having a list of things to say: “Oh I can do this, I can do that”.
Yeah, yeah, yeah, yeah. It's a difficult one because it is not like a physical in terms of “this is not is being used and is not been used”. So,
you can work out utilisation, you can't work out utilisation of the staff member, which is obviously quite difficult to
do. You hope it's 100% to be honest apart from when they are on breaks and stuff like that, and when that
doesn't happen. So I suppose, a lot of it is just individuals kind of wanting to do something and saying I can do
this. And it is the question of the bosses agreeing that they can spend time doing what they want to do.
So how do you determine that or how do you identify that at an organisational level?I don't know. I'm not too sure, at organisational level, I'm not too sure. At the department and team level, I think it
will be a little bit easier from a kind of a board level, chief exec knowing that my organisation is ready to innovate.
261
I don't know, unless everything else was fed up from the team and department level up to a certain level and then
he gets in and want a green light we are ready, we are ready But then who would determine that?
Exactly.You need a director of innovation. So, [laughs]….
So, that leads to the next question. So, can you tell me about experiences you have had in organisations that are innovation ready. So you said who would determine that? So what do you think will determine that? Apart from flexibility….Sorry, could you repeat the question?
So, experiences you have of organisations that are innovation ready. So, what made them ready?So,I don't think I've worked in an organisation that is innovation ready at an organisational level. I've worked in
teams that are but I don't think I have worked in an organisation because the problem is NHS organisations tend
to be incredibly large, so you have hospitals with 7000 employees. I don't know how, I don't know how you could
say the whole organisation is ready to innovate. I suppose technically speaking, it comes down to your definition
of innovation, as in what is it that you want to innovate. I want to try and think of something so clinical. Coding,
for example, how do you innovate clinical coding? Okay, so we are going to do something slightly different, we
are to going to get the notes in a different way, it is quite stipulated in terms of what we are doing. I have not
worked in a whole organisation because all the organisations I tend to work in, have been very large, several
thousand. So I think, I have not worked in a whole organisation that is ready for that.
So, at a team level how do you determine that? If your role, you are continuously looking at new ways of doing things, so in a way you are always, should I say that you are always innovation ready? I think so, but the problem is that it gets down to an individual level, an individual on a team. Because you could
have a team of, you know you are taking an organisation of 7000 people and boiling it down to a department of
14 people. In that department, some are going to be: “I want to change, I want to look at different stuff” and some
of them are like: “I'm quite happy doing what I'm doing”. Now is that saying that the department is not innovation
ready? Or is that? Because 50% are and 50% aren’t. Are you saying that the team are innovation ready or not?
Some are, some aren't. You get half the points. I don't know, it always comes down to an individual basis but
then how do you then score that up to go over 7000 employees? I've got this many number of people who said
yes and this many that said no, these people said “ I might be if I could do it in my own different way”. So, it is a
very very individual basis.
Really?My own view? Yeah. Even when you get it down to team psychology, if you are on a team of fourteen people,
when you have a team meeting for example and the boss goes "Right, who is ready to innovate?”, eight people
say yes, the other lot probably put their hand up because they don’t want to be the last ones out. And so, I'd say
that it is a very difficult one to measure whether a team, department or organisation are innovation ready.
Individuals? Absolutely because they will be the ones that are always looking, they will be the ones going to their
boss saying "I've seen this thing, I want to go to this conference, I want to go and speak to that person, I want to
get in some new product that is going to help us do X, Y and Z." They will be the ones kind of pushing things
forward. I think that it's rare that a whole team will kind of go "Yeah we are going to do this" altogether.
262

Yeah, but like in a trust, if you are going to innovate something or if you are going to implement an innovation, you need to get cultural acceptance from everyone.Yup.
Yeah, so how do you determine their readiness?I think ultimately it would come down to team, the boss, the team leader or team manager making a decision as
to whether the team is ready.
Yeah, yeah, yeah.Because I've had that before where it's been kind of dictated that: “We are going to go down this route” and you
kind of go “Oh well, you know”. Some people liked it, some people didn't. Would it serve an innovation? Yeah, it
would. And were we ready for that innovation? Yes, we were. Did everyone accept it? Yeah you know, kind of,
in the end probably yes, but it was a slow burn, the process. So ultimately, it was down to a subjective view of
that individual to come and say "Yes, we are ready".
So coming back to your other point, how do we know that an organisation is ready to innovate? The Chief Exec
says so. He says “I don't kind of know what we are doing, I'm really happy with how things are going, yeah we
are ready to innovate”.
Yeah, so how do you think that an organisation that is ready will differ from another that lacks readiness?Say that again?
So how do you think we can determine a ready organisation from another that lacks readiness?Apart from the obvious, this is speaking to the individuals and finding out, potentially a questionnaire or maybe a
talk. I've seen that before when we were looking at business process modelling and we were talking to say "Can
you do this? Can you do that?" And there was a score, the individuals in the organisation would score
themselves out of one to five and they will give you a score at the end of it saying that “Right, you are ready to do
this”. You can essentially do that. However the questions that would need to be worded in certain ways to kind of
being very very clear in terms of what it is that you are trying to do. I think people might get, you know what you
were saying earlier about organisational change and innovation?
Yeah.
I think people might get the two mixed up.
Yeah, definitely.And so they are going to go "We are ready for change, yeah we want to change". But innovation is not
necessarily change and change isn't innovation. So, the potential to talk it through and question their roots and
find out why organisations stand against them, one or the other.
So if for example, you are put in charge of getting an organisation ready for innovation, what are the key things that you would get the organisation to do?I think I'm trying to understand about current pressures in their workload. I think that what I have found is that
people just tend to firefight in terms of moving on from one thing to the next without taking a break, without kind
of having a look at whether they are doing things the right way. They just kind of do things the way they have
always done it since they've always known it's always worked. Really trying to understand Have we got, do we
need more people? If we got more people in, would people try to innovate a little more? Not necessarily
263

permanent staff but have we got contractors for the next 6 months, would that free up my staff to do something in
a slightly different way.
That's kind of the real challenge, freeing up people's time. The problem is, they don’t think, they just think “I've
got to move on to the next thing I've got, I've got to just get through my work load”, not necessarily “Let’s just take
a break from this for a minute and I'm going to come back to it tomorrow or whenever, I need to spend a bit of
time doing this thing, whatever it is, I am going to pitch to my boss for advice and time and now I'm going to do
things in a different way”. So previously, I might have just gone from this thing to that thing and done it exactly the
same way, but actually I have now looked to this research, I have now structured it in a different way to present it
differently. So it's cut down my time and it has given somebody else a bit more information. It's the time thing,
which is the killer for innovation.
Do you think that giving people time will always make them perceive that they are ready for change, for innovation?I think people perceive innovation as time consuming. And so therefore if you say to people that “We need to do
something different”, those guys would be like “I haven't got time to do something different”. And so therefore,
time is the one currency that people will always think of when they are at work, it is just the fact. So if you say
“Right, we are going to free up some of your time and you are going to do something different”. That’s how
you're going to get people to innovate.
But how do you deal with individuals that just cannot be bothered? Cause some people just want to get on with the day's job, isn't it?Yes, some people won't want to innovate. Some people are quite happy doing things exactly the way they have
always done it. But what you have to do is that you have to try and teach them that if you did it in a different way,
you might be able to do, you know, cut down your hours ordo whatever it is that you want to do, you know, they
might want to come out of retirement or they might just want to do something completely different.
And not just do things the same way, so I might have always looked at outpatients and I just get up and say: “I'm
fed up of doing that. If you did it in a slightly different way, then you can free up more of your time and move on to
something different. So actually, you need to find out what the benefits are to freeing up somebody's time to
innovate. What is going to be the benefit to that individual?
Yeah, you can come and say “the organisation, we were going to save X million pounds at the department level”.
Right, but you need to drill the benefits down to an individual level. And say “Right, this is going to free up 10% of
your time, you are not going to have to do that thing every day. It's now going to be once a week or once a month
or however long you need”, and that's the real thing, it's finding out individual benefits for somebody.
Okay. So what factors would you suggest would hinder readiness?Well, I suppose people who don't want to change, and that can be top down as well, so you could kind of get your
manager or deputy director or whoever to come and say “we are quite happy with the way things are doing”.
I think the time thing is always a crucial thing if you just basically come and say “no, we can't change” and I've
come across organisations who have done that in the past who say “We don't need anything new, we are happy
with the way things are and how we are doing it”. There is always a resistance to change and that can be “Well,
you know, why do we need something different we have always done it the same way” or it could be other people
trying to help you and that can also cause a lot of conflict saying they're doing something different. But once
again, I think the biggest thing is the pressure on people's time and you're going to find out that the biggest
resistance to innovate is that they haven't got the time or ability to do it.
264

Yeah. Do you think external relationships with stakeholders have an implication for readiness at an organisational level?Yes absolutely, yes. I think if your boss or somebody that you work with in your peripheral network is constantly
asking you question after question after question or asking you to do the work, you are just not going to be able
to do that. So that's why when I spoke about innovation, you need to be able to speak to your stakeholders, end
users, customers, call them what you will and say “Right, this is what I'm doing and this is what the benefits are
going to be, and so the benefits realisation come out if we have time to do this for you and a wider network of
people, and the benefits are paramount to identifying whether you want to do it or not”.
If you cannot demonstrate what the benefits are going to be your end users, whoever they are, and stakeholders
at whatever level are going to say “No, no, no, that is not important, I want you to focus on this area”.
Okay. So how do you think innovation readiness in health care might be different from other sectors?I’d say, previous to about two years ago, I would say that readiness was not really financially given in an
organisation and so kind of the readiness or the innovation would become like “Well, we never really need to
innovate because we know what we are doing, our budgets are the same, year in, year out, we treat the same
number of patients, why do we need to change?”. However, I think that about two, three, four years ago, budgets
and finances have come under constraints so people are looking to other sectors, have always been looking at
trade efficiency, looking at lean processes, whatever that is. But I think that the biggest challenge as well is that
the NHS deals with patients, deals with people, and other sectors may be a service led organisation would be
fairly similar to the NHS. However, it's always going to be how is that innovation going to benefit the end users of
the NHS at the end of the day and that's the patient. So, it's quite difficult in my area, which is analytics. How can
I benefit the patient by doing something different over here? How can it make a benefit to the end patient? And
so that's a real big key difference between the NHS is that what is that end of the day that we are trying to do.
There is no point in innovating something massive over here it has no end user justification to the patient at the
end of the day. That's it for me.
So how important is innovation and innovation readiness to the UK NHS?I’d say it is paramount. There has been a phenomenal mark in innovation in the NHS; some of it gets publicised,
some of it doesn't. You only got to have a look at some of the robotic surgery that happens nowadays, the remote
access so doctors do not need to be in your same location. You know, a phenomenal amount in terms of
analytics as well, the kind of products we can now develop to have a look at different things, tools to identify
patients who are going to come into hospital, the chances of them dying in the hospital, all these different types
of things.
I think that the NHS has been absolutely massive around innovation and it is not going to change, it is not going
to go away. I think it is going to be able to innovate even more and more over the next five years, the five year
forward view, just that now it is going to become tougher because the whole environment……
Yeah, yeah.The NHS is going to be an awful lot tougher, there is going to be a lot of competition out there, the patients are
going to become more elderly, aging population so how do we therefore, how do we treat the patients in a slightly
different way? Do we need different services from the community? So the need for innovation is only going to
increase over the next five years.
So what possible advantage do you think readiness for innovation could have in the NHS?
265

It is that people would just know what to expect. At the moment, you have people would kind of going “We have
done this, we have freed up some time, so we can develop products”. So you have to go “How can we use this
example they have had, they have freed up some time to do this, how can we then do that it?” It is getting back to
that motivation to want to innovate, so if a team kind of goes “Yeah right, we want to innovate, how do you put
them in contact with other people to kind of say “We are working in X field as well and we have done this. We
could help you do it as well and bring it to your organisation and help you save money or save time or save
whatever it is that you want to do”. So once again, this is kind of coming back to the team that I work in now,
learning from others and sharing best practices to kind of go “If they have done it over there, then why can't we
do it over here”.
And it’s economies of scale as well because one team does it, another team does it, another team does it and
they are just going to feed it up to the organisation, all different health economies, these different areas and the
benefits could be absolutely huge but people have got to want to do it as well.
Lastly, what can we do to improve the NHS innovation landscape?I think we need to talk about it more. I think a lot of it is done behind closed doors or people see it at the end goal.
They don't get necessarily see innovation as kind of a process: they would just think of innovation and think of a
really massive innovation, they won’t necessarily think of “I have made this tiny change” and that change has a
big impact to the health scene.
True.They would see some of the robotic surgery and you go “Wow that's amazing, look at that, that’s a huge
innovation”. Yes, absolutely it is. However, innovations can be really really small as well. You know, a tiny little
change in practice why is that not innovation as well? And so I think that's a real big one. Please can you say the
question again?
What can we do to improve the NHS innovation landscape?I think it is that but then it is also about giving people an opportunity to innovate as well. Giving people the
freedom and a bit more chances to experiment a bit more with their time, to have the ability to kind of be able to
go out and speak to a person, go out and learn different things. It is trying to develop the individual as well as
what will benefit the whole organisation. And so, really spending time with an individual cause then you would
encourage them to come and say, and then try and develop them. It's all right, it's simple things like doing that as
part of an annual brochure and putting in their ideas about developing something or innovating something else;
to kind of have a bit of structure in place, but not a complex structure. As complex as it needs to be.
Why do you think that some innovations are less readily adopted even in the space of evidence, so for example the remote technology care, why isn't it widely adopted?It's a difficult one but it's particularly around finances. Some of the innovations do require a heavy outline in the
first instance, and that's why a lot of these innovations are best if they are rolled out really really quickly. So
sometimes it's just a process change.
Exactly.Or we are going to do something slightly different which is going to have a big impact because I'm going to do
something slightly different, this person is going to do something slightly different rather than just….Big
innovations like that have a massive impact, not going to deny that. However, the initial financial impact is huge.
Therefore we are going to get that back, so you know that the impact finances always has.
266

Yeah true. Okay. Is there anything you would like to add?No I don't think so. I think it's going to be great to see what you do and how it looks like in the end. I think there
are a lot of people out there who wants to innovate but it keeps coming back to no time, and people are going to
say “If you want to do that in your own time, then that's fantastic”, and people are going to be like “I want to
innovate but I want to do it in what time”.
That's where the aspect of readiness comes in, because if readiness is a state of an organisation. So, if the organisational members always feel ready to innovate, then I think innovation will come naturally, so it has to do with the culture of the organisation.Yeah.
Giving them the space and the support and the time to create and do something different.Yeah.
Okay, that's it really. Thank you very much for your time.No, that's my pleasure. No worries.
Do you have any questions? No, no.
267
Appendix J: One complete transcript from the AHSN dataset (0:00) Okay. So, please can you tell me a bit about yourself and how you came into your present role?So, I've been working in the NHS since 1993.
Okay, that's long.My, the first seventeen years of that, I think it's about seventeen years, I was working in typically London acute
teaching hospitals and in a, what the NHS might call a business or general management role. So working with
clinicians of all sorts, or professionals of all sorts typically looking at how do we manage and improve services.
Mostly, on the small service end of things and then the last role within Guy’s and Tommy’s, having a more of a
cross trust role to do with cancer services so I was the general manager from oncology and haematology. As a
lead cancer manager, we would talk to and provide data and information services to all the other surgical
services around other parts of the trust. And also we were involved in developing services and informatics flow
between trusts and the network, so having a sort of wider aerial view. Most of those teaching hospitals are
intertwined with researchers and organ institute so if it's Great Ormond Street, you have the Institute of Child
Health next door. So there's a lot between research and service. So, constantly looking at being at, that sort of
leading edge of change. So I thought that would be useful and I go and apply to a strategic health authority
level…
YeahAnd then discover that that is not what SHAs do…
(Laughter)
And in a few years, I was managing an innovation fund looking at wider area improvement processes and then
during those changes I worked for someone called Richard Gleave, who was drafting the guidance on academic
health science networks and because I was supporting him in that process, got involved in helping to support the
local cancer in Kent Surrey Sussex academic health science network proposal and moved into a role where I
typically talked to companies. So I have a corporate role, I have a role around engaging with industry or
improving the engagement between industry and health system. So, during my time from Guys and Tommy’s up
until about two years ago, I did my masters in healthcare management at the University of Surrey.
Ohhhhhhh….My last, the person who oversaw my dissertation was Jane.
(Laughter)
Yeah. Okay, that's interesting. So what's your main priority presently in the AHSN?In the AHSN?
Yeah, within the AHSN.So my main priority is outside of the AHSN.
Okay.Because the future of AHSNs is going to depend more on how do we do things collectively and I am looking to
take a process that we have developed over the last two years within Kent Surrey and Sussex to see how we can
use that across fifteen academic health science networks. That gives added value to industry at a very low cost.
268

We got typically fifteen AHSNs working independently with different resources, different approaches simply by
knowing who to refer to and navigate between them at different times is a potential way of exploiting greater
benefit without anyone having to change much. So I'm quite externally focused at the moment.
So how do you see your role evolving in the future?My idea would be to own the space that covers fifteen AHSNs, but by their permission allows me to refer people
into them and to promote our collective services nationally and internationally.
Hmmm. That's huge.It would be interesting.
Definitely.I have a dream.
(Laughter)
That dream will come true. So, could you tell me, what do you think is the main role of the AHSN? (5:08)To correct market failure.
To correct?Hmmmm
How exactly?So, the NHS back in 1989 was perceived as being poor and inefficient so its levels of accountability and how it
performed were seen as a political issue. So, the Act of 1989 which was enacted in 1990 was to create a
commissioner provider split and what that did was create a number of independent organisations that owned part
of the patient pathway.
Okay.For probably seven or eight years, there was change within the NHS which was simply about how do we move
into this new paradigm whether it was something called the internal market and the intention was by giving
people more local autonomy, that they would compete and perform better. So an element of trusting people to
do things is a way of motivating them to do them so you reduce the direction that is given to them and you
encourage people to use their own initiative and then give them freedom to do things and potentially to compete
for patients. Alongside that process was the introduction of a payment mechanism which is now called payment
by results which is incomplete. Not all services are contracted on PBR mechanism. The areas that are typically
contracted for are the acute sector. There is a very different contract, now typically block contract which was what
was moved away from 25 years ago, because it's not a way of empowering people. It is, you got community and
typically mental health services are block contract, and then primary care. GP practices are funded in a very
different way again.
So what you have is from a patient or population perspective, a fragmentation of the NHS which means from an
industry perspective now is, there may be an economic opportunity by for example, diagnosing earlier and putting
a point of care testing into GP practice. But a GP practice will never buy the point of care product because it
would cost them and benefit someone else. So they are being performance managed as an organisation. And yet
the opportunity is a system wide process. So unless commissioners can move money around and reach
agreement with all of their providers, which they are typically not able to do, the system doesn't allow them to do
269

it, then you have a fragmented system with what I would describe now as better performing compared with 1990
organisations that are more efficient. And some of that has come about through scaling up so we have got rid of
a lot of small sites. People have scaled up so there is a better economic, there are more, there are economies of
scale.
And so where you have individual focus and a culture amongst senior board members who have set their career
aspiration to being in charge of an organisation, you now have a very strong organisational focus and not a
patient health or patient healthcare focus. So it is not in the interest of everyone to be sharing information on how
they do well. And so you have a competitive market and that means there is difference and government likes the
idea of having competition to drive up performance but doesn't like to admit that there is a downside which is
information or knowledge gets stuck and it is not easily moved. It is no one’s responsibility to move information
around cause that would be anti-competitive. So the competition within the system that was created doesn't
support system wide processes. So we are fixing that failure by moving information around, or moving knowledge
around. That's a personal perspective, I don't know if you would find anyone who would write that down. (10:05)Wow. That was brilliant.
(Laughter)
How has the role of the AHSNs evolved in terms of working with the NHS, the DH, private industries and the wider external networks?So at the same time, in 2012, there was further fragmentation of the NHS in Kent Surrey and Sussex, eight
primary care trusts or commissioning groups to twenty-ish commissioning groups, can't remember twenty or
twenty one, so you had a third fragmentation. And at the same time, something called the Commissioning Board
was set up, now often referred to NHS England or you now see Simon Stevens saying NHS England is the
operational name of the Commissioning Board, and the Department of Health in effect saying that the running of
the NHS is down to NHS England and it isn't the Department of Health. The Department of Health has a wider
health policy role so covering health and care, and in theory informing other government departments on the
contribution they can make towards health and health care . So I don't think Department of Health has its own,
our relationship with the Department of Health is distant. There is an interest from the Department of Health and
Biz, so the Department of Business Innovation and Skills. There is a joint office called the Office for Life Sciences
which sits between DH and OLS. And there is, currently there is a Minister for Life Sciences called George
Freeman. And George Freeman was asked to undertake something called the accelerated access review. So
they have a strong interest in how does industry work better with the NHS and vice versa. And that accelerated
access review is due to report in September about things we might do differently in the innovation space. So
indirectly, we are very interested in the DH from the accelerated access perspective because it would declare
that the academic health science network of fifteen AHSNs has a role to play in delivering those new benefits.
Yeah, okay.So it is not directly, this is because of the OLS and the relationship between Biz and DH that makes AHSNs more
valuable to DH potentially. So we have a secure? route, a stronger secure? route rather than DH direct because
that would go via NHS England. So NHS England fund us and assure us and they in turn are assured by DH,
whereas it's a shorter route to go in discussions in OLS to DH. So we have got a sort of double route.
Okay, so…..Not sure I've answered all of your questions though.
(Laughter)
I haven't touched some, local, NHS?
270

Yeah, private industry and external wider influence.It is clear from the piece of work that Ewan Ferlie, who you have probably come across….
Sorry?Ewan Ferlie, have you come across him in your……
Yes, I have He is a reasonably well known researcher on health service innovation and networks. And he has looked at how,
things like the hijacking of networks has caused them to fail. So, in the cancer network, what worked well in the
cancer network when they were set up was professionals attended and shared information as they were intended
to do, so they were addressing a failure by joining people up across a wider area called a network. They were
seen as successful so the cancer zone was effecting courage to make them the performance managing process.
And when they started focusing on performance management, the clinicians stopped attending so the hijacking
of those cancer networks caused them to fail. They were intended for professionals to share good practice by
skewing the true accountability rate through organisations, but by skewing it to the network and causing it to fail.
(15:12) And that has been important in the language of academic health service networks, of not being seen or
wishing to be seen as anything to do with performance management. But there is a support to people who are
being performance managed.
Okay. That makes sense.So our relationships with our local NHS in the fifteen AHSNs differs, and what you infer the research is indicating
is that the levels of social capital, I'm not sure if he uses that term himself, varies per AHSN.
So if I was to give an example, a comparison with the western England….
YeahTheir managing director has come from, I believe a commissioning background and knows all the other senior
people in the patch. So she started off by knowing people and having a working relationship with them. Guy
came from a SHA role, came from a performance management role and didn't, doesn't know as well all of the
same number of people. And we also have as an AHSN with the exception of the York and Humber AHSN, more
stakeholder organisations to work with. So, we have a bigger challenge in terms of engaging with stakeholders in
the NHS. So, in the Southeast, there are four commissioning groups and we have twenty. They have two
universities; we have seven, six or seven depending on where we draw the line. So their ability to manage their
stakeholders is easier because they have a smaller number. The history in Kent Surrey and Sussex is
adversarial and not cooperative. So we won't do the same, even if it was just a match of numbers, we have got a
background culture of not seeing value in collaborating.
Okay.So we have spent more time getting to where people where a few years ago…
Yeah, yeah.…and building that relationship. And in the meantime, we have now got a new form emerging around the
sustainable and transformational plans of which there will be, I think it's three within the geography of Kent Surrey
and Sussex and two that straddle the border. So our relationships aren't potentially where funding might be for
industry to have products purchased particularly where they straddle and organisations may come through that
route. The transformation fund, so we may now need to realign to new stakeholders or skew our interests to
271

those new forms, and not necessarily where the old forms but we think that the new forms are not as well formed
as people think they are. And therefore, their plans may not be in the, and our opportunity for influence may not
be as good. So we have, we are trying to establish relationships in the shifting field
Yeah…with a large number of stakeholders.
Gosh. You are so knowledgeable.(Laughter)
I'm hoping you were going to tell me that David Clane Smith told you all the same thing.
Nooooo....(Laughter)
He's been around longer in this patch. He's an interesting person cause he's got a lot of personal social capital.
Oh okay…
He's got a very good network that reaches out of the NHS, he’s in non-exec roles and yet I don't think we have
benefitted as much as others. So, again, to look at one AHSN, there's a risk of it’s not representative. When you
look at the fifteen, we have very different structures, very different sizes, very different focus, foci and different
capabilities including our networks and that's some part of what Ewan Ferlie was focusing on was those networks
between senior leaders and health systems. So if it's relevant to you, it might be worth contacting him or getting
Jane. Jane might see it as competition but he is well regarded and you might find some other papers interesting
just to read because like Clane gives a flavour of why networks work or what to address and I believe that it's
about system failure cause if the system that was set up was perfect, you wouldn't need networks.
Hmmmmm….Really?Yeah, if it was perfect, if the system with competition gave us what we need (20:16), what politicians wanted out
of the health system so without, you cannot escape from the fact that healthcare is part of society and therefore it
is political. Saying you should not politicise healthcare, well it's impossible not to politicise it because it is about
our social well-being so it's very difficult not to. So we have a very political issue and therefore it continually
moves and the politics around twenty five years ago is it wasn't good enough and now here's an opportunity for
politicians to benefit from investing in health systems. Not the same as what Tony Blair did, he doubled the
funding over a four, five year period and that hid a lot of the problems that are now emerging.
HmmmmSo there's a strong belief in competition particularly in the Conservative sort of view which competition is good.
That's their spirit, that's their mantra and yet if competition was so good, you wouldn't need to be fixing it by going
and moving information around.
TrueSo, the view was pure competition on its own would drive people to find that information and they would invest in
it but we don't do that and part of this is the problem of the politicians... I don't know if you watch things like the
Health Select Committee?
Mmm mmm...
272

If the current one on the iPlayer is there, it's worth looking at. What you would get a sense of is Simon Stevens
being accountable for things that are outside of the commissioning board's responsibility because the public and
therefore the political perspective of the NHS is that they are responsible for everything, and then you get into it,
healthcare is not the only factor in determining the health of a population.
Yeah, that's trueThere are lots of other things that contribute. Housing, employment, general state of the economy, health care is
only a part of it and yet we perceive health care as where health is, so he doesn't behave like a pure
Commissioner of Healthcare because he's also being held to account for other things.
Yeah, yeahSo he’s not allowed to commission in a hard nose way, basically .So, a lot of politics are tied into it which may be
causing some of the failure.
Okay Maybe the model is right but you are not allowed to effect the model a hundred percent and so with the fix is to
introduce networks.
Okay, makes sense.At a level that seems to be affordable, not necessarily practical. So no one has never done a "What is the
opportunity cost and therefore what should we invest in order to realise that opportunity?” So how that’s how they
came up with the figure of fifty million is good enough for fifteen AHSNs. So it's roughly fifty million a year that is
spent on the collective of AHSNs. No one ever did any sums around what size of benefit that is going to deliver
us because they look at the problem. But it's a political response and we need to fix and show that we are
working towards joining things up. Partly, the AHSNs have a strong aspect to this to do with how do we satisfy
industry who globally make significant billions of pounds worth of investment in the U.K., life science research
and the industry. And therefore it's valuable to the economy. So politically it's not only appealing to the population
for votes, it's appealing to industry for investment.
Hmmmmm. Makes sense.And so, if you go back to the other points around, when you look at what is a Chief Exec, a chief executive is
never going to be fully autonomous because they are in a very political and constantly shifting landscape around
performance.
Okay. That was very informative. Oh, I think you have answered this one already.(Laughter)
Can you tell me how the AHSN works in terms of collaborating with other organisations that focus on improving innovation? So, I know there is no Clark in this region but like other vehicles such as the strategic clinical networks and the clinical senate....I don't think we do.
Yeah. I think I got that as well. But what's the overlap between the AHSN and these other innovation vehicles? In terms of the boundaries…(25:09)
273

So, we share a common footprint with the CRN, but that is about it. What I'm saying, the Senate and what is now
called the clinical networks, they have dropped the strategic.
Okay.…they are now called clinical networks. Our approach to them was I think the word that Guy used was that we
had leadership in their strategic clinical network whose personalities were completely wrong for networking. So,
we just had a wrong character, wrong culture in the network that made it easy for us to collaborate with. We took
an approach of "that's their space; we would do something in a different space". If we come across somebody
that is awkward, we will discuss it with them and agree how to either collaborate in that small area or to
differentiate what we are doing in that area, so not a spirit of collaboration. If I was to try and say what is a good
example of a SCN and an AHSN, I would probably look to Eastern, I would say Eastern AHSN has a better
collaborative approach to their network.
There is an argument that we are both doing the same job and therefore we would be competing or we could be
collaborating. And I think we have taken the view that it was a competitive environment and that wasn't the right
culture for collaboration. And I think Eastern have gotten to the sweet point of it's a collaboration for mutual
earned trust. So their job is to, it's changed, I think if you read the networks and strategic health networks and
senate guidance, it would suggest that they are more towards the supporting of the commissioning process, and
therefore should be raising awareness of opportunities for improvement in innovation to their commissioners. The
dynamics of the health system don't allow commissioners to commission without permission from the providers
and therefore we would say you can't do it that way, you have to have commissioners and providers. And if you
look at the composition expected of STPs, it is commissioners and providers of health and social care and
anyone else that would make that collaboration work. So I think Simon Stevens is confirming a point that you
can't do what all these clinical networks were set up to do. So they have seen their funding gradually reduce
whereas we have seen ours maintained but we are not involved in what Simon Stevens is doing around STPs,
test beds, fan guards, new models of care. So strategically, there's an argument that we are irrelevant because
we are not involved in those things. My discussion with the Office of Life Science yesterday was basically saying
"If we are not going to be in the STP space, we would continue to be irrelevant and not get any funding.” So, in
terms of relationships, we have got a bit of a relationship through the industry side
Yeahof... I bumped into someone this morning, so it is real, of if they want to put something on, they would like us find
people in industry to show what they have got, talk about what they are developing, we will find a way of
producing an event like that so we would run a couple of events for their neuro disability research group. Just to
bring together a more eclectic mix of industry and researchers to talk about what's possible and mark where
current areas of research are. We have a relationship with the clinical research facility at Brighton where we have
made some introductions of companies we have come across who have lacked an evaluation, who need to do
something either as a clinical evaluation or a technical evaluation that the CRF has an interest in, so we have
made some introductions into that space.
So, the NHS is buying in Cancer Sussex, is buying large devoid of capability in that space (30:10). One of the
roles that I had in the SHA was to draft a research strategy for Kent Surrey and Sussex. What I think we alluded
to because it was difficult to confirm was our proximity to London, and the fact that I for most of my time working
in Guy's and Tommy’s had lived in Surrey, could commute to London and be part of a very rich and exciting
research organisation. So lots of people can live outside of London and will travel into London because the
communication lines work for London. So, we have London on our doorstep and partly because of the history of
investing in research and where medical schools are, there's never been a research culture, a strong research
culture in Kent, Surrey and Sussex. So, when you look at the CRN's performance, not the CRN's performance,
274
the performance in trials that are monitored or supported by the CRN in Kent, Surrey and Sussex but they are
delivered through local organisations. When it was Surrey and Sussex CRN conference local research network in
*inaudible*, there were bottom and second from bottom in terms of performance of whichever way you want to
be counted. And then they were now combined to be Kent, Surrey and Surrex CRN and they briefly were not
bottom but they are now back to being bottom again. So there is no history of lots of research and the way
research dynamics works is that if you are not the chief investigator or known to the chief investigator, your
organisation is unlikely to be chosen to be where the trial occurs. So it's an uphill struggle around how do you
generate that, the search and the enthusiasm. So, it doesn't attract staff because there isn't enough of a
concentration of world class research going on.
Okay.Hence my strategic intent of exploiting other people's resources by joining them all up again at a national level
because I have nothing to offer locally. I can talk to companies locally and say let me introduce you to.......
(Laughter)
And I have got fourteen other AHSNs and say let me introduce to you... I've got a greater draw and if I've got that
that bit of working right and can in effect provide a service to others and the exchange being when they have
finished with them and have validated what is needed to be validated, they share it back so we can copy. Then,
they are doing us a favour by validating and de-risking something that we can now take to our members so it's an
exchange of just different services
Okay. That was fantastic. I would specifically like to ask you about staff working within the NHS and how we can incorporate more time and space in their day to day working. So the first question is really, in your opinion, how would you describe and an innovative organisational culture?We have to differentiate between context and content. As an example, when I worked at the Oxford Radcliffe, the
Oxford university, I cannot remember what it is called now, it wasn't the Oxford University Hospitals at the time. I
worked in one of the largest teaching hospitals in Oxford. The capability of the staff was no different to a London
teaching hospital….
Okay…..Where they were less able to be innovative, it was their financial constraint because they were funded on an out
of London rate but had London rates of housing, travel, all that to it. So the economics didn't work for the hospital,
so they were continually constrained financially. But that didn't mean to say that the individuals weren't any less
capable of being innovative or supportive of innovation. Nothing acts as an important differential that wasn't made
by D’Arcy when he talked about ten years ago, five years ago, his innovation plan or whatever it was. He said
we should give time and space so that we could be innovative. (35:05)
Yeah, yeah…..Yeah, fine. Give it to them then. So this is a policy issue of we want to support innovation and we talk up it is
about giving people time and space and supporting an innovative culture and yet our performance management
process is still around organisational efficiency and outcomes. So it is not down to the individual organisation to
be innovative. And there, because of the context might simply squash the innovative opportunity, if you have no
cash, or the way that your organisation is managing cash, you will remove the, I forgot what the term that Trish
uses, slack resources, if you remove all of the slack resources you haven't got it. Just again, a very not
necessarily generalised example, I created opportunity in Guy's and Tommy’s by upscaling. So I had a nurse
consultant per service doing about six services. So I introduced nurse consultants into all of those, I introduced
275

the manager into most of those, some were shared managers so I upped the skill and what that drove was more
insight as to what the issues were and how to effect a change. So they got people out of hospital quicker and
safer and better because the professional care that people were receiving was simply on the bowl.
What happened when there was a slight squeeze on finances was that in the past we would say let’s generate
more income by being more efficient on a larger scale because there was opportunity to do so. A change
divisional general manager said “no I don't want you to grow your way out of this. I want you to reduce your skill
mix”.
Okay So, in that example, there is an individual with the wrong ability making a poor decision which has an impact on
the people further down the chain who are daring to be different but they are not given the freedom or opportunity
to be more innovative. It's a combination of context and capability or content.
How do you create that freedom then?So I don't think you can say 'here is an answer'. I think, so if I was to look at clinicians I met at Great Ormond
Street Hospital who are potentially world leaders in their field, who worked for the professor, the way they created
the opportunity was to go and find a job in a different hospital who believed in what they were doing and saw it as
an opportunity within Great Ormond Street Hospital because it was going to straddle children and young people
and they would say "that's out of scope". Now they have put a kick in themselves because they joined up more
closely between Great Ormond Street and University College Hospital to provide teenager and young people
services, which is what these persons want to do, so it's not necessarily what do I do within that organisation?
Your organisation might be too constraining. Someone has to be creative and determined enough to want to
pursue it. But if you are looking at what will I tell people to do, I won't say you just got to be more creative,
because it needs more than one tear of the structure to want to do something. Otherwise, people know the only
way to.
Yeah…....create the opportunities is to move an organisations or move to do what they want to do. So if I look at Sunny
Davis and how she behaves, her way of driving up the research agenda has been to shout at people louder and
being more fierce or fearful fierceful with people. That has been useful in the early days for driving things up
Yeah…..We are now in the different era where it does not need that attitude. It needs a more supportive attitude. So what
I had said to her or one of her staff is "Shouting at people at Kent, Surrey and Sussex to do more trials will never
work"
True.And it hasn't.
So you have to then say do I, and this is the competition versus collaboration or the distribution of cash issue.
(40:09) We can drive up to some degree the performance by making it competitive. Where you have failure like
in Kent, Surrey and Sussex, the only way around it will be to invest significant sums of money to build the
capability. That then has a disincentive for the staff to say “All I have to do to get money is be really rubbish.”
Hmmmm
276

And therefore what it needs is good judgment and good leadership by those who can justify it and stop people
thinking the way to behave is by doing rubbish but to reward them sufficiently and potentially to reward other
people to their different way and not necessarily your being rewarded is, we are actually going to bring someone
in cause they are not good enough. So you reward the system and to be patient orientated, that you would
reward a system for its non-performance. You would not reward the individuals for non-performance. So it costs,
there is an upfront cost, you would have to have the belief that it is worth investment. If you look at the whole
investment process, until someone has got to the point of a briefer concept of adoption, it has shown that it
delivered things and people wanted, everything else up to that point is risked investment, and someone has to
want to take that risk in order to create that opportunity with the risk it would fail and then they have to do it ten
times to get one success. Then you might get the benefits for that one to say let’s keep doing it. That's how
investors work, it's risk investment.
You talked about good leadership. Can you elaborate more on that, please?Leadership is an extremely broad….
I know(Laughter)
There are times when good leadership might be simply telling people what to do, and what you need is speed of
response and there are times when it may not be urgent or as critical where you have the opportunity to grow
your support and work in a more facilitative and supportive way. So, context is going to describe that good leader
will potentially need to be capable of being adapting to the situation.
So then again, it depends on the context and the content, back to what you were saying. Okay.So that leader has to be appropriate for the context. So are the leaders that we have developed over the last
twenty five years who have been told that the only thing that matters is organisational efficiency. Are they ever
going to be the right people to now lead and sustain the transformation plan? Well, they cannot do command and
control but they have to do facilitation and it's for the detriment of some organisations, for benefit of the
population, not for the benefit of the organisation, to the detriment of the patient. So we, there's a bit of challenge
in shifting the structure of the NHS, the focus of the NHS and it's down to, how did Simon Stevens sell it and
what's the accompanying performance management process that motivates people to behave in a better way or
a different way. What is shifting in the process? Our performance management process, I do not believe it has
changed and needs to change in order for the STPs to become authoritative and responsible so people can see
that and potentially they can see that “If I was the STP Lead, that would do my career good”. So the best pay is
sitting in an organisation, and saying “I'm just going to run my organisation”. So you need to adjust the incentives
to see what's attracting the leaders, the more capable leaders who can adapt to potentially that.
YeahYou might say surely they would do that for no more pay but I think that's unlikely.
(Laughter)
People like the fact that they can retire at a certain age with certain luxuries and they will be motivated by money
to a certain degree.
True, yeah. Okay. So in the current economic climate, what do you think are the challenges for staff working in the NHS in terms of engaging in innovative activities?
277

Understanding how you can contribute in different ways. So the culture of innovation might not mean that
everyone has to be thinking differently and looking for new ways of working (45:22). Some of it could be doing
what you are told to do because that's contributing to the innovation.
Yeah.So, being a good follower may be more important for the majority of staff. If you look at, we are often compared
with Kaiser Permanente, she is very innovative or so we are told but when you look at how they do innovation, a
small team does innovation only. They then prove the constant, they work out the reporting and informatics, it is
necessary to monitor that. It's then rolled across Kaiser Permanente and everyone is expected to then do it and
when you don't do it in Kaiser Permanente, you don't have a GMC on seat to protect you as a doctor, you are
simply sacked. So mechanisms are very different, it works for that commercial setup. It's very small, you can see
how getting the balance right of, it is not to be as innovative as an organisation. It doesn't mean everyone has to
be thinking about new ways of doing things. It is good for the organisation and for patients who we are there to
serve to be a good follower but we don't want slavish followers. We want people who will follow intelligently and
are also encouraged to say "That doesn't work". Or “here is why it doesn't work. May be if we did this”.... So
everyone can play a different role in the innovation process but I don't think it's not everyone's job to be
innovative. We would fall apart if everyone was creative.
But how can we get everyone at least ready to a certain degree for innovation?So I'm not sure we want people to be ready for innovation.
OkayI think that's not the motivation. I think this is a, I've reached and I have said to our exec team when we were
talking about our promotion material. One of our directors said we should put innovation in there somewhere.
And I said to him “innovation is a turn off for a lot of people” They feel that it is someone else's idea that is being
imposed upon them and it's innovation for innovation's sake”. So what do we mean by innovation?
YeahI think what we, the language of innovation is unhelpful sometimes.
It is, yeahWhat we want is to focus on what we have joined to do which is to provide great health care and the innovation
wherever it has come from, from somewhere else. If it works, we should be pleased to be making it better for our
patients. Then there's an argument that actually it is not about patient, it's about the population of which
healthcare plays a part in it. So constantly asking for more money for high cost cancer drugs, at the end of life
care, it's skewing our role. It's inevitable that those who only have a perspective of end of life care in cancer or
want to demand it because drug companies produce it and it's a very inactive issue. Funding is skewed towards
end of life care in cancer, which is why we don't have good prevention, early diagnosis and training services.
YeahBecause they are dull. It's not exciting and it's not innovative. We don’t see the need for it. It's a very difficult sell
but we should be looking at a population in order to be cost effective. We motivate our professional staff by
saying you are the most important person in the room, you need to provide and be fighting for your profession in
this space. So we don't have the wider picture of what is the point of the health system. The health system isn't
278
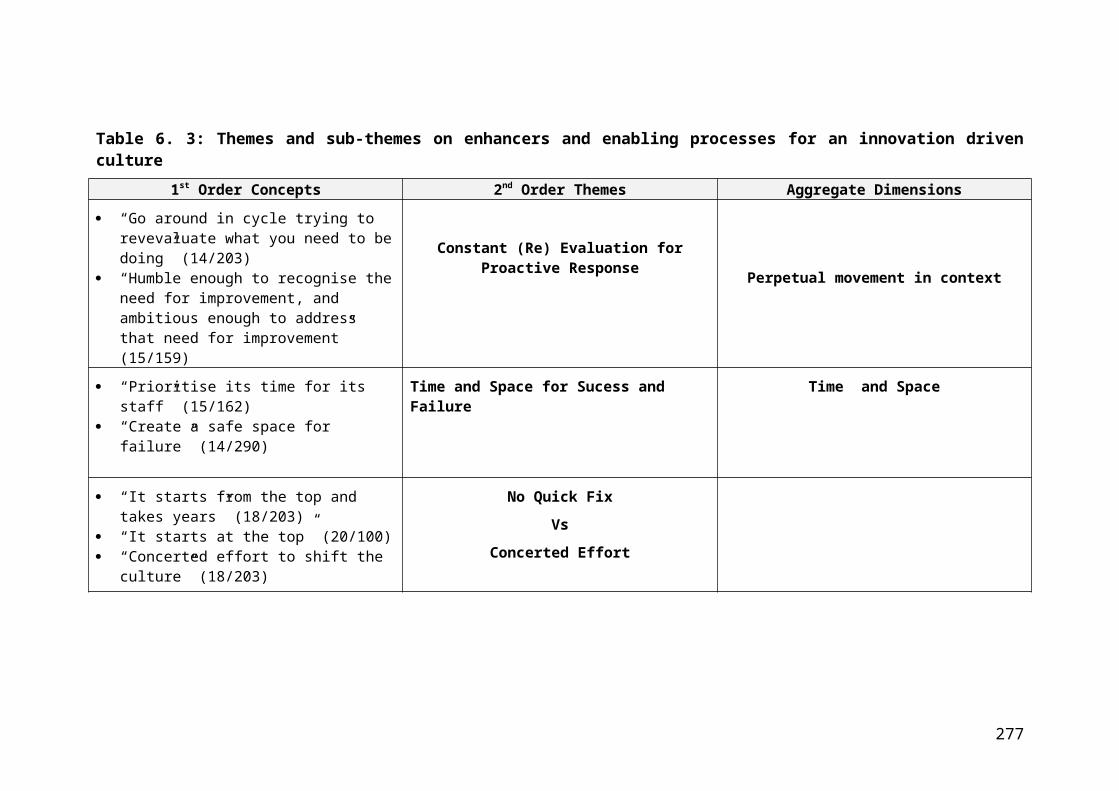
there just to spend money. It's not sustainable if you just spend money. People can come and say I want you to
spend more so the big shift is how do you get society to change its view about its own health?
HmmmmmHow does it keep a healthy lifestyle to avoid it needing healthcare? But ask a consultant medical oncologist what
we should be spending money on and they will probably say "we should be spending on that cancer drug that
GSK has just produced” cause they have a focus that is different (50:00)
YeahSo do we educate people in the view of the wider picture? What is the health service there to do? And the
problem with that is we are then back into the political arena of what are we there to do. We talk about serving
patients and being patient centric but yet when you look at the NHS and how it is structured, it's not patient
centric, it's organisational centric. But we have spent twenty five years in something that isn't patient centric,
claiming that our values are patient centric. So we are not and again politics has got in the way of understanding,
so you can only get people to play in that space if we all have a common view. So going back to the social
capital, sort of how do you get people to play in the same space is by having a common narrative. If they don't all
share a common narrative or have a common goal, they will behave in self-interest…..
Yeah… which is quite normal and should be expected
Of course. So what factors really limits the capabilities of staff to engage in innovative activities?You have to understand better what innovative activities are. If we redefine them as being a good follower, you
then need different skills from if we are saying we want you to be creative. So there isn't no one answer for that.
So ask me the question again?
What factors most limits staffs' capabilities to be innovation ready?As an individual?
Collectively.Oh. So then we might be into: Do we have the right balance of creative good leadership and good followers? So
have we got the mix, the factors in the team right? Or have we got a team full of the same people and do we
encourage lots of the same people in our career structure towards creating the same people and not creating a
balance that is necessary. So one of the team development things that they did at Guy's and Tommy’s, we put
them through a process that talked about differences in people and how to work differences and it's not Myers-
Brigg, it's a different one, it sorts of grades people on "are they affable, directive or I cannot remember what the
four things are, and what we found in the teams that seemed to be making less progress is that they were all very
affable, they all liked each other
(Laughter)
So they didn’t have a driver who was saying “I don’t get being nice, we need to get on with this. They had lots of
people going "what do you think?" "What do you think?" "Would you like to do this?" Sometimes it's about
balance and how do you use what you have and how do you recruit what you have and how do you retain what
you have. And is that part of good leadership? Probably.
So how can we create more NHS innovation champions?I don't want to create any more NHS innovation champions.
279

Why?Because they wouldn't necessarily add value….
You think so?Yeah. Do we need more followers and do we need a different perspective on what we can do in our day job? So
the concept of innovation champions or someone who is good at their job is an innovation champion. So what are
we labelling? What does the label mean and who would we give it to? I don't know at all that he exists.
Okay. So for me, innovation champion would be in an organisation, individuals and teams that are continuously looking to improve the organisation and ready for change.Isn't that what we have in the hierarchy within an organisation? Isn't that what they are being paid to do?
Yeah, but why don't we spread that to the other levels across the organisation?The levels go all the way down to the last person. So, everyone is an innovation champion but are the persons at
the bottom of the pile and they are supporting an innovation process by doing what they are asked to do. So this
concept of innovation champion, let's hold up an innovation champion, how does that help anyone? We have
separated the function or the process of being an effective organisation by saying we are going to identify
different people who aren't doing those key roles to say “oh you are an innovation champion.” What does that
mean? And how does that add value? (55:14)
Well, it just, it means having people that are passionate, how can we create a culture where people are passionate about innovation, constantly looking for new ways to do things, to produce change, to…Aren't they all researchers? Don't they already exist?
What, researchers?Yeah
No. We want staff, it can't always be researchers, because at the end of the day, you bring it down to the work level and then you have resistance amongst nurses and clinicians. But if you have people that are passionate about making change happen rather than just coming in to do their day to day job….First, you look at the organisation comes up with lots of ideas, it would probably be on a per head case.
Southeast Coast Ambulance Service, they have got lots of champions within the Southeast Coast but they don't
implement anything. What they just like doing is being championed for innovation. So we need to be clear on
what we mean by, what is, so is the title innovation champion something that is a retrospective or reward. Is it a
title given to someone because that encourages people to want to be the next champion? Or do you create
someone in a role that no one regards anyway that potentially is in conflict with the line management process?
So if you look at the NHS, it has moved from quality management. So it went through quality, total quality
management and went from ISO2000 or whatever it was, clinical quality, it created lots of roles outside of the
structure and so everyone thought well if it has something to do with quality, that's their job
Hmmmmm…..That’s our quality champion over here, here's our person over there, get them to do it. Whereas what you want is
for everyone to be a quality champion and to championate in their own way. So there's a risk if you create this
thing and you have a negative effect and people going "well, that's not my job, I'm not a quality, I'm not an
280

innovation champion, that's someone else's job". Few would want to be innovative if they can become an
innovation champion. So what we mean by innovation champion is quite critical to, we got to answer what effect
are we trying to achieve and how does human behaviour relate to something called an innovation champion?
How is the title used? Will it change behaviour and may have unforeseen consequences, not the consequence
you expect it to have. So perhaps you need a broader culture of focus on what we want to do and understand the
constraint within it. And the receptive to new ideas, culture but not that just because you have had a new idea
means that it's going to be adopted or that you are going to get rewarded for it outside of doing your day job.
But how do we create that receptive of when new ideas are accepted, a receptive culture?So there are different ways of doing it. You can create it through fear. Do as you are told or you haven't got a job.
That's one way of doing it. So is that an innovation champion? It will have the same effect. This is why it's
important, what to be calling an innovation, what are we trying to achieve by this innovation champion? Cause we
may create the wrong effect. So if we are thinking that what we want is somebody that is just receptive to
innovation, well that's about how you motivate people. So are we back to the leadership, which is leaders are
there to motivate people. So are your leaders not innovation champions? It's not a different work stream, it's the
same work stream.
Okay. So back to leadership, what's the role of leadership in increasing the capacity for innovation amongst staff. How can leadership ensure this capacity is sustained?I looked at what I did in Guy's and Tommy’s; I was able to and saw an opportunity to attract in some very capable
staff who were just sufficiently motivated and capable that they were able to support innovation (1:00:09). So
there's, how do you make it sustainable, well there is an element of, it's to do with everything, it's not a separate
work stream, it's how you do things, it is inheriting a performance process of organisations or the system. So if
you look at, if you look at how the people behave, they are motivated by getting something good out of it. If there
is an opportunity and I think it has been demonstrated through the QOF Process and looking at comparing how
QOF has supported inequalities, which is one of the things, it was intended to do. Actually, what it demonstrated
was that because QOF wasn't different, it was within the existing system and within the existing envelope of pay
and reward. Those who relate to a QOF point benefitted at the expense of someone else.
HmmmmSo it is sort of back to, are we investing something new or we are doing a different spin on what's existing. So,
the risk is that you move the problem, you don't change the problem. You get gaming going on because people
see an opportunity to game what is being offered but it's always to the net, it’s to no net benefit, it's to the
detriment of someone else to the benefit of one person or whatever.
What do you mean exactly by moving the problem, not changing the problem?So we have the QOF as an example, what they have found out is that those patients who are related to QOF
points which brought money into the practice were getting a benefit. They were being sought after to encourage
the intervention that gave them the QOF points but the bandwidth hadn't changed, the sum of money hadn't
changed. So, the people who weren't related to the QOP points got a poorer service. So that's what I mean is, if
the total sum doesn't change, the risk, is all you is you shift the problem. So someone gets a benefit and
someone gets a disbenefit and if you look at Nice, the argument from York Health Economics is, the threshold for
Nice and the approval of cancer drugs in particular has meant that whilst those cancer patients have benefitted, it
has always been to the detriment of other patients.
281

OkaySo there's a risk that you create a process that rewards and is disrewarding....
Yeah, yeahUnless you are adding to it, because as an investor, you can say if I add to it in this way, I am going to get the
long term benefits and it becomes more sustainable.
Okay, so it falls back to the context and the content again....Yes. So I think our next innovation champion, if that's the right term, is the same as the leaders of the sustainable
transformation plans. They are going to have to be innovative and champion change which is what innovation is
about over a wide area, in order to become sustainable. And that is going to permeate through all the
organisations and when they have aligned incentives and performance processes to the STPs, you would see
the potential benefits out of working across a wider area being realised. They are the innovative champions and
they are being motivated by some form of reward…
Hmmm…because it is socially good, it's good for QMAS, it's good for their career, it might be that they get an additional
fund or pay rise from it, it might be a long time benefit, because they have done an STP, they go on to a more
senior role in somewhere else. I think it's difficult to separate innovation from leadership.
Yeah, yeah Not hierarchy. We are all innovation champions but we don't call it innovation, we call it leadership.
So that hierarchy must be there.I don't think you can get away from a hierarchy and if that hierarchy isn’t there, a hierarchy will form.
TrueIt may not be a formalised hierarchy, you may, if you had a network, if everything was just networked and there is
a flat hierarchy, as in there is no hierarchy, people who are incentivised to lead for whatever reason, good and
bad will find a way of influencing, and it is the influence that is leadership. Giving somebody the title of leader
doesn't necessarily mean that they will be a good leader (1:05:08). But there are roles you could play and get
away with within a formalised structure. So do we create chaos? Do you take away all the boards of life and
organisations and see what emerges in five years time? It would be the new world order. There will be new
leadership. We would have spent five years in effect just recreating the same thing.
OkaySo, some of the language used in AHSNs is around policy which might affect things like and, it actually changes,
be clear about the problem you are trying to address. So, people come to ask about innovation and we say what
problem does this address and lots of the time I hear "it's different! It's innovative!” And that’s fine, it’s creative but
it's not necessarily what people want and therefore isn't going to be an innovation, as in we are going to change
but it's not necessarily suitable. What problem are we trying to change or what problem are trying to address and
that's relevant to, if we are going to create innovation champions, what problem are we trying to address and is
that the best way of doing it?
282

Okay.Do we just give the title to managers and say you are the innovation champion? Get on with it.
(Laughter)
Yeah. Okay. So what is the role of the AHSN in creating leadership for innovation? How do they interact with NHS leaders, if at all, to increase…In one respect, it's not our job and we have a bizarre relationship with KSS leadership, so we have people in the
leadership team of HECS, Health Education Care Services, they have an association with the local health
education group but have a national leadership as well as a national leadership. It's full of people who are not
leaders so they have a function to deal with supporting the leadership but they are not leaders. And part of the
problem is they are not perceived as being supportive of the senior leaders and are seen as supporting a policy
intent of how to encourage good leadership and that's very different. So they are not well regarded by the senior
leaders…
OkaySo we work with them possibly to our detriment. We sort of roll as if we are doing network stuff, if you go back to
what I was saying earlier, if you took away the leadership, leadership would emerge and we have assumed it.
This is just three years ago, pre STP, there was a role for System Leadership because nobody was in that space
so by bringing people together and helping them to do things, that is a form of leadership, it's a style of
leadership, it's a consensus sort of related to that type of leadership. It's not saying "I am in charge I will do it all"
it's I've brought it together because I think we can do things together and people will regard you as their leader
even if they don't call you their leader. So by supporting leadership, you become the leader.
TrueSTPs have now arrived and we had something called KSS leadership with us which was not well regarded. So,
we may have a problem in not being able to get into the right space and the dynamics locally and then the new
creation of STPs. A different way of looking at it is by setting a good example about doing change and supporting
people to do change? Are we helping to create that leadership or style, which is we should all be supporting
change. So are we doing this by setting an example process, we are encouraging people to follow, that's a style
of leadership. An informal leadership role is by doing. And you will always find that it's different in every AHSN, so
I think that some are in a better leadership role because they have more followers.
Okay. So the last question is what can the NHS learn from organisations that have succeeded in creating a culture of innovation readiness?Nothing.
(Laughter)
The risk is because the context is so critical…
Yeah…is it doesn't generalise and so unless you look at the context and understand what are the principles, you are at
risk of just annoying people by saying "here is how to do it well". If you can say well we think it's through these
factors” and you then (1:10:14) empower or enable people to have the same disposition, maybe that is the way
you are creating the environment that might enable people to do it but you have to look at everyone's
environment and say what's the common feature. And the common featured amount is the absence of cash. It's
283

squeezing people’s real work to having to work more efficiently or very good but they are probably losing that bit
of creative time to do things.
HmmmmAnd if they are poorly managed because they just feel work is just a bit of a drive, how then do they use their
discretionary time? So a lot of well-motivated people will use their discretionary effort to do things. So if you
demotivate people by making them work harder at work time, you might actually be affecting their discretionary
effort as well. So, are we back to the leadership issue?
Yeah, we areI think leadership and innovation are inseparable. How you get the language of it right...If I look back to the days
in the army, the language was consistent, it is instilled in you early and your employment, your human resource,
your market for your leaders comes from within, so everyone continues with the same language. That has a
benefit of everyone talks the same language and understands the rules of the culture as a disadvantage of the
change it takes a number of generations because it's so well ingrained.
So we haven't done that. We don't have a well ingrained language within the NHS, we all use different
languages. And that has an advantage, it's very inclusive. The disadvantage is that it takes a lot longer to do
anything.
Okay. Yeah, that's the end of the interview. (1:12:12)
284
ReferencesAbduljawad, A. and Al-Assaf, A.F. (2011) ‘Incentives for better performance in health care’, Sultan Qaboos University Medical Journal, 11(2), p. 201.
Aarons, G.A., Green, A.E., Trott, E., Willging, C.E., Torres, E.M., Ehrhart, M.G. and Roesch, S.C. (2016) ‘The roles of system and organizational leadership in system-wide evidence-based intervention sustainment: a mixed-method study’, Administration and Policy in Mental Health and Mental Health Services Research, 43(6), pp.991-1008.
Adam, T. and de Savigny, D. (2012) ‘Systems thinking for strengthening health systems in LMICs: need for a paradigm shift’, Health policy and planning, 27(suppl_4).
Allen, P., Keen, J., Wright, J., Dempster, P., Townsend, J., Hutchings, A., Street, A. and Verzulli, R. (2012) ‘Investigating the governance of autonomous public hospitals in England: multi-site case study of NHS foundation trusts’, Journal of health services research & policy, 17(2), pp.94-100.
Alexander, G., Rantz, M., Galambos, C., Vogelsmeier, A., Flesner, M., Popejoy, L., Mueller, J., Shumate, S. and Elvin, M. (2015) 'Preparing nursing homes for the future of health information exchange', Applied Clinical Informatics, 6(02), pp. 248-266.
Alexander, G. L., Popejoy, L., Lyons, V., Shumate, S., Mueller, J., Galambos, C., Vogelsmeier, A., Rantz, M. and Flesner, M. (2016) 'Exploring health information exchange implementation using qualitative assessments of nursing home leaders', Perspectives in Health Information Management, 13.
Almajali, D.A., Masa'deh, R.E. and Tarhini, A. (2016) ‘Antecedents of ERP systems implementation success: a study on Jordanian healthcare sector’, Journal of Enterprise Information Management, 29(4), pp.549-565.
Amabile, T.M. and Pratt, M.G. (2016) ‘The dynamic componential model of creativity and innovation in organizations: Making progress, making meaning’, Research in Organizational Behavior, 36, pp.157-183.
Anand, P., Exworthy, M., Frosini, F. and Jones, L. (2012) ‘Autonomy and improved performance: lessons from an NHS policy reform’, Public Money & Management, 32(3), pp.209-216.
Anandaciva, S., Ward, D., Randhawa, M. and Edge, R. (2018) Leadership in today's NHS. Delivering the impossible. London: The Kings Fund and NHS Providers.
Anderson, R. A., Issel, L. M. and McDaniel Jr, R. R. (2003) 'Nursing homes as complex adaptive systems: relationship between management practice and resident outcomes', Nursing research, 52(1), p. 12.
Ansett, S. (2005) Boundary spanner: ‘The gatekeeper of innovation in partnerships’, Accountability Forum, 6, pp. 36-44.
285

Antonacopoulou, E. P. and Gabriel, Y. (2001) 'Emotion, learning and organizational change: Towards an integration of psychoanalytic and other perspectives', Journal of Organizational Change Management, 14(5), pp. 435-451.
Apker, J., Ford, W. S. Z. and Fox, D. H. (2003) 'Predicting nurses' organizational and professional identification: The effect of nursing roles, professional autonomy, and supportive communication', Nursing Economics, 21(5), p. 226.
Armenakis, A.A. and Bedeian, A.G. (1999) ‘Organizational change: A review of theory and research in the 1990s’, Journal of management, 25(3), pp. 293-315.
Armenakis, A. A., Bernerth, J. B., Pitts, J. P. and Walker, H. J. (2007) 'Organizational change recipients' beliefs scale: Development of an assessment instrument', The Journal of Applied Behavioral Science, 43(4), pp. 481-505.
Armenakis, A. A. and Fredenberger, W. B. (1997) 'Organizational change readiness practices of business turnaround change agents', Knowledge and Process Management, 4(3), pp. 143-152.
Armenakis, A., Harris, S. and Mosshlder, K. (1993) 'Creating readiness for organisational change', Human Relations, 46, pp. 681-703.
Armenakis, A., Harris, S. and Feild, H. (1999) “Paradigms in organizational change: Change agent and change target perspectives”, in Golembiewski, R. (eds.) Handbook of organizational behavior, revised and expanded. New York: Marcel Dekker.
Armenakis, A. and Harris, S. (2002) 'Crafting a change message to create transformational readiness', Journal of Organizational Change Management, 15, pp. 169 - 183.
Armenakis, A.A. and Harris, S.G. (2009) ‘Reflections: Our journey in organizational change research and practice’, Journal of Change Management, 9(2), pp.127-142.
Armstrong, R (2018a). Miniature tooth sensor can monitor glucose, salt and alcohol levels. Available at: http://digitalhealthage.com/miniature-tooth-sensor-can-monitor-glucose-salt-and-alcohol-levels (Accessed: 18th April 2018).
Armstrong, R. (2018b) Electronic outpatient system to save NHS £50M. Digital Health Age. Available at: http://digitalhealthage.com/electronic-outpatient-system-to-save-nhs-50m (Accessed: 8th April 2018).
Aronson, J. (1995) 'A pragmatic view of thematic analysis', The Qualitative Report, 2(1), pp. 1-3.
Assarlind, M. and Aaboen, L. (2014) 'Forces affecting one Lean Six Sigma adoption process', International Journal of Lean Six Sigma, 5(3), pp. 324-340.
286

Ashkanasy, N. M., Humphrey, R. H. and Huy, Q. N. (2017) 'Integrating Emotions and Affect in Theories of Management', Academy of Management Review, 42(2), pp. 175-189
Ashton, T. (2015) ‘Measuring health system performance: A new approach to accountability and quality improvement in New Zealand’, Health Policy, 119(8), pp. 999-1004.
Attia, M. and Edge, J. (2017) ‘Becoming a reflexive researcher: a developmental approach to research methodology,’ Open Review of Educational Research, 4(1), pp. 33-45.
Attieh, R., Gagnon, M., Estabrooks, C., Legare, F., Ouimet, M., Roch, G., Ghandour, E. and Grimshaw, J. (2013) 'Organizational readiness for knowledge translation in chronic care: a review of theoretical components', Implementation Science, 8, pp. 138.
Attride-Stirling, J. (2001) 'Thematic networks: an analytic tool for qualitative research', Qualitative Research, 1(3), pp. 385-405.
Atun, R., de Jongh, T., Secci, F., Ohiri, K. and Adeyi, O. (2009) ‘Integration of targeted health interventions in health systems: a conceptual framework for analysis’, Health policy and planning, 25(2), pp.104-111.
Atun, R. (2012) ‘Health systems, systems thinking and innovation’, Health policy and planning, 27(suppl_4) pp.iv4-iv8.
Avery, G. C. and Bergsteiner, H. (2011) 'Sustainable leadership practices for enhancing business resilience and performance', Strategy & Leadership, 39(3) pp. 5-15.
Aveyard, H. (2010) Doing a literature review in health and social care: a practical guide. Maidenhead: Open University Press Maidenhead.
Baer, M. and Frese, M. (2003) 'Innovation is not enough: Climates for initiative and psychological safety, process innovations, and firm performance', Journal of Organizational Behavior, 24(1), pp. 45-68.
Bailey, C. (2010) Why keeping your head down may damage your company's future. Available at: https://dspace.lib.cranfield.ac.uk/bitstream/handle/1826/8356/Why_keeping_your_head_down.pdf?sequence=1 (Accessed: 11th February 2019)
Baird, I. S. and Thomas, H. (1985) 'Toward a contingency model of strategic risk taking', Academy of management Review, 10(2), pp. 230-243.
Baker, GR. (2011) The Role of Leaders in High Performing Healthcare Systems. Available at: https://www.kingsfund.org.uk/sites/default/files/roles-of-leaders-high-performing-health-care-systems-ross-baker-kings-fund-may-2011.pdf (Accessed: 11th February 2019)
287
Baker, C. (2017) NHS Indicators: England, October 2017. Available at: file:///Users/tosantraceyedematie/Downloads/cbp07281-oct17.pdf (Accessed: 11th
February 2019)
Bandura, A. (1977) 'Self-efficacy: toward a unifying theory of behavioral change', Psychological review, 84(2), pp. 191.
Bandura, A. (1986) Social foundations of thought and action: a social cognitive theory. Englewood Cliffs: Prentice-Hall.
Bandura, A. (1989) 'Regulation of cognitive processes through perceived self-efficacy', Developmental psychology, 25(5), pp. 729.
Bandura, A. (1990) 'Some reflections on reflections', Psychological Inquiry, 1(1), pp. 101-105.
Barlow, J. and Burn, B. (2008) All change please: Putting the best new healthcare ideas into practice. Available at: https://policyexchange.org.uk/wp-content/uploads/2016/09/all-change-please-dec-08-web.pdf (Accessed: 12th January 2014)
Barlow, J. (2011) Strengthening the spread of innovation in the UK's National Health Service. Available at:https://www.researchgate.net/profile/James_Barlow2/publication/259526997_Strengthening_the_spread_of_innovation_in_the_UK's_National_Health_Service/links/00b7d52c6da2ea27cf000000/Strengthening-the-spread-of-innovation-in-the-UKs-National-Health-Service.pdf (Accessed: 12th January 2014)
Barry, D. (1991) 'Managing the bossless team: Lessons in distributed leadership', Organizational dynamics, 20(1), pp. 31-47.
Bartunek, J. M., Balogun, J. and Do, B. (2011) 'Considering planned change anew: Stretching large group interventions strategically, emotionally, and meaningfully', Academy of Management Annals, 5(1), pp. 1-52.
Bass, B.M. (1999) ‘Two decades of research and development in transformational leadership’, European journal of work and organizational psychology, 8(1), pp.9-32.
Bate, S.P. and Robert, G. (2002) ‘Knowledge Management and communities of practice in the private sector: lessons for modernising the National Health Service in England and Wales,’ Public Administration, 80(4), pp. 643-663.
Batra, N.D. (2014) The first freedoms and America's culture of innovation: the constitutional foundations of the aspirational society. Rowman and Littlefield
Bazeley, P. (2013) Qualitative data analysis: Practical strategies. Sage.
BBC News (2018). Torbay patient Rosie Dawson describes chaos in A&E: BBC News. Available at: http://www.bbc.co.uk/news/av/health-42653694/torbay-patient-rosie-dawson-describes-chaos-in-ae (Accessed: 23rd April 2018)
288

Bernerth, J. B., Armenakis, A. A., Feild, H. S. and Walker, H. J. (2007) 'Justice, cynicism, and commitment: A study of important organizational change variables', The Journal of Applied Behavioral Science, 43(3), pp. 303-326.
Berwick, D.M. (2003) ‘Disseminating innovations in health care’, JAMA, 289(15), pp. 1969-1975.
Bessant, J. (2005) ‘Enabling Continuous and Discontinuous Innovation: Learning From the Private Sector’, Public Money and Management, 25 (1), 35–42.
Bierbaum, M (2015) Innovative business models needed in healthcare – STAT!’. Available at: https://www.beckershospitalreview.com/hospital-management administration/innovative-business-models-needed-in-healthcare-stat.html (Accessed: 22nd March 2018)
Birken, S.A., Lee, S.Y.D., Weiner, B.J., Chin, M.H., Chiu, M. and Schaefer, C.T. (2015) ‘From strategy to action: How top managers’ support increases middle managers’ commitment to innovation implementation in healthcare organizations,’ Health care management review, 40(2), p.159.
Blackman, D., O’Flynn, J. and Ugyel, L. (2013) 'A diagnostic tool for assessing organisational readiness for complex change', Australian and New Zealand Academy of Management Conference, Hobart, pp.4-6.
Boland, R. J. (1979) 'Control, causality and information system requirements', Accounting, Organizations and Society, 4(4), pp. 259-272.
Bolden, R. (2011) 'Distributed leadership in organizations: A review of theory and research', International Journal of Management Reviews, 13(3), pp. 251-269.
Bouckenooghe, D., Devos, G. and van den Broeck, H. (2009) 'Organizational change questionnaire-climate of change, processes, and readiness: Development of a new instrument', The Journal Of Psychology, 143(6), pp. 559-599.
Bowen, G. A. (2008) 'Naturalistic inquiry and the saturation concept: a research note', Qualitative Research, 8(1), pp. 137-152.
Boyatzis, R. E. (1998) Transforming qualitative information: Thematic analysis and code development. Thousand Oaks, CA: Sage Publications.
Boyne, G. A. (2002) ‘Public and private management: what’s the difference?’, Journal of Management Studies, 39, pp. 97-122.
Bozeman, B. (1987) All Organisations Are Public: Comparing Public and Private Organizations. London: Jossey-Bass.
Bradley, E. H., Curry, L. A. and Devers, K. J. (2007) 'Qualitative data analysis for health services research: developing taxonomy, themes, and theory', Health Services Research, 42(4), pp. 1758-1772.
Brant, J. and Lohse, S. (2014) ‘The open innovation model,’ International Chamber of Commerce (ICC).
289

Braun, V. and Clarke, V. (2006) 'Using thematic analysis in psychology', Qualitative research in psychology, 3(2), pp. 77-101.
Braun, V. and Clarke, V. (2013) Successful qualitative research: A practical guide for beginners. Sage.
Britten, N., Jones, R., Murphy, E. and Stacy, R. (1995) 'Qualitative research methods in general practice and primary care', Family practice, 12(1), pp. 104-114.
Brooke-Sumner, C., Sorsdahl, K., Lombard, C., Petersen-Williams, P. and Myers, B. (2018) ‘Protocol for development and validation of a context-appropriate tool for assessing organisational readiness for change in primary health clinics in South Africa’, British Medical Journal, 8(4), p.e020539.
Brown, S. P. and Leigh, T. W. (1996) 'A new look at psychological climate and its relationship to job involvement, effort, and performance', Journal of Applied Psychology, 81(4), pp. 358.
Brown, P., Fraser, K., Wong, C. A., Muise, M. and Cummings, G. (2013) 'Factors influencing intentions to stay and retention of nurse managers: a systematic review', Journal of Nursing Management, 21(3), pp. 459-472.
Bryman, A. (1996) “Leadership in organizations”, in Clegg, S.R., Hardy, C. and Nord, W.R (Eds.), Handbook of Organizational Studies (pp. 276-292). London: Sage Publications.
Bryman, A. (2012) Social research methods. 4th edn. Oxford: Oxford University Press.
Burrell, G. and Morgan, G. (1979) Sociological paradigms and organisational analysis: Elements of the sociology of corporate life. London: Heinemann
Bullinger, A.C., Rass, M., Adamczyk, S., Moeslein, K.M. and Sohn, S. (2012) ‘Open innovation in health care: Analysis of an open health platform,’ Health policy, 105(2-3), pp.165-175.
Burns, J.M. (1978) Leadership. New York, NY: Harper and Row.
Burnett, S., Benn, J., Pinto, A., Parand, A., Iskander, S. and Vincent, C. (2010) ‘Organisational readiness: exploring the preconditions for success in organisation-wide patient safety improvement programmes’, BMJ Quality & Safety, 19(4), pp.313-317.
Caley, M. and Sidhu, K. (2010) ‘Estimating the future healthcare costs of an aging population in the UK: expansion of morbidity and the need for preventative care’, Journal of Public Health, 33 (1), pp 117-122.
Camelo-Ordaz, C., Fernández-Alles, M.D.L.L. and Valle-Cabrera, R. (2008) ‘Top management team's vision and human resources management practices in innovative Spanish companies’, International Journal of Human Resource Management, 19, pp.620-638.
290

Camisón, C. and Villar-López, A. (2014) 'Organizational innovation as an enabler of technological innovation capabilities and firm performance', Journal of business research, 67(1), pp. 2891-2902.
Cankar, S.S. and Petkovsek, V. (2013) ‘Private and public-sector innovation and the importance of cross-sector collaboration’, Journal of Applied Business Research, 29(6), p.1597.
Carlfjord, S., Lindberg, M., Bendtsen, P., Nilsen, P. and Andersson, A. (2010) ‘Key factors influencing adoption of an innovation in primary health care: a qualitative study based on implementation theory’, BMC Family Practice, 11(1), p.60.
Carmeli, A., Gelbard, R. and Gefen, D. (2010) ‘The importance of innovation leadership in cultivating strategic fit and enhancing firm performance,’ The Leadership Quarterly, 21(3), pp.339-349.
Castle-Clarke S., Edwards N. and Buckingham H. (2017) Falling short: Why the NHS is still struggling to make the most of new innovations. Briefing, Nuffield Trust.
Chen, Y-Y. Shek, D. T. and Bu, F.F. (2011) 'Applications of interpretive and constructionist research methods in adolescent research: philosophy, principles and examples', International Journal of Adolescent Medicine and Health, 23(2), pp. 129-139.
Checkland, P. (1999) Systems Thinking, Systems Practice Includes a 30-year retrospective. John Wiley & Sons, Chichester
Chesbrough H. W. (2006) “Open innovation: a new paradigm for understanding industrial”, in Chesbrough H.W., Vanhaverbeke W. and West J (eds) Open innovation: researching a new paradigm. Oxford University Press.
Cho, J. Y. and Lee, E.H. (2014) 'Reducing confusion about grounded theory and qualitative content analysis: Similarities and differences', The Qualitative Report, 19(32), pp. 1.
Choi, M. and Ruona, W. E. A. (2011) 'Individual Readiness for Organizational Change and Its Implications for Human Resource and Organization Development', Human Resource Development Review, 10(1), pp. 46-73.
Choi, J. N., Sung, S. Y., Lee, K. and Cho, D. S. (2011) 'Balancing cognition and emotion: Innovation implementation as a function of cognitive appraisal and emotional reactions toward innovation', Journal of Organizational Behavior, 32(1), pp. 107-124.
Christensen, C. M., Bohmer, R. and Kenagy, J. (2000) ‘Will disruptive innovations cure health care?’, Harvard Business Review, 78, 102-12.
Christensen, C., Grossman, J. and Hwang, J. (2009) The innovator's prescription: a disruptive solution for health care. New York: McGraw-Hill
291

Christl, B., Harris, M.F., Jayasinghe, U.W., Proudfoot, J., Taggart, J. and Tan, J. (2010) ‘Readiness for organisational change among general practice staff’, BMJ Quality & Safety, pp. 1-4
Claire, B. (2013) ‘The incentives for innovation in the private sector’, Recherches Économiques de Louvain/Louvain Economic Review, 79(2), pp.45-81.
Cleveland Clinic Innovations (2017) Top 10 Medical Innovations for 2018. Available at: http://innovations.clevelandclinic.org/Summit/Top-10-Medical-Innovations/Top-10-for-2018.aspx (Accessed: April 8th 2018)
Coch, L. and French Jr, J.R. (1948) ‘Overcoming resistance to change,’ Human relations, 1(4), pp.512-532.
Cohen, W. M. and Levinthal, D. A. (1990) 'Absorptive capacity: A new perspective on learning and innovation', Administrative Science Quarterly, 35(1), pp. 128-152.
Cole, M. S., Harris, S. G. and Bernerth, J. B. (2006) 'Exploring the implications of vision, appropriateness, and execution of organizational change', Leadership & Organization Development Journal, 27, pp. 352-567.
Collins, B. (2018) Adoption and spread of innovation in the NHS. Available at: https://www.kingsfund.org.uk/publications/innovation-nhs (Accessed: 23rd April 2018).
Conner, D. R. (1998) 'How to create a nimble organization', National Productivity Review, 17(4), pp. 31-36.
Cook, D. J., Mulrow, C. D. and Haynes, R. B. (1997) 'Systematic reviews: synthesis of best evidence for clinical decisions', Annals of Internal Medicine, 126(5), pp. 376-380.
Cooper, R. G., Edgett, S. J. and Kleinschmidt, E. J. (2002) ‘Optimizing the stage-gate process: What best-practice companies do-I’, Research technology management, 45, pp. 21-27.
Corbin, J. and Strauss, A. (2008) Basics of qualitative research: Techniques and procedures for developing grounded theory. 3rd edn. SAGE Publications Inc.
Cordery, S (2017) The NHS workforce is under more pressure than ever. But there is hope Available at: https://www.theguardian.com/healthcare-network/2017/nov/07/nhs-workforce-under-pressure-hope (Accessed: 10th December 2018)
Corre, A. and Mischke, G. (2005) The innovation game: a new approach to innovation management and R&D. Springer Science & Business Media.
Coulter, A., Locock, L., Ziebland, S. and Calabrese, J. (2014) ‘Collecting data on patient experience is not enough: they must be used to improve care,’ Bmj, 348, p.g2225.
292
Creswell, J. W. (2013) Research design: Qualitative, quantitative, and mixed methods approaches. Sage publications.
Creswell, J. W. and Net Library, I. (1998) Qualitative inquiry and research design: choosing among five traditions. London; Thousand Oaks, Ca: Sage.
Cresswell, K. and Sheikh, A. (2013) 'Organizational issues in the implementation and adoption of health information technology innovations: an interpretative review', International Journal of Medical Informatics, 82(5), pp. e73-e86.
Crossan, F. (2003) 'Research philosophy: towards an understanding', Nurse Res, 11(1), pp. 46-55.
Crossan, M.M. and Apaydin, M. (2010) ‘A multidimensional framework of organisational innovation: A systematic review of the literature’, Journal Of Management Studies, 47, pp.1154-1191.
Cutler, D.M. (1995) ‘The cost and financing of health care’, The American Economic Review, 85(2), pp. 32-37.
Cutler, D.M. and McClellan, M. (2001) ‘Is technological change in medicine worth it?’ Health Affairs, 20, pp.11-29.
Cummings, T.G. and Worley, C.G. (2009) Organization Development & Change. 9th Edition, South Western Cengage Learning, Mason.
Currie, G. and Lockett, A. (2011) Distributing leadership in health and social care: concertive, conjoint or collective?’, International Journal of Management Reviews, 13(3), pp.286-300.
D'Alfonso, J., Zuniga, A., Weberg, D. and Orders, A. E. (2016) 'Leading the future we envision: nurturing a culture of innovation across the continuum of care', Nursing administration quarterly, 40(1) pp. 68-75.
D’Aveni, R. A (1994) Hypercompetition: managing the dynamics of strategic maneuvering. New York: Free Press.
Daly, J., Kellehear, A. and Gliksman, M. (1997). The public health researcher: a methodological guide. Oxford University Press.
Damanpour, F. and Evan, W. M. (1984) ‘Organisational innovation and performance: the problem of organisational lag’, Administrative Science Quarterly, 29, pp. 392–409.
Damanpour, F. (1991) 'Organisational innovation: a meta-analysis of effects of determinants and moderators', Academy Management Journal, 34(3), pp. 555-590
Damanpour, F. and Aravind, D. (2006) ‘Product and process innovations: A review of organisational and environmental determinants’, Innovation, science, and industrial change: A research handbook, pp. 38-66.
293

Damanpour, F. and Aravind, D. (2012) 'Managerial Innovation: Conceptions, Processes, and Antecedents', Management and Organization Review, 8(2), pp. 423-454.
Damanpour, F. and Gopalakrishnan, S. (2001) ‘The dynamics of the adoption of product and process innovations in organizations’, Journal of management studies, 38(1), pp.45-65.
Damanpour, F. and Schneider, M. (2006) 'Phases of the Adoption of Innovation in Organizations: Effects of Environment, Organization and Top Managers1', British Journal of Management, 17(3), pp. 215-236.
Damanpour, F. and Wischnevsky, J. D. (2006) 'Research on innovation in organizations: Distinguishing innovation-generating from innovation-adopting organizations', Journal of Engineering and Technology Management, 23(4), pp. 269-291.
Darzi A. (2008) ‘High Quality Care for All’. London: Department of Health. p 29.
Dattee, B. and Barlow, J. (2010) 'Complexity and whole-system change programmes', Journal of Health Services Research and Policy, 15 Suppl 2, pp. 19-25.
Denis, J. L., Hebert, Y., Langley, A., Lozeau, D. and Trottier, L. H. (2002) 'Explaining diffusion patterns for complex health care innovations', Health Care Management Review, 27(3), pp.60-73.
Denzin, N. (1970) The research act in sociology: a theoretical introduction to sociological methods. London: Butterworths.
Denzin, N. K. and Lincoln, Y. S. (1998) The Landscape of qualitative research: theories and issues. Thousand Oaks, Calif. London: Sage Publications.
Dess, G. G. and Picken, J. C. (2000) 'Changing roles: leadership in the 21st century', Organizational Dynamics, 28(3), pp. 18-34.
Department of Health (2011a) NHS Chief Executive Innovation Review: Call for evidence and ideas. Available at: https://www.gov.uk/government/publications/nhs-chief-executive-innovation-review (Accessed: 12th January 2014)
Department of Health (2011b) NHS Chief Executive Innovation Review: Call for evidence and ideas. Available at: https://www.gov.uk/government/publications/nhs-chief-executive-innovation-review (Accessed: 12th January 2014)
Department of Health (2013) Guide to the Healthcare System in England Including the Statement of NHS Accountability. Available at:https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/194002/9421-2900878-TSO-NHS_Guide_to_Healthcare_WEB.PDF (Accessed: 14th January 2015)
Dess, G.G. and Picken, J.C. (2000) ‘Changing roles: leadership in the 21st century,’ Organisational Dynamics, 28 (3), pp. 18–34.
294

DiCicco‐Bloom, B. and Crabtree, B. F. (2006) 'The qualitative research interview', Medical education, 40(4), pp. 314-321.
Dirksen, C. D., Ament, A. H. and Go, P. M. N. (1996) 'Diffusion of six surgical endoscopic procedures in the Netherlands. Stimulating and restraining factors', Health Policy, 37(2), pp. 91-104.
Dixon-Woods, M., Agarwal, S., Jones, D., Young, B. and Sutton, A. (2005) 'Synthesising qualitative and quantitative evidence: a review of possible methods', Journal of Health Services Research & Policy, 10(1), pp. 45-53.
Dixon-Woods, M., Amalberti, R., Goodman, S., Bergman, B. and Glasziou, P. (2011) 'Problems and promises of innovation: why healthcare needs to rethink its love/hate relationship with the new', BMJ Quality & Safety; 20 (1), pp. 47-51.
Doody, O. and Doody, C.M. (2012) ‘Transformational leadership in nursing practice,’ British Journal of Nursing, 21(20), pp.1212-1218.
Dooley, K. J. (1997) 'A complex adaptive systems model of organization change', Nonlinear dynamics, psychology, and life sciences, 1(1), pp. 69-97.
Douglas, J., Muturi, D., Douglas, A. and Ochieng, J. (2017) 'The role of organisational climate in readiness for change to Lean Six Sigma', The TQM Journal, 29(5), pp. 666-676.
Doyle, Y., and Bull, A. (2000) ‘Role of private sector in United Kingdom healthcare system’, British Medical Journal, 321(7260), pp. 563.
Drath, W. H. (2001) The deep blue sea: Rethinking the source of leadership. Jossey-Bass San Francisco, CA.
Drucker, P. F. (1985) 'The discipline of innovation', Harvard business review, 63(3) pp. 67-72.
Dubé, V. and Ducharme, F. (2014) 'Reflective practice among nurses working in a teaching hospital: An action research with promising benefits for professional development', Journal of Nursing Education and Practice, 4(8).
Duffin, C. (2011) 'Dragons' Den'initiative offers nurses chance to share clinical innovations; Christian Duffin outlines plans to reward entrepreneurial staff who put forward groundbreaking ideas to enhance health care,’ Nursing Management (Harrow), 18(8), pp.7-8.
Duncan, R. B. (1976) ‘The ambidextrous organisation: Designing dual structures for innovation,’ The management of Organisation, 1, pp.167-188.
Durham University Business School (2019) Dragons’ Den Competition. Available at: https://www.dur.ac.uk/business/research/management/entrepreneurship/dragons-den/ (Accessed: 24th January 2019)
Easterby-Smith, M., Thorpe, R. and Jackson, P. R. (2015) Management and business research. Sage.
295

Eby, L., Adams, D., Russell, J. and Gaby, S. (2000) 'Perceptions of organizational readiness for change: Factors related to employees' reactions to the implementation of team-based selling', Human Relations, 53(3), pp.419 - 442.
Edmondson, A. (1999) 'Psychological safety and learning behavior in work teams', Administrative Science Quarterly, 44(2), pp. 350-383.
Edwards, N (2014) The NHS needs the courage to 'adapt and survive' [Online]. The Independent. Available: http://www.independent.co.uk/voices/comment/the-nhs-needs-the-courage-to-adapt-and-survive-9811961.html (Accessed: 15th July 2015).
Eisenhardt, K.M. and Martin, J.A. (2000) ‘Dynamic capabilities: what are they?’, Strategic Management Journal, pp.1105-1121.
Eisele, P. (2017) ‘Assessment of Leadership for Innovation and Perceived Organizational Innovativeness: Differences between Self-Reported Individual and Social Creativity,’ International Journal of Organizational Leadership, 6(4).
Ely, M., Anzul, M., Freidman, T., Garner, D. and McCormack-Steinmetz, A. (1991) Doing qualitative research: Circles within circles. London: Falmer Press.
Englehardt, C. S. and Simmons, P. R. (2002) 'Creating an organizational space for learning', The Learning Organization, 9(1), pp. 39-47.
Erlandson, D. A. (1993) Doing naturalistic inquiry: A guide to methods. Sage.
Σπανός, Γ. Ε. and Spanos, Y. E. (2009) 'Innovation adoption: an integrative model', SPOUDAI-Journal of Economics and Business, 59(1-2), pp. 100-124.
European Commission (1995) Green Paper on Innovation. Available at: http://aei.pitt.edu/1218/1/innovation_gp_COM_95_688.pdf (Accessed: 25th
December 2014)
Evans, S., and Boyte., H.C. (1986) Free Spaces: The Sources of Democratic Change in America. New York: Harper and Row
Evans, S. and Scarbrough, H. (2014) ‘Supporting knowledge translation through collaborative translational research initiatives: Bridging’versus ‘blurring’boundary-spanning approaches in the UK CLAHRC initiative,’ Social Science & Medicine, 106, pp.119-127.
Evans, A.B., Nistrup, A., Henderson, H., Allen-Collinson, J. and Siriwardena, N.A. (2018) Reflexivity in qualitative research: Two figurational studies. SAGE Publications Ltd.
Fantasia, R., and Hirsch, E.L., (1995) “Culture in rebellion: The appropriatation and transformation of the veil in the Algerian revolution.” In Johnston, H and Klandermans, B. (eds.). Social Movements and Culture. Minneapolis: University of Minnesota Press, pp.144-159.
Fagerberg, J. (2004) ‘Innovation: A Guide to The Literature’, Georgia Institute of Technology. Available at:
296

https://smartech.gatech.edu/bitstream/handle/1853/43180/JanFagerberg_1.pdf?sequence=1&isAllowed=y (Accessed 23rd January 2018)
Faragher, J. and Williams, S. (2014) We put doctors into Dragons’ Den. Available at: https://peoplemangement.co.uk (Accessed 21st November 2018).
Feldstein, A. C. and Glasgow, R. E. (2008) 'A practical, robust implementation and sustainability model (PRISM) for integrating research findings into practice', The Joint Commission Journal on Quality and Patient Safety, 34(4), pp. 228-243.
Fennell, M. L. and Warnecke, R. B. (2013) The diffusion of medical innovations: An applied network analysis. Springer Science and Business Media.
Fereday, J. and Muir-Cochrane, E. (2006) 'Demonstrating rigor using thematic analysis: A hybrid approach of inductive and deductive coding and theme development', International Journal of Qualitative Methods, 5(1), pp. 80-92.
Ferlie, E., Fitzgerald, L., Wood, M. and Hawkins, C. (2005) 'The nonspread of innovations: the mediating role of professionals', Academy of Management Journal, 48, pp. 117 - 134.
Ferlie, E., Fitzgerald, L., Mcgivern, G., Dopson, S. and Exworthy, M. (2010), ‘Networks in health care: a comparative study of their management, impact and performance’. Book Networks in Health Care: A comparative study of their management, impact and performance.
Fiddis, R. (2016) ‘Leadership, innovation & digitisation in the public & private sectors’. The CEO Magazine. Available at: https://www.theceomagazine.com/business/leadership-innovation-digitisation-public-private-sectors/ (Accessed: 15th September 2017)
Fitzgerald, L., Ferlie, E., McGivern, G. and Buchanan, D. (2013) ‘Distributed leadership patterns and service improvement: Evidence and argument from English healthcare,’ The Leadership Quarterly, 24(1), pp.227-239.
Fleuren, M., Wiefferink, K. and Paulussen, T. (2004) 'Determinants of innovation within health care organizations: literature review and Delphi study', International Journal For Quality In Health Care: Journal Of The International Society For Quality In Health Care, 16(2), pp. 107-123.
Flott, K.M., Graham, C., Darzi, A. and Mayer, E. (2017) ‘Can we use patient-reported feedback to drive change? The challenges of using patient-reported feedback and how they might be addressed,’ BMJ Qual Saf, 26(6), pp.502-507.
Fonseca, J. (2002) Complexity and innovation in organisations. London: Routledge
Forrest J. E. (1991) ‘Practitioners’ forum: Models of the process of technological innovation’, Technology Analysis and Strategic Management, 3, pp.439–452.
Fottler, M. D. (1981) ‘Is management really generic?’, Academic Management Review, 6, pp.1-12.
297
Frambach, R. T. and Schillewaert, N. (2002) 'Organizational innovation adoption: a multi-level framework of determinants and opportunities for future research', Journal of Business Research, 55(2), pp. 163-176.
Fraser, S.W. and Greenhalgh, T. (2001) ‘Complexity science: Coping with complexity: Educating for capability,’ BMJ: British Medical Journal, 323(7316), p.799.
French, B., Thomas, L. H., Baker, P., Burton, C. R., Pennington, L. and Roddam, H. (2009) 'What can management theories offer evidence-based practice? A comparative analysis of measurement tools for organisational context', Implementation Science, 4(1), p. 28.
Frey, B. S., and Osterloh, M. (2001) Successful management by motivation: Balancing intrinsic and extrinsic incentives. Springer Science and Business Media.
Gaddis, B., Helton-Fauth, W., Scott, G., Shaffer, A., Connelly, S. and Mumford, M. (2003) 'Development of two measures of climate for scientific organizations', Accountability in Research: Policies and Quality Assurance, 10(4), pp. 253-288.
Galanakis, K. (2006) ‘Innovation process. Make sense using systems thinking’, Technovation, 26, pp.1222-1232.
Gapp, R. and Merrilees, B. (2006) 'Important factors to consider when using internal branding as a management strategy: A healthcare case study', Journal of Brand Management, 14(1-2), pp.162-176.
García-Granero, A., Llopis, Ó., Fernández-Mesa, A. and Alegre, J. (2015) ‘Unraveling the link between managerial risk-taking and innovation: The mediating role of a risk-taking climate,’ Journal of Business Research, 68(5), pp.1094-1104.
Garcia‐Sabater, J. J., Marin‐Garcia, J. A. and Perello‐Marin, M. R. (2012) 'Is implementation of continuous improvement possible? An evolutionary model of enablers and inhibitors', Human Factors and Ergonomics in Manufacturing and Service Industries, 22(2), pp. 99-112.
Gasper, P. (1999) 'Social constructivism. In R.Audi (Ed)', in 2nd (ed.) The Cambridge dictionary of philosophy. Cambridge, UK: Cambridge University Press, pp. 855.
Gergen, K. J. (1985) 'The social constructionist movement in modern psychology', American psychologist, 40(3), pp. 266.
Gergen, K. J. (1987) 'The language of psychological understanding, In H.J. Stam, T.B. Rogers, K.J. Gergen', The analysis of psychological theory: metapsychological perspective. Cambridge: Hemisphere, pp. 115-29.
Gibbons, M. T. (1987) 'Introduction: The politics of interpretation, in Gibbons, M.T. (Ed,)', Interpreting politics. New York: New York University Press, pp. 1-31.
Gifford, J., Boury, D., Finney, L., Garrow, V., Hatcher, C., Meredith, M. and Rann, R. (2012) What makes change successful in the NHS? A review of change programmes in NHS South of England. Available at:
298

https://www.roffeypark.com/wp-content/uploads2/NHS-South-of-England-What-makes-change-successful-report1.pdf (Accessed: 13th September 2014)
Gilburt, H. (2016) Supporting integration through new roles and working across boundaries. Available at: https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/Supporting_integration_web.pdf (Accessed: 13th September 2014)
Gioia, D. A., Corley, K. G. and Hamilton, A. L. (2013) 'Seeking qualitative rigor in inductive research notes on the Gioia methodology', Organizational Research Methods, 16(1), pp. 15-31.
Gist, M. E. and Mitchell, T. R. (1992) 'Self-efficacy: A theoretical analysis of its determinants and malleability', Academy of Management Review, 17(2), pp. 183-211.
Glaser, B. and Strauss, A. (1967) The Discovery of Grounded Theory: Strategies for Qualitative Research. Chicago: Aldine.
Glifford, J., Boury, D., Finney, L., Garrow, V., Hatcher, C., Meredith, M. and Rann, R. (2012) What makes change successful in the NHS? A review of change programmes in NHS South of England. Available at: http://www.roffeypark.com/wp-content/uploads2/NHS-South-of-England-What-makes-change-successful-report1.pdf (Accessed: 12th February 2013)
Godin, B. (2006) ‘The Linear Model of Innovation: The Historical Construction of an Analytical Framework’, Science, Technology and Human Values, 31, pp 639-667.
Goes, J. B. and Park, S. H. (1997) 'Interorganizational links and innovation: The case of hospital services', Academy of Management Journal, 40(3), pp. 673-696.
Goll, I. and Rasheed, A.A. (2005) ‘The relationships between top management demographic characteristics, rational decision making, environmental munificence, and firm performance,’ Organization studies, 26(7), pp.999-1023.
Gomory, R.E., (1989). From the 'ladder of science' to the product development cycle. Scout for technology, design for manufacture, shorten the time to market. Harvard Business Review, 67(6), p.99.
Gong, Y., Huang, J.C. and Farh, J.L. (2009) ‘Employee learning orientation, transformational leadership, and employee creativity: The mediating role of employee creative self-efficacy’, Academy of management Journal, 52(4), pp.765-778.
Gopalakrishnan, S. and Damanpour, F. (1997) ‘A Review of Innovation Research in Economics, Sociology and Technology Management.’ Omega 25(1) pp.15–28.
Gopalakrishnan, S. and Ganeshkumar, P. (2013) ‘Systematic reviews and meta-analysis: understanding the best evidence in primary healthcare’. Journal of family medicine and primary care, 2(1), p.9.
299

Granstrand, O. (2011). The economics of IP in the context of a shifting innovation paradigm. In: Innovation Report 2011: Shifting Innovation Paradigms and the Role of Intellectual Property. WIPO, Geneva.
Grant, R. M. (2001) “Knowledge and organization”. In Nonaka, I. and Reece, D. (eds) Managing industrial knowledge: Creation, transfer and utilization, pp. 145-169.
Greenhalgh, T., Robert, G., Macfarlane, F., Bate, P. and Kyriakidou, O. (2004) 'Diffusion of innovations in service organizations: systematic review and recommendations', Milbank Quarterly, 82, pp. 581 - 629.
Greenhalgh, T., Roberts, G., Bate, P., MacFarlane, F. and Kyriakidou, O. (2005) Diffusion of innovations in health service organisations: a systematic literature review. Malden, Mass. Oxford: BMJ Books/Blackwell.
Greenhalgh, T. (2011) 'Communities of practice', British Medical Journal, 343.
Grimshaw, J., Thomas, R., MacLennan, G., Fraser, C., Ramsay, C., Vale, L., Whitty, P., Eccles, M., Matowe, L. and Shirran, L. (2004) 'Effectiveness and efficiency of guideline dissemination and implementation strategies', Health Technol Assess, 8(6).
Griffiths, F., Cave, J., Boardman, F., Ren, J., Pawlikowska, T., Ball, R., Clarke, A. and Cohen, A. (2012) ‘Social networks–the future for health care delivery,’ Social science & medicine, 75(12), pp.2233-2241
Guba, E. G. and Lincoln, Y. S. (1994) Competiting paradigms in qualitative researh. In N.K. Denzin & Y.S. Lincoln (Eds), Handbook of qualitative research. CA Thousand Oaks: Sage.
Guest, G., Bunce, A. and Johnson, L. (2006) 'How many interviews are enough? An experiment with data saturation and variability', Field methods, 18(1), pp. 59-82.
Gumusluoglu, L. and Ilsev, A. (2009) ‘Transformational leadership, creativity, and organizational innovation’, Journal of business research, 62(4), pp.461-473.
Guzman-Castillo, M., Ahmadi-Abhari, S., Bandosz, P., Capewell, S., Steptoe, A., Singh-Manoux, A., Kivimaki, M., Shipley, M.J., Brunner, E.J. and O'flaherty, M. (2017) Forecasted trends in disability and life expectancy in England and Wales up to 2025: a modelling study. The Lancet Public Health.
Gyensare, M.A., Anku-Tsede, O., Sanda, M.A. and Okpoti, C.A. (2016) ‘Transformational leadership and employee turnover intention: The mediating role of affective commitment,’ World Journal of Entrepreneurship, Management and Sustainable Development, 12(3), pp.243-266.
Hage, J. T. (1999) 'Organizational innovation and organizational change', Annual Review of Sociology, 25(1), pp. 597-622.
Ham, C. (2014) Reforming the NHS from within, Beyond hierarchy, inspection and markets. Available at: https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/reforming-the-nhs-from-within-kingsfund-jun14.pdf (Accessed: 14th February 2015)
300
Hambrick, D. C. and Mason, P. A. (1984) 'Upper echelons: The organization as a reflection of its top managers', Academy of Management Review, 9(2), pp. 193-206.
Harvey, G., Jas, P. and Walshe, K. (2014) 'Analysing organisational context: case studies on the contribution of absorptive capacity theory to understanding inter-organisational variation in performance improvement', BMJ Qual Saf, pp. bmjqs-2014-002928.
Harris, A. (2008) 'Distributed leadership: According to the evidence', Journal of Educational Administration, 46(2), pp. 172-188.
Hauschild, S., Licht, T., and Stein, W., (2001). Creating a knowledge culture. The McKinsey Quarterly, pp. 74-76.
Health Innovation Network (2016) Communities of Practice – Cultivating Change Through Collaboration Available at: https://www.england.nhs.uk/signuptosafety/wp-content/uploads/sites/16/2015/09/ahsn-network-communities-of-practice.pdf (Accessed: 19th December 2018)
Hendy, J. and Barlow, J. (2012) 'The role of the organizational champion in achieving health system change', Social Science and Medicine, 74(3), pp. 348-355.
Hendy, J., Chrysanthaki, T., Barlow, J., Knapp, M., Rogers, A., Sanders, C., Bower, P., Bowen, R., Fitzpatrick, R., Bardsley, M. and Newman, S. (2012) 'An organisational analysis of the implementation of telecare and telehealth: the whole systems demonstrator', BMC Health Services Research, 12(1), pp. 403.
Henderson, R.M. and Clark, K.B. (1990) ‘Architectural Innovation: The Reconfiguration of Existing Product Technologies and the Failure Of Established Firms’, Administrative Science Quarterly, 35, pp.9–30.
Henderson, C., Knapp, M., Fernández, J.L., Beecham, J., Hirani, S.P., Cartwright, M., Rixon, L., Beynon, M., Rogers, A., Bower, P. and Doll, H. (2013) Cost effectiveness of telehealth for patients with long term conditions (Whole Systems Demonstrator telehealth questionnaire study): nested economic evaluation in a pragmatic, cluster randomised controlled trial. British Medical Journal, 346, p.f1035
Herbert C, Best A. (2011) ‘It’s a matter of values: partnership for innovative change,’ Healthcare Papers 11(2) pp 31–7.
Hernaus, T. (2008) 'Process-based organization design model: Theoretical review and model conceptualization', EFZG working paper series, (06), pp. 1-17.
Herscovitch, L. and Meyer, J. (2002) 'Commitment to organizational change: Extension of a three-component model', Journal of Applied Psychology, 87, pp. 474 - 487.
Hobday, M. (2005) ‘Firm-level Innovation Models: Perspectives on Research in Developed and Developing Countries’, Technology Analysis and Strategic Management, 17, pp. 124-146.
301

Hoegl, M. and Parboteeah, K. P. (2006) 'Team reflexivity in innovative projects', Research and Development Management, 36(2), pp. 113-125.
Holden, M. T. and Lynch, P. (2004) 'Choosing the Appropriate Methodology: Understanding Research Philosophy’, The Marketing Review, 4(4), pp. 397-409.
Holt, D. T., Armenakis, A. A., Feild, H. S. and Harris, S. G. (2007) 'Readiness for Organizational Change: The Systematic Development of a Scale', The Journal of Applied Behavioral Science, 43(2), pp. 232-255.
Holt, D., Helfrich, C., Hall, C. and Weiner, B. (2010) 'Are you ready? How health professionals can comprehensively conceptualize readiness for change', Journal of General Internal Medicine, 25(1), pp. 50 - 55
Holt, D. T. and Vardaman, J. M. (2013) 'Toward a comprehensive understanding of readiness for change: the case for an expanded conceptualization', Journal of Change Management, 13(1), pp. 9-18.
Hose, L. (2016) Academic Health Science Networks: Impact report 2016. Improving health and promoting economic growth: The AHSN Network.
Huber, E., Ragin, C. and Stephens, J. D. (1993) 'Social democracy, Christian democracy, constitutional structure, and the welfare state', American Journal of Sociology, 99(3), pp.711-749.
Hughes, G. (2010) ‘Mid Staffordshire NHS Foundation Trust: another progress report,’ BMJ, 27(4).
Huy, Q.N. (2011) 'How middle managers' group‐focus emotions and social identities influence strategy implementation', Strategic Management Journal, 32(13), pp.1387-1410.
Jacobs, S.R., Weiner, B.J., Reeve, B.B., Hofmann, D.A., Christian, M. and Weinberger, M. (2015) ‘Determining the predictors of innovation implementation in healthcare: a quantitative analysis of implementation effectiveness.,’ BMC health services research, 15(1), p.6.
James, K.T. (2011) Leadership in context lessons from new leadership theory and current leadership development practice. Commission on leadership and management in the NHS. The King’s Fund.
Janjua, A. (2014) Leadership vacancies in the NHS. What can be done about them? Available at: https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/leadership-vacancies-in-the-nhs-kingsfund-dec14.pdf (Accessed: 19th December 2018)
Jasperson, J.S., Carter, P.E. and Zmud, R.W. (2005) ‘A comprehensive conceptualization of post-adoptive behaviours associated with information technology enabled work systems’, MIS quarterly, 29, pp.525-557.
Jeans, M. E. (2006) 'Strengthening mentorship for leadership development', Nursing Leadership, 19(2).
302

Jennett, P. A., Gagnon, M. P. and Brandstadt, H. K. (2005) 'Preparing for success: readiness models for rural telehealth', Journal Of Postgraduate Medicine, 51(4), pp. 279-285.
Johannessen, J. A., Olsen, B. and Lumpkin, G. T. (2001) 'Innovation as newness: what is new, how new, and new to whom?', European Journal of Innovation Management, 4(1), pp. 20-31.
John, W. S. and Johnson, P. (2000) 'The pros and cons of data analysis software for qualitative research', Journal of Nursing Scholarship, 32(4), pp. 393-397.
Jones, R., Jimmieson, N. and Griffiths, A. (2005) 'The impact of organizational culture and reshaping capabilities on change implementation success: The mediating role of readiness for change', Journal of Management Studies, 42, pp. 361 - 386.
Joseph-Williams, N., Lloyd, A., Edwards, A., Stobbart, L., Tomson, D., Macphail, S., Dodd, C., Brain, K., Elwyn, G. and Thomson, R. (2017) ‘Implementing shared decision making in the NHS: lessons from the MAGIC programme’, Bmj, 357, p.j1744.
Joubish, M. F., Khurram, M. A., Ahmed, A., Fatima, S. T. and Haider, K. (2011) 'Paradigms and characteristics of a good qualitative research', World Applied Sciences Journal, 12(11), pp. 2082-2087.
Jung, D. I., Chow, C. and Wu, A. (2003) 'The role of transformational leadership in enhancing organizational innovation: Hypotheses and some preliminary findings', The Leadership Quarterly, 14(4), pp. 525-544.
Jyoti, J. and Dev, M. (2015) 'The impact of transformational leadership on employee creativity: the role of learning orientation', Journal of Asia Business Studies, 9(1), pp. 78-98.
Kanter, R. (1985) ‘Supporting innovation and venture development in established companies’ Journal of Business Venturing, 1, pp.47-60.
Kanter, R. M. (1988) When a thousand flowers bloom: structural, collective and social conditions for innovation in organisation. In: Staw BM, Cummings LL,eds. Research in Organisational Behaviour. Greenwich, Conn: JAI Press, p. 169-211.
Kanter, R. M. (2013) Nine Rules for Stifling Innovation. Available at: https://hbr.org/2013/01/nine-rules-for-stifling-innova.html (Accessed: 23rd January 2019)
Kellogg, K. C. (2009) 'Operating room: relational spaces and microinstitutional change in surgery', AJS Sociol, 115 (3), pp.657-711.
Kellermann, A.L. and Jones, S.S. (2013) ‘What it will take to achieve the as-yet-fulfilled promises of health information technology’, Health affairs, 32(1), pp.63-68.
303

Keohane, N. (2018) The NHS, innovation and productivity. Available at: http://www.smf.co.uk/wp-content/uploads/2018/06/NHS-Innovation-and-Productivity-report-web.pdf (Accessed: 23rd January 2019)
Khan, S., Timmings, C., Moore, J., Marquez, C., Pyka, K., Gheihman, G. and Straus, S. (2014) 'The development of an online decision support tool for organizational readiness for change', Implementation Science, 9(1), pp. 56.
Kilmann, R. (1984) 'Beyond the Quick Fix', Management Review, 73(11), p.24.
King, N. (1990) “Innovation at work: The research literature”, in West, M.A. and Farr, J.L. (eds.), Innovation and creativity at work: Psychological and organizational strategies. Oxford, England: John Wiley and Sons, pp. 15-59.
King, N. and Anderson, N. (2002). Managing innovation and change: A critical guide for organizations. Cengage Learning EMEA.
Khazanchi, S., Lewis, M.W. and Boyer, K.K. (2007) ‘Innovation-supportive culture: The impact of organizational values on process innovation,’ Journal of operations management, 25(4), pp.871-884.
Kimberly, J. R. and Evanisko, M. J. (1981) 'Organizational innovation: the influence of individual, organizational, and contextual factors on hospital adoption of technological and administrative innovations', Academy of Management Journal, 24(4), pp. 689-713.
Kingston University London (2016) Kingston University students pitch innovative business ideas in Dragon's Den-style entrepreneurship competition. Available at: https://www.kingston.ac.uk/news/article/1621/01-mar-2016-kingston-university-students-pitch-innovative-business-ideas-in-dragons-denstyle-entrepreneurship-competition/ (Accessed: 24th November 2018).
Klein, K. J. and Sorra, J. S. (1996) 'The challenge of innovation implementation', Academy of Management Review, 21(4), pp.1055-1080.
Klein, K. J. and Knight, A. P. (2005) 'Innovation implementation: Overcoming the challenge', Current Directions in Psychological Science, 14(5), pp. 243-246.
Kline, S.J. (1985) ‘Innovation is not a linear process’, Research Management, 28, pp. 36-45.
Kline, S.J. and Rosenberg, N. (1986) ‘An overview of innovation. the positive sum strategy: harnessing technology for economic growth’, 14, p.640
Kline, S.J. (1990) ‘Models of innovation and their policy consequences’, Paper presented at the NISTEP International Conference on Science and Technology Policy Research - 'What Should be Done? What Can be Done?', Izu, Japan, February.
Kline, S.J. (1991) ‘Styles of innovation and their cultural basis’, Chemtech, 21, pp. 525-535.
304

Kodish, S. and Gittelsohn, J. (2011) 'Systematic data analysis in qualitative health research: Building credible and clear findings', Sight and Life, 25(2), pp. 52-56.
Kogut B and Zander U. (1992) ‘Knowledge of the firm, combinative capabilities, and the replication of technology,’ Organisation Science, 3, pp. 383-397.
Konu, A. and Viitanen, E. (2008) 'Shared leadership in Finnish social and health care', Leadership in Health Services, 21(1), pp. 28-40.
Kotter, J. P. (1996) Leading change, Boston, Mass, Harvard Business School Press.
Kotler, P (2000) Marketing Management, Upper Saddle River, NJ: Prentice Hall
Kotsemir, M.N., Abroskin, A. and Meissner, D. (2013). Innovation concepts and typology – an evolutionary discussion, Basic Research Program. Working Paper
Kramer, M. and Schmalenberg, C. E. (2003) 'Magnet hospital staff nurses describe clinical autonomy', Nursing Outlook, 51(1), pp. 13-19.
Krefting, L. (1991) 'Rigor in qualitative research: The assessment of trustworthiness', American journal of occupational therapy, 45(3), pp. 214-222.
Kvale, S. and Brinkmann, S. (2009) Interviews: learning the craft of qualitative research interviewing. 2nd ed. London: SAGE.
Kyratsis, Y., Ahmad, R. and Holmes, A. (2012) ‘Making sense of evidence in management decisions: the role of research-based knowledge on innovation adoption and implementation in healthcare. study protocol’, Implementation Science, 7(1), p.22.
Lacovou, C. L., Benbasat, I. and Dexter, A. S. (1995) 'Electronic data interchange and small organizations: Adoption and impact of technology', MIS Quarterly, pp. 465-485.
Lane, P. J., Koka, B. and Pathak, S. (2002) 'A thematic analysis and critical assessment of absorptive capacity research', Academy of Management Proceedings, 2002(1), pp. M1-M6.
Lau, C. M. and Ngo, H. Y. (2004) The HR system, organisational culture, and product innovation. International business review, 13, pp.685-703.
Lave, J. and Wenger, E. (1991) Situated learning: Legitimate peripheral participation (Vol. 521423740). Cambridge: Cambridge university press.
Lee, T. W., Mitchell, T. R. and Sablynski, C. J. (1999) 'Qualitative Research in Organizational and Vocational Psychology, 1979–1999', Journal of Vocational Behavior, 55(2), pp. 161-187.
Lee, C., Hallak, R. and Sardeshmukh, S.R. (2016) ‘ Innovation, entrepreneurship, and restaurant performance: A higher-order structural model,’ Tourism Management, 53, pp.215-228.
305

Le May, A. (2009) Communities of practice in health and social care, Oxford; Malden, MA: Wiley-Blackwell Pub.
Lehman, W. E. K., Greener, J. M. and Simpson, D. D. (2002) 'Assessing organizational readiness for change', Journal of substance abuse treatment, 22(4), pp. 197-209.
Lencioni, P. (2012) The advantage: why organizational health trumps everything else in business. 1st edn. San Francisco: Jossey-Bass.
Lewin, K. (1939) “When facing danger”, in Lewin, G.W. (eds.) Resolving Social Conflict. London: Harper & Ro
Lewin, K. (1947) 'Frontiers in group dynamics: concept, method and reality in social science; social equilibria and social change', Human Relations, 1(1), pp. 5-41.
Lewin, K. (1951) Field theory in social science: selected theoretical papers (Edited by Dorwin Cartwright) Oxford, England: Harpers
Lichtenstein, B., Uhl-Bien, M., Marion, R., Seers, A., Orton, J. D. and Schreiber, C. (2006) ‘Complexity leadership theory: An interactive perspective on leading in complex adaptive system’, Management Department Faculty Publications.8.
Lichtenstein, B. B. and Plowman, D. A. (2009) 'The leadership of emergence: A complex systems leadership theory of emergence at successive organizational levels', The Leadership Quarterly, 20(4), pp. 617-630.
LIF and Vasco Advisers. (2013), ‘Innovation in European Healthcare - What can Sweden learn? An analysis of the systems for innovation in five European countries ’ LIF / Vasco Advisers. Available at: http://vascoadvisers.com. (Accessed: 13th March 2018)
Lippoldt D. and Stryszowski P. (2009) ‘Innovation in the Software Sector:’ OECD Innovation Strategy. OECD, Paris.
Lipsitz, L. A. (2012) 'Understanding health care as a complex system: the foundation for unintended consequences', Jama, 308(3), pp. 243-244.
Linden, G., Kraemer, K. L., and Dedrick, J. (2009) ‘Who captures value in a global innovation network? the case of Apple's iPod’, Communications of the ACM, 52(3), pp.140-144
Livari, J. (1992) ‘The organizational fit of information systems,’ Information Systems Journal, 2(1), pp.3-29.
Loewe, P. and Dominiquini, J., (2006). ‘Overcoming the barriers to effective innovation’, Strategy & leadership, 34(1), pp.24-31.
Long, J.C., Cunningham, F.C. and Braithwaite, J. (2013) ‘Bridges, brokers and boundary spanners in collaborative networks: a systematic review,’ BMC health services research, 13(1), p.158.
306

Luecke, R. and Katz, R. (2003) Managing creativity and innovation. Harvard Business School Press, Boston.
MacMahon, J., MacCurtain, S. and O’Sullivan, M. (2010) 'Bullying, culture, and climate in health care organizations: A theoretical framework', Culture and Climate in Health Care Organizations, pp. 82-96.
Madan, V. and Sanches, P. (2013) ‘Five tips on how the private sector can drive change in the NHS’, The Guardian. Available at: https://www.theguardian.com/healthcare-network/2013/sep/26/five-tips-private-sector-change-nhs (Accessed: 14th September 2017)
Maddux, J. E. and Lewis, J. (1995) 'Self-efficacy and adjustment', Self-efficacy, adaptation, and adjustment: Springer, pp. 37-68.
Mallett, R., Hagen-Zanker, J., Slater, R. and Duvendack, M. (2012) 'The benefits and challenges of using systematic reviews in international development research', Journal of Development Effectiveness, 4(3), pp. 445-455.
Manso, G. (2017) 'Creating Incentives for Innovation', California Management Review, 60(1), pp. 18-32.
Marion, R. and Uhl-Bien, M. (2001) 'Leadership in complex organizations', The Leadership Quarterly, 12(4), pp. 389-418.
Marion, R. and Uhl-Bien, M. (2002) Complexity v. transformation: The new leadership revisited. In Managing the Complex IV--Conference on Complex Systems and the Management of Organizations.
Marjanovic, S., Sim, M., Dubow, T., Corbett, J., Harte, E., Parks, S., Miani, C., Chataway, J., Ling, T. (2017). ‘Innovation as a driver of quality and productivity in UK healthcare: Creating and connecting receptive places’ Emerging Insights Report. Santa Monica, CA: RAND Corporation. Available at: https://www.rand.org/pubs/research_reports/RR1845.html (Accessed: 10th
September 2017)
Markus, M.L. and Robey, D. (1983) ‘The organizational validity of management information systems’, Human relations, 36(3), pp.203-225.
Markides, C. (2006) ‘Disruptive Innovation: In Need of Better Theory’, Journal of Product Innovation Management, 23(1), pp. 19-25.
Marshall, J.E., Fraser, D.M. and Baker, P.N. (2010) Reflexivity: the experience of undertaking an ethnographic study to explore issues of consent to intrapartum procedures.
Martins, E. and Terblanche, F. (2003) 'Building organisational culture that stimulates creativity and innovation', European Journal of Innovation Management, 6(1), pp. 64-74.
Martin, S.F., Beimborn, D., Parikh, M.A. and Weitzel, T. (2008) 'Organizational readiness for business process outsourcing: a model of determinants and impact on
307

outsourcing success. In Hawaii International Conference on System Sciences, Proceedings of the 41st Annual (pp. 374-374). IEEE.
Massa, L. and Tucci, C.L. (2013) Business model innovation. In: Dodgson M, Gann DM, and Philips N (eds), The Oxford Handbook of Innovation Management, Oxford, UK: Oxford University Press, pp. 420-441
Masri, F., Wood-Harper, T. and Kawalek, P. (2017) ‘Systems Thinking: Analysis of Electronic Patient Records Implementation and Knowledge Transfer Practice in NHS’, International journal of management and applied research, 4(2), pp.105-121.
Mays, N. and Pope, C. (1995) 'Rigour and qualitative research', British Medical Journal, 311(6997), pp. 109-12.
Mays, N. and Pope, C. (2000) 'Qualitative research in health care: assessing quality in qualitative research', British Medical Journal, 320(7226), pp. 50.
Mazhindu, D. and Gregory, S. (2015) ‘Dragons' Den: promoting healthcare research and innovation’, Nursing Management, 22(4), p.28.
Mazzei, M.J., Flynn, C.B. and Haynie, J.J. (2016) ‘Moving beyond initial success: Promoting innovation in small businesses through high-performance work practices,’ Business Horizons, 59(1), pp.51-60.
McDonald, R. (2015) “The Role of Organization Mission and Commitment to Excellence in the Innovation Process” In: Moore M. and Moore R. (eds) New Meanings for Marketing in a New Millennium. Developments in Marketing Science: Proceedings of the Academy of Marketing Science. Springer, Cham pp. 164-165.
McDaniel Jr, R. R., Driebe, D. J. and Lanham, H. J. (2013) 'Health care organizations as complex systems: new perspectives on design and management ', Annual Review of Health Care Management: Revisiting The Evolution of Health Systems Organization: Emerald Group Publishing Limited, pp. 3-26.
Menguc, B., Auh, S. and Yannopoulos, P. (2014) ‘Customer and supplier involvement in design: The moderating role of incremental and radical innovation capability’, Journal of Product Innovation Management, 31(2), pp.313-328.
Merriam, S. B. (1998) ‘Qualitative Research and Case Study Applications in Education. Revised and Expanded from ‘Case Study Research in Education,’ ERIC.
Merriam, S. and Tisdell, E. (2015) Qualitative research: A guide to design and implementation. John Wiley & Sons.
Meyer, A. D. and Goes, J. B. (1988) 'Organizational assimilation of innovations: A multilevel contextual analysis', Academy of Management Journal, 31(4), pp. 897-923.
Meyer, J. P. and Allen, N. J. (1991) 'A three-component conceptualization of organizational commitment', Human Resource Management Review, 1(1), pp. 61-89.
308

Meyer, M., Johnson, J. D. and Ethington, C. (1997) 'Contrasting attributes of preventive health innovations', Journal of Communication, 47(2), pp. 112-131.
Miles, M. B. and Huberman, A. M. (1994) 'Qualitative data analysis: An expanded sourcebook. 1994', Beverly Hills: Sage Publications.
Miles, I. (2004) Innovation in Public Services presentation at PRIME Conference, Manchester
Mitchell, R., Parker, V., Giles, M. and White, N. (2010) ‘Toward realizing the potential of diversity in composition of interprofessional health care teams: An examination of the cognitive and psychosocial dynamics of interprofessional collaboration’, Medical Care Research and Review, 67(1), pp.3-26.
Moore, M. (2005) ‘Break-Through Innovations and Continuous Improvement: Two Different Models of Innovative Processes in The Public Sector’, Public Money and Management, 25, pp. 43–50.
Morgan, G. (2006) Images of organization. Updated ed: Thousand Oaks, Calif. London: SAGE.
Morse, J. M., Barrett, M., Mayan, M., Olson, K. and Spiers, J. (2002) 'Verification strategies for establishing reliability and validity in qualitative research', International Journal of Qualitative Methods, 1(2), pp. 13-22
Mowery D.C. and Rosenberg N. (1979) ‘The influence of market demand upon innovation: a critical review of some recent empirical studies’, Research Policy, 8, pp 102–153.
Mulrow, C. D. (1994) 'Rationale for systematic reviews', BMJ: British Medical Journal, 309 (6954), pp. 597.
Mumford, M. D. and Gustafson, S. B. (1988) 'Creativity syndrome: Integration, application, and innovation', Psychological bulletin, 103(1), pp. 27.
Murray P and Myers A. (1997) ‘The facts about knowledge,’ Information strategy, Sept, pp. 31-33
Nagy, D., Schuessler, J. and Dubinsky, A. (2016) ‘Defining and identifying disruptive innovations’, Industrial Marketing Management, 57, pp.119-126.
Naqshbandi, M.M., Singh, S.K.G. and Ma, P. (2016) ‘The link between organisational citizenship behaviours and open innovation: A case of Malaysian high-tech sector’, IIMB Management Review, 28(4), pp.200-211.
Nembhard, I.M. and Edmondson, A.C. (2006) ‘Making it safe: The effects of leader inclusiveness and professional status on psychological safety and improvement efforts in health care teams,’ Journal of Organizational Behavior: The International Journal of Industrial, Occupational and Organizational Psychology and Behavior, 27(7), pp.941-966
309

Nemeth, C., Wears, R., Woods, D., Hollnagel, E. and Cook, R. (2008) 'Minding the gaps: creating resilience in health care', in: Henrisksen, K., Battles, JB., Keyes, MA., Grady, ML. Advances in Patient Safety: New Directions and Alternative Approaches.Rockville (MD): Agency for Healthcare Research and Quality (US)
Nesse, R. E., Kutcher, G., Wood, D. and Rummans, T. (2010) 'Framing Change for High‐Value Healthcare Systems', Journal for Healthcare Quality, 32(1), pp. 23-28.
NHS Confederation (2015) Taking a Dragons’ Den approach to evaluating healthcare innovations. Available at: https://www.nhsconfed.org/resources/2015/11/dragons-den-approach-evaluating-healthcare-innovations (Accessed: 23rd November 2018)
NHS England (2014) ‘Understanding the new NHS’. Available at: https://www.nhs.uk/NHSEngland/thenhs/about/Documents/simple-nhs-guide.pdf (Accessed: 25th June 2017)
NHS England (2017a) ‘Bed Availability and Occupancy Data – Overnight’. NHS England. Available at: https://www.england.nhs.uk/statistics/statistical-work-areas/bed-availability-and-occupancy/bed-data-overnight/. (Accessed: 24th November 2017).
NHS England (2017b) ‘Developing our academic health science networks.’ NHS England board paper, item 6, 21 July. NHS England. Available at: www.england.nhs.uk/publication/nhs-england-board-meeting-papers-21-july2017/ (Accessed: 8th March 2018).
NHS Education for Scotland (2018) systems thinking and systems leadership. Available at: http://www.central.knowledge.scot.nhs.uk/Leadership/assets/3_lm_systems-thinking-and-systems-leadership.pdf (Accessed: 4th December 2018)
NHS Improvement (2016) ‘National tariff payment system 2017/18 and 2018/19’ NHS Improvement. Available at: https://improvement.nhs.uk/resources/national-tariff-1719/ (Accessed: 6th March 2018)
NHS Office of London Clinical Commissioning Groups (2017) Today’s NHS - our current challenges (online). NHS Office of London Clinical Commissioning Groups. Available at: https://www.myhealth.london.nhs.uk/help/nhs-today (Accessed: September 12th 2017).
Nonaka I. (1994) ‘A dynamic theory of organisational knowledge creation,’ Organisation Science, 5(1), pp. 14-37.
Norman, D.A. and Verganti, R. (2014) ‘Incremental and radical innovation: Design research vs. technology and meaning change’, Design issues, 30(1), pp.78-96.
Northen Devon Healthcare NHS Trust (2015) Recruitment and retention strategy 2015-2018 Available at: https://www.northdevonhealth.nhs.uk/wp-content/uploads/2015/09/Annex-5.5-Board-
310

06.10.15-Recruitment-and-Retention-Strategy-Part-2.pdf (Accessed: 11th December 2018)
O'Connor, K. and Brown, P.B. (2003). The map of innovation: Creating something out of nothing. Crown Business.
Oksanen, K. and Ståhle, P. (2013) ‘Physical environment as a source for innovation: investigating the attributes of innovative space’, Journal of knowledge management, 17(6), pp.815-827.
Oliveira, T.C., Barrenho, E., Vernet, A., Autio, E. and Barlow, J. (2017) Developing a Global Healthcare Innovation Index. Available at: http://piru.lshtm.ac.uk/assets/files/Healthcare%20innovation%20index%20report.pdf (Accessed: 23rd January 2019)
Orlikowski, W. J. and Baroudi, J. J. (1991) 'Studying information technology in organizations: Research approaches and assumptions', Information Systems Research, 2(1), pp. 1-28.
O'Reilly, C. A. and Chatman, J. (1986) 'Organizational commitment and psychological attachment: The effects of compliance, identification, and internalization on prosocial behavior', Journal of Applied Psychology, 71(3), pp. 492.
Oostendorp, L.J., Durand, M.A., Lloyd, A. and Elwyn, G. (2015) ‘Measuring organisational readiness for patient engagement (MORE): an international online Delphi consensus study’, BMC health services research, 15(1), pp.61.
Ostlund, L.E., (1974) ‘Perceived innovation attributes as predictors of innovativeness’, Journal of consumer research, 1(2), pp.23-29.
Paina, L. and Peters, D. H. (2012) 'Understanding pathways for scaling up health services through the lens of complex adaptive systems', Health Policy Plan, 27.
Pettigrew, A. M. (1997) 'What is a processual analysis', Scandinavian Journal of Management, 13(4), pp. 337-348.
Pierce, J.L. and Delbecq, A.L. (1977) ‘Organisation structure, individual attitudes and innovation’, Academy of Management Review, 2, pp 27-37.
Plsek, P (2003). 'Complexity and the Adoption of Innovation in Health Care', Accelerating Quality Improvement in Health Care Strategies to Speed the Diffusion of Evidence-Based Innovations, Washington, D.C: National Institute for Health Care Management Foundation. National Committee for Quality Health Care.
Plsek, P. and Greenhalgh, T. (2001) 'Complexity science: the challenge of complexity in health care', British Medical Journal, 323(7317), pp. 625.
Plsek, P. and Wilson, T. (2001) 'Complexity Science: complexity, leadership, and management in healthcare organisations', British Medical Journal, 323(7315), pp. 746-749.
311

Plsek, P. (2014a) Recognizing the importance of innovation in health service delivery. AHRQ Healthcare Innovations Exchange.
Plsek, P. (2014b) Harnessing Disruptive Innovation in Health Care. AHRQ Healthcare Innovations Exchange
Pope, C. and Mays, N. (1995) 'Reaching the parts other methods cannot reach: an introduction to qualitative methods in health and health services research', British Medical Journal (Clinical research ed), 311, p. 42.
Pope, C., van Royen, P. and Baker, R. (2002) 'Qualitative methods in research on healthcare quality', British Medical Journal Quality & Safety, 11(2), pp. 148-152.
Powell, T. (2017) The structure of the NHS in England. House of Commons Library. Briefing Paper. Number CBP 07206, 7 July 2017. Pp.1-39.
Prochaska, J. M., Prochaska, J. O. and Levesque, D. A. (2001) 'A transtheoretical approach to changing organizations', Administration and Policy in Mental Health, 28(4), pp. 247-61.
Prochaska, J. O. and DiClemente, C. C. (1983) 'Stages and processes of self-change of smoking: toward an integrative model of change', Journal of Consulting Clinical and Psychology, 51(3), pp. 390-5.
Punjaisri, K. and Wilson, A. (2007) ‘The role of internal branding in the delivery of employee brand promise,’ Journal of Brand Management, 15(1), pp.57-70.
Pye, A. (2005) 'Leadership and organizing: Sensemaking in action', Leadership, 1(1), pp. 31-49.
Pym, H., (2018) NHS: How much does it spend on the private sector? BBC NEWS. Available at: https://www.bbc.co.uk/news/health-44043959 (Accessed: 23rd January 2019)
Pype, P., Krystallidou, D., Deveugele, M., Mertens, F., Rubinelli, S. and Devisch, I. (2017). Healthcare teams as complex adaptive systems: Focus on interpersonal interaction. Patient education and counseling, 100(11), pp.2028-2034.
Qu, S. Q. and Dumay, J. (2011) 'The qualitative research interview', Qualitative research in accounting & management, 8(3), pp. 238-264.
Quintas, P. (2002) ‘Implications of the Division of Knowledge for Innovation in Networks’ In Networks, Alliances and Partnerships in the Innovation Process’ pp. 135-162 Springer, Boston, MA.
Rafferty, A.M., Ball, J. and Aiken, L. H. (2001) 'Are teamwork and professional autonomy compatible, and do they result in improved hospital care?', Quality and Safety in Health Care, 10(suppl 2), pp. ii32-ii37.
Rafferty, A. E., Jimmieson, N. L. and Armenakis, A. A. (2012) 'Change Readiness: A Multilevel Review', Journal of Management, 39(1), pp.110-135
312

Rantz, M. J., Hicks, L., Petroski, G. F., Madsen, R. W., Alexander, G., Galambos, C., Conn, V., Scott-Cawiezell, J., Zwygart-Stauffacher, M. and Greenwald, L. (2010) 'Cost, staffing and quality impact of bedside electronic medical record (EMR) in nursing homes', Journal of the American Medical Directors Association, 11(7), pp. 485-493.
Rao, H. and Dutta, S. (2012) ‘Free spaces as organizational weapons of the weak: Religious festivals and regimental mutinies in the 1857 Bengal Native Army,’ Administrative Science Quarterly, 57(4), pp.625-668.
Rees, G. H. (2014) 'Organisational readiness and Lean Thinking implementation: Findings from three emergency department case studies in New Zealand', Health Services Management Research, 27(1-2), pp.1-9
Regine, B. and Lewin, R. (2000) 'Leading at the edge: How leaders influence complex systems', Emergence, 2(2), pp. 5-23.
Reinhardt, R., Bullinger, A.C. and Gurtner, S. (2015) Open innovation in health care. In Challenges and opportunities in health care management (pp. 237-246). Springer, Cham.
Reeves, R., West, E. and Barron, D. (2013) ‘Facilitated patient experience feedback can improve nursing care: a pilot study for a phase III cluster randomised controlled trial,’ BMC health services research, 13(1), p.259.
Rice, P. L. and Ezzy, D. (1999) 'Qualitative research methods: A health focus', Melbourne: Oxford University Press.
Richards, H. M. and Schwartz, L. J. (2002) 'Ethics of qualitative research: are there special issues for health services research’, Family Practice, 19(2), pp. 135-139.
Ritchie, J. and Lewis, J. (2003) Qualitative research practice: A guide for social science students and researchers. Thousand Oaks, CA: Sage Publications.
Richter, A. W., Hirst, G., van Knippenberg, D., & Baer, M. (2012) ‘Creative self-efficacy and individual creativity in team contexts: Cross-level interactions with team informational resources’, Journal of Applied Psychology, 97(6), pp. 1282-1290.
Robert, G., Greenhalgh, T., MacFarlane, F. and Peacock, R. (2009) 'Organisational factors influencing technology adoption and assimilation in the NHS: a systematic literature review', Report for the National Institute for Health Research Service Delivery and Organisation programme.
Roberts A., Marshall L. and Charlesworth A. (2012) A decade of austerity? the funding pressures facing the NHS in England 2011/12 to 2021/22. Nuffield Trust. Available at: https://www.nuffieldtrust.org.uk/files/2017-01/decade-of-austerity-full-web-final.pdf (Accessed: 13th September 2016)
Robinson, C. and Goudy, K. (2009) 'Leadership in these challenging times', Frontiers of health services management, 26(2), pp. 21.
313

Rogers, E. (2003) Diffusion of innovations. New York: Simon & Schuster Inc.
Rothwell, R. and Dodgson, M. (1991). ‘External linkages and innovation in small and medium‐sized enterprises. R and D Management, 21(2), 125-138.
Rothwell, R. (1994). ‘Towards the fifth-generation innovation process’, International Marketing Review, 11 (1), pp 7-31.
Rowlands, G., Sims, J., & Kerry, S. (2005) ‘A lesson learnt: the importance of modelling in randomized controlled trials for complex interventions in primary care’ Family Practice, 22(1), pp 132-139.
Rowley, J. (2012a) 'Conducting research interviews', Management Research Review, 35(3/4), pp. 260-271.
Rowley, E. (2012b) ‘Protocol for a qualitative study exploring the roles of ‘Diffusion Fellows’ in bridging the research to practice gap in the Nottinghamshire, Derbyshire and Lincolnshire Collaboration for Leadership in Applied Health Research and Care (CLAHRC-NDL)’, BMJ open, 2(1), p.e000604
Rowley, E., Morriss, R., Currie, G. and Schneider, J. (2012) ‘Research into practice: collaboration for leadership in applied health research and care (CLAHRC) for Nottinghamshire, Derbyshire, Lincolnshire (NDL),’ Implementation Science, 7(1), p.40.
Rubin, H. J. and Rubin, I. S. (2011) Qualitative interviewing: The art of hearing data. Sage.
Rubin, H. R., Pronovost, P. and Diette, G. B. (2001) 'The advantages and disadvantages of process‐based measures of health care quality', International Journal for Quality in Health Care, 13(6), pp. 469-474.
Rusly, F. H., Sun, P. YT. and Corner, J. L. (2015) 'Change readiness: creating understanding and capability for the knowledge acquisition process', Journal of Knowledge Management, 19(6), pp. 1204-1223.
Ryan, G. W. and Bernard, H. R. (2000) 'Data management and analysis methods', in Denzin, N. and Lincoln, Y. (eds) Handbook of Qualitative Research. pp. 769-802 [Online]. Version. Available at: http://qualquant.org/wp-content/uploads/text/2000 Ryan_Bernard.denzin.pdf (Accessed: 22nd July 2014).
Saleh, S. D. and Wang, C. K. (1993) 'The management of innovation: strategy, structure, and organizational climate', IEEE transactions on engineering management, 40(1), pp. 14-21.
Saleh, S., Khodor, R., Alameddine, M. and Baroud, M., 2016. Readiness of healthcare providers for eHealth: the case from primary healthcare centers in Lebanon. BMC health services research, 16(1), p.644.
Sandelowski, M. (1986) 'The problem of rigor in qualitative research', Advances in Nursing Science, 8(3), pp. 27-37.
314

Sanson-Fisher, R.W. (2004) ‘Diffusion of innovation theory for clinical change’, Medical journal of Australia, 180(6 Suppl), p. S55.
Saunders, M., Lewis, P. and Thornhill, A. (2012) Research methods for business students. Harlow: Pearson.
Schein, E. H. (1999) 'Kurt Lewin’s change theory in the field and in the classroom: Notes toward a model of managed learning', Reflections, 1(1), pp. 59-74.
Schein, E. H. (2010) Organizational culture and leadership. John Wiley & Sons.
Schmookler, J. (1966) Invention and Economic Growth. Harvard University Press.
Schneider, B., Brief, A. P. and Guzzo, R. A. (1996) 'Creating a climate and culture for sustainable organizational change', Organizational Dynamics, 24(4), pp. 7-19.
Schon, D. A. (1963) 'Champions for radical new inventions', Harvard Business Review, 41(2), pp. 77-86.
Schroeder, R.G., Van De Ven, A.H., Scudder, G.D., Polley, D. (1989), ‘The development of innovation ideas’. Research on the management of innovation: The Minnesota Studies, pp 107-134.
Schumpeter, J.A. (1934) The Theory of Economic Development: An Inquiry into Profits, Capital, Credit, Interest and the Business Cycle. Cambridge, MA: Harvard Economic Studies.
Schumpeter, J.A. (1939). Business Cycles: A Theoretical, Historical, and Statistical Analysis of The Capitalist Process. McGraw-Hill.
Schumpeter, J.A. (1942). Creative Destruction. Capitalism, Socialism and Democracy, 825.
Scott-Morton, M. (1991) The Corporation of the 1990s, Information Technology and Organizational Transformation, 1991. Oxford University Press: New York, NY.
Scott, K. W. (2004) 'Relating the categories in grounded theory analysis: using a conditional relationship guide and reflective coding matrix', The Qualitative Report, 9(1), pp. 112-126.
Scott, H (2011) Crossing the line: how shifting organisational boundaries are impacting roles in the NHS Available at: https://www.hsj.co.uk/efficiency/crossing-the-line-how-shifting-organisational-boundaries-are-impacting-roles-in-the-nhs/5030896.article (Accessed: 9th December 2018)
Schweizer, T.S. (2006) ‘The psychology of novelty‐seeking, creativity and innovation: neurocognitive aspects within a work‐psychological perspective,’ Creativity and Innovation Management, 15(2), pp.164-172.
Schippers, M.C., West, M.A. and Dawson, J.F. (2015) ‘Team reflexivity and innovation: The moderating role of team context’, Journal of Management, 41(3), pp.769-788.
315

Schulz, K.P., Kajamaa, A. and Kerosuo, H. (2015) ‘Creating innovative work practices through reflexive interventions’, International Journal of Work Innovation, 1(2), pp.143-160
Schmutz, J.B. and Eppich, W.J. (2017) ‘Promoting learning and patient care through shared reflection: a conceptual framework for team reflexivity in health care’, Academic Medicine, 92(11), pp.1555-1563.
Self, D. R. and Schraeder, M. (2008) 'Enhancing the success of organizational change: Matching readiness strategies with sources of resistance', Leadership & Organizational Development Journal, 30(2), pp. 167-182.
Sengupta, K. and Abdel-Hamid, T.K. (1993). ‘Alternative conceptions of feedback in dynamic decision environments: an experimental investigation’, Management Science, 39(4), pp 411-428.
Senge, P.M. (2006) The fifth discipline: the art and practice of the learning organization Rev. and updated, London: Random House Business.
Seo, M. G., Bartunek, J. M. and Barrett, L. F. (2010) 'The role of affective experience in work motivation: Test of a conceptual model', Journal of Organizational Behavior, 31(7), pp. 951-968.
Shaikh, A.A. and Karjaluoto, H. (2015) ‘Mobile banking adoption: A literature review’, Telematics and Informatics, 32(1), pp.129-142
Shea, C. M., Jacobs, S. R., Esserman, D. A., Bruce, K. and Weiner, B. J. (2014) 'Organizational readiness for implementing change: a psychometric assessment of a new measure', Implementation Science: IS, 9, pp. 7-7
Sheard, L., Jackson, C. and Lawton, R. (2017) ‘How is success achieved by individuals innovating for patient safety and quality in the NHS?’, BMC health services research, 17(1), p.640.
Shenton, A. K. (2004) 'Strategies for ensuring trustworthiness in qualitative research projects', Education for information, 22(2), pp. 63-75.
Shipton, H., Sanders, K., Atkinson, C. and Frenkel, S. (2016) ‘Sense‐giving in health care: the relationship between the HR roles of line managers and employee commitment,’ Human Resource Management Journal, 26(1), pp.29-45.
Shortell, S. M. (1999) 'The emergence of qualitative methods in health services research', Health Service Research Journal, 34(5 Pt 2), pp. 1083-90.
Shortell, S. M., Bennett, C. L. and Byck, G. R. (1998) 'Assessing the Impact of Continuous Quality Improvement on Clinical Practice: What It Will Take to Accelerate Progress', Milbank Quarterly, 76(4), pp. 593-624.
Sitkin, S. B. and Pablo, A. L. (1992) 'Reconceptualizing the determinants of risk behavior', Academy of Management Review, 17(1), pp. 9-38.
316

Simpson, D.D. and Dansereau, D.F. (2007) ‘Assessing organizational functioning as a step toward innovation’, Science & Practice Perspectives, 3(2), p.20.
Simmie, J. (2014) ‘Regional economic resilience: a Schumpeterian perspective’, Raumforschung und Raumordnung, 72(2), pp.103-116.
Sizmur, S., Raleighn, V., Picker and The King’s Fund (2018) The risks to care quality and staff wellbeing of an NHS system under pressure. Available at: https://www.picker.org/wp-content/uploads/2014/12/Risks-to-care-quality-and-staff-wellbeing-VR-SS-v8-Final.pdf (Accessed: 10th December 2018)
Snyder-Halpern, R. (1998) 'Measuring organizational readiness for nursing research programs', Western Journal of Nursing Research, 20(2), pp. 223-237.
Snyder-Halpern, R. (2001) 'Indicators of organizational readiness for clinical information technology/systems innovation: a Delphi study', International Journal of Medical Informatics, 63(3), pp. 179-204.
Snyder-Halpern, R. (2002) 'Development and pilot testing of an Organizational Information Technology/Systems Innovation Readiness Scale (OITIRS)', Proceedings / AMIA ... Annual Symposium. AMIA Symposium, pp. 702-706.
Snyder, R. A. and Fields, W. L. (2006) 'Measuring hospital readiness for information technology (IT) innovation: A multisite study of the Organizational Information Technology Innovation Readiness Scale', J Nurse Meas, 14(1), pp. 45-55.
Sofaer, S. (1999) 'Qualitative methods: what are they and why use them?', Health Service Research, 34(5 Pt 2), pp. 1101-18.
Sol, J., Beers, P. J. and Wals, A. E. (2013) 'Social learning in regional innovation networks: trust, commitment and reframing as emergent properties of interaction', Journal of Cleaner Production, 49, pp. 35-43.
Southon, F. C. G., Sauer, C. and Dampney, C. N. G. K. (1997) 'Information technology in complex health services', Journal of the American Medical Informatics Association, 4(2), pp. 112-124.
Stacey, R.D., Griffin, D., and Shaw, P. (2000). Complexity and management: Fad or radical challenge in systems thinking? New York: Routledge.
Stacey, R. D. (2011) Strategic management and organisational dynamics: the challenge of complexity to ways of thinking about organisations. 6th edn. Harlow: Financial Times Prentice Hall.
Sterman, J. D. (2000) Business dynamics: systems thinking and modeling for a complex world. London: Irwin/McGraw-Hill.
Stevens, G. (2013) 'Toward a process-based approach of conceptualizing change readiness', Journal of Applied Behavioural Science, 49(3), pp. 333 - 360.
Steventon, A., Bardsley, M., Billings, J., Dixon, J., Doll, H., Hirani, S., Cartwright, M., Rixon, L., Knapp, M., Henderson, C. and Rogers, A. (2012) ‘Effect of telehealth on
317

use of secondary care and mortality: findings from the Whole System Demonstrator cluster randomised trial,’ British Medical Journal, 344, p.e3874.
Storey, J. and Holti, R. (2013) Towards a New Model of Leadership for the NHS. Available at: https://www.leadershipacademy.nhs.uk/wpcontent/uploads/2013/05/Towards-a-New-Model-of-Leadership-2013.pdf (Accessed: 12th February 2018)
Strang, D., and Soule, S. A. (1998) ‘Diffusion in organizations and social movements: From hybrid corn to poison pills’ Annual review of sociology, 24(1), pp 265-290.
Strauss, A. and Corbin, J. (1990) Basics of qualitative research: grounded theory procedures and techniques. London: Sage Publications, Inc.
Streatfield, P.J. (2001). The paradox of control in organizations. New York: Routledge.
Styhre, A. (2002) 'Non-linear change in organizations: organization change management informed by complexity theory', Leadership & Organization Development Journal, 23(6), pp. 343-351.
Tabak, F. and Barr, S. H. (1996) 'Adoption of organizational innovations: Individual and organizational determinants', Academy of Management Proceedings: Academy of Management, pp. 388-392.
Tan, B. S. (2004) ‘The consequences of innovation’, The Innovation Journal: The Public Sector Innovation Journal, 9(3), pp 1-42.
Tani, M., Papaluca, O. and Sasso, P. (2018) ‘The system thinking perspective in the open-innovation research: A systematic review,’ Journal of Open Innovation: Technology, Market, and Complexity, 4(3), p.38.
Tappen, R.M., Wolf, D.G., Rahemi, Z., Engstrom, G., Rojido, C., Shutes, J.M. and Ouslander, J.G. (2017) ‘Barriers and Facilitators to Implementing a Change Initiative in Long-Term Care Using the INTERACT® Quality Improvement Program’, The health care manager, 36(3), pp.219-230.
Teece, D. J., Pisano, G. and Shuen, A. (1997) ‘Dynamic capabilities and strategic management’, Strategic Management Journal, 18, pp. 509–33.
The Health Foundation (2010) Evidence scan: Complex adaptive systems: The Health Foundation. Available at: https://www.health.org.uk/sites/health/files/ComplexAdaptiveSystems.pdf (Accessed: 28th April 2018).
The AHSN Network (2017). About Academic Health Science Networks. Available at: http://www.ahsnnetwork.com/about-academic-health-science-networks/ (Accessed: 27th April 2017).
318

The King's Fund (2016) How is the NHS structured? Available at: https://www.kingsfund.org.uk/audio-video/how-new-nhs-structured-&gid=1&pid=1 (Accessed: 28th April 2018)
The King’s Fund (2017a) What’s going on with A&E waiting times? The King’s Fund. Available at: https://www.kingsfund.org.uk/projects/urgent-emergency-care/urgent-and-emergency-care-mythbusters#the-ae-standard-and-performance (Accessed: 12th September 2017)
The King’s Fund. (2017b) How is the NHS performing? November 2017: Quarterly Monitoring Report. The King’s Fund. Available at: http://qmr.kingsfund.org.uk/2017/24/ (Accessed: 18th January 2018)
The King’s Fund. (2018) Adoption and spread of innovation in the NHS. The King’s Fund. Available at: https://www.kingsfund.org.uk/publications/innovation-nhs (Accessed12th March 2018)
Tidd, J. and Bessant, J. R., (2013) Managing innovation: integrating technological, market and organizational change. 5th edn. Chichester: Wiley.
Timmins, N. (2013) Changing of the Guard: lessons for the new NHS from departing health leaders. London: The Nuffield Trust.
Tjosvold, D., Tang, M. M. and West, M. (2004) 'Reflexivity for Team Innovation in China: The Contribution of Goal Interdependence', Group & Organization Management, 29(5), pp. 540-559.
Todnem By, R. (2005) 'Organisational change management: A critical review', Journal of Change Management, 5(4), pp. 369-380.
Touré, M., Poissant, L., and Swaine, B. R. (2012) ‘Assessment of organisational readiness for e-health in a rehabilitation centre’, Disability and rehabilitation, 34(2), pp.167-173.
Tranfield, D., Denyer, D. and Smart, P. (2003) 'Towards a methodology for developing evidence‐informed management knowledge by means of systematic review', British journal of management, 14(3), pp. 207-222.
Triggle, N. (2005) ‘How the NHS could learn from Sweden’ BBC. Available at:
http://news.bbc.co.uk/2/hi/health/4460098.stm (Accessed: 4th March 2018)
Triggle, N. (2018) Patients 'dying in hospital corridors: BBC News. Available at: http://www.bbc.co.uk/news/health-42572116 (Accessed: 23rd April 2018).
Tushman, M.L. and Anderson, P (1986) Technological Discontinuities and Organisational Environments. Administrative Science Quarterly, 439-465.
Tushman, M. L. and O Reilly, C. A., III (1996) 'Ambidextrous organizations: Managing evolutionary and revolutionary change', California Management Review, 38(4), pp. 8.
319
Uhl-Bien, M., Marion, R. and McKelvey, B. (2007) 'Complexity leadership theory: Shifting leadership from the industrial age to the knowledge era', The Leadership Quarterly, 18(4), pp. 298-318.
University of Southampton (2018) Student entrepreneurs secure £200, 000 at Dragons’ Den style pitching showcase. Available at: https://www.southampton.ac.uk/news/2018/05/future-worlds-den.page (Accessed: 24th November 2018)
University of Surrey (2018) The University of Surrey’s plans for a medical school. Available at: https://jobs.surrey.ac.uk/Upload/vacancies/files/4662/Plans%20for%20a%20medical%20school.pdf (Accessed: 16th December 2018)
Utterback, J. M. (1971) ‘The process of technological innovation within the firm’ Academy of management Journal,’ 14(1), pp.75-88.
Utterback, J. M., and Abernathy, W. J. (1975) ‘A dynamic model of process and product innovation’, Omega, 3(6), pp. 639-656.
Vakola, M. (2014) 'What's in there for me? Individual readiness to change and the perceived impact of organizational change', Leadership & Organization Development Journal, 35(3), pp. 195-209.
Vance, C., Zell, D. and Groves, K. (2008) 'Considering individual linear/nonlinear thinking style and innovative corporate culture', International Journal of Organizational Analysis, 16(4), pp. 232-248
Van de Ven, A. H. (1986) 'Central problems in the management of innovation', Management Science, 32(5), pp. 590-607.
Van de Ven, A. H., Polley, D. E., Garud, R. and Venkataraman, S. (2008) The Innovation Journey. New York: Oxford University Press.
Van de Ven, A. H. (2017) 'The innovation journey: you can't control it, but you can learn to maneuver it', Innovation: Organisation & Management, 19(1), pp. 39-42.
Van Bogaert, P., Peremans, L., Van Heusden, D., Verspuy, M., Kureckova, V., Van de Cruys, Z. and Franck, E. (2017) ‘Predictors of burnout, work engagement and nurse reported job outcomes and quality of care: a mixed method study,’ BMC nursing, 16(1), p.5.
Varkey, P., Horne, A. and Bennet, K.E. (2008) ‘Innovation in Health Care: A Primer’, American Journal of Medical Quality, 23(5), pp.382-388.
Varey, R.J. and Lewis, B.R. (1999) ‘A broadened conception of internal marketing’, European Journal of Marketing, 33(9/10), pp.926-944.
Verzulli, R., Jacobs, R. and Goddard, M. (2011) Do Hospitals Respond to Greater Autonomy?: Evidence from the English NHS. Available at: http://eprints.whiterose.ac.uk/137337/ (Accessed: 23rd January 2019)
320
Vincent, L. (2013) ‘Managing Innovation or Culture Change? Innovating Perspectives, 21(5), pp. 1-2
Vitale, T. R. (2018) 'Nurse leader mentorship', Nursing management, 49(2), pp. 8-10.
Walinga, J. (2008) 'Toward a Theory of Change Readiness: The Roles of Appraisal, Focus, and Perceived Control', The Journal of Applied Behavioral Science, 44(3), pp. 315-347.
Wang, G., Holmes Jr, R.M., Oh, I.S. and Zhu, W. (2016) ‘Do CEOs matter to firm strategic actions and firm performance? A meta‐analytic investigation based on upper echelons theory,’ Personnel Psychology, 69(4), pp.775-862.
Weberg, D. (2009) 'Innovation in Healthcare: A Concept Analysis', Nursing Administration Quarterly, 33(3), pp. 227-237.
Weberg, D. (2012) 'Complexity leadership: a healthcare imperative', Nursing Forum, 47(4), pp. 268-277.
Weeks, W. A., Roberts, J., Chonko, L. B. and Jones, E. (2004) 'Organizational readiness for change, individual fear of change, and sales manager performance: an empirical investigation', Journal of Personal Selling and Sales Management, 24(1), pp. 7-17.
Weiner, B., Amick, H. and Lee, S. (2008). 'Conceptualization and measurement of organizational readiness for change: a review of the literature in health services research and other fields', Medical Care Research and Review, 65, pp. 379 - 436.
Weiner, B. J., Lewis, M. A. and Linnan, L. A. (2009) 'Using organization theory to understand the determinants of effective implementation of worksite health promotion programs', Health Education Research, 24(2), pp. 292-305.
Weiner, B. J. (2009) 'A theory of organizational readiness for change', Implementation Science: IS, 4(1), pp. 67.
Wenger, E. (1999) Communities of practice: Learning, meaning, and identity. Cambridge university press.
Wenger, E., McDermott, R. A. and Snyder, W. (2002). Cultivating communities of practice: A guide to managing knowledge. Harvard Business Press.
West, M. A. and Farr, J. L. (1990) Innovation and creativity at work: psychological and organizational strategies. Chichester: John Wiley.
West, M. A. (1996) “Reflexivity and Work Group Effectiveness: A Conceptual Integration”, in West, M.A. (eds.) Handbook of West Group Psychology. Wiley, London, pp. 555-79.
West, E., Barron, D.N., Dowsett, J., Newton, J.N. (1999) ‘Hierarchies and cliques in the social networks of health care professionals: implications for the design of dissemination strategies’, Social science & medicine, 48(5), pp 633-646.
321

West, M. A. (2002) 'Sparkling fountains or stagnant ponds: An integrative model of creativity and innovation implementation in work groups', Applied Psychology, 51(3), pp. 355-387.
West, M. and Dawson, J. (2012) Employee engagement and NHS performance. London: King's Fund.
West, M.A., Eckert, R., Steward, K. and Pasmore, W.A. (2014) Developing collective leadership for health care. London: King's Fund.
Wesseling, J.H., Niesten, E.M.M.I., Faber, J. and Hekkert, M.P. (2015), ‘Business strategies of incumbents in the market for electric vehicles: Opportunities and incentives for sustainable innovation’. Business Strategy and the Environment, 24(6), pp.518-531
Wheelwright, S.C. and Clark, K.B. (1992) Revolutionizing product development: quantum leaps in speed, efficiency, and quality. Simon and Schuster.
World Health Organisation (2000) The world health report 2000: health systems: improving performance. World Health Organization. Available at: https://www.who.int/whr/2000/en/whr00_en.pdf?ua=1 (Accessed: 9th February 2019)
World Health Organisation (2014) Health services. Available at: http://www.who.int/topics/health_services/en/ (Accessed: 12th November 2018).
Wilson, T., Holt, T. and Greenhalgh, T. (2001) ‘Complexity and clinical care’, Bmj, 323(7314), pp.685-688.
Williams, D., Wells, O., Hourd, P., Chandra, A. (2008) ‘Feeling the pain: disruptive innovation in healthcare markets’, Innovation in manufacturing networks, pp. 25-34.
Williams P, Sullivan H (2009) ‘Faces of integration,’ International Journal of Integrated Care, 9(100).
Williams, I. (2011) 'Organizational readiness for innovation in health care: some lessons from the recent literature', Health Services Management Research: An Official Journal Of The Association Of University Programs In Health Administration, 24(4), pp. 213-218.
Williamson P.J. and De Meyer. (2012) ‘A ecosystem advantage: how to successfully harness the power of partners’, California management review 55, pp 24-46.
Williams, P. (2013) ‘We are all boundary spanners now?,’ International Journal of Public Sector Management, 26(1), pp.17-32.
Wisdom, J. P., Chor, K. H. B., Hoagwood, K. E. and Horwitz, S. M. (2014) 'Innovation adoption: a review of theories and constructs', Administration and Policy in Mental Health and Mental Health Services Research, 41(4), pp. 480-502.
Wolfe, R.A. (1994) ‘Organisational innovation: review, critique and suggested research directions’. Journal of Management Studies 31(3), pp. 405-431.
322

Woodman, R.W., Sawyer, J.E. and Griffin, R.W. (1993) ‘Toward a theory of organizational creativity,’ Academy of management review, 18(2), pp.293-321.
Woolliams, M., Williams, K., Butcher, D. and Pye, J. (2009) Be more critical!. A practical guide for health and social care students.
Wong, C.A., Cummings, G.G. and Ducharme, L. (2013) ‘The relationship between nursing leadership and patient outcomes: a systematic review update,’ Journal of nursing management, 21(5), pp.709-724.
Wynen, J., Verhoest, K., Ongaro, E., Van Thiel, S. and in cooperation with the COBRA network (2014) ‘Innovation-oriented culture in the public sector: Do managerial autonomy and result control lead to innovation?,’ Public Management Review, 16(1), pp.45-66.
Young, R. A. and Collin, A. (2004) 'Introduction: Constructivism and social constructionism in the career field', Journal of Vocational Behavior, 64(3), pp. 373-388.
Transport for London (2018) Youth Travel Ambassadors Programme 2017/2018. Available: http://content.tfl.gov.uk/yta-brochure-2017-18.pdf (Accessed 24th January 2019).
Zahra, S. A. and George, G. (2002) 'Absorptive Capacity: A Review, Reconceptualization, and Extension', Academy of Management Review, 27(2), pp. 185-203.
Zaltman, G., Duncan, R. and Holbek, J. (1973) Innovations and organizations. New York: London (etc): Wiley-Interscience.
Zhang, X. and Bartol, K.M. (2010) ‘Linking empowering leadership and employee creativity: The influence of psychological empowerment, intrinsic motivation, and creative process engagement’, Academy of management journal, 53(1), pp.107-128.
Zhang, S., Ke, X., Frank Wang, X.H. and Liu, J. (2018) ‘Empowering leadership and employee creativity: A dual‐mechanism perspective,’ Journal of Occupational and Organizational Psychology.
Ziman, J. (1991) ‘A neural net model of innovation’, Science and Public Policy, 18, pp. 65-75.
323