daubert autonomic homeostasis revised - acmt - …€¦ · ganglion ach ne cns ach ach ach...
TRANSCRIPT

1
Autonomics/ Neurotransmitters
G. Patrick Daubert, MD Sacramento, CA
Some (most) material plundered from various mentors and other talented toxicologists, with permission

2
Sympathetic ganglion
NE ACh
CNS ACh
ACh
ACh
Secreting hollow end-organs: Heart Lungs GI
Sympathetic innervation to heart, lungs, etc
ACh
Striated muscle
ACh
Muscarinic Nicotinic Courtesy Cynthia Aaron, MD
3
Acetylcholine
4
ACh Receptors
n Nicotinic Receptors n CNS (mainly spinal cord) n Preganglionic autonomic neurons (sympathetic and
parasympathetic) n Adrenal neuronal receptors n Skeletal muscle neuromuscular junction

5
ACh Receptors
n Muscarinic Receptors n CNS (mainly brain) n Postganglionic parasympathetic nerve endings n Postganglionic sympathetic receptors for most sweat
glands
6
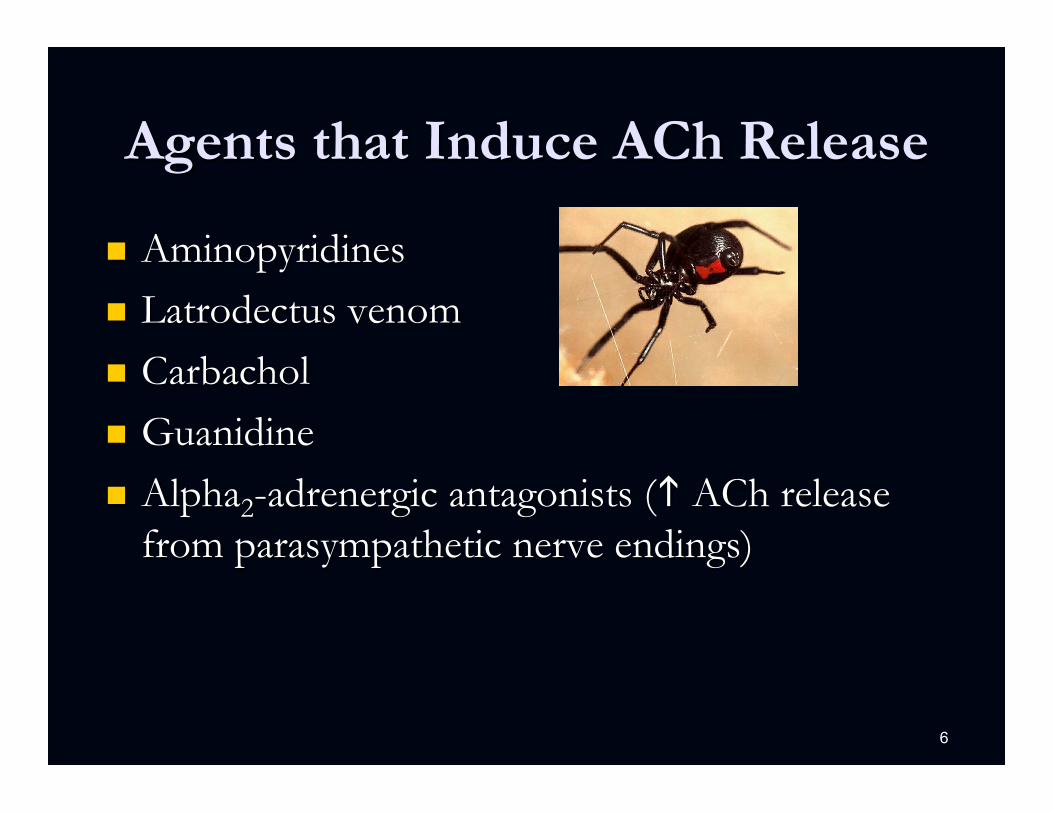
Agents that Induce ACh Release
n Aminopyridines n Latrodectus venom n Carbachol n Guanidine n Alpha2-adrenergic antagonists ( ACh release
from parasympathetic nerve endings)

7
Acetylcholinesterase Inhibitors
n [ACh] at both nicotinic and muscarinic receptors
n Produce a variety of CNS, sympathetic, parasympathetic, and NMJ effects n Carbamates n Organophosphorus compounds n Nerve agents n ‘Central’ AChE inhibitors (donepezil)
8
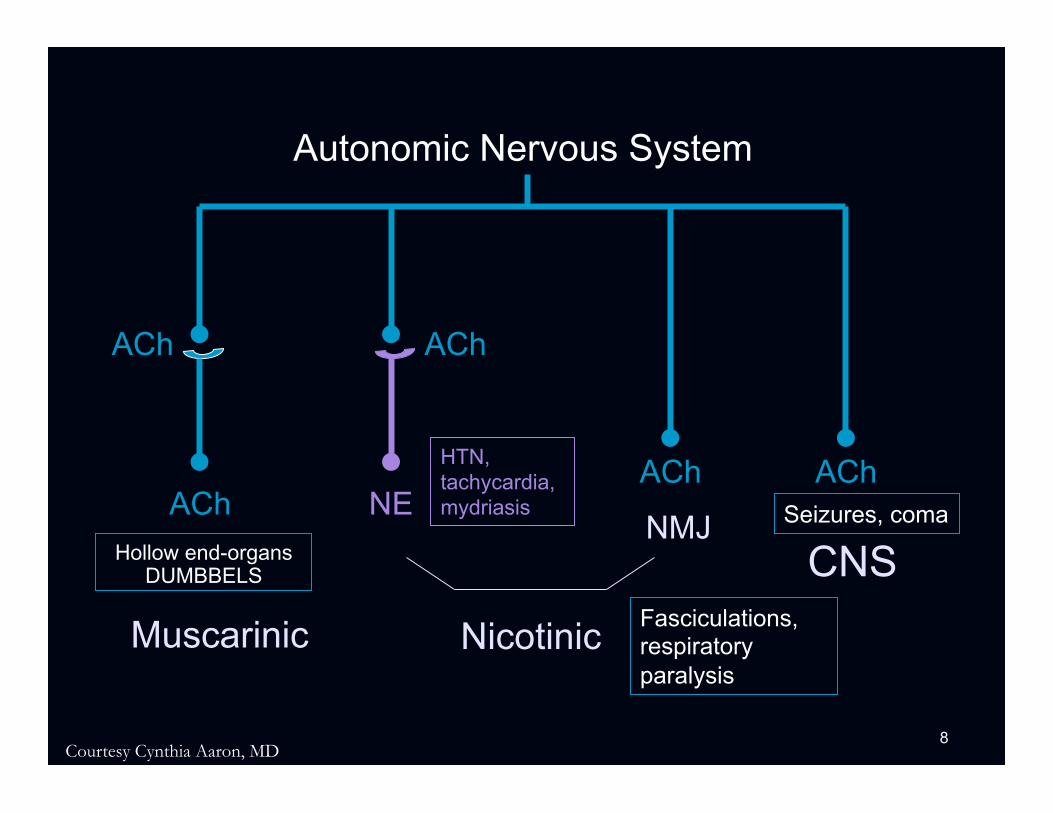
Autonomic Nervous System
ACh
CNS
ACh
NMJ
ACh ACh
ACh NE
Muscarinic Nicotinic
Hollow end-organs DUMBBELS
HTN, tachycardia, mydriasis
Fasciculations, respiratory paralysis
Seizures, coma
Courtesy Cynthia Aaron, MD

9
Question
n Which one of the following agents inhibits acetylcholine release?
A. Bupropion B. Disulfiram C. Mirtazapine D. Tizanidine E. Yohimbine
10
Answer
n Which one of the following agents inhibits acetylcholine release?
A. Bupropion B. Disulfiram C. Mirtazapine D. Tizanidine E. Yohimbine
11
Agents that Block ACh Release
n Alpha2-adrenergic agonists n Botulinum toxin n Crotalinae venoms n Elapidae beta-neurotoxins n Hypermagnesemia

12
Nicotinic Receptor Agonists
n Initial activation of receptors n Prolonged depolarization leads to inhibition
n Initial sympathomimetic, GI distress, fasciculations, seizures
n Then BP, HR, paralysis, coma

13
Nicotinic Receptor Agonists
n Nicotine alkaloids (nicotine, coniine) n Carbachol (mainly muscarinic effects) n Cytisine n Lobeline n Methacholine (minimal effects) n Succinylcholine (initial effects)

14
Nicotinic Receptor Antagonists
n NMJ blockers: weakness, paralysis n Curare, atracurium, alpha-bungarotoxin
n Peripheral neuronal blockers: autonomic ganglionic blockade n Trimethaphan (not entirely specific, may produce
NMJ blockade)

15
Nicotinic Indirect Agonists
n Bind to distinct allosteric sites on the nicotinic receptor, not ACh binding site (enhanced channel opening) n Physostigmine n Tacrine n Galantamine

16
Nicotinic Indirect Antagonists
n Bind to distinct allosteric sites on the nicotinic receptor, not ACh binding site (decreased channel opening) n Chlorpromazine n Ketamine n Phencyclidine (PCP) n Local anesthetics n Ethanol n Corticosteroids

17
Buzzwords
n Nicotine alkaloids (nicotine, coniine) n Trick to remember the hemlocks –
n Water Gate Candidate Scandal (Water hemlock, GABA, Cicutoxin, Seizures)
n Poison Control Network (Poison hemlock, Coniine, Nicotinic)

18
Muscarinic Agonists
n Peripheral: DUMBBELS n Central: Sedation, dystonia, coma, seizures
n Muscarine n Bethanachol n Pilocarpine
19
Question
n A 35-year-old man presents to hospital with vomiting, diarrhea, profuse sweating, and mild bradycardia. What is the most likely mushroom he ingested
A. Amanita phalloides B. Clitocybe dealbata C. Cortinarius orellanus D. Gyromitra esculenta E. Tricholoma equestre
20
Question
n A 35-year-old man presents to hospital with vomiting, diarrhea, profuse sweating, and mild bradycardia. What is the most likely mushroom he ingested
A. Amanita phalloides B. Clitocybe dealbata C. Cortinarius orellanus D. Gyromitra esculenta E. Tricholoma equestre

21
Buzzwords
n Mushrooms n Clitocybe Inocybe Muscarinic n (California international marathon) – sweat like crazy

22
Muscarinic Antagonists
n Peripheral: mydriasis, anhidrosis, tachycardia, urinary retention, ileus, dry and flushed skin
n Central: delirium, agitation, hallucinations, coma n Atropine n Antihistamines n Benztropine n Cyclic antidepressants n Phenothiazines n Scopolamine

23
Histamine
24
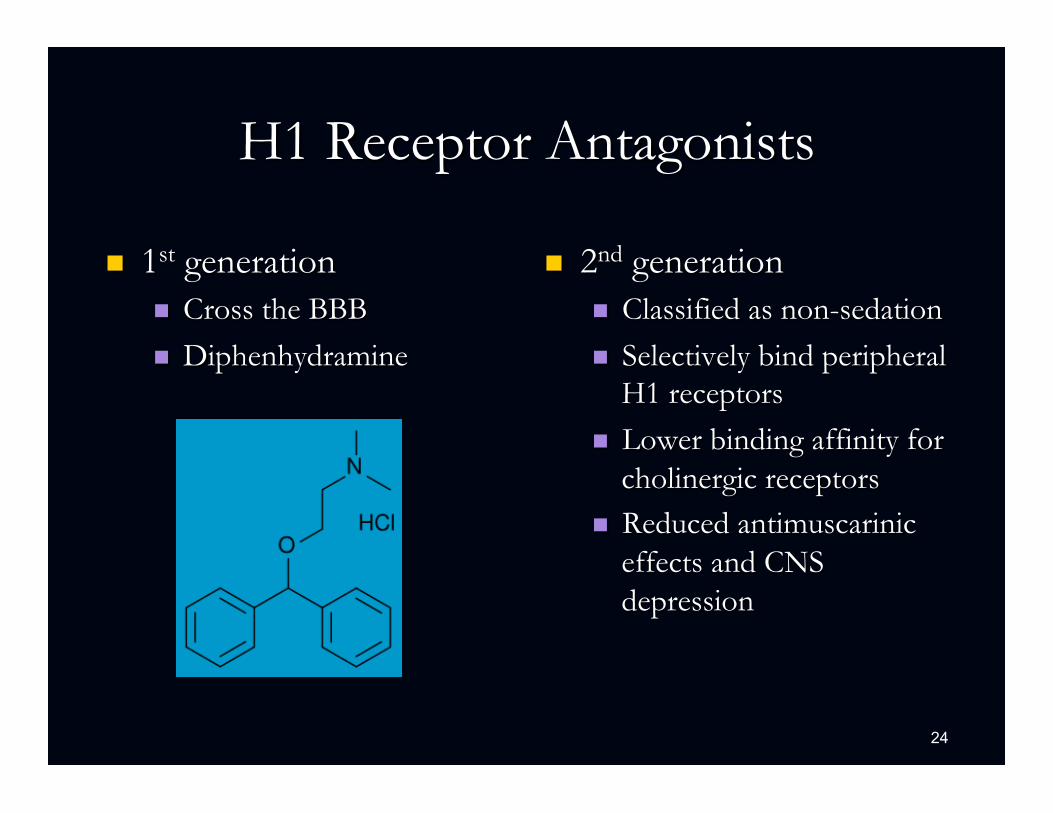
H1 Receptor Antagonists
n 1st generation n Cross the BBB n Diphenhydramine
n 2nd generation n Classified as non-sedation n Selectively bind peripheral
H1 receptors n Lower binding affinity for
cholinergic receptors n Reduced antimuscarinic
effects and CNS depression

25
H1 Receptor Antagonists
Terfenadine terfenadine carboxylate
Astemizole desmethylastemizole
n Parent compounds block Ikr n Increased risk of TdP n Withdrawn from market in 1998
CYP3A4
CYP3A4

26
H1 Receptor Antagonists
n Clinical manifestations n CNS depression n Antimuscarinic effects n Cardiac
n Na and Ikr blockade (QRS and QT prolongation) with diphenhydramine

27
H2 Receptor Antagonists
n Hydrophilic – poor access to CNS n Alter gastric pH
n May impact absorption of acid-labile drugs n e.g., ketoconazole

28
Cimetidine
n Only H2 receptor antagonist to inhibit P450 isozymes (specifically CPY3A4) n Useful in dapsone-induced methemoglobinemia n Useful in toxicity from Gyromitra esculenta
n Associated with myelosuppression if taken with drugs associated with BM suppression
n Rapid IV dosing may result in bradycardia, hypotension, and cardiac arrest
29
Serotonin
30
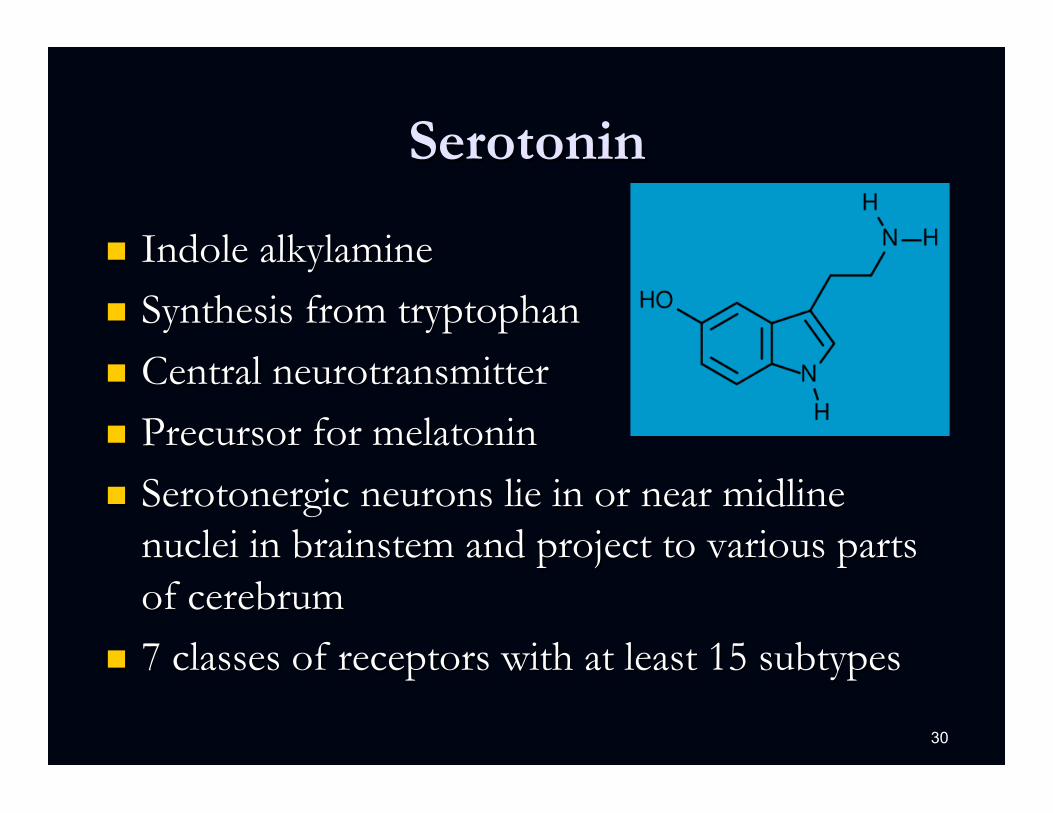
Serotonin
n Indole alkylamine n Synthesis from tryptophan n Central neurotransmitter n Precursor for melatonin n Serotonergic neurons lie in or near midline
nuclei in brainstem and project to various parts of cerebrum
n 7 classes of receptors with at least 15 subtypes

31
Serotonin Synthesis & Metabolism
Tryptophan
5-OH-Tryptophan
Serotonin
5HIAA
tryptophan hydroxylase (rate limiting)
l-aromatic acid decarboxylase
MAO, aldehyde dehydroxylase
5HIAA: 5-OH-indoleacetic acid
32
Serotonin Agonists
n Enhanced synthesis n L-tryptophan (associated with eosinophilia myalgia
syndrome) n 5-OH-tryptophan n Prescription drug (Tryptan)

33
Increased Serotonin Release
n Amphetamines (MDMA) n Cocaine n Codeine derivatives n Dexfenfluramine n Fenfluramine n L-Dopa

34
Other Serotonins
n Inhibit Serotonin Metabolism n MAO-I
n Unknown Serotonin Effect n Lithium
35
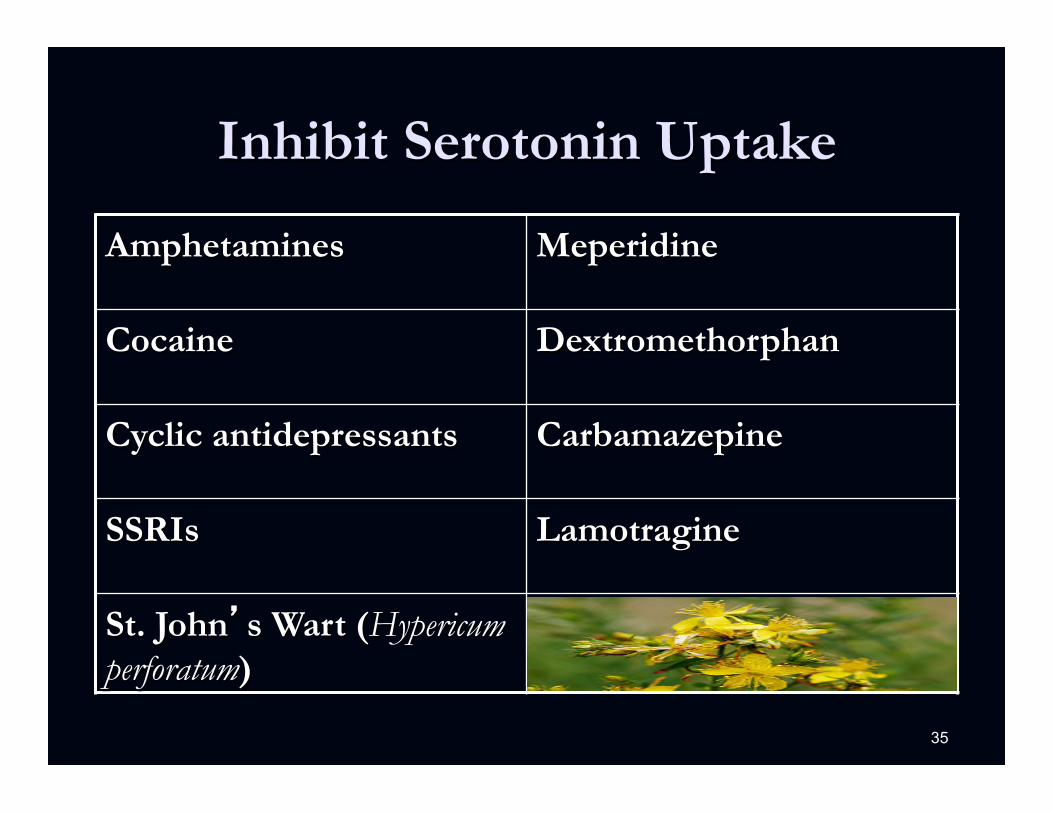
Inhibit Serotonin Uptake
Amphetamines Meperidine
Cocaine Dextromethorphan
Cyclic antidepressants Carbamazepine
SSRIs Lamotragine
St. John’s Wart (Hypericum perforatum)

36
Direct Serotonin Antagonists
5-HT1
5-HT2
Methysergide, cyproheptadine
5-HT2 Trazadone, nefazodone
5-HT2A
5-HT2C
Risperidone, olanzapine, ziprasidone, quetiapine, cyclic antidepressants
5-HT3 Ondansetron, granisetron, metoclopramide

37
Adenosine

38
Adenosine Receptor Antagonists
n Methylxanthines n Theophylline n Caffiene n Theobromine

39
Normal Adenosine Accumulation and Physiologic Response
n Adenosine accumulates in the extracellular space during conditions of fatigue n ATP utilization > ATP synthesis
n Seizures, hypoxia or ischemia promotes accumulation
n Hypoxia adenosine kinase activity
n Adenosine promotes sleepiness

40
Adenosine A1 Receptors - CNS
n Presynaptic
n Inhibits adenylyl cyclase cAMP levels
n Inhibits presynaptic N-type Ca2+ channels n Neurotransmitter release
n GABA, NE, 5-HT and Ach
n Strongest inhibition on glutamate release
Neuroscience. 112(2):319-329 (2002)

41
Ca
Glu
Glu
Glu
Ca
Adenosine Autoreceptors and Glutamate Neurotransmission
A
Adenosine R1
Ca R
Glu
Glu
Glu
AP
Pre Post
42
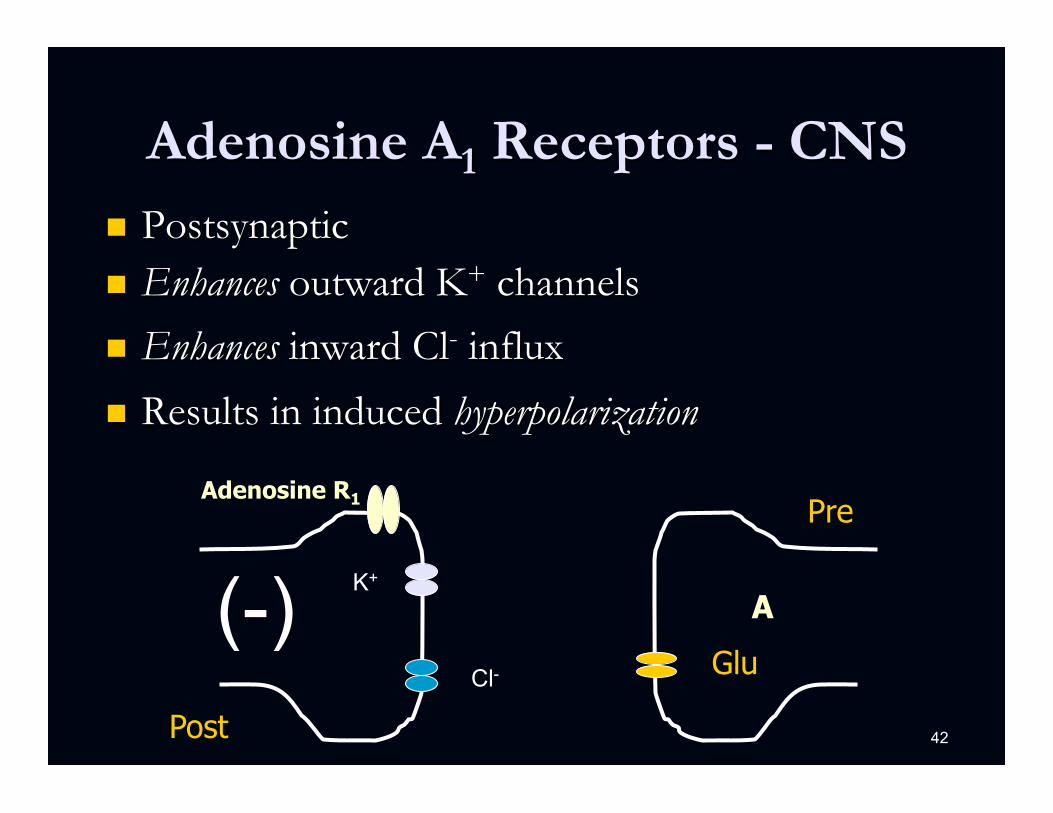
Cl-
K+
Adenosine A1 Receptors - CNS n Postsynaptic n Enhances outward K+ channels
n Enhances inward Cl- influx
n Results in induced hyperpolarization
(-) A
Adenosine R1
Glu
Pre
Post
43
Adenosine A1 Antagonism
n Cardiac n HR n Atrial inotropicity n Response to epinephrine
n CNS n Excitatory amino acid (EAA) release
n Renal n Diuresis
44
Question
n Which of the following laboratory abnormalities is consistent with acute theophylline toxicity?
A. Hyperchloremia B. Hypernatremia C. Hyperphosphatemia D. Hypokalemia E. Hypoglycemia
45
Question
n Which of the following laboratory abnormalities is consistent with acute theophylline toxicity?
A. Hyperchloremia B. Hypernatremia C. Hyperphosphatemia D. Hypokalemia E. Hypoglycemia
46
Questions?
Good Luck!!