data security and research 101 completing required forms kimberly summers, pharmd assistant chief...
TRANSCRIPT

Data Security and Research 101 Completing Required Forms
Kimberly Summers, PharmDAssistant Chief for Clinical Research
South Texas Veterans Health Care SystemResearch and Development Service
(210) 617-5300 x [email protected]
Goal of VA Privacy and Information Security
• Protecting the privacy of our veterans• Assuring the confidentiality of research
subjects’ data• Ensuring research will continue within the
VA• Ensuring the stackholder's and public’s
confidence in the integrity of the data
Concerns Regarding VA Research And Cyber-Security
• Large data sets with PHI & identifiers– VA leads the world in electronic records– VA also receives Medicare Data – Genomic medicine raises new concerns
• VA investigators have many collaborators• Abundance of devices• Recent negative publicity regarding loss of VA-
sensitive information
VHA Privacy Program
• Consists of 6 statues that govern collection, maintenance, and release of information– Provision of the Freedom of Information Act, Privacy
Act, Title 38 United States Code (U.S.C.) (U.S.C. Sections 5701, 5705, 7332), and Standard of Privacy of Individually-Identifiable Health Information, 45 Code of Federal Regulations (CFR) Parts 160 and 164, hence Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule
• VHA Handbook 1605.1addresses most requirements– Investigators must have the authority to collect, use,
or disclose private information

Investigator’s Certification: Storage and Security of VA Research Information
• February 2007– Deputy Under Secretary for Health Operations and
Management and Chief Research and Development Officer established a process by which PIs be certified as meeting the security requirements for VA research information
• All active protocols had to be certified by ACOS/Research, Information Security Officer (ISO), Privacy Officer, and Director as compliant
• The STVHCS research program (all protocols) was in jeopardy of being shut down if the entire program didn’t meet the standards
Annual Certification
• By April 15 of each year– PI must confirm all active research protocols
continue to meet the VA data security standards and requirements
• Process for annual recertification in development• Annual security training
– Cyber Security, Privacy, and Data Security
– Annual certifications are forwarded to the STVHCS Medical Center Director and VISN Director

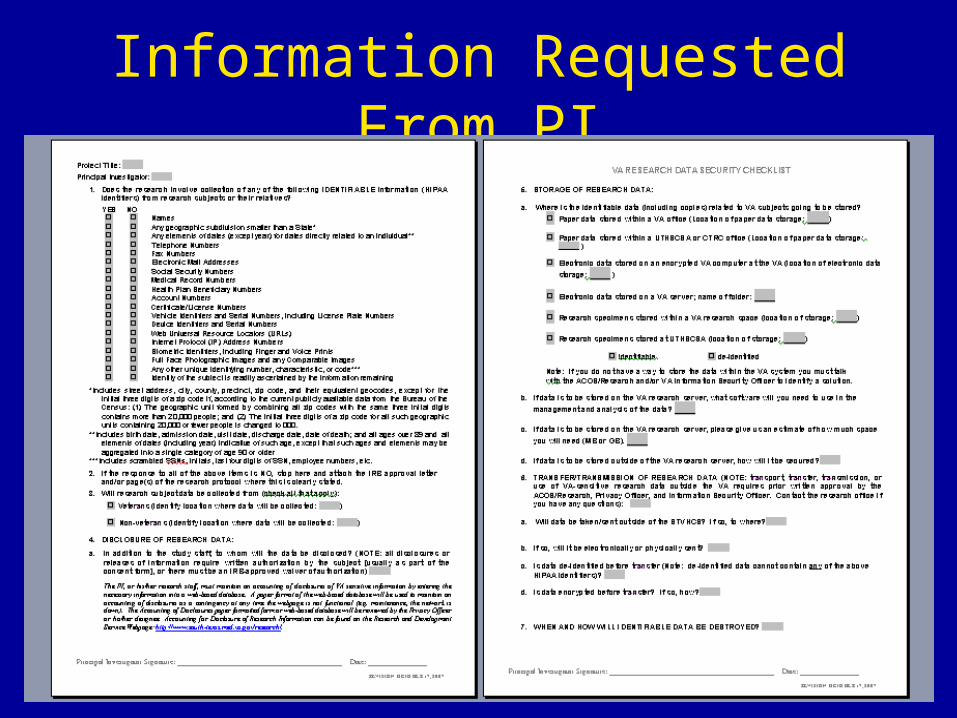
Collection, Storage, and Use of VA-Sensitive Research Data
• All protocols submitted for IRB and R&D approval must:– Contain specific information on all sites where
data will be used or stored– How data will be transmitted or transported– Who will have access to the data– How data will be secured
• Information contained in the Data Security Checklist

• Completed by R&D office based on information provided by investigator during the pre-review process
• Returned to PI for signature
• Reviewed and signed off on by the ACOS/Research and ISO
• Forwarded to Hospital Director for certification
Information Requested From PI

Background and Definitions Required to Complete VA Research Data Security
Checklist

VA-Sensitive Research Data
• Individually-identifiable research data collected on a veteran subject through a STVHCS approved protocol
• Individually-identifiable research data collected on a veteran or non-veteran within the STVHCS
• Individually-identifiable research data collected as part of a VA-funded study
Not VA-Sensitive Data
• Non-identifiable data
• Data collected on non-veterans outside of the VA on a non-VA funded project

HIPAA and Research
• Controls use of protected health information (PHI)– Within the covered entity (STVHCS)– Disclosures outside the covered entity– Allows only the “Minimum Necessary” information
• Use of PHI requires an authorization or waiver of authorization:– Informed consent / HIPAA authorization from patient– IRB waiver of authorization for exempt research
• 18 defined “HIPAA identifiers”
HIPAA Identifiers1. Names
2. ALL geographic subdivisions smaller than the state
3. All elements of dates smaller than a year and all ages over 89
4. Phone numbers
5. Fax numbers
6. E-mail addresses
7. Social Security numbers (SSN)
8. Medical record number
9. Health plan beneficiary numbers
10. Any other account numbers
11. Certificate/license numbers
12. Vehicle identifiers and license plate numbers
13. Device identifiers and serial numbers
14. WEB URL's
15. Internet IP address numbers
16. Biometric identifiers (fingerprint, voice prints, retina scan, etc)
17. Full face photographs or comparable images
18. Any other unique number, characteristic or code

HIPAA Identifiers Continued
• Any other unique number, characteristic or code– Scrambled SSN– Initials– Last four digits of SSN– Employee numbers– Etc.
• HIPPA also states that the entity does not have actual knowledge that the remaining information could be used alone or in combination with other information to identify an individual who is the subject of the information


HIPAA and The Common Rule
• Two different regulations• VA requires de-identification by both• Common Rule states the identity of the
subject can not be readily ascertained by information remaining after removal of all 18 HIPAA identifiers– After stripping all 18 identifiers the remaining
information may still be identifiable (e.g. through statistical analysis)

Keys To Coding Systems
• If non-identifiable information is linked to identifiable information with the use of log (e.g. coding system)– Logs are identifiable and VA-sensitive
research data
– Applies to data and specimen logs


If There Is No Collection of Identifiable Information
• Should be consistent with informed consent document and HIPAA authorization
• Should be consistent with protocol
• Provide IRB approval letter for exempt research or page(s) of protocol which clearly states no identifiable information will be collected

Disclosure of VA-Sensitive Research Data
Disclosure of Research Data
• Release, transfer, or provision of access to, or divulging in any other manner information outside the VA
• VHA Handbook 1605.1• STVHCS is required to maintain an accounting of all
disclosures of individually-identifiable information including those for state reporting and research
• Disclosure of de-identified data, or a limited data set, does not require an accounting

Limited Data Set
• Data set that contains PHI that excludes 16 categories of direct identifiers
• May contain identifiable information– Scrambled SSN– City, State, ZIP code– Elements of date and other numbers– Characteristics or codes not listed as direct
identifiers
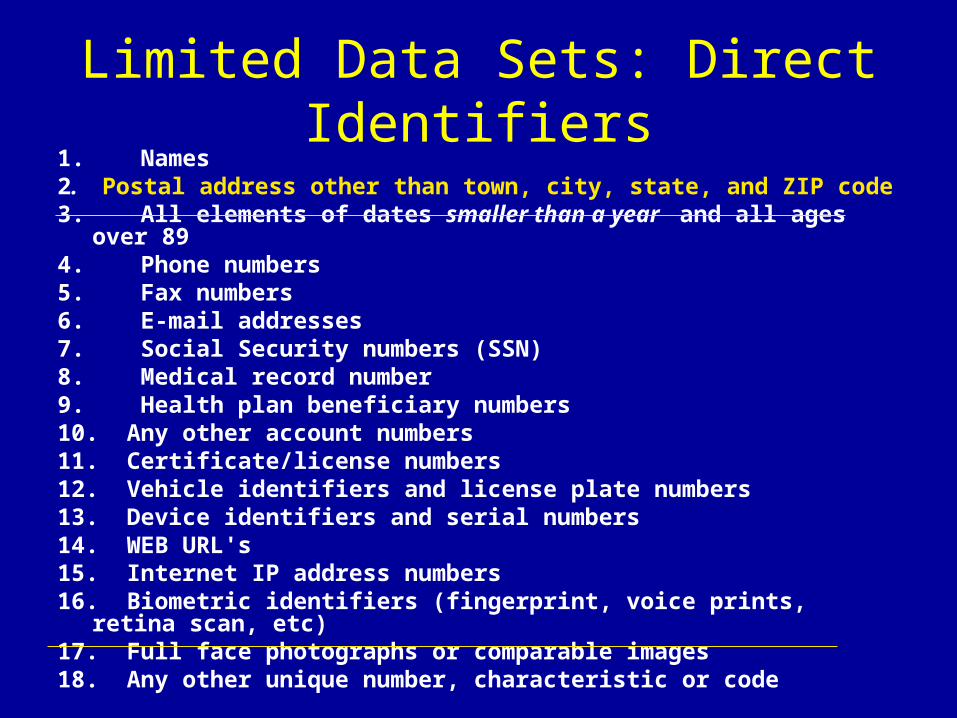
Limited Data Sets: Direct Identifiers1. Names2. Postal address other than town, city, state, and ZIP code3. All elements of dates smaller than a year and all ages over 894. Phone numbers5. Fax numbers 6. E-mail addresses7. Social Security numbers (SSN)8. Medical record number9. Health plan beneficiary numbers10. Any other account numbers 11. Certificate/license numbers12. Vehicle identifiers and license plate numbers13. Device identifiers and serial numbers14. WEB URL's15. Internet IP address numbers16. Biometric identifiers (fingerprint, voice prints, retina scan, etc)17. Full face photographs or comparable images18. Any other unique number, characteristic or code
Accounting of Disclosures For VA-Sensitive Research Excluding Limited Data Sets
• The accounting must include:– Date, nature, and purpose of the
disclosure; and– Name and address of the person or
agency to whom the disclosure is made
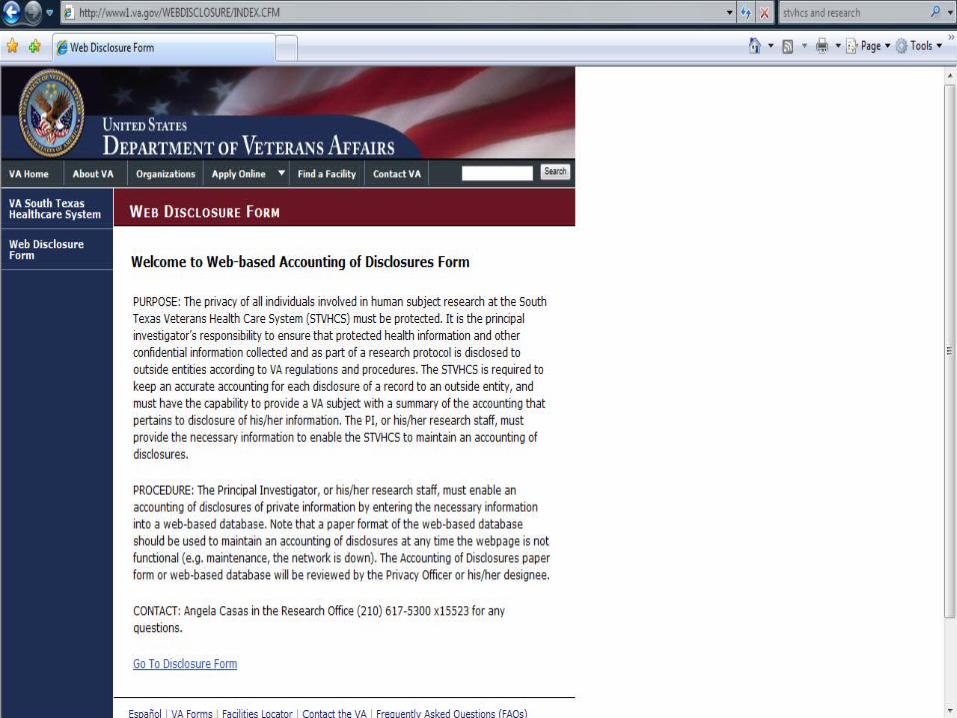
• Web-based database available– A paper format of the web-based database
will be used as a contingency if needed


Privacy Office Review
• STVHCS Privacy Officer or designee– Provide consultation as needed in the pre-
review process– Attends the R&D Committee meetings– Performs a final privacy approval prior to
activation of any research protocol• Signature required for R&D approval
– Monitors the disclosures of private information at least quarterly

STVHCS Privacy Office Contacts
• Vickie Macdonald, RHIT– (210) 617-5661– [email protected]
• Mary Wohl– (210) 617-5300 ext 15602– [email protected]

Storage of VA Research Data

Storage of VA-Sensitive Paper Research Data
• Lower risk of loss or compromise• Physical security controls
– Within the VA system• Locked room, locked cabinet • Access limited to research staff
– At the UTHSCSA• Physical security arrangements must be inspected
and approved by ACOS/Research and ISO
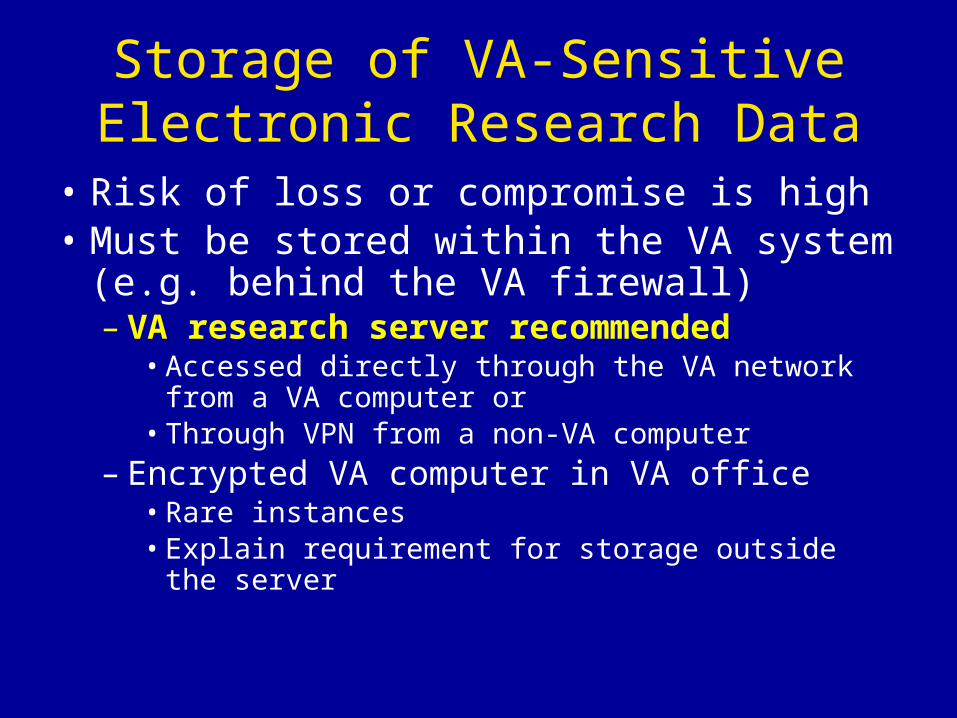
Storage of VA-Sensitive Electronic Research Data
• Risk of loss or compromise is high• Must be stored within the VA system (e.g.
behind the VA firewall)– VA research server recommended
• Accessed directly through the VA network from a VA computer or
• Through VPN from a non-VA computer– Encrypted VA computer in VA office
• Rare instances• Explain requirement for storage outside the server

VA Research Server• For instructions on how to set up an
investigator folder on the VA Research server and/or
• To obtain VPN access– Contact R&D office
• Angela Casas (210) 617-5300 x15523• [email protected]
– Contact Information Security Officer (ISO)• Gerald Steward (210) 617-5300 x14734• [email protected]

Transfer / Transmission of Research Data

Sharing Research Data: Often Appropriate and Necessary
• With collaborators • With those who have specialized
expertise• With data coordinating centers for
Multi-site studies • With outside sponsors of research

Transfer or Transmission of Research Data Outside the VA
• Transfer to entity other than the sponsor or its designated data center– Requires prior written approval from
• ACOS/Research• Privacy Officer• Information Security Officer
• Applies to any VA-sensitive research data– Including limited data-sets
• Transfer of data should be described in the protocol and consent / HIPAA authorization
• Transfer or transmission requires an accounting of disclosure
Forms For Authorization of Transfer
Data Use AgreementData Transfer Agreement for within VHAData Transfer Agreement for outside VHARemovable Storage Media Agreement
• For assistance obtaining the appropriate forms – Contact R&D office
• Angela Casas (210) 617-5300 x15523• [email protected]
• Forms will be available on STVHCS Research website in future

Loss or Compromise of VA-Sensitive Research Data
• Must be reported promptly to:– Supervisor– ACOS/Research– Information Security Officer (ISO)– Privacy Officer– IRB
• Reported as an Unanticipated Problem Involving Risk to Subjects or Others (UPIRSO)

Loss of a Device Used to Transport, Access or Store VA-Sensitive Information
• Must be reported promptly to:– Supervisor– ISO– If within a VA facility to the VA police
• If traveling or at another institution report to the security/police officers of the institution and obtain:– Case number– Name and badge number of the investigation officer– Copy of the case report, if possible

Data Security and Research: The Stakes are High
• VA must assure information security & privacy protects research subjects and facilitates current and future research– May also protect the researcher
• Negative publicity impacts the local research program and investigators, VA research in general, and VHA health care