daniel deutscher, pt, phd foto 15 th annual outcomes conference 2015 level of mckenzie education...
TRANSCRIPT

Daniel Deutscher, PT, PhDFOTO 15th Annual Outcomes Conference
2015
Level of McKenzie Education
Functional Outcomes
and Utilization
in Patients with Low Back Pain
JOSPT Dec 2014;44(12):925-936.

Background
• Common use of PT and MDT in treating LBP (Battie 1994;
Foster 1999; McKenzie & May 2003; Byrne 2006 )
• Recommendation for classification based treatment (Delitto 1995; Brennan 2006; Fritz 2007…)
McKenzie = Mechanical Diagnosis and Therapy (MDT)

Background
• Deutscher et al: Arch Phys Med Rehabil 2009; Associations between treatment processes, patient characteristics, and outcomes in outpatient physical therapy practice
– Self-exercise compliance predicts higher outcomes
– Lower self exercise compliance in patients with spinal impairments (lumbar & Cervical) compared to peripheral impairments (shoulder & knee)
– Therapeutic exercise prescribed more to patients with peripheral impairments

Background
• Therapists’ confidence in prescribing exercises to peripheral compared to spinal joints…?
• Need for more education on effectiveness of exercises for spinal impairments…?

Background
Maccabi initiates an intensive MDT educational program
• Supervised and home exercise therapy customized to a patient’s clinical presentation for LBP have been suggested as effective means to improve outcomes
• These therapy principles are important components of the McKenzie treatment-based classification system

Background
McKenzie Training process and data collection period

Background: McKenzie Classification System
Purpose
Examine associations between Level of McKenzie post-graduate training (A-D and post certification) and:
– Functional status at discharge
– Utilization (number of PT visits)
controlling for patient and therapists risk factors at admission
Methods: Design
• Practiced based evidence (PBE)
• Prospective
• No alteration of normal treatment
• Patient informed consent exempt by IRB
Methods: Patients
• 18 years old or older
• Selected lumbar area as primary impairment between April 2006 to December 2012
• Two or more visits
• Intake FS data; N=36,348– 93% Participation rate
• Intake & Discharge FS data; N=20,882– 57% Completion rate
• No exclusion criteria!!!

Methods: Clinicians
• 72 outpatient clinics throughout Israel
• 195 Therapists with no prior MDT education
• Took at least Part A
• Had at least one year of experience treating patients with LBP
• >= 40% overall completion rate per therapist
• >= 30 complete episodes per therapist
• Same therapist throughout the episode of care

Methods: Patients & Clinician
Methods: Analysis
• Descriptive statistics to examine categorical and continuous measures.
• Assess possible patient selection bias by comparing patients with complete vs. incomplete outcomes data
• Hierarchical linear regression models with patients nested within therapists.
• Assess associations between MDT educational levels & FS outcomes & number of visits after controlling for patient risk factors

Results…
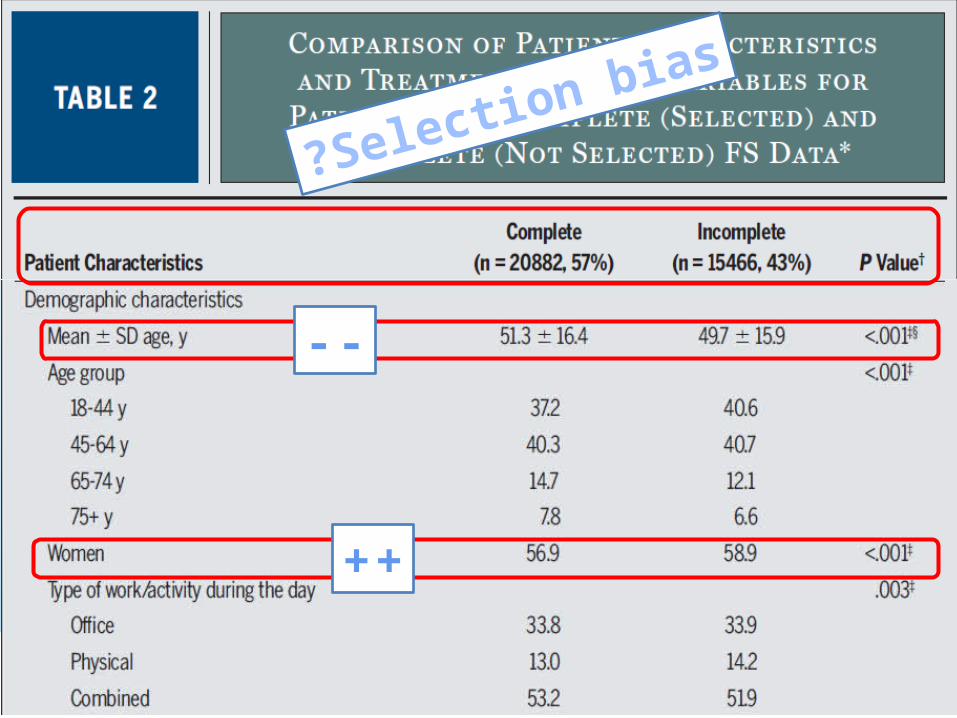
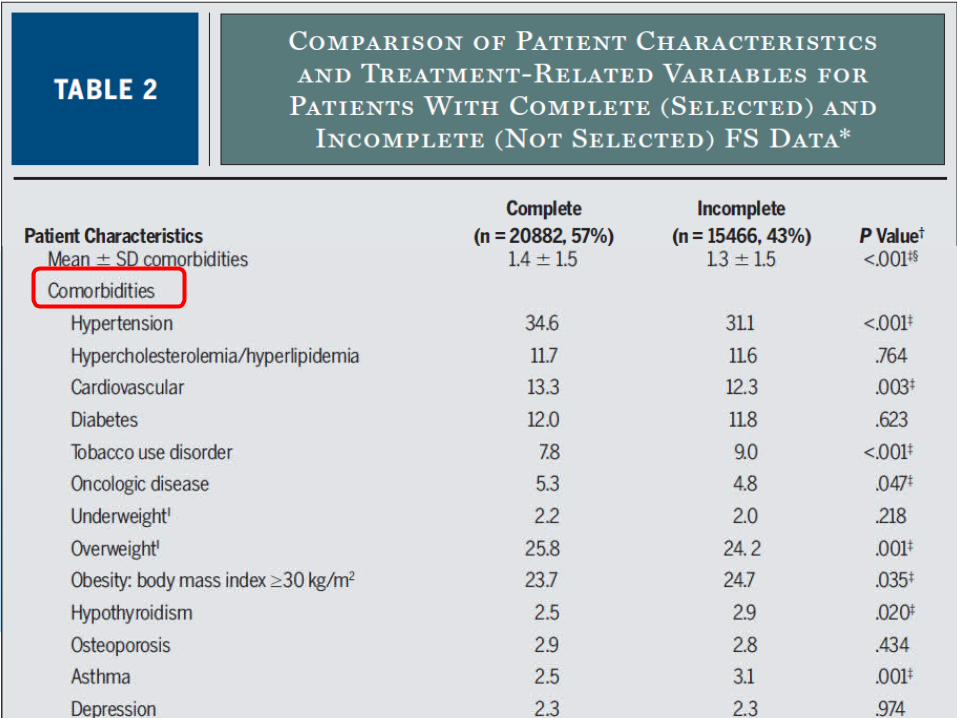
Selection bias?
--
++
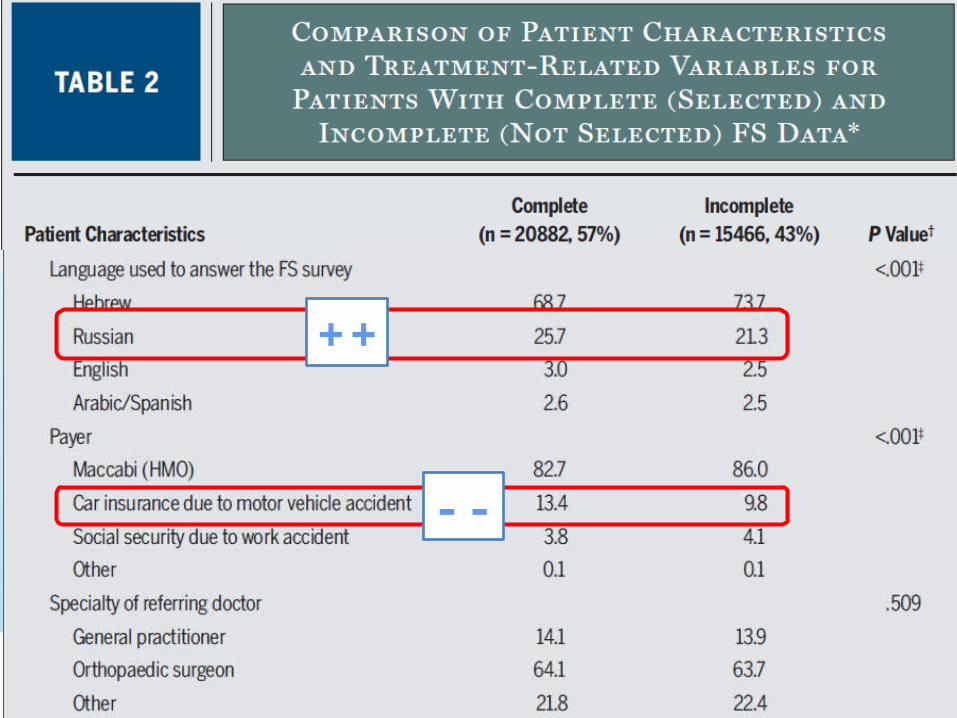
--
++

--


Results…
Selection bias?
Patients with complete or incomplete data had higher values or prevalence for characteristics predictive of both
lower and higher FS change
No support for a systematic patient selection bias

Results: Outcomes measures

Results: Functional Status Change
FS change(SD) during 2005-2008=11.1(12.9), N=7,216(Deutscher et al 2009)
MCII=5(Hart et al 2010)
Unadjusted FS change

Results: Risk Adjusted FS Outcomes
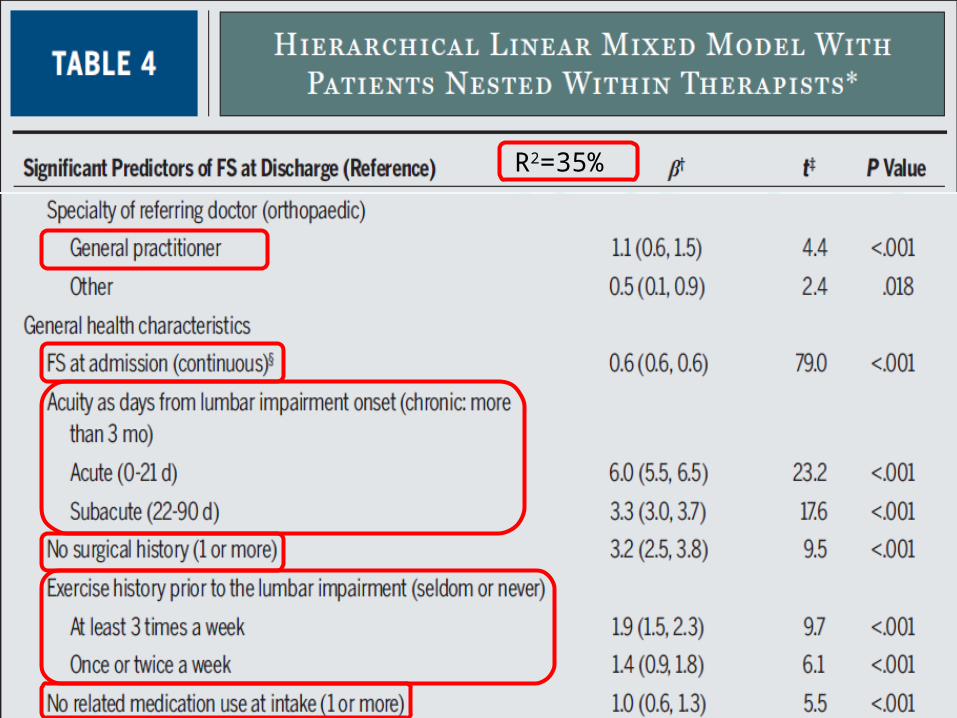
R2=35%
Results: Risk Adjusted FS Outcomes

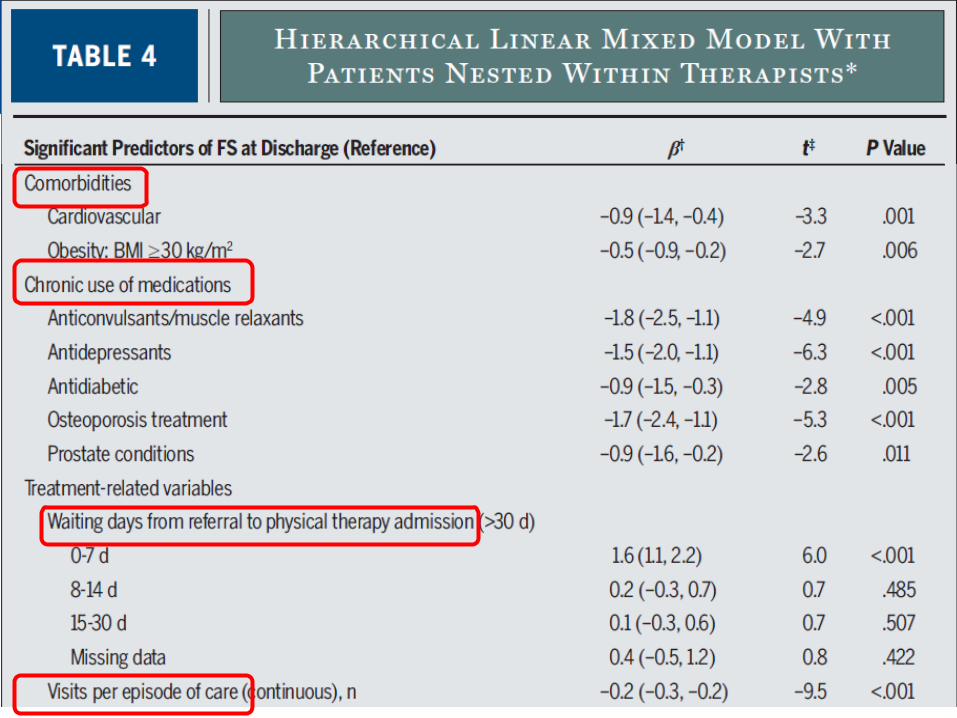
Results: Risk Adjusted FS Outcomes

Results: Risk Adjusted FS Outcomes
Adjusted FS change
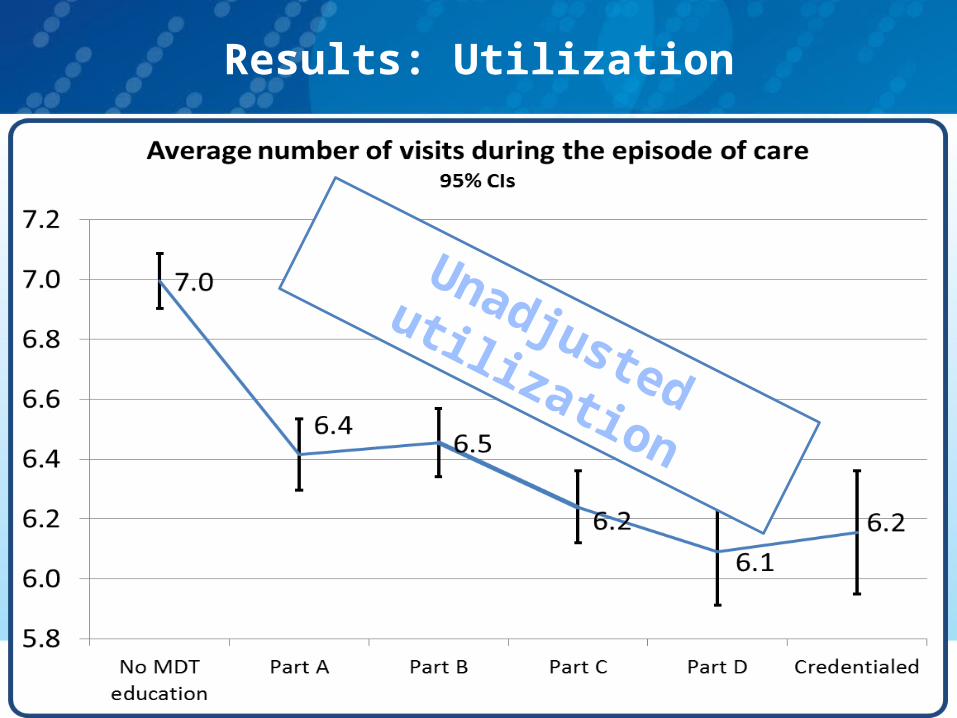
Results: Utilization
Unadjusted utilization

Results: Utilization
R2=6%
Adjusted utilization
Study limitations
• Possible patient selection bias not supported but still exists– 57% completion rate, 31% dropout (57/69=83%)
– Imbalances in group characteristics, some in favor of the selected group, and some in favor of the group not selected
– Negligible potential selection bias probably not differing by level of McKenzie education

Study limitations
• Possible therapists selection bias– Generalizability to other countries with differing physical
therapy education?
– Level of professional commitment for therapists engaged in continuing education?
– Most therapists did not take all levels of education
– Non-formal education between therapists with different levels of education

Study limitations
• Causal factors related to better outcomes are not known due to the observational design– Possible time confounder (better outcomes over time due to
the passage of time and general experience), although therapists with no McKenzie education were treated during most of the study period
– Missing confounders (patient education, socioeconomic levels, psychosocial factors, patient-therapist working alliance)
– Interventions were not included
Main results – Functional Status
• Potential for improved FS outcomes after engaging in a post-graduate McKenzie educational program
• Improvement in FS was modest
• Similar FS outcomes between educational levels Part A to CRD

Main results – Utilization
• Significant decrease in utilization associated with McKenzie training
• 11-13% decrease in number of visits at advance levels (Part C and above), 7-9% decrease in number of visits at basic levels (Parts A & B)
• Lower utilization associated with higher outcomes after adjusting for significant patient risk factors
• Potential of 1.5-3% improvement in the overall physical therapy service efficiency due to patients with lumbar impairments only (~20% of all patients).
Implications
McKenzie education may lead to a small improvement
in functional outcomes over a shorter episode of care
Future research
• McKenzie education impact on clinician practice behaviors (intervention) and outcomes
• Outcomes at diplomat postgraduate training level (Rodeghero 2015: PT fellowship-higher outcomes than residency or none)
• Impact of a modified educational process?– More active student involvement in classification &
treatment decisions?– Long term post-course implementation– Ongoing follow-up training between courses– Interactive learning in small groups (audit circles)– Additional accreditation requirements

Future research
• Specific therapists’ responses to MDT (or other) education?– Improved outcomes
– No change
– Decreased outcomes
• Therapist-Patient working alliance influence on outcomes (Hall et al 2010)
• Reflection, collaborative clinical reasoning, and patient empowerment influence on outcomes (Resnik & Hart 2003)
Therapists explained 2.2% of variance
(P<.001)

Thank You 195 participating therapists
PT Clinic & District managers
District PT directors of R&D
PT Dept. head directors
(Moshe Gutvirtz & Ditza Gottlieb)
McKenzie Inst. Instructors
Co-authors:
Mark Werneke, Dr. Linda Resnik,
Dr. Julie Fritz and Ditza Gottlieb