d2 gastrectomy
DESCRIPTION
surgical procedureTRANSCRIPT

D2 GASTRECTOMY
Dr K Suneel Kaushik Senior Resident
Surgical Oncology

Complete operative resection remains the only potentially curative modality for gastric adenocarcinoma
Assess if the patient is fit for surgery… Extent of resection? Extent of lymphnode dissection? Value of extended organ resection?

Extent of resection
Determined by site and extent of the primary neoplasm
Proximal lesions and Siewert type II and III : proximal gastrectomy with esophagectomy or Total gastrectomy
Antral lesions: Distal subtotal gastrectomy
Midbody or more extensive lesions: Total gastrectomy
Total vs partial gastrectomy
Total gastrectomy for all gastric carcinomas does not improve survival
Associated with increased morbidity and mortality
Hence R0 resection of tumors by distal or subtotal gastrectomy is preferred

Extended organ resection is reserved for node negative T4 lesions involving resection of invaded portions of diaphragm, pancreas, spleen, adrenal, colon etc

Extent of lymphadenectomy
D1 vs d2 has been the focus of 6RCTs.- British Medical research Council- Dutch Gastric cancer study group- Italian Gastric cancer study Group(IGCSG)- Wu et al (D1 vs D3)- Japanese Clinical Oncology Group (D2 vs
d2 plus)- Japanese trial (D2 vs D4)

MRC trial
D1 D2 P value
No. of patients 200 200 -
Operative mortality(%) 6.5 13 <.04
Postoperative complications(%)
28 46 <0.001
5yr overall survival(%) 35 33 NS

Italian group
D1 D2 P value
No. of patients 76 86 -
Operative mortality(%) 1.3 0 NS
Postoperative complications(%) 10.5 16.3 .29
Postoperative stay(d) 12 12 NS
5y overall survival(%) NS NS NS
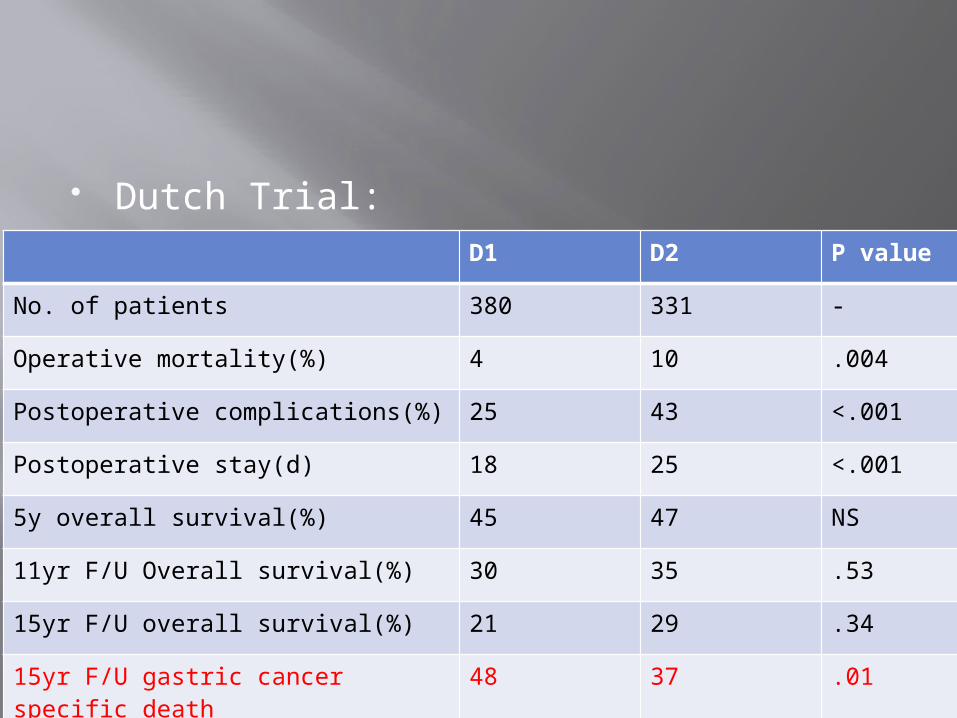
Dutch Trial:D1 D2 P value
No. of patients 380 331 -
Operative mortality(%) 4 10 .004
Postoperative complications(%) 25 43 <.001
Postoperative stay(d) 18 25 <.001
5y overall survival(%) 45 47 NS
11yr F/U Overall survival(%) 30 35 .53
15yr F/U overall survival(%) 21 29 .34
15yr F/U gastric cancer specific death
48 37 .01

Initial conclusion was that there was no role for routine use of D2 resection
It was revised after 15yr followup:
“Because spleen preserving D2 resection is safer in high volume centres it is recommended surgical approach for patients with potentially curable gastric cancer. “
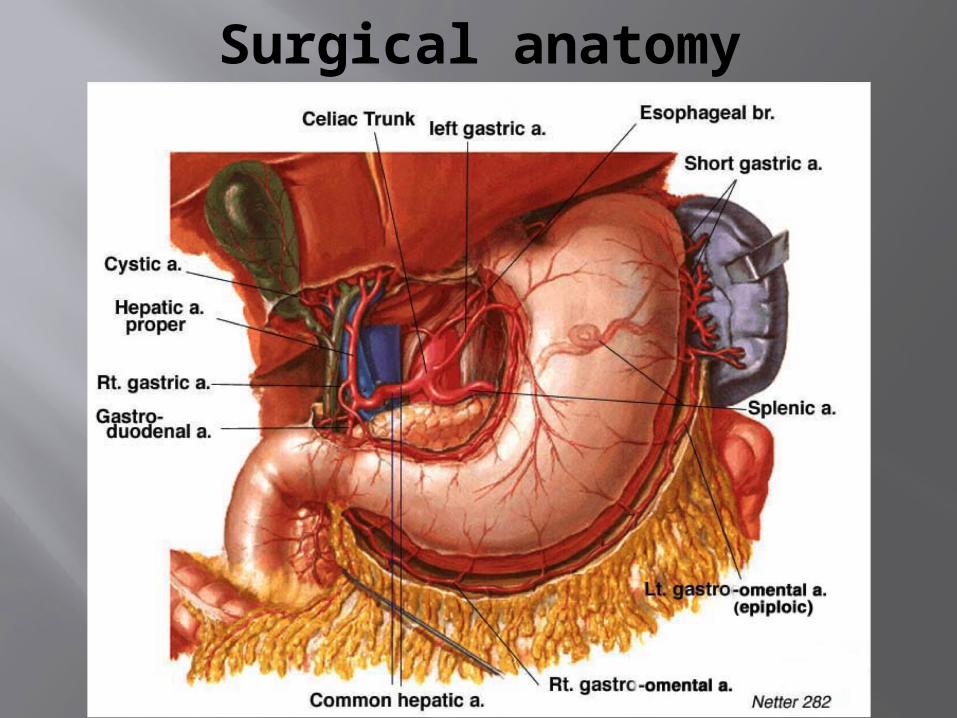
Surgical anatomy



16 nodal stations were grouped into 4N1 - The perigastric nodes directly attached along the lesser curvature and greater curvatures
N2 - The removal of nodes along the left gastric artery (station 7), common hepatic artery (station), celiac trunk (station 9), splenic hilus, and splenic artery (station 10 and 11).
N3 – Includes stations 12 through 14
N4 - stations 15 and 16 in the paraaortic and the paracolic region



Surgical Procedure
Principles:1. Extent of the lesion is determined by CT ±
EUS
2. Diagnostic laparoscopy in selected patients( advanced disease – clinical N+ /T3
3. Unresectable for cure (inoperable) : Level 3 or 4 nodes, invasion or encasement of major vascular structures, distant metastasis or peritoneal cytology positive

4. Resectable tumors :- Tis or T1 : EMR- T1b – T3 : Adequate gastric resection to
achieve negative microscopic margins ( typically ≥ 4cm from gross tumor)
- T4 : require enbloc resection of involved structures
- Include regional lymphatics : D1 or D2. D2 is the standard of care.
- Goal to examine atleast 15 nodes (NCCN)- FJ in selected patients (wh may require CRT)

4-6cm margin on either side is preferred. 2cm distal if antral lesions, proximal lesion – a lesser extent of uninvolved esophagus is acceptable.

Palliative procedures for unresectable tumors
- Palliative gastric resection - Bypass – GJ - Stenting - Gastrostomy or jejunostomy

Preop evaluation and preparation
Diagnostic evaluation Staging evaluation and assess operability Evaluate for tolerance for major surgery PFT if thoracic approach is required for
GE junction tumors Pre op antibiotic – cephalosporin single
dose just before induction

Position: - Supine with lower chest prepared in case extension of incision is required. - Consideration given for possibility of thoracic approach
Incision :- Midline- Bilateral subcostal – Chevron- Left thoracoabdominal incision

Distal Subtotal gastrectomy

Distal Subtotal Gastrectomy
Greater Curvature mobilisation :
- Dissected off the transverse colon with cautery along the avascular plane between the omentum and appendices epiploicae
- Anterior leaf of transverse mesocolon and anterior pancreatic capsule are dissected off
- Omentum is resected with the specimen along with level 4 lymphnodes.


- Dissection proceeds to the left side of abdomen and omentum dissected off the splenic flexure and inferior pole of spleen
- Left gastroepiploic vessels are identified and divided near their origin from Splenic vessels
- Preservation of short gastric vessels is critical.
Dissection of pancreatic capsule :
- A standard approach- Value is unproven, may be omitted- May result in minor pancreatic leaks- At the base of transverse mesocolon, capsule is incised and dissected from anterior surface of pancreas

Infrapyloric mobilisation :- Omentum is divided on right side upto
the duodenum- Colic branch of gastrocolic trunk(into
SMV) is identified in tranverse mesocolon and followed to its confluence with the right gastroepiploic vein.
- The right gastroepiploic vein is divided at its junction with the gastrocolic trunk and inferior pancreaticoduodenal arcade.


- Right Gastroepiploic artery is divided as it arises from the gastroduodenal artery
- Station 6 LN are dissected away from head of pancreas and included in the specimen.

Suprapyloric mobilisation- Gastrohepatic ligament is divided- Vertically in the direction of hepatic artery
proper- Right gastric artery is ligated at its origin
from either hepatic artery proper or gastroduodenal artery
- Right gastric vein is divided close to its junction with the portal vein
- Station 5 LN are dissected with the specimen


Duodenal transection:- Duodenum transected just distal to pylorus ( or
away for negative margins in distal cancers) using GIA-60 or straight Kocher clamps.
- Staple line is inverted with Lembert sutures using 3-0 monofilament absorbable material.
- Most important factor affecting the healing of stump is the adequate blood supply.

- Allows upward and forward rotation of stomach
- And easy access to node bearing areas.


D2 lymphadenectomy:
- Dividing and reflecting the peritoneum and lymphatics in superior porta hepatis from right to left and above downwards.
- Station 8: Nodal tissue dissected from right to left on anterior surface of common hepatic artery(8a), hepatic artery is gently retracted to the right side and nodal tissue between common hepatic artery and portal vein dissected(8b)


- Station 12 : Hepatoduodenal LN along the hepatic artery proper, Bile duct and portal vein are dissected
- Left gastric vein is ligated at its entry into portal or splenic vein
- Station 11: Along the upper border of pancreas and proximal splenic artery dissected

- Dissection continues medially into the coeliac axis
- Left gastric artery is ligated at its origin from coeliac trunk
- Adjacent nodal tissue is reflected towards the crura of diaphragm


- Dissection then proceeds proximally along the lesser curvature
- Nodal tissue along the 2-3cm of abdominal esophagus is dissected (Station 1)
- Station 10: may not routinely be required for distal gastrectomy

Gastric transection:- Along the line connecting about 2cm distal to
the GEJ on lesser curvature and a point 5cm proximal to the upper border of the tumor on greater curvature side
- Straight clamps are applied for 6-8cm on greater curvature side and divided with knife
- The remaining stomach from tips of straight clamps to chosen point on lesser curvature with GIA stapler.

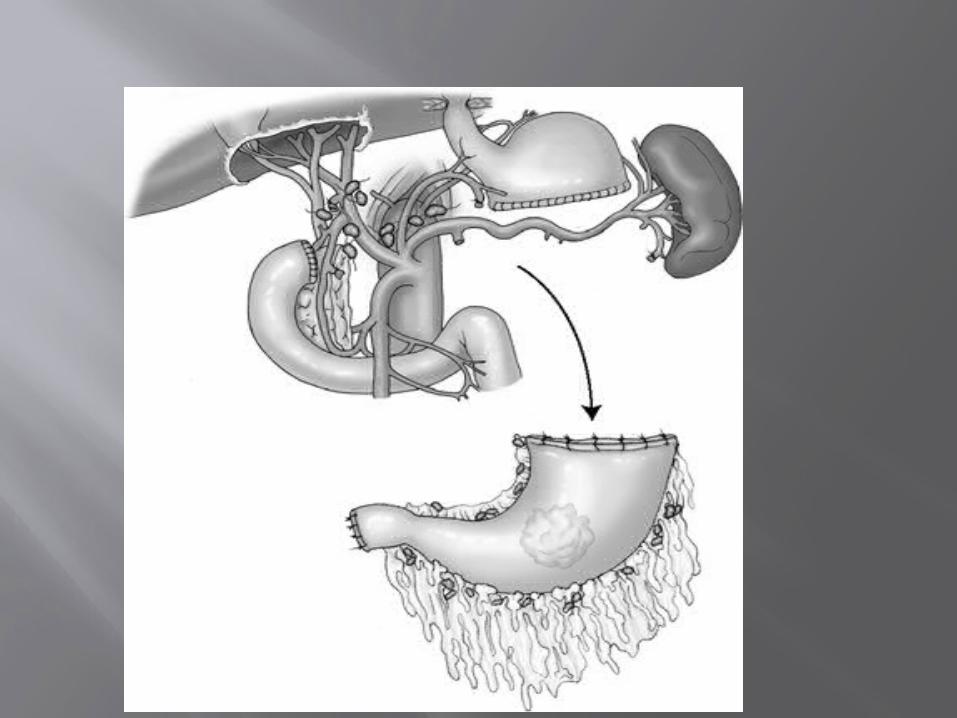

Total Gastrectomy : The paracardial LN reflected inferiorly and the entire stomach is lifted forward and the GE junction is mobilised and divided using a Satinsky atraumatic vascular clamp. ± frozen for margin.
Positive microscopic margin is a negative prognostic factor in patients who have <6nodes positive. If >5nodes positive no longer an independent predictor of poor survival.
- But because nodal status is not known in majority of patients at surgery, frozen is usually preferred.
Reconstruction : - Roux en Y Esophagojejunostomy
- Roux en Y Gastrojejunostomy
- Billroth II Loop Gastrojejunostomy (antecolic or retrocolic)
- Billroth I Gastroduodenostomy

Billroth II GJ

Standard two Layerhand Sewn anastomosis


Roux en y GJ


Following Total gastrectomy

Postoperative care
Early mobilization and pulmonary toilet Continuous Epidural analgesia Prophylactic broad-spectrum antibiotics
for 24hrs Careful fluid and electrolyte balance Packed red blood cells if Hb <7g% or
Hb ,9g% if symptomatic. NG tube removed with return of bowel
movements or when is output is low

Postgastrectomy diet consisting of six small daily meals.
FJ feeds

Complications
Morbidity : 20% Mortality : 2-3%
Pulmonary complications Anastomotic and duodenal stump leaks Intraabdominal abscess Pancreatic fistula Vit B 12, Vit D, irona nd calcium
deficiencies

Post Gastrectomy syndromes: - Alkaline reflux gastritis - Dumping syndrome - Roux Stasis Syndrome - Afferent limb Syndrome

1 Right paracardial LNs, including those along the first branch of the ascending limb of the left gastric artery.
2 Left paracardial LNs including those along the esophagocardiac branch of the left subphrenic artery
3a Lesser curvature LNs along the branches of the left gastricvartery
3b Lesser curvature LNs along the 2nd branch and distal part of the right gastric artery

4sa Left greater curvature LNs along the short gastric arteries (perigastric area)
4sb Left greater curvature LNs along the left gastroepiploic artery (perigastric area)
4d Rt. greater curvature LNs along the 2nd branch and distal part of the right gastroepiploic artery

5 Suprapyloric LNs along the 1st branch and proximal part of the right gastric artery
6 Infrapyloric LNs along the first branch and proximal part of the right gastroepiploic artery down to the confluence of the right gastroepiploic vein and the anterior superior pancreatoduodenal vein
7 LNs along the trunk of left gastric artery between its root and the origin of its ascending branch

8a Anterosuperior LNs along the common hepatic artery
8p Posterior LNs along the common hepatic artery
9 Celiac artery LNs 10 Splenic hilar LNs including those
adjacent to the splenic artery distal to the pancreatic tail, and those on the roots of the short gastric arteries and those along the left gastroepiploic artery proximal to its 1st gastric branch

11p Proximal splenic artery LNs from its origin to halfway between its origin and the pancreatic tail end
11d Distal splenic artery LNs from halfway between its origin and
the pancreatic tail end to the end of the pancreatic tail 12a Hepatoduodenal ligament LNs along the proper hepatic
artery,in the caudal half between the confluence of the right and left hepatic ducts and the upper border of the pancreas
12b Hepatoduodenal ligament LNs along the bile duct, in the caudal half between the confluence of the right and left hepatic ducts and the upper border of the pancreas 12p Hepatoduodenal ligament LNs along the portal vein in the
caudal half between the confluence of the right and left hepatic ducts and the upper border of the pancreas

13 LNs on the posterior surface of the pancreatic head cranial to the duodenal papilla
14v LNs along the superior mesenteric vein 15 LNs along the middle colic vessels 16a1 Paraaortic LNs in the diaphragmatic aortic
hiatus 16a2 Paraaortic LNs between the upper margin of
the origin of the celiac artery and the lower border of the left renal vein
16b1 Paraaortic LNs between the lower border of the left renal vein and the upper border of the origin of the inferior mesenteric artery

16b2 Paraaortic LNs between the upper border of the origin of the inferior mesenteric artery and the aortic bifurcation
17 LNs on the anterior surface of the pancreatic head beneath the pancreatic sheath
18 LNs along the inferior border of the pancreatic body
19 Infradiaphragmatic LNs predominantly along the subphrenic artery
20 Paraesophageal LNs in the diaphragmatic esophageal hiatus

110 Paraesophageal LNs in the lower thorax
111 Supradiaphragmatic LNs separate from the esophagus
112 Posterior mediastinal LNs separate from the esophagus and the esophageal hiatus