d esensitization & c ortical remodeling : using a graded motor imagery approach to treat crps...
TRANSCRIPT

DESENSITIZATION & CORTICAL REMODELING: USING A GRADED MOTOR IMAGERY APPROACH TO TREAT CRPS
Elizabeth Gaffron, MOTR/L
RIC, Center for Pain Management
AAPM&R, 2015

I have no actual or potential conflict of interest in relation to this presentation.
LEARNING OBJECTIVES
Understand the motor/autonomic pain mechanism & rational for top-down treatment approach for CRPS.
Establish what assessments & clinical features may direct clinical rational to use Graded Motor Imagery (GMI) in the treatment of CRPS.
Why do we use pain physiology education to re-conceptualize pain experience in combination with GMI?
Define the components of graded motor imagery & establish it’s value in the treatment CRPS.

CRPS – MOTOR/AUTONOMIC PAIN MECHANISM
Inflammatory Mechanisms
Autonomic/vasomotor dysfunctions
Cortical, neuroplastic changes
Alterations in central & peripheral modes of pain reception
CRPS – TREATING A PROCESS, NOT ANATOMY
Maladaptive cortical reorganization reinforcing pain & symptoms
Limb positioned outside of visual field – protective guarding, neglect & disuse
Disturbance in perceived body part relative to shape, size, temperature, orientation, positional sense
“My arm doesn’t feel like my own”
Conflict between sensory-motor cortical processing networks
Lewis & McCabe, 2010; McCabe, 2011; Harden et al., 2013

TOP DOWN – BRAIN TO BODY
• Individuals with central deficits related to body image or movement beliefs require retraining of sensory & motor function in the primary somatomotor cortex
• Training the brain representation to promote body function
• Establish fear hierarchy relative to movement, contexts, & meaning
A World of Hurt, A Guide to Classifying Pain, 2015
TREATMENT PATHWAYS - ASSESSMENTS
- Bath CRPS Body Perception Disturbance Measure
- Proprioception: limb position sense
- Sensory: 2-point discrimination testing, localization & precision testing
- Left/Right discrimination testing: signs of cortical representation
- FAB-Q, TSK, PHODA: kinesiophobia, fear-avoidance, catastrophic thinking patterns
- Canadian Occupational Performance Measure: functional deficits

“ KNOW PAIN ”• Pain is a protective mechanism influenced by multiple factors
• Pain is an “OUTPUT” of the brain
• Use of metaphors may help to reframe unhelpful thoughts about pain experience
• Understanding basic pain physiology can diminish threat, improve compliance & progression of treatment, change movement performance, promote client’s active role in goal setting & problem-solving.

RE-CONCEPTUALIZE PAIN BELIEFS

NEUROTAGS – INTERCONNECTED NEURONS
Activation of neurotags produces an OUTPUT
When the neurotag network for pain is activated, it produces the pain experience
The Graded Motor Imagery Handbook, 2012
NEUROTAGS - INPUTS
Thoughts Movements Sensations Noises Memories Emotions Vision Balance Blood pressure Nerve
messages

NEUROTAGS –PERSISTENT PAIN, CRPS
Sensitization
- Increased excitability, more easily activated- Allodynia & Hyperalgesia
Disinhibition
- Loss of precision, activation of additional neurons- Pain spreads, moves, defies anatomical structures
The Graded Motor Imagery Handbook, 2012

TRAINING THE BRAIN REPRESENTATION TO PROMOTE BODY FUNCTION

RE-CONCEPTUALIZING PAIN – GRADED MOTOR IMAGERY (GMI)
GMI was developed as a treatment strategy to engage sensory & motor networks without triggering the protective pain response.
Desensitizing neurotags using graded brain exercise.
Graded Motor Imagery (GMI) is a graded exposure program grounded in three paradigms:
Biopsychosocial (Engle, 1977) Neuromatrix (Melzack, 1989) Pain Mechanisms (Gifford & Bulter, 1997)
Priganc &Strakla, 2011; Bowering et al., 2013; The Graded Motor Imagery Handbook, 2012
Left
/Rig
ht
Dis
crim
inati
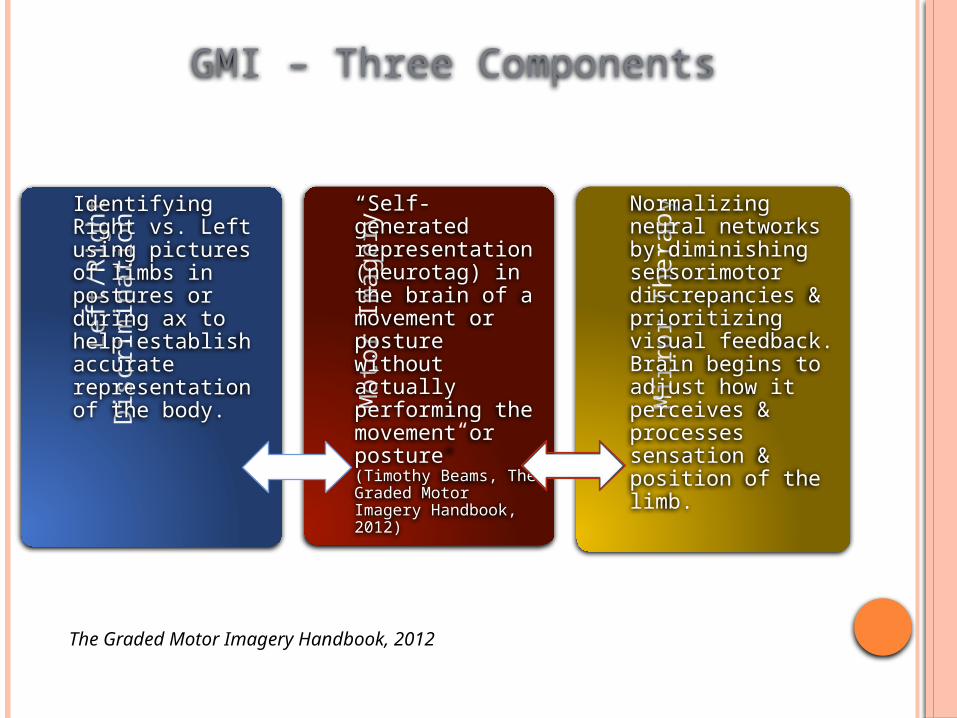
on Identifying Right vs.
Left using pictures of limbs in postures or during ax to help establish accurate representation of the body.
Moto
r Im
agery
“Self-generated representation (neurotag) in the brain of a movement or posture without actually performing the movement or posture” (Timothy Beams, The Graded Motor Imagery Handbook, 2012)
Mirr
or T
hera
py Normalizing neural networks by diminishing sensorimotor discrepancies & prioritizing visual feedback. Brain begins to adjust how it perceives & processes sensation & position of the limb.
GMI – Three Components
The Graded Motor Imagery Handbook, 2012

GMI – EVIDENCE
K. Jane Bowering, Neil E. O’Connell, Abby Tabor, Mark J. Catley, Hayley B. Leake, G. Lorimer Moseley, and Tasha R. Stanton (2013) The Effects of Graded Motor Imagery and Its Components on Chronic Pain: A Systematic Review and Meta-Analysis. J. of Pain 14(1):3-13.
Moseley,GL (2006) Graded motor imagery for pathologic pain – a randomised controlled trial. Neurology 67: 2129-34
Moseley,GL (2004) Graded motor imagery is effective for long-standing complex regional pain syndrome – a randomised controlled trial. Pain 108(1-2): 192-198

BRAIN TO PERIPHERY – GMI
Implicit motor imagery used for relearning cognitive & planning components of movements
Explicit motor imagery & mirror visual feedback are used to retrain the brain for basic motor skills by focusing on non-painful movements
Coordinated, controlled movements provide example for the brain to reset circuitry that modulates voluntary movement
Desensitizing neurotags by winding down the nervous system
Re-inhibiting neurotags for precision & definition
LEFT/RIGHT DISCRIMINATION TRAINING IMPLICIT MOTOR
IMAGERY
Pre-motor skill required for coordinated execution of movement
Unconscious mental movement
Less likely to activate the pain neurotag
Activation occurs in the premotor cortex – planning movement
Decreasing sensitization and normalizing inhibition
The Graded Motor Imagery Handbook, 2012

LEFT/RIGHT DISCRIMINATION TRAINING –WHAT’S MY BRAIN DOING?
Make a spontaneous judgment - dependent on the processing speed of CNS & attention to body part
Mentally move our own matching limb to mimic the posture of the limb- requires an intact working body schema & it’s integration of premotor processes
Confirm or deny the initial judgment –dependent on the processing speed of the CNS
Moseley, 2004; Moseley & Flor, 2012

MOTOR IMAGERY – EXPLICIT MOTOR IMAGERY
Observing or imagining movements by creating the sense of doing the activity or position without movement of the body
Provides insight into the function of motor planning pathways
Increase likelihood of activating pain neurotag
Activation in the pre- & primary motor cortex – execution of movement
McCabe, 2011; The Graded Motor Imagery Handbook, 2012
EXPLICIT MOTOR IMAGERY – WHAT’S MY BRAIN DOING?
Activation of primary motor cortex cells, which may activate the neurotags for movement
Initiates the neural hardware for both movement & sensation
The Graded Motor Imagery Handbook, 2012

MIRROR VISUAL FEEDBACK
Restoring a pain-free relationship between sensory feedback & motor intention.
Corrective visual representation of the affected limb may help to normalize the body schema.
Increase attention of affected limb, improving ownership and emotional attachment to the limb.
Activation of “movement areas” of the brain – more likely to activate neurotag.
The Graded Motor Imagery Handbook, 2012; McCabe, 2011; Lewis & McCabe, 2010
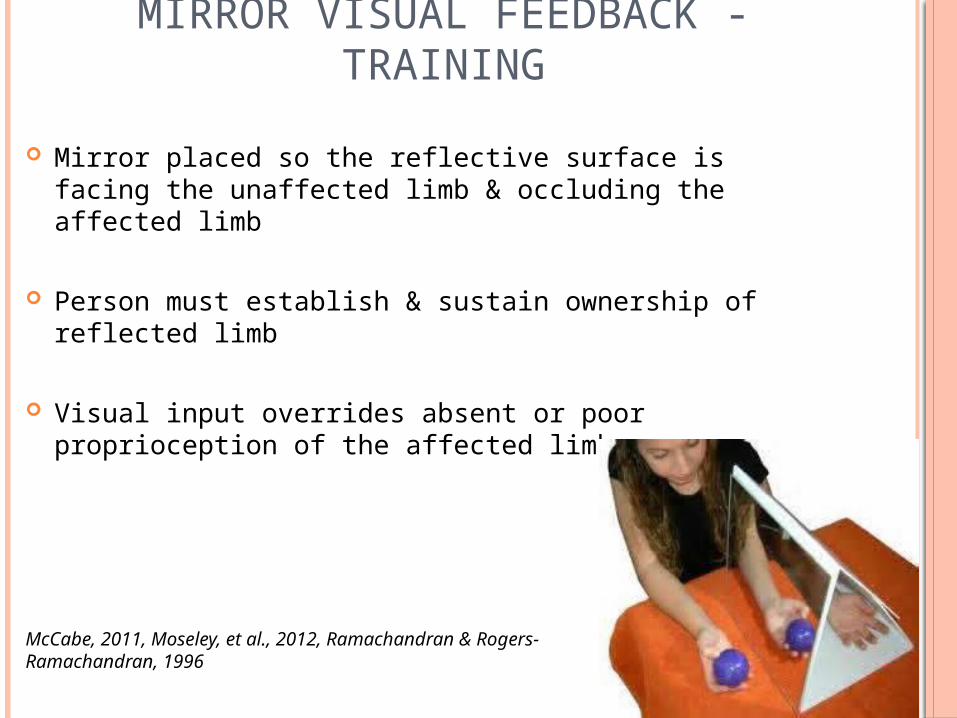
MIRROR VISUAL FEEDBACK - TRAINING
Mirror placed so the reflective surface is facing the unaffected limb & occluding the affected limb
Person must establish & sustain ownership of reflected limb
Visual input overrides absent or poor proprioception of the affected limb
McCabe, 2011, Moseley, et al., 2012, Ramachandran & Rogers-Ramachandran, 1996

MIRROR VISUAL FEEDBACK - CONTRAINDICATIONS
Reports of increased pain
Motor extinction
Exacerbation of movement disorders – tremor or dystonia
Inability to establish and sustain ownership of reflected limb
Lewis & McCabe, 2010; McCabe, 2011; Harden et al., 2013

“ You move more easily, function better and your brain has less need to make pain when you know what is going on with your body.”
(David Butler, The Graded Motor Imagery Handbook, 2012)

REFERENCES Harden, NR, Oaklander, AL, Burton, AW, Perez, RSGM, Richardson, K, Sawn,
M,Barthel et al. Complex regional pain syndrome: Practical diagnostic and treatment guidelines, 4th edition. Pain Medicine 2013; 14: 180-229
Kolski, MC & O’Connor, A. A world of hurt, a guide to classifying pain. St. Louis, MO: Thomas Land Publishing, 2015
Lewis, J & McCabe, C. Body perception disturbance in CRPS (BPD). Practical Pain Management, 2010; 60-66
Louw, A, Puentedura, E, & Mintken, P. Use of an abbreviated neuroscience education approach in the treatment of chronic low back pain: A case report. Physiotherapy Theory & Practice, 2011; 00(0): 1-13
McCabe, C. Mirror visual feedback therapy. A practical approach. Journal of Hand Therapy, 2011; April-June; 170-179
Moseley, GL. Unraveling the barriers to reconceptualization of the problem in chronic pain: The actual and perceived ability of patients & healthcare professionals to understand neurophysiology. Journal of Pain, 2003 (C) 4: 184-189
Moseley, GL, Nicholas, MK, & Hodges, PW. A randomized controlled trial of intensive neurophysiology education in chronic low back pain. Clinical Journal of Pain, 2004; 324-330
Moseley, GL. Why do people with CRPS take longer to recognize their affected hand? Neurology, 2004; 62:2182-2186

REFERENCES Moseley, GL, Butler, DS, Beams, TB, & Giles, TJ. The graded motor imagery
handbook. Adelaide: NOIgroup Publishing, 2012. Moseley, GL & Flor, H. Targeting Cortical Representations in the treatment of
chronic pain: A review. Neurorehabilitation & Neural Repair, 2012;1-7 Prignac VW& Stralka, SW. Graded motor imagery. Journal of Hand Therapy,24:
164-168