cytopenias - national university hospital · - fever - chills - rigors - hypotensive ... no...
TRANSCRIPT
Cytopenias The what, why and how
Dr Esther Chan
Associate Consultant
Haematology
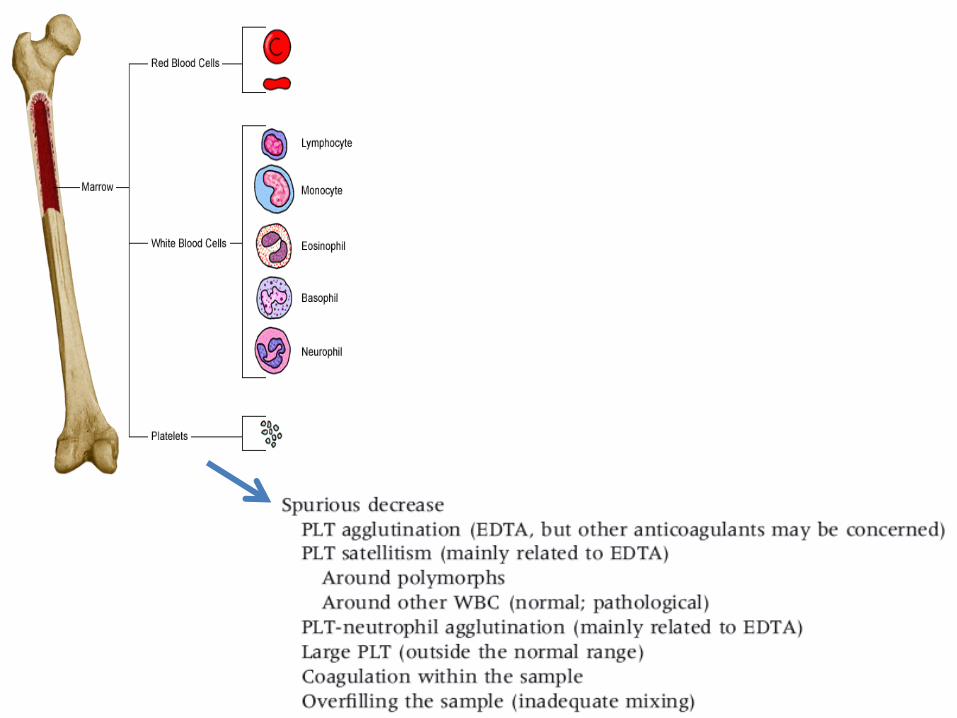
3 main cell lines
• RBC/Haemoglobin
• White cell counts
• Platelets

The WHAT

Anaemia

Leucopenia
• The only clinically relevant parameter is neutropenia
• Risk is of severe infection and this correlates to absolute neutrophil count
• ANC
– <1-0.5: Significantly increased risk of infection
– <0.5: Highest risk of infection

Thrombocytopenia
• Generally not clinically significant if >100K
• Concern of bleeding increases once Plt<30k
Summary: The What
• Drop fm pt’s baseline
• Neutrophils <1
• Platelets <100 (<30)
The WHY

How is the FBC measured?
• Haematology Analysers
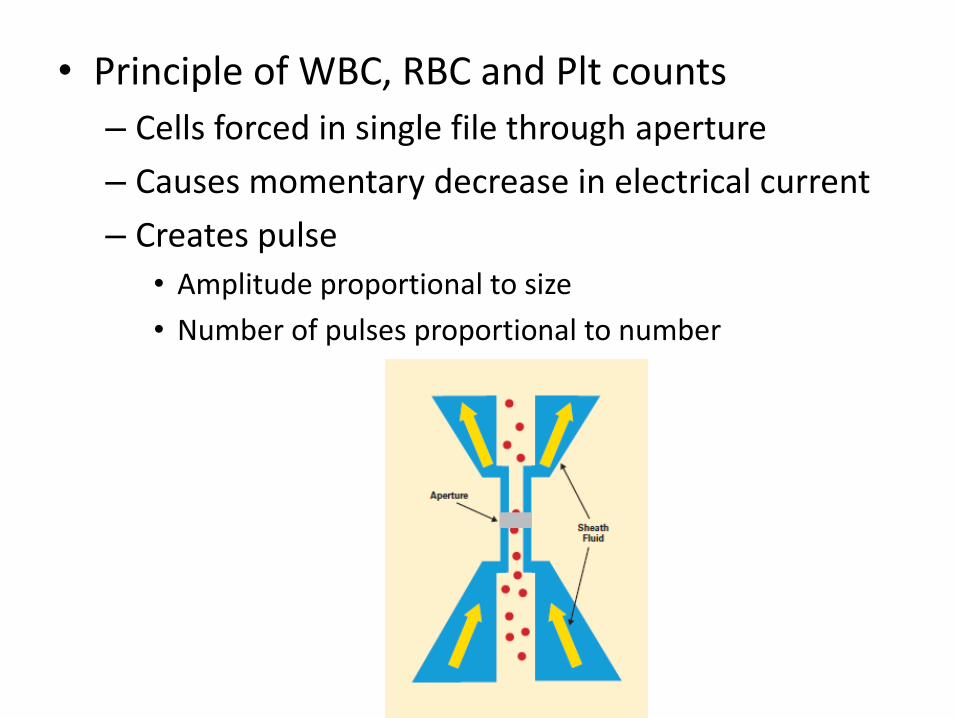
• Principle of WBC, RBC and Plt counts
– Cells forced in single file through aperture
– Causes momentary decrease in electrical current
– Creates pulse
• Amplitude proportional to size
• Number of pulses proportional to number

• Note that most modern machines combine laser, impedance, radiofrequency, direct current, peroxidase staining to optimize sensitivity
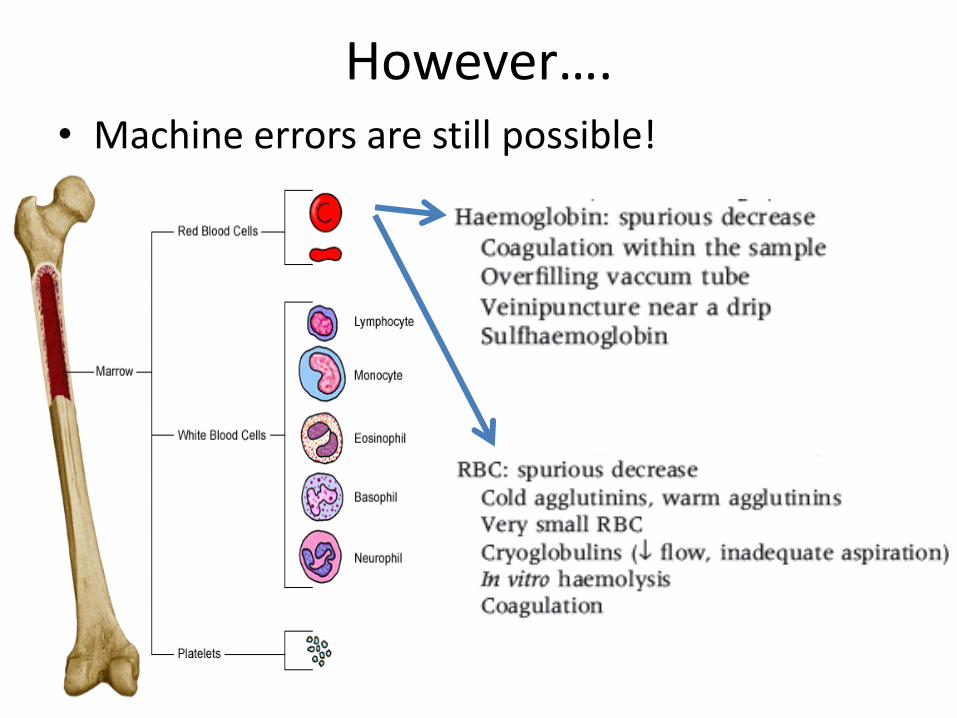
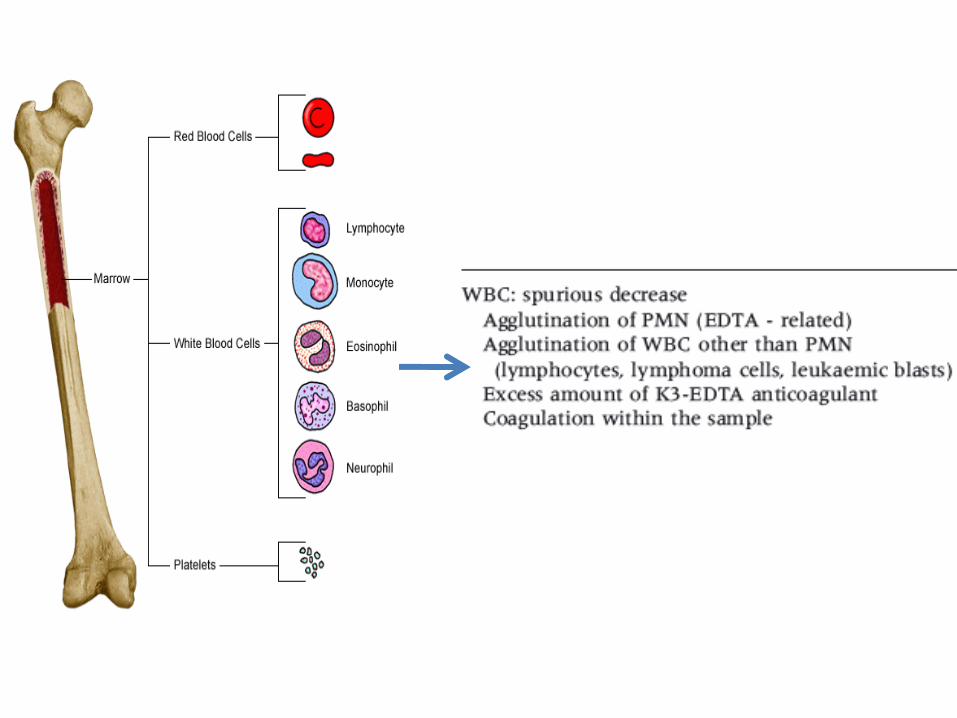
However…. • Machine errors are still possible!

The WHY - Lesson 1
• Exclude spurious low counts!
Important Approach
• Concept of
– Production issues
• Empty
• Packed
• Faulty
– Peripheral consumption/
destruction

‘Empty’
• Aplastic anemia/ Marrow hypoplasia
Causes: -idiopathic causes, - viral infections, - drug related causes, (Chemotherapy) -RT etc.
‘Packed’
• By marrow infiltration with abnormal cells
– hematological malignancies ie leukemias
– non hematological malignancies (metastasis)
• By marrow fibrosis
– Myelofibrosis

Myelodysplastic Syndrome
• Defined as acquired bone marrow disorder
• Characterised by ineffective haematopoiesis
• Proliferation of abnormal clone of cells. which replaces normal haematopoietic cells.
• Clinical manifestation of BM failure as well as tendency to transform into acute leukaemic phase
• May be primary or secondary to other causes eg. chemotherapy, radiotherapy or environmental toxins.
‘Faulty’

Peripheral destruction/consumption
• Infections
– Dengue
• Autoimmune
– SLE
• Hypersplenism
– Cirrhosis with splenomegaly
The WHY - Lesson 2
• For approach to cytopenias
– Is it
• Production problem?
• Destruction problem?
– Narrows down differentials

The HOW

On seeing cytopenias on the FBC…
• Do not interpret an FBC by itself!
1. Need for guidance from clinical history & physical examination
2. Need to take cues from the FBC/PBF


Clinical History
• Symptoms/ Signs:
- Fever - Chills - Rigors - Hypotensive - Toxic
- Malar rash - Arthritis
- Alcohol history Hypersplenism as cause of cytopenias - Splenomegaly
Sepsis as cause of cytopenia
Possible SLE with concomittant cytopenias

Signs/Symptoms
Systemic Symptoms - LOA - LOW - Fever
Clinical Signs - HEPATOMEGALY - SPLENOMEGALY - LN SWELLING - PALLOR
Possible Haematological Malignancy
• Leukaemia • Lymphoma

Cues on the FBC/PBF
• ‘Empty’ Marrow
– Pancytopenia
– No abnormal cells on the PBF
– No early white/red cells

• ‘Packed’ Marrow – Leucoerythroblastic picture
• Early RBC/WBC in the peripheral blood
• Tear drop cells
– Blasts
– Abnormal lymphoid cells
– Rouleux

• ‘Faulty’ marrow
– Dysplastic features
• RBC: Anisopoikilocytosis, Basophilic stippling
• WBC: Hypo/Hyper-granulated forms
• Plt: Plt anisocytosis, Hypogranular forms

Other factors
• Other cell lines
– Monocytopenia? Bicytopenia? Pancytopenia
• Differential Counts

Real life examples
• Case 1
• Describe the FBC
• What else would you want to know?
• What are the differentials?

Don’t forget!

• Clinical History
– Bruising
– Loss of weight
– Tired
– Fever
• Physical Examination
– Lymph nodes palpable

Initial Impression
• Leuocytosis with reduced Hb/ plts
• Associated with systemic symptoms.
Differentials:
- Sepsis (Viral)?
- Hematologic malignancy?

Other Factors:

• Final diagnosis
– Acute leukaemia
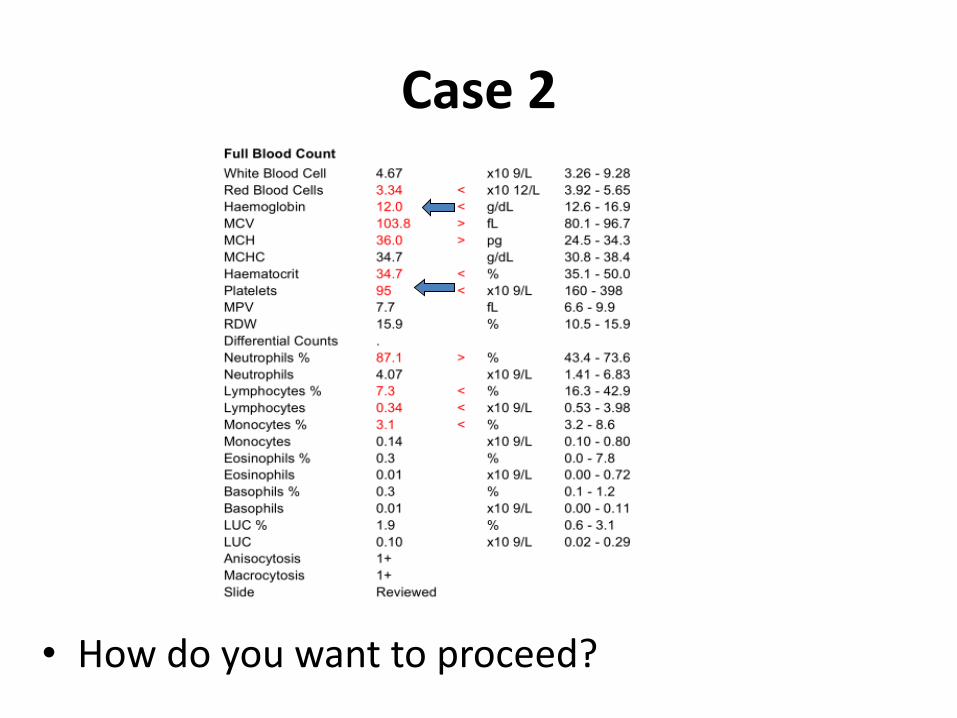
Case 2
• How do you want to proceed?

• Clinical History
– 50 year old man
– Loss of appetite and some loss of weight.
– No bleeding complications.
– Noted increased lethargy at home.
– Admitted when noted Hb low and thrombocytopenia.
– NO hypothyroidism symptoms.
– NO history of liver disease
– NO special drug use
– PE: NO hepatosplenomegaly

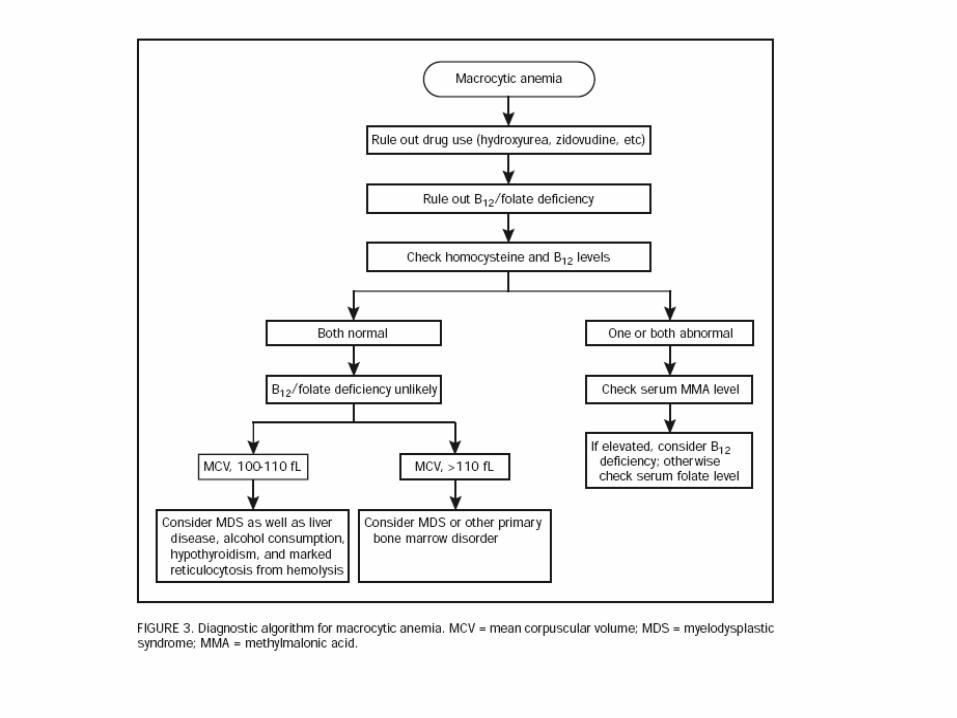
Other factors
• PBF findings
– Hyposegmented Neutrophils seen

• Diagnosis
– Myelodysplastic syndrome

Case 3
• Any thoughts?

• Clinical history
– 50yr Female
– Elective admission for Total knee replacement
– Incidental finding
• What to do next?
– Cancel operation?
– Bone Marrow Aspiration?

• Other factors
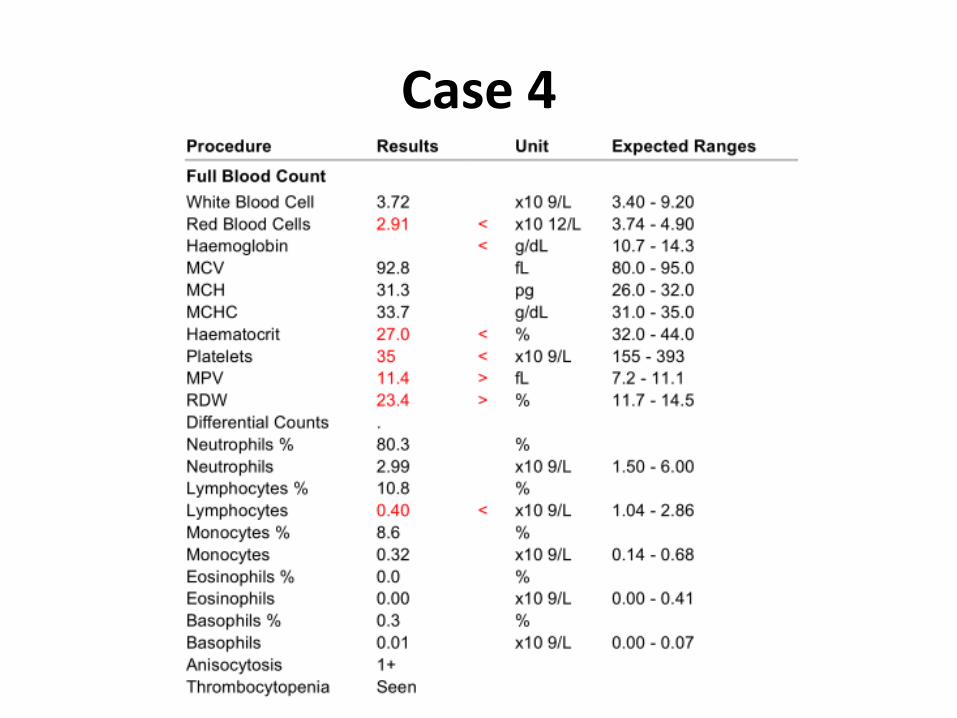
Case 4
• Clinical History
– 30yr Female
– Brought to A&E by family
– Fever for 3 days
– Drowsiness, unable to rouse from bed for 1 day

• Diagnosis
– Thrombotic Thrombocytopenic Purpura


Case 5
• History
– 60yr Male
– Well with no complaints
– FBC done as part of health screening by his company
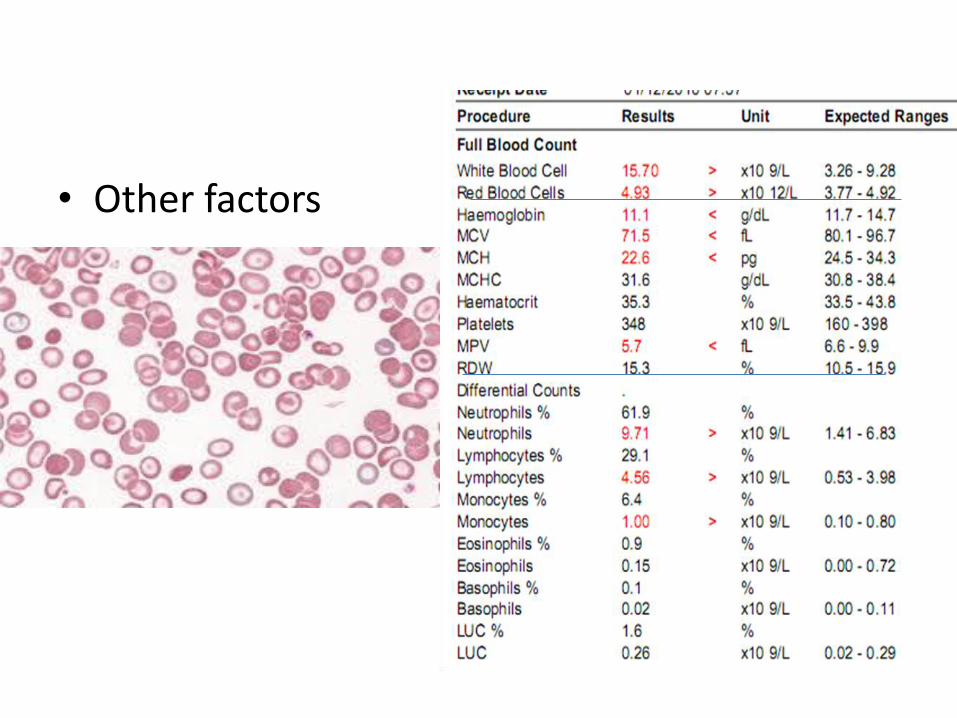
• Other factors


Classification of anemia – MCV and reticulocyte count
Microcytic
MCV
Normocytic Macrocytic
Low retics:
Iron Deficiency anemia
Sideroblastic Anemia
Normal/high retics:
Thalassemias
Low retics
Normal WBC/Platelets:
• AOCD
• Early IDA
• Renal failure
• Pure red cell aplasia
Pancytopenia
• Primary failure: AA
• Secondary failure: chemo/RT, MDS
Low retics:
Megaloblastic anemias
Non-megaloblastic:
• Liver disease
• Alcohol
• Hypothyroidism
• Drugs
• MDS
High retics:
Reticulocytosis

Summary – The HOW
• Correlate FBC with
– pt ‘s clinical picture
– & other factors (PBF/Differential counts)
• To evaluate and manage all cytopenias safely
