cytologia ecoendoscopica tracto esofago-gastro-intestinal · cytologia ecoendoscopica tracto...
TRANSCRIPT

Cytologia Ecoendoscopica Tracto Esofago-Gastro-Intestinal
Ricardo H. Bardales, MD
Outpatient Pathology Associates &
University of Minnesota


Indications for EUS-FNA
Imaging +/- sampling of any process not
adequately imaged or sampled by more
standard techniques, if it is seated in:
Mediastinum
Upper abdomen
Retroperitoneum
Pelvis

EUS-FNA Technique
Endoscopy: visualization of the gut surface.
Ecography: characterization of the GI wall, adjacent lymph nodes, pancreas, liver, spleen, and left adrenal gland.
FNA: sampling of lesions in various locations.
More cost effective than other modalities.
Higher sensitivity than CT.

EUS-FNA TECHNIQUE

EUS-FNA Lesion Sampling
Real time: there is no delay in the “eco”
transmission, capture, and conversion into
image by the computer.
Needle gauge: 19-25.
The thinner the better
Blood is the worse enemy
Cytology, cell block, and ancillary tests.

Sample collection and
processing
Material sprayed onto
a labeled slide
Air-dried for DQ
EtOH-fixed
Remaining material let
to clot for CB
Further sampling and
triage as needed

PAAF por Ecoendoscopia - Historia

En Donde Esta la Lesion? (1)
LESION LOCALIZACION FRECUENTE
GIST Estomago, intestino delgado
Neoplasias de musculo liso Esofago, estomago
Ca de celulas en anillo sello (difuso) Estomago, esofago
Gastroenteritis eosinofilica Intestino delgado, estomago
Quistes congenitos Esofago, estomago
Pancreas heterotopico Duodeno, estomago
Tumor celulas granulares & Schwanoma Esofago, estomago
Tumores endocrinos Recto, estomago, intestino delgado
Tumor glomus Estomago
Heterotopia - glandulas de Brunner Estomago
Hamartoma – glandulas de Brunner Duodenum
Linfoma Estomago, intestino delgado

En Donde Esta la Lesion? (2)
CAPA DE ORIGEN
Zona de Transicion

PAAF por Ecoendoscopia - Abordaje
Comenzar con aguja 25 g. Bloque celular with 19 g.

EE-PAAF y Patrones Citologicos
Masas Solidas (usualmente hipoecoicas)
Patron fusocelular
Patron epitelioide
Lesiones Quisticas (anecoicas)
Patron quistico
Pliegues Gastricos Engrosados

El Patron Fusocelular

GIST: Aspectos Generales
Fenotipo: celula intersticial de Cajal
Edad media: 60 a. Ligera predominancia mascul
Raro en ninos y neonatos
Localizacion:
Gastrica (65%), intestino delgado (25%),
esofago, recto, mesenterio, omento (10%).
EE: hipoecoico, adherido a la muscular propria
Conducta impredecible
Gastrico: 10% a 30% malignos
Otros: 50% malignos (omento, higado, peritoneo) Kirsch R. et al. Adv Anat Pathol 2007;14:261.

Fasciculos o remolinos cortos
GIST – Fusocelular (70%)

GIST – Fusocelular
Celulas uniformes – bordes indistintos – Fondo fibrilar

GIST – Fusocelular
Empalizada nuclear ~ Schwannoma

Nucleos – alargados, ovoides, hiperchromasia.
Vacuolas yuxtanucleares – GIST gastrico
GIST – Fusocelular

GIST - Inmunofenotipo
c-kit/CD117 membranoso
CD34

Leiomioma
Comun: esofago – Paucicelulares
Citoplasma eosinofilico - Nucleos blandos - raras mitosis
Stelow EB et al. A, J Clin Pathol 2003;119:703.

Leiomioma versus Normal

Leiomioma versus GIST

LEIOMIOMA GIST

GIST versus Leiomioma
GIST Leiomioma
Organo >estomago >esofago
Celularidad Mayor Menor
Ocasionales
celulas sueltas
Likely Unlikely
Ocasionales
nucleos sueltos
Probable Improbable
Atipia - mitosis Puede estar presente Ausente
Epithelioid cells Pueden estar presentes Ausente
Bloque cel - IHC Basofilico – CD117+ Eosinofilico – Actina+
Stelow EB et al. A, J Clin Pathol 2003;119:703.

Schwannoma
Mas comun: estomago, muscularis propria - Hipoecoico
Benigno. Puede ser grande y con mitosis (<5/HPF) Stelow EB et al. Diagn Cytopathol 2004;30:172. Miettinen M et al. Am J Surg Pathol 2001;25:846.

Schwannoma
Fusocelular/Epitelioide: 3/1 – Empalizada nuclear vaga – Carece
de cuerpos de Verrocay – linfocitos – Semeja al GIST

Duodenal LG-NET (21 x 18 mm)

Duodenal LG-NET (21 x 18 mm)
Synaptophysin

Spindle Cell Tumors of the Gut GIST Smooth
Muscle
Tumors
Schwannoma SFT Mesenteric
Fibromatosis
Neuroendocr
ine Tumor
c-kit/
CD117
+ diffuse
membran
- - - Variable weak
(Ab-depend)
-
CD34 + diffuse
(70%)
+ (10%) Rare focal + - -
SMA Variable
focal
+ - Variable focal
-
S-100
protein
+ (5%)
- + - -
Chromo
Synapto
- - - - - +
beta-
catenin
- + nuclear -
Yamaguchi U, et al. Virchows Archiv. 2004;445:142.
Montgomery E, et al. Am J Surg Pathol 2002;26:1296.
Abraham SC. Adv Anat Pathol 2007;14:178.
Fletcher CDM, et al. Hum Pathol 2002;33:459.
Greenson JK. Mod Pathol 2003;16:366.
Stelow EB, et al. Am J Clin Pathol 2008;129:219

Tumores Fusocelulares Raros? Tumor fibroso calcificante del estomago
(Agaimy AM et al. Am J Surg Pathol 2010;34:271)
Colageno estoriforme + Calcio + celulas inflamatorias
Cavidad abdominal y tejidos blandos
CD117, SMA, S100, h-caldesmon, PDGFRA (-)
Puede mostrar focal CD34+
Fibromixoma plexiforme
(Miettinen M et al. Am J Surg Pathol 2009;33:1624)
Todos en el antro gastrico
Elementos fibromixoides
Actina muscular (+), variable CD10
CD117, DOG1, CD34, desmin, proteina S100 (-)
MFH primario y metastatico
(Agaimy A et al. Virchows Arch 2007;451:949)
Actina and PDGFRA (+); CD117, CD34, S100 (-)

GIST del Colon (n=37)
Fusocelular/Epitelioide: 9/1. Edad promedio 67 a.
CD117(+) 76%; CD34(+) 59%. mutacion c-kit 36%
Diagnostico tardio: tipicamente transmural
4 casos: ≤1 cm – hallazgo incidental – no recurrencia
10 casos: ≥1 cm & mitosis ≤5/50 HPF – muerte 20%
23 casos: ≥1 cm & mitosis ≥5/50 HPF – muerte ~ 100%
Leiomiosarcomas (n=7): CD117(-), CD34(-), SMA(+), desmin (+), no mutacion gen c-kit .
GIST del colon mitoticamente activo (>5/50) parece ser mas letal que el leiomiosarcoma con similar
actividad mitotica. Miettinen M et al. Am J Surg Pathol 2000;24:1339

Leiomiosarcoma
SMA

GIST – Riesgo de Conducta Agresiva – Consenso*
Tamano (cm) Mitosis por 50 HPF
Riesgo muy bajo <2 <5
Riesgo bajo 2-5 <5
Riego intermedio <5
5-10
6-10
<5
Riesgo alto >5
>10
Cualquier tamano
>5
Cualquier cuenta mitotica
>10
* NIH – Abril 2001 Fletcher CDM, et al. Hum Pathol 2002;33:459. Blay J-Y, et al. Ann Oncol 2005;16:566.

GIST: Predictores de Malignidad
Tamano Proliferacion celular [Cuenta mitotica
Indices (Ki-67 >10%), p53]
*p16, *ezrin, apoptosis baja, telomerasa alta, marcadores de angiogenesis (MVD,
*VEGF)
Localizacion La gran mayoria de GISTs de riesgo muy bajo, bajo, e
intermedio se comportan de manera benigna.
Existe un subgrupo (~10%) que se comporta agresivamente. Corless CL. AJCP 2004;122:11. Wei Y-C, et al. Mod Pathol 2009;22:1351.
Fletcher CDM, et al. Hum Pathol 2002;33:459. Steigen SE at al. Mod Pathol 2008;21:46. Wang Q et al. World J Gastroenterol 2007;13:2626. McAuliffe JCA et al. Clin Cancer Res 2007;13:6727.

Mercado de Pisac – Cerca a Cuzco - Peru

Patron Epitelioide de Celulas Grandes

Anisocitosis y anisonucleosis
Raras mitosis
GIST – Epitelioide (20%)

GIST - Epitelioide
Nucleos uniformes ovoides a redondos – cromatina vesicular

Celulas redondas – citoplasma variable eosinofilico o claro
GIST – Epitelioide

GIST - Epitelioide
c-kit/CD117

Inmunomarcadores del GIST
CD117, CD34
*CD171 (L1): molecula de adhesion celular
*DOG1: proteina de funcion desconocida
*Expresados independientemente de c-kit or PDGFRA y
Son utiles en el diagnostico de CD117(-) GISTs
Rosai, J. Int J Surg Pathol 2010 (supl) 18;79S-87S Lee C-H et al. Adv Anat Pathol 2010;17:222

Tumor de Celulas Granulares
Mas comun: esofago distal, submucosa – Mayormente
benigno - EE: hipoecoico Stelow EB et al. Diagn Cytopathol 2004;30:172.

Tumor de Celulas Granulares
PAS(+), S100 protein(+), CD117(-), CD34(-), actina(-)

TUMOR de CELULAS
GRANULARES CELULAS PARIETALES

Pancreas Heterotopico
Estomago & duodeno
Esofago: t18, t13
Endoscopia: nodulo umbilicado
EE-PAAF: rara aspiracion
Celulas ductales y acinares
Quistico: celulas ductales (adenomioma) citodiagnostico es dificil
Rodriguez FJ et al. Diagn Cytopathol 2004;31:175

Linfomas del Tracto GI
Primarios: raros
Estomago:
H=M. Tercera edad
Bx forceps: no es Dx.
PAAF-EE: 25 g
Examenes especiales
DLBL = PAAF-EE Dx
EMZL = Biopsia
Kolve ME et al. Recent Results Cancer Res 2000;156:63.
Janssen J. Best Pract Res Clin Gastroenterol 2009;23:671.
Hiper o hipoecoico
Engrosamiento de capas 3, 4 o ambas
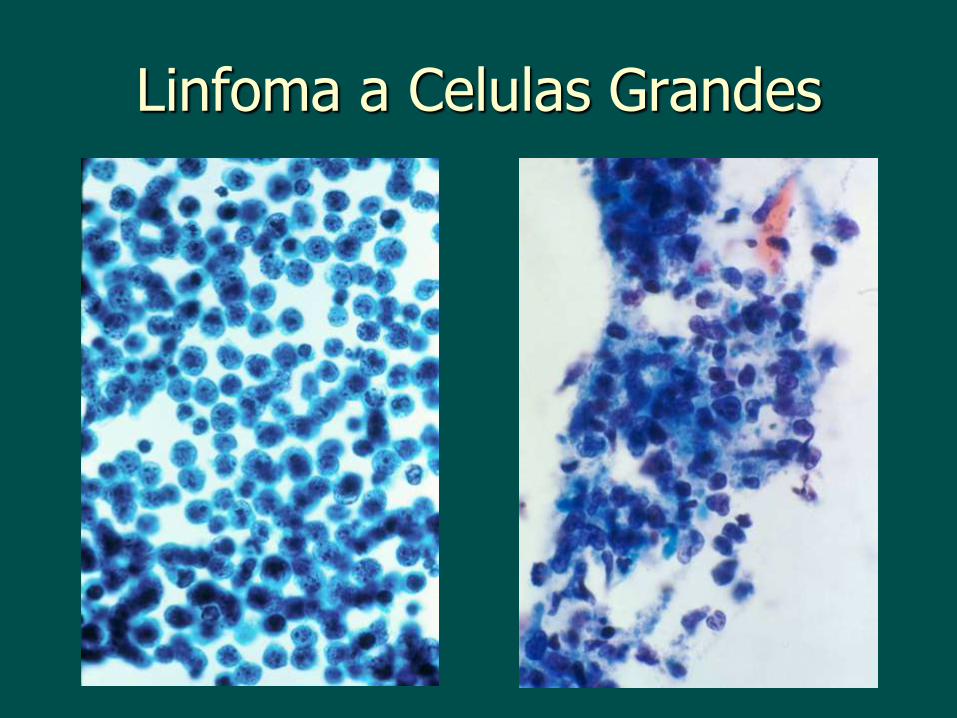
Linfoma a Celulas Grandes

Cancer Gastric Difuso (CGD)
Incidencia mundial de CG es menor. CGD esta aumentando
La expression de E-cadherina es el principal discriminador entre GCI y CGD.
CDH1 codifica E-cadherin, una glicoproteina transmembrane, critica para la adhesion intercelular.
La mayoria del CGD esporadico y hereditario no expresan E-cadherina
Perdida de E-cadherin = invasividad = metastasis
CGDH tiene mutaciones en el genCDH1
Autosomico dominante. Pacientes jovenes. Gastrectomia profilactica

Tumores No-primarios
LOBULAR CA RCC
MELANOMA AMMoL

Tumores Epitelioides Raros?
PEComa (benigno y maligno)
Estomago, duodeno, colon
Celulas epitelioides eosinofilicas
HMB45+, Actina+, desmin+, vimentin+, Melan A variable
Proteina S100 (-)
Puede ocurrir en pacientes con esclerosis tuberosa
Sarcoma sinovial
Esofago, estomago, duodeno
Monofasico o bifasico (epitelioide & fusocelular)
Epitelioide: CK+, EMA-. Fusocelular: Vimentina+, CD10+.
Ambos: CD117-, CD34-, S100-, Actina muscular-, Desmina-
Citogenetica: translocacion X;18.
Mitteldorf CA et al. World J Gastroenterol 2010;16:522. Makhlouf HR et al. Am J Surg Pathol 2008;32:275.

PEComa

Patron Epitelioide a Celulas Grandes
GIST Linfoma Carcinoma Tumor Celulas
Granular
Melanoma
Citologia Componente fusocelular
variable
Disociacion celular
Agregados & celulas sueltas
Citoplasma granular
Pleomorfico
CD117 + - - - +
CD34 + - - - -
CD45 - + - - -
Keratin - - + - -
Proteina S100
- - - + +
HMB45 - - - - +

Macchu Picchu – Cuzco - Peru

Patron Epitelioide a Celulas Pequenas

Tumores Endocrinos GI
Submucosos
Comunes en el intestino distal
Somatostatinomas, gastrinomas, carcinoide
Hipoecoicos

Gastrinoma
Rosetas – celulas redondas/ovales – plasmacitoides,
cromatina “sal y pimienta” – nucleolos inconspicuos

GI LG-NETs: Location
Ileum 31%
Rectum 21%
Appendix 18%
Colon 12%
Stomach 6%
Duodenum 4%
Jejunum 3%
Turaga KK and Kvols LK. CA Cancer J Clin 2011:61:113-132.

Recommendations WHO based on ENETS
Endocrine and neuroendocrine terms can be used interchangeably
All WD-NENs be termed NETs (Ns = Ts)
The term NECa is reserved to poorly differentiated neoplasms (HG small and large cell NE neoplasms)

Nomenclature for GI-NETs (WHO,ENETS)
LOW GRADE Neuroendocrine tumor grade 1 (G1)
INTERMEDIATE GRADE
Neuroendocrine tumor grade 2 (G2)
HIGH GRADE Neuroendocrine carcinoma grade 3 (G3)
GI-NETs, gastrointestinal neuroendocrine tumors; WHO, World Health Organization; ENETS, European Neuroendocrine Tumor Society
Kilmstra DS. Semin Oncol 2013; 40:23-36.

GI-NETs Grading System (WHO,ENETS)
LOW <2 mitoses/10 hpf, AND Ki67 index <3%
INTERMEDIATE 2-20 mitoses/10hpf, OR Ki67 index 3%-20%
HIGH >20 mitoses/hpf OR Ki67 index >20%
WD
PD
WD, well-differentiated; PD, poorly-differentiated; GI-NETs gastrointestinal neuroendocrine tumors; WHO, World Health Organization; ENETS, European Neuroendocrine Tumor Society
Kilmstra DS. Semin Oncol 2013; 40:23-36.

Antro gastrico
Tercera edad
Benigno, solitario
Celulas de musculo liso modificadas del cuerpo glomico
Debol SM et al. Diagn Cytopathol 2003;28:316.
Gu M et al. Diagn Cytopathol 2002;46:560.
Vinette-Leduc D et al. Diagn Cytopathol 2001;24:340.
Tumor Glomus

Tumor Glomus
Celulas pequenas, nucleo uniforme, no mitosis

Tumor Glomus
IHQ: SMA (+), Desmina (-), vimentina (+), keratina (-)

Linfoma MALT
Reactivo

Patron Epitelioide a Celulas
Pequenas TUMOR
ENDOCRINO
GIST
EPITELIOIDE
TUMOR
GLOMUS
LINFOMA
Agregados y celulas
sueltas (usualmente
pequenas). Rosetas.
Moderado
citoplasma.
Cromatina
sal/pimienta
Agregados y
celulas sueltas
(usualmente
grandes).
Cromatina
gruesa. Cytopl
abundante.
Agregados y
celulas sueltas
(usualmente
pequenas).
Nucleos
homogeneos e
hipercromaticos.
Predominan
celulas sueltas
irregulares
monomorphic
(usualmente
grandes).
Cromogranina (+)
Sinaptofisina (+)
NSE (+). Keratin (+)
CD117 (+)
CD34 (+)
CD117(-). Actina
(+), Calponina
(+), H-
caldesmon (+),
Vimentina (+)
Marcadores de
celulas B & T
Debol SM et al. Diagn Cytopathol 2003;28:316. Miettinen M et al. Am J Surg Pathol 2002;26:301.

El Patron Quistico

Quistes/Duplicaciones Congenitos
Ectopia del intestino anterior o posterior
EE: anecoico
Esofagico: tercio distal, intramural o extrinsico
Gastrico: curvatura mayor > menor, piloro
Ponder TB et al. Acta Cytol 2001;47:201.
Van Dam J et al. Am J Gastroenterol 1992;87:762.
Eloubeidi MA et al. Cancer 2004;102:253.

Quiste por Duplicacion del Intestino
Anterior
Raro – Semeja neoplasia – A menudo asintomatico
Epitelio: escamoso, ciliado, columnar
Distincion del quiste bronquial puede ser dificil
Imagen: a lo largo del arbol TB posterior a la carina.
Histologia: pared con doble capa de musculo liso. Sato MA et al. J Clin Ultrasound 2007
Wang B et al. Acta Cytol 2009;53:219

Pliegues Gastricos Gruesos
Diagnostico Diferencial:
Malignidad: Linitis plastica, linfoma zona marginal
Granulomatosos: Crohn’s, sarcoidosis, sifilis
Hiperplasia epithelial: gastropatias (Menetrier, Zollinger-Ellison)
Gastroenteritis eosinofilica

Linitis Plastica
EE: engrosamiento de la capa 3 y a menudo capa 4
Estomago (comun), recto, esofago distal
Primario o metastatico (mama, prostata, vejiga)
Compromiso locoregional frecuente:
EE mejor que CT
EE paracentesis
Gleeson FC et al. Gastrointest Endosc 2008;68:591.
Carter JE et al. Acta Cytol 2008;52:725.
DeWitt J et al. Clin Gastroenterol Hepatol 2007;5:609.

Linitis Plastica
Hipocelular, pequenos grupos – celulas en anillo de sello
Sobrevida: pobre - Cirugia: raramente curativa

Carcinomatosis Peritoneal en
Linitis Plastica Gastrica Lavado peritoneal al momento de la
laparotomia.
47 pacientes: candidatos para una reseccion curativa.
Carcinomatosis peritoneal Diagnostico citologico
Diagnostico molecular: quantificacion del CEA mRNA por RT-PCR
Curso clinico: carcinomatosis peritoneal en la laparotomia o seguimiento clinico.
RT-PCR muestra compromiso de la cavidad abdominal en ~80% pacientes.
Los resultados explican poque la cirugia es raramente curativa en pacientes con linitis plastica gastrica
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Peritoneal
involvement
Cytology
CEAmRNA
Clinicalcourse
Kodera Y et al. Jap J Clin Oncol 2004;34:525.
20
39 36

EE-PAAF versus Biopsia Forceps
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Diagnostic Accuracy
Forceps Biopsy
EUS-FNA
Masas Intramurales del Tracto GI Lesions
Vander Noot MR et al. Cancer 2004;102:157.
Polkowski M et al. Gastrointest Clin N Am 2005;15:33.
Hoda KM et al. Gastrointest Endosc 2009;69:1218.
60%
89%

Cytologia Ecoendoscopica Mediastino y Estadiaje Tumoral
Ricardo H. Bardales, MD
Outpatient Pathology Associates &
University of Minnesota


LN EUS-FNA: Sample Triage
SAMPLE NON-DIAGNOSTIC DIAGNOSTIC
INFECTIOUS LYMPHOID NON LYMPHOID
CULTURES
c/w KNOWN 1
STOP
NOT c/w KNOWN 1
UNKNOWN 1
CELL BLOCK
FOR IHC
FLOW CYTOMETRY
CYTOGENETICS
OTHER Stelow EB et al. Diagn Cytopathol 2004;30:301.

EUS-FNA & Mediastinal
Adenopathy of Unknown Etiology
Common isolated mediastinal abnormalities: Benign: sarcoid, TB, histoplasmosis Malignant: metastatic cancer, lymphoma
EUS-FNA is safe, accurate, and the most cost effective non surgical technique. Alters the w/u & therapy in 75% of patients
Mediastinoscopy and transtracheal biopsy Better access to the upper and anterior
mediastinum

Infectious Lymphadenopathy
Geography dependent. At HCMC TB and histoplasmosis.
Fungal and Mycobaterial stains.

Histoplasmosis

Infectious Lymphadenopathy
CRYPTOCOCCUS TUBERCULOSIS

EUS-FNA & Sarcoidosis
5% mediastinal LNs
Scant cellularity
“Tight” granulomas
Damaged cells
Often lacks necrosis
Always send cultures
Sensitivity 94%
Specificity 100%
Mishra G et al. Endoscopy 1999;31:377.
Fritscher Ravens A et al. Chest 2000;118:928.

EUS-FNA & Lymphoma
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
EUS-FNA only EUS-FNA + Ancillary
Tests
Sensitivity
Specificity
Accuracy
74%
93%
81%
44%
90%
68%
Ribeiro A et al. Gastrointest Endosc 2001;53:485.

REACTIVE LYMPHOMA

Mediastinal Large Cell B-Cell NHL
F>M 2nd to 3rd decade - Monomorphic large cells: single, clusters
– less cells and damaged if sclerosis
~ epithelial malignancy - ~ HD, syncytial variant – less cellular
EUS-FNA - Ancillary studies – Definitive diagnosis

Mediastinal Hodgkin Lymphoma
Nodular sclerosing variant
Scant cellularity; cell degeneration
~ reactive hyperplasia
~ granulomatous infection
~ germ cell tumor – more cellular
~ anaplastic lymphoma – more cellular
Syncytial variant
~ metastasis

Hodgkin Lymphoma: SV

Mediastinal Masses

Other Mediastinal Masses
Thymoma – anterosuperior
Thymic cyst – anterosuperior
Thyroid/parathyroid –anterosuperior
Germ cell – anterior, middle
Foregut cyst – middle
Neurogenic – posterior
Paraganglioma – posterior
Mesenchymal – posterior
Metastasis – anterior, middle

Nodal Staging by EUS
N0 N1
<1 cm Size >1cm
Less hypoechoic Echogenicity Hypoechoic
Oval, flat Shape Round
Poor Demarcation Sharp

EUS-FNA & Mediastinal Adenopathy
Probability of Malignancy
Patients with history of extrathoracic primary
Diagnostic sensitivity is slightly better
Metastasis from such a source is likely
Patients without history of malignancy
Benign or malignant diagnosis equal proportion
If malignant diagnosis: lung primary is diagnosed in >80% cases
Kramer H et al. Eur J Cancer 2004;40:559.
Fritscher-Ravens A et al. Am J Gastroenterol 2000;95:2278.

NSCLC
Subcarinal Lymph Node

Lung Cancer Staging
N1
Ipsilateral peribronchial
and/or hilar
N2 Ipsilateral mediastinal
and/or subcarinal
N3 Contralateral
Cervical, supraclavicular
CA
STAGE
IIIB
IIIA

NSCLC: Mediastinal LN Staging
COST
EUS+FNA = $1,975
Mediastinoscopy = $7,759
Thoracotomy = $26,028
0%
50%
100%
Accuracy
EUS
CT
EUS-FNA
Gress F et al. Ann Intern Med 1997;127:604.
Tournoy KG et al. Am J Respir Crit Care Med 2007
Micames CG et al. Chest 2007;131:539.
84
49
96
High diagnostic yield and accuracy,
detects occult metastasis, avoids
unnecessary surgery, has less
complications, and cost effective.

EUS-FNA in NSCLC Staging
N=40 patients in whom mediastinal exploration was required. Randomized to have EUS-FNA (n=19) or surgical staging (SS) (n=21).
Sensitivity:
EUS-FNA: 93%. Surgical staging: 73%
Complications: 0% EUS-FNA vs 5% SS.
Hospital stay: 0 EUS-FNA vs 2 nights SS.
“EUS-FNA reduces the need for SS in patients with lung cancer in need for mediastinal exploration.”
Tournoy KG et al. Am J Respir Crit Care Med. 2007.

EUS-FNA, CT & PET in NSCLC
Staging
113 patients with NSCLC
Diagnostic accuracy EUS-FNA CT PET
Mediastinal LNs 93% 81% 83%
Distant Metastasis 97% 89%
Celiac LN (n=11) 100% 50%
•EUS-FNA as first test has high diagnostic yield and accuracy for detecting
lung cancer metastasis to mediastinum and distant sites.
•EUS-FNA able to detect <1 cm metastasis often missed by CT.
•EUS-FNA avoided thoracotomy in 14% cases.
Singh, P. Am J Respir Crit Care Med. 2007;175:345.

EUS-FNA in NSCLC Staging
Medline, CINAHL, and citation indexing
Metaanalysis to estimate pooled sensitivity and specificity.
Patients with…. Sensitivity Especificity
Mediastinal LNs (18 studies) 83% 97%
Mediastinal LNs + by CT (8 studies) 90% 97%
Mediastinal LNs – by CT (4 studies) 58%
•Minor complications in 10 cases (0.8%).
•EUS-FNA is highly sensitive to confirm metastasis to mediastinal
LNs seen by CT.
•Potential to prevent unnecessary surgery in cases with (-) CT scan.
Micames CG et al. Chest 2007;131:539.

EUS-FNA & EBUS-TBNA in
Mediastinal Lymph Nodes
EUS-FNA (Posterior Mediast)
EBUS-TBNA (Anterior Mediast)
Both
Sensitivity >90% >90% 100%
Specificity 100% 100% 100%
Accuracy
In other study: EUS-FNA had 82% sensitivity and 80% specificity. When combined with EBUS-TBNA: accuracy was 100%.
Both techniques are complementary and may replace more invasive methods for diagnosing and staging NSCLC.
Vilmann P et al. Endoscopy 2005;37:833.
Vilmann P & Puri R. Minerva Med 2007:98:331.

Guidelines & New Proposed Classification of Lung ACA
Term NSCLC in not acceptable
Either ACA or SqCC… we need
Cytologic or tissue (CB) diagnosis and
Molecular characterization: EGFR and ALK
To provide targeted therapy
EGFR mut = ACA = Tx TKI (gefitinib, erlotinib)
ALK rearrang = ACA = Tx crizotinib
Travis WD et al. J Thorac Oncol 2011;6:244-285.

EGFR & ALK Alterations Detection Cytologic material … IHC as screening; if (-) do
PCR for EGFR or FISH for ALK….. PROMISING
Molecular testing: expensive and complex
Immunohistochemistry: cheap, widely used, easily available in a laboratory
Abs to EGFR exons: 19 deletion and 21 mutation. 92% sensitivity and 99% specificity
Abs to ALK rearrangements…
Moreira AL and Hasanovic A. Acta Cytol 2012;56:603

Esophageal Cancer Staging
T1 T2 T3 T4
T: EUS is the only imaging modality that can image wall layers
N: Majority of nodal regions visualized
M: Limited (cannot assess bone, lung, and lateral 1/3 liver)

Esophageal Nodal Staging
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Regional Celiac
EUS sensitivity
EUS-FNA accuracy
CT sensitivity
Vasquez-Sequeiros E et al. Gastrointest Endosc 2001;53:751.
Eloubeidi MA et al. Gastrointest Endosc 2001;54:714.
63%
93%
54%
77%
100%
54%

Subcarinal Lymph Node
ER

EUS-TCB & EUS-FNA in Thoracic Lesions
EUS-FNA EUS-TCB FNA + TCB
Adequacy 63% - 96% 89% 97%
Accuracy 74% - 79% 68% - 79% 98%
Complications 0.6%
EUS-FNA/TCB improves adequacy of sampling and accuracy compared with either technique alone and it is safe.
TCB appears to be better in benign conditions.
EUS-FNA & TCB are complementary and may prevent unnecessary invasive procedures.
Wittmann, J et al. Cytopathology 2006;17:27.
Storch I et al. Surg Endosc 2008;22:86.

How Many “Passes”?
Diagnostic Material 80% in the first pass, “100%” in 3 passes
Wallace et al, DDW 2000
Lymph node involvement can be focal
Hamada, et al. Br J Radiol 1997
EUS-FNA & LN Metastasis
Sensitivity 90%, specificity 100%.
Suction: ↑cellularity but not accuracy
LN site (edge vs center) doesn’t ↑accuracy
Excess blood when <25 g needle
Cytospin or CB add little diagnostic info (except for IHC)
On-site cytologic assessment and sample triage are of paramount importance.
Stelow EB et al. Diagn Cytopathol 2004;30:301.
Wallace MB et al. Gastrointest Endosc 2001;54:441.

EUS-FNA NODAL SAMPLING
EUS visualizes most mediastinal, superior abdominal, and retroperitoneal lymph nodes.
Sonographic criteria are good EUS-FNA increases accuracy and specificity.
Lymph node sampling ( 3 passes): Flow cytometry.
Cytogenetics.
Microbiology.
Serious complications: not reported.
Gastrointest Endosc 2003; 58:819-821

EUS-FNA Lymph Nodes:
Complications
Author N Comp
Wiersema (1995) 192 0
Vilmann (1995) 14 0
Bhutani (1997) 35 0
Gress (1997) 24 0
Fritscher-Ravens (2000) 153 0
O’Toole (2001) 62 0
Overall 480 0


Gracias!!!
Cytology Michael W. Stanley, M.D. HCMC Cytology Gastroenterology Shawn Mallery, M.D. Rebecca Lai, M.D

Hummingbird – Nazca Lines - Peru
AERIAL VIEW