cysticercosis of superior oblique muscle: surgical excision and reconstruction of superior oblique...
TRANSCRIPT

Cysticercosis of superior oblique muscle: surgical excision and reconstruction of superior oblique tendon
Mandeep S. Bajaj, *MD; Neelam Pushker, *MD; Seema Sen, t MD; Ramamurthy Balasubramanya, * MD
I nfection with Cysticercus cellulosae, the larval stage of Taenia solium, is the most common para
sitic disease found in human beings and is a serious health problem in developing countries. 1 Orbital cysticercosis is emerging as a frequent cause of orbital and subconjunctival masses in children and young adults.2•3 The most common site of lodgement of the cyst in the orbit is the extraocular muscles, the medial rectus being involved most frequently. 2- 5 Involvement of the superior oblique has been reported in only six cases. 2.4.6.7 We describe a patient with cysticercosis involving the superior oblique muscle who required reconstruction of the superior oblique tendon.
CASE REPORT
A 9-year-old boy presented with painful swelling of his right upper eyelid and occasional diplopia in upgaze for 6 months. In the preceding 2 weeks the swelling had suddenly increased in size, with complete drooping of his upper eyelid. Computed tomography 2 months earlier had shown a thick-walled cyst adjacent to the insertion of the superior oblique containing a hyperdense lesion suggestive of a scolex (Fig. 1, top). A 3-month course of therapy with albendazole
From *Oculoplastic and Paediatric Ophthalmology Services and tthe Division of Ocular Pathology, Dr. R.P. Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, Ansari Nagar, New Delhi, India
Originally received Feb. 27, 2002 Accepted for publication Sept. 22, 2002
Correspondence to: Dr. Neelam Pushker, Oculoplastic and Paediatric Ophthalmology Services, Dr. R.P. Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110 029, India: fax +91-11-6852919; [email protected]
This article has been peer-reviewed.
Can j Ophthalmol 2002;37:423-6
Cysticercosis of superior oblique-Bajaj et al
(15 mg/kg per day administered orally) and prednisolone (1 mg/kg per day given orally) was started. CT done 6 weeks after this treatment was started showed a reduction in the size of the cyst, with persistence of the scolex.
On examination the patient's visual acuity was 20/20 in both eyes. A diffuse swelling was noted in the nasal part of the upper eyelid, with almost complete ptosis. When the right upper eyelid was retracted, a large
Fig. 1-Contrast-enhanced axial computed tomograms. Top: Thick-walled cyst with scolex adjacent to insertion of superior oblique muscle. Bottom: Three months later, cyst has increased in size and has migrated anteriorly.
423

Cysticercosis of superior oblique-Bajaj et al
Fig. 2-Preoperative photograph, showing large cystic mass prolapsing through superior fornix.
(12 mm by 10 mm) cystic mass was seen prolapsing from the superior fornix (Fig. 2). There was marked restriction of ocular motility in upgaze. As the mass was covering most of the eyeball, it precluded detailed strabismologic evaluation. The remainder of the ocular examination was normal, as was systemic examination . CT (with 2-mm slices) showed the cyst to be larger and more anterior than on the previous scans (Fig. l, bottom). The scolex continued to be seen.
A transconjunctival anterior orbitotomy procedure was performed under general anesthesia (Fig. 3). A
thick-walled cyst measuring 25 mm by 18 mm involving the superior oblique muscle 15 mm from its insertion was seen. Continuity of the superior oblique was not observed, as the fibres of the tendon had been completely replaced by the substance of the cyst. A small portion of the belly of the superior rectus was adherent to the cyst wall (Fig. 3). The cyst was released from its surrounding attachments by means of blunt dissection and a cryoprobe, which greatly enhanced manoeuvrability (Fig. 3). Muscle clamps were applied to the superior oblique tendon, 2 mm from the cyst wall on both sides. The cyst was removed after its attachments to the superior oblique tendon were incised, which resulted in a 10-mm defect in the tendon. The defect was reconstructed with a silicone band measuring 10 mm by 3 mm by 2 mm, sutured to the cut ends of the tendon with 6-0 nylon (Fig. 3). Postoperatively, albendazole (15 mg/kg per day) and prednisolone (I mg/kg per day) were administered orally for 4 weeks, along with topical steroid and antibiotic therapy.
On gross examination the cyst measured 25 mm by 18 mm. Its wall was 2 mm to 3 mm in thickness, and the lumen contained a yellowish exudate. On light microscopic examination the fibrous cyst wall was infiltrated by chronic inflammatory cells and palisading histiocytes, with neutrophilic exudates in its lumen.
Fig. )-Intraoperative photographs. Top left: Cystic mass in superior fornix arising from superonasal part of orbit. Top right: Attachments of cyst to superior oblique tendon and belly of superior rectus muscle. Bottom left: Application of cryoprobe to cyst wall. Bottom right: Reconstruction of superior oblique tendon with silicone expander (arrow).
424 CAN J OPHTHALMOL-VOL. 37, NO. 7, 2002
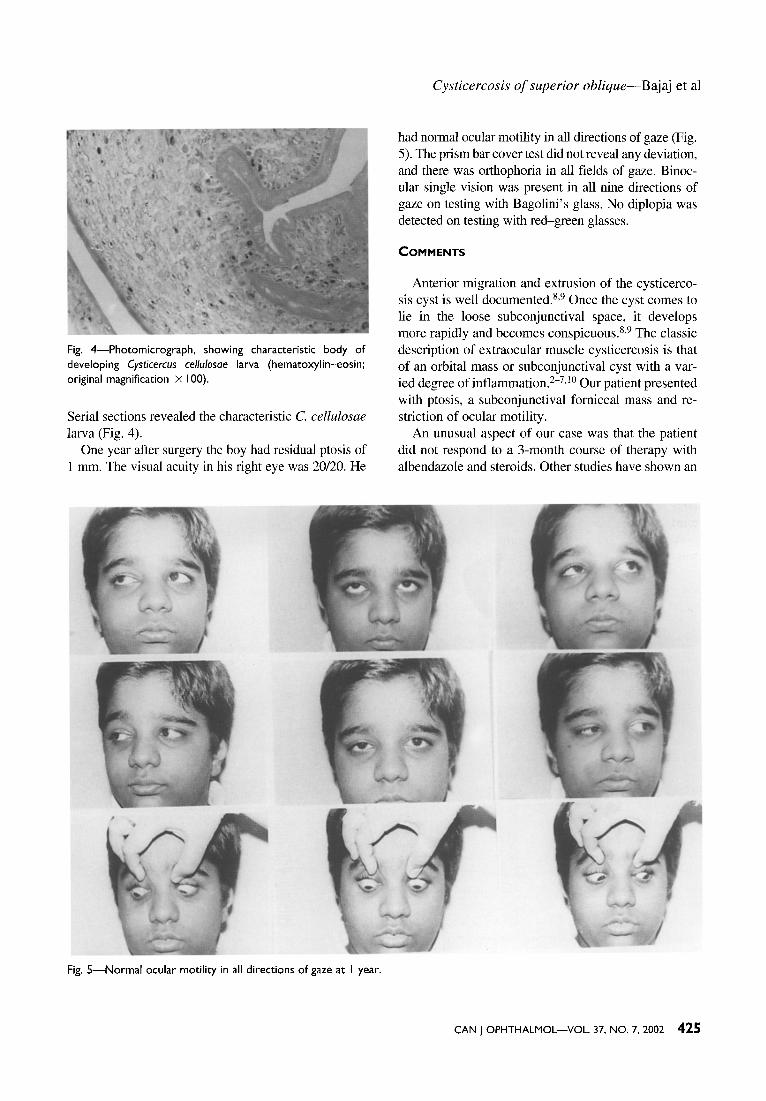
Fig. 4-Photomicrograph, showing characteristic body of developing Cysticercus cel/ulosae larva (hematoxylin-eosin; original magnification X I 00).
Serial sections revealed the characteristic C. cellulosae larva (Fig. 4).
One year after surgery the boy had residual ptosis of I mm. The visual acuity in his right eye was 20/20. He
Fig. 5-Normal ocular motility in all directions of gaze at I year.
Cysticercosis of superior oblique-Bajaj et al
had normal ocular motility in all directions of gaze (Fig. 5). The prism bar cover test did not reveal any deviation, and there was orthophoria in all fields of gaze. Binocular single vision was present in all nine directions of gaze on testing with Bagolini's glass. No diplopia was detected on testing with red-green glasses.
COMMENTS
Anterior migration and extrusion of the cysticercosis cyst is well documented. 8•9 Once the cyst comes to lie in the loose subconjunctival space, it develops more rapidly and becomes conspicuous. 8•9 The classic description of extraocular muscle cysticercosis is that of an orbital mass or subconjunctival cyst with a varied degree of inflammation.2- 7•10 Our patient presented with ptosis, a subconjunctival fomiceal mass and restriction of ocular motility.
An unusual aspect of our case was that the patient did not respond to a 3-month course of therapy with albendazole and steroids. Other studies have shown an
CAN J OPHTHALMOL-VOL. 37, NO.7, 2002 425

Cysticercosis of superior oblique-Bajaj et al
excellent response to this treatment.2.3JI Resistance to medical therapy has been attributed to chronicity of the inflammation and pericystic changes.2JI In our case the resistance to medical therapy may have due to the thickness of the cyst walL Sekhar and Honavar2
found that in patients with myocysticercosis, time to recovery with medical therapy was significantly longer in those with longer duration of symptoms than in those with shorter duration of symptoms. However, Pandey and colleaguess did not find any correlation between the size of the cyst and response to therapy.
Currently, the first line of treatment for orbital myocysticercosis is medical therapy. We found few reports on surgical excision of orbital Cysticercus cysts.tO,t2 In our patient the fibres of the superior oblique tendon were completely replaced by the cyst. Excision necessitated cutting the tendon, which resulted in a large defect in the tendon. The use of a spacer for reconstructing the defect was considered judicious, so as to prevent random, uncalibrated reattachment of the tendon, which may have resulted in serious superior oblique dysfunction. Since silicone is highly biocompatible and inert, it is routinely used extraocularly in vitreoretinal surgery, levator surgery, 13 socket reconstruction, 14 frontalis sling surgeryls and strabismus surgery,16,17 with good results. Silicone expanders have been used in patients with Brown's syndrome and superior oblique overaction to achieve weakening of the muscle,l6.17 The successful use of this material in these situations encouraged us to use it for reconstructing the superior oblique tendon in our patient. To the best of our knowledge, ours is the first report of surgical excision of a Cysticercus cyst involving the superior oblique muscle followed by a reconstructive procedure on the tendon.
Surgical intervention remains a serious challenge because of the vital attachments to surrounding orbital structures, the propensity of the cyst to rupture intraoperatively, the postoperative cicatricial response, which may lead to restrictive ocular motility disorders, and the possibility of a complicated reconstructive procedure. In our case surgical removal was necessary as medical therapy failed. Reconstruction of the superior oblique tendon with a silicone band, which acted as a spacer for the dissected part of the tendon, resulted in full ocular motility in all gazes, which translated into an excellent cosmetic and functional outcome for the patient.
In conclusion, patients with orbital myocysticerco-
426 CAN J OPHTHALMOL-VOL. 37, NO. 7, 2002
sis who do not respond to medical therapy may require surgical intervention. In such cases a complicated reconstructive procedure may be necessary.~
REFERENCES
1. Kapoor S, Kapoor MS. Ocular cysticercosis. J Pediatr Ophthalmol Strabismus 1978;15:170--3.
2. Sekhar GC, Honavar SG. Myocysticercosis: experience with imaging and therapy. Ophthalmology 1999;106: 2336-40.
3. Puskher N, Bajaj MS, Chandra M, Neena. Ocular and orbital cysticercosis. Acta Ophthalmol Scand 2001;79: 408-13.
4. Sekhar GC, Lemke BN. Orbital cysticercosis. Ophthalmology 1997;104:1599-604.
5. Pandey PK, Chaudhuri Z, Sharma P, Bhomaj S. Extraocular muscle cysticercosis: a clinical masquerade. J Pediatr Ophthalmol Strabismus 2000;37:273-8.
6. Brooks AM, Essex WB, West RH. Cysticercosis of superior oblique muscle. Aust J Ophthalmol 1983; 11:119-22.
7. Pandey PK, Chaudhuri Z, Bhatia A. Extraocular muscle cysticercosis presenting as Brown's syndrome. Am J Ophthalmol2001;131:526-9.
8. Bansal RK, Gupta A, Grewal SPS, Mohan K. Spontaneous extrusion of cysticercosis: report of three cases. Ind J Ophthalmol 1992;40:59--60.
9. Mehrotra SK, Sofat BK. Ocular myocysticercosis. Ind J Ophthalmol1975;23:39-40.
10. Sen DK. Cysticercus cellulosae in the lacrimal gland, orbit and eyelid. Acta Ophthalmol1980;58:144-7.
11. Puri P, Grover AK. Medical management of orbital cysticercosis: a pilot study. Eye 1998;12:795-9.
12. DiLoreto DA, Kennedy RA, Neigel JM, Rootman J. Infestation of extraocular muscle by Cysticercus cellulosae. Br J Ophthalmol1990;74:751-2.
13. Marcoli F, Adenis JP, Ferrara V, Ghisolfi A. Simplification in locating and dissecting the levator muscle of the upper eyelid in surgery for ptosis. J Fr Ophtalmol 1997;20: 554-60.
14. Tercan M. Thin Silastic sheet for orbital floor repair. Plast Reconstr Surg 1995;96:1238-9.
15. Carter SR, Meecham WJ, Seiff SS. Silicone frontalis sling for the correction ofblepharoptosis: indications and efficacy. Ophthalmology 1996;103:623-30.
16. Wright KW. Results of the superior oblique tendon elongation procedure for severe Brown's syndrome. Trans Am Ophthalmol Soc 2000;98:41-8.
17. Pollard ZF, Greenberg MF. Results and complications in 66 cases using a silicone tendon expander on overacting superior obliques with A-pattern anisotropias. Binocul Vis Strabismus Q 2000;15:113-20.
Key words: cysticercosis, superior oblique muscle, silicone expander, orbit