cutaneous toxicities of anti-cancer therapies - ce.mayo.edu · raf/mek/erk map kinase pathway ......
TRANSCRIPT
Cutaneous Toxicities of Anti-Cancer Therapies
Matthew R. Hall, M.D. Assistant Professor of Dermatology Mayo Clinic Florida Mayo Clinic Cutaneous Oncology Symposium Jacksonville, FL Saturday, September 24, 2016

DISCLOSURES
None

Overview
SCC Therapies EGFR Inhibitors (cetuximab, panitumumab, gefitinib, erlotinib)
Melanoma Therapies BRAF Inhibitors (Vemurafenib and Dabrafenib)
MEK/ERK Inhibitors (Trametinib, Cobimetinib)
CTLA4 Inhibitor (Ipilimumab)
PD-1 Inhibitors (Nivolumab, pembrolizumab)
Sorafenib

EGFR Inhibitors
Head and Neck SCC Monoclonal antibodies to EGFR
Cetuximab and Panitumumab
Small molecule tyrosine kinase inhibitors (specific for EGFR) Erlotinib and gefitinib

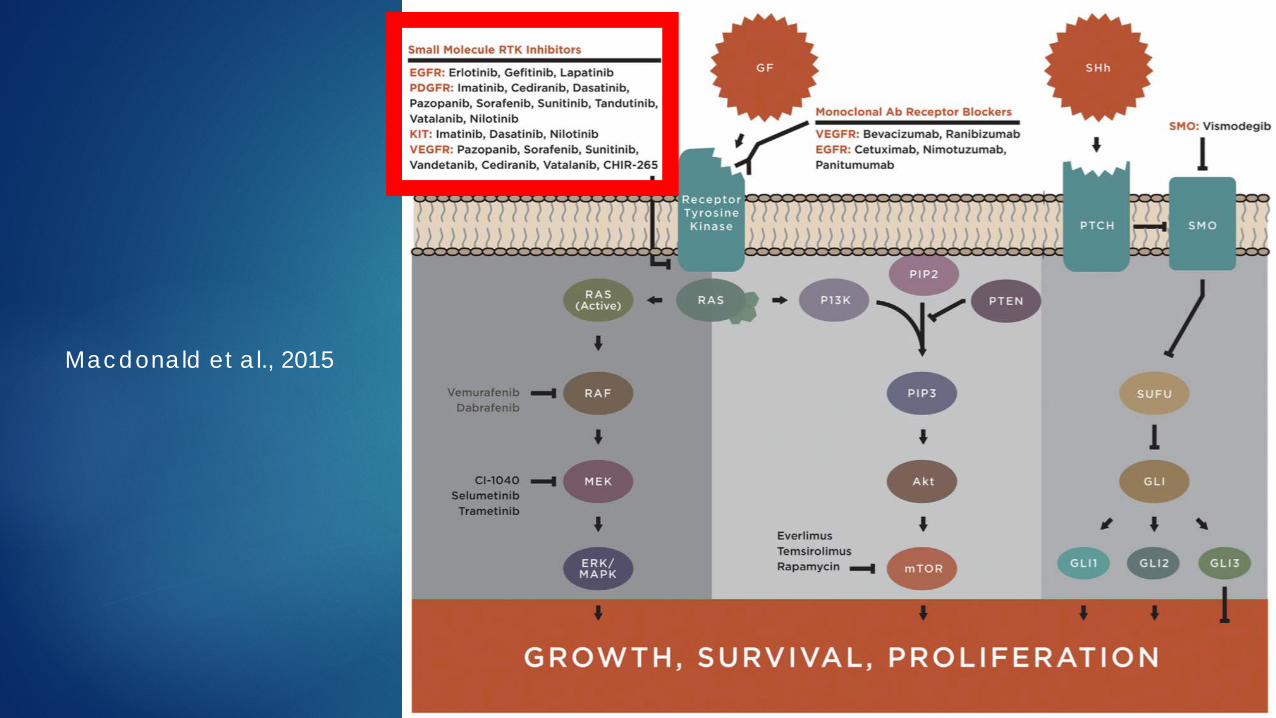
Macdonald et al., 2015

Cutaneous Toxicities of EGFR Inhibitors EGFR is expressed in epidermis and appendages
Important in epidermal and pilosebaceous function
Cutaneous toxicities are common (50-90%)
Tell patients to expect a rash, it is not a drug allergy and not reason to stop Rx
Cetuximab, panitumumab>erlotinib>gefitinib
Median onset 7-10d after drug initiation Papulopustular eruption (up to 75%)
Xerosis (30%)
Hair changes (slower growth, brittle, trichomegaly)
Mucositis
Nail changes
Photosensitivity

Papulopustular Eruption
Macdonald et al., 2015
Reyes-Habito and Roh 2014

Papulopustular Eruption
Reyes-Habito and Roh 2014

Papulopustular Eruption
Unlike acne No comedones or cystic papules
Pruritic
Severity of the eruption correlates with tumor response to EGFR inhibition and survival
Etiology EGFR downregulates IL-1 dependent inflammation in the hair follicle
Thus, EGFR blockade leads to increased follicular inflammation

Paronychia & Pyogenic Granuloma
Reyes-Habito and Roh 2014

Trichomegaly
Macdonald et al., 2015

Treatment of EGFR Inhibitor Toxicities
Papulopustular eruption
Grade 1 eruptions (<10% BSA)
Topical antibiotics (clindamycin)
Topical steroids
Topical calcineurin inhibitors (off-label)
Avoid retinoids (irritation, lack of comedones)
Grade 2 and 3 eruptions (10-30% BSA)
Tetracyclines
Low dose isotretinoin
Culture to rule out superinfection
Pruritusantihistamines (doxepin if severe)
Paronychia
Antibacterial soaks
Dilute vinegar
Dilute bleach
4% thymol in 70% EtOH
Culture
Topical steroids

Vermurafenib and Dabrafenib
Inhibitors of mutated BRAF Raf/MEK/Erk MAP kinase pathway BRAF is an activator in the Map Kinase pathway
Mutated in ~50% of melanomas

Macdonald et al., 2015

Vemurafenib
Cutaneous reactions are common and polymorphous Diffuse rash
Epidermal tumors
Keratosis pilaris-like eruption
Seborrheic dermatitis-like eruption
Hyperkeratotic hand-foot reaction
Photosensitivity
Panniculitis
Melanocytic proliferations

Vemurafenib
Rash Most commonly folliculocentric papules Morbilliform (measles-like) distribution
“Maculopapular”
Involves trunk and extremities Histology shows features of classic drug reaction
Treatment of rash Emollients Antihistamines Topical steroids
Prednisone if severe Don’t necessarily need to stop medication but can try dose reduction

Morbilliform Drug Eruption
Fitzpatrick’s Dermatology in General Medicine, 8th ed.

Keratosis Pilaris-like Eruption
Macdonald et al., 2015

Seborrheic Dermatitis-like Eruption
Macdonald et al., 2015

Hyperkeratotic Hand-Foot Eruption
Desquamation at sites of friction on palms and soles Can be painful May require dose reduction Management
Avoid friction and pressure
Topical steroids

Hyperkeratotic Hand-Foot Eruption
Macdonald et al., 2015

Vemurafenib
Epidermal tumors SCC and verrucal keratoses
Verrucal keratoses are not caused by HPV
SCCs can appear rapidly (within 1st week) Occur in up to 30% of patients
Most occur within the first 6 months (peak within 1st 18 weeks)
Generally show low grade histology
Widespread benign verrucal keratoses can occur in up to 80% Peaks within 6-12 weeks

Vemurafenib
Mechanism of SCC induction RAF blockade can lead to paradoxical MAPK activation, especially in
the presence of RAS mutations (sun damaged skin)
This unmasks pre-existing mutationstumor formation
Accounts for rapid SCC development after starting medication
Downstream concurrent inhibition of MEK leads to decreased SCC development

Verrucal Keratoses
Macdonald et al., 2015

Squamous Cell Carcinomas
Macdonald et al., 2015

Management of Epidermal Neoplasms on BRAF Inhibitors
Verrucal Keratoses Benign
May be premalignant
Monitor closely for evolution into SCC
Consider cryotherapy
SCC Excision, electrodessication and curettage, or cryotherapy if early
Consider intralesional 5-fluorouracil
Typically does not require dose reduction
Unclear whether these have increased risk of metastasis
Can be eruptive and resolve after treatment ends

Intralesional 5-FU for SCC
Intralesional 5-FU 50mg/ml Inject 0.1-0.3 ml per quadrant of the tumor
No more than 1-1.5cc at a time Tumor involutes Closely monitor patient for resolution
MEK/ERK Inhibitors
Raf/MEK/Erk MAP kinase pathway Selumetinib, Trametinib

Macdonald et al., 2015

MEK/ERK inhibitors
Similar cutaneous side effect to EGFRs rather than RAF blockade Combination of MEK and BRAF inhibitors can decrease risk of
cutaneous adverse effects Morbilliform eruption Papulopustular eruption Xerosis Alopecia Hyperpigmentation Paronychia Trichomegaly

Papulopustular Eruption
Macdonald et al., 2015

Paronychia
Macdonald et al., 2015

CTLA4 and PD-1 inhibitors
Immune checkpoint inhibitors that augment the normal immune response and produce proinflammatory skin reactions
CTLA4 inhibitor: Ipilimumab PD-1 inhibitors: Nivolumab, pembrolizumab

Ipilimumab Due to augmented immune response, autoimmune skin reactions are
common (40%) Pruritus (up to 30%) Morbilliform eruption (10-50%) Vitiligo-like hypopigmentation
Portends favorable prognosis
Less common Prurigo nodularis
Lichenoid eruption
Papulopustular eruption
Ulcerations
Photosensitivity
Toxic epidermal necrolysis (TEN) reported

Nivolumab and Pembrolizumab
Autoimmune skin eruptions Vitiligo
Pruritus
Lichenoid eruptions Do not necessitate discontinuation of the medication

Lichenoid Eruptions
Joseph et al., 2015

Pathology
Joseph et al., 2015

Sorafenib
Multikinase inhibitor to treat melanoma Small molecule inhibitors of tyrosine kinase inhibitors Inhibit VEGF, PDGF, KIT, RAF, and others
Macdonald et al., 2015

Sorafenib Many cutaneous adverse effects
Hyperkeratotic hand-foot skin reactions
Stomatitis (25%)
Alopecia (44%)
Hair color and texture changes
Morbilliform eruption
Genital eruption
New SCCs and inflammation of AKs (10%)
Subungual splinter hemorrhages (70%)
Seborrheic dermatitis-like eruption with facial edema (60%)

Hand-Foot Skin Reaction
Reyes-Habito and Roh 2014 Macdonald et al., 2015

Hyperkeratotic Hand-Foot Skin Reaction Different from hand-foot syndrome due to conventional chemotherapy
Erythema that can blister and ulcerate
Painful, hyperkeratotic plaques at sites of pressure and friction Dose-dependent reaction Treatment
Moisturizing creams and ointments Keratolyic creams (40% Urea) Gel or foam shoe inserts Potent topical steroids (clobetasol) Topical lidocaine Consider dose reduction for severe, debilitating pain Antiseptic baths of blisters or erosions
Dilute vinegar or bleach

Psoriasiform Genital Eruption
Macdonald et al., 2015