current status and indications for intermittent … · 8 corresponding faculty c allegra (italy) j...
TRANSCRIPT

1
CURRENT STATUS AND INDICATIONS FOR
INTERMITTENT PNEUMATIC COMPRESSION
A N Nicolaides
Emeritus Professor of Vascular Surgery, Imperial
College, London.
Hon. Professor of Surgery, University of Nicosia
Medical School, Cyprus

2
Disclosures
Honoraria for lectures received from:
Covidien / Medronic
Alpha Wasserman / AlphaSigma
Servier
Pierre Fabre
3
HISTORY
Intermittent Pneumatic Compression (IPC)
was developed in the late 1970s to prevent DVT
Sequential compression device (SCD) with multiple
chambers was shown to be more effective than single
chamber devices in preventing perioperative DVT
Nicolaides et al, Brit J Surg 1978;65:359-363
Nicolaides et al, Surgery 1983;94:21-26

4
Developed under the auspices of the:
Cardiovascular Disease Educational and Research Trust (UK)
European Venous Forum
North American Thrombosis Forum
International Union of Angiology and
Union Internationale du Phlebologie
PREVENTION AND TREATMENT
OF VENOUS THROMBOEMBOLISM
International Consensus Statement 2013Guidelines According to Scientific Evidence

5
EDITORIAL COMMITTEE
Chairman: AN Nicolaides,
Cochairmen: J Fareed, AK Kakkar
Members: AJ Comerota, SZ Goldhaber, R Hull, K Myers,
M Samama, J Fletcher
Editorial Secretary: E Kalodiki

6
Faculty
D Bergqvist (Sweden)
J Bonnar (Ireland)
JA Caprini (USA)
C Carter (USA)
AJ Comerota (USA)
J Conard (France)
B Eklof (Sweden)
I Elalamy (France)
J Fareed (USA)
J Fletcher (Australia)
G Gerotziafas (France)
G Geroulakos (UK)
A Giannoukas (Greece)
SZ Goldhaber (USA)
I Greer (UK)
M Griffin (UK)
R Hull (USA)
A K Kakkar (UK)
S Kakkos (Greece)
E Kalodiki (UK)
MR Lassen (Denmark)
GDO Lowe (UK)
A Markel (Israel)
K Myers (Australia)
A Nicolaides (Cyprus)
P Prandoni (Italy)
G Raskob (USA)
M Samama (France)
AC Spyropoulos (USA)
AG Turpie (Canada)
JM Walenga (USA)
D Warwick (UK)

7

8
Corresponding Faculty
C Allegra (Italy)
J Arcelus (Spain)
N Baekgaard (Denmark)
G Belcaro (Italy)
H Bjarnason (USA)
MA Cairols (Spain)
M Catalano (Italy)
D Christopoulos (Greece)
D Clement (Belgium)
F Corvalán (Chile)
E Diamantopoulos (Greece)
J Fernandes e Fernandes
(Portugal)
C Fisher (Australia)
A Gasparis (USA)
H Gibbs (Australia)
V Hadjianastassiou (Cyprus)
K Ivancev (UK)
CP Hsien (Thaiwan)
JT Hobbs (UK)
D Hoppenstead (USA)
EA Hussein (Egypt)
O Iqbal (USA)
K Ivancev (Russia)
R Kistner (USA)
TK Kim (Korea)
M Kurtoglou (Turkey)
T Kölbel (Germany)
N Labropoulos (USA)
LH Lee (Singapore)
BB Lee (USA)
Y-J Li (China)
NC Liew (Malaysia)
A Llinas (Colombia)
M Nakamura (Japan)
P Neglen (Cyprus)
L Norgren (Sweden)
H Partsch (Austria)
N Ramakrishnan (India)
G Rao (USA)
J-B. Ricco (France)
N Rich (USA)
P Robless (Singapore)
W Schobersberger (Austria)
M Seed (UK)
S Schellong (Germany)
A Scuderi (Brazil)
R Sexana (India)
E Shaydakov (Russia)
A Shevela (Russia)
R Simkin (Argentina)
W Toff (UK)
JM Trabal (Puerto Rico)
M Vandendriessche
(Belgium)
M Veller (South Africa)
L Villavincencio (USA)
R Wahi (USA)
C Wittens (TheNetherlands)
R Wong (Hong Kong)
9
Outcomes
Evidence is presented for the following outcomes
asymptomatic DVT at screening
symptomatic DVT or PE,
fatal PE,
overall mortality and
development of the post-thrombotic syndrome (PTS) when
available
The decision to use asymptomatic DVT as well as
symptomatic DVT or PE is a subjective one based on
the following arguments

10
Arguments
The relationship between asymptomatic and symptomatic VTE
including PE has been known for some time.1-3
Reduction in the incidence of asymptomatic DVT has been shown
to be associated with a reduction of symptomatic DVT and PE4-6
Large studies that were powered to study efficacy on fatal PE have
demonstrated that reduction in silent DVT is accompanied by
reduction in clinical DVT, clinical PE and fatal PE.7
1. Kakkar VV.Ann R Coll Surg Engl. Nov 1969;45:257-276.
2. Philbrick JT et al Arch Intern Med. Oct 1988;148(10):2131-2138.
3. Hull RD et al Ann Intern Med. Jun 1983;98(6):891-899.
4. Giannoukas AD et al Eur J Vasc Endovasc Surg. Nov 1995;10(4):398-404.
5. Hull RD et al Ann Intern Med. Nov 20 2001;135(10):858-869.
6. Eikelboom JW et al Lancet 2001;358:9-15.
7. Kakkar VV et al Lancet. July 12 1975;306(7924):45-51.

11
Arguments
Regulatory authorities have recognized asymptomatic proximal
DVT as a valid endpoint of clinical trials and drug evaluation
Relatively few PE occur in patients with symptomatic DVT
The majority of PE including fatal PE occur in patients with
asymptomatic DVT
Thus, asymptomatic DVT is an important stage of thromboembolic
disease that has not yet manifested itself.
12
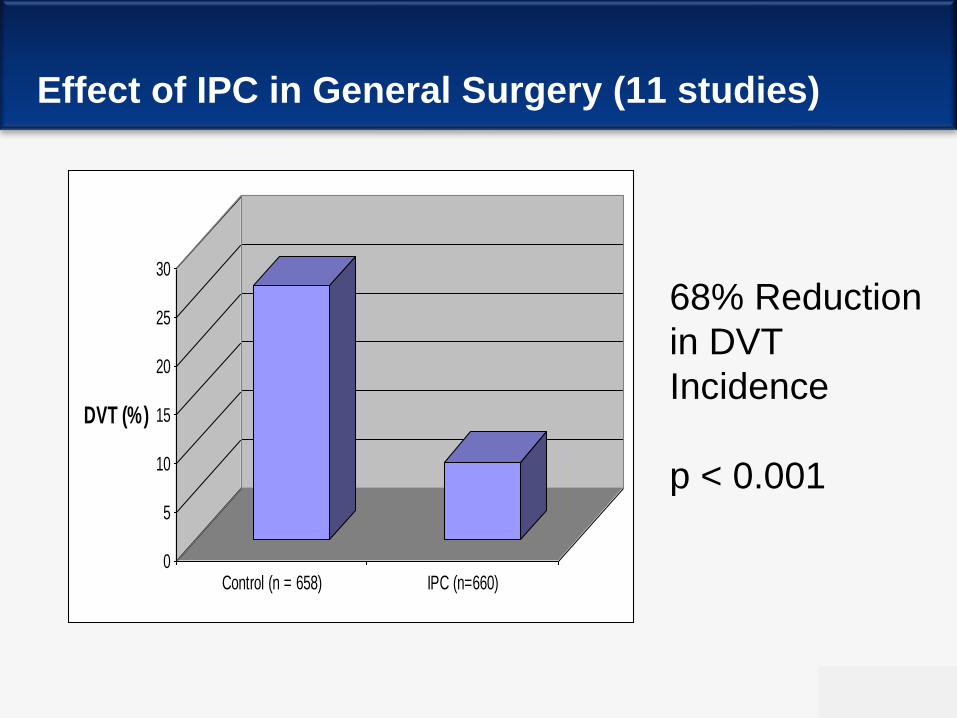
Effect of IPC in General Surgery (11 studies)
0
5
10
15
20
25
30
DVT (%)
Control (n = 658) IPC (n=660)
68% Reduction
in DVT
Incidence
p < 0.001
13
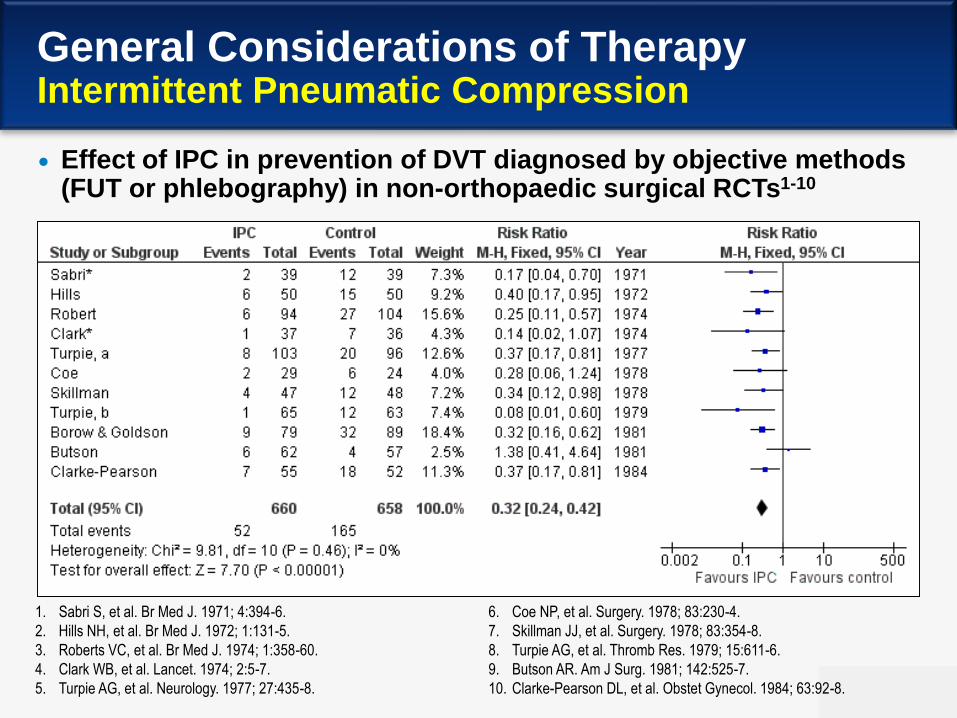
General Considerations of TherapyIntermittent Pneumatic Compression
Effect of IPC in prevention of DVT diagnosed by objective methods (FUT or phlebography) in non-orthopaedic surgical RCTs1-10
1. Sabri S, et al. Br Med J. 1971; 4:394-6.
2. Hills NH, et al. Br Med J. 1972; 1:131-5.
3. Roberts VC, et al. Br Med J. 1974; 1:358-60.
4. Clark WB, et al. Lancet. 1974; 2:5-7.
5. Turpie AG, et al. Neurology. 1977; 27:435-8.
6. Coe NP, et al. Surgery. 1978; 83:230-4.
7. Skillman JJ, et al. Surgery. 1978; 83:354-8.
8. Turpie AG, et al. Thromb Res. 1979; 15:611-6.
9. Butson AR. Am J Surg. 1981; 142:525-7.
10. Clarke-Pearson DL, et al. Obstet Gynecol. 1984; 63:92-8.
14
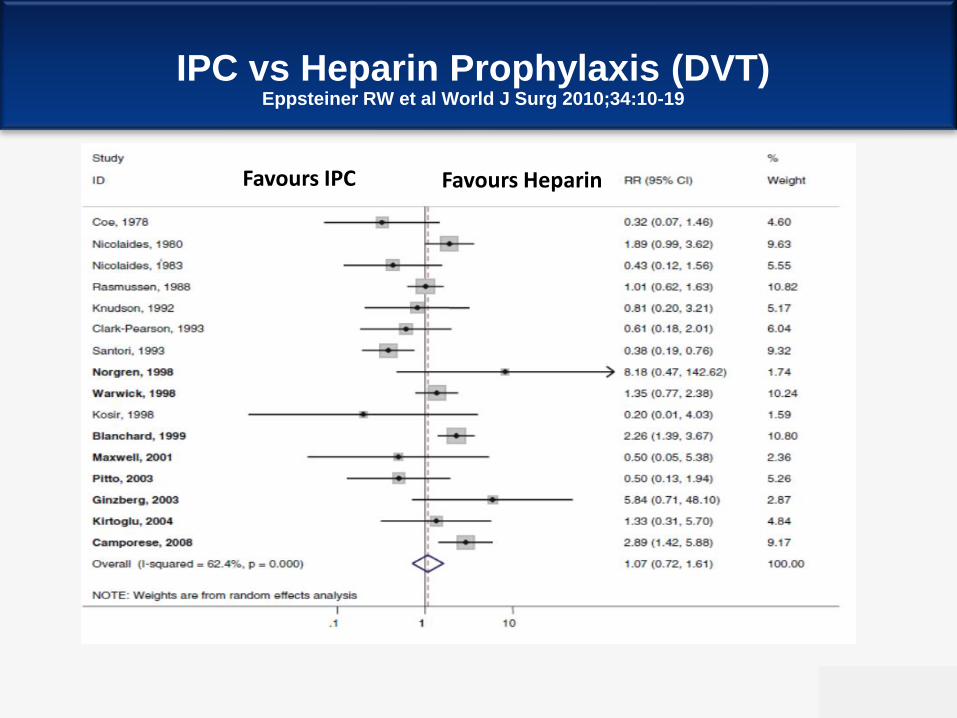
IPC vs Heparin Prophylaxis (DVT)Eppsteiner RW et al World J Surg 2010;34:10-19
Favours IPC Favours Heparin

15
IPC vs Heparin Prophylaxis (Bleeding)Eppsteiner RW et al World J Surg 2010;34:10-19
Favours IPC Favours Heparin

16
IPC in Orthopedic Surgery
IPC in Elective Hip Surgery
IPC In Elective Knee Replacement

17
Effect of Foot Impulse Technology with GEC on Proximal DVT
Hip and knee replacement (7 studies):
Proximal DVT was reduced from 26% to 10%
RR 0.39 (95% CI 0.28 to 0.54)

18
Combined Modalities
19
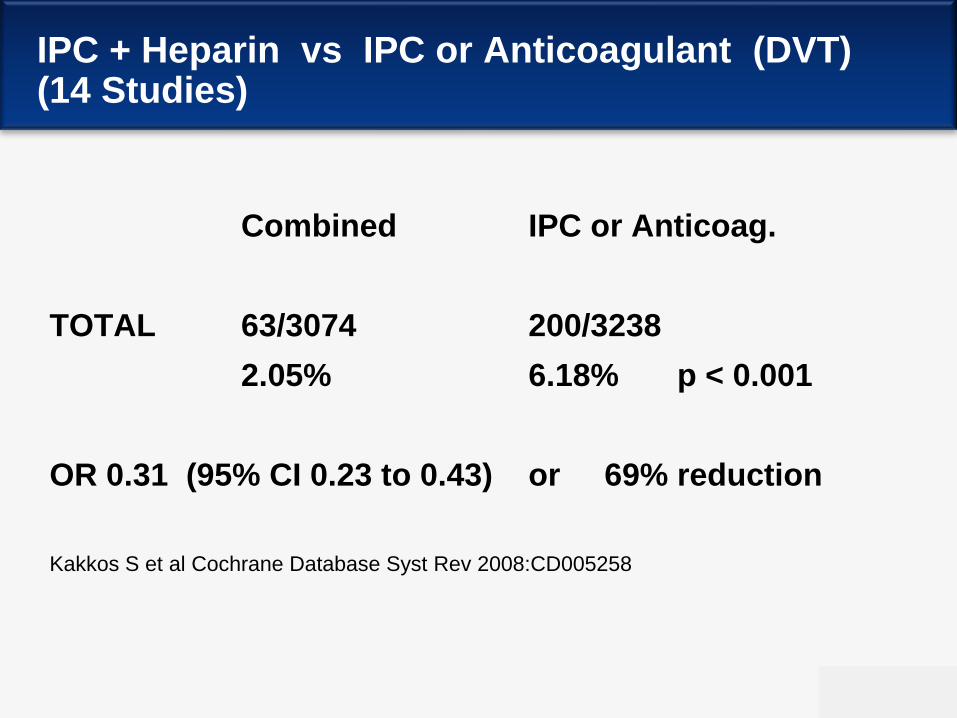
IPC + Heparin vs IPC or Anticoagulant (DVT) (14 Studies)
Combined IPC or Anticoag.
TOTAL 63/3074 200/3238
2.05% 6.18% p < 0.001
OR 0.31 (95% CI 0.23 to 0.43) or 69% reduction
Kakkos S et al Cochrane Database Syst Rev 2008:CD005258

20
IPC + Heparin vs IPC or Anticoagulant (Symptomatic PE) ( 16 Studies)
Combined IPC or Anticoag.
TOTAL 33/3838 122/4313
0.86% 2.83% p < 0.001
OR 0.34 (95% CI 0.23 to 0.50) or 67% reduction
Kakkos S et al Cochrane Database Syst Rev 2008:CD005258
21
Effect of Combined Modalities and PE(LD Heparin + SCD vs LD Heparin)
▪ Cardiac surgery (2482 randomised patients)
PE was reduced from 4% to 1.5%
RR 0.37 (95% CI 0.22 to 0.63)
Ramos et al Chest 1996
▪ Oesophagectomy (997 patients)
PE was reduced from 3.2% to 0.7%
RR 0.23 (95% CI 0.05 to 0.93)
Tsutsumi et al Surg Today 2000

22
APOLLO
A Multicenter, Randomized, Double-Blind,
Placebo-Controlled Study of patients having
abdominal surgery
ARIXTRA + IPC (n=650)
vs IPC used alone (n=659)
Turpie AG, Bauer KA, Caprini JA et al. J Thromb Haemost. 2007 Sep;5(9):1854-61

23
Conclusions
Clinal Results: 1 DVT and 1 non-fatal PE in each group
IPC + Fondaparinux reduced venographic rate by 70%
compared with IPC alone (1.7% vs. 5.3%).
IPC + Fondaparinux reduced proximal DVT from 1.7%
to 0.2% ( P = 0.037) compared with IPC alone.
Major bleeds occurred in 1.6% and 0.2% of
Fondaparinux-treated and placebo-treated patients,
respectively (P = 0.006), none being fatal or involving a
critical organ.
24
IPC and IPC+LMWH cost-effectiveness
Conclusion: IPC and IPC+LMWH are cost-effective versus LMWH after
lower-limb arthroplasty in the USA and Australia. The choice between
IPC and IPC+LMWH depends on expected bleeding risks.
R Saunders et al. ClinicoEconomics Research 2018;10:231-241

25
Conclusion
Compared to single modalities, combined
prophylactic modalities significantly decrease the
incidence of both postoperative DVT and PE in a
variety of specialties, including orthopedic, general
and cardiac surgery.
The results support their use, especially in high risk
patients (e.g. thrombophilia or previous VTE)

26
CLOTS 3 Study:
Patients with acute stroke
• Multicenter, RCT, parallel group
• Patients enrolled from Day 0 to 3 of hospital admission
• Randomized to receive either IPC or no IPC
• Duplex scanning on both legs by a blinded technician
at Day 7-10 and Day 25-30
• 6 months follo-up to determine survival and later
symptomatic VTE
27
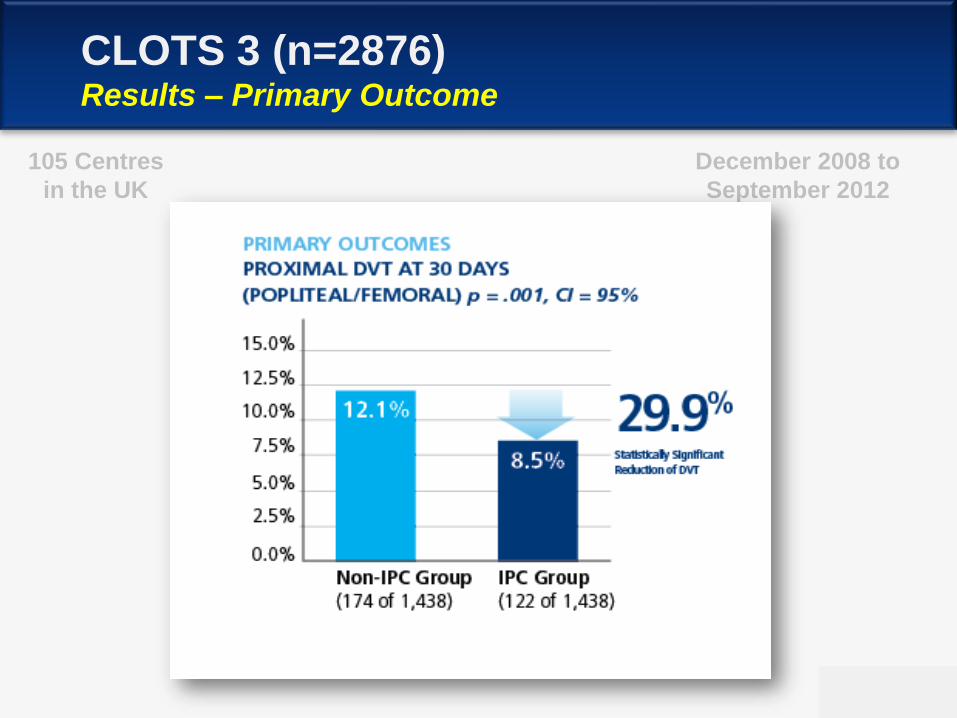
CLOTS 3 (n=2876)Results – Primary Outcome
December 2008 to
September 2012
105 Centres
in the UK

28
CLOTS 3Secondary Outcomes

29
Acute Stroke- Historical
Control vs LDUH 50% reduction in DVT (10 studies)
66% reduction in PE
LDUH vs LMWH 41% further reduction in DVT (2 studies)
Problem: Major intracranial hemorrhage increased from 1.1% to 2.6%
GEC vs GEC+IPC* 71% reduction in DVT (15.9% to 4.7%)
Control vs IPC** CLOTS3 study
25% reduction in all DVT (30 days)
35% reduction in proximal DVT (30 days)
14% reduction in mortality (6 months)
* Hemorrhagic stroke , ** Ischemic stroke

30
Recommendations - General Surgery
Moderate risk patients (major general surgery,
age >40, no additional risk factors)
(LDUH) or LMWH LE: high
IPC + GEC LE: high

31
Recommendations – General Surgery
High risk patients (major general surgery, age
> 60 or age > 40 with at least one additional
risk factor)
(LDUH) LMWH LE: high
IPC + GEC LE: high
Fondaparinux (one study) LE: moderate
Combined modalities LE: high
32
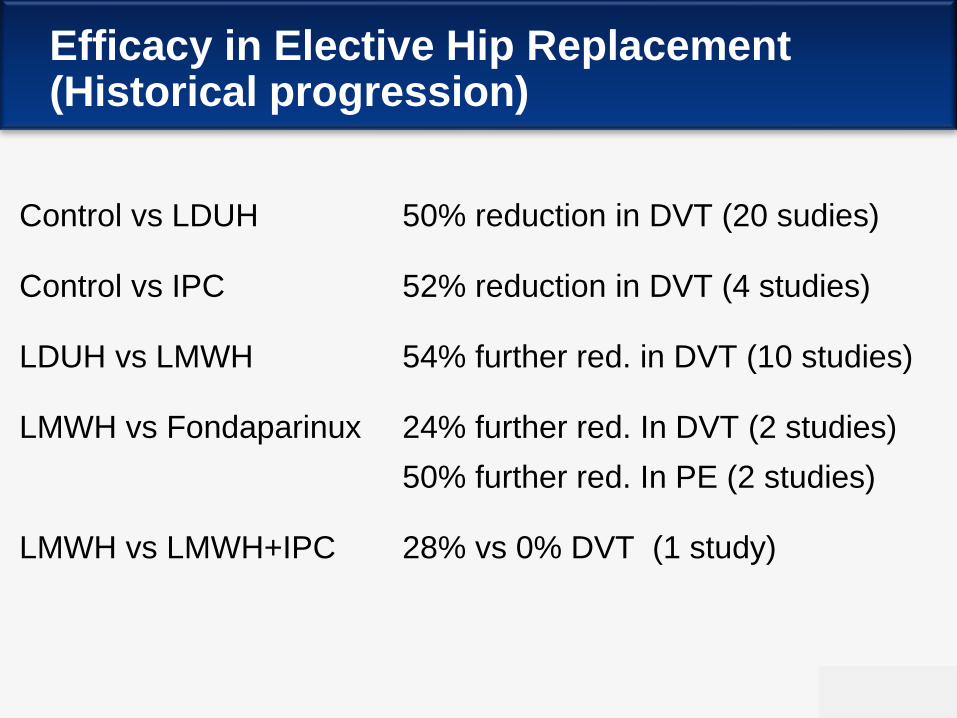
Efficacy in Elective Hip Replacement(Historical progression)
Control vs LDUH 50% reduction in DVT (20 sudies)
Control vs IPC 52% reduction in DVT (4 studies)
LDUH vs LMWH 54% further red. in DVT (10 studies)
LMWH vs Fondaparinux 24% further red. In DVT (2 studies)
50% further red. In PE (2 studies)
LMWH vs LMWH+IPC 28% vs 0% DVT (1 study)

33
Recommendationsfor Elective Hip Replacement (2013)
Fondaparinux LE: high (Most effective)
LMWH LE: high
IPC + GEC LE: high (Equivalent to LMWH)
IPC+GEC+LMWH LE: high (More effective than either)
Rivaroxaban, Dabigatran LE: high

34
Effect of IPC in PTS
1. Lowers venous pressure in the sitting position
2. Reduces edema
3. Increases fibrinolytic activity
4. Increases TFPI
5. Increases TcPO2
6. Increases oxygen diffusion barrier
7. Increases capillary perfusion
8. Increases skin nutrition
Comerota AJ J Vasc Surg 2011;53:1121-9
35
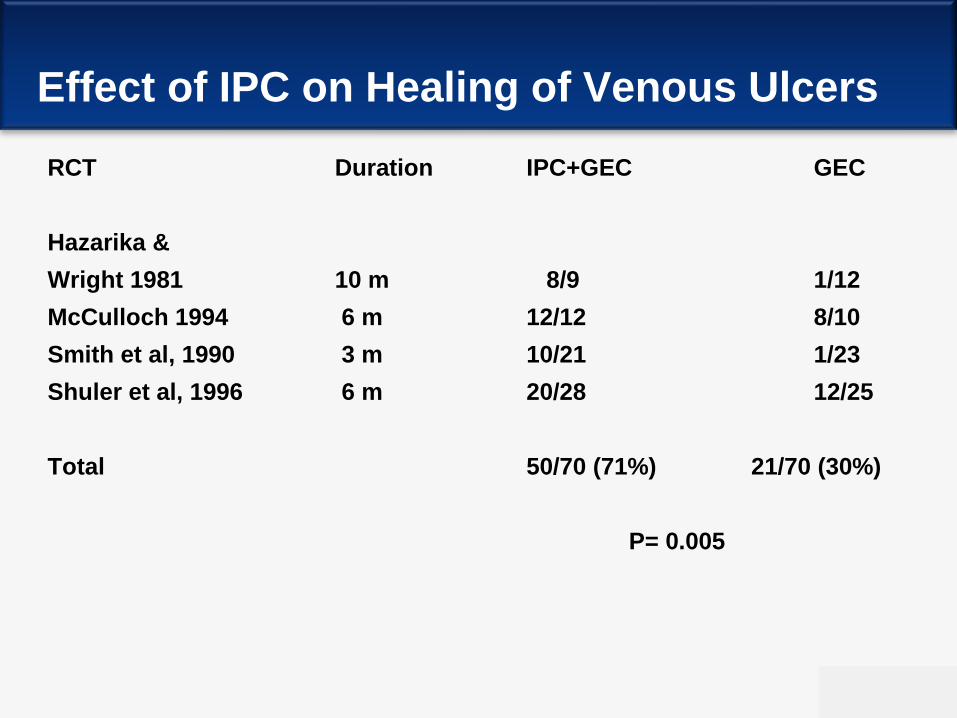
Effect of IPC on Healing of Venous Ulcers
RCT Duration IPC+GEC GEC
Hazarika &
Wright 1981 10 m 8/9 1/12
McCulloch 1994 6 m 12/12 8/10
Smith et al, 1990 3 m 10/21 1/23
Shuler et al, 1996 6 m 20/28 12/25
Total 50/70 (71%) 21/70 (30%)
P= 0.005
36
CONCLUSIONS re: IPC
IPC is an effective form of VTE prophylaxis
Use IPC for MODERATE risk patients especially if risk of
haemorrhage is high
Combine IPC with appropriate anticoagulation for high VTE risk
patients
Consider portable IPC devices for out-of-hospital use in very
high risk patients particularly when mobility at home is an issue
Use in combination with elastic compression for healing venous
ulcers