current managment in metastatic gastric cancer michele de tursi - chieti
TRANSCRIPT

CURRENT MANAGMENT IN METASTATIC GASTRIC CANCER
Michele De Tursi - Chieti
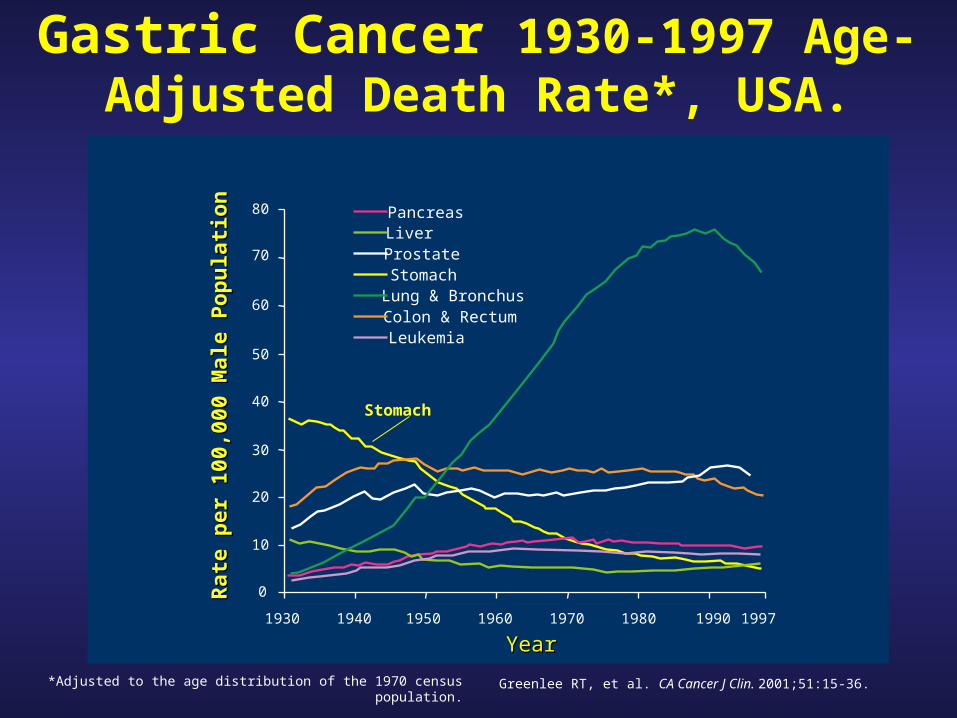
Gastric Cancer 1930-1997 Age-Adjusted Death Rate*, USA.
80
70
60
50
40
30
20
10
0
YearYear
Pancreas
Lung & Bronchus
ProstateStomach
Colon & RectumLeukemia
Liver
1930 1940 1950 1960 1970 1980 1990 1997
Rat
e p
er 1
00,0
00 M
ale
Po
pu
lati
on
Rat
e p
er 1
00,0
00 M
ale
Po
pu
lati
on
Greenlee RT, et al. CA Cancer J Clin. 2001;51:15-36.
Stomach
*Adjusted to the age distribution of the 1970 census population.

World Data 1999
•Males 511,000 new cases (11.9%)•Females 287,000 new cases (7.6%)•Total 798,000 new cases (9.9%)
•Males 397,000 deaths (13.4%)•Females 230,000 deaths (10.3%)•Total 628,000 deaths (12.1%)
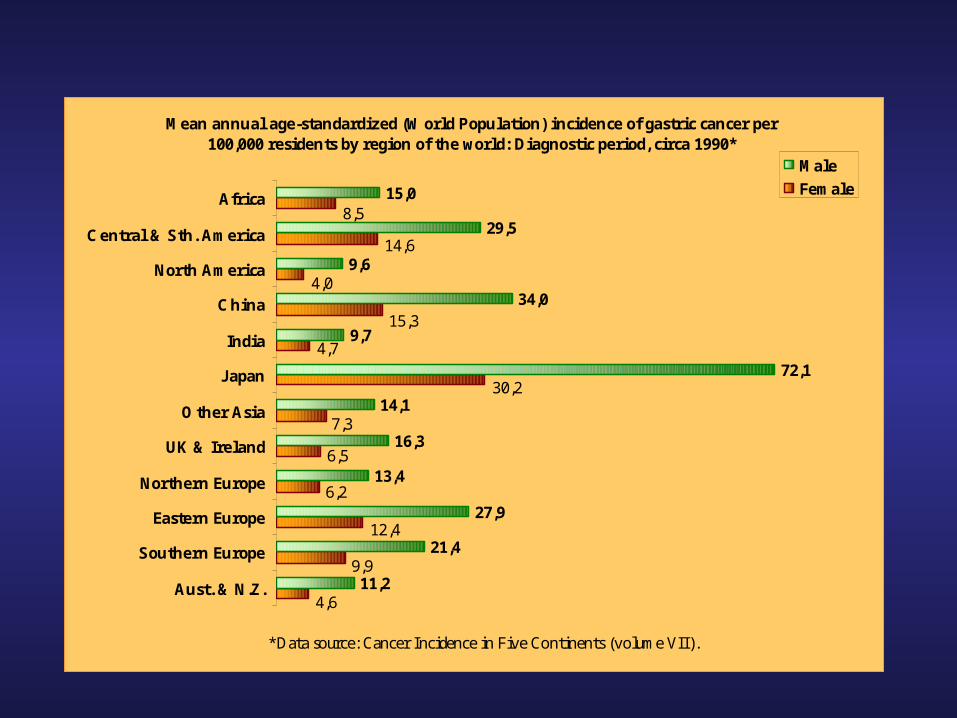
Mean annual age-standardized (World Population) incidence of gastric cancer per 100,000 residents by region of the world: Diagnostic period, circa 1990*
11,2
21,4
27,9
13,4
16,3
14,1
72,1
9,7
34,0
9,6
29,5
15,08,5
14,6
4,0
4,6
9,9
12,4
6,2
6,5
7,3
30,2
4,7
15,3
Aust. & N.Z.
Southern Europe
Eastern Europe
Northern Europe
UK & Ireland
O ther Asia
Japan
India
China
North America
Central & Sth. America
Africa
*Data source: Cancer Incidence in Five Continents (volume VII).
Male
Female

Incidence of gastric cancer in Europe
(average annual incidence per 100,000)
UK 24.8
France 18.2
Germany 29.9
Spain 23.3
Italy 30.2
The Netherlands 22.3

Gastric cancer
still a problem in Europe
And in Italy?

Torino #
Genova
Varese
Veneto*
Parma
Modena
Romagna
Firenze
Latina
Ragusa
0 5 10 15 20 25 30
%
AGE STANDARDIZED 5-YEARSRELATIVE SURVIVAL 1986-1989
Determination of prevalenceMales and females combined
Torino
Genova
Varese
Veneto
Parma
Modena
Romagna
Firenze
Latina
Ragusa
0 5 40 60 80
Rate per 100,000
CRUDE INCIDENCE 1988-1992

1993-95. Incidenza proporzionale per le prime dieci sedi tumorali
Uomini162 - polmone
188 - vescica
185 - prostata
151 - stomaco
153 - colon
155 - fegato
154 - retto
189 - rene e vene urinarie
157 - pancreas
200/2 - linfomi non Hodgkin
18.8%
10.9%
9.7%
9.4%
9.3%
6.0%
4.6%
3.6%
3.4%
3.1%

174 - mammella
153 - colon
151 - stomaco
182 - utero corpo
162 - polmone
200/2 - linfomi non-Hodgkin
154 - retto
183 - ovaio
188 - vescica
157 - pancreas
26.6%
8.5%
8,4%
6.2%
4.6%
4.1%
3.9%
3.9%
3.6%
3.6%
1993-95. Incidenza proporzionale per le prime dieci sedi tumorali
Donne
1993-95. Incidenza proporzionale per le prime dieci sedi tumorali
Donne
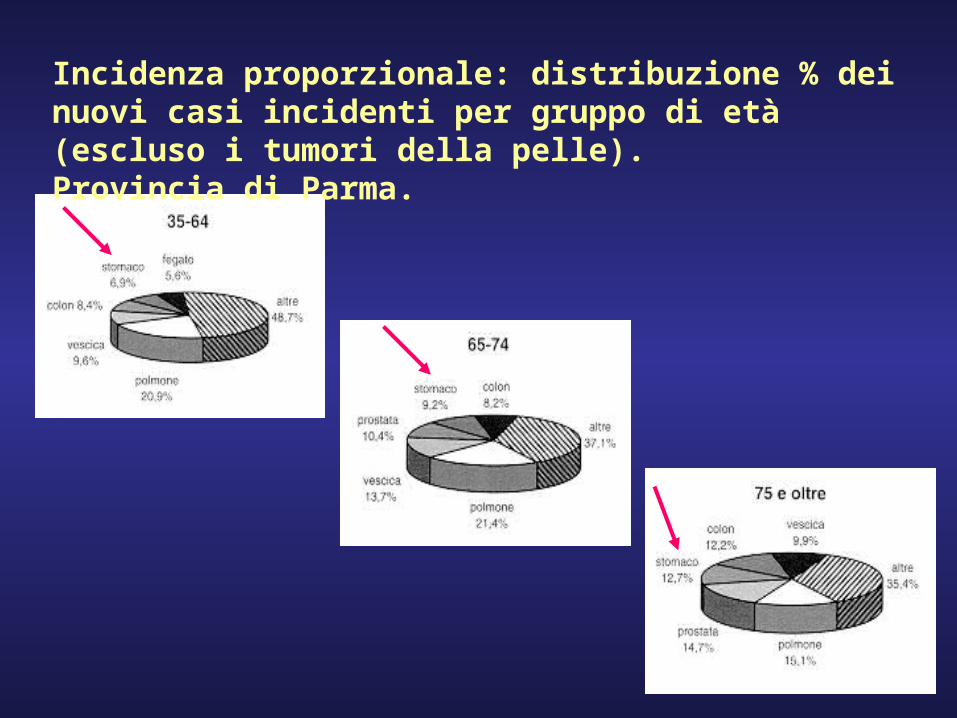
Incidenza proporzionale: distribuzione % dei nuovi casi incidenti per gruppo di età (escluso i tumori della pelle). Provincia di Parma.
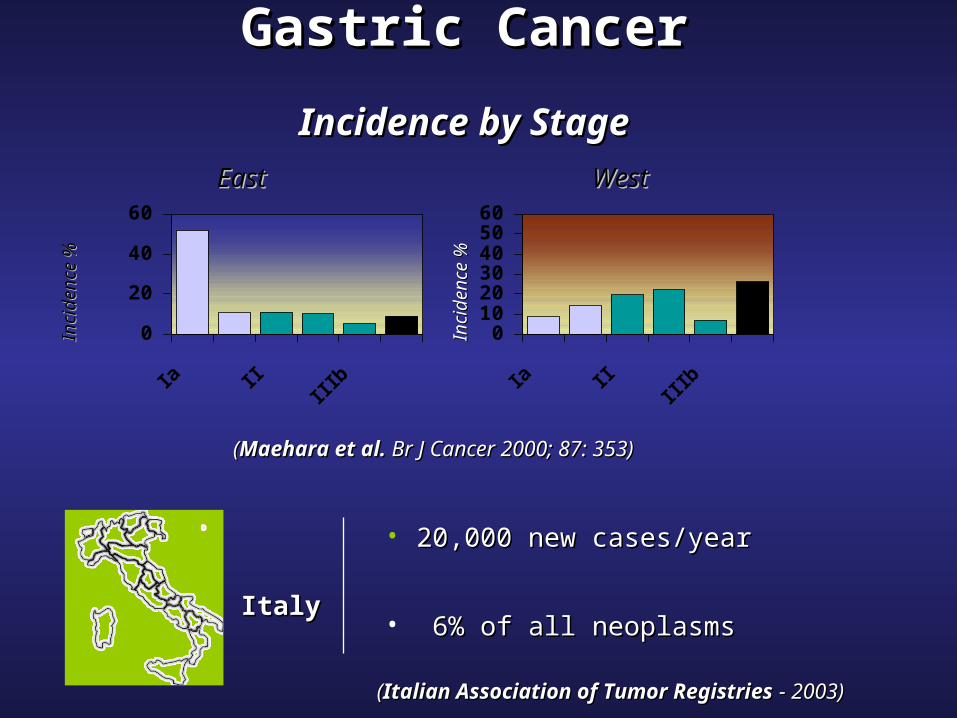
Gastric CancerGastric Cancer
Incidence by StageIncidence by Stage
• 20,00020,000 new cases/yearnew cases/year
• 6% of all neoplasms6% of all neoplasms
Inci
dence
%In
c idenc e
%
((Maehara et al. Maehara et al. Br J Cancer 2000; 87: Br J Cancer 2000; 87: 353)353)
ItalyItaly
0102030405060
Inci
dence
%In
c idenc e
%
EastEast WestWest
((Italian Association of Tumor RegistriesItalian Association of Tumor Registries - - 2003)2003)
0
20
40
60

Gastric cancer in Italy
5 years 20,000 cases/yearly survival
•25% inoperable at diagnosis (5,000)•15% inoperable at laparotomy (3,000) 0%•15% palliative surgery (3,000)
•45% radical surgery (9,000) 20-30%

5-YEAR OVERALL SURVIVALFOR CANCER TYPE
(Diagnosed between 1985-1989)
CANCER 2000
CANCER 5-YEAR OS RR EUROCARE SEER
GASTRIC 21.1 19.4 0.95
NON HODGKIN 46.7 50.3 1.11
HODGKIN 71.7 74.9 1.15
CERVIX 61.8 66.1 1.16
LUNG 9.1 13.0 1.17
OVARIAN 32.9 39.5 1.20
COLON 46.8 60.2 1.49
RECTUM 42.7 57.31.52
ENDOMETRIAL 73.2 83.2 1.69
BREAST 72.5 82.4 1.75
MELANOMA 76.0 86.1 1.84
PROSTATE 55.7 81.4 2.84
Gastric cancer
• How can we improve survival?
• Radically resected, high risk gastric canceradjuvant therapy
• Locally advanced unresectable diseasepreoperative
chemotherapy• Advanced disease
palliative chemotherapy

CARCINOMA GASTRICO AVANZATO

Sopravvivenza a due anni < 10 %Sopravvivenza a due anni < 10 %
Risposte complete 10 – 12 %Risposte complete 10 – 12 %
Sopravvivenza medianaSopravvivenza mediana 7–11 7–11
mesimesiCutsem E. et al – Cutsem E. et al – The Oncologist The Oncologist 2004 2004
Leinchman L. et al – Leinchman L. et al – Am Soc Clin OncolAm Soc Clin Oncol 1997 1997
Negli stadi avanzatiNegli stadi avanzati la la chemioterapia è limitata da chemioterapia è limitata da basso tasso di risposte, da basso tasso di risposte, da
breve durata della risposta e breve durata della risposta e da tossicità considerevoleda tossicità considerevole
Cutsem E. et al – Cutsem E. et al – The Oncologist The Oncologist 2004 2004

Carcinoma gastrico avanzatoChemioterapia vs terapia di supporto
Autore Schema N° Paz Sopr. mediana
•Pyrrhonen FEMTX 21 12.3supporto 20 3.1
•Murad FAMTX 30 9.0supporto 10 3.0
•Glimelius ELF 31 12supporto 30 4.0
Does chemotherapy prolong survival in locally advanced/metastatic gastric cancer?
• Phase II/III study – 497 patients with unresectable gastric cancer treated
with different chemotherapy regimens• Objective Response in 127(26%)• 39 (8%) pts survived longer than 2 years• 9 (2%) pts survived longer than 5 years
M. Yoshida, ASCO 2001, Abst 652
Conclusions
• Chemotherapy offers some hope of long-term survival
• Objective Response, good PS and prior gastrectomy are prognostic favourable factors
M. Yoshida, ASCO 2001, Abst 652

Carcinoma gastrico avanzatoChemioterapia dalla 1° alla 3° generazione
•Autore n° paz schema sopr. Mediana
•Wills 213 FAM 7FAMTX 10
•Webb 274 FAMTX 5.7ECF 8.9
•Vanhoefer 400 FAMTX 6.7FP 7.2
ELF 7.2•Ross 580 ECF 9.4
MCF 8.8

PELF vs. FAMTX in Metastatic Gastric Cancer
• GOIRC study on 195 patients– 98 received the PELF regimen – 97 the FAMTX scheme
• CR: PELF 13% vs FAMTX 2% (P=0.003)• PR: PELF 38% vs. FAMTX 21% (P=0.009)• No difference in TTP, duration of response or
median survival• Nausea/vomiting and diarrhea significantly
more severe with PELF; mucositis more severe with FAMTX
G. Cocconi, ASCO 2001, abst 501

Past first-line options
• FAMTX (5-FU/Doxorubicin/sequential high-dose methotrexate): response rates from 30% to 60%, median survival from 7 to 9 months (phase II studies)
• ELF (Etoposide/Folinic Acid/5-FU): RR from 27% to 53%, MS from 7.1 to 11.5 months (phase II studies)
• FUP (5-day infusion of 5-FU, Cisplatin): RR from 41% to 43%, MS from 9.0 to 10.6 (phase II studies)
ELF vs. FUP vs FAMTX (EORTC)
• Phase III randomized multicentric study – 399 eligible patients– 65 (16%): locally advanced disease– 334 (84%): metastatic disease– Intestinal and diffuse types were the most frequent
histological diagnoses– 245 patients had measurable disease and were
evaluable for response
Udo Vanhoefer JCO, Vol 18, Issue 14 (July), 2000: 2648-2657

Results
• No significant differences in overall Response Rate:– 9% with ELF, 20% with FUP, 12% with FAMTX
• No significant differences in Median Survival:– 7.2 months with ELF, 7.2 months with FUP, 6.7
months with FAMTX
Udo Vanhoefer JCO, Vol 18, Issue 14 (July), 2000: 2648-2657

• All three investigated regimens demonstrate modest clinical efficacy
• They should not be regarded as standard
treatment for advanced gastric cancer
Udo Vanhoefer JCO, Vol 18, Issue 14 (July), 2000: 2648-2657
Conclusions

R e g i m iR e g i m i C o m m e n t iC o m m e n t iFAMFAM(5-FU – Adriamicina – Mit C)(5-FU – Adriamicina – Mit C)
vecchio regime, ormai abbandonatovecchio regime, ormai abbandonato
FAMTXFAMTX(5-FU – Adriamicina – MTX)(5-FU – Adriamicina – MTX)
standard europeo, abbastanza tossicostandard europeo, abbastanza tossico
FUPFUP(5-FU – Cisplatino)(5-FU – Cisplatino)
considerato come lo standard considerato come lo standard americanoamericano
EAPEAP(Etoposide – Adriamicina – Cispl.)(Etoposide – Adriamicina – Cispl.)
regime tedesco, tossico, abbandonatoregime tedesco, tossico, abbandonato
EFLEFL(Etoposide – 5-FU – Ac.Fol)(Etoposide – 5-FU – Ac.Fol)
regime ancora utilizzato da qualche regime ancora utilizzato da qualche centrocentro
ECFECF(Epirubicina – Cisplatino – 5-FU)(Epirubicina – Cisplatino – 5-FU)
considerato come lo standard considerato come lo standard europeo; buon profilo di tossicitàeuropeo; buon profilo di tossicità
EMFEMF(Epirubicina – Mit C – 5-FU)(Epirubicina – Mit C – 5-FU)
ECF modificato, facile da ECF modificato, facile da somministraresomministrare
PELFPELF(Cisplatino – epirubicina – 5-FU)(Cisplatino – epirubicina – 5-FU)
regime intensivo italiano, necessita di regime intensivo italiano, necessita di GCSFGCSF
PLFPLF(Cisplatino – 5-FU – Ac.Fol)(Cisplatino – 5-FU – Ac.Fol)
regime tedesco, alte dosi settimanali di 5-FU regime tedesco, alte dosi settimanali di 5-FU i.c. di 24 ore; apparentemente ben tolleratoi.c. di 24 ore; apparentemente ben tollerato
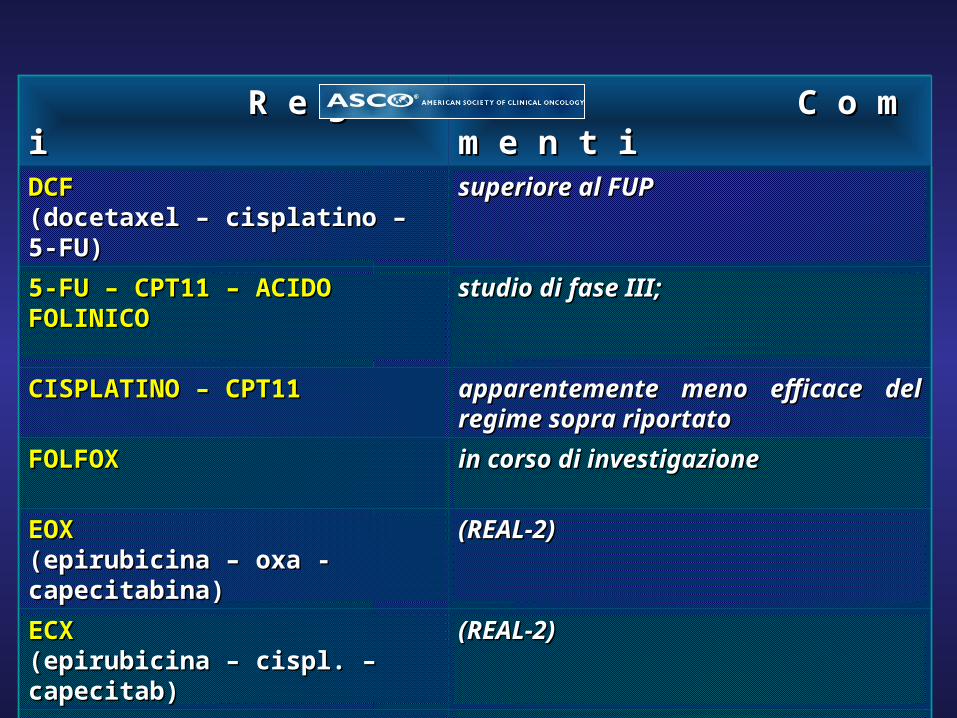
R e g i m iR e g i m i C o m m e n t iC o m m e n t iDCFDCF(docetaxel – cisplatino – 5-FU)(docetaxel – cisplatino – 5-FU)
superiore al FUPsuperiore al FUP
5-FU – CPT11 – ACIDO FOLINICO5-FU – CPT11 – ACIDO FOLINICO studio di fase III; studio di fase III;
CISPLATINO – CPT11CISPLATINO – CPT11 apparentemente meno efficace del apparentemente meno efficace del regime sopra riportatoregime sopra riportato
FOLFOXFOLFOX in corso di investigazionein corso di investigazione
EOXEOX(epirubicina – oxa - capecitabina)(epirubicina – oxa - capecitabina)
(REAL-2)(REAL-2)
ECXECX(epirubicina – cispl. – capecitab)(epirubicina – cispl. – capecitab)
(REAL-2)(REAL-2)
EOFEOF(epirubicina – oxa – 5-FU)(epirubicina – oxa – 5-FU)
(REAL-2)(REAL-2)

Today a standard-of-care regimen does not exist
ECF standard of care?
• The UK study showed a response and survival advantage with the ECF regimen as compared with FAMTX
• Median Survival remains low (8.7 months)
• Recent Italian trial: lower RR for ECF (36%) in a confirmatory phase II study (Aitini E, Tumori 87(1):20-4, 2001)
J Ajani
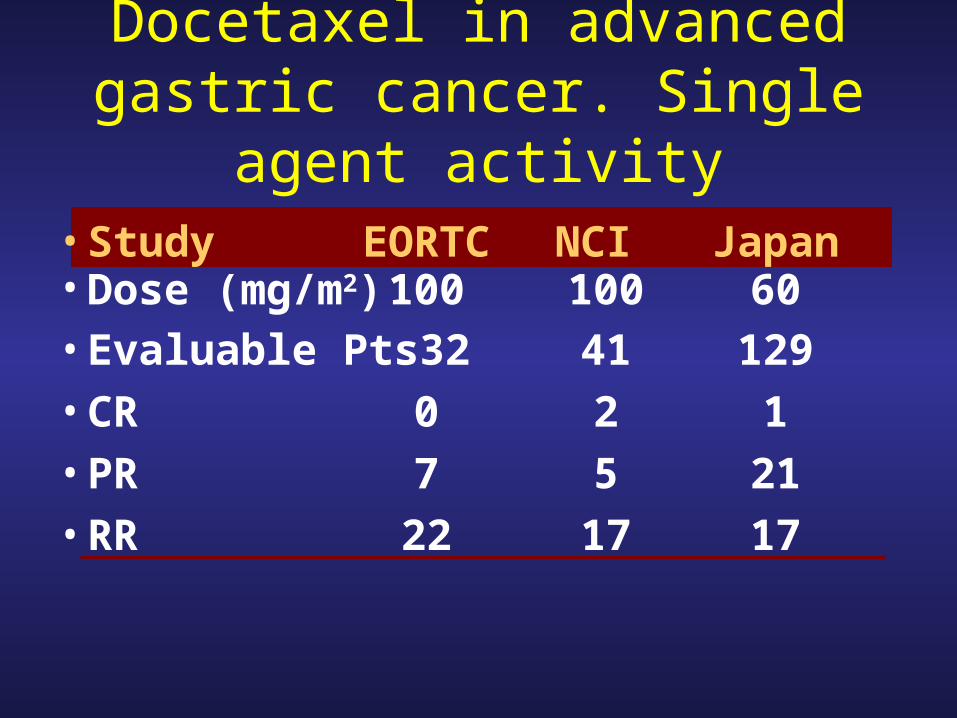
Docetaxel in advanced gastric cancer. Single agent activity
• Study EORTC NCI Japan• Dose (mg/m2) 100 100 60• Evaluable Pts 32 41 129
• CR 0 2 1
• PR 7 5 21
• RR 22 17 17

Docetaxel as a single agent: phase II trials
•Authors previous Dose N RRCT (mg/m2) elig/eval % (CI)
•Sulkes 1994 N 100 37/33 24 (9-39)
•Einzig 1995 N 100 41/36 17 (8-30)
•Vanhoefer 1999Y 100 27/25 20 (7-41)
•Mavroudis 1999N 100+G-CSF 30/30 20 (6-34)
•Taguchi 1997 Y 60 57/45 22 (11-37)
Background
• Combination chemotherapy demonstrated survival advantage
over BSC (1, 2, 3)
• Taxotere monotherapy, ORR 19 - 24% (7, 8, 9)
• TCF selected over TC as experimental arm, based on the best
ORR in the phase II part, ORR 55% versus 31% (10)
• CF is the most widely assessed regimen with the most
reproducible efficacy results (4, 5, 6)
(1) Murad et al, Cancer 1994, (2) Pyrhonen et al, Br J Cancer 1995, (3) Glimelius et al, Ann Oncol 1997, (4) Kim et al, Cancer 1993, (5) Ohtsu et al, JCO 2003, (6) Dank et
al, GI ASCO 2005, (7) Sulkes et al, Br J Cancer 1994, (8) Einzig et al Med Oncol 1996, (9) Taguchi et al, Jpn J Cancer Chemother 1998, (10) Ajani et al, JCO 2005,

RANDOMIZE
Taxotere 75 mg/m2 IV over 1 hr, D1Cisplatin 75 mg/m2 IV over 1- 3 hrs, D1 5-FU 750 mg/m2/day by CIV over 5 days
Q3W 227 patients
Cisplatin 100 mg/m2 IV over 1-3 hrs, D1 5-FU 1000 mg/m2/day by CIV over 5 days
Q4W 230 patients
• Measurable or evaluable
metastatic or measurable
locally recurrent gastric
adenocarcinoma • Age 18 years old• KPS > 70• Adequate hematological
and biochemical parameters• Signed written informed
consent
Stratification factors:
• Liver involvement, prior gastrectomy, measurable/evaluable disease, weight loss in prior 3 months, center
Tumor assessments planned every 8 weeks in both arms
Phase III Study Design (n=457)
Treatment until PD, consent withdrawn or unacceptable toxicity
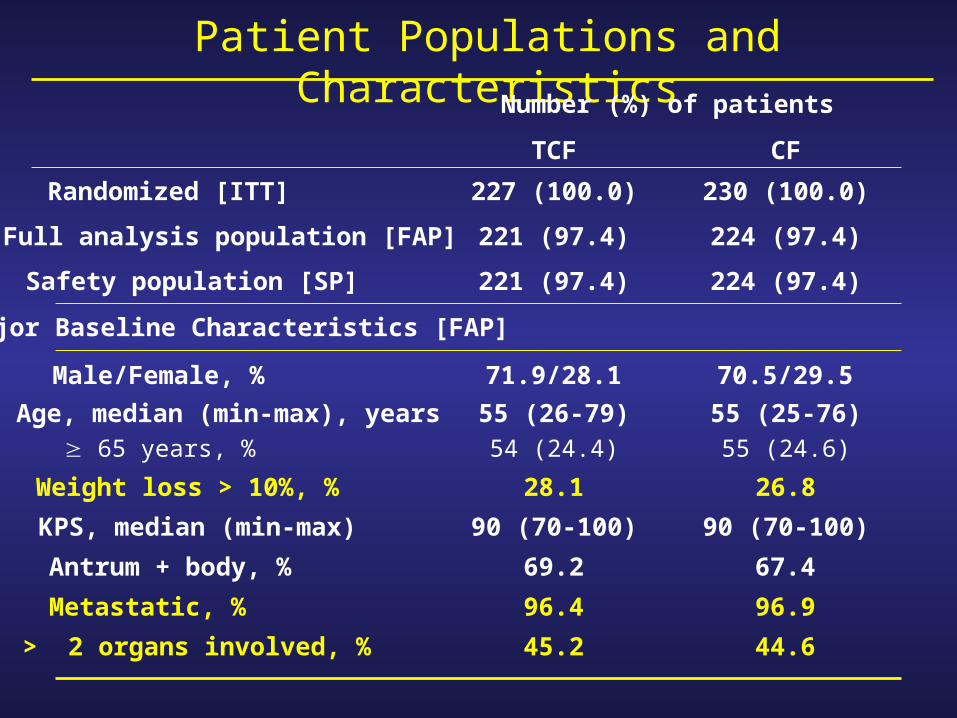
Patient Populations and CharacteristicsNumber (%) of patients
TCF CF
Male/Female, % 71.9/28.1 70.5/29.5
Age, median (min-max), years 65 years, %
55 (26-79)54 (24.4)
55 (25-76)55 (24.6)
Weight loss > 10%, % 28.1 26.8
KPS, median (min-max) 90 (70-100) 90 (70-100)
Antrum + body, % 69.2 67.4
Metastatic, % 96.4 96.9
> 2 organs involved, % 45.2 44.6
Randomized [ITT] 227 (100.0) 230 (100.0)
Full analysis population [FAP] 221 (97.4) 224 (97.4)
Safety population [SP] 221 (97.4) 224 (97.4)
Major Baseline Characteristics [FAP]

Study Endpoints
• Primary:– Time to tumor progression
• Secondary– Overall survival– Time to treatment failure– Overall response rate– Safety– Quality of life– Clinical benefit
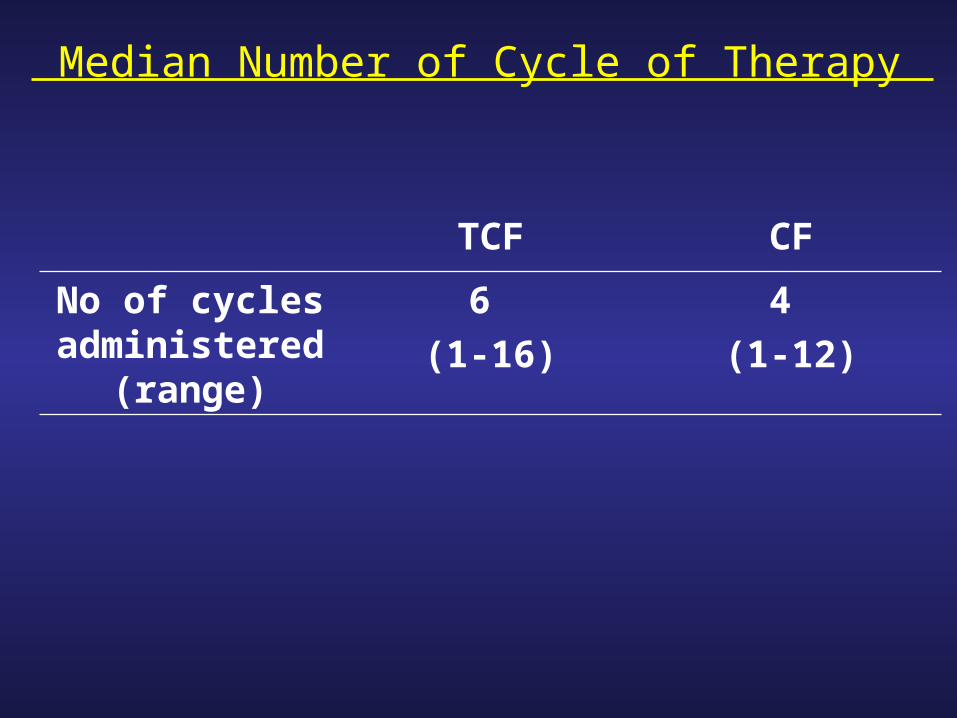
Median Number of Cycle of Therapy
TCF CF
No of cycles administered
(range)
6
(1-16)
4
(1-12)

TAX 325: Reasons for Treatment Discontinuation
TCF(n=221)
CF(n=224)
Disease progression 29.9% 43.8%
Adverse event 27.1% 25.0%
Death 10.4% 9.4%
Consent withdrawn 21.7% 11.6%
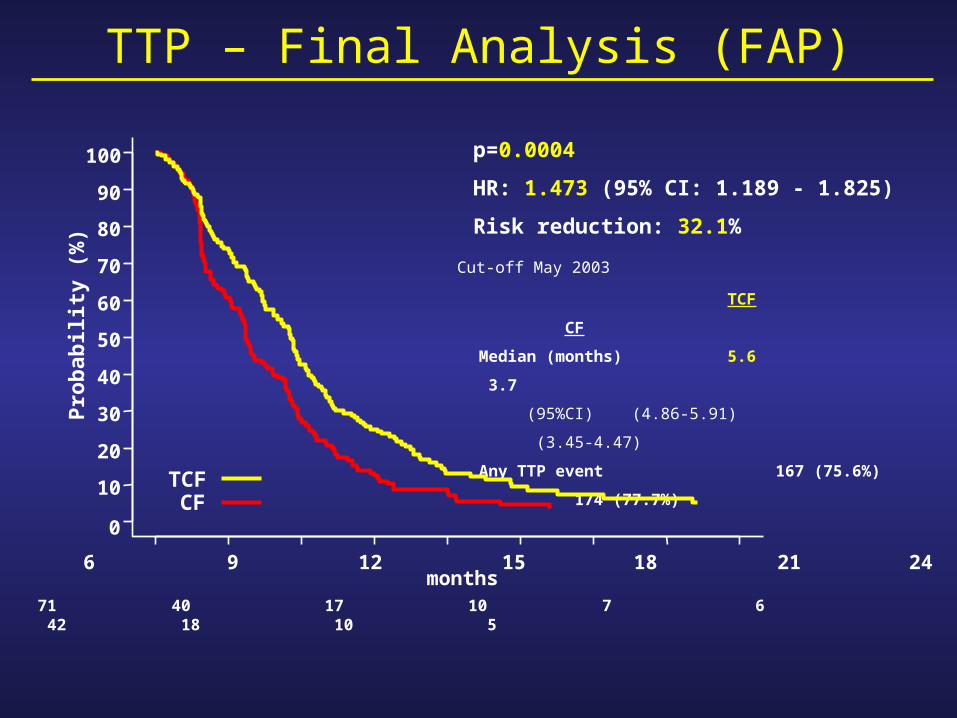
p=0.0004
HR: 1.473 (95% CI: 1.189 - 1.825)
Risk reduction: 32.1%
0 3 6 9 12 15 18 21 24 Patients at risk TCF: 221 148 71 40 17 10 7 6 CF: 224 119 42 18 10 5
months
Pro
bab
ility
(%
)
0
10
20
30
40
50
60
70
80
90
100
TCFCF
TCF CF
Median (months) 5.6 3.7
(95%CI) (4.86-5.91) (3.45-4.47)
Any TTP event 167 (75.6%) 174 (77.7%)
TTP – Final Analysis (FAP)
Cut-off May 2003

p=0.0201
HR: 1.293 (95% CI: 1.041 - 1.606)
Risk reduction: 22.7%
0 3 6 9 12 15 18 21 24 27 30 33 36 Patients at riskTCF: 221 199 149 93 68 45 36 28 22 17 12 7 5 CF: 224 195 136 87 54 35 17 11 8
months
Su
rviv
al P
rob
abili
ty (
%)
0
10
20
30
40
50
60
70
80
90
100
TCF CF
Median (months) 9.2 8.6
(95%CI) (8.38-10.58) (7.16-9.46)
Overall Survival- Final Analysis
One year survival 40.2% 31.6%
Two year survival 18.4% 8.8%
TCFCF
Cut-off May 2003
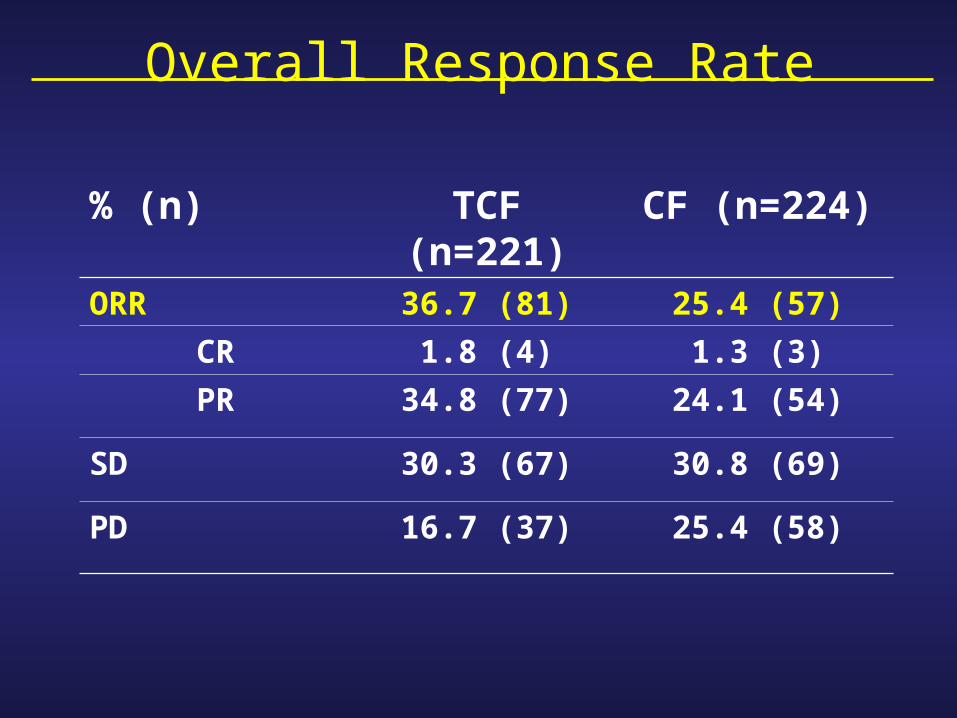
Overall Response Rate
% (n) TCF (n=221) CF (n=224)
ORR 36.7 (81) 25.4 (57)
CR 1.8 (4) 1.3 (3)
PR 34.8 (77) 24.1 (54)
SD 30.3 (67) 30.8 (69)
PD 16.7 (37) 25.4 (58)

Gr 3-4 Non-hematological Adverse Events (SP)
Data ordered by frequency of grade 3-4 in the TCF arm
Number (%) of patients
TCF (N=221) CF (N=224)
Lethargy 21.3 17.9
Stomatitis 20.8 27.2
Diarrhea 20.4 8.0
Infection 16.3 10.3
Nausea 15.8 18.8
Vomiting 14.9 18.8
Anorexia 13.1 11.6
Neuro-sensory 7.7 3.1
Venous 7.7 5.8Alopecia 5.0 1.3
At least one AE 81.4 75.4
In ≥ 5% of patients, regardless of relationship

Number (%) of patients
TCF CF
Hematological abnormalities (Grade 3-4)*
Neutropenia, %
Anemia, %
Thrombocytopenia, %
Febrile neutropenia or neutropenic infection, %
82.3
18.2
7.7
28.0
56.8
25.6
13.5
13.0
N=221 N=224
* Regardless of secondary prophylactic treatment, ** All causes Febrile neutropenia: grade 2 fever concomitant with grade 4 neutropenia Neutropenic infection: grade 2 infection concomitant with grade 3-4 neutropenia
10.4
3.6
8.5
5.4
Deaths during treatment**
( 30 days after last infusion)
Total toxic deaths
At least one SAEregardlessrelated
Hematology, SAE and Deaths (SP)
62.046.6
45.129.0

Use of G-CSF
TCF(n=221)
CF(n=224)
Percent of cycles with prophylactic G-CSF
10% 3.3%
NoG-CSF(n=219)
G-CSF(n=41)
NoG-CSF(n=222)
G-CSF(n=20)
Febrile neutropenia or neutropenic infection
28% 12% 13% 15%
In TAX325, only secondary prophylaxis with G-CSF was allowed per the study protocol.
Rationale for Assessing QoL and Clinical Benefit
Compared to best supportive care (BSC), polychemotherapy:
• Delays occurrence of symptoms (2)
• Improves quality of life (QoL) (2)
Few studies of QoL and almost none for Clinical Benefit
• ECF versus FAMTX (4): global QoL score better with ECF at 24
weeks (p=0.04)
• ECF versus MCF (5): some analyses showed QoL scores
maintained longer for ECF compared to MCF (global score,
physical, emotional and cognitive functioning, and pain)
(1) Murad et al, Cancer 1993, (2) Glimelius et al, Ann Oncol 1995, (3) Pyrhonen et al, Br J Cancer 1995, (4) Webb et al, J Clin Oncol 1997, (5) Ross et al, J Clin Oncol 2002

TAX325: Clinical Benefits and QoL Endpoints
Clinical Benefit Primary endpoint: Time to definitive worsening of Karnofsky performance status by one category compared with baseline.
Secondary endpoints : Time to definitive weight loss; Time to worsening of appetite; Pain free survival; Time to first cancer-pain related opioid
intake
QoL
•Primary endpoint: Time to definitive deterioration of 5% on the Global Health
Status (GHS) scale of EORTC QLQ-C30 compared with baseline.
• Secondary endpoints : Time to definitive deterioration of 10, 20 and 30%
on GHS; 5, 10, 20 and 30% on GHS subscales and on EUROQOL EQ-5D
visual analog scale (thermometer)
Analyses were performed in all randomized patients who received study drug
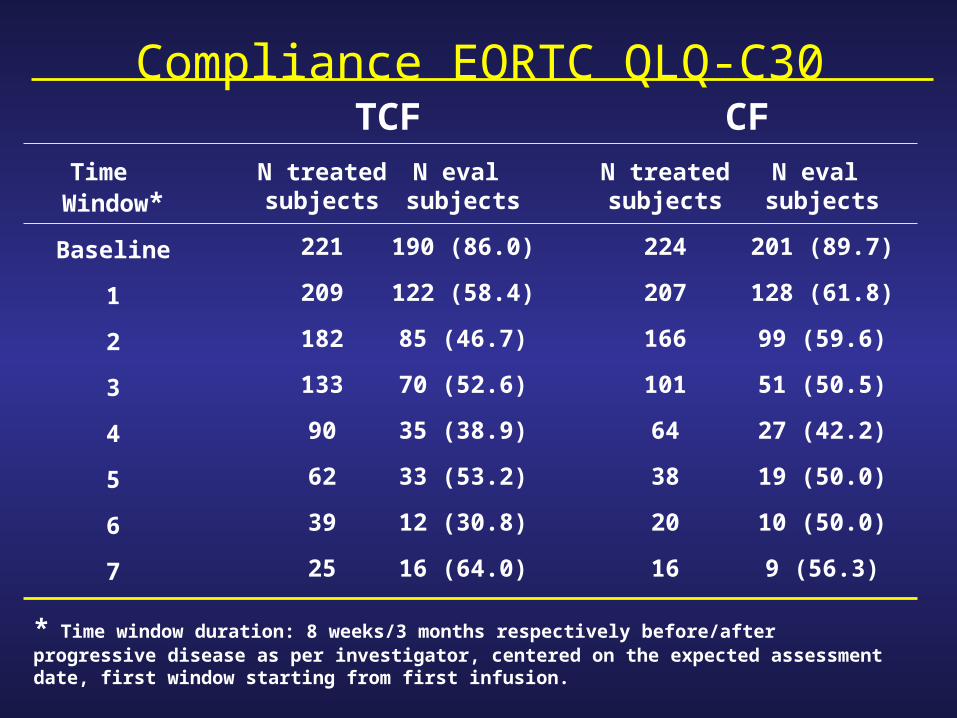
Compliance EORTC QLQ-C30
Time Window*
Baseline
1
2
3
4
5
6
7
N treatedsubjects
221
209
182
133
90
62
39
25
N eval subjects
190 (86.0)
122 (58.4)
85 (46.7)
70 (52.6)
35 (38.9)
33 (53.2)
12 (30.8)
16 (64.0)
N treatedsubjects
224
207
166
101
64
38
20
16
N eval subjects
201 (89.7)
128 (61.8)
99 (59.6)
51 (50.5)
27 (42.2)
19 (50.0)
10 (50.0)
9 (56.3)
TCF CF
* Time window duration: 8 weeks/3 months respectively before/after progressive disease as per investigator, centered on the expected assessment date, first window starting from first infusion.

Time to 5% Definitive Deterioration GHS
Log-rank p=0.0121
HR: 1.445 (95% CI: 1.082 - 1.929)
Risk reduction: 30.8%
TCF CF
Median (months) 6.5 4.2
(95%CI) (4.60-8.54) (3.71-5.39)
Events 85 (46%) 104 (52%)
0 3 6 9 12 15 18 21 24 27
Patients at riskTCF: 184 94 47 29 17 11 7 5 5 CF: 200 90 35 16 9 5
100
90
80
70
60
50
40
30
20
10
0
months
Pro
bab
ility
(%
)
TCFCF
QOL

QoL: Time to Definitive Deterioration
0.6 1 1.4 1.8 2.2 2.6
Hazard Ratio (>1 favors TCF)
QLQ-C30 Pain5%
10%
20%
30%5%
10%
20%
30%5%
10%
20%
30%
QLQ-C30 Nausea/Vomiting
EQ-5D Thermometer
0.6 1 1.4 1.8 2.2 2.6
Hazard Ratio (>1 favors TCF)
QLQ-C30 Global Health Scale5%
10%
20%
30%
5%
10%
20%
30%
5%
10%
20%
30%
5%
10%
20%
30%
QLQ-C30 Physical Functioning
QLQ-C30 Social Functioning
QLQ-C30 Appetite Loss

Time to Definitive Worsening KPS
Log-rank p=0.0088
HR: 1.379 (95% CI: 1.083 – 1.756)
Risk reduction: 27.5%
TCF CF
Median (months) 6.1 4.8
(95%CI) (4.99-7.75) (3.42-5.55)
Events 128 (58%) 141 (63%)
0 3 6 9 12 15 18 21 24 27
Patients at riskTCF: 220 137 76 42 24 12 9 8 6 CF: 224 111 50 21 9 6
100
90
80
70
60
50
40
30
20
10
0
months
Pro
bab
ility
(%
)
TCFCF
Clinical Benefit

Clinical BenefitHazard Ratio (>1 favors TCF)
Time to definitive worsening KPS (n=444)
Time to definitive 5% weight loss (n=444)
Time to definitive worsening appetite (n=425)
Pain-Free Survival (n=200)
Time to 1st cancer-pain related opioid (n=355)
0.4 0.8 1.2 1.6 2.0 2.4
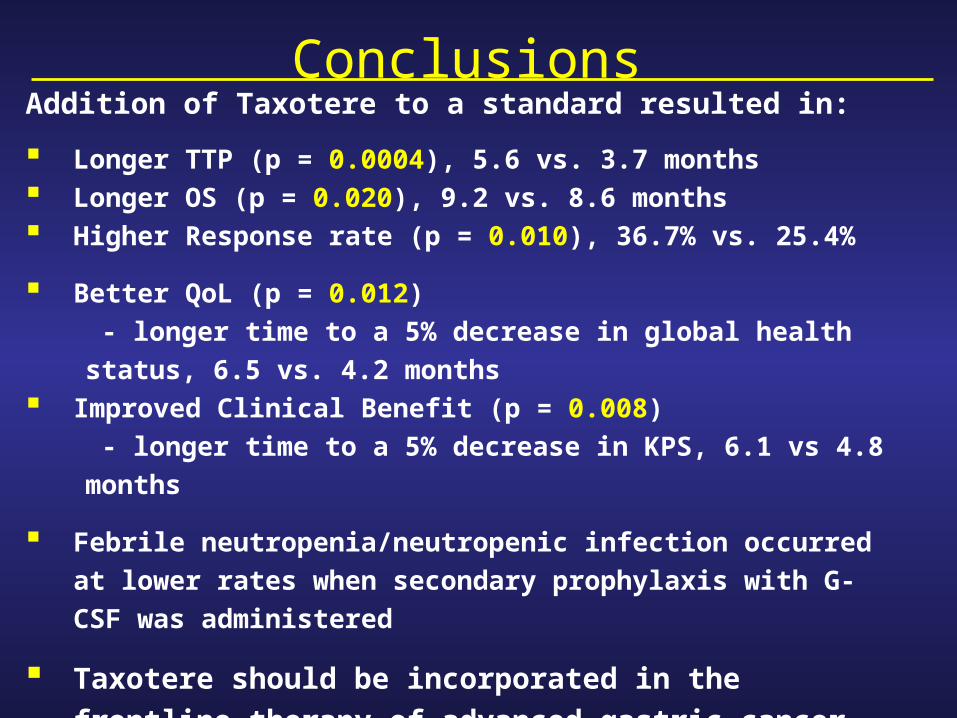
ConclusionsAddition of Taxotere to a standard resulted in:
Longer TTP (p = 0.0004), 5.6 vs. 3.7 months Longer OS (p = 0.020), 9.2 vs. 8.6 months Higher Response rate (p = 0.010), 36.7% vs. 25.4%
Better QoL (p = 0.012)
- longer time to a 5% decrease in global health status, 6.5 vs.
4.2 months Improved Clinical Benefit (p = 0.008)
- longer time to a 5% decrease in KPS, 6.1 vs 4.8 months
Febrile neutropenia/neutropenic infection occurred at lower
rates when secondary prophylaxis with G-CSF was
administered
Taxotere should be incorporated in the frontline therapy
of advanced gastric cancer and cancer of the GE junction

Overview of chemotherapy treatment in advanced gastric
cancer&
the Taxotere-Eloxatin combination rationale

Survival in patients with advanced gastric cancer: conventional regimens
Best supportive careBest supportive care
5-FU monotherapy5-FU monotherapy
FAMFAM
FAMTXFAMTX
ECF and CFECF and CF
3–4 months3–4 months3–4 months3–4 months
44––5 months5 months44––5 months5 months
44––5 months5 months44––5 months5 months
66––8 months8 months66––8 months8 months
88––9 months9 months88––9 months9 months
Median OSMedian OS
New agents in advanced gastric cancer
• Oxaliplatin
• Docetaxel
• Irinotecan
• Oral fluoropyrimidines
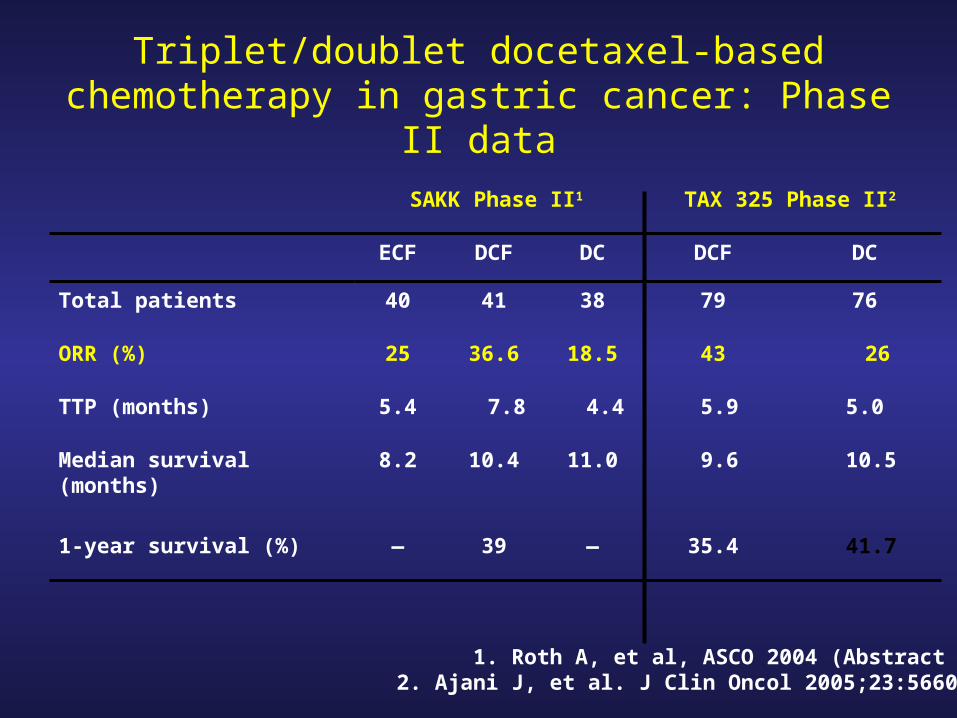
Triplet/doublet docetaxel-based chemotherapy in gastric cancer: Phase II data
41.735.4—39—1-year survival (%)
10.5 9.611.010.48.2Median survival (months)
5.0 5.9 4.4 7.85.4TTP (months)
264318.536.625ORR (%)
7679384140Total patients
DCDCFDCDCFECF
TAX 325 Phase II2SAKK Phase II1
1. Roth A, et al, ASCO 2004 (Abstract 4020).2. Ajani J, et al. J Clin Oncol 2005;23:5660–5667.

New combinations in Phase III trials
• CF vs IF (V306)• DCbF vs ECF• DS-1 vs S-1• ECF vs EOF vs EOX vs ECX (REAL-2)• CF vs DCF (TAX 325)• DC vs FLC (safety data only available)• CX vs CF (early efficacy data expected 2006)

Docetaxel plus S-1 in advancedgastric cancer: Phase III START trial
Docetaxel 40 mg/m2 onDay 1 plusS-1 80 mg/m2 on Days 1–14,q3w
S-1 80 mg/m2 on Days 1–28,q6w
Inoperable or relapsed advanced gastric/gastro-oesophageal cancer
Primary endpoint: overall survivalStudy start: February 2006
RR
n=628 patients(150 centres)

Advanced gastric cancer: summary
• Docetaxel is the first agent to demonstrate a significant survival benefit
– Docetaxel-based regimens are a standard
• Oxaliplatin-based regimens have demonstrated promising activity and a favourable safety profile
– Potential replacement for cisplatin
• Further development of various triplet combinations is needed
– Oral 5-FU agents
– Biologic agents
The potential of the oxaliplatin–docetaxel
combination
Chemotherapy in patients with advanced gastric cancer: conventional regimens
• Conventional chemotherapeutic regimens– Prolong survival– Have a high response rate
But…– Complete response rate is low– Response duration is short– Regimens may be toxic
Docetaxel–oxaliplatin: rationale• Distinct and complementary mechanisms of
action• Lack of cross-resistance• Different toxicity profiles• Favourable tolerability profiles• Both agents can be used in combination with
other chemotherapeutic agents• Both agents are active in advanced gastric
cancer
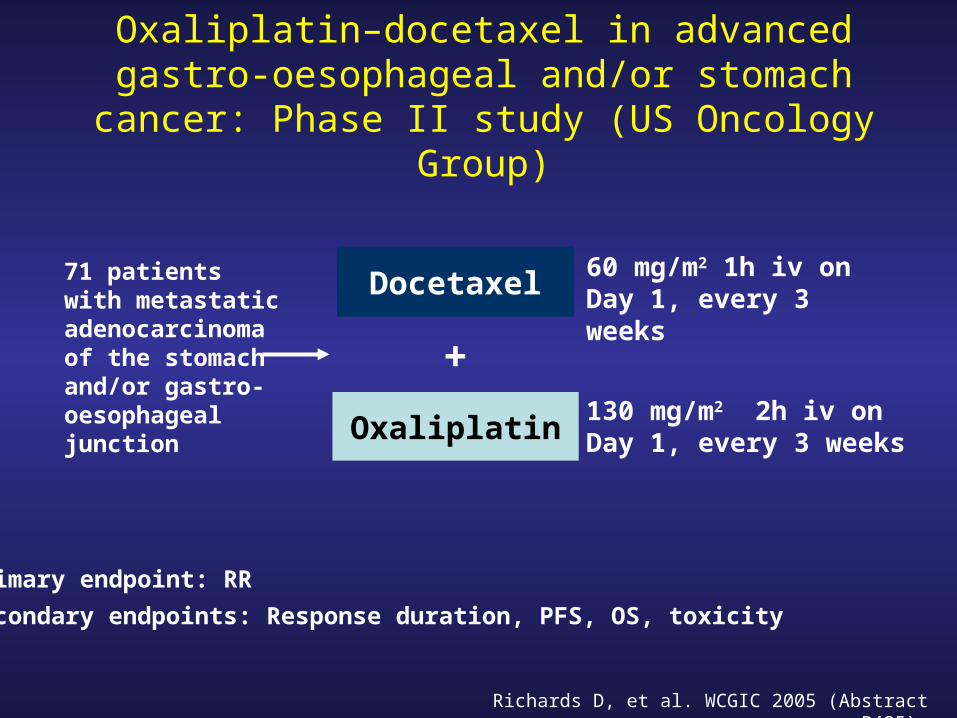
Oxaliplatin–docetaxel in advanced gastro-oesophageal and/or stomach cancer: Phase II
study (US Oncology Group)
Docetaxel71 patients with metastatic adenocarcinoma of the stomach and/or gastro-oesophageal junction
Primary endpoint: RR
Secondary endpoints: Response duration, PFS, OS, toxicity
60 mg/m2 1h iv on Day 1, every 3 weeks
Oxaliplatin130 mg/m2 2h iv on Day 1, every 3 weeks
+
Richards D, et al. WCGIC 2005 (Abstract P425).
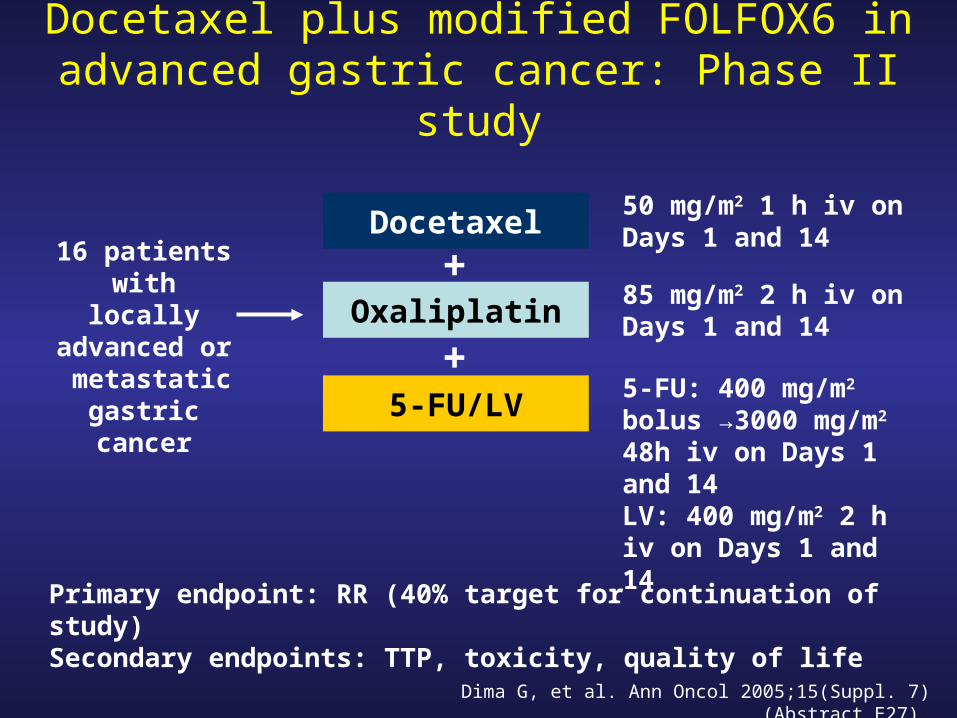
Docetaxel plus modified FOLFOX6 in advanced gastric cancer: Phase II study
Dima G, et al. Ann Oncol 2005;15(Suppl. 7) (Abstract E27).
Docetaxel16 patients with locally
advanced or metastatic
gastric cancer
Primary endpoint: RR (40% target for continuation of study)Secondary endpoints: TTP, toxicity, quality of life
50 mg/m2 1 h iv on Days 1 and 14
Oxaliplatin85 mg/m2 2 h iv on Days 1 and 14
+
5-FU/LV5-FU: 400 mg/m2 bolus →3000 mg/m2 48h iv on Days 1 and 14LV: 400 mg/m2 2 h iv on Days 1 and 14
+

Docetaxel plus modified FOLFOX6 in advanced gastric cancer: Phase II results
• Target therapeutic activity achieved:– RR 44% (PR 6, CR 1)
• Tolerability:– 3 patients had grade 2/3 leucopenia– No grade 4 leucopenia or thrombocytopenia– No febrile neutropenia– Non-haematological toxicities were mild to
moderate
Dima G, et al. Ann Oncol 2005;15(Suppl. 7) (Abstract E27).

Conclusions (I)
• Docetaxel improves patient survival when added to CF regimen
• Oxaliplatin is active in gastric cancer– Good response rate when combined with 5-
FU or to docetaxel/ epirubicin– Active in chemo-refractory patients

Conclusions (II)• Docetaxel–oxaliplatin is active in gastric cancer (first
and second line)• Docetaxel–oxaliplatin is safe
– Main toxicity is grade 3–4 haematological–Neutropenia (68%)–Febrile neutropenia (6%)
– Neurotoxicity and other non-haematological toxicities are uncommon
• Docetaxel–oxaliplatin is a promising new backbone for gastric cancer chemotherapy

Docetaxel-Cisplatin-5FU (TCF) versus
Docetaxel Cisplatin(TC) versus Epirubicin-Cisplatin-
5FU (ECF) as systemic treatment for advanced
gastric carcinoma (AGC): A randomized phase II
trial of the Swiss Group for Clinical Cancer
Research (SAKK)
A.D. Roth, R. Maibach, S. Falk, R. Stupp, P. Saletti, D. Köberle, M.M. Borner, H.P. Honegger, M. Leslie, N. Fazio
Gastric cancer
• Second most frequent cancer in the world• A majority of patients (in western
countries) present with advanced locoregional or metastatic disease
• Systemic therapy of advanced disease achieves shortlived responses translating in poor overall survival
• Need for new more efficient systemic regimens

Trial background
• ECF (epirubicin-cisplatin-5FU) currently considered by many as a standard regimen in advanced gastric cancer in Europe
• TC (docetaxel-cisplatin) and TCF (docetaxel-cisplatin-5FU) reported to be very active in this indication in previous phase I-II and II trials (Ann. Oncol 11; 301, 2000, Ann. Oncol 15; 759, 2004)
Trial objectives
• To evaluate the efficacity and tolerability of TC, TCF and ECF
• To assess TTF, TTP and OS of the three regimens respectively
• To select from TC and TCF the one which is more promising to be compared to ECF in future phase III trial

Trial design: randomized phase II
R
Advanced gastric cancer with measurable disease
Statification factors:- Center- Liver involvement- Performance status
A. ECF: - Epirubicin 50mg/m2 d1 - Cisplatin 60mg/m2 d1 - 5FU 200mg/m2/d in
continuousinfusion d1-21
B. TC: - Docetaxel 85*mg/m2 d1- Cisplatin 75mg/m2 d1
C. TCF: - Docetaxel 85*mg/m2 d1 - Cisplatin 75mg/m2 d1 - 5FU 300mg/m2/d in
continuous infusion d1-14
Each recycled q3w up to 8 cycles
* Docetaxel 75mg/m2 after first 21 patients
Eligibility criteria
• Locally advanced or metastatic gastric cancer with bidimensionally measurable lesions (≥10mm X 20mm on chest X-ray or ≥ 10mm X 10mm on CT-scan)
• PS 0 or 1• Life expectancy > 12 weeks• No previous palliative chemotherapy• Adequate hematology and biochemistry• Written informed consent
Trial endpoints
• Primary endpoint– Response rate
• Secondary endpoints– Toxicity– TTF– TTP– OS– QOL

Statistical considerations• Aim
Select the better of the two docetaxel-based regimens
• Selection criteriumResponse rate
• Probability of correct selectionIf the true absolute difference in response rate is at least 15%, then the probability of selecting the better treatment should be at least 90%
• Sample size37 patients per arm, total 111
Simon R. Cancer Treatment reports 69: 1375 - 1381 (1985)

Patient Characteristics (1)ECF TC
TCFn=40 n=38
n=41
• Age: median (range) 59 (32-71) 58 (40-70) 61 (35-78)
• Male 75% 76% 73%
• PS (0/1) 60/40% 61/39% 61/39%
• Median weight loss (3m) 2.5 Kg 4.0 Kg 3.5 Kg
• Appetite (good/fair) 48/35% 47/42% 46/36%
• Previous gastrectomy 18% 24% 32%
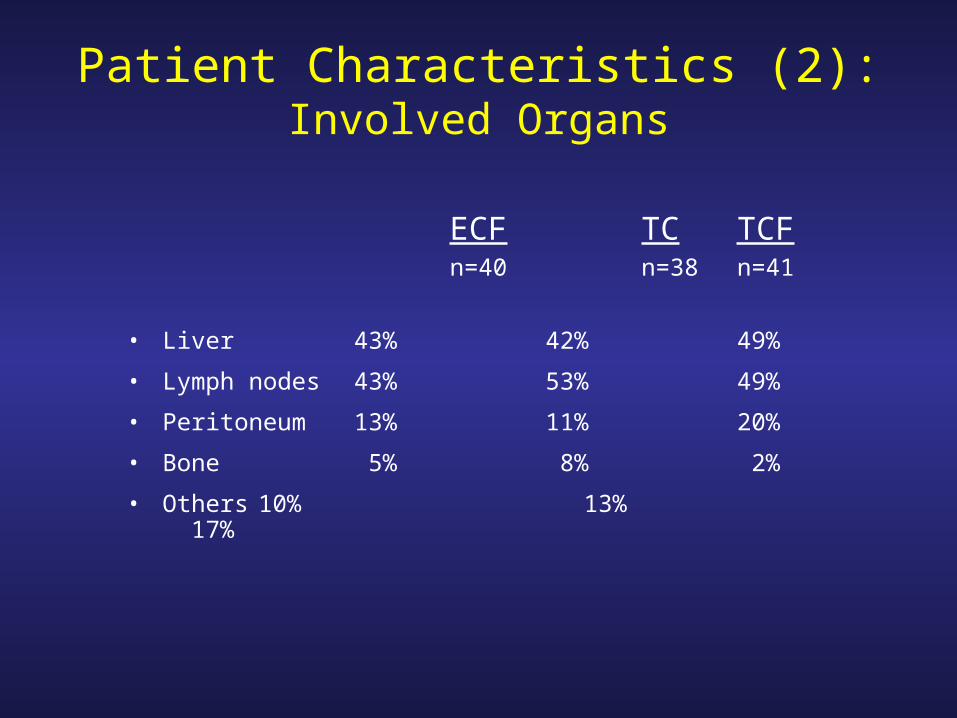
Patient Characteristics (2):Involved Organs
ECF TC TCFn=40 n=38 n=41
• Liver 43% 42% 49%
• Lymph nodes 43% 53% 49%
• Peritoneum 13% 11% 20%
• Bone 5% 8% 2%
• Others 10% 13% 17%


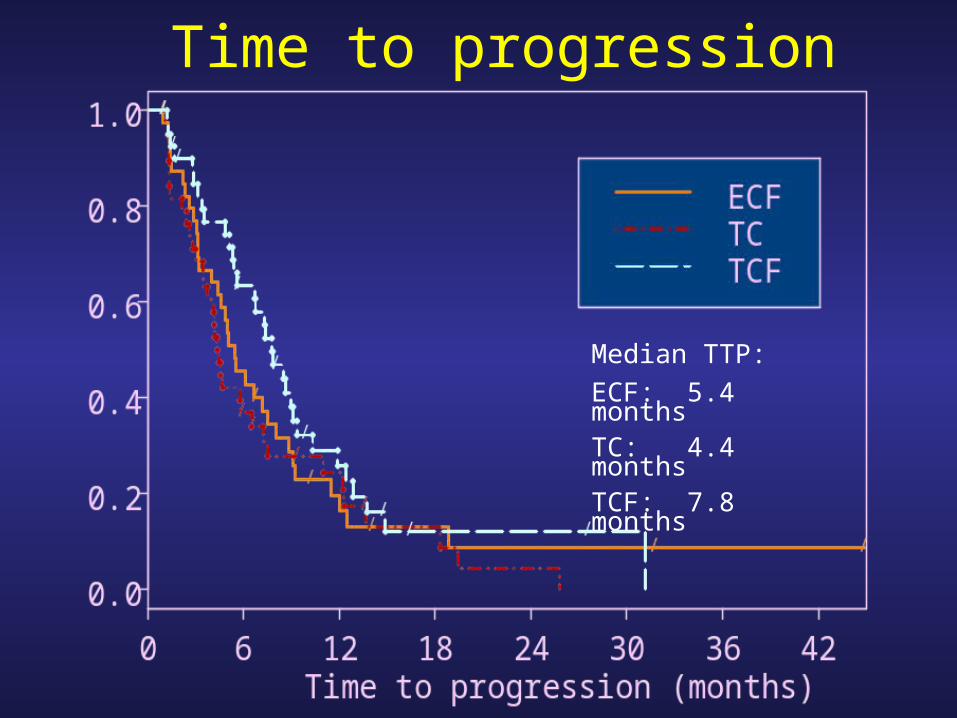
Time to progression
Median TTP:
ECF: 5.4 monthsTC: 4.4 monthsTCF: 7.8 months

Overall Survival
Median OS:
ECF: 8.2 monthsTC: 11.0 monthsTCF: 10.4 months
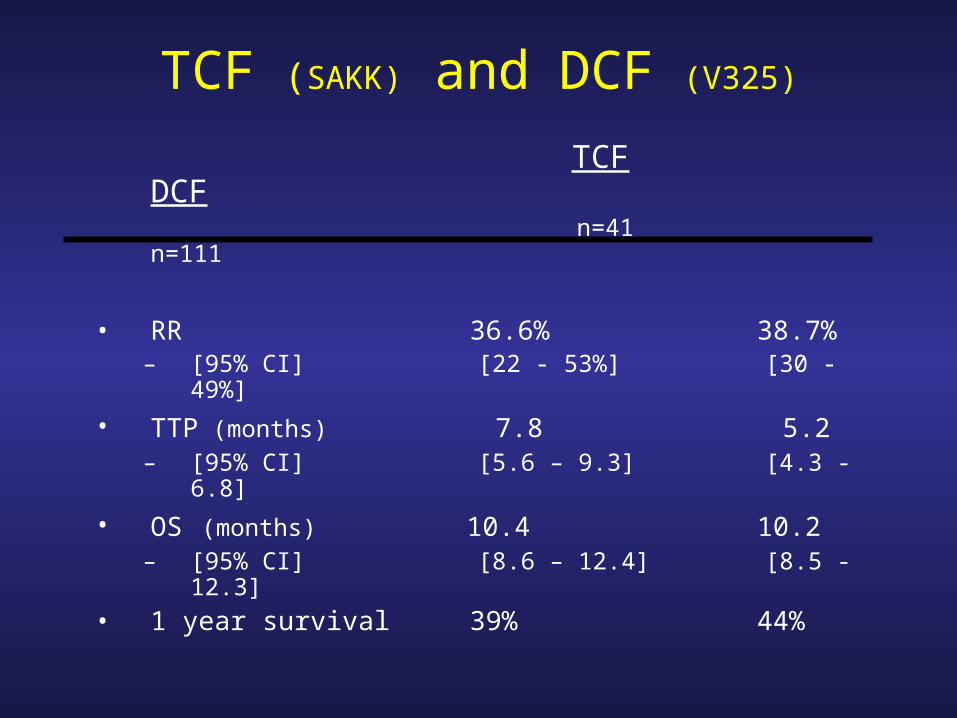
TCF (SAKK) and DCF (V325)
TCF DCF n=41 n=111
• RR 36.6% 38.7%– [95% CI] [22 - 53%] [30 -
49%]
• TTP (months) 7.8 5.2– [95% CI] [5.6 – 9.3] [4.3 -
6.8]
• OS (months) 10.4 10.2– [95% CI] [8.6 – 12.4] [8.5 -
12.3]
• 1 year survival 39% 44%

Conclusions
• Based on these RR data and on the original statistical assumptions, TCF can be considered to be more efficacious than TC, and should be preferred in future compative trials
• Docetaxel based regimens are more hematotoxic than ECF but are on the whole still relatively well tolerated
• Although there is a trend for TCF to be more efficacious than ECF in term of RR, median TTP and OS, formal comparison in a proper study is required
• The data of efficacy reported here with TCF are very similar to the data reported with DCF in 2003 (V325 phase III interim analysis, Ajani, J. ASCO proceedings 22, 249, abstr # 999)

UPFRONT ChemotherapyUPFRONT Chemotherapy
PRIMARYPRIMARY INDUCTIONINDUCTION NEOADJUVANTNEOADJUVANT
Chemotherapy for Chemotherapy for non curablenon curable patients patients
Chemotherapy for Chemotherapy for non resectablenon resectable patients patients
Chemotherapy for locally Chemotherapy for locally advancedadvanced resectableresectable
patientspatients
MAIN GOALMAIN GOAL MAIN GOALMAIN GOAL MAIN GOALMAIN GOAL
PALLIATIONPALLIATIONPATHOLOGIC PATHOLOGIC COMPLETE COMPLETE RESPONSE RESPONSE
RESECTIONRESECTION