csw nephrolithiasis pathway - seattlechildrens.org · this pathway was developed through local...
TRANSCRIPT
Diagnosis Confirmed: Proceed to
Urine analysis results on Confirmed
Phase
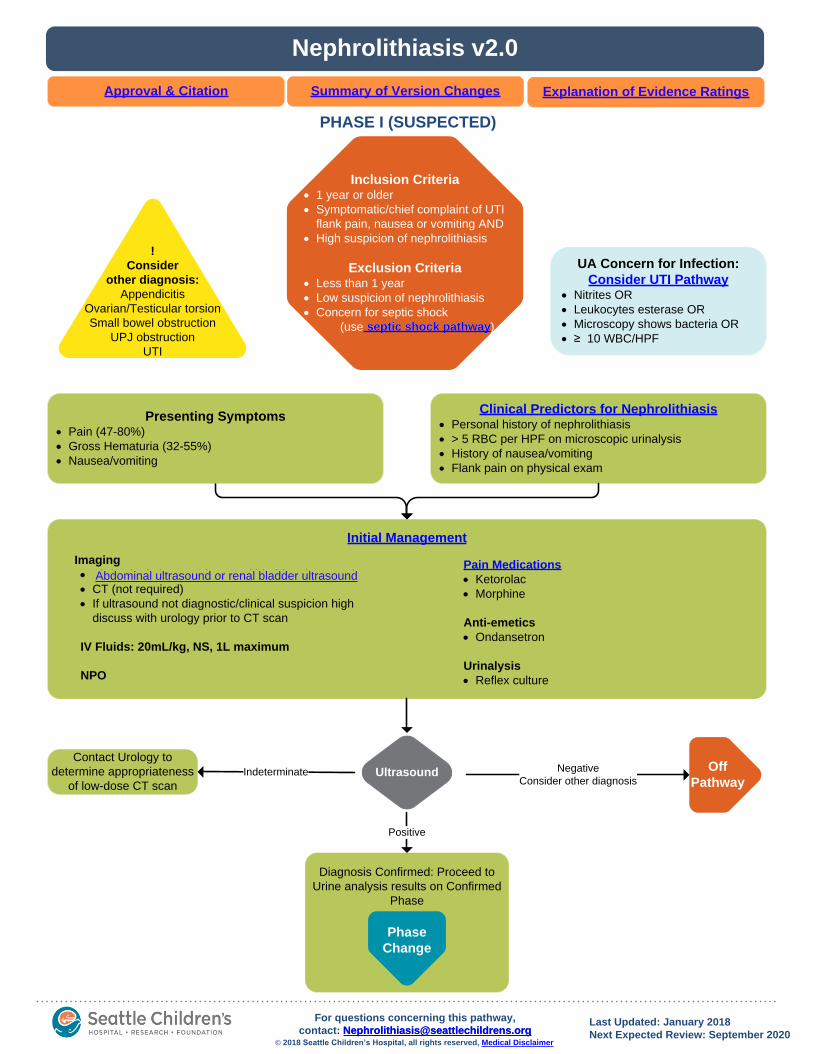
PHASE I (SUSPECTED)
Inclusion Criteria· 1 year or older
· Symptomatic/chief complaint of UTI
flank pain, nausea or vomiting AND
· High suspicion of nephrolithiasis
Exclusion Criteria· Less than 1 year
· Low suspicion of nephrolithiasis
· Concern for septic shock
(use septic shock pathway)
Nephrolithiasis v2.0
Explanation of Evidence RatingsSummary of Version Changes
Last Updated: January 2018
Next Expected Review: September 2020© 2018 Seattle Children’s Hospital, all rights reserved, Medical Disclaimer
For questions concerning this pathway,
contact: [email protected]
Approval & Citation
Initial Management
Pain Medications
· Ketorolac
· Morphine
Anti-emetics
· Ondansetron
Urinalysis
· Reflex culture
!
Consider
other diagnosis:
Appendicitis
Ovarian/Testicular torsion
Small bowel obstruction
UPJ obstruction
UTI
UA Concern for Infection:
Consider UTI Pathway· Nitrites OR
· Leukocytes esterase OR
· Microscopy shows bacteria OR
· ≥ 10 WBC/HPF
Imaging
· Abdominal ultrasound or renal bladder ultrasound
· CT (not required)
· If ultrasound not diagnostic/clinical suspicion high
discuss with urology prior to CT scan
IV Fluids: 20mL/kg, NS, 1L maximum
NPO
Presenting Symptoms· Pain (47-80%)
· Gross Hematuria (32-55%)
· Nausea/vomiting
Clinical Predictors for Nephrolithiasis· Personal history of nephrolithiasis
· > 5 RBC per HPF on microscopic urinalysis
· History of nausea/vomiting
· Flank pain on physical exam
Phase
Change
Ultrasound Indeterminate
Contact Urology to
determine appropriateness
of low-dose CT scan
Positive
Negative
Consider other diagnosis
Off
Pathway
Abdominal ultrasound or renal bladder ultrasound
septic shock pathway
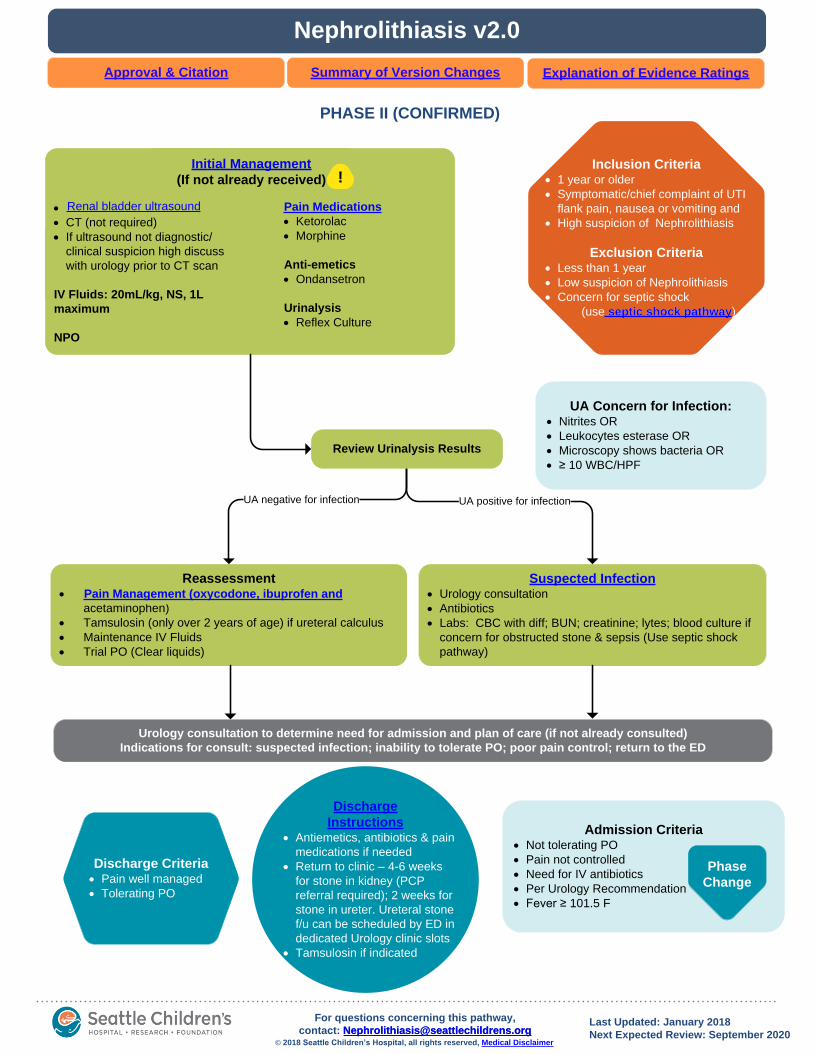
PHASE II (CONFIRMED)
Inclusion Criteria· 1 year or older
· Symptomatic/chief complaint of UTI
flank pain, nausea or vomiting and
· High suspicion of Nephrolithiasis
Exclusion Criteria· Less than 1 year
· Low suspicion of Nephrolithiasis
· Concern for septic shock
· (use septic shock pathway)
Nephrolithiasis v2.0
Approval & Citation
Admission Criteria· Not tolerating PO
· Pain not controlled
· Need for IV antibiotics
· Per Urology Recommendation
· Fever ≥ 101.5 F
Reassessment· Pain Management (oxycodone, ibuprofen and
acetaminophen)
· Tamsulosin (only over 2 years of age) if ureteral calculus
· Maintenance IV Fluids
· Trial PO (Clear liquids)
Urology consultation to determine need for admission and plan of care (if not already consulted)
Indications for consult: suspected infection; inability to tolerate PO; poor pain control; return to the ED
Suspected Infection· Urology consultation
· Antibiotics
· Labs: CBC with diff; BUN; creatinine; lytes; blood culture if
concern for obstructed stone & sepsis (Use septic shock
pathway)
Discharge Criteria· Pain well managed
· Tolerating PO
Initial Management
(If not already received)
Pain Medications
· Ketorolac
· Morphine
Anti-emetics
· Ondansetron
Urinalysis
· Reflex Culture
· Renal bladder ultrasound
· CT (not required)
· If ultrasound not diagnostic/
clinical suspicion high discuss
with urology prior to CT scan
IV Fluids: 20mL/kg, NS, 1L
maximum
NPO
UA Concern for Infection:· Nitrites OR
· Leukocytes esterase OR
· Microscopy shows bacteria OR
· ≥ 10 WBC/HPF
UA negative for infection UA positive for infection
Review Urinalysis Results
Phase
Change
Explanation of Evidence RatingsSummary of Version Changes
Discharge
Instructions· Antiemetics, antibiotics & pain
medications if needed
· Return to clinic – 4-6 weeks
for stone in kidney (PCP
referral required); 2 weeks for
stone in ureter. Ureteral stone
f/u can be scheduled by ED in
dedicated Urology clinic slots
· Tamsulosin if indicated
Renal bladder ultrasound
!
Pain Management (oxycodone, ibuprofen and
Last Updated: January 2018
Next Expected Review: September 2020© 2018 Seattle Children’s Hospital, all rights reserved, Medical Disclaimer
For questions concerning this pathway,
contact: [email protected] [email protected]
septic shock pathway
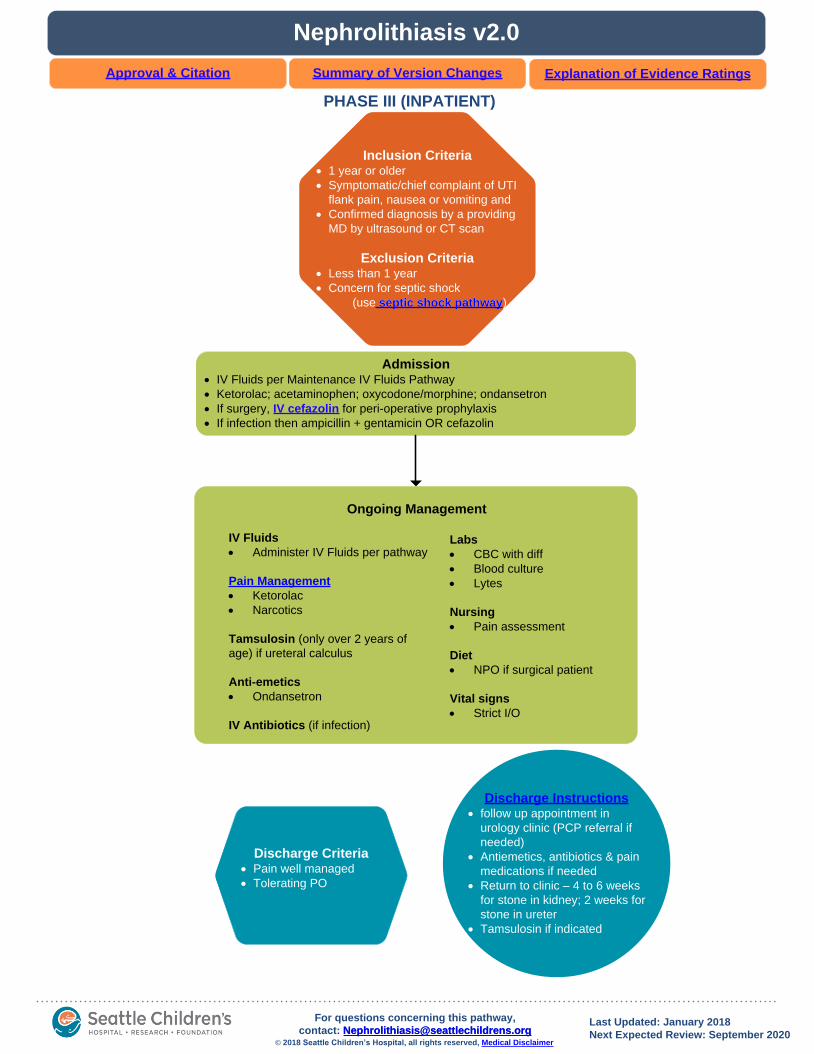
PHASE III (INPATIENT)
Nephrolithiasis v2.0
IV Fluids
· Administer IV Fluids per pathway
Pain Management
· Ketorolac
· Narcotics
Tamsulosin (only over 2 years of
age) if ureteral calculus
Anti-emetics
· Ondansetron
IV Antibiotics (if infection)
Labs
· CBC with diff
· Blood culture
· Lytes
Nursing
· Pain assessment
Diet
· NPO if surgical patient
Vital signs
· Strict I/O
Admission· IV Fluids per Maintenance IV Fluids Pathway
· Ketorolac; acetaminophen; oxycodone/morphine; ondansetron
· If surgery, IV cefazolin for peri-operative prophylaxis
· If infection then ampicillin + gentamicin OR cefazolin
Inclusion Criteria· 1 year or older
· Symptomatic/chief complaint of UTI
flank pain, nausea or vomiting and
· Confirmed diagnosis by a providing
MD by ultrasound or CT scan
Exclusion Criteria· Less than 1 year
· Concern for septic shock
· (use septic shock pathway)
Discharge Criteria· Pain well managed
· Tolerating PO
Discharge Instructions· follow up appointment in
urology clinic (PCP referral if
needed)
· Antiemetics, antibiotics & pain
medications if needed
· Return to clinic – 4 to 6 weeks
for stone in kidney; 2 weeks for
stone in ureter
· Tamsulosin if indicated
Ongoing Management
Explanation of Evidence RatingsSummary of Version ChangesApproval & Citation
Last Updated: January 2018
Next Expected Review: September 2020© 2018 Seattle Children’s Hospital, all rights reserved, Medical Disclaimer
For questions concerning this pathway,
contact: [email protected] [email protected]
septic shock pathway

Suspected Nephrolithiasis
• This phase is for patients without an imaging-confirmed diagnosis of
nephrolithiasis
• Clinical suspicion for nephrolithiasis should be high (see table below)
CLINICAL PREDICTORS FOR NEPHROLITHIASIS Odds Ratio
Personal history of nephrolithiasis OR 6.55
> 5 RBC per HPF on microscopic urinalysis OR 3.10
History of nausea/vomiting OR 2.39
Flank pain on physical exam OR 2.23
Persaud, Andre C., et al. "Pediatric urolithiasis: clinical predictors in the emergency
department." Pediatrics 124.3 (2009): 888-894.
Phase I (Suspected)
Imaging in Suspected Nephrolithiasis
Renal/Bladder Ultrasound is the recommend 1st line imaging study for children
with suspected nephrolithiasis (AUA1, ESPU2)
Urology on-call should be contacted to help guide ordering of CT in the following
situations:
•Negative ultrasound and very high suspicion of nephrolithiasis
•Hydronephrosis
•Twinkle artifact
•Ureteral dilation
1) Fulgham, Pat Fox, et al. "Clinical effectiveness protocols for imaging in the management of ureteral calculous disease: AUA
technology assessment." The Journal of urology 189.4 (2013): 1203-1213.
2) Riedmiller, H., P. Androulakakis, D. Beurton, R. Kocvara, and U. Köhl. "Guidelines on paediatric urology." European Association of
Urology (2005).
Phase I (Suspected) Phase II (Confirmed)
Phase I (Suspected) Phase II (Confirmed) Phase III (Inpatient)
Phase II (Confirmed)
Suspected Infection
• Fevers or urinalysis suspicious for infection (+ nitrates, bacteria or > 10
WBC/HPF) should prompt urological consultation and antibiotics
• Note: a completely obstructing ureteral calculus with a proximal infected
urinary system may present with a normal urinalysis; if clinical signs of
infection (i.e. high fever) and obstructing ureteral calculus is seen, these
patients should be treated as a suspected infection even in the absence of
abnormalities on the urinalysis
Phase III (Inpatient)
Pre- Operative Antibiotics
• Cefazolin or ampicillin + gentamicin are considered equal alternative 1st-line
pre-operative options according to AUA guidelines1
• Ampicillin + gentamicin should be considered when there is a history of
enterococcal or multi-drug resistant colonization/infection, or if there is a
high suspicion of current bacterial colonization
• Culture-directed peri-operative antibiotics should be utilized if a current
urine culture is available for review
Phase II (Confirmed) Phase III (Inpatient)
Follow Up
• Patients should receive education materials prior to discharge
• Patients with ureteral calculi:
• warrant shorter-interval follow-up, by 2 weeks, as they may be surgical
candidates if the calculus does not pass. Follow up for ureteral stones
only, can be scheduled by the ED in dedicated Urology follow up clinic
slots.
• Will need to strain their urine and watch for a passed calculus
Nephrolithiasis Citation & Approval
Return to Home
Approved by the CSW Nephrolithiasis Team for the September 29, 2015 go live.
CSW Nephrolithiasis Team:
Urology, Owner Jonathon Ellison, MD
Urology, Owner Paul Merguerian, MD, MS, FAAP
Urology, Stakeholder Thomas Lendvay, MD
Emergency Department, MD Russ Migita, MD
Emergency Department, CNS Sara Fenstermacher, RN
Clinical Pharmacy Eric Harvey, PharmD, MBA
Pharmacy Informatics Rebecca Ford, PharmD
Surgical Unit, CNS Kristine Lorenzo, RN
Urology Clinic Nurse Andrea Bakke, RN
Clinical Effectiveness Team:
Consultant Sara Vora, MD
Project Manager Jennifer Magin, MBA
CE Analyst Holly Clifton, MPH
CIS Informatician Mike Leu, MD, MS, MHS
Carlos Villavicencio, MD, MMI
CIS Analyst Heather Marshall
Librarian Sue Groshong, MLIS
Program Coordinator Asa Herrman
Executive Approval:
Sr. VP, Chief Medical Officer Mark Del Beccaro, MD
Sr. VP, Chief Nursing Officer Susan Heath, RN, MN, NEA-BC
Surgeon-in-Chief Bob Sawin, MD
Retrieval Website: http://www.seattlechildrens.org/pdf/nephrolithiasis-pathway.pdff
Please cite as:
Seattle Children’s Hospital, Ellison, J., Merguerian, P., Fenstermacher, S., Magin, J., Migita, R.,
Vora, S., 2015 September. Nephrolithiasis Pathway. Available from: http://www.seattlechildrens.org/
pdf/nephrolithiasis-pathway.pdf
Evidence Ratings
To Bibliography
This pathway was developed through local consensus based on published evidence and expert
opinion as part of Clinical Standard Work at Seattle Children’s. Pathway teams include
representatives from Medical, Subspecialty, and/or Surgical Services, Nursing, Pharmacy, Clinical
Effectiveness, and other services as appropriate.
When possible, we used the GRADE method of rating evidence quality. Evidence is first assessed
as to whether it is from randomized trial or cohort studies. The rating is then adjusted in the
following manner (from: Guyatt G et al. J Clin Epidemiol. 2011;4:383-94.):
Quality ratings are downgraded if studies:
· Have serious limitations
· Have inconsistent results
· If evidence does not directly address clinical questions
· If estimates are imprecise OR
· If it is felt that there is substantial publication bias
Quality ratings are upgraded if it is felt that:
· The effect size is large
· If studies are designed in a way that confounding would likely underreport the magnitude
of the effect OR
· If a dose-response gradient is evident
Guideline – Recommendation is from a published guideline that used methodology deemed
acceptable by the team.
Expert Opinion – Our expert opinion is based on available evidence that does not meet GRADE
criteria (for example, case-control studies).
Return to Home

Summary of Version Changes
· Version 1.0 (9/29/2015): Go live
· Version 2.0 (1/19/2018): Updated discharge instructions to reflect new availability of dedicated
appointments in Urology clinic for ureteral stones patients
Return to Home
Medical Disclaimer
Medicine is an ever-changing science. As new research and clinical experience broaden our
knowledge, changes in treatment and drug therapy are required.
The authors have checked with sources believed to be reliable in their efforts to provide information
that is complete and generally in accord with the standards accepted at the time of publication.
However, in view of the possibility of human error or changes in medical sciences, neither the
authors nor Seattle Children’s Healthcare System nor any other party who has been involved in the
preparation or publication of this work warrants that the information contained herein is in every
respect accurate or complete, and they are not responsible for any errors or omissions or for the
results obtained from the use of such information.
Readers should confirm the information contained herein with other sources and are encouraged to
consult with their health care provider before making any health care decision.
Return to Home
Bibliography
Identification
Screening
Eligibility
Included
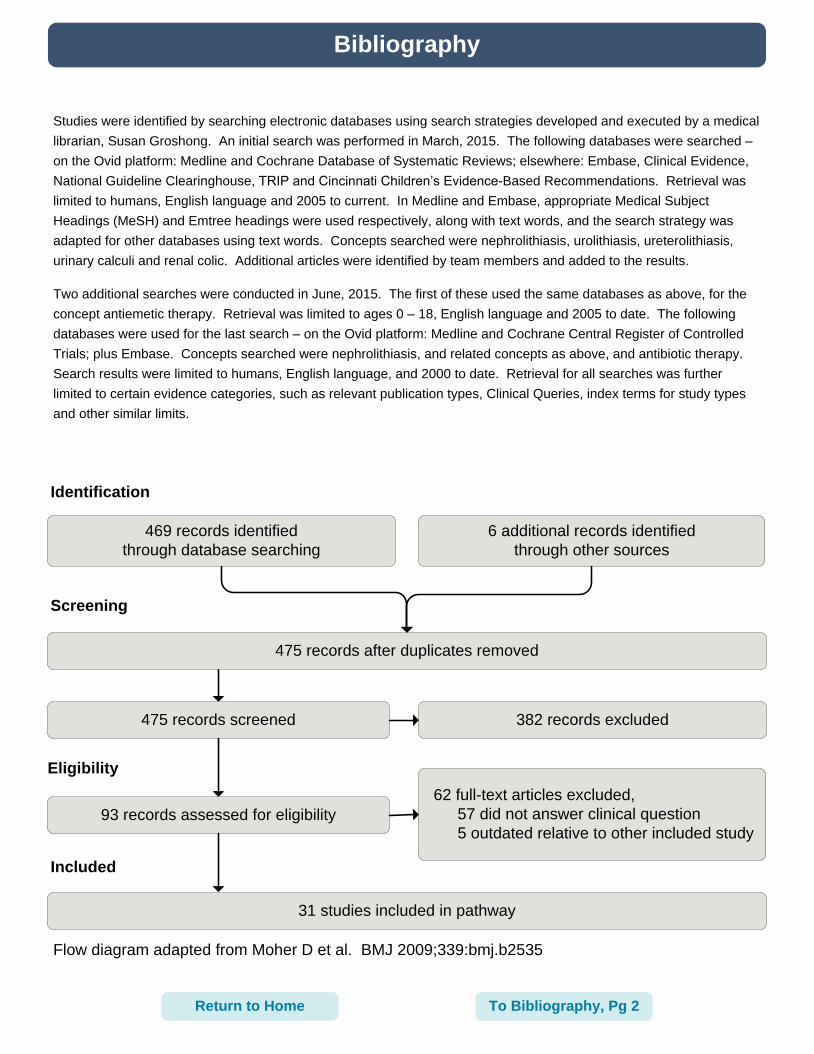
Flow diagram adapted from Moher D et al. BMJ 2009;339:bmj.b2535
Studies were identified by searching electronic databases using search strategies developed and executed by a medical
librarian, Susan Groshong. An initial search was performed in March, 2015. The following databases were searched –
on the Ovid platform: Medline and Cochrane Database of Systematic Reviews; elsewhere: Embase, Clinical Evidence,
National Guideline Clearinghouse, TRIP and Cincinnati Children’s Evidence-Based Recommendations. Retrieval was
limited to humans, English language and 2005 to current. In Medline and Embase, appropriate Medical Subject
Headings (MeSH) and Emtree headings were used respectively, along with text words, and the search strategy was
adapted for other databases using text words. Concepts searched were nephrolithiasis, urolithiasis, ureterolithiasis,
urinary calculi and renal colic. Additional articles were identified by team members and added to the results.
Two additional searches were conducted in June, 2015. The first of these used the same databases as above, for the
concept antiemetic therapy. Retrieval was limited to ages 0 – 18, English language and 2005 to date. The following
databases were used for the last search – on the Ovid platform: Medline and Cochrane Central Register of Controlled
Trials; plus Embase. Concepts searched were nephrolithiasis, and related concepts as above, and antibiotic therapy.
Search results were limited to humans, English language, and 2000 to date. Retrieval for all searches was further
limited to certain evidence categories, such as relevant publication types, Clinical Queries, index terms for study types
and other similar limits.
To Bibliography, Pg 2
469 records identified
through database searching
6 additional records identified
through other sources
475 records after duplicates removed
475 records screened 382 records excluded
62 full-text articles excluded,
57 did not answer clinical question
5 outdated relative to other included study93 records assessed for eligibility
31 studies included in pathway
Return to Home

Bibliography
Alleemudder A, Tai X-, Goyal A, Pati J. Raised white cell count in renal colic: Is there a role for
antibiotics? Urol Ann [Antibiotic]. 2014;6(2):127-129.
Bariol SV, Moussa SA, Tolley DA. Contemporary imaging for the management of urinary stones.
EAU Update Ser [Nephrolithiasis]. 2005;3(1 SPEC. ISS.):3-9.
Barrett TW, DiPersio DM, Jenkins CA, et al. A randomized, placebo-controlled trial of ondansetron,
metoclopramide, and promethazine in adults. Am J Emerg Med [Nephrolithiasis].
2011;29(3):247-255. Accessed 20110218; 8/26/2015 4:57:04 PM. http://dx.doi.org/10.1016/
j.ajem.2009.09.028.
Becker G, Caring for Australians with Renal Impairment (CARI). The CARI guidelines. kidney
stones: Uric acid stones. Nephrology [Nephrolithiasis]. 2007;12(Suppl 1):S21-5.
Best J, Kitlowski AD, Ou D, Bedolla J. Diagnosis and management of urinary tract infections in the
emergency department. Emerg med pract [Nephrolithiasis]. 2014;16(7):1-23.
Braude D, Soliz T, Crandall C, Hendey G, Andrews J, Weichenthal L. Antiemetics in the ED: A
randomized controlled trial comparing 3 common agents. Am J Emerg Med [Nephrolithiasis].
2006;24(2):177-182.
Campschroer T, Zhu Y, Duijvesz D, Grobbee DE, Lock MT. Alpha-blockers as medical expulsive
therapy for ureteral stones. Cochrane Database of Systematic Reviews [Nephrolithiasis].
2014;4.
Carter B, Fedorowicz Z. Antiemetic treatment for acute gastroenteritis in children: An updated
cochrane systematic review with meta-analysis and mixed treatment comparison in a
bayesian framework. BMJ Open [Antiemetic]. 2012;2(4).
Chua ME, Park JH, Castillo JC, Morales ML Jr. Terpene compound drug as medical expulsive
therapy for ureterolithiasis: A meta-analysis. Urolithiasis [Nephrolithiasis]. 2013;41(2):143-
151. Accessed 20130318; 3/16/2015 5:54:22 PM. http://dx.doi.org/10.1007/s00240-012-0538-
3.
Coursey CA, Casalino DD, Remer EM, et al. ACR appropriateness criteria acute onset flank pain--
suspicion of stone disease. Ultrasound Q [Nephrolithiasis]. 2012;28(3):227-233. Accessed
20120824; 3/16/2015 5:54:22 PM.
Crompton G, Cosson P. A systematic review comparing the appropriateness of the intravenous
urogram and the computed tomography urogram in terms of diagnostic accuracy and risk of
radiation dose for patients with urolithiasis. Radiography [Nephrolithiasis]. 2011;17(4):304-
310.
Edwards J, Meseguer F, Faura C, Moore AR, McQuay HJ, Derry S. Single dose dipyrone for acute
renal colic pain. Cochrane Database of Systematic Reviews [Nephrolithiasis]. 2013;6.
To Bibliography, Pg 3Return to Home
Bibliography
Egerton-Warburton D, Meek R, Mee MJ, Braitberg G. Antiemetic use for nausea and vomiting in
adult emergency department patients: Randomized controlled trial comparing ondansetron,
metoclopramide, and placebo. Ann Emerg Med [Nephrolithiasis]. 2014;64(5):526-532.e1.
Accessed 20141202; 8/26/2015 4:57:04 PM. http://dx.doi.org/10.1016/
j.annemergmed.2014.03.017.
Ernst AA, Weiss SJ, Park S, Takakuwa KM, Diercks DB. Prochlorperazine versus promethazine
for uncomplicated nausea and vomiting in the emergency department: A randomized,
double-blind clinical trial. Ann Emerg Med [Nephrolithiasis]. 2000;36(2):89-94.
Fulgham PF, Assimos DG, Pearle MS, Preminger GM. Clinical effectiveness protocols for
imaging in the management of ureteral calculous disease: AUA technology assessment. J
Urol [Nephrolithiasis]. 2013;189(4):1203-1213. Accessed 20130408; 3/16/2015 5:54:22 PM.
http://dx.doi.org/10.1016/j.juro.2012.10.031.
Holdgate A, Pollock T. Nonsteroidal anti-inflammatory drugs (NSAIDS) versus opioids for acute
renal colic. Cochrane Database of Systematic Reviews [Nephrolithiasis]. 2009;4.
Hollingsworth JM, Rogers MA, Kaufman SR, et al. Medical therapy to facilitate urinary stone
passage: A meta-analysis. Lancet [Nephrolithiasis]. 2006;368(9542):1171-1179. Accessed
20061002; 3/16/2015 5:54:22 PM.
Krambeck AE, Lieske JC. Infection-related kidney stones. Clin Rev Bone Miner Metab
[Nephrolithiasis]. 2011;9(3-4):218-228.
Lu Z, Dong Z, Ding H, Wang H, Ma B, Wang Z. Tamsulosin for ureteral stones: A systematic
review and meta-analysis of a randomized controlled trial. Urol Int [Nephrolithiasis].
2012;89(1):107-115. Accessed 20120731; 3/16/2015 5:54:22 PM. http://dx.doi.org/10.1159/
000338909.
Mezentsev VA. Meta-analysis of the efficacy of non-steroidal anti-inflammatory drugs vs. opioids
for SWL using modern electromagnetic lithotripters. Int Braz J Urol [Nephrolithiasis].
2009;35(3):293-297. Accessed 20090622; 3/16/2015 5:54:22 PM.
National GC. Guidelines on urolithiasis. . http://www.guideline.gov/
content.aspx?id=45324&search=urolithiasis;. Updated 2013. Accessed 3/17, 2015.
National GC. Guidelines on paediatric urology. . http://www.guideline.gov/
content.aspx?id=47872&search=urolithiasis;. Updated 2013. Accessed 3/17, 2015.
Niemann T, Kollmann T, Bongartz G. Diagnostic performance of low-dose CT for the detection of
urolithiasis: A meta-analysis. AJR Am J Roentgenol [Nephrolithiasis]. 2008;191(2):396-401.
Accessed 20080723; 3/16/2015 5:54:22 PM. http://dx.doi.org/10.2214/AJR.07.3414.
Parys B, McClinton S, Watson GM, et al. BAUS section of endourology guidelines for acute
management of first presentation of renal/ureteric lithiasis. Br J Med Surg Urol
[Nephrolithiasis]. 2009;2(3):134-136.
To Bibliography, Pg 4Return to Home
Bibliography
Pickard R, Starr K, MacLennan G, et al. Medical expulsive therapy in adults with ureteric colic: A
multicentre, randomised, placebo-controlled trial. Lancet [Nephrolithiasis].
2015;386(9991):341-349. Accessed 20150803; 8/26/2015 5:00:51 PM. http://dx.doi.org/
10.1016/S0140-6736(15)60933-3.
Picozzi SC, Ricci C, Gaeta M, et al. Urgent ureteroscopy as first-line treatment for ureteral
stones: A meta-analysis of 681 patients. Urol Res [Nephrolithiasis]. 2012;40(5):581-586.
Accessed 20120914; 3/16/2015 5:54:22 PM. http://dx.doi.org/10.1007/s00240-012-0469-z.
Picozzi SC, Ricci C, Gaeta M, et al. Urgent shock wave lithotripsy as first-line treatment for
ureteral stones: A meta-analysis of 570 patients. Urol Res [Nephrolithiasis]. 2012;40(6):725-
731. Accessed 20121112; 3/16/2015 5:54:22 PM. http://dx.doi.org/10.1007/s00240-012-
0484-0.
Preminger GM, Tiselius HG, Assimos DG, et al. 2007 guideline for the management of ureteral
calculi. Eur Urol [Nephrolithiasis]. 2007;52(6):1610-1631.
Steinberg PL, Nangia AK, Curtis K. A standardized pain management protocol improves
timeliness of analgesia among emergency department patients with renal colic. Qual Manag
Health Care [Nephrolithiasis]. 2011;20(1):30-36. Accessed 20101230; 3/16/2015 5:54:22
PM. http://dx.doi.org/10.1097/QMH.0b013e31820429d9.
Wang H-, Velazquez N, Zapata D, et al. Effectiveness of medical expulsive therapy for pediatric
urolithiasis: Systematic review and meta-analysis. J Endourol [Nephrolithiasis].
2014;28:A155.
Wolf JS Jr, Bennett CJ, Dmochowski RR, et al. Best practice policy statement on urologic surgery
antimicrobial prophylaxis. J Urol [Nephrolithiasis]. 2008;179(4):1379-1390. Accessed
20080317; 8/26/2015 4:57:04 PM. http://dx.doi.org/10.1016/j.juro.2008.01.068.
Return to Home