critical updates on canine and feline health · critical updates on canine and feline health ......
TRANSCRIPT

Critical Updates onCanine and Feline HealthProceedings from the Nestlé Purina Symposium at the
2009 NAVC Conference/Western Veterinary Conference

Critical Updates onCanine and Feline Health
MANAGING THE DIABETIC CAT WITH
CONCURRENT GASTROINTESTINAL DISEASE
Deborah S. Greco, DVM, PhD, DACVIM
CLINICAL AND RESEARCH EXPERIENCE
WITH PROBIOTICS
Michael R. Lappin, DVM, PhD, DACVIM
GROWING OLD GRACEFULLY:
AN OVERVIEW OF HEALTHCARE MANAGEMENT
OF THE AGING CAT
Margie Scherk, DVM, DABVP (Feline)
CHRONIC DIARRHEA IN KITTENS AND CATS:
IT CAN BE STOPPED
Debra L. Zoran, DVM, PhD, DACVIM-SAIM
3
11
16
22
Cover Photo: © Punchstock/Digital Vision

Critical Updates on Canine and Feline Health, 2009 NAVC/WVC Proceedings 3
Managing the DiabeticCat with ConcurrentGastrointestinal DiseaseDeborah S. Greco, DVM, PhD, DACVIMNestlé Purina PetCareCheckerboard SquareSt. Louis, Missouri
©2008 Jupiter/Thinkstock Images
ncomplicated diabetes in cats can be man-aged with diet and oral hypoglycemictherapy or insulin. In fact, many of these
cats with uncomplicated diabetes will be able to discon-tinue insulin with proper dietary therapy. However, about25% to 30% of diabetic cats will remain on insulin therapyfor life because their disease (pancreatic amyloidosis) hasprogressed to the point of insulin dependence. Many ofthese cats will require ancillary therapy, including antibi-otics, dietary supplements, probiotics, and even steroids tocontrol concurrent conditions such as intestinal and pan-creatic disease. This article describes the diagnosticworkup of diabetic cats with concurrent gastrointestinal(GI) disease resulting in anorexia, diarrhea, vomiting, andweight loss.
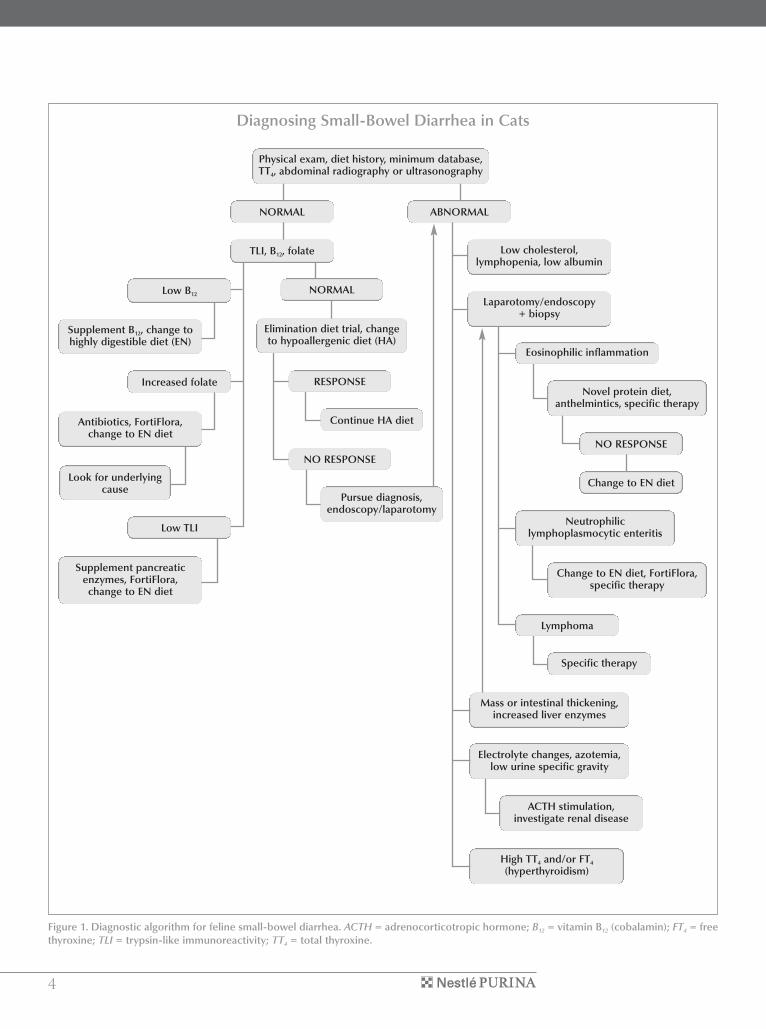
CONCURRENT GASTROINTESTINALDISEASE IN THE DIABETIC CATNonspecific diarrhea is a common finding in diabetic cats andhumans. The pathogenesis of diarrhea in diabetic people ispoorly understood, but altered motility, bacterial overgrowth,exocrine pancreatic insufficiency, gluten-induced enteropa-thy, and increased intestinal secretion are considered possiblecauses.1 Bacterial overgrowth seems a likely candidate, asdiarrhea in human patients often responds to antibiotic andprobiotic therapy. Diarrhea may be particularly difficult tomanage in diabetic cats because of the associated loss of dia-betic regulation. Figure 1 is an algorithm for the workup ofdiarrhea in diabetic cats.
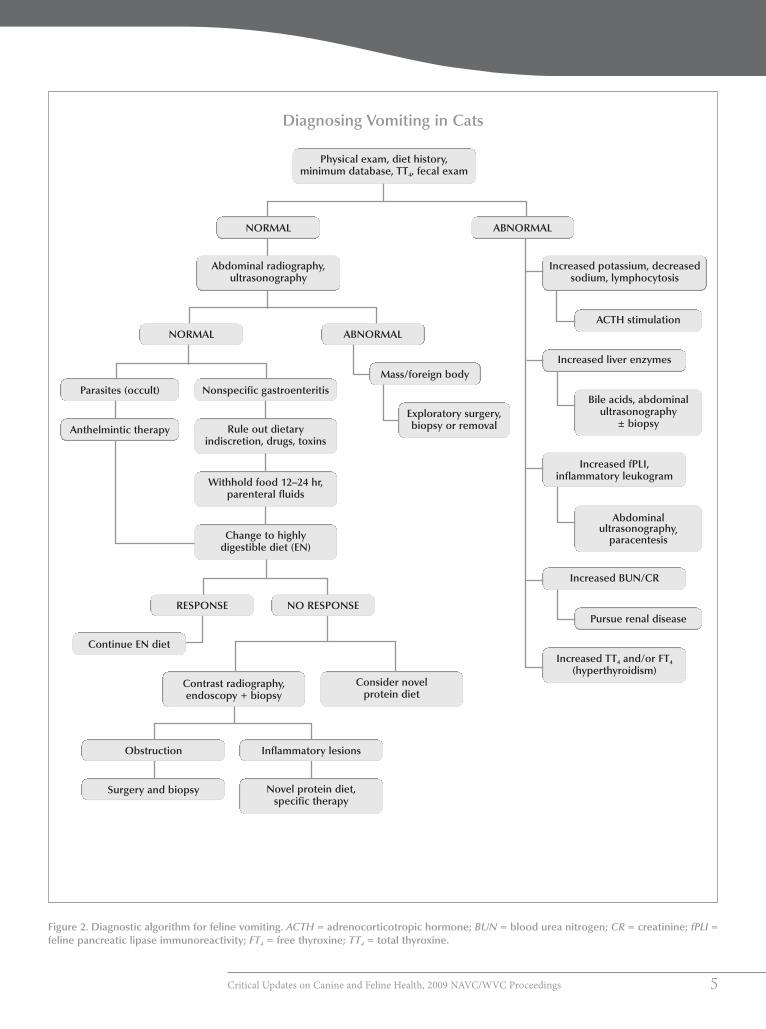
Vomiting, weight loss, and anorexia are common signsassociated with poorly regulated diabetic cats (and humans)with concurrent GI disease.1 The differential diagnosis of catswith these signs may be extensive; Figures 2, 3, and 4 illustratethe diagnostic and therapeutic approach to these patients.
Diabetic cats, particularly those that do not respond toinsulin therapy, should be screened for chronic pancreaticdisease. Nonspecific signs, such as anorexia and lethargy, are
the most common clinical signs of pancreatitis in the cat.Diarrhea, vomiting, and weight loss are also observed in catswith pancreatitis, but with less frequency. Physical examina-tion findings often include dehydration, with pallor andicterus being less common. Rarely, fever, tachypnea, abdomi-nal pain, or a palpable abdominal mass are noted on physicalexamination. In some cases, chronic pancreatitis may result inexocrine pancreatic insufficiency, which may manifest aspolyphagia, a poor haircoat, and weight loss.
DIAGNOSTIC APPROACH TOTHE DIABETIC CAT WITHGASTROINTESTINAL SIGNSMinimum DatabaseAfter a thorough history and physical examination, everypoorly regulated diabetic cat should be evaluated with a com-plete blood count, serum chemistry profile, serum totalthyroxine, urinalysis, viral titers (FeLV), and fecal examina-tion to rule out endocrine disorders, parasites, and systemicdisease as a cause of the GI signs. Azotemia, leukocytosis,hemoconcentration resulting from dehydration, and hyper-cholesterolemia are common clinicopathologic findings infeline pancreatitis.2 Macrocytic anemia may be caused bycobalamin (vitamin B12) deficiency often associated with GIdisease. Increased liver enzyme activity (ALT, ALP) and, lesscommonly, hypocholesterolemia may indicate underlyingliver disease, such as cholangiohepatitis, secondary hepaticlipidosis, or reactive hepatopathy associated with diabetesmellitus or pancreatitis. Finally, electrolyte abnormalities,such as hypocalcemia and hypokalemia, should alert the cli-nician to the possibility of pancreatitis.
A simple feces smear or rectal scraping can be stained toidentify cells such as neutrophils and eosinophils.Characteristic “safety pin” spores of Clostridium or spiro-chetes such as Campylobacter may be identified under themicroscope at high power. Acid-fast stains may identifyCryptosporidium and mycobacteria.
U
4
Figure 1. Diagnostic algorithm for feline small-bowel diarrhea. ACTH = adrenocorticotropic hormone; B12 = vitamin B12 (cobalamin); FT4 = freethyroxine; TLI = trypsin-like immunoreactivity; TT4 = total thyroxine.
Diagnosing Small-Bowel Diarrhea in Cats
Physical exam, diet history, minimum database,TT4, abdominal radiography or ultrasonography
Low cholesterol,lymphopenia, low albumin
Laparotomy/endoscopy+ biopsy
Eosinophilic inflammation
NO RESPONSE
Change to EN diet
Novel protein diet,anthelmintics, specific therapy
Neutrophiliclymphoplasmocytic enteritis
Change to EN diet, FortiFlora,specific therapy
Lymphoma
Specific therapy
ACTH stimulation,investigate renal disease
Electrolyte changes, azotemia,low urine specific gravity
TLI, B12, folate
Supplement B12, change tohighly digestible diet (EN)
Low B12
Antibiotics, FortiFlora,change to EN diet
Look for underlyingcause
Supplement pancreaticenzymes, FortiFlora,change to EN diet
Low TLI
Increased folate
NORMAL
Elimination diet trial, changeto hypoallergenic diet (HA)
Continue HA diet
NO RESPONSE
High TT4 and/or FT4
(hyperthyroidism)
ABNORMAL
RESPONSE
Pursue diagnosis,endoscopy/laparotomy
Mass or intestinal thickening,increased liver enzymes
NORMAL
Critical Updates on Canine and Feline Health, 2009 NAVC/WVC Proceedings 5
Figure 2. Diagnostic algorithm for feline vomiting. ACTH = adrenocorticotropic hormone; BUN = blood urea nitrogen; CR = creatinine; fPLI =feline pancreatic lipase immunoreactivity; FT4 = free thyroxine; TT4 = total thyroxine.
Diagnosing Vomiting in Cats
Increased TT4 and/or FT4
(hyperthyroidism)
Pursue renal disease
Abdominalultrasonography,
paracentesis
Bile acids, abdominalultrasonography
± biopsy
ACTH stimulation
Increased potassium, decreasedsodium, lymphocytosis
Increased liver enzymes
Increased fPLI,inflammatory leukogram
Increased BUN/CR
ABNORMAL
Physical exam, diet history,minimum database, TT4, fecal exam
NORMAL
Abdominal radiography,ultrasonography
ABNORMAL
Exploratory surgery,biopsy or removal
Mass/foreign body
NORMAL
Rule out dietaryindiscretion, drugs, toxins
Nonspecific gastroenteritisParasites (occult)
Withhold food 12–24 hr,parenteral fluids
Consider novelprotein diet
NO RESPONSE
Obstruction Inflammatory lesions
Contrast radiography,endoscopy + biopsy
Novel protein diet,specific therapy
Surgery and biopsy
Continue EN diet
RESPONSE
Anthelmintic therapy
Change to highlydigestible diet (EN)

6
Figure 3. Diagnostic algorithm for feline weight loss. FT4 = free thyroxine; PLE = protein-losing enteropathy; PLN = protein-losing nephropathy;RER = resting energy requirement; TT4 = total thyroxine; UPC = urine protein:creatinine ratio.
Diagnosing Weight Loss in Cats
Elevated TT4 and/or FT4
(hyperthyroidism)
Insulin, oral hypoglycemictherapy, change to dietetic
management diet (DM)
Hyperglycemia, glucosuria
Hypoalbuminemia,proteinuria
ABNORMALNORMAL
Gastrointestinal signs
NORMAL/INCREASED APPETITE
REDUCED APPETITE
Physical exam, diet history,appetite
Inadequate calorie intake
Change to energy-dense diet
Increased exercise Poor diet
Change topremium diet
Adequate diet
Perform physical exam, minimumdatabase, TT4, fecal exam
Calculate food needs(RER), increase food intake
Consider calorie-dense diet
NO
Endoscopy, biopsy
Rule out PLE
YES
See Figure 1
Diarrhea?
See Figure 2
Vomiting?
Exercise level?Adequate calorie intake?
See Figure 4
Rule outPLN, liver disease
Blood pressure, ultrasoundbiopsy, UPC
Hypoalbuminemia,hypocholesteremia,
lymphopenia
Rule out PLE
Endoscopy, biopsy

Critical Updates on Canine and Feline Health, 2009 NAVC/WVC Proceedings 7
Ancillary TestsAncillary tests should include feline pancreatic lipase immunore-activity (fPLI), trypsin-like immunoreactivity (TLI), and serumcobalamin (B12). Feline TLI (fTLI) has been shown to have lowsensitivity and questionable specificity for diagnosing feline pan-creatitis.3 However, studies have shown that the species-specificfPLI has excellent sensitivity (100%) for moderate to severe pan-creatitis and good sensitivity for mild pancreatitis (54%).4
Cobalamin is assimilated via binding to intrinsic factor (from thepancreas) and subsequent absorption in the ileum; therefore, catswith exocrine pancreatic insufficiency, ileal disease, and pancre-atitis should be screened for cobalamin deficiency.
Radiography and UltrasonographySurvey abdominal radiography is an inexpensive initial diag-nostic test for cats with poorly regulated diabetes mellitus.Radiographic findings in cats with pancreatitis may includecranial mass with or without abdominal effusion, dilatedsmall intestine, and hepatomegaly. More often, however,abdominal radiographs are normal, and ultrasound must beperformed to identify underlying pancreatic or liver disease.
Abdominal ultrasonography may be very helpful inassessing the location of disease within the GI tract.Specifically, ultrasonography may assist in detecting gastricmasses, gastric ulceration, and thickening of the stomach
Figure 4. Diagnostic algorithm for feline anorexia. fPLI = feline pancreatic lipase immunoreactivity; GI = gastrointestinal.
Diagnosing Anorexia in Cats
Physical exam, oral exam, body conditionscore, diet history, minimum databasea
Specific therapy orpursue diagnosis
Survey radiography
ABNORMAL
NORMAL
See Figure 2
Rule out pancreatitis
fPLI, ultrasonography
NORMAL
See Figure 1
Rule outdiseases and conditions
Respiratory disease
Chest radiography,endoscopy, biopsy
Dental disease/stomatitis,retrobulbar or pharyngeal
myositis
Biopsy, radiography,remove affected teeth
Pseudoanorexia,loss of senses,
blindness, anosmia
Vestibular disease,cerebral disease
Treat other primary disease
NORMAL(with GI signs)
ABNORMAL
aProvide appropriate nutritional support while pursuing diagnosis.

8
lining. The intestines can be assessed for localized disease(i.e., ileal tumor) and thickening and enlargement of mesen-teric lymph nodes, which may indicate neoplasia. Althoughthe specificity of abdominal ultrasonography for diagnosingfeline pancreatitis is relatively high, the sensitivity is low dueto a lack of standardized diagnostic criteria and interoperatorvariation. Common ultrasonographic findings in cats withpancreatitis include abdominal effusion, hyperechoic peri-pancreatic mesentery, and pancreatic hypoechogenicity.5
Endoscopy versus LaparotomyIf the history and physical exam, minimum database, andancillary tests indicate the location of the lesion within the GItract or the clinician suspects generalized GI disease or disease
localized to the stomachor colon, endoscopy canbe a valuable tool. Therisk of dehiscence is lowwith endoscopic biopsies;therefore, this is themethod of choice for catswith fragile intestines andlow protein due to pro-tein-losing enteropathies.Endoscopy is noninvasiveand can be performedmultiple times. The lim-itations include smallbiopsy size, forceps arti-
facts on biopsies, inability to biopsy the jejunum, and, mostimportant, the inability to obtain full-thickness biopsies.
If the history and physical examination indicate that the GIdisease is localized (particularly if there is a suggestion of duo-denal, ileal, or jejunal involvement), an exploratory laparotomywith full-thickness biopsies may be indicated. The disadvantagesof exploratory surgery are the length of anesthesia and the riskof dehiscence, particularly in patients with low serum protein.The advantage of laparotomy is that it allows for full-thicknessbiopsies, which may be required to diagnosis inflammatorybowel disease (IBD) and neoplasia, and biopsies of multipleorgans (e.g., liver, lymph node). GI neoplasia should be ruledout with full-thickness biopsies before adding interventionaltherapies such as corticosteroids that could mask the disease,making it difficult to diagnose properly.
TREATMENT OF THE POORLYREGULATED DIABETIC CAT WITHGASTROINTESTINAL DISEASEDietary TherapyDietary therapy is one of the most important aspects of man-aging GI disorders in the diabetic cat. However, dietary
therapy is complicated in the diabetic cat because the dietmay have a significant effect on diabetic regulation. The pres-ence of food in the GI tract provides nutrients, increasesmesenteric blood flow, and stimulates the release of digestiveenzymes and hormones.6 During acute diarrhea episodes innondiabetic patients, complete bowel rest is advocated;7 how-ever, this is not possible in diabetic cats receiving twice-dailyinsulin injections.
Highly digestible diets (e.g., Purina Veterinary Diets® ENGastroenteric®, Nestlé Purina PetCare Company, St. Louis,MO) are recommended for cats with GI diseases, includingIBD not related to food allergy.8,9 Such diets facilitate nutrientabsorption in the proximal small bowel and reduce the anti-genicity of bowel contents.8 For cats with IBD, diets with amodified (reduced) omega-6:omega-3 fatty acid ratio havebeen suggested to reduce GI inflammation.8–10 The cytokinesproduced from omega-3 fatty acids are less inflammatorythan those produced from omega-6 fatty acids.11
Carbohydrate malassimilation secondary to exocrine pan-creatic insufficiency in diabetic cats can result in bacterialovergrowth, intestinal gaseousness, osmotic diarrhea, andother adverse effects.8 Therefore, restriction of dietary carbohy-drates may also be beneficial for diabetic cats with GI disease.A low-carbohydrate, high-protein diet may ameliorate some ofthe abnormalities associated with diabetesmellitus and concur-rent GI disease. A study examining clinical cases of diabetesmellitus in cats fed a high-protein, low-carbohydrate food(Purina Veterinary Diets® DMDietetic Management®) showedthat insulin dosage could be decreased by 50% and that 25% to30% of cats could discontinue insulin altogether.12 A surprisingoutcome of feeding the diet was that there was also a significantreduction in concurrent diarrhea among cats participating inthe study.12 Low-carbohydrate canned food diets have also beenshown to improve diabetic regulation in both insulin-dependentand non–insulin-dependent diabetic cats.13,14
Prebiotics and ProbioticsA subset of fermentable fibers are those referred to as pre-biotics. By definition, these fibers are selectively fermented byhealth-promoting bacteria, resulting in an increase in thenumber or percentage of these organisms and a decrease in theprevalence of potential pathogens, such as Clostridium.13–20
Chicory, inulin, and the related fructose-containing oligosac-charides are the best studied prebiotics; their beneficial effectson GI microflora in cats are well established.13,15–17
Probiotics (such as those in Purina Veterinary Diets®FortiFlora®) are live microorganisms that, when ingested,have a beneficial effect on intestinal function by promotingimproved intestinal microbial balance. The beneficial bacteriahelp nourish the intestinal cells and protect against coloniza-tion by pathogenic bacteria, which can cause diarrhea.
A low-carbohydrate,
high-protein diet may
ameliorate some of
the abnormalities
associated with
diabetes mellitus and
concurrent GI disease.

Critical Updates on Canine and Feline Health, 2009 NAVC/WVC Proceedings 9
Probiotics are considered to be most beneficial for diarrheacaused by microflora imbalance resulting from acute enteritis,antibiotics, diet change, dietary indiscretion, and stress. Foracute cases, 2 weeks of probiotic therapy may be sufficient;however, most chronic cases will require at least 30 days oftherapy. An additional beneficial effect of probiotics is theenhancement of the GI immune system, which may beimpaired in diabetic cats.
VitaminsOlder cats, particularly those older than 10 years of age, aremore likely to be deficient in cobalamin. Furthermore, diabet-ic cats with concurrent GI disease, such as pancreatitis, may beeven more likely to suffer from cobalamin deficiency becauseof underlying pancreatic pathology. Clinical signs of cobalamindeficiency are manifested as anemia, anorexia, lack of weightgain, poor diabetic regulation, and an unthrifty appearance. Itis recommended that cats with significant GI signs have serumcobalamin levels measured by a reputable laboratory.Infiltrative disease of the GI tract may cause a decrease incobalamin absorption from the ileum; therefore, oral supple-mentation is usually not sufficient to overcome this vitamindeficiency. Injectable supplementation of 250 mcg cobal-amin/cat SC weekly for 6 weeks, then every 2 weeks, and thenonce monthly is recommended.
AntibioticsWith the advent of probiotics, antibiotic therapy to reducepathogens associated with GI disease in cats has beenreduced. However, certain infections such as Giardia requirespecific antibiotic or antiparasitic therapy to resolve clinicalsigns. Antibiotics with an anaerobic spectrum can be benefi-cial in some cases of GI disease (particularly Clostridiumperfringens–associated diarrheas). Examples of antibioticsthat may be useful in treating infectious GI diseases includethe beta-lactams (penicillin and cephalosporins), clin-damycin, and metronidazole. Tylosin powder has also beeneffective in the treatment of diarrhea in diabetic cats in theauthor’s experience and has the advantage of not beingabsorbed systemically.
SteroidsDiabetic cats with concurrent cholangiohepatitis, IBD, orpancreatitis may benefit from corticosteroid administra-tion. Short-acting oral medications, such as methyl-prednisolone or prednisolone, should be used rather thanrepositol steroids such as methylprednisolone acetate. Oralsteroids are inactivated to a certain extent in the liver (the“first-pass” effect), whereas repositol steroids remain fullyactive in the general circulation and contribute significant-ly to peripheral insulin resistance. It is unclear if certain cats
can convert prednisone to the active form, prednisolone;therefore, either prednisolone (5 mg PO q24h) or methyl-prednisolone (4 mg PO q24h) is recommended to obtainoptimal efficacy. A course of 14 days is used in acute flare-ups; a gradual reduction in daily dose to 2.5 mgprednisolone or 2 mg methylprednisolone can be used tomanage chronic cases of pancreatitis, cholangiohepatitis,and biopsy-proven IBD.
InsulinInitial insulin doses range from 0.2 to 0.5 units/kg; however,most cats are readily managed on 2 units twice daily as a start-ing dose.20 If intermediate-acting insulin is used, it must beadministered to cats twice daily because of its short durationof action. Glargine and PZI insulin may be given once daily,although the author recommends twice-daily dosing initially.In all cases, careful blood or urine monitoring should be per-formed to avoid hypoglycemic episodes.20
The injection site should be discussed with pet ownersbecause insulin absorption may be impaired in underweight,dehydrated diabetic cats. The back of the neck (scruff) iscommonly used for insulin injection. However, this site is notrecommended because of lack of blood flow and the potentialfor increased fibrosis caused by repeated injections at this site.Insulin injections should be administered along the lateralabdomen and thorax. The owner should rotate the site ofinjection daily. Many commercially available pamphlets out-line injection techniques, feeding, and hypoglycemic episodemanagement and provide a log sheet for owners to recordfood intake, clinical signs, urine glucose measurements, andinsulin dosages.
MONITORING THE DIABETIC CATWITH GASTROINTESTINAL DISEASEUrine GlucoseUrine glucose monitoring may be performed at home by own-ers, is not affected by stress, and may indicate insulin-inducedhyperglycemia (the Somogyi effect). Urine glucose is a mea-sure of trends in blood glucose and should not be used aloneto adjust insulin dosages. However, urine glucose shoulddecrease to trace or 1+ with appropriate therapy. Consistentlyhigh urine glucose indicates the need for blood glucose orglycated protein (fructosamine) evaluation. This is bestaccomplished using the Purina Glucotest® system, a homeurine glucose monitoring system for cats. The Glucotest pack-ets can be sprinkled in the litterbox over premium clumpinglitter and checked daily for color change. Diabetic cats that areanorectic may develop ketosis or ketoacidosis; unfortunately,these conditions cannot be detected by the Glucotest system.For anorectic diabetic cats, the use of urine strips that detectketones is recommended.

10
Blood GlucoseGlucose monitors designed for home monitoring in peopleare inexpensive, accurate, and rapid and require only a dropof blood. Although reasonably accurate in the blood glucoserange of 60 to 120 mg/dl (4 to 12.5 mmol/L), these monitorsare designed to read lower than the actual value as glucoseapproaches the hypoglycemic range. Such factors as altitude;patient dehydration, hematocrit, oxygen therapy, shock, orsevere infection; and out-of-date or improperly stored teststrips can all affect the monitors’ accuracy. A veterinary glu-cose monitor marketed as the Abbott AlphaTRAK® (AbbottLaboratories, Abbott Park, IL) has the highest correlation toclinical laboratory sample glucose analysis. The BayerAscensia® Contour® (Bayer HealthCare LLC, Tarrytown, NY)and the Roche Accu-Chek® Advantage (Roche Diagnostics)are both excellent human monitors but fall short of the accu-racy of the Abbott product when used in animals. Bloodglucose curves are good for identifying trends in blood glu-cose during the day and for determining if the cat is becominghypoglycemic during insulin therapy.
Glycosylated Blood ProteinsGlycosylated blood proteins are indicative of mean glucoseconcentrations in serum over an extended period and may beused to monitor long-term insulin therapy. These proteins areparticularly useful when used in conjunction with urine glu-cose monitoring and in monitoring diabetic cats that may bestressed by hospitalization and serial blood glucose curves. Asplasma glucose concentrations increase, glycosylation ofhemoglobin and serum proteins increases proportionately.Glycosylation of serum proteins, such as albumin, results inthe formation of fructosamine. Because albumin has a short-er life span than hemoglobin, fructosamine concentrationsreflect more recent changes (1 to 3 weeks) in serum glucoseconcentrations than glycosylated hemoglobin concentrations.Serum fructosamine concentrations less than 400 to 450µmol/L are associated with good to excellent glycemic con-trol; concentrations of 450 to 550 µmol/L indicate fair to goodcontrol; and concentrations greater than 550 µmol/L indicatepoor glycemic control. Caveats for the use of serum fruc-tosamine include effects caused by hypergammaglobulinemia(falsely high), hyperthyroidism (falsely low), and hypoalbu-minemia (falsely low).
SUMMARYDiabetic cats that remain on insulin as a result of irreversiblepancreatic damage from the diabetic state may exhibit GI signs
that are difficult to manage. Proper use of a diet that is low incarbohydrate and high in protein and omega-3 fatty acids mayameliorate some of the GI signs of attending conditions suchas IBD or pancreatitis. In addition, cobalamin (B12), probiotics,and ancillary medications such as antibiotics and cortico-steroidsmay improve both the GI signs and diabetic regulation.
REFERENCES1. Diehl KJ. Long-term complications of diabetes mellitus, part II: gastro-intestinal and infectious. Vet Clin North Am Small Anim Pract 1995;25(3):731-751.
2. Steiner JM. Diagnosis of pancreatitis. Vet Clin North Am Small Anim Pract2003;33:1181-1195.
3. Swift NC, Marks SL, MacLachlan NJ, et al. Evaluation of serum felinetrypsin-like immunoreactivity for the diagnosis of pancreatitis in cats.JAVMA 2000;217:37-42.
4. Forman MA, Marks SL, De Cock HEV, et al. Evaluation of serum feline pan-creatic lipase immunoreactivity and helical computed tomography versusconventional testing for the diagnosis of feline pancreatitis. J Vet Intern Med2004;18:807-815.
5. Saunders HM, VanWinkle TJ, Drobatz K, et al. Ultrasonographic findings incats with clinical, gross pathologic and histologic evidence of acute pancreat-ic necrosis: 20 cases (1994–2001). JAVMA 2002;221:1724-1730.
6. Michel KE. Nutritional management of gastrointestinal, hepatic, andendocrine diseases. In: Ettinger SJ, Feldman EC, eds. Textbook of VeterinaryInternal Medicine. 5th ed. Philadelphia: WB Saunders; 2000:258-262.
7. Jergens AE. Acute diarrhea. In: Bonagura JD, Kirk RW. Kirk’s CurrentVeterinary Therapy Small Animal Practice XII. Philadelphia: WB Saunders;1995:701-705.
8. Guilford GW. Nutritional management of gastrointestinal tract diseases ofdogs and cats. J Nutr 1994;124(suppl 12S):2663S-2669S.
9. Hall EJ, Simpson KW. Diseases of the small intestine. In: Ettinger SJ, FeldmanEC, eds. Textbook of Veterinary Internal Medicine. 5th ed. Philadelphia: WBSaunders; 2000:1182-1238.
10. Jergens AE. Inflammatory bowel disease. In: August JR, ed. Consultations inFeline Internal Medicine. 2nd ed. Philadelphia: WB Saunders; 1994:75-81.
11. Teitelbaum JE, Walker WA. Review: the role of omega 3 fatty acids in intes-tinal inflammation. J Nutr Biochem 2001;12:21-32.
12. Frank G, Anderson W, Pazak H, et al. Use of a high protein diet in the man-agement of feline diabetes mellitus. Vet Ther 2001;2(3):238-246.
13. Mazzaferro E, Greco DS, Turner AS, Fettman MJ. Treatment of feline dia-betes mellitus using an alpha-glucosidase inhibitor (acarbose) and a highprotein, low carbohydrate diet. J Feline Med Surg 2003;5(3):183-190.
14. Bennett N, Greco DS, Peterson ME, et al. Comparison of a low carbohydratevs high fiber canned diet for the treatment of diabetes mellitus in cats. J FelineMed Surg 2006;8(2):73-84.
15. Howard MD, Kerly MS, Mann FA, et al. Blood flow and epithelial cell prolif-eration of the canine colon are altered by source of dietary fiber.Vet Clin Nutr1999;6:8-15.
16. Duggan C, Gannon J, Walker WA. Protective nutrients and functional foodsfor the gastrointestinal tract. Am J Clin Nutr 2002;75:789-808.
17. Sparkes AH, Papasouliotis K, Sunvold G, et al. Effect of dietary supplemen-tation with fructooligosaccharides on fecal flora of healthy cats. Am J Vet Res1998;59:436-440.
18. Flickinger EQ, Van Loo J, Fahey GC. Nutritional responses to the presence ofinulin and oligofructose in the diets of domesticated animals: a review. CritRev Food Sci Nutr 2003;43:19-60.
19. Rao AV. Dose-response effects of inulin and oligofructose on intestinal bifi-dogenesis effects. J Nutr 1999;129:1442S-1445S.
20. Greco DS, Broussard JD, Peterson ME. Insulin therapy. Vet Clin North AmSmall Anim Pract 1995;25(3):677-689.

Critical Updates on Canine and Feline Health, 2009 NAVC/WVC Proceedings 11
Clinical and ResearchExperience withProbioticsMichael R. Lappin, DVM, PhD, DACVIMCollege of Veterinary Medicine and Biomedical SciencesColorado State UniversityFort Collins, Colorado
©2008 Jupiter/Brand X Pictures
robiotics are live microorganisms that whenadministered in adequate amounts confer ahealth effect on the host.1 There have been
many studies of the effects of probiotics on human health butvery few in small animals. According to de Vrese andSchrezenmeir in a recent review of human studies involvingprobiotics,2 well-established effects include the following:
• Prevention and/or reduction of duration and complaintsof rotavirus-induced or antibiotic-associated diarrheaas well as alleviation of complaints due to lactoseintolerance
• Reduction of the concentration of cancer-promotingenzymes and/or putrefactive (bacterial) metabolites inthe gut
• Prevention and alleviation of unspecific and irregularcomplaints of the gastrointestinal tract in healthy people
• Beneficial effects on microbial aberrancies, inflamma-tion, and other complaints in connection withinflammatory diseases of the gastrointestinal tract,Helicobacter pylori infection, or bacterial overgrowth
• Normalization of passing stool and stool consistency inindividuals suffering from obstipation or an irritablecolon
• Prevention or alleviation of allergies and atopic diseasesin infants
• Prevention of respiratory tract infections (e.g., commoncold, influenza) and other infectious diseases as well astreatment of urogenital infections
POTENTIAL BENEFITS OFPROBIOTICS IN ANIMALSInfectious diseases are very common in small animals, so thepotential beneficial effects of probiotics could affect veteri-nary practice significantly. All of the mechanisms of immune
modulation have not been characterized, and it is likely thatthese effects vary by probiotic. Many probiotics in the lacticacid bacteria group help balance the endogenous microbiota,and some can inhibit replication of pathogenic bacteria.
The proposed mechanisms of action of probiotics includecompetition for essential nutrients or receptor sites, bindingwith pathogenic bacteria, and production of inhibitory sub-stances. It is also now known that some probiotics canbeneficially influence innate and acquired immunity systemi-cally by a variety of proposed mechanisms, includinginducing cytokine production, natural killer cell activity, andboth specific and nonspecific immunoglobulin production.Some of these effects with certain probiotics are now beingdocumented in canine and feline studies.3–7
However, the beneficial effects of probiotics in clinicalstudies can be difficult to ascertain. Several recent review arti-cles in humanmedicine have suggested that probiotics providea minimal beneficial effect for a variety of human conditionssuch as Clostridium difficile diarrhea and hospital-acquiredpneumonia and that larger, more rigorously controlledmulticenter studies should be performed.8–10 These findingsemphasize that biologic effects of individual probiotics willvary and that each probiotic introduced should be rigorouslyevaluated in a controlled fashion to define its potential for clin-ical utility. In addition, the source of the probiotic should alsobe considered. For example, in a recent Canadian study, themajority of diets claiming to contain probiotics generally didnot meet the label claim when evaluated.11
Enterococcus faecium strain SF68 (NCIMB10415), whichwas originally isolated from the feces of a healthy humanbaby, was initially shown to inhibit the growth of a number ofenteropathogens.12 This bacterium is the probiotic in PurinaVeterinary Diets® FortiFlora®.
In one canine study, a group of puppies vaccinated withcanine distemper virus (CDV) and also fed E. faecium strainSF68 was compared over time with a control group that wassimilarly vaccinated but not fed the probiotic.5 A number of
P
12
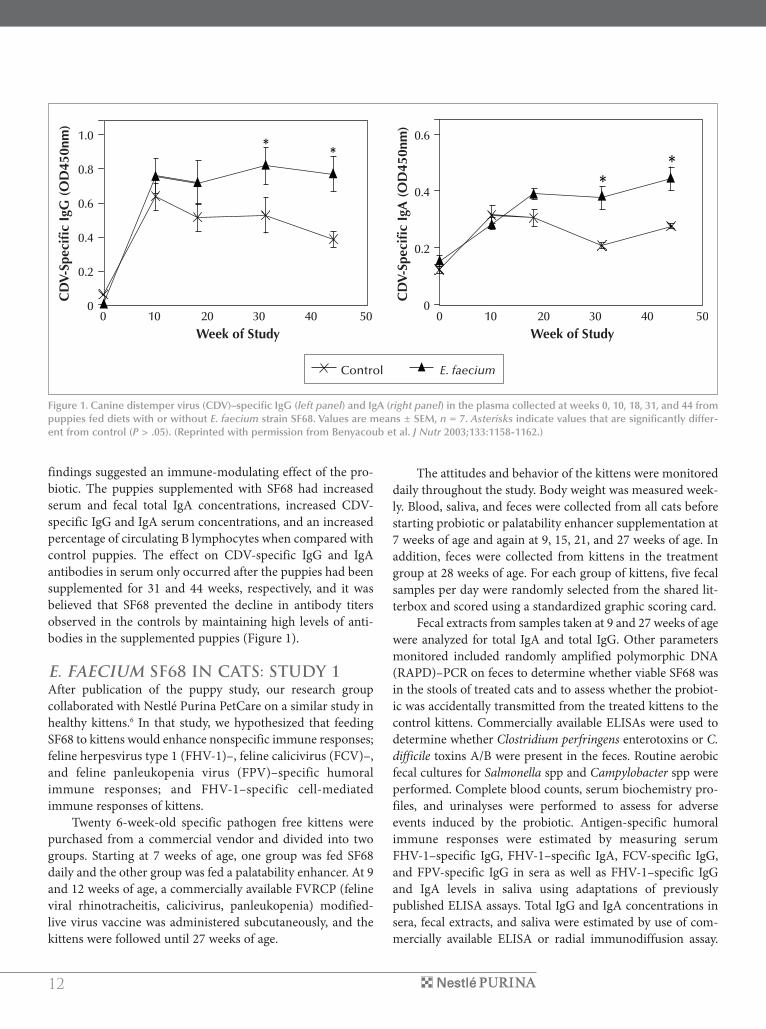
findings suggested an immune-modulating effect of the pro-biotic. The puppies supplemented with SF68 had increasedserum and fecal total IgA concentrations, increased CDV-specific IgG and IgA serum concentrations, and an increasedpercentage of circulating B lymphocytes when compared withcontrol puppies. The effect on CDV-specific IgG and IgAantibodies in serum only occurred after the puppies had beensupplemented for 31 and 44 weeks, respectively, and it wasbelieved that SF68 prevented the decline in antibody titersobserved in the controls by maintaining high levels of anti-bodies in the supplemented puppies (Figure 1).
E. FAECIUM SF68 IN CATS: STUDY 1After publication of the puppy study, our research groupcollaborated with Nestlé Purina PetCare on a similar study inhealthy kittens.6 In that study, we hypothesized that feedingSF68 to kittens would enhance nonspecific immune responses;feline herpesvirus type 1 (FHV-1)–, feline calicivirus (FCV)–,and feline panleukopenia virus (FPV)–specific humoralimmune responses; and FHV-1–specific cell-mediatedimmune responses of kittens.
Twenty 6-week-old specific pathogen free kittens werepurchased from a commercial vendor and divided into twogroups. Starting at 7 weeks of age, one group was fed SF68daily and the other group was fed a palatability enhancer. At 9and 12 weeks of age, a commercially available FVRCP (felineviral rhinotracheitis, calicivirus, panleukopenia) modified-live virus vaccine was administered subcutaneously, and thekittens were followed until 27 weeks of age.
The attitudes and behavior of the kittens were monitoreddaily throughout the study. Body weight was measured week-ly. Blood, saliva, and feces were collected from all cats beforestarting probiotic or palatability enhancer supplementation at7 weeks of age and again at 9, 15, 21, and 27 weeks of age. Inaddition, feces were collected from kittens in the treatmentgroup at 28 weeks of age. For each group of kittens, five fecalsamples per day were randomly selected from the shared lit-terbox and scored using a standardized graphic scoring card.
Fecal extracts from samples taken at 9 and 27 weeks of agewere analyzed for total IgA and total IgG. Other parametersmonitored included randomly amplified polymorphic DNA(RAPD)–PCR on feces to determine whether viable SF68 wasin the stools of treated cats and to assess whether the probiot-ic was accidentally transmitted from the treated kittens to thecontrol kittens. Commercially available ELISAs were used todetermine whether Clostridium perfringens enterotoxins or C.difficile toxins A/B were present in the feces. Routine aerobicfecal cultures for Salmonella spp and Campylobacter spp wereperformed. Complete blood counts, serum biochemistry pro-files, and urinalyses were performed to assess for adverseevents induced by the probiotic. Antigen-specific humoralimmune responses were estimated by measuring serumFHV-1–specific IgG, FHV-1–specific IgA, FCV-specific IgG,and FPV-specific IgG in sera as well as FHV-1–specific IgGand IgA levels in saliva using adaptations of previouslypublished ELISA assays. Total IgG and IgA concentrations insera, fecal extracts, and saliva were estimated by use of com-mercially available ELISA or radial immunodiffusion assay.
0 10 20 30 40 50 0 10 20 30 40 50
1.0
0.8
0.6
0.4
0.2
0
0.6
0.4
0.2
0
Week of Study Week of Study
CD
V-Sp
ecifi
cIg
G(O
D45
0nm
)
CD
V-Sp
ecifi
cIg
A(O
D45
0nm
)
E. faeciumControl
**
* *
Figure 1. Canine distemper virus (CDV)–specific IgG (left panel) and IgA (right panel) in the plasma collected at weeks 0, 10, 18, 31, and 44 frompuppies fed diets with or without E. faecium strain SF68. Values are means ± SEM, n = 7. Asterisks indicate values that are significantly differ-ent from control (P > .05). (Reprinted with permission from Benyacoub et al. J Nutr 2003;133:1158-1162.)
Critical Updates on Canine and Feline Health, 2009 NAVC/WVC Proceedings 13
*
7 9 15 21 27
P = .022
7 9 15 21 27
45
40
35
30
25
20
15
10
5
0
161514131211109876543210
Age (wk) Age (wk)
Lym
phoc
ytes
(%)
Lym
phoc
ytes
(%)
TreatmentPlacebo
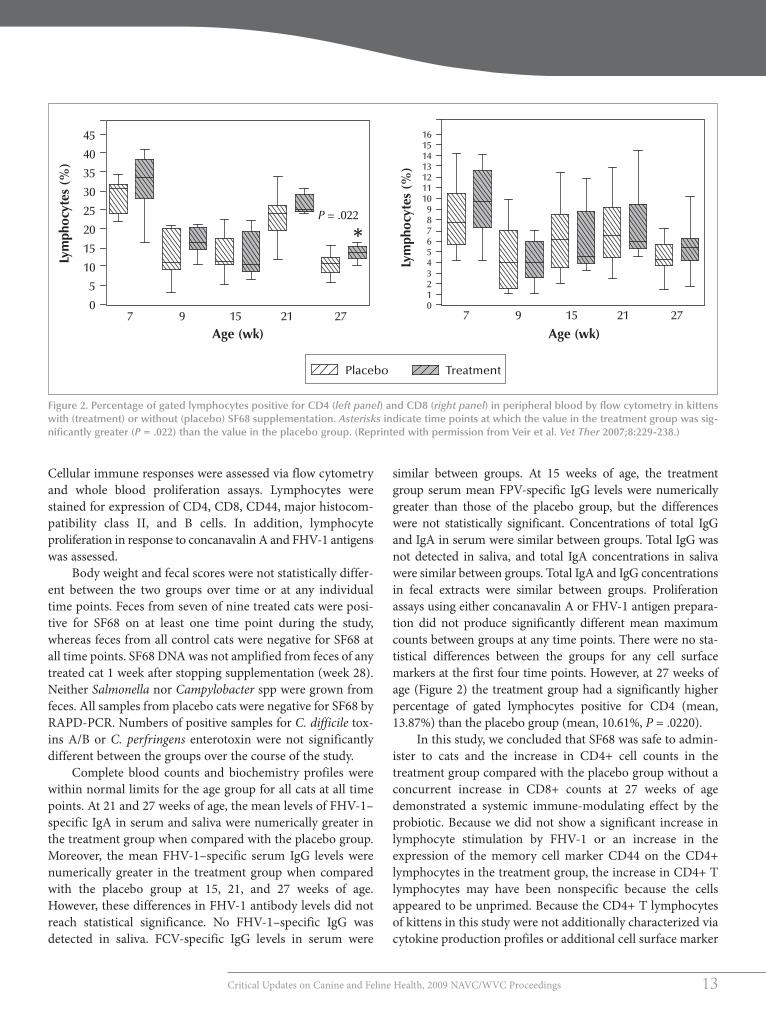
Figure 2. Percentage of gated lymphocytes positive for CD4 (left panel) and CD8 (right panel) in peripheral blood by flow cytometry in kittenswith (treatment) or without (placebo) SF68 supplementation. Asterisks indicate time points at which the value in the treatment group was sig-nificantly greater (P = .022) than the value in the placebo group. (Reprinted with permission from Veir et al. Vet Ther 2007;8:229-238.)
Cellular immune responses were assessed via flow cytometryand whole blood proliferation assays. Lymphocytes werestained for expression of CD4, CD8, CD44, major histocom-patibility class II, and B cells. In addition, lymphocyteproliferation in response to concanavalin A and FHV-1 antigenswas assessed.
Body weight and fecal scores were not statistically differ-ent between the two groups over time or at any individualtime points. Feces from seven of nine treated cats were posi-tive for SF68 on at least one time point during the study,whereas feces from all control cats were negative for SF68 atall time points. SF68 DNAwas not amplified from feces of anytreated cat 1 week after stopping supplementation (week 28).Neither Salmonella nor Campylobacter spp were grown fromfeces. All samples from placebo cats were negative for SF68 byRAPD-PCR. Numbers of positive samples for C. difficile tox-ins A/B or C. perfringens enterotoxin were not significantlydifferent between the groups over the course of the study.
Complete blood counts and biochemistry profiles werewithin normal limits for the age group for all cats at all timepoints. At 21 and 27 weeks of age, the mean levels of FHV-1–specific IgA in serum and saliva were numerically greater inthe treatment group when compared with the placebo group.Moreover, the mean FHV-1–specific serum IgG levels werenumerically greater in the treatment group when comparedwith the placebo group at 15, 21, and 27 weeks of age.However, these differences in FHV-1 antibody levels did notreach statistical significance. No FHV-1–specific IgG wasdetected in saliva. FCV-specific IgG levels in serum were
similar between groups. At 15 weeks of age, the treatmentgroup serum mean FPV-specific IgG levels were numericallygreater than those of the placebo group, but the differenceswere not statistically significant. Concentrations of total IgGand IgA in serum were similar between groups. Total IgG wasnot detected in saliva, and total IgA concentrations in salivawere similar between groups. Total IgA and IgG concentrationsin fecal extracts were similar between groups. Proliferationassays using either concanavalin A or FHV-1 antigen prepara-tion did not produce significantly different mean maximumcounts between groups at any time points. There were no sta-tistical differences between the groups for any cell surfacemarkers at the first four time points. However, at 27 weeks ofage (Figure 2) the treatment group had a significantly higherpercentage of gated lymphocytes positive for CD4 (mean,13.87%) than the placebo group (mean, 10.61%, P = .0220).
In this study, we concluded that SF68 was safe to admin-ister to cats and the increase in CD4+ cell counts in thetreatment group compared with the placebo group without aconcurrent increase in CD8+ counts at 27 weeks of agedemonstrated a systemic immune-modulating effect by theprobiotic. Because we did not show a significant increase inlymphocyte stimulation by FHV-1 or an increase in theexpression of the memory cell marker CD44 on the CD4+lymphocytes in the treatment group, the increase in CD4+ Tlymphocytes may have been nonspecific because the cellsappeared to be unprimed. Because the CD4+ T lymphocytesof kittens in this study were not additionally characterized viacytokine production profiles or additional cell surface marker

14
characterization, it could not be determined whether a Th1 orTh2 response predominated. We believed that sample size orthe duration of the study may have precluded detection of sta-tistical differences between the groups with regard to FPV,FCV, and FHV-1 antibody titers.
E. FAECIUM SF68 IN CATS: STUDY 2The results of the first feline study prompted a follow-upstudy on FHV-1.7 This virus is extremely common in cats andis frequently associated with morbidity because of recurrentocular and respiratory clinical signs associated with the dis-ease (Figure 3). In addition, there is no known drug therapythat consistently eliminates the carrier state, and vaccinationdoes not provide sterilizing immunity. We hypothesized thatfeeding SF68 would decrease clinical disease, episodes ofFHV-1 shedding, and numbers of FHV-1 DNA copies shedover time in cats with chronic FHV-1 infection.
In this study, 12 cats with chronic FHV-1 infection wereadministered either SF68 or a palatability enhancer as a placebo,monitored for clinical signs of disease and for FHV-1shedding, and evaluated for FHV-1–specific humoral andcell-mediated immune responses and fecal microbiome sta-bility. After an equilibration period, mild stress was inducedover time by switching the cats’ housing from cages to ganghousing and back repeatedly over a 5-month period.
The SF68 was well tolerated by all cats. Fecal microbialdiversity was maintained throughout the study in cats supple-mented with SF68 but decreased in cats fed the placebo,indicating a more stable microbiome in cats fed SF68. Upperrespiratory signs of disease were not exacerbated in thismodel of stress. Although results varied among cats, thoseadministered SF68 had fewer episodes of conjunctivitis than
did the placebo group during the supplementation period,suggesting that administration of the probiotic lessened mor-bidity associated with chronic FHV-1 infection.
ONGOING RESEARCH IN DOGSIn previous work, mice administered SF68 and then infectedwith Giardia intestinalis shed fewer trophozoites and Giardiaantigen than did a placebo group.13 In addition, supplementedmice had increased CD4+ cells in Peyer’s patches and in thespleen as well as increased anti-Giardia intestinal IgA and serumIgG when compared with untreated mice. This work promptedour ongoing study in dogs housed in an animal shelter.
We hypothesized that dogs housed in an animal shelterthat are fed SF68 will have decreased episodes of diarrhea andimproved fecal scores than untreated dogs in the same envi-ronment. Two identical rooms of the animal shelter are beingused. Dogs in one room are supplemented daily withFortiFlora, and dogs in the alternate room are supplementeddaily with FortiFlora carrier without SF68. Otherwise, man-agement of the rooms has been and will be identical for theduration of the study. To reduce the risk of a room influenceon the results of the study, the room in which dogs are beingsupplemented with FortiFlora will be switched three timesduring the study.
Routine shelter cleaning and disinfection protocols arebeing followed. At the time of the room switches, the study isdiscontinued for 1 week to lessen the possibility that SF68 sur-viving in the environment could influence the results of thestudy. Before cleaning the room each morning, feces in thecage of each dog are scored by one of the investigators usingthe Purina Fecal Scoring System for Dogs and Cats.
After scoring, feces from dogs with a score of 4 to 7 arecollected and transported to Colorado State University forinfectious disease testing. For each abnormal fecal sample(one sample per dog), a sample with a fecal score of 1 to 3 iscollected and analyzed from a dog housed in the same roomon the same day. Tests performed on feces after transfer toColorado State University include microscopic examinationfor parasite eggs, cysts, and oocysts after zinc sulfate centrifu-gation; immunofluorescent antibody (IFA) testing forCryptosporidium oocysts and Giardia cysts (MeriFluor®Cryptosporidium/Giardia Test Kit, Meridian Bioscience Inc.,Cincinnati, OH); and C. perfringens enterotoxin assay.
In the preliminary analysis, after completion of two ofthree time periods, the trend is for a shorter duration of diar-rhea in dogs housed in the room supplemented with SF68.
SUMMARYThere is mounting evidence derived from controlled studiesin dogs and cats that suggests that certain probiotics may haveclinical benefit beyond stabilization of gastrointestinal micro-
Figure 3. Kitten with conjunctivitis and rhinitis associated with FHV-1infection.

Critical Updates on Canine and Feline Health, 2009 NAVC/WVC Proceedings 15
biome. However, all probiotics cannot be considered equal,and not all products purported to contain probiotics havedetectable activity when tested. Further work will be requiredto define the clinical efficacy of various probiotics.
REFERENCES1. Schrezenmeir J, de Vrese M. Probiotics, prebiotics, and synbiotics—approaching a definition [review]. Am J Clin Nutr 2001;73(2 suppl):361S-364S.
2. de Vrese M, Schrezenmeir J. Probiotics, prebiotics, and synbiotics. AdvBiochem Eng Biotechnol 2008;111:1-66.
3. Baillon MLA, Marshall-Jones ZV, Butterwick RF. Effects of probioticLactobacillus acidophilus strain DSM13241 in healthy adult dogs. Am J VetRes 2004;65:338-343.
4. Marshall-Jones ZV, Baillon MLA, Croft JM, Butterwick RF. Effects ofLactobacillus acidophilus DSM13241 as a probiotic in healthy adult cats. AmJ Vet Res 2006;67:1005-1112.
5. Benyacoub J, Czarnecki-Maulden GL, Cavadini C, et al. Supplementation offood with Enterococcus faecium (SF68) stimulates immune functions inyoung dogs. J Nutr 2003;133:1158-1162.
6. Veir JV, Knorr R, Cavadini C, et al. Effect of supplementation withEnterococcus faecium (SF68) on immune functions in cats. Vet Ther2007;8:229-238.
7. Lappin MR, Veir JK, Satyaraj E, Czarnecki-Maulden G. Pilot study to evalu-ate the effect of oral supplementation of Enterococcus faecium SF68 on catswith latent feline herpesvirus 1. J Feline Med Surg. In press.
8. McNabb B, Isakow W. Probiotics for the prevention of nosocomial pneumo-nia: current evidence and opinions. Curr Opin Pulm Med 2008;14:168-175.
9. Dendukuri N, Costa V, McGregor M, Brophy JM. Probiotic therapy for theprevention and treatment of Clostridium difficile–associated diarrhea: a sys-tematic review. Can Med Assoc J 2005;173:167-170.
10. Isakow W, Morrow LE, Kollef MH. Probiotics for preventing and treatingnosocomial infections: review of current evidence and recommendations.Chest 2007;132:286-294.
11. Weese JS, Arroyo L. Bacteriological evaluation of dog and cat diets that claimto contain probiotics. Can Vet J 2003;44:212-216.
12. Lewenstein A, Frigerio G, Moroni M. Biological properties of SF68, a newapproach for the treatment of diarrhoeal disease. Curr Ther Res 1979;26:967.
13. Benyacoub J, Perez PF, Rochat F, et al. Enterococcus faecium SF68 enhancesthe immune response to Giardia intestinalis in mice. J Nutr 2005;135:1171-1176.

16
D
GrowingOldGracefully:An Overview ofHealthcareManagementof the Aging CatMargie Scherk, DVM, DABVP (Feline)Vancouver, British Columbia, Canada©2008 Jupiter/Ingram Publishing
ver the past decade, the definitions of seniorand geriatric as they pertain to cats havechanged. These changes not only reflect
greater longevity (life expectancy in cats has risen to an aver-age of 14 to 16 years of age) but also the benefits of improvedhealthcare and nutrition. We are also seeing the results of theacceptance and compliance of the general cat-owning publicwith our recommendations for vaccination protocols, dentalhygiene, and nutritional counseling and nutritionally balancedfeline-specific diets.
While we should continue to focus and expand our clienteducation efforts, the veterinary community—and to a greatextent the veterinary industry—has done a good job of clienteducation. We should be proud of ourselves!
WHAT AGING ENTAILSA cat is generally considered to be “senior” from about 9 to 12years of age and “geriatric” starting around 13 years of age;these age ranges correlate roughly with human ages of 52 to64 and 68 and older, respectively.1
At any age, there are disorders and changes particular tothat age group or stage of progression. A cat may begin tomanifest serious age-related disorders (e.g., renal insufficien-cy) at around 8 to 9 years of age on average. This does notmake that individual old—or less treatable. In addition, withaging comes a set of cellular changes that are somewhat pre-dictable and that need to be considered in our approach tohealthcare, both preventive and therapeutic.
Aging is a complex process reflecting increasing damageat the cellular and organismal level. To quote from Robbins2:Aging “begins at the moment of conception, involves . . . differ-entiation and maturation,” and, at some point, “leads to theprogressive loss of functional capacity characteristic of senes-cence, and ends in death.” Organismal aging may be affected bygenetics, nutrition, social environment, and the occurrence ofage-related diseases. Cellular aging, on the other hand, includesprogressive accumulation of sublethal injury (e.g., from free
radical damage), resulting in either the cell’s death or its dimin-ished capacity to repair itself.We can affect these changes—bothorganismal and cellular—to some degree through nutritionalintervention.
NUTRITIONAL CONSIDERATIONSOF AGINGMaintenance energy requirements (MERs) vary with age,genetic potential, health status, and gender (i.e., whether intactor altered). MERs decrease with aging in humans, dogs, andrats. In cats, some studies report no change. However, whenevaluated over longer periods, these studies have found thatfeline MERs initially decrease until about 11 years of age. 3–5 Ascats age, their lean body mass (i.e., skeletal muscle, bone, skin,organs) decreases, just as it does in other species. Because leanbody mass is a primary driver of metabolism, this results in areduction inMER. Thus, senior cats tend to gain weight (oftenbecoming overweight or obese) as their energy needs decreaseunless there is a concurrent decrease in energy intake.Interestingly, once cats enter their geriatric years, they actuallylose weight, both lean and fat. It is this loss of lean body massthat is of special concern. At this point, MERs per unit of bodyweight actually increase in cats.3–5
Key to determining the appropriate diet for any givenindividual is a nutritional assessment. This assessment shouldinclude identifying body composition, generally by using abody condition scoring (BCS) system, and checking bodyweight at every visit. Tracking the percentage weight change ishelpful in detecting trends and alerting both the practitionerand the client to insipient or blatant physiologic alterations.Use of a simple diet history form provides important nutri-tional information by revealing food fed, brand, quantity,treats, and supplements (Figure 1).
A recent study on feeding the healthy older cat6 examinedwhether feeding a complete and balanced diet, in addition tothe use of dietary antioxidants (vitamin E, beta-carotene)alone or in combination with a prebiotic (chicory root) and a
O

Critical Updates on Canine and Feline Health, 2009 NAVC/WVC Proceedings 17
Figure 1. Diet history form for feline patients. Adapted from: Laflamme DP. Nutrition for aging cats and dogs and the importance of body con-dition. Vet Clin North Am Small Anim Pract 2005:35:720 with permission from Elsevier.
Date:___________________________________________
Client’s name:____________________________________________ Cat’s name: _____________________________________
Breed: __________________________________________________ Gender: M MN F FS
Age:____________________ Body weight: __________________ Body condition score: ___/9
Activity level: High Medium Low Very low
What food(s) are currently fed for the cat’s main meal?
Dry: Never Occasional/small proportion About half Mostly Exclusively
If fed, what brands and amounts are fed most often? _____________________________________________________________
______________________________________________________________________________________________________________
Canned: Never Occasional/small proportion About half Mostly Exclusively
If fed, what brands and amounts are fed most often? _____________________________________________________________
______________________________________________________________________________________________________________
Home prepared: Never Occasional/small proportion About half Mostly Exclusively
If fed, please provide recipes used: ____________________________________________________________________________
______________________________________________________________________________________________________________
What treats and/or supplements are currently fed?
Commercial treats: No Yes
What brands and amounts are fed most often? __________________________________________________________________
Fresh foods/table scraps: No Yes
What foods and amounts are fed most often? ___________________________________________________________________
Dietary supplements: No Yes
What supplements and amounts are fed most often? _____________________________________________________________
Have there been recent changes in foods/brands fed? No Yes
If so, when and why?________________________________________________________________________________________
How is your cat’s appetite? Good Poor Any recent changes? ____________________________
How frequently does your cat defecate? 0–1×/day 2–3×/day 4× or more/day Don’t know
How would you characterize its stool? Firm/hard Formed but not hard Loose
Where does your cat spend most of its time? Indoors Outdoors About half in and half out
How much time does your cat spend exercising each day? <30 min 30–60 min More than 60 min
Are there other pets in your household? No Yes
Do you have any questions regarding your cat’s diet? _________________________________________________________
______________________________________________________________________________________________________________
DIET HISTORY FORM

18
Figure 2. Diagnostic differentials for feline weight loss. Recommended diagnostics for weight loss in cats will vary and may include CBC, serumbiochemistry panel, serum thyroxine concentration, serum cobalamin and folate concentrations, complete urinalysis, fecal flotation, FeLV/FIV test,thoracic and abdominal radiography, and abdominal ultrasonography. A gastrointestinal biopsy may also be necessary in some cases.
Differential Diagnoses for Weight Loss in Cats
Inadequate intake Excessive nutrientloss/utilization
Unable to eat(dysphagia)
Refuses to eat
Consider:• Poor food quality• Inadequate
quantity of food
Consider:• Diabetes mellitus• Hyperthyroidism• Neoplasia• Protein-losing
nephropathy• Protein-losing
enteropathy
Consider:• Oral neoplasia• Dental or orofacial
fracture• Dental disease• Dental pain• Neuropathy
Consider:• FeLV/FIV• Renal insufficiency• Renal failure• Hepatopathy• Neoplasia• Inflammatory
bowel disease• Fungal infection• Central nervous
system disease• Bored with diet
Maldigestion/malabsorption
Consider:• Inflammatory
bowel disease• Lymphoma• Exocrine
pancreaticinsufficiency
• Systemic fungalinfection
Overutilization
Consider:• Lactation• Workload
Weight loss
Poor appetiteGood appetite
blend of oils to supplement omega-3 and omega-6 fatty acids,had a beneficial effect on the health and longevity of catswhen compared with a complete and balanced diet withoutsupplementation. Ninety cats over 7 years of age (groupedinto 7–9 years of age, 10–12 years of age, and 13+ years of ageat the start) were studied in a controlled environment for 5years. As expected, all cats lost weight as they aged, but cats inthe fully supplemented group lost less weight than those inthe other two groups. Other beneficial effects noted wereimproved lean body mass scores, improved fecal microflora,fewer diseases (notably gastrointestinal) during the study, andlonger life.
Studies in geriatric cats show that the ability to digest fatdecreases with age.7 Additionally, approximately 20% of catsover 14 years of age have a reduced ability to digest protein.This is of clinical relevance when we try to design the optimalnutritional regimen for our older feline patients: Protein andfat restriction may well be contraindicated in individual cats.Especially if they are underweight, older cats will benefit froma more energy-dense, highly digestible diet to help offset age-related digestive and metabolic changes.
The skinny older cat, especially if inappetent or anorec-tic, has a limited ability to conserve its body’s proteins. Thisresults in a negative nitrogen balance, protein:calorie malnu-trition, and deterioration of protective mechanisms, affectingimmunity, red cell hemoglobin content, muscle mass, andtissue-healing ability. Inappetence and anorexia must bedealt with promptly and adequately. Cats have limited stor-age of many nutrients and a restricted ability to downregulatenumerous metabolic processes. Cats were designed to eatmultiple small meals that are high in protein and moderate infat per day. Hepatic lipidosis is always a risk when catsbecome inappetent, especially in the previously obese cat.
It is essential to calculate daily caloric and protein require-ments, just as one routinely calculates fluid needs as part of atherapeutic plan (calories: 50 kcal/kg ideal body weight/day; 4g protein/kg ideal body weight/day). Appetite stimulants,including cyproheptadine (1 mg/cat PO bid) and mirtazapine(3 mg/cat PO q72h), may help jump-start a cat’s appetite, butone must be wary to not lose sight of total calories consumed.If a cat is eating, but not enough, supportive feeding (assistedsyringe or tube feeding) must be considered.

Critical Updates on Canine and Feline Health, 2009 NAVC/WVC Proceedings 19
For a patient with apparent maldigestion, such as thatseen with chronic small intestinal disease, folate and cobal-amin supplementation have been shown to be beneficial(folate: 0.5 to 1.0 mg/cat/day PO for 1 month; cobalamin: 250mg/cat SC once weekly for 6 weeks).8,9
Weight loss in older cats can be a frustrating and worri-some change (Figures 2 and 3). Although possibly normal in theolder individual, weight loss may have serious clinical implica-tions for the cat. It is important that its cause be determined.
AGE-ASSOCIATED CONDITIONS ANDCHANGES IN CATSAs cats age, we see a marked increase in metabolic distur-bances related to the urinary tract (e.g., chronic renalinsufficiency, pyelonephritis and certain forms of lower uri-nary tract disorders, calcium oxalate ureteronephrolithiasis),endocrine system (e.g., hyperthyroidism, diabetes mellitus),osteoarthritis (OA), dental diseases, and neoplasia. Certaininfectious diseases (e.g., FIP) become more likely in the olderindividual. A decline in functioning of the senses occurs fre-quently, and behavioral changes suggestive of cognitivedysfunction may be seen in some individuals.
Ophthalmologic aging changes include iris atrophy,melanin deposition on the irises, and lenticular sclerosis.Although the former do not appear to affect vision, lenticularsclerosis results in a decreased acuity that is usually mostobvious in dim lighting. Impaired hearing is fairly common inolder cats, with selective frequencies being affected, similar towhat occurs in older humans. The result of these alterations inperception may be “nocturnal yowling” as the individualstrives to orient itself with the help of cues from the caregiver.Other causes of this behavior include hyperthyroidism orhypertension (both presumably resulting in agitation), cogni-tive dysfunction, or pain.
Development of inappropriate elimination behavior mayhave several age-associated causes. Pain from arthritis maymake getting to or into the litterbox difficult. Past experiencesof discomfort from cystitis or difficult stool passage mayresult in aversion to litterbox use. Urge incontinence (urinaryor fecal) may result in the inability to get to the litterbox intime, resulting in the development of an alternative locationfor elimination. Hyperthyroidism may result in defecation ofnormal or diarrheic feces outside the litterbox.
We also see conditions related to altered hydration andnutritional requirements, such as “constipation.” Constipationis largely a sign of dehydration. Cellular water content has pri-ority over fecal water content; thus, primary treatment shouldbe directed at rehydration and correction of the underlyingcause(s) of that problem, rather than the consistency of thestool and its movement (e.g., with laxatives). Use of promotil-ity agents, laxatives, osmotic agents, and fiber-enriched diets
Figure 3. Diagnostic algorithm for cats with weight loss.
Diagnosing Weight Lossin Cats
ABNORMAL
Consider:• Renal insufficiency• Renal failure• FeLV/FIV• Hepatopathy• Neoplasia
ABNORMAL
Consider:• Inflammatory
bowel disease• Neoplasia• Fungal infection
NORMAL
Consider:• Central nervous
system disease
NORMAL
Seek localizing lesion (perform diagnostics; see Figure 2)
Perform gastrointestinal biopsy
should be used conservatively and after rehydration has beenaddressed.
Because of most older cats’ reduced ability to reclaimwater from their urine, special attention should be paid tocounseling the client regarding hydration. Many cats willaccept circulating water fountains and flavored broths.Increasing the proportion of canned food fed and addingwater to the food are the easiest ways to address the increasedfluid needs of the cat. Subcutaneous fluid injections adminis-tered at home become part of daily maintenance care formany elderly cats.
Normal radiographic changes seen in the older felinepatient include an increase in sternal contact of the heart. Adecrease in bone density may be seen in very elderly individ-uals. Some minor calcific changes may occur in thepulmonary parenchyma of normally aging cats. Spondylosis,especially of the lumbar vertebrae, should be looked for, butbony changes may be seen in any part of the spinal column;degenerative, proliferative, or lytic changes of the joints alsooccur. Calcifications may be noted in the kidneys; these areoften insignificant, representing calcification of old bloodclots. Differentiation from nephroliths can be made by ultra-sound. Similarly, adrenal calcification should not beoverinterpreted in cats, as it may be a normal age-relatedchange. Although some radiographic findings mentionedhere can be incidental (e.g., altered cardiac silhouette,spondylosis, renal calcification), they can also signify seri-ous disease in some cats.

20
THE PAINS OF AGINGOral diseases such as periodontal disease, gingival recession,odontoclastic resorptive lesions, stomatitis, and oral masses areall potentially painful. Optimizing oral health cannot beoveremphasized, yet clients may express concern about anes-thetizing the elderly cat for dental prophylaxis or to address anexisting dental problem. Several papers have looked at risk fac-tors for anesthesia. Properly classifying the patient using theAmerican Society of Anesthesiologists’ classification system (see
box above) and takingappropriate precautions(e.g., preanesthetic bloodwork, intraoperative mon-itoring) were found tominimize perianestheticcomplications in cats; agewas not found to be a riskfactor.10,11 Reminding ourclients that the majority ofanesthetic procedures inhuman medicine are per-formed on elderly patientsmay provide reassurance
that safe anesthesia is possible, allowing their cat to benefit fromdental prophylaxis or other anesthetic procedures.
Surgical manipulation of tissue results in inflammation,direct trauma, and cell damage, all of which will initiate the painresponse. Similarly, common procedures, including blood col-lection, intravenous catheter placement, and restraint of a thinor arthritic patient, may be uncomfortable for patients. In addi-tion, numerous potentially chronic painful conditions afflictsenior and geriatric cats. Bacterial cystitis and pyelonephritisoccur more frequently in older cats, and although the incidenceof interstitial/sterile cystitis or inflammatory bowel disease isnot different than in younger cats, these conditions still causepain in older cats. In addition, the likelihood of neoplasiaincreases with increasing age. The need for analgesia must beconsidered as part of any treatment plan for the older cat.
Recognition of degenerative joint disease (DJD) pain andother forms of chronic pain is a relatively recent focus in veteri-nary medicine. The incidence of DJD or OA (which is a form of
DJD characterized by cartilage deterioration of diarthrodial syn-ovial joints) appears to be much more common than previouslythought and is probably a major cause of discomfort in agingcats. Secondary OA may be caused by joint trauma (i.e., frac-tures, ligamentous injuries), infectious or immune-mediatedinflammation, compensation for congenital or developmentalconditions, and neoplastic, endocrine (diabetic), or metabolicconditions. OA involves a cascade of mechanical and biochemi-cal events resulting in articular cartilage deterioration, synovialmembrane inflammation, soft-tissue changes, and osteophyteformation with bone remodeling.
In one study of the prevalence of DJD in cats, Hardie andcolleagues12 reviewed 100 radiographs (taken as part of a diag-nostic workup for multiple reasons) of cats older than 12 yearsof age and found that 90% of these cats showed evidence ofDJD. Interestingly, in only four of these patients’ medicalrecords was a concern noted for DJD. Does this mean that, asin dogs, the clinical signs of OA in cats do not correlate wellwith radiographic findings, or that we are very poor at recog-nizing the signs? Godfrey13 performed another retrospectiveradiographic study looking at cats of all ages. This studyshowed radiographic changes suggestive of OA in 22% of cats;in 33% of these cats’ medical records, clinical signs werenoted. In a third study,14 the prevalence of radiographic signsof DJD or OA in 218 cats was 33.9%, and the prevalence ofclinical signs was 16.5%; most of these signs were in cats olderthan 10 years of age.
Lameness is not a common clinical sign of DJD in cats.Rather, the signs are insidious and can be erroneously attrib-uted to aging. They include inappropriate elimination (oftenadjacent to the litterbox), decreased grooming, antipathy tobeing combed, reluctance to jump up or down, sleeping more,moving less, withdrawing from human interaction, and pos-sibly even hiding. When activity monitors have been attachedto the collars of cats with DJD, activity counts increased withNSAID treatment, suggesting alleviation of musculoskeletaldiscomfort.15 More information on recognizing pain in cats isavailable on the International Veterinary Academy of PainManagement website at www.ivapm.org.
CARING FOR THE ELDERLY CATOlder feline patients have particular therapeutic and nursingneeds. It is important to keep the hospital stay as short andstress free as possible because older cats are less tolerant of thehospital environment and are more prone to depression andstress or anxiety. Some problems may be masked and unde-tectable even with careful and thorough examination, yetmake their presence known when the patient is stressed.
Many of the medical conditions that older cats developrequire ongoing home care, such as subcutaneous fluid admin-istration, frequent medication administration, and dietary
Class 1—Normal, healthy patientClass 2—Patient with mild systemic diseaseClass 3—Patient with severe systemic diseaseClass 4—Patient with severe systemic disease that is a
constant threat to lifeClass 5—Moribund patient not expected to survive
without the procedure
ASA Physical Status Classification System
Slow, gentle
persistence with
acute and empathic
observation is crucial
in the care and
handling of older cats.

Critical Updates on Canine and Feline Health, 2009 NAVC/WVC Proceedings 21
manipulation. We should do everything we can to keep ouraging patients as comfortable as possible. For example:
• Some cats prefer medications administered subcuta-neously rather than orally; when the agent exists inusable subcutaneous format, this is often an easier routefor clients to take.
• The potential need for analgesia should be considered foreach elderly patient.
• Palatability of diets, especially in the face of declining sens-es, is especially important. In addition, many older catsneed an increase rather than a decrease in biologicallyavailable protein. When possible, diet changes should beintroduced slowly to minimize the risk of food aversion.
Slow, gentle persistence with acute and empathic observationis crucial in the care and handling of older cats.
A screening program for older cats is an excellent man-agement tool. Offering such programs as part of an overallwellness approach provides the best preventive medical careand gives the clinic a more predictable income base. At theauthor’s clinic, the mature cat program consists of an exami-nation, a urinalysis, a blood pressure determination, and ablood panel, including CBC with differential; serum chem-istry profile with amylase, lipase, and electrolytes; and a basalserum thyroxine measurement. We recommend this screen-ing annually for all cats starting at 8 years of age and twiceannually for cats older than 14 years of age or once abnormal-ities have been detected to assist in the management of theseproblems. With the introduction of the Healthy Cats for Lifeprogram sponsored by the American Association of FelinePractitioners (www.healthycatsforlife.com), the new recom-mendation is semiannual wellness exams in cats of all ages toincrease the opportunity to detect illness in cats by teachingpet owners the 10 subtle signs of sickness. Client acceptanceof this and other wellness programs is very high.
Finally, when is enough, enough? Although we have theability to help and prolong life, the quality of such must befirst and foremost in the practitioner’s and client’s minds.Remember: “Just because we can, doesn’t mean we should.”The author refers the reader to a paper on ethical issues in
geriatric feline medicine.16 We can help and do a lot; we justhave to know when to stop.
We are fortunate to practice in times that allow us to notonly recognize changes and conditions associated with agingbut also influence the experience of growing older. Withcourage and perspective, we can improve the lives of ourpatients, making their older years more enjoyable for boththem and their human companions.
REFERENCES1. Metzger FL. Senior and geriatric care programs for veterinarians. Vet Clin
North Am Small Anim Pract 2005;35:743-753.2. Cellular injury and cellular death. In: Cotran RS, Kumar V, Robbins SL, eds.
Robbins: Pathologic Basis of Disease. 5th ed. Philadelphia: WB Saunders;1994:32-33.
3. Laflamme DP, Ballam JM. Effect of age on maintenance energy require-ments of adult cats. Compend Contin Educ Pract Vet 2002;24(suppl 9A):82.
4. Cupp C, Perez-Camargo G, Patil A, et al. Long-term food consumption andbody weight changes in a controlled population of geriatric cats [abstract].Compend Contin Educ Pract Vet 2004;26(suppl 2A):60.
5. Armstrong PJ, Lund EM. Changes in body composition and energy balancewith aging. Vet Clin Nutr 1996;3:83-87.
6. Cupp CJ, Jean-Philippe C, Kerr WW, et al. Effect of nutritional interventionson longevity of senior cats. Intern J Appl Res Vet Med 2006;4(1):34-50.
7. Perez-Camargo G. Cat nutrition: what’s new in the old? Compend ContinEduc Pract Vet 2004;26(suppl 2A):5-10.
8. Simpson KW, Fyfe J, Cornetta A, et al. Subnormal concentrations of serumcobalamin (vitamin B12) in cats with gastrointestinal disease. J Vet InternMed 2001;15(1):26-32.
9. Reed N, Gunn-Moore D, Simpson K. Cobalamin, folate and inorganic phos-phate abnormalities in ill cats. J Feline Med Surg 2007;9(4):278-288.
10. Hosgood G, Scholl DT. Evaluation of age and American Society ofAnesthesiologists (ASA) physical status as risk factors for perianestheticmorbidity and mortality in the cat. J Vet Emerg Crit Care 2002;12(1):9-15.
11. Brodbelt DC, Pfeiffer DU, Young LE, et al. Risk factors for anaesthetic-relateddeath in cats: results from the confidential enquiry into perioperative smallanimal fatalities (CEPSAF). Br J Anaesth [serial online]. 2007;99(5): 617-623.Available at: http://bja.oxfordjournals.org/cgi/content/full/99/5/617. AccessedNovember 3, 2008.
12. Hardie EM, Roe SC, Martin FR. Radiographic evidence of degenerative jointdisease in geriatric cats: 100 cases (1994–1997). JAVMA 2002;220(5):628-632.
13. Godfrey DR. Osteoarthritis in cats: a retrospective radiological study. J SmallAnim Pract 2005;46:425-429.
14. Clarke SP, Mellor D, Clements DN, et al. Prevalence of radiographic signs ofdegenerative joint disease in a hospital population of cats. Vet Rec 2005;157:793-799.
15. Lascelles BD, Hansen BD, DePuy V, et al. Evaluation of client specific out-come measures and activity monitoring to measure pain relief in cats withosteoarthritis. Proc 2nd World 33rd Annu Vet Orthop Soc Conf 2006.
16. Rollin BE. Ethical issues in geriatric feline medicine. J Feline Med Surg2007;9(4):326-334.

22
Chronic Diarrheain Kittens and Cats:It Can Be StoppedDebra L. Zoran, DVM, PhD, DACVIM-SAIMCollege of Veterinary Medicine and Biomedical SciencesTexas A&M UniversityCollege Station, Texas
hronic diarrhea is the second most commonproblem in kittens adopted from animalshelters and is often caused by dietary issues,
infectious agents, or parasitism. Diarrhea in adult cats oftenhas different causes than diarrhea in kittens, with inflamma-tory bowel disease (IBD) and food allergy being commoncauses; however, the condition remains a frustrating problemin cats. This overview discusses some of the more commoncauses of diarrhea in kittens and cats as well as the bestapproaches for diagnosis and treatment. The role of dietarytherapy in the management of feline diarrhea is also discussed.
DETERMINING THE CAUSEOF THE DIARRHEAThe first step in assessing kittens (or cats) with diarrhea is todetermine whether the diarrhea is primarily of small- orlarge-bowel character. By doing this, the practitioner canbegin to narrow the focus of the differentials list and diagnos-tic plan. This is particularly helpful for large-bowel diarrhea,which is caused by diseases of the colon; these diseases are farfewer in number and have fewer diagnostic options thansmall-bowel diarrhea in kittens or cats.
The list of potential causes of diarrhea in kittens is narrowerthan for adult cats and primarily includes anatomic/structural(foreign body/intussusception), drug- or toxin-related, infec-tious/parasitic, and nutritional causes. Diarrhea in kittens maybe mild and more of a nuisance or a severe, hemorrhagic, life-threatening condition. Because this is a common problem,knowledge of the most frequently encountered causes of diar-rhea in kittens and cats is essential in formulating appropriatediagnostic and treatment plans for these small patients.
SELECTED INFECTIOUS CAUSES OFDIARRHEA IN KITTENS AND CATSTritrichomonas Infection1–5
Trichomoniasis, caused by Tritrichomonas foetus, has recentlybeen recognized as a pathogen in kittens and adult cats in the
United States. This protozoan is the same organism that caus-es abortion, early embryonic death, and pyometra in infectedcattle. In cats, however, the organism infects the large intestin-al mucosa and causes chronic large-bowel diarrhea, which isinitially characterized by hematochezia, increased frequencyof defecation, increased mucus, and tenesmus. With chronic-ity, the diarrhea can become small-bowel or mixed characterdue to changes in the bacterial flora from antibiotic therapy,dietary changes, or simply disruption of the normal florafrom the infection. Other clinical signs include painful defe-cation in an otherwise healthy, alert, and active kitten oryoung adult cat and anal hyperemia and swelling. Most infect-ed cats are young (average age, 9 months), but infection canoccur at any age.
Cats that are exposed to the organism are highly likely tobecome infected (in a recent study, all eight cats that wereexposed to the trophozoites became infected—the organismwas cultured from their feces throughout the 200 days of thestudy), and infection is likely to be persistent. However, infec-tion with T. foetus does not necessarily correlate with thedegree of clinical signs, as there are many cats that culturepositive for the organism but are completely asymptomatic.The prevalence of this infection in the general population isunknown, but in a paper that reported the prevalence of pos-itive cats at a large international show, 31% (36/117 cats) wereaffected. The infection can be easily misdiagnosed as giardia-sis unless the observer is trained to recognize the differencesin the two species. Coinfection with Giardia spp has beendocumented in 12% of cats. Infections are most commonlyfound in young cats from crowded housing conditions (e.g.,cat “collectors,” catteries, rescue groups, shelters), which mayreflect an increased opportunity for exposure or, alternatively,environmental stress and immature immune function inyoung cats.
Diagnosis of this infection can be made by one of fourapproaches, which are listed here in order of relative ease ofusing the test: (1) direct examination of a fecal smear for the
C

Critical Updates on Canine and Feline Health, 2009 NAVC/WVC Proceedings 23
trophozoites, (2) fecal cultures for the organism (using theInPouch™ TF kit, BioMed Diagnostics, White City, OR), (3)polymerase chain reaction (PCR) testing of feces (must besubmitted to specific labs), and (4) colonic mucosal biopsy.The fecal smear test is the least expensive but has the lowestsensitivity (14%), so errors in diagnosis can be made by inex-perienced observers or in cats with intermittent shedding orsevere diarrhea, resulting in reduced observation of tropho-zoites. However, it is still the easiest and potentially fastestway to make a definitive diagnosis. The InPouch TF kit ismore sensitive than the fecal exam but takes up to 12 days togrow the organism for diagnosis. The samples can be sent toa lab for culture, or the culture kits can be obtained and usedin the practice setting. Most commonly, when the organism iscultured in the pouch, PCR testing is used to confirm infec-tion with T. foetus because other protozoa can grow easily inthis medium. PCR testing is the most sensitive method ofdiagnosis, but it is also more expensive and the results takelonger to obtain.
Therapy for cats infected with trichomonads is difficultbecause no safe, readily available drug exists for treating theinfection. Ronidazole at a dosage of 30 to 50 mg/kg POq12–24h (powder-on-feed antibiotic used in the treatment ofturkey canker) has been shown to reduce diarrhea in cats withtrichomoniasis and clear the infection; however, some catsmay continue to shed the organism for life. In a recent study byGookin, ronidazole at 30 mg/kg once daily was as effective astwice-daily dosing and was less likely to result in side effects.Ronidazole is not approved for use in cats and is potentiallyhepatotoxic and neurotoxic. The most common adverse eventis neurotoxicity, the signs of which include abnormal behav-iors, ataxia, seizures, and tremors. This drug should be usedonly in circumstances in which the owners understand therisks and when the diagnosis of trichomoniasis is confirmed. Itshould not be used empirically to treat cats with undiagnoseddiarrhea. All other antibiotics and antiparasiticides, includingenrofloxacin, fenbendazole, metronidazole, and tylosin, havenot been shown to be effective against T. foetus and, in somecats, may exacerbate diarrhea by altering the normal flora orresult in delay of clinical remission. Clinical remission of thediarrhea (not necessarily clearing of infection) has been shownto occur in almost all infected cats, usually by 2 years of age.However, many cats that have this infection are not acceptableindoor pets because of the malodorous feces they produce.
At this time, there is no evidence that this organism iszoonotic, but it certainly is infectious to other cats; thus, appro-priate infection prevention measures should be instituted.
Cryptosporidiosis4,6Cryptosporidium parvum is a coccidian parasite that infects themicrovilli of the intestinal epithelium of kittens and immuno-
suppressed cats. The disease caused by this infection can rangefrom an asymptomatic carrier to mild, transient illness to pro-longed, life-threatening malabsorption syndromes. In someadult cats, the organism can cause intestinal infiltrates similar tothose observed with classic IBD, and because the organisms arevery small, the disease can be difficult to diagnose. In addition,most affected cats have small-bowel diarrhea, but the diseasevaries considerably between individuals.
Cryptosporidiosis has a high prevalence rate in cats (8%to 87% by serology); therefore, diagnosis should be made bydetection of the organism in feces using an ELISA test orimmunofluorescence assays on feces. The organisms can beobserved in feces at high power, but they are extremely small(less than 4 µm) and can be easily missed unless special stainsor assays using immunofluorescence and careful observationare employed. Further complicating the diagnosis, the organ-isms are shed intermittently, causing infected cats to oftenhave negative fecal fluorescence exams. Thus, repeated examsmay be required to make a definitive diagnosis.
Treatment of kittens infected with cryptosporidiosis isvery difficult because the drugs purported to be effectiveagainst this organism are either toxic or ineffective in cats(e.g., nitazoxanide, paromomycin). Metronidazole, tylosin,and other commonly used antimicrobials are ineffective ineradicating the organism. They may improve diarrhea if abacterial component is active, but in most cases these antimi-crobials are not helpful. However, azithromycin (5 to 10mg/kg PO q12–24h) is effective in humans, and although itseffectiveness in cats for this infection is unknown, its use inthese cases should be considered.
Because cryptosporidiosis is zoonotic, the person han-dling the infected feces needs to use appropriate precautions,such as wearing gloves and cleaning any utensils with a disin-fectant (e.g., bleach).
Giardiasis4,6–9Giardia spp are a frequent cause of diarrhea in cats and kit-tens, with a prevalence rate reported to be 4% nationally, butthe infection rate is much higher in shelters and some geo-graphic areas. In many adult cats, Giardia spp infections aresubclinical or transient, but in kittens, infection is classicallyassociated with an acute onset of malodorous, pale, mucoiddiarrhea. Many of these cats start with large-bowel diarrhea,but it is very common for the diarrhea to become small-boweldue to factors such as bacterial changes and chronic infectioncausing inflammation and secretory changes.
The diagnosis is relatively straightforward when thetrophozoites or cysts are identified on fresh fecal smears or aflotation. However, because the cysts are shed intermittentlyand can be misidentified or confused with other fecal arti-facts, the sensitivity of this approach is only about 50%. The

24
sensitivity increases to 90% if zinc sulfate flotation is used toexamine three separate fecal samples.
A recent study conducted in animal shelters evaluated theperformance of commercially available tests for detectingGiardia spp in cats. The highest sensitivity and specificity forGiardia spp were achieved with the human-based ProSpecT®Giardia Microplate Assay (Alexon Inc., Sunnyvale, CA), withresults of 91.2% and 99.4%, respectively. The SNAP Giardiatest kit (IDEXX Laboratories, Westbrook, ME), an in-housediagnostic test that detectsGiardia cyst wall protein 1 (GCWP-1) in feline and canine feces, had a sensitivity of 85.3% and aspecificity of 100%. When fecal flotation was combined withthe SNAP test, the sensitivity increased to 97.8%.
Treatment of giardiasis in cats and kittens has not changeddrastically for many years and includes specific antiprotozoaltherapy combined with environmental control. Metronidazole,at a dosage of 25 mg/kg PO q12h for 7 days, continues to be a
highly effective therapyfor the disease in affectedcats. Fenbendazole hasbeen anecdotally reportedto be effective in cats at adosage of 50 mg/kg POq24h for 5 days, but onlyone clinical study has beenreported; in that study, thecats were coinfected withCryptosporidium and theresponse to treatment wasless than optimal (50%).Therefore, the true effec-tiveness of this drugagainst Giardia spp is not
known. Studies are under way using Drontal® Plus (BayerAnimal Health, Shawnee Mission, KS)—an antiparasiticidaltherapy labeled for use in dogs—to control Giardia infectionsin cats. Preliminary data show a reduction in shedding of cystsand a clearing of the infection in treated cats, but additionalstudies are needed to demonstrate safety and efficacy.Vaccination with the commercially available Giardia vaccine(GiardiaVax, Fort Dodge Animal Health, Overland Park, KS) isineffective in preventing infection or shedding of cysts and isnot recommended for routine use in household cats.
Because reinfection is a major cause of persistence orrecurrence of infection in a household, cattery, or shelter set-ting, institution of appropriate environment control measuresis essential. These measures include environmental decontam-ination (i.e., cleaning of all floors, cages, litterboxes, andsurfaces that have been in contact with feces with quaternaryammonium or bleach containing disinfectants), coat cleaning(i.e., bathing or shaving long-haired cats), and isolation of
affected animals during the diarrheic phase to prevent infec-tion by co-grooming, etc. This organism is zoonotic; therefore,appropriate education about handling of infected cats and kit-tens is an important aspect of the environmental controlprocedures implemented.
DIARRHEA IN ADULT CATSDiarrhea, with or without other signs of GI disturbance suchas inappetence, vomiting, or weight loss, is a common reasonfor cats to be presented for veterinary care. As with kittens,infectious, mechanical, nutritional, and parasitic causes mustall be considered. However, in adult cats, the most commoncauses of diarrhea are inflammatory (e.g., IBD) or dietary(e.g., dietary sensitivity or intolerance). Other less commonbut important causes include neoplasia (e.g., lymphoma) andspecific diseases (e.g., endocrinopathies, hepatopathies,regionally specific causes such as histoplasmosis).
Inflammatory Bowel DiseaseIBD10,11 in cats is characterized by persistent clinical signs(e.g., diarrhea, inappetence, vomiting, weight loss) consistentwith GI disease that occur concurrently with histologic evi-dence of mucosal inflammation and mucosal architecturalalterations, including crypt abscesses, fibrosis, and villousblunting. Recent papers12,13 show that increases in lympho-cytes and plasma cells alone are insufficient for a diagnosis ofIBD. Further, in many cases, even though clinical signs mayimprove following steroid therapy, the numbers of lympho-cytes and plasma cells often remain unchanged, indicatingthat the diagnosis of IBD may be in question. A number ofpossible causes of intestinal inflammation must be consideredin the diagnostic process, including infectious causes, foodsensitivity/intolerance (discussed below in “Dietary Inter-vention in Gastrointestinal Disease”), hyperthyroidism orother endocrinopathies, neoplastic or protozoal causes, andparasitic triggers. These should be investigated thoroughly orempirical therapy should be instituted before settling on thediagnosis of idiopathic IBD.
Food sensitivity can be particularly difficult to distin-guish from IBD or other intestinal disorders. In one study,food sensitivity was reportedly responsible for at least 30% ofall feline GI problems. Thus, appropriate food trials are anextremely important component of diagnosis and therapy ofcats with GI disease or suspected IBD.
In addition to food trials, the diagnostic plan for a cat withchronic diarrhea should include multiple fecal examinations ortherapeutic deworming, assessment of thyroid and FeLV/FIVstatus, and intestinal vitamin (cobalamin) status. Serum cobal-amin levels in cats commonly decrease with severe distal boweldisease, and in cats with hypocobalaminemia, the diarrhea willbe persistent until replacement therapy is instituted. Cobalamin
Knowledge of the
most frequently
encountered causes
of diarrhea in kittens
and cats is essential
in formulating
appropriate diagnostic
and treatment plans.

Critical Updates on Canine and Feline Health, 2009 NAVC/WVC Proceedings 25
therapy (250 mcg/cat IM q1wk) in some cats may be lifelong,while in others, once the clinical disease resolves, the supple-mentation can be discontinued. In addition, radiography andultrasonography are important in assessing the presence of infil-trative diseases such as FIP granulomas, histoplasmosis, orlymphosarcoma. Ultimately, however, intestinal biopsies—obtained either endoscopically or during an exploratorysurgery—are essential, for both the diagnosis of IBD and rulingout other specific causes of the clinical signs.
In humans, recent studies indicate a strong association ofIBD development with a breakdown of normal tolerancemechanisms, host susceptibility, and the enteric microflora. Itis quite likely that these same factors are important in felineIBD, and in studies using experimental models of IBD, theresident microflora are essential cofactors in driving theinflammatory response. Further, modulation of the entericmicroenvironment in humans with IBD has been shown toreduce proinflammatory cytokines in the mucosa and thusdecrease the inflammation. Unfortunately, accurate, readilyaccessible methods of assessing the bacterial numbers andspecies populating the small intestine are not yet available. Inaddition, studies in cats with IBD assessing modulation of theenteric flora (using probiotics, prebiotics, or other specifictherapy for cytokines) are only in the early stages of study.
At this time, therapy of IBD in cats continues to includeinflammatory suppression and antibiotic therapy. The mosteffective therapies involve using steroids (prednisolone orprednisone 1 to 2 mg/kg PO q12h) or other drugs that inter-rupt the proinflammatory pathways that are active in the gut.In some cats that are intolerant of steroids, or in those inwhich steroids are no longer effective, chlorambucil orcyclosporine immunosuppressive therapy may be necessaryand may be effective. Traditional nonsteroidal anti-inflamma-tory therapy is not beneficial in intestinal IBD; however, incolonic IBD, sulfasalazine or mesalamine may be consideredbecause these drugs are locally acted on by the microflorareleasing their anti-inflammatory effects. These drugs havenot been studied for efficacy or safety in cats. Antibiotic ther-apy with metronidazole (5 to 10 mg/kg PO q12h) has beeneffectively used for a number of years and continues to be rec-ommended for initial therapy of IBD. There is also a widelyheld belief that metronidazole is effective, not only because ofits antibacterial properties but also because of concurrentimmune modulation properties. Some data support theseideas; however, the specific role of metronidazole in IBD ther-apy is still not completely known. An alternative antibioticfrequently used in antibiotic therapy of IBD in cats is tylosin at20 to 40 mg/kg PO q12h.
Finally, general agreement exists among gastroenterologiststhat elimination diets or novel protein, highly digestible diets(discussed below in “Dietary Intervention in Gastrointestinal
Disease”) are beneficial in cats with IBD. Nevertheless, agree-ment also exists that dietary management alone is seldomsuccessful; thus, control of the aberrant inflammatory processand bacterial components is still necessary. Further, at this pointin our understanding, we still do not know which componentsof the diet (e.g., carbohydrate, protein, minerals) are importantin the pathogenesis or therapy of IBD or if other aspects ofnutritional support (e.g., fatty acids, probiotics, other nutraceu-tical therapies) may reduce the inflammatory response.Increasing data in human IBD show that probiotics and antiox-idant, prebiotic nutraceuticals may be important components oftherapy.
Gastrointestinal Lymphoma14
Alimentary lymphoma is one of the most commonly diagnosedneoplasms of the cat. The incidence of this disease has increasedsignificantly over the past 15 years. Despite the common preva-lence of this disease, appropriate diagnosis and treatment can bechallenging. The two main forms of feline alimentary lym-phoma are small cell (lymphocytic, well-differentiated,low-grade) lymphoma and large cell (lymphoblastic, high-grade) lymphoma. These two diseases are related; however, eachpresents its own diagnostic and therapeutic challenges.Additionally, it can be difficult to differentiate these malignan-cies from other nonneoplastic diseases such as IBD and otherchronic inflammatory conditions of the GI tract.
Cats with small cell lymphoma tend to have a disease thathas a slow onset and progression with a nebulous and chronichistory of weight loss. For some cats, thickened intestinal loopsor abdominal masses are found incidentally. Mesenteric lymphnodesmay bemildly tomoderately enlarged and potentially pal-pable, but this is not a finding unique to lymphoma; many GIdiseases can cause mesenteric lymphadenopathy. In rare cases,cats may present with acute signs associated with intussuscep-tion, obstruction, or perforation with septic peritonitis; however,weight loss and lethargy may be the only presenting signs formany cats. Cats presenting with signs consistent with small cellalimentary lymphoma are often geriatric. These older cats canhave many diseases that would cause similar signs or may beconcurrent with lymphoma. A few of the diagnostic differentialsfor these signs include chronic pancreatitis, chronic renal failure,IBD, infectious causes of small-bowel inflammation, or intestin-al or visceral mast cell disease. It is important to do a thoroughworkup with a systematic approach to ensure that nothing isoverlooked. Finally, cats with small cell lymphoma can easily livefor 2 or more years with supportive care and anti-inflammatorytherapy/chemotherapy (dietary therapy, prednisolone, or chlo-rambucil), further complicating the diagnostic picture.
Procurement of a diagnostic tissue sample is the key toachieving a definitive diagnosis of lymphoma in a cat. Fineneedle aspirates are rarely helpful for small cell lymphoma.

26
The neoplastic lymphocytes are well differentiated and appearnormal. Without tissue architecture, it is often impossible todifferentiate a normal lymphocyte from a small neoplasticlymphocyte. Endoscopic biopsies are more accurate than ini-tially thought, and because they are less invasive thanan exploratory laparotomy and often require the patientto spend less time under anesthesia, they are still a viable
diagnostic option if appro-priate biopsy samples areobtained. Approximately70% of the time, a diag-nostic sample can becollected via endoscopy;however, this methodrequires the neoplastictissue to be within theendoscopic retrieval zone(i.e., colon, duodenum,ileum, stomach). Althoughmost cats have superficialneoplastic lesions in themucosa, allowing for en-doscopic biopsy, some
cats have lesions located deeper in the intestinal wall. Theselesions can be missed because endoscopy does not provide afull-thickness sample. Surgical exploration of the abdomenallows for the highest yield; however, it is the most invasiveapproach to retrieving a diagnostic sample. With a surgicalapproach, full-thickness biopsies and biopsies of lymph nodeand liver tissue can be procured. In cats with GI lymphoma,care must be taken to anastomose any surgical sites carefully.Intestinal anastomoses often dehisce more readily because ofdelayed or inefficient healing secondary to tumor infiltration.
Often, the above steps are adequate for a diagnosis of smallcell alimentary lymphoma. However, in rare cases, the diagnosisremains elusive. These cases may require additional diagnosticssuch as immunohistochemical analysis or flow cytometry toassess cell markers and identify populations of neoplastic cells.The demonstration of a clonal population of lymphocytes is thesingle best way to achieve a diagnosis of lymphoma.
DIETARY INTERVENTION INGASTROINTESTINAL DISEASEHighly Digestible (Enteric) DietsThe use of diet to assist in the management of diarrhea is nota new concept. Nevertheless, the type of diet used to helpman-age the problem has become an increasingly complex issue. Inmany, if not most, cases of simple diarrhea (especially in kit-tens), the best approach is to feed a highly digestible diet.
“Highly digestible” is not defined in a regulatory sense butgenerally indicates a product with protein digestibility of
greater than 87% (typical diets are 78% to 81%), and thedigestibility of fat and carbohydrate should be greater than 90%(typical diets are 77% to 85% digestible and 69% to 79%digestible, respectively). In general, the commercially availablediets in this category are formulated with a single, highlydigestible protein and carbohydrate source, have moderate tolow levels of fat and some soluble fiber, but generally have verylow concentrations of insoluble fiber. Protein sources with thehighest availability and digestibility are meats and meat meals.Some pet foodmanufacturers add omega-3 fatty acids (fish oil),fructooligosaccharides or mannooligosaccharides (prebiotics),and antioxidant vitamins and minerals.
Another dietary intervention that has received attentionin gastrointestinal therapy is the use of probiotics. In a 2007study,15 kittens given a diet supplemented with the probioticEnterococcus faecium SF68 had a significantly lower incidenceof naturally occurring diarrhea compared with kittens thatwere fed a regular kitten food during early postweaning andgrowth. Additionally, kittens receiving the probiotic supple-ment had higher serum IgA levels compared with kittens inthe other group, and when kittens receiving the supplementdeveloped diarrhea, it resolved more quickly compared withkittens in the other group.15 Probiotics have been shown toimprove immune function and microflora balance.16,17
Products from different companies have different formu-lations and additives, so individual animals may responddifferently to each diet. The key is to remember that differenthighly digestible diets from different companies should betried if an animal does not respond to the diet tried, because itdoesn’t mean that all diets in that category will be ineffective.
Novel Protein or Elimination Diets18–23Food sensitivity and food intolerance are the most commonadverse reactions to food in cats. Food allergy or food hyper-sensitivity is an adverse reaction to a food or food additivewith a proven immunologic basis. Conversely, food intoler-ance is a nonimmunologic, abnormal physiologic response toa food or food additive. Food poisoning, food idiosyncrasy,and pharmacologic reactions to foods also fall under this cat-egory of adverse reactions to food.
The specific food allergens that cause problems in cats havebeen poorly documented, with only a limited number of studiesdescribing the clinical lesions associated with adverse food reac-tions. In these reports, more than 80% of the cases in cats wereattributed to beef, dairy products, or fish. The incidence of foodallergy in cats is unknown but in most studies is estimated to beonly 15% to 20% of all food-related causes of diarrhea.
Food intolerance is believed to contribute to 60% to 65% offeline diarrhea cases; this rate was supported in two separatestudies in which a majority of cats responded to dietary therapywith a highly digestible diet. The causes of dietary intolerance
General agreement
exists among
gastroenterologists
that elimination diets
or novel protein,
highly digestible
diets are beneficial
in cats with IBD.

Critical Updates on Canine and Feline Health, 2009 NAVC/WVC Proceedings 27
that need to be considered in feline diets are primarily proteinand carbohydrates—both the sources and the amounts.
The diagnosis of both food sensitivity and intolerance isbased on a dietary elimination trial. The major differencebetween these two types of adverse food reactions is thelength of time on the diet that is required to achieve aresponse. Cats with a food sensitivity require 6 to 12 weeks onthe diet before an improvement will be seen. On the otherhand, cats with food intolerance or a nonimmunologic formof adverse reaction to food will generally respond to the newdiet in 7 to 14 days, depending on the severity of the diarrheaand concurrent bacterial disruption.
A variety of commercial and homemade elimination diets,as well as diets formulatedwith hydrolyzed proteins, can be usedin cats with suspected food sensitivity or intolerance. The key isto select a diet that has a novel protein source (based on a care-ful dietary history) and is balanced and nutritionally adequate(commercial diets are best for this). However, homemade elim-ination diets may be needed to find an appropriate test diet.Becausemany cats have consumed a variety of commercial dietscontaining a number of protein sources, homemade diets maybe beneficial because they can bemade from single meat-sourceproteins (and thus are highly digestible) that are truly novel (e.g.,alligator, venison) and have only a single, highly digestible car-bohydrate source. If a homemade diet must be used forlong-term therapy, a nutritionist should formulate a completeand balanced diet containing the necessary protein sources.
In most cats with food sensitivity, avoiding the offendingfood is the most effective therapy and will result in completeresolution of signs. Short-term steroid therapy can be used todecrease the concurrent intestinal inflammation until theappropriate food sources can be identified.
It is very rare for young cats with chronic diarrhea to havea true dietary hypersensitivity to protein or other dietary com-ponents. However, that does not mean that the use of“hypoallergenic” (e.g., novel protein, limited antigen) orhydrolyzed diets should not be used in kittens with diarrhea.Novel antigen diets are often beneficial in cats and kittens withchronic diarrhea not because they are a unique protein source,but because they are a single, meat-source protein that is high-ly digestible. This, together in a diet with a single, highlydigestible carbohydrate source and no additives or flavoringsthat may cause digestive upset, makes these diets very effectivefor therapy of diet-induced diarrheas in kittens and cats.
Hydrolyzed diets may be very helpful in treating GI dis-turbance because these diets have only peptides and otherfood components in a more elemental form, which requiresless digestion in the gut. Although these diets may be quitebeneficial for some kittens with diarrhea, they can also causeworsening diarrhea in others. Hydrolyzed diets have a placein the dietary management of diarrhea, but they should be
considered just another option in the menu of many dietarytherapeutic strategies.
Increased Dietary FiberMany, if not most, commercial pet foods contain smallamounts of soluble or insoluble fiber or both. However, the“high” fiber diets are generally those products containingincreased amounts of insoluble fibers. Fiber amounts havegenerally been designated as normal (less than 5% dry mat-ter), mildly increased (5% to 10% dry matter), moderatelyincreased (10% to 15% dry matter), and greatly increased orhigh fiber (15% to 30% dry matter).
The primary use of high-fiber diets in cats with GI dis-ease is in the dietary management of colitis. In particular, thecommon uses of dietary fiber in cats are to enhance orimprove colonic motility due to hair or other irritant forms ofcolitis and to improve or resolve mild forms of colonic IBDthat are responsive to dietary fiber. The key point to remem-ber is this: Not all cats with colonic disease will respondappropriately to diets high in fiber or to certain types ofdietary fiber. In these cats, highly digestible diets or novel pro-tein diets should be considered alternative choices for therapy.
REFERENCES1. Gookin JL, Stebbins ME, Hunt E, et al. Prevalence of and risk factors forfeline Tritrichomonas foetus and Giardia infection. J Clin Microbiol 2004;42:2707-2710.
2. Gookin JL, Foster DM, Poore MF, et al. Use of a commercially available cul-ture system for diagnosis of Tritrichomonas foetus infection in cats. JAVMA2003;222:1376-1379.
3. McReynolds CA, Lappin MR, Ungar B, et al. Regional seroprevalence ofCryptosporidium parvum–specific IgG of cats in the United States. VetParasitol 1999;80:187-195.
4. Marks SL, Willard MD. Diarrhea in kittens. In: August JR, ed. Consultationsin Feline Internal Medicine. Vol 5. St. Louis: Elsevier; 2006:133.
5. Gookin JL, Dybas D. An owner’s guide to diagnosis and treatment of catsinfected with Tritrichomonas foetus. Updated April 28, 2008. Available at:http://cvm.ncsu.edu/docs/documents/ownersguide_tfoetus_revised042808.pdf. Accessed November 12, 2008.
6. Marks SL, Cheney JM, Taton-Allen GF, et al. Prevalence of enteric zoonoticorganisms in cats. JAVMA 2000;216:687-692.
7. Mekaru SR, Marks SL, Felley AJ, et al. Comparison of direct immunofluores-cence, immunoassays, and fecal flotation for detection of Cryptosporidiumspp. and Giardia spp. in naturally exposed cats in 4 Northern California ani-mal shelters. J Vet Intern Med 2007;21:959-965.
8. Marks SL, Kass PH, Melli A. Evaluation of zinc sulfate fecal flotation and twoimmunoassays for the detection of Giardia duodenalis in naturally infectedkittens [abstract]. J Vet Intern Med 2004;18:388.
9. Stein JE, Radecki SV, LappinMR. Efficacy ofGiardia vaccination in the treat-ment of giardiasis in cats. JAVMA 2003;222:1548-1551.
10. Jergens AE, Crandall JM. Clinical staging of inflammatory bowel disease. In:August JR, ed. Consultations in Feline Internal Medicine. Vol 5. St. Louis:Elsevier; 2006:127.
11. Roudebush P. Adverse reactions to foods: allergies versus intolerance. In:Ettinger SJ, Feldman EC, eds. Textbook of Veterinary Internal Medicine. 6thed. St. Louis: Elsevier; 2005:153.
12. Allenspach K, Wieland B, Gröne A, Gaschen F. Chronic enteropathies in

Copyright © 2009 Nestlé Purina PetCare Company,St. Louis, MO
This information has not been peer reviewed and does not necessarily reflect theopinions of, nor constitute or imply endorsement or recommendation by, the Publisher.The Publisher is not responsible for any data, opinions, or statements provided herein.
VET 2548
dogs: evaluation of risk factors for negative outcome. J Vet Intern Med 2007;21:700-708.
13. DayMJ, Bilzer T,Mansell J, et al. Histopathological standards for the diagnosis ofgastrointestinal inflammation in endoscopic biopsy samples from the dog and cat:a report from the World Small Animal Veterinary Association GastrointestinalStandardization Group. J Comp Pathol 2008;138(suppl 1):S1-S43.
14. Wilson H. Feline alimentary lymphoma: demystifying the enigma. Clin TechSmall Anim Pract. In press.
15. Czarnecki-Maulden GL, Cavadini C, Lawler DF, Benyacoub J. Incidence ofnaturally occurring diarrhea in kittens fed Enterococcus faecium SF68. Com-pend Contin Educ Vet 2007;29(suppl 2A):37.
16. Marshall-Jones ZV, BaillonML, Croft JM, Butterwick RF. Effects of LactobacillusacidophilusDSM13241 as a probiotic in healthy adult cats.Am J Vet Res 2006;67:1005-1012.
17. Rastall RA. Bacteria in the gut: friends and foes and how to alter the balance.J Nutr 2004;134:2022S-2026S.
18. Cave N. Hydrolyzed diets. Vet Clin North Am Small Anim Pract 2006;36:1251-1268.
19. Guilford WG. Dietary therapy of feline diarrhea. N Z Vet J 2003;51:262-274.20. Leistra M,Willemse T. Double-blind evaluation of two commercial hypoaller-
genic diets in cats with adverse food reactions. J Feline Med Surg 2002;4: 185-188.21. Waisglass SE, Landsberg GM, Yager JA, Hall JA. Underlyingmedical conditions
in cats with presumptive psychogenic alopecia. JAVMA 2006;228:1705-1709.22. Verlinden A, Hesta A, Millet S, Janssens GP. Food allergy in dogs and cats: a
review. Crit Rev Food Sci Nutr 2006;46:259-273.23. Laflamme DS, Long GM. Evaluation of two diets in the nutritional manage-
ment of cats with naturally occurring chronic diarrhea.Vet Ther 2004;5:43-51.