crit care nurs q vol. 28, no. 1, pp. 22-40 thoracic trauma · thoracic trauma 23 fundamental to...
TRANSCRIPT

Crit Care Nurs QVol. 28, No. 1, pp. 22-40© 2005 Uppincott Williams & Wilkins, Inc.
Thoracic TraumaThe Deadly Dozen
Linda Yamamoto, MBA/HCA, BSN, RN, PHN;Crissy Schroeder, ADN, RN; Derek Morley, BSN, RN;Cathie Beliveau, ADN, BA, RN, CCRN
Deadly Dozen ... Lethal Six ... Hidden Six ... Major thoracic injuries are known as the DeadlyDozen. The Lethal Six (airway obstruction, tension pneumothorax, cardiac tamponade, open pneu-mothorax, massive hemothorax, and flail chest) are immediate, life-threatening injuries that requireevaluation and treatment during primary survey. The Hidden Six (thoracic aortic disruption, tra-cheobronchial disniption, myocardial contusion, traumatic diaphragmatic tear, esophageal disrup-tion, and pulmonary contusion) are potentially life-threatening injuries that should be detectedduring secondary survey. Each of these may present as immediately life-threatening or potentiallylife-threatening events. This article provides an overview of these 12 injuries and appropriate man-agement for each. Case studies are included. Key words: airway obstruction, aortic disruption,cardiac tamponade, flail chest, esophageal disruption, massive hemothorax, myocardial con-tusion, open pneumothorax, pulmonary contusion, tension pneumothorax, tracheobronchialdisruption, traumatic diaphragmatic hernia
THORACIC INJURIES account for approx-imately 25% of trauma-related deaths.
They contribute to an additional 25% ofdeaths in the United States annually. Great ves-sels injuries, or disruption of the heart, usu-ally result in immediate death. Early deaths,those that occur within 30 minutes to 3 hours,are due to cardiac tamponade, tension pneu-mothorax, aspiration, or airway obstruction.'Although some of these injuries (most of themcardiac) require emergent surgical interven-tion, most injuries to the lungs and pleura canbe treated nonoperatively by applying certainfundamental principles of initial trauma man-agement, which can substantially reduce mor-bidity and mortality related to these injuries. Athorough knowledge of the pathophysiologyof cardiac and pleuropuknonary injuries is ofutmost importance for optimal treatment.
From the Critical Care Services, Scripps MercyHospital, San Diego, Calif.
Corresponding author: Linda Yamamoto, MBA/HCA,BSN, RN, PHN, Critical Care Services, Scripps Mercy Hos-pital, 4077 Fifth Ave, San Diego, CA 92103 (e-mail;yamamoto. linda@scrippshealth. org).
A rapid initial assessment should be com-pleted upon arrival at the trauma center. As-sessment is based on a series of diagnosticclues obtained from directed data collection.Index of suspicion is the initial data collectedto form this diagnostic set. Orderly evalua-tion will identify injuries that are life threat-ening, for example, tension pneumothorax,open pneumothorax, and massive hemo-thorax. The secondary assessment will iden-tify the majority of lung and pleural injuries,which include pulmonary contusions, pneu-mothorax, and hemothoraces.
AIRWAY OBSTRUCTION
The first priority in treating trauma patientsis airway management. The cornerstones ofairway management are adequate oxygena-tion, ventilation, and protection from aspira-tion. Immediate airway control can preventdeath. Airway obstruction can be a primaryproblem or the result of other injury. Al-though the source of, and approach to, an ob-struction may be slightly different, the prin-ciples of basic and advanced life support are
22
Thoracic Trauma 23
fundamental to managing obstructions. Initialpriorities with all trauma patients are evalu-ation and management of the airway, breath-ing, and circulation, cervical spine with stabi-lization, and level of consciousness.
The most common causes of airway ob-struction are the tongue, avulsed teeth, den-tures, secretions, and blood. But, expandinghematomas that cause compression ofthe tra-chea, and thyroid cartilage or cricoid frac-tures resulting in hemorrhage and edema mayalso be sources of obstruction. Airway com-promise can be acute, insidious, progressive,and/or recurrent. The single most frequentindication for intubation is an unconsciouspatient suffering compromised ventilatory ef-fort. Key issues in managing airway difficultyinclude the follow ing:
1. Delivering adequate oxygen to vital or-gans
2. Maintaining a patent airway3. Ensuring adequate ventilation4. Protecting the cervical spine5. Recognizing the need for endotracheal
intubation6. Knowing how to utilize rapid sequence
intubation7. Being proficient in surgical airway
techniques^8. Preventing hypercarbia is critical!
Upon clinical evaluation, patients presentwith signs of anxiety, hoarseness, stridor,air hunger, hypoventilation, use of accessorymuscles, sternal and supraclavictilar retrac-tions, diaphragmatic breathing, altered men-tal status, apnea, and cyanosis (sign of preter-minal hypoxia). • Cyanosis is a very late signof preterminal hypoxia, since it requires atleast 5 g of reduced hemoglobin to be clini-cally detectable. Trauma patients may be ane-mic to such a degree that they do not haveenough hemoglobin to appear cyanotic. In-dications for airway interventions are dividedinto 3 broad categories outlined in Table 1.'
Basic management for airway compromiseincludes
1. securing an intact airway,2. protecting the airway if jeopardized,
and
3. providing an airway if partially ob-structed or totally obstructed.
Basic, advanced, and surgical airway inter-vention techniques must be performed, eventhough the patient may have a cervical spineinjury. Indications for surgical cricothyroido-tomy are edema of the glottis, fracture of thelarynx, or severe hemorrhage obstructing theairway. Remember, when in doubt, intubate;protect the cervical spine, and intubate early,especially in cases of neck hematomas or pos-sible airway edema. Airway edema can be in-sidious and progressive, and may make de-layed intubation more difficult, if not impos-sible.
Three young men, all aged 22 years, were in-volved in a motor vehicle crash (MVC) while driv-ing in a sports utility vehicle. The restrained driverlost control at approximately 45 mph and hit acar parked on the side of the road. No one wasejected, but the 2 passengers were not restrainedand sustained significant injuries. The 3 victimswere transported to the emergency department(ED) for treatment.
The driver was awake upon arrival. He hadabrasions over his chest and face, was complain-ing of some chest pain, and was breathing at arate of 28 breaths per minute (bpm). He statedthat upon impact, he hit the steering wheel withhis chest. An arterial blood gas on room air re-flected a pH of 7.44, PCO2 of 32, Pao2 of 53,and HCO3 of 24. Auscultation revealed decreasedbreath sounds and rales on the right side. A chestx-ray (CXR) was performed and showed mild pul-monary infiltration in the right lower lobe, consis-tent with pulmonary contusion.
PULMONARY CONTUSION
Pulmonary contusion is the most common,potentially lethal, chest injtiry. The resultingrespiratory failure develops over time ratherthan immediately. Puimonary contusion isthe bruising of lung tissue resulting from ashock wave of force through the parenchyma.Diffuse hemorrhage follows, as well as in-terstitial and alveolar edema,'* causing im-pairment of gas exchange at the gas tissueinterface. The most common mechanism ofinjury causing pulmonary contusion is MVC.

24 CRITICAL CARE NURSING QUARTERLY/JANUARY-MARCH 2005
Table 1. Indications for invasive airway management*
Absolute indicationsObstructionApneaHypoxiaExpanding neck hematomas
Strong relative indicationsSignificant craniocerebra! injury (coma, increased intracranial pressure, central nervous system
trauma, etc)Ventilatory compromise (disruption of the thoracic bellows mechanism)Massive retroperitoneal hemorrhage/hematomas (causing displacement of the intraperitoneal
viscera and upward pressure on the diaphragm)Combative patient with life-threatening injuries
Relative indicationsSevere maxillofaeial traumaExtensive pulmonary contusion
'Adapted from Phillips.'
Up to 87% of patients with pulmonary con-tusions have at least one other associatedchest injury.'' The greater the degree of pul-monary contusion, the greater the degreeof ventilatory impairment. Pulmonary contu-sion is usually the result of a high-velocity-deceleration injury such as an impact witha steering wheel. The initial force of the in-jury causes tissue rupture. Additional damageoccurs as the tissue "springs back." For thisreason, it is more cotnmon to see pulmonarycontusion injuries in younger patients, be-cause their chest walls are more flexible andstretch due to the external forces, whereasthe elderly w ith stiffer, thinner chest wallsare more prone to rib fractures.^ Greatercontusions are sustained in those individualsw ith thin-wall chests, because there is lessprotection provided by muscle and adiposetissue.
Clinically, patients present to the ED withsigns of respiratory distress, including dysp-nea, and PaO2 less than 60 on rootn air. Ausctil-tation of breath sounds may reveal decreasedbreath sotinds, rales, and wheezing over thenext 24 hotirs. Upon assessment, the patientmay complain of chest pain or have abrasionson the chest or back. Patients may also exhibitineffective cough with hemoptysis. None of
these signs, or symptoms, are specific for pul-monary contusion, but hemoptysis has beenreported in up to 50% of patients.'' Chestx-ray reveals consolidation and pulmonary in-filtration at the area of injury, but these find-ings may lag 12 to 24 hours. If abnormal-ities are seen on the admission x-ray, thepulmonary contusion is severe. For this rea-son, the cornerstone of diagnosis is clinicalsuspicion based on the history and mecha-nism of injury.''
Some patients can be treated without in-tubation and mechanical ventilatory support.The management of patients who sustain pul-monary contusions is based on 3 factors^:overall stability of the patient, adequacy ofoxygenation, and pulmonary mechanics. Forpatients who do not need ventilatory support,the following criteria^ should be met:
1. Pao2 more than 60 on 50% inspired oxy-gen,
2. respiratory rate less than 24 bpm,3. spontaneous tidal volume more than 5
tnL/kg, and4. vital capacity exceeding 10 mL/kg.
The driver was piaced on 100% Oj by facemask and given morphine suiphate (MS04),4 mg, intravenous (IV), for pain. On reassess-ment an hour iater, he continued to exhibit

Thoracic Traum.a 25
dyspnea with weak cough. He had difficultyclearing bioody sputum from his airway.The pijysician decided to intubate the pa-tient and piaced him on mechanical venti-lation.
Progressively, the patient may show de-creased lung compliance and increased workof breathing, with a stiff, wet lung picture re-quiring endotracheal intubation and mechan-ical ventilation. Intubation should be under-taken if a PaO2 of 60 mm Hg with an FiO2of 50% cannot be maintained. When usingthe PaO2/FiO2 ratio to determine whether tointubate, the normal ratio is 500, with in-tubation being indicated for patients withratios below 300.' While on ventilatory sup-port, the ideal inspired oxygen should not ex-ceed 50% while maintaining a PaO2 of morethan 60 mm Hg. If the level of oxygen cannotbe maintained, positive end-expiratory pres-sure or continuous positive airway pressure is
Initial treatment of pulmonary contusionincludes supplemental oxygen therapy, mon-itoring oxygen saturations, aggressive pul-monary toilet to help clear bloody secretionsfrom the airway, and administration of anal-gesics. Because ptilmonary contusion leads tocapillary membrane leak, judicious fltiid man-agement is essential to minimize the forma-tion of edema in the injured region of thelung.''
Hemoptysis, or blood in the endotrachealtube, is a sign of pulmonary contusion. Intu-bated patients require frequent suctioning toclear blood, tissue, and mucus from the air-w ay. For patients with moderate to severe con-tusion, intubation and intermittent mandatoryventilation, as w ell as positive end-expiratorypressure, provides better results if ventilatoryassistance is needed.'' It is the nurse's respon-sibility to monitor secretions. They should be-come thinner and contain less blood over thefirst few days posttrauma. Intubation and me-chanical ventilation are not always indicated,especially if the patient is able to maintainspontaneous ventilation with adequate PaO2,and is able to clear secretions w ith coughing.For patients who are mechanically ventilated.
it is important for the RN to motiitor arterialblood gas results, peak inspiratory pressures,and lung compliance. Rising peak inspiratorypressures with decreased compliance may in-dicate the need for pressure-control ventila-tion to avoid barotrauma.
Barotrauma results from overdistention andrupture of the alveoli. Secretions trappedin the lower airways may cause obstruc-tion. On inspiration, the ventilator cycles gaspast the partial obstruction into the alveoli.Consequently, when the expiration of gas isblocked, the lung remains inflated. When thecycle repeats itself, the alveolus ruptures.^Barotrauma can be reduced by maintainingadequate analgesia and sedation levels. Ifthe patient is not responsive to conventionalventilation therapy, and has a catastrophic pul-monary contusion, then pressure-limiting ven-tilatory modes, such as jet ventilation, areconsidered. Adult extracorporeal membraneoxygenation is also an option. Pneumonia isthe most common complication of pulmonarycontusion and, when present, worsens theprognosis.''
Fluid management remains controversial.However, if the patient has a significant pul-monary contusion, placement of a pulmonaryartery catheter may facilitate the monitoringof fluid resuscitation.
The front passenger was second to ar-rive at the ED. He was ciearly in respi-ratory distress with a respiratory rate of34 bpm, and using accessory muscles. Heexhibited asymmetric chest wali movement,with ieft expansion greater than right. Ex-amination showed shaiiow depth of breath-ing; lung sounds were diminished bilater-aliy. He presented with 100% O2 by nonre-breatherface mask. Heart rate was 120 bpm.The nurse palpated crepitus on his rightchest wali. As the patient's respiratory statusworsened, a significant paradoxicai move-ment of a segment of rib was noticed onhis right iateral chest Recognizing this as afiail segment, the nurse anticipated the needfor endotracheal intubation for ventiiatorysupport, and pain controi via epiduraicatheter.
26 CRITICAL CARE NURSING QUARTERLY/JANUARY-MARCH 2005
FLAIL CHEST
Flail chest is a common major injury to thechest wall, occurring in approximately 20% ofadmitted trauma patients. There is an associ-ated mortality rate, as high as 50% in some se-ries. It can be even higher in patients olderthan 60 years. The diagnosis of flail chest in-jury is made on the basis of fractures of 2 ormore ribs, in 2 or more separate locations,causing an unstable segment. The flail seg-ment classically involves anterior (sternal sep-aration) or lateral rib fractures. Posterior ribfractures rarely produce a flail segment be-cause of the heavy musculature that providesstability.' These fractures create a free-floatingsegment of rib or sterntim, resulting in a para-doxical movement relative to the rest of thechest wall during inspiration and expiration.The segment follows pleural pressure insteadof respiratory muscle activity, which is suckedin during inspiration and protrudes out dur-ing expiration. This movement may not beevident on initial assessment because inter-costal muscles in spasm act as a splint for theflail segment. This may be a contributing fac-tor in the failure to identify flail chest withinthe first 6 hours in up to 30% of patientswith this injury. As the patient's pulmonarystatus worsens, the paradoxical movementof the flail segment will increase. Althoughthe paradoxical motion of the unstable flailcan greatly increase the work of breathing,the main cause of hypoxetnia of flail chest isthe underlying pulmonary contusion, whichinvariably occurs with flail chest.'* Nonethe-less, paradoxical movement prevents full ex-pansion of the underlying lung, decreasingminute ventilation. I*ain is a contributing fac-tor, preventing the patient from taking fullbreaths.''
As mentioned previously, the diagnosis offlail chest injury is made on the basis of frac-tures of 2 or more ribs, in 2 or more sepa-rate locations, with resultant paradoxical mo-tion of that segment of the chest wall. Thechest wall must be observed for several res-piratory cycles and dtiring coughing. Patientswith flail chest present with asymmetric chest
movement and signs of respiratory distress, in-cluding increased respiratory rate and work ofbreathing, and decreased tidal volumes. Crepi-tus may be palpated around the flail segment,and patients will complain of chest pain. Overtime, the patient fatigues and requires me-chanical ventilation to maintain adequate oxy-genation and minute ventilation.
Treatment of flail chest includes appropri-ate airway management, supplemental oxy-gen therapy to maintain the PaO2 at levels of80 to 100 mm Hg, and pain control. Stabilizingthe flail segment to reestablish the thoracicbellows effect, and promoting air exchange isessential. Positioning the patient with the in-jured side down, as well as IV pain medica-tions, may be temporarily beneficial. Splint-ing the flail segment with rolled towels ortape may be beneficial if it increases the pa-tient's tidal volumes. Sandbags should not beused, as they add unnecessary resistance torespiratory efforts. Contrary to the standardtreatment for trauma patients, fluids shotildbe used cautiously in the setting of flail chestbecause of the high probability of underly-ing pulmonary contusion. Excessive IV flu-ids wUl contribute to edema of the injuredarea ofthe lung.^ Although the primary indica-tion for endotracheal intubation and mechani-cal ventilation is respiratory decompensation,ventilatory therapy in patients with significantflail chest injuries should be individualized(Table 2).
Intubation/tracheostomy and mechatiicalventilation are indicated if the respiratory rateis faster than 35 bpm, or less than 8 bpm,if PaO2 is below 60 mm Hg on supplemen-tal oxygen at 50%, if PaC02 is acutely above55 mm Hg, or if vital capacity is less than15 mL/kg.'' ' For segments larger than 4to 6 in, or multiple flail segments, positive-pressure ventilation is the optimal solution.Internal splinting through positive-pressureventilation not only corrects paradoxicalchest movement but it also decreases thework of breathing and pain. It is not uncom-mon for patients to be mechatiically ventilatedfor up to 3 weeks as the fracture heals. Surgi-cal internal stabilization is a quicker treatment
Thoracic Trauma 27
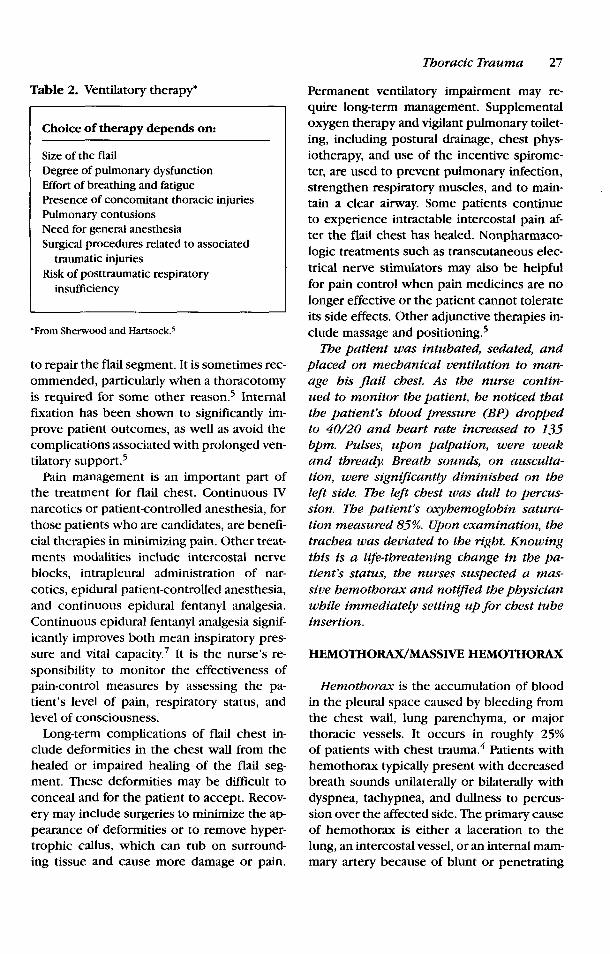
Table 2. Ventilatory therapy*
Choice of therapy depends on:
Size of the flailDegree of pulmonary dysfunctionEffort of breathing and fatiguePresence of concomitant thoracic injuriesPulmonary contusionsNeed for general anesthesiaSurgical procedures related to associated
traumatic injuriesRisk of posttraumatic respiratory
insufficiency
•From Sherwood and Hartsock.'
to repair the flail segment. It is sometimes rec-ommended, particularly when a thoracotomyis required for some other reason.^ Internalfixation has been shown to significantly im-prove patient outcomes, as well as avoid thecomplications associated with prolonged ven-tilatory support.^
Pain management is an important part ofthe treatment for flail chest. Continuous FVnarcotics or patient-controlled anesthesia, forthose patients who are candidates, are benefi-cial therapies in minitnizing pain. Other treat-ments modalities include intercostal nerveblocks, intrapleural administration of nar-cotics, epidural patient-controlled anesthesia,and continuous epidural fentanyl analgesia.Continuous epidural fentanyl analgesia signif-icantly improves both mean inspiratory pres-sure and vital capacity. It is the nurse's re-sponsibility to monitor the effectiveness ofpain-control measures by assessing the pa-tient's level of pain, respiratory status, andlevel of consciousness.
Long-term complications of flail chest in-clude deformities in the chest wall from thehealed or impaired healing of the flail seg-ment. These deformities may be difficult toconceal and for the patient to accept. Recov-ery may include surgeries to minimize the ap-pearance of deformities or to remove hyper-trophic callus, w hich can rub on surround-ing tissue and cause more damage or pain.
Permanent ventilatory impairment may re-quire long-term management. Supplementaloxygen therapy and vigilant pulmonary toilet-ing, including postural drainage, chest phys-iotherapy, and use of the incentive spirome-ter, are used to prevent pulmonary infection,strengthen respiratory muscles, and to main-tain a clear airway. Some patients continueto experience intractable intercostal pain af-ter the flail chest has healed. Nonpharmaco-logic treatments such as transcutaneous elec-trical nerve stimulators may also be helpfulfor pain control when pain medicines are nolonger effective or the patient catinot tolerateits side effects. Other adjunctive therapies in-clude massage and positioning.^
The patient was intubated, sedated, andpiaced on mechanical ventilation to man-age his flail chest. As the nurse contin-ued to monitor the patient, he noticed thatthe patient's blood pressure (BP) droppedto 40/20 and heart rate increased to 135bpm. Puises, upon palpation, were weakand thready. Breath sounds, on auscuita-tion, were significantly diminished on theleft side. The ieft chest was duli to percus-sion. The patient's oxyhemoglobin satura-tion measured 85%. Upon examination, thetrachea was deviated to the right Knowingthis is a life-threatening change in the pa-tient's status, the nurses suspected a mas-sive hemothorax and notified the physicianwhile immediately setting up for chest tubeinsertion.
HEMOTHORAX/MASSIVE HEMOTHORAX
Hemothorax is the accumulation of bloodin the pleural space caused by bleeding fromthe chest wall, lung parenchyma, or majorthoracic vessels. It occurs in roughly 25%of patients w ith chest trauma.'' Patients withhemothorax typically present with decreasedbreath sounds unilaterally or bilaterally withdyspnea, tachypnea, and dullness to percus-sion over the affected side. The primary causeof hemothorax is either a laceration to thelung, an intercostal vessel, or an internal mam-mary artery because of blunt or penetrating

28 CRITICAL CARE NURSING QUARTERLY/JANUARY-MARCH 2005
trauma. Bleeding in these types of cases is usu-ally self-Umiting and does not require surgicalintervention. Radiographic films may not re-veal a fluid collection of less than 300 mL.Bleeding from parenchymal lacerations oftenstops on its own because of the low pul-monary pressures and high concentrationsof tissue thromboplastin in the lung. Smallhemothoraces usually seal themselves withina few days.
Accumulation of greater than 1500 mL ofblood is considered a massive hemothoraxthat can have disastrous results. A left-sidedmassive hemothorax is more common thanthe right-sided one, and is typically associatedwith aortic rupture.^ A massive hemothoraxis commonly due to penetrating trauma withhilar or systemic vessel disruption.
Because the chest cavity can hold most ofa patient's circulatory volume, it is possiblefor the patient to become hemodynamicailyunstable emergently in the case of a mas-sive hemothorax. Signs of shock, like hypoten-sion, decreased venous return, and cyanosisare common because of hypovolemia and in-creased pressure in the thorax. Neck veinsmay be flat, secondary to hypovoletnia, ordistended because of the mechanical effectsof intrathoracic pressure. A mediastinal shiftand/or tracheal deviation is a classic signcaused when the contents of the chest cav-ity are shifted aw ay from the blood accu-mtilation because of increased intrathoracicpressure.^
Treatment of acute hemothorax includessupplemental oxygen therapy and, in mostcases, the insertion of a large (36-38 French)chest tube (tube thoracostomy) just anteriorto the midaxillary line at the fourth or fifthintercostal space to allow for chest decom-pression. A moderate-size hemothorax (500-1500 mL) that stops bleeding after a thoracos-tomy is usually treated with a closed drainagesystem. It is the responsibility of the RN tomaintain and monitor the chest tube drainagesystem, and the color and amount of thedrainage. The RN should have blood availablebefore decompression and be prepared to au-totransfiise the blood.
Table 3. Indications for exploratory thora-cotomy*
> 1500 mL of blood evacuated after initialchest tube insertion
>200 mL/hour for > 4 consecutive hours> 150 mL/hour for 3 hours for the elderlyHemodynamicaily instability systolic
blood pressure < 80 mm Hg despiteaggressive blood/volume resuscitation
At least 2 functioning chest tubes are inplace and signs of exsanguinationoccurs
'From Powell et al' and Sherwood and Hartsock.'
In the case of a massive hemothorax, intu-bate the patient. Shock is a compelling indica-tion for intubation. A chest tube is also placed,and urgent thoracotomy is performed. Thereare 5 indications''^ for performing an tirgentthoracotomy (Table 3)'"' when there are signsof exsanguination. However, if it is greaterthan 1500 to 2000 mL, or continues to bleedmore than 100 to 200 mL per hour, then an ex-ploratory thoracotomy must be performed tofind the source of hemorrhage and to removeclots from the mediastinum. Surgery is emer-gent in these patients because insertion of achest tube drainage system prevents any tam-ponade of the hemorrhage and rapid exsan-guination is possible.
A chest tube was inserted at the fourthintercostal space with the immediate evac-uation of 1600 mL of blood. The patientregained symmetric expansion of his chestwail and his tidal volumes doubled onthe ventilator. His BP increased to 70/50mm Hg. Transfusion therapy was initiatedaccording to hospital protocol. The nurse as-sisted in transporting the patient to the op-erating room (OR) for an emergency thora-cotomy.
Almost simultaneously, the third pas-senger arrived in the ED. He too wasunrestrained in the sports utility vehicieand arrived in respiratory distress. Pre-hospital providers initiated 100% O2 bynonrebreather facemask. Oxyhemogiobin

Thoracic Trauma 29
saturation measured 89%, respiratory ratewas 38 bpm, heart rate was 120 bpm,and BP was 80/60 mm Hg. Examinationalso revealed asymmetrical chest wall move-ment, labored breathing, and absent breathsounds on the right side. He was immedi-ately intubated and bag ventilated. Chest x-ray showed a right pneumothorax with nearcomplete collapse of the right iung.
PNEUMOTHORAX
Pneumothoraces in blunt thoracic traumaare most frequently caused when a fracturedrib penetrates lung parenchyma. But it canalso be caused by deceleration or barotraumawithout associated rib fractures.^ The loss ofnegative intrapleural pressure results in thepartial, or total, collapse of the lung, with aresulting accumulation of air in the pleuralspace. Typically, a loss of more than 40% lungvolume because of a pneumothorax precip-itates respiratory distress in the patient un-less there is preexisting lung disease, in whichcase an even smaller loss in lung volume maynot be tolerated. Most often, intrapleural airleak is self-limiting because the progressivecollapse and decreasing ventilation of the af-fected lung seal the leak. In other cases, thelung may collapse completely.^
Patients will present with respiratory dis-tress, including dyspnea, tachypnea, andtachycardia. Decreased, or absent, breathsounds can be heard over the affected areawith hyper resonance to percussion if thepneumothorax is large. Patients may oftencomplain of chest pain, but it may not de-velop for hours. Chest x-ray demonstrates apleural stripe fallen away from the chest wall,with absence of lung markings beyond thestripe. Small pneumothoraces may not be vis-ible with x-ray. A small pneumothorax (lessthan 1-2 cm) can be observed with follow-upx-rays, taken within 6 to 8 hours, and by mon-itoring the patient's respiratory status, and of-ten, needs no further treatment. Larger pneu-mothoraces require the insertion of a chesttube. The classic chest tube insertion site atthe second intercostals space is a less opti-
mal site for tratima patients whose injuries aretypically a combination of pneumothorax andhemothorax and require a more distal site.
As the x-ray technician removed the filmfrom under the patient's back, she noticedan approximately 3-cm-small wound on hisright posterolateral chest wall with bubblesaround the site and an apparent "suckingsound." Suspecting this was the cause of hispneumothorax, the nurse prepared an oc-clusive dressing and prepared for chest tubeinsertion.
OPEN PNEUMOTHORAX
Open pneumothorax is caused when a pen-etrating chest trauma opens the pleural spaceto the atmosphere, leading to a collapsedlung and a sucking chest wound. Historicallydescribed as early as the 13th century, openpneumothorax is a common combat injury,but in civilian life, it is most likely caused bypenetrating injury or impalement.^ In injurieswhere the wound is greater than two thirdof the diameter of the trachea, the air willpreferentially enter the wound during respi-ration, thereby, inhibiting normal ventilation,and lead to profound hypoventilation andhypoxia. The increased intrathoracic pressurecan also cause the mediastinum to shift tothe opposite side. This, in combination withreduced venous return, can lead to decreasedcardiac performance and hemodynamicinstability.
Signs and symptoms are proportional to thesize of the defect. Signs and symptoms in-clude, but are not limited to, visible defects,restlessness, dyspnea, tachypnea, cyanosis,asymmetrical chest expansion, hypoxia, andreduced venous return.'" Respiratory distressis a common finding with these patients, asis decreased breath sounds on the side of theinjury. The presence of a thoracic injury withapparent sucking action and possibly gas bub-bles at the wound site is most obvious. Itis important to note that wound appearancecan be deceiving. A large, menacing-lookingw ound may prove superficial, whereas asmall, otherwise unassuming w ound may

30 CRITICAL CARE NURSING QUARTERLY/JANTJARY-MARCH 2005
actually be responsible for the patient'sinjuries.
Treatment is aimed at returning normal ven-tilation and closing the wotmd. The first stepis to assure an adequate airway, and intu-bate, if necessary. Then, locate the woundand place a sterile occlusive dressing overit to promote normal ventilation. A stan-dard method involves placing a nonporousdressing (eg, petroleum-impregnated dress-ing) over the wound and taping it on 3 sides.This acts as a 1-w ay valve, allow ing air to es-cape during expiration but becomes occlu-sive during inspiration. The RN must monitorthe patient carefully for signs of a developingpneumothorax, such as hypotension, respira-tory difficulty, decreased pulse pressure, hy-poxia, and jugular venous distention (JVD).To help prevent this, a chest tube is insertedat another site to treat the pneumothorax af-ter the dressing is applied.^ These patients areoften intubated, and mechanically ventilated,to ensure control over ventilation. The woundshould be cleaned and debrided prior to sim-ple closure. Surgical exploration and closuremay be required for larger wounds.
The patient was placed slightly on his leftside and supported with pillows to visual-ize the wound better and to facilitate theinsertion of a chest tube. The nurse placeda dressing over the site and taped it on 3sides while waiting for the physician to re-turn to insert the chest tube. Inadvertently,the patient rolled onto his back again whilethe nurse documented his assessment Sud-denly, the high-pressure alarm sounded onthe ventilator. The RN noticed that the pa-tient's BP dropped to 60/45 mm Hg. Eur-ther assessment revealed distended neckveins. The dressing had become occlusive be-cause the surrounding pillows prevented airfrom escaping. The nurse suspected that hispatient had developed a tension pneumo-thorax.
TENSION PNEUMOTHORAX
Tension pnetimothorax is a life-threateningsituation that reqtiires immediate recognition
and treatment. It is the accumulation of air,or blood, in the pletiral space without anexit, causing an increase of intrathoracic pres-sure, and compression of the great vessels,lung, heart, and trachea. The results of thiscompression are a failure to ventilate and de-creased cardiac output. This injury may bean immediate restilt of the primary trauma,a delayed complication from an tmdetectedinjury, or an undesirable result from treat-ment such as mechanical ventilation or an in-advertently clamped chest tube. Patients willexhibit signs of shock, including hypoten-sion and decreased cardiac output, and se-vere respiratory distress due to compressionof the heart and lungs.'*' Asymmetric chestwall movement may be visible, as well as dis-tended neck veins. Tracheal deviation is aclassic sign due to increased intrathoracicpressure causing mediastinal shift, but may bedifficult to detect in intubated patients. Pa-tients may also become cyanotic from pro-longed hypoxia.''
Treatment is aimed at decompressing thechest to release the trapped air or blood. Sup-plemental oxygen is provided, and immediatedecompression is accomplished by inserting a12- or l4-gauge angiocatheter into the secondintercostal space in the midciavicular line ofthe affected hemithorax.* As air or blood isreleased, ventilation should improve, and thecause of injury should then be investigatedand treated appropriately. A chest tube is in-serted in the fourth intercostal space in themidaxillary line, to allow lung re-expansion,and to prevent further episodes. Pain manage-ment and pulmonary toileting are also initi-ated at this point. It is imperative for the RNto closely monitor patients w ho are at highrisk for tension pneumothorax (Table 4)^ toquickly recognize and treat the patient if thesituation arises.
The dressing was released on one sideto relieve the pressure in his chest cavityand the patient's BP retumed to baseline.A chest tube was inserted at a more iat-erai site and the patient was transportedto the OR for wound debridement andclosure.
Thoracic Trauma 31
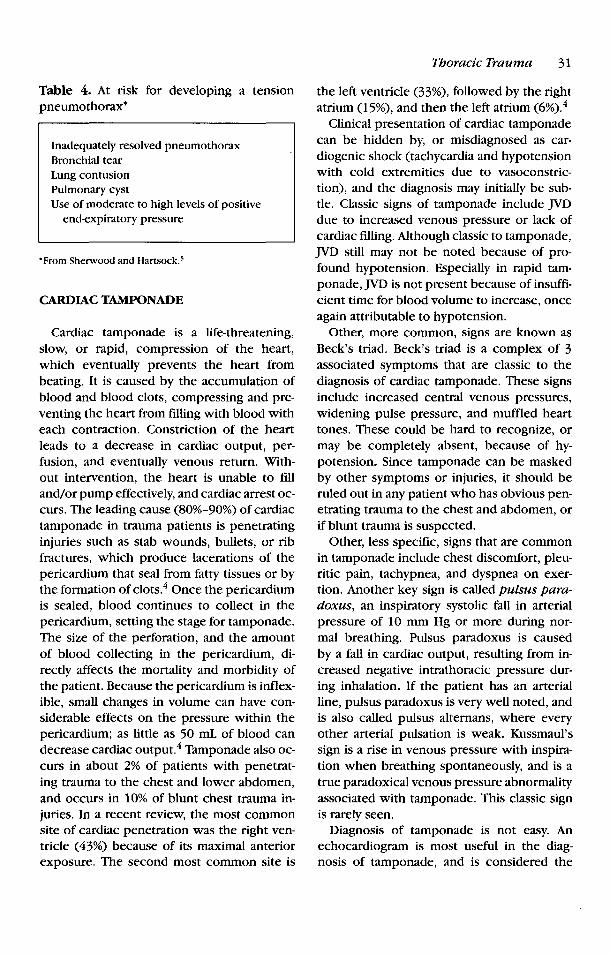
Table 4. At risk for developing a tensionpneumothorax*
Inadequately resolved pneumothoraxBronchial tearLung contusionPulmonary cystUse of moderate to high levels of positive
end-expiratory pressure
•From Sherwood and Hartsock.'
CARDIAC TAMPONADE
Cardiac tamponade is a life-threatening,slow, or rapid, compression of the heart,which eventually prevents the heart frombeating. It is caused by the accumulation ofblood and blood clots, compressing and pre-venting the heart from filling with blood witheach contraction. Constriction of the heartleads to a decrease in cardiac output, per-ftision, and eventually venous return. With-out intervention, the heart is unable to filland/or pump effectively, and cardiac arrest oc-curs. The leading cause (80%-90%) of cardiactamponade in trauma patients is penetratinginjuries such as stab wounds, bullets, or ribfractures, which produce lacerations of thepericardium that seal from fatty tissues or bythe formation of clots.'* Once the pericardiumis sealed, blood continues to collect in thepericardium, setting the stage for tamponade.The size of the perforation, and the amountof blood collecting in the pericardium, di-rectly affects the mortality and morbidity ofthe patient. Because the pericardium is inflex-ible, small changes in volume can have con-siderable effects on the pressure within thepericardium; as little as 50 mL of blood candecrease cardiac output.^ Tamponade also oc-curs in about 2% of patients with penetrat-ing trauma to the chest and lower abdomen,and occurs in 10% of blunt chest trauma in-juries. In a recent review, the most commonsite of cardiac penetration was the right ven-tricle (43%) because of its maximal anteriorexposure. The second most common site is
the left ventricle (33%), followed by the rightatrium (15%), and then the left atrium (6%).''
Clinical presentation of cardiac tamponadecan be hidden by, or misdiagnosed as car-diogenic shock (tachycardia and hypotensionwith cold extremities due to vasoconstric-tion), and the diagnosis may initially be sub-tle. Classic signs of tamponade include JVDdue to increased venous pressure or lack ofcardiac filling. Although classic to tamponade,JVD still may not be noted because of pro-found hypotension. Especially in rapid tam-ponade, JVD is not present because of insuffi-cient time for blood volume to increase, onceagain attributable to hypotension.
Other, more common, signs are known asBeck's triad. Beck's triad is a complex of 3associated symptoms that are classic to thediagnosis of cardiac tamponade. These signsinclude increased central venous pressures,widening pulse pressure, and muffled hearttones. These could be hard to recognize, ormay be completely absent, because of hy-potension. Since tamponade can be maskedby other symptoms or injuries, it should beruled out in any patient who has obvious pen-etrating trauma to the chest and abdomen, orif blunt trauma is suspected.
Other, less specific, signs that are commonin tamponade include chest discomfort, pleu-ritic pain, tachypnea, and dyspnea on exer-tion. Another key sign is called pulsus para-doxus, an inspiratory systolic fall in arterialpressure of 10 mm Hg or more during nor-mal breathing. Pulsus paradoxus is causedby a fall in cardiac output, resulting from in-creased negative intrathoracic pressure dur-ing inhalation. If the patient has an arterialline, pulsus paradoxus is very well noted, andis also called pulsus alternans, where everyother arterial pulsation is weak. Kussmaul'ssign is a rise in venous pressure with inspira-tion when breathing spontaneously, and is atrue paradoxical venous pressure abnormalityassociated with tamponade. This classic signis rarely seen.
Diagnosis of tamponade is not easy. Anechocardiogram is most useful in the diag-nosis of tamponade, and is considered the

32 CRITICAL CARE NURSING QUARTERLY/JANUARY-MARCH 2005
most readily available and efficient tool, if tim-ing permits. Echocardiogram may characteris-tically demonstrate right atrium or ventriclechamber collapse.
Treatment of cardiac tamponade hinges onaggressive airway control, oxygenation, cir-culatory support, and rapid transport to atrauma center for definitive treatment.'' Rapiditifusion of IV fluids will increase venouspressure and improve cardiac output. It alsoallows time for needed interventions. The ul-timate treatment of tamponade is drainageor removal of blood and clots from the peri-cardial sac, preferably by needle paracente-sis guided by echocardiography, fluoroscopy,or computerized tomography (CT). The nee-dle tip w ould be evident on imaging, whichhelps ensure safety when penetrating the peri-cardium. Surgical drainage is desirable in pa-tients w ith intrapericardial bleeding, and inthose with clotted hemopericardium. Traumapatients who undergo a pericardiocentesiswill usually require surgical inspection, andpossible repair, of the heart. Medical treat-ment of tamponade remains controversial,but should include inotropic support, as wellas supporting the body's compensatory mech-anisms to reduce the elevated vascular resis-tance. Cardiac tamponade is a life-threatetiingemergency, and removal of blood from thepericardium is the only intervention that w iUsustain life.
Nursing management of a patient with car-diac tamponade would include ventilatorysupport/airway protection, assistance withemergent pericardiocentesis, if indicated, andhemodynamic support, including fluid resus-citation. The patient would most likely be re-covered and monitored in the intensive careutiit (ICU) for several days, and then trans-ferred to a telemetry floor for further motii-toring before discharge. Patients would be dis-charged home with individualized foUow-upinstructions if they are without complicationsdtiring hospitalization.
Prognosis of tamponade is excellent as longas the trauma patient is treated promptly, be-fore hypovolemic or cardiogenic shock oc-curs, or ptilseless electrical activity. Pulseless
electrical activity caused by tamponade intrauma patients carries a poor prognosis andrequires critical thinking for recognition anditnmediate life-saving interventions.
AORTIC DISRUPTION
Aortic disruption, resulting from blunttrauma, is the leading cause of immediatedeath. Disrupting the blood flow in the aortaimpedes perfusion to vital organs and to ex-tremities. Depending upon w^here the disrup-tion is in the aorta, the size, or entirety, of thedisruption determines the significance of theprognosis. Disruption of the aorta is any in-terference within the aorta, such as a smalltear, laceration, occlusion, or complete rup-ture. An occlusion of the aorta carries a goodprognosis if it is diagnosed quickly and inter-ventions are immediate. Each year, 5000 to8000 people in the United States die as a re-sult of aortic or great vessel rupture.'^
The most common mechanism is rapid de-celeration from a high-speed impact such asthat experienced by the patients whose casestudy is described in this article. Rapid decel-eration can cause shearing forces on the aortaand other great vessels. Depending on the de-gree of force, it can cause either partial orcomplete tears. If the tear is complete, it isusually fatal at the scene. Patients who survivethe initial injury have a high likelihood of sur-vival if the disruption is identified and treatedrapidly. If the injury is not identified, one thirdof the patients die within the first 6 hours.^
The most common site of tears or rupturein the aorta is in the descending portion dis-tal to the left subclavian artery at the liga-mentum arteriosum. The descending aorta,which is fixed to the vertebrae, decelerates atthe same rate as the body would deceleratein a high-speed accident. The heart and theaortic arch often continue to move laterallyand itiferiorly into the left hemithorax. Theresultant force is a combination of shearing,torsion, and bending that produces maximalstress. There are also 2 other sites in the as-cending aorta where rupttire occurs: •wherethe aorta leaves the pericardial sac and at the

Thoracic Trauma 33
entry to the diaphragm. Other less commonmechanisms include falls from a great heightor sport-related impacts (ie, football, hockey).
The clinical presentation of a disruptedaorta can be very specific, but some patientsremain symptom free. In those cases, criti-cal thinking doctors and nurses are requiredto recognize it before too much time haselapsed. Up to 50% of patients will have noexternal signs of chest trauma, so the singlemost important factor in establishing the di-agnosis is a high index of suspicion based onmechanism of injury.'*
Possible signs include a pulse deficit in anyarea, particularly lower extremities or the leftarm, hypotension, unexplained by other in-juries, or hypertension of the upper extremi-ties compared with the lower extremities. Thepatient may experience sternal or posteriorinterscapular pain and may have dyspnea orrespiratory distress. Auscultation of a precor-dial or interscapular systolic murmur is alsovery specific. Depending on the location ofthe disruption, the patient may have hoarse-ness, attributable to a hematoma causing pres-sure around the aortic arch or complete lowerextremity paralysis.'
Diagnostics include plain film x-ray, w hichwould show^ a w idened mediastinum (>8 cm)or an obscured aortic knob.' Other findingsthat are suggestive of an aortic disruption areleft apical pleural cap, tracheal deviation tothe right, and elevation and rightward devia-tion of the right mainstem bronchus." A CTscan is done, particularly if the CXR is ques-tionable, but its overall accuracy is approx-imately 53%.' Aortography remains the goldstandard for detecting aortic injuries. Aortog-raphy allows visualization ofthe aorta and anytears, aneurysms, occlusions, or hematomasthat may be present. Ultimately, the disrup-tion will require surgical intervention, but un-til the patient is ready for surgery, the ma-jor focus is to keep the blood pressure ina specified range, usually less than 90 mmHg. Blood pressure is of utmost importance.If pressure is too high, it could cause theaorta to completely rupttire and the patient toexsanguinate.
Nursing management includes airway pro-tection, intubation, oxygen delivery, and care-ftil administration of fluids. Hypotension is ac-ceptable as long as the patient can tolerate it.Stimulation is reduced; pain control is a toppriority to aid in keeping BP low. Continu-ous monitoring for hemodynamic stability iskey.
Prognosis completely depends on earlyrecognition and prompt treatment, but manypatients who survive the operative period stilldie within the first week after injury.'' Postin-jury complications that require monitoringinclude hypertension, paraplegia, bowel is-chemia, renal failure, graft leaks, and infec-tion. It is important for the nurse to remem-ber that any organ system below the level ofdisruption may be damaged during the periodof hypoperfusion. Renal and bowel functionneed to be monitored. Blood pressure needsto be kept low to aid in healing of new graftsand to prevent rebleeding. The patient's reha-bilitative plan will need to be tailored to hisor her particular disabilities, whether perma-nent or temporary.
Two young men were involved in ahigh-speed MVC during which their vehicieplunged off an interstate freeway, down a20-ft embankment, across a second highway,and then crashed into a retaining wall. Perparamedics, there was considerable vehicledamage. Both airbags deployed.
The driver R.G., reportedly unrestrained,arrived at the trauma center, awake, alert,and cooperative. He denied pain, but didcomplain of thirst His vital signs were sta-ble. Both primary and secondary exami-nations failed to reveal any significant in-juries. However, the history of a high-speedcrash, coupled with possible ejection, raisedthe ievei of suspicion for a potentially se-rious or a life-threatening injury. Per pro-tocol, a portable CXR was obtained in thetrauma resuscitation room. The CXR imagedemonstrated a widened mediastinum. Thetrauma surgeon ordered a CT scan of thechest. The 16 array helical CT scanner im-ages demonstrated a traumatic transectionofthe descending thoracic aorta.

34 CRITICAL CARE NURSING QUARTERLY/JANUARY-MARCH 2005
The patient was taken to the OR emer-gently for thoracotomy and aortic repairPostoperatively, he was taken to the surgicalICU, intubated on ventilator support, withchest tubes, an arterial iinefor BP monitor-ing, centrai venous pressure catheter, and apulmonary artery catheter. He spent 4 daysin the ICU for careful monitoring and BPcontrol. He continued to progress on the sur-gical ward. He went home postinjury day 7in good condition.
The passenger E.L arrived awake andalert, complaining ofmiid tenderness to hischest. His chief complaint was left lowerextremity pain. His vital signs were sta-ble. Primary examination revealed no life-threatening injuries. Secondary examina-tion revealed a gross deformity of his ieft hip,left knee, and left ankle. Despite the extrem-ity injuries, E.L. had a good puise as wellas movement. Chest x-ray demonstrated awidened mediastinum. Again, secondary tothe high-energy event of a high-speed MVC,there was suspicion for aortic injury. CTscanconfirmed a mid-descending thoracic aor-tic tear. The patient remained hemodynam-icaily stable, but was taken to the OR emer-gently for aortic repair, followed by orthope-dic fixation of his iower extremity injuries.
The patient tolerated the surgeries well andrecovered uneventfully in the ICU for 3 days.He was discharged 5 days later without com-plications, with instructions to follow-up withthe trauma service in the clinic.^
MYOCARDIAL CONTUSION
Myocardial contusion, unlike concussion,results in actual histopathological changes.Upon trauma to the myocardium, cellular in-jury occurs with extravasation of erythrocytesinto the muscle wall, along with necrotic ar-eas of myocardial fibers, myocardial edema,interstitial, and subendocardial hemorrhage.''With or without necrosis, or even contusion,it is believed that injured myocardial cellscontract less forcefully, contributing to di-minished cardiac output.'^ The reported in-cidence of myocardial contusion ranges be-
tween 3% and 75% in studies of blunt chesttrauma."* High-speed deceleration collisionsare the most common cause, but speeds lessthan 35 mph have also contributed. Myocar-dial contusion should be suspected in all pa-tients involved in MVCs of 20 mph or greater,especially if there is damage to the steeringwheel or the patient complains of chest pain.It is estimated that at least 20% of patientswith steering wheel impact sustain cardiaccontusions, 16% of which are fatal."* The mostfrequent scenario is an unrestrained driver ina high-speed crash, hitting the steering wheelwith his chest. Other, less cotnmon, mecha-nisms include falls from a height and directblo ws to the chest, particularly in sport-related incidents. Sometimes, direct traumato the abdomen has been found to generateenough upward force into the chest cavity toproduce blunt cardiac injury.'' The clinicalsignificance of cardiac contusion is directlyrelated to its complications and associatedinjuries, including dysrhythmia, traumaticmyocardial infarction, thromboembolus, re-duced left ventricle ejection fraction and/orcardiac output, valvular injuries, congestiveheart failure, ventricular aneurysm, pericar-dial efftision, coronary artery laceration, andcardiac rupture.''
Clinical presentation of myocardial contu-sion is the presence of dysrhythmias. Sinustachycardia is the most common dysrhythmia.Other dysrhythmias include premature atrialcontractions, atrial fibrillations, right bundlebranch block, ST elevation and T-wave flatten-ing, and premature ventricular contractions.
Dysrhythmias in a chest trauma patientshould always indicate cardiac contusion, un-til proven otherwise. If evidence of externalchest trauma (such as fractures, the imprintof a steering wheel, or complaints of angina-like pain despite the absence of dysrhythmias)exists, one should suspect cardiac contusion.Tenderness, ecchymosis, or swelling of thechest waU are also diagnostic. Other findingsthat may suggest contusion include chest pain(usually unrelieved by nitrates), auscultationof a pericardial friction rub, or an S3 gallop.But once again, myocardial contusion may be

Thoracic Trauma 35
unrecognized and may only be detected whenserious complications develop.
Diagnosis of a cardiac contusion reliesmainly on an admission electrocardiogram(ECG). As previously stated, if cardiac/chesttrauma is even suspected, the patient must beruled out for cardiac contusion. If an admis-sion ECG is abnormal, the patient should beadmitted for continuous heart motiitoring anda follow-up ECG 24 to 48 hours later Mostarrhythmias usually occur within that timeframe. An echocardiogram, CK and CKMB,and troponin levels are frequently assessed asa secondary tool once an abnormal ECG hasbeen obtained. CK and CKMB are nonspecificto myocardial injury and are usually elevatedin trauma patients because of skeletal muscleinjury. Associated with elevated troponin lev-els, they depict a cardiac event of some sort.Troponin measures myocardial contractileproteins (not found in skeletal muscle). Theyare released into circulation only after loss ofmembrane integrity. The latest studies showthat positive cardiac enzymes offer the high-est accuracy in the diagnosis of cardiac injury.However, there is no one diagnostic methodthat is unanimously accepted at this time.
Treatment of cardiac contusion is still verycontroversial, as are the related diagnostics.It is recommended the patient be monitoredcontinuously for symptomatic arrhythmias,especially ventricular irritability or conduc-tion defects. If arrhythmias occur, then the pa-tient is treated per the algorithms in advancedcardiac life support.
Prognosis of cardiac contusion is verypromising. Despite the fact that the injuryis usually not clinically significant, complica-tions can occur Patients older than 50 yearsand those with preexisting cardiac disease areat higher risk for significant cardiac compli-cations following blunt chest trauma.'^ With-out serious complications, or any major asso-ciated injuries, there is complete recovery.
MYOCARDIAL RUPTURE
Myocardial rupture is an acute traumatictear of the ventricles, atria, intraventricular
septum, intraatrial septum, chordae, papil-lary muscles, or valves. Rupture of the my-ocardium is rare, but usually fatal. Patientswho survive rupttire of the heart usually havesustained either right- or left-sided atrial rup-ture. Mortality rates range from 50% to 85%."Most survivors of myocardial rupture survivebecause of cardiac tamponade.
Myocardial rupture occurs when blood-filled chambers are compressed with enoughforce to generate a tear in the chamber wall orsepttim, or to rupture a cardiac valve. Rup-ture of the heart is usually caused by bluntchest trauma from an MVC or a fall. Just as acontusion ofthe heart occurs, sufficient forcecan completely rupture the heart dependingupon the phase ofthe cardiac cycle at the timeof impact.
Clinical signs include all signs of cardiactamponade and hypovolemic shock due to ex-treme hemorrhaging. Patients may also haveevidence of sternal fracture, as well as nu-merous rib fractures, including the first rib.Tamponade symptoms include muffled hearttones, JVD due to increased venous pressure,hypotension utirelieved by fluid resuscitation,tachycardia, and arrhythmias. The patient mayalso be cyanotic from the upper chest to thehead.'*
Treatment of myocardial rupture is im-mediate surgical intervention to repair theheart. One third of patients quickly exsan-guinate and the remaining two third havean intact pericardium, which ends up pro-tecting them from immediate exsanguination.Consequently, the only survivors paramedicswould likely encounter are those with cardiactamponade.''
TRACHEOBRONCHIAL DISRUPTION
Traumatic disruption of the tracheo-bronchial tree is a rare, but potentiallylife-threatening, injury caused by blunt orpenetrating trauma. Blunt injury occurs inabout 1% of cases. This is due to large amountof thoracic bony protection surrounding themajor airway structures. Direct trauma to thetrachea, including the mainstem bronchus.

36 CRITICAL CARE NURSING QUARTERLY/JANUARY-MARCH 2005
may be bltmt or penetrating. Injury to a majorbronchus is an unusual, and fatal, injurythat is frequently overlooked. The injurymay occur at any level, but the majorityof such injtiries result from blunt trauma,and occur within an inch of the carina. Inblunt trauma, the impact creates a suddenincreased pressure in the airway against theglottis. Approximately 80% of patients withmajor airway injuries die at the scene as aresult of asphyxia due to interruption or air-way obstruction compounded by aspirationof blood and intrapulmonary hemorrhage."Thirty percent of the remaining patients whoreach the hospital alive do not often survivebecause of associated injuries.
The incidence of tracheobronchial injuriesis 3%, with a mortality rate of 30%; 50% ofwhom die within the first hour"* Trachealinjuries are devastating and are frequentlycaused by severe rapid deceleration injuriesor compressive forces. Traction is producedduring deceleration and restilts in the lung be-ing pulled away from the mediastinum. Whenthe amount of traction overcomes the elastic-ity of the trachea, the trachea ruptures.''
Three fourths of all tracheobronchial in-juries in penetrating trauma involve the cer-vical trachea, and one fourth involve thethoracic and bronchus. Cervical tracheal in-juries present with upper airway obstruc-tion, unrelieved by oxygen, and cyanosis.Symptoms may include local pain, dysphagia,hemoptysis, subcutaneous emphysema, andcough. Bronchial injuries frequently presentwith hemoptysis, subcutaneous emphysema,or tension pneumothorax with a mediastinalshift.
Eighty percent of major bronchial injuriesoccur within 2 cm of the carina.''* Tra-cheobronchial injuries often leak into thepleural space, mediastintim, and/or the lungparenchyma. An intrapleural lesion results ina massive air leak, and is the most devastat-ing of the tracheobronchial injuries. Clinicalsigns of a mediastinal rupture are pneumo-mediastinum and subcutaneous emphysema.Intraparenchymal injuries ustially seal sponta-neously if the lung is adequately expanded.
Penetrating trauma is overt and is often associ-ated with esophageal, carotid artery, and jugu-lar vein trauma and reqtiires immediate surgi-cal repair.
Clinical findings depend on the type and ex-tent of the injury. Penetrating wounds to theneck or chest usually present w ith an associ-ated air leak, such as subcutaneous emphy-sema, or bleeding, such as hemoptysis. Pen-etrating injuries to the tracheobronchial treeare usually associated v ith major intratho-racic vascular, esophageal, and/or pulmonaryinjuries. This can usually be detected if thepatient presents with a pnetimothorax, andis relieved by chest tube insertion. The pres-ence of a large air leak, which persists andrequires multiple chest tubes to expand thelung, should alert you to the diagnosis. The pa-tient must undergo immediate bronchoscopyto detect the bronchial tear.
Patients with severe blunt trauma must beexamined w ith a high index of suspicion, es-pecially when the first 3 ribs are involved.Fractures of the larynx are a rare injuryand are indicated by the following triad: (1)hoarseness, (2) subcutaneous emphysema,and (3) palpable fracture crepitus. Other signsof tracheobronchial disruption are dyspnea,cough, hemoptysis, sternal tenderness, andnoisy breathing. Hatnman's sign (crunchingsotmd during systole) may be heard on aus-cultation of the heart because of air in themediastinum.'' The patient may also presentin severe respiratory distress or with totalairway obstruction. Observations of laboredrespiratory effort may be the only clue to tra-cheobronchial injury and/or airway obstruc-tion. Noisy breathing indicates partial airwayobstruction that suddenly may become com-plete and the absence of breathing suggeststhat complete obstruction already exists. Apersistent pneumothorax despite a function-ing chest tube is an important clue to a tra-cheobronchial injury.'
Ninety percent of patients will have anabnormal admission x-ray.' Chest radiographmay reveal subcutaneous or mediastinal em-physema, pleural effusion, pnetimothorax, orfracttires of ipsilateral ribs 1 through 5, and

Thoracic Trauma 37
mediastinal hematoma. More specific signsare peribronchial air, deep cervical emphy-sema, and dropped lung (lung apex rests atthe level of hilum)."
Stabilization of the airway is of utmost im-portance. Treatment of tracheobronchial in-juries may require only airway maintenanceuntil the acute inflammatory and edema pro-cesses resolve. Fiberoptic bronchoscopy mayalso be helpful in diagnosing an injury or fa-cilitating airway placement. If a distal injury ispresent, intubation can best be accomplishedby visualization of the bronchi with a flexiblebronchoscope, and then passing an endotra-cheal tube over the scope. If the patient is sta-ble, administer oxygen at 100% and performan immediate bronchoscopy.
An attempt to intubate is warranted if thepatient's airway is totally obstructed or ifthe patient is in severe respiratory distress.Place an endotracheal tube into the mainstembronchus of the uninjured side to improveventilation of the uninjured lung. An emer-gent tracheostomy must be performed if theairway is obstructed, secondary to a rupturedcervical trachea, or intubation was unsuc-cessful. This is usually followed by operativerepair
DIAPHRAGMATIC RUPTURE
Approximately 0.8% to 1.6% of patientswith blunt trauma have a rupture. Blunttrauma accounts for 75% of cases while pen-etrating trauma accounts for 25% of cases.'^Since no distinctive signs and symptoms areassociated with penetrating diaphragmatic in-juries, a high index of suspicion is required fordiagnosis.
The left side ofthe diaphragm is more proneto injury (65%-85% of cases)' because it isnot protected by the liver The left postero-lateral portion of the diaphragm is the weak-est, and therefore, the most common site ofrupture and herniation. The size of the dis-ruption is determined by the mechanism ofinjury. In blunt trauma, the defect in the di-aphragm is typically between 5 and 15 cm. Inpenetrating trauma, the defect is usually be-
tween 3 and 2.6 cm.'^ A rupture or tear ofthediaphragm may allow^ herniation of abdominalcontents, such as the stomach, small bowel,or spleen, into the thorax. Herniation may re-sult in respiratory compromise because of im-pairment of lung capacity, and displacementof normal lung tissue. Penetrating injuries be-low the nipple line should be evaluated forthe potential of diaphragmatic injury, and con-current abdotninal stab wounds to the lateralchest walls and flanks can be associated withdiaphragmatic lacerations. Delay in diagnosisis common because of attention to associatedinjuries and because many ruptures are notrecognized on CXR or CT.
The clinical picture depends on the sizeand site of injury, the presence of the hertii-ation, and associated injuries. Diaphragmaticinjuries are difficult to diagnose at first be-cause bleeding is tnitiimal and the patient is of-ten asymptomatic. Physical examination doesnot reveal diaphragmatic lacerations unlessassociated injuries exist. In the acute phase,patients may demonstrate decreased breathsounds on the side of the injury and bowelsounds may be heard in the chest. The la-tent phase is characterized by intermittent vis-ceral herniation of any abdominal structurethrough the defect. In the latent phase, pa-tients complain of belching, nausea, vomiting,and vague abdominal pain. Common organsthat herniate include the liver on the right andthe colon, stomach, small bowel, and spleenon the left. Tension viscerothorax is a compli-cation of diaphragmatic rupture; usually thestomach herniates and undergoes volvulus,massively dilates, and causes left lung collapseand mediastinal shift to the right.
Clinical findings include marked respiratorydistress, dyspnea (decreased breath soundson the affected side), palpation of abdominalcontents upon insertion of a chest tube, aus-cultation of bowel sounds in the chest, andparadoxical movement of the abdomen withbreathing.'^
Chest x-rays are usually normal or nonspe-cific unless a substantial injury exists. In blunttrauma, CXRs are diagnostic initially in only25% to 50% of cases.' The presence of a

38 CRITICAL CARE NURSING QUARTERLY/JANUARY-MARCH 2005
nasogastric tube within the chest or the pres-ence of abdominal viscera denotes a perfo-rated diaphragm. Diaphragmatic injuries arenot clearly identified, or are missed initially,if the chest film is misinterpreted as show-ing an elevated left diaphragm, acute gastricdilatation, loculated pnetimo-hemothorax, ora subpulmonary hematoma. The followingstudies" may help in diagnosing diaphrag-matic injury:
• Chest radiograph may reveal blurringof the diaphragm, arched diaphragmaticshadow, bowel or extraneous bubbles inthe chest, nasogastric tube in the leftchest.
• Ultrasound is used to visualize large dis-ruptions or herniation. However, it maymiss small tears from penetrating injuries.
• Computerized tomography, with fine cutsthrough the diaphragm, may detect smallruptures of the diaphragm.
• Magnetic resonance imaging may aid inthe diagnosis because it can accurately vi-sualize the diaphragm's anatomy.
Diagnostic procedures• Diagnostic peritoneal lavage—peritoneal
lavage in the presence of diaphragmaticrupture may be falsely negative as muchas 25% of the time." It is still themost sensitive test for detecting diaphrag-matic injury in penetrating lower tho-racic trauma (red blood cell [RBC] thresh-old of 5000 or 10,000 RBC/mm^). Inblunt trauma, the standard RBC thresh-old is 100,000 RBC/mm'. Diagnosticperitoneal lavage is insensitive to di-aphragmatic injury at this threshold.' Theobvious need for laparotomy is an abso-lute contraindication to diagnostic peri-toneal lavage. Relative contraindicationsinclude morbid obesity, a history of multi-ple abdominal surgeries, and pregnancy.
• Diagnosis can be made by return of lavagefluid from a thoracostomy tube.'
General supportive measures are the main-stay of medical therapy. A confirmed diag-nosis, or the suggestion of blunt diaphrag-matic injury, is an indication for surgery. Whilesurgery is the only definitive treatment, place-
ment of a nasogastric or orogastric tube canbe done to decrease the amount of bowelgas and limit the hernia's size, in additionto decreasing the ileus and reducing the ob-struction. Blunt diaphragmatic injuries typi-cally produce large tears measuring 5 to 10cm or longer Persons with traumatic herniasfrequently have concomitant injuries who re-quire emergent exploration. Surgical repair isnecessary, even for small tears, because anydefect will not heal spontaneously.
Complications may occur in up to 64%of patients w ith blunt diaphragmatic in-jury and include intra-abdominal abscess andpneumonia.'" Paralysis of the diaphragm iscotnmon. The late complications of an undi-agnosed traumatic hernia include all ofthe fol-lowing: bowel herniation, incarceration, andstrangulation; tension hemothorax secondaryto massive bow el herniation; pericardial tam-ponade from herniation into the pericardialsac; and diaphragmatic paralysis that may re-cover after repair.'^
Early deaths usually are a result of associatedinjuries, not due to the diaphragmatic injury.There is a 25% to 40% mortality rate associ-ated with diaphragmatic tears, primarily be-cause ofthe severity of associated injuries.'^
ESOPHAGEAL INJURY
Esophageal rupture is the most rapidly fatalinjury. Mortality rate is 18% and increases sig-nificantly if the diagnosis is delayed or missed.Death is imminent if diagnosis is delayed.Most esophageal injuries are caused by pen-etrating trauma. Cervical esophageal injuryis more common than thoracic esophagus.Blunt injury is rare (0.1% incidence),' but islethal if unrecognized. It is usually caused bya forceful injection of gastric contents intothe esophagus from a severe blow to the up-per abdomen, resulting in a linear tear in thelower esophagus allowing leakage into themediastinum. The esophagus has no serosalcovering and any perforation results in di-rect drainage into the mediastinum."* Contam-inated material is pulled into the pleural spaceby negative intrathoracic pressure and results

Thoracic Trauma 39
Table 5. Signs and symptoms according to location of esophageal injury*
Injury
Cervical perforation
Cervical esophageal perforation
Intrathoracic perforation
Abdominal esophageal tear
Signs and Symptoms
Crepitus
Cervical tendernessPainResistance of passive range of motion of the neckDyspneaHoarsenessBleeding from mouth or nasogastric tubeCoughStridor
Neck crepitusMediastinal emphysemaMediastinitis
Peritoneal irritationDyspneaPleuritic pain
•From Mason."
in subcutaneous or mediastinal emphysema,pleural effusion, retro esophageal air, and un-explained fever within 24 hours of injury.
Esophageal injuries should be consideredin any patient who presents with a hemo-thorax or pneumothorax without any rib frac-tures, or in any patient who sustains a severeblow to the lower sternum or epigastrium,who presents with pain and/or shock out ofproportion to the clinical findings.^
Clinical symptoms are subtle and vague,and vary according to the site of rupture andthe degree of contamination. Substernai pleu-ritic chest pain, with radiation to the neck orshoulders, is the most common symptom ofesophageal injury. Swallow ing and neck flex-ion may cause pain. There are many othersigns and symptoms depending on the loca-tion ofthe injury (Table 5).'^
Diagnosis requires correlation of the indexof suspicion with physical findings, radiologi-cal studies, and fiberoptic examination. Typi-cal CXR findings are mediastinal emphysema,pneumothorax, hydrothorax, and/or widenedmediastinum. Because of concomitant in-juries, the CXR may not demonstrate any ab-normalities and an esophagogram should be
performed. The presence of mediastinal air,usually on the left side, is basis for diagno-sis. Esophagoscopy or an esophagogram re-veals the site of esophageal tear and whetherit connects to one or both pleural spaces.'^Esophagoscopy is reliable in 60% of injuries,but with esophagoscopy combined with anesophagogram, esophageal injuries are de-tected 90% of the time.' Recognizing injuryto the esophagus is difficult because of itsrarity, insufficient clinical signs in the initial24 hours, and the presence of other injuries.Missed injuries and delay in treatment resultsin the rapid development of sepsis and asso-ciated high risk of death. Therefore, promptaggressive investigation, including radiogra-phy, endoscopy, and thoracoscopy, must beperformed
Nursing management begins with attentionto airway, ventilation, oxygenation, and circu-latory support. The general treatment for anyesophageal tear or perforation is suspensionof all oral intake, placement of a nasogastrictube with continuous suction, and antibiotictherapy.'* A large-bore IV catheter should beplaced for volume replacement and adminis-tration of rv medication therapy. Continuing
40 CRITICAL CARE NURSING QUARTERLY/JANUARY-MARCH 2005
monitoring for signs of peritonitis and respi-ratory insufficiency is necessary.
If pneumothorax or hydrothorax is present,then a chest tuhe is placed. Medical man-agement is gastric decompression, antihiotictherapy, combined with operative repair con-sisting of hypassing the affected region, anddrainage of the pleural space.''
SUMMARY
Major thoracic injuries are known as the"Deadly Dozen." Each of these injuries maypresent as immediate life threatening or po-
tentially life threatening. The potentially life-threatening nature of these injuries demandsan organized approach hy skilled and know l-edgeahle physicians, nurses, and therapists.Applications of certain fundamental princi-ples of initial trauma management must heapplied. Assessment should he hased on ahigh index of suspicion and a thoroughknowledge of pathophysiology is importantfor optimal treatment. Recognizing the signsand symptoms of these traumatic injuries aswell as accurately diagnosing and managingthese injuries are crucial for hetter patientoutcomes.
REFERENCES
1. Powell MA, McMahon D, Peitzman AB. Thoracic in-jury. In: Peitzman AB, Rhodes M, Schuab CW, YealyDM, eds. The Trauma Manual. Philadelphia, Pa: Lip-pincott Williams & Wilkins; 1998:199-225.
2. O'Connor Re, Levine BJ. Airway management in thetrauma setting. In: Ferrera PC, Coluceiello SA, MarxJA, Verdile VP, Gibbs MA, eds. Trauma Management:An Emergency Medicine Approach. St. Louis, Mo:Mosby; 2001:52-74.
3. Phillips TF. Airway management. In: Moore EE, Mat-tox KL, Feliciano DV, eds. Trauma. 2nd ed. Norwalk,Conn: Appleton & Lange; 1991:127-145.
4. Hubble MW, Hubble JP Principles of AdvancedTrauma Care. Albany, NY: Delmar; 2002.
5. Sherwood SF, Hartsock RL. Thoracic injuries. In: Mc-Quillian KA, Von Rueden KT, Hartstock RL, Flynn MB,Whalen E, eds. Trauma Nursing From Resuscita-tion Through Rehabilitation. 3rd ed. Philadelphia,Pa: Saunders; 2002:543-590.
6. Eddy AC, Carrico CJ, Rusch VW. Injury to the lungand pleura. In: Moore EE, Mattox KL, Feliciano DV,eds. Trauma. 2nd ed. Norwalk, Conn: Appleton &Lange; 1991:357-371.
7. CogbiU TH, Landercasper J. Injury to chest wall.In: Moore EE, Mattox KL, Feliciano DV, eds.Trauma. 2nd ed. Norwalk, Conn: Appleton & Lange;1991:327-355.
8. Sawyer MAJ. Blunt chest trauma. eMed J [serialonline]. 2004. Available at: http://www.emedicine.com/med/topic3638.htm. Accessed September 15,2004.
9. Henneman EA, Henneman PL, Osman KS. Ventila-tion and gas transport: pulmonary, thoracic and fa-cial injuries. In: Neff JA, Kidd PS. Trauma Nursing:
The Art and Science. St. Louis, Mo: Mosby; 1993:143-193.
10. Bayley EW, Turcke SA. A Comprehensive Curricu-lum for Trauma Nursing. Boston, Mass: Jones &Bartlett; 1992.
11. Rosen CL, Wolfe RE. Blunt chest trauma. In: Fer-rera PC, Coluceiello SA, Marx JA, Verdile VP, GibbsMA, eds. Trautna Management: An EmergencyMedicine Approach. St. Louis, Mo; Mosby; 2001:232-258.
12. Schwab RA. Myocardial contusion. Available at:http://www.thrombosis-consult/articles/Textbook/77myocardial contusion.htm. Accessed March 11,2004.
13. Mulder DS, Barkin, JS. Injury to the trachea,bronchus, and esophagus. In: Moore EE, Mattox KL,Feliciano DV, eds. Trauma. 2nd ed. Norwalk, Cotin:Appleton & Lange; 1991:343-355.
14. Mosesso VJ. Penetrating chest trauma. In: Ferrera PC,Coluceiello SA, Marx JA, Verdile VP, Gibbs MA, eds.Trauma Management: An Emergency Medicine Ap-proach. St. Louis, Mo; Mosby; 2001:259-278.
15. Johnson JM, Steinberg SR. Diaphragmatic hernias,acquired. eMed. Available at: http://www. eme-ducube,cin/med/topics3487.htm. Accessed May 5,2004.
16. Welsford M. Diaphragmatic injuries. eMed. Availableat: http://www.emedicine.com/emerg/topicl36.htm. Accessed May 5, 2004.
17. Mason PJ. Abdominal injuries. In: McQuillian KA,Von Rueden KT, Hartstock RL, Flynn MB, Whalen E,eds. Trauma Nursing Erom Resuscitation ThroughRehabilitation. 3rd ed. Philadelphia, Pa: Saunders;2002:512-547.
