crisis care concordat event -...
TRANSCRIPT

Crisis Care Concordat Event Presentations
17 September 2014

Thames Valley Crisis Concordat – Agenda Wednesday 17 September 2014
Objectives:
•To develop a regional perspective of the Crisis Care Concordat
•To positively engage all local signatories of the Crisis Care Concordat
•To collectively commit to regional and local declarations and action plans

Welcome Stuart Bell
Key Note Address (Video) Norman Lamb
Policy Context and expectation Sarah McClinton (HMG)
Patient expectations Videos
What does good look like? Dr Caroline Dollery
Plenary Questions All
COFFEE
DH & Mind Support Jim Symington / Naomi Phillips
Regional Perspectives SCAS, TVP, BHFT, OHFT
LUNCH
Locality Work All
Next Steps, Summary and Close Stuart Bell

Sarah McClinton Director, Mental Health and Disability
Department of Health
Thames Valley Crisis Care Concordat Event 17 September 2014
The Mental Health Crisis Care Concordat

Welcome and introductions
Closing the Gap: priorities for essential change in mental health sets out our immediate ambitions for mental health.

Welcome and introductions
The Mental Health Crisis Care Concordat is a shared agreement made by over 20 national organisations about how we respond to people in mental health crisis

Signatory organisations
• Department of Health
• Home Office
• NHS England
• NHS Confederation Mental Health Network
• Mind
• Association of Ambulance Chief Executives
• Association of Chief Police Officers
• Local Government Association and ADASS
• Royal College of Psychiatrists

Concordat: The joint Statement
“We commit to work together to improve the system of care and support so people in crisis because of a mental health condition are kept safe and helped to find the support they need – whatever the circumstances in which they first need help - and from whichever service they turn to first.”

What is the Concordat?
The Concordat is about joining up service responses to people who are suffering from mental health crisis.
In 2012-13 police made nearly 22,000 detentions under section 136 of the Mental Health Act.
Two thirds (14053) of these people were taken to hospital for a psychiatric assessment.
But a third of these people (7,761) were taken to police cells, often because the NHS could not respond quickly enough. Even allowing for pressures on NHS resources – we must all accept that this proportion is too high

Making the Concordat a reality
We have work under way
• The Department of Health and Mind are working on local implementation, the website and brand identity
• NHS England are taking forward their commitments as part of their Parity of Esteem programme, and are developing a Crisis Care Delivery Framework
• Association of Ambulance Chief Executives - have introduced a protocol for ambulance responses
• CQC – have surveyed and mapped health based places of safety

Making the Concordat a local reality in Thames Valley
Making the Concordat a local reality

Thank you [email protected] www.crisiscareconcordat.org.uk

What does good look like?
Dr Caroline Dollery GP Clinical Director, East of England
Strategic Clinical Network [email protected]

Evidence, what evidence?
• Urban myths abound • But we have some very strong evidence • And with a strong basis in personalised care
• References: Centre for Mental health surveys
2001, 2007 • Closing the Gap 2014

Areas of development
The public
National initiatives
System enablers
Commissioning
Information development

System alignment
• Parity programme • Mental health Intelligence Network • CCG MH leadership programme • Acute and unplanned care review & the Crisis
Concordat • Self Harm : implementing NICE & outcomes

Whole population suicide prevention
Improvement of mental health of whole population with a universally proportionate approach facilitating greater access to interventions for higher-risk groups • reducing suicide risk in high risk groups • improving mental health in specific groups • reducing access to lethal means Cross-Government suicide prevention strategy HMG, 2012

Self Harm
• NICE self harm care is being given in only 42%. This is leading to repeat self harm, suicide, early death from other causes (especially alcohol-related)
• Clinical management can be effective, including preventing repetition
• Very wide variation between hospitals in service provision, in spite of official guidance
• Aim is to provide training to all staff who encounter people with self harm
• Self-harm: Recent findings of relevance to treatment, prevention and policy guidance Nav Kapur, keith Hawton

Wellbeing
Places mental health and wellbeing 'at the heart' of new system and highlights key role of DsPH in public mental health Current mental health strategy (HMG, 2011) adopts twin track approach to: • Promote mental wellbeing and prevent mental
disorder to the whole population • Offer early treatment to people with mental
disorder • Public Health White Paper (DH, 2010) • JCPMH public mental health commissioning guidance (Campion & Fitch, 2012)

Wellbeing
• Applied to 700,000 population in East Midlands
• Information highlights key opportunities for action at primary, secondary and tertiary levels of promotion and prevention

Suicide prevention
Levels of suicide and self-harm • Important to measure at local level • Varies according to level of risk factors and
higher risk groups • Informs the required level of coverage of
interventions

National levels of self-harm
• 7% among 11-16 year olds have tried to harm, hurt or kill themselves (Green et al, 2005)
• 5.6% of adults attempt suicide during their lifetime (McManus et al, 2009)
• 4.9% of adults have self-harmed • 16.7% of adults thought about committing
suicide at some point in their life

Why look at suicide in primary care?
• Suicide risk and mental illness – elevated risk – even higher in some sub-groups (e.g. recently discharged) • Contact with health services – 25% in contact with mental health services – 75% in contact with GP (including MH patients) • potential for suicide prevention at population level • Mental illness and GP consultations – frequent consultations – consultations closer to the time of death

Risk and protective factors
Population approach recognises importance of upstream approach to risk and protective factors • Both size of impact of factors and numbers
affected are important to consider • Identification of local levels of such factors
facilitates coordinated action to address such factors
• Results in prevention of self-harm and suicide

Adolescent self harm
Adolescent mental disorder (Green et al, 2005) • 7% among 11-16 year olds • 28% among 11-16’s with emotional disorder (4%) • 21% among 11-16’s with conduct disorder (6%) • 18% among 11-16’s with ADHD (3.5%) • Depressive disorder (OR 11.2) (Meltzer et al,
2001) • Emotional disorder (OR 3.4) • Other mental disorder (OR 3.9)

Integrated approaches
Highlights importance of cross-sector coordination: • Primary and secondary care • Public Health service providers • Local government • Social care service providers • Third sector social inclusion providers • Education providers • Employers • Criminal justice services

International:Detroit initiative • Six Dimensions of Perfect Care
– Safe – Effective – Patient centred – Timely – Efficient – Equitable
– ‘Crossing the Quality Chasm’ Institute of Medicine – Pursuing Perfect Depression Care:Prof. Ed Coffey – http://www.rcpsych.ac.uk/workinpsychiatry/qualityimprovemen
t/managedclinicalnetwork/qualitysafetyworkstream/newsandevents/suicidepreventionconference.aspx

10 Rules for Perfect Care
• Care = relationships • Care is customized • Care is patient centred • Share knowledge • Manage by fact • Make safety a system priority • Embrace transparency • Anticipate patient needs • Continually reduce waste • Professionals cooperate

Improving early recognition
Largest risk factor for suicide and self-harm is mental disorder BUT most with mental disorder – no intervention • Less than 3% of adults see secondary mental
health services • Improving recognition of health professionals,
teachers and general population

Zero Suicide approach
Goal: “Promote the adoption of ‘zero suicides’ as an aspirational goal by health care and community systems. The HFHS Perfect Depression Care program provides an example of this promising approach.” • 2012 National Strategy for Suicide Prevention: • GOALS AND OBJECTIVES FOR ACTION • A report of the U.S. Surgeon General and of the National Action Alliance for
Suicide Prevention

Zero suicide
“If zero is not the right goal, then what is?”

Value for money for prevention
• Parenting interventions for children with conduct • disorder £8 • Early detection and treatment of depression at work £5 • Early intervention for the stage which precedes • psychosis (Clinical High Risk State) £10 • First episode psychosis £18 • Screening and brief interventions in primary care for • alcohol misuse £12 Savings from early intervention of mental disorder per £ invested (DH, 2011)

Tackling causes Key messages (1) Services should: • continue successful safety focus on wards: – preventing absconding, – ensuring safe detention • be vigilant about suicide risk from opiates – clinicians should check patients’ access to these drugs • improve safety in CR/HT – caution is needed with patients who live alone, – who refuse treatment and – when patients first discharged from hospital

Key messages
• Services should: – maintain measures that help to reduce risk including:
• introduction or maintenance of assertive outreach, • provision of dual diagnosis services,
• address the economic difficulties of patients who might be at risk of suicide including: – advice on debts, – housing – employment

What works? Phase 1 (Lancet, 2012)
National policies and recommendations Safety First (2001): 12 steps to a safer service • Removal of ligature points • Assertive outreach • 24-hour crisis team • 7-day follow-up • Non-compliance • Dual diagnosis • Criminal justice information sharing • Multi-disciplinary review • Training in suicide risk management

Do mental health services implement policies?
• Do they make a difference?

Risk assessment and management
should: – be individual to each patient – assess current risk factors and past history – include a management plan that follows on from the
risk assessment. • should not:
– ignore past history – equate the completion of a checklist with good risk
formulation and management – rely on a generic plan of clinical management

Website: http://www.bbmh.manchester.ac.uk/cmhr/research/ - follow link to National Confidential Inquiry

Sharing good practice
• Depression and suicide prevention: Detroit workshop and pathfinder sites
• CAMHS: defining what children and young people really need; removing barriers; removing waiting times; including them in designing services and developing resilience
• Physical and mental health: South Essex, North Essex, Bedfordshire, South Central, London

Commissioning
• New approaches: – Year of Care tariff; alliance contracting – Street triage – Recovery colleges and safe houses – Pioneer programmes: NW London – Developing relationships: voice of patients,
families and carers. Co production – Importance of self care, self management – Role of Health and Wellbeing Boards


Jim Symington & Naomi Phillips, Concordat Implementation Team
Improving outcomes for people experiencing mental
health crisis in England
Thames Valley Concordat Event Wednesday 17 September

“It feels like I literally have to have one foot off the bridge before I can access services.”
‘Listening to experience. An independent inquiry into acute and crisis mental healthcare’, Mind 2011
‘We commit to work together to improve the system of care and support so people in crisis because of a mental health condition are kept safe and helped to find the support they need…
‘We will work together, and with local organisations…
‘Jointly, we hold ourselves accountable…’
Concordat - the joint statement

National context: Recent evidence and policy
National context: evidence & policy

• Mind’s Listening to Experience report
• HMIC/CQC A Criminal Use of Police Cells? report • CQC survey on the use of s136 and map of health-based places
of safety
• Independent Commission on Mental Health and Policing – Lord Adebowale report, London
• Mental health bed shortages and people shipped around
country or held under Section
Growing evidence
National context: evidence & policy

• Mental health patients at highest risk of suicide in first two weeks after leaving hospital
• 24 deaths in England and Wales in patients who had been restrained by ward staff in the previous 24 hours
• Suicides soon after discharge and deaths following restraint should be ‘never events’ in NHS
• “Health professionals should ensure the adverse events that preceded the admission have been addressed.“ (Professor Louis Appleby)
National Confidential Inquiry into Suicide and Homicide by People with Mental Illness
July 2014
National context: evidence & policy

Year 1 priority :
‘…themed work on the experience and outcomes for people experiencing a mental health crisis.’
CQC : A fresh start for the regulation and inspection of mental health services (November 2013)
National context: evidence & policy

‘We are clear that we expect parity of esteem between mental and physical health services…
‘We are committed to achieving change by putting more power into people’s hands at a local level.’
National context: evidence & policy
No health without mental health. A cross-government mental health outcomes strategy for people of all ages. HM Government, 2011

‘By March 2015, we expect measurable progress towards achieving true parity of esteem, where everyone who needs it has timely access to evidence-based services. ‘We expect every community to have plans to ensure no one in crisis will be turned away, based on the principles set out in the soon to be published Mental Health Crisis Care Concordat.’
Government 'Mandate' to NHS England,
National context: evidence & policy

Five key changes :
• Better support for self-care
• Right advice, right place, first time
• Highly responsive urgent care services outside of hospital
• People with more serious or life threatening emergency needs receive treatment in centres with the right facilities and expertise
• Connecting urgent and emergency care services - system more than just the sum of its parts
NHS England Update on Urgent and Emergency Care Review (Aug 2014) (Willetts) August 2014
National context: evidence & policy

Making the Concordat a local reality
Making the Concordat a local reality

Making the Concordat a local reality
Signatories: 22 national bodies involved in health, policing, social care, housing, local government and Mind Supporters: a number of voluntary and community sector organisations involved in mental health services and support, housing, equalities, and social care Mind is working on behalf of the Concordat partners to help make the Concordat a reality in every local area across England
“We won't give up until everyone experiencing a mental health problem gets support and respect.”

“What should I expect if I, or the people that depend on me, need help in a mental health
crisis?”
• Access to support before crisis point
• Urgent and emergency access to crisis care
• Quality of treatment and care when in crisis
• Recovery and staying well / preventing future crises
Making the Concordat a local reality

• Joint statement – ambition for every locality to have at least this in place by end 2014
• Action plan with timescales outlining operational protocols for working together
• Review progress and local governance arrangements
Local Crisis Care Declarations
Making the Concordat a local reality

• Up to local crisis care partnerships to decide
• Perspective of a person experiencing a mental health crisis should be central. Unlikely to know which CCG or other boundary they fall in – just want to know they will get a appropriate and quality help wherever they are
What is a locality?
Making the Concordat a local reality
Making the Concordat a local reality

Local Declarations - who needs to be involved?
Making the Concordat a local reality
Many local organisations want to support the Declaration because of their commitment to improve mental health care and may want to make a specific contribution within the action plan for continuous improvements.
There are also some ‘essential’ organisations which must sign a local Crisis Declaration:
• NHS providers of Urgent and Emergency Care (Emergency Departments within local hospitals)
• Public / independent providers of NHS funded mental health services
• Public / independent providers of substance misuse services
• Clinical Commissioning Groups • NHS England Local Area teams (primary
care commissioners) • Commissioners of social services • The Police Service • Police and Crime Commissioners • The Ambulance Service

Making the Concordat a local reality

Making the Concordat a local reality

Support to help local Crisis Declarations
Support to help local Crisis Declarations

Support to help local Crisis Declarations
Supporting local developments
• Regional events to support development of local
partnerships
• Website with good practice, useful contacts and templates • Helpdesk and online support –
• Additional targeted support, for a fee

Continuing role for national partners
• Bi-annual meetings to track national signatories’ action plans and overall progress
• National annual conference to share good practice and
problem solve
• Evaluate and report impacts of Concordat changes
Support to help local declarations and action plans

More detailed help for localities: a pathway
approach
Detailed help and guidance

Background to local Declarations work – local data
• What does the joint strategic needs assessment tell you? • S136 assessments, locations and outcomes • Beds (e.g. acute, Child and Adolescent Mental Health Services
(CAMHS), recovery, Psychiatric Intensive Care Unit (PICU, out of area) • Non-medicalised settings (e.g. Crisis Resolution and Home Treatment
Teams (CRHT), crisis house) • Mental health presentations at A&E including frequent attenders? • Crisis plans/Wellness Recovery Action Plans (WRAPs) /Rainy Day
plans/Advance statements (% for those on Care Programme Approach • User feedback • Audit programme (e.g. CORE participation) • Data gaps and data quality
Detailed help and guidance

NICE: Quality standard for service user experience in adult mental health.
Quality Statement 6, access to services
• People in crisis referred to mental health secondary care services are seen within 4 hours;
• Service users have access to a local 24-hour helpline staffed by mental health and social care professionals;
• Crisis resolution and home treatment teams are accessible 24 hours a day, 7 days a week, regardless of diagnosis.
Detailed help and guidance

Law and existing Guidance • Hospital, step-down and community services should be
commissioned at a level that allows for beds to be readily available in response to a person in urgent need, as required by statute (s140 MHA)
• Police custody to be used only in ‘exceptional’ circumstances (s136)
• For people are already known to mental health services, crisis plan and any advance statements should be available and followed where possible (Care Programme Approach).
•
Detailed help and guidance
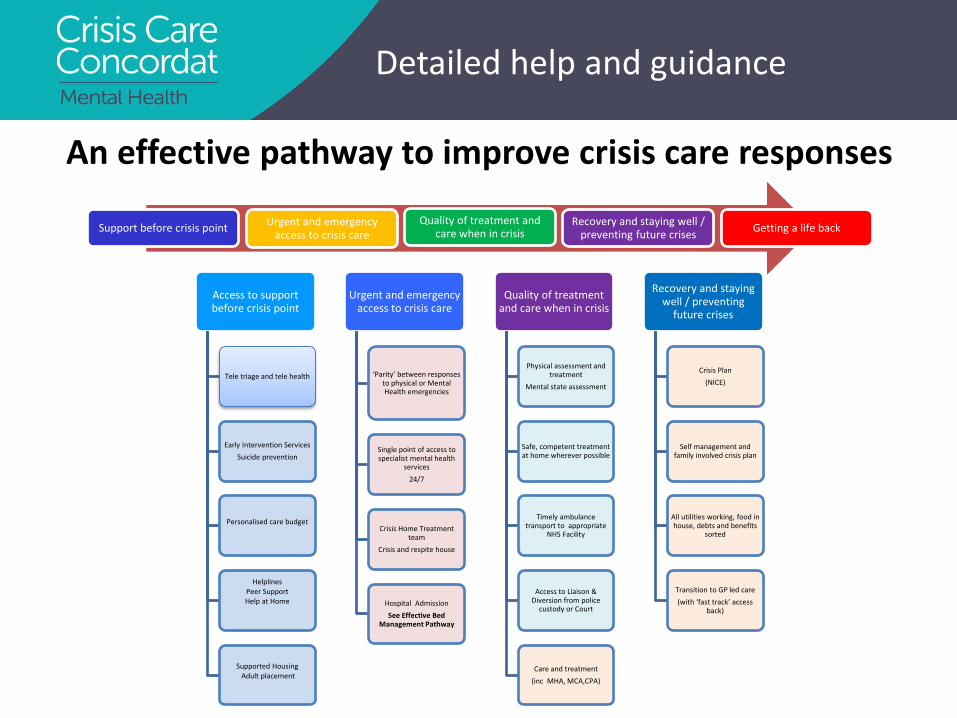
An effective pathway to improve crisis care responses
Access to support before crisis point
Tele triage and tele health
Early Intervention Services Suicide prevention
Personalised care budget
Helplines Peer Support Help at Home
Supported Housing Adult placement
Urgent and emergency access to crisis care
‘Parity’ between responses to physical or Mental Health emergencies
Single point of access to specialist mental health
services 24/7
Crisis Home Treatment team
Crisis and respite house
Hospital Admission See Effective Bed
Management Pathway
Quality of treatment and care when in crisis
Physical assessment and treatment
Mental state assessment
Safe, competent treatment at home wherever possible
Timely ambulance transport to appropriate
NHS Facility
Access to Liaison & Diversion from police
custody or Court
Care and treatment (inc MHA, MCA,CPA)
Recovery and staying well / preventing
future crises
Crisis Plan (NICE)
Self management and family involved crisis plan
All utilities working, food in house, debts and benefits
sorted
Transition to GP led care (with ‘fast track’ access
back)
Support before crisis point Urgent and emergency access to crisis care
Quality of treatment and care when in crisis
Recovery and staying well / preventing future crises Getting a life back
Detailed help and guidance

Thank you [email protected] www.crisiscareconcordat.org.uk

Serving with pride and confidence
Thames Valley Police and the Mental Health Crisis Care Concordat
Assistant Chief Constable Alan Baldwin

Serving with pride and confidence
“The test of police efficiency is the absence
of crime and disorder...”
Robert Peel 1829

Serving with pride and confidence
“..I set.... chief constables one clear
objective: cut crime.....I’ve told them to cut crime.”
• Theresa May Home Secretary 2011

Serving with pride and confidence
Serious Case Reviews – Vulnerable People
• Holly and Jessica • Victoria Climbie • Baby P • Rotherham • Pilkington • ........Information sharing

Serving with pride and confidence
Man on the Clapham Omnibus...
• What is exceptional....?

Serving with pride and confidence
• 15- 20% of uniform police time relates to Mental Health
• Nationally S136 usage is rising
• Custody is not used on an “exceptional” basis as POS.
• 90% of cases transported by police.
• 140 people restrained.
• Called 555 occasions for disorder.
• 1200 MH “Fear for Welfare” calls
Operational Context
Serving with pride and confidence
.........
• Contact, restraint, transport and accommodation provided by the enforcement arm of the state is not the right place, ethically, morally or legally for people suffering mental health crises.
• Police legitimacy – procedural justice and the fair, legal, proportionate and ethical use of power.

Serving with pride and confidence
....and our staff....
• Dozens of police officers under criminal investigation relating to deaths and injury of people suffering mental health crises.
• To walk away? The ethical dilemma.

Serving with pride and confidence
Thames Valley Police is committed to: • working together to deliver a high quality response when
people with mental health problems urgently need help
• working in partnership to deliver against the expectations of the Concordat action plan
• meeting statutory responsibilities contained within ECHR, PACE, Mental Health Act, Mental Capacity Act and supporting Codes of Practice

Serving with pride and confidence
Challenges
• Knowledge and awareness
• Use of Custody
• Restraint
• Transport
• Senior oversight arrangements

Serving with pride and confidence
Proposed Police Actions
• Training
• Custody as POS only “exceptionally”
• Risk-assessed restraint by officers - high threshold
• Transport only in exceptional circumstances
• Mental health street triage schemes
• Strategic and operational partnership engagement

Mental Health Crisis Care Concordat.
Sue Putman Clinical Lead, Mental Health & Learning Disability.

Key Partnership Areas for SCAS.
• Alternative Care Pathways. • MH Practitioners in EOC. • Anticipatory Care Plans. • Education.
AMAE:

Alternative Care Pathways (ACPs).
If I need emergency help for my mental health, this is treated with as much urgency and respect as
if it were a physical health emergency.

MH Practitioners in EOC.

Anticipatory Care Plans.
Every effort is made to understand and communicate with me. Staff
check any relevant information that services have about me and, as far as possible, they follow my wishes and any plan that I have voluntarily
agreed to.

Education.

Summary of benefits…….
• Improved patient care. • Improved partnership
working. • Improved data/monitoring.

Berkshire Crisis Concordat Helen Mackenzie Director of Nursing and Governance

CQC MHA Assessment and Application for Detention Thematic
Inspection Patient’s told us:
• "When you are being shipped off it's really scary because you don't know the hospital. At least if you are in Reading you can get staff you know.”
• “If you are sectioned there are all these people you don't know and that's really scary.”
• “I have usually been assessed by people I did not know.”
• “Speaking to my GP would help.”

Building on the CQC Inspection
• CEO took the initiative – he did not want another central initiative that did not add value to the patients in crisis in Berkshire
• Action plan – bring commitments into the public domain • Good commitment from TVP, SCAS, CCG
commissioners, 6 LA’s, BHFT, RBH

Challenges
• System complexities • Remote bodies for primary care commissioning • Competing priorities – Heatherwood and Wexham Park • 5 substance misuse providers

Next steps
• Draft concordat in place – 1st October upload planned • Not planning for perfection but evolution • Commitment to review • January stakeholder workshop/conference

Caring, safe and excellent
Oxford Health NHS Foundation Trust
Rob Bale Clinical Director Adult Mental Health Services

Caring, safe and excellent
Oxford Health NHS Foundation Trust
• Community and mental health services for children and young people across Oxfordshire, Buckinghamshire, Wiltshire, Swindon, Bath and North East Somerset
• Adult and Older Adult mental health services across Oxfordshire and Buckinghamshire
• Community Health Services for Oxfordshire • Thames Valley Forensic Services

Caring, safe and excellent
What are we doing to improve care? • User and carer
engagement • Increasing access • Restructuring Adult
Services • Service Developments • Pilot Projects • Staff training • Safer Care initiatives
• Increasing staffing on wards
• Improving our buildings
• Research • Partnership working • Strengthening
leadership • Recovery

Caring, safe and excellent
Adult Restructuring
Community • 7 days per week, 7am to
9pm • Removal of institutional
barriers • Locality focus • Evidence based packages
of care • Single point of access
Inpatient wards • Dedicated consultant
time • Increased staffing • Modern matron per ward • Clear model of care

Caring, safe and excellent
Access to Mental Health Services in A+E • Reconfigured services in Oxfordshire. • Newly Commissioned services in
Buckinghamshire – Multidisciplinary team – 7 days per week – Rapid assessments – Dr to Dr contact – Teaching training and support – Advanced assessment skills

Caring, safe and excellent
Street Triage • Department of Health money to deliver pilot • Led by TVP – supported by OH, Thames
Valley Local Area Team • Opportunity to develop partnership working • Support from Mental Health Charities • Clear operational policy • Data collection and evaluation • Its working!

Caring, safe and excellent
Improving our facilities • Whiteleaf Health and Well Being Centre
(Aylesbury) – 80 ensuite bedrooms – 3 hospital S136 suites
• Highfield Adolescent Unit • Upgrading existing acute IP wards • Increased number of Oxfordshire S136
suites

Caring, safe and excellent
What do we need to work on? • Ensuring Mental Health is everybody's
business • Real alternatives to admission • Earlier intervention • Timely access to beds • Timely access to S12 doctors/AMHP’s • Improved information systems • Recovery

Caring, safe and excellent
Each locality needs to focus on a number of questions: • What local actions have there been to date regarding the
CCC? • Are there any gaps, has a gap analysis completed? • Is there agreement on local ‘actions’ in plan? • Are plans fully inclusive? Do they include children, LD
and older adults? • When are declarations and plans likely to be
finalised/agreed and signed? • Is there a need for a Thames Valley wide declaration? • Are there any actions which could be applied at a
regional TV scale? Is so, what are they?

Caring, safe and excellent
Outputs of the discussion: • An assessment of how complete current draft
plans are • A list of actions that need to take place before
the end of December • Who will manage the process to completion • A list of TV-wide CCC actions • Definition of what role the group would like the
SCN to play