crafting an art regimen for initiation or salvage: are...
TRANSCRIPT

NORTHWEST AIDS EDUCATION AND TRAINING CENTER
Crafting an ART Regimen for Initiation or Salvage: Are NRTI’s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director, NW AETC ECHO
Last Updated: 1/22/15

NRTI-Sparing Regimens: Outline
• Treatment initiation • Switching for maintenance • Salvage therapy • Future questions and directions


Why Consider NRTI-Sparing Regimens?
• NRTI’s are the backbone of first-line and salvage regimens • However, toxicity can be limiting
- Tenofovir à renal and bone effects - Abacavir à hypersensitivity if B*5701(+), ?CV effects - Older NRTI’s à many short and long-term side effects
• Resistance may preclude use

Data for Use as Initial Therapy NRTI SPARING-REGIMENS

PI-Containing Dual Regimens for Initial Therapy
Study NRTI-Sparing Regimen
Comparator N Follow-up Efficacy Outcomes and Issues
NEAT/ ANRS 143
DRV/r + RAL
DRV/r + 2 NRTI’s
805 96 weeks Non-inferior
More failures and resistance if CD4 <200 or VL >100K
RADAR DRV/r + RAL
DRV/r + 2 NRTI’s
83 48 weeks Inferior More failures and treatment discontinuations
ACTG 5262 DRV/r + RAL
None 112 96 weeks High rate of failure (26%)
High rates of RAL resistance if VL >100K
PROGRESS LPV/r + RAL
LPV/r + 2 NRTI’s
206 96 weeks Non-inferior
Few participants with VL >100K
SPARTAN ATV (300 mg BID) + RAL
ATV/r + 2 NRTI’s
94 Stopped at 24 weeks
Inferior More failures with resistance and more jaundice
NEAT/ANRS143: Raffi F et al. Lancet. 2014;384:1942-51. RADAR: Cutrell JM et al. PLoS One. 2014 Aug 29;9(8):e106221. ACTG 5262: Taiwo B et al. AIDS. 2011;13;25(17):2113-22. PROGRESS: Reynes J et al. AIDS Res Hum Retroviruses. 2013 Feb;29(2):256-65. SPARTAN: Kozal MJ et al. HIV Clin Trials. 2012 May-Jun;13(3):119-30.
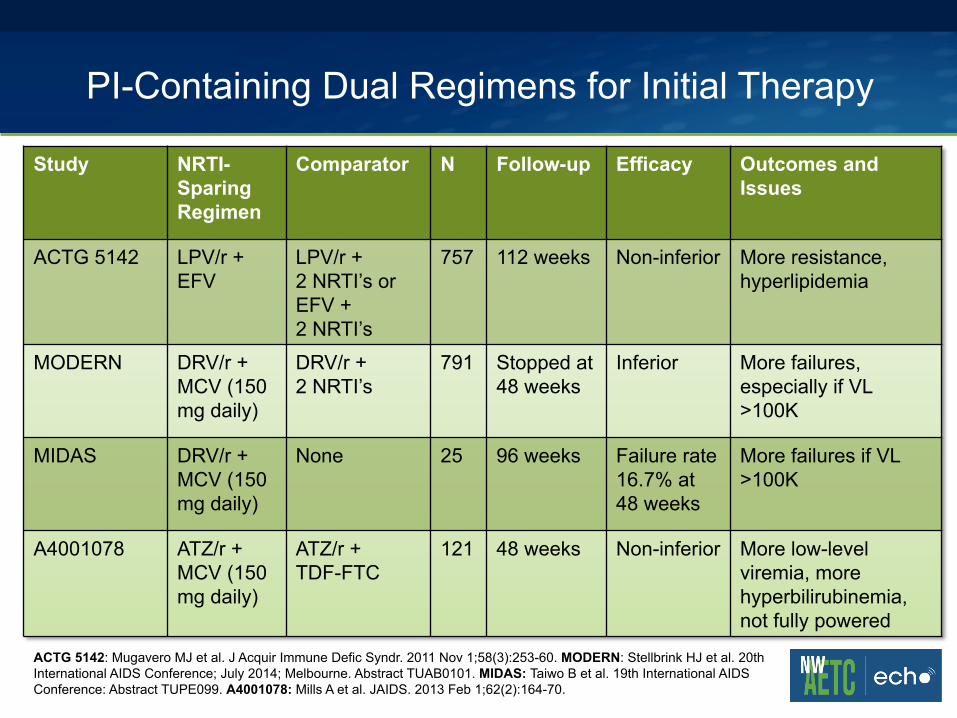
PI-Containing Dual Regimens for Initial Therapy
Study NRTI-Sparing Regimen
Comparator N Follow-up Efficacy Outcomes and Issues
ACTG 5142 LPV/r + EFV
LPV/r + 2 NRTI’s or EFV + 2 NRTI’s
757 112 weeks Non-inferior More resistance, hyperlipidemia
MODERN DRV/r + MCV (150 mg daily)
DRV/r + 2 NRTI’s
791 Stopped at 48 weeks
Inferior More failures, especially if VL >100K
MIDAS DRV/r + MCV (150 mg daily)
None 25 96 weeks Failure rate 16.7% at 48 weeks
More failures if VL >100K
A4001078 ATZ/r + MCV (150 mg daily)
ATZ/r + TDF-FTC
121 48 weeks Non-inferior More low-level viremia, more hyperbilirubinemia, not fully powered
ACTG 5142: Mugavero MJ et al. J Acquir Immune Defic Syndr. 2011 Nov 1;58(3):253-60. MODERN: Stellbrink HJ et al. 20th International AIDS Conference; July 2014; Melbourne. Abstract TUAB0101. MIDAS: Taiwo B et al. 19th International AIDS Conference: Abstract TUPE099. A4001078: Mills A et al. JAIDS. 2013 Feb 1;62(2):164-70.

“NRTI-Lite” Regimens for Initial Therapy
Study NRTI-Sparing Regimen
Comparator N Follow-up Efficacy Issues
GARDEL LPV/r + 3TC
LPV/r + 2 NRTI’s
426 48 weeks Non-inferior
Comparator NRTI’s mostly AZT & 3TC
ACTG 5303 DRV/r + MVC (150 mg daily) + FTC
DRV/r + TDF/FTC
254 Ongoing…
GARDEL: Cahn P et al. 14th European AIDS Conference. Brussels; Sept. 2013. Abstract LBPS7/6. ACTG 5303: https://clinicaltrials.gov/ct2/show/NCT01400412

NRTI-Sparing or “Lite” Regimens for Initial Therapy: Summary
• Studies limited by unusual dosing, outdated comparators, insufficient power, and other issues
• Most studies show lower efficacy or more side effects without improving pill burden or dosing frequency
• Two trials with the most reassuring results used boosted lopinavir, which is no longer a recommended agent
• Need well-designed trials of modern drugs! - ie. boosted darunavir + dolutegravir +/- 3TC/FTC

Data for Use as Maintenance Therapy NRTI SPARING-REGIMENS

New Data from IAS 2014 Switching to 2-Drug Regimen for Maintenance
Study NRTI-Sparing Regimen
Comparator N Follow-up Efficacy Outcomes and Issues
SALT ATZ/r + 3TC
ATZ/r + 2 NRTI’s
286 48 weeks Non-inferior
OLE LPV/r + 3TC or FTC
LPV/r + 2 NRTI’s
239 48 weeks Non-inferior
HARNESS ATZ/r + RAL
ATZ/r + 2 NRTI’s
109 Stopped at 48 weeks
Inferior More virological rebound and low-level viremia
MARCH MVC (150 mg BID) + boosted PI
MVC (300 mg BID) + 2 NRTI’s
560 Ongoing…
SALT: Perez-Molina JL et al. 20th International AIDS Conference; July 2014; Melbourne. Abstract LBPE 18. OLE: Gatell JM et al. 20th International AIDS Conference; July 2014; Melbourne. Abstract LBPE17. HARNESS: Van Lunzen J et al. 20th International AIDS Conference; July 2014; Melbourne. Abstract LBPE19. MARCH: https://clinicaltrials.gov/ct2/show/NCT01384682

Data for Use as Salvage Therapy NRTI SPARING-REGIMENS

NRTI-Sparing Regimens for Salvage Therapy Randomized Trials
Study ART History
NRTI-Sparing Regimen
Comparator N F/u Efficacy Issues
OPTIONS PI failure >2 active agents, no NRTI’s
>2 active agents + NRTI’s
360 48 weeks
Non-inferior
Greater mortality in NRTI arm; only powered to detect 15% non-inferiority
SECOND-LINE
NNRTI failure
LPV/r + RAL
LPV/r + 2 or 3 NRTI’s
541 48 weeks
Non-inferior
Open-label, genotype optional, included AZT, endpoint VL <200
EARNEST NNRTI failure
LPV/r + RAL then LPV/r
LPV/r + NRTI’s
1277 96 weeks
Dual therapy non-inferior
More resistance and less VL suppression with LPV/r monotherapy
OPTIONS: Tashima K et al. 20th CROI. Atlanta, March 2013. Abstract 153LB. SECOND-LINE: Boyd MA et al. Lancet. 2013 Jun 15;381(9883):2091-9. EARNEST: Paton NI et al. N Engl J Med. 2014 Jul 17;371(3):234-47.

NRTI-Sparing Regimens for Salvage Therapy Observational Studies
Study ART History
NRTI-Sparing Regimen
Comparator N F/u Efficacy Outcomes and Issues
Imaz et al. 2011
Triple-class failure
>2 active agents, no NRTI’s
>2 active agents, + NRTI’s
122 48 weeks
Non-inferior
INROADS Failing or naïve with resistance
DRV/r + ETR
None 54 48 weeks
100% VL suppressed (failing); 87% (naïve)
75% study completion; 2 acquired ETR resistance
Nozza et al. 2011
Triple class failure or resistance
RAL + ETR + MVC (all BID)
None 28 96 weeks
96% VL <50 copies
Imaz et al. 2009
Triple class resistance
RAL + ETR + DRV/r (all BID)
None 32 24 weeks
94% VL<50 copies
Imaz et al. J Antimicrob Chemother. 2011 Feb;66(2):358-62. INROADS: Ruane P et al. 7th IAS Conference. Kuala Lumpur, Malaysia. July 2013. Abstract WEPE515. Nozza et al. JAIDS. 2011 April;56(4):e113-e115. Imaz et al. J Acquir Immune Defic Syndr. 2009 Nov 1;52(3):382-6.

Should Cost Be a Consideration?
• VERITAS (Trottier et al, Nov 2014): - 31 subjects with MDR HIV, on >4 ARV’s (w/1 inactive NRTI) - 3TC or FTC removed in 29 (94%); AZT or TDF in others - 1 or 2 ARV removals à mean annual savings of $3319 CDN or
$8630 CDN respectively
VERITAS: Trottier L et al. J Int AIDS Soc. 2014; 17(4Suppl 3): 19815.

Future Questions and Directions
• Will we worry so much with tenofovir alafenamide (TAF)? • What about dolutegravir? Need data for the following:
- Dolutegravir + boosted PI (+/- 3TC or FTC) - Rilpivirine + boosted darunavir + dolutegravir
• How might cabotegravir (GSK-744) or rilpivirine-LA fit in?

NRTI-Sparing Regimens Take Home Points
• Most data for initial therapy is limited by design/dosing issues • Dual therapy options should be used only in unique cases
and perhaps for maintenance in select patients • Anecdotally, “NRTI-lite” regimens like 3TC/FTC + boosted PI
+ integrase seem to work well, but we need data • More advanced HIV disease equates to higher risk of failure • Could consider including NRTI’s for salvage, at least until
suppressed, then simplify

Case Question
• A patient previously treated with multiple NRTI’s, efavirenz, and boosted lopinavir transfers care to you. He has been off ART and viral load is 9,400. Prior genotypes show K103N, E138A, M184V, M41L, T215Y, K219Q, and PI mutations (but no darunavir-associated mutations).
• He has never taken integrase inhibitors. You plan to restart ART with boosted darunavir, etravirine, and dolutegravir.
• Would you add lamivudine (3TC) or emtricitabine (FTC)? A) Yes, would add indefinitely B) Yes, would add until viral load suppressed then withdraw C) No, would not add