covid-19 tests english - wordpress.com
TRANSCRIPT

SARS-COV 2 VIRUS HAS NEVER BEEN ISOLATED COVID-19 SWABS PRODUCE UP TO 95% OF FALSE POSITIVES
ALL CERTIFIED BY HEALTH AUTHORITIES
With the most complete analysis on Covid-19 tests
Dr. Stefano Scoglio, Ph.D., B.Sc.
I have argued, among other things, that the virus cannot be considered isolated, because what is considered as “isolated” is indeed a complex matrix, made up of more or less centrifuged pharyngeal or broncho-alveolar fluid, in which, according to my calculations, there are about 30 billion viral-like particles (human and bacterial nucleic acids, extra-cellular vesicles, exosomes, etc.), and this complex matrix, without knowing if there is and how much virus there is, is defined as the "isolated virus”. As reported by an important study on exosomes (a little known branch of biology, which through has been around for about 50 years), most of the human pathological liquids used for testing, are made for the most part of human genome particles, up to 99.6% (see my paper “The new Pathology of asymptomaticity and the invalid swab test”).
CDC and EU Commission acknowledge that the virus has never been isolated
But now, I have finally found official proof that the virus was never truly isolated! It is unequivocally recognized by both the European Commission and the US CDC, the most important national health organization in the world. Let's start with the European Commission, which in its document of 16 April last wrote:
"Since no virus isolates with a quantified amount of the SARS-CoV-2 are currently available ..." 1
Before analyzing in detail this statement, which still seems to me self-evident, let's see what the CDC writes:
"Since no quantified virus isolates of the 2019-nCoV are currently available..." 2
In short, both Europe and the US say the same thing: they call a material in which the virus has not been quantified "isolated virus". But if it hasn't been quantified, how can it be an isolated virus? In any language, isolated means separate from any other substance, thus constituting the 100% isolate. When you make an extract, for example of phycocyanins, you are satisfied with 80% to say that it is “pure" phycocyanin: it is not really that, but you accept it as a convention
European Commission, Working Document of Commission Services, Current performance of COVID-19 1
test methods and devices and proposed performance criteria, April 16 2020, p.19
Centers for Disease Control and Prevention, Division of Viral Diseases, CDC 2019-Novel Coronavirus 2
(2019-nCoV) Real-Time RT-PCR Diagnostic Panel , 13/07/2020, p.39.
because you are satisfied with the 80% concentration. But here, it is not even known how much of the virus there would be! In the meantime, this proves that what is called an "isolated virus" is, as I have always maintained, a complex matrix of which the virus would constitute only a percentage. But what percentage: 1%, 5%, 50%? Dunno, no one knows, it could be made up of 99% of something else, but we continue to call it "isolated"! And there's more: if I knew the virus, if I had identified it adequately, I would be able to recognize it within the complex matrix, and therefore I could quantify it. The fact that no one has quantified it, as both the EU Commission and the CDC admit, means that the virus, in addition to never having been truly isolated, has never even been identified, described in its natural constitution, because otherwise it would have been quantified within the complex matrix. This implies that all the gene sequences that are presented to us as the "isolated virus" are but hypothetical constructions elaborated on the computer, mere artifices (as it has been explicitly declared by the German Drosten group in their establishment of their swab test! 3
Finally, if we have never isolated or identified the virus, what is in the swabs? What is in the vaccines being prepared? And above all, how can we say that this alleged virus, which at the present state of knowledge is completely unknown, is responsible for whatever pathology is?
After demonstrating how the same European and American health authorities claim that the virus has never been isolated, we will now see how the same health authorities, first of all our Istituto Superiore di Sanità, admit that the Covid-19 swab tests are completely unreliable. I have already written some posts and articles on how swabs and serological tests for Covid-19 are unreliable, in fact wholly meaningless, given that they have no real link to an alleged SARS-Cov2 virus, which has never been isolated. We have also seen how this unreliability has even been certified by the European Commission and the Istituto Superiore di Sanità, which last April-May published documents stating that 78 different swabs tests were circulating in Europe, none of which validated by independent bodies, none evaluated or authorized in advance, and even the vast majority of whom did not even state which gene sequences they used (see my “The new pathology of 4
asymptomaticity and the invalid swab test”); therefore potentially containing anything. At this point I wanted to investigate the matter, and I discovered further elements, both scientific and legal.
Corman VM et al., Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR, Euro Surveill. 3
2020 Jan 23; 25(3): 2000045.
European Commission, Working Document of Commission Services, Current performance of COVID-19 4
test methods and devices and proposed performance criteria, April 16 2020.

The regulatory situation
First of all, it must be said that swab tests fall under the new REGULATION (EU) 2017/746 OF THE EUROPEAN PARLIAMENT AND COUNCIL of 5 April 2017 relating to in vitro diagnostic medical devices, which repeals Directive 98/79 / EC.In the previous, repealed legislation, in general, the affixing of the CE mark, which is primarily a safety only mark, was enough, with the exception of some in vitro diagnostic devices listed in Annex II, and dealing with already (presumably) known viruses (HIV 1 and 2, HTLV I and II and hepatitis B, C and D). For those, a technical and efficacy evaluation is required by a Notified Body, that is a validation body recognized by the EU. Now, we know from the European Commission Document of April 16 last year that none of the 78 swab test models in circulation at that date have been evaluated or submitted to any recognized evaluation body, and that even this would not even have been possible since almost none of those 78 swabs provides an adequate technical data sheet, including the specification of the gene sequences used. How is it possible? After all, SARS Cov2 should be an even more important virus than those of hepatitis or HIV, which have never led to the closure of the economy and social life of entire nations. It is possible because the Regulation of Directive 98/79 EC lists only the aforementioned viruses, and since SARS Cov 2 is a new virus it is not included. Yes, but we have just seen that this regulation has been repealed by the 2017 regulation, which in turn places even more stringent requirements than the previous one, requiring preliminary efficacy assessments by recognized validation bodies for all in vitro diagnostic devices, which also includes Covids-19 swabs. So why have swab tests been introduced in the market without any validation or preliminary evaluation, and even without the specifications on the gene sequences used? Because, as we say in Italy, “fatta la legge trovato l’inganno” (the law made, the cheating found”): the 2017/46 Regulation of 5 April 2017 will come into force, for in vitro diagnostic devices, only on 26 May 2022 ! And with this, the Covid-19 swabs enjoyed the free interregnum, not being included, as they relate to a new virus, in the 1998 Regulation; and not yet being subjected to a 2017 Regulation that would have outlawed them all, but which will not come into force until mid-2022! The question that needs to be asked, and which cannot fail to have legal relevance, is: these tests have been completely without evaluation and validation, and are in circulation only thanks to the fact that a regulatory vacuum has been created between the 1998 Regulation, which limited the list of viruses only to the known ones (but which by analogy should also apply to the new emerging ones) and the 2017 Regulation, which repeals the 1998 one but does enter into force only in 2022; in short, if these Covid-19 swabs are used only thanks to a legislative anomaly, and in 2022 they would be completely illegal; is it permissible that the fate of entire nations and of the entire world economy is entrusted to such barely legal swab tests? No, it should not be admissible, and if it is, it will be only because the legal form is made to prevail over substance. But now we come to the scientific substance of swab tests. The first argument is that they are completely meaningless because the virus has never been isolated, and therefore there is no realistic marker to support its action. I

have dealt with this elsewhere; but it seems that on this point the ears of those who should intervene tend to be shut (even if we will continue to shout the truth). So let's pretend that this is not the problem, that the virus has been isolated. We will see that even from this point of view, the Covid-19 tests remain completely unreliable and meaningless.
The question of the virus mutation
One of the fundamental problems is the supposed constant mutation of the virus. As the Istituto Superiore di Sanità itself writes (confirming what I have always been saying):
"... the virus can in fact mutate and new nucleotide sequences deposited in databases can reveal whether these mutations can in turn make a particular test less effective or even ineffective ... It is important to point out that for the diagnosis of this emerging virus, with a state of the art in flux, the actual performance of the observed device may differ from that determined by the initial performance study conducted by the manufacturer for the purposes of CE marking, in a previous state of the art.” 5
As I have always argued too: if at GISAID, where the gene sequences of SARS-Cov 2 are collected, there are now over 100,000 different sequences, and they are constantly increasing, what is the value of a test developed in February 2020 in China and used in July 2020 in Europe, when the virus has certainly mutated? To understand this, it would suffice to say that most of the swabs in circulation were structured (if they were) on the virus sequenced by the Chinese in Wuhan. But in Italy it was both the Spallanzani and the San Raffaele hospitals who provided different gene sequences, and both, in addition to pseudo-isolating the virus with the same phony methods that I have described elsewhere, immediately made it clear that they were viruses modified with respect to to the one “isolated” in China ; and in a study organized by several Italian medical centres (Sacco, San 6
Raffaele, etc.), when they analyzed 59 liquid samples from Covid-19 patients from different centres in Central and Northern Italy, they found very notable mutations, to the point that :
“A mean of 6 nucleotide substitutions per viral genome was observed, without significant differences between synonymous and non-synonymous
Gruppo di Lavoro ISS Test Diagnostici COVID-19, Dispositivi diagnostici in vitro per COVID-19. Parte 2: 5
evoluzione del mercato e informazioni per gli stakeholder , Rapporto ISS COVID-19 n. 46/2020, 23 Maggio 2020, p. 8
Capobianchi M.R. et al., Molecular characterization of SARS-CoV-2 from the first case of COVID-19 in 6
Italy, Clin Microbiol Infect, 2020 Jul;26(7):954-956.
mutations, indicating genetic drift as a major source for virus evolution." 7
This study shows that not only does the virus change from continent to continent, from nation to nation, but even from province to province, and in fact from person to person! So are there 7 billion different viruses that just look alike? Is there a virus so magical that it incorporates 7 billion mutations? And above all: what is the use, in this context, of a universal swab test, which has only one or at most 3 gene sequences? As the ISS itself states, "... these mutations can in turn make a particular test less effective or even ineffective", and yet no one, among the political or legal authorities, bothered to verify whether the tests that support and maintain the pseudo- pandemic, whether or not they correspond to the countless mutations of this super-virus! The constant mutation of SARS-Cov2, such as to make it unrecognizable, has also been confirmed internationally: an American article, which also includes Robert Gallo among the authors, found dozens of mutations increasing over time in parallel with the alleged spread of the virus from Asia to Europe to the USA ; 8
while an Asian author analyzed 85 different SARS-Cov2 genomic sequences available at GISAID, and found 53 different SARS-Cov2 strains from various areas of China, Asia, Europe and the United States. 9
In short, if the virus constantly changes, then the swab test is useless, because it looks for a virus that is always previous and always different from the one currently in circulation. This alone would be enough to understand that the Covid-19 swab test is completely, 100%, fallacious! This is what happens in reality. The "Drosten PCR Test" and the Institute Pasteur test, the two tests considered to be the most reliable (although neither have been externally validated), both focus on the E gene, even if the Drosten test uses it as preliminary test, while the Institut Pasteur uses it as a definitive test. According to the authors of the Drosten test, the E-gene test is able to detect all Asian viruses, thus being both very non-specific (all viral strains) and limited to a geographical area (Asia). Furthermore, the Institute Pasteur test, one of the most adopted in Europe, uses the E-Gene test as the final test, although it is well known that the SARS-Cov2 virus (or virus) believed to circulate in Europe would be different from the Asian ones. And then in April, WHO changed the algorithm "... recommending that from now on a test can be considered positive even if only the dosage of the E gene (which will probably detect all Asian viruses!) gives a positive result.” In short, for the WHO and its followers, everything is good to maintain 10
the tragic farce of the pandemic!
Lai A. et al., Molecular Tracing of SARS-CoV-2 in Italy in the First Three Months of the Epidemic, Viruses 7
2020, 12, 798; doi:10.3390/v12080798.
Pachetti M. et al., Emerging SARS-CoV-2 mutation hot spots include a!novel RNA-dependent RNA 8
polymerase variant, J Transl Med (2020) 18:179 https://doi.org/10.1186/s12967-020-02344-6.
Phan Tung, Genetic diversity and evolution of SARS-CoV-2, Infection, Genetics and Evolution, 81 (2020), 9
104260.
Engelbrecht T, Demeter K., COVID19 PCR Tests are Scientifically Meaningless, Jun 27 2020, p.21. 10
https://off-guardian.org/2020/06/27/covid19-pcr-tests-are-sc

The question of RT-PCR cycles
Another serious problem of the Covid-19 swabs, which use the RT-PCR method, is that the reliability of this method depends on the number of cycles (replications) that are used to find the SARS-Cov2 virus. Prof. Stephen Bustin, one of the world authorities of PCR, wrote in a recent article regarding the identification of the presence of SARS-Cov 2:
"… The most widely used method is quantitative fluorescence-based reverse transcription polymerase chain reaction (RT-qPCR). Despite its ubiquity, there is a significant amount of uncertainty about how this test works, potential throughput and reliability." 11
Probably this is above all due to the question of the PCR cycles that are normally performed. In an interview with the late David Crow, a valuable Canadian researcher, Bustin states:
"... the cycle number per se is not a good measure ... most instruments, when you get above a cycle number of 35, then you start worrying about the reliability of your result ... so, you want to be sure that your results are within the 20 to 30 cycles ... "
And since the majority of swab PCR tests use up to and beyond 40 cycles, Crow asks Bustin:
"... if you get up to 40 cycles, you could get a ghost, the PCR could string bases together casually ..."
And Bustin replies: “I would be very unhappy about 40 cycles…”. 12
So let's see how many cycles are normally used in Covid-19 tests. Maybe you remember the recent controversy, fuelled by dr. Remuzzi of the San Raffaele Hospital in Milan, that the swabs that find the virus only with a high number of cycles refer to cases of very low virality, thus considered non-infectious:
“Remuzzi reports that the positivity in the swabs of the Mario Negri study emerged only after 34-38 cycles of amplification. But the more it is amplified, the weaker and more uncertain the signal becomes, suggesting traces of viral RNA now residual and inactive. In short, no infection." 13
Bustin S.A, Nolan T., RT-qPCR Testing of SARS-CoV-2: A Primer, Int. J. Mol. Sci. 2020, 21, 3004; 11
doi:10.3390/ijms21083004, p. 1
David Crow, The Infectious Myth: https://infectiousmyth.podbean.com/e/the-infectious-myth-stephen-12
bustin-on-challenges-with-rt-pcr/
Luca Carra, Debolmente positivi: realtà o illusione?, Internazionale, 23 Giugno 2020. 13

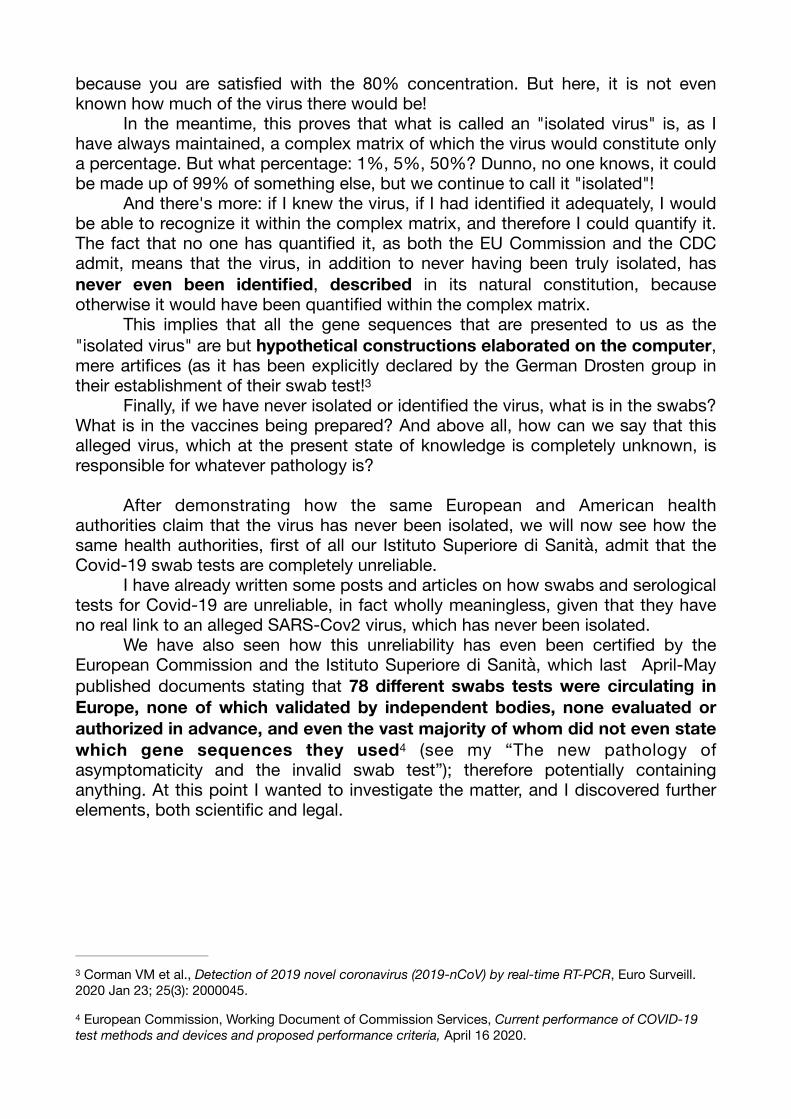
This is in accordance with what Prof. Bustin maintains: at or above 30 cycles, and particularly above 35 cycles, the reliability of the swab test collapses, and at most, to save the day, it can be argued that the presence of viruses is so weak that it is no longer infectious. The substance does not change: either the virus is created by the PCR as a "ghost", as Crow and Bustin claim, or it’s without any viral load. Either way, why they continue using these swab tests results to terrorize people and prolong various types of lockdowns? And that swab tests normally use around or above 35 PCR cycles is confirmed by this table which reports on a series of different tests with their average number of cycles:
This table includes, due to space requirements, only 6 of the 22 swabs analyzed and tested by FIND (Foundation for Innovative New Diagnostics), an organization often indicated by health authorities as a reliable tool for evaluating diagnostic tools. As can be seen from the table I have reconstructed, all are at 14
least around 35 cycles, and several are above 35 cycles, sometimes even close to
https://www.finddx.org/covid-19/sarscov2-eval-molecular/ 14

40. And consider that these are the averages, which means that in 30-35% of cases it goes beyond 40 cycles. And this is also confirmed for Cepheid's Xpert Xpress test, which the American FDA deemed so important and reliable to issue an emergency authorization for , skipping all the verification steps. Well, even this very important 15
test adopts an excessive number of cycles:
The average referred to the E gene, which is non-specific and typical of all coronaviruses (as we shall see), is around 34-35 cycles; but the average referred to the N2 gene, which should be more specific than SARS-Cov2 (we will see that it is not so even for this gene), is expected to be around 37-38 cycles! This means that in most cases the swabs test gives a phantom results, or in any case, even if one believes that they actually get the virus, s/he would have to admit that it’s in such a weakened state that no longer constitutes any danger. Thus, there is no longer any reason to terrorize with the threat of “asymptomatic positives”, because clearly they are individuals unable to infect anything. But the truth goes deeper, because the swabs produce results without any meaning, ghosts results that are in no way indicative of the presence of a SARS-Cov 2.
The question of cross-reactivity, or lack of specificity.
Let's take the three most important swab test models used by many of the circulating tests: that of the Institut Pasteur, as taken up by the WHO; that of the German-European group of Drosten; and that of the American CDC. That of the Institut Pasteur (as reported by a WHO document), is so at risk of non-specificity (i.e. of capturing viruses or viral-like particles other than SARS-Cov2 with swabs) that in one of its 3 primers (the gene sequences with which one goes to search for the virus) there is even a gene sequence typical of human DNA, that of chromosome 8:
Kubina R, Dziedzic A, Molecular and Serological Tests for COVID-19. A Comparative Review of SARS-15
CoV-2 Coronavirus Laboratory and Point-of-Care Diagnostics, Diagnostics 2020, 10, 434; doi:10.3390/diagnostics10060434, p. 6

Here the risk of having a positive result is present even without any virus at all, since all human beings have that CTCCCTTTGTTGTGTTGT sequence as part of their gene pool.
The American CDC instead uses other gene sequences, related to the N gene, that of the virus nucleocapsid. This choice to focus on the N gene, in its two versions N1 and N2, is due to the fact that the E gene, according to the CDC, “…also detects SARS-related coronaviruses”; which means that for the CDC the WHO swab can, in addition to binding to the human genome, catch other coronaviruses mistaking them for SARS-Cov 2. But what guarantees are there that the N1 and N2 genes are more specific? All coronaviruses have a nucleocapsid, and therefore N-type genes. The CDC claims that the N2 gene is specific to SARS-Cov2; but even on this there is no agreement, given that for some researchers it is not:
“…we found out that only one of them (RdRP_SARSr-P2) was almost specific for the new coronavirus and the other introduced probes would detect the other types of coronaviruses. In this regard, the false-positive test results may extend for COVID-19” 16
This means that there is no certainty even on the specificity of the N2 gene used by the CDC model, especially if we consider that precisely the N genes are typical of all coronaviruses. And note how the authors, even for the gene they consider specific, define it as “almost” specific, in the sense that even that is not completely specific!
Kakhki RK et al, COVID-19 target: A specific target for novel coronavirus detection, Gene Reports 20 16
(2020) 100740.
And when we come to the Drosten test, the European swab test, things become even more evident. First, we see here in an openly stated way, that these virus isolations and definitions are all computer processing, with no physical presence of the virus:
“The present report describes the establishment of a diagnostic workflow for detection of an emerging virus in the absence of physical sources of viral genomic nucleic acid.” 17
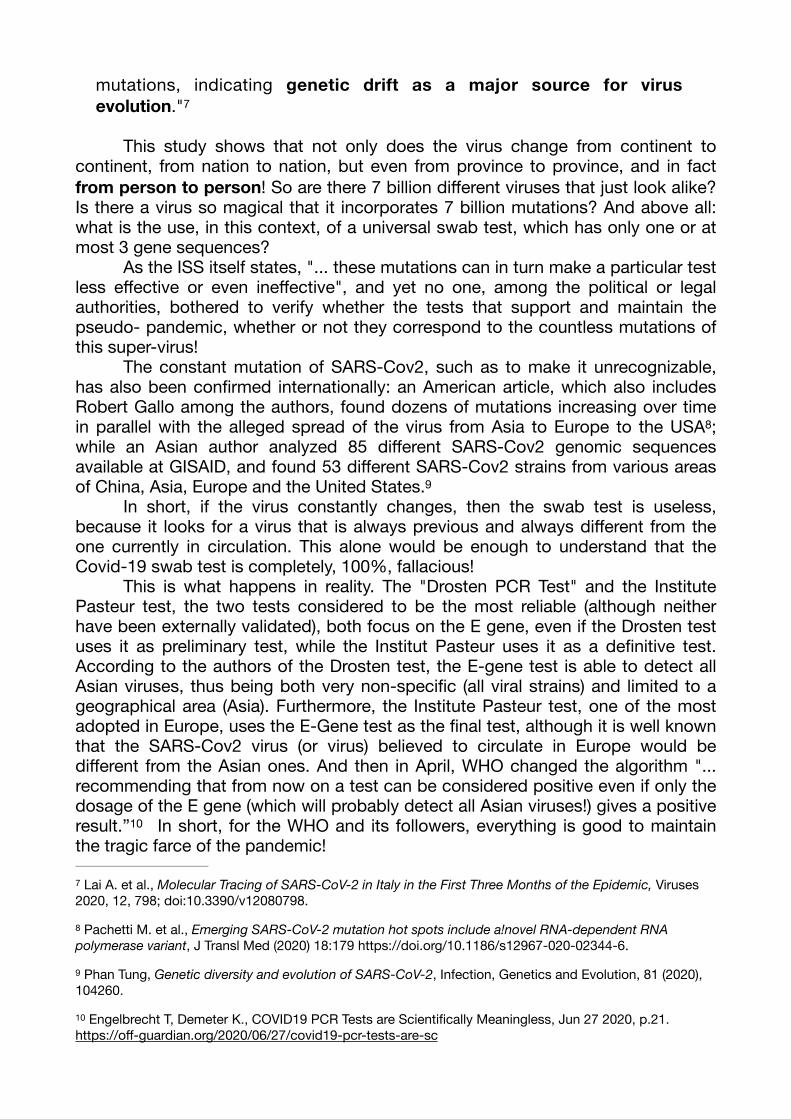
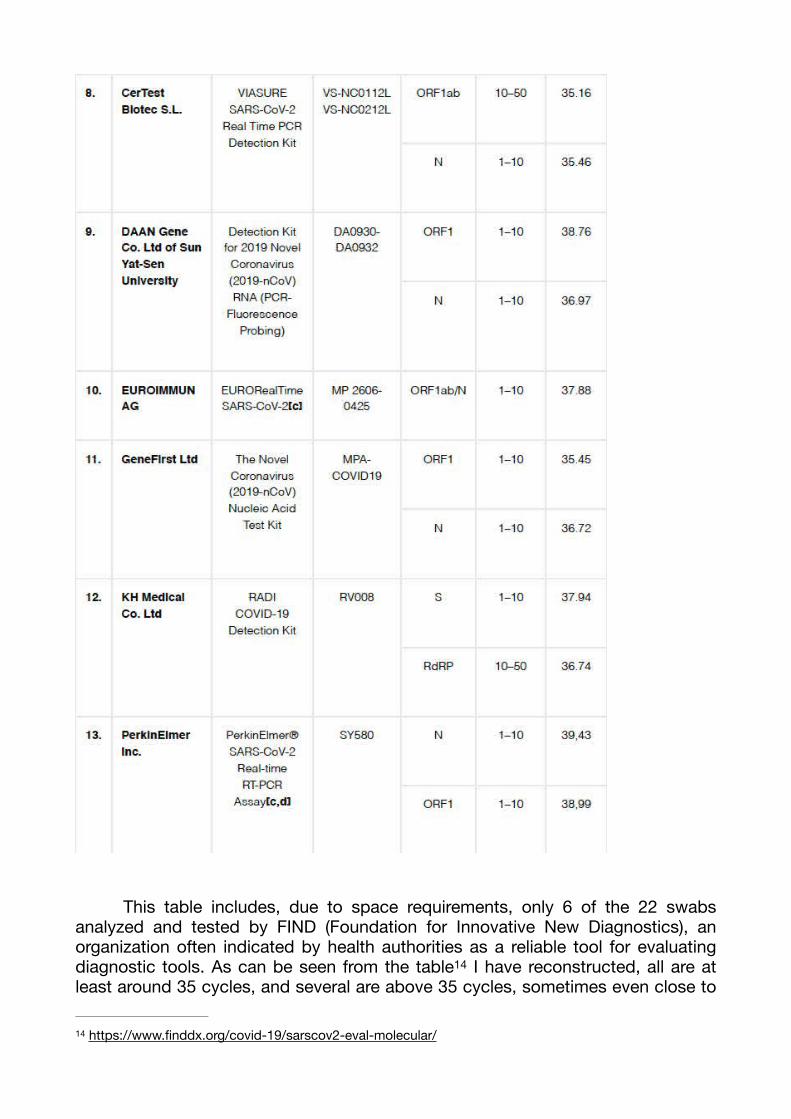
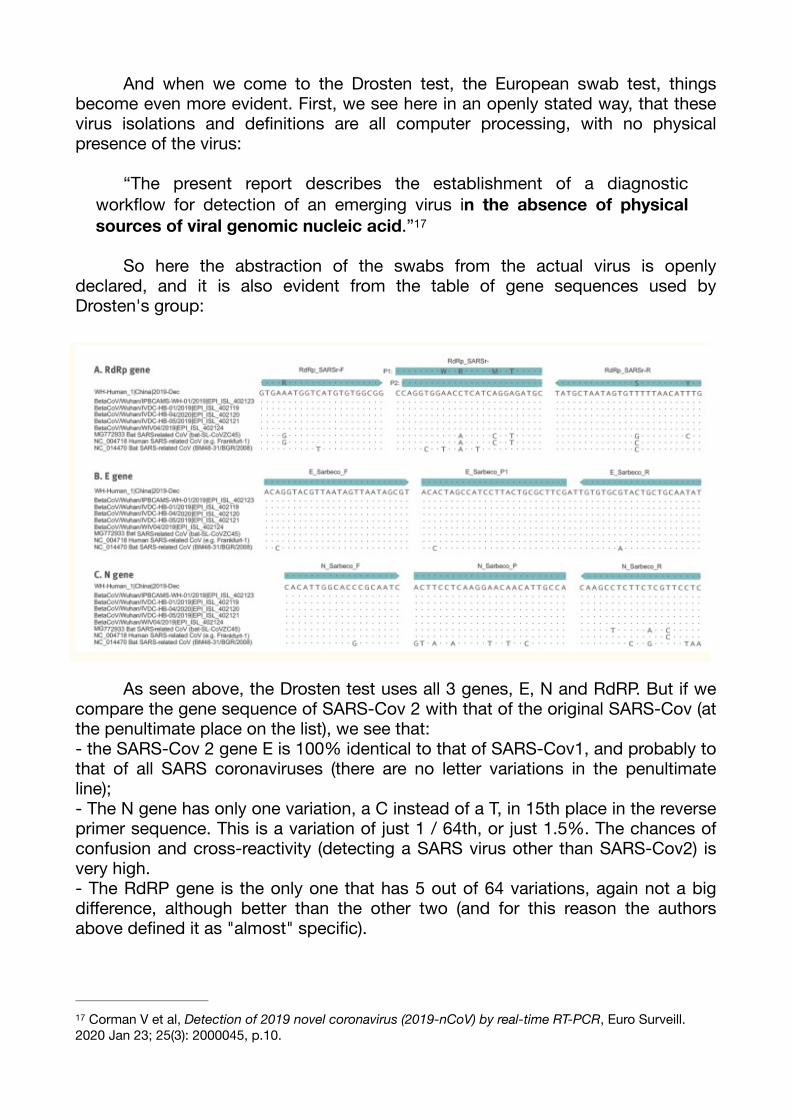
So here the abstraction of the swabs from the actual virus is openly declared, and it is also evident from the table of gene sequences used by Drosten's group:
As seen above, the Drosten test uses all 3 genes, E, N and RdRP. But if we compare the gene sequence of SARS-Cov 2 with that of the original SARS-Cov (at the penultimate place on the list), we see that:- the SARS-Cov 2 gene E is 100% identical to that of SARS-Cov1, and probably to that of all SARS coronaviruses (there are no letter variations in the penultimate line);- The N gene has only one variation, a C instead of a T, in 15th place in the reverse primer sequence. This is a variation of just 1 / 64th, or just 1.5%. The chances of confusion and cross-reactivity (detecting a SARS virus other than SARS-Cov2) is very high.- The RdRP gene is the only one that has 5 out of 64 variations, again not a big difference, although better than the other two (and for this reason the authors above defined it as "almost" specific).
Corman V et al, Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR, Euro Surveill. 17
2020 Jan 23; 25(3): 2000045, p.10.
In total we have a difference of only 6 nucleotides out of 214, a percentage of just 2.8%. And for this reason, even when independent authors tested the efficiency of the Drosten test, they concluded that the test showed:
“…a lot of cross-reactions with Coronavirus BtRs-BetaCoV (MK211374- MK211378), SARS coronavirus Urbani (MK062179-MK062184), Bat coronavirus (KY770858-KY770859), SARS coronavirus (AH013708-AH013709), and others”.
And also the RdRP gene, which should be more specific:
“…covers many coronavirus isolates, including Bat SARS-like Coronavirus (MG772904-MG772932), Rhinolophus pusillus Coronavirus (KY775091), Bat SARS-like Coronavirus (MG772903) and many others”.
In short, all the main test swabs lack specificity, and are affected by a high cross-reactivity, ie they produce a high amount of false positives. This truth, which should immediately put an end to the madness of the pseudo-pandemic pushed by these phony tampons, is finally, last but not least, openly confirmed by the Istituto Superiore di Sanità itself, a body of the Italian government.
ISS of the Italian Government: in this epidemic situation, the swab tests give up to 91% of false positives!
In the document In Vitro Diagnostic Devices for COVID-19. Part 2: evolution of the market and information for stakeholders, on 23 May 2020, the Istituto Superiore d Sanità makes an already in-depth analysis of the test-swab devices in circulation, underlining the tension between sensitivity, the ability to detect as much RNA possible viral, and specificity, i.e. the need for such viral RNA to refer only to the virus you are looking for, in this case SARS-Cov2.
"A very sensitive test in detecting the target of interest is more likely to also detect related but distinct targets that are not of interest, meaning that it may be less specific."
The ISS then explains that this voltage is modulated by another factor, namely that of "prevalence". In the epidemiological field, prevalence describes the percentage of the population affected by a certain pathology. In the case of a presumptively viral disease such as Covid-19, the prevalence indicates how many current Covid-19 patients there are out of the total population.Why is this data important in relation to the reliability of the swab tests? Because the greater the percentage of the affected population, the greater the circulation of the virus, and therefore the greater the probability that the swab test actually detects that virus rather than others, thus reducing the gap between sensitivity and specificity.
The ISS takes a table that considers the effect of the prevalence on the effectiveness of tampons. The table was published by FIND, an authoritative international organization already seen above; and thus, the data that emerges from the FIND table, accepted and re-proposed by the ISS, has value not only for Italy, but for the whole world. Writes the ISS introducing the Table:
"In the following table, taken from the Rapid diagnostic tests for COVID-19 document, it is shown with a numerical example how the ability to correctly identify positives (PPV column) is related both to the sensitivity and specificity of the test, and to the prevalence of the marker in the target population, exemplified by four cohorts of 1,000 individuals with four different prevalence values: 2%, 5%, 10% and 30%. “
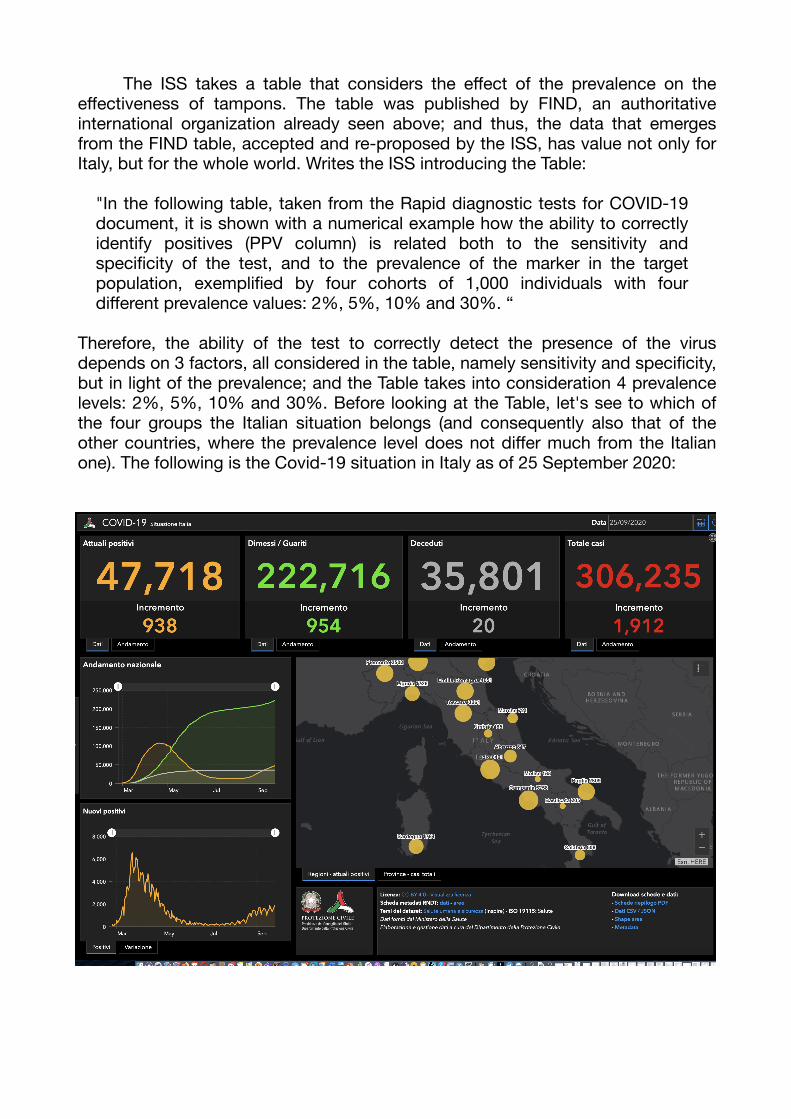
Therefore, the ability of the test to correctly detect the presence of the virus depends on 3 factors, all considered in the table, namely sensitivity and specificity, but in light of the prevalence; and the Table takes into consideration 4 prevalence levels: 2%, 5%, 10% and 30%. Before looking at the Table, let's see to which of the four groups the Italian situation belongs (and consequently also that of the other countries, where the prevalence level does not differ much from the Italian one). The following is the Covid-19 situation in Italy as of 25 September 2020:

The number to consider is that of the current positives, that is 47,718, which represents just 0.079% of the Italian population, very far even from the lowest level of 2%. Even if we wanted to exaggerate, and take into consideration the total number of cases that have occurred from the beginning to today, we would have that the number of 306,235 is equal to 0.5% of the Italian population. Using this second number is statistically completely wrong, but I did it to underline that not even taking all the official Covid-19 cases (i.e. WITH Covid and not FOR Covid) from the beginning of the pseudo-pandemic to date, would not even reach nowhere near 2% of the population. Let's finally see the Table:
Therefore, the ability of the test to correctly detect the presence of the virus depends on 3 factors, all considered in the table, namely sensitivity and specificity, but in light of the prevalence. The decisive number is the PPV, which is the ability of the test to actually detect the virus. The numbers that interest us are those related to the 2% level, which in the case of Italy is actually much lower, at around 0.1%. This means that the numbers in this table are even optimistic! Meanwhile, here are considered 3 models of swab tests: high performance, medium performance, and low performance. At the 2% prevalence level, these are the true and false positive levels given by the swabs:

Level True positive False positives
2% High performance 49.2% 50.8%
2% Average performance 14.8% 85.2%
2% Low performance 9.3% 90.7%
So, at best, swab tests give 50% false positives, and at worst they give nearly 91% false positives! On average, we can say that swabs give 85.2% of false positives! In all cases, the Istituto Superiore di Sanità certifies that the swab tests are completely unreliable! Will there be any politicians who want to hear this official truth, which could not be more official?
What is the most likely number between 50% and 91% of false positives? Having previously seen the unreliability of the gene sequences of the main swab tests, and above all the fact that they all use more than 35 PCR cycles, and therefore that the swabs can only be low-performing, the most realistic number is 91% of false positive! But even if they were somewhere in between, for example the result of the "average performance" of 85%, things would not change. Swab tests are completely unreliable, and this is confirmed by the Italian Istituto Superiore di Sanità, but most importantly on the ground of the work done by the internationally authoritative organization FIND : what else do you need to stop the tragic farce of swab tests and asymptomatic positives?
And here we come to the last consideration, even if it would not even be necessary. The numbers we have seen refer to the prevalence level of 2%; but in Italy today the level is 0.1%. An adequate statistical adjustment would require ad hoc work. But if we consider that in the passage from 30% to 2% prevalence (15 times reduction) the values are reduced from 95% to 49.3%, by about half (50%); we can reasonably estimate that going from 2% to 0.1% (20 times reduction), the values undergo at least the same halving. This means that the range of false positives goes from 50.3 to 75% at best; and about 90.7 to 95% at worst. An even more compelling reason to scream loudly: STOP THE SCAM OF THIS FALSE PANDEMIC, which generates a prevalence of just 0.1% (while the model itself speak of prevalence up to 30%!); and which is based on swab tests which produce up to 95% of false positives!