covid-19 at oxford university hospitals: sustaining morale
TRANSCRIPT

Copyright © University of Oxford 2020. Professor Karthik Ramanna and Senior Case Writer Sarah McAra prepared this case and are grateful to Professor Meghana Pandit for her comments. Certain details of the case may have been fictionalised to serve pedagogical purposes. Cases are developed solely as the basis for class discussion and are not intended to serve as endorsements, sources of primary data, or illustrations of effective or ineffective management. No part of this publication may be reproduced or transmitted in any form or by any means, whether by photocopying or storing in any medium by electronic means or otherwise, except as permitted by law, without permission in writing from the University of Oxford.
COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis 14 May 2020 – REV: 10 June 2020 17 March 2020, 7:30 am: Professor Meghana Pandit, Chief Medical Officer (CMO) of Oxford University Hospitals (OUH), was already in her office at the heart of John Radcliffe Hospital (JR Hospital). It had been 48 days since the first cases of COVID-19 were detected in the UK, and the hospital was caring for several patients who had become infected with the disease. COVID-19 was caused by the novel coronavirus that had spread around the world at dizzying speeds, crippling heath care systems worldwide. OUH was in the early stage of the pandemic; the peak of the crisis was expected to hit Oxford in two- to four-weeks’ time. Pandit and the management team had to prepare OUH’s four hospital facilities and 12,000-person workforce, which served 2.5 million people in the Oxfordshire area1, to manage the anticipated peak of patients who would require urgent and intensive care on a scale never seen before. Under guidance from the National Health Service (NHS), OUH had cancelled routine appointments but was continuing to provide elective (non-urgent) and day-case surgeries for patients who did not need to spend the night at the hospital. This was to ensure health care workers could continue to treat patients before the COVID-19 crisis strained hospital capacity, and to prevent an unmanageable backlog of appointments after the crisis.2 But that morning, Pandit received an email from a concerned surgeon: health care workers did not want to continue certain elective surgical procedures. They believed that they did not have sufficient personal protective equipment (PPE), and thus felt at risk of exposure to the highly contagious virus. Indeed, hospitals around the UK were experiencing shortages of PPE, the vital safety gear that provided protection against viruses that were spread via droplets and aerosols.3 As the CMO, Pandit was required to implement the guidance of the NHS, but she also had to maintain the safety – and morale – of her frontline health care workers. Pandit had to act within the context of constantly changing government guidance, which could hamper quick and informed decision making. Just five days earlier, on 12 March, the UK officially moved from the ‘contain’ phase of its coronavirus strategy, aimed at preventing the spread of the disease by isolating cases, to the ‘delay’ phase, aimed at slowing the now inevitable spread of the disease to ease pressure on the health care system. New guidance came out rapidly, changing by the day. The previous night Prime Minister Boris Johnson had announced strict social distancing and self-isolation measures for at-risk groups, which included those aged 70 and over, those with underlying health conditions and those who were pregnant. The NHS had yet to issue guidance about if and how these applied to health care workers. Full adherence would significantly deplete the OUH’s already strained workforce. The pandemica On 31 December 2019, Chinese authorities publicly announced that they were investigating several cases of pneumonia of unknown cause in Wuhan City in the Hubei Province of China. By 7 January 2020, the cause was identified as a new coronavirus, a type of virus that originated in animals and jumped to humans. Days later, authorities had traced the outbreak
a Information about the pandemic and COVID-19 reflects the data available as of 17 March 2020.
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
2
back to a seafood market in Wuhan City.4 The virus became known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which caused the coronavirus disease (COVID-19).5 It was a novel virus, meaning that no one had immunity and no vaccine existed.
The virus spread quickly throughout Wuhan, and hospitals became overrun with COVID-19 patients.6 The Chinese government took a number of steps to curb transmission, suspending travel in Wuhan, implementing stay-at-home policies and closing public venues such as schools and factories. But the virus also started to spread outside of Wuhan as millions of people travelled before the lockdown. By the end of January, cases were confirmed in the US, France, Australia, South Korea, India, Russia, Spain, the UK and more.7 As global transmission continued, on 11 March, the World Health Organization (WHO) declared COVID-19 a pandemic. In the two weeks prior, the number of cases outside of China had increased 13-fold: there were 118,000 cases in 114 countries, and more than 4,000 people had died. The WHO cited concerns over ‘the alarming levels of spread and severity’ of COVID-19.8
COVID-19
Scientists worked rapidly to understand SARS-CoV-2. Most transmission seemed to occur when an infected person had symptoms. However, early evidence suggested that pre-symptomatic contagion was also possible, where a carrier spread the virus before showing symptoms. This was due to the long incubation period: on average, people became sick 5 to 6 days after infection, though the incubation period ranged from 1 to 14 days.9 The virus was also highly transmissible, as measured by the reproduction number (R0, pronounced ‘R naught’): the average number of cases that one infected person caused while infectious. The WHO estimated that the R0 was between 2 and 2.5, meaning that one infected person caused, on average, two or more other infections.10 This was higher than influenza and severe acute respiratory syndrome (SARS).11
COVID-19 could either be asymptomatic or cause respiratory illness with mild to critical symptoms, and even death. The most common symptoms were a fever, dry cough and fatigue. Early reports from China found that 80% of cases were mild to moderate, 14% were severe, and 6% were critical.12 Most people with mild cases did not require hospital care. Patients with more severe cases required hospital intervention and often experienced severe pneumonia. The majority of patients with critical cases required mechanical ventilation. The WHO advised that all hospitalised patients be monitored frequently as conditions could deteriorate quickly.13 The elderly and those with underlying health conditions, such as hypertension or cardiovascular disease, were at highest risk of severe illness and death. The WHO estimated a crude fatality rate (reported deaths divided by reported cases) of 3-4%.14
As of March 2020, there was no vaccine for SARS-CoV-2. Experts estimated that it would be at least a year until a vaccine was available.15 Vaccine development for coronaviruses was particularly challenging, with prior research indicating the potential for serious side effects.16 Furthermore, there was no proven treatment for COVID-19, though several drugs were being trialled, many of which had been developed for other health conditions.17
Experts turned to lessons from prior pandemics to inform responses to COVID-19, though there remained several key differences that limited direct comparisons. (See Exhibit 1a for other major viral outbreaks in the UK and Exhibit 1b for more information on pandemic responses.)
Influenza
COVID-19 was frequently compared to influenza since both presented with respiratory symptoms and were spread in similar ways.18 There were different types of influenza, from seasonal flu to H1N1, the strain that caused the deadly 1918 influenza pandemic and the 2009 swine flu outbreak. Despite sharing similar symptoms, COVID-19 had a higher proportion of severe cases and a higher mortality rate than seasonal influenza.19 A January 2020 study from
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
3
Wuhan found that patients with severe cases of COVID-19 were hospitalised for an average of 11 days, compared to 5 to 6 days for severe flu cases.20 Care for COVID-19 patients was also more intensive, often requiring ‘two to three medical staff at one time, all in protective gear, for hours and hours’, according to a WHO senior advisor.21 Finally, influenza could be managed through vaccines and antivirals, neither of which were available for COVID-19. SARS SARS-CoV-2 was also similar to the SARS virus that spread in 2002-03. First identified in southern China, SARS reached 26 countries, infected more than 8,000 people, and caused around 800 deaths for a fatality rate of 10%.22 There was no vaccine for SARS at the time, but the outbreak was contained within eight months23 due to a number of public health interventions and international cooperation.24 (Refer to Exhibit 1b for more information.) SARS and SARS-CoV-2 were both coronaviruses and were genetically similar.25 For both, the median time between infection and showing symptoms was around 5 days.26 However, SARS was most contagious when patients had symptoms; it did not appear to spread when an individual had no or mild symptoms. This meant that isolation and contact tracing efforts were effective since it was evident when a patient was highly contagious.27 SARS therefore largely spread within hospitals, whereas COVID-19 was spreading both in hospitals and the wider community.28 Health care in the UK: The NHS The Department of Health and Social Care (DHSC) was responsible for health care in the UK, with the tax-funded NHS providing the majority of health services.29 The NHS was established in 1948 offering free, universal health care, key principles that underpinned the complex system that evolved in the following decades. By 2018, the NHS served an average of a million people a day and had a workforce of 1.7 million, making it one of the world’s largest employers.30 In England, the health service was run by NHS England, a part of the DHSC. NHS England relied on a commissioning system with separate purchasers and providers: commissioners purchased health care services from providers who competed in an internal marketplace. Most commissioners were local bodies that determined what health services their communities needed. Providers were largely NHS trusts and foundation trustsb, such as OUH; these were self-governing bodies that offered hospital and community health care services. There were over 200 trusts across England.31 To ensure they met NHS standards, trusts were regulated by the Care Quality Commission (CQC), which inspected and monitored the quality of health and social care, and NHS Improvement, which regulated the finances, performance and governance of the trusts.32 In 2018/19, NHS England allocated £84 billion to local commissioning and £30 billion to national services and central functions.33 A strained system The NHS had come under significant financial strain in recent years. While the NHS had been ringfenced from national austerity measures introduced in 2010, its real-term funding grew less than 1% a year on average from 2009 to 2018, compared to a historic average annual growth of 3.7%.34 Spending on social care fell as well, adding pressure to the health care system as community support diminished.35 Funding did not keep up with demand, and the total NHS provider deficit grew from £791 million in 2016/17 to £991 million in 2017/18.36 The funding slow down came at a time of rising health care needs, with demand for hospital services growing faster than the population. The share of older people in the population was increasing, as was the prevalence of long-term, complex health issues.37 In 2018 and 2019, the Conservative government promised to increase health and social care spending.38
b Foundation trusts had more independence from government than traditional trusts, but still had to comply with NHS regulations. However, differences between traditional trusts and foundation trusts had diminished over the years.
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
4
Compared to health care systems in similar OECD countries, the NHS had fewer physical and human resources.39 For instance, the UK had fewer hospital beds per 1,000 than similar countries.40 The number of beds had been declining over time as policy shifted to prioritise day surgeries and community care (e.g., support outside of the hospital). However, this had contributed to capacity challenges. From July to September 2019, 126 out of 170 hospital trusts had bed occupancy rates above 85%, the level experts generally considered to be safe.41 Occupancy rates were expected to be even higher in the winter months that followed.42 The NHS also had fewer doctors and nurses than comparable counties. In 2018, the UK had 2.9 doctors per 1,000 people, compared to the OECD average of 3.5 (2017), and 7.8 nurses per 1,000 people, below the OECD average of 8.8.43 Nurse recruitment and retention had been a particular area of concern, especially with the number of foreign nurses falling since the UK started to plan its exit from the EU in 2016. In 2018, 11% of nursing positions were vacant.44 The strains on the system took a toll on morale among health care workers. A 2016 study found that NHS general practitioners were the most stressed among 11 developed countries, due to ‘relentless workloads, endless bureaucracy and the shortest amount of time spent with patients’.45 A 2019 survey of NHS staff found that 40% had felt unwell in the prior year due to work stress, while nearly 30% said that they ‘often think about leaving their organisation’.46 In 2019, the NHS had failed to meet a number of key targets. Data released in December 2019 showed that waiting times for accident and emergency (A&E) services hit record highs, as did the number of people on waiting lists for treatment, including cancer services.47 ‘These figures show an NHS on its knees and it is no wonder that most leaders predict that this winter will be the worst on record,’ said an NHS executive. ‘More and more patients are turning up at emergency departments and there is a limit as to how many they can cope with.’48 Oxford University Hospitals The OUH NHS Foundation Trust, a teaching hospital in Oxfordshire, had a renowned reputation for world-leading research and clinical excellence.49 It was among the largest hospital trusts in the country, with 60 wards and 48 operating theatres across four locations. Its services included A&E; trauma and orthopaedics; maternity, obstetrics and gynaecology; new-born care; general and specialist surgery; cardiac services; critical care; cancer; renal and transplant; neurosurgery and maxillofacial surgery; and infectious diseases and blood disorders. OUH had 1,185 beds, with 64 for critical care. OUH managed more than a million patient contracts a year, including patients who came from other parts of the UK to access specialist services.50 Its admissions in 2018/19 included 101,100 emergency and unplanned patients, 20,300 elective inpatients, and 84,900 day-case patients.51 OUH had a workforce of 11,800, which included 3,800 nurses and midwives, 1,800 doctors and 1,600 health care support workers.52 However, the trust had been struggling with staffing shortages. Reflecting nationwide trends, maintaining the nurse workforce had been a particular challenge. OUH had a nurse vacancy rate of 14.1% in 2018/19.53 A teaching hospital, OUH was also home to 825 trainee doctors and 448 educational supervisors.54 The trust worked in partnership with The Oxford Deanery, the local office of Health Education England that coordinated training for health care professionals. In addition, there were thousands of academic researchers who worked with OUH clinicians.55 OUH was a member of The Shelford Group, England’s 10 largest teaching and research NHS hospital trusts, which were all of similar size and complexity. The Shelford Group reportedly had significant influence in making policy recommendations to national NHS teams. While OUH generated a £13 million surplus in 2018/19 through one-off items such as the sale of land, funding remained a challenge.56 As noted in the OUH annual report, ‘Funding growth continues to be inadequate to meet rising demand for services, to recruit and retain the staff
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
5
needed to deliver care within national waiting time standards and to meet continuing expectations that services’ quality and responsiveness will improve each year.’57 OUH had made some notable service improvements in recent years. For instance, in 2019 only 8 patients waited more than 52 weeks for an elective surgery, compared to 203 patients in 2018.58 However, OUH had also missed several performance targets, including A&E wait times. Its emergency, cancer and elective care services had been particularly under pressure.59 OUH was led by an experienced team of medical and management professionals (see Exhibit 2 for an organisational chart). The team was headed by CEO Dr Bruno L Holthof, who joined OUH in 2015 after serving as CEO of Antwerp Hospital Network for more than a decade. Chief Operating Officer (COO) Sara Randall, who had trained as a nurse before moving into operational management, oversaw OUH’s four clinical services divisions. (Refer to Exhibit 2.) Each division was responsible for the day-to-day management and provision of clinical services, ensuring they aligned with OUH’s policies and procedures. Randall worked closely with CMO Pandit and Chief Nursing Officer (CNO) Sam Foster to oversee clinical management, including quality and safety, operational performance, finances and workforce management.60 Pandit and Foster managed OUH’s teams of doctors and nurses, respectively. Professor Meghana Pandit at OUH Pandit had started her medical career in obstetrics and gynaecology in Oxford, training at JR Hospital. After becoming a consultant (i.e., senior doctor), she then moved into various clinical management positions. Her interest in management prompted her to complete an MBA from Oxford Brookes University. She became the CMO of University Hospitals Coventry and Warwickshire NHS Trust from 2012 to 2018, and deputy chief executive from 2014 to 2018. There, she oversaw 500 doctors as the Responsible Officer, the senior doctor who ensured all doctors met national standards. She then joined OUH as CMO in January 2019, with responsibilities including clinical safety and outcomes, medical education, and research and development. She was Responsible Officer for over 1,000 doctors. At OUH, Pandit made improving the safety culture a priority. While OUH provided high quality care and was a world-renowned teaching hospital, it still experienced a number of safety challenges. Following an inspection in 2018, the CQC had downgraded OUH from ‘good’ to ‘requires improvement’ due to shortfalls in safety and leadership.61 The CQC found that some surgical areas did not use incident reporting effectively, and that some services did not always have sufficient nursing staff.62 Furthermore, according to the CQC’s report, ‘[m]anagers across the trust did not always promote a positive culture that supported and valued staff’.63 OUH had also experienced several serious safety incidents, including eight ‘never events’ in 2017/18.64 A never event was a serious, wholly-avoidable patient incident, such as conducting a surgical procedure on the wrong limb or leaving behind a surgical object.65 Pandit observed that clinicians thought they would be blamed for mistakes and therefore were hesitant to report errors. This attitude had been prevalent for many years. In 2015, an NHS survey found that only around half of OUH staff believed that the hospital treated staff involved with errors or incidents fairly.66 (See Exhibit 3 for survey results over time.) Research from the British Medical Association found that a ‘culture of fear and blame’ was endemic across the NHS.67 Pandit believed these safety challenges were tied to the bureaucratic and risk-averse culture that had long been ingrained at the hospital. A 2010 study of the OUH organisation concluded that its culture was highly hierarchical.68 The study found that OUH’s academic physicians and scientists were more than twice as likely to agree that the hospital was ‘very formalised and structured’ than ‘very dynamic and entrepreneurial’, and that staff members’ actions were more likely to be governed by bureaucracy than by a willingness to take risks.69 OUH doctors also reported a sense of competition and individualism; as one respondent said, ‘We need to balance “being first” with maintaining integrity and being people-centric’.70
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
6
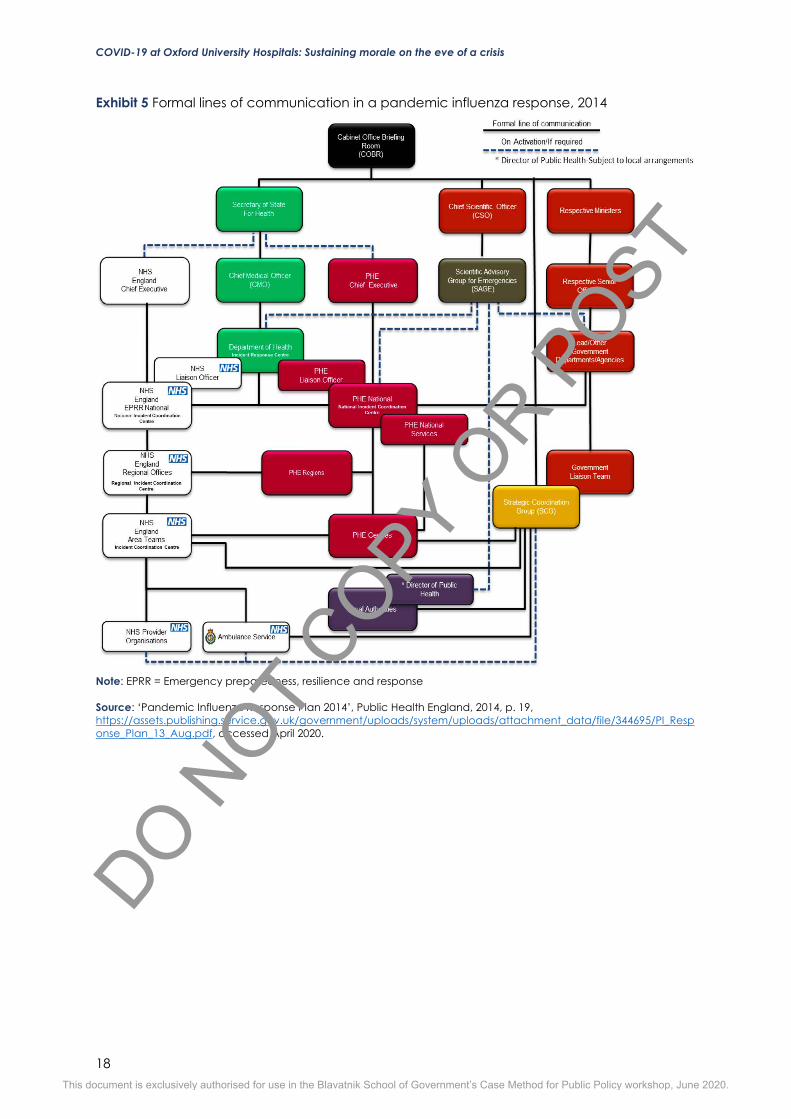
Pandit wanted to usher in a culture based on trust and communication, where clinicians could learn from mistakes. However, building a new culture of trust could be a slow and difficult task, especially when operating in the bureaucratic, target-focused environment of the NHS.71 She implemented a number of safety initiatives to help foster a new culture. In January 2019, Pandit and the CNO started to send out weekly safety messages to the staff to highlight key issues.72 In March 2019, Pandit piloted a Patient Safety Response (PSR) team. This was a multidisciplinary team of doctors, nurses and managers who met daily to review patient safety incidents from the prior 24 hours deemed to be of moderate severity or above. Such incidents could include an unexpected death, a fall or fracture, or a never event. The team assessed what went wrong and decided how to address each incident. Pandit also introduced safety huddles where clinical workers on a given ward came together each day and answered four questions about the prior 24 hours: (1) What went well? (2) What did not go well? (3) What can we learn from this? (4) What are our plans and risks for today? Prior to the COVID-19 crisis, the huddles were being rolled out ward by ward to ensure buy-in. Results from a 2019 NHS survey found that OUH staff believed the safety culture had improved. (Refer to Exhibit 3.) Nearly 65% of staff thought that the trust treated people involved with errors and incidents fairly.73 While this was a step in the right direction, Pandit knew that there was still much to do. But with the arrival of COVID-19, the pace of change had been accelerated – for instance, the huddles had to be more rapidly deployed hospital-wide. ‘Coronavirus: action plan’ The UK confirmed its first case of COVID-19 at the end of January 2020, and the number of cases started to grow rapidly in March. (See Exhibit 4.) As the crisis intensified, the government developed national policies that were cascaded through the health care system. The response was based on the UK’s pandemic influenza preparedness plans.74 (See Exhibit 5 for lines of communication in a pandemic influenza outbreak.) The national response was coordinated by the Cabinet Office Briefing Room (COBRA), the crisis response team led by Prime Minister Johnson and Secretary of State for Health and Social Care Matt Hancock.75 COBRA was made up of relevant government departmental leaders and received advice from the UK’s chief medical officers as well as the Science Advisory Group for Emergencies (SAGE), a team of subject-area experts.76 COBRA weighed up scientific advice against other concerns such as economics, security, politics and diplomacy.77 The DHSC was the main government agency responsible for responding to the outbreak, working closely with Public Health England (PHE) and the NHS. Established in 2013, PHE was an executive agency that brought together a number of specialists to provide research and advice on public health. During a pandemic, PHE was responsible for developing a detailed assessment of the disease and, based on scientific evidence, issuing guidance on appropriate infection control measures, such as when to close schools or to restrict public gatherings.78 NHS England was responsible for the command, control, communication and coordination of health care services in England during a pandemic, adhering to protocols and guidance set out by the DHSC and PHE. An NHS England national response board provided overall direction and advice; there would ‘not be scope for significant regionalisation or localisation except for operational requirements or loss of supplies’.79 A national operations team coordinated the operational and logistical response. Regional and local NHS teams were also established.80 On 3 March, the DHSC released the ‘Coronavirus: action plan’ outlining a phased response to COVID-19: contain, delay, mitigate and research. At the time, the UK was in the contain phase focused on preventing the virus from spreading. This involved detecting cases early and tracing and isolating contacts of those who were infected. But the virus continued to spread quickly, and the UK moved from the contain stage to the delay stage on 12 March. The goal
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
7
was now to slow the spread of the virus to mitigate the impact on the NHS, primarily by delaying the peak of cases until after the winter. Tests would now be prioritised for those at risk of serious illness, namely hospital patients with critical respiratory infections and flu-like symptoms.81 Scientific advice continued to change rapidly. New evidence from the UK, China and Italy suggested that a greater share of COVID-19 patients would need to be treated in intensive care units than originally anticipated.82 Experts at Imperial College London released updated models showing that without intervention, the number of cases in the UK would exceed critical care bed capacity in early April, and that the eventual peak of cases would be 30 times critical care bed capacity. Measures such as social distancing and isolation of the vulnerable would reduce peak demand by two-thirds, though the peak would still be 8 times the capacity of critical care beds.83 Stricter measures would also curtail the number of deaths considerably.84 Based on this advice, Johnson introduced social distancing guidance on 16 March.85 He called on the public to cease all non-essential travel and contact; this meant working from home where possible and avoiding social venues such as pubs and restaurants, though schools were not yet closed. A person with symptoms had to self-isolate at home for seven days, and anyone in the same household as someone with symptoms had to self-isolate for 14 days. Johnson said minimising social contact was ‘particularly important’ for at-risk groups: people over the age of 70, those with underlying health conditions and those who were pregnant.86 Infection prevention & PPE The DHSC and PHE provided guidance on infection prevention and control for hospital settings. The latest guidance as of 13 March included: segregating patients with COVID-19 symptoms from other patients; maintaining proper hand and respiratory hygiene to avoid spreading the disease between patients; and ensuring health workers wore appropriate personal protective equipment (PPE), which entailed donning, removing and disposing of PPE correctly.87 PPE was a vital tool for reducing the spread of highly infectious diseases that were transmitted through droplets or aerosols. PPE made up the largest component of the UK’s national pandemic influenza stockpiles, which were managed by PHE.88 Meanwhile, NHS Supply Chain, which sourced and delivered supplies across the NHS, managed PPE and other resources for typical use. In early March, NHS frontline workers started to warn about shortages of PPE. The Independent reported that some NHS staff could not access PPE, and that some hospitals were expected to run out of PPE within weeks. Indeed, some hospital trusts were already rationing supplies until they could replenish their stocks.89 On 9 March, PHE announced that it would start to release some of the national PPE stockpile ‘in a controlled manner to help ensure the uninterrupted supply to the NHS’.90 NHS Supply Chain started to restrict orders for other protective items in high demand such as hand sanitiser and face visors.91 Health care workers grew frustrated by PHE’s changing advice on protective gear. Initially, PHE had advised health care workers who treated suspected COVID-19 patients to wear full PPE gear: a filtering facepiece respirator (FFP3) mask, a visor, a surgical gown and two pairs of gloves.92 But new guidance issued on 6 March stated that only a regular surgical mask, gloves and a plastic apron were required.93 Some NHS staff found this level of protection ‘totally inadequate’ and believed that the change was primarily driven by availability of supply, not by best practices for protection.94 COVID-19 at OUH Oxfordshire’s first case of COVID-19 was confirmed on 8 February. By 16 March, there were 36 cases.95 (See Exhibit 6.) OUH was a designated surge centre selected to care for COVID-19 patients in the UK.96 The OUH had 64 intensive care beds (with ventilators), but the NHS had asked the trust to prepare 125 intensive care beds for the anticipated peak. This would require
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
8
rapidly acquiring new equipment, rearranging space in the hospital, and allocating and training a sufficient number of staff to operate the equipment and treat ventilated patients. In preparing for the peak, OUH was supported by regional coordination centres and a local-area integrated care system (ICS), which was a partnership between NHS organisations and local councils. These teams provided mutual aid for OUH’s equipment needs and helped with the flow of policies from the national team to the local team. While this was vital support, Pandit noted that the structure could pose some challenges: ‘The various co-ordination centres increase email traffic, ask for completion of spreadsheets within short timescales and can be confusing.’ Moreover, she added, ‘Nobody can tell you how to manage your own organisation with its own culture and history.’97 While there were systems in place for crisis management, the COVID-19 crisis was unlike anything the NHS had seen before. As Pandit explained, ‘All executive directors in the NHS have training to be a “Gold Commander”c who has overall responsibility for responding to an incident, and all NHS organisations have plans for pandemic flu on their shelves. However, this pandemic is completely different because of its global nature, its infectious nature and the level of anxiety about an impending “peak” that was modelled to be on 11 April.’98 Pandit had to make countless decisions in a context of huge uncertainty. ‘We are not trained to manage a health care crisis of this scale,’ she said. ‘Instead, I draw upon my clinical training in obstetrics wherein I was exposed to several crises, though they were not on a mass scale, and on my exposure to major incidents like an overcrowded emergency room or the failure of IT, etc. Management of this crisis requires leadership that is brave, courageous, empathetic and one that communicates well with consistent messaging.’99 A morning in the pandemic100 Pandit arrived at work early on 17 March, the day after Johnson issued the strict new social distancing guidance, though before any lockdown measures had been put in place. She had not yet received any advice from the NHS about how the measures applied to health workers. After first seeing the CEO for a morning check-in on the changing guidance, at 8:00 am Pandit went to her office where her two deputies were preparing for the daily PSR meeting. The deputies were both consultants who split their time between management and medical practice. A nursing executive also phoned in to the meeting from his office. The team reviewed three safety incidents from the prior 24 hours and determined if any action was required. The discussion quickly wrapped up, and in the minutes before the next meeting, the deputies updated Pandit on several ongoing matters, such as how they planned to implement social distancing measures for a large meeting that week. At 8:15 am, Pandit and the deputies were then joined in the office by two of OUH’s infectious disease experts; they wanted to ensure they were all aligned on the strategy and messaging for the upcoming all-staff meeting at 8:30 am. The group identified four areas where they expected staff would want answers: staff testing for COVID-19, annual leave, triage protocols and self-isolation of pregnant staff. Staff testing: Across NHS hospitals, staff were calling for more testing of frontline health care workers. Without tests, some workers without any symptoms had to self-isolate if members of their households were symptomatic. At the same time, some workers without symptoms might not know they were infected and could unknowingly spread the virus to other patients. To date, the NHS had not provided clarity about which staff should be tested and when. Given this lack of information, Pandit asked the team, ‘What are other trusts doing? What about The Shelford Group?’ One of the infectious disease consultants had heard that at least two other trusts were testing staff, but would seek further information on the details. c For major incidents, each NHS organisation implemented a command-and-control structure led by a Gold Commander, who was responsible for the strategic response, a Silver Commander, who determined tactical priorities for securing and allocating resources, and a Bronze Commander, who managed frontline operations.
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
9
Annual leave: The team expected questions about the use of annual leave. Pandit confirmed that if staff had already booked leave for the next couple of weeks, they should use it if desired. OUH would need as many staff available as possible to support the surge expected in April. Triage: Pandit explained that the hospital would move to a single point of entry for triage. However, the NHS had not yet issued guidance about how to make the difficult decisions for prioritising care if demand exceeded hospital capacity.101 Pandit asked, ‘What are the ethical considerations around this?’ She had recently attended a meeting with an Oxford medical ethics expert, but the discussion did not directly apply to OUH’s needs. One of the consultants said that an Italian hospital had published a report on their ethical considerations for triage; he had seen an English translation on Twitter and would track it down to see what they advised. Pregnant staff: Johnson’s announcement the night before had included pregnant women among the high-risk groups who should minimise social contact. But Pandit and the doctors gathered in her office had seen no evidence that pregnant women were at a higher risk of experiencing severe symptoms of COVID-19.102 They were hesitant to implement the advice, but they would have to await NHS’s national guidance on the matter. At 8:30 am, Pandit and the others made their way to the all-staff meeting. The management team had decided to hold the meeting on short notice. Some executives had been hesitant about the idea: they did not want to have staff members together in a confined space, against social distancing guidance. But Pandit felt it was important, and said they would find a way to make it work safely. ‘We must stand up and show them we are leading,’ she said. They held the meeting at one of the lecture theatres at JR Hospital, and staff sat staggered a few seats apart. The meeting was livestreamed into a second lecture theatre with additional space, and online across the other hospitals in the network. A team of executives and infectious disease experts stood at the front of the lecture theatre to lead the meeting. CEO Holthof opened by welcoming the staff, and passed the microphone on to the infectious disease experts. They explained that all COVID-19 patients were confined to the parts of the hospital that had been prepared to manage infectious diseases. However, they expected that they would have to expand to other areas in future. They also acknowledged that some staff had been concerned about using PPE, and emphasised the importance of putting the gear on and taking it off correctly and safely. Next, Pandit explained that they were preparing for the peak to hit in two to four weeks. They were developing plans for how to handle both COVID-19 positive and negative patients, and would create a single point of triage. They were starting to move patients to different wards to make more bed space, she said, and specified which wards would be moved next. The hospital would likely need more capacity when the peak hit, but, as she said, ‘We don’t know how many new critical care beds we will need each night – it could be 1, or it could be 20.’ Pandit passed the microphone to an operations executive, who told the staff that they had cancelled all routine appointments (for non-urgent issues) for the coming two weeks. However, they planned to continue to treat all elective and day cases (for patients who did not need to spend the night at the hospital). A nursing director then spoke about how they were collaborating with other organisations, such as health centres and charities, to help return patients to their homes as quickly and safely as possible to free up hospital beds. Next, an HR executive took the microphone. The people management team was looking into what psychological support they could provide staff, and how they could implement work-from-home measures proportionately and fairly. The executive emphasised the need for management to communicate with staff clearly, and noted how important the team huddles would be to share the latest COVID-19 guidance. They would communicate the changing information using email, phone and cascades through team huddles.
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
10
A finance executive came to the stage next. He was aware that there had been some slow deliveries, and that staff were concerned about getting supplies. They were looking to manage equipment like PPE more centrally. He asked the divisions to agree to a list of their anticipated PPE needs, and then to return their excess PPE to central. A central team would then reallocate equipment based on need. Finally, an IT executive spoke about technical changes and support: they were making a number of digital tools available at short notice, and would ensure that all clinical apps could be accessed from personal devices. At 9:00 am, the session was turned over to questions from the staff. The relevant leader took the microphone to respond to each. Q: What should pregnant staff do following the PM’s guidance on self-isolation? Pandit said they were trying to get clarity on the NHS’s advice and would let staff know as soon as possible. Q: What should members of my household do? An infectious disease expert acknowledged that this would be a difficult time for families, especially for those with children. All health care workers and members of their households had to remain vigilant: wash hands frequently, maintain social distancing and ensure that children did not play with friends. Q: Is it safe to continue paediatric surgery? Evidence emerging from China suggests that asymptomatic children are shedding the virus at high rates, and I am concerned for my surgical team. Pandit said that they would look into this and seek advice from the NHS.
Q: Would there be changes to annual leave? The HR executive explained that leave that had already been booked would not be cancelled; using leave was important for resilience and everyone should get a break when they needed it. However, if the crisis intensified, staff might be asked to cancel their annual leave. This would be managed locally by individual teams.
Q: If schools are closed, what will be the effect on health care staff? Will we need to take annual leave to care for our children? This would be a significant challenge, the HR executive acknowledged. They were looking to see if they could keep the hospital’s nursery open to support critical staff, and were considering if they could implement interim policies to help. Q: Will junior doctor rotations (moving specialities) go ahead on 1 April? An operations executive answered that as of that moment, the rotations were planned to proceed. Q: We are concerned about access to PPE. Is there enough supply? The finance executive reiterated that they were working on securing PPE. He asked teams to be clear about their PPE needs for 24-, 48-, and 72-hour periods so that they could allocate equipment effectively.
Q: How do we get more hand sanitiser? A procurement executive came to the stage to respond. Some supplies like hand sanitiser were being rationed and managed by NHS Supply Chain. They planned to centralise stocks as quickly as possible then redistribute as needed. Q: Will there be COVID-19 testing for staff? Pandit explained that there was no guidance on this. ‘We are awaiting advice, and this is a frustration for us,’ she said. Q: Is there a standard letter for cancelling appointments? When should we reschedule appointments? An operations executive said that rescheduling dates would depend on the individual services, and that cancellations would be different in each division. They were also looking to see if some appointments could be done remotely. Q: There is anxiety around having access to PPE and adequate fit testing (ensuring the PPE was worn properly and securely). What support is in place? An infectious disease expert explained that there was indeed a requirement that fit testing be done by an accredited professional, but acknowledged that there was a limited number of people who could do this at the
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
11
moment. A video was in development to provide guidance on the proper fitting of PPE, and they were assessing if this would be acceptable. She also said that some other trusts were implementing ‘fit checks’ instead, where employees checked each other’s gear. She then went over some of the basic tips for ensuring PPE was on properly. During the Q&A, a member of the audience also wanted to highlight the positive developments that were happening at the hospital. He recounted that the day before, they had decided to move a certain ward at 4:10 pm, and by 6:00 pm all of the changes were completed. He thanked all of the staff for their hard work, and everyone warmly applauded. At the end of the Q&A, CEO Holthof took up the microphone to conclude. They would move away from in-person meetings to more emails and person-to-person chains. Answers were changing every day, and they would communicate new information as quickly as possible. It would be a stress test of the cascade system and team huddles. The meeting concluded at 9:30 am, and Pandit returned to her office. A senior doctor stopped her along the way, raising a question about the guidance on pregnant women self-isolating. He and Pandit were equally concerned about the impact this would have on the workforce, and she assured him that she would seek clarity. Back in her office, Pandit quickly ran through her emails; she received at least 50 messages during the all-staff. Then at 9:45 am, she and an operations executive headed to a meeting at the nearby Manor Hospital (Manor), a private hospital managed by the Nuffield Trust charity. This was the first time Pandit had ever worked with the private hospital. Pandit opened the meeting with one of Manor’s operations leaders: ‘Does Manor have any capacity to support our cardiovascular surgeries?’ OUH could move its theatre crews to Manor to perform the surgeries, so as not to rely on Manor staff. OUH would ensure that these staff all had the proper approvals and references necessary to work in private hospitals. Pandit also asked how else Manor could support them – with supplies? with other services? Manor likely could not help with supplies, but there was potential to support other clinical services, pending approval from Nuffield Trust. Pandit did not yet want to hash out the details; Manor would seek approval from the Nuffield Trust, then reach out to the OUH operations team to go over specifics. Pandit returned to her office by 10:30 am. She had a few minutes to review emails – and to get a much-needed cup of coffee – before her next meeting. She needed to now shift her headspace from crisis management to people management: she next had to conduct a difficult disciplinary meeting. Pandit’s colleagues came into the office a few minutes before the 11:00 am meeting to align and strategise. The disciplinary meeting wrapped up at 11:30 am, and Pandit and one of her deputies remained in the office to finalise the disciplinary documents. Pandit also returned to her emails – another 50 by now – as they discussed some of the technical challenges they had faced in bringing meetings online: the video programme had been crashing, but they were not sure if it was the software’s systems or the hospital’s servers. An executive then appeared at the office with an urgent update. One of the divisions wanted to cancel nearly all children’s surgical procedures: the doctors and nurses believed they required full PPE gear, and felt too exposed without it. However, NHS guidance stipulated that full PPE was not required. Pandit asked, ‘What level of PPE do they need? Are the regular masks and surgical gowns not enough?’ She said she would find out more information about the PPE supply and assess what to do. ‘That is one of the issues with communications at the moment,’ said Pandit. ‘You hear that there is no PPE and it spreads like wildfire.’ Shortly after, Pandit opened an email from a concerned surgeon. After the all-staff meeting, wrote the surgeon, he was not reassured about staff protection. He wrote that he did not think elective surgeries and day patient cases should proceed as it put doctors at risk if they did not
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
12
have proper protection. Pandit was in a difficult position: the national NHS team mandated that these surgeries proceed, and she was responsible for ensuring that OUH complied with NHS standards. However, her doctors did not feel safe performing them. At some point did she have to shut off such dialogue from her staff and mandate that the doctors comply? But Pandit did not have time to respond right away. She had to leave for her next meeting at 11:50 am with a leader from the medical education team to discuss plans for junior doctors. As Pandit made her way down the hall to the meeting, several people congratulated her on the successful staff meeting that morning. In the hours since the all-staff meeting, the Oxford Deanery and Health Education England issued new guidance on junior doctor rotations: they would not be proceeding on 1 April, unless local clinical needs required it.103 Pandit launched into the meeting to discuss: ‘We need to determine what our junior doctors need. They need clarity of placements, clarity around movement to other wards, reassurance on PPE, and clarity on assessments.’ They then discussed which of these were junior doctor-specific issues for the medical education team to address, such as assessments, and which were general staff issues, such as PPE. They identified which groups of junior doctors needed immediate answers, since some were on different schedules, and considered plans to quickly but safely onboard junior doctors to new wards if they had to move. It was important to continue to train and assess junior doctors so that they did not cut off the supply of clinicians. However, it was also crucial to protect the education supervisors’ time and wellbeing. They were looking at potentially using video conferencing and shortened meetings with supervisors. Additionally, the medical education executive emphasised the importance of supporting junior doctors during this difficult time: they needed to be able to decompress, build resilience and maintain physical health. This could not be mandated from the top down, but there were ways to create spaces within the hospital setting where junior doctors – and other doctors – could rest and recuperate. Pandit returned to her office, grabbing a quick lunch to eat while she reviewed her emails. One of her deputies came to the office to check in on some ongoing activities. They also discussed options for building out the workforce: they were looking to recruit military doctors, research doctors and nurses, and medical students who were graduating early. Managing a crisis: decision by decision Pandit finished her lunch and prepared for an executive meeting at 1:00 pm. In the five hours since she arrived at work, she had needed to make numerous decisions amidst changing information. She and her team had received new guidance from the Oxford Deanery on junior doctor training, and were still awaiting guidance from the NHS about how to implement Johnson’s new social distancing measures. And there were some areas where they had no national guidance, including staff testing and ethical guidelines for triage. Each day of the crisis was filled with new and pressing decisions. Of particular urgency today was to determine how to respond to her concerned surgeons who did not want to perform elective procedures without full PPE. Should she simply order the doctors and nurses to do their jobs? Would that hamper morale when it was needed most? Where could she turn to for additional information on how to approach the situation? And how should she communicate the decision to her staff?
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST
COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
13
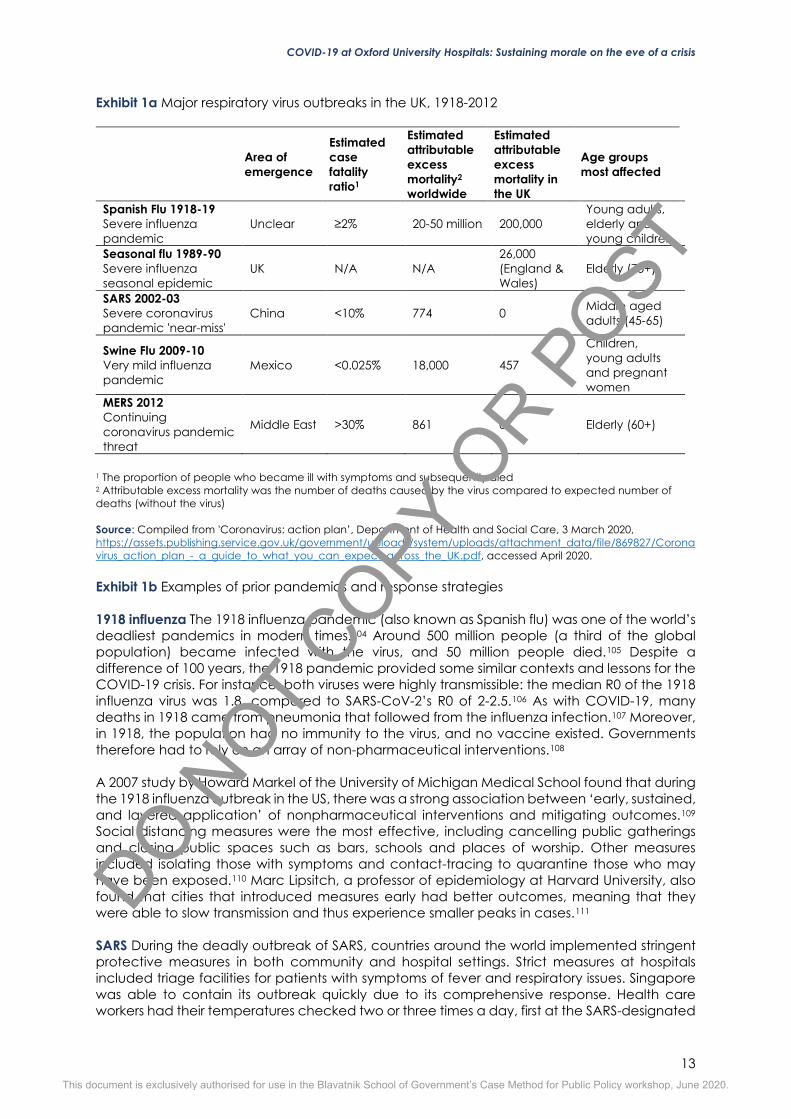
Exhibit 1a Major respiratory virus outbreaks in the UK, 1918-2012
Area of emergence
Estimated case fatality ratio1
Estimated attributable excess mortality2 worldwide
Estimated attributable excess mortality in the UK
Age groups most affected
Spanish Flu 1918-19 Severe influenza pandemic
Unclear ≥2% 20-50 million 200,000 Young adults, elderly and young children
Seasonal flu 1989-90 Severe influenza seasonal epidemic
UK N/A N/A 26,000 (England & Wales)
Elderly (75+)
SARS 2002-03 Severe coronavirus pandemic 'near-miss'
China <10% 774 0 Middle aged adults (45-65)
Swine Flu 2009-10 Very mild influenza pandemic
Mexico <0.025% 18,000 457
Children, young adults and pregnant women
MERS 2012 Continuing coronavirus pandemic threat
Middle East >30% 861 0 Elderly (60+)
1 The proportion of people who became ill with symptoms and subsequently died 2 Attributable excess mortality was the number of deaths caused by the virus compared to expected number of deaths (without the virus) Source: Compiled from 'Coronavirus: action plan’, Department of Health and Social Care, 3 March 2020, https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/869827/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf, accessed April 2020. Exhibit 1b Examples of prior pandemics and response strategies 1918 influenza The 1918 influenza pandemic (also known as Spanish flu) was one of the world’s deadliest pandemics in modern times.104 Around 500 million people (a third of the global population) became infected with the virus, and 50 million people died.105 Despite a difference of 100 years, the 1918 pandemic provided some similar contexts and lessons for the COVID-19 crisis. For instance, both viruses were highly transmissible: the median R0 of the 1918 influenza virus was 1.8, compared to SARS-CoV-2’s R0 of 2-2.5.106 As with COVID-19, many deaths in 1918 came from pneumonia that followed from the influenza infection.107 Moreover, in 1918, the population had no immunity to the virus, and no vaccine existed. Governments therefore had to rely on an array of non-pharmaceutical interventions.108 A 2007 study by Howard Markel of the University of Michigan Medical School found that during the 1918 influenza outbreak in the US, there was a strong association between ‘early, sustained, and layered application’ of nonpharmaceutical interventions and mitigating outcomes.109 Social distancing measures were the most effective, including cancelling public gatherings and closing public spaces such as bars, schools and places of worship. Other measures included isolating those with symptoms and contact-tracing to quarantine those who may have been exposed.110 Marc Lipsitch, a professor of epidemiology at Harvard University, also found that cities that introduced measures early had better outcomes, meaning that they were able to slow transmission and thus experience smaller peaks in cases.111 SARS During the deadly outbreak of SARS, countries around the world implemented stringent protective measures in both community and hospital settings. Strict measures at hospitals included triage facilities for patients with symptoms of fever and respiratory issues. Singapore was able to contain its outbreak quickly due to its comprehensive response. Health care workers had their temperatures checked two or three times a day, first at the SARS-designated
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
14
hospital, then at all health care facilities, as mandated by the Ministry of Health. These measures helped to detect and isolate cases early.112 The Ministry of Health also mandated the temperature screening of children in schools as well as in-bound passengers at airports. While testing in these community contexts ultimately did not identify SARS patients, they helped assure the public that proper protective measures were in place.113 A 2006 review of Singapore’s response found that strong ‘command, control and coordination systems’ were crucial in responding to the outbreak, especially as information changed rapidly and had to be communicated and implemented throughout the health care system.114 In Toronto, which experienced the largest SARS outbreak in North America, the public health body implemented early identification and contact-tracing measures. The province’s Ministry of Health banned visitors (excluding on compassionate grounds) and nonessential staff from the hospitals and ceased outpatient and elective inpatient services.115 Hospitals were required to screen all patients, staff and visitors for SARS symptoms, and health care workers had to wear protective gear (gloves, gowns, eye protection, respirators) when treating all patients.116 (However, this constant use of the respirators and protective equipment ‘was stressful for health care workers’.117) The province’s public health body also implemented ‘work quarantine’ measures where quarantined health care workers could continue to work under strict infection-control precautions but were required to isolate themselves from personal contacts and to avoid public transit.118,119 This was meant ‘to prevent a shortage of essential health care staff.’120
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST
COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
15
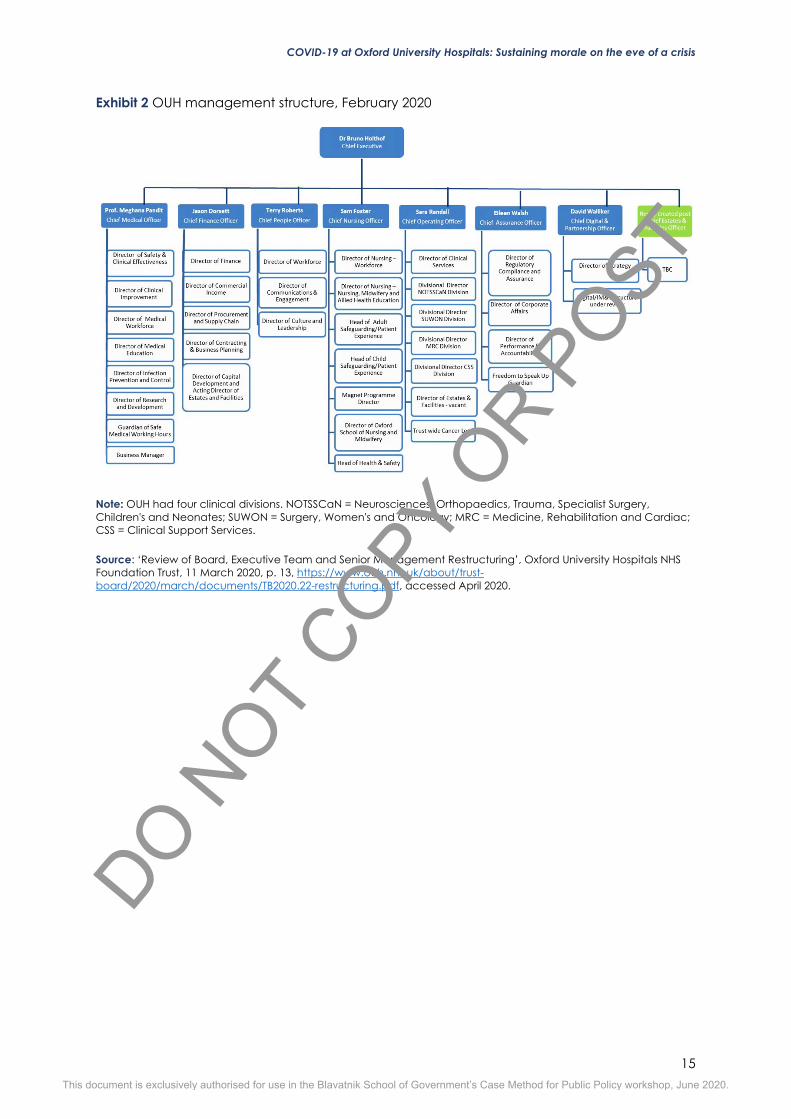
Exhibit 2 OUH management structure, February 2020
Note: OUH had four clinical divisions. NOTSSCaN = Neurosciences, Orthopaedics, Trauma, Specialist Surgery, Children's and Neonates; SUWON = Surgery, Women's and Oncology; MRC = Medicine, Rehabilitation and Cardiac; CSS = Clinical Support Services. Source: ‘Review of Board, Executive Team and Senior Management Restructuring’, Oxford University Hospitals NHS Foundation Trust, 11 March 2020, p. 13, https://www.ouh.nhs.uk/about/trust-board/2020/march/documents/TB2020.22-restructuring.pdf, accessed April 2020.
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST
COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
16
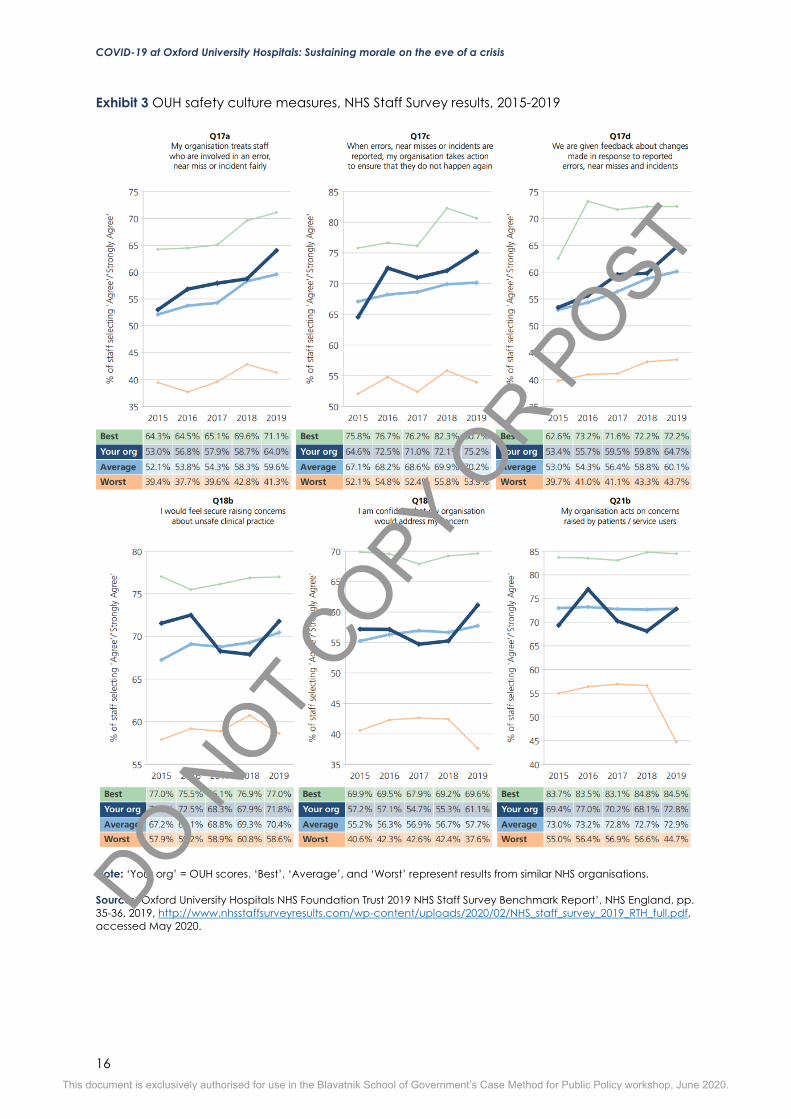
Exhibit 3 OUH safety culture measures, NHS Staff Survey results, 2015-2019
Note: ‘Your org’ = OUH scores. ‘Best’, ‘Average’, and ‘Worst’ represent results from similar NHS organisations. Source: ‘Oxford University Hospitals NHS Foundation Trust 2019 NHS Staff Survey Benchmark Report’, NHS England, pp. 35-36, 2019, http://www.nhsstaffsurveyresults.com/wp-content/uploads/2020/02/NHS_staff_survey_2019_RTH_full.pdf, accessed May 2020.
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST
COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
17
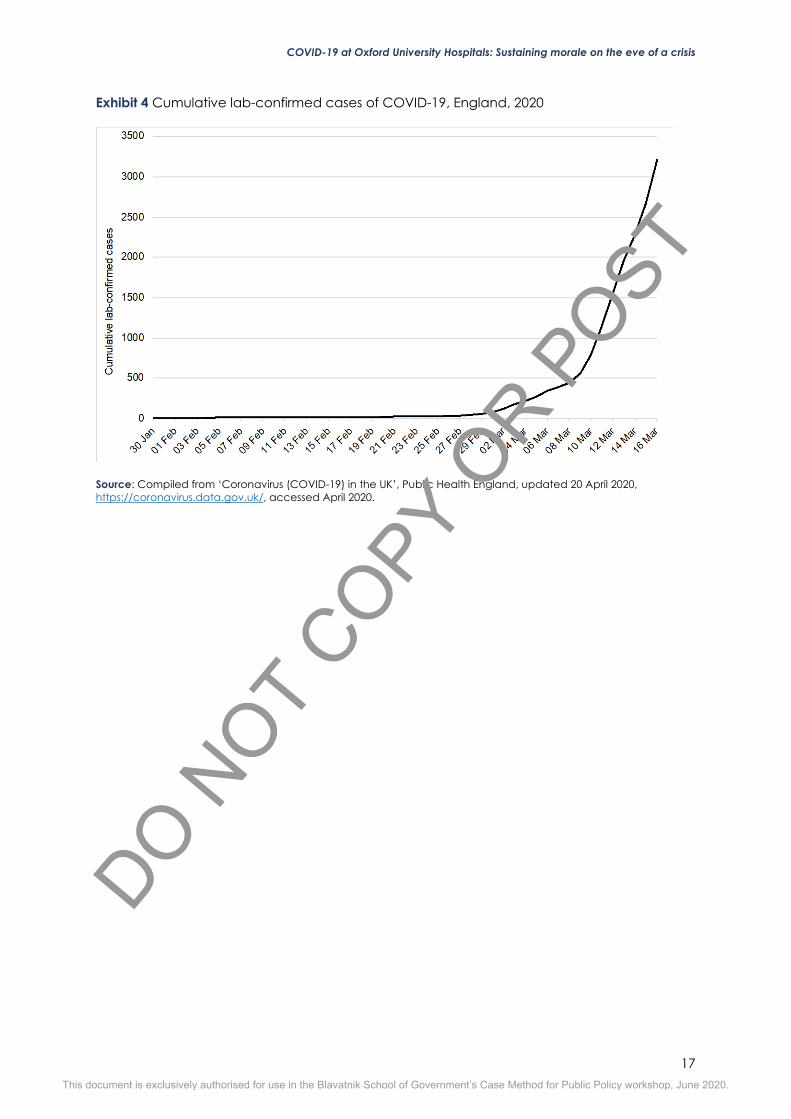
Exhibit 4 Cumulative lab-confirmed cases of COVID-19, England, 2020
Source: Compiled from ‘Coronavirus (COVID-19) in the UK’, Public Health England, updated 20 April 2020, https://coronavirus.data.gov.uk/, accessed April 2020.
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST
COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
18
Exhibit 5 Formal lines of communication in a pandemic influenza response, 2014
Note: EPRR = Emergency preparedness, resilience and response
Source: ‘Pandemic Influenza Response Plan 2014’, Public Health England, 2014, p. 19, https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/344695/PI_Response_Plan_13_Aug.pdf, accessed April 2020.
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
19
Exhibit 6 Cumulative lab-confirmed cases of COVID-19, Oxfordshire, 2020
Source: Compiled from ‘Coronavirus (COVID-19) in the UK’, Public Health England, updated 20 April 2020, https://coronavirus.data.gov.uk/, accessed April 2020.
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
20
1 ‘Oxford Health NHS Foundation Trust’, NHS, 23 July 2019, https://www.nhs.uk/Services/Trusts/Overview/DefaultView.aspx?id=2411, accessed April 2020. 2 Sarah Newey, ‘NHS considers cancelling non-emergency surgery to free up resources for coronavirus response’, The Telegraph, 14 March 2020, https://www.telegraph.co.uk/global-health/science-and-disease/nhs-considers-cancelling-non-emergency-surgery-free-resources/, accessed May 2020. 3 Shaun Lintern, ‘Coronavirus: Doctors warn UK hospitals running out of protective equipment for staff’, The Independent, 9 March 2020, https://www.independent.co.uk/news/health/coronavirus-nhs-hospitals-masks-nurses-doctors-a9385131.html, accessed April 2020. 4 ‘Novel Coronavirus (2019-nCoV) Situation Report – 1’, World Health Organization, 21 January 2020, https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200121-sitrep-1-2019-ncov.pdf?sfvrsn=20a99c10_4, accessed March 2020. 5 ‘Naming the coronavirus disease (COVID-19) and the virus that causes it’, World Health Organization, https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it, accessed March 2020. 6 Annelies Wilder-Smith, Calvin J Chiew, and Vernon J Lee, ‘Can we contain the COVID-19 outbreak with the same measures as for SARS?’, The Lancet Infectious Diseases, 5 March 2020, https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30129-8/fulltext, accessed March 2020. 7 ‘Timeline: How the new coronavirus spread’, Al Jazeera, updated 14 April 2020, https://www.aljazeera.com/news/2020/01/timeline-china-coronavirus-spread-200126061554884.html, accessed April 2020. 8 ‘WHO Director-General's opening remarks at the media briefing on COVID-19 - 11 March 2020’, World Health Organization, 11 March 2020, https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020, accessed April 2020. 9 ‘Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19)’, World Health Organization, 16-24 February 2020, p. 12, https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf, accessed March 2020. 10 ‘Coronavirus disease 2019 (COVID-19) Situation Report – 46’, World Health Organization, 6 March 2020, https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200306-sitrep-46-covid-19.pdf?sfvrsn=96b04adf_2, accessed March 2020. 11 Joseph Eisenberg, ‘R0: How scientists quantify the intensity of an outbreak like coronavirus and predict the pandemic’s spread’, The Conversation, 5 February 2020, updated 27 March 2020, https://theconversation.com/r0-how-scientists-quantify-the-intensity-of-an-outbreak-like-coronavirus-and-predict-the-pandemics-spread-130777, accessed March 2020. 12 ‘Report of the WHO-China Joint Mission…’, World Health Organization, p. 12. 13 ‘Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected’, World Health Organization, 13 March 2020, https://www.who.int/docs/default-source/coronaviruse/clinical-management-of-novel-cov.pdf, accessed April 2020. 14 ‘Coronavirus disease 2019 (COVID-19) Situation Report – 46’, World Health Organization. 15 Megan Molteni, ‘Everything You Need to Know About Coronavirus Vaccines’, Wired, 4 March 2020, https://www.wired.com/story/everything-you-need-to-know-about-coronavirus-vaccines/, accessed April 2020. 16 Molteni, ‘Everything You Need to Know About Coronavirus Vaccines’, Wired. 17 Sarah Boseley, ‘Doctors look to HIV and Ebola drugs for coronavirus cure’, The Guardian, 20 February 2020, https://www.theguardian.com/science/2020/feb/20/doctors-hiv-ebola-drugs-coronavirus-cure-covid-19, accessed April 2020. 18 ‘Coronavirus disease 2019 (COVID-19) Situation Report – 46’, World Health Organization. 19 Ibid. 20 Pien Huang, ‘How The Novel Coronavirus And The Flu Are Alike ... And Different’, NPR, 20 March 2020, https://www.npr.org/sections/goatsandsoda/2020/03/20/815408287/how-the-novel-coronavirus-and-the-flu-are-alike-and-different?t=1585211845934, accessed March 2020. 21 Ibid. 22 Wilder-Smith, Chiew, and Lee, ‘Can we contain the COVID-19 outbreak with the same measures as for SARS?’. 23 Ibid. 24 JS Mackenzie, P Drury, A Ellis, et al. ‘The Who Response to SARS And Preparations For The Future’, in S Knobler, A Mahmoud, and S Lemon, et al., editors, Learning from SARS: Preparing for the Next Disease Outbreak: Workshop Summary, Washington (DC): National Academies Press (US), 2004, https://www.ncbi.nlm.nih.gov/books/NBK92476/, accessed March 2020. 25 Wilder-Smith, Chiew, and Lee, ‘Can we contain the COVID-19 outbreak with the same measures as for SARS?’. 26 Ibid. 27 Ibid., and Todd Pollack in Kate Whiting, ‘Two experts explain what other viruses can teach us about COVID-19 – and what they can’t’, World Economic Forum, 20 March 2020, https://www.weforum.org/agenda/2020/03/coronavirus-covid-19-mers-sars-experts/, both accessed March 2020. 28 Wilder-Smith, Chiew, and Lee, ‘Can we contain the COVID-19 outbreak with the same measures as for SARS?’. 29 ‘United Kingdom: Healthcare report’, Economist Intelligence Unit, 15 December 2019, via EIU. 30 Nick Triggle, ‘10 charts that show why the NHS is in trouble’, BBC News, 24 May 2018, https://www.bbc.co.uk/news/health-42572110, accessed April 2020.
Notes
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
21
31 ‘NHS statistics, facts and figures’, NHS Confederation, 14 July 2017, https://www.nhsconfed.org/resources/key-statistics-on-the-nhs, accessed May 2020. 32 ‘How is the NHS structured?’, The King’s Fund, 11 April 2016, https://www.kingsfund.org.uk/audio-video/how-new-nhs-structured, accessed April 2020. 33 ‘Department of Health and Social Care Annual Report and Accounts 2018-19,’ Department of Health and Social Care, 11 July 2019, p. 3, https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/832765/dhsc-annual-report-and-accounts-2018-to-2019.pdf, accessed March 2020. 34 ‘United Kingdom: Healthcare report’, Economist Intelligence Unit. 35 Ibid. 36 Ibid. 37 ‘Oxford University Hospitals NHS Foundation Trust Annual Report and Accounts for 1 April 2018 – 31 March 2019’, 2019, p. 87, https://www.ouh.nhs.uk/about/publications/documents/ouh-nhs-ft-full-accounts-2018-19.pdf, accessed March 2020. 38 ‘United Kingdom: Healthcare report’, Economist Intelligence Unit. 39 Mark Dayan, Deborah Ward, Tim Gardner and Elaine Kelly, ‘How good is the NHS?’, The Health Foundation, the Institute for Fiscal Studies, The King’s Fund and the Nuffield Trust, 2018, p. 11, https://www.nuffieldtrust.org.uk/files/2018-06/the-nhs-at-70-how-good-is-the-nhs.pdf, accessed April 2020. 40 Ibid., p. 11. 41 Carl Baker, ‘NHS Key Statistics: England, February 2020’, House of Commons Library, 20 February 2020, p. 30, available at, https://commonslibrary.parliament.uk/research-briefings/cbp-7281/; and Denis Campbell, ‘NHS England “on its knees” as performance figures hit new lows’, The Guardian, 13 December 2019, https://www.theguardian.com/society/2019/dec/13/nhs-england-on-its-knees-as-performance-figures-hit-new-lows, accessed April 2020. 42 Denis Campbell, ‘NHS England “on its knees” as performance figures hit new lows’, The Guardian, 13 December 2019, https://www.theguardian.com/society/2019/dec/13/nhs-england-on-its-knees-as-performance-figures-hit-new-lows, accessed April 2020. 43 ‘United Kingdom: Healthcare report’, Economist Intelligence Unit. 44 Ibid. 45 Denis Campbell, ‘NHS has the west's most stressed GPs, survey reveals’, The Guardian, 19 January 2016, https://www.theguardian.com/society/2016/jan/19/nhs-has-the-wests-most-stressed-gps-survey-reveals, accessed April 2020. 46 ‘NHS Staff Survey 2019 National results briefing’, NHS England, February 2020, pp. 16 & 21, https://www.nhsstaffsurveys.com/Caches/Files/ST19_National briefing_FINAL V2.pdf, accessed April 2020. 47 Baker, ‘NHS Key Statistics: England, February 2020’, p. 30. 48 Niall Dickson quoted in Campbell, ‘NHS England “on its knees” as performance figures hit new lows’. 49 ‘Oxford University Hospitals NHS Foundation Trust’, Health Education England, n.d., http://www.oxforddeanery.nhs.uk/specialty_schools/foundation_school/trusts_info__job_descriptions/oxford_university_hospitals.aspx, accessed May 2020. 50 ‘OUH NHS Foundation Trust Annual Report and Accounts for 1 April 2018 – 31 March 2019’, p. 9. 51 Ibid., p. 14. 52 Ibid., p. 10. 53 Ibid., p. 200. 54 Ibid., p. 193. 55 Ibid., p. 65. 56 Ibid., p. 22. 57 Ibid., p. 15. 58 Ibid., p. 5. 59 Ibid., p. 15. 60 ‘Review of Board, Executive Team and Senior Management Restructuring’, Oxford University Hospitals NHS Foundation Trust, 11 March 2020, https://www.ouh.nhs.uk/about/trust-board/2020/march/documents/TB2020.22-restructuring.pdf, accessed April 2020. 61 ‘Oxford University Hospitals NHS Foundation Trust Inspection report’, Care Quality Commission, 7 June 2019, https://www.cqc.org.uk/sites/default/files/new_reports/AAAJ4270.pdf, accessed May 2020. 62 Ibid., p. 4. 63 Ibid., p. 11. 64 ‘Board Quality Report’, Oxford University Hospitals NHS Foundation Trust, 16 January 2019, p.13, https://www.ouh.nhs.uk/about/trust-board/2019/january/documents/TB2019.06-board-quality-report.pdf, accessed May 2020. 65 ‘OUH NHS Foundation Trust Annual Report and Accounts for 1 April 2018 – 31 March 2019’, p. 227. 66 ‘Oxford University Hospitals NHS Foundation Trust 2019 NHS Staff Survey Benchmark Report’, NHS England, p. 35, 2019, http://www.nhsstaffsurveyresults.com/wp-content/uploads/2020/02/NHS_staff_survey_2019_RTH_full.pdf, accessed May 2020. 67 ‘Caring, supportive, collaborative? Doctors’ views on working in the NHS’, British Medical Association, 2018, https://www.bma.org.uk/media/2035/bma-caring-supportive-collaborative-survey-report-sept-2018.pdf, accessed May 2020.
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
22
68 Pavel V Ovseiko and Alastair M Buchan, ‘Organizational Culture in an Academic Health Center: An Exploratory Study Using a Competing Values Framework’, Academic Medicine, June 2012, vol. 87, no. 6, pp. 709-718 doi: 10.1097/ACM.0b013e3182537983. 69 Ibid. 70 Ibid. 71 John R Drew and Meghana Pandit, ‘Why healthcare leadership should embrace quality improvement’, British Medical Journal, 31 March 2020, http://dx.doi.org/10.1136/bmj.m872, accessed May 2020. 72 ‘OUH NHS Foundation Trust Annual Report and Accounts for 1 April 2018 – 31 March 2019’, p. 173. 73 ‘NHS Staff Survey 2019’, Oxford University Hospitals NHS Foundation Trust, 27 February 2020, https://www.ouh.nhs.uk/about/trust-board/2020/march/documents/TB2020.27-staff-survey.pdf, accessed April 2020. 74 ‘UK Influenza Pandemic Preparedness Strategy 2011’, Department of Health, 10 November 2011, https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/213717/dh_131040.pdf, accessed April 2020. 75 Steven Swinford, ‘Michael Gove insists he is happy in support role to Matt Hancock’, The Times, 23 March 2020, via Factiva. 76 'Coronavirus: action plan’, Department of Health and Social Care, 3 March 2020, https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/869827/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf, accessed April 2020. 77 Ian Boyd, ‘Coronavirus: a former member of SAGE explains how the science advisory group really works’, The Conversation, 24 March 2020, https://theconversation.com/coronavirus-a-former-member-of-sage-explains-how-the-science-advisory-group-really-works-134077, accessed April 2020. 78 ‘Pandemic Influenza Strategic Framework,’ Public Health England, 2014, https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/344696/PI_Strategic_Framework_13_Aug.pdf, accessed April 2020. 79 ‘Operating Framework for Managing the Response to Pandemic Influenza’, NHS England, 15 December 2017, https://www.england.nhs.uk/wp-content/uploads/2017/12/nhs-england-pandmic-influenza-operating-framework-v2.pdf, accessed April 2020. 80 Ibid. 81 ‘Coronavirus testing’, Public Health England, 14 March 2020, https://www.gov.uk/government/news/coronavirus-testing, accessed April 2020. 82 Clive Cookson, ‘UK’s original coronavirus plan risked “hundreds of thousands” dead’, Financial Times, 16 March 2020, https://www.ft.com/content/249daf9a-67c3-11ea-800d-da70cff6e4d3, accessed April 2020. 83 Neil M Ferguson, Daniel Laydon, Gemma Nedjati-Gilani et al., ‘Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand’, Imperial College London, 16 March 2020, https://doi.org/10.25561/77482. 84 Heather Stewart, Sarah Boseley, Peter Walker and Larry Elliott, ‘PM tells Britons to avoid non-essential travel and contact’, The Guardian, 16 March 2020, https://www.theguardian.com/world/2020/mar/16/pm-tells-britons-to-avoid-non-essential-contact-with-others, accessed April 2020. 85 Ibid. 86 ‘PM statement on coronavirus: 16 March 2020’, Prime Minister’s Office, 16 March 2020, https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-16-march-2020, accessed April 2020. 87 ‘COVID-19: infection prevention and control,’ Public Health England, 10 January 2020, updated 13 March 2020, available at https://web.archive.org/web/20200314173818/https://www.gov.uk/government/publications/wuhan-novel-coronavirus-infection-prevention-and-control, accessed April 2020. 88 ‘Operating Framework for Managing the Response to Pandemic Influenza’, NHS England. 89 Shaun Lintern, ‘Coronavirus: Doctors warn UK hospitals running out of protective equipment for staff’, The Independent, 9 March 2020, https://www.independent.co.uk/news/health/coronavirus-nhs-hospitals-masks-nurses-doctors-a9385131.html, accessed April 2020. 90 Ibid. 91 Ibid. 92 Denis Campbell and Mattha Busby, ‘“Not fit for purpose”: UK medics condemn Covid-19 protection’, The Guardian, 16 Mar 2020, https://www.theguardian.com/society/2020/mar/16/not-fit-for-purpose-uk-medics-condemn-covid-19-protection, accessed April 2020. 93 Campbell and Busby, ‘“Not fit for purpose”: UK medics condemn Covid-19 protection’, and ‘COVID-19: infection prevention and control guidance’, Public Health England, updated 6 March 2020, available at https://web.archive.org/web/20200310230352/https://www.gov.uk/government/publications/wuhan-novel-coronavirus-infection-prevention-and-control/wuhan-novel-coronavirus-wn-cov-infection-prevention-and-control-guidance, both accessed April 2020. 94 Campbell and Busby, ‘“Not fit for purpose”: UK medics condemn Covid-19 protection’. 95 ‘COVID-19: track coronavirus cases’, Public Health England, published 10 March 2020, updated 14 April 2020, available at https://www.gov.uk/government/publications/covid-19-track-coronavirus-cases, accessed April 2020. 96 Roseanne Edwards, ‘Coronavirus - Oxford hospitals trust is chosen to be a UK Covid-19 “surge” centre’, Banbury Guardian, 17 March 2020, https://www.banburyguardian.co.uk/health/coronavirus/coronavirus-oxford-hospitals-trust-chosen-be-uk-covid-19-surge-centre-2481491, accessed April 2020. 97 Meghana Pandit, e-mail correspondence with case writers, 13 April 2020. 98 Ibid. 99 Ibid. 100 This section is based on case writer observations during a field visit on 17 March 2020.
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST

COVID-19 at Oxford University Hospitals: Sustaining morale on the eve of a crisis
23
101 Gareth Iacobucci, ‘Covid-19: all non-urgent elective surgery is suspended for at least three months in England’, British Medical Journal, 18 March 2020, https://www.bmj.com/content/368/bmj.m1106, accessed April 2020. 102 See, for instance, ‘Coronavirus infection and pregnancy’, Royal College of Obstetricians and Gynaecologists, n.d., https://www.rcog.org.uk/en/guidelines-research-services/guidelines/coronavirus-pregnancy/covid-19-virus-infection-and-pregnancy/#general, accessed May 2020. 103 Pushpinder Mangat, Keith Gardiner, Rowan Parks, Sheona MacLeod, and Colin Melville, ‘Supporting the COVID-19 response: Plans for Management of Medical Training Rotations’, Health Education England, 16 March 2020,https://www.hee.nhs.uk/sites/default/files/documents/Plans%20for%20management%20of%20medical%20training%20rotations.pdf, accessed Apirl 2020. 104 Nina Strochlic and Riley D Champine, ‘How some cities “flattened the curve” during the 1918 flu pandemic’, National Geographic, 27 March 2020, https://www.nationalgeographic.com/history/2020/03/how-cities-flattened-curve-1918-spanish-flu-pandemic-coronavirus/, accessed March 2020. 105 ‘1918 Pandemic (H1N1 virus)’, Centers for Disease Control and Prevention, 20 March 2019, https://www.cdc.gov/flu/pandemic-resources/1918-pandemic-h1n1.html, accessed March 2020. 106 Sara Goudarzi, ‘Lessons from Past Outbreaks Could Help Fight the Coronavirus Pandemic’, Scientific American, 23 March 2020, https://www.scientificamerican.com/article/lessons-from-past-outbreaks-could-help-fight-the-coronavirus-pandemic1/, accessed March 2020. 107 Qianying Lin, Shi Zhao and Daozhou Gao et al, ‘A conceptual model for the coronavirus disease 2019 (COVID-19) outbreak in Wuhan, China with individual reaction and governmental action', International Journal of Infectious Diseases, volume 93, April 2020, pp. 211-216, available at https://doi.org/10.1016/j.ijid.2020.02.058. 108 Goudarzi, ‘Lessons from Past Outbreaks Could Help Fight the Coronavirus Pandemic’. 109 Ibid. 110 Ibid. 111 Ibid. 112 Tan Chorh-Chuan, ‘SARS in Singapore-key lessons from an epidemic,’ Annals-Academy of Medicine Singapore, 35.5 (2006), pp. 345-9, http://www.annals.edu.sg/pdf/35VolNo5200606/V35N5p345.pdf, accessed April 2020. 113 Ibid. 114 Ibid. 115 Tomislav Svoboda, Bonnie Henry, Leslie Shulman, Erin Kennedy, Elizabeth Rea, Wil Ng, Tamara Wallington et al., ‘Public health measures to control the spread of the severe acute respiratory syndrome during the outbreak in Toronto,’ New England Journal of Medicine 350, no. 23 (2004): 2352-2361, https://www.nejm.org/doi/pdf/10.1056/NEJMoa032111, accessed April 2020. 116 Ibid. 117 Ibid. 118 Ibid. 119 Elena Cherney, ‘The SARS outbreak: New quarantines ordered in Canada’, Wall Street Journal, 27 May 2003, via ProQuest, accessed April 1, 2020. 120 Svoboda, Henry, Shulman, Kennedy, et al., ‘Public health measures to control the spread of the severe acute respiratory syndrome during the outbreak in Toronto’.
This document is exclusively authorised for use in the Blavatnik School of Government’s Case Method for Public Policy workshop, June 2020.
DO NOT
COPY OR P
OST