cover adivasi 2020 - scstrti
TRANSCRIPT






IMPACT OF PANDEMICSON TRIBAL CULTURE OF ODISHA :With Special Reference to COVID –19

3IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
IMPACT OF PANDEMICS ON TRIBALCULTURE OF ODISHA:
With Special Reference to COVID - 19
HISTORY OF EPIDEMICSAND PANDEMICS ININDIAIndia, being a third-world country, hasencountered a variety of epidemicsand pandemics through time. Severalaccounts of influenza, cholera,dengue, smallpox and several othershave been recorded throughouthistory; while we have been able toeradicate some; many diseases stillcontinue to pose a threat to thecommunity. It is not uncommon forsudden and rapid outbreaks to occurin India and many articles direct thecause for this in such developingcountries being malnutrition, lack ofsanitation and lack of a proper publichealth system (Rice et.al, 20001 , John,et.al 2). Epidemics is an unusualoccurrence in a community or regionof disease, specific health relatedbehaviour or other health-relatedevents clearly in excess of expected
occurrence. It is a sudden, severewidespread outbreak of a disease pre-existing in the community.
Pandemics, on the other hand, refer tothe worldwide spread of diseases.These are the global health problemsthat need to be addressed and treatedviciously along with proper measuresto avoid transmission to othercountries. There have been asignificant number of pandemicsthroughout history and in manyinstances; their control had beendifficult because of the lack of aproper, working global surveillancesystem3 . As far as India is concerned,there have been only two major,significant pandemics throughouthistory. While cholera had beenpredominant throughout the 19thcentury with increasing death tollsevery year, the influenza pandemiccame later on in the early 20thcentury4 5. The influenza pandemic
1 Rice AL, Sacco L, Hyder A, Black RE. 2000. Malnutrition as an underlying cause of childhooddeaths associated with infectious diseases in developing countries. Bulletin of the World Healthorganization. 2000; 78:1207-21.
2 John TJ, Dandona L, Sharma VP, Kakkar M. 2011. Continuing challenge of infectious diseasesin India. The Lancet. 2011;15; 377(9761):252-69.
3 Hughes JM, Wilson ME, Pike BL, Saylors KE, Fair JN, LeBreton M, Tamoufe U, Djoko CF,Rimoin AW, Wolfe ND. The origin and prevention of pandemics. Clinical Infectious Diseases.2010 Jun15; 50(12):1636-40
4 Ramamurthy T, Sharma NC. Cholera outbreaks in India. In Cholera Outbreaks 2014 (pp. 49-85). Springer, Berlin, Heidelberg
5 Mills, Ian D. “The 1918-1919 influenza pandemic-the Indian experience.” The Indian Economic& Social History Review23.1 (1986):1-40.
I

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-194
In the last 100 years, flu became thenew plague. Although the firstinfluenza epidemic is recorded in the16th century, the flu became pandemicfrom the time of the 1889-90 flu, nowcalled the Russian flu. The Spanish Fluof 1918-19 was the most damaging asit infected a third of the entirepopulation of the world with morepeople dying from it than from WorldWar 1. Then followed the Asian Fluof 1957-58, the Hong Kong Flu of 1968-69 and, more recently, the Swine Fluof 2009-10, which ended up infectingmore than a billion people and killinga few lakhs.
In the last 50 years, there has beenanother interesting pattern:pandemics originating in bats. It
6 Mishra B. 2015 resurgence of influenza a (H1N1) 09: Smouldering pandemic in India?. Journalof global infectious diseases. 2015;7(2):56
7 https://odishabytes.com/pandemics-in-history-shipping-the-virus/8 https://odishabytes.com/pandemics-in-history-2-rats-and-the-plague/
was short but devastating and after along time, quite recently, came yetanother flu pandemic by the H1N1strain6
Before the 20th century, the plaguecaused by rats was the recurringpandemic (there had been otherpandemics though like cholera andsmall pox). There had been three bigplague pandemics, the last being in thelate 19th century. And rats were seenas responsible for the plague and theyhad spread it by travelling on ships.Two small articles by Sujit Mahapatraon 20th April7 and 25th April8 providesa glimpse of the history of Pandemicsand the carriers all over the world.
started in 1976 with Ebola, whichravaged West Africa and killed 13,500people; the Nipah virus of 1998 witha 78% fatality; and then theCoronaviruses of the last 20 years:SARS of 2002, which spread to 29countries with 774 deaths; MERS in2012 that spread to 28 countriesresulting in 858 deaths; and of courseCOVID-19, the pandemic that hasdevastated the world more thananyone in this world today. Thecoronaviruses are also contagiousviruses causing respiratory diseaseslike the flu. In fact, the Centers forDisease Control and Prevention(CDC) of the US estimates, threequarters of new or emerging diseasesthat infect humans originate inanimals.
Scientists discovered the bat origins ofcertain viruses after the outbreak ofSARS or Severe Acute RespiratorySyndrome in 2003. It was discoveredthat bats contain hundreds of othercoronaviruses, a group of relatedviruses causing respiratory ailmentsranging from harmless ones like thecommon cold to MERS that had afatality rate of 34%. As they grow,(COVID-19 is a novel coronavirus ora new strain of the virus), the differentstrains infect bats, which seem to beco-evolving with the viruses. Hence,bats have powerful immune systemsand do not fall sick. But when theseviruses jump from them to other

5IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
species such as a civet or a pangolinor a human, the result can be deadly,as we see now.
It seems, Ships have always played asignificant role in pandemics inhistory. After all, as many of us nowknow, the word ‘quarantine’, was firstused in the 14th century for ships thatwere made to wait for 40 days outsideVenice before passengers wereallowed to disembark. This is becausethe bubonic plague, which had wipedout about a third of Europe and amuch of Asia, was supposed to havea 37-day period from infection todeath. Hence, it was assumed thatanyone healthy after 40 days was safefrom infecting others.
Ships have historically been seen asthe transporters of pandemics, whendiseases travel across geographies asthey have been used for internationaltrade. The voyages of ChristopherColumbus and others led todecimation of entire indigenouspopulations in the Americas with thespread of small pox, measles and theplague, which were foreign to thenatives. This story continued till the20th century with most pandemics.That is because the ships carried therats that carried the plague. Therefore,elaborate protocols were followedearlier to ensure that ships were rid ofrats.
The 21st century pandemics such asSARS and MERS unlike the plaguewere not spread by rats or rat flea, andair travel played a significant role inthe transport of infectious diseases. Atthe same time, COVID-19 has broughtthe attention back to ships as theyaccounted for the first horror story ofthe epidemic outside China.
1.1 THE 19th CENTURYPANDEMICS
First Cholera Pandemic (1817)
This is considered to be the first majorepidemic of the 19th century in British-colonized India and was described asprobably the most terrifying of all9. Itis believed that the year 1817 hadbrought a very heavy rainfall leadingto flooding which could have been thecause for such a rapid spread10. Whilethe Europeans living in India then andthe elite were not seriously affected,the slum dwellers and people in ruralpoverty were hit the worst11. This wasprobably due to the differences inliving conditions, personal hygieneand practices.
Second Cholera Pandemic (1829)
The second outbreak started around1826 from Bengal and spread throughthe rivers to various parts of northernIndia. After affecting the UnitedProvinces (UP), its impact was huge
9 Arnold, David. 1986. ‘Cholera and colonialism in British India’ Past & Present. 113:118- 151.10 Collins, A. E. “The geography of cholera.” Cholera and the Ecology of Vibrio cholerae. Springer,
Dordrecht, 1996. 255-294.11 Pollitzer R, Swaroop S, Burrows W. History of the disease. Cholera. World Health Organization,
Geneva, Switzerland.1959:11-50.

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-196
on areas around Punjab and Delhi butmost significant is its pandemicspread to countries like China12 13.Cholera spread far and wide, all alongthe trade routes from China affectingseveral cities and villages alike. In eachplace, it lasted for a few weeks andkilled hundreds of people every day14.
Third Cholera Pandemic (1852)
The third cholera pandemic startedaround 1852 and lasted till the late1860s. It is significant in historybecause of its spread to countries thatwere until then not affected. ThoughIndia was not its major area ofimpact, in the later phase ofpandemic, small spurts of cases werenoted in Bengal. It spread to severalother countries like Persia, Arabia andthen to Russia due to the worldwidespread of serotype of Vibrio whichwas initially endemic to India.
Fourth Cholera Pandemic (1863)
This began around 1863. While somesuggest that the major choleraepidemic in 1865 was brought toMecca by the Haj pilgrims from India,others disagree stating that it was ajust a recrudescence15. However, it is
agreed that it was from Mecca that theinfection spread to several countries16
17 . The Kumbh Mela at Hardwar inApril 1867 has been considered to beresponsible for the epidemic spreadof cholera in northern India18. TheMadras Presidency in 1877 was theworst hit and the cholera epidemicwas responsible for about 10% of theannual mortality then19.
Fifth Cholera Pandemic (1881)
The fifth cholera pandemic wasconsiderably less fatal as compared tothe previous four. It was during thispandemic (1881-1869) that RobertKoch proved that cholera wastransmitted through the fecal-oralroute, after studying the outbreaks inCalcutta and Egypt20.
Bombay Plague Epidemic (1896)
This plague began in September 1896in colonial Bombay creating a lot ofsocial and political frenzy. The rapidgrowth of commerce in Bombay led toan increase in population and therebyovercrowding. The anti-plaguecampaign was started to battle thisepidemic and it was based on thebelief that the focus of the infections
12 Pollitzer, Robert. ‘Cholera studies:1. History of the disease ’. Bulletin of the World HealthOrganization 10.3 (1954):421.
13 Barua, Dhiman. “History of cholera.” Cholera. Springer, Boston, MA, 1992.1-3614 Macnamara, Nottidge Charles. A history of Asiatic cholera. MacMillan,187615 Omar W. The Mecca Pilgrimage: Its Epidemiological Significance and Control. Postgraduate
medical journal. 1952;28(319):269.16 Bryceson, AD. Cholera, the flickering flame. (1977):363-36517 Lacey, Stephen W. Cholera: calamitous past, ominous future. Clinical Infectious Diseases 20.5
(1995):1409-141918 Arnold, David.”Cholera and colonialism in British India.”Past & Present 113(1986):118- 15119 Whitcombe E, Famine mortality. Economic and Political Weekly (1993):1169-1179.20 Howard-Jones, Norman. Robert Koch and the cholera vibrio: a centenary. British medical journal
(Clinical research ed.)288.6414 (1984):379

7IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
was from the slums. The plague killedthousands and many people wereforced out of the city.
Sixth Cholera Pandemic (1899)
The sixth cholera pandemic beganaround 1899 and major outbreakswere noted in Bombay, Calcutta, andMadras21. While the infectionthroughout the 20th century wascaused by O1 serotype of Vibriocholera and confined mostly throughthe Asian subcontinent, the sixthcholera pandemic brought aboutsurprising challenges. The sixthcholera pandemic lasted for about 25years (1899-1973)22.
1.2 THE 20th CENTURYPANDEMICS
Influenza Pandemic (1918)
This is also known as the Spanish Fluof 1918-19. This has been known tohave caused around 20- 50 milliondeaths worldwide and is consideredmost devastating23 . This was causedby the H1N1 strain of Influenza andwas severe. The first episode of thedisease began in early 1918 and laterin autumn, it began to spread all
around the world, India consideredto be the foci24. The second wave ofthe attack began in Bombay in 1918and spread to other parts of northernIndia and Sri Lanka from where itspread worldwide25. Improvement inthe virulence and velocity of the virusstrain and the monsoon bringinghumidity are considered to be the keyfactors in increasing the severity andspread26.
Polio Epidemic (1970-1990)
India was the worst affected by polioamong the developing countries untilthe late 1990s. The incidence of polioin India was very high in both urbanand rural states and the most affectedwas the state of Uttar Pradesh27. Butwith improvement in surveillance, thedesired results were achieved andIndia was declared polio-free status inJanuary 2011 and emphasis has beenlaid on maintaining the guard toprevent resurgence28.
Small Pox Epidemic (1974)
It is known as one of the worst smallpox epidemics of the 20th century.India contributed to about 85% ofthis epidemic worldwide. This
21 Ramamurthy T, Sharma NC. Cholera outbreaks in India. In Cholera Outbreaks 2014 (pp. 49-85). Springer, Berlin, Heidelberg
22 Kaper JB, Morris JG, Levine MM. Cholera. Clinical microbiology reviews. 1995 1;8(1):48-8623 Colwell, Rita R. “Global climate and infectious disease: the cholera paradigm.” Science 274.5295
(1996):2025-2031.24 Johnson NPAS, Mueller J. Updating the accounts: global mortality of the 1918-1920" Spanish”
influenza pandemic. Bull Hist Med. 2002; 76:105–11525 Chandra S, Kassens-Noor E. The evolution of pandemic influenza: evidence from India, 1918–
19. BMC infectious diseases. 2014; 14(1):51026 Johnson NPAS, Mueller J. Updating the accounts: global mortality of the 1918-1920" Spanish”
influenza pandemic. Bull Hist Med. 2002; 76:105– 11527 John, T. Jacob, and Vipin M. Vashishtha. Eradicating poliomyelitis: India’s journey from
hyperendemic to polio-free status. The Indian journal of medical research 137.5 (2013): 88128 Patterson K D, Pyle G F. The geography and mortality of the 1918 influenza pandemic. Bull
Hist Med. 1991; 65:4–21.

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-198
epidemic broke out in three differentvillages of West Bengal, Bihar andOdisha but it was impossible toestablish a connection between themand hence it was treated as threedifferent epidemics. The disease wasintroduced into different areas bydifferent sources. While over 15,000people died in this epidemic,thousands of the survived but mostended up with disfigurement andblindness29 30. Small pox was the firstdisease to be combated globally andwas declared eradicated by WHO in198031.
Surat Plague Epidemic (1994)
Plague cases in Surat were firstreported in Sept 1994 and which itspread to other cities in India. Fewerthan 1,200 people were found positiveand it lasted for less than two weeksbut it is considered important due toits high fatality and created worldwiderepercussions. It is said to have beeninitially difficult for doctors todiagnose it but when they did, allnecessary precautions are taken tocontain its spread32 [37].
1.3 THE 21st CENTURYPANDEMICS
Plague of Northern India (2002)
The Plague of Northern India brokeout in Shimla district of HimachalPradesh in February 2002. It was asmall and less serious epidemic. Also,as soon as the plague was detected,immediate measures were taken likefumigation, evacuation, andchemoprophylaxis that lead to furthercontrol of the epidemic33.
Dengue Epidemic (2003)
In 2003 during September, thereoccurred an outbreak of Dengue Feverin Delhi. It reached its peak aroundOctober-November and lasted untilearly December. The mortality ratewas around 3%. It became a majoroutbreak in India in spite of thewidespread preventive measurestaken to control Dengue Fever34.
SARS Epidemic (2003)
SARS (severe acute respiratorysyndrome), is considered as the firstserious infectious disease outbreak ofthe twenty-first century. It initially
29 John TJ. Understanding the scientific basis of preventing polio by immunization. Pioneeringcontributions from India. Proc Indian Natl Sci Acad.2003; B69:393–422
30 The control and eradication of smallpox in South Asia, Internet Archive, 2018, Available from:https://web.archive.org/web/20081019023043/ http://www.smallpoxhistory.ucl.ac.uk
31 Greenough P. Intimidation, coercion and resistance in the final stages of the South Asian smallpox eradication campaign, 1973–1975. Social science & medicine.19951;41(5):633- 45
32 Fenner F. Global eradication of small pox. Reviews of infectious diseases.19821;4(5):916- 3031 Greenough P. Intimidation, coercion and resistance in the final stages of the South Asian small
pox eradication campaign, 1973–1975. Social science & medicine.19951;41(5):633- 4532 Fenner F. Global eradication of small pox. Reviews of infectious diseases.19821;4(5):916- 3033 Dutt, Ashok K., Rais Akhtar, and Melinda McVeigh. Surat plague of 1994 re- examined. Southeast
Asian journal of tropical medicine and public health 37. 4(2006):75534 Gupta, Manohar Lal, and Anuradha Sharma. Pneumonic plague, northern India, 2002. Emerging
Infectious Diseases13.4 (2007):664.

9IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
35 Singh N P, Jhamb R, Agarwal S K, Gaiha M, Dewan R, Daga M K, Chakravarti A, Kumar S. The2003 outbreak of dengue fever in Delhi, India. Headache. 2005 1; 114:61
36 Dikid,T.Emerging & re-emerging infections in India : An overview .The Indian journal of medicalresearch 138.1 (2013): 19
37 Manchanda V, Gupta S, Bhalla P. Meningococcal disease: History, epidemiology, pathogenesis,clinical manifestations, diagnosis, antimicrobial susceptibility and prevention. Indian J MedMicrobiol 2006;24:7-19
38 Mavalankar D, Shastri P, Bandyopadhyay T, Parmar J, Ramani KV. Increased mortality rateassociated with chikungunya epidemic, Ahmedabad, India. Emerging infectious diseases.2008;14(3):412
39 Kaur P, Ponniah M, Murhekar M V, et al. Chikungunya outbreak, South India, 2006. EmergInfect Dis. 2008;14(10):1623–1625.doi:10.3201/ eid1410.07056
40 Mavalankar, Dileep, PriyaShastri and Parvathy Raman.”Chikungunya epidemic in India: a majorpublic-health disaster.” The Lancet infectious diseases 7.5 (2007):306-307
41 Nationwide data on outbreak, The Hindu”. Chennai, India. 9 October 2006.Archived.
started in the Guandong province ofChina in 2003 and spread quickly toabout 30 countries across Asia,Americas and Europe and accountedfor a total of 8,439 cases and 812deaths, within 7 to 8 months35 36.
Meningococcal MeningitisEpidemic (2005)
In early 2005, a sudden surge had beennoted in meningococcaemia andmeningococcal meningitis cases inIndia. Cases were reported from Delhiand the surrounding states of UttarPradesh and Maharashtra. Casemanagement, early detection throughsurveillance was aimed at preventionof spread37 .
Chikungunya Outbreak (2006)
Around 3.4 million cases ofChikungunya were reported inAhmedabad 2006. In December, thereoccurred another epidemic in SouthIndia where the states of AndhraPradesh, Karnataka and Tamil Naduwere affected. The volatile nature ofthis epidemic was attributed to theherd immunity to the then isolatedgenotype38.Major efforts were taken
for mosquito control and severalawareness campaigns were initiatedby the television and print media39.
Dengue Outbreak (2006)The outbreak began in earlySeptember of 2006 and the first casewas reported from Delhi. By the endof September, it began to spread toother states like Rajasthan, Kerala,Gujarat, Chandigarh and UttarPradesh40. The ministry of health setup a control room to monitor theoutbreak and provide technicalassistance that led to the efficientmanagement of the disease.
Gujarat Jaundice epidemic (2009)Modasa town in Gujarat witnessed theoutbreak of hepatitis B in 200941 Thisis of significance because almost alloutbreaks of viral hepatitis in Indiawere considered to be due to hepatitisE which is feco-orally transmitted [50].It was a long-lasting epidemic andcontrol was achieved by mass publicawareness and health actions.
H1N1 Flu Pandemic (2009)
The H1N1 Flu pandemic began in May2009 and spread globally by July 2009.

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1910
By August 2010, it was declaredpandemic. Three strains of influenzaviruses were circulating then.
Odisha Jaundice Epidemic (2014)
The outbreak began in November2014 in Kantalbai, a remote village inOdisha. This led to a district levelinvestigation and it was confirmed tobe jaundice caused by the Hepatitis Evirus42. This 2014 Odisha Jaundiceepidemic was one of the manyoutbreaks in Odisha and the mostcommon cause being HEV43. This istransmitted enterically and hasaffected several people, especially ofthe low socioeconomic category.Surveillance for clean water andsanitation was proposed as the controlmeasure44.
Indian Swine Flu Outbreak (2015)
It refers to the outbreak of the 2009H1N1 flu pandemic in India whichwas still present as of March 2015. Thisoutbreak in 2015 is considered as aresurgence of the infection and the
most plausible reasons are consideredto be low temperature, decreasing hostimmunity and failure of vaccinationcampaign after 201045. According tothe NCDC data in India, Rajasthan,Maharashtra, and Gujarat were theworst affected states in India duringthis pandemic.
Nipah Outbreak (2018)
The virus was first noted in the late1990s in Singapore and Malaysia. Thenatural host for this disease is the fruitbat and transmission is from directperson to person contact [60]. ThisNipah virus outbreak began in May2018 in Kozhikode District, Kerala.This is the first Nipah virus outbreakreported in Kerala and the thirdknown to have occurred in India, withthe most recent previous outbreakbeing in 200746. Spread of awarenessabout this infection, isolation of theinfected and post-outbreaksurveillance led to the control of thisoutbreak.
42 Dangi T, Jain B, Singh AK, Mohan M, Dwivedi M, Singh JV, et al. Influenza virus genotypescirculating in and around Lucknow, Uttar Pradesh, India, during post pandemic period, August2010-September 2012. Indian J Med Res. 2014; 139:418–26
43 Integrated Disease Surveillance Programme (IDSP). National Center for Disease Control, DGHS,MOH & FW, Government of India. Disease Outbreak Reported and Responded by States. 2012.http://www.idsp.nic.in
44 Kelly R. India Weekly Outbreak Reports 2013. Emerging Disease and Other Health ThreatsWinnter Park, Florida: Flutrakers.com, Inc. 2015 https://flutrackers.com/forum/ forum/india/india-emerging-diseases-and-other-health- threats/158406-india-weekly-outbreakreports-2014
45 Paul, Sourabh, et al. “Investigation of jaundice outbreak in a rural area of Odisha, India: Lessonslearned and the way forward.” Community Acquired Infection 2.4 (2015):131
46 NCDC, Ministry of Health (2019), H1N1 Swine Flu- number of cases and deaths from 2012-2019 Data. Available from: https://ncdc.gov.in/showfile. php?lid=280

11IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
IIHISTORY OF EPIDEMICSIN TRIBAL ODISHAThere is hardly adequate accessiblecomprehensive literature tounderstand the history of epidemics,their impact, prevention anderadication in the context of tribalOdisha. There are, however, sporadicliterature indicating how the tribalpeople perceive sickness andepidemics as manifestation of thewrath and anger of malevolent deitiesor spirits. The diseases and epidemicswere then, and have been now,addressed through many religiousand magico-religious practices basedon the speculations of the priests,shamans, magico-religious healersand such others who are believed tobe capable of making directconnection between the members ofthe community and the gods,goddesses, ancestral spirits, naturalinfluences, etc. There is also somesporadic literature on the treatmentpractices, ethno-medicine and drugadministration in case of certaincommon and uncommon diseases, butindications on comprehensivehealthcare system to prevent, fight andabate an epidemic by the tribalcommunities of Odisha are hardlyfound in the accessible and availableliterature. Therefore, in this attempt,it has been tried to exhaustively usethe available resources to develop ahistorical connection betweenepidemic management in tribal
Odisha and the current case ofmanaging Covid 19.
An Indian Council of HistoricalResearch Scholar – Susanta Barikprovided an appealing review of theepidemic management during theColonial and pre-Colonial times. Thereview has also cited cases of certaintribal communities in Odisha inconnection with epidemic occurrenceand its management in tribal areas ofthe state. Following are excerpts fromhis article - Disease and Medicine inthe Colonial Odisha during 19thCentury
The British began to face healthproblem as the climate of Odisha wasdifferent from other parts of BritishIndia. At the initial stages the Britishtried their best to save from variousepidemic diseases. During late 19thcentury the British took measures toprevent different kinds of diseases likeSmallpox, Cholera, Malaria,Diarrhoea, and Kalazar. Smallpox hadendangered the lives of the nativepeople as well as the Europeans. Manyamong the Europeans either died orleft the state because of the epidemicdiseases. However, the British settleddown in every nook and corner of thestate and began to look after the sickpeople. They were also given detailedinformation about flora and fauna andcultural practices of the new territory.They gradually began to redefine thethings which they saw in terms of theirown territory and perception. Theirwork encompassed not only theunderstanding and possible conquestof new disease but also extension of

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1912
western cultural values to the rest ofthe world (Pati, 200147, Barik, 201548).
During Pre-Colonial period theseepidemic diseases were there but theirtreatment was very much localised.The people were lackingcommunication as well as modernmedical facilities. Generally, peoplewere using the traditional medicine.Besides, there were native medicalpractitioners Kaviraj or Vaidyas whopreferred to practise medicineaccording to the rules laid down in theHindu religious books (Shastras)49 . Italso appears that in most part of thetribal Odisha the people used plants,herbs, different body parts of birdsand animals as medicine for curingdiseases.
Another interesting aspect was thatthere has been an age-old belief amongthe tribes that some sickness, disease,wounds and accidents are caused bythe evil spirit of the jungle and to getcure from it, the malevolent spirit hasto be propitiated. Following this belief,the people offers some meat, rice beer,fowl or bird etc.to the spirit and this issaid to cure the person. Such a beliefin malevolent spirit is common notonly among the tribal people of theworld but also most of the rural areasof the world. But at the same time thebelief in the evil spirit and ghostcontinues side by side (Pati, 2001, p.15)
It is also a fact that introduction ofmodern medicine and implementationof vaccination policy in Odisha byEuropeans was a challenge for them.The people in Odisha were not readyto accept it as they were preoccupiedwith their traditional superstitiousbeliefs. It was in the late 19th centuryPasteur Koch and other madeadvances in bacteriology and installedconfidence among British medicalmen in India that epidemic diseasecould be prevented by westernscientific knowledge. It was duringthis period Kalazar first appeared inthe Kutia tribes in 1869. Odisha hadalready become a hunting ground fordeadly epidemic diseases like Cholera,Smallpox and Malaria fever. Smallpoxwas a devastating misfortune. It wasa highly contagious viral disease. Itkilled severely large numbers andseriously maimed survivors throughsever scarring of the skin withpockmarks, blindness and infertility.During 19th century Smallpox wasone of the main epidemic diseases inOdisha. Mortality rate with thisdisease was very high and it mainlyaffected the poor section of society.Another dreaded epidemic diseasewas defined as ³malaria´. It wasessentially an economic diseasesapping the vigour and physique ofthe community. It lowers one’s vitalitythereby preparing the ground for other
47 Pati Biswamoy, 2001. Situating Social History, Orissa (1800-1997), Orient Longman, New Delhi,p.14
48 Barik, S, 2015 Disease and Medicine in the Colonial Odisha during 19th Century, Odisha Review,September 2015, p. 25-27
49 Iris Bruijn, 2009. Ships Surgeons of the Dutch East India Company: Commerce and the Progressof Medicine in the Eighteenth Century (Amsterdam University Press), p-55

13IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
disease like Tuberculosis etc. It ispointed out that Malaria fever and toa greater extent Cholera became ahighly political disease whichthreatened the slender basis of thecritical point of intervention betweencolonial state and indigenous society.Throughout the colonial rule, Choleraleaked across all the preventivehurdles and caused epidemic havocall over Odisha. As the British wereunable to control the diseases, theyfrequently resorted to blame thenatural obstacles and opium eatinghabit of the native for the spread of thedisease (Tahir, 2013, p.3). Althoughthe western medical discourse answerto Malaria was quinine. This methodwas applied in Odisha and quininewas sold through the agency of postoffices. However, this was totallyinadequate to curb the menace ofMalaria. It had little impact on theindigenous system of Malariatreatment. In the indigenous treatmentfor the fever, capsicum, borak, maceand papal ground mixed together withlime juice and of which one rateweight (about two gram) was giventhree times a day with juice of greenginger. A similar preparation, butmixed with goat urine was alsoprescribed in cases of fever. In the case
of Kala-zar, since its etymology wasunknown prior to 1903, the westernmedical science had failed to preventthe disease. The indigenous practiceshad hegemonic challenge to deal withthe western medicine in Odisha. Insome cases, the Kalazar disease wassuccessfully treated by traditionaldoctors. Through the process ofcolonization of Odisha modernmedicine compelled the indigenouspractitioners to rethink about theirown system. Institutionally theprocess was revived by the westernscholars. However, the greatestobstacle for the survival and spread ofindigenous medicine was strongdislike on their knowledge to theKaviraj and Vaidyas to pass on theirknowledge to the upcominggenerations (Tahir, 2013. P-4).
Another scholar in history, SamuelLimma50 provided an interestingreading on probing Small pox andCholera in Mayurbhanj district during1905 to 1960. The scholar has made aneffort to explore the public healthscenario of the people and probinghow the colonial public health systemfunctioning in the specific disease andparticular region, e.g. smallpox51 andcholera52 in the context of a tribal
50 Limma, S. 2015. People and Public Health: Probing Smallpox and Cholera in Mayurbhanj ofOdisha, 1905-60, Odisha Review, October 2015. P. 60-65
51 The disease is also known by the Latin names Variola or Variolavera, derived from varius(³spotted´) or varus (³pimple´). The last naturally occurring case of smallpox (Variola minor)was diagnosed on 26 October 1977
52 Cholera is an infection of the intestine by the bacterium Vibrio cholerae. This may result insunken eyes, cold skin, decreased skin elasticity, and wrinkling of the hands and feet. Thedehydration may result in the skin turning bluish. Symptoms start two hours to five days afterexposure

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1914
region like Mayurbhanj of Odisha.Mayurbhanj was a princely statebefore merging with the Indian stateof Odisha in 1948, it was situated onthe south of the then Chhotnagpurregion, on the south-west of Bengaland north of Odisha Province. Thenorth-west region is covered bySimilipal mountain area. Majority ofthe people of this region belong toSanthal tribal community, the peopleof this community is living both in thehill and plain areas.
Sitala or Sital Puja during the monthsof April-May is a tribal ritual innorthern Odisha that is conducted tosecure overall well-being of thecommunities from dreaded diseasesand epidemics. The small pox was aknown epidemic of the past and itstreatment means appropriate actionsto cool down (sitala) the anger andwrath of the malevolent spirit whoinflicted the disease. The Ayurvedictexts also provide evidences to theprocesses and practices related to sitalaas a treatment to cure fever duringsmall pox. The term sitala had beenused in Bhavaprakasha in connectionwith the cold treatment for the feverthat accompanied smallpox53. Thegoddess Sitala Devi54, it was believed,
53 Ramanna, M. Western Medicine and Public Health in Colonial Bombay: 1845-1895, OrientLongman Private Limited, New Delhi, p.125-126
54 Arnold, D. Colonizing the Body: State Medicine and Epidemic Disease in Nineteenth CenturyIndia, University of California Press, Berkley, p.125
55 Bhattacharya, S., Harrison, M., Worboys, M. 2005. Fractured States: Smallpox, Public Healthand Vaccination Policy in British India 1800-1947, Orient Longman Private Limited, New Delhi,p.1
56 Ray, K., 1998. History of Public Health: Colonial Bengal 1921-1947, KB Bagchi & Company,Calcutta, 1998, pp. 61, 62.
made her presence known througheruptions and to thwart her was toincur her displeasure. She wastherefore pacified by cooling offerings.To counter smallpox, inoculation hadlong been in use in India (Ramanna,p. 126).
Smallpox epidemics were customarilytreated as major events in South Asia,receiving the attention of the rulingelites, government agencies, medicalpractitioners, civilian commentatorsand ordinary people. The diseaseevoked widespread fear, and it isimportant not to ignore this fact.British officials in colonial India wereaware that smallpox could transcendracial and geographical barriers, evenif they were often unsure about whythis was so55.
Cholera known as mainly a water-borne disease, originated in India. Itwas one of the most frequentepidemics in eastern India. In India,the occurrence of cholera wasattributed to the wrath of the choleradeity for violation of Hindu religionby slaughtering cattle for feedingBritish troops camped in a sacredgrove56. The modern history of cholerabegins from 1817 when it first attracted

15IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
attention by its fearful ravages inJessore57 and soon ran its pandemiccourse within two years over thewhole world. The report 1920 on thenature of this disease, prepared by DrJames Jameson in compliance with theorders of the Indian Government,proved that cases of the so-calledcholera morbus had been known toend fatally (Ray, 1998, p. 62).
Both the two diseases smallpox andcholera were significant because thepeople unusually and unknowinglysuffered in large numbers. Thecolonialists partially succeeded tocheck the fatal diseases, then the freeIndia government also applied thesame policy which is prevalent tillnow.
The paper presents accounts on theresults of simultaneous occurrence oftwo epidemics - Small pox andCholera in Mayurbhanj district. Basedon archival official data the paperfinds three major periods when theSmall pox outbreak happened inMayurbhanj i.e. during 1904-05 to1919-20; during 1925-26 to 1934-35,and during 1955-56 to 1960-61.Similarly, the outbreak of Cholera intwo major periods i.e during 1904-05to 1910-11, and during 1995-96 to 1960-61. The last naturally occurring caseof smallpox (Variola minor) wasdiagnosed on 26 October 1977. The
epidemic could be controlled byextensive vaccination andprophylactic measures. During thespread of epidemic when the Colonialgovernment faced problems ofoutreach to cure the patients, itindirectly encouraged application oflocal medicines – Ayurveda and folkmedicine prescribed by the Kaviraj andtribal folk-healers. The recompilationof data presented in the paper has beencited here to understand the gravityof the situation in Mayurbhanj duringthe visit of the two epidemics. The dataindicates that the Small Pox hadattained its peak in 1934-35 while theCholera attained peak in 1908-09 withcorresponding highest deaths in thesaid years.
57 Jessore is a district in the southwestern region of Bangladesh. It is bordered by India to thewest, Khulna District and Satkhira District to the south, Magura and Narail to the east, andJhenaidah District to the north.
58 Nayak, P., Sodha, S.V., Laserson, K.F. et al. A cutaneous Anthrax outbreak in Koraput Districtof Odisha-India 2015. BMC Public Health 19, 470 (2019). https://doi.org/10.1186/s12889-019-6787-0
The author argues that ‘during theperiod under study both in thecolonial and post-colonial period, thehealth scenario remained same likeuneven advance both under thecolonialists and post-colonial timeseven in the two five-year plan periods.It is really no doubt that vast numberof lives could be saved due to theBritish medical or health care policy.But the health scenario had notchanged phenomenally over theperiod and also even after 1947’.
A similar study on Anthrax outbreakin Koraput region has been publishedby Nayak et.al.58 in their article on ‘A

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1916
Source: Samuel Limma, 2015
cutaneous Anthrax outbreak inKoraput District of Odisha-India2015’. The study reported on acutaneous anthrax outbreak mostlyamong males in a tribal community ofKoraput district, Odisha. Thiscommunity has a history of recurrentanthrax outbreaks that occurseasonally, from April to June.Investigation by the authorsdemonstrated clustering of humancases in areas of animal deaths withhuman illness strongly associatedwith eating and handling the carcassesof ill cattle, low vaccination coverageof livestock and inadequate carcass
disposal practice in affected sub-districts likely contributed to theoutbreak and to the ongoing risk in thecommunity.
The study states that ‘Anthraxcontinues to be enzootic in under-developed areas of the world lackingadequate preventive measures. Rapiddiagnosis, isolation, treatment withantimicrobials and other adjuvanttherapies among human anthrax casesand measures against transmission areessential to minimize diseaseprogression and to help controloutbreaks quickly and effectively.

17IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
With 1% prevalence of culturepositivity among outbreak householdcattle, Koraput district has endemiclivestock anthrax and inadequatevaccination coverage; these factorslikely contribute to continuoustransmission of anthrax in this region’.
Further, socio-cultural practices suchas slaughtering of sick animals, eatingor handling meat from infectedanimals, and dumping of deadcarcasses in the open have contributedto anthrax transmission in outbreaksreported from Africa and SoutheastAsian countries. Scavenging carcassmeat for consumption is culturallyacceptable to some of the local tribesin Koraput district and is associatedwith anthrax transmission. Low socio-economic status and poor educationof the tribal community combinedwith poor public health infrastructurecreates a synergy of risk factors thatare conducive for zoonotictransmission of anthrax to the humanpopulation. Increasing the tribalcommunity’s awareness about riskfactors for illness may help avertfuture outbreaks. As part of theresponse to this outbreak, healtheducation camps were organized tosensitize the community on behavioralchange for anthrax prevention. All thevillagers were educated throughsimple health messages from thecommunity health workers such as“not to handle the sick animal withoutprotection,” “safe disposal of deadanimal with disinfection,” “not toconsume raw meat,” “cook it wellbefore eating,” etc.
According to the study, in previousoutbreaks, delayed reporting of illpersons and poor communityawareness about the illness wereimportant risk factors for continuedtransmission of infection.Furthermore, unreported livestockdeaths and seasonal variation ofanthrax transmission in the districtmay also contribute to the persistenceof outbreaks. Lack of anthrax culturecapacity or other diagnostic methodsin the district laboratory limitsdetection of anthrax in animal, humanand environmental samples. There isneed to strengthen the laboratorysurveillance system at the district levelboth for animal and human health,and the building of a more reliablesample transportation andcommunication system. The lag-phasebetween reporting of the outbreak andthe specimen sample collection oftenleads to delayed diagnosis andconfirmation of the outbreak.
The study also provides insights formanagement of the outbreak ofepidemic. After outbreak detection,enhanced skills in field epidemiologyare necessary for rapid response andthorough investigation. India isactively working toward improvingepidemiologic capacity quantitativelyand qualitatively. In 2012, the IndiaEpidemic Intelligence Service (EIS)programme was launched by India’sNational Centre for Disease Control,Delhi in collaboration with the UnitedStates Centers for Disease Control andPrevention. This 2-year intensivetraining in field epidemiology aims toincrease the number of public health

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1918
professionals with specialized skills toinvestigate outbreaks with analyticalepidemiology. This outbreakinvestigation was led by an EIS officerand demonstrates the benefit ofapplying these skills in India to betterunderstand active public healthproblems and guide evidence-basedinterventions.
The authors provide to understand thatthe epidemiology of anthrax involveshuman, animal, and environmentalhealth. The One Health approachintegrates and synergizes these multipledisciplines toward disease control andprevention strategies of zoonoticdiseases such as anthrax. The authorsused this outbreak investigation as anopportunity to strengthen the inter-sectoral coordination between thehuman and animal health departmentsin the district. After the outbreak wasidentified among human cases, theanimal health department was engagedto trace the tracks and hides of infectedanimals, treat infected animals, andimmediately destroy dead carcasses.While surveillance for human cases wasongoing, the dispatching andtransaction of livestock from the areawas stopped. Such coordinationbetween animal and human healthdepartments, as is promoted under theGlobal Health Security Agenda, willfacilitate early case detection, control,and prevention of zoonotic diseaseoutbreaks in the future, the authorsopined.
Adding to the above, the authors are
of the view that seasonality of anthraxoutbreak is a complex phenomenon.Several studies have hypothesizedthat seasonality, climate conditionsand/or human activities areassociated with anthrax outbreaks, butthere is minimal evidence about theirassociation. However, outbreakpatterns vary from region to regionbased on the diverse predisposingenvironmental conditions existing inthe area. The majority of the anthraxoutbreaks in India are reportedbetween the months from Septemberto January (post-monsoon). Incontrast, the investigation of historicalanthrax cases in Koraput showed apredominance of cases occurring fromApril to June (pre-monsoon). Anthraxis a re-emerging disease of publichealth importance in India. Livestockvaccination, surveillance for early casedetection, and education among thecommunity regarding animal tohuman transmission and carcassdisposal is crucial for prevention,detection, and control of outbreaks.The vaccination strategy of animalsshould expand to larger geographicareas with more comprehensive goalsto vaccinate more livestock andvariety of livestock.
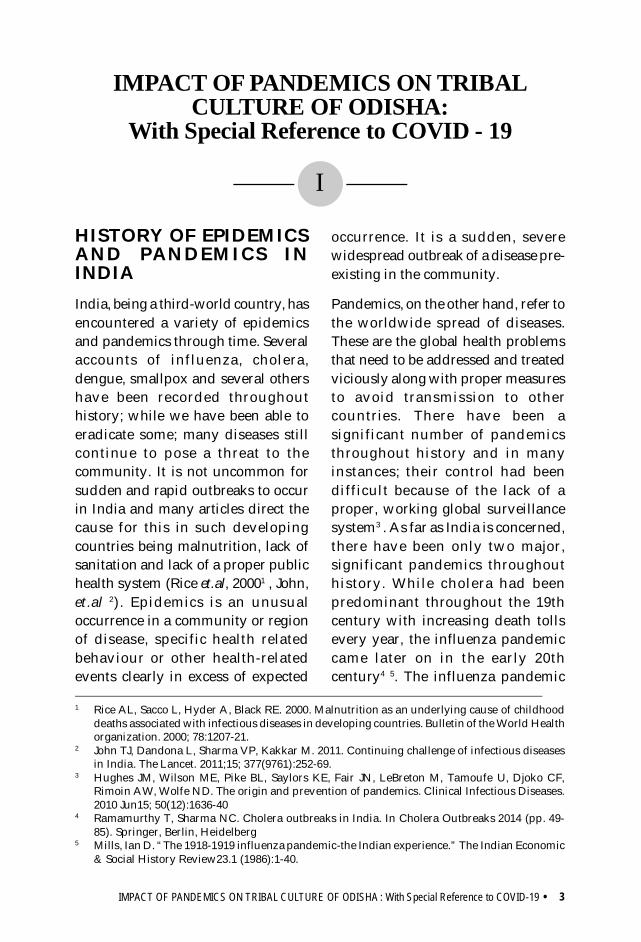
I.G.K. Menon, the then DeputyDirector of Pasteur Institute atCoonoor in India reported the Asianinfluenza pandemic59 during 1957-58.According to him, Asian influenzaappears to have reached India viaMadras in May 1957. The main
59 Menon, I. G. K. 1959. The 1957 Pandemic of Influenza in India. Bull. World Health Organization.20, 199-224

19IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
pandemic wave swept through thesubcontinent within the next 12weeks; cases occurring thereafterrepresent the permanent infiltration ofthe new virus into the population.Between 19 May 1957 and 8 February1958 there were reported 4,451,758cases, with 1098 deaths. The authorhas discussed the attack-rates by age-group, by occupational group, by Stateand in closed communities such asschools. The disease, in India aselsewhere, seems generally to haverun a mild course, although nauseaand vomiting and symptoms relatedto the nervous system were relativelyfrequently seen.
The paper provides a short history ofthe migration of the pandemic fromSingapur to India. The first intimationthat the influenza outbreak in South-East Asian countries such as Japan andMalaya were about to spread to Indiawas received at the Government ofIndia Influenza Centre at Coonoor on11 May 1957. It was decided to keep aspecial watch on the arrival of infectedcases at Calcutta and Madras and toisolate the virus from such cases.Information was received on 15 Maythat the S.S. Rajula, which had leftSingapore on 9 May with 1622passengers and about 200 crewmembers, had been directed toproceed to Madras instead of to its firstport of call in India, Negapatam, inview of an outbreak of influenza onboard affecting 254 persons in sevendays. On the ship’s arrival at Madrason the morning of 16 May it was foundthat there were 44 active cases ofinfluenza on board, four of them
showing temperatures above 103°F(39.4°C). The steamer was placed inquarantine at sea and was boarded bya medical team which examined all onboard and gave the necessarytreatment. A laboratory team fromCoonoor collected throat washingsfrom the patients. These specimenswere collected on 16 and 17 May andsent to Coonoor with adequatesafeguards for preservation and safetyin transit. The first isolation of thevirus from the cases from the steamerwas made on 22 May. The strain wassent to the World Influenza Centre inLondon and identified there as A/Asia/57 virus.
Four of the nurses who boarded thesteamer on 16 May came down withfever on 18 May, i.e., 48 hours afterexposure to infection. If this is takenas the first date of the epidemic inIndia, it can be stated that thepandemic was noticed in North Chinain January, Shanghai in February,Canton in March, Hong Kong in April,Singapore early in May and Madrasin mid-May, or the 20th week of theyear. Within six weeks from 18 May ithad spread all over India. In each area,the pattern was one of sweepingspread through the most crowdedcapital and other cities, followed by arelatively slow spread across villagesand other towns.
The maximum spread of the epidemicappeared to take place in the 23rdweek (2-8 June). In the same period,along with other cities in the Southernand Northern States, Sambalpur inOdisha was worst affected. The main
IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1920
wave of influenza would thus appearto have swept across the countrywithin a period of 12 weeks ending on10 August 1957.
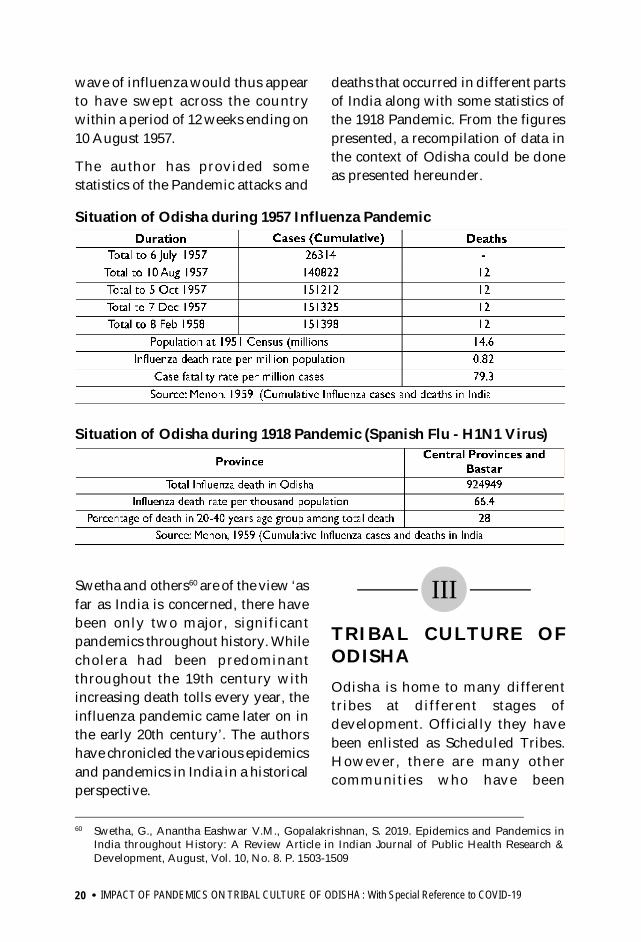
The author has provided somestatistics of the Pandemic attacks and
deaths that occurred in different partsof India along with some statistics ofthe 1918 Pandemic. From the figurespresented, a recompilation of data inthe context of Odisha could be doneas presented hereunder.
Swetha and others60 are of the view ‘asfar as India is concerned, there havebeen only two major, significantpandemics throughout history. Whilecholera had been predominantthroughout the 19th century withincreasing death tolls every year, theinfluenza pandemic came later on inthe early 20th century’. The authorshave chronicled the various epidemicsand pandemics in India in a historicalperspective.
III
60 Swetha, G., Anantha Eashwar V.M., Gopalakrishnan, S. 2019. Epidemics and Pandemics inIndia throughout History: A Review Article in Indian Journal of Public Health Research &Development, August, Vol. 10, No. 8. P. 1503-1509
TRIBAL CULTURE OFODISHAOdisha is home to many differenttribes at different stages ofdevelopment. Officially they havebeen enlisted as Scheduled Tribes.However, there are many othercommunities who have been
Situation of Odisha during 1957 Influenza Pandemic
Situation of Odisha during 1918 Pandemic (Spanish Flu - H1N1 Virus)

21IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
advocating in favour of their inclusionin the list of Scheduled Tribes. Eachtribe possesses its distinct identity interms of social organization, cultureand language. The tribes in Odisha aresort of territorially bounded units. Intheir life style, beliefs, values andworldview each tribe differs distinctlyfrom the other. Similarly, many tribesspeak their own language and sometribes have their own scripts, forexample, Ho, Kondh, Santal andSaora. The script of the Santals havealready been included in the 8 th
schedule of the constitution.
The tribal people in Odisha have theirdwellings on hills and plains orfoothills, in linearly fashioned orscattered habitations. The dualism inhabitation is important for anunderstanding of social, cultural andlinguistic variations. Similarly,geographic location, physiographiccondition of living, degree of isolationand exposure to the outer world andmainstream society are other factorsimportant for understanding variationamong the different ethnic groups orscheduled tribes.
There are individual tribes havingethno-cultural variations. In otherwords, there are ethnic groups whohave many sub-groups with distinctvariations among the sub-groups. Forexample, the tribe Kondh has sub-tribes such as Kutia Kondh, DongariaKondh, Malia Kondh, Penga Kondh,etc. and the tribe Saora has sub-tribessuch as Lanjia Saora, Arsi Saora,Shudha Saora. Taking the sub-groupstogether, the Kondh and the Saora arefound as numerous in the state.
3.1 Cultural variations amongtribes of Odisha
All the tribes in Odisha exhibits theiruniqueness in identity through manycultural chaacteristics that aredifferent from each other. One of suchcharacteristics is the settlementpattern. The Dravidian tribes such asKondh have linear housing pattern ina settlement, arranged in rows ofhouses. The different sections ofKondhs such as Dongaria Kondh,Kutia Kondh, Malia Kondh, PengaKondh do have a linear pattern. Thealignment and orientation of anyKondh village in relation to the shrineof Earth Goddess (Dharni) and SunGod is almost same everywhere. Theshrines dedicated to the two deities arecentrally located within the settlementplaced linearly between two rows ofhouses. All the sections of Kondhsfollow one basic model although theyexhibit variations to a certain degree.Excepting the Kondhs, most othertribes exhibit scattered settlementpattern where the houses are foundspread out and keep distance fromeach other. For example, the Mundaspeaking tribes have scatteredsettlement structures. Each Mundaspeaking tribe maintains its ownstructural arrangements. Thevariations noticed among them couldbe due to cross cultural influences,convergence and divergence. Thearchitectural plans of houseconstruction are also different fromtribe to tribe. Tribes like Bonda,Dongaria Kondh, Juang, Gadaba,Koya, Lanjia Saora, Santal etc. exhibittheir distinctiveness in clothing,

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1922
adornments, hair style. From the verylook of a man’s wear or woman’s wearone could know which tribe he or shebelongs to. Nevertheless, each tribehas its own peculiarities.
The tribes of Odisha pursue theirsubsistence economy in a variety ofways by means of small-scaletechnologies which vary from tribe totribe. While some subsists on shiftingcultivation or slope agriculture, someothers depend on settled ricecultivation and pastoralism and a fewother maintain a nomadic or semi-nomadic life style, who mostly subsiston food gathering. Significantvariations are noticed in each mode ofsubsistence. For example, the practiceof shifting cultivation by Juang differsfrom that of the Lanjia Saora andDongaria Kondh. The practice ofsettled rice cultivation and pastoralismof Gadaba differs from that of Koya.In their tools and technologies thereare significant variations too.However, most of the tribes in Odishadepend on a substantial degree uponforest collections and tree products.The women in tribal societies hold thekey to their economy.
The sixty-two scheduled tribesinhabiting Odisha can be broadlyclassified into three ethno-linguisticgroups, such as, Munda (Austro-Asiatic), Dravidian and Odia (Indo-Aryan). Twenty-six of the saidscheduled tribes are Munda speakers.The STs included are Bhumij, Birhor,Bondo Paroja, Desua Bhumija, Didayi,Gadaba, Ho, Juang, Kharia, Kol, Kol-Lohara, Kolha, Kora, Korua, Lodha,
Mahali, Mankidi, Mankirdia, Mirdha,Munda, Munda Lohara, Mundari,Parenga, Santhal, Saora/Savar/Saura/Sahara and Shabar Lodha. Thelist of Munda dialect spoken by thetribes are Birhor (Mankidia), Gata(Didayi), Gorum (Parenga), Gutob(Gadaba), Ho (Ho, Kolha), Juang,Kharia (Kharia, Mirdha), Koda, Mahili(Mahali), Mundari (Munda), Remo(Bonda), Santali and Sora (LanjiaSaora, Juari, Arsi), Korwa, Bhumija.
Fourteen scheduled tribes such asChenchu, Dal, Dharua, Gandia, Gond,Jatapu, Kandha Gauda, Kondh, Kisan,Konda Dora, Koya, Madia, Oraon andParoja are Dravidian speakers. TheDravidian dialect spoken by the tribesare: Parji (Dharua), Koya, Kui (Kondh,Kutia Kondh), Kuvi (Dongaria Kondh,Konda Dora, Jatapu), Ollari (section ofGadaba), Kurukh/Oraon (Oraon),Gondi (Gond), Madia, Pengu (PengaKondh) and Kisan.
As many as twenty-two scheduledtribes are Odia speakers. They includeBagata, Baiga, Banjara/Banjari,Bathudi, Bhottada/Dhotada, Bhuiya/Bhuiyan, Bhumia, Bhunjia, Binjhia,Ghara, Holva, Kawar, Kharwar, Koli/Malhar, Kotia, Kulis, Matya,Omanatya, Pentia, Rajuar, Sounti andTharua.
The tribal communities differ fromeach other in respect of certain socio-cultural practices, religious beliefs,values and mores. In many casescultural affinities do exist in processes

23IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
and practices but their interpretationsmake the difference. Their worldviewand philosophy of life in a given socio-ecological complex also differs inmany respects. The tribal communitieswho are in transition betweentradition and modernity and reside inrelatively mainstream localities differsignificantly with the tribalcommunities who live in remotepockets. These differences are markedmost in the context of maintaining thetraditional socio-cultural practices. Itis, however, commonly seen that thetraditional religious beliefs andpractices continue to be there with allthe tribes. The tribal communities whohave accepted other religion aredifferent in this consideration. Withinthe same community, the oldergeneration have been following theirtraditional beliefs and practices whilethe younger generation have beenfollowing dictates of the other religionthey have accepted. The religion is animportant aspect of tribal culture andis deeply related to their worldviewand philosophy of life.
To understand the tribal religiousbeliefs and practices the variousrituals and festivals provide the bestopportunity. The tribal religiousrituals and festivals are seasonspecific and very much linked to theirsubsistence setting. Since, almost alltribal communities subsist on landand forest-based livelihoods, their
calendar of rituals and festivals fallsat phases of agricultural operations,forest collections, and other workactivities. If one tries to build acategorization of the rituals andfestivals in consideration to thesubsistence related work activitiesand other economic pursuits then itwould appear like - rituals andfestivals before starting agriculturalactivities, during the intermittentharvests, final harvest and post-harvest. By and large, major ritualsand festivals falls during these stagesof agriculture that showcase thereligious beliefs and practices, theirtheology and eschatology. The life-cycle rituals may come up any time.Over the years, there have been manychanges in the religious beliefs andpractices of the tribal communities.Certain rituals and festivals of thegreat traditions (Hindu religiouspractices) have been adopted by thetribal communities and have beenincorporated in their ritual calendar.The ritual calendar of the tribalcommunities has been presentedhereunder for an understanding ofthe seasonality, typology andimportant practices involved in theirsocio-cultural processes. It providesa reference to examine what ritualsand festivals have been affectedduring the official restrictions due toCOVID-19.

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1924
3.2 Ritual calendar of tribes of OdishaTribe Ritual/ Festival Timing Description Bagata Dussera Sept-Oct Worshipping of fishing basket and trident Baiga Chaita Navami Mar-Apr Perform shaill dance wearing wooden mask
Banjara Guru Navami Sept-Oct Worship performed by Brahmin priest
Bathudi Dussera Sept-Oct Dehuri/Guru perform worship, sacrifice goat, cocks
Raja June Festival without worships
Bhottada
Chaita Parab Mar-Apr Pujari worships earth goddess and sacrifices goat, sheep and fowls for soil fertility and bumper harvest.
Amba Nuakhia Apr-May Pujari offers worship and sacrifices to earth goddess Nuakhia Aug-Sept New eating of rice Dussera Sept-Oct Worships and sacrifices conducted
Bhumia Balijatra Mar-Apr Disari sacrifices goat during fertility rites. Young girls dance and trance as a medium for the sprit called Debata. Village deity Budhi Thakurani worshipped.
Bhumij
Dhulla Puja Apr-May For well-being of village
Karama Aug-Sept Naya/ Dehuri performs the ritual for prosperity of the village
Bandna Parab Oct-Nov New eating ritual
Binjhal
Maghaparab March Dongar Debata is worshipped with fowl, goat sacrifice Mahulbhaja Parab/
Chaita Parab Mar-Apr First eating of Mahula flowers. Village deity, forest deity worshipped with sacrifices
Haral Parab Jul-Aug Ancestor worship for welfare of the children by keeping unboiled rice and milk at their feet
Karama Aug-Sept Jhankar worships Karamasani deity for good fortune. Badakarama is observed in every three years in which un-boiled rice, milk, sweets and liquor are offered
Puspuni/ Madhen Parab Dec-Jan Village deity is worshipped with rice, pulses and animal
sacrifice
Binjhia Karama Aug-Sept Kalo worships the village deity, Gramsiri and sacrifices cocks and goats before the deity
Mankirdia
Maka Parab/ Magha Parab Jan-Feb
Dehuri conducts rituals. Fowls are sacrificed. Supreme deity Sing Bonga (Sun God) and the village deity (Dasauli) are worshipped at Zaheera.
Hero Jan-Feb Dancing and merry making Baha/ Chaita Parab Mar-Apr Ritual for first fruit of Mahua and ceremonial hunting
Chuktia Bhunjia
Vimsen Puja Mar-Apr Fowls are sacrificed, wine is offered before the deity for bumper Mahua flowering
Mati Puja Sept-Oct Buck, fowls and pig are sacrificed for bumper crop
Dussera Oct-Nov
Pujari (priest), Kataria (sacrifice executant) and Chhataria (umbrella holder) worship Goddess Suna Dei. Bucks and parrots are sacrificed for good agriculture and prosperity of villagers
Dharani Puja Nov-Dec Buck sacrificed for preventing illness of all kinds
Dal
Mati Jatra/ Penchhada Puja May-Jun
Earth Worship. Brahmin worships under a Tulsi plant in the middle of village
Asadhakhai Jun-Jul Communal worship in village and then at forest
Puspuni Nov-Dec Bhoi/ Jani/ Bisal sacrifice fowls before home deities of all households
Dharua Lendipanda Jan-Feb
Palasi (village priest) sacrifices fowls, goats, pigs etc. before Birbu (Earth) goddess at the beginning of agricultural cycle. First eating of Mahua
Ghia Panda Apr-May Annual hunting ceremony
Dongaria
Meria Mar-Apr Ritual with buffalo sacrifice for well-being of people, fertility of soil, health and happiness of villagers
Bihan Puja Mar-Apr Ritual for sowing seeds

25IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
Dongaria Kondh
Bihan Puja Mar-Apr Ritual for sowing seeds Ghantaparab Apr-May For fulfilment of wants Mandiarani Jul-Aug For good harvest of Ragi
Dhan Nuakhia Aug-Sep First rice offering to village deity Pidika Sep-Oct Bumper crop of castor seeds
Punapadi Oct-Nov First eating of red gram, small millets and jawar
Gadaba
Chait Parab Mar-Apr No work. Merry making. Ceremonial hunting ritual
Bandapana Parab Jul Disari sacrifices fowls before Thakurani – village deity represented by a stone slab at Hundi (shrine)
Dussera Sep-Oct Disari performs worship to Thakurani Pus Parab Dec
Gond Chaita Parab Mar-Apr
Devaril (village priest) and Katora (clan priest) sacrifice pig and fowls in the rituals like worship of Akipen (village god) and Auwal (mother goddess) during first eating of new crops and for successful germination of seeds before sowing new millets. Blood of the sacrificed animal is sprinkled over the seeds and the charmed seeds offered to gods are sown in the fields for good harvesting.
Hill Kharia
Makar Sankranti Jan Ancestor worship. Take holy dip in the hill streams. Gather around fire and eat cake.
Bhandar Puja Jan-Feb Worship the village deity and Bhandar Thakurani with sacrifice of goats and fowls for good honey collection. Make community feast, perform songs and change dance.
Ho Maghe Jan-Feb
Supreme deity Sing Bonga and village deity Dasauli worshipped at Jaheera by Dehuri. Along with this, other festivals of the year like Baha, Damurai, Heru, Jamnama, Kolon, Batauli are also performed in similar manner. All festivals are associated with agricultural operations.
Holva Chaitra Parab Mar-Apr Pujari worships during new mango eating ceremony
Amus Aug-Sep New rice eating ceremony
Jatapu Pongal/ Pondugu Jan Disari officiates in social functions and Jani worships the
village deity.
Bhagudi Mar-Apr Worship with sacrifice of fowls, pigs and goats is offered to Jahar – supreme deity and Jakeri goddess.
Juang
Amba Nua Mar-Apr Dharam Devata (Sun God), Basumata (mother earth) and Gramsiri (village deity) are worshipped
Dhan Nua Aug-Sep The gods and goddesses are worshipped
Pus Punei Dec-Jan Nagam or Dehuri sacrifices a pig and sprinkles its blood over the grains for good germination
Kawar Dussera Oct-Nov Worship double edged sword (Jhagna Khanda) and swords of strife
Kisan
Bihanbuna Apr-May First sowing of seeds Gamha Jul-Aug Installation of Kendu twigs in crop fields Nuakhai Aug-Sep Eating new rice Dussera Sep-Oct Worshipping village deities
Pius Punei Dec-Jan Ancestor worship with dance and merry-making
Kol
Magha Pudi, Jamnam, Jan-Feb Post harvesting ritual, eating new rice
Makar Jan Ancestor worship Baparaba Mar-Apr Eating new mango, jackfruit
Phulbanguni May-Jun Use of sal flowers Asadhi Jun-Jul Ritual for agriculture Gamha Jul-Aug Ritual for cattle health
Kol Lohar
Makara Jan Deities offered with sacrifice of animals and birds through rituals at village shrine
Nuakhai Aug-Sep Ancestor worship, eating new rice and community feast
Karama Sep-Oct Well-being of people, dancing, drinking and enjoying special foods
Konda Dora
Makara Jan-Feb Ancestor worship Dussera Sep-Oct Sacrifice of animals and birds at village shrine
Dhan Nuakhia Oct-Nov Eating new rice Dussera Sep-Oct Sacrifice of goats, sheep and fowls at village shrine

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1926
Kora Dussera Sep-Oct Sacrifice of goats, sheep and fowls at village shrine Pus Punei Dec-Jan Post-harvest ritual
Koya
Bhimpandu Jan-Feb Worshipping of rain god and seeds consecration
Bijapandu Apr-May Mango eating festival. Worship earth goddess and offering sacrifice of fowls, pigs and eggs
Kurumpandu Aug-Sep Ritual for first eating of minor millets Dussera Sep-Oct New eating of rice
Kutia Kondh
Karu Biha Dakina (Meria) Feb-Mar Buffalo sacrifice to Dharani Penu
Chait Parab Mar-Apr Ceremonial hunting Taka Kalu Jul-Aug Ritual at swidden for bumper crop
Puni Kalu Dec-Jan Post-harvest ritual at village shrine, merry making enjoying Katul drink
Lanjia Saora
Udan abdur Mar-Apr Ritual before village deity for mango new-eating Tankuna Abdur Jun-Jul Storing mango kernel
Osana abdur Jul-Aug New eating of minor millet Rogan abdur Nov-Dec New eating of red gram
Lodha
Sital Puja/ Nateunhanri Apr-May
Sacrifice of animals and birds to village deity. Annual ancestor worship
Manas Puja May-Jun Seed sowing ritual Jathel Jul-Aug Ritual to protect cattle from diseases
Ashtami Puja Sep-Oct Offering sacrifice to gods and goddesses at village shrine Bandana Puja Oct-Nov Rice new eating ritual
Mahali Maa-mane Jan-Feb Ritual for harvesting and using new fruits, leaves, wild
grass for thatching and collection of wood Baha Feb-Mar Naya worships the village Pirha for welfare of the village Sharai Oct-Nov Naya sacrifices fowl at village outskirts
Malhar Makar Jan-Feb Ancestral worship
Munda Karama Sep-Oct Well-being of people, dancing, enjoying feast Sarhul Oct-Nov Reaping of paddy by magico-religious head
Omanatya Amnua Mar-Apr New eating of mango
Akhi Muthi Apr-May Pujari offers ritual for sowing seeds Pus Purnima Dec-Jan Post-harvest ritual
Oraon
Fagu Feb-Mar Naega offers sacrifice before village deities Chaita Parab Mar-Apr Merry making
Sarhul Apr-May Ritual for using sal flowers Bisu shikar Aug-Sep Ceremonial annual hunting
Karama Aug-Sep Ritual before village shrine
Parenga Chaita Parab Mar-Apr Worship Nangasery and offer goat and fowl sacrifice
before proceeding for annual hunting Bandapana Jul-Aug New eating of pumpkin leaves Puspunei Dec-Jan Offering sacrifice to cattle god
Paroja
Chaita Parab Mar-Apr Annual ceremonial hunting Bihanthapa Apr-May Seed sowing ceremony
Asadhi Parab Jun-Jul Ritual to protect cattle from diseases Langaldhua Jul-Aug Ritual for consecration of agricultural implements Bhadparab Aug-Sep Eating of new rice
Pentia Ambanua Mar-Apr Mango new eating
Nuakhia Aug-Sep Eating of new rice. Disari sacrifices a goat before village shrine
Rajuar Makar Jan Ancestor worship and community feast Karam Aug-Sep Ritual before village shrine
Nuakhia Aug-Sep Eating of new rice
Santal
Magha-sim Jan-Feb Dancing and merry making Baha Mar-Apr Ritual for first eating of Mahua and ceremonial hunting
Erok-sim May-Jun Seed sowing ritual Hariham-sim Jul-Aug Ritual at the time of sprouting of seeds Iri-guldi-sim Aug-Sep Offering minor millets to deities
Saharai Nov Cattle worship Jantal Dec-Jan New eating of rice

27IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
The annual cycle of rituals of the tribesis in tune with the cycle of economicactivities, and surrounded socio-economic interests and well-being ofthe tribal communities. A ritual isprescribed order for performing aconcatenation of rites, and a rite is atraditional performance to whichconventional symbolic meaning isattached by those who believe in it.The rituals are commonly but notalways ceremonial in nature. A ritualbrings human beingsinterrelationships with gods, ancestralspirits, and other supernatural entities.Rituals, indeed, make overt religionand er-enact the interrelationshipsbetween cosmographical,supernatural and social worlds.
Fixed and recurrent group rites whichhave nearly equal significance for allor most members of the social groupin which they are performed rangefrom familial ceremonies to thosewhich apply to whole societies. Thetime of observance of these rites iscorrelated with the rhythmic cyclicalchanges in nature. Indeed many ofthese rites follow the annual cycle ofseasons vis-à-vis the positions of thesun and the moon in the zodiac duringa calendar year. Among the tribes ofOdisha, excepting those that areHinduized (Example: Raj Gonds,Rajkuli Bhuiyans, Desia Kondh,
Bathudi, Bhumij, Mirdha, and OdiaJuangs) observance of daily, weeklyand monthly rites is almost nil. Mostof the rituals of the tribes are seasonaland annual.
As most of the tribes of Odisha,practice agriculture in some form orthe other, and as rest others have avital stake in agriculture, sowing,planting, first fruit eating and harvestrites are common amongst them. Theircommon cyclic rites revolve round thepragmatic problems of ensuring astable economic condition,recuperation of the declining fertilityof soil, protection of crops fromdamage, human and livestock welfare,safety against predatory animals andvenomous reptiles and to insure agood yield of annual and perennialcrops.
The annual cycle of rituals commenceright from the initiation of agriculturaloperation, for instance, among theJuang, Bhuiyan, Kondh, Saora,Gadaba, Jharia, Didayi, Koya andBonda who practice slope agriculturethe annual cycle begins with the firstclearing of hill slopes during theHindu month of Chaitra (March-April) and among others, it starts withthe first fruit eating ceremony ofmango in the month of Baisakh (April-May). All the rituals centering
Source: P.K. Nayak: Social, Cultural and Linguistic Variations in Tribal Odisha, in Tribes of Odisha,SCSTRTI publication
Saunti
Makara Jan Ancestor worship and sacrifice of fowls Raja June Ritual before village deity, dance and merry making
Gamha Jul-Aug Installation of Kendu twigs in crop fields Nuakhia Dec-Jan Rice new eating
Tharua Makara Jan Ancestor worship and eating of special food Randia Gamha Jul-Aug Ritual for cattle and enjoy special food

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1928
agricultural operation, first fruiteating, human, livestock and cropwelfare are observed by the membersof a village on a common date whichis fixed by the village headman inconsultation with the village priest.
Thus, the ideological system of all thetribes surrounds supernaturalism.The pantheon, in ost cases, consistsof the Sun God, the Mother Earth andlower hierarchy of Gods. Besides,there are village tutelaries, naturespirits, presiding deities and ancestralspirits who are also propitiated andoffered sacrifices. Gods and spiritsare classified into benevolent andmalevolent categories. A peculiarityof the tribal mode of worship is theoffering of blood of an animal or abird, because such proitiations andobservance of rites are explicitlydirected towards happiness andsecurity in this world, abundance ofcrops, livestock, plants andprogenies. Sickness is not natural toa tribal, it is considered as an outcomeof the machination of some evil spiritsor indignation of ancestral spirits orgods. Sometimes, sickness is alsoconsidered as the consequence ofcertain lapses on the part of anindividual or group. Therefore,riddance must be sought throughpropitiation and observance ofrituals.
The tribal festivals and rituals,excepting the life cycle rituals arespecific to seasons and work activities.The festivals and rituals, withreference to their ritual calendar maybe categorized under three mainseasons – Summer, Rainy and Winter.The summer starts with the month ofChaitra (March – April) when thetribals get ready to start theiragricultural production activities. Therituals conducted during this periodare commonly known as Chaita Parabor Benta Parab and different tribalcommunities celebrate their ritualsand festivals having different namesduring Chaitra (Mar-Apr) to Jyestha(May-June). In the rainy season manyfestivals and rituals are conducted bythe tribes of Odisha. Most of suchrituals are related to the stages ofagricultural operations. While most ofsuch rituals are conducted in themonths of June-July, e.g. Asadhi Pujaof most tribes, Mandiarani of Kondhs,certain elaborate rituals and festivalslike Karam in northern Odisha,Nuakhai in western Odisha areconducted during August-September.The Dussera, Kali Puja comes with thematuring of crops and the harvestfestivals starts from then to end withthe Pus Punei in the winter season.Almost all the tribe in Odisha conductharvest festivals in one way or theother.

29IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
IV
IMPACT OF COVID-19ON TRIBAL RITUALSAND FESTIVALSThe present description is based onobservations and peer notes on theimpact of the covid 19 on the ritualsand the festivals conducted by thetribal communities during the lockdown phases and the early unlockingtimes, more particularly, during themonth of April to July of 2020. Thefollowing narrations provide tounderstand the way Covid 19 affectedthe tribal life and culture during thestated period. Within the frame of timeand considering the limitations onphysical access for gatheringinformation from various nook andcorner of the tribal Odisha, theinformation is based on the notes frompersonal communications, newsitems, social media communicationsand such other indirect methods. Theunderstanding of the impact of Covid19 on the tribal life and culture is thusindicative and could not be illustrativeor detailed due to typical limitations.
The tribal rituals and festivals arescheduled with reference to Odiamonths and follows a lunar calendar.The cycle of rituals following Odiacalendar starts from Baisakh (April-May) with the beginning ofagricultural season and in that way theyearly ritual cycles end with the pre-agricultural season celebration ChaitaParab. With the end of the Chaita
Parab the agricultural activities takestart in full pace. This year, by theadvent of Covid in Odisha the tribalpeople had completed many post-harvest rituals that come betweenJanuary to March and were preparingfor grand celebration of Chaita Parab.Suddenly, the restrictions on groupactivities as a covid preventivemeasure came as a bolt in the blue tothe tribal communities. Before, theycould understand anything aboutCovid properly, they only understoodthat the government restrictions maynot allow them to celebrate the ChaitaParab in fun fare as they used to do inearlier years. The Chaita Parab insouthern Odisha is more elaboratecompared to any other part of tribalOdisha. For a month and more, themany tribal communities in southernOdisha stop working for anything butremain engaged in celebrating theParab, singing, dancing, enjoyingspecial food and by that feeling thecharm of life. The daily wagers, skilledlabours engaged on contract terms inthe unorganized sector, the migrantworkers, and street vendors almoststop working during the Chaita Parab.The Parab gives them the real feel ofgroup life, blissful life with kin andkith, refreshing memories of theircultural affairs and testing their skillsin fun filled ceremonial huntingexpeditions. The Parab brings with itthe humming of the young hearts inlove that in many cases lead to thenuptial ties. Chaita Parab means a lotto the tribal communities in southernOdisha irrespective of the differencesin terms of rich and poor, well-off orpoverty-stricken.

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1930
The Baiga celebrate Chaita Navamiwith grand fervour and by performingShaill dance wearing wooden masks.By coincidence, the Covid 19 arrivedin Odisha during that period and forthat many administrative restrictionswere imposed to prevent masscongregations in religious, politicaland other activities. However, this didnot affect the celebration of ChaitaNavami of the Baigas as on theoccasion everybody wore woodenmasks. Having the tradition ofwearing masks in Chaita Parab, it waseasy for the Baiga to adopt to maskwearing habit as a preventive measureto contain Covid. Baiga, being asmaller community in Odisha live inremote places away from regularofficial surveillance for which theCovid 19 restrictions made no bigdifference for them, especially inconducting their rituals and festivals.
The Bhottada community couldmanage to perform their Chaita Parabin small gathering maintainingreasonable social distance. Duringcelebration of the Parab the priestcalled Pujari takes the lead to performthe worship and sacrifice of goats,sheep and fowls requesting the godsand goddesses to bless them withbountiful agricultural productions.The Dishari followed by some othercommunity leaders performed ritualsat the shrine. However, communityfeast or such feastive gathering wastotally avoided with apprehensions ofPolice action prescribed under Covidguidelines and preventive procedures.
Balijatra and Budhi Thakurani Puja ofthe Bhumia community is celebrated
in the months of March to May. WhileBalijatra is conducted to seek theblessings of gods and goddesses forgood germination, adequate rainfalland bumper harvest from cropping,the Budhi Thakurani puja offered tothe village deity is considered aninsurance against the evil effects ofmalevolent spirits and to ensureoverall well-being of the villagers.While in the first occasion, sacrifice ofgoat is made, in the second oneusually no sacrifice or in certain casessacrifice of a fowl is made. During thisyear, due to the Covid restrictions therituals could not be conducted withmuch fun fare but were conducted inlimited version. The Bhumia believethat the Budhi Thakurani, the villagegoddess saves the villagers fromepidemics and ill-luck and hence herworship may never be neglectedunder any circumstances.
In the northern Odisha, the Bhumij arefound in numbers in various paprts ofMayurbhanj district. The communityobserved Dhulla Puja for the overallwell-being of the community and toget rid of the novel corona virus. Inmany villages the Dehuri performedthe ritual seeking blessings of thesupreme gods and goddesses to keepthe pandemic away from theirvillages. Certain rituals conducted aspart of Dhulla Puja in the sacredgroves Zaheera was intended to savethe villagers from the corona virus.The Mankidia community performedtheir Baha ritual during the early Aprilwhen they conducted the rituals butall the villages could not conduct theceremonial hunting. The Ho

31IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
community also conducted the Bihafestival as per their traditions.
The Mankidia permanent settlementsin rehabilitation colonies onlyrestricted themselves to theperformances at the Zaheera andcould not dare to go on ceremonialhunting apprehending that the mattergoes to the knowledge of police andproceedings to that effect may occur.However, the community memberswho had been camping in their makeshift huts in different places, especiallyin the remote areas of Mayurbhanj andSukinda of Jajpur district couldmaintain the annual ceremonialhunting as part of the celebrations.
The Juang festival of mango neweating and the Akshaya Tritiya wasimpacted to some extent. The festivalsare conducted at Pirh level. This yeardue to restrictions on Covid – 19, massgathering at the Pirh level wasavoided by the community leaders.The major impact, however, was seenon celebration of Raja festival whichis celebrated with pomp and show incommunities like Juang, PaudiBhuiyan, Bathudi and such othertribes residing in Keonjhar andMayurbhanj districts.
In the western Odisha also, there wasnot much impact on the rituals andfestivals conducted by the tribalcommunities in the early summerseason. The Chaita festival of theOraons were over in most of thevillages by the time the Covid – 19guidelines came into operation. TheKisan community members reducedthe grand worships of Bihanbuna to
the minimum and performed most ofthe rituals at the household level. Thepriests with one or two followersconducted the required rituals at theshrines and conducted rituals athousehold level too. After theBihanbuna ritual the tribal householdsmaintained their agricultural activitiesat their level.
Chaita Parab is a festival that iscelebrated by almost all ethnic groupsof the state. It is a time when thevillagers who had migrated out insearch of wages and fortune come backto their villages to integrate with theirfamilies or villagers. For about a monththe tribals in South Odisha live in afestive mood giving themselves a timeout from regular schedule of work. Thisyear the pandemic hit the Chaita Parabbadly. Their people who were workingelsewhere inside and outside the stategot stranded at different places andwere kept in camps. Bus, train and allother means of transport weredisrupted. Worries clouded both sides;the migrant labour in the camp and thelarger family in village.
On the other hand, rathercoincidentally, there are some inbuiltsystems in celebration of Chaita Parab,especially in South Odisha, thathelped implementation of theadvisories. Usually, temporaryblockades are put at village entrypoints where groups of tribal people,more commonly the women, gatherand demand ding dong from the by-passers and strangers to pass that way.One may plead stating that he doesn’thave a coin even to pay for the toll and

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1932
may kindly be allowed to cross theblockade, that is also grantedgenerously. This system, in the earlyhours of the corona spread, preventedthe entry of outsiders into the village,and even passing by the village inmany cases. This time the Chaita Parabblockade assumed to be of importancein blocking the entry of Corona intotribal villages.
Chaita Parab, that spans over about amonth, keep people in good humourwhen they do not work and enjoybeing together, cooking dishes athome, migrant workers probably tookleave from work contractors, peoplevisit their kith and kin in othervillages, fowls purchased out of theding-dongs make a group feast. Everyhousehold, be it relatively richer orultra-poor, therefore secure foodstufffor the month. This year it waswonderful. Sufficient food at home asthe government provided threemonths ration quota under publicdistribution system in advance as apreparatory towards preventingpeople going out in search of work andearning. The Anganwadi didi used tobe very particular about supplyingentitlements to women and children,old and disable expressed happinessover people around attending themthroughout the day, children invillages enjoyed with their peergroups. The young people in thevillage who usually were rushing totowns for mobile upload of romanticsongs had to remain engaged intraditional recreational activities in thevillage. The village life looked vibrantexcept for the fact that roaming around
was not allowed. The police force hadleast to enforce as the communitypolicing proved strong enough.
The Bonda, Bhotada, Bhumia, Kondh,Gadaba, Gond, Jatapu, Koya,Omanatya, Paroja are the major tribalcommunities in the South Odisha whocelebrate Chaita Parab in pomp andshow. The men, women, childrencome to the streets decoratingthemselves with leaves and twigs anddemand dongs from the passer-by.Children takes a refreshing timehunting crabs in the streams. Ritualsare conducted at the village shrinecalled Nisani Munda. As the eveningcomes the tribal tunes startreverberating when the communityfolks, especially in Kondh and Gadabavillages, engage themselves in the‘Sailodi’ dance that is very typicalduring the Chaita Parab. This year, theSailodi dance could not be performedas the community members submittedto the norms of social distancingimposed by the state administration.
In the similar manner, many ritualsand festivals that comes by the timeof late summer and early rains, e.gHaral Parab of Binjhal community;Matijatra, Penchhadapuja andAsadhakhai of Dal community;Ghanta Parab and Mandiarani ofDongaria Kondh community;Bandapana Parab of Gadaba, Parenga,Paroja and Kondh community; Asadhiof Kol community; Manas Puja andJathel of Lodha community;Langaldhua Parab of Parojacommunity and Hariham-sim ritual ofSanthal community. Personal

33IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
communications with contacts inthese communities reveals that therehas been no remarkable impact onconducting of the rituals and festivalsabiding by the norms of socialdistancing.
The Bandapana Parab that is quitesignificant for communities inKoraput region with reasonable socialgathering at village level did not faceany difficulty for the Covid. It is aritual when prayer is offered toMother Earth for a good crop. With theapproach of the rainy season, theDishari declares and schedules day forthe Bandapana Parab. Usually the dayis decided looking at the condition ofrain and crops in the fields. This year,due to scanty rainfall, the crops havenot grown well to the appreciablelevel. Despite that, the tribal Disharisconducted the ritual during themiddle of July. The crops that aregrown by the streams have grown welldue to availability of critical irrigation.Hence, the rituals have beenconducted in such fields without anyhassles as the fields remained awayfrom the surveillance of police andadministration for social distancingand other Covid norms.
Bandapana Parab has a specialsignificance. It is conducted at the timewhen the crops have grown to acertain height and require protection.The protection is meant as protectionfrom cattle and other herbivores andprotection from pests and insects.Hence, usually a fencing is madearound the fields and scare crows areerected in middle of fields during the
Bandapana Parab. These are activitiesthat by default maintains socialdistance. Hence, there was no issue ofCovid guidelines impacting thecelebration of the Parab. Special dishesare prepared at household level andno community feast is conducted.
The Parab was celebrated on differentdays in different villages. Thehouseholds collected branches ofKendu and Jamun trees from theforests and river sides. After dulyinvoking the respective gods andgoddesses they planted the branchesin the middle of their crop lands. Thereis a prevailing belief that by doing sothe crops could be saved from pestinfestations. Children in villages makedifferent types of effigy and put themon those branches as scarecrows. Thecrop fields showing such effigiesindicate that the Bandapana Parab hasbeen done. In many places in Koraput,the effigies could be seen in most ofthe crop fields by middle of July.Personal communications with manytribal community members indicatedthat in most of the villages the Parabwas celebrated during the week endswhen shut down was imposed inmany parts of the district.
Madan Krisani, belonging to Parojacommunity is a knowledgeable personon the tribal culture in the Koraputregion. According to him, in the tribaldances people usually cling to eachother in a chain. However, the Covidguidelines brought them someawareness as well as challenges toinnovate their dances. The dances likeDhemsa, Sailodi and other local forms

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1934
could be innovated in a manner so thatsocial distance between participantscan be well maintained. Usually,during the Chaita Parab all tribaldances are showcased in villages.However, this time there wasremarkable difference observed thisyear when the participants in a dancechain separated themselves from eachother and performed as solo dancers.
It seems, the Covid – 19 could notstrongly impact the conducting ofrituals and festivals except limiting itto performances at shrines andhousehold level without socialgatherings. Further, the spread ofCovid in the initial days remainedconfined mostly to the cities and henceit had little impact on the tribalcultural life in the remote pockets ofthe state.
In-built prevention measures incustomary and cultural practices
There has been ample publicity on theimportance of traditional healthcaresystems and their applicability incontaining Covid. Small notes in socialmedia circles provide to understandthat social, cultural habits arepreventing spread of Covid amongIndia’s tribals.
Many ground-level observations onthe way the tribal communities havebeen responding to Covid – 19Pandemic attest this. News articles,write-ups in social media circulations,interactions with tribal peopleindicates and highlights the use oftraditional herbs and medicines, aswell as the social distancing and
hygiene norms rooted in tribal culture,that have relatively kept them safefrom the coronavirus pandemic. Thecultural practices rather help intackling the disease and has proveduseful in contracting pandemic likeCorona (SIC), as the basic maintenanceof hygiene at home and workplacealong with the social distancing havebeen prescribed as the key behavioursto contain the virus. It also credited thewashing of hands with hearth ashes,leaving shoes outside the door, groupssitting with sizeable distance betweenindividuals and other habits of ruraland tribal culture for preventingCovid-19 infections. Administratorsand experts are also of opinion that thetribal way of life is built around socialdistancing, and people have becomemore vigilant about allowingoutsiders in.
According to local tribal leaders, thespread of Corona virus has happenedin limited scale in their areas becauseof two main reasons — the tribals’traditional way of life is conducive tomaintaining social distancing, and thegovernment has been proactive inspreading awareness about theprecautions necessary to combat thedisease. Tribal people have not onlyphysically resisted the entry ofoutsiders in their villages, but havealso voluntarily informedlocal anganwadi workers and healthdepartment officials to quarantinethose who returned to the villages andtried to enter their houses secretly.
Arrangement of houses maintainsocial distancing by default

35IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
There are tribal villages where thehouses are linearly arranged, e.gKandha with or without physical gapsbetween two houses. There are alsotribal villages where houses arelocated on a scattered manner, withone house located distantly from theother, e.g Lanjia Saora, Gond. In thecase of scattered houses, theboundaries are large enough to keepthe neighbours at a distance, unlikeurban residences or even modernvillages, where houses are bunchedtogether. In the case of housesbunched together or clinging to eachother, the families hardly cometogether inside the houses, exceptunder special circumstances likerituals and festivals. In both the casesthere is default social behaviour thatthe people do not intermingle in thehouses. Whether one see it as aphysical barrier or behavioural self-restraint, default social distancing iswell observed.
Social distancing in work traditionsas a customary behaviour
In their work traditions and also incasual daily life habits, the tribalsmaintain adequate physical distance.By habit they walk mostly in rows,instead of groups, and while walkingthey maintain reasonable distancefrom one another. According to SureshWadaka, a Dongaria Kandha of villageKhambesi under Kurli GramPanchayat of Rayagada district, whenthe tribal people walk the way,especially slopes they maintain adistance so that if someone skids thenthe following person would not be
affected and also can extend a helpinghand. Further, when the women walkwith headloads, if they do notmaintain physical distance then thereis every possibility that if the personin front falls down then the whole linewould fall down. In very practicalsense, this behaviour of maintaininga distance between two persons is alsoconducive to their work traditions inconsideration to the terrains. Anyvisitor into the tribal areas wouldobviously witness this queue-walkingmaintaining a reasonable physicaldistance whether it be while going tomarket, going to agricultural fields orother villages, while going on ahunting expedition or while walkingto the sago palm tree for an eveningdrink. While working in forest,especially for forest collections, theydo not work in groups and hence thesocial distancing norm is maintainedby customary practice. It is thiscustomary behaviour that becameincidental to the benefits ofprescriptive social distancing in theCovid context.
Social distancing at market places
The tribal people visit weekly marketsonce a week. They carry theiragricultural or other products tomarket walking in a queue and oncein market, they put up separate makeshift stalls or sit on the groundseparately to transact their produces.While also collecting their entitlementsfrom PDS centres or Anganwadi theyalso observe behaviour that conformsto social distancing and they alsoexhibit unfathomable patience waitingfor their turn.

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1936
Consider a ritual or worship beingorganized in the village or in a sacredgrove. The usual scene is that thepriest takes his seat at the designatedplace and performs. The communitypeople sit scattered at theirconvenience and observe the occasionat ease. The mothers with their kidsmaintain a distance for their privacyin caring the child. There is no strictrestriction on the sitting posture,gesture or pattern of participation. Thecustomary behaviours have beenshaped up through years ofmaintaining norms and traditions. Thetribes who have traditions ofmaintaining sacred groves, forexample, the Santhals, Bhumij, Ho/Kolha, Bathudi, Hill Kharia, Oraonsand many other tribes in the NorthernOdisha exhibit the traditional ways ofmaintaining social distancing. Thetribes in the Southern Odisha, forexample, Kandha, Paraja, Bhatra,Omanatya, Saora and many othertribes also have their shrines andsacred groves where they showcasetheir default norms of socialdistancing in a customary way.
The police personnel, healthproviders, frontline workers broughtthe message of social distancing to thetribal folks to contain the Corona virus.Just by tip of information regardingthe essentials of maintaining socialdistancing lest that the vulnerabilitydue to spread of Corona claim lives,the tribals took care of everything elsethemselves. Barriers were erected atthe boundaries of several tribalvillages to prevent outsiders fromsneaking in. Even their own people
who were stranded elsewhere werenot allowed inside the village. Peoplefrom the neighbourhoods, traderswho used to come to villages to collectagricultural produces, outsiders whoused to visit tribal villages for differentpurposes were denied access into thevillages. In case migrant workerscoming back from other statesmanaged to enter the village, theywere immediately brought to theattention of local health workers, andsent into isolation by the villagersthemselves. They might know thescientific significance of the lockdown,but tribals are very aware aboutkeeping distance from others, and areable to maintain social distancing intheir routine life.
No doubt, the traditional way of lifeof tribal is acknowledged by many asthe “proper way” to keep a disease likeCovid-19 at bay.
V
REAFFIRMING TRUSTON ETHNOMEDICINEThe public health crisis triggered bySARS-CoV-2, the cause of the COVID-19 disease has a profound impact inre-affirming trust on traditionalmedicine or ethnomedicine. In asituation when the health-care centresin the tribal areas are not up to markto provide medical care to contain theCovid, the tribal people have beenshowing greater interest in theirtraditional medicine. As a result, theold systems and magico-religious

37IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
practices are being revisited by theethnic groups in remote areas.
Regardless of geographicalconsiderations the tribal communitiesin Odisha seems to have come back totheir traditional knowledge,livelihoods and use or management ofnatural resources as a response tomaintain their well-being andhealthcare. Over the years, manystudies and research have beenconducted on the ‘little traditions’ ofethnomedicine but the Covid – 19 hastriggered the scope for application ofsuch knowledge systems.
The pandemic has provoked severepublic health and socioeconomicimpacts worldwide, hereby raisingattention to animal–humaninteractions. It has increased thedemand for local remedies. Medicinalplants like ginger and turmeric aremarketed as ‘immune boosters’ thatcure or protect against thecoronavirus. Through (social) media,YouTube, TV and word-of-mouth,self-identified traditional healersargue that while Western doctorsstruggle to combat this new virus, theyalready know the cure, which theymake using herbs from their ownbackyard or local markets. AlthoughCovid is a new disease and its curewith traditional medicines has notbeen justified yet, the fear of this newdisease and the absence of a cure orvaccine drives the global demand fortraditional remedies to providegeneral health improvement andpotential cures.
Traditional medicine is ridiculed whenit is improperly publicized in market.For example, the iconic yoga guru andAyurved businessman Baba Ramdevdrew criticism from healthprofessionals for publicizing his‘finding’ that ashvagandha (Withaniasomnifera) may ward off the virus. Themost emblematic ethnomedicinal stir,however, was that of the ridiculedprescription of bovine urine and dungas medicine. Ayurved works with aparticular framework of bio-elementsand diagnostic tools and, as such,anything, even excrement, can berendered medicinal, depending on thepatient’s conditions. The tribaltraditional medicine has not been thatpublicized or badly criticized.
The pandemic has rather led peopleto consider immigration back to ruralareas; that is, a lifestyle closer to naturefor their well-being and good health.Indigenous communities have putlimits to access of outsiders into theirhabitations during this ongoingpandemic. Concurrently,communities are encouragingmembers to return to the land for foodand social distancing. A likely andvery positive outcome is a revitalizedconnection with family and the landand improvements tointergenerational transmission ofknowledge, both of which will lead tostronger food security andsovereignty. Although this pandemichas traumatized tribals and shaken thesocial, economic, cultural andreligious bases of their life, yet it is alsoredefining human attitudes towards

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1938
natural resources. Althoughindigenous people and othercommunities in rural areas areeconomically marginalized, theyrepresent a real hub of traditionalknowledge., although, however,isolation caused by the COVID-19pandemic has significantly influencedtheir robust socio-cultural andreligious bonds.
Natural immunity
Many tribal people themselves andtheir healers do believe that they havegood natural immunity that keepsthem safe from many diseases. Theirextreme exposure to the naturalenvironment is attributed to be thereasons of their disease preventionand tolerance. Tribals are naturallyimmune to several diseases, as theystill thrive upon forest products likefruits, root vegetables and variousherbal products.
One of the tribal ways of respondingto sneezing, cold and cold fever is byway of administering decoctions ofroots, barks, leaves and spices. Thesemedicinal decoctions are known indifferent names in differentcommunities. However, the mostcommonly used term is Kaadha. TheKaadha is prepared out of severalherbs, leaves, roots like Tulsi (Ocimumsanctum), Arjun (Terminalia arjuna),Patalgaruda (Rouwolfia serpentina),Guava (Psidium guajava), Guluchi(Tinospora cordifolia), Kalmegh(Andrographis paniculata), Gangasiuli(Nyctanthes arbor-tristis), Satavari(Asparagus recemosus), Cinnamon,black pepper, ginger, turmeric, etc
with jaggery and such other materialsthat provides superior immunity. Thetribes in the remote areas and also inthe mainstream drink Kadhaa asmedicines and also as regularly as teawhen feel sick out of cold, fever, fluand that kind of ailments. The Kaadhaworks in the body as preventive andcurative medicine. The Kaadha isconsidered an efficacious preparationand formulation in Ayurvedicliteratures. However, the tribalKaadha preparation is different fromthe Ayurvedic texts as they mix upfresh naturally available multipleingredients in estimated quantitiesbased on their past experiences.Kaadha in tribal society is time testedefficacious medicine which ispreventive, curative and ameliorative.
Preventive healthcare
The tribal way of treating a disease isdifferent. However, what matters inthe Covid context is to ensurepreventive healthcare. In the wake ofthe Covid, the frontline workers of thegovernment departments wereassigned with duties related to Covidmanagement and hence the tribalpeople started taking recourse topreventive healthcare systems. Goodfood, less exposure, maintaining socialdistance and affirming trust onpreventive traditional healthcarepractices have been considered as thekey preventive measures they took toprevent Covid.
According to Laxmi Bhatra, a triballady known to have good knowledgein ethno-medicine in Kotpad areastated that those who have been taking

39IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
Chhapra, a paste made from red ants, a traditional delicacy in Bastar, havegood immunity to fight any healthproblem. The tribes in Mayurbhanjand Sundergarh are quite acquaintedwith the preparations from the eggs ofred ants. However, no personaltestimonial is available to indicate ifthe tribal people in those districtsbelieve that the preparations out of redants develops their immunity.
Effect of fumigants for homesanitation
The tribal people have a strongconviction that certain fumigants havewonderful effects in keeping thehouses sanitized and anti-septic whichhelps in preventing the diseases likeSmall pox, Chicken pox and for thatmatter, Covid also. Budura Jani, inBelghar under Kutia KandhaDevelopment Agency is of opinionthat by burning neem leaves, dry skinof onion and garlic, turmeric, sal resin,etc together or separately, the housecan be purified and sanitized. To abatethe Covid, Kutia Kondhs and likethem many other tribal communitiesinsists on using fumigants at home.
Managing the mentally -ills
The most important challenge for thetribal people during the Covid dayshas been to manage the patients withmental health problems. Withhospitals closed and restrictionsimposed on general movements,attending the mentally sick people isconsidered a difficult task. NabaghanWadaka, a Dongaria Kondh inKhambesi village and Mohan Murmu
of Baripada holds that the magico-religious beliefs have made acomeback to treat the mentally sickpeople. Thus, the importance of themagico-religious healers has increasedin tribal societies. With magico-religious performances, with orwithout sacrifices, the mentally ill andtheir family members are feelingcomfortable. Thus, the magico-religious beliefs have ben acting as ameasure for the mentally sick people.The cultural values, life style, worldview and ethos did not allow them tohave fear psychosis from Covid-19.However, counselling is required tosustain mental health of the tribals.
Traditional birth attendants recalledby community
At many places in the remote tribalpockets, people have relatively lessaccess to the health infrastructures.The Covid restrictions added to thealready existing difficulties. Further,the ASHA, Anganwadi worker andgrassroots health workers wereassigned with duties to handleessential requirements on priority. Thesituation created a stir in the tribalcommunities, with the pregnantwomen and more particularly on thetribal women at advanced stages ofpregnancy. Reports from here andthere indicate that the situationbrought importance to the traditionalbirth attendants. The tribal peoplepreferred home delivery overinstitutional delivery because of theapprehensions that going to thehospitals might become a cause ofgetting inflicted with Covid. Thus, the

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1940
traditional birth attendants have beenback into action in remote tribalpockets. Along with their come back,there has been a comeback of the homeremedies that applies to commonproblems of pregnant and lactatingwomen and infants.
Preventive behavioural aspects
Along with these preventive practices,certain regular day to day behavioursalso had its influence over containingCorona in tribal villages. The tribalwomen are very particular aboutwashing their clothes properly whilebathing and drying them properlybefore reusing. The traditional systemof women veiling their faces withsaree, as a gesture, also works like amask. In many remote villages ofBonda and Gadaba, washing clotheseach day with ashes from the hearthis still in vogue. Hari Pangi, a knowntribal herbalist in Semiliguda ofKoraput district observed thatwashing clothes with ashes fromhearth is a continuing tradition.However, during the Covid, as hestated, he has been advising people tomix the ashes of neem leaves andbanana sheaths to make thesanitisation more effective. Accordingto Padmanabha Jani of Dasmantpur,where Cholera outbreak happenedabout a decade ago, maintaining homesanitation with sprinkling of turmericwater, neem leave pastes, regularwashing of floors with cow dung,drinking water from tube wells andmaintaining social distance by practiceare some of the reasons for which theCovid has not been a cause of worry
for the tribal habitations located inremote pockets. In times of Corona,people have made white circles at thehand pumps and solar pumps to markminimum social distance to bemaintained.
Awareness actors and campaigns
Anganwadi and ASHA didi are thetwo key persons who conductedmassive awareness campaigns intribal villages. about hand wash, handsanitization, house sanitization,maintaining social distance andcovering faces with clean towel, sareeor mask whatever was available. Thelocal NGOs too contributed to their bit.Customarily, women used to covertheir faces by saree veils as a gestureof shyness, thus the advisory made nodifference to them. The young boysused to tie kerchiefs on face in stylewhile going out.
Some systems were created in thevillages especially about socialdistancing. Usually during regularwork days the women used to rush towater sources to fetch water in groups.When they were advised to stay athome, they did not have to rush towater sources and hence could easilyadopt to go out to water sources oneafter one, whether for bathing or fetchwater for cooking, maintaining a timegap. The social distancing thus did notpose a challenge. If there was shortageof water or issue of frequenting towater sources to wash utensils, thenthe leaf plates and cups were bestchosen alternatives. In many tribalvillages, Anganwadi didi installed

41IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
hand washing point at entrance ofvillage, children had enough fun withfrequent hand washing with soap,neem paste, turmeric paste and theelders followed the children. It didn’tseem as if corona threw life out of gearin tribal villages.
The impact of social distancing on thetribal group life has been manifold. Itrequired setting of norms, ratificationof norms and punishment system inthe village and could be establishedsoon. Many typical tribal villagescould go back to their traditional clan/village Panchayat system of self-ruleand devised systems complementaryto the restrictions and guidelines setby the state administration to preventcommunity spread of the pandemic.However, the impact of socialdistancing could be realized in closureof SHG activities other than makingmasks and door to door campaigning,marriages had to be postponed, ritualsand religious affairs were cut shortfrom community occasions toindividual practices.
VICONCLUDING REMARKSTribal communities in Odisha havesustained many epidemics andtolerated many diseases in epidemicform. They have justified to be saidself-reliant and resilient in many ways.Their social and cultural way of life,customs and traditions, values andmores have many in-built solutionswhich proves instrumental at the time
of crisis like that observed during theCovid management. The tribal peoplehave also shown responsive copingmechanisms to prevent the spread ofthe disease and at the same time tomanage their economies within theframework of guidelines andoccasional circulars issued by the stateand central government. They havebeen maintaining social distance intheir own ways, covering their faceswith kerchiefs, towels, saree andmasks if available. They have beenreaching out to NGOs for aids andservices. Many coping mechanismshave been adopted towardssanitization and maintainingsanitation. Hardly examples of suchcoping mechanisms have beenbrought to common knowledgebecause of restrictions on movement.
Specific studies on impact ofepidemics and pandemics on tribalculture is rare. There are rathersporadic notes on how certain tribalcultures have responded to situationsof epidemics and pandemics. In thepast, the tribal areas of Odisha havecome across several epidemics. Somememory of such epidemics and theirmanagement at community level arestill living with the older generations,and very little effort fordocumentation of these memorieshave been made. However, it is a factthat in case of outbreak of an epidemicin a smaller geography around tribalhabitations, the people generallyattribute it to the wrath and anger ofcertain deities and spirits. Towardsthat many religious practices areconducted with or without executing

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1942
sacrifices. The philosophy of sacrificebeing – offering a life to god seekingwell being of many. Oral lore provideevidences that with the outbreak of anepidemics, the villagers, guided bytheir religious head, have abandonedvillages and shifted to new locationsbelieving that the god or goddess whobrought the epidemics wanted themto leave the village for some reason,or in other words, the gods andgoddesses reclaimed their space. Across-examination of the uninhabitedvillages in tribal areas, some of whichfeaturing in census reports, mayprovide further evidences ofabandoning villages attributing thereasons to certain epidemics. It mayhelp re-constructing the culturalresponses to epidemics andcomparing it with the culturalparadigms today as well. In thecontext of Pandemic, as many eldertribal people mentioned, the parochialtraditions have rather remained silentand the universal traditions havereigned over. Thus, it may beconstrued that epidemicsmanagement brings about reflectionsof parochial traditions or littletraditions while pandemic reflects theuniversal traditions or great traditions.The Covid prevention management intribal areas stand testimony to this.
Then, the usual question that strikesis whether or not the lockdown andrelated restrictions influenced thetribal culture? There are manycontextual answers to it that may notbe possible to be generalized.However, looking at the groundsituations, it would be convincing to
state that the Covid has triggered asituation for the tribal communities tobehave as self-contained units. TheCovid related lockdown andrestrictions has not been able to impactthe traditional economy of the tribalcommunities although theirrelationship with market economy hasbeen impacted. Larger religiousfestivals have been impacted but nohard impact on the belief systemscould be realized. The religious andlife-cycle rituals do not seem to havebeen halted or withdrawn rather hasbeen cut short to some extent. Ampleevidences have been generated tobelieve that the tribal communitieshave been re-affirming trust on theirold systems. The publicity on gravityof Covid and the cases showing thathealth providers are falling prey toCovid, the tribal people have beenshowing relative self-constraint to visithealth centers for general treatment.For many small ailments they havetaken recourse to their folk medicineor ethno-medicine. The Covid phobiacaused larger dependence on thetraditional birth attendants, traditionalherbalists, magico-religious healers,local non-tribal vaidyas some ofwhom had become nondescripts intheir community.
They have shown preventive socialbehaviour by restricting their exposureand putting blockades to entry ofoutsiders into their villages. There aremany cases, where communitymembers expressed solidarity with in-migrating villagers and advised themto take official quarantine facilitiesthan preferring home quarantine. The

43IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-19
religious leaders took the lead inexercising religious governance,performing specific rituals at villagelevel for well-being of the communitymembers. Such rituals as are usuallyconducted to ward off the evil spiritsbelieved to have caused an epidemicwere hardly conducted for Covid,because they do not believe any oftheir gods or goddesses caused it.They don’t hold their gods andgoddesses responsible for pandemiclike covid that has occurrence beyondboundaries.
For sake of maintaining theirhousehold economy and householdfood security they have rebuilt theirties with forest. Leaving apart thesubsidized rations under publicdistribution system, an increasingdependency is observed on wildedibles that they believe providesnatural immunity. The non-timberforest produce has been optimallyharvested during the early days ofCovid restriction this year. Thanks tosupport of the state coming at the righttime for procurement of largercollections like Sal seed and economicNTFPs like Kendu leaves.
The lockdown caused increased levelof social solidarity, although breach ofmutual trust, fear and apprehensionsruled in the case of the mainstreamcommunities. During the course ofCovid prevention phase the tribalpeople have come together as anendowed social capital and leveragedadequately on their cooperative laboursystems and group solidarity. In manytribal villages the cooperative labour
system had relatively dwindledbecause of people running towardscash economy in nearby cities, bytaking up individual enterprises,vending and other wage-earningopportunities. During the lockdown,extraordinary examples of cooperativelabour management and excellentexhibits of group farming has beenseen. The lockdown affected themainstreams, made the marketsvolatile, individual enterprisessuffered setbacks but the tribalcommunities became better organizedand their philosophy of life has startedgoing back to the old times and livinga life clinging to culture. Extension oflockdown would result in more re-organizing, solidarity building,showcasing cultural diversities andexhibiting tribal communities as self-contained units and re-establishingtheir traditional socio-political normsin self-governance. As many eldertribal people stated, more thelockdown continues, more and morethey will realize compactness in theirsocio-cultural-religious-politicalaffairs.
Odisha has stood strong throughseveral epidemics and pandemics.Good medical care and propertraditional practices have made itpossible to fight every infection andluckily, we have been able to eveneradicate a few. It can be establishedthat throughout time, many infectiousdiseases have become widespread dueto the mere lack of sanitation andcrowded environment. The tropicalclimate and the seasonal rains in tribalOdisha is yet another important factor

IMPACT OF PANDEMICS ON TRIBAL CULTURE OF ODISHA : With Special Reference to COVID-1944
contributing to several vector-borneinfections outbreaks in the past andmany more to come. Though it hasbeen difficult to throw light on impactof the epidemics and pandemics ontribals of Odisha due to lack ofsufficiently available data on ahistorical time line, sincere effortshave been put into including most ofthe important, notable ones. This iswritten with a hope that it may helpmedical professionals understand
where they had gone wrong incontrolling an outbreak in the past orhow they succeeded to lead byexample. It may not be out of contextto say the tribal areas in Odisha mayface more outbreaks in the days tocome but preparedness has to be givenimmense importance and control ofspread should be the number onepriority of the doctors and other healthcare workers, with due respect to thetribal culture, ethos and sentiments.

