cost-effectiveness of radiofrequency catheter...
TRANSCRIPT

Cost-Effectiveness of Radiofrequency Catheter AblationCompared With Antiarrhythmic Drug Therapy for
Paroxysmal Atrial FibrillationMatthew R. Reynolds, MD, MSc; Peter Zimetbaum, MD; Mark E. Josephson, MD; Ethan Ellis, MD;
Tatyana Danilov, MD; David J. Cohen, MD, MSc
Background—Radiofrequency catheter ablation (RFA) has emerged as an important treatment strategy for atrialfibrillation (AF). The potential cost-effectiveness of RFA for AF, relative to antiarrhythmic drug (AAD) therapy, hasnot been fully explored from a US perspective.
Methods and Results—We constructed a Markov disease simulation model for a hypothetical cohort of patients withdrug-refractory paroxysmal AF, treated either with RFA with/without AAD or AAD alone. Costs and quality-adjustedlife-years were projected over 5 years. Model inputs were drawn from published clinical trial and registry data, from newregistry and trial data analysis, and from data prospectively collected from patients with AF treated with RFA at ourinstitution. We assumed no benefit from ablation on stroke, heart failure or death, but did estimate changes inquality-adjusted life expectancy using data from several AF cohorts. In the base case scenario, cumulative costs withthe RFA and AAD strategies were $26 584 and $19 898, respectively. Over 5 years, quality-adjusted life expectancy was3.51 quality-adjusted life-years with RFA versus 3.38 for the AAD group. The incremental cost-effectiveness ratio forRFA versus AAD was thus $51 431 per quality-adjusted life-year. Model results were most sensitive to time horizon,the relative utility weights of successful ablation versus unsuccessful drug therapy, and to the cost of an ablationprocedure.
Conclusions—RFA with/without AAD for symptomatic, drug-refractory paroxysmal AF appears to be reasonablycost-effective compared with AAD therapy alone from the perspective of the US health care system, based on improvedquality of life and avoidance of future health care costs. (Circ Arrhythmia Electrophysiol. 2009;2:362-369.)
Key Words: atrial fibrillation � ablation � antiarrhythmia agents � cost-benefit analysis
Since its earliest reports a little more than a decade ago1,2
radiofrequency catheter ablation (RFA) for atrial fibril-lation (AF) has undergone rapid evolution in its techniquesand emerged as an important option in the treatment ofpatients with AF.3 Several small, randomized studies haveestablished that ablation reduces AF recurrence more effec-tively than antiarrhythmic drugs (AADs) in patients who havefailed previous AAD treatment4 and yields superior improve-ments in symptoms and quality of life.5–7
Clinical Perspective on p 369
Because the population of patients with AF is large andgrowing,8 management decisions about AF are likely to haveimportant implications for future population health and healthcare spending.9,10 To date, information regarding the potentialcost-effectiveness of catheter ablation for AF relative tomedical therapy is limited. Although a few previous studies
have suggested that the up-front costs of catheter ablation maybe partly—if not fully—offset by the avoidance of later AF-related resource use11–14 or adverse events such as stroke,15 noneof these studies has directly integrated data on changes in qualityof life related to maintenance of sinus rhythm.
To gain a better understanding of the benefits and costs ofAF ablation relative to medical therapy, we developed adisease-simulation Markov model for a hypothetical cohort ofpatients with paroxysmal AF who had failed previous treat-ment with 1 or more AADs. Drawing from a variety ofsources, we estimated costs, quality-adjusted life expectancy,and cost-effectiveness of RFA with/without AAD relative tocontinued AAD therapy alone over a 5-year time horizon.
MethodsModeling Strategy and Basic AssumptionsWe developed a Markov disease-simulation model comparing RFAwith/without AAD with AAD therapy alone for patients with
Received November 23, 2008; accepted March 19, 2009.From the Beth Israel Deaconess Medical Center (M.R.R., P.Z., M.E.J.,E.E., T.D.), Boston, Mass; and St Luke’s Mid-America Heart Institute (D.J.C.),
Kansas City, Mo.Charles I. Berul, MD, handled this article.The online-only Data Supplement is available at http://circep.ahajournals.org/cgi/content/full/CIRCEP.108.837294/DC1.Correspondence to Matthew R. Reynolds, MD, MSc, Division of Cardiology, Baker 4, Beth Israel Deaconess Medical Center, 185 Pilgrim Road,
Boston, MA 02215. E-mail [email protected]© 2009 American Heart Association, Inc.
Circ Arrhythmia Electrophysiol is available at http://circep.ahajournals.org DOI: 10.1161/CIRCEP.108.837294
362
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
paroxysmal AF refractory to 1 or more AADs. This population waschosen because consensus guidelines have endorsed ablation in thesepatients3,16; because ablation appears to potentially yield betterresults in patients with paroxysmal AF compared with patients withpersistent AF17–19; and because there is a larger body of randomizedevidence available for patients with paroxysmal AF (as opposed tothose with persistent AF or mixed populations) from which to derivemodel parameters. The published literature suggests that the majorityof patients currently referred for ablation are male, under age 60, anddo not have advanced heart failure.4 We therefore modeled outcomesfor a cohort of 60-year-old men without severe structural heartdisease.
The model has a 5-year time horizon, which we believe is longenough to capture most of the major changes in resource consump-tion and quality of life after an initial decision on AF managementand because this corresponds roughly with the longest follow-up ofoutcomes with either ablation or AAD therapy published in theliterature.20,21 The impact of time horizon was tested in sensitivityanalysis. The cycle length was 1 month, and all analyses were basedon the societal perspective. Future costs and quality-adjusted life-years (QALYs) were discounted at 3% per year, and this rate wasalso varied in sensitivity analysis.22 We used TreeAge Pro 2005software (TreeAge, Williamstown, Mass) for all model programmingand calculations.
For the sake of estimating cost-effectiveness over a medium-termtime horizon, we assumed that patients assigned to drug therapycannot “cross over” to ablation within the model. This constructionmore accurately estimates the true incremental value of ablationcompared with drug therapy, as opposed to one that ultimatelycompared an up-front ablation strategy with “delayed” ablation afteradditional drug failure, assuming that the rate of drug failure wouldbe significant.5,6,13
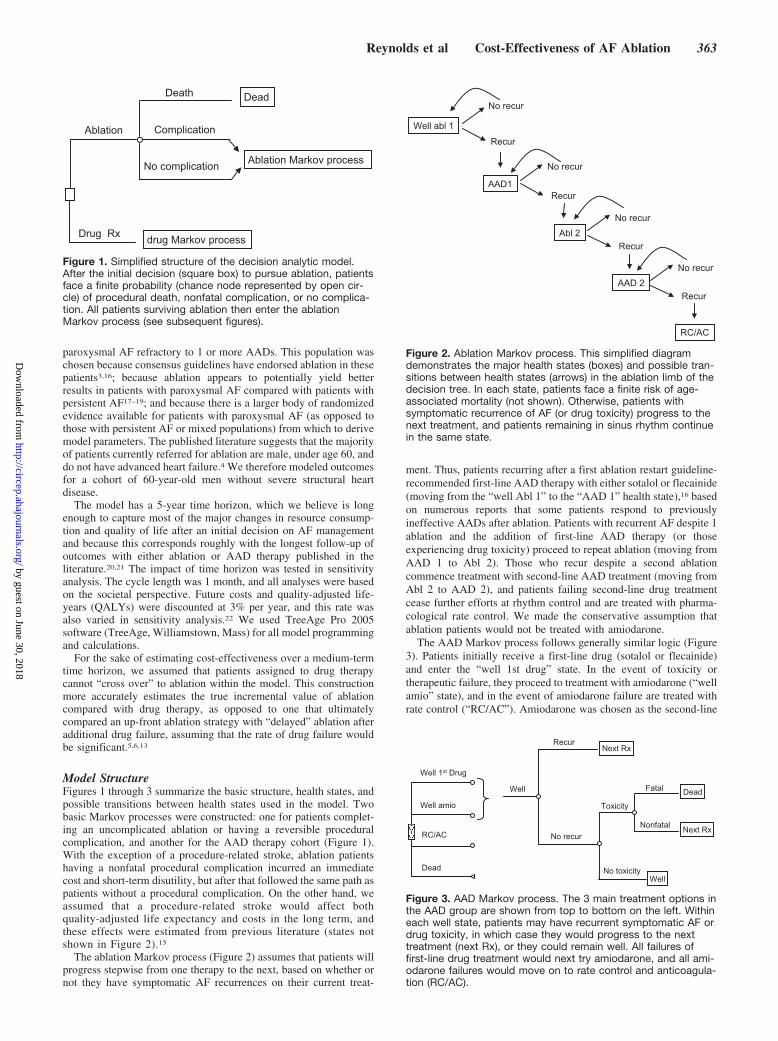
Model StructureFigures 1 through 3 summarize the basic structure, health states, andpossible transitions between health states used in the model. Twobasic Markov processes were constructed: one for patients complet-ing an uncomplicated ablation or having a reversible proceduralcomplication, and another for the AAD therapy cohort (Figure 1).With the exception of a procedure-related stroke, ablation patientshaving a nonfatal procedural complication incurred an immediatecost and short-term disutility, but after that followed the same path aspatients without a procedural complication. On the other hand, weassumed that a procedure-related stroke would affect bothquality-adjusted life expectancy and costs in the long term, andthese effects were estimated from previous literature (states notshown in Figure 2).15
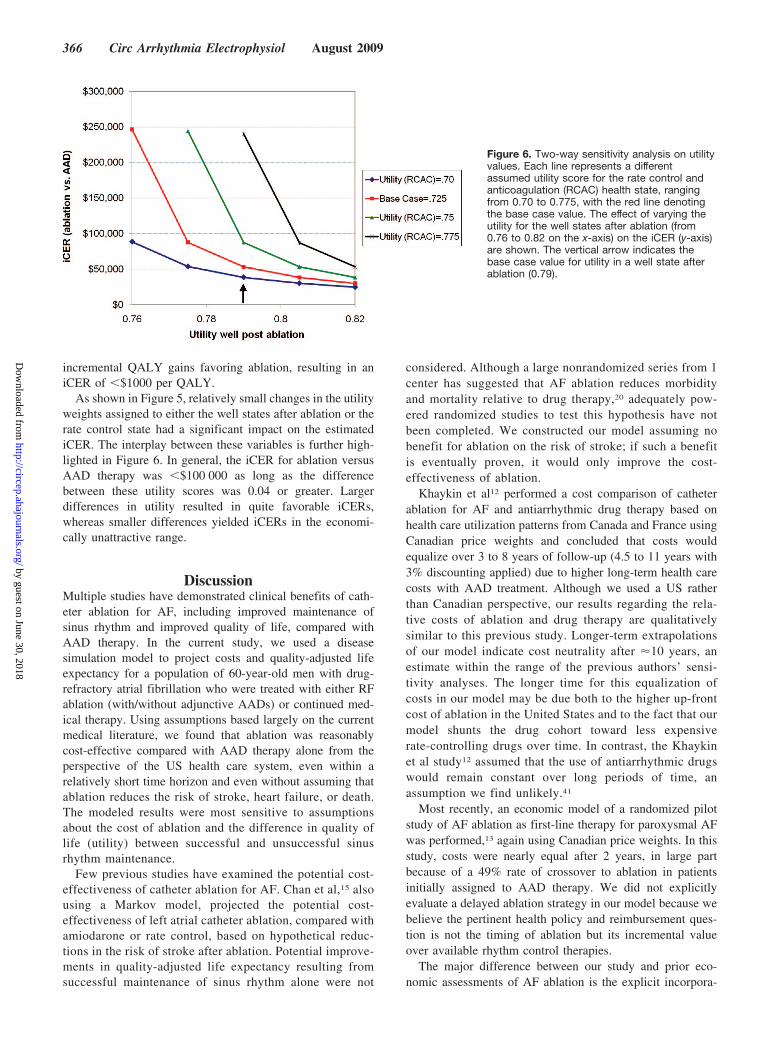
The ablation Markov process (Figure 2) assumes that patients willprogress stepwise from one therapy to the next, based on whether ornot they have symptomatic AF recurrences on their current treat-
ment. Thus, patients recurring after a first ablation restart guideline-recommended first-line AAD therapy with either sotalol or flecainide(moving from the “well Abl 1” to the “AAD 1” health state),16 basedon numerous reports that some patients respond to previouslyineffective AADs after ablation. Patients with recurrent AF despite 1ablation and the addition of first-line AAD therapy (or thoseexperiencing drug toxicity) proceed to repeat ablation (moving fromAAD 1 to Abl 2). Those who recur despite a second ablationcommence treatment with second-line AAD treatment (moving fromAbl 2 to AAD 2), and patients failing second-line drug treatmentcease further efforts at rhythm control and are treated with pharma-cological rate control. We made the conservative assumption thatablation patients would not be treated with amiodarone.
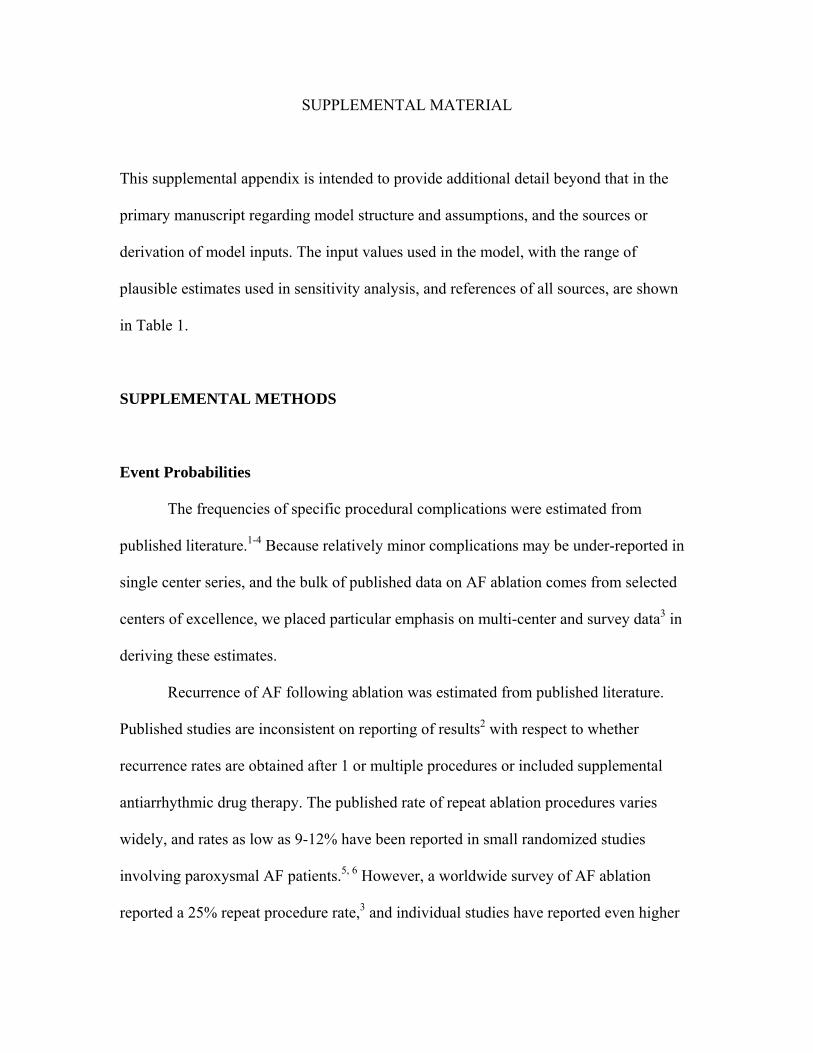
The AAD Markov process follows generally similar logic (Figure3). Patients initially receive a first-line drug (sotalol or flecainide)and enter the “well 1st drug” state. In the event of toxicity ortherapeutic failure, they proceed to treatment with amiodarone (“wellamio” state), and in the event of amiodarone failure are treated withrate control (“RC/AC”). Amiodarone was chosen as the second-line
Ablation
Drug Rx drug Markov process
No complication
Complication
Death Dead
Ablation Markov process
Figure 1. Simplified structure of the decision analytic model.After the initial decision (square box) to pursue ablation, patientsface a finite probability (chance node represented by open cir-cle) of procedural death, nonfatal complication, or no complica-tion. All patients surviving ablation then enter the ablationMarkov process (see subsequent figures).
Well abl 1
No recur
Recur
AAD1Recur
No recur
Abl 2No recur
Recur
AAD 2No recur
Recur
RC/AC
Figure 2. Ablation Markov process. This simplified diagramdemonstrates the major health states (boxes) and possible tran-sitions between health states (arrows) in the ablation limb of thedecision tree. In each state, patients face a finite risk of age-associated mortality (not shown). Otherwise, patients withsymptomatic recurrence of AF (or drug toxicity) progress to thenext treatment, and patients remaining in sinus rhythm continuein the same state.
Well 1st Drug
Well amio
RC/AC
Dead
Well
No recur
RecurNext Rx
Toxicity
Fatal Dead
Nonfatal Next Rx
No toxicityWell
Figure 3. AAD Markov process. The 3 main treatment options inthe AAD group are shown from top to bottom on the left. Withineach well state, patients may have recurrent symptomatic AF ordrug toxicity, in which case they would progress to the nexttreatment (next Rx), or they could remain well. All failures offirst-line drug treatment would next try amiodarone, and all ami-odarone failures would move on to rate control and anticoagula-tion (RC/AC).
Reynolds et al Cost-Effectiveness of AF Ablation 363
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

agent for all patients in the drug arm, based on its superiority overother drugs at maintaining sinus rhythm.23–25
All patients face a background rate of mortality based on their ageand sex and can therefore transition from any health state directly todeath in either arm of the model (not shown in figure).26 Aside fromsmall risks of procedural death or fatal drug toxicity (see Appendix),the model assumes that the risk of death is the same for all healthstates and interventions except after major stroke after an ablation.Further, because the potential for either drug therapy or ablation toreduce the long-term risk of stroke has not been proven, we assumedthat the incidence of stroke would be the same for both therapies andtherefore did not explicitly consider stroke as an outcome in themodel, except as a potential complication of ablation. In keepingwith current recommendations,3 we also assumed that long-termanticoagulation practices and related costs and complications wouldbe equivalent between groups.
Risks of both fatal and nonfatal antiarrhythmic drug toxicity weretaken from the literature (see online-only Data Supplement) andapplied equally to ablation and nonablation patients. In the ablationarm of the model, it was assumed that patients having drug toxicityafter a single ablation would have recurrent AF and undergo repeatablation, whereas patients having drug toxicity after 2 ablationswould then be treated with rate control.
Model InputsInputs for the model were drawn from a variety of sources, includingcompleted clinical trials, a large registry of patients with new-onsetAF, prospectively collected data from patients treated at our institu-tion, and analysis of Medicare claims data. Risks of events wereallowed to vary over time by incorporating probability tables andtunnel states into the model. The base case estimate, range of valuesused in sensitivity analysis, data sources, and additional details areprovided in the Appendix. Some general discussion regarding datasources and key inputs is provided here.
Event ProbabilitiesThe risks of procedural complications after AF ablation were takenfrom published randomized and nonrandomized series and a largeinternational survey on AF ablation outcomes.27 The likelihood ofsuccessful sinus rhythm maintenance for each of the strategies inboth the ablation and drug arms of the model were taken as much aspossible from recent randomized studies5,28,29 but were cross refer-enced with more general sources.27
We assumed a single-procedure efficacy rate of 60% for ablationand calibrated the model to achieve a 25% rate of repeat ablation(with some patients achieving successful rhythm control on AADtherapy after 1 ablation) and a 10% overall failure rate with theablation strategy. We assumed that 75% of patients treated withfirst-line drugs (and no ablation) would recur within 1 year and that65% of patients treated with amiodarone as second-line therapywould recur within 1 year. These recurrence rates with AAD therapyare slightly higher than in a recent AAD comparative efficacy trial24
but are consistent with recurrence rates in recent randomized studiescomparing ablation with drug therapy in patients with paroxysmalAF with previous drug failure.5,28,29
CostsThe costs of drug therapy for AF were primarily derived from theFRACTAL registry30 and the health economic substudy of theAFFIRM trial.31 The cost of catheter ablation was estimated from ourlocal cost-accounting system, and recently published estimates from theUnited States and Canada12,15 were used in sensitivity analysis.
Quality-of-Life AdjustmentAlthough quality of life has been assessed in studies of many AFinterventions,32 there is very little published information availableregarding utilities in patients with AF,33 particularly in AF ablationpopulations. To address this lack of data, we derived utilities for 3separate populations of patients with AF to estimate the likely
changes that might be observed after successful ablative or drugtherapy.
For drug-treated patients, we used SF-12 questionnaire34 datafrom the FRACTAL registry35 and calculated utilities for thesepatients using the method proposed by Brazier.36 For ablationpatients, we used a similar transformation of responses to the SF-36questionnaire37,38 to estimate the change in utility experienced by aprospective cohort of patients undergoing catheter ablation at BethIsrael Deaconess Medical Center. Finally, we also calculated utilitiesusing SF-36 data for patients enrolled in the Atrial Fibrillation versusAntiarrhythmic Drugs (A4) trial5,39 to estimate the comparativechanges in utility for patients treated with drugs versus ablation.Based on these analyses, the change in utility from baseline tosuccessful sinus rhythm maintenance was set at 0.065 (see Appendixfor additional details). In the model, utilities corresponding with eachhealth state were summed over the amount of time spent in thathealth state to calculate QALYs.
Secondary AnalysesOne-way sensitivity analyses40 for all model inputs were performedand plotted in a “tornado” diagram. Two-way sensitivity analysiswas performed on the utility of successful sinus rhythm maintenanceafter ablation and the utility of the rate control health state to betterdisplay the joint impact of these important variables on the model’scost-effectiveness estimates.
ResultsBase-Case ResultsFigure 4A and 4B display the state probabilities for theablation and AAD cohorts, respectively, plotted against time.Based on the model inputs, 60% of ablation patients remainwell after a single procedure, �10% eventually fail alltherapies and progress to a rate control and anticoagulationstrategy, and the remainder of ablation patients either achievecontrol of their AF with a second ablation and/or adjunctiveAAD therapy or die during follow-up. For the AAD cohort,the majority of patients fail first-line treatment over 1 yearand transition to amiodarone. However, over time, roughlytwo thirds of patients fail AAD treatment altogether and progressto a rate-control and anticoagulation strategy. Based on the lowestimates of fatality from procedural complications or drugtoxicity, projected all-cause mortality was equivalent betweengroups (7.7% ablation versus 7.8% AAD).
In the base-case scenario, cumulative costs with the RFAand AAD strategies were $26 584 and $19 898, respectively.The initial difference in costs between strategies is roughly$10 000 but narrows over time as a larger proportion of AADpatients have symptomatic recurrences, leading to increasedresource consumption and changes in therapy. Over 5 years,the RFA cohort lived 3.51 QALYs, versus 3.38 for the AADgroup. The incremental cost-effectiveness ratio (iCER) forRFA versus AAD was thus $51 431/QALY. Removing theage- and sex-related background mortality from the modelincreased costs in both groups to a similar extent andmodestly increased the incremental quality-adjusted life ex-pectancy in favor of ablation (3.64 versus 3.50 QALYs),slightly reducing the iCER to $47 333 per QALY.
Sensitivity AnalysisFigure 5 displays the impact of varying key input variables onthe iCER. Within the plausible ranges for these variables (seealso Appendix), the model was insensitive to changes to the
364 Circ Arrhythmia Electrophysiol August 2009
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

discount rate, the probability or cost of procedural complica-tions or drug toxicity, or assumptions about the efficacy orcost of first-line antiarrhythmic drug therapy. In no case didchanges in these parameters increase the iCER above $60 000per QALY.
The model was moderately sensitive to the cost of amiod-arone therapy, the cost of drug loading, the cost of AF careunder a rate control strategy, and the assumed rate of singleprocedure efficacy with ablation. Changes in these parametersdid not increase the iCER to more than $80 000 per QALY.
The model results were most sensitive to the time horizonof the analysis, the cost of ablation, and to the relative utilityweights of successful ablation versus unsuccessful drugtherapy. Predictably, higher assumed values for the cost ofablation increased the iCER, which was �$100 000 perQALY at a single procedure ablation cost of $20 000.Holding all other parameters constant, a time horizon of 3years resulted in incremental costs of �$9900 and an unfa-vorable iCER of $157 000 per QALY, whereas a timehorizon of 10 years resulted in near cost neutrality and larger
Figure 4. State probabilities over time for theablation (A) and AAD (B) arms of the model.Based on the defined transition probabilities,roughly 60% of ablation patients remained wellafter a single procedure, 10% eventually failedall treatments, and the remainder achievedsuccess with concomitant AAD therapy and/ora second ablation. In the AAD arm, roughly50% of patients fail both first and second-linedrug therapy within 2 years and are subse-quently treated with rate control and anticoagu-lation only (RC/AC).
Incremental Cost-Effectiveness: RFA vs. AAD
iCER ($thousand/QALY)
0 50 100 150 200 250 300
First line drug cost ($6000 -$2500)Discount Rate (0-5%)
Amiodarone Rx Cost ($5000 - $1200)Single procedure success (70%-50%)
Cost of Drug Load ($7000 - 0)Rate Control Cost ($5000-$900/yr)
Ablation Cost ($10,000-20,000)Utility: rate control (0.69 - 0.76)
Time horizon (10 - 3 years)Utility: ablation success (0.82 - 0.76)
Figure 5. Tornado diagram displaying theresults of key 1-way sensitivity analyses on theiCER for ablation compared with AAD therapy.The base-case result is denoted by the verticalline, and the changes to the iCER by varyingindividual parameters within plausible limits(shown in parentheses) are shown in the hori-zontal bars.
Reynolds et al Cost-Effectiveness of AF Ablation 365
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
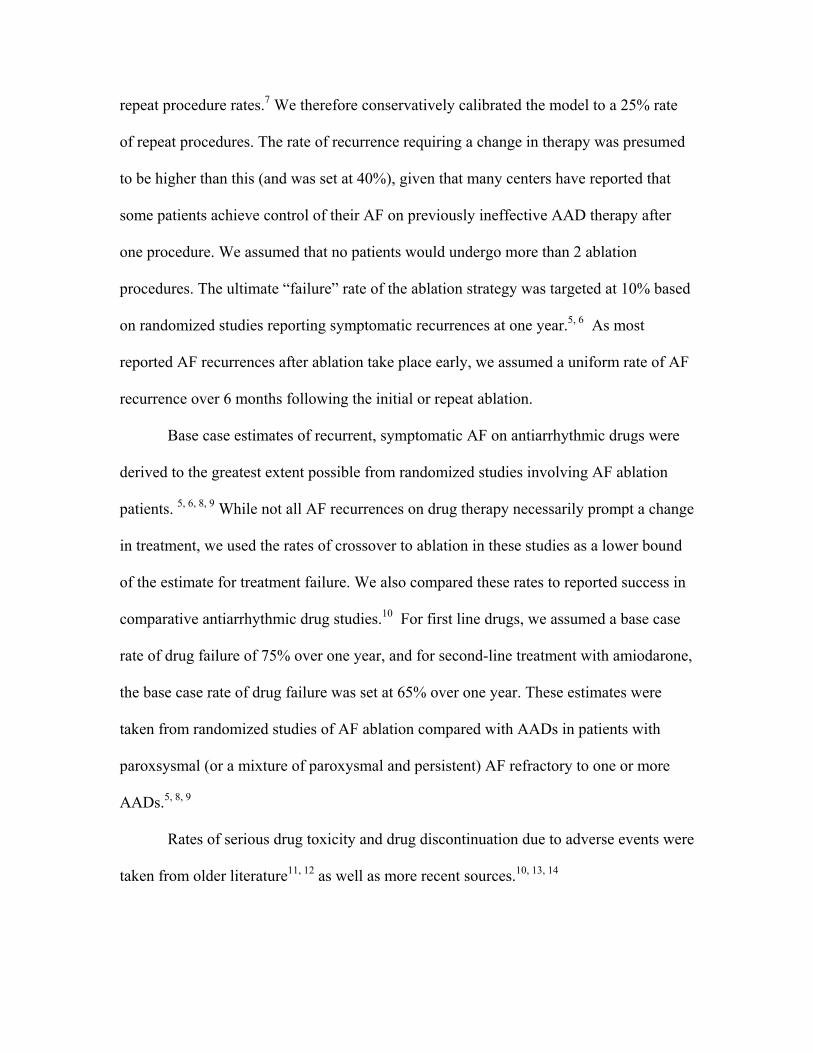
incremental QALY gains favoring ablation, resulting in aniCER of �$1000 per QALY.
As shown in Figure 5, relatively small changes in the utilityweights assigned to either the well states after ablation or therate control state had a significant impact on the estimatediCER. The interplay between these variables is further high-lighted in Figure 6. In general, the iCER for ablation versusAAD therapy was �$100 000 as long as the differencebetween these utility scores was 0.04 or greater. Largerdifferences in utility resulted in quite favorable iCERs,whereas smaller differences yielded iCERs in the economi-cally unattractive range.
DiscussionMultiple studies have demonstrated clinical benefits of cath-eter ablation for AF, including improved maintenance ofsinus rhythm and improved quality of life, compared withAAD therapy. In the current study, we used a diseasesimulation model to project costs and quality-adjusted lifeexpectancy for a population of 60-year-old men with drug-refractory atrial fibrillation who were treated with either RFablation (with/without adjunctive AADs) or continued med-ical therapy. Using assumptions based largely on the currentmedical literature, we found that ablation was reasonablycost-effective compared with AAD therapy alone from theperspective of the US health care system, even within arelatively short time horizon and even without assuming thatablation reduces the risk of stroke, heart failure, or death.The modeled results were most sensitive to assumptionsabout the cost of ablation and the difference in quality oflife (utility) between successful and unsuccessful sinusrhythm maintenance.
Few previous studies have examined the potential cost-effectiveness of catheter ablation for AF. Chan et al,15 alsousing a Markov model, projected the potential cost-effectiveness of left atrial catheter ablation, compared withamiodarone or rate control, based on hypothetical reduc-tions in the risk of stroke after ablation. Potential improve-ments in quality-adjusted life expectancy resulting fromsuccessful maintenance of sinus rhythm alone were not
considered. Although a large nonrandomized series from 1center has suggested that AF ablation reduces morbidityand mortality relative to drug therapy,20 adequately pow-ered randomized studies to test this hypothesis have notbeen completed. We constructed our model assuming nobenefit for ablation on the risk of stroke; if such a benefitis eventually proven, it would only improve the cost-effectiveness of ablation.
Khaykin et al12 performed a cost comparison of catheterablation for AF and antiarrhythmic drug therapy based onhealth care utilization patterns from Canada and France usingCanadian price weights and concluded that costs wouldequalize over 3 to 8 years of follow-up (4.5 to 11 years with3% discounting applied) due to higher long-term health carecosts with AAD treatment. Although we used a US ratherthan Canadian perspective, our results regarding the rela-tive costs of ablation and drug therapy are qualitativelysimilar to this previous study. Longer-term extrapolationsof our model indicate cost neutrality after �10 years, anestimate within the range of the previous authors’ sensi-tivity analyses. The longer time for this equalization ofcosts in our model may be due both to the higher up-frontcost of ablation in the United States and to the fact that ourmodel shunts the drug cohort toward less expensiverate-controlling drugs over time. In contrast, the Khaykinet al study12 assumed that the use of antiarrhythmic drugswould remain constant over long periods of time, anassumption we find unlikely.41
Most recently, an economic model of a randomized pilotstudy of AF ablation as first-line therapy for paroxysmal AFwas performed,13 again using Canadian price weights. In thisstudy, costs were nearly equal after 2 years, in large partbecause of a 49% rate of crossover to ablation in patientsinitially assigned to AAD therapy. We did not explicitlyevaluate a delayed ablation strategy in our model because webelieve the pertinent health policy and reimbursement ques-tion is not the timing of ablation but its incremental valueover available rhythm control therapies.
The major difference between our study and prior eco-nomic assessments of AF ablation is the explicit incorpora-
Figure 6. Two-way sensitivity analysis on utilityvalues. Each line represents a differentassumed utility score for the rate control andanticoagulation (RCAC) health state, rangingfrom 0.70 to 0.775, with the red line denotingthe base case value. The effect of varying theutility for the well states after ablation (from0.76 to 0.82 on the x-axis) on the iCER (y-axis)are shown. The vertical arrow indicates thebase case value for utility in a well state afterablation (0.79).
366 Circ Arrhythmia Electrophysiol August 2009
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

tion of quality-of-life adjustment as it pertains to sinusrhythm maintenance, which permits the expression of resultsin dollars per QALY, the recommended metric of cost-effectiveness analysis.22 The utility weights used in ouranalysis were derived from analysis of empirical SF-12 andSF-36 data from 3 separate AF populations (2 treated withablation), with highly concordant results (see Appendix). Inthese populations, mean utilities varied from �0.72 to 0.80,which agree well with cross-sectional EQ-5D scores pub-lished by the Euro Heart Survey for AF.33
Our sensitivity analyses indicate that until and unlessmorbidity and mortality benefits are proven, the cost-effectiveness of AF ablation relative to AAD therapy willremain highly contingent on the incremental gains in qualityof life the procedure can provide, at least over a short- tomedium-term time horizon. This implies that AF ablation isunlikely to be cost-effective for patients who enjoy preservedbaseline quality of life despite their AF or for patients whosequality of life is not likely to substantially improve despiteelimination of AF (eg, patients with poor quality of lifemainly due to other health problems). We believe theseobservations offer insights into patient selection for AFablation that are congruent with clinical judgment and currentconsensus recommendations.3,16
Our model may suggest additional insights into whatfactors may increase or decrease the likelihood of ablationbeing cost-effective. Increased single-procedure efficacy, re-duced procedural cost, and/or increased symptomatic benefitwould all improve the cost-effectiveness of ablation relativeto AADs. On the other hand, a short time horizon, reducedcosts for drug loading and follow-up care, better baselinequality of life, a smaller change in quality of life afterablation, and a greater probability of symptom reduction onAAD therapy would all tend to make ablation less attractivefrom a cost-effectiveness perspective.
We believe the assumptions used in our base case wereconservative and, if anything, slightly biased against ablation.For example, longer time horizons would improve the cost-effectiveness of ablation, but we do not think that the currentevidence base permits extrapolation of results beyond 5 years.Additional conservative assumptions in our model includednot using amiodarone (known to have greater efficacy thanalternative drugs) in the ablation arm of the model andestimating single-procedure efficacy with ablation at 60%,with a 25% rate of repeat ablation. Although centers ofexcellence have reported better results than these, we thinkthat these estimates are probably representative of currentgeneral practice.18 Although nonrandomized studies42–44 havesuggested that AF ablation in patients with reduced leftventricular systolic function can improve left ventricularfunction, functional status, and quality of life, we did notincorporate improvements in heart failure into our model.
Our study has important limitations. First, the results ofthis model cannot be directly applied to other subsets of theAF population (eg, newly detected, persistent, or long-standing persistent) because the baseline characteristics ofthose patients, the ablation methods required to achievelong-term success, and the outcomes with ablation and drugtherapy are probably all different than those we estimated.
We did not model all possible treatment strategies for patientswith paroxysmal AF. In selected patients, pharmacologicalrate control alone or pacemaker implantation in conjunctionwith ablation of the AV junction may be reasonable alterna-tives. At present, however, there are limited data directlycomparing these strategies with ablation from which to drawmodel inputs, and our model assumed that patients wereseeking rhythm control strategies because of dissatisfactionwith rate control alone.
As always with cost-effectiveness modeling studies, oursrequired simplifying assumptions and use of some uncertainparameters. One area of particular difficulty in this model wasestimating when symptomatic AF recurrences would prompta change in therapeutic strategy, as trials of AF interventionstypically report all detected recurrences (or time to firstrecurrence) regardless of whether or not such recurrenceswould actually be considered a true therapeutic failure. Forthis reason, we attempted to define model parameters thatmimic published results, for example, in terms of repeatablation, drug discontinuation, and concomitant use of AADsafter ablation.
Finally, we recognize that not all technical approaches tocatheter ablation for AF are the same and that ablationtechniques are rapidly evolving. This was another reason thatwe chose to focus on ablation for paroxysmal AF, in whichthe procedural focus remains more or less focused on elec-trical isolation of the pulmonary veins.3
Sources of FundingDr Reynolds was supported by grant K23 HL077171 from theNational Institutes of Health.
DisclosuresDr Reynolds reports consulting fees from Biosense Webster andSanofi-Aventis. Dr Josesphson reports consulting fees fromBiosense Webster.
References1. Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G,
Garrigue S, Le Mouroux A, Le Metayer P, Clementy J. Spontaneousinitiation of atrial fibrillation by ectopic beats originating in the pulmo-nary veins. N Engl J Med. 1998;339:659–666.
2. Jais P, Haissaguerre M, Shah DC, Chouairi S, Gencel L, Hocini M,Clementy J. A focal source of atrial fibrillation treated by discrete radio-frequency ablation. Circulation. 1997;95:572–576.
3. Calkins H, Brugada J, Packer DL, Cappato R, Chen SA, Crijns HJG,Damiano RJ, Davies DW, Haines DE, Haissaguerre M, Iesaka Y,Jackman W, Jais P, Kottkamp H, Kuck KH, Lindsay BD, Marchlinski FE,McCarthy PM, Mont JL, Morady F, Nademanee K, Natale A, Pappone C,Prystowsky E, Raviele A, Ruskin JN, Shemin RJ. HRS/EHRA/ECASexpert consensus statement on catheter and surgical ablation of atrialfibrillation: recommendations for personnel, policy, procedures andfollow-up. Heart Rhythm. 2007;4:816–861.
4. Noheria A, Kumar A, Wylie JV Jr, Josephson ME. Catheter ablation vsantiarrhythmic drug therapy for atrial fibrillation: a systematic review.Arch Intern Med. 2008;168:581–586.
5. Jais P, Cauchemez B, Macle L, Daoud E, Khairy P, Subbiah R, Hocini M,Extramiana F, Sacher F, Bordachar P, Klein G, Weerasooriya R,Clementy J, Haissaguerre M. Catheter ablation versus antiarrhythmicdrugs for atrial fibrillation: the A4 Study. Circulation. 2008;118:2498–2505.
6. Oral H, Pappone C, Chugh A, Good E, Bogun F, Pelosi F Jr, Bates ER,Lehmann MH, Vicedomini G, Augello G, Agricola E, Sala S, Santinelli
Reynolds et al Cost-Effectiveness of AF Ablation 367
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

V, Morady F. Circumferential pulmonary-vein ablation for chronic atrialfibrillation. N Engl J Med. 2006;354:934–941.
7. Wazni OM, Marrouche NF, Martin DO, Verma A, Bhargava M, SalibaW, Bash D, Schweikert R, Brachmann J, Gunther J, Gutleben K, PisanoE, Potenza D, Fanelli R, Raviele A, Themistoclakis S, Rossillo A, BonsoA, Natale A. Radiofrequency ablation vs antiarrhythmic drugs as first-linetreatment of symptomatic atrial fibrillation: a randomized trial. JAMA.2005;293:2634–2640.
8. Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, SingerDE. Prevalence of diagnosed atrial fibrillation in adults: national impli-cations for rhythm management and stroke prevention: the AnTicoagu-lation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA.2001;285:2370–2375.
9. Coyne KS, Paramore C, Grandy S, Mercader M, Reynolds MR,Zimetbaum P. Assessing the direct costs of treating nonvalvular atrialfibrillation in the United States. Value Health. 2006;9:348–356.
10. Wattigney WA, Mensah GA, Croft JB. Increasing trends in hospital-ization for atrial fibrillation in the United States, 1985 through 1999.Circulation. 2003;108:711–716.
11. Goldberg A, Menen M, Mickelsen S, MacIndoe C, Binder M, Nawman R,West G, Kusumoto FM. Atrial fibrillation ablation leads to long-termimprovement of quality of life and reduced utilization of healthcareresources. J Interv Card Electrophysiol. 2003;8:59–64.
12. Khaykin Y, Morillo CA, Skanes AC, McCracken A, Humphries K, KerrCR. Cost comparison of catheter ablation and medical therapy in atrialfibrillation. J Cardiovasc Electrophysiol. 2007;18:907–913.
13. Khaykin Y, Wang X, Natale A, Wazni OM, Skanes AC, Humphries KH,Kerr CR, Verma A, Morillo CA. Cost comparison of ablation versus antiar-rhythmic drugs as first-line therapy for atrial fibrillation: an economic eval-uation of the RAAFT pilot study. J Cardiovasc Electrophysiol. 2009;20:7–12.
14. Weerasooriya R, Jais P, Le Heuzey JY, Scavee C, Choi KJ, Macle L,Raybaud F, Hocini M, Shah DC, Lavergne T, Clementy J, HaissaguerreM. Cost analysis of catheter ablation for paroxysmal atrial fibrillation.Pacing Clin Electrophysiol. 2003;26:292–294.
15. Chan PS, Vijan S, Morady F, Oral H. Cost-effectiveness of radiofre-quency catheter ablation for atrial fibrillation. J Am Coll Cardiol. 2006;47:2513–2520.
16. Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA,Halperin JL, Le Heuzey JY, Kay GN, Lowe JE, Olsson SB, PrystowskyEN, Tamargo JL, Wann S, ACC/AHA Task Force M, Smith SC Jr, JacobsAK, Adams CD, Anderson JL, Antman EM, Halperin JL, Hunt SA,Nishimura R, Ornato JP, Page RL, Riegel B, ESC Committee for PracticeGroup, Priori SG, Blanc JJ, Budaj A, Camm AJ, Dean V, Deckers JW,Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J,Osterspey A, Tamargo JL, Zamorano JL. ACC/AHA/ESC 2006Guidelines for the Management of Patients With Atrial Fibrillation: areport of the American College of Cardiology/American Heart Asso-ciation Task Force on Practice Guidelines and the European Society ofCardiology Committee for Practice Guidelines (Writing Committee toRevise the 2001 Guidelines for the Management of Patients With AtrialFibrillation). Circulation. 2006;114:e257–e354.
17. Oral H, Knight BP, Tada H, Ozaydin M, Chugh A, Hassan S, ScharfC, Lai SW, Greenstein R, Pelosi F Jr, Strickberger SA, Morady F.Pulmonary vein isolation for paroxysmal and persistent atrial fibril-lation. Circulation. 2002;105:1077–1081.
18. Cheema A, Vasamreddy CR, Dalal D, Marine JE, Dong J, Henrikson CA,Spragg D, Cheng A, Nazarian S, Sinha S, Halperin H, Berger R, CalkinsH. Long-term single procedure efficacy of catheter ablation of atrialfibrillation. J Interv Card Electrophysiol. 2006;15:145–155.
19. Neumann T, Vogt J, Schumacher B, Dorszewski A, Kuniss M, NeuserH, Kurzidim K, Berkowitsch A, Koller M, Heintze J, Scholz U, WetzelU, Schneider MAE, Horstkotte D, Hamm CW, Pitschner HF. Circum-ferential pulmonary vein isolation with the cryoballoon technique:results from a prospective 3-center study. J Am Coll Cardiol. 2008;52:273–278.
20. Pappone C, Rosanio S, Augello G, Gallus G, Vicedomini G, Mazzone P,Gulletta S, Gugliotta F, Pappone A, Santinelli V, Tortoriello V, Sala S,Zangrillo A, Crescenzi G, Benussi S, Alfieri O. Mortality, morbidity, andquality of life after circumferential pulmonary vein ablation for atrialfibrillation: outcomes from a controlled nonrandomized long-term study.J Am Coll Cardiol. 2003;42:185–197.
21. Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, SchronEB, Kellen JC, Greene HL, Mickel MC, Dalquist JE, Corley SD. A com-
parison of rate control and rhythm control in patients with atrial fibrillation.N Engl J Med. 2002;347:1825–1833.
22. Weinstein MC, Siegel JE, Gold MR, Kamlet MS, Russell LB. Recom-mendations of the panel on cost-effectiveness in health and medicine.JAMA. 1996;276:1253–1258.
23. Roy D, Talajic M, Dorian P, Connolly S, Eisenberg MJ, Green M, Kus T,Lambert J, Dubuc M, Gagne P, Nattel S, Thibault B. Amiodarone toprevent recurrence of atrial fibrillation: Canadian Trial of Atrial Fibril-lation Investigators. N Engl J Med. 2000;342:913–920.
24. Singh BN, Singh SN, Reda DJ, Tang XC, Lopez B, Harris CL, FletcherRD, Sharma SC, Atwood JE, Jacobsen AK, Lewis HD, Raisch DW,Ezekowitz MD. Amiodarone versus sotalol for atrial fibrillation. N EnglJ Med. 2005;352:1861–1872.
25. AFFIRM Investigators. Maintenance of sinus rhythm in patients withatrial fibrillation: an AFFIRM substudy of the first antiarrhythmic drug.J Am Coll Cardiol. 2003;42:20–29.
26. National Center for Health Statistics. United States Life Tables, 2003.Available at: http://www.cdc.gov/nchs/products/pubs/pubd/lftbls/life/1966.htm. Accessed September 1, 2006.
27. Cappato R, Calkins H, Chen SA, Davies W, Iesaka YL, Kalman J, KimYH, Klein G, Packer D, Skanes A. World-wide survey on the methods,efficacy, and safety of catheter ablation for human atrial fibrillation.Circulation. 2005;111:1100–1105.
28. Pappone C, Augello G, Sala S, Gugliotta F, Vicedomini G, Gulletta S,Paglino G, Mazzone P, Sora N, Greiss I, Santagostino A, LiVolsi L,Pappone N, Radinovic A, Manguso FS, V. A randomized trial ofcircumferential pulmonary vein ablation versus antiarrhythmic drugtherapy in paroxysmal atrial fibrillation. J Am Coll Cardiol. 2006;48:2340 –2347.
29. Stabile G, Bertaglia E, Senatore G, De Simone A, Zoppo F, Donnici G,Turco P, Pascotto P, Fazzari M, Vitale DF. Catheter ablation treatment inpatients with drug-refractory atrial fibrillation: a prospective, multi-centre, randomized controlled study (Catheter Ablation for the Cure ofAtrial Fibrillation Study). Eur Heart J. 2006;27:216–221.
30. Reynolds MR, Essebag V, Zimetbaum P, Cohen DJ. Healthcare resourceutilization and costs associated with recurrent episodes of atrial fibril-lation: the FRACTAL registry. J Cardiovasc Electrohysiol. 2007;18:628–633.
31. Marshall DA, Levy AR, Vidaillet H, Fenwick E, Slee A, Blackhouse G,Greene HL, Wyse G, Nichol G, O’Brien BJ. Cost-effectiveness of rhythmversus rate control in atrial fibrillation. Ann Intern Med. 2004;141:653–661.
32. Reynolds MR, Ellis E, Zimetbaum P. Quality of life in atrial fibrillation:measurement tools and impact of interventions. J Cardiovasc Electrophysiol.2008;19:762–768.
33. Dagres N, Nieuwlaat R, Vardas PE, Andresen D, Levy S, Cobbe S,Kremastinos DT, Breithardt G, Cokkinos DV, Crijns HJ. Gender-relateddifferences in presentation, treatment, and outcome of patients with atrialfibrillation in Europe: a report from the Euro Heart Survey on AtrialFibrillation. J Am Coll Cardiol. 2007;49:572–577.
34. Ware J, Kosinski M, Keller SD. A 12-item short-form health survey:construction of scales and preliminary tests of reliability and validity.Med Care. 1996;34:220–233.
35. Reynolds MR, Lavelle T, Essebag V, Cohen DJ, Zimetbaum P. Influenceof age, gender, and AF recurrence on quality of life outcomes in apopulation of new-onset AF patients: the FRACTAL registry. AmHeart J. 2006;152:1097–1103.
36. Brazier JE, Roberts J. The estimation of a preference-based measure ofhealth from the SF-12. Med Care. 2004;42:851–859.
37. Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey(SF-36), I: conceptual framework and item selection. Med Care. 1992;30:473–483.
38. Brazier J, Roberts J, Deverill M. The estimation of a preferenced basedmeasure of health from the SF-36. J Health Econ. 2002;21:271–292.
39. Reynolds MR, Cauchemez B, Macle L, Daoud EG, Jais P Health stateutilities improve with catheter ablation for AF more than with drugtherapy: analysis from a randomized trial [abstract]. Circulation. 2007;115:e574–e575.
40. Briggs A, Sculpher M, Buxton M. Uncertainty in the economic evaluationof health care technologies: the role of sensitivity analysis. Health Econ.1994;3:95–104.
41. Nieuwlaat R, Prins MH, Le Heuzey JY, Vardas PE, Aliot E, Santini M,Cobbe SM, Widdershoven JWMG, Baur LH, Levy S, Crijns HJGM.Prognosis, disease progression, and treatment of atrial fibrillation patients
368 Circ Arrhythmia Electrophysiol August 2009
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

during 1 year: follow-up of the Euro Heart Survey on atrial fibrillation.Eur Heart J. 2008;29:1181–1189.
42. Chen MS, Marrouche NF, Khaykin Y, Gillinov AM, Wazni O, MartinDO, Rossillo A, Verma A, Cummings J, Erciyes D, Saad E, Bhargava M,Bash D, Schweikert R, Burkhardt D, Williams-Andrews M, Perez-Lugones A, Abdul-Karim A, Saliba W, Natale A. Pulmonary vein iso-lation for the treatment of atrial fibrillation in patients with impairedsystolic function. J Am Coll Cardiol. 2004;43:1004–1009.
43. Gentlesk PJ, Sauer WH, Gerstenfeld EP, Lin D, Dixit S, Zado E,Callans D, Marchlinski FE. Reversal of left ventricular dysfunctionfollowing ablation of atrial fibrillation. J Cardiovasc Electrophysiol.2007;18:9 –14.
44. Hsu LF, Jais P, Sanders P, Garrigue S, Hocini M, Sacher F, Takahashi Y,Rotter M, Pasquie JL, Scavee C, Bordachar P, Clementy J, HaissaguerreM. Catheter ablation for atrial fibrillation in congestive heart failure.N Engl J Med. 2004;351:2373–2383.
CLINICAL PERSPECTIVEStudies of selected patients with atrial fibrillation have shown that a clinical strategy involving radiofrequency catheterablation results in a higher likelihood of remaining in sinus (normal) rhythm than a strategy of using only antiarrhythmicdrugs, along with greater improvements in quality of life. Catheter ablation, however, is an expensive procedure; thereforethe added costs of catheter ablation must be weighed against the proven benefits before this strategy can be endorsed ona widespread basis. In the current study, we created a disease simulation model (Markov model) to assess thecost-effectiveness of radiofrequency catheter ablation, compared with continued antiarrhythmic drug therapy withoutablation, for patients with paroxysmal atrial fibrillation. The model projected likely outcomes for each treatment over aperiod of 5 years, based on previously published studies, as well as analysis of some newly collected quality-of-life data.We found that the initial extra costs of ablation are partly offset over time by a reduced need for repeat episodes of carefor atrial fibrillation and that the radiofrequency catheter ablation strategy was associated with slightly betterquality-adjusted life expectancy over this time frame. Combining these findings resulted in a cost-effectiveness ratio of�$51 000 per quality-adjusted life-year gained, a value generally considered acceptable within the US health care system.
Reynolds et al Cost-Effectiveness of AF Ablation 369
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from

David J. CohenMatthew R. Reynolds, Peter Zimetbaum, Mark E. Josephson, Ethan Ellis, Tatyana Danilov and
Drug Therapy for Paroxysmal Atrial FibrillationCost-Effectiveness of Radiofrequency Catheter Ablation Compared With Antiarrhythmic
Print ISSN: 1941-3149. Online ISSN: 1941-3084 Copyright © 2009 American Heart Association, Inc. All rights reserved.
Avenue, Dallas, TX 75231is published by the American Heart Association, 7272 GreenvilleCirculation: Arrhythmia and Electrophysiology
doi: 10.1161/CIRCEP.108.8372942009;2:362-369; originally published online April 17, 2009;Circ Arrhythm Electrophysiol.
http://circep.ahajournals.org/content/2/4/362World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circep.ahajournals.org/content/suppl/2009/04/30/CIRCEP.108.837294.DC1Data Supplement (unedited) at:
http://circep.ahajournals.org//subscriptions/
is online at: Circulation: Arrhythmia and Electrophysiology Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Answer
Permissions and Rights Question andunder Services. Further information about this process is available in thepermission is being requested is located, click Request Permissions in the middle column of the Web pageClearance Center, not the Editorial Office. Once the online version of the published article for which
can be obtained via RightsLink, a service of the CopyrightCirculation: Arrhythmia and Electrophysiologyin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 30, 2018http://circep.ahajournals.org/
Dow
nloaded from
SUPPLEMENTAL MATERIAL
This supplemental appendix is intended to provide additional detail beyond that in the
primary manuscript regarding model structure and assumptions, and the sources or
derivation of model inputs. The input values used in the model, with the range of
plausible estimates used in sensitivity analysis, and references of all sources, are shown
in Table 1.
SUPPLEMENTAL METHODS
Event Probabilities
The frequencies of specific procedural complications were estimated from
published literature.1-4 Because relatively minor complications may be under-reported in
single center series, and the bulk of published data on AF ablation comes from selected
centers of excellence, we placed particular emphasis on multi-center and survey data3 in
deriving these estimates.
Recurrence of AF following ablation was estimated from published literature.
Published studies are inconsistent on reporting of results2 with respect to whether
recurrence rates are obtained after 1 or multiple procedures or included supplemental
antiarrhythmic drug therapy. The published rate of repeat ablation procedures varies
widely, and rates as low as 9-12% have been reported in small randomized studies
involving paroxysmal AF patients.5, 6 However, a worldwide survey of AF ablation
reported a 25% repeat procedure rate,3 and individual studies have reported even higher
repeat procedure rates.7 We therefore conservatively calibrated the model to a 25% rate
of repeat procedures. The rate of recurrence requiring a change in therapy was presumed
to be higher than this (and was set at 40%), given that many centers have reported that
some patients achieve control of their AF on previously ineffective AAD therapy after
one procedure. We assumed that no patients would undergo more than 2 ablation
procedures. The ultimate “failure” rate of the ablation strategy was targeted at 10% based
on randomized studies reporting symptomatic recurrences at one year.5, 6 As most
reported AF recurrences after ablation take place early, we assumed a uniform rate of AF
recurrence over 6 months following the initial or repeat ablation.
Base case estimates of recurrent, symptomatic AF on antiarrhythmic drugs were
derived to the greatest extent possible from randomized studies involving AF ablation
patients. 5, 6, 8, 9 While not all AF recurrences on drug therapy necessarily prompt a change
in treatment, we used the rates of crossover to ablation in these studies as a lower bound
of the estimate for treatment failure. We also compared these rates to reported success in
comparative antiarrhythmic drug studies.10 For first line drugs, we assumed a base case
rate of drug failure of 75% over one year, and for second-line treatment with amiodarone,
the base case rate of drug failure was set at 65% over one year. These estimates were
taken from randomized studies of AF ablation compared with AADs in patients with
paroxsysmal (or a mixture of paroxysmal and persistent) AF refractory to one or more
AADs.5, 8, 9
Rates of serious drug toxicity and drug discontinuation due to adverse events were
taken from older literature11, 12 as well as more recent sources.10, 13, 14
Costs
The cost of an AF ablation procedure was set at $15,000. The mean encounter-
level cost of hospital care (procedure + median 1 night observation) in 82 patients who
underwent AF ablation and provided informed consent to participate in an economic and
quality of life study at our institution was $11,898. This does not include physician fees
for the operator or anesthesiologist, when present, and does not include pre-procedure
evaluation (such as an office visit and standard pre-procedure imaging). The higher cost
of an ablation procedure therefore included these additional expenses.
The costs for procedural complications were estimated from an analysis of
Medicare Provider Analysis and Review (MedPAR) files.15 We identified Medicare
admissions to US hospitals between 2001-2006 (N=8288) with AF as the principal
diagnosis during which an RFA was performed (based on diagnosis and procedure
codes), and excluded patients who underwent implantation of a pacemaker or ICD, or had
a surgical ablation during the same hospitalization, or who had a discharge diagnosis of
atrial flutter, Wolff-Parkinson-White syndrome, AV nodal tachycardia, or prior
pacemaker or ICD. The incremental cost of each of the defined procedural complications
was determined by regression modeling on the outcome of hospital costs, adjusting for
demographics, comorbid diagnoses, and the year of treatment.
Following successful ablation without AF recurrence we assumed follow-up costs
of $1300 in the first year (to include short term anticoagulation in all patients, and follow-
up office visits and routine diagnostic testing)4, and $200 per year thereafter.
Follow-up costs for patients in the AAD cohort were taken from the FRACTAL
registry16 (specifically, the group with no documented symptomatic recurrences during

the first year of follow-up, N=650) and a sub-study of the AFFIRM trial.P
17P It was
assumed that antiarrhythmic drug toxicity or a change in antiarrhythmic drug therapy
would incur the costs of a typical telemetry unit hospital admission.
Utilities.
We are aware of no previously published data on health state utilities measured in
an AF ablation population. To address this, we estimated utilities using raw item
responses to the SF-36 and SF-12 general health surveys from three populations of AF
patients – one treated almost exclusively with drug therapy, and two involving AF
ablation. Results of these analyses are plotted together in Figure 1.
We first transformed SF-12 responses to utilities using the method proposed by
Brazier and colleaguesP
18P for patients enrolled in the FRACTAL registry, a population of
~1000 subjects enrolled at the time for first AF diagnosis. P
19, 20P In order to estimate the
change in utility achieved with successful pharmacologic rhythm control of AF, we
compared baseline utilities with follow-up values from 3, 6, and 12 months in patients
with no documented recurrences of AF during the first year of registry follow-up (N=507,
see Figure 1). Baseline mean utility was 0.76 ± 0.13. In paired comparisons at 6 and 12
months, the mean increase in utilities in this group were 0.042 and 0.046, respectively
(p<.0001 by the signed rank test for both comparisons).
We next performed a similar transformation of SF-36 data to utilities for patients
enrolled in the A4 study, a randomized trial comparing antiarrhythmic drugs with
catheter ablation for patients with paroxysmal AF despite ≥1 attempts at drug therapy
(N=112).P
8, 21P Baseline mean utility scores were 0.72 in the ablation group and 0.71 the

AAD group (p=0.22, see Figure 1). At 6 and 12 months, mean utility scores in the
ablation group had increased significantly, by 0.053 and 0.064, respectively, in paired
comparisons (p<0.001 by signed rank for both comparisons). Assessment of changes in
utility in the AAD group were hampered by the 67% rate of crossover to ablation in the
study; prior to crossover, utility scores did not appear to improve at all in AAD patients.
In Figure 1, utilty results are plotted for the AAD group using a “last carried forward”
assumption for crossover patients.
Lastly, we obtained SF-36 data on 78 consecutive patients undergoing catheter
ablation for paroxysmal or persistent AF at Beth Israel Deaconess Medical Center who
provided informed consent to collection of quality of life data. Mean baseline utilities in
this population were 0.74 ± 0.13. As with the A4 ablation patients, utility scores
significantly increased in this population after ablation. While follow-up of this cohort is
ongoing, interim analysis has shown mean changes of 0.064 and 0.059 in paired
comparisons at 6 and 12 months, respectively (p<0.01 by signed rank test for both
comparisons).
Based on the above data, we used a baseline utility value 0.725 for our model,
which is closest to that seen in A4 study, but similar to that obtained from our local
population. We set the increase in utility with successful AF treatment at 0.065, which
was approximately equal to the 12-month change in the A4 study population, and the 6-
month change in our local population (based on preliminary data). While the increase in
utility with successful pharmacologic management in FRACTAL was slightly smaller
(~0.045), the FRACTAL population appeared to be less severely impaired at baseline,
and was a new-onset population, rather than a paroxysmal population seeking alternative

treatment after failing one more drugs. Further, we did not feel the improvement in
utility with successful AAD treatment in the model should differ from that with
successful ablative therapy. We therefore set the utility for each of the model’s ‘well’
states following ablation or AAD therapy to 0.79.
We believe the utility change of 0.065 with successful sinus rhythm maintenance
in this population may be a conservative estimate, because the above data comparing pre-
and post-ablation scores were based on all respondents, not just those who remained in
sinus rhythm during follow-up.

SUPPLEMENTAL TABLES
Table 1: Event probabilities
Variable Base Case (Range) Sources Event probabilities Procedural complications
Procedural death 0.05% (0–0.12%) 1, 3, 22 Vascular access 1.2% (0.9–5%) 1, 3, 22 Perforation/tamponade 0.8% (0.6–1.5%) 1-4 Stroke 0.3% (0.1–0.5%) 1-4 Transient ischemic attack 0.4% (0.1–0.6%) 1-3 PV stenosis 0.4% (0.1–1.6%) 1-4 Pnuemothorax/hemothorax 0.18% (0–0.4%) 1-3 Phrenic nerve palsy 0.1% (0–0.2%) 1-3
Follow-up Events Recur after 1st ablation (6 months) 40% (25–50%) 3, 9, 22 AAD success post 1st ablation 30% (20-40%) Extrapolation from 3
and 5 Redo ablation 25% (9 – 30%) 3, 5, 6, 22 Recur after 2nd ablation 50% (40-60%) Extrapolation from 3 Success on drugs after 2nd ablation (6 months)
35% (20-50%) Assumption
Recur on IC/sotalol (no ablation) (over 12 months)
75% (60-90%)
5, 8-10
Toxicity on IC/sotalol Fatal Nonfatal
0.5% year one, (0-3%), then 0.32% per year 9.5% year one (5-25%), then 1.28% per year
11-14
Recur on amiodarone (no ablation) (over 12 months)
65% (50-80%)
5, 8, 10
Toxicity on amiodarone Fatal Nonfatal
0.1% per year (0-1%) 9.9% year one (5%-20%), then 0.9% (0.5 – 3%) per year
12-14, 23
Costs Ablation procedure $15,000
($10,000 - $20,000) Cost-accounting, 4, 24
Procedural complication
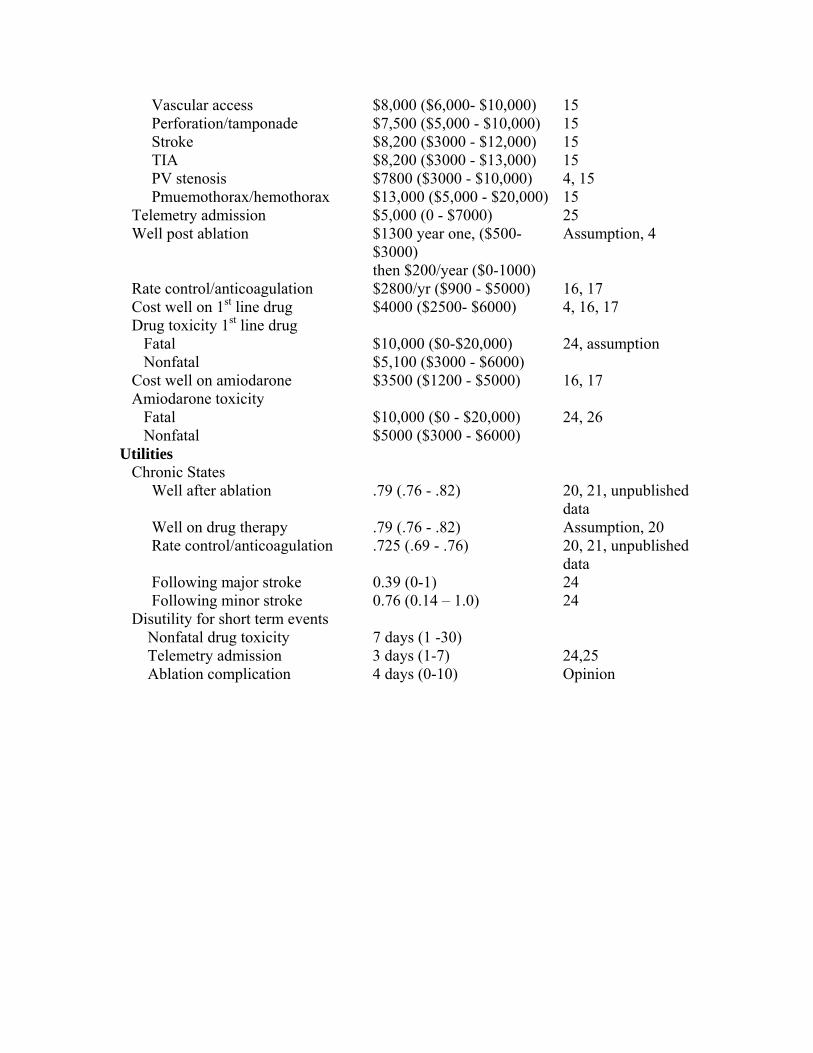
Vascular access Perforation/tamponade Stroke TIA PV stenosis Pmuemothorax/hemothorax
$8,000 ($6,000- $10,000) $7,500 ($5,000 - $10,000) $8,200 ($3000 - $12,000) $8,200 ($3000 - $13,000) $7800 ($3000 - $10,000) $13,000 ($5,000 - $20,000)
15 15 15 15 4, 15 15
Telemetry admission $5,000 (0 - $7000) 25 Well post ablation $1300 year one, ($500-
$3000) then $200/year ($0-1000)
Assumption, 4
Rate control/anticoagulation $2800/yr ($900 - $5000) 16, 17 Cost well on 1st line drug $4000 ($2500- $6000) 4, 16, 17 Drug toxicity 1st line drug Fatal Nonfatal
$10,000 ($0-$20,000) $5,100 ($3000 - $6000)
24, assumption
Cost well on amiodarone $3500 ($1200 - $5000) 16, 17 Amiodarone toxicity Fatal Nonfatal
$10,000 ($0 - $20,000) $5000 ($3000 - $6000)
24, 26
Utilities Chronic States Well after ablation .79 (.76 - .82) 20, 21, unpublished
data Well on drug therapy .79 (.76 - .82) Assumption, 20 Rate control/anticoagulation .725 (.69 - .76) 20, 21, unpublished
data Following major stroke 0.39 (0-1) 24 Following minor stroke 0.76 (0.14 – 1.0) 24 Disutility for short term events Nonfatal drug toxicity 7 days (1 -30) Telemetry admission 3 days (1-7) 24,25 Ablation complication 4 days (0-10) Opinion
SUPPLEMTNAL FIGURES AND FIGURE LEGENDS
Figure 1. Changes in utility scores following treatment with either antiarrhythmic drugs
or catheter ablation in 3 study populations: the FRACTAL registry (green line), the
randomized A4 study (ablation group = red line; drug therapy group = blue line) and a
consecutive series of patients treated with catheter ablation at Beth Israel Deaconess
Medical Center. For all groups, baseline utility scores ranged from 0.71 – 0.76, and for
the 3 groups that maintained sinus rhythm, increased to 0.79 – 0.81. Utility scores did not
improve in A4 control group patients. See text for details.
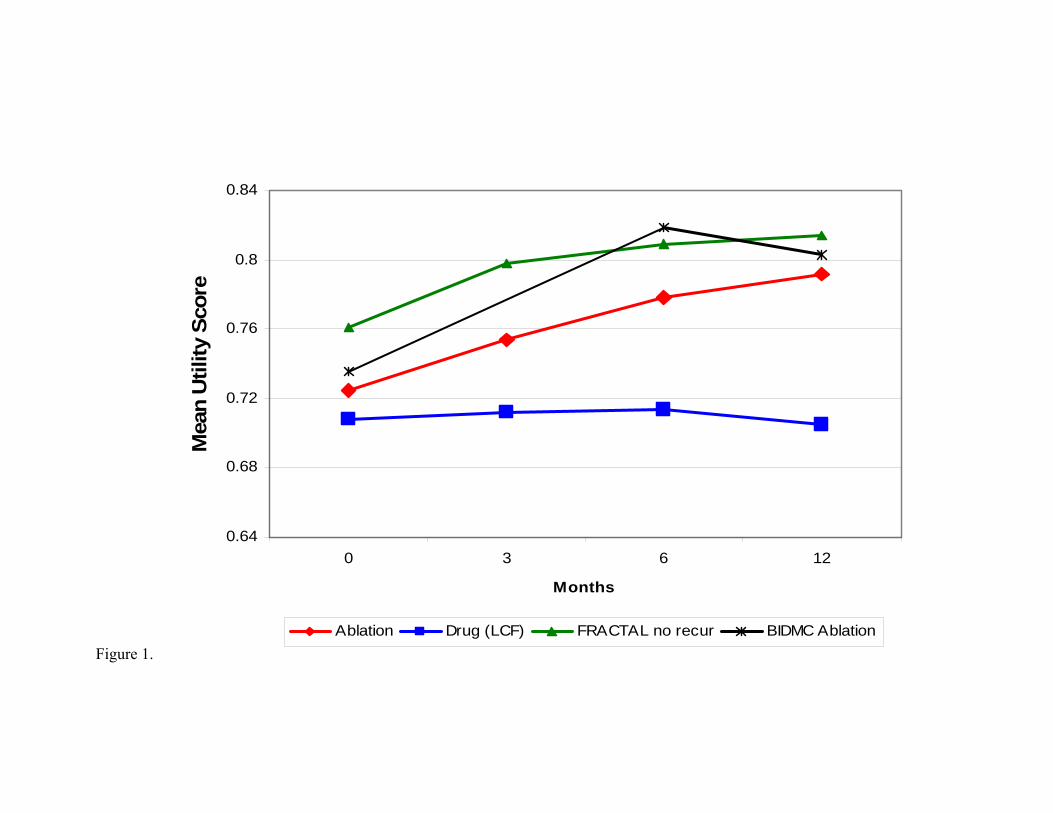
Figure 1.
0.64
0.68
0.72
0.76
0.8
0.84
0 3 6 12
Months
Mea
n U
tility
Sco
re
Ablation Drug (LCF) FRACTAL no recur BIDMC Ablation

REFERENCES 1. Bertaglia E, Zoppo F, Tondo C, Colella A, Mantovan R, Senatore G, Bottoni N,
Carreras G, Coro L, Turco P, Mantica M, Stabile G. Early complications of
pulmonary vein catheter ablation for atrial fibrillation: a multicenter prospective
registry on procedural safety. Heart Rhythm. 2007;4:1265-1271.
2. Calkins H, Brugada J, Packer DL, Cappato R, Chen SA, Crijns HJG, Damiano RJ,
Davies DW, Haines DE, Haissaguerre M, Iesaka Y, Jackman W, Jais P, Kottkamp
H, Kuck KH, Lindsay BD, Marchlinski FE, McCarthy PM, Mont JL, Morady F,
Nademanee K, Natale A, Pappone C, Prystowsky E, Raviele A, Ruskin JN,
Shemin RJ. HRS/EHRA/ECAS expert consensus statement on catheter and
surgical ablation of atrial fibrillation: recommendations for personnel, policy,
procedures and follow-up. Heart Rhythm. 2007;4:816-861.
3. Cappato R, Calkins H, Chen SA, Davies W, Iesaka Yl, Kalman J, Kim Y-H,
Klein G, Packer D, Skanes A. World-wide survey on the methods, efficacy, and
safety of catheter ablation for human atrial fibrillation. Circulation.
2005;111:1100-1105.
4. Khaykin Y, Morillo CA, Skanes AC, McCracken A, Humphries K, Kerr CR. Cost
comparison of catheter ablation and medical therapy in atrial fibrillation. J
Cardiovasc Electrophysiol. 2007;18:907-913.
5. Pappone C, Augello G, Sala S, Gugliotta F, Vicedomini G, Gulletta S, Paglino G,
Mazzone P, Sora N, Greiss I, Santagostino A, LiVolsi L, Pappone N, Radinovic
A, Manguso FS, V. A randomized trial of circumferential pulmonary vein

ablation versus antiarrhythmic drug therapy in paroxysmal atrial fibrillation. J Am
Coll Cardiol. 2006;48:2340-2347.
6. Wazni OM, Marrouche NF, Martin DO, Verma A, Bhargava M, Saliba W, Bash
D, Schweikert R, Brachmann J, Gunther J, Gutleben K, Pisano E, Potenza D,
Fanelli R, Raviele A, Themistoclakis S, Rossillo A, Bonso A, Natale A.
Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of
symptomatic atrial fibrillation: a randomized trial. JAMA. 2005;293:2634-2640.
7. Cheema A, Vasamreddy CR, Dalal D, Marine JE, Dong J, Henrikson CA, Spragg
D, Cheng A, Nazarian S, Sinha S, Halperin H, Berger R, Calkins H. Long-term
single procedure efficacy of catheter ablation of atrial fibrillation. J Interv Card
Electrophysiol. 2006;15:145-155.
8. Jais P, Cauchemez B, Macle LD, E., Khairy P, Subbiah R, Hocini M, Extramiana
F, Sacher F, Bordachar P, Klein G, Weerasooriya R, Clementy J, Haissaguerre M.
Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: The A4 Study.
Circulation 2008;118:2498-2505.
9. Stabile G, Bertaglia E, Senatore G, De Simone A, Zoppo F, Donnici G, Turco P,
Pascotto P, Fazzari M, Vitale DF. Catheter ablation treatment in patients with
drug-refractory atrail fibrillation: a prospective, multi-centre, randomized
controlled study (Catheter Ablation for the Cure of Atrial Fibrillation Study). Eur
Heart J. 2006;27:216-221.
10. Singh BN, Singh SN, Reda DJ, Tang XC, Lopez B, Harris CL, Fletcher RD,
Sharma SC, Atwood JE, Jacobsen AK, Lewis HD, Raisch DW, Ezekowitz MD.
Amiodarone versus sotalol for atrial fibrillation. N Engl J Med. 2005;352:1861-
1872.
11. Eckman MH, Falk RH, Pauker SG. Cost-effectiveness of therapies for patients
with nonvalvular atrial fibrillation. Arch Intern Med. 1998;158:1669-1677.
12. Roy D, Talajic M, Dorian P, Connolly S, Eisenberg MJ, Green M, Kus T,
Lambert J, Dubuc M, Gagne P, Nattel S, Thibault B. Amiodarone to prevent
recurrence of atrial fibrillation. Canadian Trial of Atrial Fibrillation Investigators.
N Engl J Med. 2000;342:913-920.
13. The AFFIRM Investigators. Maintenance of sinus rhythm in patients with atrial
fibrillation: an AFFIRM substudy of the first antiarrhythmic drug. J Am Coll
Cardiol. 2003;42:20-29.
14. Zimetbaum P, Ho KKL, Olshansky B, Hadjis T, Lemery R, Friedman PA,
Cannom DS, Chen XH, Josephson ME. Variation in the utilization of
antiarrhythmic drugs in patients with new-onset atrial fibrillation. Am J Cardiol.
2003;91:81-83.
15. Reynolds MR, Brown PP, Kugelmass AD, Cohen DJ, Simon AW, Culler SD.
Frequency and cost of complications of catheter ablation for atrial fibrillation in
Medicare patients (abstract). Circulation. 2008;117:e457.
16. Reynolds MR, Essebag V, Zimetbaum P, Cohen DJ. Healthcare resource
utilization and costs associated with recurrent episodes of atrial fibrillation: the
FRACTAL registry. J Cardiovasc Electrohysiol. 2007;18:628-633.

17. Marshall DA, Levy AR, Vidaillet H, Fenwick E, Slee A, Blackhouse G, Greene
HL, Wyse G, Nichol G, O'Brien BJ. Cost-effectiveness of rhythm versus rate
control in atrial fibrillation. Ann Intern Med. 2004;141:653-661.
18. Brazier JE, Roberts J. The estimation of a preference-based measure of health
from the SF-12. Med Care. 2004;42:851-859.
19. Reynolds MR, Lavelle T, Essebag V, Cohen DJ, Zimetbaum P. Influence of age,
gender, and AF recurrence on quality of life outcomes in a population of new-
onset AF patients: the FRACTAL registry. Am Heart J. 2006;152:1097-1103.
20. Giedrimas A, Berezin R, Zimetbaum P, Reynolds MR. Preference-based health
measure of new-onset atrial fibrillation in the FRACTAL registry. Circulation.
2007;115:e586 (abstract).
21. Reynolds MR, Cauchemez B, Macle L, Daoud EG, Jais P. Health state utilities
improve with catheter ablation for AF more than with drug therapy: analysis from
a randomized trial. Circulation. 2007;115:e574-575 (abstract).
22. Calkins H, Reynolds MR, Spector P, Sondhi M, Xu Y, Martin A, Williams CJ,
Sledge I. Treatment of atrial fibrillation with anti-arrhythmic drugs or radio-
frequency ablation: two systematic literature reviews and meta-analyses.
Circulation. 2008;118:S773.
23. Hohnloser SH, Kuck KH, Lilienthal J. Rhythm or rate control in atrial fibrillation-
-Pharmacological Intervention in Atrial Fibrillation (PIAF): a randomised trial.
Lancet. 2000;356:1789-1794.
24. Chan PS, Vijan S, Morady F, Oral H. Cost-effectiveness of radiofrequency
catheter ablation for atrial fibrillation. J Am Coll Cardiol. 2006;47:2513-2520.

25. Agency for Healthcare Research and Quality. Healthcare Cost & Utilization
Project. Available at: http://www.ahrq.gov/data/hcup/. Accessed October 1, 2008.
26. Catherwood E, Fitzpatrick D, Greenberg ML, Holzberger PT, Malenka DJ,
Gerling BR, Birkmeyer JD. Cost-effectiveness of cardioversion and
antiarrhythmic therapy in nonvalvular atrial fibrillation. Ann Intern Med.
1999;130:625-636.