cost-effectiveness analysis of a risk-adapted algorithm of plerixafor use for autologous peripheral...
TRANSCRIPT

Biol Blood Marrow Transplant 19 (2013) 87e93
American Society for BloodASBMTand Marrow Transplantation
Cost-Effectiveness Analysis of a Risk-Adapted Algorithmof Plerixafor Use for Autologous Peripheral BloodStem Cell Mobilization
Ivana N.M. Micallef 1,*, Shirshendu Sinha 2, Dennis A. Gastineau 1,Robert Wolf 3, David J. Inwards 1, Morie A. Gertz 1, Suzanne R. Hayman 1,William J. Hogan 1, Patrick B. Johnston 1, Martha Q. Lacy 1, Stephen M. Ansell 1,Francis Buadi 1, David Dingli 1, Angela Dispenzieri 1, Mark R. Litzow1,Luis F. Porrata 1, Jeffrey L. Winters 4, Shaji Kumar 1
1Division of Hematology/Blood & Marrow Transplantation, Mayo Clinic College of Medicine, Rochester, Minnesota2Department of Medicine, Division of Transfusion Medicine, Mayo Clinic College of Medicine, Rochester, Minnesota3Department of Pharmacy, Division of Transfusion Medicine, Mayo Clinic College of Medicine, Rochester, Minnesota4Department of Laboratory Medicine/Pathology, Division of Transfusion Medicine, Mayo Clinic College of Medicine, Rochester,Minnesota
Article history:
Received 20 April 2012Accepted 11 August 2012Key Words:PlerixaforCost effective analysisRisk-adapted algorithmStem cell mobilization
Financial disclosure: See Acknowle* Correspondence and reprint re
of Hematology/Blood & Marrow TrSW, Rochester, MN 55905.
E-mail address: micallef.ivana@
1083-8791/$ e see front matter �http://dx.doi.org/10.1016/j.bbmt.20
a b s t r a c tHistorically, up to 30% of patients were unable to collect adequate numbers of peripheral blood stem cells(PBSCs) for autologous stem cell transplantation (ASCT). Plerixafor in combination with granulocyte colony-stimulating factor (G-CSF) has shown superior results in mobilizing peripheral blood (PB) CD34þ cells incomparison to G-CSF alone, but its high cost limits general use. We developed and evaluated risk-adaptedalgorithms for optimal utilization of plerixafor. In plerixafor-1, PBSC mobilization was commenced withG-CSF alone, and if PB CD34 on day 4 or day 5 was <10/mL, plerixafor was administered in the evening, andapheresis commenced the next day. In addition, if on any day, the daily yield was <0.5 � 106 CD34/kg,plerixafor was added. Subsequently, the algorithm was revised (plerixafor-2) with lower thresholds. If day-4PB CD34 <10/mL for single or <20/mL for multiple transplantations, or day-1 yield was <1.5 � 106 CD34/kg, orany subsequent daily yield was <0.5 � 106 CD34/kg, plerixafor was added. Three time periods were analyzedfor results and associated costs: January to December 2008 (baseline cohort; 319 mobilization attempts in 278patients); February to November 2009 (plerixafor-1; 221 mobilization attempts in 216 patients); andDecember 2009 to June 2010 (plerixafor-2; 100 mobilization attempts in 98 patients). Plerixafor-2 showsa significant improvement in PB CD34 collection, increased number of patients reaching minimum andoptimal goals, fewer days of apheresis, and fewer days of mobilization/collection, albeit at increased costs. Inconclusion, although the earlier identification of ineffective PBSC mobilization and initiation of plerixafor(plerixafor-2) increases the per-patient costs of PBSC mobilization, failure rates, days of apheresis, and totaldays of mobilization/collection are lower.
� 2013 American Society for Blood and Marrow Transplantation.
INTRODUCTIONHigh-dose chemotherapy and autologous stem cell trans-
plantation (ASCT) has become a standard procedure formanypatients with non-Hodgkin lymphoma (NHL), Hodgkinlymphoma, and plasma cell disorders (including multiplemyeloma, POEMS syndrome and immunoglobulin light chainamyloidosis). A requirement to undergo ASCT is adequatemobilization and collection of hematopoietic progenitor cellseither from the bone marrow (BM) or, preferably, from theperipheral blood (PB). The most common strategy forobtaining peripheral blood stem cells (PBSCs) is with gran-ulocyte colony-stimulating factor (G-CSF) alone or in combi-nationwith chemotherapy. Historically, using thesemethods,up to 30% of patients fail to collect a minimum number ofCD34 cells to support ASCT [1,2]. Pusic et al. [2], in a retro-spective review of 1,834 patients undergoing stem cellmobilization for ASCT, demonstrated that 18.6% and 18.8% of
dgment on page 93.quests: Ivana N.M. Micallef, MD, Divisionansplantation, Mayo Clinic, 200 First St,
mayo.edu (I.N.M. Micallef).
2013 American Society for Blood and Marrow12.08.010
patients failed to collect �2 � 106 CD34/kg with G-CSF aloneand G-CSF and chemotherapy, respectively. In addition, only28.7%collected>5�106CD34/kg,whichwasconsidered tobethe optimal cell dose. Similarly, Gertz et al. [1] demonstrateda failure rate of 22% in patients undergoing PBSCmobilizationformultiplemyeloma, NHL, andHodgkin lymphoma. Of 1,775patients undergoing stem cell mobilization, 10% had poorcollections defined at <2 � 106 CD34/kg, and 12% hadno collections attempted as their PB CD34þ cells remained<10/mL. Likewise, only 53% of patients collected the optimalcell dose of >5 � 106 CD34/kg. In the 47% of patients whocollected less than the optimal cell dose, increased resourceconsumption was demonstrated including increased use ofgrowth factors, antibiotics, remobilization attempts, trans-fusion support, increased apheresis procedures, and morefrequent hospitalizations. Other studies have shown thathigher CD34 cell doses result in faster engraftment, shorterhospitalizations, less anti-infective agents, and fewer red celland platelet transfusions, and some studies also showed animproveddisease-free andoverall survival compared to lowerCD34 cell doses [3-8].
Plerixafor is a partial antagonist of the a-chemokinereceptor CXCR4. It reversibly inhibits SDF-1 binding to
Transplantation.

I.N.M. Micallef et al. / Biol Blood Marrow Transplant 19 (2013) 87e9388
CXCR4 [9,10]. It has been shown that an interaction betweenSDF-1 ligand and CXCR4 is important for homing andretention in the BM. When this interaction is interrupted,there is rapid egress of the stem cells from the BM into thePB. Recent phase III studies have shown that plerixafor incombination with G-CSF results in increased mobilization ofCD34þ cells compared to G-CSF alone [11,12]. In addition,plerixafor þ G-CSF have also been shown to successfullymobilize the majority of patients who previously failed tomobilize with either growth factor alone or in combinationwith chemotherapy [13,14].
Plerixafor given in combinationwith G-CSF received Foodand Drug Administration (FDA) approval in December 2008for autologous PBSC mobilization in patients with multiplemyeloma and NHL [15]. However, its high cost has restrictedits universal use in autologous stem cell mobilization. It wasunclear if it should be reserved as a remobilization strategyor for selected patients known to be at high risk for mobili-zation failure. Therefore, we developed a risk-adapted algo-rithm for patients undergoing upfront autologous PBSCmobilization with G-CSF alone. In this algorithm, patientsdemonstrating ineffective stem cell mobilization character-ized by a low PB CD34 cell count during mobilization or byapheresis yield would initiate plerixafor. We hypothesizedthat targeting the patients who were mobilizing poorlywould result in a cost savings compared to universal use ofplerixafor in all patients undergoing upfront mobilizationand be preferable to reserving plerixafor as a remobilizationstrategy.
PATIENTS AND METHODSAll patients provided written informed consent for use of their medical
records. Approval from the Mayo Clinic Institutional Review Board wasobtained in accordance with federal regulations and the Declaration ofHelsinki. All patients undergoing first-time mobilization for ASCT witheither growth factor alone or chemotherapy were included. Patients whoparticipated in the phase II and phase III clinical trials with upfrontplerixaforþG-CSF were excluded from the analysis. Patients who previouslyhad failed to mobilize prior to 2008 were also excluded.
The endpoints analyzed were total CD34þ cells collected during first-time mobilization and remobilization, percentage of patients achieving �2and �4 � 106 CD34/kg, days of apheresis, days of mobilization and collec-tion, plerixafor use including percentage of patients who required plerixaforand number of days of plerixafor, and total costs per patient. For the costanalysis, the costs included the acquisition cost of drugs (G-CSF, granulocytemacrophage colony-stimulating factor, plerixafor, and cyclophosphamide),daily apheresis costs, and cryopreservation costs (Table 1). Supportive carecosts including transfusions, antimicrobials, hospitalization, nursing costs,and the patient’s personal costs were not included. Remobilization costswere added to the first mobilization procedure for the patient’s total costs.
From January 2008 to June 2010, we identified 592 patients from ourprospectively maintained transplantation database who were undergoingtheir first attempt at PBSC mobilization. These patients were divided into 3groups: those mobilized during 2008 served as the “baseline” cohort before
Table 1Cost Analysis Assumptions
Costs Included Cost Costs Not Included
G-CSF $500 per day Chemotherapy if used as salvagetherapy
GM-CSF $500 per day TransfusionsPlerixafor $6,250 per day AntimicrobialsApheresis $1,500 per day Hospital stayCryopreservation $1,500 per
apheresisPatients’ personal costs of foodand lodging
Cyclophosphamide $500 per dose Staffing costseweekend,overtime
G-CSF indicates granulocyte colony-stimulating factor; GM-CSF, gran-ulocyte macrophage colony-forming unit.
the FDA approval of plerixafor, those mobilized using the initial risk-adaptedalgorithm from February to November 2009 were designated “plerixafor-1,”and those using the revised risk-adapted algorithm used from December2009 to June 2010 were designated “plerixafor-2.” Minimal CD34 collectedwas defined as �2 � 106 CD34/kg, and optimal CD34 collected was definedas �4 � 106 CD34/kg.
ApheresisSeveral Fenwal Amicus, version 2.5 (Fenwal Inc., Lake Zurich, IL)
apheresis systems were used. All PBSC collections had an endpoint of 5-hourprocessing time. Anticoagulant was ACD-A (Baxter Healthcare Corp.,Deerfield, IL) or a mixture of ACD-A, normal saline, and heparin [16].
If the patient’s preprocedure peripheralWBC count was>35�109/L, themaximum blood flow rate was 65 mL/min. This was done, as previousstudies demonstrated an adverse effect of a high WBC count on CD34þ cellyields [17,18]. For patients with a WBC count of >35 � 109/L, additionalsettings were as follows: cycle volume 1,000mL, citrate infusion rate 2.5 mg/kg/min, and anticoagulant ratio 13:1. The plasma flush setting was 8 mL. Ifthe patient’s preprocedure peripheral WBC count was �35 � 109/L, thefollowing settings were used: cycle volume 1,400 mL, maximum blood flowrate 90 mL/min, citrate infusion rate 2.50 mg/kg/min, and anticoagulantratio 12:1. The plasma flush setting was 8 mL.
The mononuclear cell offset was 1.5 mL, and the RBC offset was 5.0 mLregardless of the patient’s preprocedure WBC count. If the patient’s pre-procedure preplatelet count was �300 � 109/L, then the RBC offset startedat 6.0 mL. For all collections, the operator observed the first cycle mono-nuclear cell transfer to determine if the RBCs passed completely through theright cassette. If the RBCs did not reach the top of the cassette, the operatorincreased the RBC offsets to the next level for each succeeding cycle until theRBCs reached the top of the right cassette [19].
Baseline Cohort AlgorithmPBSCmobilization consisted of G-CSF given subcutaneously (10 mg/kg/d)
for 4 days with a PB CD34 count measured on day 4. If day 4 PB CD34 countwas �10/mL, apheresis was commenced the following day. If day 4 PB CD34was <10/mL, G-CSF was continued, and the PB CD34 count was measureddaily; once the PB CD34 count was �10/mL, apheresis was started thefollowing day. At the transplantation physician’s discretion, G-CSF could beincreased to 16 mg/kg twice a day. For patients who received chemotherapyin combination with G-CSF, G-CSF was commenced at 5 mg/kg/d, startingday þ1 postchemotherapy. When the WBC count reached >1 � 109/L daily,PB CD34 measurements were commenced. When CD34 reached �10/mL,apheresis commenced. Apheresis was continued daily with G-CSF untileither goal was achieved or until the daily yield was <0.5 � 106 CD34/kg. Ifeither total apheresis was <2 � 106 CD34/kg or if PB CD34 remained <10/mLafter multiple days, then the mobilization attempt was stopped andconsidered a mobilization failure.
Plerixafor-1 Cohort AlgorithmPBSCmobilization consisted of G-CSF given subcutaneously (10 mg/kg/d)
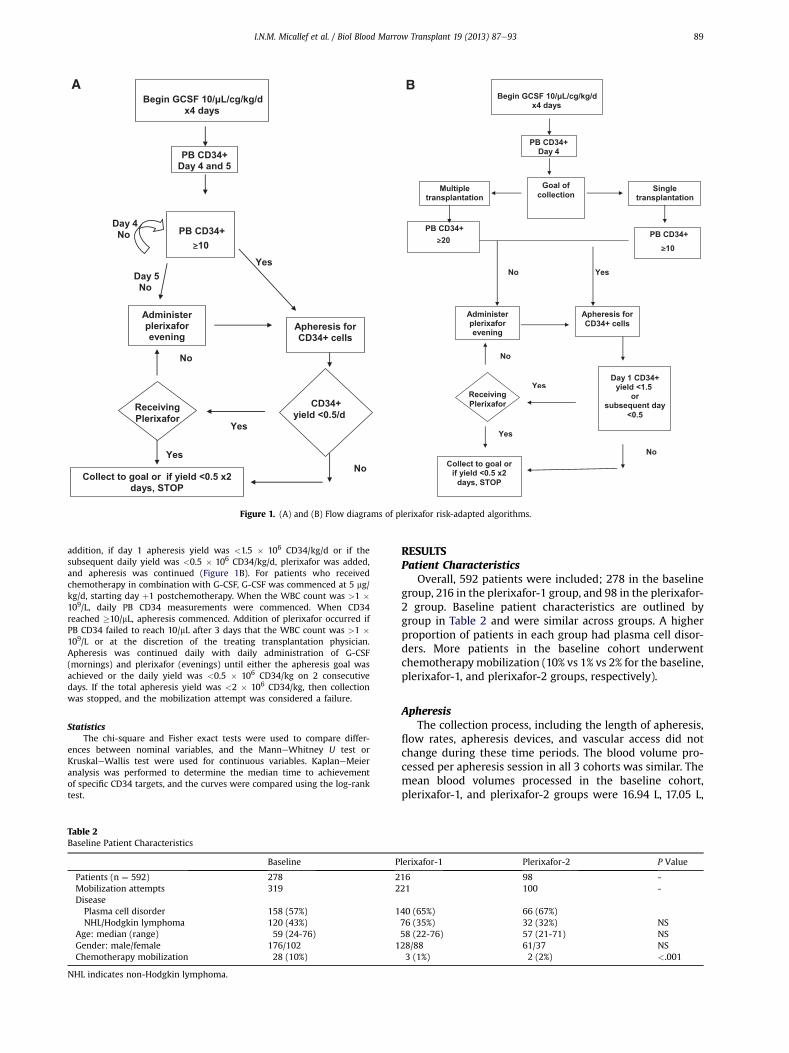
for 4 days with a PB CD34 count measured on day 4. If day 4 PB CD34 countwas �10/mL, apheresis was commenced the following day. If day 4 PB CD34was <10/mL, G-CSF was continued, and the PB CD34 count was measured onday 5. If the PB CD34 count was �10/mL, apheresis was started the followingday. If day 5 PB CD34 was <10/mL, then plerixafor was added (0.24 mg/kg/d)in the evening of day 5, and apheresis was initiated the following day. Inaddition, if the apheresis yield on any day was <0.5 � 106 CD34/kg/d,plerixafor was added, and apheresis was continued (Figure 1A). For patientswho received chemotherapy in combination with G-CSF, G-CSF wascommenced at 5 mg/kg/d, starting day þ1 postchemotherapy. When theWBC count was>1�109/L, daily PB CD34measurements were commenced.When CD34 reached �10/mL, apheresis commenced. In chemotherapymobilization, the addition of plerixafor was at the discretion of the treatingtransplantation physician. Apheresis was continued daily with dailyadministration of G-CSF (mornings) and plerixafor (evenings) until eitherthe apheresis goal was achieved or the daily yield was <0.5 � 106 CD34/kgon 2 consecutive days. If the total apheresis yield was <2 � 106 CD34/kg,then collection was stopped, and the mobilization attempt was considereda failure.
Plerixafor-2 Cohort AlgorithmAs before, PBSC mobilization consisted of G-CSF given subcutaneously
(10 mg/kg/d) for 4 days with a PB CD34 count checked on day 4. If day 4PB CD34 count was �10/mL, or �20/mL if collecting for more than1 transplantation, then apheresis was commenced the following day. Ifday 4 PB CD34 was <10/mL, or <20/mL if collecting for more than1 transplantation, then plerixafor was added (0.24 mg/kg/d) on theevening of day 4, and apheresis was initiated the following day. In
Yes
CD34+
yield <0.5/d
Collect to goal or if yield <0.5 x2
days, STOP
Receiving
Plerixafor
Yes
Apheresis for
CD34+ cells
Yes
Day 5
No
Administer
plerixafor
evening
PB CD34+
10
Begin GCSF 10/µL/cg/kg/d
x4 days
PB CD34+
Day 4 and 5
No
No
Day 4
No
Day 1 CD34+
yield <1.5
or
subsequent day
<0.5
Collect to goal or
if yield <0.5 x2
days, STOP
Receiving
Plerixafor
Yes
Apheresis for
CD34+ cells
Yes
Administer
plerixafor
evening
PB CD34+
10
x4 days
PB CD34+
Day 4
No
No
Multiple
transplantation
Goal of
collection
Single
transplantation
PB CD34+
20
No
Yes
Begin GCSF 10/µL/cg/kg/d
Figure 1. (A) and (B) Flow diagrams of plerixafor risk-adapted algorithms.
I.N.M. Micallef et al. / Biol Blood Marrow Transplant 19 (2013) 87e93 89
addition, if day 1 apheresis yield was <1.5 � 106 CD34/kg/d or if thesubsequent daily yield was <0.5 � 106 CD34/kg/d, plerixafor was added,and apheresis was continued (Figure 1B). For patients who receivedchemotherapy in combination with G-CSF, G-CSF was commenced at 5 mg/kg/d, starting day þ1 postchemotherapy. When the WBC count was >1 �109/L, daily PB CD34 measurements were commenced. When CD34reached �10/mL, apheresis commenced. Addition of plerixafor occurred ifPB CD34 failed to reach 10/mL after 3 days that the WBC count was >1 �109/L or at the discretion of the treating transplantation physician.Apheresis was continued daily with daily administration of G-CSF(mornings) and plerixafor (evenings) until either the apheresis goal wasachieved or the daily yield was <0.5 � 106 CD34/kg on 2 consecutivedays. If the total apheresis yield was <2 � 106 CD34/kg, then collectionwas stopped, and the mobilization attempt was considered a failure.
StatisticsThe chi-square and Fisher exact tests were used to compare differ-
ences between nominal variables, and the ManneWhitney U test orKruskaleWallis test were used for continuous variables. KaplaneMeieranalysis was performed to determine the median time to achievementof specific CD34 targets, and the curves were compared using the log-ranktest.
Table 2Baseline Patient Characteristics
Baseline P
Patients (n ¼ 592) 278 2Mobilization attempts 319 2DiseasePlasma cell disorder 158 (57%) 1NHL/Hodgkin lymphoma 120 (43%)
Age: median (range) 59 (24-76)Gender: male/female 176/102 1Chemotherapy mobilization 28 (10%)
NHL indicates non-Hodgkin lymphoma.
RESULTSPatient Characteristics
Overall, 592 patients were included; 278 in the baselinegroup, 216 in the plerixafor-1 group, and 98 in the plerixafor-2 group. Baseline patient characteristics are outlined bygroup in Table 2 and were similar across groups. A higherproportion of patients in each group had plasma cell disor-ders. More patients in the baseline cohort underwentchemotherapymobilization (10% vs 1% vs 2% for the baseline,plerixafor-1, and plerixafor-2 groups, respectively).
ApheresisThe collection process, including the length of apheresis,
flow rates, apheresis devices, and vascular access did notchange during these time periods. The blood volume pro-cessed per apheresis session in all 3 cohorts was similar. Themean blood volumes processed in the baseline cohort,plerixafor-1, and plerixafor-2 groups were 16.94 L, 17.05 L,
lerixafor-1 Plerixafor-2 P Value
16 98 -21 100 -
40 (65%) 66 (67%)76 (35%) 32 (32%) NS58 (22-76) 57 (21-71) NS28/88 61/37 NS3 (1%) 2 (2%) <.001

Figure 2. (A) Kaplan-Meier cumulative incidence plot of percentage ofpatients achieving CD34 stem cell yield of 2 � 106 CD34/kg based on numberof days. (B) Kaplan-Meier cumulative incidence plot of percentage of patientsachieving CD34 stem cell yield of 4 � 106 CD34/kg based on number of days.
Table 3First Mobilization Results
Patient Cohorts Baseline (n ¼ 278) Plerixafor-1 (n ¼ 216) Plerixafor-2 (n ¼ 98) P Value
CD34 collected (�106/kg)Median 5.6 6.1 7.8Range 0-26 0.1-28 1.6-29.3 <.001Mean 5.9 7 8.3�4 � 106/kg (%) 201 (72%) 181 (84%) 91 (93%) <.001�2 � 106/kg (%) 226 (81%) 206 (95%) 97 (99%) <.001
Day-1 apheresis yield 2.3 (0-26) 2.4 (0.03-28) 3.7 (0.5-29) <.001Mobilization failures 52 (19%) 10 (5%) 1 (1%) <.001Remobilizations 39 (14%) 5 1 <.001Plerixafor use 0 82 (38%) 57 (58%) <.001Indication for plerixafor useDay-4 CD34 <10 - 9 34Day-4 CD34 <20 - - 10Day-5 CD34 <10 - 33 -Day-1 apheresis yield <1.5 � 106/kg - - 10Any apheresis yield <0.5 � 106/kg - 40 3
Days of plerixaforMedian - 3 2 .007
I.N.M. Micallef et al. / Biol Blood Marrow Transplant 19 (2013) 87e9390
and 16.99 L, respectively (P ¼ NS). The median bloodvolumes processed in the baseline cohort, plerixafor-1, andplerixafor-2 groups were 15.99 L, 16.01 L, and 16.10 L,respectively (P ¼ NS).
First Mobilization ResultsThe median CD34 collected during the first mobilization
attempt was 5.6 � 106 CD34/kg in the baseline groupcompared to 6.1 in the plerixafor-1 group and 7.8 in theplerixafor-2 group (Table 3). Significantly more patients wereable to achieve an optimal goal of PBSC in the plerixafor-2group compared to the plerixafor-1 and baseline groups. Inthe baseline cohort, 72% and 81% of patients were able tocollect goals of �4 � 106 CD34/kg and �2 � 106 CD34/kg,respectively. In the plerixafor-1 group, 84% collected �4 �106 CD34/kg, and 95% collected �2 � 106 CD34/kg. In theplerixafor-2 group, 93% collected �4 � 106 CD34/kg and 99%collected�2�106 CD34/kg (P< .001). Themedian estimatedtime to achieving the goal of 4 � 106 CD34/kg was 2 days(95% confidence interval, 2-3), for the baseline andplerixafor-1 groups compared to 2 days (95% confidenceinterval, 1-2) for the plerixafor-2 cohort (P < .001 forcomparison of the cumulative incidence plots, log-rank test,Figure 2A).
The minimum required goal of �2 � 106 CD34/kg wasachieved in 81%, 95%, and 99% of patients in the baseline,plerixafor-1, and plerixafor-2 groups, respectively. Thus,more patients achieved the minimal and optimal CD34results in the plerixafor-2 group compared to either thebaseline or plerixafor-1 groups (P < .001). Conversely, 19% ofpatients in the baseline group failed to mobilize, comparedwith 5% and 1% in the plerixafor-1 and plerixafor-2 groups,respectively (Table 3). The median estimated time toachieving the goal of 2 � 106 CD34/kg was 1 day for all thegroups (P < .001 for comparison of the cumulative incidenceplots, log-rank test, Figure 2B).
Examining other parameters of collection success, day 1apheresis yield (�106 CD34 cells/kg, range) was 2.3 (0-26),2.4 (0.03-28.2), and 3.7 (0.5-29.3), respectively, for thebaseline, plerixafor-1, and plerixafor-2 cohorts (P < .001).Similarly, the cumulative day-1 and 2 apheresis yield (�106
CD34 cells/kg, range) was 4.3 (0-26), 4.4 (0.1-28.2), and 6.5(0.95-29.3), respectively, for the baseline, plerixafor-1, andplerixafor-2 cohorts (P < .001). Overall, the number ofpatients receiving plerixafor during their first mobilization in
each groupwas 0 in the baseline group, 38% in the plerixafor-1 group, and 58% in the plerixafor-2 group.
In the plerixafor-2 group, 57 of 98 patients (58%) receivedplerixafor. Of these 57 patients, 34 and 10 received plerixaforon the evening of day 4 due to a day-4 PB CD34 number of<10 and <20, respectively. Ten patients received plerixaforon day 1, due to day-1 yield <1.5 � 106 CD34/kg, and 3received plerixafor after day 1, due to subsequent daily yieldof <0.5 � 106 CD34/kg.
We also examined the mobilization outcomes based onthe disease types, plasma cell disorders (myeloma andamyloidosis), or lymphomas (NHL or Hodgkin). Overall, the

Table 4Cost Analysis
Baseline Plerixafor-1 Plerixafor-2 P Value
Patients 280 219 98Total cost per patient*
Median $12,500 $12,500 $20,000Minimum $3,000 $5,000 $5,500Maximum $146,750 $93,500 $89,750 .01Mean $17,150 $21,532 $20,617
* Cost analysis includes remobilization costs and has been added to theoriginal mobilization regardless of when the remobilization occurred.
I.N.M. Micallef et al. / Biol Blood Marrow Transplant 19 (2013) 87e93 91
rate of failure to collect the minimum required and theoptimal number of CD34 cells was higher for the lymphomascompared with the plasma cell diseases. Among the plasmacell group, 7% and 14% failed to collect at least 2 and 4millionCD34 cells/kg, respectively, compared with 14% and 29%,respectively, for the lymphoma group (P < .001 for bothcomparisons). We also examined the results with each of thealgorithms within each group. Among the plasma cell group,21%, 11%, and 5% of patients failed to collect the optimal goalof 4 million CD34 cells/kg in the baseline, plerixafor-1, andplerixafor-2 groups, respectively (P < .01). In comparison, inthe lymphoma group, 37%, 26%, and 13% of patients failed tocollect the optimal goal of 4 million CD34 cells/kg in thebaseline, plerixafor-1, and plerixafor-2 groups, respectively(P < .01). Examining the ability to collect the minimum goalof 2million CD34 cells/kg,14%, 2%, and 0% of patients failed toreach the goal in the baseline, plerixafor-1, and plerixafor-2groups among the plasma cell group, respectively (P < .01).Similarly, 25%, 9%, and 3% of patients among the lymphomagroup failed to reach the goal in the baseline, plerixafor-1,and plerixafor-2 groups, respectively (P < .01). Overall, 33%of the plasma cell group and 47% of the lymphoma groupused plerixafor with the plerixafor-1 algorithm (P ¼ .04)compared with 53% of the plasma cell group and 69% of thelymphoma group (P ¼ NS) with the plerixafor-2 algorithm.
Total Mobilization (First and Remobilization) ResultsThirty-nine patients (14%) in the baseline group under-
went at least 1 further attempt at mobilization, compared to5 in the plerixafor-1 group and only 1 patient in theplerixafor-2 group. The median days of apheresis includingremobilization attempts were 2 (range, 0-13) in the baselinecohort, compared to 3 (range,1-12) in the plerixafor-1 group,and 2 (range 1-9) in the plerixafor-2 group (P¼ .01). The totaldays of mobilization and collection were similarly less in theplerixafor-2 group (median 5 days vs 7 days in the baselineand the plerixafor-1 groups). The median (�106 /kg, range)CD34 cell dose collected including remobilization attemptswas 5.2 (0-26), 6.2 (0.4-28), and 7.8 (2.5-29), respectively, inthe baseline, plerixafor-1, and plerixafor-2 groups.
EngraftmentTwo hundred ten (76%), 188 (87%), and 96 patients (98%),
respectively, from the baseline, plerixafor-1, and plerixafor-2groups have so far undergone transplantations. The mediantimes to neutrophil engraftment were 13 days (range,10-50),14 days (9-28), and 14 days (10-45) for the baseline,plerixafor-1, and plerixafor-2 groups, respectively. Themedian times to platelet engraftment were 13 days (0-57), 13days (0-83), and 13 days (10-29), for the baseline, plerixafor-1, and plerixafor-2 groups, respectively. Thus, engraftmenttimes were similar across all 3 groups.
Cost AnalysisThe median total costs of mobilization per patient,
including any remobilization attempt, was $12,500 in thebaseline group, $12,500 in the plerixafor-1 group, and$20,000 in the plerixafor-2 group (Table 4). Although boththe median and mean costs were higher in the plerixafor-2group, the range was narrower, and there were feweroutliers.
DISCUSSIONAdequate PBSC collection is a requirement for ASCT.
Before the FDA approval of plerixafor, approximately 20% of
patients failed to mobilize adequate numbers of CD34þ cells,with growth factor alone or in combination with chemo-therapy. In patients with NHL, the failure rate was higher atapproximately 30% to 35%, with only 29% of patients col-lecting the optimal dose. In multiple myeloma, the failurerate was approximately 15%, and only 30% of patients failedto collect the optimal dose [1]. Numerous studies in the pasthave shown various factors that are associated with poormobilization, including cumulative amounts and type ofchemotherapy, particularly lenalidomide, alkylating agents,purine analogs, and platin-containing regimens. Despitesome patients having none of these risk factors, a substantialnumber mobilized suboptimal numbers of CD34 cells.Because plerixafor is administered on day 4 regardless ofwhether it is an upfront planned G-CSF þ plerixafor mobili-zation or, as outlined in our risk-adapted algorithm based onday-4 CD34 count, pre-existing factors that may increase thelikelihoodof poormobilizationandhence the requirement forplerixafor, were not analyzed. In addition, the treatmentapproaches before mobilization had not changed during thestudy period and hence given the sequential nature, we didnot anticipate there being differences between the groups interms of premobilization clinical factors.
In our study, the baseline cohort (before the FDA approvalof plerixafor) had a failure rate of 19%, which is similar to thatpreviously reported by Pusic et al. [1] and by Gertz et al. [2]Plerixafor in combination with G-CSF is a very effectivemobilization regimen and results in adequate stem cellcollections in the majority of patients [11,12]. However, thereare significant cost implications with the administration ofthe drug and, as evidenced by the fact that the majority ofpatients with multiple myeloma collect optimal stem cellyields, it may not be necessary in all patients.
We developed this risk-adapted algorithm for patientswho experienced ineffective stem cell mobilization, asmeasured by PB CD34 count during mobilization, therebytargeting the patient population who is at risk of poor orfailed mobilization. These are the patients that usuallyrequire increased apheresis days and potentially higherposttransplantation resource utilization of transfusions,antimicrobials, and hospitalizations, if adequate PBSCmobilization is not achieved. Because of the retrospectivenature of this analysis, additional costs including duration ofhospital stay, transfusions, antimicrobial costs, board andlodging costs, and posttransplantation complications werenot collected. The goal of this risk-adapted algorithm was toreduce mobilization failures, increase CD34 mobilizationyields, and limit costs.
PB CD34þ cell counts correlate with the CD34þ apheresiscollection. In a retrospective review of 1,556 patientsundergoing PBSC mobilization at Mayo Clinic, Rochester,Minnesota, it was demonstrated that a day-4 PB CD34 countof approximately 10 cells/mL is associated with a higher

I.N.M. Micallef et al. / Biol Blood Marrow Transplant 19 (2013) 87e9392
likelihood of achieving the minimum threshold needed forASCT of 2 � 106 CD34/kg. In patients with plasma celldisorders, a day-4 PB CD34 count of >10/mL correlated with87% of patients achieving a collection of�4� 106 CD34/kg in5 or less apheresis. When higher apheresis yields are needed,it was found that a day-4 PB CD34 count of �21 was thecutoff required. In patients with a day-4 PB CD34 count of�21, 89% achieved a goal of 8 � 106 CD34/kg compared withonly 49% whose day-4 PB CD34 count was <21. Amongpatients with lymphoma, a day-4 PB CD34 count of �10correlated to 93% success rate of achieving at least 2 � 106
CD34/kg compared to only 45% in those patients who hada PB CD34 count of <10 on day-4. In both the lymphoma andplasma cell disorder cohorts, day-1 apheresis collection alsopredicted total apheresis yield. Day-1 collection of <0.8 inplasma cell disorders and <1.1 � 106 CD34/kg in patientswith lymphoma, predicted for failure to obtain a totalapheresis yield of 2 � 106 CD34/kg [20].
After analysis of plerixafor-1, it became evident that theday-4 PB CD34 count was most important. The majority ofpatients whose PB CD34 count was inadequate (<10) on day4, subsequently received plerixafor because of either lowCD34 count on day 5 or poor daily yield (<0.5�106 CD34/kg)resulting in the addition of plerixafor [21,22]. Patients whohad a day-1 yield of <1.5 also predictably required plerixafordue to subsequent poor daily yields. Therefore, in design ofplerixafor-2, the day-5 PB CD34 count was eliminated, theday-1 yield of <1.5 � 106 CD34/kg and a higher PB CD34target for patients collecting for more than 1 transplantationwere added [23]. The hypothesis for the design of plerixafor-2 was by administering plerixafor earlier to the patients whorequired it because of poor yields, may lessen the number ofdays of apheresis, days of plerixafor use, and improve thetotal apheresis yield.
Our hypothesis for plerixafor-2 was correct, in that theearlier identification of ineffective PBSC mobilization andinitiation of plerixafor (plerixafor-2) improved the results ofPBSC mobilization. This risk-adapted algorithm resulted inmore patients achieving the minimum and optimal yield ofCD34þ cells. The mobilization failure rate was 1%. The use ofthe plerixafor-2 algorithm resulted in fewerdays of apheresis,fewer days of plerixafor, and fewer total days of mobilizationand collection, as compared to the plerixafor-1 algorithm. Anadded benefit was of scheduling in the apheresis unit, asmostpatients complete apheresis by the middle of the week and,therefore, other elective apheresis procedures can be sched-uled later in the week. Weekend scheduling of stem cellcollections has also been avoided. Patients, as well as clinicalstaff, have reported improved satisfaction with a pre-determined plan, rather than waiting for the PB CD34 countto reach the cutoff and initiate apheresis. Lower failure ratesalso translate to fewerdelays in transplantation. Some studieshave reported a survival benefit for “supermobiliziers,” and itremains unclear if collecting more stem cells will translateinto improved survival [4,24]. The1-year survival in the phaseIII studies with G-CSF þ/� plerixafor showed no differencebetween the randomized 2 arms; thus, as of yet, therewas nosurvival benefit in the patients treated with plerixafor [25].Long-term follow-up studies are ongoing, to allow this to bestudied further. Last, because ASCT does not cure all patients,many will require further chemotherapy posttransplantationeither for relapse or as maintenance in multiple myeloma. Ithas been demonstrated that higher CD34þ stem cell yieldsused forASCTare associatedwith improvedgraft durability. Inpatients with NHL, higher CD34þ stem cell doses were
associatedwith ahigher percentageof patientswith a plateletcount of 150 � 109/L at 100 days, 6 months, and 12 monthsposttransplantation [24]. Thus, higher CD34þ cell doses at thetime of ASCT may affect the ability to give further chemo-therapy to treat relapse/progression posttransplantation.
The use of this risk-adapted algorithm of plerixafor-2 wasalso associated with increased costs compared to the base-line and plerixafor-1 cohorts. However, there are a number ofpotential unmeasured costs, which were not included in thecost analysis. This includes both mobilization costs and wellas posttransplantation costs. Posttransplantation costsincluding costs of transfusions, antimicrobials, and hospi-talizationsmay also be increased by slower engraftmentwithless than optimal CD34 cell yields [3,5-8,26]. Two recentstudies, in fewer patients, looking at cost analysis of “just-in-time” salvage plerixafor have also shown higher costs asso-ciated with plerixafor use [27,28].
Chemotherapy mobilization was at the discretion of thetransplantation physician. Although the number of patientsundergoing chemotherapy primed mobilization in eachcohort was small, it is worthwhile to note that with theintroduction of plerixafor, from baseline to plerixafor-1 andplerixafor-2, the number of patients undergoing chemo-therapy for mobilization purposes decreased from 10% to 1%to 2% (P < .001). For patients undergoing chemotherapy-primed mobilization, the period of cytopenias during mobi-lization is associated with potential need for transfusions,antimicrobials, and hospitalizations for complications. Theadditional time for the patient and their personal costs, if theyare away from home, also need to be factored in. Had thesebeen captured in this analysis, it is possible that the costs ofthe baseline cohort would have increased because 10% ofthese patients had undergone chemotherapy mobilizationcompared to only 1% to 2% of plerixafor-1 and plerixafor-2.
Alternatively, in the plerixafor-2 cohort, 58% of patientsrequired plerixafor for a median of 2 days at a median costper patient of $20,000. If plerixafor had been used univer-sally in all patients for a median of 2 days, the median costwould have been approximately $34,000 per patient. Thus,this risk-adapted algorithm allows for selecting the patientswho truly need plerixafor as demonstrated by ineffectiveperipheral stem cell mobilization and thereby is a cost savingcompared to universal use. A recent economic analysis byKymes et al. [29], from the Washington University trans-plantation database determined that using G-CSF þ plerix-afor as upfront mobilization in patients with diffuse large Bcell lymphoma was cost effective. In that analysis, althoughthe cost of providing plerixafor was higher compared toG-CSF alone, there was a benefit in quality-adjusted lifeyears. The expected lifetime cost of providing plerixafor forpatients with diffuse large B cell lymphoma was $25,567more than with G-CSF alone; however, the benefit was anaccumulated 1.74 more quality-adjusted life years and,therefore, it was deemed to be cost effective [29]. In ouranalysis, we did a cost comparison of the differentapproaches in the baseline group, plerixafor-1 algorithm,and plerixafor-2 algorithm. We did not analyze utilityendpoints.
In conclusion, this study demonstrates that a risk-adaptedalgorithm for the use of plerixafor in autologous PBSCmobilization can be effectively implemented. Although theearlier identification of poor mobilizers and addition ofplerixafor does result in higher per-patient costs over base-line, it is associated with higher apheresis yields, fewer daysof mobilization and collection, and lower failure rates.

I.N.M. Micallef et al. / Biol Blood Marrow Transplant 19 (2013) 87e93 93
ACKNOWLEDGMENTThe authors thank the Bone Marrow Transplant (BMT)
data staff for management of the database, the nurses, andallied health staff for caring for the patients, and the BMTnurse coordinators, nurse practitioners, and physicianassistants for their help in implementing the algorithm.
Financial disclosure: The authors have nothing to disclose.
REFERENCES1. Gertz MA, Wolf RC, Micallef IN, Gastineau DA. Clinical impact and
resource utilization after stem cell mobilization failure in patients withmultiple myeloma and lymphoma. Bone Marrow Transplant. 2010;45:1396-1403.
2. Pusic I, Jiang SY, Landua S, et al. Impact of mobilization and remobili-zation strategies on achieving sufficient stem cell yields for autologoustransplantation. Biol Blood Marrow Transplant. 2008;14:1045-1056.
3. Blystad AK, Delabie J, Kvaløy S, et al. Infused CD34 cell dose, but nottumour cell content of peripheral blood progenitor cell grafts, predictsclinical outcome in patients with diffuse large B-cell lymphoma andfollicular lymphoma grade 3 treated with high-dose therapy. Br JHaematol. 2004;125:605-612.
4. Bolwell BJ, Pohlman B, Rybicki L, et al. Patients mobilizing largenumbers of CD34þ cells (’super mobilizers’) have improved survival inautologous stem cell transplantation for lymphoid malignancies. BoneMarrow Transplant. 2007;40:437-441.
5. Gordan LN, Sugrue MW, Lynch JW, et al. Poor mobilization of periph-eral blood stem cells is a risk factor for worse outcome in lymphomapatients undergoing autologous stem cell transplantation. LeukLymphoma. 2003;44:815-820.
6. Limat S, Woronoff-Lemsi MC, Deconinck E, et al. Cost-effectiveness ofCD34þ dose in peripheral blood progenitor cell transplantation fornon-Hodgkin’s lymphoma patients: a single centre study. Bone MarrowTransplant. 2000;25:997-1002.
7. O’Shea D, Giles C, Terpos E, et al. Predictive factors for survival inmyeloma patients who undergo autologous stem cell transplantation:a single-centre experience in 211 patients. Bone Marrow Transplant.2006;37:731-737.
8. Toor AA, Ayers J, Strupeck J, et al. Favourable results with a singleautologous stem cell transplant following conditioning with busulphanand cyclophosphamide in patients with multiple myeloma. Br J Hae-matol. 2004;124:769-776.
9. De Clercq E. The AMD3100 story: the path to the discovery of a stemcell mobilizer (Mozobil). Biochem Pharmacol. 2009;77:1655-1664.
10. DiPersio JF, Uy GL, Yasothan U, Kirkpatrick P. Plerixafor. Nat Rev DrugDiscov. 2009;8:105-106.
11. DiPersio JF, Micallef IN, Stiff PJ, et al. Phase III prospective randomizeddouble-blind placebo-controlled trial of plerixafor plus granulocytecolony-stimulating factor compared with placebo plus granulocytecolony-stimulating factor for autologous stem-cell mobilization andtransplantation for patients with non-Hodgkin’s lymphoma. J ClinOncol. 2009;27:4767-4773.
12. DiPersio JF, Stadtmauer EA, Nademanee A, et al. Plerixafor and G-CSFversus placebo and G-CSF to mobilize hematopoietic stem cells forautologous stem cell transplantation in patients with multiplemyeloma. Blood. 2009;113:5720-5726.
13. Calandra G, McCarty J, McGuirk J, et al. AMD3100 plus G-CSF cansuccessfully mobilize CD34þ cells from non-Hodgkin’s lymphoma,Hodgkin’s disease and multiple myeloma patients previously failingmobilization with chemotherapy and/or cytokine treatment: compas-sionate use data. Bone Marrow Transplant. 2008;41:331-338.
14. Micallef IN, Stiff PJ, DiPersio JF, et al. Successful stem cell remobilizationusing plerixafor (mozobil) plus granulocyte colony-stimulating factorin patients with non-Hodgkin lymphoma: results from the plerixaforNHL phase 3 study rescue protocol. Biol Blood Marrow Transplant. 2009;15:1578-1586.
15. Brave M, Farrell A, Ching Lin S, et al. FDA review summary: mozobilin combination with granulocyte colony-stimulating factor tomobilize hematopoietic stem cells to the peripheral blood for collec-tion and subsequent autologous transplantation. Oncology. 2010;78:282-288.
16. Burgstaler EA, Pineda AA, Winters JL. Hematopoietic progenitor celllarge volume leukapheresis (LVL) on the Fenwal Amicus blood sepa-rator. J Clin Apher. 2004;19:103-111.
17. Burgstaler EA, Pineda AA. The negative effect of high peripheralwhite blood cell count on CD34þ cell recovery. J Clin Apher. 2002;17:148.
18. Burgstaler EA, Pineda AA, Winters JL. Effects of high whole blood flowrates and high peripheral white blood cell counts on CD34þ yield andcross-cellular contamination. Cytotherapy. 2003;5:446.
19. Burgstaler EA, Winters JL. Manual color monitoring to optimize hem-atopooietic progenitor cell collection on the Fenwal Amicus. J ClinApher. 2011;26:123-130.
20. Sinha S, Gastineau D, Micallef I, et al. Predicting PBSC harvestfailure using circulating CD34 levels: developing target-based cutoffpoints for early intervention. Bone Marrow Transplant. 2011;46:943-949.
21. Micallef I, Ansell SM, Buadi F, et al. A risk adapted approach utilizingplerixafor in autologous peripheral blood stem cell mobilization. ASHAnnual Meeting Abstracts. 2009;114:3211.
22. Micallef IN, Inwards DJ, Dispenzieri A, et al. A risk adapted approachutilizing plerixafor in autologous peripheral blood stem cell mobiliza-tion. Biol Blood Marrow Transplant. 2010;16:S197-S198.
23. Micallef IN, Sinha S, Gastineau DA, Wolf R, Inwards DJ, Gertz MA,Hayman SR, Hogan WJ, Johnston PB, Lacy MQ, Ansell SM, Buadi F,Dingli D, Dispenzieri A, Litzow MR, Porrata LF, Winters JL, Kumar S. Acost effective analysis of a risk-adapted algorithm for plerixafor use inautologous peripheral blood stem cell mobilization. Biol Blood MarrowTransplant. 2011 Feb;17(Suppl 2):S159-S160.
24. Stiff PJ, Micallef I, Nademanee AP, et al. Transplanted CD34(þ) cell doseis associated with long-term platelet count recovery followingautologous peripheral blood stem cell transplant in patients withnon-Hodgkin lymphoma or multiple myeloma. Biol Blood MarrowTransplant. 2011;17:1146-1153.
25. Micallef IN, Stiff P, Stadtmauer E, et al. Similar 1 year survival ofpatients receiving plerixafor (Mozobil) plus G-CSF versus placebo plusG-CSF mobilized autologous grafts: results from two phase 3randomized trials in patients with NHL or MM undergoing autologoustransplantation after front-line or rescue mobilization. ASH AnnualMeeting Abstracts. 2009;114:2319.
26. Pavone V, Gaudio F, Console G, et al. Poor mobilization is an inde-pendent prognostic factor in patients with malignant lymphomastreated by peripheral blood stem cell transplantation. Bone MarrowTransplant. 2006;37:719-724.
27. Li J, Hamilton E, Vaughn L, et al. Effectiveness and cost analysis of "just-in-time" salvage plerixafor administration in autologous transplantpatients with poor stem cell mobilization kinetics. Transfusion. 2011;51:2175-2182.
28. Vishnu P, Roy V, Paulsen A, Zubair AC. Efficacy and cost-benefit analysisof risk-adaptive use of plerixafor for autologous hematopoieticprogenitor cell mobilization. Transfusion. 2012;52:55-62.
29. Kymes SM, Pusic I, Lambert DL, Gregory M, Carson KR, DiPersio JF.Economic evaluation of plerixafor for stem cell mobilization. Am JManag Care. 2012;18:33-41.