corporate policy & procedures controlled substances...
TRANSCRIPT

Controlled Substances
Corporate Policy & Procedures
Manual
Number: VII-B-245
Date Approved October 3, 2018
Approved by: Chief Medical Officer; and Chief Operating Officer
Date Effective January 11, 2019
Next Review (3 years from Effective
Date)
January 2022
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms – please refer to the Definitions section.
Purpose To ensure that control of and access to controlled substances is in compliance with the appropriate legislation and the Guidelines for the Secure Distribution of Narcotic and Controlled Drugs in Hospitals (1990).
Policy Statement
Controlled substances shall be safeguarded in a manner that ensures patient/resident/ client1 safety and permits full auditing of the product from receipt through to patient administration. All ordering and administration of controlled substances shall be by health care professional and shall be within the confines of relevant legislation and ensuing Covenant Health policies.
Applicability
This policy and procedure applies to all Covenant Health facilities, staff, medical staff, volunteers, students and any other persons acting on behalf of Covenant Health.
Responsibility
Health care professionals shall demonstrate compliance with this policy, procedure and legislative requirements. The Accountable Leader/designate of the site is responsible for:
all matters related to controlled substances as per the regulations governing narcotic and controlled substances;
delegating the responsibilities of purchasing, receipt of drug deliveries, inventory control and distribution to the manager of Pharmacy/site pharmacist/contract provider; and
delegating the responsibilities of secure storage on patient care units, access to the secure storage, inventory on patient care units and administration to the unit administrator.
1 Hereafter, all references to 'patients' includes residents and clients.

Controlled Substances Date Effective: Jan. 11, 2019
Policy No. VII-B-245 Page 2 of 10
Principles Controlled substances are regulated by the Controlled Drugs and Substances Act and are under the control of the Office of Controlled Substances Division of Health Canada. Controlled substances inventory logs will be numerical, used sequentially, and retained for a period of at least two years.
Procedure 1. STORAGE AND KEYS 1.1 Controlled substances shall be kept in the unit-designated locked storage area. Exception: 1.1.1 When a controlled substance is in the possession of a patient/family
member or health care professional while accompanying a patient to other departments/hospitals/facilities for tests or procedures.
1.1.2 Controlled substances dispensed by Pharmacy as pass medications shall be kept in a secure storage area as per 1.1 above until the patient leaves on pass.
1.1.3 Controlled substances that require refrigeration will be stored securely
with a lock. 1.2 As per Guidelines for the Secure Distribution of Narcotic and Controlled Drugs
in Hospitals (1990), one set of keys will be supplied per each locked storage cabinet.
1.2.1 Any exception to this must be approved by the Site Administrator in
consultation with the Pharmacy Manager or Director.
1.2.2 The key used to access controlled substance storage must be secured or shall be in the possession of a health care professional at all times.
1.2.3 The controlled substances key and patient controlled analgesia (PCA)
pump keys shall be kept separate from one another and from other keys.
1.2.4 The health care professional in charge is responsible for the key and consequently for the contents in locked storage during their shift. The health care professional may delegate this responsibility only to another health care profession.
1.2.5 The unit administrator or delegate is responsible for ensuring that only
health care professionals have access to the controlled substances key and that end of shift counts are completed per policy.
1.2.6 The unit administrator or delegate is responsible to ensure staff who have
identification (ID) access cards to access controlled substance do not share their ID access cards with any other staff.

Controlled Substances Date Effective: Jan. 11, 2019
Policy No. VII-B-245 Page 3 of 10
1.3 Lost keys or ID access cards are immediately communicated to the appropriate management personnel.
1.3.1 The health care professional in charge is responsible for ensuring that
security of contents is maintained until the lock can be changed. 1. 3.2 The appropriate unit administrator or designate must be notified. 1. 3.3 The health care professional in charge or delegate shall sign for and
receive a new lock and key. 1.3.4 If the missing key reappears, it must be returned to Facilities
Management/Physical Plant as soon as possible for disposal.
Exception: Controlled substance cabinets which have a locking Medeco key mechanism will not need to be replaced if key is found as they cannot be duplicated. Lost or missing Medeco key must still be reported as stated in the policy.
1.4 Controlled substances may be stored in automated dispensing cabinets
(example: Pyxis). 1.4.1 The health care professional in charge is responsible to investigate count
discrepancies in locked storage in the automated dispensing cabinets (refer to Section 4). The health care professional may delegate this responsibility only to another health care professional.
1.5 Once a dose of controlled substance has been removed from locked storage,
the medication must remain in the possession of the health care professional until administered. Any amount not immediately administered from a single use dosage form must be wasted and properly documented according to the policy and procedure.
Exception: Controlled substances removed for a patient to be administered
while out on pass or temporary transfer to another care provider. 2. ADMINISTRATION 2.1 For each dose of a controlled substance withdrawn from the storage area, the
following information must be recorded on the daily record of controlled substance administration, or automated dispensing cabinet record as outlined below:
patient name
drug name, dosage form, and quantity removed
drug quantity remaining
date and time of withdrawal
authorized prescriber, and
signature/electronic ID of the health care professional who

Controlled Substances Date Effective: Jan. 11, 2019
Policy No. VII-B-245 Page 4 of 10
withdrew the dose from the storage area
initials may be used provided a signature log is maintained 2.2 When a controlled substance has been administered by a health care
professional while accompanying patients going to other departments / hospitals/facilities for tests or procedures, documentation will be completed as soon as possible Upon return, any unused controlled substances are to be wasted into a sharps/biohazard container and witnessed as such by another health care professional.
3. WASTAGE 3.1 Two health care professional signatures or initials (provided a signature log is
maintained), both of whom have witnessed the destruction, are required for all wastage (including breakage and partially used ampoules, tablets, IV bags or syringes) of controlled substances. See Covenant Health policy #VII-A-55, Automated Medication Dispensing Machines, for wastage in automated dispensing cabinets.
Exception:
1. If there are not two health care professionals available, the wastage may be witnessed by another staff member. That staff member must sign that they witnessed the destruction.
2. Used narcotic patches are to be disposed of in a sharps/biohazard container and do not require a witness.
3.2 All wastage must be disposed in the sharps/ biohazard containers in a manner
that prevents the drugs from being recovered. Do not pour any wastage into the sink or toilet.
4. DISCREPANCIES: COUNTING AND REPORTING 4.1 For patient care units where controlled substances are not stored in automated
dispensing cabinets: 4.1.1 A perpetual inventory (e.g. Record of Controlled Substances Drug
Administration Log) of all controlled substances shall be kept. 4.1.2 At minimum, when authority is transferred (at staff changes) all balances
of controlled substances shall be verified by two health care professionals via physical count.
Unless physically impossible, the health care professional shall be one from the incoming shift and one from the outgoing shift.
Both staff members must verify and sign the daily Record of Controlled Substance Drug Administration Log by:
Controlled Substances Date Effective: Jan. 11, 2019
Policy No. VII-B-245 Page 5 of 10
1. Reviewing that all controlled substances removed from storage since the last count is accurately and completely documented. This includes confirming that the quantities deducted from the perpetual inventory are consistent with the dose administered, that any wastage has been co-signed as being witnessed, that balance totals brought forward to new sheets are accurate and that all the information (as outlined in Section 2.1) is complete.
2. Both health care professionals must visually examine the actual controlled substance products and verify the amount remaining is correct.
3. Both health care professionals must verify the correct counts of controlled substances are recorded on the Record of Controlled Substances Drug Administration Log.
If a discrepancy occurs a recount must be performed. Refer to 4.3 if discrepancy remains.
4.2 For patient care units where controlled substances are stored in automated
dispensing cabinets. See policy/procedure regarding, Automated Medication Dispensing Machines, for count verification procedures.
4.3 For all patient care units where controlled substances are stored, the nurse in
charge shall ensure that all inventory discrepancies are resolved. The charge nurse must verify the count if discrepancy remains. All staff must remain on unit until loss is recovered or all charts, administrations and documentations are verified.
4.3.1 For any controlled substances that have not been accounted for before
authority is transferred, including those in an automated dispensing cabinet, a Controlled Drug and Controlled Substances Discrepancy Resolution Report (Appendix 1) shall be completed and forwarded to the unit administrator. Further investigation may be required dependant on the type of discrepancy. Refer to the Pyxis User Manual for the discrepancy resolution procedure for automated dispensing cabinets.
Exception: A discrepancy directly involving a patient who has been reported through the incident reporting system (RLS) need not be reported via the Narcotic and Controlled Substance Discrepancy Reporting Form.
4.3.2 For bulk oral liquids, an unexplained discrepancy of 10% or less of the
original volume is allowed.
4.3.3 The unit administrator shall conduct a thorough investigation of all discrepancy incidents, and identify any recurring trends. Trends in narcotic or controlled substance discrepancies will be reported to senior
Controlled Substances Date Effective: Jan. 11, 2019
Policy No. VII-B-245 Page 6 of 10
leadership and appropriate investigation and action plans will be implemented.
4.3.4 The theft or suspected theft of controlled substances shall be immediately
reported to Protective Services and Pharmacy Services by the person who discovers the alleged theft.
4.3.5 The unit administrator shall complete the Health Canada Loss or Theft
Report Form for Controlled Substances and Precursors (Appendix 2) and forward to Health Canada for any unexplained loss or any theft or suspected theft of a narcotic within ten days of discovery thereof. The unit administrator will forward a copy to Pharmacy Services for informational purposes.
5. TRANSFER, DELIVERY AND RECEIPT 5.1 When transferring controlled substances from one area inventory to another in
the same site, a unit health care professional or a Pharmacy technician/ assistant must deduct the amount transferred from the inventory (Record of Controlled Substances Drug Administration Log) of the area sending the controlled substance and the same individual must add the amount received to the inventory of the area receiving the controlled substance.
5.2 Two health care professional members’ signatures, one from the transferring
unit and one from the receiving unit are required on each Record of Controlled Substances Drug Administration Log when transferring controlled substance products between units in the same site. For procedure when borrowing from an automated dispensing cabinet, see Policy/Procedure regarding Automated Medication Distribution or Pyxis Manual.
5.3 Controlled substances transported within the site must be transported in a
secure and safe manner. Examples include the use of a locked delivery cart; use of an opaque container; ensuring delivery container is in the staff member’s possession at all times.
5.4 Only health care professionals may requisition and/or pick up controlled
substances from Pharmacy. When picking up medications from Pharmacy, staff must present Hospital ID and Pharmacy staff must verify the ID prior to release of the medications.
5.5 Only health care professionals and pharmacy personnel may deliver controlled
substances within the hospital. 5.6 A form of secured mechanical transportation is permitted to deliver controlled
substances within the same site (i.e. tube system with security features such as password access).
Controlled Substances Date Effective: Jan. 11, 2019
Policy No. VII-B-245 Page 7 of 10
5.7 Requests received by a patient care unit from another site to borrow controlled substances must be referred to the Pharmacy department. The Pharmacy department will follow their internal operational process.
6. PATIENT SPECIFIC NARCOTIC (PSN)
6.1 PSN is a restricted narcotic that is required for the care of a specific patient
while they are admitted, but will not be routinely stocked in patient care areas.
6.1.1 PSN does not apply when a patient care area has an approved Required Organizational Practice Exception for the specified narcotic. (Refer to the High Alert Medications policy, #VII-A-30, for more information regarding Required Organization Practice Exceptions.)
6.2 PSN include by are not limited to the following items:
6.2.1 High potency narcotics restricted:
HYDROmorphone 10mg/mL
HYDROmorphone 50mg/mL
morphine 50mg/mL
6.2.2 Narcotics restricted by Health Canada:
methadone all strengths and forms used for the treatment of addiction
6.2.3 Non-formulary and/or restricted narcotics (e.g. meperidine as per
provincial formulary restrictions).
6.2.4 Patients own narcotic medications following approval by pharmacy.
6.2.5 Patient-specific narcotic epidural infusions
6.3 Pharmacy will label the product directly with:
computer generated patient label
“Please return to Pharmacy when Discontinued” label
appropriate auxiliary labels
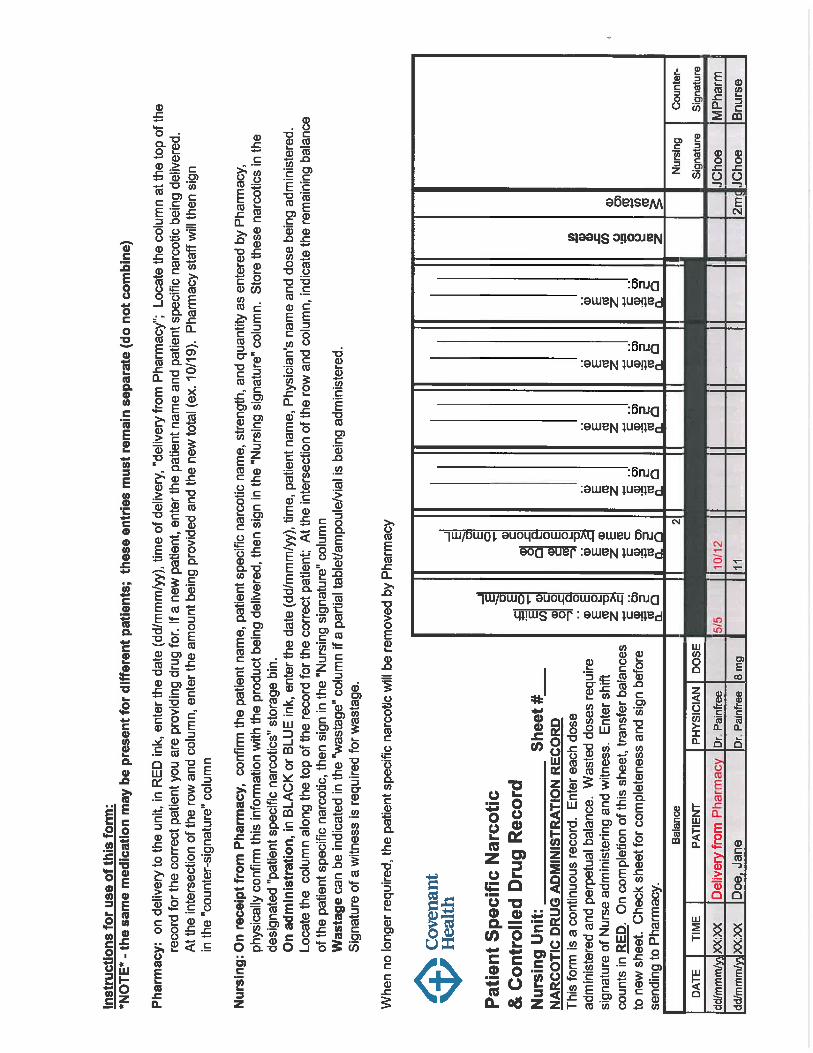
6.4 PSNs will be recorded on a Patient Specific Narcotic and Controlled Drug record. (Appendix 3).
6.4.1 On delivery to the unit, in RED ink, enter the date (dd/mm/yy), and time of
delivery (delivery from pharmacy). 6.4.2 Locate the column at the top of the record for the correct patient. If it is a
new patient, enter patient and PSN being delivered. 6.4.3 At the intersection of the row and column, enter the amount being
provided and the new total (e.g. 10/19). Pharmacy staff will then sign in the “counter signature” column
Controlled Substances Date Effective: Jan. 11, 2019
Policy No. VII-B-245 Page 8 of 10
6.4.4 On receipt, nursing staff will confirm the patient name, PSN, strength and
quantity as entered by pharmacy. Nursing will physically confirm this information with the product being delivered, then sign in the “Nursing signature” column. Store these narcotics in designated PSN storage bins.
6.4.5 PSN storage area is to be labelled with:
High Alert Medication labels
CAUTION High Potency Medication Confirm Dose label
6.5 Nursing Procedures:
6.5.1 On receipt from Pharmacy, a patient care unit health care professional will confirm patient name, PSN name, strength, and quantity as entered by Pharmacy.
6.5.2 Physically confirm all of this information with the product being delivered.
6.5.3 Patient care unit health care professional will sign in the “Nursing
signature” column on the “Patient Specific Narcotic and Controlled Drug Record” sheet.
6.5.4 On administration, in BLACK ink, enter the date (dd/mm/yy), time, patient
name, authorized prescriber, and dose being administered.
6.5.5 Locate the column along the top of the record for the correct patient.
6.5.6 At the intersection of the row and column, indicate the remaining balance of the PSN, then sign in the “Nursing Signature” column.
6.5.7 Wastage can be indicated in the “wastage” column if a partial tablet/
ampoule/vial is being administered.
6.5.8 Signature of a witness is required.
6.6 When no longer required, the patient specific narcotic will be removed by Pharmacy.
7 DISCHARGED PATIENTS 7.1 Refer to Covenant Health policy #VII-B-120, Bridge Supply of Medication for
Discharged Patients for provision of medications to discharged patients. 7.2 For patients being transferred to continuing care beds, including sub-acute and
hospice beds, a sufficient supply of controlled substances may be provided by Pharmacy to last until the receiving facility’s supply can be accessed. Refer to applicable Pass Medications policy.
Controlled Substances Date Effective: Jan. 11, 2019
Policy No. VII-B-245 Page 9 of 10
8. COCAINE and METHADONE 8.1 Cocaine 8.1.1 When possible, cocaine shall be dispensed in the smallest practical
quantity required for administration, in unit dose containers. 8.2 Methadone
8.2.1 In order for a Covenant Health physician/NP to maintain methadone treatment in the hospital setting, the patient must be undergoing current methadone treatment from an authorized prescriber at a methadone clinic.
8.2.2 Physicians must meet specific requirements for initiating or maintaining
methadone treatment per the College of Physicians and Surgeons of Alberta, Opioid Agonist Treatment Program. Nurse practitioners must meet specific requirements as outlined in the CARNA document entitled Prescribing Standards for Nurse Practitioners (2018).
8.2.3 The most responsible health practitioner is required to inform the patient's
community practitioner of the patient's hospitalization and to coordinate the issuance of a methadone prescription prior to patient discharge.
Definitions Authorized prescriber means means a health care professional who is permitted by Federal and Provincial legislation, her/his regulatory college, Covenant Health, and practice
setting (where applicable) to prescribe medications. Controlled substances refers to any substance included in Schedule I, II or III of the Controlled Drugs and Substances Act as amended or repealed from time to time or those drugs deemed by the employer to be handled like a “controlled substance” at the patient care unit, site, or regional level. Schedules can be found on-line http://laws-lois.justice.gc.ca/eng/acts/C-38.8/page-24.html#docCont Key may include electronic means of opening locked storage areas. If the electronic key is assigned to a specific staff members (i.e. via their staff ID badge) and the access to the locked storage area can be traced back to the specific staff member, the requirement for a single key to a locked storage area does not apply. Health care professional means an individual who is a member of a regulated health discipline, as defined by the Health Disciplines Act [Alberta] or the Health Professions Act [Alberta], and who practices within a defined scope and role. Signature - implies hand written, or an electronic signature. Unit administrator -means the out of scope person responsible for the daily operations of the patient care unit.

Controlled Substances Date Effective: Jan. 11, 2019
Policy No. VII-B-245
Page 10 of 10
Related Documents
Appendix 1 – Narcotic and Controlled Substances Discrepancy Reporting Form Appendix 2 – Loss or Theft Report Form for Controlled Substances and Precursors Appendix 3 – Patient specific Narcotic and Controlled Drug record Covenant Health Policies/Procedures:
VII-A-30, High Alert Medications
VII-B-125, Medication Orders
VII-A-50, Medication Administration
VII-B-120, Bridge Supply of Medication for Discharged Patients
III-55, Records Management
Medications for Residence on Pass to Family and Community – Continuing Care Manual (corporate policy in development)
VII-A-55, Automated Dispensing Machines (ADM. Pyxis®)
Patients Own Medications (corporate policy in development)
I-35, Identification Cards
References Pharmacy Services procedure VIII-35 Patient Specific Narcotics. June 20158 Section 56 Class Exemption for Practitioners Prescribing Methadone to Inpatients in a
Hospital Setting. Accessed July 19, 2018 @ https://www.canada.ca/en/health-canada/services/health-concerns/controlled-substances-precursor-chemicals/policy-regulations/policy-documents/section-56-class-exemption-practitioners-prescribing-methadone-inpatients-a-hospital-setting.html
Alberta College of Physicians and Surgeons. Opiod Agonist Treatment Program. accessed
January 4, 2018 @ http://www.cpsa.ca/physician-prescribing-practices/methadone-program/
Pharmacy and Drug Act, Canada. Current as of January 1, 2017. Available @
http://www.qp.alberta.ca/documents/Acts/P13.pdf Prescribing Standards for Nurse Practitioners. June 2018. College and Association of
Registered Nurses of Alberta. Accessed July 19, 2018 @ http://nurses.ab.ca/content/dam/carna/pdfs/DocumentList/Standards/NP_PrescribingStandards_June2018.pdf
Revisions
December 11, 2015 March 11, 2013
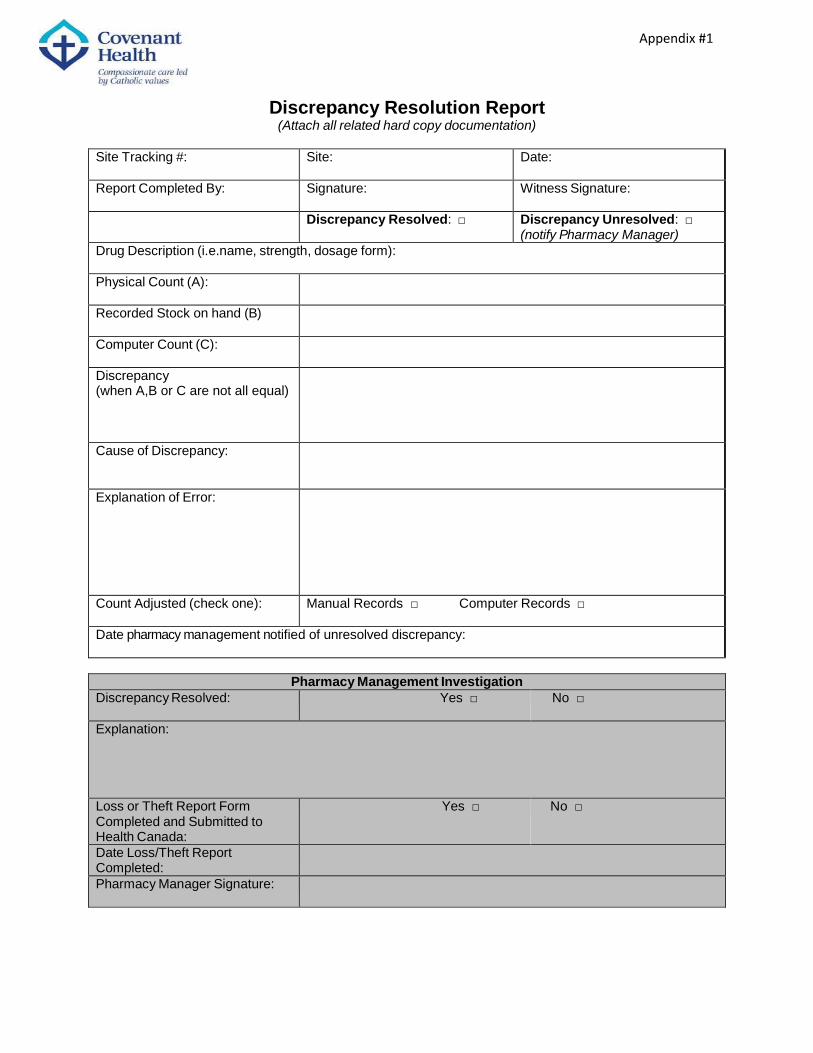
Appendix #1
Discrepancy Resolution Report (Attach all related hard copy documentation)
Site Tracking #: Site: Date:
Report Completed By: Signature: Witness Signature:
Discrepancy Resolved: □ Discrepancy Unresolved: □ (notify Pharmacy Manager)
Drug Description (i.e.name, strength, dosage form):
Physical Count (A):
Recorded Stock on hand (B)
Computer Count (C):
Discrepancy (when A,B or C are not all equal)
Cause of Discrepancy:
Explanation of Error:
Count Adjusted (check one): Manual Records □ Computer Records □
Date pharmacy management notified of unresolved discrepancy:
Pharmacy Management Investigation
Discrepancy Resolved: Yes □ No □
Explanation:
Loss or Theft Report Form Completed and Submitted to Health Canada:
Yes □ No □
Date Loss/Theft Report Completed:
Pharmacy Manager Signature:
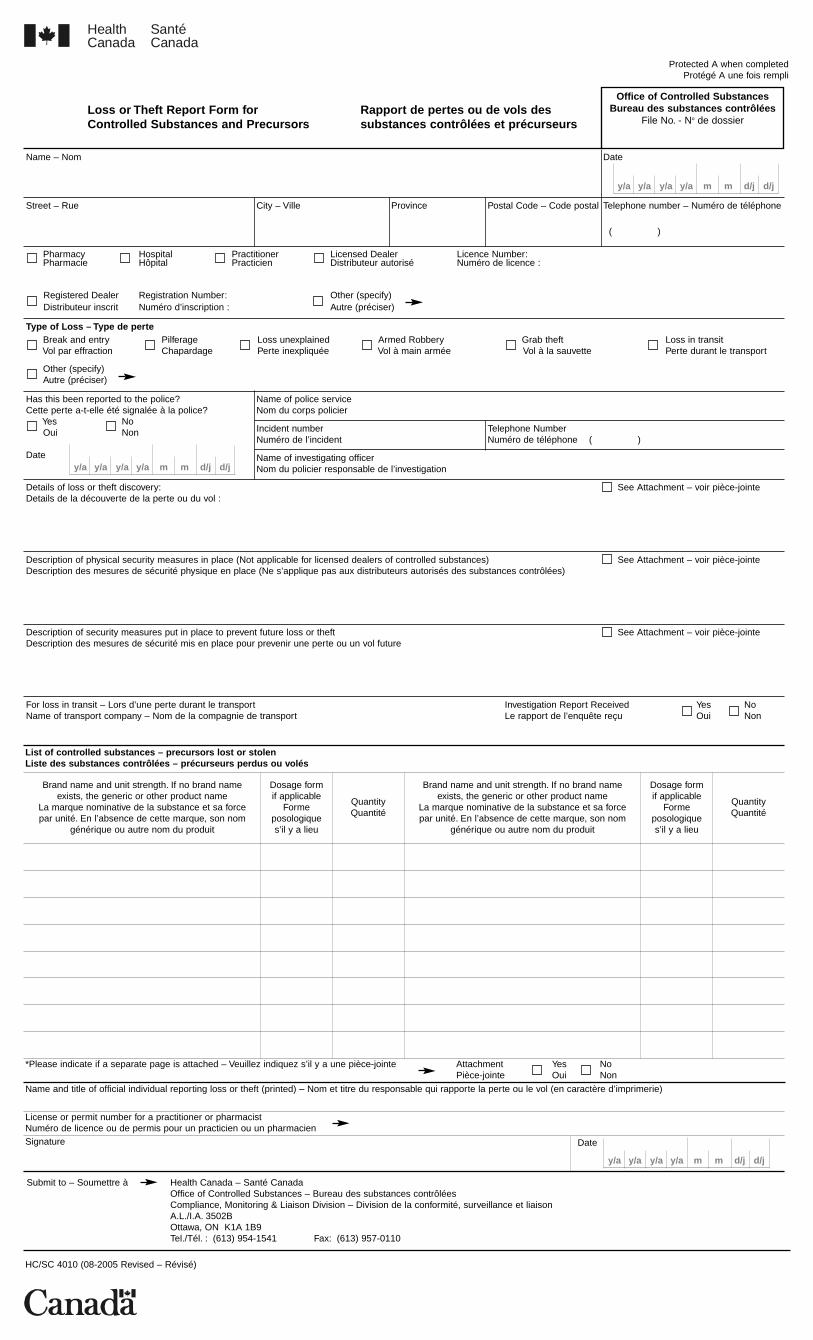
Protected A when completedProtégé A une fois rempli
Loss or Theft Report Form for Rapport de pertes ou de vols desControlled Substances and Precursors substances contrôlées et précurseurs
Health Canada
SantéCanada
Name – Nom Date
Street – Rue City – Ville Province Postal Code – Code postal Telephone number – Numéro de téléphone
( )
Pharmacy Hospital Practitioner Licensed Dealer Licence Number:Pharmacie Hôpital Practicien Distributeur autorisé Numéro de licence :
Registered Dealer Registration Number: Other (specify)Distributeur inscrit Numéro d’inscription : Autre (préciser)
Type of Loss – Type de perteBreak and entry Pilferage Loss unexplained Armed Robbery Grab theft Loss in transitVol par effraction Chapardage Perte inexpliquée Vol à main armée Vol à la sauvette Perte durant le transport
Other (specify)Autre (préciser)
Has this been reported to the police?Cette perte a-t-elle été signalée à la police?
Yes NoOui Non
Date
Name of police serviceNom du corps policier
Incident numberNuméro de l’incident
Telephone NumberNuméro de téléphone ( )
Name of investigating officerNom du policier responsable de l’investigation
Details of loss or theft discovery: See Attachment – voir pièce-jointeDetails de la découverte de la perte ou du vol :
Description of physical security measures in place (Not applicable for licensed dealers of controlled substances) See Attachment – voir pièce-jointeDescription des mesures de sécurité physique en place (Ne s’applique pas aux distributeurs autorisés des substances contrôlées)
Description of security measures put in place to prevent future loss or theft See Attachment – voir pièce-jointeDescription des mesures de sécurité mis en place pour prevenir une perte ou un vol future
For loss in transit – Lors d’une perte durant le transport Investigation Report Received Yes NoName of transport company – Nom de la compagnie de transport Le rapport de l’enquête reçu Oui Non
Office of Controlled SubstancesBureau des substances contrôlées
File No. - No de dossier
y/a y/a y/a y/a m m d/j d/j
y/a y/a y/a y/a m m d/j d/j
List of controlled substances – precursors lost or stolenListe des substances contrôlées – précurseurs perdus ou volés
Brand name and unit strength. If no brand nameexists, the generic or other product name
La marque nominative de la substance et sa forcepar unité. En l’absence de cette marque, son nom
générique ou autre nom du produit
Dosage formif applicable
Formeposologiques’il y a lieu
QuantityQuantité
Brand name and unit strength. If no brand nameexists, the generic or other product name
La marque nominative de la substance et sa forcepar unité. En l’absence de cette marque, son nom
générique ou autre nom du produit
Dosage formif applicable
Formeposologiques’il y a lieu
QuantityQuantité
*Please indicate if a separate page is attached – Veuillez indiquez s’il y a une pièce-jointe Attachment Yes NoPièce-jointe Oui Non
Name and title of official individual reporting loss or theft (printed) – Nom et titre du responsable qui rapporte la perte ou le vol (en caractère d’imprimerie)
License or permit number for a practitioner or pharmacistNuméro de licence ou de permis pour un practicien ou un pharmacienSignature
y/a y/a y/a y/a m m d/j d/j
Date
Submit to – Soumettre à Health Canada – Santé CanadaOffice of Controlled Substances – Bureau des substances contrôléesCompliance, Monitoring & Liaison Division – Division de la conformité, surveillance et liaisonA.L./I.A. 3502BOttawa, ON K1A 1B9Tel./Tél. : (613) 954-1541 Fax: (613) 957-0110
HC/SC 4010 (08-2005 Revised – Révisé)