corporate governance manual - southport and … · corporate governance manual ... to all documents...
TRANSCRIPT

Corporate Governance Manual
Approved by the Board of Directors August 2015
Integrated Care Organisation

Foreword Corporate governance is the system by which an organisation is directed and controlled in order to achieve its objectives and meet the necessary standards of accountability and probity. Effective governance is essential for a Trust to achieve its objectives and fundamental to effective corporate governance is having a robust system of internal control. Legislation such as the NHS Act 2006 and Health and Social Care Act 2012 set out the legal framework within which the Trust must operate. It is a statutory requirement that the Trust Board specify their terms of reference, schedule of reservation and delegation of powers, and the financial framework within which the Trust operates. These key documents comprise the Corporate Governance Manual, which contains:
The Standing Orders, as a framework for Board governance
The Standing Financial Instructions, as a framework for financial governance
The Scheme of Reservation and Delegation, as a framework for internal governance
It is essential that all employees know of the existence of these documents and are aware of their responsibilities as set out within as failure to comply with the Corporate Governance Manual could lead to disciplinary proceedings. Any queries relating to the contents of these documents should be directed to the Company Secretary in the first instance who will be pleased to provide clarification. Ann Marr Interim Accountable Officer August 2015
For
ewor
d
Page 1 of 150
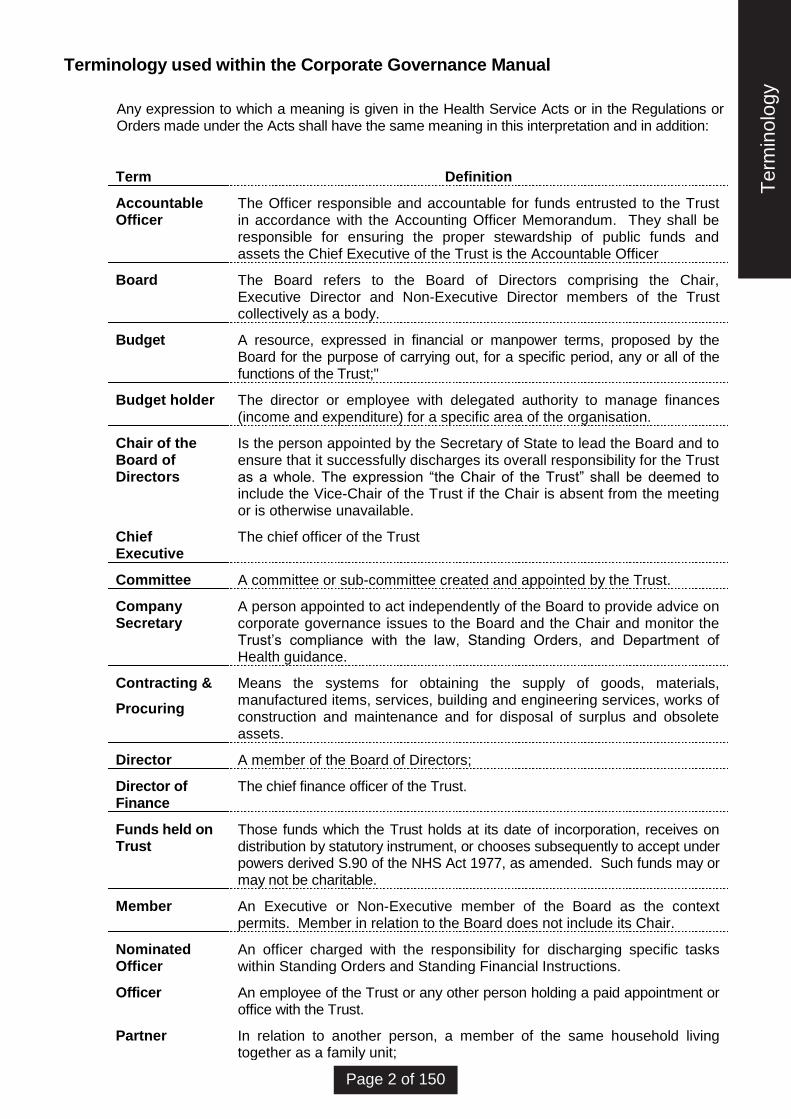
Terminology used within the Corporate Governance Manual
Any expression to which a meaning is given in the Health Service Acts or in the Regulations or Orders made under the Acts shall have the same meaning in this interpretation and in addition:
Term Definition
Accountable Officer
The Officer responsible and accountable for funds entrusted to the Trust in accordance with the Accounting Officer Memorandum. They shall be responsible for ensuring the proper stewardship of public funds and assets the Chief Executive of the Trust is the Accountable Officer
Board The Board refers to the Board of Directors comprising the Chair, Executive Director and Non-Executive Director members of the Trust collectively as a body.
Budget A resource, expressed in financial or manpower terms, proposed by the Board for the purpose of carrying out, for a specific period, any or all of the functions of the Trust;"
Budget holder The director or employee with delegated authority to manage finances (income and expenditure) for a specific area of the organisation.
Chair of the Board of Directors
Is the person appointed by the Secretary of State to lead the Board and to ensure that it successfully discharges its overall responsibility for the Trust as a whole. The expression “the Chair of the Trust” shall be deemed to include the Vice-Chair of the Trust if the Chair is absent from the meeting or is otherwise unavailable.
Chief Executive
The chief officer of the Trust
Committee A committee or sub-committee created and appointed by the Trust.
Company Secretary
A person appointed to act independently of the Board to provide advice on corporate governance issues to the Board and the Chair and monitor the Trust’s compliance with the law, Standing Orders, and Department of Health guidance.
Contracting &
Procuring
Means the systems for obtaining the supply of goods, materials, manufactured items, services, building and engineering services, works of construction and maintenance and for disposal of surplus and obsolete assets.
Director A member of the Board of Directors;
Director of Finance
The chief finance officer of the Trust.
Funds held on Trust
Those funds which the Trust holds at its date of incorporation, receives on distribution by statutory instrument, or chooses subsequently to accept under powers derived S.90 of the NHS Act 1977, as amended. Such funds may or may not be charitable.
Member An Executive or Non-Executive member of the Board as the context permits. Member in relation to the Board does not include its Chair.
Nominated Officer
An officer charged with the responsibility for discharging specific tasks within Standing Orders and Standing Financial Instructions.
Officer An employee of the Trust or any other person holding a paid appointment or office with the Trust.
Partner In relation to another person, a member of the same household living together as a family unit;
Ter
min
olog
y
Page 2 of 150

Term Definition
Standing Financial Instructions
(SFIs) regulate the conduct of the Trusts financial matters
Standing Orders
(SOs) regulate the business conduct of the Trust
Trust Southport & Ormskirk Hospital NHS Trust
All references to the masculine gender will be deemed to apply equally to the feminine gender when used within these instructions.
Ter
min
olog
y
Page 3 of 150
STANDING
ORDERS
Southport & Ormskirk Hospital NHS Trust
Sta
ndin
g O
rder
s
Page 4 of 150

CONTENTS
SECTION
INTRODUCTION 1
INTERPRETATION 2
THE TRUST BOARD: COMPOSITION OF MEMBERSHIP, TENURE, AND ROLE OF
MEMBERS.
3
MEETINGS OF THE TRUST 4
ARRANGEMENTS FOR THE EXERCISE OF FUNCTIONS BY DELEGATION 5
COMMITTEES AND SUB-COMMITTEES 6
DECLARATION OF INTERESTS AND REGISTER OF INTERESTS 7
DISABILITY OF DIRECTORS IN PROCEEDING ON ACCOUNT OF PECUNIARY
INTEREST
8
STANDARDS OF BUSINESS CONDUCT 9
CUSTODY OF THE SEAL AND SEALING OF DOCUMENTS 10
Sta
ndin
g O
rder
s
Page 5 of 150

RECORD OF AMENDMENTS
NO SECTION DATE
1 Updated document Issued for implementation July 2007
2 Document reviewed November 2008
3 Document updated May 2010
4 Document reviewed August 2011
5 Document reviewed May 2013
6 Document reviewed May 2014
7 Document reviewed July 2015
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
Sta
ndin
g O
rder
s
Page 6 of 150

1 INTRODUCTION
1.1 Statutory Framework
1.1.1 Southport & Ormskirk Hospital NHS Trust (the Trust) is a body corporate which was
established under the Southport & Ormskirk Hospital NHS Trust National Health Service Trust
(Establishment) Order 1999 No 890 (the Establishment Order) The principal place of business
of the Trust is Southport District General Hospital, Town Lane, Kew, PR8 6PN.
1.1.2 NHS Trusts are governed by statute, mainly the National Health Service and Community Care
Act 1990 (NHS & CC Act 1990) and the National Health Service Act 1977 (NHS Act 1977) the
NHS Act 1999, the Health and Social Care Act 2001, the National Health Service Act 2006
and the Health and Social Care Act 2012. The statutory functions are conferred on the Trust
by this legislation.
1.1.3 As a statutory body the Trust has specific powers to contract in its own name and to act as a
corporate trustee. In the latter role it is accountable to the Charity Commission for those funds
deemed to be charitable as well as to the Secretary of State for Health.
1.1.4 The Code of Accountability (See Appendices) requires the Trust to adopt Standing Orders
(S.O.s) for the regulation of its proceedings and business. The Trust must also adopt Standing
Financial Instructions (SFIs) as an integral part of Standing Orders setting out the
responsibilities of individuals.
1.1.5 The Trust will also be bound by such other statutes and legal provisions which govern the
conduct of its affairs.
1.2 NHS Framework
In addition to the statutory requirements, the Secretary of State, through the Department of
Health issues further directions and guidance. These are normally issued under cover of a
circular or letter.
1.2.1 The Code of Accountability requires that, inter alia, Boards draw up a schedule of decisions
reserved to the Board known as the ‘Reservation of Powers’, and ensure that management
arrangements are in place to enable responsibility to be clearly delegated to senior executives
(a Scheme of Delegation). The code also requires the establishment of audit and
remuneration committees with formally agreed terms of reference. The Codes of Conduct -
(see Appendices) - makes various requirements concerning possible conflicts of interest of
Board members.
1.2.2 The Code of Practice on Openness in the NHS (see Appendices) and Freedom of Information
Act 2000 sets out the requirements for public access to information on the NHS.
1.3 Delegation of Powers
1.3.1 The Trust has powers to delegate and make arrangements for delegation. The Standing
Orders set out the detail of these arrangements. Under the Standing Order relating to the
Arrangements for the Exercise of Functions (SO 5) the Trust is given powers to "make
arrangements for the exercise, on behalf of the Trust of any of their functions by a committee,
sub-committee or joint committee appointed by virtue of (SO 6) or by an officer of the Trust, in
each case subject to such restrictions and conditions as the Trust thinks fit or as the Secretary
of State may direct". Delegated powers are covered in a separate document (Scheme of
Reservation and Delegation). This document has effect as if incorporated into the Standing
Orders.
1.4 Standing Orders
1.4.1 It is the duty of the Chief Executive to ensure that existing and new Directors and senior officers
are notified of and understand their responsibilities within Standing Orders and Standing
Sta
ndin
g O
rder
s
Page 7 of 150
Financial Instructions. Updated copies shall be issued Directors and senior officers. The
Company Secretary will maintain a record of all recipients.
1.4.2 Standing Orders shall be reviewed annually by the Trust. The requirement for review extends
to all documents having the effect as if incorporated in SOs.
1.5 Policy Statements
1.5.1 The Trust Board will from time to time agree and approve Policy statements/ procedures
which will apply to all or specific groups of staff employed by the Trust. The decisions to
approve such policies and procedures will be recorded in an appropriate Trust Board minute
and will be deemed where appropriate to be an integral part of the Trust's Standing Orders
and Standing Financial Instructions. The Standing Orders and Standing Financial Instructions
must be read in conjunction with the following guidance and any other issued by the Secretary
of State for Health:
- Caldicott Guardian 1997;
- Human Rights Act 1998;
- Freedom of Information Act 2000;
- Data Protection Act 1998;
- Equality Act 2010;
- Bribery Act 2010.
1.5.2 Notwithstanding the application of SO 1.5.1, these Standing Orders and Standing Financial
Instructions must be read in conjunction with the following Policy statements:
- the Staff Code of Personal and Business Conduct and Declarations of Interest Policy
for the Trust staff;
- the Trust Disciplinary Policy which shall have effect as if incorporated in these
Standing Orders.
2. INTERPRETATION
2.1 Chair’s Responsibility
2.1.1. Save as permitted by law, at any meeting the Chair of the Trust shall be the final authority on
the interpretation of Standing Orders (on which he should be advised by the Chief Executive
or Company Secretary).
3. THE TRUST BOARD: COMPOSITION OF MEMBERSHIP, TENURE AND ROLE OF MEMBERS
3.1 Introduction
3.1.1 All business shall be conducted in the name of the Trust.
3.1.2 All funds received in trust shall be in the name of the Trust as corporate trustee. In relation to
funds held on trust, powers exercised by the Trust as corporate trustee shall be exercised
separately and distinctly from those powers exercised as a Trust.
3.1.3 The powers of the Trust established under statute shall be exercised by the Board meeting in
public session except as otherwise provided in Standing Order 4.
3.1.4 The Trust has resolved that certain powers and decisions may only be exercised or made by
the Board in formal session. These powers and decisions are set out in ‘Reservation of
Powers‘ and have effect as if incorporated into the Standing Orders.
Sta
ndin
g O
rder
s
Page 8 of 150

3.2 Composition of the Trust
3.2.1 In accordance with the Establishment Order and Membership and Procedure Regulations
1990 (as amended) the composition of the Board of the Trust shall be:
A Non-Executive Chair, appointed by the Secretary of State (advised by the NHS Trust
Development Authority)
Up to 5 Non-Executive Directors excluding the Chair (appointed by the NHS Trust
Development Authority)
Up to 5 Executive Directors (but not exceeding the non-executive membership) including:-
the Chief Executive
the Director of Finance
a medical practitioner
a registered nurse or midwife
The Trust shall have not more than 11 and not less than 8 members (unless otherwise
determined by the Secretary of State for Health and set out in the Trust’s Establishment
Order or such other communication from the Secretary of State).
3.3 Terms of Office
The regulations governing the period of tenure of office of the Chair and Directors and the
termination or suspension of office of the Chair and Directors are contained in the
Membership and Procedure Regulations 1990 (as amended).
3.3.1 Chair and Non-executive Directors
The Chair and non-executive directors shall be appointed for a term of office not exceeding
four years as the Secretary of State may specify on making the appointment.
The Chair may resign their office at any time during the period of which they were appointed
by giving notice in writing to the Secretary of State. The non-executive directors may resign
their office at any time during the period of which they were appointed by giving notice in
writing to the Chair.
Where during the period of directorship a non executive director of a trust is appointed Chair
of the trust, their tenure of office as a non-executive director shall be terminated when their
appointment as the Chair takes effect.
If the Secretary of State is of the opinion that it is not in the interests of the health service for a
person appointed as a Chair or non-executive director of an NHS trust to continue to hold
office, the Secretary of State may forthwith terminate the person’s tenure of office.
If a Chair or non-executive director of an NHS trust has not attended a meeting of the trust for
a period of three months, the Secretary of State shall forthwith terminate their tenure of office
unless the Secretary of State is satisfied that-
(a) the absence was due to a reasonable cause; and
(b) the Chair or non-executive director will be able to attend meetings of the trust within such
period as the Secretary of State considers reasonable.
Where a person has been appointed the Chair or non-executive director of an NHS trust-
(a) if he becomes disqualified for appointment under regulation 11 Membership and
Procedure Regulations 1990 (as amended) the appointing authority shall forthwith notify them
in writing of such disqualification; or
(b) if it comes to the notice of the appointing authority that at the time of their appointment he
was so disqualified it shall forthwith declare that he was not duly appointed and so notify them
in writing, and upon receipt of any such notification, their tenure of office, if any, shall be
terminated and he shall cease to act as Chair or non-executive director.
Sta
ndin
g O
rder
s
Page 9 of 150

If it appears to the Secretary of State that the Chair or non-executive director of an NHS trust
has failed to comply with regulation 20 (disclosure etc. on account of pecuniary interest) he
may forthwith terminate that person's tenure of office.
3.3.2 Accountable Officer and Chief Finance Officer
The Accountable Officer (Chief Executive) and the Chief Finance Officer (Director of Finance)
shall hold office for as long as they hold the post in the trust.
3.3.3 Executive Directors
If an executive director is suspended from their post in the trust they shall be suspended from
performing their function as a director for the period of the suspension.
An executive director may resign their office at any time by giving notice in writing to the Chief
Executive, who will in turn notify the Remuneration & Nominations Committee. The Chief
Executive may resign their office at any time by giving notice in writing to the Chair who will in
turn notify the Remuneration & Nominations Committee.
3.3.4 Appointing Chief Executive & Other Directors
The Trust shall appoint a Nominations committee whose members shall be the Chair and
Non-Executive Directors of the Trust whose function will be to appoint the Chief Executive as
a Director of the Trust. The Committee will co-opt the Chief Executive as a member when
appointing the Executive directors of the Trust.
3.4 Disqualification as a Director
The following may not become or continue as a Director:
(a) A person who has received a prison sentence or suspended sentence of three months or
more in the last five years.
(b) A person who has been the subject of a bankruptcy restriction order or interim order..
(c) Anyone who has been dismissed (except by redundancy) by any NHS body.
(d) Anyone who is under a disqualification order under the Company Directors
Disqualification Act 1986.
(e) Anyone who has been removed from trusteeship of a charity.
3.5 Appointment of Vice-Chair
3.5.1 For the purpose of enabling the proceedings of the Trust to be conducted in the absence of
the Chair, the Directors of the Trust may appoint a Non-Executive Director from amongst them
to be Vice-Chair for such a period, not exceeding the remainder of their term as Non-
Executive Director, as they may specify on appointing him/her.
3.5.2 Any Non-Executive Director so elected may at any time resign from the office of Vice-Chair by
giving notice in writing to the Chair and the Directors of the Trust may thereupon appoint
another Non-Executive Director as Vice-Chair in accordance with Standing Order 3.4.1.
3.5.3 In order to appoint the Vice-Chair, nominations, including self-nominations, will be invited
within a period of time set by the Board. Where there is more than one nomination a postal
vote will be conducted and the results announced at the subsequent meeting of the Board. In
the event of there being only one nomination and this being acceptable to the Directors
present, the Board will be requested to confirm that person as Vice-Chair at the meeting in
Sta
ndin
g O
rder
s
Page 10 of 150

which the nomination is made.
3.5.4 In the event of nominations recording equal number of votes Standing Orders will apply, and
the Chair of the Board will use a casting vote at the meeting following the postal vote.
3.6 Powers of Vice-Chair
3.6.1 Where the Chair of an NHS Trust has died or has otherwise ceased to hold office or where he
has been unable to perform their duties as Chair owing to illness, absence from England and
Wales or any other cause, references to the Chair in the Schedule to these Regulations shall,
so long as there is no Chair able to perform their duties, be taken to include references to the
Vice-Chair.
3.7 Joint Members
3.7.1 Where more than one person is appointed jointly to a post mentioned in regulation 2(4)(a) of
the Membership, Procedure and Administration Arrangements Regulations those persons
shall count for the purpose of Standing Order 3.2 as one person.
3.7.2 Where the office of a member of the Board is shared jointly by more than one person:
(a) either both of those persons may attend or take part in meeting of the Board;
(b) if both are present at a meeting they should cast one vote if they agree;
(c) in the case of disagreements no vote should be cast;
(d) the presence of either or both of those persons should count as the presence of one
person for the purposes of Standing Order 4.1.4.
3.8 Role of Members
The Board will function as a unitary Board, Non-Executive and Executive Directors will be full and
equal members. Their role as members of the Board of Directors will be to consider the key
strategic and managerial issues facing the Trust in carrying out its statutory and other functions.
(1) Chief Executive
The Chief Executive will be responsible for the overall performance of the executive
functions of the Trust. He/she is the Accountable Officer for the Trust and will be
responsible for ensuring the discharge of obligations under Financial Directions and in line
with the requirements of the Accountable Officer Memorandum for Trust Chief Executives.
(2) Director of Finance
The Director of Finance will be responsible for the provision of financial advice to the Trust
and to its members and for the supervision of financial control and accounting systems.
He/she will be responsible along with the Chief Executive for ensuring the discharge of
obligations under relevant Financial Directions.
(3) Executive Members
Executive Members will exercise their authority within the terms of these Standing Orders
and Standing Financial Instructions and Scheme of Reservation and Delegation.
(4) Non-Executive Members
The Non-Executive Members will not be granted nor will they seek to exercise any
individual executive powers on behalf of the Trust. They may however, exercise collective
authority when acting as members of or when chairing a committee of the Trust which has
delegated powers.
(5) Chair
Sta
ndin
g O
rder
s
Page 11 of 150
The Chair will be responsible for the operation of the Board and chair all Board meetings.
The Chair has certain delegated executive powers. The Chair must comply with the terms
of appointment and with these Standing Orders.
The Chair will liaise with the NHS Trust Development Authority over the appointment of
Non-Executive Directors and once appointed will take responsibility either directly or
indirectly for their induction, their portfolios of interests and assignments, and their
performance.
The Chair will work in close harmony with the Chief Executive and will ensure that key and
appropriate issues are discussed by the Board in a timely manner with all the necessary
information and advice being made available to the Board to inform the debate and
ultimate resolutions.
(6) Non-Voting Members
In preparation for Foundation Trust status the Board appointed two non-voting Members,
one Non-Executive and one Executive, to strengthen the Board composition. Both Non-
voting members may exercise their authority within the terms of these Standing Orders,
Standing Financial Instructions and Scheme of Reservation and Delegation. Non-voting
members may participate in discussions at Board but do not have voting rights.
3.9 Schedule of Matters Reserved to the Board and Scheme of Delegation
The Board has resolved that certain powers and decisions may only be exercised by the Board in
formal session. These powers and decisions are set out in the Schedule of Matters Reserved to
the Board and shall have effect as if incorporated into the Standing Orders. Those powers which
it has delegated to officers and other bodies are contained in the Scheme of Delegation.
3.10 Lead Roles for Board Members
The Chair will ensure that the designation of lead roles or appointments of Board Members as
required by any statutory or regulatory guidance will be made in accordance with that statutory
requirement.
4. MEETINGS OF THE TRUST
4.1 Openness
4.1.1 All ordinary meetings of the Board are open meetings and members of the public can attend
these meetings. As such they are considered to be meetings where the public may observe
the decision-making process of the Trust. They are not open meetings where the public have
a right to contribute to the debate. Contributions from the public at such meetings can be
considered at the discretion of the Chair.
4.1.2 Exceptionally, there may be items of a confidential nature on the agenda of these ordinary
meetings from which the public may be excluded. Such items will be business that:-
relates to a member of staff;
relates to a patient;
would commercially disadvantage the Trust if discussed in public; or,
would be detrimental to the operation of the Trust.
Members and Officers or any employee of the Trust in attendance shall not reveal or disclose
the contents of papers marked ‘In Confidence’ or minutes headed ‘Items Taken in Private’
outside of the Trust, without the express permission of the Trust. This prohibition shall apply
equally to the content of any discussion during the Board meeting which may take place on
such reports or papers.
Sta
ndin
g O
rder
s
Page 12 of 150

4.1.3 Before each meeting of the Trust a public notice of the time and place of the meeting, and the
public part of the agenda, shall be displayed at the Trust’s office at least three clear days
before the meeting (required by the Public Bodies (Admission to Meetings) Act 1960 SI(4)(a).
4.1.4 Admission of the Public and the Press – The public and representatives of the press shall be
afforded facilities to attend all formal meetings of the Board but shall be required to withdraw
upon the Board resolving as follows:
“That representatives of the press and other members of the public be excluded from the
remainder of this meeting having regard to the confidential nature of the business to be
transacted, publicity on which would be prejudicial to the public interest” (Section 1(2) Public
Bodies (Administration to Meetings) Act 1960).
4.1.5 The Chair (or person presiding the meeting) shall give such directions as he thinks fit in regard
to the arrangements for meetings and accommodation of the public and representatives of the
press such as to ensure that the Board’s business shall be conducted without interruption and
disruption and, without prejudice to the power to exclude on grounds of the confidential nature
of the business to be transacted. The public will be required to withdraw upon the Board
resolving as follows:
“That in the interests of public order the meeting adjourn for (the period to be specified) to
enable the Board to complete business without the presence of the public” (Section 1 (8)
Public Bodies (Administration to Meetings Act 1960).
4.1.6 Nothing in the Standing Orders shall require the Board to allow members of the public or
representatives of the press to record proceedings in any manner whatsoever, other than in
writing, or to make any oral report of proceedings as they take place without the prior
agreement of the Board.
4.2 Calling Meetings
4.2.1 The ordinary meetings of the Board shall be held at regular intervals unless the Board shall by
resolution otherwise decide. The meetings shall be held at such places as the Board may
from time to time appoint. These meetings are open to the public to enable staff and
members of the public to attend.
4.2.2 The Chair may call a meeting of the Board at any time.
4.2.3 One third or more members of the Board may requisition a meeting in writing. If the Chairman
refuses, or fails to call a meeting within seven days of a requisition being presented, the
members signing the requisition may forthwith call a meeting.
4.3 Notice of Meetings
4.3.1 Regular Meetings of the Trust –
Agendas will be sent to members at least 6 days before the meeting and supporting papers,
whenever possible, shall accompany the agenda, they will be despatched no later than three
clear days before the meeting, except in an emergency. Failure to serve such a notice on
more than three Directors will invalidate the meeting. A notice shall be presumed to have
been served at the time one day after posting or emailing.
4.3.2 Exceptional Meetings of the Trust –
Before each meeting of the Trust, a notice of the meeting, specifying the business proposed to
be transacted at it, and signed by the Chair or by an officer of the Trust authorised by the
Chair to sign on their behalf shall be delivered to every Director/member electronically, or sent
by post to their usual place of residence, so as to be available to them at least three clear days
before the meeting.
Lack of service of the notice on any Director/member shall not affect the validity of a meeting.
4.3.3 Meetings Called By Directors –
Sta
ndin
g O
rder
s
Page 13 of 150

In the case of a meeting called by Directors in the event the Chair has not called the meeting,
the notice shall be signed by those Directors and no business shall be transacted at the
meeting other than that specified in the notice.
4.3.4 Public Notice-
Before each meeting of the Board a public notice of the time and place of the meeting, and the
public part of the agenda, shall be displayed at the Trust's office at least three clear days
before the meeting. (Required by the Public Bodies (Admission to Meetings) Act 1960 S.I. (4)
(a).)
4.4 Agendas and Petitions
4.4.1 The Trust may determine that certain matters shall appear on every agenda for a meeting of
the Trust and shall be addressed prior to any other business being conducted
4.4.2 A Director/member desiring a matter to be included on an agenda shall make their request in
writing to the Company Secretary at least 10 clear days before the meeting. The request
should state whether the item of business is proposed to be transacted in the presence of the
public and should include appropriate supporting information. Requests made less than 10
days before a meeting may be included on the agenda at the discretion of the Chair who will
approve the agenda 9 clear days before the meeting.
4.4.3 Where a petition has been received by the Trust the Chair of the Board shall include the
petition as an item for the agenda of the next Board meeting.
4.5 Notice of Motion
4.5.1 Subject to the provision of Standing Orders ‘Motions: Procedure at and during a meeting’ and
‘Motions to rescind a resolution’ a member of the Board wishing to move a motion shall send a
written notice to the Company Secretary who will ensure that it is brought to the immediate
attention of the Chair.
4.5.2 The notice shall be delivered at least fifteen clear days before the meeting. The Company
Secretary shall include in the agenda for the meeting all notices so received that are in order
and permissible under governing regulations. This Standing Order shall not prevent any
motion being withdrawn or moved without notice on any business mentioned on the agenda
for the meeting.
4.6 Emergency Motions
Subject to the agreement of the Chair, and subject also to the provision of Standing Order
‘Motions: Procedure at and during a meeting’, a member of the Board may give written
notice of an emergency motion after the issue of the notice of meeting and agenda, up to
one hour before the time fixed for the meeting. The notice shall state the grounds of
urgency. If in order, it shall be declared to the Board at the commencement of the business
of the meeting as an additional item included in the agenda. The Chair's decision to include
the item shall be final.
4.7 Motions: Procedure at and during a meeting
i) Who may propose - A motion may be proposed by the Chair of the meeting or any
member present. It must also be seconded by another member.
ii) Contents of motions - The Chair may exclude from the debate at their discretion
any such motion of which notice was not given on the notice summoning the meeting
other than a motion relating to:
- the reception of a report;
- consideration of any item of business before the Board;
- the accuracy of minutes;
- that the Board proceed to next business;
Sta
ndin
g O
rder
s
Page 14 of 150
- that the Board adjourn;
- that the question be now put.
iii) Amendments to motions - A motion for amendment shall not be discussed unless it
has been proposed and seconded. Amendments to motions shall be moved relevant
to the motion, and shall not have the effect of negating the motion before the Board. If
there are a number of amendments, they shall be considered one at a time. When a
motion has been amended, the amended motion shall become the substantive motion
before the meeting, upon which any further amendment may be moved.
iv) Rights of reply to motions
a) Amendments
The mover of an amendment may reply to the debate on their amendment
immediately prior to the mover of the original motion, who shall have the right
of reply at the close of debate on the amendment, but may not otherwise
speak on it.
b) Substantive/original motion
The member who proposed the substantive motion shall have a right of reply
at the close of any debate on the motion.
v) Withdrawing a motion - A motion, or an amendment to a motion, may be withdrawn.
vi) Motions once under debate - When a motion is under debate, no motion may be
moved other than:
- an amendment to the motion;
- the adjournment of the discussion, or the meeting;
- that the meeting proceed to the next business;
- that the question should be now put;
- the appointment of an 'ad hoc' committee to deal with a specific item of business;
- that a member/director be not further heard;
- a motion under Section l (2) or Section l (8) of the Public Bodies (Admissions to
Meetings) Act l960 resolving to exclude the public, including the press (see
Standing Order).
In those cases where the motion is either that the meeting proceeds to the ‘next
business’ or ‘that the question be now put’ in the interests of objectivity these should
only be put forward by a member of the Board who has not taken part in the debate
and who is eligible to vote.
If a motion to proceed to the next business or that the question be now put, is carried,
the Chair should give the mover of the substantive motion under debate a right of
reply, if not already exercised. The matter should then be put to the vote.
4.8 Motion to Rescind a Resolution
(1) Notice of motion to rescind any resolution (or the general substance of any resolution)
which has been passed within the preceding six calendar months shall bear the
signature of the member who gives it and also the signature of three other members,
and before considering any such motion of which notice shall have been given, the
Board may refer the matter to any appropriate Committee or the Chief Executive for
recommendation.
(2) When any such motion has been dealt with by the Board it shall not be competent for
any director/member other than the Chair to propose a motion to the same effect
within six months. This Standing Order shall not apply to motions moved in pursuance
of a report or recommendations of a Committee or the Chief Executive.
Sta
ndin
g O
rder
s
Page 15 of 150

4.9 Chair of Meeting
At any meeting of the Board, the Chair, if present, shall preside. If the Chair is absent from the
meeting the Vice-Chair, if there is one and he is present, shall preside. If the Chair and Vice-
Chair are absent the Directors present shall choose a Non-Executive Director to preside.
4.10 Chair’s Ruling
Statements of Directors made at meetings of the Trust shall be relevant to the matter under
discussion at the material time and the decision of the Chair of the meeting on questions of
order, relevancy, regularity (including procedure on handling motions) and any other matters
shall be final including their interpretation of the Standing Orders and Standing Financial
Instructions.
4.11 Quorum
No business shall be transacted at a meeting of the Board unless one third of the whole
number of voting directors are present including at least one Executive Director and one Non-
Executive Director. Directors attending via video or telephone conferencing will be considered
present and count towards the quorum.
An officer in attendance for an Executive Director but without formal acting up status may not
count towards the quorum.
If the Chair or a member has been disqualified from participating in the discussion on any matter
and/or from voting on any resolution by reason of the declaration of a conflict of interest SO 7 he
shall no longer count towards the quorum. If a quorum is then not available for the discussion
and/or the passing of a resolution on any matter, that matter may not be discussed further or
voted upon at that meeting. Such a position shall be recorded in the minutes of the meeting.
The meeting must then proceed to the next business. The above requirement for at least one
executive director to form part of the quorum shall not apply where the executive Directors are
excluded from a meeting due to a conflict of interests.
4.13 Voting
Save as provided under SO 4.16 Suspension of Standing Orders - If a consensus decision is
not reached at a meeting then the question shall be determined by a majority of the votes of
the Directors present. Directors attending via telephone or video conferencing are considered
present and therefore have a vote. In the case of any equality of votes, the Chair presiding the
meeting shall have a second and casting vote.
All questions put to the vote shall, at the discretion of the Chair of the meeting, be determined by
oral expression or by a show of hands. A paper ballot may also be used if a majority of the
Directors present so request.
If at least one-third of the Directors present so request, the voting (other than by paper ballot) on
any question may be recorded to show how each Director /member present voted or abstained.
If a Director/member so requests, their vote shall be recorded by name upon any vote (other than
by paper ballot).
In no circumstances may an absent Director/member vote by proxy. Absence is defined as
being absent at the time of the vote.
An officer who has been appointed formally by the Board to act up for an Executive Director
during a period of incapacity or temporarily to fill an Executive Director vacancy, shall be entitled
to exercise the voting rights of the Executive Director. An officer attending the Board to represent
an Executive Director without formal acting up status may not exercise the voting rights of the
Executive Director. An officer’s status when attending a meeting shall be recorded in the
minutes.
Sta
ndin
g O
rder
s
Page 16 of 150

Non-voting Directors are able to take part within Board discussions and provide their opinion
but do not have voting rights on the Board.
4.14 Minutes
The Minutes of the proceedings of a meeting shall be drawn up and submitted for agreement
at the next ensuing meeting where they will be approved by the Board
No discussion shall take place upon the minutes except upon their accuracy or where the Chair
considers discussion appropriate. Any amendment to the minutes shall be agreed and recorded
at the next meeting.
The names of the Chair and Members present and those in attendance at the meetings shall
be recorded.
Any matters arising from the Minutes shall be subject to discussion at Chair’s discretion. Where
providing a record of a public meeting the minutes shall be made available to the public (required
by Code of Practice on Openness in the NHS).
4.15 Annual Public Meeting
The Trust will publicise and hold an annual public meeting in accordance with the NHS Trusts
(Public Meetings) Regulations 1991 (SI(1991)482). The meeting shall take place no later than
30 September each year. The Annual Report and Annual Accounts of the preceding year shall
be presented at that meeting.
4.16 Suspension of Standing Orders
Except where this would contravene any statutory provision or any direction made by the
Secretary of State, any one or more of the Standing Orders may be suspended at any
meeting, provided that at least two-thirds of the Board are present, including one Executive
Director and one Non-Executive Director, and that a majority of those present vote in favour of
suspension.
A decision to suspend SOs shall be recorded in the minutes of the meeting.
A separate record of matters discussed during the suspension of SOs shall be made and
shall be available to the Directors.
No formal business may be transacted while SOs are suspended.
The Audit Committee shall review every decision to suspend SOs.
4.17 Variation and Amendment of Standing Orders
These Standing Orders shall be amended only if:
• a notice of motion under SO 4.7 has been given; and
upon recommendation of the Chair or Chief Executive included on the agenda for the
meeting; and
• no fewer than half the total of the Trust’s Non-Executive Directors vote in favour of
amendment; and
• at least two-thirds of the Directors were present at the meeting where the variation or
amendment was being discussed; and
• the variation proposed does not contravene a statutory provision or direction made by
the Secretary of State.
5. ARRANGEMENTS FOR THE EXERCISE OF FUNCTIONS BY DELEGATION
Sta
ndin
g O
rder
s
Page 17 of 150

5.1 Introduction
5.1.1 Subject to the ‘Scheme of Reservation and Delegation’, and such directions as may be given by
the Secretary of State, the Board may make arrangements for the exercise, on behalf of the
Trust, of any of its functions by a committee or sub-committee, appointed by virtue of SO 6.0 or
by a Director /member or an officer of the Trust in each case subject to such restrictions and
conditions as the Board thinks fit.
5.1.2 S16B of the NHS Act 1977 allows for regulations to provide for the functions of Trusts to be
carried out for the Trust by third parties. The Trusts (Membership, Procedure and
Administration Arrangements) Regulations 2000 also allow for functions of the Trust to be
carried out in the following ways:
(i) by another Trust;
(ii) jointly with one or more NHS Trust;
(iii) by arrangement with the appropriate Trust, by a joint committee or joint sub-committee of
the Trust and one or more other health service bodies;
(iv) in relation to arrangements under s63 (1) of the Health Services and Public Health Act
1968, jointly with one or more Trusts.
5.1.3 Where a function is delegated by these regulations to another NHS body, then that Trust or
health service body exercises the function in its own right; the receiving Trust has
responsibility to ensure that the proper delegation is in place. In other situations, i.e.
delegation to committees, sub committees or officers, the Trust delegating the function retains
full responsibility.
5.2 Framework for Delegation of Trust Board Authority
The ultimate responsibility for decisions taken under delegated powers remains with the
Board, and the Trust must ensure that due regard has been given and can clearly
demonstrate it has not come to an unreasonable decision. To avoid possible allegations of
unlawful exercise of discretion by the Board, a committee or Director/member acting under
delegated powers record in writing the matters which have been taken into account in
reaching that decision, especially where significant sums or legal commitments are involved.
In making any decisions under delegated powers, a committee or Director/member must have
due regard to the established policies of the Trust and shall not depart from them without due
reason and consideration. Any such departure and the reason for it shall be drawn to the
attention of the Board at the earliest opportunity.
In exercising any delegated power a committee or Director/member must comply with any
statutory provisions or requirements.
In cases of doubt or difficulty and/or where no policy guidelines exist, decisions should be
referred to the Board.
The Board may require any particular delegated matter to be referred back to them for a
decision.
5.3 Emergency Powers
The powers which the Board has retained to itself within these Standing Orders, SO 1.3.1, may
in emergency be exercised by the Chair and the Chief Executive after having consulted at least
two Non-Executive Directors. The exercise of such powers by the Chair and the Chief Executive
shall be reported to the next formal meeting of the Board for ratification in public session.
5.4 Delegation to Committees
The Board shall agree from time to time to the delegation of executive powers to be exercised by
committees or sub-committees, which it has formally constituted in accordance with directions
issued by the secretary of State. The constitution and terms of reference of these committees,
Sta
ndin
g O
rder
s
Page 18 of 150
sub-committees or joint committees, and their specific executive powers shall be approved by
the Board, in respect of its sub-committees.
5.5 Delegation to Officers
5.5.1 Those functions of the Trust which have not been retained as reserved by the Board or
delegated to other committee, sub-committee or joint committee shall be exercised on behalf
of the Board by the Chief Executive. The Chief Executive shall determine which functions
he/she will perform personally and shall nominate officers to undertake the remaining
functions for which he/she will still retain accountability to the Board.
5.5.2 The Chief Executive shall prepare a scheme of delegation (as detailed within the ‘Scheme of
Reservation and Delegation’) identifying his/her proposals which shall be considered and
approved by the Board, subject to any amendment agreed during the discussion. The Chief
Executive may periodically propose amendment to the Scheme of Reservation and Delegation
which shall be considered and approved by the Board as indicated above.
5.5.3 Nothing in the Scheme of Reservation and Delegation shall impair the discharge of the direct
accountability to the Board or the Director of Finance or of any other executive director to provide
information and advise the Board in accordance with any statutory or Department of Health
requirements. Outside these statutory requirements the role of the Director of Finance shall be
accountable to the Chief Executive for operational matters.
5.5.4 The arrangements made by the Board as set out in the ‘Scheme of Reservation and
Delegation’ shall have effect as if incorporated in these Standing Orders.
5.6 Duty to report non-compliance with Standing Orders
5.6.1 All members of the Board and staff have a duty to disclose any non-compliance with these
Standing Orders to the Chief Executive as soon as possible. Full details of the non-
compliance and any justification for non-compliance and the circumstances around the non-
compliance, shall be reported to the next formal meeting of the Audit Committee for them to
recommend action or ratification to the Board.
Failure to comply with the Standing Orders is a disciplinary matter, which could result
in dismissal.
6. APPOINTMENT OF COMMITTEES AND SUB-COMMITTEES
6.1 Appointment of Committees
6.1.1 Subject to such directions (and to guidance issued by the Department of Health) as may be
given by the Secretary of State, the Board may appoint committees of the Board. The Board
shall determine the membership and terms of reference of committees and sub-committees
and shall if it requires to, receive and consider reports of such committees.
6.2 Joint Committees
6.2.1 Joint committees may be appointed by the Board by joining together with one or more other
Trusts or health service bodies, consisting wholly or partly of the Chair and members of the
Board or other health service bodies or wholly of persons who are not members of the Board
or other health service bodies in question.
6.2.2 A committee or joint committee appointed under this regulation may, subject to such directions
as may be given by the Secretary of State or the Trust or other health service bodies in
question, appoint sub-committees consisting wholly or partly of members of the committee or
joint committee (whether or not they are members of the Trust or other health service bodies
in question); or wholly of persons who are not members of the Trust or other health service
bodies or the committee of the Trust or other health service bodies in question.
Sta
ndin
g O
rder
s
Page 19 of 150

6.3 Applicability of Standing Orders and Standing Financial Instructions to Committees
6.3.1 The Standing Orders of the Trust, as far as they are applicable, shall as appropriate apply to
meetings of any committees or sub-committee established by the Trust. In which case the
term “Chair” is to be read as a reference to the Chair of other committee as the context
permits, and the term “member” is to be read as a reference to a member of other committee
also as the context permits. (There is no requirement to hold meetings of committees
established by the Board in public.)
6.4 Terms of Reference
6.4.1 Each such committee or sub-committee shall have such terms of reference and powers and
be subject to such conditions (as to reporting back to the Board), as the Board shall decide
and shall be in accordance with any legislation and regulation or direction issued by the
Secretary of State. Such terms of reference shall have effect as if incorporated into the
Standing Orders.
6.5 Delegation of powers by Committees to Sub-Committees
6.5.1 Committees may establish sub-committees but may not delegate their executive powers to a
sub-committee unless expressly authorised by the Board.
6.6 Approval of Appointments to Committees
6.6.1 The Board shall approve the appointments to each of the committees which it has formally
constituted. Where the Board determines and regulations permit, that persons, who are
neither Directors nor officers, shall be appointed to a committee, the terms of such
appointment shall be within the powers of the Board as defined by the Secretary of State.
6.6.2 The Board shall define the powers of such appointees and shall agree allowances, including
reimbursement for loss of earnings, and/or expenses in accordance where appropriate with
national guidance.
6.6.3 Where the Trust is required to appoint persons to a committee and/or to undertake statutory
functions as required by the Secretary of State, and where such appointments are to operate
independently of the Trust such appointment shall be made in accordance with the regulations
laid down by the Secretary of State.
6.6.4 The appointment of Board members to the committees and sub-committees of the Trust
comes to an end on the termination of their term of office as Board members.
6.7 Committee Structure
The committees established by the Board are:
a) Audit Committee In line with the requirements of the NHS Audit Committee Handbook,
NHS Codes of Conduct and Accountability and the Higgs report, an Audit Committee
will be established and constituted to provide the Board with an independent and
objective review on its financial systems, financial information and compliance with
laws, guidance, and regulations governing the NHS. The Terms of Reference will be
approved by the Board and reviewed on a periodic basis.
The Higgs report recommends a minimum of three non-executive directors be
appointed, unless the Board decides otherwise, of which one must have significant,
recent and relevant financial experience.
b) Remuneration and Nominations Committee In line with the requirements of the NHS
Codes of Conduct and Accountability and the Higgs report a Remuneration and
Nominations Committee will be established and constituted.
The Higgs report recommends the committee be comprised exclusively of Non-
Sta
ndin
g O
rder
s
Page 20 of 150

Executive Directors, a minimum of three, who are independent of management. The
Board has determined that the Remuneration & Nominations Committee will comprise
all of the Non-Executive Directors and as such will have fully delegated powers from the
Board.
The purpose of the Committee will be to decide appropriate remuneration and terms of
service for the Chief Executive and other Executive Directors including:
(i) all aspects of salary (including any performance-related elements/bonuses);
(ii) provisions for other benefits, including pensions and cars;
(iii) arrangements for termination of employment and other contractual terms;
(iv) ensure a formal, rigorous and transparent procedure for Board appointments
is followed;
(v) consider Board succession planning; and
(vi) review Board composition.
c) Charitable Funds Committee In line with its role as a corporate trustee for any funds
held in trust, either as charitable or non charitable funds, the Trust Board will establish a
Trust and Charitable Funds Committee to administer those funds in accordance with
any statutory or other legal requirements or best practice required by the Charities
Commission.
d) Finance, Performance & Investment Committee The Committee is established to
provide the Board with assurance regarding all aspects of the financial arrangements
of the Trust, including that financial issues of the Trust are being appropriately
addressed. The Committee will establish the overall methodology, processes and
controls which govern capital investments, ensure that robust processes are followed
and evaluate, scrutinise and monitor investments.
e) Quality & Safety Committee The Committee is established to provide the Board with
assurance regarding the effectiveness of all aspects of the clinical governance
arrangements of the Trust, with a particular focus on quality and risk management.
f) Workforce Committee The committee is established to provide assurance that the
Workforce and Organisation Development Strategies are effectively implemented and
that key workforce developments are effectively implemented in the Trust.
6.8 Other Committees
The Board may also establish other committees as required to discharge the Trust’s
responsibilities.
6.9 Confidentiality
6.9.1 A member of a committee shall not disclose a matter dealt with by, or brought before, the
committee without its permission until the committee shall have reported to the Board or shall
otherwise have concluded on that matter.
6.9.2 A Director of the Trust or a member of a committee shall not disclose any matter reported to the
Board or otherwise dealt with by the committee, notwithstanding that the matter has been
reported or action has been concluded, if the Board or committee resolves that it is confidential.
7. DECLARATIONS OF INTERESTS AND REGISTER OF INTERESTS
7.1 Declaration of Interests
7.1.1 The Code of Accountability requires Board members to declare interests, annually or as and
when they arise, which are relevant and material to the NHS board of which they are a
member. All existing Board members should declare such interests. Any Board members
appointed subsequently should do so on appointment. Anyone declaring an interest should
refer to the Trust’s Policy for the Declaration of Interests.
Sta
ndin
g O
rder
s
Page 21 of 150

7.1.2 Interests, which should be regarded as “relevant and material”, are:
a) Directorships, including Non-Executive Directorships held in private companies or PLCs
(with the exception of those of dormant companies).
b) Ownership or part-ownership of private companies, businesses or consultancies likely or
possibly seeking to do business with the NHS.
c) Majority or controlling share holdings in organisations likely or possibly seeking to do
business with the NHS.
d) A position of authority in a charity or voluntary organisation in the field of health and
social care.
e) Any connection with a voluntary or other organisation contracting for NHS services.
f) Research funding/grants that may be received by an individual or their department.
g) Interests in pooled funds that are under separate management.
7.1.3 If Board Directors have any doubt about the relevance of an interest, this should be discussed
with the Chair or Company Secretary. Financial Reporting Standard No 8 (issued by the
Accounting Standards Board) specifies that influence rather than the immediacy of the
relationship is more important in assessing the relevance of an interest. The test of relevance
is whether the interest might reasonably be thought by the public to affect the way in which an
individual discharges his or her duties. The test therefore is not just whether an individual’s
actions will be influenced by the interest but whether the public might reasonably think this
may be the case. The interests of partners in professional partnerships including general
practitioners should also be considered.
7.1.4 At the time Board Directors' interests are declared, they should be recorded in the Board minutes
and the Register of Interests. Any changes in interests should be declared at the next Board
meeting following the change occurring and recorded in the minutes of that meeting.
7.1.5 Board Directors' directorships of companies likely or possibly seeking to do business with the
NHS should be published in the Trust's Annual Report. The information should be kept up to
date for inclusion in succeeding Annual Reports.
7.1.6 If it comes to the knowledge of an employee of the Trust that a contract in which they have a
direct or indirect financial interest has been, or is proposed to be, entered into by the Trust he
shall at once declare this position in writing to the Company Secretary as soon as practicable.
7.1.7 During the course of a Board meeting, if a conflict of interest is established, the
Director/members concerned should declare such likely conflict of interest and withdraw from the
meeting, unless requested to remain by the Board members present. The Director/member
should play no part in the relevant discussion or decision.
7.1.8 Where a possible conflict of interest arises in relation to the award of a contract, special care
must be taken. Personal interests and potential conflicts of interest may come about through:
a) Financial interests – for example, where someone involved has significant
shareholdings or voting rights in a company or partnership
b) Decisions affecting individuals who share the interests of organisation staff – for
example, family members or members of societies, clubs or other organisations
c) Acceptance of hospitality from current or prospective business contacts, and
d) Acceptance of gifts
7.1.9 Where any potential for conflict of interest arises staff should inform a senior member of staff
and/or line manager, following the Trust Declaration of Interests Policy.
7.1.10 All members of staff [including contractors and temporary staff] are required to declare any
potential conflicts of interest.
Sta
ndin
g O
rder
s
Page 22 of 150

7.2 Negotiations
Staff should not become involved in any form of negotiation on behalf of Southport & Ormskirk
Hospital NHS Trust if they have personal interests in other parties. Should such a
circumstance occur this must be reported following the Trust Declaration of Interests Policy.
7.3 Interests in Companies
If staff do find themselves working alongside and/or doing business with a company in which
they have an interest or are employed by, they must declare this to their Line Manager and
report it following the Trust Declaration of Interests Policy.
7.4 Register of Interests
7.4.1 The Chief Executive will ensure that a Register of Interests is established to record formally
declarations of interests of Board. In particular the Register will include details of all
directorships and other relevant and material interests which have been declared by both
Executive and Non-Executive Directors, as defined in SO 7.1.2.
7.4.2 These details will be kept up to date by means of an annual review of the Register in which
any changes to interests declared during the preceding twelve months will be incorporated.
7.4.3 The Company Secretary as responsibility for maintaining the Register of Interests, including
an annual review, and ensuring it is available to the public.
8. DISABILITY OF DIRECTORS IN PROCEEDINGS ON ACCOUNT OF PECUNIARY INTEREST
8.1 Definition
8.1.1 Subject to the following provisions of this Standing Order (which is taken from the Membership
Procedure Regulations 1990 (as amended), if the Chair or a member has any pecuniary
interest, direct or indirect, in any contract, proposed contract or other matter and is present at
a meeting of the Trust Board at which the contract or other matter is the subject of
consideration, he shall at the meeting and as soon as practicable after its commencement
disclose the fact and shall not take part in the consideration or discussion of the contract or
other matter or vote on any question with respect to it.
8.1.2 The Trust Board may exclude the Chair or a member of the Trust Board from a meeting of the
Board while any contract, proposed contract or other matter in which that person has a
pecuniary interest is under consideration.
8.1.3 Any remuneration, compensation or allowances payable to the Chair or a Director by virtue of
the NHS (consolidation) Act 2006 Schedule 3 Part 1 para 10. (NHS Act 1997 Schedule 5A
paragraph 11(4); 1999 Act Schedule 1) (pay and allowances) shall not be treated as pecuniary
interest for the purpose of this regulation.
8.1.4 Subject to paragraph 8.1.3 and any conditions imposed by the Secretary of State, the Chair or
a Director/member shall be treated for the purpose of this regulation as having indirectly a
pecuniary interest in a contract, proposed contract or other matter if:
a) the Director/member, or a nominee of theirs, is a Director of a company or other body,
not being a public body, with which the contract was made or is proposed to be made
which has a direct pecuniary interest in the other matter under consideration; or
b) the Director/member is a partner of, or is in the employment of a person with whom
the contract was made or is proposed to be made or who has a direct pecuniary
interest in the other matter under consideration. In the case of married persons living
together or co-habitees, the interest of one spouse/co-habitee shall, if known to the
Sta
ndin
g O
rder
s
Page 23 of 150

other, be deemed to be also the interest of that spouse/co-habitee.
For the sake of clarity the following definition of terms is to be used in interpreting this
Standing Order.
‘Spouse’ shall include any person who lives with another person in the same household (any
pecuniary interest one spouse shall, if known to the other spouse, be deemed to be an interest
of that other spouse).
‘Contract’ shall include any proposed contract or other course of dealing.
8.1.5 The Chair or a Director/member shall not be treated as having pecuniary interest in any
contract, proposed of other matter by reason only:
a) of theirs (or a person connected to them) membership of a company or other body if
they have no beneficial interest in any securities of that company or other body;
b) of an interest in any company, body or person with which they are connected as
mentioned in paragraph 8.1.2 which is so remote or insignificant that it cannot
reasonably be regarded as likely to influence a member in the consideration or
discussion of or in voting on, any question with respect to that contract or matter.
c) the total nominal value of those securities does not exceed £5,000 or one-hundredth
of the total nominal value of the issued share capital of the company or body,
whichever is the less.
Provided however, that where paragraph (c) above applies the person shall nevertheless be
obliged to disclose/declare their interest in accordance with SO 7.1.2.
8.2 Powers of the Secretary of State
8.2.1 The Secretary of State may, subject to such conditions as he may think fit to impose, remove
any disability imposed by this Standing Order in any case in which it appears to them in the
interests of the National Health Service that the disability shall be removed.
8.3 Waiver of Standing Orders made by the Secretary of State for Health
8.3.1 Under regulation 11(2) of the NHS (Membership and Procedure Regulations SI 1999/2024
(‘the regulations’), there is a power for the Secretary of State to issue waivers if it appears to
the Secretary of State in the interests of the health service that the disability in regulation 11
(which prevents a Chair or a member from taking part in the consideration or discussion of, or
voting on any question with respect to, a matter in which he has a pecuniary interest) is
removed.
8.3.2 Definition of Chair for the purpose of interpreting this waiver and for the purposes of SO 8.3.3 the
‘relevant Chair’ is:
a) at a meeting of the Board, the Chair of the Board;
b) at a meeting of a Committee –
i. in a case where the member in question is the Chair of that Committee, the
Chair of the Trust;
ii. in the case of any other member, the Chair of that Committee.
8.3.3 A waiver will apply in relation to the disability to participate in the proceedings of the Trust on
account of a pecuniary interest.
It will apply to:
a) A member of Southport & Ormskirk Hospital NHS Trust (‘the Trust’), who is a
healthcare professional, within the meaning of regulation 5(5) of the Regulations, and
Sta
ndin
g O
rder
s
Page 24 of 150
who is providing or performing, or assisting in the provision or performance, of –
i. services under the NHS Act 1977; or
ii. services in connection with a pilot scheme under the NHS Act 1977;
for the benefit of persons for whom the Trust is responsible.
b) Where the ‘pecuniary interest’ of the member in the matter which is the subject of
consideration at a meeting at which he is present:-
i. arises by reason only of the member’s role as such a professional providing
or performing, or assisting in the provision or performance of, those services
to those persons;
ii. has been declared by the relevant chair as an interest which cannot
reasonably be regarded as an interest more substantial than that of the
majority of other persons who:-
a) are members of the same profession as the member in question,
b) are providing or performing, or assisting in the provision or
performance of, such of those services as he provides or performs, or
assists in the provision or performance of, for the benefit of persons
for whom the Trust is responsible.
8.3.4 Conditions which apply to the waiver and the removal of having a pecuniary interest
The removal is subject to the following conditions:
a) the members must disclose his/her interest as soon as practicable after the
commencement of the meeting and this must be recorded in the minutes,
b) the relevant chair must consult the Chief Executive before making a declaration in
relation to the member in question pursuant to paragraph 8.3.2 b) above, except
where that member is the Chief Executive;
In the case of a meeting of the Trust:
a) the member may take part in the consideration or discussion of the matter which must
be subjected to a vote and the outcome recorded;
b) may not vote on any question with respect to it.
In the case of a meeting of the Committee:
a) the member may take part in the consideration or discussion of the matter which must
be subjected to a vote and the outcome recorded;
b) may vote on any question with respect to it; but
c) the resolution which is subject to the vote must comprise a recommendation to, and
be referred for approval by, the Trust Board.
8.4 Committees and Sub-Committees Responsibilities
8.4.1 This regulation applies to a committee or sub-committee of the Trust as it applies to the Trust
Board and applies to any member of any such committee or sub-committee (whether or not he
is also a Director of the Trust) as it applies to a Director of the Trust.
9. STANDARDS OF BUSINESS CONDUCT
9.1 Policy
9.1.1 Staff must comply with the national guidance contained in HSG(93)5 `Standards of Business
Conduct for NHS Staff'. The following provisions should be read in conjunction with that
guidance, and with the Trust’s policies on ‘Standards of Business Conduct and Declaration of
Interest Policy and Staff Code of Personal and Business Conduct, which are provided in the
Appendices to the Corporate Governance Manual.
Sta
ndin
g O
rder
s
Page 25 of 150

9.1.2 It is the responsibility of all Trust staff to ensure that they are not placed in a position which
risks, or appears to risk, conflict between their private interests and their official duties.
9.1.3 It is an offence under the Bribery Act 2010 (previously the Prevention of Corruption Acts 1906
and 1916) for an employee of the Trust to accept corruptly any inducement or reward for
doing, or refraining from doing, anything in their official capacity, or corruptly showing favour or
disfavour in the handling of contracts.
9.1.4 It is the responsibility of the Trust to ensure that its officers are aware that breach of the
provision of these Acts renders them liable to prosecution and may also lead to the termination
of their contracts of employment and superannuation rights within the NHS.
9.2 Interest of Officers in Contracts
9.2.1 If it comes to the knowledge of a Director or an officer of the Trust that a contract in which he
has any pecuniary interest not being a contract to which he is himself a party, has been, or is
proposed to be, entered into by the Trust he shall, at once, give notice in writing to the Chief
Executive or Company Secretary of the fact that he is interested therein. In the case of
married persons or persons living together as partners, the interest of one partner shall, if
known to the other, be deemed to be also the interest of that partner.
9.2.2 An officer must also declare to the Chief Executive any other employment or business or other
relationship of their partner, or of a cohabiting spouse, that conflicts, or might reasonably be
predicted could conflict with the interests of the Trust.
9.2.3 The Trust will require interests, employment or relationships so declared to be entered in a
register of interests of staff.
9.3 Canvassing of, and Recommendations by, Directors in Relation to Appointments
9.3.1 Canvassing of Directors of the Trust or members of any committee of the Trust directly or
indirectly for any appointment under the Trust shall disqualify the candidate for such
appointment. The contents of this paragraph of the Standing Order shall be included in
application forms or otherwise brought to the attention of candidates.
9.3.2 A Director of the Trust shall not solicit for any person any appointment under the Trust or
recommend any person for such appointment: but this paragraph of this Standing Order shall
not preclude a Director from giving written testimonial of a candidate's ability, experience or
character for submission to the Trust.
9.3.3 Unsolicited informal discussions outside appointments panels or committees, should be
declared to the panel or committee.
9.4 Relatives of Directors or Officers
9.4.1 Candidates for any staff appointment shall when making application disclose in writing
whether they are related to any Director or the holder of any office under the Trust. Failure to
disclose such a relationship shall disqualify a candidate and, if appointed, render them liable to
dismissal.
9.4.2 The Chair and every member and officer of the Trust shall disclose to the Trust Board any
relationship with a candidate of whose candidature that Director or officer is aware. It shall be the
duty of the Chief Executive to report to the Trust any such disclosure made.
9.4.3 On appointment, Directors (and prior to acceptance of an appointment in the case of Executive
Directors) should disclose to the Trust whether they are related to any other Director or holder of
any office under the Trust.
9.4.4 Where the relationship of an officer or another Director to a Director of the Trust is disclosed, the
Standing Order headed `Disability of Directors in Proceedings on Account of pecuniary Interest'
Sta
ndin
g O
rder
s
Page 26 of 150

SO 8 shall apply.
10 CUSTODY OF SEAL AND SEALING OF DOCUMENTS
10.1 Custody of Seal
The Common Seal of the Trust shall be kept by the Chief Executive or Company Secretary in
a secure place.
10.2 Sealing of Documents
10.2.1 Where it is necessary that a document shall be sealed, the seal shall be affixed in the
presence of two senior managers duly authorised by the Chief Executive, and not from the
originating department, and shall be attested by them.
10.2.2 The Executive Directors and Company Secretary are authorised by the Chief Executive to use
the Seal of the Trust.
10.3 Requirements to Seal
10.3.1 It is a legal requirement to place any property transactions e.g. purchase, sale, lease, under
seal.
10.3.2 Before any building, engineering, property or capital document is sealed it must be approved
and signed by the Director of Finance (or an officer nominated by them) and authorised and
countersigned by the Chief Executive (or an officer nominated by them who shall not be within
the originating directorate).
10.4 Register of Sealing
10.4.1 The Company Secretary on behalf of the Chief Executive shall keep a register, an entry of
every sealing shall be made and numbered consecutively in a book provided for that purpose,
and shall be signed by the persons who shall have approved and authorised the document
and those who attested the seal. A report of all sealings shall be made to the Board at least
annually.
10.5 Signature of documents
10.5.1 Where the signature of any document will be a necessary step in legal proceedings involving the
Trust, it shall be signed by the Chief Executive or an officer acting on their behalf, unless any
enactment otherwise requires or authorises, or the Board shall have given the necessary
authority to some other person for the purpose of such proceedings.
10.5.2 The Chief Executive or nominated officers shall be authorised, by resolution of the Board, to
sign on behalf of the Trust any agreement or other document (not required to be executed as
a deed) the subject matter of which has been approved by the Board or committee or sub-
committee to which the Board has delegated appropriate authority, as per the Reservation of
Powers and Scheme of Delegation.
Sta
ndin
g O
rder
s
Page 27 of 150
STANDING
FINANCIAL
INSTRUCTIONS
Southport & Ormskirk Hospital NHS Trust
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 28 of 150

CONTENTS
SECTION
INTRODUCTION 1
AUDIT 2
ALLOCATIONS / PAYMENT BY RESULTS, BUSINESS PLANNING, BUDGETS,
BUDGETARY CONTROL, AND MONITORING 3
ANNUAL ACCOUNTS AND REPORTS 4
BANK AND OPG ACCOUNTS 5
INCOME, FEES AND CHARGES AND SECURITY OF CASH, CHEQUES AND OTHER
NEGOTIABLE INSTRUMENTS 6
NHS SERVICE AGREEMENTS FOR PROVISION OF SERVICES 7
TERMS OF SERVICE, ALLOWANCES AND PAYMENT OF MEMBERS OF THE
BOARD OF DIRECTORS AND EMPLOYEES 8
NON-PAY EXPENDITURE 9
EXTERNAL BORROWING AND INVESTMENTS 10
CAPITAL INVESTMENT, PRIVATE FINANCING, FIXED ASSET REGISTERS AND
SECURITY OF ASSETS 11
STOCKS, STORES AND RECEIPT OF GOODS 12
DISPOSALS AND CONDEMNATIONS, INSURANCE, LOSSES AND SPECIAL
PAYMENTS 13
INFORMATION TECHNOLOGY 14
PATIENTS' PROPERTY 15
FUNDS HELD ON TRUST 16
TENDERING AND CONTRACTING PROCEDURES 17
ACCEPTANCE OF GIFTS AND HOSPITALITY BY STAFF 18
DECLARATIONS OF INTEREST BY STAFF 19
RETENTION OF DOCUMENTS 20
RISK MANAGEMENT 21
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 29 of 150

RECORD OF AMENDMENTS
NO SECTION DATE
1 Updated document Issued for implementation July 2007
2 Document reviewed November 2008
3 Document updated May 2010
4 Document reviewed August 2011
5 Document reviewed May 2013
6 Document reviewed May 2014
7 Document reviewed June 2015
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 30 of 150

1. INTRODUCTION
1.1 General
1.1.1 These Standing Financial Instructions (SFIs) are issued in accordance with the Trust
(Functions) Directions 2000 issued by the Secretary of State which require that each Trust
shall agree Standing Financial Instructions for the regulation of the conduct of its members
and officers in relation to all financial matters with which they are concerned. They shall have
effect as if incorporated in the Standing Orders (SOs).
1.1.2 The Code of Conduct and Accountability in the NHS issued by the Department of Health
requires that each NHS organisation shall give, and may vary or revoke, Standing Financial
Instructions for the regulation of the conduct of its members and officers in relation to all
financial matters with which they are concerned. These Standing Financial Instructions (SFIs)
are issued in accordance with the Code.
1.1.3 These SFIs detail the financial responsibilities, policies and procedures to be adopted by the
Trust. They are designed to ensure that its financial transactions are carried out in accordance
with the law and government policy in order to achieve probity, accuracy, economy, efficiency
and effectiveness. They should be used in conjunction with the Schedule of Decisions
Reserved to the Board of Directors (Scheme of Reservation) and the Scheme of Delegation
adopted by the Trust.
1.1.4 These SFIs identify the financial responsibilities, which apply to everyone working for the Trust
(see also 1.2.2 below) and its constituent organisations including Trading Units. They do not
provide detailed procedural advice. These statements should therefore be read in conjunction
with the detailed departmental and financial procedure notes. The Director of Finance must
approve all financial procedures.
1.1.5 Should any difficulties arise regarding the interpretation or application of any of the SFIs then
the advice of the Director of Finance must be sought before acting. The user of these SFIs
should also be familiar with and comply with the provisions of the Trust’s SOs.
Failure to comply with the Standing Financial Instructions is a disciplinary matter,
which could result in dismissal.
1.1.6 Duty to report non-compliance with the Standing Financial Instructions All members of
the Board of Directors and staff have a duty to disclose any non-compliance with these
Standing Financial Instructions to the Director of Finance and Chief Executive as soon as
possible. If the Standing Financial Instructions are not complied with, full details of the non-
compliance and any justification for non-compliance and the circumstances around the non-
compliance shall be reported to the next formal meeting of the Audit Committee for them to
recommend action or ratification to the Board.
1.2 Terminology
1.2.1 Wherever the title Chief Executive, Director of Finance, or other nominated officer is used in
these instructions, it shall be deemed to include such other directors or employees who have
been duly authorised to represent them.
1.2.2 Wherever the term "employee" is used and where the context permits it shall be deemed to
include employees of third parties contracted to the Trust when acting on behalf of the Trust.
Including nursing and medical staff and consultants practising on the Trust premises and
members of staff of the PFI contractor or trust staff working the contractor under retention of
employment model.
1.3 Responsibilities and Delegation
1.3.1 The Board of Directors exercises financial supervision and control by:
a) formulating the financial strategy;
b) requiring the submission and approval of budgets within overall income;
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 31 of 150

c) defining and approving essential features in respect of important procedures and
financial systems (including the need to obtain value for money)
d) ensuring appropriate audit provision; and
e) defining specific responsibilities placed on directors and employees as indicated in the
Scheme of Delegation document
1.3.2 The Board of Directors has resolved that certain powers and decisions may only be exercised
by the Board of Directors in formal session. These are set out in the “Scheme of Reservation
to the Board of Directors” document, published within the Scheme of Delegation. The Board
of Directors will delegate responsibility for the performance of its functions in accordance with
the Scheme of Delegation document adopted by the Trust.
1.3.3 Within the SFIs, it is acknowledged that the Chief Executive is ultimately accountable to the
Board of Directors, and for ensuring that the Board of Directors meets its obligation to perform
its functions within the available financial resources. The Chief Executive has overall
executive responsibility for the Trust's activities, is responsible to the Board of Directors for
ensuring that its financial obligations and targets are met, and has overall responsibility for the
Trust’s system of internal control.
1.3.4 The Chief Executive and Director of Finance will, as far as possible, delegate their detailed
responsibilities but they remain accountable for financial control.
1.3.5 It is a duty of the Chief Executive to ensure that existing directors and employees and all new
appointees are notified of and understand their responsibilities within these Instructions. All
staff shall be responsible for ensuring conformity with the Standing Orders, Standing Financial
Instructions and financial procedures of the Trust.
1.3.6 The Director of Finance is responsible for:
a) implementing the Trust’s financial policies and for co-ordinating any corrective action
necessary to further these policies; (The SFIs themselves do not provide detailed
procedural advice. These statements should therefore be read in conjunction with the
detailed departmental and financial procedure notes).
b) maintaining an effective system of internal financial control including ensuring that
detailed financial procedures and systems incorporating the principles of separation of
duties and internal checks are prepared, documented and maintained to supplement
these instructions;
c) ensuring that sufficient records are maintained to show and explain the Trust’s
transactions, in order to disclose, with reasonable accuracy, the financial position of
the Trust at any time;
and, without prejudice to any other functions of directors and employees to the Trust,
the duties of the Director of Finance include:
d) the provision of financial advice to other members of the Board of Directors, and
employees;
e) the design, implementation and supervision of systems of internal financial control;
and
f) the preparation and maintenance of such accounts, certificates, estimates, records
and financial reports as the Trust may require for the purpose of carrying out its
statutory duties.
1.3.7 All directors and employees, individually and collectively, are responsible for:
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 32 of 150

a) the security of the property, assets and resources of the Trust;
b) avoiding loss;
c) exercising economy and efficiency in the use of resources; and
d) conforming with the requirements of Standing Orders, Standing Financial Instructions,
Financial Procedures and the Scheme of Reservation and Delegation.
1.3.8 Any contractor or employee of a contractor who is empowered by the Trust to commit the
Trust to expenditure or who is authorised to obtain income shall be covered by these
instructions. It is the responsibility of the Chief Executive to ensure that such persons are
made aware of this.
1.3.9 For all members of the Board and any employees who carry out a financial function, the form
in which financial records are kept and the manner in which directors and employees
discharge their duties must be to the satisfaction of the Director of Finance.
2. AUDIT
2.1 Audit Committee
2.1.1 In accordance with Standing Orders the Board of Directors shall formally establish an Audit
Committee, with clearly defines terms of reference and following guidance from the NHS Audit
Committee Handbook, which will provide an independent and objective view of internal control
by:
a) overseeing Internal and External Audit and Counter Fraud services;
b) reviewing financial and information systems and monitoring the integrity of the
financial statements and reviewing of significant financial reporting judgements;
c) the monitoring of compliance with Standing Orders and Standing Financial
Instructions;
d) reviewing schedules of losses and compensation and making recommendations to
the Board of Directors.
e) reviewing the effective implementation of corporate governance measures to enable
the Trust to implement best practice as set out in appropriate guidance. This will
include the Assurance Framework and control related disclosure statements, for
example the Annual Governance Statement and supporting assurance processes;
together with any accompanying audit statement, prior to endorsement by the Board of
Directors.
f) reviewing schedules of debtors/creditors balances over 6 months and £5,000 old and
explanations / action plans.
g) review the establishment and maintenance of an effective system of integrated
governance, risk management and internal control, across the whole of the
organisation’s activities (both clinical and non-clinical), that supports the achievement
of the organisation’s objectives.
2.1.2 The Board of Directors shall satisfy itself that at least one member of the Audit Committee has
recent and relevant financial experience.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 33 of 150

2.1.3 Where the Audit Committee considers there is evidence of ultra vires transactions, evidence
of improper acts, or if there are other important matters that the committee wish to raise, the
Chair of the Audit Committee should raise the matter at a full meeting of the Board of
Directors (to the Director of Finance in the first instance.)
2.1.4 It is the responsibility of the Director of Finance to ensure adequate internal and external audit
services are provided and the Audit Committee shall be involved in the selection process
when an audit service provider is changed.
2.2 Director of Finance
2.2.1 The Director of Finance is responsible for:
a) ensuring there are arrangements to review, evaluate and report on the effectiveness
of internal control including the establishment of an effective internal audit function and
the coordination of other assurance arrangements;
b) ensuring that the internal audit is adequate and meets the NHS Internal Audit
Standards;
c) ensuring that the Trust maintains adequate Counter Fraud and Corruption
arrangements and deciding at what stage to involve the police in cases of fraud,
misappropriation, and other irregularities not involving fraud or corruption;
d) ensuring that an annual internal audit report is prepared for the consideration of the
Audit Committee and the Board of Directors. The report must cover:
i) a clear opinion on the effectiveness of internal controls in accordance with
current assurance framework guidance issued by the Department of Health
including for example compliance with control criteria and standards,
ii) major internal financial control weaknesses discovered,
iii) progress on the implementation of internal audit recommendations,
iv) progress against plan over the previous year,
v) strategic audit plan,
vi) a detailed plan for the coming year.
2.2.2 The Director of Finance or designated auditors are entitled without necessarily giving prior
notice to require and receive:
a) access to all records, documents and correspondence relating to any financial or
other relevant transactions, including documents of a confidential nature;
b) access at all reasonable times to any land, premises, members of the Board of
Directors or employee of the Trust;
c) the production of any cash, stores or other property of the Trust under a member of
the Board of Directors or employee's control; and
d) explanations concerning any matter under investigation.
2.3 Internal Audit
2.3.1 The NHS Trust Accounting Officer Memorandum requires the Trust to have an internal audit
function.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 34 of 150

2.3.2 Role of Internal Audit
The role of internal audit embraces two key areas:
The provision of an independent and objective opinion to the Accountable Officer, the
Board of Directors and the Audit Committee on the degree to which risk management,
control and governance support the achievement of the organisation’s agreed objectives.
The provision of an independent and objective consultancy service specifically to help line
management improve the organisation’s risk management, control and governance
arrangements.
Internal Audit will review, appraise and report upon:
a) the extent of compliance with, and the financial effect of, relevant established policies,
plans and procedures;
b) the adequacy and application of financial and other related management controls;
c) the suitability of financial and other related management data;
d) the extent to which the Trust’s assets and interests are accounted for and
safeguarded from loss of any kind, arising from:
i) fraud and other offences,
ii) waste, extravagance, inefficient administration,
iii) poor value for money or other causes.
e) Internal Audit shall also independently verify the Assurance Statements in accordance
with guidance from the Department of Health.
2.3.3 Whenever any matter arises which involves, or is thought to involve, irregularities concerning
cash, stores, or other property or any suspected irregularity in the exercise of any function of a
pecuniary nature, the Director of Finance must be notified immediately.
2.3.4 The Head of Internal Audit will normally attend Audit Committee meetings and has a right of
access to all Audit Committee members, the Chair and Chief Executive of the Trust.
2.3.5 The Head of Internal Audit shall be accountable to the Director of Finance. The reporting
system for internal audit shall be agreed between the Director of Finance, the Audit Committee
and the Head of Internal Audit. The agreement shall be in writing and shall comply with the
guidance on reporting contained in the NHS Internal Audit Manual. The reporting system shall
be reviewed at least every 3 years. Where, in exceptional circumstances, the use of normal
reporting channels is thought to limit the objectivity of the audit, the Head of Internal Audit shall
have access to report direct to the Chair or a non-executive member of the Trust’s Audit
Committee.
2.3.6 Managers in receipt of audit reports referred to them, have a duty to take appropriate remedial
action within the agreed time-scales specified within the report. The Director of Finance shall
identify a formal review process to monitor the extent of compliance with audit
recommendations. Where appropriate, remedial action has failed to take place within a
reasonable period, the matter shall be reported to the Director of Finance.
2.4 External Audit
2.4.1 The External Auditor is appointed by the Audit Commission and paid for by the Trust. The
Audit Committee must ensure a cost-efficient service. If there are any problems relating to the
service provided by the External Auditor, then this should be raised with the External Auditor
and referred on to the Audit Commission if the issue cannot be resolved.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 35 of 150
2.5 Fraud, Bribery and Corruption
2.5.1 The Chief Executive and Director of Finance shall monitor and ensure compliance with the
NHS Contractual requirements for countering fraud, bribery and corruption, as well as any
other requirements as may be instructed by NHS Protect periodically.
2.5.2 The Trust shall nominate a suitable person to carry out the duties of the Local Counter Fraud
Specialist as specified by NHS Protect and the Department of Health Fraud and Corruption
Manual and guidance.
2.5.3 The Local Counter Fraud Specialist shall report to the Trust Director of Finance and shall work
with the staff in NHS Protect, in accordance with the Department of Health Fraud and
Corruption Manual.
2.5.4 The Local Counter Fraud Specialist will provide a written plan and report, at least annually on
counter fraud and corruption work within the Trust.
2.6 Security Management
2.6.1 In line with their responsibilities, the Trust Chief Executive will monitor and ensure
compliance with Directions issued by the Secretary of State for Health on NHS security
management
2.6.2 The Trust shall nominate a suitable person to carry out the duties of the Local Security
Management Specialist (LSMS) as specified by the Secretary of State for Health guidance
on NHS security management.
2.6.3 The Chief Executive has overall responsibility for controlling and coordinating security.
However, key tasks are delegated to the Director of Finance and the appointed Local
Security Management Specialist (LSMS).
3 ALLOCATIONS / PAYMENT BY RESULTS, BUSINESS PLANNING, BUDGETS, BUDGETARY CONTROL, AND MONITORING
3.1 Preparation and approval of business plans / Service Development Strategy (Local
Delivery Plan) and budgets
3.1.1 The Chief Executive will compile and submit to the Board of Directors an Annual Business
Plan that takes into account financial targets and forecast limits of available resources. The
annual business plan will contain:
a) a statement of the significant assumptions on which the plan is based;
b) details of major changes in workload, delivery of services or resources required to
achieve the plan.
3.1.2 Prior to the start of the financial year the Director of Finance will, on behalf of the Chief
Executive, prepare and submit budgets relating to income and expenditure for approval by the
Board of Directors. Such budgets will:
a) be in accordance with the aims and objectives set out in the Trust’s annual business
plan / Service Development Strategy, and the commissioners’ local delivery plans;
b) accord with workload and manpower plans;
c) be produced following discussion with appropriate budget holders;
d) be prepared within the limits of available funds;
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 36 of 150
e) identify potential risks; and
f) be based on reasonable and realistic assumptions.
3.1.3 The Director of Finance shall monitor the financial performance against budgets, periodically
review it and report to the Board of Directors. Any significant variances should be reported by
the Director of Finance to the Board of Directors as soon as they come to light and the Board
of Directors shall be advised of action to be taken in respect of such variances.
3.1.4 All budget holders must provide information as required by the Director of Finance to enable
budgets to be compiled.
3.1.5 All budget holders will sign up to their allocated budgets at the commencement of each
financial year.
3.1.6 The Director of Finance has a responsibility to ensure that adequate training is delivered on an
on-going basis to all budget holders to help them manage successfully.
3.2 Budgetary delegation
3.2.1 The Chief Executive may delegate the management of a budget to permit the performance of
a defined range of activities, including pooled budget arrangements under Section 31 of the
Health Act 1999. This delegation must be in writing and be accompanied by a clear definition
of:
a) the amount of the budget;
b) the purpose(s) of each budget heading;
c) individual and group responsibilities;
d) authority to exercise virement;
e) achievement of planned levels of service; and
f) the provision of regular reports.
3.2.2 The Chief Executive and delegated budget holders must not exceed the budgetary total or
virement limits set by the Board of Directors.
3.2.3 Any budgeted funds not required for their designated purpose(s) revert to the immediate
control of the Chief Executive, subject to any authorised use of virement.
3.2.4 Non-recurring budgets should not be used to finance recurring expenditure without the
authority in writing of the Chief Executive, as advised by the Director of Finance.
3.3 Budgetary control and reporting
3.3.1 The Director of Finance will devise and maintain systems of budgetary control. These will
include:
a) regular financial reports to the Board of Directors in a form approved by the Board of
Directors containing:
i) income and expenditure to date showing trends and forecast year-end
position;
ii) balance sheet, including movements in working capital,
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 37 of 150

iii) cash flow statement and details of performance within Prudential Borrowing
Code.
iii) capital project spend and projected out-turn against plan,
iv) explanations of any material variances from plan/budget;
v) details of any corrective action where necessary and the Chief Executive's
and/or Director of Finance's view of whether such actions are sufficient to
correct the situation;
b) the issue of timely, accurate and comprehensible advice and financial reports to each
budget holder, covering the areas for which they are responsible;
c) investigation and reporting of variances from financial, and workload budgets;
d) the monitoring of management action to correct variances;
e) arrangements for the authorisation of budget transfers;
f) advising the Chief Executive and Board of Directors of the consequences of changes
in policy, pay awards and other events and trends affecting budgets and shall advise
on the economic and financial impact of future plans and projects; and.
g) review of the bases and assumptions used to prepare the budgets.
In the performance of these duties the Director of Finance will have access to all budget
holders on budgetary matters and shall be provided with such financial and statistical
information as is necessary.
3.3.2 Each budget holder is responsible for ensuring that:
a) any likely overspending or reduction of income which cannot be met by virement is not
incurred without the prior consent of the Board of Directors;
b) officers shall not exceed the budget limit set;
c) the amount provided in the approved budget is not used in whole or in part for any
purpose other than that specifically authorised subject to the rules of virement; and,
d) no permanent employees are appointed without the approval of the Chief Executive
other than those provided for in the budgeted establishment as approved by the Board
of Directors.
3.3.3 The Chief Executive is responsible for identifying and implementing cost improvements and
income generation initiatives in accordance with the requirements of the Annual Business Plan
and a balanced budget.
3.4 Capital expenditure
3.4.1 The general rules applying to delegation and reporting shall also apply to capital expenditure.
(The particular applications relating to capital are contained in Section 11.) A Project Manager
will be identified who will assume responsibility for the budget relating to the scheme.
3.5 The Monitoring returns
3.5.1 The Chief Executive is responsible for ensuring that the appropriate monitoring forms are
submitted to the requisite monitoring organisation within the specified time-scales.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 38 of 150

4 ANNUAL ACCOUNTS AND REPORTS
4.1 Accounts
The Director of Finance, on behalf of the Trust, will:
(a) prepare financial returns in accordance with the accounting policies and guidance
given by the Department of Health and the Treasury, the Trust’s accounting policies,
and generally accepted accounting practice;
(b) prepare and submit annual financial reports to the Department of Health certified in
accordance with current guidelines;
(c) submit financial returns to the Department of Health for each financial year in
accordance with the timetable prescribed by the Department of Health.
The Trust’s annual accounts must be audited by an auditor appointed by the Audit
Commission. The Trust’s audited annual accounts must be presented to a public meeting
and made available to the public.
4.2 Annual Reports
The Trust will publish an annual report, in accordance with guidelines on local accountability,
and present it at a public meeting. The document will comply with the Department of Health's
Manual for Accounts.
5 BANK AND OPG ACCOUNTS
5.1 General
5.1.1 The Director of Finance is responsible for managing the Trust banking arrangements and for
advising the Trust on the provision of banking services and operation of accounts. In line with
‘Cash Management in the NHS’ Trusts should minimize the use of commercial bank accounts
and consider using Governance Banking Service (GBS) accounts for all banking services.
5.1.2 The Board of Directors shall approve the banking arrangements.
5.2 Bank and OPG accounts
5.2.1 The Director of Finance is responsible for:
a) bank accounts and GBS accounts; and other forms of working capital financing that
may be available from the Department of Health.
b) establishing separate bank accounts for the Trust’s non-exchequer funds;
c) ensuring payments made from bank or GBS accounts do not exceed the amount
credited to the account except where arrangements have been made;
d) reporting to the Board of Directors all arrangements made with the Trust’s bankers for
accounts to be overdrawn (together with the remedial action taken); and
All accounts should be held in the name of the Trust. No officer other than the Director of
Finance shall open any account in the name of the Trust or for the purpose of furthering Trust
activities.
5.3 Banking procedures
5.3.1 The Director of Finance will prepare detailed instructions on the operation of bank and GBS
accounts, which must include:
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 39 of 150
a) the conditions under which each bank and GBS account is to be operated;
b) the limit to be applied to any overdraft; and
c) those authorised to sign cheques or other orders drawn on the Trust’s accounts.
5.3.2 The Director of Finance must advise the Trust’s bankers in writing of the conditions under
which each account will be operated.
5.3.3 The Director of Finance shall approve security procedures for any cheques issued without a
hand-written signature e.g. lithographed. Manually produced cheques shall be signed by the
authorised officer(s) in accordance with the bank mandate.
All cheques shall be treated as controlled stationery, in the charge of a duly designated officer
controlling their issue.
5.4 Tendering and Review
5.4.1 The Director of Finance will review the commercial banking arrangements of the Trust at
regular intervals to ensure they reflect best practice and represent best value for money by
periodically seeking competitive tenders for the Trust’s business banking.
5.4.2 Competitive tenders should be sought at least every 5 years. The results of the tendering
exercise should be reported to the Board of Directors. This review is not applicable to GBS
accounts.
6 INCOME, FEES AND CHARGES AND SECURITY OF CASH, CHEQUES AND OTHER NEGOTIABLE INSTRUMENTS
6.1 Income systems
6.1.1 The Director of Finance is responsible for designing, maintaining and ensuring compliance
with systems for the proper recording, invoicing, collection and coding of all monies due.
6.1.2 All such systems shall incorporate, where practicable, in full the principles of internal check
and separation of duties.
6.1.3 The Director of Finance is also responsible for the prompt banking of all monies received.
6.2 Fees and charges other than Trust Contract.
6.2.1 The Trust shall follow the Department of Health’s advice in the ‘Costing Manual’ in setting
prices for NHS service agreements.
6.2.2 The Director of Finance is responsible for approving and regularly reviewing the level of all
fees and charges other than those determined by the Department of Health or by Statute.
Independent professional advice on matters of valuation shall be taken as necessary. Where
sponsorship income (including items in kind such as subsidised goods or loans of equipment)
is considered the guidance in the Department of Health’s Commercial Sponsorship – Ethical
standards in the NHS shall be followed. See also Standing Orders.
6.2.3 All employees must inform the Director of Finance promptly of money due arising from
transactions which they initiate/deal with, including all contracts, leases, tenancy agreements,
private patient undertakings and other transactions.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 40 of 150

6.3 Debt recovery
6.3.1 The Director of Finance is responsible for the appropriate recovery action on all outstanding
debts, including a formal follow up procedure for all debtor accounts. Overpayments should
be detected (or preferably prevented) and recovery initiated.
6.3.2 Income not received should be dealt with in accordance with losses procedures.
6.4 Security of cash, cheques and other negotiable instruments
6.4.1 The Director of Finance is responsible for:
a) approving the form of all receipt books, agreement forms, or other means of officially
acknowledging or recording monies received or receivable; (No form of receipt which
has not been specifically authorised by the Director of Finance should be issued).
b) ordering and securely controlling any such stationery;
c) the provision of adequate facilities and systems for employees whose duties include
collecting and holding cash, including the provision of safes or lockable cash boxes,
the procedures for keys, and for coin operated machines; and
d) prescribing systems and procedures for handling cash and negotiable securities on
behalf of the Trust.
6.4.2 Official money shall not under any circumstances be used for the encashment of private
cheques, nor IOUs.
6.43 Staff shall be informed in writing on appointment of their responsibilities and duties for the
collection, handling or disbursement of cash, cheques etc.
6.4.4 All cheques, postal orders, cash etc., shall be banked promptly intact under arrangements
approved by the Director of Finance.
6.4.5 The holders of safe keys shall not accept unofficial funds for depositing in their safes unless
such deposits are in special sealed envelopes or locked containers. It shall be made clear to
the depositors that the Trust is not to be held liable for any loss, and written indemnities must
be obtained from the organisation or individuals absolving the Trust from responsibility for any
loss.
6.4.6 Any loss or shortfall of cash, cheques or other negotiable instruments, however occasioned,
shall be the monitored and recorded within the Finance Department. Any significant trends
should be reported to the Director of Finance and Internal Audit via the incident reporting
system. Where there is prima facie evidence of fraud, bribery or corruption this should be
reported in accordance with the Trust’s Fraud and Corruption Reporting Arrangements (See
Appendices) and the guidance provided by NHS Protect. Where there is no evidence of fraud
or corruption the loss should be dealt with in line with the Trust’s Losses and Compensations
Procedures.
7 NHS SERVICE AGREEMENTS FOR PROVISION OF SERVICES
7.1 Service Level Agreements
7.1.1 The Chief Executive, as the Accountable Officer, is responsible for ensuring the Trust enters
into suitable Service Level Agreements (SLA) with service commissioners for the provision of
NHS services.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 41 of 150

All SLAs should aim to implement the agreed priorities contained within the Annual Plan and
wherever possible, be based upon integrated care pathways to reflect expected patient
experience. In discharging this responsibility, the Chief Executive should take into account:
the standards of service quality expected;
the relevant national service framework (if any);
the provision of reliable information on cost and volume of services;
the NHS National Performance Assessment Framework;
that SLAs build where appropriate on existing Joint Investment Plans;
that SLAs are based on integrated care pathways.
7.1.2 A good SLA will result from a dialogue of clinicians, users, carers, public health professionals
and managers. It will reflect knowledge of local needs and inequalities. This will require the
Chief Executive to ensure that the Trust works with all partner agencies involved in both the
delivery and the commissioning of the service required. The SLA will apportion responsibility
for handling a particular risk to the party or parties in the best position to influence the event
and financial arrangements should reflect this. In this way the Trust can jointly manage risk
with all interested parties.
7.1.3 The Chief Executive, as the Accountable Officer, will need to ensure that regular reports are
provided to the Board detailing actual and forecast income from the SLA. This will include
information on costing arrangements, which increasingly should be based upon Healthcare
Resource Groups (HRGs). Where HRGs are unavailable for specific services, all parties
should agree a common currency for application across the range of SLAs.
8 TERMS OF SERVICE, ALLOWANCES AND PAYMENT OF MEMBERS OF THE BOARD OF DIRECTORS AND EMPLOYEES
8.1 Remuneration Committee
8.1.1 In accordance with Standing Orders the Board of Directors shall establish a Remuneration
Committee, with clearly defined terms of reference, specifying which posts fall within its area
of responsibility, its composition, and the arrangements for reporting.
8.1.2 The Committee will:
a) agree appropriate remuneration and terms of service for the Chief Executive and
other executive directors (and other senior employees), including:
i) all aspects of salary (including any performance-related elements/bonuses);
ii) provisions for other benefits, including pensions and cars;
iii) arrangements for termination of employment and other contractual terms;
b) agree the remuneration and terms of service of executive directors (and other senior
employees) to ensure they are fairly rewarded for their individual contribution to the
Trust - having proper regard to the Trust's circumstances and performance and to the
provisions of any national arrangements for such staff where appropriate;
c) monitor and evaluate the performance of individual executive directors (and other
senior employees); and
d) oversee appropriate contractual arrangements for such staff including the proper
calculation and scrutiny of termination payments taking account of such national
guidance as is appropriate.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 42 of 150
8.1.3 The Committee shall be accountable for taking decisions on the remuneration and terms of
service of executive directors. Minutes of the Committee meetings should record such
decisions.
8.1.4 The Board of Directors will approve proposals presented by the Chief Executive for setting of
remuneration and conditions of service for those employees not covered by the Committee.
8.1.5 The Trust will pay allowances to the Chair and non-officer members of the Board in
accordance with instructions issued by the Secretary of State for Health
8.2 Funded establishment
8.2.1 The manpower plans incorporated within the annual budget will form the funded
establishment.
8.2.2 The funded establishment of any department may not be varied without the approval of the
Chief Executive or individual nominated within the relevant section of the Scheme of
Reservation and Delegation. The Finance Department are responsible for verifying that
funding is available.
8.3 Staff appointments
8.3.1 No Executive Director or employee may engage, re-engage, or re-grade employees, either on
a permanent or temporary nature, or hire agency staff, or agree to changes in any aspect of
remuneration:
a) unless authorised to do so by the Chief Executive; and
b) within the limit of their approved budget and funded establishment as defined in the
Scheme of Reservation and Delegation.
8.3.2 The Board of Directors will approve procedures presented by the Chief Executive for the
determination of commencing pay rates, condition of service, etc., for employees.
8.4 Processing of the payroll
8.4.1 The Director of Human Resources in conjunction with the Director of Finance is responsible
for:
a) specifying timetables for submission of properly authorised time records and other
notifications;
b) the final determination of pay and allowances; including verification that the rate of pay
and relevant conditions of service are in accordance with current agreements.
c) making payment on agreed dates; and
d) agreeing method of payment.
8.4.2 The Director of Human Resources will issue instructions regarding:
a) verification and documentation of data;
b) the timetable for receipt and preparation of payroll data and the payment of
employees and allowances;
c) maintenance of subsidiary records for superannuation, income tax, social security and
other authorised deductions from pay;
d) security and confidentiality of payroll information;
e) checks to be applied to completed payroll before and after payment;
f) authority to release payroll data under the provisions of the Data Protection Act;
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 43 of 150

g) methods of payment available to various categories of employee;
h) procedures for payment by cheque, bank credit, or cash to employees;
i) procedures for the recall of cheques and bank credits
j) pay advances and their recovery;
k) maintenance of regular and independent reconciliation of pay control accounts;
l) separation of duties of preparing records and handling cash; and
m) a system to ensure the recovery from leavers of sums of money and property due by
them to the Trust.
8.4.3 Appropriately nominated managers have delegated responsibility for:
a) processing a signed copy of the contract/appointment form and such other
documentation as may be required immediately upon an employee commencing duty.
b) submitting time records, and other notifications in accordance with agreed timetables;
c) completing time records and other notifications in accordance with the Director of
Human Resource’s instructions and in the form prescribed by the Director of Human
Resources; and
d) submitting termination forms in the prescribed form immediately upon knowing the
effective date of an employee's resignation, termination or retirement. Where an
employee fails to report for duty in circumstances that suggest they have left without
notice, the Director of Human Resources must be informed immediately. In
circumstances where fraud might be expected this must be reported to the Director of
Finance.
8.4.4 Regardless of the arrangements for providing the payroll service, the Director of Human
Resources in conjunction with the Director of Finance shall ensure that the chosen method is
supported by appropriate (contracted) terms and conditions, adequate internal controls and
audit review procedures and that suitable arrangements are made for the collection of payroll
deductions and payment of these to appropriate bodies.
8.5 Contracts of employment
8.5.1 The Board of Directors shall delegate responsibility to a manager for:
a) ensuring that all employees are issued with a Contract of Employment in a form
approved by the Board of Directors and which complies with employment and Health
& Safety legislation; and
b) dealing with variations to, or termination of, contracts of employment.
9 NON-PAY EXPENDITURE
9.1 Delegation of authority
9.1.1 The Board of Directors will approve the level of non-pay expenditure on an annual basis and
the Chief Executive will determine the level of delegation to budget holders.
9.1.2 The Chief Executive will set out:
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 44 of 150

a) the list of managers who are authorised to place requisitions for the supply of goods
and services should be updated and reviewed on an ongoing basis and annually by
the Supplies Department; and
b) where the authorisation system is computerised the list will be maintained within the
computerised system and the ‘signature’ will be in the form of electronic authorisation
in accordance with the access and authority controls maintained within the
computerised system; and
c) the maximum level of each requisition and the system for authorisation above that
level.
The Chief Executive shall set out procedures on the seeking of professional advice regarding
the supply of goods and services.
9.2 Choice, requisitioning, ordering, receipt and payment for goods and services
9.2.1 The requisitioner, in choosing the item to be supplied (or the service to be performed) shall
always obtain the best value for money for the Trust. In so doing, the advice of the Trust’s
advisor shall be sought. Where this advice is not acceptable to the requisitioner, the Director
of Finance (and/or the Chief Executive) shall be consulted.
9.2.2 The Director of Finance shall be responsible for the prompt payment of properly authorised
accounts and claims in accordance with the Better Payment Practice Code (BPPC). Payment
of contract invoices shall be in accordance with contract terms, or otherwise, in accordance
with national guidance.
9.2.3 The Director of Finance will:
a) advise the Board of Directors regarding the setting of thresholds above which
quotations (competitive or otherwise) or formal tenders must be obtained; and, once
approved, the thresholds should be incorporated in Scheme of Reservation and
Delegation and regularly reviewed;
b) prepare procedural instructions where not already provided in the Scheme of
Delegation or procedure notes for budget holders on the obtaining of goods, works
and services incorporating the thresholds;
c) be responsible for the prompt payment of all properly authorised accounts and claims;
d) be responsible for designing and maintaining a system of verification, recording and
payment of all amounts payable. The system shall provide for:
i) A list of directors/employees (including specimens of their signatures)
authorised to approve or incur expenditure. Where the authorisation system
is computerised the list will be maintained within the computerised system and
the ‘signature’ will be in the form of electronic authorisation in accordance with
the access and authority controls maintained within the computerised system.
ii) Certification that:
- goods have been duly received, examined and are in accordance
with specification and the prices are correct (including for those
invoices below passive approval limits stipulated within SoRD);
- work done or services rendered have been satisfactorily carried out in
accordance with the order, and, where applicable, the materials used
are of the requisite standard and the charges are correct;
- in the case of contracts based on the measurement of time, materials
or expenses, the time charged is in accordance with the time sheets,
the rates of labour are in accordance with the appropriate rates, the
materials have been checked as regards quantity, quality, and price
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 45 of 150

and the charges for the use of vehicles, plant and machinery have
been examined;
- where appropriate, the expenditure is in accordance with regulations
and all necessary authorisations have been obtained;
- the account is arithmetically correct;
- the account is in order for payment.
iii) A timetable and system for submission to the Director of Finance of accounts
for payment; provision shall be made for the early submission of accounts
subject to cash discounts or otherwise requiring early payment.
iv) Instructions to employees regarding the handling and payment of accounts
within the Finance Department.
e) be responsible for ensuring that payment for goods and services is only made once
the goods and services are received, (except as below).
9.2.4 Prepayments outside of normal commercial arrangements, for example fully comprehensive
maintenance contracts, rental, insurance are only permitted where exceptional circumstances
apply. In such instances:
a) prepayments are only permitted where the financial advantages outweigh the
disadvantages (i.e. cashflows must be discounted to NPV using the National Loans
Fund (NLF) rate.
b) the appropriate officer in conjunction with the Procurement Department must provide,
in the form of a written report, a case setting out all relevant circumstances of the
purchase. The report must set out the effects on the Trust if the supplier is at some
time during the course of the prepayment agreement unable to meet their
commitments;
e) the Director of Finance will need to be satisfied with the proposed arrangements
before contractual arrangements proceed (taking into account the EU public
procurement rules where the contract is above a stipulated financial threshold);
e) the Budget Holder is responsible for ensuring that all items due under a prepayment
contract are received and they must immediately inform the appropriate Director or
Chief Executive if problems are encountered.
9.2.5 Official Orders must:
a) be consecutively numbered;
b) be in a form approved by the Director of Finance;
c) state the Trust terms and conditions of trade; and
d) only be issued to, and used by, those duly authorised by the Chief Executive.
9.2.6 Managers must ensure that they comply fully with the guidance and limits specified by the
Director of Finance and that:
a) all contracts other than for a simple purchase permitted within the Scheme of
Delegation or delegated budget, leases, tenancy agreements and other commitments
which may result in a liability are notified to the Director of Finance in advance of any
commitment being made;
b) contracts above specified thresholds are advertised and awarded in accordance with
EU and GATT rules on public procurement and comply with the White Paper on
Standards, Quality and International Competitiveness (CMND 8621);
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 46 of 150

c) where consultancy advice is being obtained, the procurement of such advice must be
in accordance with guidance issued by the Department of Health;
Where an officer certifying accounts relies upon other officers to do preliminary
checking, they shall wherever possible, ensure that those who check delivery or
execution of work act independently of those who have placed orders and negotiated
prices and terms.
d) no order shall be issued for any item or items to any firm which has made an offer of
gifts, reward or benefit to directors or employees, other than:
i) isolated gifts of a trivial character or inexpensive seasonal gifts, such as
calendars;
ii) conventional hospitality, such as lunches in the course of working visits;
e) no requisition/order is placed for any item or items for which there is no budget
provision unless authorised by the Director of Finance on behalf of the Chief
Executive;
f) all goods, services, or works are ordered on an official order except works and
services executed in accordance with a contract and purchases from petty cash or on
purchasing cards;
g) verbal orders must only be issued very exceptionally - by an employee designated by
the Chief Executive and only in cases of emergency or urgent necessity. These must
be confirmed by an official order, and clearly marked "Confirmation Order".
h) orders are not split or otherwise placed in a manner devised so as to avoid the
financial thresholds;
i) goods are not taken on trial or loan in circumstances that could commit the Trust to a
future un-competitive purchase;
j) changes to the list of directors/employees authorised to certify invoices are notified to
the Director of Finance;
k) purchases from petty cash are restricted in value and by type of purchase in
accordance with instructions issued by the Director of Finance;
l) petty cash records are maintained in a form as determined by the Director of Finance;
and,
j) orders are not required to be raised for utility bills, NHS Recharges; audit fees and ad
hoc services such as private hospital fees. Payments must be authorised in
accordance with the delegated limits set for non pay.
9.2.7 The Chief Executive and Director of Finance shall ensure that the arrangements for financial
control and financial audit of building and engineering contracts and property transactions
comply with the guidance contained within CONCODE and the NHS Trust Capital Accounting
Manual. The technical audit of these contracts shall be the responsibility of the relevant
Director.
9.2.8 Under no circumstances should goods be ordered through the Trust for personal or private
use.
9.3 Joint finance arrangements with local authorities and voluntary bodies
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 47 of 150

9.3.1 Payments to local authorities and voluntary organisations made under the powers of section
28A of the NHS Act shall comply with procedures laid down by the Director of Finance which
shall be in accordance with these Acts.
10 EXTERNAL BORROWING AND INVESTMENTS
10.1 Public Dividend Capital
10.1.1 The Director of Finance will advise the Board concerning the Trust’s ability to pay dividend on,
and repay Public Dividend Capital and any proposed new borrowing, within the limits set by
the Department of Health. The Director of Finance is also responsible for reporting periodically
to the Board concerning the PDC debt and all loans and overdrafts.
10.1.2 The Board will agree the list of employees (including specimens of their signatures) who are
authorised to make short term borrowings on behalf of the Trust. This must contain the Chief
Executive and the Director of Finance.
10.1.3 The Director of Finance must prepare detailed procedural instructions concerning
applications for loans and overdrafts.
10.1.4 All short-term borrowings should be kept to the minimum period of time possible, consistent
with the overall cashflow position, represent good value for money, and comply with the
latest guidance from the Department of Health.
10.1.5 Any short-term borrowing must be with the authority of two members of an authorised panel,
one of which must be the Chief Executive or the Director of Finance. The Board must be
made aware of all short term borrowings at the next Board meeting.
10.1.6 All long-term borrowing must be consistent with the plans outlined in the current Annual Plan
and be approved by the Board.
10.2 Investment
10.2.1 Temporary cash surpluses must be held only in such public or private sector investments as
notified by the Secretary of State and authorised by the Board.
10.2.2 The Director of Finance is responsible for advising the Board on investments and shall
report periodically to the Board concerning the performance of investments held.
10.2.3 The Director of Finance will prepare detailed procedural instructions on the operation of
investment accounts and on the records to be maintained.
11 CAPITAL INVESTMENT, PRIVATE FINANCING, FIXED ASSET REGISTERS AND SECURITY OF ASSETS
11.1 Capital investment
11.1.1 Before the start of the financial year the Board is responsible for approving the annual capital
plan.
The Chief Executive:
a) shall ensure that there is an adequate appraisal and approval process in place for
determining capital expenditure priorities, based on the Estates Strategy and with the
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 48 of 150

involvement of the Director of Finance, Medical Director, Estates Team and IT Team,
and the effect of each proposal upon business plans;
b) is responsible for the management of all stages of capital schemes and for ensuring
that schemes are delivered on time and to cost;
c) shall ensure that a Project Board is established for schemes over £500,000;
d) each individual scheme is identified and has a monthly expenditure profile; and
e) shall ensure that the capital investment is not undertaken without the availability of
resources to finance all revenue consequences, including capital charges.
11.1.2 For capital expenditure proposals the Chief Executive shall ensure (in accordance with the
limits outlined in the Scheme of Delegation):
a) that a business case (in line with the guidance contained within the NHS Trust Capital
Accounting Manual) is produced setting out:
i) an option appraisal of potential benefits compared with known costs to
determine the option with the highest ratio of benefits to costs; and
ii) appropriate project management and control arrangements; and
iii) the involvement of appropriate Trust personnel and external agencies; and
b) that the Director of Finance has certified professionally to the costs and revenue
consequences detailed in the business case.
11.1.3 For capital schemes where the contracts stipulate stage payments, the Chief Executive will
issue procedures for their management, incorporating the recommendations of
“CONCODE/Estatecode” and the NHS Trust Capital Accounting Manual.
The Director of Finance shall assess on an annual basis the requirement for the operation of
the construction industry tax deduction scheme in accordance with Inland Revenue guidance.
The Director of Finance shall issue procedures for the regular reporting of expenditure and
commitment against authorised expenditure.
11.1.4 The approval of a capital programme shall not constitute approval for expenditure on any
scheme.
The Chief Executive shall issue to the manager responsible for any scheme:
a) specific authority to commit expenditure;
b) authority to proceed to tender;
c) approval to accept a successful tender
The Chief Executive will issue a scheme of delegation for capital investment management in
accordance with “CONCODE/Estatecode” and the NHS Trust Capital Accounting Manual
guidance and the Trust's Standing Orders.
11.1.5 The Director of Finance shall issue procedures governing the financial management, including
variations to contract, of capital investment projects and valuation for accounting purposes.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 49 of 150

11.2 Estates Capital Schemes
11.2.1 Project Managers must engage a Quantity Surveyor where the overall scheme cost (including
VAT, equipment and fees) exceeds £100,000. The role of the Quantity Surveyor is to value
stage payments and to challenge and support the value for money of the agreed works costs.
In addition the Quantity Surveyor should aid the Project Manager in forecasting final outturn
figures for the scheme.
11.2.2 The Project Manager has the authority to sign off staged payment certificates for their own
schemes up to £100,000. Certificates above this value need to be authorised by the Director
of Finance.
11.2.3 If the Quantity Surveyor or the Project Manager (if the scheme is below £100,000) forecasts
that the outturn is likely to be in excess of the budgeted scheme value then a request must be
made to use the capital contingency budget.
11.2.4 A detailed explanation of why the capital contingency budget is needed will be required. In all
cases the use of the capital contingency budget will be reported to the Board.
11.3 IT Capital Schemes
11.3.1 Smaller IT projects can be managed using the current controls in place, i.e., requisition and
purchase order authorisation and monthly monitoring with the Capital Accountant.
11.3.2 Larger IT projects will have a Project Manager who will report to a Project Board on a regular
basis. The Project Manager must provide forecast outturn figures to the Project Board at
each meeting. If an overspend is predicted then a request must be made to use the capital
contingency budget.
11.3.3 A detailed explanation of why the capital contingency budget is needed will be required. In all
cases the use of the capital contingency budget will be reported to the Board.
11.4 Medical Equipment
11.4.1 There is an allocation made each year for medical equipment and it is the responsibility of the
Medical Director to ensure each clinical area provides details of the medical equipment
required.
11.4.2 A standard form should be completed for each piece of equipment requested detailing why it
is required, its cost (including VAT) together with a quote, any ongoing revenue consequences
and a priority ranking as follows:
1. Equipment not functioning, service halted
2. Equipment unsafe – about to be withdrawn
3. Equipment giving sub-standard results – clinical risk acknowledged
4. Enhancement of service
5. New service: it is unlikely that any bid which falls into this category would be
supported. Any new service would be subject to a Business Case, which would
include costs of equipment.
11.4.3 All the forms will be collated and all requesters are invited to present their case and provide
evidence of the priority rankings above.
11.4.4 Based on the information received, the Committee will decide which pieces of equipment can
be funded from the capital allocation provided and will write out to the successful bidders with
instructions on how to purchase.
11.4.5 Purchasing will follow the normal controls of an electronic requisition to the Capital
Accountant.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 50 of 150

11.5 Private finance
The Trust should normally test for PFI when considering capital procurement. When the
Board proposes, or is required, to use finance provided by the private sector the following
should apply:
(a) The Director of Finance shall demonstrate that the use of private finance represents
value for money and genuinely transfers risk to the private sector.
(b) Where the sum involved exceeds delegated limits, the business case must be referred
to the appropriate DOH for approval or treated as per current guidelines.
(c) The proposal must be specifically agreed by the Trust in the light of such professional
advice as should reasonably be sought in particular with regard to vires.
(d) The selection of a contractor/finance company must be on the basis of competitive
tendering or quotations.
11.6 Asset registers
11.6.1 The Chief Executive is responsible for the maintenance of registers of assets, taking account
of the advice of the Director of Finance concerning the form of any register and the method of
updating, and arranging for a physical check of assets against the Asset Register to be
conducted once a year.
11.6.2 The Trust shall maintain an Asset Register recording fixed assets. As a minimum, the
minimum data set to be held within these registers shall be as specified in the Capital
Accounting Manual as issued by the Department of Health.
11.6.3 Additions to the fixed Asset Register must be clearly identified to an appropriate budget holder
and be validated by reference to:
a) properly authorised and approved agreements, architect's certificates, supplier's
invoices and other documentary evidence in respect of purchases from third parties;
b) stores, requisitions and wages records for own materials and labour including
appropriate overheads; and
c) lease agreements in respect of assets held under a finance lease and capitalised.
11.6.4 Where capital assets are sold, scrapped, lost or otherwise disposed of, their value must be
removed from the accounting records and each disposal must be validated by reference to
authorisation documents and invoices (where appropriate).
11.6.5 The Director of Finance shall approve procedures for reconciling balances on fixed assets
accounts in ledgers against balances on fixed Asset Registers.
11.6.6 The value of each asset shall be adjusted to current values in accordance with methods
specified in the Capital Accounting Manual issued by the Department of Health.
11.6.7 The value of each asset shall be depreciated using methods and rates as specified in the
Capital Accounting Manual issued by the Department of Health.
11.6.8 The Director of Finance shall calculate and pay capital charges as specified by the
Department of Health.
11.7 Security of assets
11.7.1 The overall control of fixed assets is the responsibility of the Chief Executive advised by the
Director of Finance.
Asset control procedures (including fixed assets, cash, cheques and negotiable instruments,
and also including donated assets) must be approved by the Director of Finance. This
procedure shall make provision for:
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 51 of 150

a) recording managerial responsibility for each asset;
b) identification of additions and disposals;
c) identification of all repairs and maintenance expenses;
d) physical security of assets;
e) periodic verification of the existence of, condition of, and title to, assets recorded;
f) identification and reporting of all costs associated with the retention of an asset; and
g) reporting, recording and safekeeping of cash, cheques, and negotiable instruments.
11.7.2 All significant discrepancies revealed by verification of physical assets to fixed Asset Register
shall be notified to the Director of Finance.
11.7.4 Whilst each employee has a responsibility for the security of property of the Trust, it is the
responsibility of directors and senior employees in all disciplines to apply such appropriate
routine security practices in relation to NHS property as may be determined by the Board of
Directors. Any breach of agreed security practices must be reported in accordance with
instructions.
11.7.5 Any damage to the Trust's premises, vehicles and equipment, or any loss of equipment,
stores or supplies must be reported by directors and employees in accordance with the
procedure for reporting losses.
11.7.6 Where practical, assets should be marked as Trust property.
12 STOCK, STORES AND RECEIPT OF GOODS
12.1 Stocks are defined as those goods normally utilised in day to day activity, but which at a given
point in time have not been used or consumed. There are three broad types of store:-
a) Controlled stores - specific areas designated for the holding and control of goods;
b) Wards & departments - goods required for immediate usage to support operational
services.
c) Manufactured Items - where goods and consumables are being made or processes
are being applied which add to the raw material cost of the goods.
12.2 Such stocks should be kept to a minimum and for;
a) controlled stores and other significant stores (as determined by the Director of
Finance) should be subjected to an annual stocktake or perpetual inventory
procedures; and
c) valued at the lower of cost and net realisable value.
12.3. Subject to the responsibility of the Director of Finance for the systems of control, overall
responsibility for the control of stores shall be delegated to an employee by the Chief
Executive. The day-to-day responsibility may be delegated by them to departmental
employees and stores managers/keepers, subject to such delegation being entered in a
record available to the Director of Finance. The control of any Pharmaceutical stocks shall be
the responsibility of a designated Pharmaceutical Officer; the control of any fuel oil of a
designated estates manager.
12.4 The responsibility for security arrangements and the custody of keys for all stores and
locations shall be clearly defined in writing by the designated manager. Wherever practicable,
stocks should be marked as NHS property.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 52 of 150

12.5 The Director of Finance shall set out procedures and systems to regulate the stores including
records for receipt of goods, issues, and returns to stores, and losses. Stocktaking
arrangements shall be agreed with the Director of Finance and there shall be a physical check
covering all items in store at least once a year.
12.6 Where a complete system of stores control is not justified, alternative arrangements shall
require the approval of the Director of Finance.
12.7 The designated manager shall be responsible for a system approved by the Director of
Finance for a review of slow moving and obsolete items and for condemnation, disposal, and
replacement of all unserviceable articles. The designated Officer shall report to the Director of
Finance any evidence of significant overstocking and of any negligence or malpractice (see
also 13, Disposals and Condemnations, Losses and Special Payments). Procedures for the
disposal of obsolete stock shall follow the procedures set out for disposal of all surplus and
obsolete goods.
12.8 Receipt of Goods
12.8.1 A delivery note shall be obtained from the supplier at the time of delivery and shall be signed
by the person receiving the goods. All goods received shall be checked, by the appropriate
department, as regards quantity and/or weight and inspected as to quality and specification.
Instructions shall be issued to staff covering the procedures to be adopted in those cases
where a delivery note is not available.
12.8.2 All goods received shall be entered onto an appropriate goods received/stock record (whether
a computer or manual system) on the day of receipt. If goods received are unsatisfactory, the
records shall be marked accordingly. Further, where the goods received are found to be
unsatisfactory, or short on delivery, they shall only be accepted on the authority of the
designated officer and the supplier shall be notified immediately.
12.8.3 For goods supplied via the NHS Logistics central warehouses, the Chief Executive shall
identify those authorised to requisition and accept goods from the store. The authorised
person shall check receipt against the delivery note to satisfy themselves that the goods have
been received. The Finance Department will make payment on receipt of an invoice. This
may also apply for high-level low volume items such as stationery.
12.9 Issue of Stocks
12.9.1 The issue of stocks shall be supplied by an authorised requisition note and a receipt for the
stock issued shall be returned to the designated officer. Where a ‘topping up’ system is used,
a record shall be maintained as approved by the Director of Finance. Regular comparisons
shall be made of the quantities issued to wards/departments etc. and explanations recorded of
significant variations.
12.9.2 All transfers and returns shall be recorded on forms/systems provided for the purpose and
approved by the Director of Finance.
13 DISPOSALS AND CONDEMNATIONS, INSURANCE, LOSSES AND SPECIAL PAYMENTS
13.1 Disposals and condemnations
13.1.1 The Director of Finance must prepare detailed procedures for the disposal of assets including
condemnations, and ensure that these are notified to managers.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 53 of 150

13.1.2 When it is decided to dispose of a Trust asset, the head of department or authorised deputy
will determine and advise the Director of Finance of the estimated market value of the item,
taking account of professional advice where appropriate.
13.1.3 All unserviceable articles shall be:
a) condemned or otherwise disposed of by an employee authorised for that purpose by
the Director of Finance;
b) recorded by the condemning officer in a form approved by the Director of Finance
which will indicate whether the articles are to be converted, destroyed or otherwise
disposed of. All entries shall be confirmed by the countersignature of a second
employee authorised for the purpose by the Director of Finance.
13.1.4 The condemning officer shall satisfy themselves as to whether or not there is evidence of
negligence in use and shall report any such evidence to the Director of Finance who will take
the appropriate action.
13.2 Losses and special payments
13.2.1 The Director of Finance must prepare procedural instructions on the recording of and
accounting for condemnations, losses, and special payments. Trust senior management must
comply with NHS contractual requirements in ensuring that suspected fraud, bribery or
corruption is reported and investigated by the Trust LCFS.
13.2.2 Any employee or officer discovering or suspecting a loss of any kind must either immediately
inform their head of department, who must immediately inform the Director of Finance who will
liaise with the Chief Executive or inform an officer charged with responsibility for responding to
concerns involving loss confidentially. This officer will then appropriately inform the Director of
Finance who will liaise with the Chief Executive.
Where a criminal offence is suspected, the Director of Finance must immediately inform the
police if theft or arson is involved. In cases of fraud, bribery or corruption or of anomalies
which may indicate fraud, bribery or corruption, the Director of Finance must inform their Local
Counter Fraud Specialist who will report the incident on the NHS Protect case management
database.
13.2.3 For losses apparently caused by theft, arson, neglect of duty or gross carelessness, except if
trivial the Director of Finance must immediately notify:
a) the Board of Directors, and
b) the External Auditor.
c) NHS Protect (if appropriate, through the Local Security Management Specialist)
13.2.4 Within limits delegated by the Department of Health the Board of Directors shall approve the
writing-off of all losses and special payments in accordance with the Scheme of Delegation.
13.2.5 The Director of Finance shall be authorised to take any necessary steps to safeguard the
Trust's interests in bankruptcies and company liquidations.
13.2.6 For any loss, the Director of Finance should consider whether any insurance claim can be
made.
13.2.7 The Director of Finance shall maintain a Losses and Special Payments Register in which
write-off action is recorded. All losses and special payments must be reported to the Audit
Committee.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 54 of 150
13.3 Compensation Claims
13.3.1 The Trust is committed to effective and timely investigation and response to any claim which
includes allegations of clinical negligence, employee and other compensation claims. The
Trust will follow the requirements and note the recommendations of the Department of Health,
and the NHS Litigation Authority (NHSLA) in the management of claims. Every member of
staff is expected to co-operate fully, as required, in assessment and management of each
claim.
13.3.2 The Trust will seek to reduce the incidence and adverse impact of clinical negligence,
employee and other litigation by :-
- Adopting prudent risk management strategies including continuous review.
- Implementing in full the NHS Complaints Procedure, thus providing an alternative
remedy for some potential litigants.
- Adopting a systematic approach to claims handling in line with the best current and
cost effective practice.
- Following guidance issued by the NHSLA relating to clinical negligence.
- Achieving the Care Quality Commission Fundamental Standards for Quality and
Safety.
- Implementing an effective system of Quality Governance
13.3.3 The Director of Nursing and Quality is responsible for clinical negligence: for managing the
claims process and informing the Board of Directors of any major developments on claims
related issues.
14 INFORMATION TECHNOLOGY
14.1 Responsibilities and duties of the Chief Operating Officer and Medical Director
14.1.1 The Chief Operating Officer, who is the Senior Information Risk Officer and therefore
responsible for the accuracy and security of the Trust’s data, and the Medical Director, who is
responsible for Information Technology, shall:
a) devise and implement any necessary procedures to ensure adequate (reasonable)
protection of the Trust's data, programs and computer hardware for which they is
responsible from accidental or intentional disclosure to unauthorised persons, deletion
or modification, theft or damage, having due regard for the Data Protection Act 1998
(updated 2000) and the Computer Misuse Act 1990.
b) ensure that adequate (reasonable) controls exist over data entry, processing, storage,
transmission and output to ensure security, privacy, accuracy, completeness, and
timeliness of the data, as well as the efficient and effective operation of the system;
c) ensure that adequate controls exist such that the computer operation is separated
from development, maintenance and amendment;
d) ensure that adequate controls exist to maintain the security, privacy, accuracy and
completeness of financial data sent via transmission networks.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 55 of 150

e) ensure that an adequate management (audit) trail exists through the computerised
system and that such computer audit reviews as they may consider necessary are
being carried out.
14.1.2 The Director of Finance shall satisfy themselves that new financial systems and amendments
to current financial systems are developed in a controlled manner and thoroughly tested prior
to implementation. Where this is undertaken by another organisation, assurances of
adequacy will be obtained from them prior to implementation.
14.1.3 The Chief Operating Officer shall publish and maintain a Freedom of Information (FOI)
Publication Scheme, or adopt a model Publication Scheme approved by the Information
Commissioner. A Publication Scheme is a complete guide to the information routinely
published by a public authority. It describes the classes or types of information about our
Trust that we make publicly available.
14.2 Responsibilities and duties of other Directors and Officers in relation to computer
systems of a general application
14.2.1 In the case of computer systems which are proposed General Applications all responsible
directors and employees will send to the Medical Director:
a) details of the outline design of the system;
b) in the case of packages acquired either from a commercial organisation, from the
NHS, or from another public sector organisation, the operational requirement.
14.3 Contracts for Computer Services with other health bodies or outside agencies
14.3.1 The Chief Operating Officer shall ensure that contracts for computer services with another
health organisation or any other agency shall clearly define the responsibility of all parties for
the security, privacy, accuracy, completeness, and timeliness of data during processing,
transmission and storage. The contract should also ensure rights of access for audit
purposes.
14.3.2 Where another health organisation or any other agency provides a computer service the Chief
Operating Officer shall periodically seek assurances that adequate controls are in operation.
14.4 Requirement for Computer Systems which have an impact on corporate financial
systems
14.4.1 Where computer systems have an impact on corporate financial systems the Director of
Finance shall satisfy them self that:
a) systems acquisition, development and maintenance are in line with corporate policies
such as an Information Technology Strategy;
b) data produced for use with financial systems is adequate, accurate, complete and
timely, and that a management (audit) trail exists;
c) Finance staff have access to such data; and
d) such computer audit reviews as are considered necessary are being carried out.
14.5 Risk Assessment
14.5.1 The Medical Director shall ensure that risks to the Trust arising from the use of IT are
effectively identified and considered and appropriate action taken to mitigate or control risk.
This shall include the preparation and testing of appropriate disaster recovery plans.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 56 of 150

15 PATIENTS' PROPERTY
15.1 The Trust has a responsibility to provide safe custody for money and other personal property
(hereafter referred to as "property") handed in by patients, in the possession of unconscious or
confused patients, or found in the possession of patients dying in hospital or dead on arrival.
15.2 The Chief Executive is responsible for ensuring that patients or their guardians, as
appropriate, are informed before or at admission by:
- notices and information booklets,
- hospital admission documentation and property records,
- the oral advice of administrative and nursing staff responsible for admissions,
that the Trust will not accept responsibility or liability for patients’ property brought into its
premises, unless it is handed in for safe custody and a copy of an official patient’s property
record is obtained as a receipt.
15.3 The Director of Finance must provide detailed written instructions on the collection, custody,
investment, recording, safekeeping, and disposal of patients' property (including instructions
on the disposal of the property of deceased patients and of patients transferred to other
premises) for all staff whose duty is to administer, in any way, the property of patients. The
said instructions shall cover the necessary arrangements for withdrawal of cash or
disbursement of money held in accounts of patients who are incapable of handling their own
financial affairs. Due care should be exercised in the management of a patient's money in
order to maximise the benefits to the patient.
15.4 A patient’s property record, in a form determined by the Director of Finance shall be
completed in respect of the following:
a) property handed in for safe custody by any patient (or guardian as appropriate); and
b) property taken into safe custody having been found in the possessions of:
- mentally disordered patients
- confused and/or disorientated patients
- unconscious patients
- patients dying in hospital
- patients found dead on arrival at hospital (property removed by police)
c) A record shall be completed in respect of all persons in category b, including a nil
return if no property is taken into safe custody.
15.5 The record shall be completed by a member of the hospital staff in the presence of a second
member of staff and the patient (or representative) where practicable. It shall then be signed
by both members of staff and by the patient, except where the latter is restricted by physical or
mental incapacity. Any alterations shall be validated by signature as required in the original
entry on the record.
15.6 Where Department of Health instructions require the opening of separate accounts for
patients' monies, these shall be opened and operated under arrangements agreed by the
Director of Finance.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 57 of 150

15.7 Patients’ income, including pensions and allowances, shall be dealt with in accordance with
current Department of Works and Pensions instructions. For long stay patients, the Chief
Executive shall ensure that positive action is taken to use their funds effectively and so reduce
balances accruing.
15.8 Refunds of cash handed in for safe custody will be dealt with in accordance with current
Department of Works and Pensions instructions. Property other than cash, which has been
handed in for safe custody, shall be returned to the patient as required, by the officer who has
been responsible for its security. The return shall be receipted by the patient or guardian as
appropriate and witnessed.
15.9 The disposal of property of deceased patients shall be effected by the officer who has been
responsible for its security, such disposal shall be in accordance with written instructions
issued by the Director of Finance, in particular, where cash or valuables have been deposited
for safe custody, they shall only be released after written authority has been given by the
Director of Finance. Such authority shall include details of the lawful kin or other person
entitled to the cash and valuables in question.
15.10 In all cases where property of a deceased patient is of a total value in excess of £5,000 (or
such other amount as may be prescribed by any amendment to the Administration of Estates,
Small Payments, Act 1965), the production of Probate or Letters of Administration shall be
required before any of the property is released. Where the total value of property is £5,000 or
less, forms of indemnity shall be obtained.
15.11 Property handed over for safe custody shall be placed into the care of the appropriate
administrative staff. Where there are no administrative staff present, in which case the
property shall be placed in the secure care of the most senior member of nursing staff on duty.
15.12 In respect of deceased patients, if there is no will and no lawful next of kin the property vests
in the Crown and particulars shall, therefore, be notified to the Treasury Solicitor.
15.13 Any funeral expenses necessarily borne by the Trust are a first charge on a deceased
person’s estate. Where arrangements for burial or cremation are not made privately, any
element of the estate held by the Trust may be appropriated towards funeral expenses, upon
the authorisation of the Director of Finance.
15.14 Staff should be informed, on appointment, by the appropriate departmental or senior manager
of their responsibilities and duties for the administration of the property of patients.
15.15 Where patients' property or income is received for specific purposes and held for safekeeping
the property or income shall be used only for that purpose, unless any variation is approved by
the donor or patient in writing.
16 FUNDS HELD ON TRUST
16.1 General
16.1.1 The Trust has a responsibility as a corporate trustee for the management of funds it holds on
trust. The management processes may overlap with those of the organisation of the Trust, the
trustee responsibilities must be discharged separately and full recognition given to its dual
accountabilities to the Charity Commission.
16.1.2 The reserved powers of the Board of Directors and the Scheme of Delegation make clear
where decisions where discretion must be exercised are to be taken and by whom.
16.1.3 As management processes overlap most of the sections of these Standing Financial
Instructions will apply to the management of funds held on trust.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 58 of 150

16.1.4 The over-riding principle is that the integrity of each trust must be maintained and statutory
and trust obligations met. Materiality must be assessed separately from exchequer activities
and funds.
16.1.5 Charitable Funds are those gifts, donations and endowments made under the relevant
charities legislation and held on trust for purposes relating to the Trust and the objectives of
which are for the benefit of the NHS in England. They are administered by the Board of
Directors acting as Trustees.
16.1.6 The Director of Finance shall maintain such accounts and records as may be necessary to
record and protect all transactions and funds of the Trust as trustees of non-exchequer funds,
including an Investment Register.
16.2 Existing Charitable Funds
16.2.1 The Director of Finance shall arrange for the administration of all existing funds. A “Deed of
Establishment” must exist for every fund and detailed codes of procedure shall be produced
covering every aspect of the financial management of charitable funds, for the guidance of
fund managers. The Deed of Establishment shall identify the restricted nature of certain
funds, and it is the responsibility of fund managers, within their delegated authority, and the
Charitable Funds Committee, to ensure that funds are utilised in accordance with the terms of
the Deed.
16.2.2 The Director of Finance shall periodically review the funds in existence and shall make
recommendations to the Charitable Funds Committee regarding the potential for
rationalisation of such funds within statutory guidelines.
16.2.3 The Director of Finance shall ensure that all funds are currently registered with the Charities
Commission in accordance with the Charities Act 1993 or subsequent legislation.
16.3 New Charitable Funds
16.3.1 The Director of Finance shall, recommend the creation of a new fund where funds and/or
other assets, received for charitable purposes, cannot adequately be managed as part of an
existing fund. All new funds must be covered by a Deed of Establishment and must be
formally approved by the Charitable Funds Committee.
16.3.2 The Deed of Establishment for any new fund shall clearly identify, inter alia, the objects of the
new fund, the nominated fund manager, the estimated annual income and, where applicable,
the Charitable Funds Committee’s power to assign the residue of the fund to another fund
contingent upon certain conditions e.g. discharge of original objects.
16.4 Sources of New Funds
16.4.1 All gifts accepted shall be received and held in the name of the Charity and administered in
accordance with the Charity’s policy, subject to the terms of specific funds. As the Charity can
accept gifts only for all or any purposes relating to the NHS, officers shall, in cases of doubt,
consult the Director of Finance before accepting any gift. Advice to the Board of Directors on
the financial implications of fund raising activities by outside bodies or organisations shall be
given by the Director of Finance.
16.4.2 All gifts, donations and proceeds of fund-raising activities, which are intended for the Charity’s
use, must be handed immediately to the Director of Finance via the Cash Office to be banked
directly to the Charitable Funds Bank Account.
16.4.3 In respect of Donations, the Director of Finance shall:-
a) provide guidelines to officers of the Trust as to how to proceed when offered funds.
These will include:-
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 59 of 150

i) the identification of the donor’s intentions;
ii) where possible, the avoidance of creating excessive numbers of funds;
iii) the avoidance of impossible, undesirable or administratively difficult objects;
iv) sources of immediate further advice; and
v) treatment of offers for personal gifts.
b) provide secure and appropriate receipting arrangements, which will indicate that
donations have been accepted directly into the appropriate fund and that the donor’s
intentions have been noted and accepted.
16.4.4 In respect of Legacies and Bequests, the Director of Finance shall be kept informed of and
record all enquiries regarding legacies and bequests. Where required, the Director of Finance
shall:-
a) provide advice covering any approach regarding:-
i) the wording of wills;
ii) the receipt of funds/other assets from executors;
b) after the death of a testator all correspondence concerning a legacy shall be dealt with
on behalf of the Charity by the Director of Finance who alone shall be empowered to
give an executor a good discharge.
c) where necessary, obtain grant of probate, or make application for grant of letters of
administration;
d) be empowered to negotiate arrangements regarding the administration of a Will with
executors and to discharge them from their duty; and
e) be directly responsible, in conjunction with the Charitable Funds Committee, for the
appropriate treatment of all legacies and bequests.
16.4.5 In respect of fund-raising, the final approval for major appeals will be given by the Board of
Directors. Final approval for smaller appeals will be given by the Charitable Funds
Committee. The Director of Finance shall:-
a) advise on the financial implications of any proposal for fund-raising activities;
b) deal with all arrangements for fund-raising by and/or on behalf of the Charity and
ensure compliance with all statutes and regulations;
c) be empowered to liaise with other organisations/persons raising funds for the Charity
and provide them with an adequate discharge;
d) be responsible for alerting the Charitable Funds Committee and the Board of
Directors to any irregularities regarding the use of the Charity’s name or its registration
numbers; and
e) be responsible for the appropriate treatment of all funds received from this source.
16.4.6 In respect of Trading Income (see also NHS Charitable Funds Guidance Chapter 6), the
Director of Finance shall:-
a) be primarily responsible, along with designated fund managers, for any trading
undertaken by the Charity; and
b) be primarily responsible for the appropriate treatment of all funds received from this
source.
16.4.7 In respect of Investment Income, the Director of Finance shall be responsible for the
appropriate treatment of all dividends, interest and other receipts from this source (see below).
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 60 of 150

16.5 Investment Management
16.5.1 The Charitable Funds Committee shall be responsible for all aspects of the management of
the investment of charitable funds as delegated under the terms of the approved investment
policy. The issues on which the Director of Finance shall be required to provide advice to the
Charitable Funds Committee shall include:-
a) the formulation of investment policy which meets statutory requirements (Trustee
Investment Act 1961) with regard to income generation and the enhancement of
capital value;
b) the appointment of advisers, brokers and, where appropriate, investment fund
managers and:-
i) the Director of Finance shall recommend the terms of such appointments;
and for which
ii) written agreements shall be signed by the Chief Executive;
c) pooling of investment resources and the preparation of a submission to the Charity
Commission for them to make a scheme;
d) the participation by the Charity in common investment funds and the agreement of
terms of entry and withdrawal from such funds;
e) that the use of assets shall be appropriately authorised in writing and charges raised
within policy guidelines;
f) the review of the performance of brokers and fund managers;
g) the reporting of investment performance.
16.5.2 The Director of Finance shall prepare detailed procedural instructions concerning the
receiving, recording, investment and accounting for Charitable Funds.
16.6 Expenditure from Charitable Funds
16.6.1 Expenditure from Charitable Funds shall be managed by the Charitable Funds Committee on
behalf of the Board of Directors. In so doing the committee shall be aware of the following:-
a) the objects of various funds and the designated objectives;
b) the availability of liquid funds within each trust;
c) the powers of delegation available to commit resources;
d) the avoidance of the use of exchequer funds to discharge endowment fund liabilities
(except where administratively unavoidable), and to ensure that any indebtedness to
the Exchequer shall be discharged by trust funds at the earliest possible time;
e) that funds are to be spent rather than preserved, subject to the wishes of the donor
and the needs of the Trust; and
f) the definitions of “charitable purposes” as agreed by the Department of Health with
the Charity Commission.
16.6.2 Delegated authority to incur expenditure which meets the purpose of the funds are set out in
the Scheme of Delegations; exceptions are as follows:-
a) Any staff salaries/wages costs require Charitable Funds Committee approval
b) No funds are to be “overdrawn” except in the exceptional circumstance that Charitable
Funds Committee approval is granted.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 61 of 150

16.7 Banking Services
16.7.1 The Director of Finance shall advise the Charitable Funds Committee and, with its approval,
shall ensure that appropriate banking services are available in respect of administering the
Charitable Funds. These bank accounts should permit the separate identification of liquid
funds to each trust where this is deemed necessary by the Charity Commission.
16.8 Asset Management
16.8.1 Assets in the ownership of or used by the Trust, shall be maintained along with the general
estate and inventory of assets of the Trust. The Director of Finance shall ensure:-
a) that appropriate records of all donated assets owned by the Trust are maintained, and
that all assets, at agreed valuations are brought to account;
b) that appropriate measures are taken to protect and/or to replace assets. These to
include decisions regarding insurance, inventory control, and the reporting of losses;
c) that donated assets received on trust shall be accounted for appropriately;
d) that all assets acquired from Charitable Funds which are intended to be retained
within the funds are appropriately accounted for.
16.9 Reporting
16.9.1 The Director of Finance shall ensure that regular reports are made to the Charitable Funds
Committee and Board of Directors with regard to, inter alia, the receipt of funds, investments
and expenditure.
16.9.2 The Director of Finance shall prepare annual accounts in the required manner, which shall be
submitted, to the Board of Directors within agreed timescales.
16.9.3 The Director of Finance shall prepare an annual trustees’ report and the required returns to
the Charity Commission for adoption by the Charitable Funds Committee.
16.10 Accounting and Audit
16.10.1 The Director of Finance shall maintain all financial records to enable the production of reports
as above and to the satisfaction of internal and external audit.
16.10.2 Distribution of investment income to the charitable funds and the recovery of administration
costs shall performed on a basis determined by the Director of Finance.
16.10.3 The Director of Finance shall ensure that the records, accounts and returns receive adequate
scrutiny by internal audit during the year. They will liaise with external audit and provide them
with all necessary information.
16.10.4 The Charitable Funds Committee shall be advised by the Director of Finance on the outcome
of the annual audit.
16.11 Taxation and Excise Duty
16.11.1 The Director of Finance shall ensure that the Charity’s liability to taxation and excise duty is
managed appropriately, taking full advantage of available concessions, through the
maintenance of appropriate records, the preparation and submission of the required returns
and the recovery of deductions at source.
17 TENDERING AND CONTRACT PROCEDURE
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 62 of 150

17.1 Duty to Comply
17.1.1 The procedure for making all contracts by or on behalf of the Trust shall comply with the
Standing Orders and Standing Financial Instructions (except where Suspension of Standing
Orders is applied).
17.1.2 The Trust shall comply as far as is practicable with the requirements of the Department of
Health "Capital Investment Manual" and “Estate code” in respect of capital investment and
estate and property transactions.
17.2 EU Directives Governing Public Procurement
17.2.1 Directives by the Council of the European Union promulgated by the Department of Health
(DoH) prescribing procedures for awarding all forms of contracts shall have effect as if
incorporated in the Standing Orders and Standing Financial Instructions. Procedure notes
detailing EU thresholds and the differing procedures to be adopted must be maintained within
the Trust.
17.3 Formal Competitive Tendering
17.3.1 The Trust shall ensure that competitive tenders are invited for:
the supply of goods, materials and manufactured articles and
for the rendering of services including all forms of management consultancy services
(other than specialised services sought from or provided by the Department of Health);
for the design, construction and maintenance of building and engineering works (including
construction and maintenance of grounds and gardens); and for disposals.
Where the Trust elects to invite tenders for the supply of healthcare these Standing Financial
Instructions shall apply as far as they are applicable to the tendering procedure.
17.3.2 Formal tendering procedures are not required where:
(a) the estimated expenditure or income does not, or is not reasonably expected to, exceed
the limit set in the Scheme of Reservation and Delegation, (this figure to be reviewed
annually); or
(b) the supply is proposed under special arrangements negotiated by the Department of
Health in which event the said special arrangements must be complied with; or
(c) regarding disposals as set out in Standing Financial Instruction ‘Disposals and
Condemnations’.
Formal tendering procedures may be waived in the following circumstances:
(d) in very exceptional circumstances where the Chief Executive decides that formal
tendering procedures would not be practicable or the estimated expenditure or income
would not warrant formal tendering procedures, and the circumstances are detailed in
an appropriate Trust record;
(e) where the requirement is covered by an existing contract;
(f) where a consortium arrangement is in place and a lead organisation has been
appointed to carry out tendering activity on behalf of the consortium members;
(g) where the timescale genuinely precludes competitive tendering but failure to plan the
work properly would not be regarded as a justification for a single tender;
(h) where specialist expertise is required and is available from only one source;
(i) when the task is essential to complete the project, and arises as a consequence of a
recently completed assignment and engaging different consultants for the new task
would be inappropriate;
(j) there is a clear benefit to be gained from maintaining continuity with an earlier project.
However in such cases the benefits of such continuity must outweigh any potential
financial advantage to be gained by competitive tendering;
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 63 of 150

(k) for the provision of legal advice and services providing that any legal firm or partnership
commissioned by the Trust is regulated by the Law Society for England and Wales for
the conduct of their business (or by the Bar Council for England and Wales in relation to
the obtaining of Counsel’s opinion) and are generally recognised as having sufficient
expertise in the area of work for which they are commissioned.
The Director of Finance will ensure that any fees paid are reasonable and within
commonly accepted rates for the costing of such work.
(l) where allowed and provided for in the NHS Trust Capital Accounting Manual.
The waiving of competitive tendering procedures should not be used to avoid competition
or for administrative convenience or to award further work to a consultant originally
appointed through a competitive procedure.
The Procurement Manager and Head of Technical Services can authorise waiving of
competitive procedures up to £10,000. The Director of Finance can authorise waiving of
competitive tendering procedures up to £75,000. Waiving of competitive tendering
procedures above £75,000 requires sign off by the Chief Executive and Director of
Finance.
Where it is decided that competitive tendering is not applicable and should be waived, the
fact of the waiver and the reasons should be documented and recorded in an appropriate
Trust record and reported to the Audit Committee at each meeting.
17.3.3 Fair and Adequate Competition
Where the exceptions set out in SFI Nos. 17.1 and 17.3.2 apply, the Trust shall ensure that
invitations to tender are sent to a sufficient number of firms/individuals to provide fair and
adequate competition as appropriate, and in no case less than two firms/individuals, having
regard to their capacity to supply the goods or materials or to undertake the services or works
required.
17.3.4 Building and Engineering Construction Works
Competitive Tendering cannot be waived for building and engineering construction works
and maintenance (other than in accordance with Concode) without Departmental of Health
approval.
17.3.5 Items which subsequently breach thresholds after original approval
Items estimated to be below the limits set in this Standing Financial Instruction for which
formal tendering procedures are not used which subsequently prove to have a value above
such limits shall be reported to the Chief Executive, and be recorded in an appropriate Trust
record.
17.4 Contracting/Tendering Procedure
17.4.1 Invitation to tender
(i) All invitations to tender shall state the date and time as being the latest time for the
receipt of tenders and be published via EU-Supply website and/or Contracts Finder
website.
(ii) Every tender for goods, materials, services or disposals shall embody such of the
NHS Standard Contract Conditions as are applicable.
(iii) Every tender for building or engineering works (except for maintenance work, when
Estmancode guidance shall be followed) shall embody or be in the terms of the
current edition of one of the Joint Contracts Tribunal Standard Forms of Building
Contract or Department of the Environment (GC/Wks) Standard forms of contract
amended to comply with concode; or, when the content of the work is primarily
engineering, the General Conditions of Contract recommended by the Institution of
Mechanical and Electrical Engineers and the Association of Consulting Engineers
(Form A), or (in the case of civil engineering work) the General Conditions of Contract
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 64 of 150

recommended by the Institute of Civil Engineers, the Association of Consulting
Engineers and the Federation of Civil Engineering Contractors. These documents
shall be modified and/or amplified to accord with Department of Health guidance and,
in minor respects, to cover special features of individual projects.
17.4.2 E-tendering solutions
The Trust obtains support from the North of England Commercial Procurement
Collaborative.
17.4.3 Expressions of Interest/Invitations to Tender:
Expressions of interest shall be invited via the OJEU website, the national advertising portal
services for healthcare services.
Invitations to tender shall be sent out electronically via EU-supply. Evidence of the invitation
process and a full audit trail will be held electronically by EU-supply.
17.4.4 Receipt of tenders/tender opening:
EU-supply is a secure website which ensures that tenders are held in safekeeping before
being opened. Access is restricted to the Trust Procurement Manager and Deputy
Procurement Manager. An audit trail is automatically generated which includes date and
time of receipt.
17.4.5 Admissibility
i) If for any reason the designated officers are of the opinion that the tenders received
are not strictly competitive (for example, because their numbers are insufficient or any
are amended, incomplete or qualified) no contract shall be awarded without the
approval of the Chief Executive.
(ii) Where only one tender is sought and/or received, the Chief Executive and Director of
Finance shall, as far practicable, ensure that the price to be paid is fair and
reasonable and will ensure value for money for the Trust.
17.4.6 Acceptance of formal tenders
(i) Any discussions with a tenderer which are deemed necessary to clarify technical
aspects of their tender before the award of a contract will not disqualify the tender. All
clarification questions received and responses given must be recorded.
(ii) The lowest tender, if payment is to be made by the Trust, or the highest, if payment is
to be received by the Trust, shall be accepted unless there are good and sufficient
reasons to the contrary. Such reasons shall be set out in either the contract file, or
other appropriate record.
It is accepted that for professional services such as management consultancy, the
lowest price does not always represent the best value for money. Other factors
affecting the success of a project include:
(a) experience and qualifications of team members;
(b) understanding of client’s needs;
(c) feasibility and credibility of proposed approach;
(d) ability to complete the project on time.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 65 of 150

Where other factors are taken into account in selecting a tenderer, these must be
clearly recorded and documented in the contract file, and the reason(s) for not
accepting the lowest tender clearly stated.
(iii) No tender shall be accepted which will commit expenditure in excess of that which
has been allocated by the Trust and which is not in accordance with these Instructions
except with the authorisation of the Chief Executive.
(iv) The use of these procedures must demonstrate that the award of the contract was:
(a) not in excess of the going market rate / price current at the time the contract was
awarded;
(b) that best value for money was achieved.
(v) All tenders should be treated as confidential and should be retained for inspection.
17.4.7 Tender reports to the Board of Directors
Reports to the Board of Directors will be made on an exceptional circumstance basis only.
17.4.8 List of approved firms (see SFI No. 17.3.4)
(a) Responsibility for maintaining list
A manager nominated by the Chief Executive shall on behalf of the Trust maintain
lists of approved firms from who tenders and quotations may be invited. These shall
be kept under frequent review. The lists shall include all firms who have applied for
permission to tender and as to whose technical and financial competence the Trust is
satisfied. All suppliers must be made aware of the Trust’s terms and conditions of
contract.
(b) Building and Engineering Construction Works
(i) Invitations to tender shall be made only to firms included on the approved list of
tenderers compiled in accordance with this Instruction or on the separate
maintenance lists compiled in accordance with Estmancode guidance (Health Notice
HN(78)147).
ii) Firms included on the approved list of tenderers shall ensure that when engaging,
training, promoting or dismissing employees or in any conditions of employment,
shall not discriminate against any person because of colour, race, ethnic or national
origins, religion or sex, and will comply with the provisions of the Equal Pay Act
1970, the Sex Discrimination Act 1975, the Race Relations Act 1976, and the
Disabled Persons (Employment) Act 1944 and any amending and/or related
legislation.
iii) Firms shall conform at least with the requirements of the Health and Safety at
Work Act and any amending and/or other related legislation concerned with the
health, safety and welfare of workers and other persons, and to any relevant British
Standard Code of Practice issued by the British Standard Institution. Firms must
provide to the appropriate manager a copy of its safety policy and evidence of the
safety of plant and equipment, when requested.
(c) Financial Standing and Technical Competence of Contractors
The Director of Finance may make or institute any enquiries they deems appropriate
concerning the financial standing and financial suitability of approved contractors.
The Director with lead responsibility for clinical governance will similarly make such
enquiries as is felt appropriate to be satisfied as to their technical / medical
competence.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 66 of 150

17.4.9 Exceptions to using approved contractors
If in the opinion of the Chief Executive and the Director of Finance or the Director with lead
responsibility for clinical governance it is impractical to use a potential contractor from the list of
approved firms/individuals (for example where specialist services or skills are required and
there are insufficient suitable potential contractors on the list), or where a list for whatever
reason has not been prepared, the Chief Executive should ensure that appropriate checks are
carried out as to the technical and financial capability of those firms that are invited to tender or
quote.
An appropriate record in the contract file should be made of the reasons for inviting a tender
or quote other than from an approved list.
17.5 Quotations: Competitive and non-competitive
17.5.1 General Position on quotations
Quotations are required where formal tendering procedures are not adopted and where the
intended expenditure or income exceeds, or is reasonably expected to exceed the sum
defined In the Scheme of Reservation and Delegation.
17.5.2 Competitive Quotations
(i) Quotations should be obtained from at least 3 firms/individuals based on specifications
or terms of reference prepared by, or on behalf of, the Trust.
(ii) Quotations should be in writing unless the Chief Executive or their nominated officer
determines that it is impractical to do so in which case quotations may be obtained by
telephone. Confirmation of telephone quotations should be obtained as soon as possible
and the reasons why the telephone quotation was obtained should be set out in a
permanent record.
(iii) All quotations should be treated as confidential and should be retained for inspection.
(iv) The Chief Executive or their nominated officer should evaluate the quotation and select
the quote which gives the best value for money. If this is not the lowest quotation if
payment is to be made by the Trust, or the highest if payment is to be received by the
Trust, then the choice made and the reasons why should be recorded in a permanent
record.
17.5.3 Non-Competitive Quotations
Non-competitive quotations in writing may be obtained in the following circumstances:
(i) the supply of proprietary or other goods of a special character and the rendering of
services of a special character, for which it is not, in the opinion of the responsible
officer, possible or desirable to obtain competitive quotations;
(ii) the supply of goods or manufactured articles of any kind which are required quickly
and are not obtainable under existing contracts;
(iii) miscellaneous services, supplies and disposals;
(iv) where the goods or services are for building and engineering maintenance the
responsible works manager must certify that the first two conditions of this SFI (i.e.: (i)
and (ii) of this SFI) apply.
17.5.4 Quotations to be within Financial Limits
No quotation shall be accepted which will commit expenditure in excess of that which has
been allocated by the Trust and which is not in accordance with Standing Financial
Instructions except with the authorisation of either the Chief Executive or Director of Finance.
17.6 Authorisation of Tenders and Competitive Quotations
Providing all the conditions and circumstances set out in these Standing Financial
Instructions have been fully complied with, formal authorisation and awarding of a contract
may be decided by the staff as defined in the Scheme of Reservation and Delegation.
These levels of authorisation may be varied or changed. Formal authorisation must be put
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 67 of 150

in writing. In the case of authorisation by the Board of Directors this shall be recorded in
their minutes.
17.7 Instances where formal competitive tendering or competitive quotation is not
required
Where competitive tendering or a competitive quotation is not required the Trust should
adopt one of the following alternatives:
(a) the Trust shall use the NHS Supply Chain, North of England Commercial
Procurement Collaborative or Crown Commercial Services for procurement of all
goods and services unless the Chief Executive or nominated officers deem it
inappropriate. The decision to use alternative sources must be documented.
(b) If the Trust does not use the NHS Supply Chain, North of England Commercial
Procurement Collaborative or Crown Commercial Services - where tenders or
quotations are not required, because expenditure is below the levels defined in the
Scheme of Reservation and Delegation, the Trust shall procure goods and services in
accordance with procurement procedures approved by the Director of Finance.
17.8 Private Finance for capital procurement
The Trust should normally market-test for PFI (Private Finance Initiative funding) when
considering a capital procurement. When the Board proposes, or is required, to use finance
provided by the private sector the following should apply:
(a) The Chief Executive shall demonstrate that the use of private finance
represents value for money and genuinely transfers risk to the private sector.
(b) Where the sum exceeds delegated limits, a business case must be referred
to the appropriate Department of Health for approval or treated as per current
guidelines.
(c) The proposal must be specifically agreed by the Board of the Trust.
(d) The selection of a contractor/finance company must be on the basis of
competitive tendering or quotations.
17.9 Compliance requirements for all contracts
The Board may only enter into contracts on behalf of the Trust within the statutory powers
delegated to it by the Secretary of State and shall comply with:
(a) The Trust’s Standing Orders and Standing Financial Instructions;
(b) EU Directives and other statutory provisions;
(c) any relevant directions including the NHS Trust Capital Accounting Manual,
Estatecode and guidance on the Procurement and Management of
Consultants;
(d) NHS Standards of Business Conduct
(e) such of the NHS Standard Contract Conditions as are applicable.
(f) contracts with Trusts must be in a form compliant with appropriate NHS
guidance.
(g) Where appropriate contracts shall be in or embody the same terms and
conditions of contract as was the basis on which tenders or quotations were
invited.
(h) In all contracts made by the Trust, the Board shall endeavour to obtain best
value for money by use of all systems in place. The Chief Executive shall
nominate an officer who shall oversee and manage each contract on behalf of
the Trust.
17.10 Personnel and Agency or Temporary Staff Contracts
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 68 of 150
The Chief Executive shall nominate officers with delegated authority to enter into contracts of
employment, regarding staff, agency staff or temporary staff service contracts.
17.11 Healthcare Services Agreements
Service agreements with NHS providers for the supply of healthcare services shall be drawn
up in accordance with the NHS and Community Care Act 1990 and administered by a trust.
Such service agreements are not contracts in law and therefore not enforceable by the
courts. However, a contract with a Foundation Trust, being a Public Benefits Corporation, is
a legal document and is enforceable in law.
The Chief Executive shall nominate officers to commission service agreements with
providers of healthcare in line with a commissioning plan approved by the Board of Directors
(refer to Scheme of Reservation and Delegation).
17.12 Disposals
Competitive Tendering or Quotation procedures shall not apply to the disposal of:
(a) any matter in respect of which a fair price can be obtained only by negotiation
or sale by auction as determined (or pre-determined in a reserve) by the Chief
Executive or their nominated officer;
(b) obsolete or condemned articles and stores, which may be disposed of in
accordance with the supplies policy of the Trust;
(c) items to be disposed of with an estimated sale value of less than that defined
on the Scheme of Delegation, this figure to be reviewed on a periodic basis;
(d) items arising from works of construction, demolition or site clearance, which
should be dealt with in accordance with the relevant contract;
(e) land or buildings concerning which DH guidance has been issued but subject
to compliance with such guidance.
17.13 In-house Services
17.13.1 The Chief Executive shall be responsible for ensuring that best value for money can be
demonstrated for all services provided on an in-house basis. The Trust may also determine
from time to time that in-house services should be market tested by competitive tendering.
17.13.2 In all cases where the Board of Directors determines that in-house services should be
subject to competitive tendering the following groups shall be set up:
(a) Specification group, comprising the Chief Executive or nominated officer/s and
specialist.
(b) In-house tender group, comprising a nominee of the Chief Executive and
technical support.
(c) Evaluation team, comprising normally a specialist officer, a supplies officer and
a Director of Finance representative.
17.13.3 All groups should work independently of each other and individual officers may be a member
of more than one group but no member of the in-house tender group may participate in the
evaluation of tenders.
17.13.4 The evaluation team shall make recommendations to the Board of Directors.
17.13.5 The Chief Executive shall nominate an officer to oversee and manage the contract on behalf
of the Trust.
17.14 Applicability of SFIs on Tendering and Contracting to funds held in trust
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 69 of 150
These Instructions shall not only apply to expenditure from Exchequer funds but also to works,
services and goods purchased from the Trust’s trust funds and private resources.
18. ACCEPTANCE OF GIFTS AND HOSPITALITY BY STAFF
18.1 The Director of Finance shall ensure that all staff are made aware of the Trust policy on
acceptance of gifts and other benefits in kind by staff. This policy should follow the guidance
contained in the Department of Health Standards of Business Conduct for NHS Staff and is
also deemed to be an integral part of the Standing Orders and Standing Financial Instructions.
19 DECLARATIONS OF INTEREST BY STAFF
19.1 The Director of Finance shall ensure that all staff are made aware of the Trust policy on the
declarations of interest. This policy should follow the guidance contained in the Department of
Health Standards of Business Conduct for NHS Staff and is also deemed to be an integral part
of the Standing Orders and Standing Financial Instructions.
20 RETENTION OF DOCUMENTS
20.1 Context
All NHS records are public records under the terms of the Public Records Act 1958 section 3
(1) – (2). The Secretary of State for Health and all NHS organisations have a duty under this
Act to make arrangements for the safe keeping and eventual disposal of all types of records.
In addition, the requirements of the Data Protection Act 1998 and the Freedom of Information
Act 2000 must be achieved.
20.2 Accountability
The Chief Executive and senior managers are personally accountable for records
management within the organisation. Additionally, the organisation is required to take positive
ownership of, and responsibility for, the records legacy of predecessor organisations and/or
obsolete services. Under the Public Records Act all NHS employees are responsibility for any
records that they create or use in the course of their duties. Thus any records created by an
employee of the NHS are public records and may be subject to both legal and professional
obligations.
The Chief Executive shall be responsible for maintaining archives for all documents required
to be retained under the direction contained in Department of Health guidance, ‘Records
Management Code of Practice’.
20.3 Types of Record Covered by The Code of Practice
The guidelines apply to NHS records of all types (including records of NHS patients treated on
behalf of the NHS in the private healthcare sector) regardless of the media on which they are
held:
Patient health records (electronic or paper based)
Records of private patients seen on NHS premises;
Accident and emergency, birth and all other registers;
Theatre registers and minor operations (and other related) registers;
Administrative records (including e.g. personnel, estates, financial and accounting
records, notes associated with complaint-handling);
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 70 of 150
X-ray and imaging reports, output and other images;
Photographs, slides and other images;
Microform (i.e. fiche / film)
Audio and video tapes, cassettes, CD-ROM etc.
Emails;
Computerised records;
Scanned records;
Text messages (both out-going from the NHS and in-coming responses from the patient)
20.4 The documents held in archives shall be capable of retrieval by authorised persons.
20.5 Documents held in accordance with the Records Management Code of Practice shall only be
destroyed at the express instigation of the Chief Executive, records shall be maintained of
documents so destroyed.
21 RISK MANAGEMENT
21.1 Programme of Risk Management
The Chief Executive shall ensure that the Trust has a programme of risk management, in
accordance with current Department of Health assurance framework requirements, which
must be approved and monitored by the Board of Directors.
The programme of risk management shall include:
a) a process for identifying and quantifying risks and potential liabilities;
b) engendering among all levels of staff a positive attitude towards the control of risk;
c) management processes to ensure all significant risks and potential liabilities are
addressed including effective systems of internal control, cost effective insurance
cover, and decisions on the acceptable level of retained risk;
d) contingency plans to offset the impact of adverse events;
e) audit arrangements including; Internal Audit, clinical audit, health and safety review;
f) a clear indication of which risks shall be insured;
g) arrangements to review the Risk Management programme.
The existence, integration and evaluation of the above elements will assist in providing a
basis to make an Annual Governance Statement within the Annual Report and Accounts as
required by current Department of Health guidance.
21.2 Insurance: Risk Pooling Schemes administered by NHSLA
The Board shall decide if the Trust will insure through the risk pooling schemes administered
by the NHS Litigation Authority or self insure for some or all of the risks covered by the risk
pooling schemes. If the Board decides not to use the risk pooling schemes for any of the risk
areas (clinical, property and employers/third party liability) covered by the scheme this
decision shall be reviewed annually.
21.3 Insurance arrangements with commercial insurers
21.3.1 There is a general prohibition on entering into insurance arrangements with commercial
insurers. There are, however, three exceptions when Trust’s may enter into insurance
arrangements with commercial insurers. The exceptions are:
(1) Trust’s may enter commercial arrangements for insuring motor vehicles owned by the
Trust including insuring third party liability arising from their use;
(2) where the Trust is involved with a consortium in a Private Finance Initiative contract
and the other consortium members require that commercial insurance arrangements
are entered into; and
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 71 of 150

(3) where income generation activities take place. Income generation activities should
normally be insured against all risks using commercial insurance. If the income
generation activity is also an activity normally carried out by the Trust for a NHS purpose
the activity may be covered in the risk pool. Confirmation of coverage in the risk pool
must be obtained from the Litigation Authority. In any case of doubt concerning a Trust’s
powers to enter into commercial insurance arrangements the Director of Finance should
consult the Department of Health.
21.3.2 Arrangements to be followed by the Board of Directors in agreeing Insurance cover
(1) Where the Board decides to use the risk pooling schemes administered by the NHS
Litigation Authority the Director of Finance shall ensure that the arrangements entered
into are appropriate and complementary to the risk management programme. The
Director of Finance shall ensure that documented procedures cover these
arrangements.
(2) Where the Board decides not to use the risk pooling schemes administered by the NHS
Litigation Authority for one or other of the risks covered by the schemes, the Director of
Finance shall ensure that the Board is informed of the nature and extent of the risks that
are self insured as a result of this decision. The Director of Finance will draw up formal
documented procedures for the management of any claims arising from third parties
and payments in respect of losses which will not be reimbursed.
(3) All the risk pooling schemes require Scheme members to make some contribution to
the settlement of claims (the ‘deductible’). The Director of Finance should ensure
documented procedures also cover the management of claims and payments below the
deductible in each case.
Sta
ndin
g F
inan
cial
Inst
ruct
ions
Page 72 of 150

SCHEME OF
RESERVATION
AND DELEGATION
Southport & Ormskirk Hospital NHS Trust
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 73 of 150

Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 74 of 150

CONTENTS
SECTION
RECORD OF AMENDMENTS
SCHEDULE OF DELEGATED MATTERS 1
INTRODUCTION 2
RESERVATION OF POWERS TO THE BOARD OF DIRECTORS 3
DELEGATION OF POWERS 4
DELEGATED MATTERS Table A
DELEGATED FINANCIAL LIMITS Table B
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 75 of 150
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 76 of 150

RECORD OF AMENDMENTS
NO SECTION DATE
1 Updated document Issued for implementation July 2007
2 Document Reviewed November 2008
3 Document Reviewed May 2009
4 Document Reviewed May 2010
5 Document Reviewed August 2011
6 Document Reviewed May 2013
7 Document Reviewed May 2014
8 Document Reviewed July 2015
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 77 of 150

Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 78 of 150

1. SCHEDULE OF DELEGATED MATTERS
DELEGATED MATTERS
Delegated Matter
STANDING ORDERS/STANDING FINANCIAL INSTRUCTIONS
TABLE A
Delegated Matter Reference
No.
AUDIT ARRANGEMENTS 20
AUTHORISATION OF CLINICAL TRIALS 34
AUTHORISATION OF NEW DRUGS 32
BANK/GBS ACCOUNTS (EXCLUDING CHARITABLE FUND ACCOUNTS)
CAPITAL EXPENDITURE 8
CLINICAL AUDIT
COMMERCIAL SPONSORSHIP
COMPLAINTS (PATIENTS & RELATIVES)
CONFIDENTIAL INFORMATION 31
DATA PROTECTION ACT 29
DECLARATION OF INTERESTS 28
DISPOSAL AND CONDEMNATIONS 16
ENVIRONMENTAL REGULATIONS
EXTERNAL BORROWING 5
FINANCIAL PLANNING/BUDGETARY RESPONSIBILITY 3
FINANCIAL PROCEDURES 19
FIRE PRECAUTIONS
FIXED ASSETS 10
FRAUD, BRIBERY AND CORRUPTION
FUNDS HELD ON TRUST 13
HEALTH & SAFETY 37
HOSPITALITY/ GIFTS (ACCEPTANCE OF) 27
INFECTIOUS DISEASES & NOTIFIABLE OUTBREAKS 35
IM&T
LEGAL PROCEEDINGS 21
LOSSES, WRITE-OFFS & COMPENSATION 17
MEETINGS
MEDICAL
NON PAY EXPENDITURE 6
NURSING
PATIENTS SERVICES AGREEMENTS 14
PATIENTS’ PROPERTY
PERSONNEL & PAY 11
QUOTATIONS, TENDERING & CONTRACT PROCEDURES 9
RECORDS 30
REPORTING INCIDENTS TO THE POLICE 18
RISK MANAGEMENT
SEAL 26
SECURITY MANAGEMENT
SETTING OF FEES & CHARGES 15
MATERIALS MANAGEMENT AND RECEIPT & DISTRIBUTION OF GOODS 7
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 79 of 150

TABLE B - DELEGATED FINANCIAL LIMITS
Delegated Limit Reference
No. Charitable Funds 1
Losses and Special Payments 2
Petty Cash Disbursements 3
Requisitioning Goods And Services And Approving
Payments
4
Agency Staff 4.1
Revenue Requisitions (including call off requisitions) 4.2
Maintenance contract requisitions 4.3
Capital Requisitions 4.4
Purchase order approval 4.5
Non Purchase order invoice approval 4.6
Removal Expenses 4.7
Quotations and Tenders 5
Virement 6
2 INTRODUCTION 2.1. Reservation of Powers
SO 5.1 of the Standing Orders provides that "subject to such directions as may be given by the Secretary of State, the Trust Board may make arrangements for the exercise, on behalf of the Trust, of any of its functions by a committee or sub-committee or by the Chair or a director or by an officer of the Trust, in each case subject to such restrictions and conditions as the Board thinks fit". The Code of Accountability also requires that there should be a formal schedule of matters specifically reserved to the Trust Board. The purpose of this document is to detail how the powers are reserved to the Board of Directors, while at the same time delegating to the appropriate level the detailed application of Trust policies and procedures. However, the Board of Directors remains accountable for all of its functions, even those delegated to committees, sub committees, individual directors or officers and would therefore expect to receive information about the exercise of delegated functions to enable it to maintain a monitoring role.
2.2. Role of the Chief Executive
All powers of the Trust which have not been retained as reserved by the Board of Directors or delegated to an executive committee or sub-committee shall be exercised on behalf of the Board of Directors by the Chief Executive. All powers delegated by the Chief Executive can be re-assumed by them should the need arise. As Accountable Officer the Chief Executive is accountable to the Department of Health for the funds devolved to the Trust.
2.3 Caution over the Use of Delegated Powers
Powers are delegated to directors and officers on the understanding that they would not exercise delegated powers in a manner which in their judgement was likely to be a cause for public concern.
2.4 Absence of Directors or Officer to Whom Powers have been Delegated
In the absence of a director or officer to whom powers have been delegated those powers shall
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 80 of 150
be exercised by that director or officer's superior unless alternative arrangements have been approved by the Board of Directors. If the Chief Executive is absent powers delegated to them may be exercised by the nominated officer acting in their absence usually the Deputy Chief Executive/Director of Finance.
If it becomes clear to the Board of Directors that the Accountable Officer is incapacitated and will be unable to discharge their responsibilities over a period of four weeks or more, the Board of Directors should appoint an acting Accountable Officer, usually the Deputy Chief Executive/Director of Finance, pending the Accountable Officers return. The same applies if, exceptionally, the Accountable Officer plans an absence of more that four weeks during which they cannot be contacted.
3. RESERVATION OF POWERS TO THE BOARD OF DIRECTORS
3.1 Accountability
The NHS Code of Conduct and Code of Accountability which have been adopted by the Trust requires the Board of Directors to determine those matters on which decisions are reserved unto itself. Board members share corporate responsibility for all decisions of the Board. These reserved matters are set out in paragraphs 3.3 to 3.10 below.
Decisions reserved to the board generally represent matters for which it is held accountable to the Secretary of State, while at the same time delegating to the appropriate level the detailed application of Trust policies and procedures. However, the Board remains accountable for all of its functions, even those delegated to individual committees, sub-committees, directors or officers and would therefore expect to receive information about the exercise of delegated functions to enable it is maintain a monitoring role.
3.2 Duties
It is the Board’s duty to: act within statutory financial and other constraints; be clear what decisions and information are appropriate to the Board of Directors and
draw up Standing Orders, a schedule of decisions reserved to the Board and Standing Financial Instructions to reflect these,
ensure that management arrangements are in place to enable responsibility to be clearly delegated to senior executives for the main programmes of action and for performance against programmes to be monitored and senior executives held to account;
establish performance and quality measures that maintain the effective use of resources and provide value for money;
specify its requirements in organising and presenting financial and other information succinctly and efficiently to ensure the Board can fully undertake its responsibilities;
establish Audit and Remuneration Committees on the basis of formally agreed terms of reference that set out the membership of the committee, the limit to their powers, and the arrangements for reporting back to the main Board.
3.3 General Enabling Provision
The Board of Directors may determine any matter, for which it has authority, it wishes in full session within its statutory powers.
3.4 Regulations and Control
Approval of Standing Orders (SOs), a schedule of matters reserved to the Board of Directors and Standing Financial Instructions for the regulation of its proceedings and business.
Suspend Standing Orders.
Vary or amend the Standing Orders.
Ratification of any urgent decisions taken by the Chair and Chief Executive in public session in accordance with the Standing Orders.
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 81 of 150
Approval of a scheme of delegation of powers from the Board of Directors to Committees.
Requiring and receiving the declaration of Board members’ interests which may conflict with those of the Trust and determining the extent to which that director may remain involved with the matter under consideration.
Requiring and receiving the declaration of officers’ interests which may conflict with those of the Trust.
Approval of arrangements for dealing with complaints.
Adoption of the organisational structures, processes and procedures to facilitate the discharge of business by the Trust and to agree modifications thereto.
To receive reports from committees including those which the Trust is required by legislation or regulation to establish and to take appropriate action thereon.
To confirm the recommendations of the Trust's committees where the committees do not have executive powers.
Approval of arrangements relating to the discharge of the Trust's responsibilities as a corporate trustee for funds held on trust.
To establish terms of reference and reporting arrangements of all committees and sub-committees that are established by the Board of Directors.
Approval of arrangements relating to the discharge of the Trust's responsibilities as a bailer for patients' property.
Authorise use of the seal.
Ratify or otherwise instances of failure to comply with Standing Orders brought to the Chief Executive’s attention in accordance with Standing Orders.
Disciplining Board members’ or employees who are in breach of Statutory Requirements or Standing Orders.
Approval of the Trust’s Major Incident Plan.
3.5 Appointments / Dismissal
Appoint the Vice Chair of the Board of Directors.
Appoint the Senior Independent Director.
The appointment and dismissal of committees (and individual members) that are directly accountable to the Board of Directors.
The disciplining and dismissal of Executive Directors and disciplinary procedures of the Trust.
Confirm the appointment of members of any committee of the Trust or the appointment of representatives on outside bodies.
3.6 Policy Determination
The approval of Trust management policies including: Human Resources policies incorporating the arrangements for the appointment, removal
and remuneration of staff.
Ensure proper and widely publicised procedures for voicing complaints, concerns about misadministration, breaches of Code of Conduct, and other ethical concerns.
Approve a list of employees authorised to make short term borrowings on behalf of the Trust.
3.7 Strategy and Business Plans and Budgets
Definition of the strategic aims and objectives of the Trust.
Approve proposals for ensuring quality and developing clinical governance in services
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 82 of 150

provided by the Trust, having regard to any guidance issued by the Secretary of State.
Approval and monitoring of the Trust's strategy for the management of risk.
Approval annually of plans in respect of the application of available financial resources.
Overall approval of programmes of investment to guide the letting of contracts for the supply of clinical services.
Approve Outline and Final Business Cases for Capital Investment.
Approve budgets.
Approve annually Trust’s proposed business plan
Ratify proposals for acquisition, disposal or change of use of land and/or buildings
Approve PFI proposals.
Approve proposals on individual contracts, including purchase orders (other than NHS contracts) of a capital or revenue nature amounting to, or likely to amount to over £500,000 per annum or £1,500,000 in total if the period of the contract is longer than 3 years.
Approve proposals in individual cases for the write off of losses or making of special payments above the limits of delegation to the Chief Executive and Director of Finance.
Approve proposals for action on litigation against or on behalf of the Trust where the likely financial impact is expected to exceed £10,000 or contentious or novel or likely to lead to extreme adverse publicity, excluding claims covered by the NHS risk pooling schemes.
Review use of NHS risk pooling schemes.
Approve the opening of bank accounts.
Approve individual compensation payments.
3.8 Audit Arrangements
To approve audit arrangements (including arrangements for separate audit funds held on trust) and receive reports of the Audit Committee meetings and take appropriate action:
Receive the annual management letter received from the external auditor and agreement of proposed action, taking account of the advice, where appropriate, of the Audit Committee.
Receive an annual report from the Internal Auditor and agree action on recommendations where appropriate of the Audit Committee.
3.9 Annual Report and Accounts
Receipt and approval of the Trust’s Annual Report and Annual Accounts.
Receipt and approval of the Annual Report and Annual Accounts for funds held on Trust.
3.10 Monitoring
Receive such reports as the Board sees fit from Committees in respect of their exercise of
powers delegated.
Continue appraisal of the affairs of the Trust by means of the provision to the Board as the Board may require from Directors, Committees and officers of the Trust as set out in management policy statements. All monitoring returns required by the Department of Health and the Charity Commission shall be reported, at least in summary, to the Board.
Receive reports from the Director of Finance on financial performance against budgets
and the Annual Business Plan. Receive reports from the Chief Executive on actual and forecast income from SLA.
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 83 of 150
4 DELEGATION OF POWERS
4.1 Delegation to Committees The Board of Directors may determine that certain of its powers shall be exercised by Standing
Committees. The composition and terms of reference of such committees shall be that determined by the Board of Directors from time to time taking into account where necessary the requirements of the Secretary of State and/or the Charity Commissioners (including the need to appoint an Audit Committee and a Remuneration and Terms of Service Committee). The Board of Directors shall determine the reporting requirements in respect of these committees. In accordance with SO 6.1 committees may not delegate executive powers to sub-committees unless expressly authorised by the Board of Directors.
4.2 Delegation to Officers 4.2.1 Standing Orders and Standing Financial Instructions set out in some detail the financial
responsibilities of the Chief Executive, the Director of Finance and other directors. 4.2.2 The following responsibilities are defined through the Accountable Officer Memorandum for
Chief Executives of NHS Trusts:
The Accountable Officer has responsibility for ensuring that the Trust carries out its’ functions in a way that ensures proper stewardship of public money and assets. The specific personal responsibilities of a Trust Accountable Officer: The propriety and regularity of the public finances for which they are answerable; The keeping of proper accounts; Prudent and economical administration The avoidance of waste and extravagance; and The efficient and effective use of all the resources in their charge.
Accountable Officers must make sure that their arrangements for delegation promote good management and that they are supported by the necessary staff with an appropriate balance of skills. Arrangements for internal audit should accord with the objectives, standards and practices set out in the NHS Internal Audit Standards.
4.2.3 Schedule of Delegation Delegated matters in respect of decisions which may have a far reaching effect must be reported
to the Chief Executive. The ‘Delegated to’ authority is in accordance with the: Standing Orders
and Standing Financial Instructions. The ‘Operational Responsibility’ shown below is the lowest level to which authority is delegated.
Table A - Delegated Authority, Table B - Delegated Financial Limits, Delegation to lower levels is only permitted with written approval of the Chief Executive who will,
before authorising such delegation, consult with other Senior Managers as appropriate. All items concerning Finance must be carried out in accordance with Standing Financial Instructions and Standing Orders.
Delegated Authority
DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
1. Standing Orders/Standing Financial Instructions
a) Final authority in interpretation of Standing Orders
Chair Chair
b) Notifying Directors and employees of their responsibilities within the Standing Orders and Standing Financial Instructions and
Chief Executive Executive Director/Head of Department
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 84 of 150

DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
ensuring that they understand the responsibilities
c) Responsibility for security of the Trust’s property, avoiding loss, exercising economy and efficiency in using resources and conforming with Standing Orders, Financial instructions and financial procedures
Chief Executive All Directors and Employees
d) Suspension of Standing Orders Board of Directors Board of Directors
e) Review suspension of Standing Orders Audit Committee Audit Committee
f) Variation or amendment to Standing Orders Board of Directors Board of Directors
g) Emergency powers relating to the authorities retained by the Board of Directors.
Chair and Chief Executive with two non-executives
Chair and Chief Executive with two non-executives
h) Disclosure of non-compliance with Standing Orders to the Chief Executive (report to the Board of Directors).
All staff All staff
i) Disclosure of non-compliance with SFIs to the Director of Finance (report to the Audit Committee)
All staff All staff
j) Advice on interpretation or application of SFIs and this Scheme of Delegation
Director of Finance/Company Secretary
Director of Finance/Company Secretary/Internal Audit
Table A - Delegated Matters
DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
1. Audit Arrangements
a) Ensure an adequate internal and external audit services, for which they are accountable, is provided (and involve the Audit Committee in the selection process when / if an audit service provider is changed.)
Director of Finance Director of Finance
b) Review, appraise and report in accordance with NHS Internal Audit Standards and best practice.
Audit Committee Head of Internal Audit
c) Provide an independent and objective view on internal control and probity.
Audit Committee Internal Audit / External Audit
d) Ensure cost-effective audit service. Audit Committee Director of Finance
e) Implement recommendations Chief Executive Relevant Officers
2. Authorisation of Clinical Trials &
Research Projects
Chief Executive Medical Director
3. Authorisation of New Drugs Chief Executive Drugs and Therapeutics Committee
4. Bank/GBS Accounts/Cash (Excluding Charitable Fund (Funds Held on Trust) Accounts)
a) Operation:
Managing banking arrangements and operation of bank accounts (Board of Directors approves arrangements)
Director of Finance
Assistant Director of Finance
Opening bank accounts Director of Finance Director of Finance
Authorisation of transfers between Trust bank accounts
Director of Finance To be completed in accordance with bank mandate/internal procedures
Approve and apply arrangements for the electronic transfer of funds
Director of Finance To be completed in accordance with bank mandate/internal procedures
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 85 of 150

DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
Authorisation of:
- RFT payment runs - BACS payment runs - Cheque payments
- Manual cheques
Director of Finance
To be completed in accordance with bank mandate/internal procedures
b) Investments:
Investment of surplus funds in accordance with the Trusts investment policy
Preparation of an investment procedures
Director of Finance
Deputy Director of Finance
c) Petty Cash Director of Finance Refer To Table B Delegated Limits
5. Capital Expenditure
a) Programme:
Ensure that there is adequate appraisal and approval process for determining capital expenditure priorities and the effect that each has on business plans / Service development Strategy
Chief Executive
Director of Finance
Preparation of Capital Investment Programme
Chief Executive Director of Finance
Preparation of a business case Chief Executive Director of Finance
Financial monitoring and reporting on all capital scheme expenditure including variations to contract
Director of Finance
Director of Finance
Authorisation of capital requisitions Director of Finance Refer to Table B Delegated Limits
Assessing the requirements for the operation of the construction industry taxation deduction scheme.
Director of Finance
Assistant Director of Finance
Responsible for the management of capital schemes and for ensuring that they are delivered on time and within cost.
Chief Executive
Director of Finance
Ensure that capital investment is not undertaken without availability of resources to finance all revenue consequences.
Chief Executive
Director of Finance
Issue procedures to support:
o capital investment o Staged payments
Chief Executive Director of Finance
Issue procedures governing financial management, including variation to contract, of capital investment projects and valuation for accounting purposes.
Director of Finance
Deputy Director of Finance
Issuing the capital scheme project manager with specific authority to commit capital, proceed / accept tenders in accordance with the SO’s and SFI’s
Medical equipment purchases from the overall annual capital plan
Chief Executive
Medical Equipment Bids Committee
Director of Finance,
Medical Director
b) Private Finance:
Demonstrate that the use of private finance represents best value for money and transfers risk to the private sector. Proposal to use PFI must be specifically agreed by the Board of Directors
Chief Executive
Director of Finance
c) Leases (property and equipment)
Granting and termination of leases with Annual rent < £100k
Granting and termination of leases of > £100k should be reported to the Board of
Chief Executive
Board of Directors
Director of Finance
Chief Executive / Director of Finance
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 86 of 150
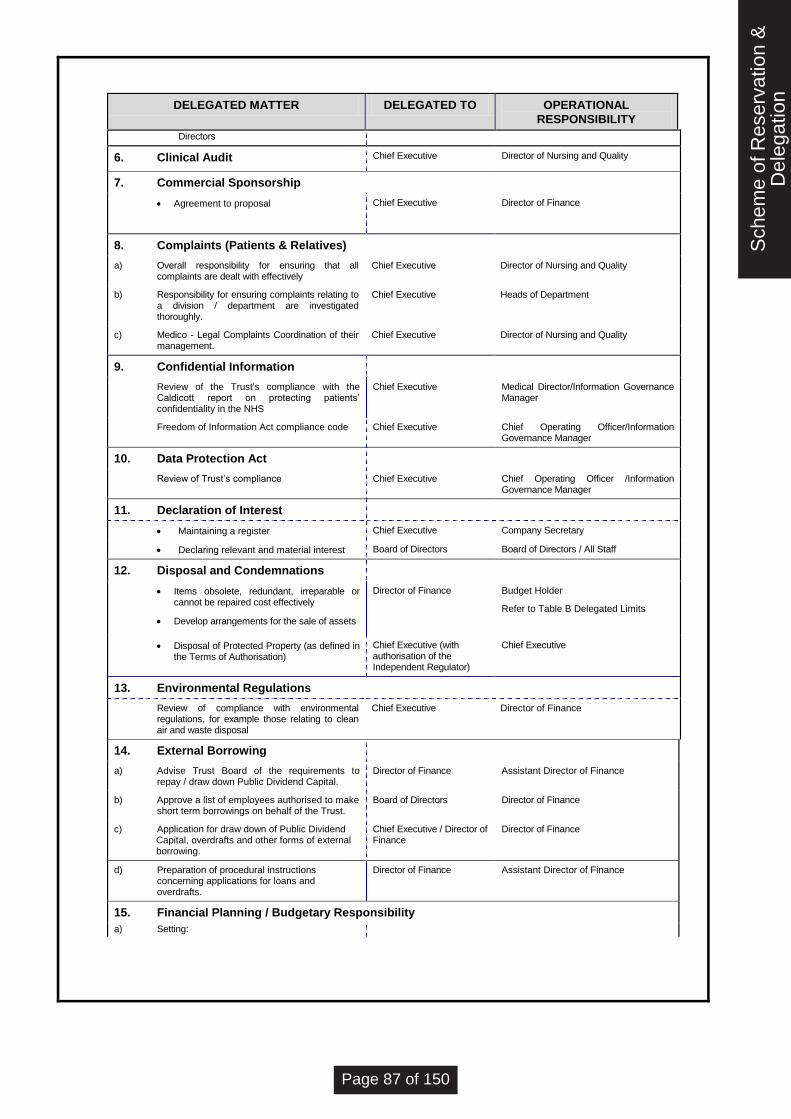
DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
Directors
6. Clinical Audit Chief Executive Director of Nursing and Quality
7. Commercial Sponsorship
Agreement to proposal Chief Executive
Director of Finance
8. Complaints (Patients & Relatives)
a) Overall responsibility for ensuring that all complaints are dealt with effectively
Chief Executive Director of Nursing and Quality
b) Responsibility for ensuring complaints relating to a division / department are investigated thoroughly.
Chief Executive Heads of Department
c) Medico - Legal Complaints Coordination of their management.
Chief Executive Director of Nursing and Quality
9. Confidential Information
Review of the Trust's compliance with the Caldicott report on protecting patients’ confidentiality in the NHS
Chief Executive Medical Director/Information Governance Manager
Freedom of Information Act compliance code Chief Executive Chief Operating Officer/Information Governance Manager
10. Data Protection Act
Review of Trust’s compliance Chief Executive Chief Operating Officer /Information Governance Manager
11. Declaration of Interest
Maintaining a register Chief Executive Company Secretary
Declaring relevant and material interest Board of Directors Board of Directors / All Staff
12. Disposal and Condemnations
Items obsolete, redundant, irreparable or cannot be repaired cost effectively
Develop arrangements for the sale of assets
Director of Finance
Budget Holder
Refer to Table B Delegated Limits
Disposal of Protected Property (as defined in the Terms of Authorisation)
Chief Executive (with authorisation of the Independent Regulator)
Chief Executive
13. Environmental Regulations
Review of compliance with environmental regulations, for example those relating to clean air and waste disposal
Chief Executive Director of Finance
14. External Borrowing
a) Advise Trust Board of the requirements to repay / draw down Public Dividend Capital.
Director of Finance Assistant Director of Finance
b) Approve a list of employees authorised to make short term borrowings on behalf of the Trust.
Board of Directors Director of Finance
c) Application for draw down of Public Dividend Capital, overdrafts and other forms of external borrowing.
Chief Executive / Director of Finance
Director of Finance
d) Preparation of procedural instructions concerning applications for loans and overdrafts.
Director of Finance Assistant Director of Finance
15. Financial Planning / Budgetary Responsibility
a) Setting:
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 87 of 150
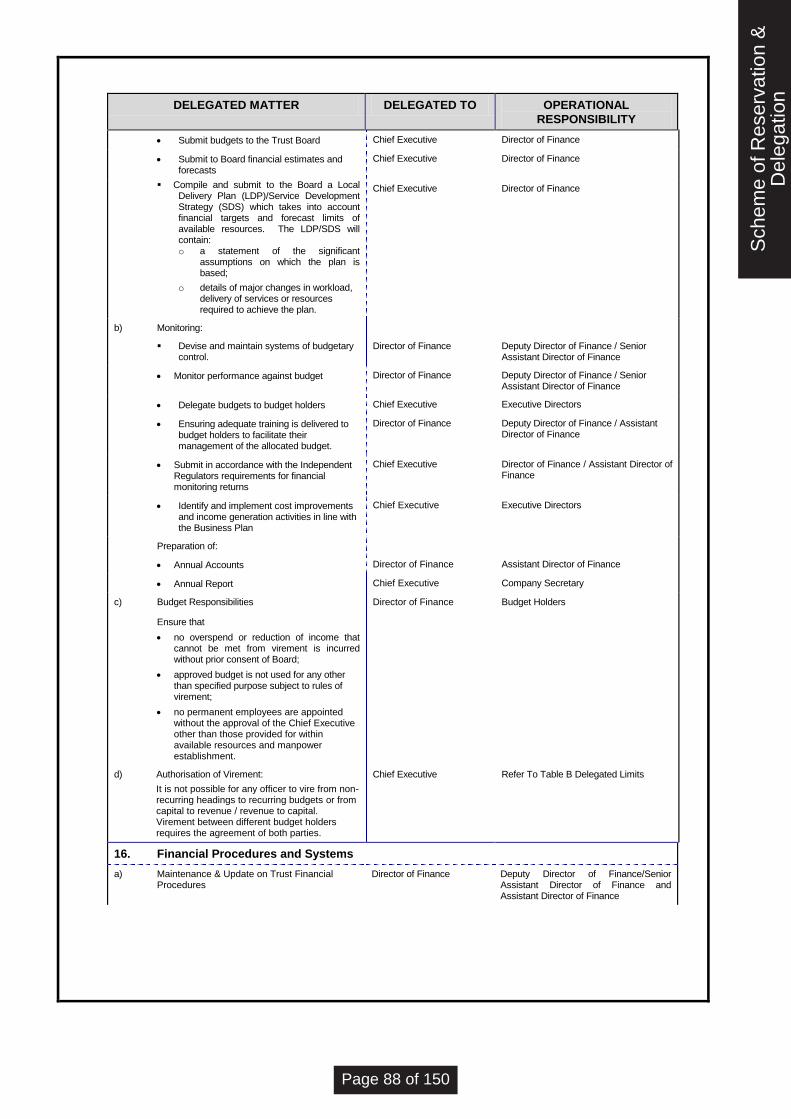
DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
Submit budgets to the Trust Board Chief Executive Director of Finance
Submit to Board financial estimates and forecasts
Chief Executive Director of Finance
Compile and submit to the Board a Local Delivery Plan (LDP)/Service Development Strategy (SDS) which takes into account financial targets and forecast limits of available resources. The LDP/SDS will contain: o a statement of the significant
assumptions on which the plan is based;
o details of major changes in workload, delivery of services or resources required to achieve the plan.
Chief Executive Director of Finance
b) Monitoring:
Devise and maintain systems of budgetary control.
Director of Finance
Deputy Director of Finance / Senior Assistant Director of Finance
Monitor performance against budget Director of Finance Deputy Director of Finance / Senior Assistant Director of Finance
Delegate budgets to budget holders Chief Executive Executive Directors
Ensuring adequate training is delivered to budget holders to facilitate their management of the allocated budget.
Director of Finance Deputy Director of Finance / Assistant Director of Finance
Submit in accordance with the Independent Regulators requirements for financial monitoring returns
Chief Executive Director of Finance / Assistant Director of Finance
Identify and implement cost improvements and income generation activities in line with the Business Plan
Chief Executive Executive Directors
Preparation of:
Annual Accounts
Director of Finance
Assistant Director of Finance
Annual Report Chief Executive Company Secretary
c) Budget Responsibilities
Ensure that
no overspend or reduction of income that cannot be met from virement is incurred without prior consent of Board;
approved budget is not used for any other than specified purpose subject to rules of virement;
no permanent employees are appointed without the approval of the Chief Executive other than those provided for within available resources and manpower establishment.
Director of Finance Budget Holders
d) Authorisation of Virement:
It is not possible for any officer to vire from non-recurring headings to recurring budgets or from capital to revenue / revenue to capital. Virement between different budget holders requires the agreement of both parties.
Chief Executive Refer To Table B Delegated Limits
16. Financial Procedures and Systems
a) Maintenance & Update on Trust Financial Procedures
Director of Finance Deputy Director of Finance/Senior Assistant Director of Finance and Assistant Director of Finance
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 88 of 150

DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
b) Responsibilities:-
Implement Trust’s financial policies and co-ordinate corrective action.
Ensure that adequate records are maintained to explain Trust’s transactions and financial position.
Providing financial advice to members of the Board of Directors and staff.
Ensure that appropriate statutory records are maintained.
Designing and maintaining compliance with all financial systems
Director of Finance Deputy Director of Finance
17. Fire precautions
Ensure that the Fire Precautions and prevention policies and procedures are adequate and that fire safety and integrity of the estate is intact.
Chief Executive Director of Finance/Director of Nursing and Quality
18. Fixed Assets
a) Maintenance of asset register including asset identification and monitoring
Chief Executive Director of Finance/ Assistant Director of Finance / Capital Asset Accountant
b) Ensuring arrangements for financial control and financial audit of building and engineering contracts and property transactions comply with CONCODE and ESTATECODE.
Director of Finance Director of Finance/ Assistant Director of Finance / Capital Asset Accountant
c) Calculate and pay capital charges in accordance with the requirements of the Independent Regulator
Director of Finance Assistant Director of Finance/ Capital Asset Accountant
d) Responsibility for security of Trust’s assets including notifying discrepancies to the Director of Finance and reporting losses in accordance with Trust’s procedures
Chief Executive All staff
19. Fraud, Bribery & Corruption (See
also 36)
a) Monitor and ensure compliance with NHS contractual requirements on fraud, bribery and corruption including the appointment of the Local Counter Fraud Specialist.
Chief Executive and Director of Finance
Local Counter Fraud Specialist.
b) Notify NHS Protect of all Frauds and, if appropriate, External Audit
Director of Finance Local Counter Fraud Specialist.
20. Funds Held on Trust (Charitable and Non Charitable Funds)
a) Management:
Funds held on trust are managed appropriately.
Charitable Funds Committee
Assistant Director of Finance
b) Maintenance of authorized signatory list of nominated fund holders.
Director of Finance Assistant Director of Finance
c) Expenditure Limits Director of Finance Refer To Table B Delegated Limits
d) Developing systems for receiving donations Director of Finance Assistant Director of Finance
e) Dealing with legacies Director of Finance Assistant Director of Finance
f) Fundraising Appeals Charitable Funds Committee
Assistant Director of Finance
Preparation and monitoring of budget Director of Finance Fund Raising Manager with advice from Divisional Accountant.
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 89 of 150

DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
Reporting progress and performance against budget.
Director of Finance Fund Raising Manager with advice from Divisional Accountant.
g) Operation of Bank Accounts:
Managing banking arrangements and operation of bank accounts
Director of Finance
Assistant Director of Finance
Opening bank accounts Director of Finance Director of Finance
h) Investments:
Nominating deposit taker
Charitable Funds Committee
Director of Finance
Placing transactions Director of Finance Charitable Funds Committee
i) Regulation of funds with Charities Commission Director of Finance
Assistant Director of Finance
21. Health and Safety
Review of all statutory compliance with legislation and Health and Safety requirements including control of Substances Hazardous to Health Regulations
Chief Executive Risk Manager
22. Hospitality/Gifts (Acceptance of)
a) Keeping of hospitality register Chief Executive Company Secretary
b) Applies to both individual and collective hospitality receipt items. See Appendix B for limits.
All staff declaration required in Trust’s Hospitality Register
23. Infectious Diseases & Notifiable
Outbreaks
Chief Executive Medical Director /Infection control officer
24. Information Management & Technology
Developing systems in accordance with the Trust’s IM&T Strategy.
Implementing new systems ensure they are developed in a controlled manner and thoroughly tested.
Seeking third party assurances regarding systems operated externally.
Medical Director Head of IT
Ensure that contracts for computer services define responsibility re security, privacy, accuracy, completeness and timeliness of data during processing and storage.
Chief Operating Officer Head of IT/Information Governance Manager
Ensure that risks to the Trust from use of IT are identified and considered and that disaster recovery plans are in place.
Medical Director Head of IT
25. Legal Proceedings
a) Engagement of Trust’s Solicitors / Legal Advisors
Chief Executive Director of Finance/Company Secretary
b) Approve and sign all documents which will be necessary in legal proceedings, i.e. executed as a deed.
Chief Executive/Chair Director of Finance/Company Secretary
c) Sign on behalf of the Trust any agreement or document not requested to be executed as a deed.
Chief Executive Director of Finance/Company Secretary
26. Losses, Write-off & Compensation
a) Prepare procedures for recording and accounting for losses and special payments
Director of Finance
Assistant Director of Finance
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 90 of 150

DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
Losses
Losses of cash due to theft, fraud, overpayment & others.
Director of Finance
Director of Finance
Fruitless payments (including abandoned Capital Schemes)
Bad debts and claims abandoned.
Damage to buildings, fittings, furniture and equipment and loss of equipment and property in stores and in use due to:
Culpable causes (e.g. fraud, theft, arson).
Reviewing appropriate requirement for insurance claims
Director of Finance Director of Finance
d) A register of all of the payments should be maintained by the Finance Department and made available for inspection
Director of Finance Director of Finance
e) A report of all of the above payments should be presented to the Finance Committee
Director of Finance Director of Finance
Special Payments
Compensation payments by Court Order
Chief Executive Director of Finance
Exgratia Payments:-
To patients/staff for loss of personal effects
For clinical negligence after legal advice
For personal injury after legal advice
Other clinical negligence and personal injury
Other ex-gratia payments
27. Meetings
a) Calling meetings of the Trust Board Chair Company Secretary
b) Chair all Trust Board meetings and associated responsibilities
Chair Chair
28. Medical
Medical Leadership Medical Director Medical Director
Programmes of medical education Medical Director Medical Director
Medical staffing plans Medical Director Medical Director
Medical Research Medical Director Medical Director
29. Non Pay Expenditure
a) Maintenance of a list of managers authorised to place requisitions/orders and accept goods in accordance with Table B
Chief Executive Procurement and Commercial Services Manager/Director of Finance/Chief Pharmacist (restricted to Pharmaceutical products only)
b) Obtain the best value for money when requisitioning goods / services
Chief Executive Procurement and Commercial Services Manager/Director of Finance/Chief Pharmacist
c) Non-Pay Expenditure for which no specific budget has been set up and which is not subject to funding under delegated powers of virement. (Subject to the limits specified above in (a)
Chief Executive
Director of Finance/ Deputy Director of Finance
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 91 of 150

DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
d) Develop systems for the payment of accounts Director of Finance Assistant Director of Finance
e) Prompt payment of accounts Director of Finance Assistant Director of Finance
f) Financial Limits for ordering / requisitioning goods and services
Director of Finance Refer To Table B Delegated Limits
g) Approve prepayment arrangements Director of Finance Assistant Director of Finance
h) Controls in place to match invoices to purchase orders using a 3 way matching system – invoice lines to purchase order lines, quantity and price and receipts. Price tolerance is £10 or 10% of invoice value.
Director of Finance Assistant Director of Finance
i) Passive approval of low value invoices Director of Finance Refer to Table B Delegated Limits
30. Nursing
Compliance with statutory and regulatory arrangements relating to professional nursing and midwifery practice.
Director of Nursing and Quality
Director of Nursing and Quality
Matters involving individual professional competence of nursing staff.
Director of Nursing and Quality
Director of Nursing and Quality
Compliance with professional training an development of nursing staff.
Director of Nursing and Quality
Director of Nursing and Quality
Quality assurance of nursing processes.
Clinical Governance Arrangements
Director of Nursing and Quality
Director of Nursing and Quality
31. Patient Services Agreements
a) Negotiation of Trust Contract and Non Commercial Contracts
Chief Executive Director of Finance /Deputy Director of Finance
b) Quantifying and monitoring out of area treatments
Director of Finance Deputy Director of Finance /Senior Assistant Director of Finance
c) Reporting actual and forecast income Chief Executive Deputy Director of Finance /Senior Assistant Director of Finance
d) Costing Trust Contract and Non Commercial Contracts
Director of Finance Deputy Director of Finance /Senior Assistant Director of Finance
e) Reference costing / Payment by Results Director of Finance Deputy Director of Finance
f) Ad hoc costing relating to changes in activity, developments, business cases and bids for funding
Director of Finance Deputy Director of Finance /Senior Assistant Director of Finance or nominated Deputy
32. Patients’ Property (in conjunction with financial advice)
a) Ensuring patients and guardians are informed about patients’ monies and property procedures on admission
Chief Executive Directorate Nursing Managers
b) Prepare detailed written instructions for the administration of patients’ property
Director of Finance Assistant Director of Finance /Directorate Nurse Managers
c) Informing staff of their duties in respect of patients’ property
Director of Finance Assistant Director of Finance
/Directorate Nurse Managers d) Issuing property of deceased patients (See SFI
15.9, 15.10)
<£4,999 in accordance with agreed Trust policies.
>£5,000 only on production of a probate letter of administration
Director of Finance
Assistant Director of Finance
33. Personnel & Pay
a) Nomination of officers to enter into contracts of employment regarding staff, agency staff or consultancy service contracts
Chief Executive
Director of Human Resources / Directorate Managers
b) Develop Human resource policies and strategies for approval by the board including training, industrial relations.
Director of Human Resources
Director of Human Resources
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 92 of 150
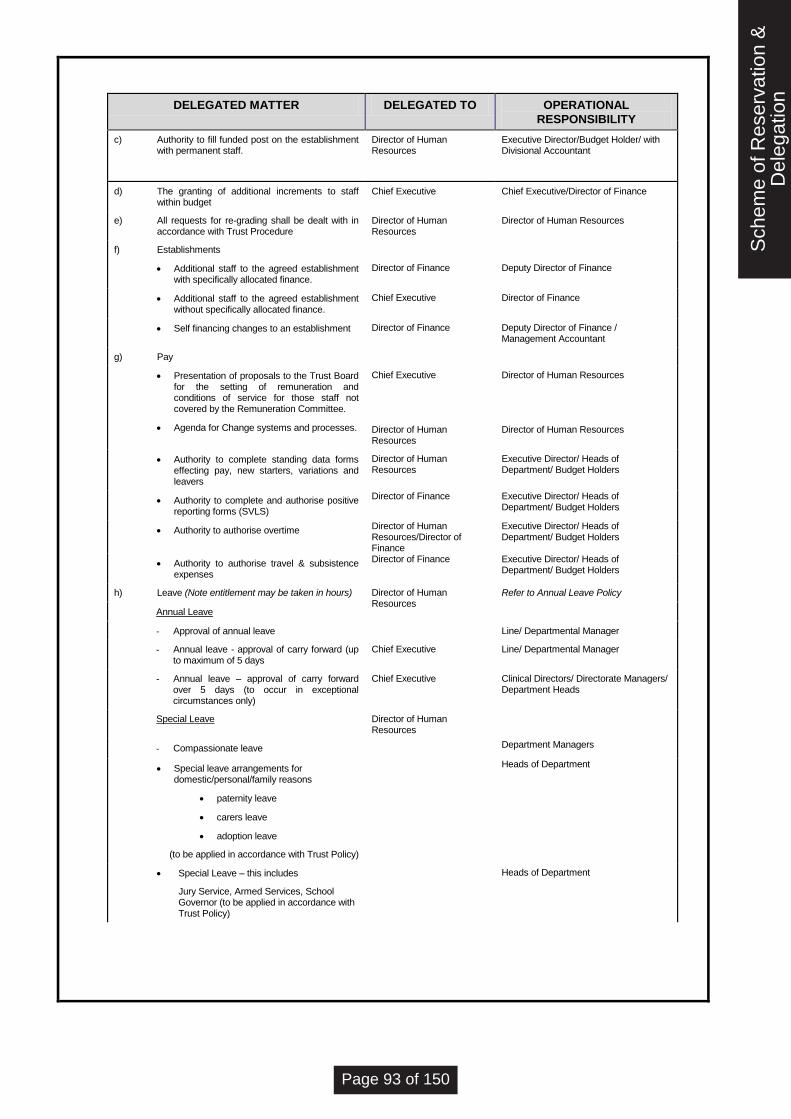
DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
c) Authority to fill funded post on the establishment with permanent staff.
Director of Human Resources
Executive Director/Budget Holder/ with Divisional Accountant
d) The granting of additional increments to staff within budget
Chief Executive Chief Executive/Director of Finance
e) All requests for re-grading shall be dealt with in accordance with Trust Procedure
Director of Human Resources
Director of Human Resources
f) Establishments
Additional staff to the agreed establishment with specifically allocated finance.
Director of Finance
Deputy Director of Finance
Additional staff to the agreed establishment without specifically allocated finance.
Chief Executive Director of Finance
Self financing changes to an establishment Director of Finance Deputy Director of Finance / Management Accountant
g) Pay
Presentation of proposals to the Trust Board for the setting of remuneration and conditions of service for those staff not covered by the Remuneration Committee.
Agenda for Change systems and processes.
Chief Executive
Director of Human Resources
Director of Human Resources
Director of Human Resources
Authority to complete standing data forms effecting pay, new starters, variations and leavers
Director of Human Resources
Executive Director/ Heads of Department/ Budget Holders
Authority to complete and authorise positive reporting forms (SVLS)
Director of Finance Executive Director/ Heads of Department/ Budget Holders
Authority to authorise overtime Director of Human Resources/Director of Finance
Executive Director/ Heads of Department/ Budget Holders
Authority to authorise travel & subsistence expenses
Director of Finance Executive Director/ Heads of Department/ Budget Holders
h) Leave (Note entitlement may be taken in hours) Director of Human Resources
Refer to Annual Leave Policy
Annual Leave
- Approval of annual leave Line/ Departmental Manager
- Annual leave - approval of carry forward (up to maximum of 5 days
Chief Executive Line/ Departmental Manager
- Annual leave – approval of carry forward over 5 days (to occur in exceptional circumstances only)
Chief Executive Clinical Directors/ Directorate Managers/ Department Heads
Special Leave Director of Human Resources
- Compassionate leave Department Managers
Special leave arrangements for domestic/personal/family reasons
paternity leave
carers leave
adoption leave
(to be applied in accordance with Trust Policy)
Heads of Department
Special Leave – this includes
Jury Service, Armed Services, School Governor (to be applied in accordance with Trust Policy)
Heads of Department
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 93 of 150

DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
Leave without pay Clinical Director/ Directorate Managers/ Heads of Department
Medical Staff Leave of Absence – paid and unpaid
Clinical Director with advice from Medical Director
Time off in lieu Line /Departmental Manager
Maternity Leave - paid and unpaid Director of Human Resources
Automatic approval with guidance
Sick Leave Director of Human Resources
i) Extension of sick leave on pay Director of Human Resources
ii) Return to work part-time on full pay to assist recovery
Director of Human Resources
Study Leave Chief Executive
Study leave outside the UK Chief Executive
Medical staff study leave (UK)
- Consultant / Non Career Grade
- Career Grade
Medical Director
Medical Director
Post Graduate Tutor
All other study leave (UK) Director of Human Resources
Executive Directors /Clinical Director/ Directorate Managers/ Department Heads
i) Removal Expenses, Excess Rent and House Purchases maximum £8,000
Authorisation of payment of removal expenses incurred by officers taking up new appointments (providing consideration was promised at interview)
Director of Human Resources
Executive Director
Refer to Table B Delegated Limits
j) Grievance Procedure
All grievances cases must be dealt with strictly in accordance with the Grievance Procedure and the advice of the Director of Human Resources must be sought when the grievance reaches the level of Divisional General Managers / Heads of Department
Director of Human Resources
Executive Director/Clinical Director/Appeals Board
k) Authorised - Car Users
h) Leased car
i) Regular user allowance
Chief Executive
Director of Finance
Chief Executive/ Director of Finance
Chief Executive/ Director of Finance
l) Mobile Phone Users / Blackberries Director of Finance Clinical Director/ Directorate Manager/Department Head
m) Renewal of Fixed Term Contract
Director of Human Resources
Executive Director with advice from Divisional Accountant
n) Staff Retirement Policy
Authorisation of extensions of contract beyond normal retirement age in exceptional circumstances
Chief Executive Director of Human Resources
Authorisation of return to work in part time capacity under the flexible retirement scheme.
Chief Executive Director of Human Resources
o) Redundancy Chief Executive Director of Human Resources
p) Ill Health Retirement
Decision to pursue retirement on the grounds of ill-health following advice from the Occupational Health Department.
Chief Executive Director of Human Resources
q) Disciplinary Procedure (excluding Executive Directors)
Chief Executive To be applied in accordance with the Trust’s Disciplinary Procedure
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 94 of 150

DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
r) Waiting List Payments
Approval of Rates of Pay
Chief Executive
Executive Directors
s) Ensure that all employees are issued with a Contract of employment in a form approved by the Board of Directors and which complies with employment legislation.
Director of Human Resources
Human Resources Managers
t) Engagement of staff not on the establishment
a. Management Consultants
Refer to Table B
Booking of bank staff
a. nursing Director of Nursing and Quality
Senior Nurse Manager/ Manager of Nurse bank
b. other Clinical Directors Executive Director/ Budget Holder
Booking of agency staff
a. nursing Director of Nursing and Quality
Senior Nurse Manager/ Manager of Nurse bank
b. other Clinical Director Executive Director/ Budget Holder
34. Quotation, Tendering & Contract Procedures
a) Services:
Best value for money is demonstrated for all services provided under contract or in-house
Chief Executive
Director of Finance /Procurement and Commercial Services Manager/Clinical Director/Directorate manager/Department Heads
Nominate officers to oversee and manage the contract on behalf of the Trust.
Chief Executive Director of Finance
b) Competitive Tenders:
Authorisation Limits
Chief Executive
Refer To Table B Delegated Limits
Maintain a register to show each set of competitive tender invitations despatched.
Chief Executive Procurement and Commercial Services Manager, Director of Finance, Pharmacy Manager
Receipt and custody of tenders prior to opening
Chief Executive FAO Chief Executive – C/o the General Office
Opening Tenders Chief Executive Two officers from the approved list as authorised by the Audit Committee
Decide if late tenders should be considered Chief Executive Chief Executive/ Director of Finance/Procurement and Commercial Services Manager
Ensure that appropriate checks are carried out as to the technical and financial capability of the firms invited to tender or quote.
Chief Executive Director of Finance
Note : The final five steps above are fully incorporated within the Trust electronic tendering process and in these instances witness is required to the status on the web-based system on a Trust PC screen.
Two officers from the approved list as authorised by the Audit Committee
c) Quotations Chief Executive Refer To Table B Delegated Limits
d) Waiving the requirement to request
tenders - subject to SOs (reporting to the Board)
Chief Executive
Refer To Table B Delegated Limits
quotes - subject to SOs Chief Executive or Director of Finance
Refer To Table B Delegated Limits
35. Records
a) Review Trust’s compliance with the Records Management Code of Practice
Chief Executive Executive Directors
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 95 of 150

DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
b) Ensuring the form and adequacy of the financial records of all departments
Director of Finance Deputy Director of Finance
36. Reporting of Incidents to the Police
a) Where a criminal offence is suspected
criminal offence of a violent nature
arson or theft
other
Chief Executive Senior Manager On call/Directorate Managers/Department Heads/Hospital Co - coordinator
b) Where a fraud is involved (reporting to NHS Protect)
Director of Finance Director of Internal Audit / Local Counter Fraud Specialist
c) Deciding at what stage to involve the police in cases of misappropriation and other irregularities not involving fraud or corruption.
Director of Finance Director of Finance
37. Risk Management
Ensuring the Trust has a Risk Management Strategy and a programme of risk management
Chief Executive Director of Nursing and Quality /Head of Risk
Ensuring the Trust has an active Board Assurance Framework
Chief Executive Company Secretary
Developing systems for the management of risk.
Director of Nursing and Quality
Head of Risk
Developing incident and accident reporting systems
Director of Nursing and Quality
Head of Risk
Compliance with the reporting of incidents and accidents
Director of Nursing and Quality
All staff
38. Seal
a) The keeping of a register of seal and safekeeping of the seal
Chief Executive Company Secretary
b) Attestation of seal in accordance with Standing Orders
Chair /Chief Executive Director of Finance / Company Secretary (report to Trust Board)
c) Property transactions and any other legal requirement for the use of the seal.
Chair /Chief Executive Director of Finance / Company Secretary (report to Trust Board)
39. Security Management
a) Monitor and ensure compliance with Directions issued by the Secretary of State for Health on NHS security management including appointment of the Local Security Management Specialist.
Chief Executive Deputy Chief Executive / Local Security Management Specialist.
40. Setting of Fees and Charges (Income)
a) Private Patient, Overseas Visitors, Income Generation and other patient related services.
Director of Finance Deputy Director of Finance
b) Non patient care income Director of Finance Deputy Director of Finance
c) Informing the Director of Finance of monies due to the Trust
Director of Finance All Staff
d) Recovery of debt Director of Finance Assistant Director of Finance
e) Security of cash and other negotiable instruments
Director of Finance Assistant Director of Finance
41. Materials Management and Receipt & Distribution of Goods
a) Responsibility for systems of control over materials management and receipt & distribution of goods including management of issues and returns
Director of Finance Director of Finance/Procurement and Commercial Services Manager / Clinical Directors / Directorate Managers / Department Heads
b) Responsibility for Stockholding arrangements at Ward / Departmental locations covering
Director of Finance Procurement and Commercial Services Manager/ Clinical Directors / Directorate
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 96 of 150

DELEGATED MATTER DELEGATED TO OPERATIONAL
RESPONSIBILITY
agreement on stock levels and periodic reporting including year end stock take values
Managers / Department Heads
c) Passive approval of low value invoices Director of Finance Refer to Table B Delegated Limits
d) Responsibility for controls of pharmaceutical stock.
Designated Pharmaceutical officer
Head of Pharmacy
Table B – Delegated Financial Limits
All thresholds are inclusive of VAT irrespective of recovery arrangements. Details of procurement thresholds from 1 January 2014 are provided (net of VAT)
Proposed Financial Limits (Subject to funding available in
budget) Includes:-
1. BUSINESS CASES
1.1 Revenue Investments
Trust Board Over £250,000 p.a. After review by F,P & I
Finance, Performance & Investment Committee
£50,000 to £250,000 p.a. After review by SEMT
Senior Executive Management Team
£25,0000 to £50,000 p.a. After review by DDoF and DDoP
Deputy Director of Finance/Deputy Director of
Performance Up to £25,000
1.2 Capital Investments
Trust Board Over £250,000. Subject to capital resource limit (CRL)
Finance, Performance & Investment Committee £50,000 to £250,000. Subject to capital resource limit (CRL)
Director of Finance Up to £50,000 Subject to capital resource limit (CRL)
2. QUOTATIONS AND TENDERS
2.1 Procurement and Commercial Services Manager / Divisional General Managers / Head of Department / Head of Technical Services as appropriate £10,000 to £30,000
Quotations: These must be advertised through Contracts Finder.
Two officers as per the approved signatory list
Procurement and Commercial Services Manager / Director of Finance
Over £30,000
(in compliance with EC thresholds as appropriate updated January 2014)
Competitive Tenders for goods/services: These must be advertised through Contracts Finder.
Supplies Manager/Director of Finance
Supplies and Services £111,676
Works £4,322,012 EU Limits
Waiving requirements for quotes or tenders –
subject to full compliance with SO’s (and reported
to the Audit Committee):
Chief Executive and Director of Finance
Between £75,000 and £111,676 Limit for waiving tenders
Chief Executive or Director of Finance Up to £75,000
Limit for waiving tends and quotations
Procurement and Commercial Manager / Head of Technical Services Up to £10,000 Limit for waiving quotations
2.2 Purchase order approval (excluding pharmacy):-
Chief Executive or Director of Finance Over £100,000 Limit subject to budget availability.
Procurement and Commercial Manager Up to £100,000
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 97 of 150

Proposed Financial Limits (Subject to funding available in
budget) Includes:-
Deputy Procurement Manager Up to £50,000
Senior Purchasing Officer Up to £20,000
Purchasing Officer
Up to £10,000
2.3 Pharmacy purchase order approval
Chief Executive (or Director of Finance) Over £50,000
Medical Director Up to £50,000
Chief/Deputy Pharmacist Up to £25,000
Senior Pharmacy Technicians Up to £10,000
3. REQUISITIONING GOODS AND SERVICES AND APPROVING PAYMENTS
3.1 Revenue expenditure
Trust Board Over £500,000
Chief Executive Up to £500,000
Director of Finance Up to £250,000
Energy Manager Up to £200,000
Limit specifically for Dalkia (Veolia Group) Energy Centre monthly invoices.
Deputy Director of Finance Up to £100,000
Executive Directors Up to £50,000
Head of Technical Services Up to £20,000
Budgetholders/ Divisional Finance Managers/Senior Facilities staff Up to £10,000
Medical Staffing department Up to £5,000
** For operational purposes, the Director of Finance has a £10m approval limit on the finance system. However, approvals above the DoF limit of £250k are subject to Chief Exec and/or Board approval.
3.2 Capital requisitions/Capital non PO invoice approval (Subject to annual programme being approved by Trust Board)
Trust Board Over £250,000
Subject to Board approval of the annual capital plan..
Chief Executive/ Director of Finance Up to £250,000
Capital Accountant Up to £100,000
Assistant Director of Finance Up to £10,000
Estates stage payment certificates
Chief Executive (with Board approval) Over £250,000
Director of Finance Up to £250,000
Project Scheme Manager Up to £100,000
Capital Contingency authorisation
Finance & Investment Committee Up to £100,000
Director of Finance Up to £50,000
Assistant Director of Finance Up to £10,000
** For operational purposes, the Director of Finance has a £10m approval limit on the finance system. However, approvals above the DoF limit of £250k are subject to Chief Exec and/or Board approval.
3.3 Removal Expenses:-
Director of Human Resources Up to £5,000
Remuneration Committee Over £5,000
3.4 Passive approval of low value invoices
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 98 of 150
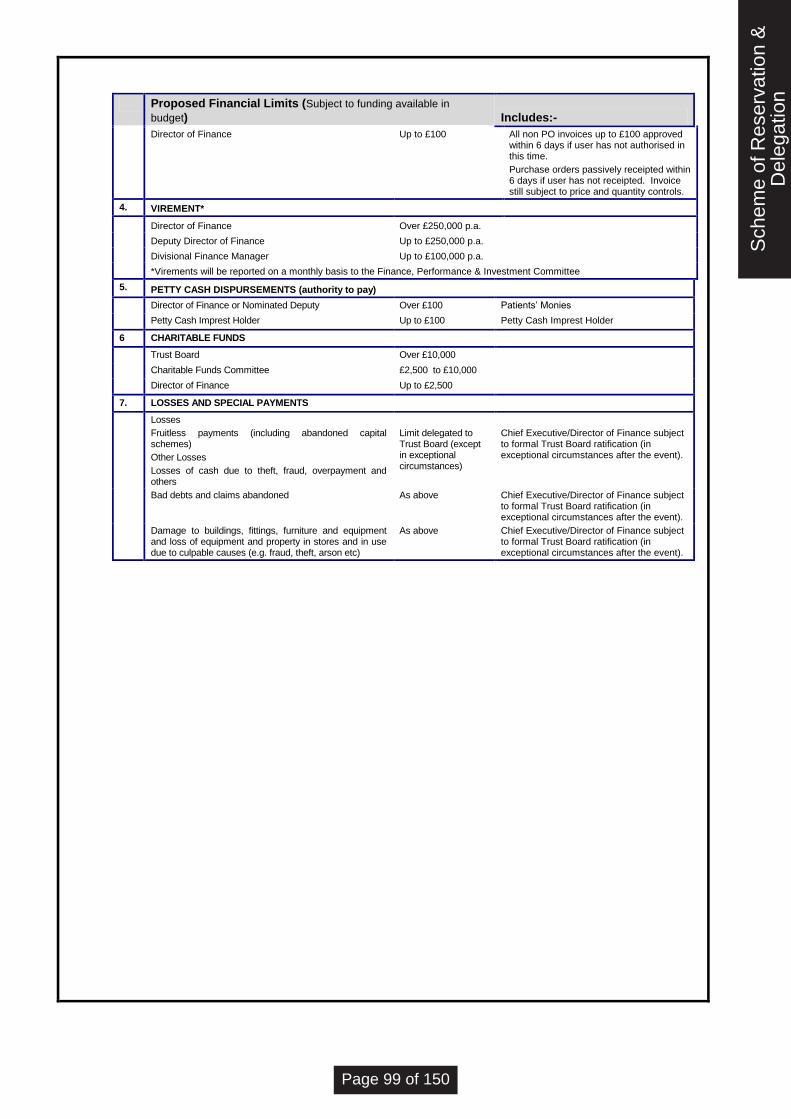
Proposed Financial Limits (Subject to funding available in
budget) Includes:-
Director of Finance Up to £100 All non PO invoices up to £100 approved within 6 days if user has not authorised in this time.
Purchase orders passively receipted within 6 days if user has not receipted. Invoice still subject to price and quantity controls.
4. VIREMENT*
Director of Finance Over £250,000 p.a.
Deputy Director of Finance Up to £250,000 p.a.
Divisional Finance Manager Up to £100,000 p.a.
*Virements will be reported on a monthly basis to the Finance, Performance & Investment Committee
5. PETTY CASH DISPURSEMENTS (authority to pay)
Director of Finance or Nominated Deputy Over £100 Patients’ Monies
Petty Cash Imprest Holder Up to £100 Petty Cash Imprest Holder
6 CHARITABLE FUNDS
Trust Board Over £10,000
Charitable Funds Committee £2,500 to £10,000
Director of Finance Up to £2,500
7. LOSSES AND SPECIAL PAYMENTS
Losses
Fruitless payments (including abandoned capital schemes)
Other Losses
Losses of cash due to theft, fraud, overpayment and others
Limit delegated to Trust Board (except in exceptional circumstances)
Chief Executive/Director of Finance subject to formal Trust Board ratification (in exceptional circumstances after the event).
Bad debts and claims abandoned As above Chief Executive/Director of Finance subject to formal Trust Board ratification (in exceptional circumstances after the event).
Damage to buildings, fittings, furniture and equipment and loss of equipment and property in stores and in use due to culpable causes (e.g. fraud, theft, arson etc)
As above Chief Executive/Director of Finance subject to formal Trust Board ratification (in exceptional circumstances after the event).
Sch
eme
of R
eser
vatio
n &
Del
egat
ion
Page 99 of 150
APPENDICES
Southport & Ormskirk Hospital NHS Trust
App
endi
ces
Page 100 of 150

App
endi
ces
Page 101 of 150

RECORD OF AMENDMENTS
NO SECTION DATE
1 Updated document Issued for implementation July 2007
2 Document Reviewed November 2008
3 Document Reviewed May 2009
4 Document Reviewed May 2010
5 Document Reviewed August 2011
6 Document Reviewed May 2013
7 Document Reviewed May 2014
8 Document Reviewed June 2015
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
App
endi
ces
Page 102 of 150

I N D E X O F A P P E N D I C E S
CONTENTS APPENDIX
Accountable Officer Memorandum for Chief Executives of NHS Trusts A
Code of Conduct for NHS Boards B
Code of Accountability for NHS Boards C
Code of Conduct for NHS Managers D
Board of Directors Code of Conduct E
Standards of Business Conduct for NHS Staff F
Staff Code of Personal and Business Conduct G
Fraud, Bribery and Corruption Reporting Arrangements H
Trust Policies I
App
endi
ces
Page 103 of 150

AC C O U N T AB L E O F F I C E R M E M O R AN D U M F O R C H I E F E X E C U T I V E S O F N H S T R U S T S
1. You are hereby appointed as the NHS officer responsible and accountable for funds entrusted to your
Trust. This memorandum describes your responsibilities as an Accountable Officer, and relates them
to my overall accountability for funds voted by Parliament for the National Health Service. In fulfilling
your role as Accountable Officer you will also wish to bear in mind your responsibilities to the Trust
Board of which you are a member. The corporate role of the Board is clearly set out in the Codes of
Conduct and Accountability issued by the Secretary of State in April 1994.
Functions of NHS Trusts
2. The functions of Trusts are:-
to enter into and fulfil service agreements with commissioning bodies;
to meet their statutory duties;
to maintain and develop their relationships with patients, local partner organisations and the wider
local community, their commissioning agencies and their suppliers.
The essence of your role as Accountable Officer is to see that the Trust carries out these functions in a
way which ensures the proper stewardship of public money and assets. The paragraphs below set out
this responsibility in more detail.
Relationship between the Accounting Officer and Accountable Officers
3. My responsibilities as Accounting Officer are set out in a memorandum sent to me on appointment. In
essence, I am responsible for the propriety and regularity of public finances in the NHS; for the keeping
of proper accounts; for prudent and economical administration; for the avoidance of waste and
extravagance; and for the efficient and effective use of all the resources in my charge.
4. Your role as Accountable Officer for your Trust is very similar to mine as Accounting Officer for the NHS
in England. I require you to observe the same general requirements as are laid on me, and to ensure
that the Trust's officers also abide by them. Your Trust is an integral part of the NHS and is largely
dependent on public funding even though this is routed through contracts with purchasers.
5. Trusts have the following key relationships:-
with commissioning bodies, through service agreements to deliver health services to agreed
specifications;
with their local partners and wider communities, through working in partnership to promote the
objectives of the local Health Improvement Programme, holding at least one public meeting a
year, through publishing business plans, an annual report and accounts; and through
compliance with the Code of Practice on Openness in the NHS issued in 1995;
with patients, through the management of standards of patient care;
accountability to the Secretary of State and to Parliament for the performance of their functions
and meeting statutory financial duties.
6. This memorandum deals with the fourth relationship. The first three are covered in other guidance.
7. NHS Trusts are directly accountable to the Secretary of State for Health, who delegates to me
responsibility for the supervision of trust performance. I am accountable both to the Secretary of State
and, in my Accounting Officer role, directly to Parliament. A similar dual accountability applies to the
Chief Executives of Trusts, who are responsible both to their Boards and, via the Accounting Officer, to
Parliament. You are therefore accountable through me to Parliament for the stewardship of resources
within your Trust.
App
endi
ces
Page 104 of 150

Statutory Accounts
8. I sign the Summarised Accounts of health bodies in England, and the Appropriation Accounts of the
Department of Health, and by virtue of this responsibility I can be summoned to appear before the
Committee of Public Accounts (PAC) to deal with questions arising from those accounts or from reports
made to Parliament by the Comptroller and Auditor General.
9. The summarised accounts are derived from the statutory accounts of individual Trusts. You are,
together with the Director of Finance, (as set out in Part 1 of the Trust Finance Manual and in the
booklet "The role of the Director of Finance in the NHS" - EL (94)18) responsible for ensuring that the
accounts of the Trust which are presented to the Board for approval are prepared under principles and
in a format directed by the Secretary of State with the approval of the Treasury. These accounts must
disclose a true and fair view of the Trust's income and expenditure, cash flows, gains and losses, and
of its state of affairs. You will sign these accounts, along with the Director of Finance, on behalf of the
Board.
10. Reflecting your role as Accountable Officer, you will sign a statement in the accounts (as indicated in
the Manual for Accounts) outlining your responsibilities as Accountable Officer.
11. The PAC will continue to regard me as the main respondent to any enquiries, especially where the
issues are wider than an individual Trust. The Committee may however call other witnesses, and I may
require you to accompany me at a hearing. I shall in any event look to you for support and information
in my dealings with the PAC.
Effective management systems
12. You should ensure that the Trust has in place effective management systems which safeguard public
funds. You should assist the Chairman to implement the requirements of corporate governance as
exemplified in the Codes of Conduct and Accountability. Managers at all levels should:-
have a clear view of their objectives and the means to assess achievements in relation to those
objectives;
be assigned well-defined responsibilities for making the best use of resources;
have the information, training and access to the expert advice they need to exercise their
responsibilities effectively.
Managers should be appraised and held to account for the responsibilities assigned to them under (a)
and (b) above.
13. You are responsible for achieving value for money from the resources available to the Trust, for
avoiding waste and extravagance in the organisation's activities. You are also responsible for following
through the implementation of any recommendations affecting good practice as set out on reports from
such bodies as the Audit Commission and the National Audit Office (NAO).
14. You should provide such information as is requested by the NAO. You should co-operate with external
auditors in any enquiries into the use your trust has made of public funds. I may also ask you to
provide information on any points raised by external auditors which generate public or Parliamentary
interest. Your arrangements for internal audit should comply with those described in the NHS Internal
Audit Manual. You must ensure prompt action is taken in response to concerns raised by both external
and internal audit.
15. Effective and sound financial management and information are of fundamental importance. Whilst this
is the operational responsibility of the Director of Finance you, as the Chief Executive and Accountable
Officer, have a primary duty to see that these functions are properly discharged. As the Chief
Executive of a trading body you are required to ensure the continuing financial viability of the Trust, in
particular to ensure that expenditure is contained within available levels of income, and to achieve any
other financial objectives set by the Secretary of State for Health with the consent of the Treasury, as
appropriate. You should also ensure that the assets of the Trust are properly safeguarded.
Regularity and propriety of expenditure
16. You have a particular responsibility for ensuring that expenditure by the Trust complies with
Parliamentary requirements. The basic principle which must be observed is that funds should be
applied only to the extent and for the purpose authorised by Parliament. You must:-
App
endi
ces
Page 105 of 150
draw the attention of Parliament to losses or special payments by appropriate notation of the
statutory accounts;
obtain sanction from the NHS Executive for any expenditure which exceeds the limit delegated to
the Trust; this includes any novel, contentious or repercussive expenditure, which is by definition
outside your delegation;
ensure that all items of expenditure, including payments to staff, fall within the legal powers of the
Trust, exercised responsibly and with due regard to probity and value for money;
comply with guidance issued by the NHS Executive on classes of payments which you should
authorise personally, such as termination payments to general and senior managers.
17. The Codes of Conduct and Accountability issued to NHS Boards by the Secretary of State under cover
of EL(94)40 on 28 April 1994 are fundamental in exercising your responsibilities for regularity and
probity. As a Board member you have explicitly subscribed to the Codes; you must promote their
observance by all staff.
18. As the Accountable Officer you have a responsibility to see that appropriate advice is tendered to the
Board on all matters of financial probity and regularity, and more broadly on all considerations of
prudent and economical administration, efficiency and effectiveness. The Director of Finance has a
special responsibility to support you in this role; you should ensure that he or she is fully aware of this
obligation and has the requisite skills and experience.
19. If the Board or the Chairman is contemplating a course of action which you consider would infringe the
requirements of propriety and regularity, you should set out in writing to the Chairman and the Board
your objection to the proposal and the reasons for it. If the Board decides nonetheless to proceed, you
should seek a written instruction to take the action in question. You should ensure that the audit
committee, which has specific terms of reference and delegated powers to inquire into matters of
propriety and regularity, and which may require your attendance before it at any time, receives copies
of the documents which describe your objections.
20. You should also inform the NHS Executive, if possible before the Board takes its decision or in any
event before the decision is implemented so that the Executive can if necessary intervene with the
Board and inform the Treasury.
21. If the Board is contemplating a course of action which raises an issue not of formal propriety or
regularity but affects your responsibility for obtaining value for money from the Trust's resources, it is
your duty to draw the relevant factors to the attention of the Board. If the outcome is that you are
overruled it is normally sufficient to ensure that your advice and the overruling of it are clearly apparent
from the papers. If exceptionally you have given clear advice that the course proposed could not
reasonably be held to represent good value for money and the Board seems likely to overrule you, you
should inform the NHS Executive so that it can intervene if necessary. In such cases, and in those
described in paragraph 19 above, the Accountable Officer should as a member of the Board vote
against the course of action rather than merely abstain from voting.
App
endi
ces
Page 106 of 150

App
endi
ces
Page 107 of 150

C O D E O F C O N D U C T F O R N H S B O AR D S
Public service values must be at the heart of the National Health Service. High standards of corporate and
personal conduct based on a recognition that patients come first, have been a requirement throughout the NHS
since its inception. Moreover, since the NHS is publicly funded, it must be accountable to Parliament for the
services it provides and for the effective and economical use of taxpayers’ money. There are three crucial public
service values which must underpin the work of the health service.
Accountability – everything done by those who work in the NHS must be able to stand the test of
parliamentary scrutiny, public judgements on propriety and professional codes of conduct.
Probity – there should be an absolute standard of honesty in dealing with the assets of the NHS: integrity
should be the hallmark of all personal conduct in decisions affecting patients, staff and suppliers, and in the
use of information acquired in the course of NHS duties.
Openness – there should be sufficient transparency about NHS activities to promote confidence between
the NHS organisation and its staff, patients and the public.
General Principles
Public service values matter in the NHS and those who work in it have a duty to conduct NHS business with
probity. Board members must act with due prudence and should take and consider professional advice on
anything in which the board members do not have expertise themselves. They have a responsibility to respond
to staff, patients and suppliers impartially, to achieve value for money from the public funds with which they are
entrusted and to demonstrate high ethical standards of personal conduct. The success of this Code depends on
a vigorous and visible example from boards and the consequential influence on the behaviour of all those who
work within the organisation. Boards have a clear responsibility for corporate standards of conduct and
acceptance of the Code should inform and govern the decisions and conduct of all board directors.
Openness and Public Responsibilities
Health needs and patterns of provision of health care do not stand still. There should be a willingness to be open
with the public, patients and with staff as the need for change emerges. It is a requirement that major changes
are consulted upon before decisions are reached. Information supporting those decisions should be made
available, in a way that is understandable, and positive responses should be given to reasonable requests for
information and in accordance with the Freedom of Information Act 2000. NHS business should be conducted in
a way that is socially responsible. As a large employer in the local community, NHS organisations should forge
an open and positive relationship with the local community and should work with staff and partners to set out a
vision for the organisation in line with the expectations of patients and the public. NHS organisations should
demonstrate to the public that they are concerned with the wider health of the population including the impact of
the organisation’s activities on the environment. The confidentiality of personal and individual patient information
must, of course, be respected at all times.
Public Service Values in Management
It is unacceptable for the board of any NHS organisation, or any individual within the organisation for which the
board is responsible, to ignore public service values in achieving results. Chairs and board directors have a duty
to ensure that public funds are properly safeguarded and that at all times the board conducts its business as
efficiently and effectively as possible. Proper stewardship of public monies requires value for money to be high
on the agenda of all NHS boards.
Accounting, tendering and employment practices within the NHS must reflect the highest professional standards.
Public statements and reports issued by the board should be clear, comprehensive and balanced, and should
fully represent the facts. Annual and other key reports should be issued in good time to all individuals and
groups in the community who have a legitimate interest in health issues to allow full consideration by those
wishing to attend public meetings on local health issues.
Public Business and Private Gain
Chairs and board directors should act impartially and should not be influenced by social or business
relationships. No one should use their public position to further their private interests. Where there is a potential
for private interests to be material and relevant to NHS business, the relevant interests should be declared and
recorded in the board minutes, and entered into a register which is available to the public. When a conflict of
interest is established, the board director should withdraw and play no part in the relevant discussion or decision.
Hospitality and Other Expenditure
Board directors should set an example to their organisation in the use of public funds and the need for good
App
endi
ces
Page 108 of 150

value in incurring public expenditure. The use of NHS monies for hospitality and entertainment, including
hospitality at conferences or seminars, should be carefully considered. All expenditure on these items should be
capable of justification as reasonable in the light of the general practice in the public sector. NHS boards should
be aware that expenditure on hospitality or entertainment is the responsibility of management and is open to be
challenged by the internal and external auditors and that ill-considered actions can damage respect for the NHS
in the eyes of the community.
Relations with Suppliers
NHS boards should have an explicit procedure for the declaration of hospitality and sponsorship offered by, for
example, suppliers. Their authorisation should be carefully considered and the decision should be recorded.
NHS boards should be aware of the risks in incurring obligations to suppliers at any stage of a contracting
relationship. Suppliers should be selected on the basis of quality, suitability, reliability and value for money.
The Department of Health has issued guidance to NHS organisations about Standards of Business Conduct (ref
HSG (93)5).
Staff
NHS boards should ensure that staff have a proper and widely publicised procedure for voicing complaints or
concerns about maladministration, malpractice, breaches of this code and other concerns of an ethical nature.
The board must establish a climate:
that enables staff who have concerns to raise these reasonably and responsibly with the right parties;
that gives a clear commitment that staff concerns will be taken seriously and investigated; and
where there is an unequivocal guarantee that staff who raise concerns responsibly and reasonably will be
protected against victimisation.
(Ref: Whistleblowing in the NHS, letter dated 25 July 2003 from the Director of HR in the NHS)
Compliance
Board directors should satisfy themselves that the actions of the board and its directors in conducting board
business fully reflect the values in this Code and, as far as is reasonably practicable, that concerns expressed by
staff or others are fully investigated and acted upon. All board directors of NHS organisations are required, on
appointment, to subscribe to the Code of Conduct.
App
endi
ces
Page 109 of 150

C O D E O F AC C O U N T AB I L I T Y F O R N H S B O AR D S
This Code of Practice is the basis on which NHS organisations should seek to fulfil the duties and
responsibilities conferred upon them by the Secretary for Health.
Status
NHS authorities and trusts are established under statute as corporate bodies so ensuring that they
have separate legal personality. Statuses and regulations prescribe the structure, functions and
responsibilities of the boards of these bodes and prescribe the way chairman and members of boards
are to be appointed.
Code of Conduct
All board members of NHS authorities and trusts are required, on appointment, to subscribe to the
Code of Conduct. Chairman and non-executive directors of NHS boards are responsible for taking
firm, prompt and fair disciplinary action against any executive director in breach of the Code of
Conduct. Breaches of the Code of Conduct by the chairman or non-executive member of the board
should be drawn to the attention of the non-executive regional Policy Board member.
All staff should subscribe to the principles of the NHS Code of Conduct and chairmen, directors and
their staff should be judged upon the way the code is observed.
Statutory Accountability
The Secretary of State for Health has statutory responsibility for the health of the population of
England and uses statutory powers to delegate functions to NHS authorities and trusts, who are thus
accountable to the Secretary of State and to Parliament. The Chief Executive and NHS Executive are
responsible for directing the NHS, ensuring national policies are implemented and for the effective
stewardship of NHS resources.
NHS Trusts assume responsibility for ownership and management of hospitals or other
establishments or facilities defined in an order transferring them by authority of the Secretary of State
to whom they are accountable through the NHS Executive.
NHS authorities are responsible for procuring health services and administering provision of general
medical, dental ophthalmic and pharmaceutical services in accordance with regulations made by the
Secretary of State to whom they are accountable through the NHS Executive.
NHS authorities and trusts finances are subject to external audit by the Audit Commission. The
chairman and Director of Finance are directly responsible for the organisation’s annual accounts.
NHS Boards must continue to cooperate fully with the NHS Executive and the Audit Commission when
required to account for the use they have made of public funds, the delivery of patient care and other
services, and compliance with statutes, directions, guidance and policies of the Secretary of State.
The Chief Executive of the NHS Executive, as Accounting Officer for the NHS, is accountable to
Parliament through the Committee of Public Accounts.
The Board of Directors
NHS Boards comprise executive board members and part-time non-executive board members under
a part-time chairman appointed by the Secretary of State. Together they share corporate
responsibility for all decisions of the board. There is a clear division of responsibility between the
chairman and the chief executive: the chairman’s role and board functions are set out below; the chief
executive is directly accountable to the chairman and non-executive members of the board for the
operation of the organisation and for implementing the board’s decisions. Boards are required to meet
regularly and to retain full and effective control over the organisation: the chairman and non-executive
board members are responsible for monitoring the executive management of the organisation and are
responsible to the Secretary of State for the discharge of these responsibilities. The NHS Executive
has a key role in maintaining the line of accountability to the Secretary of State. Regional non-
executive members of the Policy Board will always be available to chairmen and non-executive
App
endi
ces
Page 110 of 150

member on matters of grave concern to them relating to the effectiveness of the board.
NHS Boards have six key functions for which they are held accountable by the NHS Executive on
behalf of the Secretary of State:
to set the strategic direction of the organisation within the overall policies and priorities of the
Government and the NHS, define its annual and longer term objectives and agree plans to
achieve them,
to oversee the delivery of planned results by monitoring performance against objectives and
ensuring corrective action is taken when necessary,
to ensure effective financial stewardship through value for money, financial control and
financial planning and strategy,
to ensure that high standards of corporate governance and personal behaviour are maintained
in the conduct of the business of the whole organisation,
to appoint, appraise and remunerate senior executives, and
to ensure that there is effective dialogue between the organisation and the local community on
its plans and performance and that these are responsive to the community’s needs.
In fulfilling these functions the Board should:
specify its requirements in organising and presenting financial and other information succinctly
and efficiently to ensure the board can fully undertake its responsibilities,
be clear what decisions and information are appropriate to the board and draw up standing
orders, a schedule of decisions reserved to the board and standing financial instructions to
reflect this,
established performance and quality targets that maintain the effective use of resources and
provide value for money,
ensure that management arrangements are in place to enable responsibility to be clearly
delegated to senior executives for the main programmes of action and for performance
against programmes to be monitored and senior executives held to account,
establish audit and remuneration committees on the basis of formally agreed terms of
reference which set out the membership of the sub-committee, the limit to their powers, and
the arrangements for reporting back to the main board, and
act within statutory financial and other constraints.
The Role of the Chairman
The chairman is responsible for leading the board and for ensuring that it successfully discharges its
overall responsibility for the organisation as a whole.
It is the chairman’s role to:
provide leadership to the board,
enable all board members to make a full contribution to the board’s affairs and ensure that the
board acts as a team,
ensure that key and appropriate issues are discussed by the board in a timely manner,
ensure the board has adequate support and is provided efficiently with all the necessary data
on which to base informed decisions,
lead non-executive board members through a formally-appointed remuneration committee of
the main board on the appointment, appraisal and remuneration of the chief executive and
(with the latter) other executive board members,
appoint non-executive board members to an audit committee of the main board, and
advise the Secretary of State through the regional member of the Policy Board on the
performance of non-executive board members.
A complementary relationship between the chairman and chief executive is important. The chief
executive is accountable to the chairman and other non-executive members of the board for ensuring
that its decisions are implemented, that the organisation works effectively, in accordance with
Government policy and public service values and for the maintenance of proper financial stewardship.
The chief executive should be allowed full scope, within clearly defined delegated powers, for action in
fulfilling the decisions of the board.
App
endi
ces
Page 111 of 150
Non-executive Board Members
Non-executive board members are appointed by or on behalf of the Secretary of State to bring an
independent judgement to bear on issues of strategy, performance, key appointments and
accountability through the NHS Executive to Ministers and to the local community.
Non-executive board members will be able to contribute to board business from a wide experience
and a critical detachment. They have a key role in working with the chairman in the appointment of
the chief executive and other board members. With the chairman, they comprise the remuneration
committee responsible for the appraisal and remuneration decisions affecting executive board
members. Non-executive board members normally comprise the audit committee.
In addition, they undertake specific functions agreed by the board including functions including
oversight of staff relations with the general public and the media, participation in professional conduct
and competency enquiries, staff disciplinary appeals and procurement of information management
and technology.
Members of NHS authority and trust boards currently play important roles in relation to the handling
and monitoring of non-clinical complaints. Being both informed and impartial, non-executives are able
to act effectively as lay conciliators or adjudicators in relation to individual complaints. With the chief
executive, they can also take responsibility for ensuring that their authority or trust’s complaints
procedures are operated effectively and that lessons learned from them are implemented.
Reporting and Controls
It is the board’s duty to present through the timely publication of an annual report, annual accounts and
other means, a balanced and readily-understood assessment of the authority’s or trust’s performance
to:
the NHS Executive, on behalf of the Secretary of State,
the Audit Commission and its appointed auditors, and
the local community.
The detailed financial guidance issued by the NHS Executive, including the role of internal and
external auditors, must be scrupulously observed. The Standing Orders of boards should prescribe
the terms of which committees and sub-committees of the board may be delegated functions, and
should include the schedule of decisions reserved for the board.
Declaration of Interests
It is a requirement that chairmen and all board members should declare any conflict of interest, that
arises in the course of conducting NHS business. That requirement continues in force. Chairmen and
board members should declare on appointment any business interests, position of authority in a
charity or voluntary body in the field of health and social care and any connection with a voluntary or
other body contracting for NHS services. These should be formally recorded in the minutes of the
board, and entered into a register which is available to the public. Directorships and other significant
interests held by NHS board members should be declared on appointment, kept up to date and set out
in the annual report.
Employee Relations
NHS boards must comply with legislation and guidance from the NHS Executive on behalf of the
Secretary of State, respect agreements entered into by themselves or in on their behalf and establish
terms and conditions of service that are fair to the staff and represent good value for taxpayers’
money. Fair and open competition should be the basis for appointment to posts in the NHS.
The terms and conditions agreed by the board for senior staff should take full account of the need to
obtain maximum value for money for the funds available for patient care. The board should ensure
through the appointment of a remuneration and terms of service committee that executive board
members’ total remuneration can be justified as reasonable. All board members’ total remuneration
for the organisation of which they are a board member should be published in the annual report.
App
endi
ces
Page 112 of 150

App
endi
ces
Page 113 of 150
C O D E O F C O N D U C T F O R N H S M AN AG E R S
As an NHS manager, I will observe the following principles:
make the care and safety of patients my first concern and act to protect them from risk;
respect the public, patients, relatives, carers, NHS staff and partners in other agencies;
be honest and act with integrity;
accept responsibility for my own work and the proper performance of the people I manage;
show my commitment to working as a team member by working with all my colleagues in the NHS and the
wider community;
take responsibility for my own learning and development.
This means in particular that:
1. I will:
respect patient confidentiality;
use the resources available to me in an effective, efficient and timely manner having proper regard to the
best interests of the public and patients;
be guided by the interests of the patients while ensuring a safe working environment;
act to protect patients from risk by putting into practice appropriate support and disciplinary procedures
for staff; and
seek to ensure that anyone with a genuine concern is treated reasonably and fairly.
2. I will respect and treat with dignity and fairness, the public, patients, relatives, carers, NHS staff and partners
in other agencies. In my capacity as a senior manager within the NHS I will seek to ensure that no one is
unlawfully discriminated against because of their religion, belief, race, colour, gender, marital status, disability,
sexual orientation, age, social and economic status or national origin.
I will also seek to ensure that:
the public are properly informed and are able to influence services;
patients are involved in and informed about their own care,
their experience is valued, and they are involved in decisions;
relatives and carers are, with the informed consent of patients, involved in the care of patients;
partners in other agencies are invited to make their contribution to improving health and health services;
and
NHS staff are:
– valued as colleagues;
– properly informed about the management of the NHS;
– given appropriate opportunities to take part in decision making.
– given all reasonable protection from harassment and bullying;
– provided with a safe working environment;
– helped to maintain and improve their knowledge and skills and achieve their potential; and
– helped to achieve a reasonable balance between their working and personal lives.
3. I will be honest and will act with integrity and probity at all times. I will not make, permit or knowingly allow to
be made, any untrue or misleading statement relating to my own duties or the functions of my employer.
I will seek to ensure that:
the best interests of the public and patients/clients are upheld in decision-making and that decisions are
not improperly influenced by gifts or inducements;
NHS resources are protected from fraud and corruption and that any incident of this kind is reported to the
NHS Counter Fraud Services;
judgements about colleagues (including appraisals and references) are consistent, fair and unbiased and
are properly founded; and
open and learning organisations are created in which concerns about people breaking the Code can be
raised without fear.
4. I will accept responsibility for my own work and the proper performance of the people I manage. I will seek to
ensure that those I manage accept that they are responsible for their actions to:
the public and their representatives by providing a reasonable and reasoned explanation of the use of
resources and performance;
patients, relatives and carers by answering questions and complaints in an open, honest and well
researched way and in a manner which provides a full explanation of what has happened, and of what will
App
endi
ces
Page 114 of 150
be done to deal with any poor performance and, where appropriate giving an apology; and
NHS staff and partners in other agencies by explaining and justifying decisions on the use of resources
and give due and proper consideration to suggestions for improving performance, the use of resources and
service delivery.
I will support and assist the Accountable Officer of my organisation in his or her responsibility to answer to
Parliament, Ministers and the Department of Health in terms of fully and faithfully declaring and explaining
the use of resources and the performance of the local NHS in putting national policy into practice and
delivering targets.
For the avoidance of doubt, nothing in paragraphs two to four of this Code requires or authorises an NHS
manager to whom this Code applies to:
make, commit or knowingly allow to be made any unlawful disclosure;
make, permit or knowingly allow to be made any disclosure in breach of his or her duties and obligations
to his or her employer, save as permitted by law.
If there is any conflict between the above duties and obligations and this Code, the former shall prevail.
5. I will show my commitment to working as a team by working to create an environment in which:
teams of frontline staff are able to work together in the best interests of patients;
leadership is encouraged and developed at all levels and in all staff groups; and
the NHS plays its full part in community development.
6 I will take responsibility for my own learning and development.
I will seek to:
take full advantage of the opportunities provided;
keep up to date with best practice; and
share my learning and development with others.
IMPLEMENTING THE CODE
1. The Code should be seen in a wider context that NHS managers must follow the ‘Nolan Principles on
Conduct in Public Life’, the ‘Corporate Governance Codes of Conduct and Accountability’, the ‘Standards of
Business Conduct’, the ‘Code of Practice on Openness in the NHS’ and standards of good employment
practice.
2. In addition many NHS managers come from professional backgrounds and must follow the code of conduct
of their own professions as well as this Code.
In order to maintain consistent standards, NHS bodies need to consider suitable measures to ensure that
managers who are not their employees but who
(i) manage their staff or services; or
(ii) manage units which are primarily providing services to their patients also observe the Code.
3. It is important to respect both the rights and responsibilities of managers.
To help managers to carry out the requirements of the Code, employers must provide reasonable learning
and development opportunities and seek to establish and maintain an organisational culture that values the
role of managers. NHS managers have the right to be:
treated with respect and not be unlawfully discriminated against for any reason;
given clear, achievable targets;
judged consistently and fairly through appraisal;
given reasonable assistance to maintain and improve their knowledge and skills and achieve their
potential through learning and development; and
reasonably protected from harassment and bullying and helped to achieve a reasonable balance
between their working and personal lives.
Breaching the Code
4. Alleged breaches of the Code of Conduct should be promptly considered and fairly and reasonably
investigated. Individuals must be held to account for their own performance, responsibilities and conduct
where employers form a reasonable and genuinely held judgement that the allegations have foundation.
Investigators should consider whether there are wider system failures and organisational issues that have
contributed to the problems. Activity, the purpose of which is to learn from and prevent breaches of the
Code, needs to look at their wider causes.
App
endi
ces
Page 115 of 150

5. Local employers should decide whether to investigate alleged breaches informally or under the terms of
local disciplinary procedures. It is essential however that both forms of investigation should be, and be seen
to be, reasonable, fair and impartial. If Chief Executives or Directors are to be investigated, the employing
authority should use individuals who are employed elsewhere to conduct the investigation. The NHS
Confederation, the Institute of Healthcare Management and the Healthcare Financial Management
Association are among the organisations who maintain lists of people who are willing to undertake such a
role.
Application of Code
6. This Code codifies and articulates certain important contractual obligations that apply to everyone holding
management positions. These include Chief Executives and Directors who as part of their duties are
personally accountable for achieving high quality patient care. The Department of Health will in the next few
months issue a proposed new framework of pay and contractual arrangements for the most senior NHS
managers. Under this framework the job evaluation scheme being developed as part of the ‘Agenda for
Change’ negotiations is likely to be used as the basis for identifying which other managerial posts (in
addition to Chief Executives and Directors) should be automatically covered by the Code. The new
framework will also specify compliance with the Code as one of the core contractual provisions that should
apply to all senior managers.
7. For all posts at Chief Executive/Director level and all other posts identified as in paragraph 6 above, acting
consistently with the Code of Conduct for NHS Managers Directions 2002, employers should:
include the Code in new employment contracts;
incorporate the Code into the employment contracts of existing postholders at the earliest practicable
opportunity.
Action
8. Employers are asked to:
(i) incorporate the Code into the employment contracts of Chief Executives and Directors at the earliest
practicable opportunity and include the Code in the employment contracts of new appointments to that
group;
(ii) identify any other senior managerial posts, i.e. with levels of responsibility and accountability similar to
those of Director-level posts, to which they consider the Code should apply. (The new framework for pay
and contractual arrangements will help more tightly define this group in due course.)
(iii) investigate alleged breaches of the Code by those to whom the Code applies promptly and reasonably
as at paragraphs four to five;
(iv) provide a supportive environment to managers (see paragraph three above).
App
endi
ces
Page 116 of 150
B O AR D O F D I R E C T O R S C O D E O F C O N D U C T
1 Introduction
1.1 Public service values are and must remain at the heart of the National Health Service. High standards
of corporate and personal conduct based on a recognition that patients come first are an essential
component of public services. Moreover, since the NHS is publicly funded it must be accountable to
Parliament for the services it provides and for the effective and economical use of those public funds.
1.3 As an NHS Trust, Southport and Ormskirk NHS Hospital Trust is required to comply with the principles
of best practice applicable to corporate governance in the NHS/health sector and with any relevant
code of practice.
1.4 The expectations of the NHS in respect of standards of corporate conduct are set out in guidance
issued by the Department of Health and in a Code of Conduct and Code of Accountability in the NHS
issued by the Department of Health. This Code is consistent with that guidance and, together with the
Standing Orders, Standing Financial Instructions and Scheme of Reservation and Delegation, forms
part of the framework designed to promote the highest possible standards of conduct and behaviour
within the Trust. The Code applies at all times when directors and employees are carrying out the
business of the Trust or representing the Trust.
2 Principles of Public Life
2.1 All directors and employees are expected to abide by the ‘Nolan’ principles, which are the basis of the
ethical standards expected of public office holders:
Nolan Principles
Selflessness
Holders of public office should act solely in terms of public interest. They should not do so in order to gain
financial or other material benefits for themselves, their family or friends.
Integrity
Holders of public office should not place themselves under any financial or other obligation to outside
individuals or organisations that might seek to influence them in the performance of their official duties.
Objectivity
In carrying out public business, including making public appointments, awarding contracts, recommending
individuals for rewards and benefits, holders of public office should make choices on merit alone.
Accountability
Holders of public office are accountable for their decisions and actions to the public and must submit
themselves to whatever scrutiny is appropriate to their office.
Openness
Holders of public office should be as open as possible about all the decisions and action they take: they
should give reasons for their decisions and restrict information only when the wider public interest clearly
demands.
Honesty
Holders of public office have a duty to declare any private interests relating to their public duties and to
take steps to resolve any conflicts arising in a way that protects the public interest.
Leadership
Holders of the public office should promote and support these principles by leadership and example.
App
endi
ces
Page 117 of 150

2.2 Board members are also expected to comply with the Professional Standards Authority’s ‘Standards for
members of NHS Boards and Clinical Commissioning Group governing bodies in England’. (Appendix
A).
3 General Principles
3.1 NHS Employees have a duty to conduct NHS business with probity, to respond to staff, patients and
suppliers impartially, to achieve value for money from the public funds with which they are entrusted
and to demonstrate high ethical standards of personal conduct. The general duty of the Board of
Directors collectively, and of each Director individually, is to act with a view to promoting the success of
the organisation so as to maximise the benefits for stakeholders as a whole, including the public. The
Board of Directors undertakes to set a vigorous and visible example in the conduct of its business and
to promote the highest corporate standards of conduct. The Board of Directors will lead in ensuring
that the standing orders, standing financial instructions and scheme of reservation and delegation
conform to best practice and serve to enhance standards of conduct. The Board of Directors accepts
its clear responsibility for corporate standards of conduct and expects that this Code will inform and
govern the decisions and conduct of all Board directors.
3.2 Openness and Public Responsibilities
Health needs and therefore health services do not stand still. There should be a willingness to be open
with the public, patients and staff as services develop and change. It is a statutory requirement that
major changes are consulted upon before decisions are reached. Information supporting those
decisions, and other decisions made by the Board of Directors, should be made available in way that is
understandable. Positive responses should be given to reasonable requests for information and in
accordance with the Freedom of Information Act 2000 and other applicable legislation, and directors
and employees must not seek to prevent a person from gaining access to information to which they are
legally entitled.
NHS business should be conducted in a way that is socially responsible. As the largest employee in
the local community the Trust wishes to maintain an open and positive relationship with the local
community and work with staff and partners to set out a vision for the organisation in line with the
expectations of patients and the public. The Trust will seek to demonstrate to the public that it is
concerned with the wider health of the population including the impact of the Trust’s activities on the
environment.
The Trust has adopted policies and procedures to protect confidentiality of personal information and to
ensure compliance with the Data Protection Act, the Freedom of Information Act and other relevant
legislation which will be followed at all times by Board Directors and all staff. Directors and employees
must not disclose any confidential information except in specified lawful circumstances.
3.3 Public Services Values in Management
It is unacceptable for the Board of any NHS organisation, or any individual within the organisation for
which the board is responsible, to ignore public service value in achieving results. Board Members
have a duty to ensure that public funds are properly safeguarded and that at all times the Board
conduct its business as economically, efficiently and effectively as possible – as required by statute.
Accounting, tendering and employment practices within the Trust must therefore reflect the highest
professional standards. Public statements and reports issued by or on behalf of the Board should be
clear, comprehensive and balanced, and should fully represent the facts. Annual and other key reports
should be issued in good time to all individuals and groups in the community who have a legitimate
interest in health issues to allow full consideration by those wishing to attend public meetings on local
health issues.
The standards of conduct expected by the Trust are set out in the Standing Financial Instructions and
accompanying Scheme of Reservation and Delegation which will be followed at all times by Board
directors and all staff.
3.4 Public Business and Private Gain
App
endi
ces
Page 118 of 150

The Chair and Board of Directors should act impartially and not be influenced by social or business
relationships. Directors have a statutory duty to avoid a situation in which they have (or can have) a
direct or indirect interest that conflicts (or may conflict) with the interests of the Trust. None should use
their public position to further their private interests. Where there is potential for private interests to be
material and relevant to NHS business the nature and extent of the relevant interests must be declared
at the earliest opportunity and recorded in the Board minutes and entered into the register of interests
which is available to the public.
When a conflict of interest is established the Board Director must withdraw and play no part in the
relevant discussion or decision. The Chair will advise directors in respect of any conflicts of interest
that arise during Board of Directors meetings, including whether the interest is such that the director
should withdraw from the meeting for the period of the discussion. In the event of disagreement it is for
the Board of Directors to decide whether a director must withdraw from the meeting. The Company
Secretary will provide advice on any conflicts that arise between meetings.
The Standing Orders defines those interests which must be declared by Directors and will be followed
at all times by Board directors and all staff. It is responsibility of each Director to update the register
entry if their interests change. A pro forma is available from the Company Secretary. Failure to register
a relevant interest in a timely manner may constitute a breach of this code.
3.5 Hospitality and Other Expenditure
The Board will set an example in the use of public funds and the need for good value in incurring public
expenditure, including hospitality at conferences or seminars, will be carefully considered. All
expenditure on these items should be capable of justification as reasonable in the light of the general
practice in the public sector. The Board is conscious of the fact that expenditure on hospitality or
entertainment is the responsibility of management and is open to be challenged by the internal and
external auditors and that ill-considered actions can damage the reputation of the Trust and respect for
the NHS in the eyes of the community.
The Board has adopted the Standards of Business Conduct Policy within its Standing Orders which will
be followed at all times by Board directors and all staff. Directors must not accept gifts or hospitality
other than in compliance with this policy and the Trust Policy for the Acceptance of Gifts, Hospitality
and Sponsorship.
3.6 Relations with Suppliers
The Board acknowledges the need for an explicit procedure for the declaration of hospitality and
sponsorship offered by, for example, suppliers. Their authorisation should be carefully considered and
the decisions recorded. The Board is mindful of the risks in incurring obligations to suppliers at any
stage of a contracting relationship. Directors have a statutory duty not to accept a benefit from a third
party by reason of being a Director or for doing (or not doing) anything in that capacity. Suppliers
should be selected on the basis of quality, suitability, reliability and value for money.
The Board has adopted Standing Financial Instructions and the Standards of Business Conduct Policy
which will be followed at all times by Board Directors and all staff.
3.7 Whistleblowing
The Board acknowledges that staff must have a proper and widely publicised procedure for voicing
complaints or concerns about maladministration, malpractice, breaches of this Code and other
concerns of an ethical nature.
The Board has adopted a whistleblowing policy on raising matters of concern which will be followed by
the Board Directors and all staff when invoked.
The Board affirms that:
Staff who have concerns should raise these reasonably and responsibly with the right parties as
identified by the Trust.
The Trust gives a clear commitment that staff concerns will be taken seriously and investigated.
The Trust gives an unequivocal guarantee that staff who raise concerns responsibly and
reasonably in accordance with its policies will be protected against victimisation.
App
endi
ces
Page 119 of 150
4 Code Provisions
4.1 Directors are expected to conduct themselves in a manner that reflects positively on the Trust and not
to conduct themselves in a manner that could reasonably be regarded as bringing the Trust into
disrepute.
Directors must:
Act in the best interests of the Trust and adhere to its values and this Code of conduct.
Uphold the SCOPE values of the Trust (see Appendix B) and ensure that their conduct is at all
times:
Supportive
Caring
Open and Honest
Professional
Efficient
Respect others and treat them with dignity and fairness.
Seek to ensure that no one is unlawfully discriminated against and promote equal opportunities
and social inclusion.
Be honest and act with integrity and probity.
Contribute to the workings of the Board of Directors in order for it to fulfil its role and functions.
Recognise that the Board of Directors is collectively responsible for the exercise of its powers and
the performance of the Trust, but, where appropriate, raise concerns and provide appropriate
challenge regarding the running of the Trust or a proposed action.
Whilst operating as a unitary Board recognise the differing roles of the Chair, Senior Independent
Director, Chief Executive, Executive Directors and Non-Executive Directors.
Make every effort to attend meetings where appropriate.
Adhere to good practice in respect of the conduct of meetings and respect the views of others.
Take and consider advice on issues where appropriate.
Respect the confidentiality of the information they are made privy to as a result of their role as a
director.
Declare any conflict of interest to the Board of Directors as soon as they become aware of it.
Not use their position for personal advantage or seek to gain preferential treatment.
Comply with the Trust’s Standard of Business Policy, as set out in the Standing Orders, in relation
to the acceptance of gifts and hospitality.
Conduct themselves in such a manner as to reflect positively on the Trust, and be ambassadors of
the Trust when attending events in their role as a director.
Accept responsibility for their performance, learning and development.
5 Compliance
App
endi
ces
Page 120 of 150
5.1 The directors of the Board will satisfy themselves that the actions of the Board and its directors in
conducting Board business fully reflect the values, general principles and provisions in this Code and,
as far as is reasonably practicable, that concerns expressed by staff or others are fully investigated and
acted upon.
5.2 All Board directors, on appointment, will be required to subscribe to this Code of Conduct. Compliance
with the Code will be routinely monitored by the Chair and included as part of each Board director’s
annual appraisal.
Declaration:
I, (print name) agree to abide by
the Board of Directors Code of Conduct of Southport & Ormskirk Hospital NHS Trust.
Signature:
Designation:
Date:
App
endi
ces
Page 121 of 150

Appendix A
STANDARDS FOR MEMBERS OF NHS BOARDS AND CLINICAL COMMISSIONING GROUP GOVERNING BODIES IN ENGLAND
All members of NHS Boards and CCG governing bodies should understand and be committed to the practice of
good governance and to the legal and regulatory frameworks in which they operate. As individuals they must
understand both the extent and limitations of their personal responsibilities.
Personal behaviour
1. As a member I commit to:
The values of the NHS Constitution
Promoting equality
Promoting human rights
In the treatment of patients and service users, their families and carers, the community,
colleagues and staff, and in the design and delivery of services for which I am responsible.
2. I will apply the following values in my work and relationships with others:
Responsibility: I will be fully accountable for my work and the decisions that I make, for the
work and decisions of the Board, including delegated responsibilities, and for the staff and
services for which I am responsible
Honesty: I will act with honesty in all my actions, transactions, communications, behaviours
and decision-making, and will resolve any conflicts arising from personal, professional or
financial interests that could influence or be thought to influence my decisions as a Board
member
Openness: I will be open about the reasoning, reasons and processes underpinning my
actions, transactions, communications, behaviours and decision-making and about any
conflicts of interests
Respect: I will treat patients and service users, their families and carers, the community,
colleagues and staff with dignity and respect at all times
Professionalism: I will take responsibility for ensuring that I have the relevant knowledge and
skills to perform as a Board member and that I reflect on and identify any gaps in my
knowledge and skills, and will participate constructively in appraisal of myself and others. I will
adhere to any professional or other codes by which I am bound
Leadership: I will lead by example in upholding and promoting these Standards, and use
them to create a culture in which their values can be adopted by all
Integrity: I will act consistently and fairly by applying these values in all my actions,
transactions, communications behaviours and decision-making, and always raise concerns if I
see harmful behaviour or misconduct by others
To justify the trust placed in med by patients, service users, and the public, I will abide by these Standards
at all times when at the service of the NHS.
I understand that care, compassion and respect for others are central to quality in healthcare; and that the
purpose of the NHS is to improve the health and well-being of patients and service users, supporting them
to keep mentally and physically well, to get better when they are ill and, when they cannot fully recover, to
stay as well as they can to the end of their lives.
I understand that I must act in the interests of patients, service users and the community I serve, and that I
must uphold the law and be fair and honest in all my dealings.
App
endi
ces
Page 122 of 150

Technical competence
3. As a Member, for myself, my organisation, and the NHS, I will seek:
Excellence in clinical care, patient safety, patient experience, and the accessibility of services
To make sound decisions individually and collectively
Long term financial stability and the best value for the benefit of patients, service users and
the community
4. I will do this by:
Always putting the safety of patients and safety users, the quality of care and patient
experience first, and enabling colleagues to do the same
Demonstrating the skills, competencies, and judgement necessary to fulfil my role and
engaging in training, learning and continuing professional development
Having a clear understanding of the business and financial aspects of my organisation’s work
and of the business, financial and legal contexts in which it operates
Making the best use of my expertise and that of my colleagues while working within the limits
of my competence and knowledge
Understanding my role and powers, the legal, regulatory, and accountability frameworks and
guidance within which I operate, and the boundaries between the executive and the non-
executive
Working collaboratively and constructively with others, contributing to discussions, challenging
decisions, and raising concerns effectively
Publicly upholding all decisions taken by the Board under due process for as long as I am a
member of the Board
Thinking strategically and developmentally
Seeking and using evidence as the basis for decisions and actions
Understanding the health needs of the population I serve
Reflecting on personal, Board and organisational performance, and on how my behaviour
affects those around me; and supporting colleagues to do the same
Looking for the impact of decisions on the services we and others provide, on the people who
use them, and on staff
Listening to patients and service users, their families and carers, the community, colleagues,
and staff, and making sure people are involved in decisions that affect them
Communicating clearly, consistently and honestly with patients and service users, their
families and carers, the community, colleagues, and staff, and ensuring that messages have
been understood
Respecting patients’ rights to consent, privacy and confidentiality, and access to information,
as enshrined in data protection and freedom of information law and guidance
Business practices
5. As a member, for myself and my organisation, I will seek:
To ensure my organisation is fit to serve its patients and service users, and the community
To be fair, transparent, measured, and thorough in decision-making and in the management of
public money
To be ready to be held publicly to account for my organisation’s decisions and for its use of
public money
App
endi
ces
Page 123 of 150

6. I will do this by:
Declaring any personal, professional or financial interests and ensuring that they do not
interfere with my actions, transactions, communications, behaviours or decision-making, and
removing myself from decision-making when they might be perceived to do so
Taking responsibility for ensuring that any harmful behaviour, misconduct or systems
weaknesses are addressed and learnt from, and taking action to raise any such concerns that
I identify
Ensuring that effective complaints and whistleblowing procedures are in place and in use
Condemning any practices that could inhibit or prohibit the reporting of concerns by members
of the public, staff, or Board members about standards of care or conduct
Ensuring that patients and service users and their families have clear and accessible
information about the choices available to them so that they can make their own decisions
Being open about the evidence, reasoning and reasons behind decisions about budget,
resource, and contract allocation
Seeking assurance that my organisation’s financial, operational, and risk management
frameworks are sound, effective and properly used, and that the values in these Standards are
put into action in the design and delivery of services
Ensuring that my organisation’s contractual and commercial relationships are honest, legal,
regularly monitored, and compliant with best practice in the management of public money
Working in partnership and co-operating with local and national bodies to support the delivery
of safe, high quality care
Ensuring that my organisation’s dealings are made public, unless there is a justifiable and
properly documented reason for not doing so.
App
endi
ces
Page 124 of 150
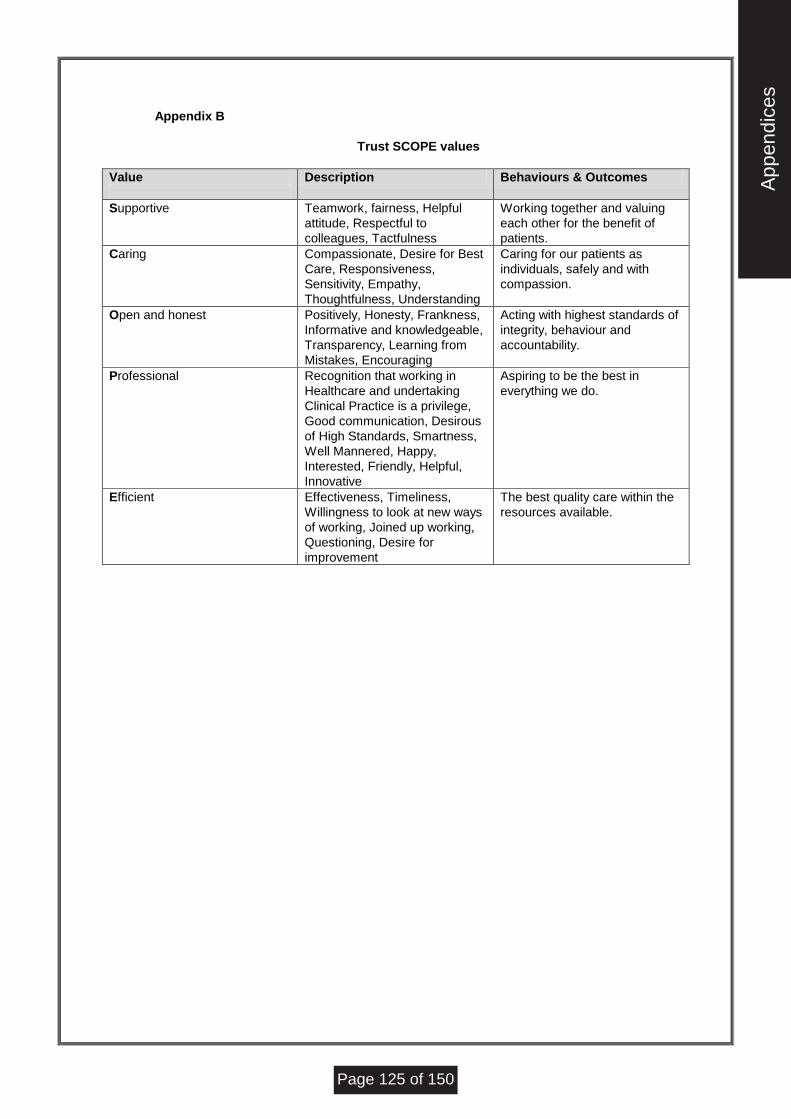
Appendix B
Trust SCOPE values
Value
Description Behaviours & Outcomes
Supportive Teamwork, fairness, Helpful
attitude, Respectful to
colleagues, Tactfulness
Working together and valuing
each other for the benefit of
patients.
Caring Compassionate, Desire for Best
Care, Responsiveness,
Sensitivity, Empathy,
Thoughtfulness, Understanding
Caring for our patients as
individuals, safely and with
compassion.
Open and honest Positively, Honesty, Frankness,
Informative and knowledgeable,
Transparency, Learning from
Mistakes, Encouraging
Acting with highest standards of
integrity, behaviour and
accountability.
Professional Recognition that working in
Healthcare and undertaking
Clinical Practice is a privilege,
Good communication, Desirous
of High Standards, Smartness,
Well Mannered, Happy,
Interested, Friendly, Helpful,
Innovative
Aspiring to be the best in
everything we do.
Efficient Effectiveness, Timeliness,
Willingness to look at new ways
of working, Joined up working,
Questioning, Desire for
improvement
The best quality care within the
resources available.
App
endi
ces
Page 125 of 150

S T AN D AR D S O F B U S I N E S S C O N D U C T F O R N H S S T AF F
Whilst the Standards for Business Conduct for NHS Staff remain in place since its publication some of the
offences referred to have been superseded by more recent legislation. These standards should therefore be
read in conjunction with the Staff Code of Personal and Business Conduct for more up-to-date advice and
guidance.
Executive Summary
To assist NHS employers and staff in maintaining strict ethical standards in the conduct of NHS business, the
Management Executive has prepared the attached guidance:-
Brief summary of the main provisions of the Prevention of Corruption Acts 1906 and 1916 - Part A.
General policy guidelines - Part B.
These cover:-
the standards of conduct expected of all NHS staff where their private interests may conflict with
their public duties; and
the steps which NHS employers should take to safeguard themselves and the NHS against conflict
of interest.
Action checklist for NHS Managers -Part C. (omitted from this extract)
Short guide for staff - Part D.
Ethical Code of the Institute of Purchasing and Supply (IPS) (reproduced courtesy of IPS) - Part E.
Action
NHS authorities and Trusts should:-
ensure that these guidelines are brought to the attention of all staff, and are effectively
implemented;
develop local conflict of interest policies and the machinery to implement them, in consultation with
staff and local staff representatives;
satisfy themselves that their policies and implementation procedures are regularly reviewed and
kept up to date.
Part A
Prevention of Corruption Acts 1906 - summary of main provisions
Acceptance of gifts by way of inducements or rewards Under the Prevention of Corruption Acts, 1906 and
1916, it is an offence for employees corruptly to accept any gifts or consideration as an inducement or reward
for:-
doing, or refraining from doing, anything in their official capacity; or
showing favour or disfavour to any person in their official capacity.
Under the Prevention of Corruption Act 1916, any money, gift or consideration received by an employee in public
service from a person or organisation holding or seeking to obtain a contract will be deemed by the courts to
have been received corruptly unless the employee proves the contrary.
Part B1
NHS Management Executive (NHSME) - general guidelines
Introduction
App
endi
ces
Page 126 of 150

These guidelines, which are intended by the NHSME to be helpful to all NHS employers and their employees, re-
state and reinforce the guiding principles previously set out in Circular HM(62)21 (now cancelled), relating to the
conduct of business in the NHS.
Responsibility of NHS employers
NHS employers are responsible for ensuring that these guidelines are brought to the attention of all employees;
also that machinery is put in place for ensuring that they are effectively implemented.
Responsibility of NHS staff
It is the responsibility of staff to ensure that they are not placed in a position which risks, or appears to risk,
conflict between their private interests and their NHS duties. This primary responsibility applies to all NHS staff,
i.e. those who commit NHS resources directly (e.g. by the ordering of goods) or those who do so indirectly (e.g.
by the prescribing of medicines). A further example would be staff who may have an interest in a private nursing
home and who are involved with the discharge of patients to residential facilities.
Guiding principle in conduct of public business
It is a long established principle that public sector bodies, which include the NHS, must be impartial and honest
in the conduct of their business, and that their employees should remain beyond suspicion. It is also an offence
under the Prevention of Corruption Acts 1906 and 1916 for an employee corruptly to accept any inducement or
reward for doing, or refraining from doing anything, in his or her official capacity, or corruptly showing favour, or
disfavour, in the handling of contracts (see Part A).
Staff will need to be aware that a breach of the provisions of these Acts renders them liable to prosecution and
may also lead to loss of their employment and superannuation rights in the NHS.
Principles of conduct in the NHS
NHS staff are expected to:-
ensure that the interest of patients remains paramount at all times;
be impartial and honest in the conduct of their official business;
use the public funds entrusted to them to the best advantage of the service, always
ensuring value for money.
It is also the responsibility of staff to ensure that they do not:-
abuse their official position for personal gain or to benefit their family or friends;
seek to advantage or further private business or other interests, in the course of their
official duties.
Implementing the guiding principles
Casual gifts
Casual gifts offered by contractors or others, e.g.) at Christmas time, may not be in any way connected with the
performance of duties so as to constitute an offence under the Prevention of Corruption Acts. Such gifts should
nevertheless be politely but firmly declined. Articles of low intrinsic value such as diaries or calendars, or small
tokens of gratitude from patients or their relatives, need not necessarily be refused. In cases of doubt staff
should either consult their line manager or politely decline acceptance.
Hospitality
Modest hospitality provided it is normal and reasonable in the circumstances, e.g.) lunches in the course of
working visits, may be acceptable, though it should be similar to the scale of hospitality which the NHS as an
employer would be likely to offer.
Staff should decline all other offers of gifts, hospitality or entertainment. If in doubt they should seek advice from
their line manager.
App
endi
ces
Page 127 of 150

Declaration of interests
NHS employers need to be aware of all cases where an employee, or his or her close relative or associate, has
a controlling and/or significant financial interest in a business (including a private company, public sector
organisation, other NHS employer and/or voluntary organisation), or in any other activity or pursuit, which may
compete for an NHS contract to supply either goods or services to the employing authority.
All NHS staff should therefore declare such interests to their employer, either on starting employment or on
acquisition of the interest, in order that it may be known to and in no way promoted to the detriment of either the
employing authority or the patients whom it serves.
One particular area of potential conflict of interest which may directly affect patients, is when NHS staff hold a
self beneficial interest in private care homes or hostels. While it is for staff to declare such interests to their
employing authority, the employing authority has a responsibility to introduce whatever measures it considers
necessary to ensure that its interests and those of patients are adequately safeguarded. This may for example
take the form of a contractual obligation on staff to declare any such interests. Advice on professional conduct
issued by the General Medical Council recommends that when a doctor refers a patient to a private care home
or hostel in which he or she has an interest, the patient must be informed of that interest before referral is made.
In determining what needs to be declared, employers and employees will wish to be guided by the principles set
out in paragraph 5 above, also the more detailed guidance to staff contained in Part D.
NHS employers should:-
ensure that staff are aware of their responsibility to declare relevant interests (perhaps by
including a clause to this effect in staff contracts:;
consider keeping registers of all such interests and making them available for inspection
by the public;
develop a local policy, in consultation with staff and local staff interests, for implementing
this guidance. This may include the disciplinary action to be taken if an employee fails to
declare a relevant interest, or is found to have abused his or her official position, or
knowledge, for the purpose of self-benefit, or that of family or friends.
Preferential treatment in private transactions
Individual staff must not seek or accept preferential rates or benefits in kind for private transactions carried out
with companies with which they have had, or may have, official dealings on behalf of their NHS employer. (This
does not apply to concessionary agreements negotiated with companies by NHS management, or by recognised
staff interest, on behalf of all staff - for example, NHS staff benefits schemes.)
Contracts
All staff who are in contact with suppliers and contractors (including external consultants), and in particular those
who are authorised to sign Purchase Orders, or place contracts for goods, materials or services, are expected to
adhere to professional standards of the kind set out in the Ethical Code of the Institute of Purchasing and Supply
(IPS), reproduced at Part E.
Favouritism in awarding contracts
Fair and open competition between prospective contractors or suppliers for NHS contracts is a requirement of
NHS Standing Orders and of EC Directives on Public Purchasing for Works and Supplies. This means that:-
no private, public or voluntary organisation or company which may bid for NHS business
should be given any advantage over its competitors, such as advance notice of NHS
requirements. This applies to all potential contractors, whether or not there is a
relationship between them and the NHS employer, such as a long-running series of
previous contracts;
each new contract should be awarded solely on merit, taking into account the
requirements of the NHS and the ability of the contractors to fulfil them.
NHS employers should ensure that no special favour is shown to current or former employees or their close
relatives or associates in awarding contracts to private or other businesses run by them or employing them in a
senior or relevant managerial capacity. Contracts may be awarded to such businesses where they are won in
App
endi
ces
Page 128 of 150

fair competition against other tenders, but scrupulous care must be taken to ensure that the selection process is
conducted impartially, and that staff who are known to have a relevant interest play no part in the selection.
Warnings to potential contractors
NHS employers will wish to ensure that all invitations to potential contractors to tender for NHS business include
a notice warning tenderers of the consequences of engaging in any corrupt practices involving employees of
public bodies.
Outside employment
NHS employees are advised not to engage in outside employment which may conflict with their NHS work, or be
detrimental to it. They are advised to tell their NHS employing authority if they think they may be risking a
conflict of interest in this area: the NHS employer will be responsible for judging whether the interests of patients
could be harmed, in line with the principles of conduct in the NHS noted above. NHS employers may wish to
consider the preparation of local guidelines on this subject.
Private practice
Consultants (and associate specialists) employed under the Terms and Conditions of Service of Hospital
Medical and Dental Staff are permitted to carry out private practice in NHS hospitals subject to the conditions
outlined in the handbook (A Guide to the Management of Private Practice in the NHS”. (See also PM(79)11).
Consultants who have signed new contracts with Trusts will be subject to the terms applying to private practice
in those contracts.
Other grades may undertake private practice or work for outside agencies, providing they do not do so within the
time they are contracted to the NHS, and they observe the conditions in paragraph 20 above. All hospital
doctors are entitled to fees for other work outside their NHS contractual duties under “Category 2” (paragraph 37
of the TCS of Hospital Medical and Dental staff) e.g.) examinations and reports for life insurance purposes.
Hospital doctors and dentists in training should not undertake locum work outside their contracts where such
work would be in breach of their contracted hours. Career grade medical and dental staff employed by NHS
Trusts may agree terms and conditions different from the National Terms and Conditions of Service.
Rewards for Initiative
NHS employers should ensure that they are in a position to identify potential intellectual property rights (IPR), as
and when they arise, so that they can protect and exploit them properly, and thereby ensure that they receive
any rewards or benefits (such as royalties) in respect of work commissioned from third parties, or work carried
out by their employees in the course of their NHS duties. Most IPR are protected by statute; e.g.) patents are
protected under the Patents Act 1977 and copyright (which includes software programmes) under the Copyright
Designs and Patents Act 1988. To achieve this NHS employers should build appropriate specifications and
provisions into the contractual arrangements which they enter into before the work is commissioned, or begins.
They should always seek legal advice if in any doubt in specific cases.
With regard to patents and inventions, in certain defined circumstances the Patents Act gives employees a right
to obtain some reward for their efforts, and employers should see that this is affected. Other rewards may be
given voluntarily to employees who within the course of their employment have produced innovative work of
outstanding benefit to the NHS. Similar rewards should be voluntarily applied to other activities such as giving
lectures and publishing books and articles.
In the case of collaborative research and evaluative exercises with manufacturers, NHS employers should see
that they obtain a fair reward for the input they provide. If such an exercise involves additional work for an NHS
employee outside that paid for by the NHS employer under his or her contract of employment, arrangements
should be made for some share of any rewards or benefits to be passed on to the employee(s) concerned from
the collaborating parties. Care should however be taken that involvement in this type of arrangement with a
manufacturer does not influence the purchase of other supplies from that manufacturer.
Commercial sponsorship for attendance at courses and conferences
Acceptance by staff of commercial sponsorship for attendance at relevant conferences and courses is
acceptable, but only where the employee seeks permission in advance and the employer is satisfied that
acceptance will not compromise purchasing decisions in any way.
App
endi
ces
Page 129 of 150

On occasions when NHS employers consider it necessary for staff advising on the purchase of equipment to
inspect such equipment in operation in other parts of the country (or exceptionally, overseas), employing
authorities will themselves want to consider meeting the cost, so as to avoid putting in jeopardy the integrity of
subsequent purchasing decisions.
Commercial sponsorship of posts - “linked deals”
Pharmaceutical companies, for example, may offer to sponsor, wholly or partially, a post for an employing
authority. NHS employers should not enter into such arrangements, unless it has been made abundantly clear
to the company concerned that the sponsorship will have no effect on purchasing decisions within the authority.
Where such sponsorship is accepted, monitoring arrangements should be established to ensure that purchasing
decisions are not, in fact, being influenced by the sponsorship agreement.
Under no circumstances should employers agree to “linked deals” whereby sponsorship is linked to the
purchase of particular products, or to supply from particular sources.
“Commercial in-confidence”
Staff should be particularly careful of using, or making public, internal information of a “commercial in-
confidence” nature, particularly if its disclosure would prejudice the principle of a purchasing system based on
fair competition. This principle applies whether private competitors or other NHS providers are concerned, and
whether or not disclosure is prompted by the expectation of personal gain (see paragraphs 16 18 above and
Part E).
However, NHS employers should be careful about adopting a too restrictive view on this matter. It should
certainly not be a cause of excessive secrecy on matters which are not strictly commercial per se. For example,
the term “commercial in confidence” should not be taken to include information about service delivery and
activity levels, which should be publicly available. Nor should it inhibit the free exchange of data for medical
audit purposes, for example, subject to the normal rules governing patient confidentiality and data protection. In
all circumstances the overriding consideration must be the best interests of patients.
Part C – Action checklist for NHS Managers (Omitted from this extract)
Part D
Short guide for staff
References are to paragraphs in Part B of “Standards of business conduct for NHS staff” (Annex to HSG(93)5).
Do:-
make sure you understand the guidelines on standards of business conduct, and consult your line
managers if you are not sure;
make sure you are not in a position where your private interests and NHS duties may conflict (3);
declare to your employer any relevant interests (10-14). If in doubt, ask yourself:-
i. am I, or might I be, in a position where I (or my family/friends) could gain from the connection
between my private interests and my employment?
ii. do I have access to information which could influence purchasing decisions?
iii. could my outside interest be in any way detrimental to the NHS or to the patients’ interests?
iv. do I have any other reasons to think I may be risking a conflict of interest?
If still unsure - Declare it!
adhere to the ethical code of the Institute of Purchasing and Supply if you are involved in any way with the
acquisition of goods and services (16);
seek your employer’s permission before taking on outside work, if there is any question of it adversely
affecting your NHS duties (20). (Special guidance applies to doctors);
obtain your employer’s permission before accepting any commercial sponsorship (26).
Do not:-
accept any gifts, inducements or inappropriate hospitality (see 7 - 9);
abuse your past or present official position to obtain preferential rates for private deals (15);
unfairly advantage one competitor over another (17) or show favouritism in awarding contracts (18);
misuse or make available official “commercial in confidence” information (29).
App
endi
ces
Page 130 of 150

Part E
Institute of Purchasing and Supply - Ethical Code (Reproduced by kind permission of IPS)
Introduction
The code set out below was approved by the Institute’s Council on 26th
February 1977 and is building on IPS
members.
Precepts
Members shall never use their authority or office for personal gain and shall seek to uphold and enhance the
standing of the Purchasing and Supply profession and the Institute by:-
a) maintaining an unimpeachable standard of integrity in all their business relationships both inside
and outside the organisations in which they are employed;
b) fostering the highest possible standards of professional competence amongst those for whom they
are responsible;
c) optimising the use of resources for which they are responsible to provide the maximum benefit to
their employing organisation;
d) complying both with the letter and the spirit of:-
i. the law of the country in with they practice;
ii. such guidance on professional practice as may be issued by the Institute from
time to time;
iii. contractual obligations.
e) rejecting any business practice which might reasonably be deemed improper.
Guidance
In applying these precepts, members should follow the guidance set out below:-
Declaration of interest. Any personal interest which may impinge or might reasonably be deemed
by others to impinge on a member’s impartiality in any matter relevant to his or her duties should
be declared.
Confidentiality and accuracy of information. The confidentiality of information received in the
course of duty should be respected and should never be used for personal gain; information given
in the course of duty should be true and fair and never designed to mislead.
Competition. While bearing in mind the advantages to the member’s employing organisation of
maintaining a continuing relationship with a supplier, any relationship which might, in the long term,
prevent the effective operation of fair competition, should be avoided.
Business gifts. Business gifts other than items of very small intrinsic value such as business
diaries or calendars should not be accepted.
Hospitality. Modest hospitality is an accepted courtesy of a business relationship. However, the
recipient should not allow him or herself to reach a position whereby he or she might be deemed by
others to have been influenced in making a business decision as a consequence of accepting such
hospitality; the frequency and scale of hospitality accepted should not be significantly greater than
the recipient’s employer would be likely to provide in return.
When it is not easy to decide between what is and is not acceptable in terms of gifts or hospitality,
the offer should be declined or advice sought from the member’s superior.
App
endi
ces
Page 131 of 150
STAFF CODE OF PERSONAL AND BUSINESS CONDUCT
1. INTRODUCTION
1.1 Scope
a) The purpose and aim of this Code of Conduct is to raise awareness and provide guidance
regarding the standards of personal and business conduct and behaviour that Southport and
Ormskirk Hospital NHS Trust (‘the Trust’) expects from all of those working for it.
b) Consequently, this Code applies to all staff and volunteers, regardless of role or position, and
forms part of the Trust’s corporate governance arrangements. It should be seen as
complementary to local or departmental procedures or codes, which may give more detailed
guidance, as well to relevant professional codes of conduct.
c) The Code is consistent with other Trust policies and rules including the Trust’s Standing
Orders and Financial Instructions. Staff should make themselves aware of other such policies.
d) The Trust Code supplements the NHS Code of Conduct for Managers (2002), as well as
endorsing and updating the NHS Standards of Business Conduct (1993) which are applicable
to all NHS personnel. Staff should familiarise themselves with these documents, which are
available at:
http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidanc
e/DH_4005410 (NHS Code of Conduct for Managers)
http://www.dh.gov.uk/en/PublicationsAndStatistics/LettersAndCirculars/HealthServiceGuidelin
es/DH_4017845 (NHS Standards of Business Conduct)
1.2 Principles
Staff are reminded of the Committee on Standards in Public Life's First Report which established The
Seven Principles of Public Life, also known as the ‘Nolan principles’. These over-arching principles
underpin this Code and apply to all aspects of public life and to all those who serve the public in any
way. These are: Selflessness; Integrity; Objectivity; Accountability; Openness; Honesty; and,
Leadership.
Staff should also observe the more specific principles set out in the 2004 NHS Code of Conduct for
Managers, but which are relevant to all NHS personnel. These are included in the following:
a) Make the care and safety of others your primary concern and act to protect them from risk or
harm.
b) Respect and safeguard the interests of others in all that you do.
c) Act as a positive ambassador for, and representative of, the Trust and NHS at all times.
d) Be honest and act with integrity at all times, justifying public trust and confidence;
e) Accept responsibility for your own work and proper performance and (where appropriate) for
that of line managed staff;
f) Show commitment to working as a team member by working with all colleagues in the Trust,
the NHS, and the wider community; and,
App
endi
ces
Page 132 of 150
g) Take responsibility for personal learning and development.
Staff are to uphold the SCOPE values of the Trust and ensure that their conduct is at all times:
Supportive
Caring
Open and Honest
Professional
Efficient
2. IMPLEMENTATION
a) Implementation of the Code will be supported through a variety of communication
mechanisms, including team briefings and departmental communications.
b) All new employees will receive a copy of the Code within Induction information and further
advice will be provided by departmental managers.
c) Staff who have questions regarding the Code, or require more detailed guidance, are advised
to contact their manager or the Company Secretary.
d) The Trust acknowledges that this Code cannot spell out appropriate conduct and behaviour
for every possible situation. However, staff are expected to make informed judgements about
what is right and proper using the information and principles contained within this Code as a
basis.
e) Failure to meet the standards and requirements of this Code may result in disciplinary action
against an employee, or action for breach of their employment contract. In some instances,
breaches of this Code may also equate to criminal offences and the Trust’s Counter Fraud
Specialist or other relevant authorities may be notified.
f) Staff have an obligation to report suspected breaches of this Code. The Trust is an open and
learning organisation in which concerns about people breaking the Code can be raised without
fear.
g) For the avoidance of doubt, nothing in this Code requires or authorises an NHS employee to
whom this Code applies to:
Make, commit or knowingly allow to be made any unlawful disclosure;
Make, permit or knowingly allow to be made any disclosure in breach of his or her
duties and obligations to his or her employer, save as permitted by law.
If there is any conflict between the above duties and obligations and this Code, the former
shall prevail.
3. CODE OF CONDUCT
The following standards of conduct are expected of all staff and volunteers.
3.1. Act always in such a manner as to promote and safeguard the interests and well being of
patients, relatives, carers, members of the public and Trust colleagues.
3.2. Always treat patients with the dignity and respect they deserve.
3.3. Respect patient confidentiality at all times.
App
endi
ces
Page 133 of 150
3.4. Uphold and enhance the good standing, reputation and interests of the Trust in the provision
of services to the local community and beyond;
3.5. Ensure that no action or omission on your part, or within your sphere of work, is detrimental to
the interests, condition or safety of patients.
3.6. Decline any duties or responsibilities unless you are able to perform them in a safe manner.
Ensure your manager is notified in such circumstances.
3.7. Adopt a pro-active, responsible and co-operative attitude towards Health and Safety and take
every reasonable precaution to avoid personal injury and injury to patients, relatives, carers,
members of the public and Trust colleagues. (Health & Safety Policy)
3.8. Use the Trust and NHS resources available to you in an effective, efficient and timely manner,
having proper regard to the best interests of patients.
3.9. Accept responsibility for your own work and performance, and for all your decisions and
actions in relation to your duties and responsibilities.
3.10. Ensure that all decisions are made fairly without bias, prejudice or adverse influence.
3.11. Work in a collaborative and co-operative manner with health care professional staff and
colleagues, recognising and respecting their particular skills, supporting the right of all people
to be treated with dignity and respect at work.
3.12. Ensure that no-one you come into contact with in the course of your work receives less
favourable treatment, or is victimised or harassed, on the grounds of race, creed, colour,
ethnic origin, gender, disability, marital status, sexual orientation, age, religion or any other
unjustifiable grounds.
3.13. Be aware of and respect the customs, values and spiritual beliefs of patients and colleagues.
3.14. Where it is possible to influence, ensure that your colleagues are:
Valued;
Properly informed;
Given opportunities to take part in decision-making;
Helped to maintain and improve their knowledge and skills and to achieve their
potential; and,
Helped to achieve a reasonable balance between their working and personal lives.
3.15. Take responsibility for your own learning and development by keeping up to date with
mandatory training, seeking to take full advantage of the opportunities provided; keeping up to
date with best practice; and sharing learning and development with others.
3.16. Seek to ensure that anyone with a genuine concern is treated reasonably and fairly.
3.17. Avoid any abuse of the privileged relationship which exists with patients and of the privileged
access allowed to their person, property or residence.
3.18. Refuse politely to accept any gift, favour or hospitality from patients, carers or any other party
which might be interpreted as seeking to exert undue influence to obtain preferential
consideration. Staff should not accept significant personal gifts or hospitality from contractors
and outside suppliers. (see Appendix 1, NHS Standards of Business Conduct)
App
endi
ces
Page 134 of 150
3.19. Be aware of the potential for conflict of interests between private obligations outside work and
the requirements of your NHS role. (see Appendix 1, NHS Standards of Business Conduct)
3.20. Be alert to any conduct or behaviour which may constitute criminal offences against the
Trust’s assets or resources, such as fraud, bribery or corruption, and report your concerns or
suspicions appropriately. (see Anti Fraud and Bribery Policy)
3.21. Act with honesty and integrity and do not make, permit or knowingly allow to be made, any
untrue or misleading statement relating to your own duties or activities, or to any of the
functions or services of Trust.
3.22. Respect confidential information obtained in the course your work and refrain from disclosing
such information without the consent of the data controller, or a person entitled to act on their
behalf (except where a disclosure is required under the terms of the relevant safeguarding
procedures, or by law, or by the order of a court, or is a qualifying disclosure made in
accordance with the Public Interest Disclosure Act 1998).
3.23. Be aware of the potential to provide good role models for health promotion in the community.
Specifically, be aware of and comply with the following policy(ies):
Alcohol, Drugs and Substance Misuse Policy.
3.24. Dress in a manner that is consistent with the requirements of your job, utilising uniforms
and/or protective clothing when provided, ensuring safety for patients and other staff and
presenting a good public image of yourself and the Trust.
3.25. Through agreed procedures and without fear of recrimination, bring to the attention of the
appropriate level of management any deficiency in the provision of service, impropriety or
breach of procedure.
3.26. Be aware of, and adhere to, current Trust policies and procedures relevant to your sphere of
work, as well as corporately.
3.27. Be punctual, both in starting work on time and in returning from breaks.
Further specific guidance is contained in Appendix 1.
4. MONITORING AND COMPLIANCE
The HR Department will monitor those matters which are brought to their attention. Other departments
and colleagues will be duly notified where matters relate to their areas of responsibility.
5. REVIEW
This Code of Conduct will be reviewed by the Company Secretary within 2 years of ratification by the
Audit Committee. It may be reviewed at an earlier date to update it in line with employment law or good
practice.
6. REFERENCES
Code of Conduct for NHS Managers, DoH 2002
NHS Standards of Business Conduct, DoH 1993, [HSG (93)5]
Code of Conduct: Code of Accountability in the NHS, DoH 2004
Trust Governance Manual
Gifts & Hospitality Policy
App
endi
ces
Page 135 of 150

Declaration of Interests Policy
Dignity at Work Policy
Alcohol and Substance Misuse Policy
Disciplinary Policy
Health & Safety Policy
Anti Fraud & Bribery Policy
Whistleblowing Policy
App
endi
ces
Page 136 of 150

Appendix 1
NHS STANDARDS OF BUSINESS CONDUCT [HSG (93)5] - STAFF GUIDANCE
Scope of Responsibility
This section refers to the requirements contained within the 1993 NHS Standards of Business
Conduct [HSG (93)5] which remains in force and which all Trust staff and volunteers are expected to
familiarise themselves with and adhere to. Indeed, for many NHS bodies, compliance with these
standards forms part of the employee’s contract of employment.
It is the responsibility of all Trust staff and volunteers to personally ensure that they are not, by their
conduct or actions, placed in a position which risks, or appears to risk, conflict between their private
interests and their NHS duties and responsibilities.
Staff and volunteers should also be aware that the behaviour of immediate family members and
partners (either personal or business) could also create potential conflicts.
Interests may be financial or non-financial (i.e. political or religious). Similarly, the receipt of gifts or
hospitality may not be conducive to NHS roles and requirements.
Guiding Principle in the Conduct of Public Business
The NHS, along with other public sector bodies, must be fair, impartial and honest in the conduct of
business and decision-making and therefore, staff should act with probity, integrity and transparency at
all times, remaining beyond suspicion.
Clarifications to the 1993 NHS Standards of Business Conduct
The Business Standards were first issued in 1993 and much has changed in the NHS and beyond
since then, not least the introduction of relevant, new legislation relating to Fraud and Bribery. This
section updates guidance relating to the original Standards document and makes reference to the new
legislation which must also be considered when reviewing compliance against the requirements
contained in the Business Standards.
Parts A & B
Bribery Act 2010
For any relevant activities undertaken prior to 1st July 2011, the Standards state that it is an offence
under the Prevention of Corruption Acts 1906 and 1916 for an employee to accept an inducement or
reward for doing, or refraining from doing anything in his or her official capacity, or corruptly showing
favour or disfavour in the handling of contracts.
From the 1st July 2011, such activities undertaken by anyone associated with the Trust would now be
offences under the more extensive Bribery Act 2010. This Act creates a number of specific offences
including:
the offering, promising or giving a bribe;
the requesting, agreeing to receive or accepting a bribe;
bribing a foreign public official;
the new corporate offence for commercial organisations (including NHS bodies) where they fail to
prevent bribery by those acting on their behalf.
A bribe may be defined as “an inducement or reward offered, promised or provided to someone
to perform their functions or activities improperly in order to gain a personal, commercial,
regulatory and/or contractual advantage.”
A bribe may take the form of payment, gifts, hospitality, promise of contracts or employment, or some
App
endi
ces
Page 137 of 150

other form of benefit or gain. The individuals engaged in the actual bribery activity do not have to be
those who instigate the offence(s), or ultimately benefit from it. All parties involved are potentially
subject to prosecution.
Paragraphs 7, 8 and 15 to 19 of Part B of the Business Standards expressly relate to areas of NHS
functions and activity where breaches may lead to prosecution for potential bribery or corruption-
related offences.
Fraud Act 2006
In January 2007, the Fraud Act 2006 came into force. This introduced new, specific fraud offences.
Consequently, a person is guilty of fraud if he/she is in breach of any of the following, which provide
the three main ways of committing the offence:
Fraud by false representation;
Fraud by failing to disclose information;
Fraud by abuse of position.
For example, failing to disclose information (such as a conflicting personal business or outside
interest) when under a legal obligation to do so (as may be required by an NHS contract of
employment) may constitute a fraud offence. Paragraphs 10 to 14 and 20 of the Business Standards
(Part B) expressly relate to the requirement of NHS staff to declare all relevant interests.
Similarly, as noted in Paragraphs 6 and 29 of Part B, using commercially confidential NHS information
for private gain (either by oneself or another) could also constitute a criminal abuse of position offence
under the Fraud Act.
Summary
Staff should be aware that a breach of any provision of the Acts referred to above renders them
potentially liable for prosecution and may also lead to disciplinary action, as well as loss of
employment and pension rights in the NHS.
Offences under both the Fraud Act 2006 and the Bribery Act 2010 carry sanctions including up to 10
years imprisonment and/or an unlimited fine.
In addition, those in the public sector should be mindful that additional sanctions are also occasionally
brought under the common law offence of Misconduct in Public Office, which also carries a potential
10 year sentence.
Further advice and guidance on fraud, bribery or corruption may be obtained from the Trust’s Local
Counter Fraud Specialist and reference may also be made to the Trust’s Anti Fraud and Bribery
Policy.
The paragraph references in Parts A and B of the Business Standards referred to above should not be
considered definitive or exhaustive and any potential breach of any of the principles and requirements
contained in the Standards of Business Conduct would be reviewed on a case-by-case basis to
identify which offences (under various Acts) may or may not have been committed.
What Staff Should Do:
Make sure you understand the guidelines; consult your line manager if you are not sure.
Adhere to the ethical code of the Institute of Purchasing and Supply if you are involved in any
way with the acquisition of goods and services.
Make sure you are not in a position where your private interests and NHS duties may conflict.
Declare to your employer any relevant interests.
Seek your employer’s permission before taking on other employment which may adversely
affect your ability to fulfil your NHS employment obligations or which conflict (or may be seen
to conflict) with your obligation to the Trust.
Refuse and report any gifts or hospitality which is either inappropriate, excessive or which
could be seen to compromise or influence your judgement and or NHS duties.
App
endi
ces
Page 138 of 150

The Trust maintains Registers of Interests and Gifts/Hospitality and it is the personal
responsibility of each member of staff to notify any relevant interests/activities and report any offer
of hospitality or gifts accordingly.
If In Doubt, Ask Yourself…
Am I, or might I be, in a position where, I, or my family/friends/partner, could gain from the
connection between my interests and my NHS employment?
Do I have access to information which could influence purchasing decisions?
Could my outside interests be in any way detrimental to the Trust or to patient interests?
Do I have any other reason to think I may be risking a conflict of interest?
If I read about my private interest, or my receipt of a gift or hospitality, in a newspaper would I
feel embarrassed about it? (The Newspaper Test)
If you are still unsure – Declare It!
Do Not:
Accept any inappropriate gift or hospitality. (There may be circumstances where modest
hospitality and casual gifts are acceptable – seek advice from your line manager). Staff should
refer to the Gifts and Hospitality policy.
Abuse your NHS position to obtain preferential treatment for yourself, family or friends.
Unfairly advantage one competitor over another or show favouritism awarding contracts.
Misuse, make available or make inappropriate reference to official ‘commercial’ or ‘‘in
confidence’ information.
App
endi
ces
Page 139 of 150

CODE OF CONDUCT FOR PAYMENT BY RESULTS
Introduction - the purpose of the Code of Conduct
1. The effective implementation of Payment by Results (PbR) will depend on constructive relationships
between all parties operating within the system.
2. PbR introduces a degree of transparency in NHS financial flows that is almost unprecedented. The new
system challenges organisations to manage successfully in a dynamic environment and creates incentives
for increasing productivity and making efficient use of resources.
3. This Code of Conduct (‘the Code’) is aimed at all commissioners and providers – and other bodies with
regulatory and/or performance management responsibilities – operating within the PbR system (as defined
in the glossary of terms), but without prejudice to any future Government decision on extending the scope of
PbR (In 2006, PbR applies to acute services provided by NHS Trusts, NHS Foundation Trusts and to Independent
Sector providers operating under the Extended Choice Network). Its purpose is to establish the underpinning
principles that should govern organizational behaviour under PbR and set expectations as to how the
system should operate. In this way, the Code of Conduct should minimise as well as guide the resolution of
disputes under PbR.
4. However, the Code must be effective both now and in the context of any future changes to roles and
responsibilities in the NHS. Therefore, the Code will form part of the Operating Framework (as defined in the
Glossary) and will be reviewed from time to time, subject to consultation in line with Cabinet Office
guidelines.
5. PbR should be implemented according to the principles laid out in the Code and complying with relevant
guidance. Moreover, it is essential for organisations operating under PbR to recognise their ongoing
relationships as part of a wider healthcare system. This means taking a dynamic and long-term view that
facilitates improvements to quality and service innovation, fitting with other key policy goals (e.g.
transforming care pathways for people with long-term conditions).
6. Under PbR, activity is paid for on the basis of the number and complexity (i.e. casemix) of cases treated.
Importantly, the casemix classifications, prices and payment rules are set at national level and are not
subject to local negotiation except as specifically defined in PbR guidance. However, PbR does not negate
the need for contracts between commissioners and providers, which must continue to specify the range of
services commissioned as well as any referral or treatment protocols (i.e. care pathway description) and
relevant performance criteria.
7. The Code is not intended to deal with outstanding policy issues or give detailed guidance although the
Department recognises the need for consistency between the Code and the wider policy framework.
Furthermore, the Code will rely on effective contractual, regulatory and performance management
mechanisms for its enforcement.
The scope and objectives of Payment by Results (PbR)
8. PbR has been designed to contribute towards the achievement of several of the key objectives of health
system reform. These objectives are complementary but at times need careful management to ensure they
work together successfully in practice.
9. The key objectives are summarised as follows:
improve efficiency and value for money through enhanced service quality, as both commissioners
and providers can retain and invest surpluses and savings to improve services;
facilitate choice, by enabling funds to go to the services chosen by patients;
facilitate plurality and increase contestability, enabling funds to go to any provider (whether NHS
or Independent Sector) who can treat patients at tariff (Through the development of its Competition
Policy, the Department of Health will critically examine the ‘fitness for purpose’ of the current tariff as a pricing
mechanism consistent with the overarching objective of creating a level playing field under Free Choice from
2008) and at NHS standards, and enabling providers to compete on an equal basis to provide
services;
enable service innovation and improve quality, by rewarding providers whose services attract
patients and focussing negotiations between providers and commissioners on quality and
innovation, because the price is fixed;
drive the introduction of new models of care closer to where people live and work, by enabling
funds to go to providers offering care in non-traditional and community based settings;
reduce waiting times, by rewarding providers for the volume of work done;
make the system fairer and more transparent, through consistent fixed price payments to
providers based on volume and complexity of activity; and
get the price ‘right’ for services, by paying a price that ensures value for money for the taxpayer
and incentivises the provision of innovative, high quality patient care.
10. PbR can and should be implemented in way that contributes towards achieving the above objectives.
However, it is important that all parties operating in the system are also clear what the policy is not designed
to achieve. This includes increasing the overall amount of cash in the system. The NHS works within fixed
App
endi
ces
Page 140 of 150
spending limits at national and local level. PbR is not, of itself, a mandate for providers to supply activity.
The impact of PbR locally will therefore be on the technical efficiency of service provision and on the flow of
funds under contracts between commissioners and providers.
Tariff Setting
11. The following principles shall apply to tariff setting:
The Secretary of State will be responsible for maintaining the system of Payment by Results –
including The tariff setting function
consistent with his/her obligations to provide a national health service in England and
other applicable Law (As defined under National Health Service Act 1977)
The Department of Health will involve key stakeholders in establishing or reviewing the tariff
setting function
The remit and responsibilities of the tariff setting function will be set out in published Terms of
Reference
The tariff setting process shall be open and transparent
The Department of Health will ensure that exercise of the tariff setting function involves key
stakeholders
In exceptional circumstances and only to the extent necessary in pursuit of his/her obligations to
provide a health service in England, the Secretary of State may require particular, in-year changes
to the national tariff and will ensure that:
• proposals for such changes take account of input from key stakeholders;
• the process for implementing such changes is open and transparent; and,
• commissioners and providers are given reasonable notice of the details of such changes
12. For the purposes of this Code, ‘key stakeholders’ shall include a representative group of commissioners and
providers as well as those bodies responsible for performance management and regulation, including
Monitor and the Healthcare Commission.
General conduct of commissioners, providers and other organisations participating in Payment by
Results (PbR)
13. PbR should support the provision of a service that is
Responsive to the needs of patients and public
Responsible and accountable to patients and public
High quality, striving for excellence
Efficient and effective in its use of resources
14. This means that all organisations operating PbR, and individuals working within them, will:
Put patients’ interests first, balancing the needs of individuals with those of the wider population served
Ensure that patients get appropriate, responsive, high quality care, close to home where possible and
when it’s needed
Ensure that patients have a choice when it is appropriate
Provide appropriate and transparent information for patients, their carers and the wider public
Ensure care is provided efficiently with the best possible outcome
Work together to innovate, developing better services, closer to where people live and work
Behave and treat each other transparently, openly and fairly
Share information with each other wherever appropriate
Work together to anticipate and resolve problems
Consult and involve each other in decisions and changes wherever appropriate
15. In implementing PbR, commissioners and providers jointly will also observe the following principles:
PbR is a national, rules-based system maintained by the Secretary of State and defined in Department
of Health guidance as amended from time to time
All casemix classifications, prices, payment rules, data definitions, information standards and reporting
obligations applicable to PbR are as defined in national guidance, as amended from time to time
PbR is a prospective payment system and therefore in individual cases, the applicable tariff will be
greater or less than the actual cost of activity and such differences shall not prejudice the
commissioning or provision of services under this Code.
The tariff is not intended to subsidise the cost of activities outside the scope of PbR. Equally, any
funding for activities outside the scope of PbR shall not be intended to subsidise the costs of activity to
which the tariff applies. The only exception to this general principle is where funding is agreed to
reimburse specific costs that are incurred incidentally in the provision of services under PbR, but are
excluded from the tariff, in line with national guidance (e.g. ‘pass through’ payments for new
technologies).
Providers have the autonomy to retain and invest surpluses gained under PbR.
The national guidance that constitutes PbR is not subject to local negotiation, except for, and only to
the extent afforded by, any local flexibilities specified in such guidance, including the Operating
App
endi
ces
Page 141 of 150
Framework.
Commissioner responsibilities
16. The following principles shall apply to commissioners under PbR:
‘Commissioning’ is the process that determines how the health and healthcare budget is used and must
result in a good deal, both for patients and taxpayers.
Commissioning will not be the responsibility of a single organisation, but will be a partnership between
PCTs, general practice (‘practices’) and local government.
Commissioners will undertake regular health needs assessment and forecast demand for health
services and keep these under review, taking account of advice from providers and the accuracy of
previous assessments and forecasts
PCTs will collaborate with practices to ensure that taxpayers’ money is used to best effect on behalf of
patients. PCTs will carry out the analysis to support assessment of local needs and to provide the
clinical and management information that will be needed by their practices.
Practices will look to identify gaps in existing services and pathways that need improvement. PCTs will
use the aggregated intelligence of their practices and their local needs assessment to identify broader
requirements for service change or development. PCTs will signal the future service needs to providers
and engage with clinical networks to ensure effective delivery of complex care pathways.
PCTs will act as agents of their practices and secure contracts with providers for the provision of health
services – including elective and unscheduled care – in line with their health needs assessment and
demand forecasts having regard to patient preferences and the impact of Patient Choice. Such
contracts will reflect minimum performance requirements as specified from time to time by the
Department of Health in line with national standards and targets (The Department of Health will develop a
national template contract that will incorporate national standards (quality, safety and service levels), the national
tariff and penalty schedules (Health Reform in England: update and next steps, Department of Health, December
2005; Annex D)
PCTs will remain responsible for the actions of their practices and other primary care professionals in
referring patients to providers and for services under PbR
Commissioners will specify care pathways – including referral and treatment protocols – in line with
patient preferences and on the basis of available evidence as to clinical and cost effectiveness
Commissioners will adhere to, and ensure that their agents adhere to, any specified care pathways in
line with the principle set out above
Under PbR, PCTs will pay for all activity that is delivered on behalf of their populations and as per their
contractual or statutory obligations (or as otherwise implied by the terms of previous contracts or by
commissioners’ actions)
Commissioners will not discriminate against or disadvantage particular patients or providers in
exercising their responsibilities under this Code, including when contracting for services or authorising
activity on behalf of their populations.
Participants who are both commissioners and providers of services will act transparently to avoid
conflict of interests.
Provider Responsibilities
17. The following principles shall apply to providers under PbR:
Providers will remain responsible for developing and maintaining services and for the performance of
those services
Providers will secure contracts with commissioners or otherwise obtain authority to provide services to
patients as a condition of claiming payment under PbR. The exception to this general principle is for
Non-Contract Activity as defined under national guidance as it applies to unscheduled care.
In consideration of the prices paid for services under PbR, providers will deliver high quality care in line
with good clinical practice and any specific performance requirements enshrined in their contracts with
commissioners (see 16.6 above)
Providers will specify any clinical criteria that they intend to apply systematically and in order to decline
to treat particular groups of patients, either in their Directory of Services ( A provider’s Directory of Services
must therefore include any Service Specific Booking Guidance to be used to determine the eligibility of patients for
services) where appropriate, or in contracts with commissioners. These criteria will be used to ensure the
clinical appropriateness of referrals and treatments and
should not be manipulated for purely financial reasons. Furthermore, providers should not make
unilateral changes to such criteria without having agreed corresponding changes to contracts with
commissioners.
Providers will adhere to, and ensure their agents adhere to, any specified care pathways in line with
their contractual obligations and consistent with commissioners’ responsibilities set out above
In support of the commissioners responsibilities regarding health needs assessment and demand
forecasting, providers will supply information about demand and activity, including demand for
unscheduled care, in line with their contracts.
App
endi
ces
Page 142 of 150

Providers will be responsible for the timeliness and accuracy of data required as part of the transaction
process under PbR and in support of commissioners responsibilities in reviewing health needs
assessment and demand forecasts
Providers will not discriminate against or disadvantage particular patients or commissioners when
operating PbR, including when accepting or declining to treat individual patients and in the provision of
services generally.
Participants who are both commissioners and providers of services will act transparently to avoid
conflict of interests.
Information sharing
18. The following principles shall apply to all parties within the system:
Commissioners will give patients the support and information they need to make the right healthcare
choices and providers will support commissioners in this by maintaining an up-to-date Directory of
Services.
The Department of Health and commissioners will make available to all providers, including
Independent Sector providers, the same information about forecast demand, capacity and performance
requirements, proposed service changes/developments, and other procurements to ensure equity of
access across the system.
Providers will make available to commissioners information about capacity and quality, in accordance
with their contracts.
Providers may implement changes to clinical coding and counting (i.e. classifications) practices in
pursuit of improvements in data quality and the accuracy of transactions under PbR.
Changes to coding and counting practices will be implemented in good faith and at all times comply
with national data definitions and information standards.
Providers will notify commissioners of the details of any proposed changes to coding and counting
practices in advance and confirm the date from which such changes are implemented.
Any changes to coding and counting practices by individual providers shall not affect the information
basis upon which contracts have been agreed or result directly in claims for additional payment, or loss
of income, under PbR until the start of the next financial year.
The Department of Health will keep under review the risk of activity inflation (i.e. volume or casemix)
associated with improved coding and counting.
Activity Specification, Demand Management and Capacity
19. The following principles shall apply to commissioners and providers operating PbR:
Demand Management is a joint responsibility. Decisions on the use of healthcare resource should be
made in the best interests of patients, the public, and not the financial interests of individual
organisations.
It is the commissioner's responsibility to manage demand from primary care referrals and attendances
at A&E. Providers should co-operate with commissioners in this and will take steps to mitigate the risk of
supplier-induced demand (6 Supplier-induced demand may include any lowering of admission or treatment
thresholds and/or non-compliance with referral and treatment protocols), including:
• periodically reviewing admission/intervention thresholds, length of stay and consultant-to-
consultant referrals; and,
• by participating in periodic utilisation reviews.
Providers are responsible for managing their capacity, for honouring patient appointments and for their
obligations in meeting demand for unscheduled care. Commissioners should co-operate with providers
in this and will be responsible for the accuracy of their demand forecasts and keep these under regular
review to mitigate the risk of ‘under-commissioning’. In addition, PCTs will be responsible for the actions
of their agents both in referring patients to hospital and in providing unscheduled or ‘out of hours’ care
as these affect the accuracy of demand forecasts and therefore capacity management and risk across
the system.
Under PbR, planned activity volumes are important management tools, but will not determine payment
or the allocation of financial risk between commissioners and providers. Nevertheless, the Department
of Health may seek to mitigate the risk of demand volatility by setting a differential tariff for activity above
and/or below a pre-defined threshold. In such cases, both the differential tariffs and the thresholds will
be set nationally in line with the principles outlined at Paragraph 11 above.
The use of ‘caps and floors’ on activity is inconsistent with the fundamental principle of PbR that
payment should be based on the number and complexity of cases treated.
Instead, PCTs will establish demand management strategies. The aim will be to enhance quality and
efficiency and to ensure that budgets are not breached. The tools of demand management are
likely to include:
• benchmarking information for all GP practices;
• clinical pathways and protocols that are developed by local clinicians, covering areas
App
endi
ces
Page 143 of 150
vulnerable to volatile demand or supplier-induced demand;
• clinical advice and support for struggling GP practices;
• facilitating clinical groups to agree training and development, and clinical protocols reflecting
agreed clinical priorities locally;
• appropriate use of preventative intervention strategies to improve health and efficiency;
• target conversion ratios from outpatient to inpatient/day case lists for specific procedures and
agreement on a sustainable and affordable profile for reducing overall waiting list size.
It is good practice for commissioners and providers to specify trigger points in the monitoring of
activity as part of an overall strategy for managing demand and capacity. Where activity levels
exceed these trigger points, commissioners and providers should work together to identify the causes
of excess demand and commissioners should revise their forecasts and demand management
strategies accordingly. Where activity levels significantly exceed these trigger points, commissioners
and providers should work together to prioritise patients on the basis of clinical need. Such action
may include changes to referral and treatment protocols to ensure that limited resources are targeted
effectively. However, such action shall not extend to withholding payment to providers for activity duly
delivered.
20 While these principles will continue to apply as PbR is expanded to cover emergency, ambulance, long-
term conditions and mental health, it is important to bear in mind that appropriate casemix classifications
may not always be based on individual patient attendances, procedures or hospital admissions.
Patient choice, referrals and treatment thresholds
22. Under payment by results (PbR) in 2006/7, patient choices for elective care, and where patients are treated
in emergencies, will determine how around 30% of NHS funds are spent.
23 The following principles shall apply to all parties within the system:
Providers may offer a restricted range of services to patients only to the extent this is consistent with
their contracts with commissioners and based on the provider’s Directory of Services on the date the
contract was agreed or subsequently amended. For NHS Foundation Trusts any restrictions on the
range of services offered to patients must be consistent with their Terms of Authorisation.
For services provided under Patient Choice, once a patient appointment has been booked this must be
honoured and appropriate treatment subsequently provided – in line with contracts
– irrespective of whether the tariff covers the costs of doing so.
Furthermore, patients choosing a particular provider must be treated by that provider as long as this is
in the patient’s interest.
Finally, providers will work with commissioners to monitor treatment thresholds and ensure patients are
treated appropriately.
Innovation to improve access to, or quality of, services
23. The following principles shall apply to all parties operating within the system:
Commissioners and providers will collaborate to innovate in services and care pathways.
The Tariff is a fixed price and should not be subject to local negotiation. However, certain ‘local
flexibilities’ may be provided for under PbR guidance and should be used to support technical innovation
and/or improved access to services in the interest of NHS patients.
Examples of local flexibilities under PbR may include:
•Tariff sharing (i.e. ‘unbundling) to support improved access to services (e.g. by funding elements of
acute care outside a hospital setting)
• Pass through payments to support the use of new technology (e.g. minimally invasive procedures)
• ‘One stop shop’ payments for outpatient clinics involving multidisciplinary or multi-specialty teams
and/or multiple diagnostic tests.
As a point of principle, local flexibilities under PbR must be applied as defined in national guidance as
amended from time to time.
Moreover, such arrangements should only occur if they
• are agreed in advance;
• have agreed, quantified outcomes;
• define who carries the financial risk if planned changes are not delivered with standard tariff applying
in default.
The procurement of services by commissioners under PbR must be open and transparent to ensure
contestability and equity of access among providers.
Commissioners and providers will make information available about services procured using local
flexibilities under PbR to inform patients’ choices (e.g. as part of a commissioner’s advice to patients
about the choice of services available and in a provider’s Directory of Services) and will publish the tariffs
used for local flexibilities to ensure transparency across the system.
Billing and Payment
App
endi
ces
Page 144 of 150

24. The following principles shall apply to all parties operating within the system:
Billing and payments will be prompt, fair and accurate.
Providers and commissioners will agree definitions of activity, and timescales within which activity is
paid for, through contracts.
Providers will code and bill for activity fairly, accurately and promptly in line with national guidance on
reporting under PbR. This guidance will be reviewed annually and reporting timescales will be reduced
in support of the principle that billing and payment should be ‘right first time’.
Commissioners will pay invoices promptly, as defined in their contracts. Any queries raised about an
invoice shall be confined to specific items and should not delay payment for the remaining items. Any
query that remains outstanding at the point an invoice becomes due shall be referred to dispute
resolution and will not be grounds for delaying payment of the undisputed amount.
Commissioners and providers will agree processes for resolving disputes in line with the cross-
government pledge on alternative dispute resolution, as illustrated by national model contracting
arrangements. (The process for resolving disputes should be set out in contracts. SHAs will be the final arbiter of
disputes between NHS Trusts. For disputes involving NHS Foundation Trusts, the national model contract includes a
dispute resolution procedure. Looking ahead, the Department will introduce a national template that will form the
basis of contracts for all providers of NHS services (Health Reform in England: Update & Next Steps; Department of
Health, December 2005))
Commissioners and providers will collaborate to resolve disputes in a timely fashion and by the end of
the next quarterly billing period or after three separate monthly billing periods as appropriate to their
contracts. Regulators and performance managers will monitor instances of dispute and take action to
address risks associated with organisations involved in frequent or protracted disputes.(The monitoring of
disputes will be at the discretion of regulators and performance managers and any subsequent intervention against
organisations will be proportionate to the risk to either the commissioning or provision of NHS services or the wider
public interest in minimising NHS transaction costs may provide for payment of interest on such sums, for the period
held in an escrow account, as part of any settlement of a dispute and in favour of either the commissioner or
provider. )In addition, the Department of Health will consider the merits of collecting data on disputes so
that details of organisations involved in frequent or protracted disputes may be made public.
The number of payment disputes will be kept to a minimum.
Disputes should not take place where the financial sums or other matters concerned are not material.
When a payment is disputed, the undisputed amount should be paid forthwith and only the disputed
amount should be held in an escrow account until the dispute has been resolved. In addition, contracts
25. As a general principle, billing and payment should not be disputed in bad faith or to manage cash flow.
Enforcement
26. The following principles shall apply to all parties operating within the system:
It is an overarching principle of this Code that it should be enforceable through contracts and
embedded in NHS regulatory and performance management arrangements
The Department of Health will work with the Healthcare Commission and Monitor to explore how
compliance with the Code may be included in assessment criteria for Standards for Better Health
standards on corporate governance.
The boards of all participants in PbR should formally adopt the Code. In particular, all organisations
providing and commissioning care for NHS patients will comply with this Code.
Contracts for services provided under PbR should be consistent with this Code.
The Secretary of State requires compliance with the Code by all NHS Bodies operating PbR, including
Health Authorities, NHS Trusts and PCTs. The Department of Health will therefore ensure that
compliance with the Code is integrated into performance management arrangements and may publish
details of non-compliance on an exception basis. Moreover, organizations responsible for performance
management will be expected to take action to address non-compliance. Persistent non-compliance by
individual NHS Trusts or PCTs may be penalised through intervention and/or direction on behalf of the
Secretary of State. (The question of sanctions is under active consideration and will be the subject of a separate
statement early in the new financial year.)
Independent Sector providers will sign up to the Code as part of any relevant accreditation or
procurement process and so that compliance with the Code is a condition of their contracts to provide
NHS services.
Non-compliance will be addressed through the relevant mechanisms outlined above and in a manner
proportionate to the extent and impact of the non-compliance.
An assurance framework will be established to underpin improvements to data quality under PbR and
will include an appropriate audit regime
Any cases of suspect fraud involving an organisation operating PbR activity will be referred to and dealt
with by the appropriate authorities.
Glossary of Terms
All parties operating within the system - Parties include all commissioners and providers (as defined below) the
App
endi
ces
Page 145 of 150

tariff setting body, Department of Health, and all other bodies involved in the administration of PbR and/or with
relevant regulatory or performance management responsibilities.
Caps and floors - The term ‘cap’ refers to a pre-agreed limit on the amount of activity for which a commissioner
will pay a provider. The term ‘floor’ refers to a pre-agreed minimum amount of activity for which a commissioner
commits to pay a provider.
Code (i.e. ‘the Code) - The PbR Code of Conduct as amended from time to time
Commissioners - The term commissioners covers all organisations operating under PbR to the extent they
participate in the procurement of services for NHS patients including Primary Care Trusts, Primary Care
Practices participating in Practice Based Commissioning, Local Authorities and their authorised agents,
including Commissioning Consortia and any Procurement Agency (e.g. Shared Service)
Contracts - These are relationships of rights and obligations between (at least) two parties operating under PbR
and normally including a commissioner and a provider. A contract is formed by the parties (or their authorised
agents’) offer and acceptance (i.e. agreement) and its terms and conditions may be specified in writing, or
otherwise defined by the parties’ actions, and amended from time to time by agreement. For the purposes of this
Code, contracts shall include Service Level Agreements (SLAs) subject to arbitration by the Secretary of State
and/or a delegated authority (i.e. NHS Contracts as defined under the NHS and Community Care Act 1990);
and, legally binding contracts subject to determination in the courts.
Directory of Services - A list and description of each provider’s services – including any Service Specific Booking
Guidance – compiled and made available to commissioners and patients to underpin the operation of Patient
Choice and as required by Department of Health guidance as amended from time to time.
Independent Sector Providers - All providers other than NHS Trusts, PCTs, NHS Foundation Trusts or other
statutory body providing NHS services
Law - The law in England, including any enforceable community right within the meaning of S2 (1) European
Communities Act 1972
Monitor - The independent regulator of NHS Foundation Trusts established under the Health & Social Care
(Community Health & Standards) Act 2003
Operating Framework - From 06/07, an annual statement will be published on the ‘rules’ governing how the
system should operate during implementation of Health Reform in England (Health Reform in England: Update &
Next Steps; Department of Health, December 2005)
PCT (Primary Care Trust)- Any Primary Care Trust in England
Providers- The term providers covers all organisations who either currently, or in future may provide services
within the scope of PbR, including: NHS Acute Trusts, NHS Foundation Trusts, Mental Health Trusts,
Consultants, Independent Sector Providers, Primary Care Practices, GPs, Pharmacies, community services,
social services and the voluntary sector.
Service Specific Booking Guidance- Guidance for use by commissioners and their agents in making referrals
and bookings on behalf of patients that details any criteria to be used systematically by a provider to determine
patients’ eligibility for specific services. SHA (Strategic Health Authority) A Strategic Health Authority in England
Stakeholders- The term stakeholders covers all parties operating within the system, and groups within those
stakeholders, including clinicians and managers. It also includes patients and members of the public.
Tariff sharing- Tariff sharing refers to the splitting of the fixed tariff price between one or more providers who are
providing different elements of the treatment covered by the fixed price.
Terms of Authorisation- The terms under which NHS Foundation Trusts may be authorised to provide services
under the Health and Social Care
Treatment thresholds- Treatment thresholds refer to the clinical threshold above which a specific treatment is
judged appropriate for a specific condition.
Trigger points- The term trigger points refer to pre-agreed levels of referrals and/or activity indicating unplanned
increases in demand.
App
endi
ces
Page 146 of 150

App
endi
ces
Page 147 of 150
F R A U D , B R I B E R Y A N D C O R R U P T I O N R E P O R T I N G A R R A N G E M E N T S
INTRODUCTION
The purpose of this document is to inform all employees of the Trust of their responsibility to
report any matter of concern which they may have regarding any acts, events or circumstances
of fraud, bribery or corruption which involve, or which they believe involve or impact upon the
Trust or NHS.
Examples of such issues include losses and thefts of goods or money, false claims for expenses,
obtaining contracts, services or benefits by deception, accepting or offering payments to
influence corporate decisions (particularly in respect of procurement), or any other dishonest act
resulting or likely to result, in financial loss to the Trust or NHS.
NHS Protect & Local Counter Fraud Specialists
NHS Protect is the body with responsibility for combating, amongst other things, fraud, bribery
and corruption in the NHS. Almost every health body is required to maintain its own appointed
Local Counter Fraud Specialist (LCFS) who is responsible for undertaking a range of anti fraud
and corruption activities in the health body. These activities include investigating suspected or
actual instances of fraud, bribery or corruption. The LCFS works closely NHS Protect and, if
required, the Police and other law enforcement agencies.
Notifying Suspected or Actual Fraud, Bribery or Corruption
There are a number of ways which employees, members of the public or anyone else can report
suspicions or concerns that they may have. These are listed below.
The Local Counter Fraud Specialist (LCFS)
The Trust has a nominated officer, who is trained to conduct investigations to a criminal standard.
Suspicions may be reported directly to them via telephone number 0151 285 4500. This is the
number for Mersey Internal Audit Agency (MIAA) who provide the Trust with its LCFS service,
under contract.
Direct of Finance
The Director of Finance has a responsibility for ensuring that matters of actual or suspected
fraud, bribery and corruption in the Trust are appropriately dealt with. The LCFS reports to the
Director of Finance.
The National Fraud and Corruption Reporting Line
Tel: 0800 028 40 60 (Free phone Mon-Fri 8am-6pm). Suspicions and concerns can be reported
in confidence and, if required, anonymously. All calls are handled professionally and discreetly.
NHS Fraud & Corruption Confidential Reporting Form (online)
http://www.reportnhsfraud.nhs.uk/
Concerned individuals may also refer to the Trust’s Counter Fraud and Corruption Policy,
Whistleblowing Policy. Further information for staff may also be obtained via the Counter Fraud
page on the Trust intranet.
App
endi
ces
Page 148 of 150

Responsibilities
Whichever route is taken, the responsibility for agreeing the most appropriate course of action
lies with the Director of Finance. The responsibility for investigating reported issues lies with the
Local Counter Fraud Specialist in association with the NHS Protect.
Protection of Notifying Individuals
The Trust recognises its responsibilities under the Public Interest Disclosure Act 1998, an outline
of which can be found in the Trust Whistle Blowing Policy. It is important to understand that the
Trust is required by law to protect employees who do report matters of genuine concern for
investigation and is committed to take appropriate measures to support and protect them.
However, the Trust may be required to disclose the identity of anyone making a referral or
alleging criminality, if required to do so under an appropriate legal obligation or instruction.
Summary
It is everybody’s responsibility to report suspicions of Fraud, Bribery and Corruption. All matters
will be dealt with in the strictest confidence.
App
endi
ces
Page 149 of 150

T R U S T P O L I C I E S
A copy of all Trust policies are available on the Trust Intranet including the following key
documents:
Risk Management Strategy
Records Management Strategy
Purchasing & Logistics Strategy
Counter Fraud & Corruption Policy
Tendering and Quotation Policy
Records Management Strategy
Research Governance Policy
Intellectual Property Policy
Acceptance of Gifts & Hospitality Policy
Declaration of Interests Policy
Whistleblowing Policy
Commercial Sponsorship Policy
Disciplinary Policy
App
endi
ces
Page 150 of 150