coronary slow flow phenomenon 冠状动脉慢血流现象 hui yongming beijing fengtai hospital...
TRANSCRIPT
Coronary Slow Flow Phenomenon
冠状动脉慢血流现象 Hui YongMing Beijing Fengtai Hospital Medical Center of FengTai DistrictTeaching Hospital of Capital Medical University

• Coronary slow flow phenomenon (CSFP) is characterized by angiographically normal coronary arteries (no significant stenosis, spasm, dissection or thrombus) with delayed opacification of the distal vasculature.
It was first described by Tambe et al. in 1972.
• Currently, although CSFP is a well known phenomenon by the invasive cardiologists, its etiology, pathophysiologic mechanisms, clinical manifestations and prognosis are not well known.
• Some studies show that CSFP may lead to angina pectoris and true myocardial infarction.

• Overall, CSFP is observed in approximately 1% of the patients undergoing CAG.
• Mangieri et al. reported an incidence of 7% of this phenomenon in patients suspected to have cardiovascular disease;
• In our study, 4% incidence in CAG pats with suspected to have cardiovascular disease.
40 CSFP pats received long term follow-up study in our centre.

• male , 40 years• Exertional chest distress 6 months ,no chest
pain, hospitalizing on Nov 15, 2007 • EH 2 years; Smoking/drinking 20 years• Chol 4.43 mmol/L (2.83-5.17)• LDL 2.18 mmol/L (0-3.20)• HDL 1.43 mmol/L (1.00-1.60)• TG 5.43 mmol/L (0.56-1.71)• UA 493 umol/L (140-420)• UCG : LV 45 , LA 35 , IVS 9 , EF 60% • Positive exercise testing• ECG
CASE1


CAG on Nov 23, 2007

• Diagnosis : CSFP• Medicine : ASP 100mg/day
Control hypertension A calcium channel blocker ACEI
Therapy of dyslipidemia
Bad compliance for drug therapy

2 months after leaving hospital
• Persisting Chest pain 22 Hr hospitalizing on Jan 29, 2008
• ECG: Ⅰ 、 avL , V2-V5 ST↑0.1 ~ 0.5mV• Myocardial enzyme :CK 1706 , CK-MB
218


Diagnosis: ASTEMITherapy : chest pain relaxed only conventional conservative
therapy

CAG on the 3th day after AMI

Intensify anticoagulating and anti-platelet for one week
• ASP 300mg Qd• Clopidogrel 75 mg Qd• Tirofiban 0.1ug/kg/min 72h,• Clexane 0.6ml , IH , Q12h• Dipyridamole


CAG on 2 weeks after AMI
Follow up*Interval ischemia symptom,
especially afetr stopping anti-coagulating and anti-platelet therapy
*ARR
male , 47 yearsExertional chest distress,no chest pain, EH 、 Smoking 、 DrinkingPositive exercise testingHeight 168CM, Weight 80Kg
Chol 5.13 mmol/L (2.83-5.17)LDL 2.18 mmol/L (0-3.20)HDL 1.43 mmol/L (1.00-1.60)TG 7.43 mmol/L (0.56-1.71)UA 583 umol/L (140-420)
CASE2



• ASP 100mg Qd• Clopidogrel 75 mg Qd• Dipyridamole

Pathophysiological Mechanisms of CSFP Remain Uncertain
• Early phase of atherosclerosis
• Maybe relate to small vessel dysfunction (endothelial thicken, capillary damage , reduced small vessels diameter)
• imbalance between vasoconstrictor and vasodilatory factors
Beltrame et al. report the presence of an increased resting coronary vasomotor tone in coronary resistance vessels in CSFP patients, and an improvement in coronary blood flow by using a calcium T-channel blocker in CSFP pats, suggesting the presence of microvascular spasm.
• platelet function disorder • There has been evidence that inflammation plays an important role in development as well as
evolution of atherosclerosis

• Goel etal. have shown higher prevalence of positive exercise testing in CSFP patients compared with control subjects with normal coronary flow.
• Ersan Tatli documented the presence of myocardial ischemia using myocardial perfusion scintigraphy.
• Amasyali reported that CSFP may play a significant role in the pathogenesis of ventricular fibrillation of the patient.
• In our study, CSFP commonly in pats with middle-aged, smoker, untypical symptom, resting
ECG change, positive exercise testing .
• So, CSFP is not purely an incidental angiographic finding; on the contrary, it may lead to angina pectoris and true myocardial ischemia, infarction.
Some Clinical studies

Slow coronary flow phenomenon a kind of coronary disease ? slow coronary flow syndrome ?
Classification and Prognosis

Pathophysiological mechanisms
Epicardial Vessel or/and Microvessel Disorder
Coronary slow flow phenomenon
Clinical symptoms & events

Evaluation methods of Coronary Flow
• TIMI: Thrombolysis In Myocardial Infarction.• Corrected TIMI Frame Count (CTFC)• TMPG: TIMI myocardial perfusion grade.• MBG: myocardial blush grade.• Coronary Doppler• Myocardial Contrast Echocardiography
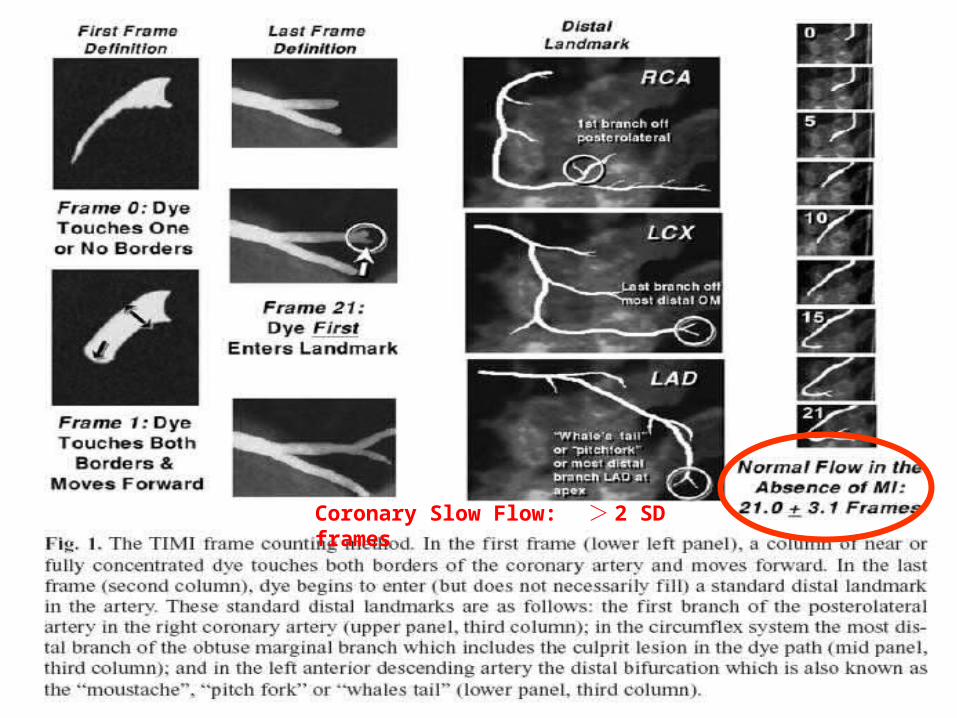
Coronary Slow Flow: > 2 SD frames

Corrected TIMI Frame Count(CTFC)
CSFP was defined as a corrected TIMI frame count . 1) with a contrast infusion rate of 3.5 ml/s at 460 mbar 2) All the values initially published as “frame counts” referred to
the video format standard in the United States, 30 frames / second.
3) The length of the LAD is 1.7 times greater than the LCX and the RCA. Thus, a correction factor was introduced in the TFC system when analyzing the LAD
Normal Flow Value LAD 36±2.6 21±2.1 (after correct) LCX 22±4.1 RCA 20±3.0 average 21±3.1Diagnosis of CSFP: Patients with a corrected TIMI frame count
greater than 2 SD were considered as having CSFP.
1 、 CSFP remains uncertain
2 、 Its etiology pathophysiologic mechanisms evaluation medthod therapy prognosis deserve further
investigation.
Conclusion

• Control risk factors of coronary heart disease • Therapy of dyslipidemia• Nitrovasodilators: noneffective• Dipyridamole , Persantin : effective• A calcium channel blocker: limited• Drug of improving endothelium function ( ACEI 、 Vitamin C 、 E) ??• Long-term Dual anti-platelet cohesion therapy
Necessity ? ( if no contraindiction ) How long ?
Conclusion- Therapy Strategy

Thanks !