core stability exercise principles - sportstg · pdf filespine conditions core stability...
TRANSCRIPT

SPINE CONDITIONS
Core Stability Exercise PrinciplesVenu Akuthota, ' Andrea Feneiro, ' Tamara Moore,^ and Michael Fredericson^
^Department of Physical Medicine and Rehabilitation, University of Colorado School of Medidne, Aurora, CO;^Sports and Orthopedic Leaders Physical Therapy, Oakland, CA; ^Division of Physical Medicine andRehabilitation, Stanford University School of Medicine, Stanford, CA
AKUTHOTA. V., A. FERREIRO, T. MOORE, and M. FREDERICSON. Core stability exercise principles. CUTT. Sports Med.Rep., Vol. 7, No. 1, pp. 39-44, 2008. Core stahiüty is essential for proper load balance within the spine, pelvis, and kinetic chain. Theso-called care is the group of trunk muscles that surround the spine and abdominal viscera. Abdominal, gluteal, hip ^rdle, paraspinal, andother mivicles work in concert to provide spind stability. Core stability and its motor control have been shown to he imperative for initiationof functior\al limb movements, as needed in athletics. Sports medicine practitioners use core strengthening techniques to improveperftmnance and prevent injury. Core strengthening, often called lumbar stabilization, also has been used as a therapeutic exercisetreatment regimen for low hack pain conditions. This article summarises the armtomy ofthe core, the progression of core strengthening, theavailable evidence for its theoretical construct, and its efficacy in muscuíos/ceietoi conditions.
INTRODUCTION
Core stability (or core strengtbening) bas become a well-known fitness trend tbat has started to transcend into tbesports medicine world. Popular fitness programs, sucb asPilâtes, yoga, and Tai Cbi, follow core strengtbeningprinciples. Broad benefits of core stabilization bave beentouted, from improving atbletic performance and preventinginjuries, to alleviating low back pain. Tbe purpose of tbisarticle is to review tbe available evidence on tbe benefits ofcore strengtbening, present relevant anatomy, and outlinecore stabilizing exercise principles.
The core can be described as a muscular box witb tbeabdominals in tbe front, paraspinals and gluteals in tbe back,tbe diapbragm as tbe rtxif, and tbe pelvic floor and hip girdlemusculature as tbe bottom (1). Witbin this box are 29 pairsof muscles that belp to stabilize tbe spine, pelvis, and kineticcbain during functional movements. Without these muscles,tbe spine would become mecbanically unstable witb com-pressive forces as little as 90 N. a load mucb less tban tbeweigbt of the upper body (2). When tbe system works as itsbould. tbe result is proper force distribution and maximumforce generation witb minimal compressive, translational, or
Address fiir cimcspondencet Venu Akuthota, M.D,. Depanment of Physical Medi-cine and Rehabilitation, University of Qilorado Schot>l of Medicine, Aurora, COäO,)09 (E-mail: venu,akiithota®uchiic,edu).
CuTTmi Spans Medicine ReportsCopyright O 2008 by the American College of Sports Medicine
sbearing forces at tbe joints of tbe kinetic cbain (3). Thecore is particularly important in sports because it provides"proximal stability for distal mobility" (4)-
Ipso facto, core stabiliry exercises appear to be especiallyimportant in cases of spinal instability. Gross spinal insta-bility is an obvious radiograpbic displacement of vertebrae,often witb associated neurologic deficit and deformity.However, functional or clinical instability is not as easilydefined. Panjabi describes "clinical instability as tbe loss oftbe spine's ability to maintain its pattems of displacementunder pbysiologic loads so tbere is no initial or additionalneurologic deficit, no major deformity, and no incapacitatingpain" (5). Tbe spine stability system consists of tbe followinginteracting elements:
• Neuromuscular control (neural elements)• Passive subsystem (osseous and ligamentous elements)• Active subsystem (muscular elements)
In otber words, stability of the spine is not only dependenton muscular strengtb, but alsti proper sensory input tbatalerts tbe central nervous system about interaction betweentbe body and tbe environment, providing constant feedbackand allowing refinement of movement (6). Tbus a completecore stabilizing program would consider sensory and motorcomponents related to tbese systems for optimal spinalstabilization. Recently, tbe Queensland pbysiotherapy groupproduced research drawing a great deal of attention to tbedeep core musculature, specifically tbe transversus abdominisand multifidi, for core stability ( 1 ). However, McGilland otber biomecbanists empbasize larger "prime mover"muscles, sucb as tbe abdominal obliques and quadratus
39
lumbomm, in ptoviding stability (7). It appears a coordi'nated contraction of all deep and superficial cote muscles isneeded for optimal spinal stabilization (8).
ANATOMY
core acts througb the tboracolumbar fascia, "nature'sback belt." Tbe transversus abdominis bas large attacbmentsto the middle and posterior layers of tbe tboracolumbar fascia(9). Additionally, tbe deep lamina of tbe posterior layerattaches to tbe lumbarspinous processes. In essence, tbetboracolumbar fascia serves as part of a "hoop" around thetrunk (7) that provides a connection between tbe lower limband the upper limb (10). Witb contraction of the muscularcontents, tbe tboracolumbar fascia also functions as aproprioceptor, providing feedback about trunk positioning.
Two types of muscle fibers comprise tbe core muscles:slow-twitch and fast-twitcb. Slow-twitcb fibers make upprimarily tbe local muscle system (the deep muscle layer).Tbese muscles are shorter in length and are suited forcontrolling intersegmental motion and responding tochanges in posture and extrinsic loads. Key local musclesinclude transversus abdominus, multifidi, intemal oblique,deep transversospinalis, and tbe pelvic floor muscles. Multi-fidi have been found to atrophy in people with chronic lowback pain (LBP) {11). On the otber hand, fast-twitch fiberscomprise tbe global muscle system (the superficial musclelayer). Tbese muscles are long and possess large lever arms,allowing them to produce large amounts of torque and grossmovements. Key global muscles include erector spinae,external oblique, rectus abdominis muscles, and quadratuslumborum (wbicb McGill states is a major stabilizer of thespine) (12).
The abdominals serve as a particularly vital component ofthe core. Tbe transversus abdominis bas received attentionfor its stabilizing effects. It bas fibers tbat run borizontally(except for tbe most inferior fibers, wbicb run parallel to tbeintemal oblique muscle), creating a belt around the abdo-men. "Hollowing in" of tbe abdotnen creates isolatedactivation of tbe transversus ahdominis. Tbe transversusabdominis and multifidi bave been .shown to contract 30 msbefore movement of tbe shoulder and 110 tns beforemovement of tbe leg in beaitby people, tbeoretically tostabilize tbe lumbar spine (13,14). However, patients witbLBP have delayed contraction of tbe transversus abdominisand multifidi prior to limb movement (14). Tbe intemaloblique and tbe transversus abdominis work together toincrease the intra-abdominal pressure from tbe htxip createdvia tbe thoracolumbar fascia. Increased intra-abdominalpressure bas been shown to impart stififhess to the spine(7). The external oblique, the largest and most superficialabdominal muscle, acts as a cbeck of anterior pelvic tilt. Theabdominals (and multifidi) need to engage only to 5%-10%of tbeir maximal volitional contraction to stiffen spinesegments (15).
Tbe bip musculature is vital to all ambulatory activities,and plays a key role in stabilizing the trunk and pelvis in gait(16). Poor endurance and delayed firing ofthe hip extensor(gluteus maximus) and abductor (gluteus médius) muscles
have previously been noted in people with LBP and othermusculoskeletal conditions such as ankle sprains (17). Thepsoas is only a feeble flexor of tbe lumbar spine (9).However, it does bave tbe potential to exert massive com-pressive forces on tbe lumbar disks. In activities tbat pro-mote maximal psoas contraction, sucb as full sit-ups, itcan exert a compressive load on tbe L5-S1 disk equal to100 kg of weigbt (9). Tigbtness of tbe bip flexor (psoas)can cause LBP by increasing compressive loads to tbe lum-bar disks.
Tbe diaphragm serves as the roof of tbe "muscular box" oftbe core, and tbe pelvic floor serves as tbe floor. Contractionof tbe diaphragm increases intra-abdominal pressure, thusadding to spinal stability. Pelvic floor musculature iscoactivated with traasversus abdominis contraction (18).Recent studies (19) bave indicated tbat people witbsacroiliac pain bave impaired recruitment of tbe diapbragmand pelvic floor. Tbus diaphragmatic breatbing techniquesand pelvic fioiir activation may be an important part ofa core-strengthening program.
MEASURING CORE STABILITY
Research on core stability exercises bas been hampered bya lack of consensus on bow to measure core strength. If coreinstability and core weakness can be measured, outcomes canbe followed and a proper emphasis can be placed upon corestrengthening in certain individuals. Delitto and others
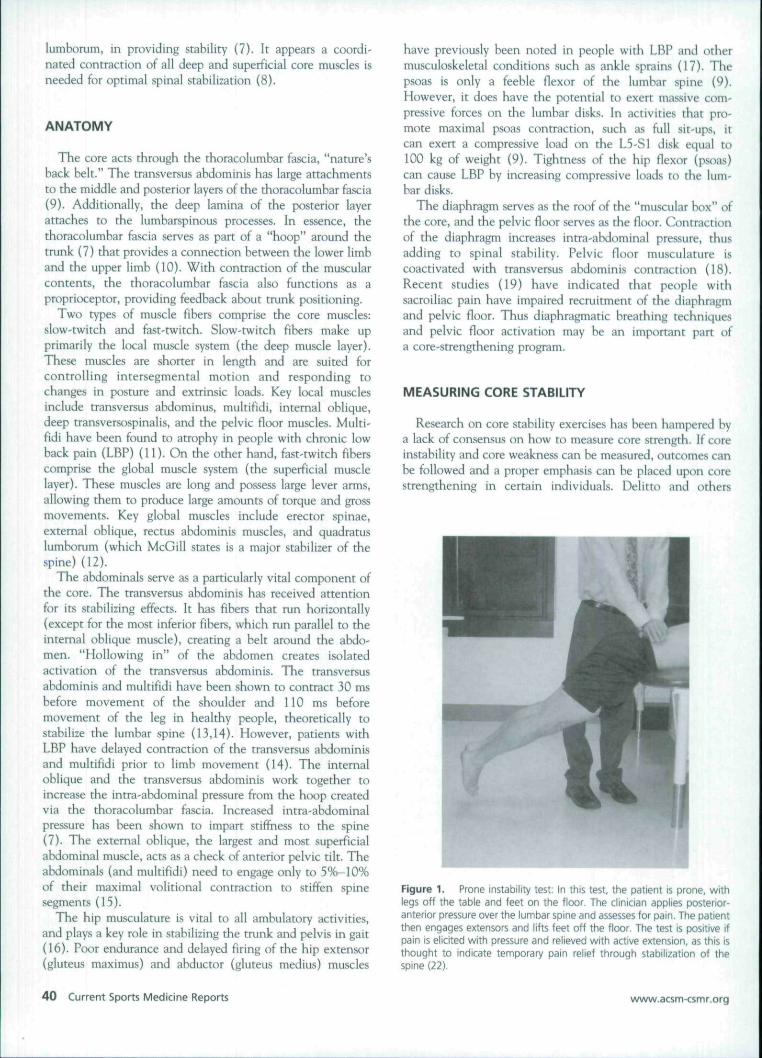
Figure 1. Prone instability test: In this test, the patient is prone, withlegs off the table and feet on the floor. The clinician applies posterior-anterior pressure over the lumbar spine and assesses for pain. The patientthen engages extensors and lifts feet off the floor. The test is positive ifpain is elicited with pressure and relieved with active extension, as this isthought to indicate temporary pain relief through stabilization of thespine (22),
4 0 Current Sports Medicine Reports w\ftn«.acsm<smr.org

bave proposed tbat stabilization exercises would work best inindividuals wbo are young, witb increased flexibility (post-partum, generalized ligamentous laxity), or witb examfindings suggesting an interspinal segment witb increasedpainful movement (20,21). The prone instability test is anexample of a physical exam maneuver testing for clinicalinstability (22) (Fig. 1). Measures can include triplanar,weigbt-bearing evaluation of the global core as well asisolated measures of particular muscles (4) (Fig. 2 Table 1).
DEVELOPING A CORE EXERCISE PROGRAM
Exercise of tbe core musculature is more than trunkstrengtbening. Lack of sufficient coordination in coremusculature can lead to decreased efficiency of movement,md compensatory patterns, causing strain and overuseinjuries. Tbus motor releaming of inbibited muscles may bemore important tban strengtbening in patients witb LBP andotber musculoskeletal injuries.
A core exercise program sbould be done in stages withgradual progression. It sbould start witb restoration of normalmuscle length and mobility to correct any existing muscleimbalances. Adequate muscle length and flexibility arenecessary for proper joint function and efficiency of move-ment. Muscle imbalances can occur wbere agonist musclesbecome dominant and sbort while antagonists would becomeinbibited and weak. One example of a muscle imbalancepattern includes tigbtness and over-activity of tbe primarybip flexor (iiiopsoas). which in turn causes reciprocalinhibition of the primary bip extensor (gluteus maximus).
TABLE I. Measuring core stability; the core score
L Prone instability test
2, Prone extension endurance test (Biering-Sorenaon paraspinalendurance strength)
3. Side bridge endurance test (quadratu!> lumbomm endurance stretch)
4. Pelvic bridging
5, Leg lowering test (lower abdominal strength)
6, Trunk curl
7. Hip extemal rotation strength
8. Modified Trendelenburg test (single leg squat witb observationinfrontal plane)
9, Single 1^ squat in sagittal plane
10, Single \cg squat in transverse plane
Furtber up tbe kinetic chain, tbis particular muscle imbal-ance leads to increased lumbar extension, witb excessiveforce on tbe posterior elements of the spine. In addition,postural muscles have a tendency to become tight due toconstant activity in order to fight tbe forces of gravity.
Then, activation of the deep core musculature should betaught through lumbo-pelvic stability exercises. When tbisbas been mastered, more advanced lumbo-pelvic stabilityexercises on tbe pbysioball can be added. Finally, tberesbould be transitioning to tbe standing position, facilitatingfunctional movement exercises tbat promote balance andccx>rdination of precise movement. Tbe goal of advancedcore stabilization is to train functional movements ratbertban individual muscles (3).
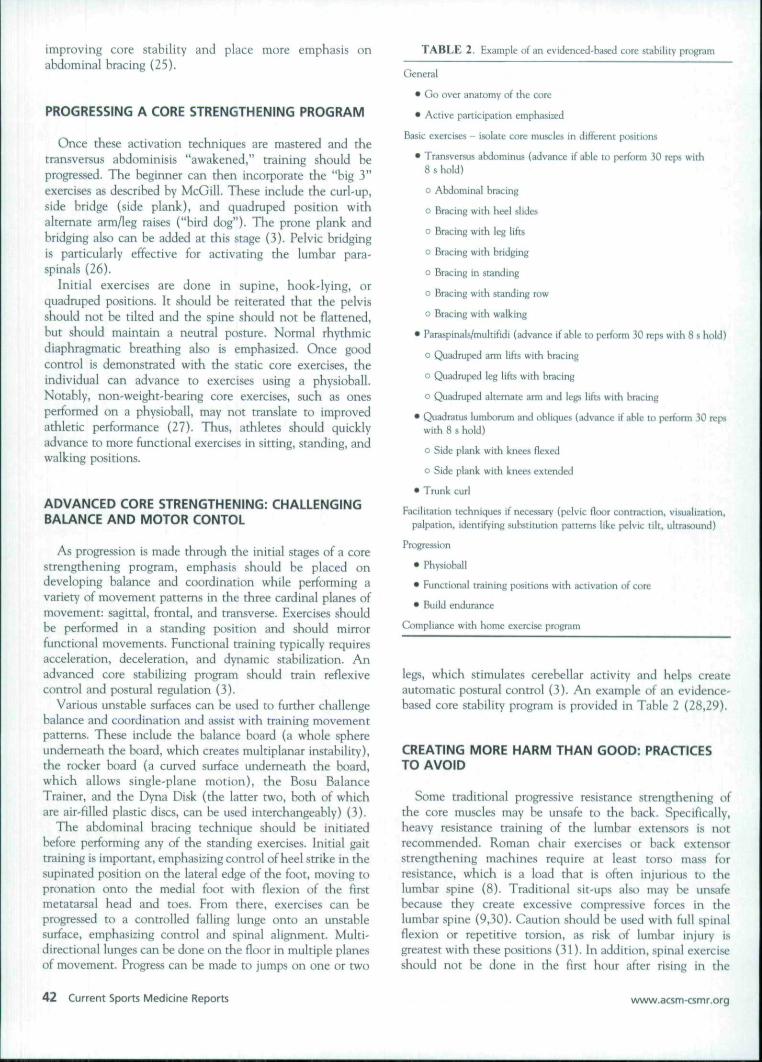
Figure 2. Advanced functional training techniques for core stability.Transverse plane core exercises in standing position. This resistive,dynamic trunk pattern challenges the core in the transverse plane. Thisrequires strict bracing of the abdominals and locking the ribs and pelvistogether to avoid unnecessary spinal torsion. The athlete activates theabdominal brace before movement. It is important to emphasize posturalalignnnent with scapulae retracted and depressed. The athlete shouldmaintain neutral spine angles throughout movement. Progression caninvolve greater resistance or weight.
BEGINNING A CORE STRENGTHENING PROGRAM
Warm-up can include tbe "cat" and "camel" stretcbes anda sbort aerobic program. A core stability exercise programbegins witb recognition of tbe neutral spine position (mid-range between lumbar flexion and extension), touted to bethe position of power and balance for optimal atbleticperformance in many sports (8).
Tbe first stage of core stability training begins witb leam-ing to activate tbe abdominal wall musculature. Individualswho are not adept at volitionally activating motor pathwaysor individuals witb chronic low back pain and fear-avoidancebebavior may require extra time and instruction to leam torecruit muscles in isolation or witb motor pattems (23).Cueing individuals on abdominal bollowing, wbicb mayactivate the transversus abdominis, as well as abdominalbracing, which activates many muscles including tbe trans-versus abdomin is, extemal obliques, and intemal obliques, isan important beginning step. One study showed tbatperforming abdominal bollowing and bracing prior toperforming abdominal curls facilitated activation of tbetransversus abdominis and internal obliques througbout tbeabdominal curling activity (22,24).
Grenier and McGill, bowever, found little utility of theabdominal hollowing to cue the transversus abdominis into
Volume 7 • Number 1 • January/February 2008 Core Stability Exercise Principles 41
improving core stability and place more emphasis onabdominal bracing (25).
PROGRESSING A CORE STRENGTHENING PROGRAM
Once tbese activation tecbniques are mastered and thetransversus abdominisis "awakened," training sbould beprogressed. The beginner can tben incorporate tbe "big 3"exercises as described by McGill. Tbese include tbe curl-up,side bridge (side plank), and quadruped position withalternate arm/leg raises ("bird dog"). The prone plank andbridging also can be added at tbis stage (3). Pelvic bridgingis particularly effective for activating tbe lumbar para-spinals (26).
Initial exercises are done in supine, book-lying, orquadruped positions. It should be reiterated that the pelvissbould not be tilted and tbe spine sbould not be flattened,but should maintain a neutral posture. Normal rhythmicdiaphragmatic breatbing also is emphasized. Once goodcontrol is demonstrated with the static core exercises, theindividual can advance to exercises using a physioball.Notably, non-weigbt-bearing core exercises, sucb as onesperformed on a physioball, may not translate to improvedathletic performance (27). Thus, athletes sbould quicklyadvance to more functional exercises in sitting, standing, andwalking positions.
ADVANCED CORE STRENGTHENING: CHALLENGINGBALANCE AND MOTOR CONTOL
As progression is made tbrougb tbe initial stages of a corestrengtbening program, empbasis sbould be placed ondeveloping balance and coordination wbile performing avariety of movement pattems in tbe tbree cardinal planes ofmovement: sagittal, frontal, and transverse. Exercises shouldbe performed in a standing position and sbould mirrorfunctional movements. Functional training typically requiresacceleration, deceleration, and dynamic stabilization. Anadvanced core stabilizing program sbould train reflexivecontrol and postural regulation (3).
Various unstable surfaces can be used to furtber cballengebalance and coordination and assist with training movementpatterns. These include the balance board (a whole sphereunderneath tbe board, which creates multiplanar instability),tbe rocker board (a curved surface undemeatb the board,which allows single-plane motion), the Bosu BalanceTrainer, and the Dyna Disk (tbe latter two, botb of whichare air-filled plastic discs, can be used interchangeably) (3).
The abdominal bracing technique sbould be initiatedbefore performing any of the standing exercises. Initial gaittraining is important, emphasizing control of heel strike in tbesupinated position on the lateral edge of tbe foot, moving topronation onto tbe medial foot witb flexion of the firstmetatarsal head and toes. From tbere, exercises can beprogressed to a controlled falling lunge onto an unstablesurface, empbasizing control and spinal alignment. Multi-directional lunges can be done on the floor in multiple planesof movement. Progress can be made to jumps on one or two
TABLE 2. Example of an evidenced-based core stability program
General
• Go over anatomy of the core
• Active participation emphasized
Basic exercises - isolate core muscles in different positions
• Transversus ahdominus (advance if able Ko perform 30 reps with8 s hold)
o Abdominal bracing
o Bracing witb heel slides
o Bracing with leg lifts
o Bracing with bridging
o Bracing in standing
o Bracing with standing row
o Bracing with walking
• Paraspinals/multifidi (advance if able to perform 30 reps with 8 s hold)
o Quadruped arm Yiks with bracing
o Quadmped leg lifts with bracing
o Quadmped alternate ami and legs lifts with bracing
• Quadratus lumbonjm and obliques (advance if able to perform 30 repswitb 8 s hold)
o Side plank witb knees flexed
o Side plank with knees extended
• Trunk curl
Facilitation techniques if necessary (pelvic floor contraction, visualization,palpation, identifying substitution pattems like pelvic till, ultrasound)
Progression
• Physioball
• Functional training positions witb activation of core
• Build endurance
Gimphancc witb bome exercise program
legs, wbicb stimulates cerebellar activity and belps createautomatic postural control (3). An example of an evidence-based core stability program is provided in Table 2 (28,29).
CREATING MORE HARM THAN GOOD: PRACTICESTO AVOID
Some traditional progressive resistance strengthening ofthe core muscles may be unsafe to the hack. Specifically,heavy resistance training of the lumbar extensors i.s notrecommended. Roman chair exercises or back extensorstrengthening machines require at least torso mass forresistance, wbich is a load tbat is often injurious to tbelumbar spine (8). Traditional sit-ups also may be unsafebecause they create excessive compressive forces in thelumbar spine (9,30). Caution should be used witb full spinalflexion or repetitive torsion, as risk of lumbar injury isgreatest witb these positions (31). In addition, spinal exerciseshould not be done in the first hour after rising in the
42 Current Sports Medicine Reports www.acsm<smr.org
morning. Tbis is due to the fact that bydrostatic pressure intbe disk is increased during tbat time (32).
WHO SHOULD HAVE CORE STABILITY PRESCRIBED?
Certain predictors can be used to determine wbichpatients will be more likely to benefit from lumbar stabiliza-tion programs. One study (28) found tbe following factorscould be used to assess wbich patients would be likely torespond favorably to core stabilization:
• Younger age (<40)• Greater general flexibility (bamstring lengtb greater
tban 90°, postpartum)• Positive prone instability test• Presence of aberrant movement during spinal range of
motion (painful arc of motion, abnormal lumbopelvicrbytbm, and using arms on tbighs for support)
Stuge et al. also proposed tbe following pbysical maneu-vers as predicting a good response from stabilization exercisein postpartum women (33):
• Positive posterior pelvic pain provocation (P4) test (alsocalled thigh thrust test)
• Positive active straight leg raise• Positive pain provocation (persists greater tban 5 s after
palpation) witb palpation of PSIS region (long dorsalsacroiliac ligament)
• Positive pain provocation (persists greater tban 5 s afterpalpation) witb palpation of pubic sympbysis
• Positive Trendelenburg sign
EFFICACY OF CORE-STRENGTHENING EXERCISE FORTREATMENT OF BACK PAIN
Tbere is ample evidence tbat individuals witb cbronicLBP and sacroiliac pain lack proper recruitment of coremuscles and exhibit core weakness (6,11,14,26,34,35). Tberealso is evidence of increased fatigability, decreased crosssection, and fatty infiltration of paraspinal muscles inpatients witb chronic LBP (6). Even high-level atbletessbow signs of core instability, and tbis may set tbem up formore musculoskeletal injuries (4,36-39). Female atbletesmay be particularly susceptible to injury to tbe anteriorcruciate ligament if core weakness is found (36-38). Inaddition, tbese patients seem to bave increased difficultywitb balance and decreased ability to compensate forunexpected trunk perturbation. Patients witb back pain alsoseem to over-activate superficial global muscles wbereascontrol and activation of tbe deep spinal muscles is impaired.Thus core stability exercises have strong theoretical basis forprevention of different musculoskeletal conditions and thetreatment of spinal disorders.
Level 1 evidence for stabilization exercises is mixed andmainly comes from studies on LBP. To our knowledge, therehave been five randomized trials that have supported.stabilization exercises for LBP (33,40-43). However, tbereare some metbodological flaws in some of tbese studies.
including lack of tme controls, significant attrition rate,and statistical vagaries (21,44). Two otber randomized trialsfurther question the superiority of stabilization exercises(29,45). Tbe control groups in both of tbese studies includedgeneralized strengthening components in addition to otherfeatures (21). Systemic reviews also have come to tbeconclusion tbat stabilization is helpiiil for spinal disordersbut may not be superior to otber tberapeutic exerciseregimens (46-48).
CORE STRENGTHENING AND INJURY PREVENTION
Some evidence in tbe literature supports tbe notion tbatcore stabilization programs may be used to help preventinjury in athletics. Leeton and colleagues (36) performed aprospective study looking at 140 male and female intercolle-giate basketball and track atbletes. Tbey found tbat injuredathletes linjuries included anterior cruciate ligament (ACL)rupture, iliotibial band syndrome, patellofemoral pain, andstress fracture in tbe lower extremity] bad significantlydecreased strengtb in bip abduction and extemal rotationcompared witb non-injured athletes. Hip extemal n>tationstrength was most useful in predicting injury (36).
Some literature supports using neuromuscular training toprevent ACL injuries in atbletes. Tbese programs includemuscle co-contraction to provide joint stability, balance andperturbation training, and plyometric exercises. Hewitt andcolleagues conducted a prospective study comparing injuriesin female bigb scbool atbletes with preseason neuromusculartraining, including single-leg functional core stability train-ing, witb a control group of female and male athletes withoutpreseason neuromuscular training (37). Non-contact ACLinjury risk was significantiy less in the group of femaleathletes with neuromuscular training. In a similar study,Heidt and colleagues found that preseason neuromusculartraining in female high scbool soccer players led to sig-nificantly fewer injuries overall, but no difference in ACLinjuries between groups (39).
Specific core stability programs in prevention of atbleticinjuries bave not been well studied. Additionally, coreprograms have not been proven to enhance athletic per-formance. Despite these facts, many of these programshave been promoted in lay literature for use in performanceenhancement.
CONCLUSIONS
Core strengtbening bas a strong tbeoretical basis intreatment and prevention of LBP, as well as otber muscu-loskeletal afflictions, as is evidenced by its widespreadclinical use. Studies bave shown tbat these programs maybelp decrease pain and improve function in patients witbLBP. However studies are limited, and some show conflictingresults. Future studies are needed to elucidate precise corestrengtbening programs and tbeir effects on treatment andprevention of LBP, in comparison witb other exercisetraining programs.
Volume 7 • Number 1 • January/February 2008 Core Stability Exercise Principles 43

References
1. Richardson, C , G. Jull, P. Hodges, and ]. Hides. Therapeutic exercise farSpinal SegTTienwi Stabilization in Low Back Pain: Scientific Basis and ClinicalApproach. Edinburgh, NY: Churcbill Livingstone, 1999.
2. Crisco, J.J., M.M. Panjabi, 1. Yamamoto, and T.R, Oxland. Stability oftbe human ligamentous lumbar spine. Part 11: experiment. Clin. Biomech.7:27-32, 1992.
3. Fredericson, M., and T. Moore. Muscular balance, core stability, andinjury prevention for middle- and long-distance runners. Phys. Med.Rehahil. Clin. N. Am. 16:669-689, 2005,
4. Kibler, W.B., J. Press, and A. Sciascia. Tbe role of core stabiliry inatbletic function. Sports Med. .36:189-198, 2006.
5. Panjabi, M.M, Clinical spinal instability and low back pain. ) . Electro-myogr. Kinesiol. 13:371-379, 2003.
6. Hodges, P,W, Core stability exercise in cbronic low back pain, Orthop.Clin. North Am. 34:245-254, 2003.
7. McGill, S. Low Back Disorders: E\Aàence-Based Prevertmn and ReheM-itation. Champaign, IL: Human Kinetics, 2002.
8. Akuchota, V,, and S.F. Nadler. Core strengcbening. Arch. Phys. Med.Rehahil. 85:86-92, 2004.
9. Bogduk, N, Clinical Anatomy of the Lumbar Spine arvi Sacrum, 3rd ed.New York: Cburcbill Livingstone, 1997.
10. VIeeming, A., A.L, Pool-Goudzwaard, R. Stoeckart, et al. The posteriorlayer of the thoracolumbar fascia. Its íunctíon in load transfer from spineto legs. Spine. 2:753-758. 1995.
11. Hides, J.A., CA, Richardson, and G,A, Jull. Mulrifidusmuscle recoveryis not automatic after resolution of acute, first-episixie low back pain.Spine, 21:2763-2769, 1996.
12. McGili, S.M. Low back stabiliry: from formal description to issuesfor performance and rehabilitation. Exerc. Sport Sei. Rev. 29:26-31,2001.
13. Hixlges, P.W., and C A . Richardson. Altered trunk muscle recruitmentin people witb low back pain with upper limb movement at differentspeeds. Arch. Phys. Med. Rehabil. 80:1005-1012, 1999.
14. Hodges, P.W., and CA, Richardson. Inefficient muscular stabilization ofthe lumbarepine associated witb low back pain. A motor controlevaluation of transversus abdominis. Spine. 21:2640-2650, 1996,
15. Cbolewicki, j . , K. Julum, and S.M, McGill, Inrra-abdominal pres-sure mechanism for stabilizing the lumbar spine. ]. Biomech. 32:13-17,1999.
16. Lyons, K., J. Perry, J,K. Gronley, et ai. Timing and relative intensity of hipextensor and abductor muscle action during level and stair ambulation.An EMG study, Phys. Ther. 63:1597-1605. 1983.
I?, Beckman, S.M,, and T.S. Buchanan, Ankle inversion injury andbypermobility: effect on bip and ankle muscle clectromyograpby onsetlatency. Arch. Phys- Med. Rehabil. 76:1138-1143, 1995.
18, Sapsford, R. Explanation of medical terminology (letter). NeuTOurol.Urodyn. 19:633, 2000,
19, O'Sullivan, P,B,, D.J. Beales, j.A, Beetham, et al. Altered motor controlstrategies in subjects with sacroiliac joint pain during the active straight'leg-raise test. Spine, 27:E1-E8, 2002.
20, Delitto, A., R,E. Erbard, and R.W. Bowling, A trearment-ba.scd classi-fication approach to low back syndrome: identifying and staging patientsfor conservative treatment, Phys. Ther. 75:470-485, 1995.
21, Fritï, J.M.. J,A. Cleland, and j.D. Childs, Subgrouping patients witb lowback pain: evolution of a classification approach to physical therapy,J, Orï/iop, Sports Phys. Ther. 37:290-302, 2007,
22, Hicks, G.E., J.M, Fritz, A, Delitto, and J, Mishock. Inter-rater reliabilityof clinical examination measures for identification of lumbar segmentalinstability. Arch, Phys. Med. Rehabil. 84:1858-1864, 2003,
23, Klenorman, L., P.D, Slade, 1,M, Stanley, ei d. The prediction of chro-nicity in patients witb an acute attack of low back pain in a generalpractice setting. Spine. 20:478^84, 1995,
24, Bamct, F., and W. Gilleard, Tbe use of lumbar spinal stabilizationtechniques during the performance of abdominal strengthening exercisevariations. ]. Sports Med. Phys. Fitness. 45:38-43, 2005,
25, Grenier, S.G., and S,M. McGill. Quantification of lumbar stability byusing two different abdominal activation .strategies. Arch, Phys. Med.RehabÜ. 88:54-62, 2007.
26, Arokoski, J,P,, T. Valta, M. Kankaanpaa, and O. Airaksinen. Activa-tion of lumbar paraspinal and abdominal muscles during therapeutic
exercises in chronic low back pain patients. Arch. Phys. Med. Rehahit.85:823-832, 2004.
27. Stanton, R,, P,R, Rcabum. and B. Humpbries. The effect of short-termSwiss ball training on core stability and running economy. ], StrengthGond, Res, 18:522-528, 2004.
28. Hicks, G., J.M. Friti, and A, Delinto, Preliminary development of aclinical prediction rule for determining wbich patients witb low buckpain will respond to a stabilization exercise program. Arch. Phys. Med.ReWjit 86:1753-1762, 2005.
29. Caims, M,C.. N,E, Foster, and C Wright, Randomized controlled trialof specific spinal stabilization exercises and conventional pbysiotbcrapyfor recurrent low back pain. Spine. 31:E67O-E68], 2006,
30. Juker, D,, S. McGill, P. Kropf, and T, Stefïcn. Quantitative intramuscu-lar myoelectric activity of lumbar portions of psoas and tbe abdominalwallduringawidevarietyoftasks, Med, Sa, S/xmsEiCTC. ÎO:30I-Î!0, 1998,
31. Farfan, H.F., J.W. Cossette, G,H, Robenson, ei cd. Tbe effects of torsionon tbe lumbar intervertébral joints: tbe role of torsion in tbe productionof disc degeneration. J. Bone Joint Surg. Am. 52:468-497, 1970,
32. Adams, M.A., P. Dolan, and W.C Hutton. Diurnal variations in thestresses on the lumbar spine. Spine. 12:130-137, 1987,
33. Stuge, B., E. Laerum, G. Kirkesola, and N. Vollestad. The efficacy of atreatment program focusing on specific stabilizing exercises for pelvic gir-dle pain after pa-gnancy: a randomized controlled trial. Spine. 29:351-359,2004.
34. Newcomer, K.L,, T.D. Jacohson, D,A, Gabriel, et al. Muscle activationpattems in subjects with and witbout low back pain. Arch. Phys. Med.Rehainl. 83:816-821, 2002.
35. Hungerford, B., W. Gilleard, and P, Hodges. Evidence of alteredlumbopelvic muscle recruitment in the presence of sacroiliac joint pain.Spine, 28:1593-1600, 2003,
56. Leeton, D.T., M.L Ireland, and J.D. Willson. Core stability measures asrisk factors fot lower extremity injury in athletes, Med, Sd. Sports Exerc.36:926--934. 2004.
37. Hewett, T,E,, T.N, Lindenfeld, J.V, Riccobene, and F,R, Noyes. Theeffect of neuromuscular training on the incidence of knee injury infemale atbletes, A prospective study. Am, } . Spam Med. 27:699-706,1999,
38. Hewett, T,E., G.D, Myer, and K.R, Ford. Reducing knee and anteriorcruciate ligament injuries among female atbletes: a sy.stcmatic review ofneuromuscular training interventions, /, Knee Surg. 18:82-88. 2005.
39. Heidt, R.S, Jr, L.M. Sweeterman. and R,L. Carlonas, Avoidance ofsoccer injuries with preseason conditioning. Am. J. Sports Med. 27:699-706. 1999,
40. Goldby, L.J.. A.P. Moore, J. Doubst, and M.E. Trew. A randomizedcontrolled trial investigating tbe efficacy of musculoskeleta! physiother-apy on cbronic low back di,sorder, .Spine. 31:1083-1093, 2006.
41. Hides, J.A., G.A. Jull, and C A . Richardson. Long-term effects ofspecific stabilizing exercises for first-epistxie low back pain. Spine,26:E243-E248, 2001.
42. O'Sullivan, P.B.. G.D, Phyty, L.T. Twomey, and G.T, Allison.Evaluation of specific stabilizing exercise in the treatment of cbroniclow back pain witb radiologie diagnosis of spondylolysis or spondylolis-thcsis. Spine. 22:2959-2967, 1997.
43. Shaughnessy. M., and B. Caulfield. A pilot study to investigate tbe effectof lumbar stabilization exercise training on functional ability and qualityof life in patients witb chronic low hack pain, ¡ni. } . Rehcdñl. Res.27:297-301. 2004.
44. Foster, N.E., K. Konstantinou, M. Lewis, et ai. A randomized controlledtrial investigating tbe efficacy of musculoskeletal physiotherapy onchronic low back disorder (comment). Spine, 31:2405-2406,2006.
45. Koumantakis, G,A., P,J. Watscin, and J,A, Oldbam. Trunk musck-stabilization training plus general exercise versus general exercise only:randomized controlled trial of patients with recurrent lowhack pain,Phys. Ther. 85:209-225. 2005,
46. Liddle, S,D., G.D. Baxter, and J.H. Gracey. Exercise and low back pain:what works? Pam. 107:176-190, 2004.
47. Hayden, J,A„ M.W. van Tulder. A. Matmivaara. and B.W. Koes,Exercise tberapy for treatment of non-specific low hack pain. GochrtwieDatabase Syst. Rev. 3:CDOOO35, 2005,
48. Slade. S.C., and J.L. Keating, Trunk-strengthening exercises for chroniclowback pain: a systematic review. J, Manipulative Phyüol. Ther.29tl63-173. 2006.
44 Current Sports Medicine Reports www.acsnKsmr.org
