copyright © 2006, duke internal medicine residency curriculum and dhts technology education...
TRANSCRIPT

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Wrist, Hand, Ankle, and Foot
Glen Xiong, MDChristopher Meyer, MD
Gordon Reeves, MDAmir Kahn, MD
Editor: Amy Shaheen, MD, Assistant Professor of Clinical Medicine
Duke University Medical Center

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Learning Objectives
• Demonstrate the basic elements of the wrist and hand exam and understand the clinical implications of findings.
• Understand the diagnostic approach to and management of carpal tunnel syndrome.
• Understand and be able to apply the Ottawa Ankle Rules.• Understand the basic management of foot fractures
including indications for emergent and non-emergent referrals.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Wrist and Hand

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Hand and Wrist Exam
• Inspection– Start with hands open and palms facing down
• Evaluate alignment of digits, muscular atrophy (thenar eminence), bony enlargement, swelling
– Inspect nails• Pitting, onycholysis, brown yellow
discoloration (Psoriasis)• Redness and telangectasias of nail-fold
capillaries (connective tissue disease)
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
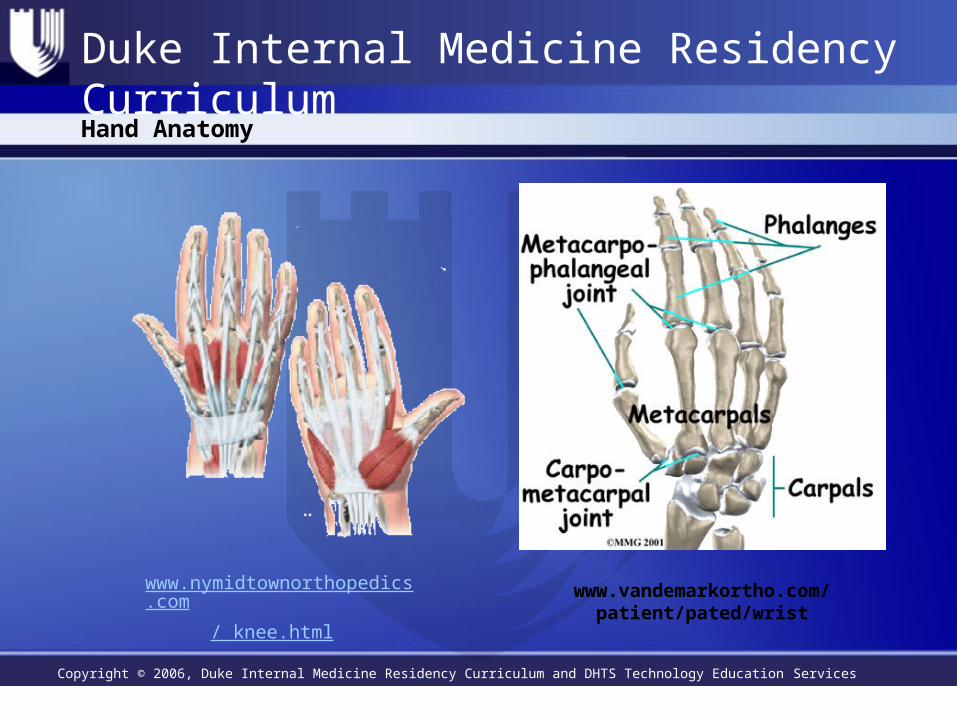
Hand Anatomy
www.vandemarkortho.com/ patient/pated/wrist
www.nymidtownorthopedics.com
/ knee.html
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Hand and Wrist Exam Cont
• Hand Function– Ask patient to open and close the hand
• Look for smooth and full movement
– Grip strength• Objective measurement of strength of
hand and forearm muscles• Can be estimated by gripping of the
examiner’s fingers• Dynometer is more accurate and
reproducible

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Hand and Wrist Exam Cont.
• Hand Function continued– Evaluate range of motion of wrist and
all hand joints– Evaluate sensation of the hand
•Pulp of index finger – median nerve•Pulp of the 5th finger – ulnar nerve•Dorsal web space between the
thumb and index finger – radial nerve

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Hand and Wrist Exam Cont
• DIP and PIP joints– Palpate by squeezing the joints
medially and laterally between the thumb and index finger
– Evaluate for enlargement, tenderness and/or synovial thickening

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Hand and Wrist Exam Cont
• MCP Joint– Palpate by squeezing the joint from between
the thumb and fingers– Swelling seen as fullness in the “valleys”
normally found between the knuckles– Pain with squeezing or swelling
• Single joint– Trigger finger, posttraumatic arthritis
• Multiple joints– RA (symmetric), psoriatic arthritis
(asymmetric or symmetric)

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Hand and Wrist Exam Cont
• Palpate the eight carpal bones by squeezing between your index finger and thumb
• Palpate the wrist with thumb over dorsal aspect and fingers beneath– Palpate the groove of the wrist, the
distal radius and ulna– Palpate the anatomic snuff box
•More visible with lateral extension of the thumb away from the hand

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Hand and Wrist Exam Cont
• Palpate flexor tendons – Feel for tenderness or cyst formation– Pain with passive stretching of the tendon in
extension indicates active tenosynovitis• Palpate palmar fascia
– Feel for nodularity – Nodularity may indicate palmar fibrosis,
which leads to Dupuytren’s contractures

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Hand and Wrist Exam Cont
• Inspect the dorsum of the hand– Evaluate for mucinous cysts
• may indicate herpetic whitlow, foreign body reaction, abscess or dermatofibroma
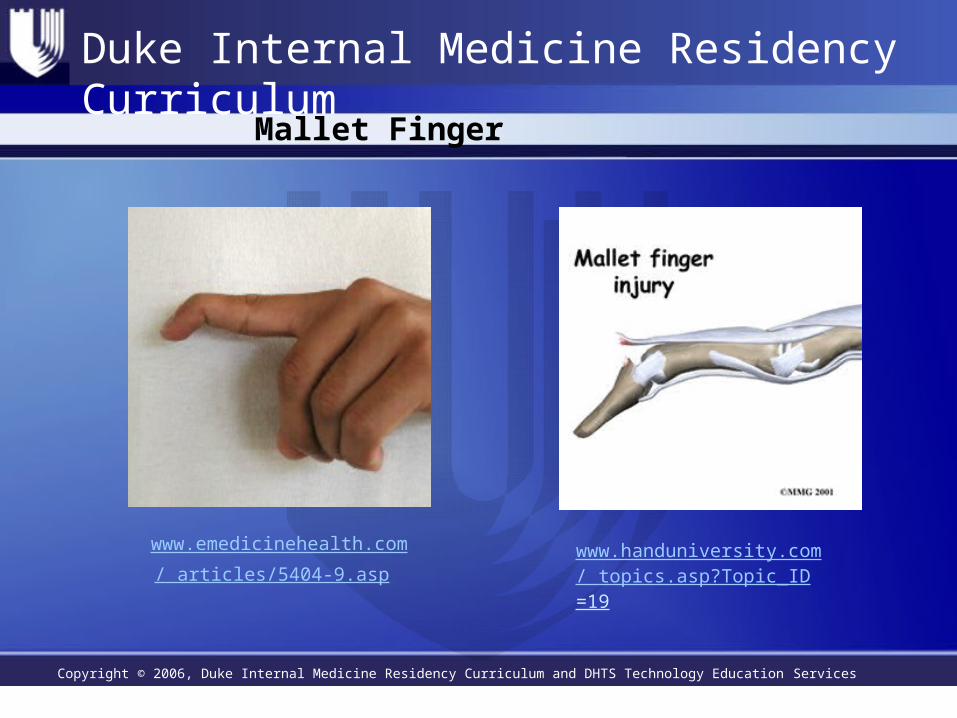
– Ask patient to actively extend DIP joints against resistance • Deficiency in patients with repeated blows
to the tip of the finger– Mallet finger
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Mallet Finger
www.handuniversity.com/ topics.asp?Topic_ID=19
www.emedicinehealth.com
/ articles/5404-9.asp

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Clincal Pearls
• Bony enlargement of PIPs (Bouchard’s node) and/or DIPs (Heberden’s Node) with minimal inflammation – likely OA
www.healthinplainenglish.com/. ../osteoarthritis/

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Clincal Pearls
• Symmetric deformity/inflammation in MCPs, PIPs, wrists over several weeks – likely RA– If DIP involvement and/or asymmetric with
nail changes consider psoriatic arthritis• Thenar atrophy – likely median nerve
compression from carpal tunnel syndrome• Hypothenar atrophy – ulnar nerve compression

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Clinical Pearls Cont.
• Loss of smooth motion of trigger finger + flexor tendon tenderness over MCP + pain with extension of the finger = likely trigger finger
• Flexion contractures of the ring, 5th, and 3rd fingers – think dupuytren’s contractures
• Inability to flex tip and characteristic deformity = mallet finger
• Tenderness over “snuffbox” – consider scaphoid fracture
• Tenderness over over ulnar styloid – consider Colles’ Fracture

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Carpal Tunnel Syndrome10
ACP medicine (Online) ACP medicine [electronic resource]. New York, N.Y. : WebMD

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Carpal Tunnel Syndrome3,4
• Pain and loss of hand function due to median nerve compression as it passes through the carpal tunnel in the wrist
• Prevalence – approx 3% of the adult population.• Women more than men approx 3:2 or 1. • Associated conditions (up to 1/3 of cases)
– Pregnancy, diabetes, hypothyroidism, inflammatory arthritis, amyloidosis, Colle’s fracture, use of corticosteroids and estrogens.
• Associated occupations (repetitive wrist/hand activities)– Food processing, manufacturing, construction, logging
• Natural History is variable – can lead to permanent nerve damage and hand dysfunction or be self-limiting.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
CTS – Diagnosis4
• Little to no data on physical diagnosis in pts presenting to PCP – studies generally based on referral population.
• Three tests most predictive of electrodiagnosis:– Hand symptom diagrams (pt fills in hand diagram depicting
symptoms): +LR 2.4, -LR 0.5• Classic or probable pattern: at least 1 of digits 1,2,3; wrist pain
radiating proximally; palmar pain unless solely ulnar.
– Hypalgesia: +LR 3.1, -LR not significant• Diminished sensation to painful stimuli on the palmar aspect
index finger
– Weak thumb abduction strength testing: +LR 1.8, -LR 0.5• Weakness in mov’t of thumb to right angle of hand.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
CTS – Diagnosis cont4
• May be helpful but not well validated – Square wrist sign (requires calipers), – Flick sign (ask pt to show you what they do when symptoms at their worst –
pt flicks wrist) – Close fist sign (symptoms reproduced when open and close fist x 60 sec).
• Phalen and Tinel signs found to be of limited utility.• Thenar atrophy – low sensitivity but specific. Likely represents
advanced disease.• Electrodiagnosis
– Although used as the gold standard for diagnosis in most studies of clinical diagnosis has false positives and false negatives.
– Best used in symptomatic pts to confirm diagnosis, e.g. prior to surgery, or to identify nerve entrapment at other locations.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
CTS – Treatment5,6
• Conservative treatment– Wrist splints – neutral position; relieve symptoms in up to
80% of pts.– NSAIDs
• Not supported by evidence, but typically done in practice– Activity modification– Corticosteroid injections – after above treatments have failed
• Short-term (1-3 months) improvement in symptoms compared to placebo or oral steroids. Long term not studied.
• No improvement compared to splinting + NSAIDs in one study– Ineffective or mixed results
• Likely ineffective - Diuretics, pyridoxine, non-steroidal anti-inflammatory drugs, yoga and laser-acupuncture
• There is conflicting evidence for the efficacy of ultrasound and oral steroids.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
CTS – Treatment cont7,8
• Surgical division of transverse carpal ligament– Although response to conservative treatment is initially
good, most have recurrence. – Failure of conservative treatments or thenar atrophy are
indications for referral.– Surgery provides better relief than splinting at 3mo and 1yr
f/u. – Good results with low complication rates– Can require weeks of missed work to recover– Various techniques can be open or endoscopic
• alternatives to standard open carpal tunnel release not clearly better.
• Conflicting evidence if endoscopic carpal tunnel release allows quicker return to ADLs/work.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Common causes of foot pain9,10
• Forefoot– Hallux valgus, hammer toe (PIP flexion), claw toe (PIP and
DIP), and mallet toe (isolated DIP)• Footwear with greater forefoot width and depth, orthoses, rarely
surgery
– Morton neuroma: entrapment neuropathy of the interdigital nerve, esp between 3rd and 4th metatarsal heads
• Orthoses, glucocarticoid injection, surgical excision.
• Midfoot– Arthritic changes or arch deformity– Tarsal tunnel syndrome – post tib nerve entrapment
• Pain and paresthesia over plantar and distal foot, + Tinel sign• Splinting, NSAIDs, steroid injection, surgical decompression.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Ankle & Foor
Ankle & Foot

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Ankle Tendons and ligaments
Lateral view of tendons and ligaments responsible for maintaining ankle articulation.
Wexler RK. The Injured Ankle. Am Fam Physician. 1998 Feb 1;57(3):474-80.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Ankle tendons & ligaments (2)
Medial view of tendons and ligaments responsible for maintaining ankle articulation.
Wexler RK. The Injured Ankle. Am Fam Physician. 1998 Feb 1;57(3):474-80.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Common Causes of Foot Pain10
ACP medicine (Online) ACP medicine [electronic resource]. New York, N.Y. : WebMD

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Common causes of foot pain9,10
• Hindfoot – Plantar fasciitis – most common cause (up to 15% of foot
symptoms requiring medical attention)• Runners, military, obesity, prolonged standing, pesplanus,
reduced ankle ROM• Pain over plantar heel to midfoot. • Most pts improve regardless of therapy in 6-12 months.• Orthoses, avoid barefoot walking, plantar and heel cord
stretches, NSAIDs, steroid injections, surgery.
– Achilles tendonitis or associated bursitis• Running/sports, ankylosing spondylitis, Reither syndrome,
fluoroquinolones (also associated with rupture), steroid use• Orthoses - particularly heel lifts, NSAIDs.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Plantar Fasciitis Exercises
• Towel StretchSit on the floor with your legs stretched out in front of you. Loop a towel around the top of the injured foot. Slowly pull the towel towards to keeping your body straight. Hold for 15 to 30 seconds then relax - repeat 10 times. (http://www.plantarfasciitisbraces.com/plantar_fasciitis_stretching_exercises.html)

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Plantar Fasciitis Exercises
• Calf/Achilles StretchStand facing a wall place your hands on the wall chest high. Move the injured heel back and with the foot flat on the floor. Move the other leg forward and slowly lean toward the wall until you feel a stretch through the calf, hold and repeat.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Plantar Fasciitis Exercises
• Stair StretchStand on a step on the balls for your feet, hold the rail or wall for balance. Slow lower the heel of the injured foot to stretch the arch of your foot.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Ottawa Ankle Rules
• Clinical "decision rules" to predict fractures, allowing radiography to be used more selectively
• 750 adult patients were evaluated in two emergency departments after presenting with acute blunt ankle injuries
• Follow-up study by applying the rules during evaluation of 2,342 patients with acute ankle injuries
Stiell et al. Implementation of the Ottawa ankle rules. JAMA 1994;271:827-32.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Ottawa Ankle Rules
An ankle radiographic series is required only if patient has pain in malleolar zone and any one of the following findings:1. Bone tenderness at the posterior edge or tip of the lateral malleolus2. Bone tenderness at the posterior edge or tip of the medial malleolus3. Inability to bear weight both immediately and in emergency department
Stiell et al. Implementation of the Ottawa ankle rules. JAMA 1994;271:827-32.

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Ottawa Foot Rules
A foot radiographic series is required only if patient has pain in midfoot zone and any one of the following findings: 1. Bone tenderness at the base of the fifth metatarsal2. Bone tenderness at the navicular3. Inability to bear weight both immediately and in emergency department

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Ottowa Ankle & Foot Rules
Ottawa Ankle & Foot Rules
http://www.healthservices.gov.bc.ca/msp/protoguides/gps/anklex.pdf

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Toe Fractures
• Most common type of foot fracture– Estimate to account for 9% of all fractures seen in the primary
care setting • Commonest etiologies: axial loading (“stubbing” toe),
hyperabduction, or crush injury • Clinical presentation usually localized pain; although also with
difficulty fitting into shoe or altered walking

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Toe Fractures: Clinical Presentation
• Ecchymosis and edema within first hours after injury• Point tenderness characteristic of underlying fracture; however
diffuse soft tissue inflammation and tenderness is common• Rotational deformity of nail bed (relative to adjacent nail beds)
indicative of displacement• Distal phalynx fracture can present as subungal hematoma

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Toe Fractures: Diagnosis
• Plain films should be obtained with AP, oblique and lateral views• Remember to evaluate for additional fractures after identifying one
fracture site is important—often multiple phalanges involved• Distal phalynx fractures commonly are comminuted

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Toe Fractures: Indications for Referral
• Emergent referral for open proximal phalanx fractures, fractures associated with gross contamination, or circulatory instability
• Dislocation of great toe, instability of reduced great toe fracture, or displaced intra-articular fractures (can lead to DJD)
• Management of open fractures in diabetics or immunosuppressed patients
• Complications from toe fractures (nonunion, chronic pain, osteomyelitis)

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Toe Fractures: Primary Care Mgmt
• “Buddy taping” (taping fractured to adjacent toe) with cushioning agent in between to prevent maceration (gauze, etc) mainstay of treatment– Pain unrelieved with buddy taping may require further
immobilization via short leg walking cast with foot plate• APAP or NSAIDs usually adequate analgesia• Continue immobilization until point tenderness resolves (usually 4-
6 weeks)

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Metatarsal Fractures
• Second most common type of foot fracture after toe fractures• Risk factors include osteoporosis, sedentary lifestyle,
benzodiazepine use, diabetes (particularly in patients with >25 years of disease or increased physical activity)
• Twisting or direct blows are most common mechanism of traumatic injury– First metatarsal infrequently injured due to increased relative
stability

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Metatarsal Fractures: Stress Fracture
• First described in 1855 as "march fractures" due to predilection for military recruits
• In contrast to traumatic fractures, occur with repeated administration of forces not powerful enough to cause fracture with single occurrence
• Second most common type of stress fracture in athletes (other than tibial stress fracture)

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Metatarsal Fractures: Presentation
• Traumatic fractures present typically with localized pain and difficulty ambulating
• Contrastingly stress fractures more sub-clinical– Dull aching pain during or immediately after activity– May present with poorly localized forefoot pain
• Pain with axial loading (applied pressure perpendicular to phalanx) differentiates fracture from soft tissue injury
• Greater pain with direct palpation compared to resisting plantar/dorsiflexion differentiates from tendon injury
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Metatarsal Fractures: Referral Indications
• Tenderness of the tarsometatarsal joint (Lisfranc joint) • Compartment syndrome rarely occurs
– Pain with passive toe flex/extension early sign– Pallor, parasthesia, out of proportion pain, tense swelling
should prompt consideration– Diminished or absent pulse is late finding
• Other indications include displaced 1st metatarsal fractures, multiple fractures, intraarticular fractures, displaced fractures near metatarsal head

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Metatarsal Fractures: Management
• Obtain AP, lateral, oblique plain film views• Minimally displaced/nondisplaced fractures: non weight bearing
for 3-5 days, elevation and ice for 24 hrs; then progressive weight bearing – After point tenderness resolves and callus formed on f/u plain
film injury considered healed--usually at least six weeks• Displaced fractures (greater than 3-4 mm or 10 deg angulation in
dorsal or plantar plane) reduced with regional block and placement of toes in Chinese finger trap

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Metatarsal Fractures: Management
• Initial mgmt of displaced fractures followed by placement in bivalved cast for 1-3 weeks, then converted to short-leg walking cast with progressive weight bearing
• Stress fracture usually treated only with cessation of inciting activity for 4-8 weeks followed by gradual reintroduction– Fifth metatarsal stress fractures are exception due to high
rates of nonunion and should be referred to orthopedics


Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
Please click here to complete the course evaluation
References follow this slide

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
References
1. Bickley L: Bates’ Guide to Physical Examination and History Taking 7th Edition. Lippincott Williams & Wilkins. 1999.
2. Klippel J: Primer on Rheumatic Diseases, Edition 12. Arthritis Foundation, 2001.
3. Katz JN, Simmons BP.Related Articles, Links Clinical practice. Carpal tunnel syndrome. N Engl J Med. 2002 Jun 6;346(23):1807-12. Review.
4. D'Arcy CA, McGee S.Related Articles, Links The rational clinical examination. Does this patient have carpal tunnel syndrome? JAMA. 2000 Jun 21;283(23):3110-7. Review.
5. O'Connor D, Marshall S, Massy-Westropp N. Non-surgical treatment (other than steroid injection) for carpal tunnel syndrome. Cochrane Database Syst Rev. 2003;(1):CD003219. Review.
6. Marshall S, Tardif G, Ashworth N. Local corticosteroid injection for carpal tunnel syndrome. Cochrane Database Syst Rev. 2002;(4):CD001554. Review
7. Verdugo RJ, Salinas RS, Castillo J, Cea JG. Surgical versus non-surgical treatment for carpal tunnel syndrome. Cochrane Database Syst Rev. 2003;(3):CD001552. Review

Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Duke Internal Medicine Residency Curriculum
References Cont.
8. Scholten RJ, Gerritsen AA, Uitdehaag BM, van Geldere D, de Vet HC, Bouter LM. Surgical treatment options for carpal tunnel syndrome. Cochrane Database Syst Rev. 2004 Oct 18;(4):CD003905. Review.
9. Essentials of musculoskeletal care / American Academy of Orthopaedic Surgeons, American Academy of Pediatrics ; Letha Yurko Griffin, editor. Rosemont, IL : American Academy of Orthopaedic Surgeons, 2005.
10. ACP medicine (Online) ACP medicine [electronic resource]. New York, N.Y. : WebMD
11. Fracture care by family physicians. A review of 295 cases Fam Pract 1994 Mar;38(3):238-44
12. Fracture care by family physicians -- J Am Board Fam Pract 1993 Mar-Apr;6(2):179-81
13. DeLee: DeLee and Drez's Orthopaedic Sports Medicine, 2nd ed., Copyright © 2003 Saunders
14. www.uptodate.com