copd
DESCRIPTION
copdTRANSCRIPT

CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)
Chronic obstructive pulmonary disease (COPD) is a disease of the lung. The lungs are the organs found in the chest which are invloved in breathing. Air enters the nose and mouth, then travels to the lungs via the trachea, which divides into smaller airways called bronchi and, subsequently, bronchioles. (See diagram below). The lung tissue itself is a spongy material, consisting of a series of folded membranes (the alveoli) which are located at the ends of very fine branching air passages (bronchioles). COPD is a disease of the smaller airways in the lungs. COPD encompases chronic obstructive bronchitis with obstruction of small airways and emphysema with enlargement of air spaces, destruction of lung parenchyma, loss of lung elasticity and closure of small airways.RISK FACTORS FOR CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)
Cigarette smoke is by far the most important factor in the development of COPD. If you smoke 30 cigarettes per day, you are 20 times more likely to die from COPD than non-smokers. The more you smoke, the greater your risk of severe disease. Smoking a pack a day for more than 20 years is considered a significant risk in the development of COPD. COPD is therefore largely preventable if you do not smoke.
Familial factors: A family history of COPD may increase your risk of having the disease. This may relate to hyper-reactive airways, a feature of asthma.
Alpha-1-antitrypsin deficiency: This substance is found in several places throughout the body and is important in preventing cells from breaking down, particularly those in the lungs and liver. People who do not have enough of this enzyme are at increased risk of emphysema and cirrhosis of the liver.
Exposure to air pollution. Recurrent airway infections: This may be important in the development
and progression of COPD. Prompt use of antibiotics and vaccinations may help reduce the impact of infections.
Other factors such as urbanization, social class, occupation and diet may also have some impact in the development of COPD, but their overall effect is not known.
PathogenesisChronic obstructive pulmonary disease (COPD) is a descriptive term given to the syndrome seen mostly in the elderly, who have airflow obstruction, not completely relieved by therapy. At least two distinct pathological processes may occur concurrently or separately in different subjects lead to COPD.These are:1. Emphysema which is due to destruction of alveolar walls2. Chronic bronchitis with hyper secretion of mucus,

CHRONIC BRONCHITIS – Chronic bronchitis is defined as a disease characterized by hypersecretion of mucus sufficient to cause cough and sputum on most days for at least three months in a year for two or more consecutive years. This happens in the absence of any other specific respiratory or cardiovascular disease. In the initial stages the inflammation of the bronchi is intermittent and recurrent, later it becomes established. The larger air passages are affected during the early part of the disease, later obstructive features set in when the smaller airways are also affected. Infection leads to periodic aggravation of the symptoms and the sputum, which is mucoid, becomes purulent during these episodes. As the airways obstruction progresses, emphysema sets in. These two processes become established in the majority of cases so that the condition is termed chronic bronchitis emphysema syndrome (CBES). The disease is more common in damp, cold, and dusty regions. Atmospheric pollution is accompanied by a higher incidence of CBES. PATHOGENESISCOPD encompases chronic obstructive bronchitis with obstruction of small airways and emphysema with enlargement of air spaces, destruction of lung parenchyma,loss of lung elasticity and closure of small airways.The inflammatory process in COPD differs from that in asthma in several ways. The type of inflammatory cells,inflammatory mediators, final outcome and response to treatment are different. In COPD the inflammation affects the peripheral airways-the bronchioles. The cells are macrophages, CD8 lymphocytes and neutrophils. The lung parenchyma is affected. Unlike as in asthma there is no preponderance of eosinophils.Oxidative stress also plays a significant role in the pathogenesis. Even though the lungs bear the main bruntof the disease, systemic effects also occur. Muscle weakness and wasting may develop as part of the systemic disorder.
.
CLINICAL FEATURESThe clinical picture is varied depending on the severity and duration. The most frequent early symptom is cough recurring year after year, especially so in winter months.Later the cough becomes constant. Expectoration is mucoid and the sputum is tenacious, especially on waking up in the morning. Main complaint is the feeling of tightness of the chest.Physical examination reveals mild wheeze which disappears as the patient clears the bronchi by expectoration. Variable degrees of bilateral rhonchi and coarse crepitations are heard as adventitious sounds.

Initially acute infections give rise to fever and purulent sputum. As the infection becomes established, fever and other general symptoms come down. At this stage the quantity and character of the sputum are more reliable indicators of infection. The sputum becomes copious in amount when bronchiectatic changes develop.With the development of emphysema the chest assumes the inspiratory position and the respiratory excursions are considerably diminished. At this stage dyspnea is far out of proportion to the physical findings in the chest.
DIAGNOSISChronic bronchitis should be diagnosed from the history of recurrent cough extending over several years,mucopurulent sputum and the physical findings of bronchial obstruction and emphysema. X-ray is normal in the early stages but the features of emphysema may be evident later. X-ray may be helpful in identifying precipitating conditions like pneumonia, pneumothorax during the time of an exacerbation. HRCT is useful in quantifying the severity of emphysematous changes and locating areas with bronchiectatic changes. Lung function tests show reduction in vital capacity,increase in the closing volume and features of airway obstruction . Based on the spirometry values severity of obstruction can be categorised as mild,moderate severe and very severe.
EMPHYSEMA – Emphysema is defined as a pathological increase in the size of airspaces distal to the terminal bronchioles, with destruction of the alveolar walls. The term hyperinflation is used to denote non-pathological overdistension.
EtiologyDiseases of the airways: Chronic bronchitis, prolonged exposure to irritants and dusts (heavy cigarette smoking),and chronic partial bronchial obstruction.Conditions associated with alpha-1 antitrypsin deficiency:Persons who have alpha-1 antitrypsin deficiency develop emphysema by the third or fourth decade of life.Chronic bronchial asthma leads on to emphysema as a sequel. Persons who have to hold breath for prolonged periods for diving under water for collecting shells, clayand the like develop emphysema over a period of 15-20years. Bidi or cigarette smoking and repeated respiratory infections accelerate the process.Several pneumoconioses give rise to emphysema as part of the pathological process or as compensatory mechanism, e.g. coal worker’s pneumoconiosis, silicosis.Occupational causes: Several occupations which require forced expiratory effort as seen in furnace blowers,goldsmiths, and users of wind instruments predispose to the development of emphysema in susceptible subjects.Exposure to cadmium leads to the development of emphysema and pulmonary fibrosis.

Pathology: The lungs are in the inflated position occupying the whole of the pleural cavity. Since the elastic tissue is damaged, the lungs lose their elasticity and they fail to collapse when the chest is opened during autopsy. The diaphragm is depressed and respiratory excursions are diminished. The alveoli are overdistended. The septa rupture and neighbouring alveoli coalesce to form air cysts. The pulmonary vascular bed is progressively diminished and pulmonary arterial hypertension results.Reduction of alveolar surface area leads to impairment of gas exchange. Right ventricular hypertrophy and corpulmonale may develop. Emphysematous bullae may rupture to produce spontaneous pneumothorax.
CLINICAL FEATURESThe main symptom is exertional dyspnea. As the condition progresses, even ordinary activity like talking, eating or lying flat may cause dyspnea.The chest is distended in the position of full inspiration. Expansion is diminished and the accessory muscles of respiration are active.Expiration becomes an active process due to loss of elasticity of the lung. Infective episodes occur frequently.Physical examination reveals barrel-shaped chest with diminished expansion, hyper-resonance on percussion,obliteration of cardiac and liver dullness and diminished breath sounds with prolonged expiration. Due to increased intrathoracic pressure especially during expiration, the neck veins become distended during expiration and collapse during inspiration. The apex beat is felt feebly because of interposition of the distended lung. Right ventricular hypertrophy produces a heaving impulse in the epigastrium and subxiphoid region. Left parasternal heave may not be evident on account of the inflated lung covering the heart SPECIAL FORMS OF EMPHYSEMACompensatory emphysema: This is the condition in which the normal lung tissue undergoes hypertrophy to compensate for extensive damage to the other lung or other parts of the same lung. Being a compensatory phenomenon, this is asymptomatic. The respiratory excursion of the normal lung is increased in this case.Atrophic emphysema: This condition is the result of senile atrophy of inter-alveolar septa. The total lung volume is not increased.Bullous emphysema: In this condition air spaces exceeding 1 cm in diameter develop either congenitally or as a part of acquired generalized emphysema. With passage of time these bullae enlarge and become giant bullous emphysema. They may rupture to produce pneumothorax. At times the bullae may get infected to produce abscesses
ANOTHER TYPEThere are two main types of emphysema, based on the changes taking place in the lung: panlobular (panacinar) and centrilobular (centroacinar)Both types may occur in the same patient. In the panlobular (panacinar) type, there is destruction of the respiratory bronchiole, alveolar duct, and alveoli. All air spaces within the lobule are essentially enlarged, but there is little inflammatory disease. The patient with this type of emphysema typically has a hyperinflated (hyperexpanded) chest (barrel chest on physical examination), marked dyspnea on exertion, and weight loss. To move air into and out of the lungs, negative pressure is required during inspiration, and an adequate level of positive pressure must be attained and maintained during expiration.The resting position is one of inflation. Instead of being an involuntary passive act, expiration becomes active and requires mus.In the centrilobular (centroacinar) form, pathologic changes take place mainly in the center of the secondary lobule, preserving the peripheral portions

of the acinus. Frequently, there is a derangement of ventilation–perfusion ratios, producing chronic hypoxemia, hypercapnia (increased CO2 in the arterial blood),polycythemia, and episodes of right-sided heart failure. This leads to central cyanosis, peripheral edema, and respiratory failure.The patient may receive diuretic therapy for edema.Alpha-1 Antitrypsin DeficiencyAlpha-1 antitrypsin (AAT) is one among the serine protein inhibitors which occurs in the plasma. It is an inhibitor of neutrophil elastase. It has also got anti-inflammatory properties. AAT is a glycoprotein normally secreted by the liver and circulating in blood. It moves with the alpha-I band on serum protein electrophoresis. 90% of the trypsininhibitory activity of serum is attributable to AAT.From the plasma, AAT diffuses into lung tissues, where it acts as an anti-elastase, the elastase being secreted by neutrophils. Elastase is capable of destroying the connective tissue framework of alveolar walls. Excessive destruction of alveolar walls may lead to emphysema.Cigarette smoking which predisposes to accumulation of neutrophils in the lung aggravates the destructive process.Cigarette smoke also inhibits AAT directly. AAT deficiency may be congenital or acquired. The gene frequency of the defect occurs in 1 in 2000 to 1 in 5000 of the population. In the congenital form it is transmitted as an autosomal recessive. More than 75 alleles of AAT gene are known. In the inherited form the hepatic production of AAT is less than 15% of normal.Patients with AAT deficiency develop panacinar emphysema by the third or fourth decade of life. The congenital form may also be associated with hepatitis and jaundice in the newborn and cirrhosis liver in adults. Such patients show accumulation of abnormal AAT in hepatocytes.AAT deficiency can be treated by replacing AAT byIV infusion weekly or monthly to individuals whose serum AAT levels are below 1 mmol/L and who have abnormal lung functions. AAT for therapeutic purposes is obtained from pooled plasma. AAT can also be administered as an aerosol.PATHOPHYSIOLOGY
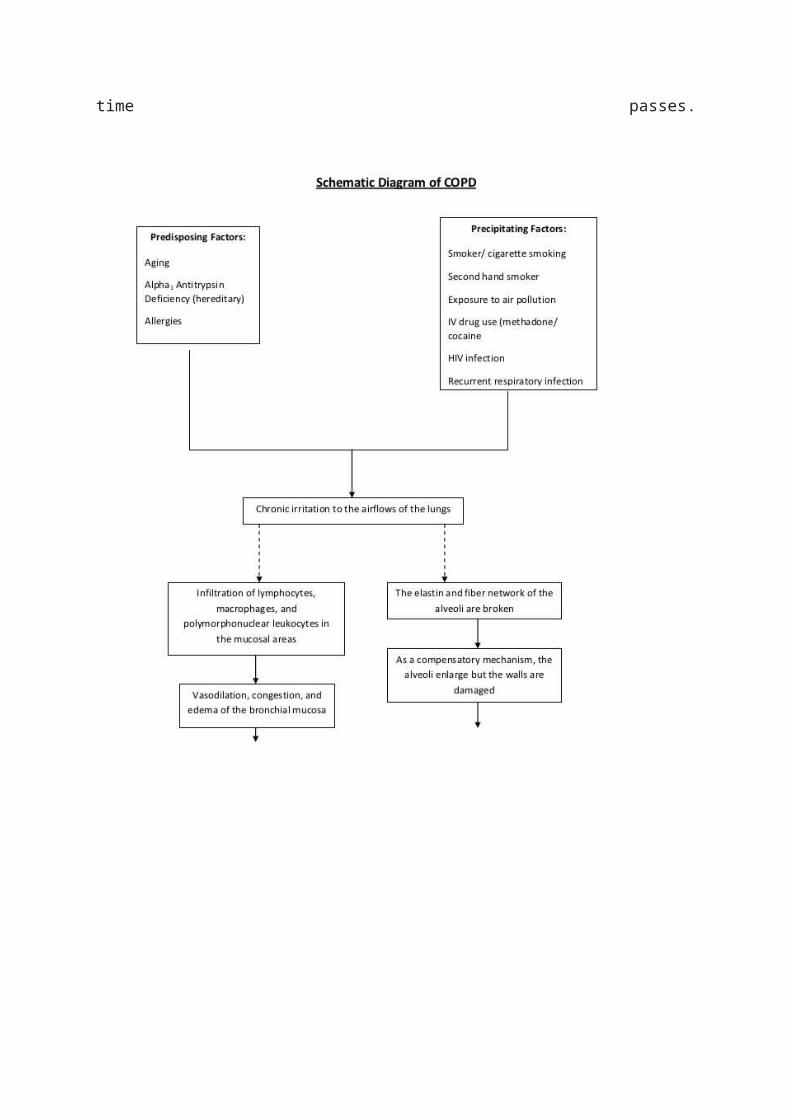
COPD develops as a significant and chronic inflammatory response to inhaled irritants. Chronic bacterial infections may also add to this inflammatory state. The inflammatory cells involved include neutrophil granulocytes and macrophages, two types of white blood cell. Those who smoke additionally haveTc1 lymphocyte involvement and some people with COPD have eosinophil involvement similar to that in asthma. Part of this cell response is brought on by inflammatory mediators such as chemotactic factors. Other processes involved with lung damage include oxidative stress produced by high concentrations of free radicals in tobacco smoke and released by inflammatory cells, and breakdown of the connective tissue of the lungs by proteases that are insufficiently inhibited by protease inhibitors. The destruction of the connective tissue of the lungs is what leads to emphysema, which then contributes to the poor airflow and, finally, poor absorption and release of respiratory gases.General muscle wasting that often occurs in COPD may be partly due to inflammatory mediators released by the lungs into the blood.
Narrowing of the airways occurs due to inflammation and scarring within them. This contributes to the inability to breathe out fully. The greatest reduction in air flow occurs when breathing out, as the pressure in the chest is compressing the airways at this time. This can result in more air from the previous breath remaining within the lungs when the next breath is started, resulting in an increase in the total volume of air in the lungs at any given time, a process called hyperinflation or air trapping.Hyperinflation from exercise is linked to shortness of breath in COPD, as it is less comfortable to breathe in when the lungs are already partly full.
Some also have a degree of airway hyper responsiveness to irritants similar to those found in asthma. Low oxygen levels and, eventually, high carbon dioxide levels in the blood can

occur from poor gas exchange due to decreased ventilation from airway obstruction, hyperinflation and a reduced desire to breathe. During exacerbations, airway inflammation is also increased, resulting in increased hyperinflation, reduced expiratory airflow and worsening of gas transfer. This can also lead to insufficient ventilation and, eventually, low blood oxygen levels. Low oxygen levels, if present for a prolonged period, can result in narrowing of the arteries in the lungs, while emphysema leads to breakdown of capillaries in the lungs. Both these changes result in increased blood pressure in the pulmonary arteries, which may cause cor pulmonale.
The main pathological process can be summarized as follows:1. Inflammation of the bronchi with enlargement of mucous glands and smooth muscle hyperplasia, all leading to wall thickening2. Acinar distension due to the destruction of lung parenchyma probably mediated by imbalance of protease-antiprotease (alpha-1 antitrypsin) enzymes causing loss of support of small airways3. Fibrosis and narrowing of the airways leading to increase in airway resistance.The capillary bed is distorted and truncated and this aggravates the progression of pulmonary arterial hypertension. The pulmonary arteries become distended and atheromatous. Pulmonary hypertension gives rise to right ventricular hypertrophy and dilatation. Chronic

corpulmonale supervenes as time passes.

SYMPTOMS HISTORYThe three most common symptoms in COPD are cough, sputum production, and exertional dyspnea. A careful history, however, usually reveals the presence of symptoms prior to the acute exacerbation. The development of exertional dyspnea, often described as increased effort to breathe, heaviness, air hunger, or gasping, can be insidious. It is best elicited by a careful history focused on typical physical activities and how the patient’s ability to perform them has changed.Activities involving significant arm work, particularly at or above shoulder level, are particularly difficult for patients with COPD.As COPD advances, the principal feature is worsening dyspnea on exertion with increasing intrusion on the ability to perform vocational or avocational activities.In the most advanced stages, patients are breathless doing simple activities of daily living.Accompanying worsening airflow obstruction is an increased frequency of exacerbations (described below). Patients may also develop resting hypoxemia and require institution of supplemental oxygen.PHYSICAL FINDINGSIn the early stages of COPD, patients usually have an entirely normal physical examination. Current smokers may have signs of active smoking, including an odor of smoke or nicotine staining of fingernails. In patients with more severe disease, the physical examination is notable for a prolonged expiratory phase and may include expiratory wheezing. In addition, signs of hyperinflation include a barrel chest and enlarged lung volumes with poor diaphragmatic excursion as assessed by percussion. Patients with severe airflow obstruction may also exhibit use of accessory muscles of respiration, sitting in the characteristic “tripod” position to facilitate the actions of the sternocleidomastoid, scalene, and intercostals muscles. Patients may develop cyanosis, visible in the lips and nail beds.Although traditional teaching
is that patients with predominant emphysema, termed “pink puffers,” are thin and noncyanotic at rest and have prominent use of accessory muscles, andpatients with chronic bronchitis are more likely to be heavy and cyanotic (“blue bloaters”), current evidence demonstrates that most patients have elements of both bronchitis and emphysema and that the physical examination does not reliably differentiate the two entities.Advanced disease may be accompanied by systemic wasting, with significant weight loss,bitemporal wasting, and diffuse loss of subcutaneous adipose tissue. This syndrome has been associated with both inadequate oral intake and elevated levels of inflammatory cytokines (TNF-α). Such wasting is an independent poor prognostic factor in COPD. Some patients with advanced disease have paradoxical inward movement of the rib cage with inspiration (Hoover’s sign), the result of alteration of the vector of diaphragmatic contraction on the rib cage as a result of chronic hyperinflation.Signs of overt right heart failure, termed cor pulmonale, are relatively infrequent since the advent of supplemental oxygen therapy.Clubbing of the digits is not a sign of COPD, and its presence alert the clinician to initiate an investigation for causes of clubbing. In this population, the development of lung cancer is the most likely explanation for newly developed clubbing.Often the cough will be associated with sputum production that is whitish in color, mucoid in quality and is worse in the morning. During acute exacerbations the mucus will often turn purulent and the patient may have a fever. Some patients will have a history of hemoptysis. Anteriorposterior diameter of the chest may be increased. cyanosis, signs of right heart failure (cor pulmonale) including enlarged tender liver, neck vein distention especially during expiration. Key Indicators for Considering the Diagnosis of COPDChronic cough: Present intermittently or every day. Often present throughout the day; seldom only nocturnal Chronic sputum Any pattern of chronic sputum production: production may indicate COPDAcute bronchitis: Repeated episodesDyspnea that is: Progressive (worsens over time), Persistent (present every day)Worse on exercise, Worse during respiratory, infectionsHistory of exposure to Tobacco smoke (including risk factors: popular local preparations)Occupational dusts and chemicals and smoke from home cooking and heating fuel.Diagnosis: Chronic bronchitis should be diagnosed from the history of recurrent cough extending over several years, muco purulent sputum and the physical findings of bronchial obstruction and emphysema. X-ray is normal in the early stages but the features of emphysema may be evident later. X-ray may be helpful in identifying precipitating conditions like pneumonia, pneumothorax during the time of an exacerbation. HRCT is useful in quantifying the severity of emphysematous changes and locating areas with bronchiectatic changes. Lung function tests show reduction in vital capacity,increase in the closing volume and features of airway obstruction Based on the spirometry values severity of obstruction can be categorised as mild,moderate severe and very severe.
computed tomography scan of the chest may show the distribution of emphysema throughout the lungs and can also be useful to exclude other lung diseases.Unless surgery is planned, however, this rarely affects management.
An analysis of arterial blood is used to determine the need for oxygen; this is recommended in those with an FEV1 less than 35% predicted, those with a peripheral oxygen saturation of less than 92% and those with symptoms of congestive heart failure.
In areas of the world where alpha-1 antitrypsin deficiency is common, people with COPD (particularly those below the age of 45 and with emphysema affecting the lower parts of the lungs) should be considered for testing.

Check pulmonary function tests (PFT’s). Two main components are measured to make the diagnosis: the forced expiratory volume in one second (FEV1), which is the greatest volume of air that can be breathed out in the first second of a breath, and the forced vital capacity (FVC), which is the greatest volume of air that can be breathed out in a single large breath. Normally, 75–80% of the FVC comes out in the first second and a FEV1/FVC ratio of less than 70% in someone with symptoms of COPD defines a person as having the disease.Based on these measurements, spirometry would lead to over-diagnosis of COPD in the elderly. The National Institute for Health and Care Excellence criteria additionally require a FEV1 of less than 80% of predicted.
MRC shortness of breath scale
Grade
Activity affected
1 Only strenuous activity
2 Vigorous walking
3 With normal walking
4 After a few minutes of walking
5 With changing clothing
GOLD grade
Severity FEV1 % predicted
Mild (GOLD 1) ≥80
Moderate (GOLD 2) 50–79
Severe (GOLD 3) 30–49
Very severe (GOLD 4)
<30 or chronic respiratory failure

Prevention
Most cases of COPD are potentially preventable through decreasing exposure to smoke and improving air quality.Annual influenza vaccinations in those with COPD reduce exacerbations, hospitalizations and death.. Pneumococcal vaccination may also be beneficial.
TREATMENT Management of chronic respiratory failure: When hypoxemia becomes severe, i.e. PaO2 below 55 mm Hg or SaO2 below 80% at rest, continuous oxygen inhalation may haveto be instituted for at least 18 hours a day. Oxygen therapy helps to reduce pulmonary arterial tension and allay cor pulmonale. In intractable cases lung transplantation mayhave to be considered.
Table 1
SMOKES, a consultation checklist for chronic obstructive pulmonary disease
S: smoking cessation
M: medication - inhaled bronchodilator, vaccines (influenza, pneumococcus), stop unnecessary treatment (nebuliser, inhaled corticosteroids)
O: oxygen - is it needed?
K: komorbidity - cardiac dysfunction, sleep apnoea, osteoporosis, depression, asthma
E: exercise and rehabilitation
S: surgery - lung volume reduction surgery, single-lung transplantationgeneral measures: Most effective single step to prevent deterioration is to stop smoking. This single measure itself affords considerable relief of symptoms.Environmental allergens and pollutants must be avoidedby the patient.Other general measures include improvement in general health, regular exercise, deep-breathing exercises,adequate sleep, treatment of obesity, and eradication of foci of sepsis in the throat, nose and paranasal sinuses. If these measures are started during the early phase of the disease, further progression can be arrested. Steam inhalations help to improve vital capacity, relieve
:DRUG THERAPY
Bronchodilators
Inhaled bronchodilators are the primary medications used. There are two major types, β2 agonists and anticholinergics; both exist in long-acting and short-acting forms. They reduce shortness of breath, wheeze and exercise limitation, resulting in an improved quality of life. then inhaled corticosteroids are typically added. With respect to long-acting agents, it is unclear if tiotropium (a long-acting anticholinergic) or long-acting beta agonists (LABAs) are better, and it may be worth trying each and continuing the one that worked best.Both types of agent appear to reduce the risk of acute exacerbations by 15–25%.While both may be used at the same time, any benefit is of questionable significance.short-acting β2 agonists available including salbutamol (Ventolin)

and terbutaline.They provide some relief of symptoms for four to six hours. Long-acting β2 agonists such as salmeterol and formoterol are often used as maintenance therapy.
There are two main anticholinergics used in COPD, ipratropium and tiotropium. Ipratropium is a short-acting agent while tiotropium is long-acting. Tiotropium is associated with a decrease in exacerbations and improved quality of life, and tiotropium provides those benefits better than ipratropium.It does not appear to affect mortality or the over all hospitalization rate.
Anticholinergics can cause dry mouth and urinary tract symptoms. They are also associated with increased risk of heart disease and stroke.
Corticosteroids
Corticosteroids are usually used in inhaled form but may also be used as tablets to treat and prevent acute exacerbations. While inhaled corticosteroids (ICS) have not shown benefit for people with mild COPD, they decrease acute exacerbations in those with either moderate or severe disease. prednisolone 30-40 mg daily for 14 days
Other medication
Long-term antibiotics, specifically those from the macrolide class such as erythromycin, reduce the frequency of exacerbations in those who have two or more a year. This practice may be cost effective in some areas of the world. Concerns include that of antibiotic resistance and hearing problems with azithromycin. Methylxanthines such as theophylline generally cause more harm than benefit and thus are usually not recommended, but may be used as a second-line agent in those not controlled by other measures.
Mucolytics may be useful in some people who have very thick mucous but are generally not needed. Cough medicines are not recommended.
alpha-1-antitrypsin deficiency, may also be treated with weekly or monthly injections of
alpha-1-antitrypsin. Oxygen therapyIf you have severe airflow limitation you may require home oxygen therapy, sometimes for up to 19 hours per day. Oxygen can be administered via nasal prongs (small plastic tubes into your nose) or via a mask. This treatment has been shown to prolong life in patients with severe COPD who have stopped smoking. The best benefit from oxygen treatment is obtained if you have quit smoking. Furthermore, oxygen is flammable, so smoking is in fact dangerous during this treatment. Nonpharmacological measures: Noninvasive positive pressure ventilation and oxygen therapy at home using a simple nasal mask which eliminates the need for endotracheal intubation is beneficial. Long-term oxygen therapy has shown improved survival with better quality of life.
SURGICAL MANAGEMENT Bullectomy. A bullectomy is a surgical option for select patients with bullous emphysema. Bullae are enlarged airspaces that do not contribute to ventilation but occupy space in the thorax;these areas may be surgically excised. Many times these bullae compress areas of the lung that do have adequate gas exchange.Bullectomy may help reduce dyspnea and improve lung function. It can be done thoracoscopically (with a video-assisted thoracoscope) or via a limited thoracotomy incisionLung volume reduction surgery (LVRS): This has been found to be useful in selected cases. The rationale for this technique is to reduce the volume of over inflated emphysematous lung by 20-30%, in order to improve the elastic recoil of the lungs, to improve the configuration of the diaphragm, chest wall mechanics and gas exchange.Lung transplantation: This procedure is in vogue for more than a decade in advanced countries, it is still not available in India. Transplantation of a single lung or both heart and lungs as a whole is

possible. Transplantation should be considered if the recipient is below 55 years of age, and is free from underlying conditions such as advanced diabetes, malignancy, hepatic or renal failure and conditions which impair mechanics of the chest wall.The donor should be ABO and HLA compatible with normal lungs, preferably between 12 and 50 years of age and with normal cardiopulmonary anatomy. Usually cadaver lungs are used for transplantation. Complications may occur as in the case of any other major organtransplantation.Indications1. Incurable respiratory failure—chronic or acute due topulmonary causes2. Irreversible structural and functional abnormalities inthe lung such as fibrosis, extensive bronchiectasis,cystic disease, emphysema and others.Other Vaccinations: It is important that you have your yearly influenza vaccination,
and pneumococcal vaccine. This will help reduce effective exacerbations from these infections;
Diuretics: If your chronic bronchitis is complicated by right heart failure, you may be treated with tablets to remove the excess fluid;
Acute exacerbations of COPD: Acute attacks should be treated with bronchodilators, supplemental oxygen, antibiotics and glucocorticoids;
Depression: COPD is a chronic disease that may lead to significant disability, so some patients may become depressed. Counselling and antidepressant medications may help you overcome this;
Weight control: It is important that you maintain a healthy weight and nutrition. In advanced disease you may notice marked weight loss. You should have a high fat content and nutritious diet to prevent muscle wasting. Alternatively, if you are markedly overweight or obese you should try to reduce your weight to a healthy range with diet an exercise, in order to reduce demands on your lung function.
COPD OF COMPLICATIONS:Secondary polycythaemia: This is an increase in the number of red blood cells in the blood to try to compensate for reduced oxygen levels. The blood subsequently becomes ‘thicker’ with sluggish flow which can lead to clotting;Hypoxaemic respiratory failure (type I respiratory failure): PaO2 is less than 60 mm Hg (8 kPa) with a normal or low PaCO2. This is caused by ventilation-perfusion mismatch with either/both:
Under-ventilated alveoli (eg pulmonary oedema, pneumonia or acute asthma).
Venous blood bypasses ventilated alveoli (eg right to left cardiac shunts).
Hyperventilation increases CO2 removal but does not increase oxygenation, as
blood leaving unaffected alveoli is almost fully saturated.
Hypercapnic respiratory failure (type II respiratory failure): PaCO2 is more than 50
mm Hg (6.5 kPa) and indicates inadequate alveolar ventilation. Any ventilation-
perfusion mismatch will affect PaO2 and therefore hypoxaemia is also common.

Respiratory failure may be acute or chronic
Acute hypercapnic respiratory failure develops over minutes to hours. The pH is
usually therefore less than 7.3.
Chronic respiratory failure develops over several days or longer. There is sufficient time
for renal compensation and an increase in bicarbonate so the pH is usually only slightly
decreased. Clinical markers of long-standing hypoxaemia include polycythaemia
and cor pulmonale.
Causes-Common causes of type I respiratory failure
Chronic obstructive pulmonary disease (COPD).
Pneumonia.
Pulmonary oedema.
Pulmonary fibrosis.
Asthma.
Pneumothorax.
Pulmonary embolism.
Pulmonary hypertension.
Cyanotic congenital heart disease.
Bronchiectasis.
Acute respiratory distress syndrome.
Kyphoscoliosis.
Obesity
Add notes to aCommon causes of type II respiratory failure
COPD.
Severe asthma.
Drug overdose, poisoning.
Myasthenia gravis.
Polyneuropathy.
Poliomyelitis.
Muscle disorders.
Head injuries and neck injuries.
Obesity.
Pulmonary oedema.

Adult respiratory distress syndrome.
Hypothyroidism.
Pneumothorax: This is leakage of air from the lung into the surrounding
pleural space due to rupture of a bulla (dilated air space). This can lead to
collapse of the lung and may require insertion of a chest drain;
Respiratory failure: This is often caused by acute infective exacerbations. Death can sometimes occur from a severe decline in respiratory function.Cor pulmonale is failure of the right side of the heart, the side that pumps blood to the lungs. This problem occurs when the heart has to work harder to pump blood through damaged lungs, such as when a person's lungs are damaged because of chronic obstructive pulmonary disease (COPD).People with cor pulmonale are short of breath because of their damaged lungs. They may have swollen legs and a swollen abdomen because of fluid retention (edema).Pneumonia is a lung infection that can make you very sick. You may cough, run a fever, and have a hard time breathing. It can usually be treated at home, but some people need to go to the hospital. Pneumonia can be caused by bacteria or a virus. Antibiotics are used to treat pneumonia caused by bacteria.

NURSING MANAGEMENT patient educationPatient education is a major component of pulmonary rehabilitation and includes a broad variety of topics. Depending on the length and setting of the program, topics may include normal anatomy and physiology of the lung, pathophysiology and changes with COPD, medications and home oxygen therapy, nutrition, respiratory therapy treatments, symptom alleviation, smoking cessation, sexuality and COPD, coping with chronic disease,communicating with the health

care team, and planning for the future (advance directives, living wills, informed decision making about health care alternatives).
Pulmonary rehabilitationChest physiotherapy has been shown to help remove fluid in the airways. Various techniques are available such as steam inhalation, which assists sputum removal and improves your ventilation. Your doctor will also enter you into exercise or pulmonary rehabilitation programs which have been shown to increase exercise tolerance, relieve symptoms and improve your quality of life. Blowing into an air pillow repeatedly for 10-15 times twice a day and bending over a pillow held firmly on to the abdomen, in order to push the diaphragm up during expiration are simple maneuvers which can be practised at home.
Breathing Exercises. The breathing pattern of most people with COPD is shallow, rapid, and inefficient; the more severe the disease, the more inefficient the breathing pattern. With practice,this type of upper chest breathing can be changed to diaphragmatic breathing, which reduces the respiratory rate, increases alveolar ventilation, and sometimes helps expel as much air as possible during expiration (technique). Pursedlip breathing helps to slow expiration, prevents collapse of small airways, and helps the patient to control the rate and depth of respiration.It also promotes relaxation, enabling the patient to gain control of dyspnea and reduce feelings of panic.Inspiratory Muscle Training. Once the patient masters diaphragmatic breathing, a program of inspiratory muscle trainingmay be prescribed to help strengthen the muscles used in breathing. This program requires that the patient breathe against resistance for 10 to 15 minutes every day. As the resistance is graduallyincreased, the muscles become better conditioned. Conditioning of the respiratory muscles takes time, and the patient is instructed to continue practicing at home Activity Pacing. A patient with COPD has decreased exercise tolerance during specific periods of the day. This is especially true on arising in the morning, because bronchial secretions collect in the lungs during the night while the person is lying down. The patient may have difficulty bathing or dressing. Activities requiring the arms to be supported above the level of the thorax may produce fatigue or respiratory distress but may be tolerated better after the patient has been up and moving around for an houror more. Working with the nurse, the patient can reduce these limitations by planning self-care activities and determining the best time for bathing, dressing, and daily activities.Self-Care Activities. As gas exchange, airway clearance, and the breathing pattern improve, the patient is encouraged to assume increasing participation in self-care activities. The patient is taught to coordinate diaphragmatic breathing with activities such as walking, bathing, bending, or climbing stairs. The patient should bathe, dress, and take short walks, resting as needed to avoid fatigue and excessive dyspnea. Fluids should always be readily available, and the patient should begin to drink fluids without having to be reminded. If postural drainage is to be done at home,

the nurse instructs and supervises the patient before discharge or in the outpatient setting.Physical Conditioning. Physical conditioning techniques include breathing exercises and general exercises intended to conserve energy and increase pulmonary ventilation. There is a close relationship between physical fitness and respiratory fitness.Graded exercises and physical conditioning programs using treadmills, stationary bicycles, and measured level walks can improve symptoms and increase work capacity and exercise tolerance. Any physical activity that can be done regularly is helpful. Lightweight portable oxygen systems are available for ambulatory patients who require oxygen therapy during physicalactivity.Oxygen Therapy. Oxygen supplied to the home comes in compressed gas, liquid, or concentrator systems. Portable oxygen systems allow the patient to exercise, work, and travel. To help thepatient adhere to the oxygen prescription, the nurse explains the proper flow rate and required number of hours for oxygen use as well as the dangers of arbitrary changes in flow rates or durationof therapy. The nurse cautions the patient that smoking with or near oxygen is extremely dangerous. The nurse also reassures the patient that oxygen is not “addictive” and explains the need for regular evaluations of blood oxygenation by pulse oximetry or arterial blood gas analysis.Nutritional Therapy. Nutritional assessment and counseling are important aspects in the rehabilitation process for the patient with COPD. Approximately 25% of patients with COPD are undernourished .A thorough assessment of caloric needs and counseling about meal planning and supplementation are part of therehabilitation process.Coping Measures. Any factor that interferes with normal breathing quite naturally induces anxiety, depression, and changes in behavior. Many patients find the slightest exertion exhausting.Constant shortness of breath and fatigue may make the patient irritable and apprehensive to the point of panic. Restricted activity(and reversal of family roles due to loss of employment), the frustration of having to work to breathe, and the realization that the disease is prolonged and unrelenting may cause the patient toreact with anger, depression, and demanding behavior. Sexual function may be compromised, which also diminishes self-esteem. In addition, the nurse needs to provide education and support tothe spouse/significant other and family because the caregiver role in end-stage COPD can be difficult.
NURSING PRIORITIES
1. Maintain airway patency.
2. Assist with measures to facilitate gas exchange.
3. Enhance nutritional intake.
4. Prevent complications, slow progression of condition.
5. Provide information about disease process/prognosis and treatment
regimen.
Discharge Goals

1. Ventilation/oxygenation adequate to meet self-care needs.
2. Nutritional intake meeting caloric needs.
3. Infection treated/prevented.
4. Disease process/prognosis and therapeutic regimen understood.
5. Plan in place to meet needs after discharge.
1. Ineffective Airway Clearance
Nursing Diagnosis
Ineffective Airway Clearance
May be related to
Bronchospasm
Increased production of secretions; retained secretions; thick, viscous
secretions
Allergic airways
Hyperplasia of bronchial walls
Decreased energy/fatigue
Possibly evidenced by
Statement of difficulty breathing
Changes in depth/rate of respirations, use of accessory muscles
Abnormal breath sounds, e.g., wheezes, rhonchi, crackles
Cough (persistent), with/without sputum production
Desired Outcomes
Maintain airway patency with breath sounds clear/clearing.
Demonstrate behaviors to improve airway clearance, e.g., cough effectively
and expectorate secretions.
Nursing Interventions Rationale
Auscultate breath sounds. Note adventitious breath
sounds (wheezes, crackles, rhonchi).
Some degree of bronchospasm is present with
obstructions in airway and may or may not be
manifested in adventitious breath sounds such as
scattered, moist crackles (bronchitis); faint sounds,
with expiratory wheezes (emphysema); or absent
breath sounds (severe asthma).

Nursing Interventions Rationale
Assess and monitor respirations and breath sounds,
noting rate and sounds (tachypnea, stridor, crackles,
wheezes). Note inspiratory and expiratory ratio.
Tachypnea is usually present to some degree and
may be pronounced on admission or during stress or
concurrent acute infectious process. Respirations may
be shallow and rapid, with prolonged expiration in
comparison to inspiration.
Note presence and degree of dyspnea as for reports
of “air hunger,” restlessness, anxiety, respiratory
distress, use of accessory muscles. Use 0–10 scale or
American Thoracic Society’s “Grade of
Breathlessness Scale” to rate breathing difficulty.
Ascertain precipitating factors when possible.
Differentiate acute episode from exacerbation of
chronic dyspnea.
Respiratory dysfunction is variable depending on the
underlying process such as infection, allergic reaction,
and the stage of chronicity in a patient with
established COPD. Note: Using a 0–10 scale to rate
dyspnea aids in quantifying and tracking changes in
respiratory distress. Rapid onset of acute dyspnea
may reflect pulmonary embolus.
Assist patient to assume position of comfort (elevate
head of bed, have patient lean on overbed table or sit
on edge of bed).
Elevation of the head of the bed facilitates respiratory
function by use of gravity; however, patient in severe
distress will seek the position that most eases
breathing. Supporting arms and legs with table,
pillows, and so on helps reduce muscle fatigue and
can aid chest expansion.
Keep environmental pollution to a minimum such
as dust, smoke, and feather pillows, according to
individual situation.
Precipitators of allergic type of respiratory reactions
that can trigger or exacerbate onset of acute episode.
Encourage abdominal or pursed-lip breathing
exercises.
Provides patient with some means to cope
with or control dyspnea and reduce air-trapping.
Observe characteristics of cough (persistent, hacking,
moist). Assist with measures to improve effectiveness
of cough effort.
Cough can be persistent but ineffective, especially if
patient is elderly, acutely ill, or debilitated. Coughing is
most effective in an upright or in a head-down position
after chest percussion.

Nursing Interventions Rationale
Increase fluid intake to 3000 mL per day within cardiac
tolerance. Provide warm or tepid liquids. Recommend
intake of fluids between, instead of during, meals.
Hydration helps decrease the viscosity of secretions,
facilitating expectoration. Using warm liquids may
decrease bronchospasm. Fluids during meals can
increase gastric distension and pressure on the
diaphragm.
Monitor and graph serial ABGs, pulse oximetry, chest
x-ray.
Establishes baseline for monitoring progression or
regression of disease process an
complications. Note: Pulse oximetry readings detect
changes in saturation as they are happening, helping
to identify trends before patient is symptomatic.
However, studies have shown that the accuracy of
pulse oximetry may be questioned if patient has
severe peripheral vasoconstriction.
2. Impaired Gas Exchange
Nursing Diagnosis
Impaired Gas Exchange
May be related to
Altered oxygen supply (obstruction of airways by secretions, bronchospasm;
air-trapping)
Alveoli destruction
Alveolar-capillary membrane changes
Possibly evidenced by
Dyspnea
Abnormal breathing
Confusion, restlessness
Inability to move secretions
Abnormal ABG values (hypoxia and hypercapnia)
Changes in vital signs
Reduced tolerance for activity
Desired Outcomes

Demonstrate improved ventilation and adequate oxygenation of tissues by
ABGs within patient’s normal range and be free of symptoms of respiratory
distress.
Participate in treatment regimen within level of ability/situation.
Nursing Interventions Rationale
Assess and record respiratory rate, depth. Note use of
accessory muscles, pursed-lip breathing, inability to
speak or converse.
Useful in evaluating the degree of respiratory distress
or chronicity of the disease process.
Elevate head of bed, assist patient to assume position
to ease work of breathing. Include periods of time in
prone position as tolerated. Encourage deep-slow or
pursed-lip breathing as individually needed or
tolerated.
Oxygen delivery may be improved by upright position
and breathing exercises to decrease airway collapse,
dyspnea, and work of breathing. Note: Recent
research supports use of prone position to increase
Pao2.
Assess and routinely monitor skin and mucous
membrane color.
Cyanosis may be peripheral (noted in nailbeds) or
central (noted around lips/or earlobes). Duskiness and
central cyanosis indicate advanced hypoxemia.
Encourage expectoration of sputum; suction when
indicated.
Thick, tenacious, copious secretions are a major
source of impaired gas exchange in small airways.
Deep suctioning may be required when cough is
ineffective for expectoration of secretions.
Auscultate breath sounds, noting areas of decreased
airflow and adventitious sounds.
Breath sounds may be faint because of decreased
airflow or areas of consolidation. Presence of wheezes
may indicate bronchospasm or retained secretions.
Scattered moist crackles may indicate interstitial fluid
or cardiac decompensation.
Palpate for fremitus. Decrease of vibratory tremors suggests fluid collection
or air-trapping.
Monitor level of consciousness and mental status.
Investigate changes.
Restlessness and anxiety are common manifestations
of hypoxia. Worsening ABGs accompanied by

Nursing Interventions Rationale
confusion/ somnolence are indicative of cerebral
dysfunction due to hypoxemia.
Evaluate level of activity tolerance. Provide calm, quiet
environment. Limit patient’s activity or encourage bed
or chair rest during acute phase. Have patient resume
activity gradually and increase as individually
tolerated.
During severe, acute or refractory respiratory distress,
patient may be totally unable to perform basic self-
care activities because of hypoxemia and dyspnea.
Rest interspersed with care activities remains an
important part of treatment regimen. An exercise
program is aimed at increasing endurance and
strength without causing severe dyspnea and can
enhance sense of well-being.
Evaluate sleep patterns, note reports of difficulties and
whether patient feels well rested. Provide quiet
environment, group care or monitoring activities to
allow periods of uninterrupted sleep; limit
stimulants such as caffeine; encourage position of
comfort.
Multiple external stimuli and presence of dyspnea may
prevent relaxation and inhibit sleep.
Monitor vital signs and cardiac rhythm. Tachycardia, dysrhythmias, and changes in BP can
reflect effect of systemic hypoxemia on cardiac
function.
3. Imbalanced Nutrition
Nursing Diagnosis
Nutrition: imbalanced, less than body requirements
May be related to
Dyspnea; sputum production
Medication side effects; anorexia, nausea/vomiting
Fatigue
Possibly evidenced by
Weight loss; loss of muscle mass, poor muscle tone
Reported altered taste sensation; aversion to eating, lack of interest in food
Desired Outcomes
Display progressive weight gain toward goal as appropriate.
Demonstrate behaviors/lifestyle changes to regain and/or maintain
appropriate weight.
Nursing Interventions Rationale
Ascertain understanding of individual nutritional needs To determine informational needs of client and SO.
Assess dietary habits, recent food intake. Note degree
of difficulty with eating. Evaluate weight and body size
(mass).
Patient in acute respiratory distress is often anorectic
because of dyspnea, sputum production, and
medications. In addition, many COPD patients
habitually eat poorly, even though respiratory
insufficiency creates a hypermetabolic state with
increased caloric needs. As a result, patient often is
admitted with some degree of malnutrition. People
who have emphysema are often thin with wasted
musculature.
Auscultate bowel sounds. Diminished or hypoactive bowel sounds may reflect
decreased gastric motility and constipation (common
complication) related to limited fluid intake, poor food
choices, decreased activity, and hypoxemia.
Give frequent oral care, remove expectorated
secretions promptly, provide specific container for
disposal of secretions and tissues.
Noxious tastes, smells, and sights are prime
deterrents to appetite and can produce nausea and
vomiting with increased respiratory difficulty.
Encourage a rest period of 1 hr before and after
meals. Provide frequent small feedings.
Helps reduce fatigue during mealtime, and provides
opportunity to increase total caloric intake.
Avoid gas-producing foods and carbonated
beverages.
Can produce abdominal distension, which hampers
abdominal breathing and diaphragmatic movement
and can increase dyspnea.

Nursing Interventions Rationale
Avoid very hot or very cold foods. Extremes in temperature can precipitate or aggravate
coughing spasms.
Weigh as indicated. Useful in determining caloric needs, setting weight
goal, and evaluating adequacy of nutritional
plan. Note:Weight loss may continue initially, despite
adequate intake, as edema is resolving.
Administer supplemental oxygen during meals as
indicated.
Decreases dyspnea and increases energy for eating,
enhancing intake.
4. Risk for Infection
Nursing Diagnosis
Risk for Infection
Risk factors may include
Inadequate primary defenses (decreased ciliary action, stasis of secretions)
Inadequate acquired immunity (tissue destruction, increased environmental
exposure)
Chronic disease process
Malnutrition
Desired Outcomes
Verbalize understanding of individual causative/risk factors.
Identify interventions to prevent/reduce risk of infection.
Demonstrate techniques, lifestyle changes to promote safe environment.
Nursing Interventions Rationale
Monitor temperature. Fever may be present because of infection
or dehydration.
Review importance of breathing exercises, effective
cough, frequent position changes, and adequate fluid
intake.
These activities promote mobilization and
expectoration of secretions to reduce risk of
developing pulmonary infection.

Nursing Interventions Rationale
Observe color, character, odor of sputum. Odorous, yellow, or greenish secretions suggest the
presence of pulmonary infection.
Demonstrate and assist patient in disposal of tissues
and sputum. Stress proper handwashing (nurse and
patient), and use gloves when handling or disposing of
tissues, sputum containers.
Prevents spread of fluid-borne pathogens.
Monitor visitors; provide masks as indicated. Reduces potential for exposure to infectious illnesses
such as upper respiratory infection (URI).
Encourage balance between activity and rest. Reduces oxygen consumption or demand imbalance,
and improves patient’s resistance to infection,
promoting healing.
Discuss need for adequate nutritional intake. Malnutrition can affect general well-being and lower
resistance to infection.
Recommend rinsing mouth with water and spitting, not
swallowing, or use of spacer on mouthpiece of inhaled
corticosteroids.
Reduces localized immunosuppressive effect of drug
and risk of oral candidiasis.
Obtain sputum specimen by deep coughing or
suctioning for Gram’s stain, culture and sensitivity.
Done to identify causative organism and susceptibility
to various antimicrobials.
Administer antimicrobials as indicated. May be given for specific organisms identified by
culture and sensitivity, or be given prophylactically
because of high risk.
5. Knowledge Deficit
Nursing Diagnosis
Knowledge Deficit
May be related to
Lack of information/unfamiliarity with information resources

Information misinterpretation
Lack of recall/cognitive limitation
Possibly evidenced by
Request for information
Statement of concerns/misconception
Inaccurate follow-through of instructions
Development of preventable complications
Desired Outcomes
Verbalize understanding of condition/disease process and treatment.
Identify relationship of current signs/symptoms to the disease process and
correlate these with causative factors.
Initiate necessary lifestyle changes and participate in treatment regimen.
Nursing Interventions Rationale
Explain and reinforce explanations of individual disease
process. Encourage patient and SO to ask questions.
Decreases anxiety and can lead to improved
participation in treatment plan.
Instruct and reinforce rationale for breathing exercises,
coughing effectively, and general conditioning
exercises.
Pursed-lip and abdominal or diaphragmatic breathing
exercises strengthen muscles of respiration, help
minimize collapse of small airways, and provide the
individual with means to control dyspnea. General
conditioning exercises increase activity tolerance,
muscle strength, and sense of well-being.
Stress importance of oral care and dental hygiene. Decreases bacterial growth in the mouth, which can
lead to pulmonary infections.
Discuss importance of avoiding people with active
respiratory infections. Stress need for routine influenza
and pneumococcal vaccinations.
Decreases exposure to and incidence of acquired acute
URIs.
Discuss individual factors that may trigger or aggravate
condition (excessively dry air, wind, environmental
temperature extremes, pollen, tobacco smoke, aerosol
These environmental factors can induce or aggravate
bronchial irritation, leading to increased secretion
production and airway blockage.

Nursing Interventions Rationale
sprays, air pollution). Encourage patient and SO to
explore ways to control these factors in and around the
home and work setting.
Review the harmful effects of smoking, and advise
cessation of smoking by patient and SO.
Cessation of smoking may slow or halt progression of
COPD. Even when patient wants to stop smoking,
support groups and medical monitoring may be
needed. Note: Research studies suggest that “side-
stream” or “second-hand” smoke can be as detrimental
as actually smoking.
Provide information about activity limitations and
alternating activities with rest periods to prevent fatigue;
ways to conserve energy during activities (pulling
instead of pushing, sitting instead of standing while
performing tasks); use of pursed-lip breathing, side-
lying position, and possible need for supplemental
oxygen during sexual activity.
Having this knowledge can enable patient to make
informed choices or decisions to reduce dyspnea,
maximize activity level, perform most desired activities,
and prevent complications.
Discuss importance of medical follow-up care, periodic
chest x-rays, sputum cultures.
Monitoring disease process allows for alterations in
therapeutic regimen to meet changing needs and may
help prevent complications.
Review oxygen requirements and dosage for patient
who is discharged on supplemental oxygen. Discuss
safe use of oxygen and refer to supplier as indicated.
Reduces risk of misuse (too little or too much) and
resultant complications. Promotes environmental and
physical safety.
Instruct patient and SO in use of NIPPV as appropriate.
Problem-solve possible side effects and identify
adverse signs and symptoms (increased dyspnea,
fatigue, daytime drowsiness, or headaches on
awakening).
NIPPV may be used at night or periodically during day
to decrease CO2 level, improve quality of sleep, and
enhance functional level during the day. Signs of
increasing CO2 level indicate need for more aggressive
therapy.
Instruct asthmatic patient in use of peak flow meter, as Peak flow level can drop before patient exhibits any

Nursing Interventions Rationale
appropriate. signs and symptoms of asthma during the “first time”
after exposure to a trigger. Regular use of the peak flow
meter may reduce the severity of the attack because of
earlier intervention.
Provide information and encourage participation in
support groups (American Lung Association, public
health department).
These patients and their SOs may experience anxiety,
depression, and other reactions as they deal with a
chronic disease that has an impact on their desired
lifestyle. Support groups or home visits may be desired
or needed to provide assistance, emotional support,
and respite care.
Refer for evaluation of home care if indicated. Provide
a detailed plan of care and baseline physical
assessment to home care nurse as needed on
discharge from acute care.
Provides for continuity of care. May help reduce
frequency of rehospitalization.
Discuss respiratory medications, side effects, adverse
reactions.
Frequently these patients are simultaneously on several
respiratory drugs that have similar side effects and
potential drug interactions. It is important that patient
understand the difference between nuisance side
effects (medication continued) and untoward or adverse
side effects (medication possibly discontinued or
dosage changed).
Demonstrate technique for using a metered-dose
inhaler (MDI), such as how to hold it, taking 2–5 min
between puffs, cleaning the inhaler.
Proper administration of drug enhances delivery and
effectiveness.
Devise system for recording prescribed intermittent
drug and inhaler usage.
Reduces risk of improper use and overdosage of prn
medications, especially during acute exacerbations,
when cognition may be impaired.
Recommend avoidance of sedative antianxiety agents Although patient may be nervous and feel the need

Nursing Interventions Rationale
unless specifically prescribed or approved by physician
treating respiratory condition.
for sedatives, these can depress respiratory drive
and protective cough mechanisms. Note: These
drugs may be used prophylactically when patient is
unable to avoid situations known to increase stress
or trigger respiratory response.
Other Possible Nursing Diagnoses
1. Self-Care deficit, specify—intolerance to activity, decreased
strength/endurance, depression, severe anxiety.
2. Home Maintenance, ineffective—intolerance to activity, inadequate support
system, insufficient finances, unfamiliarity with neighborhood resources.
3. Infection, risk for—decreased ciliary action, stasis of secretions, tissue
destruction, increased environmental exposure,chronic disease process,
malnutrition.