copd guidelines update: opportunities for growth and
TRANSCRIPT

10/22/2019
1
COPD Guidelines Update:Opportunities for Growth and
Transitions of CareRobert J. Kuhn, PharmD - UK
Lauren Kormelink, PharmD - UK
Rachael Hiday, PharmD - IU Health
Sarah Vickery, PharmD - Ephraim McDowell Danville
Agenda
• Introduction and Development Plan - BK
• New COPD Guidelines - Dr. Lauren Kormelink
• Transitions in Care- Selection of Programs
• Ambulatory Care COPD Clinic, Indianapolis Indiana Dr. Rachael Hiday
• EMMC- Transition clinic and follow up - Dr. Sarah Vickey
• Special Thanks to :
• Dr. Emily Henderson, PharmD
• KSHP

10/22/2019
2
2019 Guideline Update: Chronic Obstructive Pulmonary Disease (COPD)Lauren Kormelink, PharmD, BCACP
Clinical Pharmacy Specialist – Adult Pulmonology
UK HealthCare
Faculty Disclosure
I have no conflicts of interest to disclose regarding this presentation.

10/22/2019
3
Educational Need/Practice Gap
COPD is very prevalent in the state of Kentucky.
The GOLD workgroup released updated treatment guidelines for COPD in the spring of 2019.
In order to provide Kentuckians with optimal COPD treatment outcomes, practitioners across the state should be able to implement the most updated evidence based treatment approaches.
Objectives
Upon completion of this educational activity, you will be able to: Review risk factors and pathophysiology of COPD
Recommend initial pharmacologic and non-pharmacologic interventions for a patient with newly diagnosed COPD
Assess appropriateness of a patient’s current COPD treatment and determine when changes are warranted
Evaluate need for COPD exacerbation treatment
10/22/2019
4
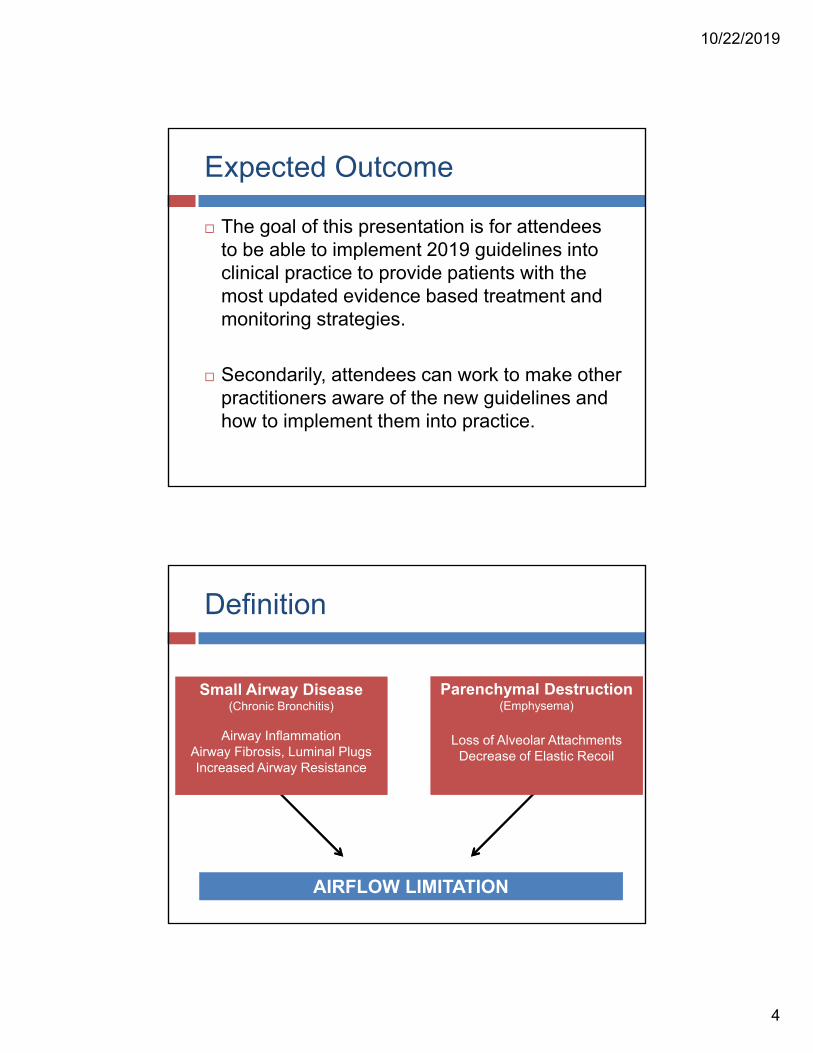
Expected Outcome
The goal of this presentation is for attendees to be able to implement 2019 guidelines into clinical practice to provide patients with the most updated evidence based treatment and monitoring strategies.
Secondarily, attendees can work to make other practitioners aware of the new guidelines and how to implement them into practice.
Definition
Small Airway Disease(Chronic Bronchitis)
Airway InflammationAirway Fibrosis, Luminal PlugsIncreased Airway Resistance
Parenchymal Destruction(Emphysema)
Loss of Alveolar AttachmentsDecrease of Elastic Recoil
AIRFLOW LIMITATION
10/22/2019
5
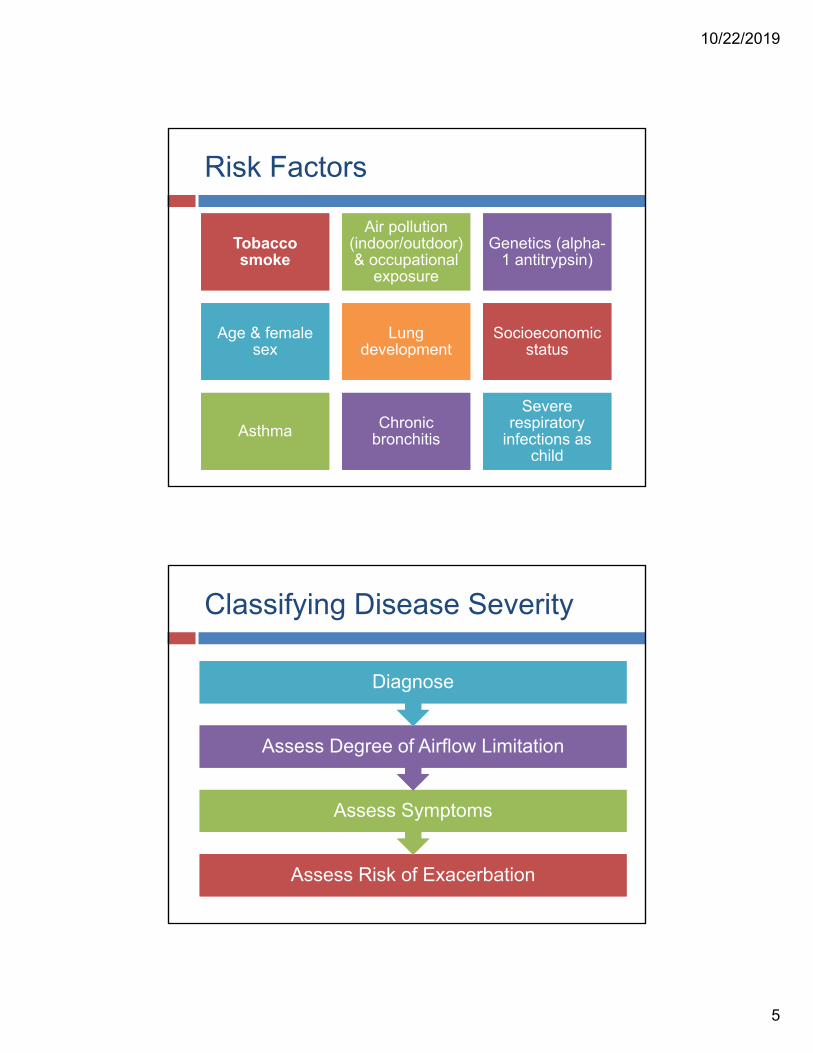
Risk Factors
Tobacco smoke
Tobacco smoke
Air pollution (indoor/outdoor) & occupational
exposure
Air pollution (indoor/outdoor) & occupational
exposure
Genetics (alpha-1 antitrypsin)
Genetics (alpha-1 antitrypsin)
Age & female sex
Age & female sex
Lung development
Lung development
Socioeconomic status
Socioeconomic status
AsthmaAsthma Chronic bronchitisChronic
bronchitis
Severe respiratory
infections as child
Severe respiratory
infections as child
Classifying Disease Severity
Assess Risk of ExacerbationAssess Risk of Exacerbation
Assess SymptomsAssess Symptoms
Assess Degree of Airflow LimitationAssess Degree of Airflow Limitation
DiagnoseDiagnose

10/22/2019
6
COPD Diagnosis
COPD Diagnosis
Symptoms
Risk Factors
and Personal History
SpirometricTesting
Dyspnea: Progressive over timeWorsens with exercise
Persistent
Chronic CoughMay be intermittent
May be productive or non-productive
Presence of wheeze
Sputum ProductionChronic or intermittent but
recurrent
Risk Factors (current or past)-especially tobacco smoke or environmental/occupational
exposures
Family History of COPD
Recurrent Lower Respiratory Tract Infections
Grading Airflow Limitation
Grading Airflow Limitation
Grade Severity FEV1 Percent Predicted
GOLD 1 Mild ≥ 80
GOLD 2 Moderate 50-79
GOLD 3 Severe 30 to 49
GOLD 4 Very Severe < 30
Determined by spirometry (FEV1/FVC <0.7)
Must be post-bronchodilator FEV1
Predicted FEV1 is calculated based on population norms accounting for body habitus, age, gender, etc.
10/22/2019
7
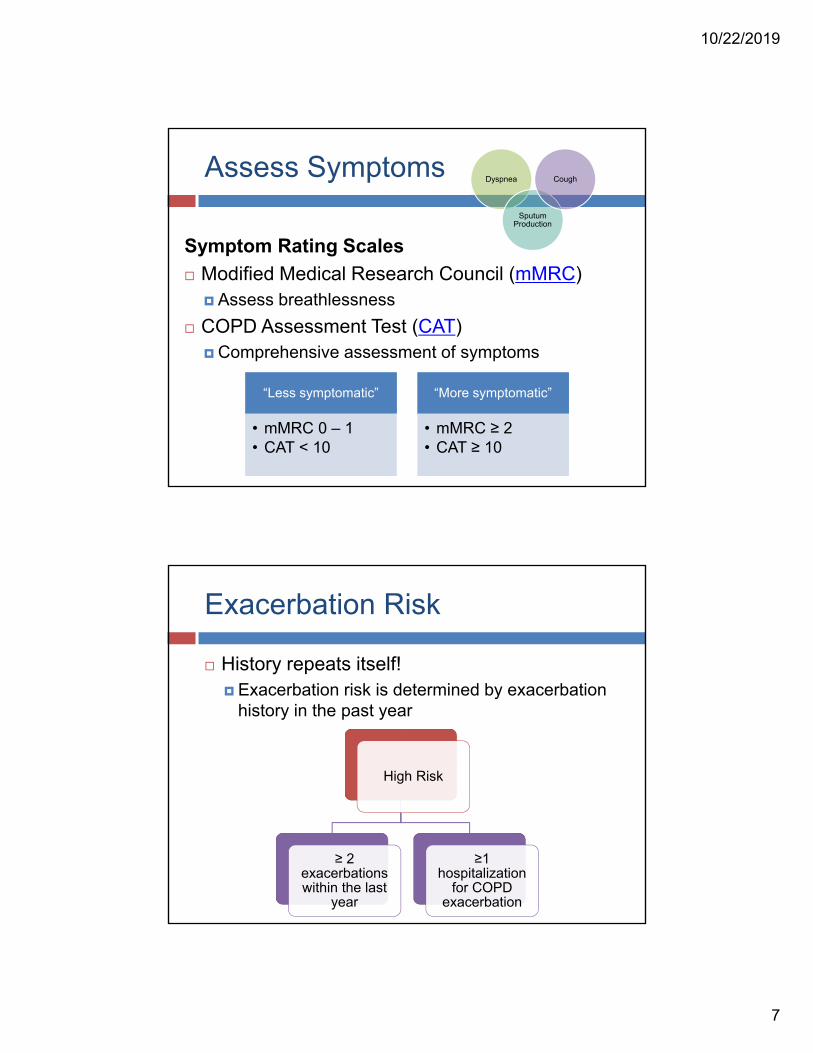
Assess Symptoms
Symptom Rating Scales
Modified Medical Research Council (mMRC) Assess breathlessness
COPD Assessment Test (CAT) Comprehensive assessment of symptoms
Dyspnea
Sputum Production
Cough
“Less symptomatic”
• mMRC 0 – 1• CAT < 10
“More symptomatic”
• mMRC ≥ 2• CAT ≥ 10
Exacerbation Risk
High Risk
≥ 2 exacerbations within the last
year
≥1 hospitalization
for COPD exacerbation
History repeats itself! Exacerbation risk is determined by exacerbation
history in the past year

10/22/2019
8
ABCD Assessment Tool
Exacerbation History
2 or moreOR
1 or more requiring
hospitalization
0 or 1 not requiring
hospitalization
mMRC 0-1CAT <10
mMRC ≥ 2CAT ≥ 10
Symptoms
GOLD GROUP
Group C
In Summary:
Spirometry:
Confirmation of diagnosis
Grading: Assessment of airflow limitation
Grouping:
Assessment of symptoms/risk of exacerbation
Post-bronchodilator
FEV1/FVC < 0.7
GRADE FEV1
GOLD 1 ≥ 80%GOLD 2 50-79%GOLD 3 30-49%GOLD 4 < 30%
GROUP
C D
A B
Ex: JZ is a 48 yo male with GOLD Grade 3 Group D COPD
10/22/2019
9
The Case of MK
MK is a 68 yo female with no significant PMH and newly diagnosed COPD presenting to the pharmacist led COPD management clinic
2 year history of chronic, dry cough and dyspnea on exertion with 1 self limiting lower respiratory infection in the past year Retired, operated her own hair salon x 30 years
Lives at home with husband
Smokes ½ PPD (recent decrease from 1-1.5)
FEV/FVC= 0.67, ppFEV1=55%, MMRC=2
MK continued…
How would you classify MK’s COPD?
A. GOLD Grade 1 Group A
B. GOLD Grade 2 Group A
C. GOLD Grade 1 Group B
D. GOLD Grade 2 Group B
E. MK does not meet diagnostic criteria for COPD

10/22/2019
10
MK continued…
Which of the following are risk factors for MK’s COPD?
A. Occupational exposure
B. Tobacco smoke exposure
C. Gender
D. A and B
E. A, B, and C
COPD Management
10/22/2019
11
Treatment Goals
Reduce Symptoms
Relieve Symptoms
Improve Exercise Tolerance
Improve Health Status
Reduce Risk
Prevent Disease
Progression
Prevent and Treat
Exacerbations
Reduce Mortality
Non-Pharmacologic Treatment
Risk factor reduction Smoking cessation!!!!
Assess at every visit
Vaccinations Influenza, pneumonia per CDC recommendations
Pulmonary rehabilitation Group B, C, and D
Supplemental oxygen To help maintain O2 saturations >88-90%

10/22/2019
12
Maintenance Therapies
Maintenance Pharmacologic Therapy
Bronchodilator
Beta-2 Agonists
SABA/LABA
Muscarinic Antagonists
SAMA/LAMA
Methylxanthine
Anti-inflammatory
ICS (LOW DOSE ONLY)
PDE-4 Inhibitor
Oral Corticosteroids
Macrolide Antibiotics
Other
SABA: Short acting beta agonistLAMA: Long acting beta agonistSAMA: Short acting muscarinic antagonistLAMA: Long acting muscarinic antagonistICS: Inhaled corticosteroidPDE-4: Phosphodiesterase type 4
10/22/2019
13
Types of Inhaled Medications
Metered Dose Inhaler (MDI) i.e. “HFA®,” “Aerosphere®”
Soft Mist Inhaler (SMI) Type of MDI
i.e. “Respimat®”
Dry Powder Inhaler (DPI) i.e. “Ellipta®,” “RespiClick®,” “Diskus®,”
“Neohaler®,” “Redihaler®,” “Flexhaler®,” “Twisthaler®,” or “Handihaler®”
Solutions for nebulization Standard nebulizer machine vs. vibrating mesh
Agent Selection
Patient history
Insurance formulary
Drug delivery
Ease of device use for patient
Patient preference

10/22/2019
14
Inhaler Assessment and Education
Continuous counseling Importance of adherence
Appropriate inhaler technique
Controller vs. rescue inhaler
Continuous assessment Demonstration of inhaler technique
Teach back method
Check refill history when possible
Barriers to treatment
Initial Treatment

10/22/2019
15
Initial Treatment
Based on ABCD Assessment tool
** Disclaimer from the guidelines: “There is a lack of high-quality evidence supporting initial pharmacologic treatment strategies in newly diagnosed COPD patients”
Blood Eosinophils
Type of WBC often indicative of inflammatory or allergic response by the immune system
Some trials have demonstrated better performance of ICS therapy in patients with eosinophilia Mostly subgroup analyses
Some trials failed to exclude patients with asthma
New guidelines have expert opinion-based cutoffs This is likely an area of future research
Still must weigh risk/benefits of ICS
10/22/2019
16
Group A
Treat with any bronchodilator Could be short or long acting
Short acting can be PRN or scheduled
Can be beta agonist or muscarinic antagonist
Combination SABA/SAMA > monotherapy Better improvement in FEV1 and symptoms
Group B
LABA or LAMA is acceptable No evidence to support one over the other
Long-acting bronchodilators Formulated once or twice daily
Increased compliance vs QID regimens
Severe breathlessness (mMRC 4) LABA + LAMA as initial therapy

10/22/2019
17
Group C
LAMA superior to LABA in prevention of exacerbations Supported by two head to head trials Tiotropium vs. Salmeterol
Vogelmeier C, et al. N Engl J Med 2011; 364 (12): 1093-1103.
Tiotropium vs. Indacaterol Decramer ML, et al. Lancet Respir Med 2013; 1(7):524-
533.
Group D
Individual patient
LAMA•Most patients
LABA/LAMA• CAT≥20
• Exercise limitation• Dyspnea
ICS/LABA• Eosinophils ≥300 cells/μL
• H/O asthma

10/22/2019
18
MK continued…
Which non-pharmacologic treatments are appropriate for MK?
A. Tobacco cessation/assessment of readiness to quit
B. PPSV 23 and Influenza Vaccine today
C. PCV 13 and Influenza Vaccine today
D. A and B
E. A and C
MK continued…
In addition to PRN albuterol, which option would be appropriate initial treatment for MK’s group B COPD?
A. Salmeterol 50 mcg – 1 puff PO BID
B. Tiotropium 2.5 mcg – 2 puffs PO daily
C. Fluticasone/Salmeterol 100/50 mcg – 1 puff PO BID
D. A or B
E. A, B, or C
10/22/2019
19
Therapy adjustment after initial treatment
Follow up Pharmacologic Treatment
Management Cycle
Well-managed disease Every 3-6 months
After therapy change with no exacerbation 6-12 weeks
After acute exacerbation Within 4 weeks
10/22/2019
20
Monitoring Tests
Spirometry At least annually
ABCD Grouping At every visit to assess disease progression/severity
Imaging In some cases
Eosinophils counts Initial visit or if you are considering starting ICS therapy
Targeted Adjustments

10/22/2019
21
Dyspnea:
LAMA or LABA monotherapy Try LAMA/LABA
LABA/ICS Try LAMA/LABA
Try LABA/LAMA/ICS
If at any point, ICS is ineffective or causes ADRs, take it off
Patient reports persistent breathlessness or exercise limitations
Exacerbations:
If on monotherapy: try LAMA+LABA
ICS/LABA (if appropriate)
If on LAMA/LABA: try LAMA/LABA/ICS
Azithromycin
Roflumilast
If on LABA/ICS: try LAMA/LAMA
LAMA/LABA/ICS
Patient presents with persistent exacerbations +/- dyspnea

10/22/2019
22
Roflumilast
Phosphodiesterase-4 inhibitor
Reduce inflammation by decreasing the breakdown of cAMP
DOES NOT REDUCE SYMPTOMS
FDA Approved to reduce moderate to severe exacerbations in patients with
Chronic bronchitis
Severe or very severe COPD Grade 3-4
i.e. FEV1<50%
History of exacerbations requiring hospitalization or steroid/antibiotic courses
Roflumilast
Precautions and Side Effects: Neuropsychiatric effects Increased anxiety, depression, sleep disturbances
Avoid in depression with suicidality
Weight Loss 20% of patients lost 5-10% of body weight
7% of patients lost >10% of body weight
Avoid in underweight, frail population
Diarrhea 9.5%
Severe weight
loss 7.5%
Nausea 4.7%
Headache 4.4%
Back pain 3.2%
Insomnia 2.4%

10/22/2019
23
Macrolide Antibiotics
Chronic use = anti-inflammatory effect NOT antimicrobial
May reduce rate of exacerbations, NOT symptoms
Little to no benefit in current smokers
Dosing Azithromycin 250 mg/day or 500 mg MWF
Erythromycin 500 mg BID
Studies lack data for use > 1 year
Concern for antimicrobial resistance, QTcprolongation, and impaired hearing test with chronic use
Other Treatments
Studied, but no/little evidence in support Mucolytics N-acetylcysteine
Carbosysteine
Leukotriene modifiers
Simvastatin
Vitamin D supplementation
Chronic Systemic Steroids Risk>Benefit in most cases
Methylxanthines Risk>Benefit in most cases
10/22/2019
24
MK continued…
MK returns to clinic 6 mo later She quit smoking using NRT (3 mo tobacco free)
Reports continued dyspnea, even at rest
mMRC = 3, no exacerbation in past 6 mo
Current medications: Albuterol HFA 1-2 puffs PO Q4-6Hr PRN
Tiotropium 2.5 mcg – 2 puffs PO daily
Demonstrated good technique of each inhaler device and states she misses 1-2 doses per month of maintenance inhaler
MK continued…
Which of the following is the best intervention for MK?
A. Stop tiotropium, start umeclidinium/vilanterol
B. Continue tiotropium, add salmeterol
C. Continue tiotropium, add fluticasone
D. Stop tiotropium, start salmeterol
E. Stop tiotropium, start fluticasone/salmeterol

10/22/2019
25
Acute worsening of respiratory symptoms that results in the need for additional therapy Increased dyspnea, coughing, changes in
sputum amount and/or color
Often triggered by respiratory viral infections
Treating Exacerbations
Consequences of Exacerbations
Exacerbations
Negative Impact on Quality of
Life
Impact on Symptoms and Lung Function
Increased Economic
Costs
Increased Mortality
Accelerated Lung
Function Decline

10/22/2019
26
Management: Exacerbations
Oxygen Bronchodilators
Systemic Corticosteroids Antibiotics
Location of treatment
80% of exacerbations are treated in the outpatient setting

10/22/2019
27
Bronchodilators
Increase use of SABA
No difference between nebulization vs. MDI Sicker patients may do better with nebulized SABA if unable to take
deep breath without coughing
MDI: Use 1 puff PO every hour for 2-3 doses, then every 2-4 hours based on response
Educate patients about COPD action plan
Systemic Corticosteroids
Role in therapy: Shorten recovery time
Improves lung function
Reduces risk of early relapse
Reduces length of hospital stay
Prednisone 40 mg daily for 5 days Trials have shown:
5 days course is non-inferior to 14 day course
PO steroids non-inferior to IV steroids
For patients with contraindications to systemic steroids, can consider budesonide 2 mg nebulization Q6Hr for 5-7 days

10/22/2019
28
Antibiotics
Antibiotic therapy is warranted when:Patient exhibits 3 cardinal symptoms Increased dyspnea
Increased sputum volume
Increased sputum purulence
OR increased sputum purulence + Increased dyspnea or sputum volume
Patient requiring mechanical ventilation
Treatment duration: 5-7 days
Antibiotic Selection
Most common pathogens are S. pneumoniae, H. influenza, M. catarrhalis, and atypical organisms
Macrolide• Azithromycin 500mg PO on day once, then 250 mg PO daily on days 2-5
Tetracycline• Doxycycline 100mg PO BID x 5-7 days
Beta-lactams• Aminopenicillin + β-lactamase inhibitor
• Amoxicillin/clavulanic acid 875 mg PO BID x 7 days• Ampicillin/sulbactam 3G IV Q6H x 7 days
• 2nd or 3rd generation cephalosporin
Respiratory fluoroquinolone• ONLY if severe exacerbation + β-lactam allergy (or failure)

10/22/2019
29
Key points
All patients should increase SABA use Continue maintenance therapy
For moderate or severe, use glucocorticoids Prednisone 40 mg PO daily x 5 days
No additional benefit of longer duration or IV therapy
If evidence of bacterial infection Antibiotics targeting common pathogens x 5-7
days

10/22/2019
30
Post Exacerbation Transition
Education Inhaler technique, Maintenance vs. Rescue
COPD Action Plan
Medication Access Prior Authorizations, financial assistance, network
pharmacies
Appropriate Follow up With outpatient team within 4 weeks
MK continued…
MK returns to clinic 3 months after her last visit
increased dyspnea, frequent coughing, increased use of albuterol inhaler x 48 hours
O2 sat 99% on room air, no signs of acute respiratory failure
Current medications: Umeclidinium/Vilanterol
Albuterol 1-2 puffs PO Q4-6Hr PRN
Adherent to her medications, but feels like the powder inhaler is getting stuck in her throat

10/22/2019
31
MK continued…
Which of the following is appropriate treatment for MK’s current COPD exacerbation in addition to increased albuterol use?
A. Prednisone 40 mg PO daily x 5 days
B. Doxycycline 100 mg PO BID x 5 days
C. Oxygen
D. A and B
E. A, B, and C
MK continued…
Which counseling point is pertinent to ensure MK is using her dry powder inhaler correctly?
A. Always use a spacer with the DPI inhaler
B. Inhale a deep, steady breath
C. Hold inhaler upright (perpendicular to floor)
D. Clean inhaler with soap and water after each use

10/22/2019
32
Chronic Obstructive Pulmonary Disease
Based on GLOBAL STRATEGY FOR THE DIAGNOSIS, MANAGEMENT AND PREVENTION OF COPD, GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE LUNG DISEASE (GOLD) 2019. AVAILABLE FROM:
HTTP://WWW.GOLDCOPD.ORG/.
Appendix Slides

10/22/2019
33
mMRC Dyspnea Scale
CAT Assessment

10/22/2019
34
Short-Acting Beta 2-Agonists (SABA)
Medication Formulation Strength Daily Dose Max Dose/Day
Albuterol*generic only*
Nebulization solution
0.63 mg/3 mL1.25 mg/3 mL2.5 mg/3 mL
5 mg/mL
1.25-5 mg Q4-8H prn30 mg/day
Albuterol(Proventil®
HFA, ProAir® HFA,
Ventolin® HFA)
MDI
90 mcg 1-2 puff Q4-6H prn 1,080 mcg/day
Albuterol(ProAir®
RespiClick)DPI
Levalbuterol(Xopenex®)
Nebulizationsuspension
0.31 mg/3 mL0.63 mg/3 mL1.25 mg/3 mL
1.25 mg/0.5 mL
0.63-1.25 mg Q6-8H 3.75 mg/day
Levalbuterol(Xopenex®
HFA)MDI 45 mcg 1-2 puff Q4-6H prn 540 mcg/day
Short-Acting Muscarinic Antagonists (SAMA)
Medication Formulation Strength Daily Dose Max Dose/Day
Ipratropium bromide
(Atrovent® HFA)
MDI 17 mcg 2 puffs QID 204 mcg/day
Ipratropium bromide
*generic only*
Nebulization solution
500 mcg/2.5 mL
1 vial Q6-8H 2000 mcg/day

10/22/2019
35
Long-Acting Beta2-Agonists (LABA)
Medication Formulation Strength Daily Dose Max Dose/DayArformoterol(Brovana®)
Nebulization suspension
15 mcg/2mL 1 vial nebulized BID 30 mcg/day
Formoterol(Perforomist®)
Nebulization suspension
20 mcg/2mL 1 vial nebulized BID 40 mcg/day
Indacaterol(Arcapta®
Neohaler®)DPI 75 mcg 1-4 puffs QD 300 mcg/day
Olodaterol(Striverdi® Respimat®)
SMI 2.5 mcg 2 puffs QD 5 mcg/day
Salmeterol(Serevent®
Diskus)DPI 50 mcg 1 puff BID 100 mcg/day
Long-Acting Muscarinic Antagonists (LAMA)
Medication Formulation Strength Dosing Max Dose/Day
Aclidinium bromide(Tudorza® Pressair) MDI 400 mcg 1 puff BID 800 mcg/day
Glycopyrrolate bromide
(Seebri® Neohaler®)DPI 15.6 mcg 1 puff BID 31.2 mcg/day
Glycopyrrolate bromide
(Lonhala® Magnair™)Nebulization
solution25 mcg 1 vial BID 50 mcg/day
Tiotropium bromide(Spiriva® Handihaler) DPI 18 mcg 1 puff QD 18 mcg/day
Tiotropium bromide(Spiriva® Respimat®) SMI
1.25 mcg2.5 mcg
2 puffs QD 2.5 mcg/day
Umeclidinium(Incruse® Ellipta) DPI 62.5 mcg 1 puff QD 62.5 mcg/day
10/22/2019
36
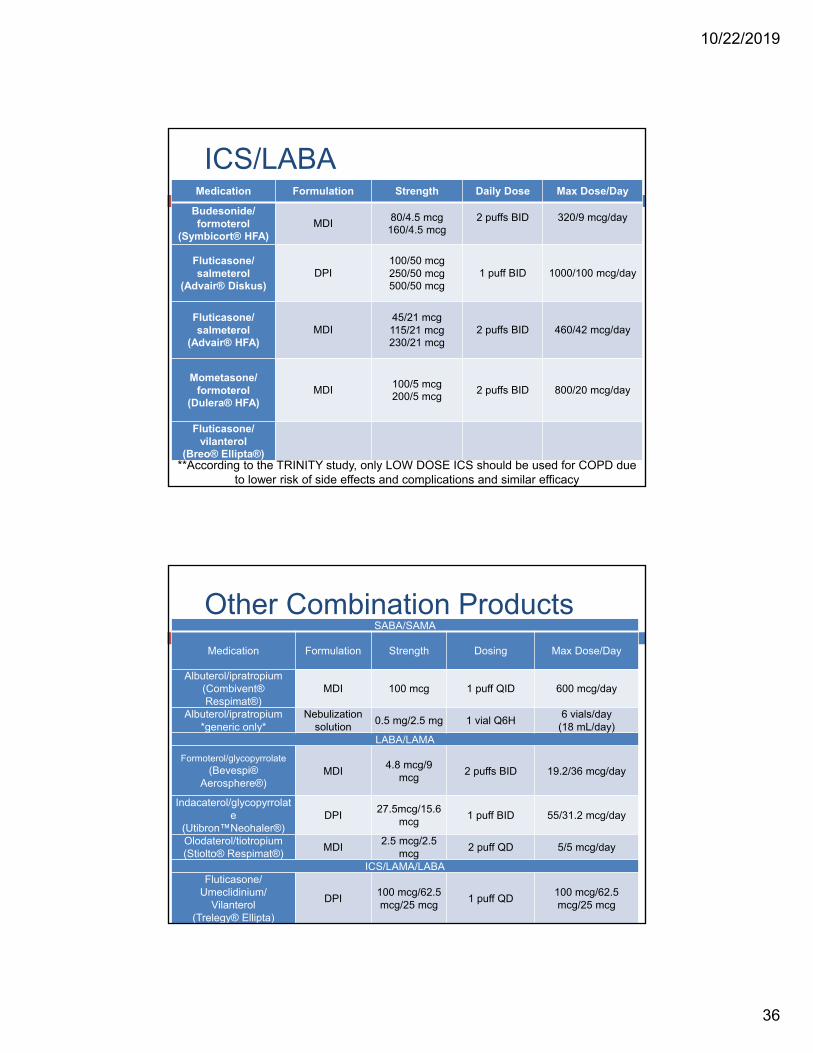
ICS/LABAMedication Formulation Strength Daily Dose Max Dose/Day
Budesonide/ formoterol
(Symbicort® HFA)MDI
80/4.5 mcg160/4.5 mcg
2 puffs BID 320/9 mcg/day
Fluticasone/ salmeterol
(Advair® Diskus)DPI
100/50 mcg250/50 mcg500/50 mcg
1 puff BID 1000/100 mcg/day
Fluticasone/ salmeterol
(Advair® HFA)MDI
45/21 mcg115/21 mcg230/21 mcg
2 puffs BID 460/42 mcg/day
Mometasone/ formoterol
(Dulera® HFA)MDI
100/5 mcg200/5 mcg
2 puffs BID 800/20 mcg/day
Fluticasone/vilanterol
(Breo® Ellipta®)**According to the TRINITY study, only LOW DOSE ICS should be used for COPD due
to lower risk of side effects and complications and similar efficacy
Other Combination ProductsSABA/SAMA
Medication Formulation Strength Dosing Max Dose/Day
Albuterol/ipratropium(Combivent®Respimat®)
MDI 100 mcg 1 puff QID 600 mcg/day
Albuterol/ipratropium *generic only*
Nebulization solution
0.5 mg/2.5 mg 1 vial Q6H6 vials/day
(18 mL/day)LABA/LAMA
Formoterol/glycopyrrolate(Bevespi®
Aerosphere®)MDI
4.8 mcg/9 mcg
2 puffs BID 19.2/36 mcg/day
Indacaterol/glycopyrrolate
(Utibron™Neohaler®)DPI
27.5mcg/15.6 mcg
1 puff BID 55/31.2 mcg/day
Olodaterol/tiotropium(Stiolto® Respimat®)
MDI2.5 mcg/2.5
mcg2 puff QD 5/5 mcg/day
ICS/LAMA/LABAFluticasone/
Umeclidinium/Vilanterol
(Trelegy® Ellipta)
DPI100 mcg/62.5 mcg/25 mcg
1 puff QD100 mcg/62.5 mcg/25 mcg

10/22/2019
37
Inhaled Corticosteroids (ICS)Medication Formulation Strength Low Daily Dose Medium Daily Dose High Daily Dose
Beclomethasonedipropionate
(QVAR® RediHaler™)MDI
40 mcg80 mcg
80-240 mcg/day 240-480 mcg/day> 480 mcg/day
Budesonide(Pulmicort® Flexhaler™)
DPI90 mcg180 mcg
180-600 mcg/day 600-1,200 mcg/day > 1,200 mcg/day
Budesonide(Pulmicort Respules®)
Nebulization suspension
0.25 mg/2 mL0.5 mg/2 mL1 mg/2 mL
0.5 mg/day 1 mg/day 2 mg/day
Ciclesonide(Alvesco®)
MDI80 mcg160 mcg
80-160 mcg/day160-320 mcg/day > 320 mcg/day
Fluticasone furoate(Arnuity® Ellipta®)
DPI100 mcg200 mcg
ICS-naïve: 100 mcg/day
prior ICS: 200 mcg/day
Fluticasone propionate(Flovent® Diskus®)
DPI50 mcg100 mcg250 mcg
100-300 mcg/day > 300-500 mcg/day> 500 mcg mcg/day
Fluticasone propionate(Flovent® HFA)
MDI44 mcg110 mcg220 mcg
88-264 mcg/day > 264-440 mcg/day >440 mcg mcg/day
Mometasone(Asmanex® Twisthaler®)
DPI110 mcg220 mcg
220 mcg/day 440 mcg/day > 440 mcg/day
**According to the TRINITY study, only LOW DOSE ICS should be used for COPD due to lower risk of side effects and complications and similar efficacy
Copay Savings Programs for commercially insured patients
Advair® HFA and Diskus ($50) – https://www.advair.com/coupon‐and‐savings.html
Alvesco ($17) – https://www.alvesco.us/HCP/Savings‐Card/
Arnuity ($10) – https://www.arnuity.com/arnuity‐savings‐and‐offers/index.html
Asmanex ($15) – https://www.activatethecard.com/7575/#
Bevespi® ($0) – https://www.bevespi.com/bevespi‐coupon.html
Combivent® ($10) – https://www.combivent.com/savings/card
Daliresp® ($25) – https://www.daliresp.com/savings‐program.html
Dulera® HFA ($15) – https://www.activatethecard.com/7575/#
Incruse® Ellipta ($10) – https://www.incruse.com/incruse‐savings‐and‐offers/index.html
Ipratroprium bromide ($4) – https://www.goodrx.com/coupon
Lonhala® Magnair® ($20) – https://www.lonhalamagnair.com/savings/sign‐up.cfm
ProAir® RespiClick ($25) – https://proair.com/respiclick/savings/
Proventil® HFA (-$15) – https://www.proventilhfa.com/pfha/index.xhtml
Pulmicort ($20) – https://www.pulmicortflexhalertouchpoints.com/savings‐card.html
QVAR Redihaler ($15) – https://www.qvar.com/redihaler/savings
Seebri Neohaler ($0) – https://www.seebri.us/savings/seebri‐savings‐card.html
Spiriva® Respimat and Handilaer ($0) – https://www.spiriva.com/copd/copay/step1
Stiolto® ($0) – https://www.stiolto.com/savings
Symbicort® HFA ($0) – https://www.mysymbicort.com/copd/symbicort‐savings‐offer/registration.html
Trelegy® ($10) – https://www.trelegy.com/savings/
Tudorza® ($25) – https://www.tudorza.com/savings‐program.html
Utibron® ($0) – https://www.utibron.com/savings/utibron‐savings‐card.html