coordination of care initiative mora area community...2019/05/23 · 5/23/2019 1 coordination of...
TRANSCRIPT

5/23/2019
1
Coordination of Care InitiativeNorth East MN Area Community
Community Meeting
May 28, 2019
2
Download meeting agenda and slide handout:
• Agenda
• Handout

5/23/2019
2
3
Welcome&
Introductions
4
Meeting Agenda and Objectives
Describe coordination of care efforts across Minnesota
and review updated North East MN
community data
Understand improvements in care transitions in
delirium prevention and management
Recognize initiative participation and celebrate
community accomplishments to improve care
transitions
5/23/2019
3
5
Coordination of Care Initiative Update
6
Coordination of Care Initiative Goals
• Improve quality of care for Medicare beneficiaries
who transition among care settings
• Reduce 30-day hospital readmission rates and
admission by 20% by 2019
• Increase the number of days at home
• Establish sustainable, transferrable transition
practices across the spectrum of care
5/23/2019
4
7
Coordination of Care Communities
8
Success Stories Webinar Series
Successful Strategies for Sustained
Community Improvement
Tuesday, January 22, 2019, 12–1:00pm – More
At Your Service: Benefits of Home
Health Agencies Working with their QIN
Tuesday, February 26, 2019, 12–1:00pm – More
Using Data to Drive Community
Quality Improvement Efforts
Tuesday, March 26, 2018, 12–1:00pm – More
Home-based Innovative Strategies
to Prevent Readmissions
Tuesday, April 23, 2019, 12–1:00pm – More
Changing the Culture: Improving
Recognition and Management of Sepsis
Thursday, May 30, 2019, 12–1:00pm – More
Achieving Community Goals by Partnering
with Aging and Disability Resource Centers
Tuesday, June 25, 2019, 12–1:00pm – Register
This six-webinar series highlights the innovative work the Lake Superior QIN COC partners have done across care settings and in the community to improve transitions of care and reduce readmissions.
Download the webinar series flier
5/23/2019
5
9
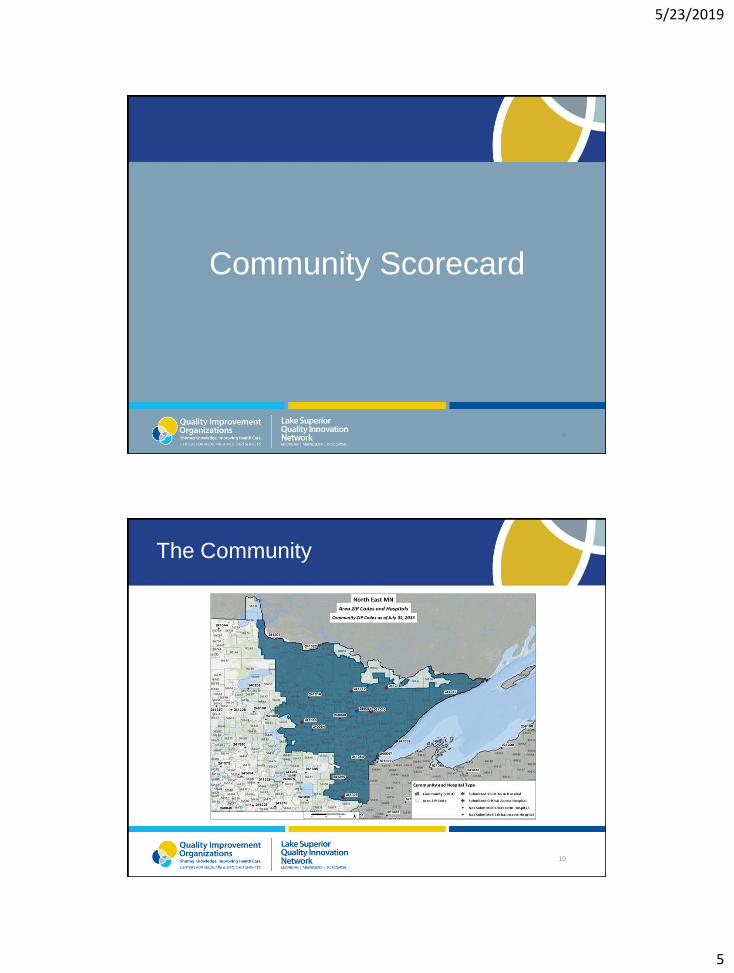
Community Scorecard
10
The Community

5/23/2019
6
11
Admissions (community)
12
Admissions (comparative)
5/23/2019
7
13
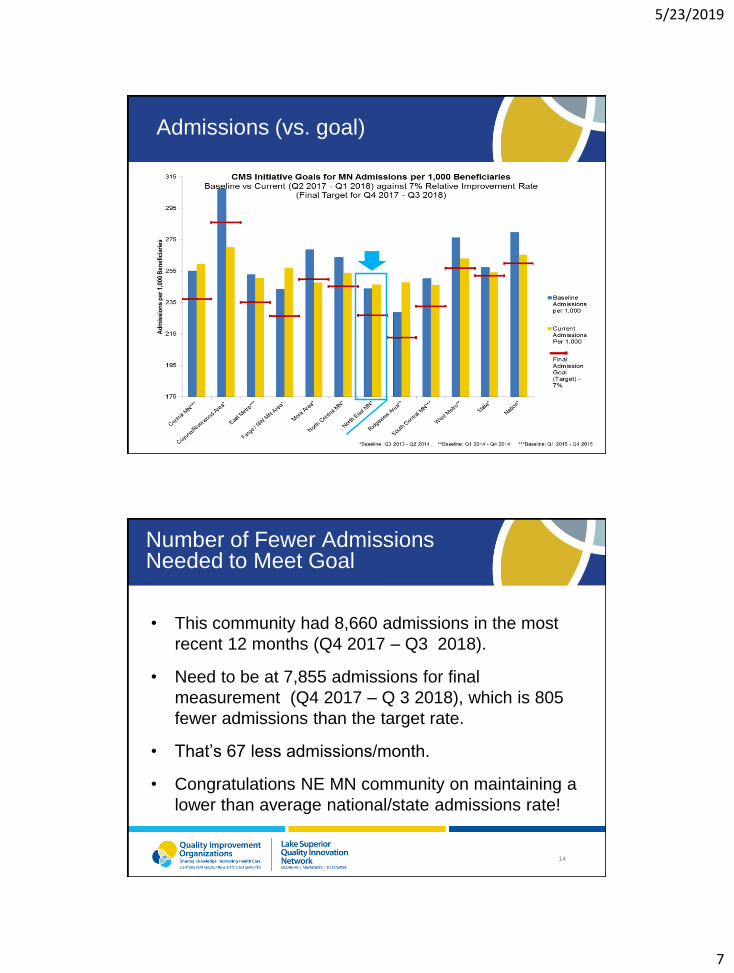
Admissions (vs. goal)
14
Number of Fewer Admissions Needed to Meet Goal
• This community had 8,660 admissions in the most
recent 12 months (Q4 2017 – Q3 2018).
• Need to be at 7,855 admissions for final
measurement (Q4 2017 – Q 3 2018), which is 805
fewer admissions than the target rate.
• That’s 67 less admissions/month.
• Congratulations NE MN community on maintaining a
lower than average national/state admissions rate!

5/23/2019
8
15
Readmissions (community)
16
Readmissions (comparative)
5/23/2019
9
17
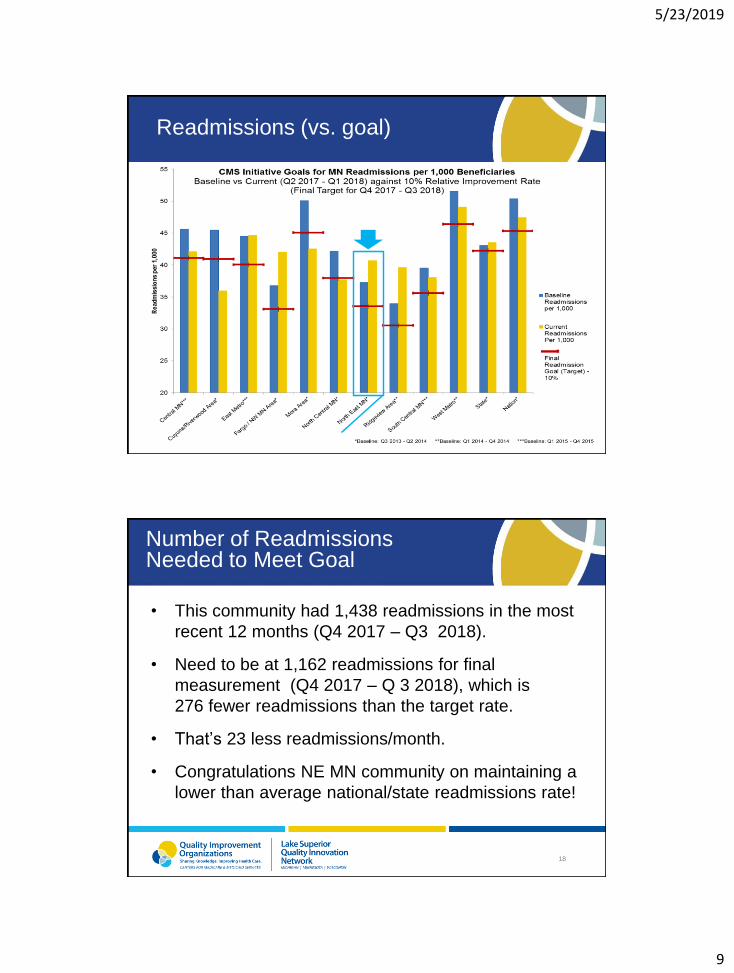
Readmissions (vs. goal)
18
Number of Readmissions Needed to Meet Goal
• This community had 1,438 readmissions in the most
recent 12 months (Q4 2017 – Q3 2018).
• Need to be at 1,162 readmissions for final
measurement (Q4 2017 – Q 3 2018), which is
276 fewer readmissions than the target rate.
• That’s 23 less readmissions/month.
• Congratulations NE MN community on maintaining a
lower than average national/state readmissions rate!

5/23/2019
10
19
ED Visits (community)
20
ED Visits (comparative)

5/23/2019
11
21
Workgroup Updates
Medication SafetyCommunication
Resources/Patient Engagement
22
Featured Presentation
—
5/23/2019
12
Place picture here
MHA Delirium Discharge Order Bundle
Charisse Coulombe, MS, MBA, CPHQ, CPPSMinnesota Hospital Association
Aminata Cham, APRN, MSN, ACNS-BCFairview/Health East Care System
May 28, 2019
Agenda/Outline
1. Introduction
2. MHA Quality and Patient Safety Committee Structure
3. Delirium Committee 2019 priorities and tools
4. Clinical review
5. Discharge Order Bundle deep dive
6. Questions
5/23/2019
13
Minnesota Hospital Association

5/23/2019
14
MHA Overview
MHA Quality & Patient Safety Division
Dedicated QPS staff for over 19 years
13 expert committees
Partnership for Patients contractor for the last 7 years
5/23/2019
15
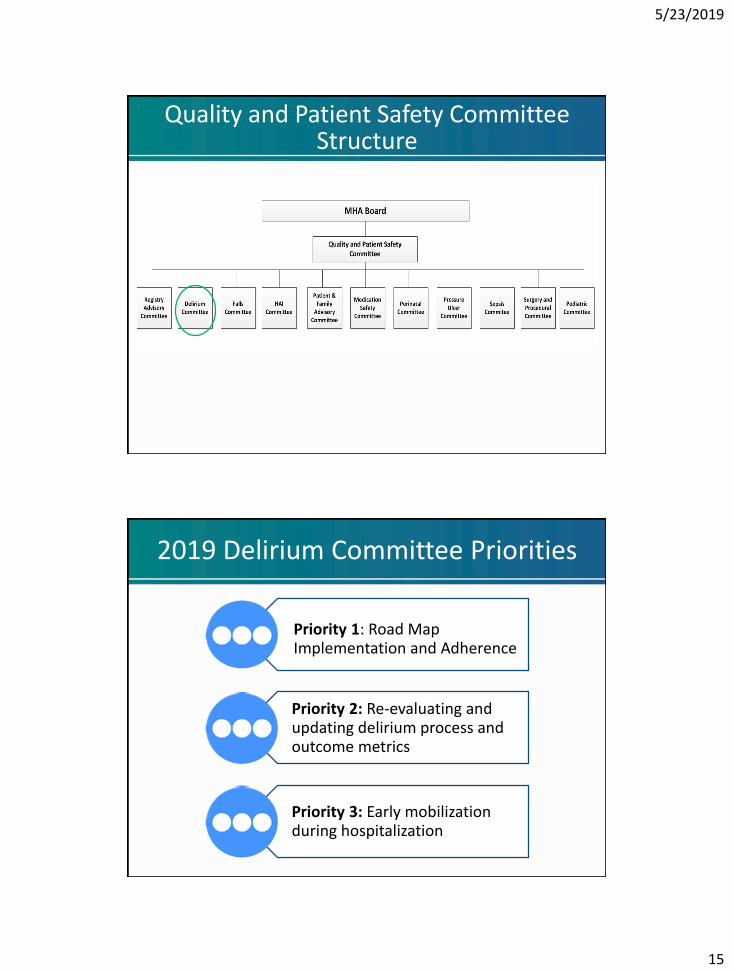
Quality and Patient Safety Committee Structure
2019 Delirium Committee Priorities
Priority 1: Road Map Implementation and Adherence
Priority 2: Re-evaluating and updating delirium process and outcome metrics
Priority 3: Early mobilization during hospitalization
5/23/2019
16
Place picture hereMHA Delirium Committee 2019WorkPlan Priority 1
Priority 1: Delirium Road Map
5/23/2019
17
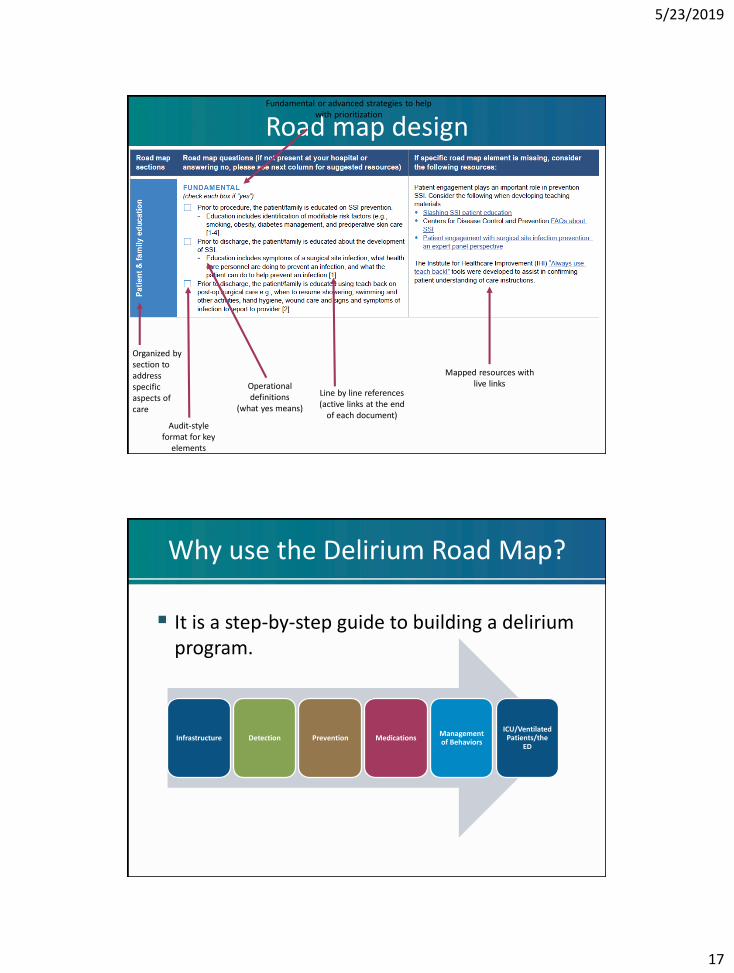
Road map design
Operational definitions
(what yes means)
Organized by section to address specific aspects of care
Audit-style format for key
elements
Line by line references (active links at the end
of each document)
Mapped resources with live links
Fundamental or advanced strategies to help with prioritization
Why use the Delirium Road Map?
It is a step-by-step guide to building a delirium program.
Infrastructure Detection Prevention MedicationsManagement of Behaviors
ICU/Ventilated Patients/the
ED
5/23/2019
18
Delirium Road Map
MHA Delirium Road Map (PDF)
https://www.mnhospitals.org/Portals/0/Documents/patientsafety/Delirium/Delirium%20Road%20Map.pdf (URL)
Now that we’ve updated our website, I would add the new look, which shows an icon of the road map directly on the webpage.
What does the road map data tell us?
2018
1. Education for nurses
2. Education for physicians/residents
3. Reaching the executive team
4. Coordination of care
5/23/2019
19
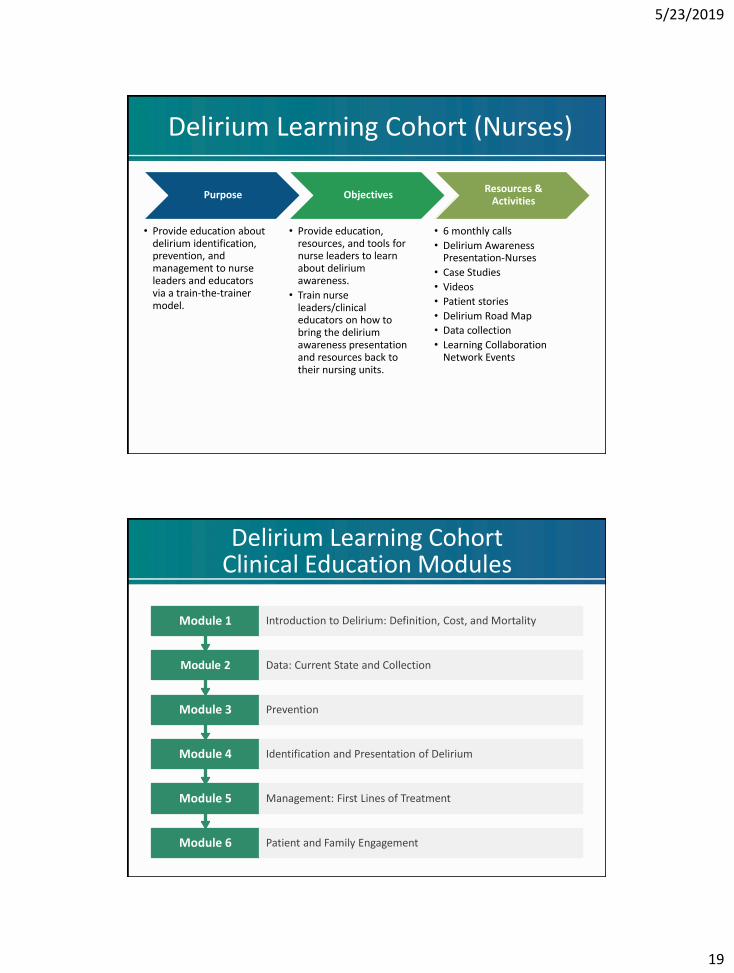
Delirium Learning Cohort (Nurses)
Purpose
• Provide education about delirium identification, prevention, and management to nurse leaders and educators via a train-the-trainer model.
Objectives
• Provide education, resources, and tools for nurse leaders to learn about delirium awareness.
• Train nurse leaders/clinical educators on how to bring the delirium awareness presentation and resources back to their nursing units.
Resources & Activities
• 6 monthly calls
• Delirium Awareness Presentation-Nurses
• Case Studies
• Videos
• Patient stories
• Delirium Road Map
• Data collection
• Learning Collaboration Network Events
Delirium Learning Cohort Clinical Education Modules
Module 6 Patient and Family Engagement
Module 5 Management: First Lines of Treatment
Module 4 Identification and Presentation of Delirium
Module 3 Prevention
Module 2 Data: Current State and Collection
Module 1 Introduction to Delirium: Definition, Cost, and Mortality
5/23/2019
20
Delirium Learning Cohort Example Toolkit
Delirium Fact Sheet (Physicians and Residents)

5/23/2019
21
SBAR(Executives and Leadership)
Place picture here
Delirium Discharge Order Bundle
Aminata Cham, APRN, MSN, ACNS-BCFairview/Health East Care System
5/23/2019
22
Delirium Discharge Order Bundle
Goal: Coordinate with post-acute organizations to identify and address areas of opportunity in delirium prevention and management to prevent delirium related readmissions
Delirium
An acute disorder of attention and cognition.
Common, serious, costly, under recognized and often
fatal.
Current approach to diagnosis and treatment of delirium
remains a clinical diagnosis.
5/23/2019
23
Diagnosis
Underrecognized and easily overlooked.
Only 12 to 35% of delirium cases are recognized.
Current reference standard diagnostic criteria are:• DSM-5
• ICD-10
Over 24 delirium instruments have been used in published studies.
CAM-most widely used instrument.
Currently, there are at least 11 diagnostic codes for delirium in ICD-9 and 23 codes in ICD-10.
Only 3% of delirium cases are coded in medical records.
DSM V
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
Disturbance in attention (i.e., reduced ability to direct, focus, sustain, and shift attention) and awareness.
Change in cognition (e.g., memory deficit, disorientation, language disturbance, perceptual disturbance) that is not better accounted for by a preexisting, established, or evolving dementia.
The disturbance develops over a short period (usually hours to days) and tends to fluctuate during the course of the day.
There is evidence from the history, physical examination, or laboratory findings that the disturbance is caused by a direct physiologic consequence of a general medical condition, an intoxicating substance, medication use, or more than one cause.
5/23/2019
24
Significance
In the united states, >2.6million adults 65years and older each year develop delirium
Total cost range from $16,303 to $64,421 per patient
Accounts for >$164 billion in annual healthcare expenditure
Included on the pt. safety agenda
Targeted as an indicator of healthcare quality for seniors
Hold significant societal implications
Key Clinical Predisposing Factors
Advanced Age- 65 and
older
Cognitive impairment,
such as dementia
Multiple co-morbidities
History of delirium 5
5/23/2019
25
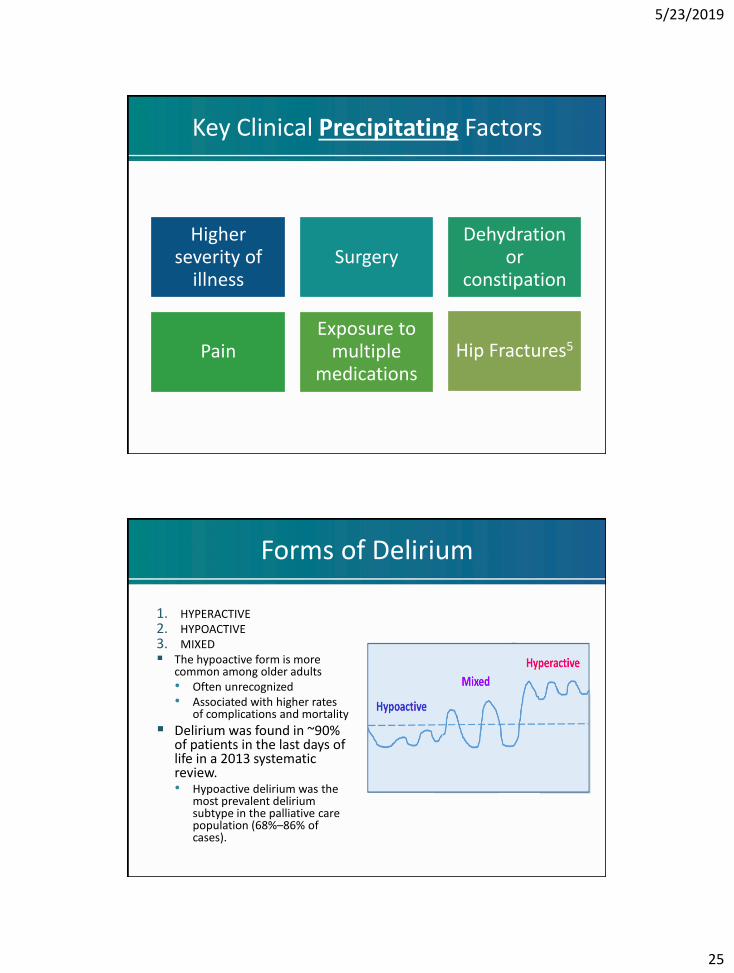
Key Clinical Precipitating Factors
Higher severity of
illnessSurgery
Dehydration or
constipation
PainExposure to
multiple medications
Hip Fractures5
Forms of Delirium
1. HYPERACTIVE2. HYPOACTIVE3. MIXED The hypoactive form is more
common among older adults• Often unrecognized• Associated with higher rates
of complications and mortality
Delirium was found in ~90% of patients in the last days of life in a 2013 systematic review.• Hypoactive delirium was the
most prevalent delirium subtype in the palliative care population (68%–86% of cases).
5/23/2019
26
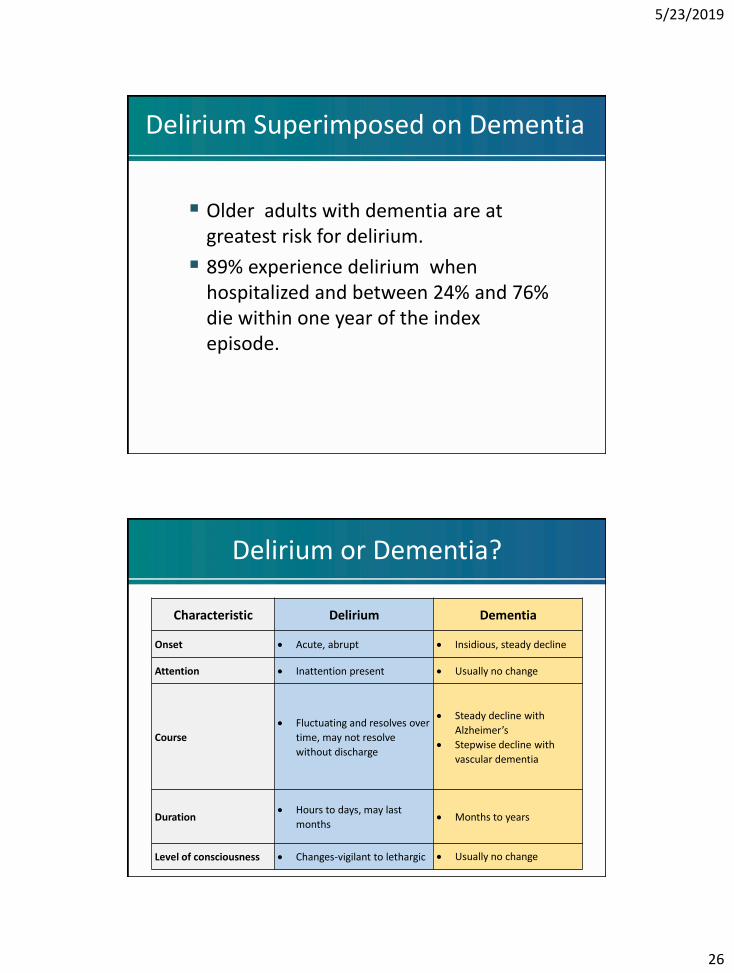
Delirium Superimposed on Dementia
Older adults with dementia are at greatest risk for delirium.
89% experience delirium when hospitalized and between 24% and 76% die within one year of the index episode.
Delirium or Dementia?
Characteristic Delirium Dementia
Onset Acute, abrupt Insidious, steady decline
Attention Inattention present Usually no change
Course
Fluctuating and resolves over
time, may not resolve
without discharge
Steady decline with
Alzheimer’s
Stepwise decline with
vascular dementia
Duration Hours to days, may last
months Months to years
Level of consciousness Changes-vigilant to lethargic Usually no change
5/23/2019
27
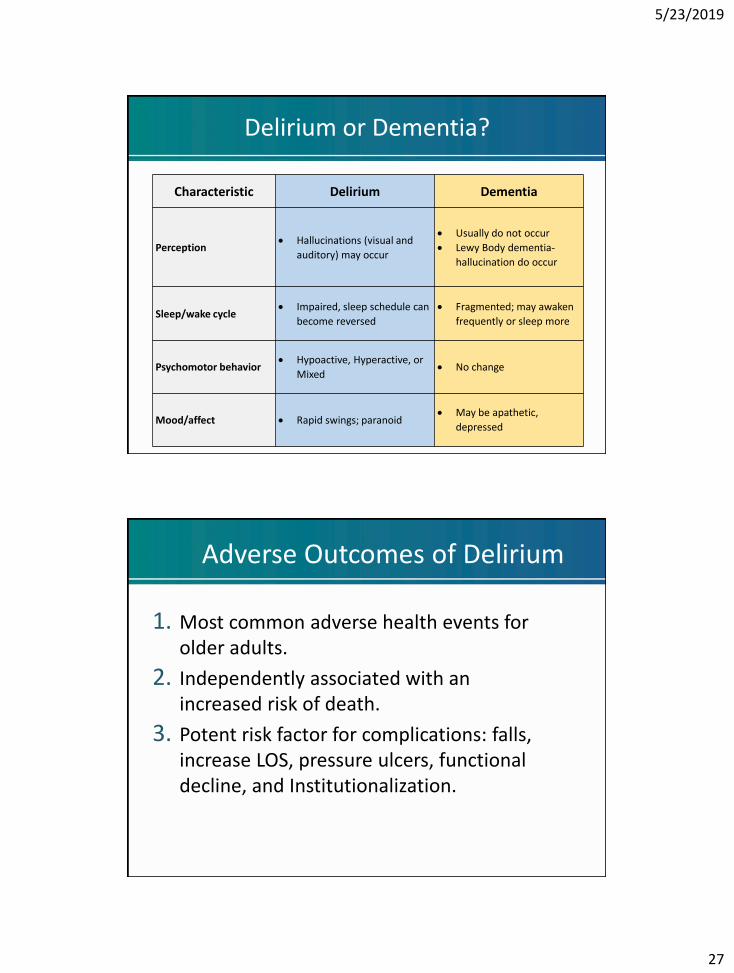
Delirium or Dementia?
Characteristic Delirium Dementia
Perception Hallucinations (visual and
auditory) may occur
Usually do not occur
Lewy Body dementia-
hallucination do occur
Sleep/wake cycle Impaired, sleep schedule can
become reversed
Fragmented; may awaken
frequently or sleep more
Psychomotor behavior Hypoactive, Hyperactive, or
Mixed No change
Mood/affect Rapid swings; paranoid May be apathetic,
depressed
Adverse Outcomes of Delirium
1. Most common adverse health events for older adults.
2. Independently associated with an increased risk of death.
3. Potent risk factor for complications: falls, increase LOS, pressure ulcers, functional decline, and Institutionalization.
5/23/2019
28
5/23/2019
29
MHA Delirium Discharge Order Bundle
Clinician Section
Clinician Section
Continue to assess for signs of delirium, such as: disturbance in attention and awareness; change in cognition that is not accounted for by dementia, develops over a short period, and fluctuates throughout the day.
Minimize high-risk medications and other medications with high anti-cholinergic effects:
• Opioids (e.g., Meperidine, Morphine, Fentanyl, Hydromorphone)
• Benzodiazepines (e.g., Diazepam, Lorazepam, Alprazolam)
• First Generation Antihistamines (e.g., Diphenhydramine, Hydroxyzine, Meclizine)
• Muscle Relaxants (e.g. Cyclobenaprine, Chlorzoxazone, Metaxalone)
• Hypnotics (e.g., Zolpidem, Eszopiclone, Zopiclone)
5/23/2019
30
Ensure Patients Have Sensory Aids
Address sensory impairment by: • Determining which, if any, sensory
aids are used by the patient • Ensuring sensory aids are
available and in reach of patient • Resolving reversible cause of the
impairment, such as impacted ear wax
Sensory aids include: • Hearing aids • Eyeglasses• Amplifiers• Dentures
Assess and Manage Pain
How
Assess for pain regularly using objective scale 6
Look for nonverbal signs of pains, especially for patients with
communication difficulties or ventilated patients 6
Why
Pain is a risk factor for delirium 26
When pain is not properly assessed and treated, patient
may receive sedatives and narcotics that place them at risk
for delirium 26
5/23/2019
31
Encourage Mobility
Patients with early mobility protocol are:
• Out of bed earlier
• Out of the ICU and hospital earlier
• Less likely to be readmitted to the hospital in 12 months following discharge
• Less likely to die in 12 months following discharge
Sleep Promotion and Environment
Sleep promotion
• Low-level lighting at night 9
• Avoid nursing or medical procedures during sleeping hours 6
• Schedule medication rounds to avoid disturbing sleep 6
• Reduce noise during sleeping hours 6
Environment
• Clock or calendar in view of patient 6
• Normal day/night variation in illumination 6
• Limit room and staff changes 9
5/23/2019
32
Hydration and Nutrition
Encourage patient to drink adequate fluids
Screen for comorbidities that would affect fluid balance (congestive heart failure, chronic kidney disease)
Promote Cognitive Stimulation
Encourage hobbies
Puzzles
Reading
5/23/2019
33
Questions
Contact Information
Charisse Coulombe
5/23/2019
34
References
1. Adamis, D. et. al., Delirium scales: A review of current evidence. Journal of Aging and Mental Health, 2010. 14(5): p.543- 555.
2. Angle, C. (2016). Standardizing management of adults with delirium hospitalized on medical-surgical units. The Permanente Journal. doi:10.7812/tpp/16-002
3. Brummel, N. E., & Girard, T. D. (2013). Preventing delirium in the intensive care unit. Critical Care Clinics, 29(1), 51-65. doi:10.1016/j.ccc.2012.10.007
4. Confusion Assessment Method (CAM). (n.d.). Retrieved from http://www.medscape.com/viewarticle/481726
5. Waszynski, C. M. (2012). The Confusion Assessment Method (CAM). Best Practices in Nursing Care to Older Adults, (13). Retrieved from https://consultgeri.org/try-this/general-assessment/issue-13.pdf
6. Delirium: prevention, diagnosis and management (2010). https://www.nice.org.uk/guidance/cg103/chapter/1-guidance
7. Ely, E. W., Inouye, S. K., Bernard, G. R., Gordon, S., Francis, J., May, L., … Dittus, R. (2001). Delirium in mechanically ventilated patients. JAMA, 286(21), 2703. doi:10.1001/jama.286.21.2703
8. Family Engagement and Empowerment (n.d.). http://www.icudelirium.org/family.html
9. Fong, T. G., Tulebaev, S. R., & Inouye, S. K. (2009). Delirium in elderly adults: diagnosis, prevention and treatment. Nature Reviews Neurology, 5(4), 210-220. doi:10.1038/nrneurol.2009.24
10. Girard, T. D., Jackson, J. C., Pandharipande, P. P., Pun, B. T., Thompson, J. L., Shintani, A. K., … Wesley Ely, E. (2010). Delirium as a predictor of long-term cognitive impairment in survivors of critical illness. Critical Care Medicine, 38(7), 1513-1520. doi:10.1097/ccm.0b013e3181e47be1
11. Gleason, O. (n.d.). Delirium - American Family Physician. http://www.aafp.org/afp/2003/0301/p1027.html
References
12. Inouye, S. K., Westendorp, R. G., & Saczynski, J. S. (2014). Delirium in elderly people. The Lancet, 383(9920), 911-922. doi:10.1016/s0140-6736(13)60688-1
13. Leslie, D. L., & Inouye, S. K. (2011). The importance of delirium: Economic and societal costs. Journal of the American Geriatrics Society, 59, S241-S243. doi:10.1111/j.1532-5415.2011.03671.x
14. Managing delirium among elderly patients in the ED. (n.d.). Retrieved from http://www.physiciansweekly.com/managing-delirium-elderly-patients/
15. Pandharipande, P., Girard, T., Jackson, J., Morandi, A., Thompson, J., Pun, B., … Brummel, N. (2013). Long-term cognitive impairment after critical illness. New England Journal of Medicine, 369(3), 1306-1316. doi:10.1056/NEJMoa1301372
16. Rudolph, J. L., & Marcantonio, E. R. (2011). Postoperative delirium. Anesthesia & Analgesia, 112(5), 1202-1211. doi:10.1213/ane.0b013e3182147f6d
17. Sessler, C. N., Gosnell, M. S., Grap, M. J., Brophy, G. M., O'Neal, P. V., Keane, K. A., … Elswick, R. K. (2002). The Richmond agitation–sedation scale. American Journal of Respiratory and Critical Care Medicine, 166(10), 1338-1344. doi:10.1164/rccm.2107138
18. Schweickert WD, et al. Lancet. 2009;373:1874-1882.
19. Vasilevskis, E. E., Han, J. H., Hughes, C. G., & Ely, E. W. (2012). Epidemiology and risk factors for delirium across hospital settings. Best Practice & Research Clinical Anaesthesiology, 26(3), 277-287. doi:10.1016/j.bpa.2012.07.003.
20. American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
21. Agarwal, V., O’Neill, P. J., Cotton, B. A., Pun, B. T., Haney, S., Thompson, J., … Pandharipande, P. (2010). Prevalence and risk factors for development of delirium in burn intensive care unit patients. Journal of Burn Care & Research: Official Publication of the American Burn Association, 31(5), 706–715. http://doi.org/10.1097/BCR.0b013e3181eebee9
5/23/2019
35
References
22. DeCrane, S. K., Sands, L., Ashland, M., Lim, E., Tsai, T. L., Paul, S., & Leung, J. M. (2011). Factors Associated with Recovery from Early Postoperative Delirium. Journal of Perianesthesia Nursing : Official Journal of the American Society of PeriAnesthesia Nurses / American Society of PeriAnesthesia Nurses, 26(4), 231–241. http://doi.org/10.1016/j.jopan.2011.03.001
23. Tomlinson, E. J., Phillips, N. M., Mohebbi, M., & Hutchinson, A. M. (2016). Risk factors for incident delirium in an acute general medical setting: a retrospective case-control study. Journal of Clinical Nursing, 26(5-6), 658-667. doi:10.1111/jocn.13529
24. Watkins, C. C., & Treisman, G. J. (2015). Cognitive impairment in patients with AIDS – prevalence and severity. HIV/AIDS (Auckland, N.Z.), 7, 35–47. http://doi.org/10.2147/HIV.S39665
25. Elsamadicy, A. A., Wang, T. Y., Back, A. G., Lydon, E., Reddy, G. B., Karikari, I. O., & Gottfried, O. N. (2017). Post-operative delirium is an independent predictor of 30-day hospital readmission after spine surgery in the elderly (≥65 years old): A study of 453 consecutive elderly spine surgery patients. Journal of Clinical Neuroscience, 41, 128-131. doi:10.1016/j.jocn.2017.02.040
26. Kalish, V. B., Gillham, J. E., & Unwin, B. K. (2014). Delirium in Older Persons: Evaluation and Management. American Family Physician, 1(90), 150-158. Retrieved from http://www.aafp.org/afp/2014/0801/p150.html#commenting
27. Hipp, D. M., & Ely, E. W. (2012). Pharmacological and Nonpharmacological Management of Delirium in Critically Ill Patients. Neurotherapeutics, 9(1), 158–175. http://doi.org/10.1007/s13311-011-0102-9
28. Freter, S., Dunbar, M., Koller, K., MacKnight, C., & Rockwood, K. (2015). Risk of Pre-and Post-Operative Delirium and the Delirium Elderly At Risk (DEAR) Tool in Hip Fracture Patients. Canadian Geriatrics Journal, 18(4), 212–216. http://doi.org.aurarialibrary.idm.oclc.org/10.5770/cgj.18.185
References
29. Kuczmarska, A., Ngo, L. H., Guess, J., O’Connor, M. A., Branford-White, L., Palihnich, K., … Marcantonio, E. R. (2015).Detection of Delirium in Hospitalized Older General Medicine Patients: A Comparison of the 3D-CAM and CAM-ICU. Journal of General Internal Medicine, 31(3), 297-303. doi:10.1007/s11606-015-3514-0
30. Han, J. H., Wilson, A., Vasilevskis, E. E., Shintani, A., Schnelle, J. F., Dittus, R. S., … Ely, E. W. (2013). Diagnosing Delirium in Older Emergency Department Patients: Validity and Reliability of the Delirium Triage Screen and the Brief Confusion Assessment Method. Annals of Emergency Medicine, 62(5), 457-465. doi:10.1016/j.annemergmed.2013.05.003
31. Sarutzki-Tucker, A., & Ferry, R. (2014). Beware of Delirium. The Journal for Nurse Practitioners, 10(8), 575-581. doi:10.1016/j.nurpra.2014.07.003
32. Scheffer, A. C., Van Munster, B. C., Schuurmans, M. J., & De Rooij, S. E. (2011). Assessing severity of delirium by the delirium observation screening scale. International Journal of Geriatric Psychiatry, 26(3), 284-291. doi:10.1002/gps.2526
33. Gaudreau, J., Gagnon, P., Harel, F., Tremblay, A., & Roy, M. (2005). Fast, Systematic, and Continuous Delirium Assessment in Hospitalized Patients: The Nursing Delirium Screening Scale. Journal of Pain and Symptom Management, 29(4), 368-375. doi:10.1016/j.jpainsymman.2004.07.009
34. Clegg, A. & Young, B. Which medications to avoid in people at risk for delirium: systematic review. Age and Aging, 2011. 40(1): p. 23-29.
35. Rosenbloom-Brunton, D., Henneman,E. and Inouye, S. (2010). Feasibility of family participation in delirium prevention program for the older hospitalized patient. Journal of Gerontological Nursing. 36(9). p. 22-25. 36. Mailhat, T., Cossette, S., Bourbonnds, A. et. al. (2014). Evaluation of a nurse mentoring intervention to family caregivers in the management of delirium after cardiac surgery (MENTOR _ D): a study protocol for a randomized controlled pilot trial. BioMedCentral. https://doi.org/10.1186/1745-6215-15-306.37. Halloway, S. (2014). A family approach to delirium: a review of literature. Age & Mental Health. 18(2).38. ICU Delirium for Patients and Families. www.icudelirium.org/family.html
5/23/2019
36
71
Appreciation!
Recognition!
Celebration!
72
National/Regional Accomplishments
National
• 90,961 hospital readmissions avoided
• 388 communities
• 1.1 billion dollars cost avoided
Regional (Lake Superior QIN – MI, MN, WI)
• 15,500 hospital readmissions avoided
• 26 communities
• 199 million dollars cost avoided
5/23/2019
37
73
North East MNAccomplishments
Participation:
• 232 individual participants
• 78 different organizations
• Assisted Living Facilities
• Clinics
• Community organizations
• Government groups
• Health plans
• Health Systems
• Home Health Agencies
• Hospice programs
• Hospitals
• Nursing Homes
• Pharmacy Groups
• University
• Resource suppliers
74
North East MNAccomplishments
Workgroups:
Started summer 2015
• Communication – Duluth area
• Exacerbation of Chronic Conditions (CHF/COPD)
– Virginia area
• Medications-related issues – Duluth area
• Resources/Patient Engagement – Duluth area
• Social Support – Virginia Area
5/23/2019
38
75
North East MN Accomplishments
What changes has your organization
made to improve care transitions,
care coordination or reduce
unnecessary hospital readmissions
in the past four years?
76
Recognition
5/23/2019
39
77
Celebration!
78
Contact Info
Janelle Shearer, Stratis Health
952-853-8553 or 877-787-2847
5/23/2019
40
This material was prepared by the Lake Superior
Quality Innovation Network, under contract with the
Centers for Medicare & Medicaid Services (CMS), an
agency of the U.S. Department of Health and Human Services.
The materials do not necessarily reflect CMS policy.
11SOW-MN-C3-19-114 052319