contingency management advanced clinical management of addiction module luke mitcheson clinical...
TRANSCRIPT
Contingency ManagementAdvanced Clinical Management of Addiction Module
Luke MitchesonClinical Psychologist
Objectives
•Understand what CM is and aims to achieve
•Understand the evidence base
•Consider implementation issues
Introduction to Contingency Management• What is Contingency Management?
• How has it been used in General Health Care?
• How has it been delivered in drug misuse? • BBV• Methadone Maintenance
• What is the evidence for effectiveness? • CM in drug use (data from NICE)• What NICE had to say
• Delivering CM in practice
THEORY
What is Contingency Management?
Conditioning in which an operant (voluntary) response is brought under stimulus control by virtue of presenting reinforcement contingent upon the occurrence of the operant response
OR
The basic process by which an individual's behaviour is shaped by reinforcement or by punishment
Based on operant conditioning principles (Skinner)
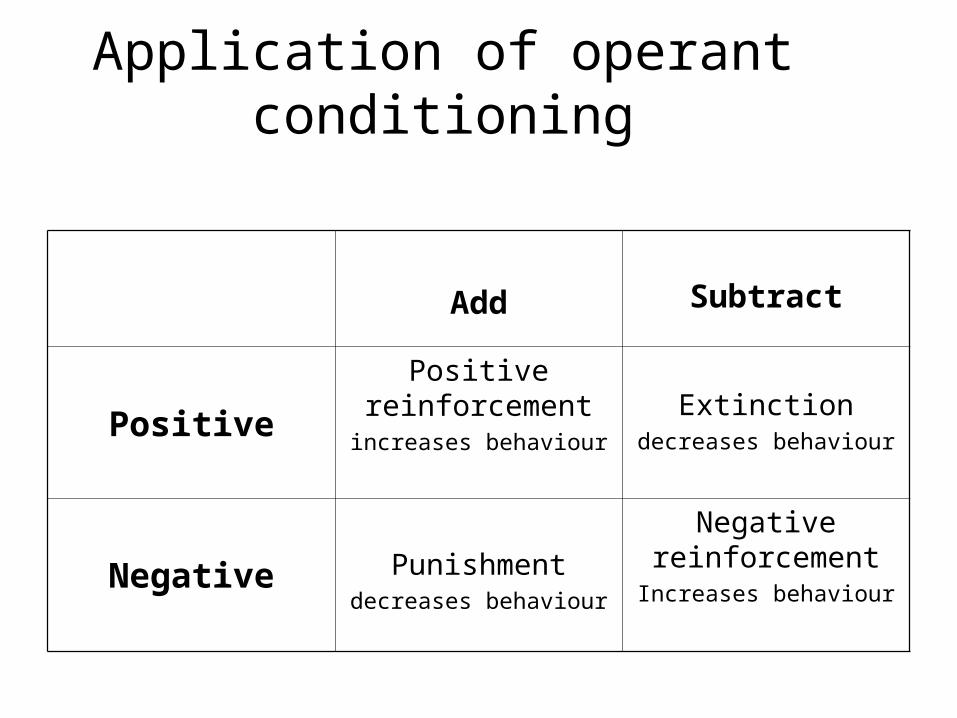
Application of operant conditioning
Add Subtract
Positive
Positive reinforcement
increases behaviour
Extinctiondecreases behaviour
Negative Punishmentdecreases behaviour
Negative reinforcement
Increases behaviour
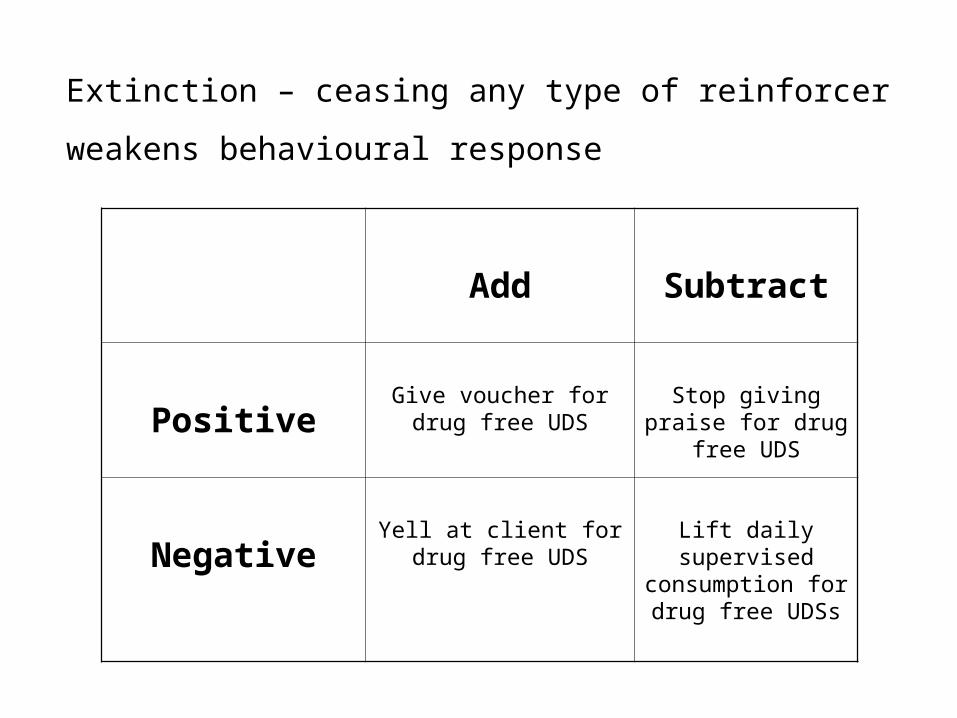
Add Subtract
PositiveGive voucher for drug
free UDSStop giving praise for drug free UDS
NegativeYell at client for drug
free UDSLift daily supervised
consumption for drug free UDSs
Extinction – ceasing any type of reinforcer
weakens behavioural response

The Essential Elements
– A discrete behaviour under voluntary control
– Quantifiable targets – e.g. child does 15 minutes piano practice
– Identified reinforcement (incentives, rewards) - e.g. praise, vouchers, prizes, privileges, cash
– Clear contingent relationship between behaviour and reinforcement (schedules of reinforcement which are consistent and immediate(at least initially) )
– All reinforcement takes place in a context of already existing contingencies (AB-C)
EVIDENCE
Use in General Health Care – Children – Star Charts (NICE – Nocturnal Enuresis)
– Attendance for mammograms, cervical smears, TB screening/treatment (Giuffrida & Torgenson, 1997, BMJ)
– Challenging behaviour in learning difficulties (Howlin et al 2009)
– Depression (Martel et al, 2004)
– The Quality and Outcomes Framework for primary care (Lester and Rowland, 2007)
– Attendance at the gym (Charness & Gneezy 2009)
– Smoking cessation (Volpp et al 2009)
– Medication compliance (Claassen et al 2007)
NICE view of CM
An effective and cost-effective intervention for improving treatment outcomes for problem drug users (NICE, 2007)
–The only recommended intervention for stimulant drug users

CM in Drug Misuse
• Adherence to healthcare interventions – e.g. Hep B vaccinations
• Stimulants – abstinence
• Methadone – reduce illicit opiate/stimulant ‘use-on-top’
• Detoxification – improved adherence
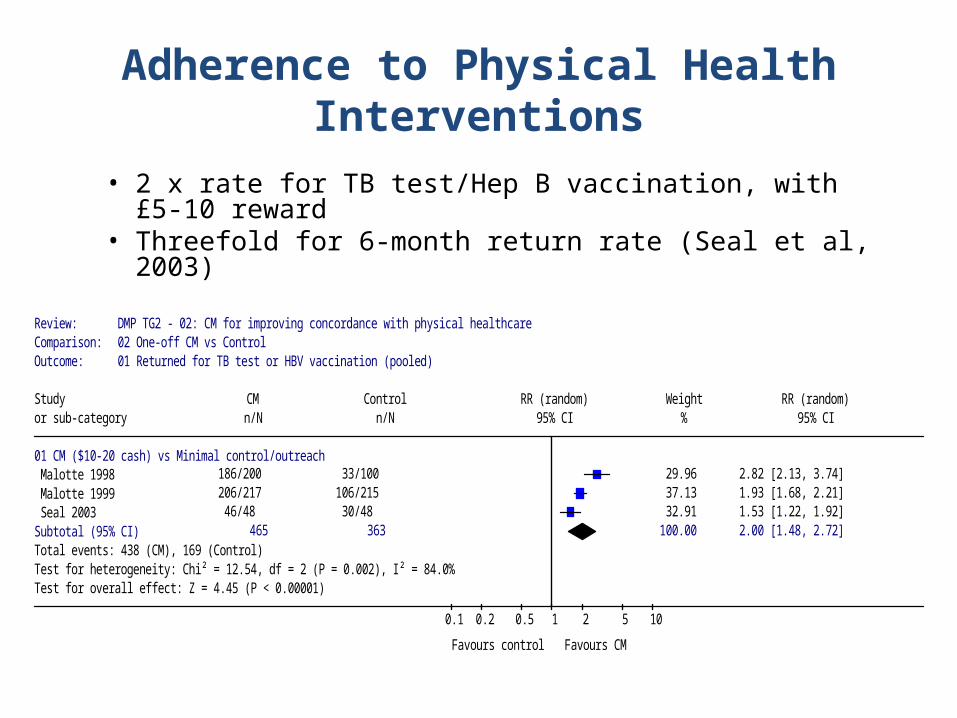
Adherence to Physical Health Interventions
• 2 x rate for TB test/Hep B vaccination, with £5-10 reward• Threefold for 6-month return rate (Seal et al, 2003)
Review: DMP TG2 - 02: CM for improving concordance with physical healthcareComparison: 02 One-off CM vs Control Outcome: 01 Returned for TB test or HBV vaccination (pooled)
Study CM Control RR (random) Weight RR (random)or sub-category n/N n/N 95% CI % 95% CI
01 CM ($10-20 cash) vs Minimal control/outreach Malotte 1998 186/200 33/100 29.96 2.82 [2.13, 3.74] Malotte 1999 206/217 106/215 37.13 1.93 [1.68, 2.21] Seal 2003 46/48 30/48 32.91 1.53 [1.22, 1.92] Subtotal (95% CI) 465 363 100.00 2.00 [1.48, 2.72]Total events: 438 (CM), 169 (Control)Test for heterogeneity: Chi² = 12.54, df = 2 (P = 0.002), I² = 84.0%Test for overall effect: Z = 4.45 (P < 0.00001)
0.1 0.2 0.5 1 2 5 10
Favours control Favours CM
Methadone Maintenance- CM for Illicit Drug Use
• Most substantial evidence base
• Large and consistent effect
• Participants shown to remain abstinent for as long as 6 months
• Cost effective• QALY health care costs alone = £15,000• QALY including criminal justice = £74
Review: DMP TG3 - 06: Opioid agonist + CMComparison: 01 MMT + CM versus MMT + Control Outcome: 06 continuous periods of abstinence (in weeks)
Study MMT + CM MMT+ Control RR (random) Weight RR (random)or sub-category n/N n/N 95% CI % 95% CI
05 3 weeks PETRY2002 11/19 5/23 17.08 2.66 [1.12, 6.33] SCHOTTENFELD2005 17/40 17/40 24.00 1.00 [0.60, 1.66] STITZER1992 8/25 2/25 9.52 4.00 [0.94, 17.00] SILVERMAN1998 12/20 2/19 10.36 5.70 [1.46, 22.18] PRESTON2000 13/29 6/28 17.95 2.09 [0.92, 4.73] RAWSON2002 19/30 8/30 21.09 2.38 [1.24, 4.56] Subtotal (95% CI) 163 165 100.00 2.19 [1.31, 3.65]Total events: 80 (MMT + CM), 40 (MMT+ Control)Test for heterogeneity: Chi² = 11.07, df = 5 (P = 0.05), I² = 54.8%Test for overall effect: Z = 2.99 (P = 0.003)
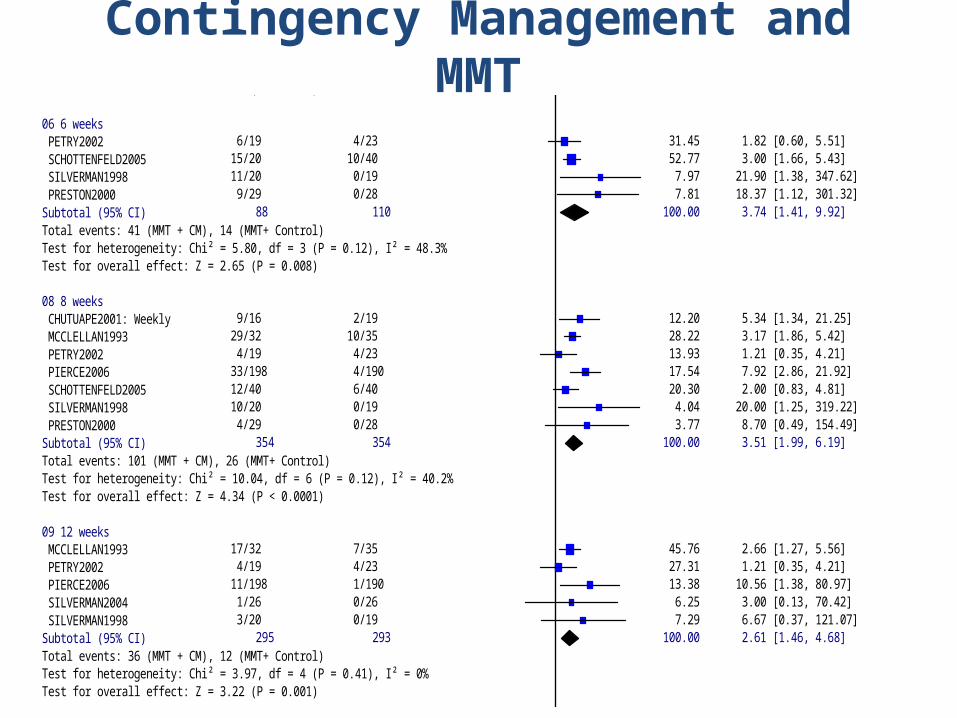
06 6 weeks PETRY2002 6/19 4/23 31.45 1.82 [0.60, 5.51] SCHOTTENFELD2005 15/20 10/40 52.77 3.00 [1.66, 5.43] SILVERMAN1998 11/20 0/19 7.97 21.90 [1.38, 347.62] PRESTON2000 9/29 0/28 7.81 18.37 [1.12, 301.32] Subtotal (95% CI) 88 110 100.00 3.74 [1.41, 9.92]Total events: 41 (MMT + CM), 14 (MMT+ Control)Test for heterogeneity: Chi² = 5.80, df = 3 (P = 0.12), I² = 48.3%Test for overall effect: Z = 2.65 (P = 0.008)
08 8 weeks CHUTUAPE2001: Weekly 9/16 2/19 12.20 5.34 [1.34, 21.25] MCCLELLAN1993 29/32 10/35 28.22 3.17 [1.86, 5.42] PETRY2002 4/19 4/23 13.93 1.21 [0.35, 4.21] PIERCE2006 33/198 4/190 17.54 7.92 [2.86, 21.92] SCHOTTENFELD2005 12/40 6/40 20.30 2.00 [0.83, 4.81] SILVERMAN1998 10/20 0/19 4.04 20.00 [1.25, 319.22] PRESTON2000 4/29 0/28 3.77 8.70 [0.49, 154.49] Subtotal (95% CI) 354 354 100.00 3.51 [1.99, 6.19]Total events: 101 (MMT + CM), 26 (MMT+ Control)Test for heterogeneity: Chi² = 10.04, df = 6 (P = 0.12), I² = 40.2%Test for overall effect: Z = 4.34 (P < 0.0001)
09 12 weeks MCCLELLAN1993 17/32 7/35 45.76 2.66 [1.27, 5.56] PETRY2002 4/19 4/23 27.31 1.21 [0.35, 4.21] PIERCE2006 11/198 1/190 13.38 10.56 [1.38, 80.97] SILVERMAN2004 1/26 0/26 6.25 3.00 [0.13, 70.42] SILVERMAN1998 3/20 0/19 7.29 6.67 [0.37, 121.07] Subtotal (95% CI) 295 293 100.00 2.61 [1.46, 4.68]Total events: 36 (MMT + CM), 12 (MMT+ Control)Test for heterogeneity: Chi² = 3.97, df = 4 (P = 0.41), I² = 0%Test for overall effect: Z = 3.22 (P = 0.001)
10 16 weeks MCCLELLAN1993 8/32 0/35 100.00 18.55 [1.11, 308.90] Subtotal (95% CI) 32 35 100.00 18.55 [1.11, 308.90]Total events: 8 (MMT + CM), 0 (MMT+ Control)Test for heterogeneity: not applicableTest for overall effect: Z = 2.03 (P = 0.04)
11 26 weeks SILVERMAN2004 11/26 0/26 100.00 23.00 [1.43, 371.00] Subtotal (95% CI) 26 26 100.00 23.00 [1.43, 371.00]Total events: 11 (MMT + CM), 0 (MMT+ Control)Test for heterogeneity: not applicableTest for overall effect: Z = 2.21 (P = 0.03)
0.001 0.01 0.1 1 10 100 1000
Favours MMT+Control Favours MMT + CM
Contingency Management and MMT

CM for Opiate Detoxification
• More likely to detox successfully• More likely to achieve abstinence
Review: DMD 8: Detoxification + psychosocial interventionComparison: 02 (Detoxification + CM) versus (detoxification + control) Outcome: 01 Completion of detoxification
Study CM control RR (fixed) Weight RR (fixed)or sub-category n/N n/N 95% CI % 95% CI
01 CM Bickel 1997: CM+CRA 10/19 4/20 10.97 2.63 [0.99, 6.98] Hall 1979: CM 25/40 21/41 58.37 1.22 [0.83, 1.79] Higgins 1984: CM 5/9 2/10 5.33 2.78 [0.71, 10.94] Higgins 1986: CMmeth 9/13 7/13 19.70 1.29 [0.69, 2.39] McCaul 1984: CM 7/10 2/10 5.63 3.50 [0.95, 12.90] Subtotal (95% CI) 91 94 100.00 1.60 [1.18, 2.16]Total events: 56 (CM), 36 (control)Test for heterogeneity: Chi² = 5.40, df = 4 (P = 0.25), I² = 25.9%Test for overall effect: Z = 3.07 (P = 0.002)
0.01 0.1 1 10 100
Favours control Favours CM
Discussion
How ethical do you think it is to use offer service users vouchers ?
21
So why isn’t CM routinely used?
• In a survey of all NHS drug clinics for opiate users in England, NO SERVICE was identified as providing a structured CM programme (Weaver et al, 2007)
22
Concerns….1. The acceptability and perceptions of CM to the
general public and service users, the attitudes of staff and senior managers.
In particular, these concerns include:
• The intervention may ‘reward’ illicit drug use
• The effects will not be maintained long-term
• The system is open to abuse as drug users may ‘cheat’ their drug tests
23
2. The unusual circumstances required to conduct RCTs and non-representativness of participants (exclusion criteria)
3. The costs associated with its implementation
4. Staff are not trained: major training programme required to implement
5. Cultural difference between US health care system and publicly funded English system
6. Incentive-based systems will not work outside the healthcare system (USA) in which they were developed
7. Differences in the welfare benefits systems between the USA and England (will UK users lose benefits?)
IMPLEMENTATION

25
Key issues in implementing a CM programme (Petry, 2006)
• Robust, routine testing for drug misuse• Targets agreed in collaboration with service
users• Incentives provided in a timely and
consistent manner• Relationship between treatment goal and
incentive schedule understood by service users
• Incentives that are perceived to be reinforcing and support a drug-free lifestyle
26
5 key aspects of implementing CM (Kellogg et al, 2005)
1. Rewards should be given frequently2. Should be easy to earn rewards at the
start3. Rewards to include material goods and
services that are of use and value to service users
4. Connection between reward and behaviour clear
5. Increased emphasis on reward-oriented not punishment-oriented approaches
27
Frequency and ease of earning rewards at the start
• Closely linked
• Frequent rewards = stronger connection to behaviour
• Target behaviour must not be too difficult: ‘successive approximation’ (e.g. Elk et al, 1995)
28
Material goods and services
• Rewards should be genuinely rewarding for service user
• For example, vouchers and clinic privileges should all be chosen in conjunction with service user
29
Connection between reward and behaviour
• Rewards are more effective if their distribution is directly connected to specific and observable behaviours
• The greater the delay in receiving the reinforcement, the weaker its effect

30
Reward-oriented rather than punishment-oriented
• Almost all trials showing efficacy of CM have been reward-oriented (e.g. Higgins et al, 1993; Stitzer et al, 1992)
• Adding a punitive aspect to a CM reward-oriented treatment has not found to be effective (Iguchi et al, 1988)
31
Maintenance of behaviour after reinforcement
• Don’t terminate a CM programme until target behaviour is stabilised
• Reduce frequency and value of rewards towards end of programme (e.g. Higgins 1993, 1994; Petry 2004,2005)
32
Implementing CM in the NHS
• Major studies of implementation in services where initially there was considerable resistance
• Positive shifts in staff attitudes (McGovern et al, 2004; Kellogg et al, 2005; Kirby et al, 2006; Ritter and Cameron, 2006)
33
1. Endorsement of the programme by senior management and clinicians
2. Provision of a comprehensive education and training programme
3. Recognition by staff that CM is an intervention aimed at changing behaviours not simply reinforcing people for generally good behaviour
4. Shift in focus of service to one that is reward orientated
Kellogg et al (2005)

34
Factors to be considered when developing an programme in the NHS
• Integration of CM with key working responsibilities of staff
• Identification of groups of drug users who are most likely to benefit
• Development of near patient testing• Impact of service users benefits
35
Reinforcement schedules
• Clinic privileges (Stitzer et al, 1992; 1986)
• Voucher reinforcement (Petry et al, 2000)
• Cash (Malotte et al, 1998; Seal et al, 2003)
• Prizes (Petry et al, 2005; Prendegast et al, 2006)
TRIAGE
TRIAGE
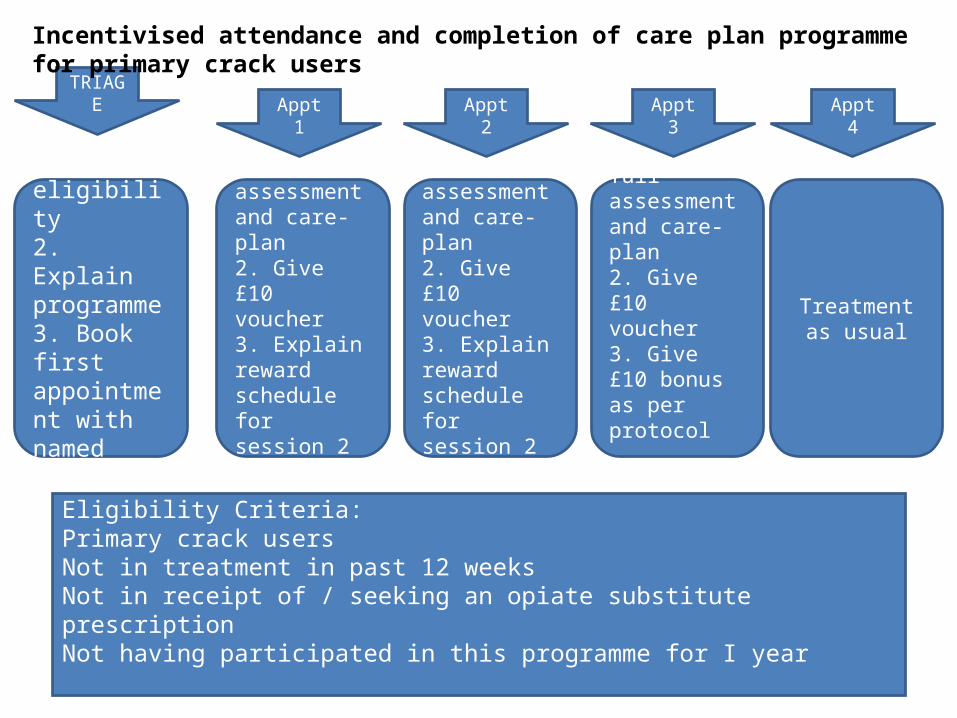
1. Ensure eligibility2. Explain programme3. Book first appointment with named worker
1. Work on full assessment and care-plan2. Give £10 voucher3. Explain reward schedule for session 2 and 3
1. Work on full assessment and care-plan2. Give £10 voucher3. Give £10 bonus as per protocol
1. Work on full assessment and care-plan2. Give £10 voucher3. Explain reward schedule for session 2 and 3
Treatment as usual
TRIAGEAppt 1 Appt 2 Appt 3 Appt 4
Incentivised attendance and completion of care plan programme for primary crack users
Eligibility Criteria: Primary crack usersNot in treatment in past 12 weeksNot in receipt of / seeking an opiate substitute prescriptionNot having participated in this programme for I year
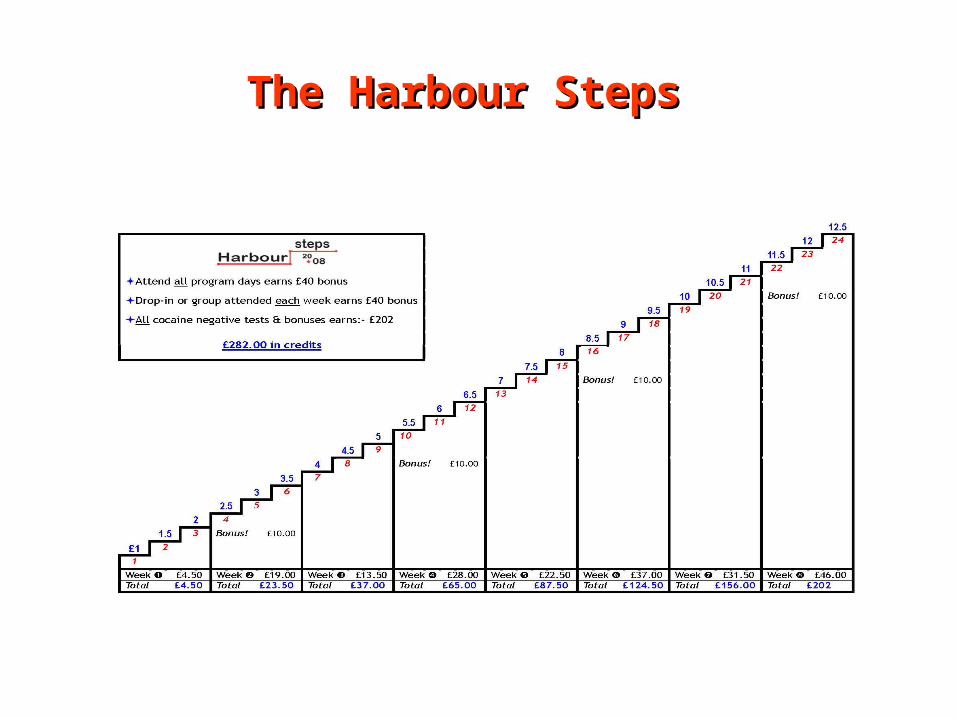
The Harbour StepsThe Harbour Steps

Lambeth voucher-CMLambeth voucher-CM
► 24 tests on Monday, Wednesday & Friday► Escalating schedule starting at £1► Up by £0.5 for each successive –ive test► Bonus for each series of 6 –ive tests► Re-set following +ive test or DNA► Return to previous level for 6 –ives (if time)► £40 bonus if client attends all 24 sessions► Total voucher value possible = £282► Harbour voucher credits recorded in account book and
withdrawn on treatment days
References• Higgins ST, Budney AJ, Bickel WK, Foerg FE, Donham R, Badger GJ. Incentives improve
outcome in outpatient behavioral treatment of cocaine dependence. Arch Gen Psychiatry 1994; 51: 568-76.
• Lussier JP, Heil SH, Mongeon JA, Badger GJ, Higgins ST. A meta-analysis of voucher-based reinforcement therapy for substance use disorders. Addiction 2006; 101:192-203.
• Petry NM, Peirce JM, Stitzer ML, Blaine J, Roll JM, Cohen A, et al. Effect of prize-based incentives on outcomes in stimulant abusers in outpatient psychosocial treatment programs: A national drug abuse treatment clinical trials network study. Arch Gen Psychiatry 2005. ; 62:1148-56
• Peirce JM, Petry NM, Stitzer ML, Blaine J, Kellogg S, Satterfield F, et al. Effects of lower-cost incentives on stimulant abstinence in methadone maintenance treatment: a National Drug Abuse Treatment Clinical Trials Network study. Arch Gen Psychiatry 2006. ; 63:201-8.
• Kellogg SH, Burns M, Coleman P, Stitzer M, Wale JB, Kreek MJ. Something of value: the introduction of contingency management interventions into the New York City Health and Hospital Addiction Treatment Service. J Subst Abuse Treat 2005; 28: 57-65
• Petry NM, Alessi SM, Hanson T, Sierra S. Randomized trial of contingent prizes versus vouchers in cocaine-using methadone patients. J Consult Clin Psychol 2007; 75: 983-91
• Olmstead TA, Petry NM. The cost-effectiveness of prize-based and voucher-based contingency management in a population of cocaine- or opioid-dependent outpatients. Drug Alcohol Depend 2009. ; 102:108-15.