conservative care & musculoskeletal management
TRANSCRIPT

CONSERVATIVE CARE &MUSCULOSKELETAL MANAGEMENT
Published: 6/18/2018

CONTENTS

1 The Opioid Epidemic
2 Cost of Musculoskeletal Injuries
3 Conservative Care Options
4 Conservative Care & Common Injuries
5 Cases of Using PT First
9 Everflex and Its Goals
10 Orthopaedic Section, APTA Inc. Clinical Practice Guidelines

WHAT IS THE OPIOID EPIDEMIC?
In the late 1990s, pharmaceutical companies reassured the medical
community that patients would not become addicted to opioid
pain relievers, and healthcare providers began to prescribe them
at greater rates. Increased prescriptions of opioid medications led
to widespread misuse of both prescription and non-prescription
opioids before it became clear that these medications could
indeed be highly addictive. In 2017, the U.S. Department of Health
and Human Services declared a public health emergency.
Public A�airs. “What Is the U.S. Opioid Epidemic?” HHS.gov, HHS.gov, 6 Mar. 2018, www.hhs.gov/opioids/about-the-epidemic.

According to a report issued by the United States Bone and
Joint Initiative (USBJI), an estimated 126.6 million Americans
(one in two adults) are a�ected by a musculoskeletal
condition comparable to the total percentage of Americans
living with a chronic lung or heart condition. The cost is an
estimated $213 billion in annual treatment, care, and lost
wages.
COST OF MUSCULOSKELETAL INJURIESON HEALTHCARE SYSTEM
ONE IN TWO AD U L TS$21 3 BILLION
A STUDY PUBLISHED IN THE JOURNALOF PAIN ESTIMATED THE COST OF ALLPAIN TO BE EVEN MORE — BETWEEN$560 AND $635 BILLION DOLLARS.
United States Bone and Joint Initiative: The Burden of Musculoskeletal Diseases in the United States (BMUS), Third Edition, 2014. Rosemont, IL. Available at http://www.boneandjointburden.org. Accessed on May 21, 2018.
1. Physical Therapy
2. Wellness & Injury Prevention Programs
3. Work-Related Task Training Programs
4. Psychological Evaluation
NON-CONSERVATIVEOPTIONS
• Medications• Imaging• Surgeries• Injections
CONSERVATIVE CARE OPTIONSWhy P T 1 s t?A study, published in the journal Health ServicesResearch (HSR) in 2011, reviewed 62,707 episodes of physical therapy over a 5-year period. Patients who visited a physical therapist directly for outpatient care (27%) had fewer visits and lower overall costs on average than those who were referred by a physician.
An additional study in the journal of Health Science Research in May of 2018, also notes that physical therapy as an initial treatment for low back pain is e�ective, saves money, but also dramatically reduces the chance of a patient being prescribed an opioid medication.
Bottom line, the subjects in this study experienced lower costs after 1 year and reduced their likelihood of being prescribed an opioid medication by 87% vs. those patients that never visited a physical therapist.
A Comparison of Health Care Use for Physician-Referred and Self-Referred Episodes of Outpatient Physical Therapy. doi.org/10.111/J.1475-6773.2011.01324.x.
Frogner, Bianca K., et al. “Physical Therapy as the First Point of Care to Treat Low Back Pain: An Instrumental Variables Approach to Estimate Impact on Opioid Prescription, Health Care Utilization, and Costs.” Health Services Research, 2018, doi: 10.111/1475-6773.12984.
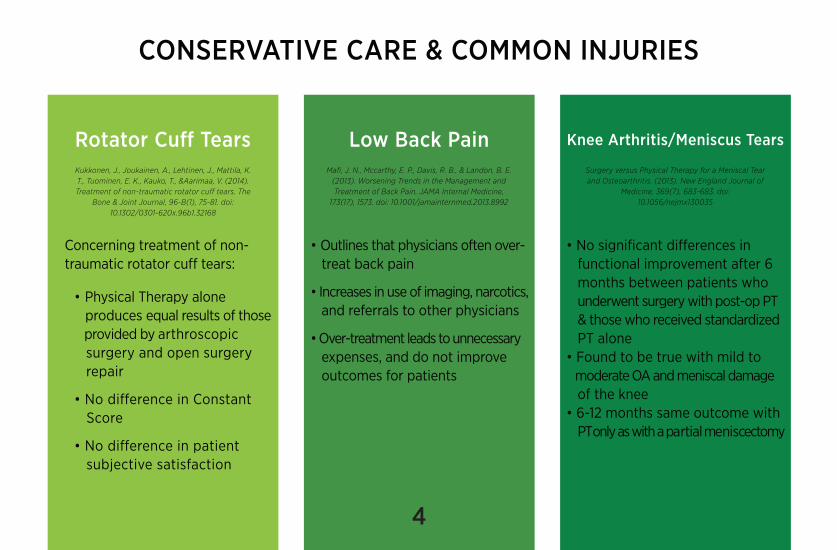
Rotator Cu� Tears
Concerning treatment of non-traumatic rotator cu� tears:
• Physical Therapy alone produces equal results of those provided by arthroscopic surgery and open surgery repair
• No di�erence in Constant Score
• No di�erence in patient subjective satisfaction
Low Back Pain
• Outlines that physicians often over- treat back pain
• Increases in use of imaging, narcotics, and referrals to other physicians
• Over-treatment leads to unnecessary expenses, and do not improve outcomes for patients
Knee Arthritis/Meniscus Tears
• No significant di�erences in functional improvement after 6 months between patients who underwent surgery with post-op PT & those who received standardized PT alone• Found to be true with mild to moderate OA and meniscal damage of the knee• 6-12 months same outcome with PT only as with a partial meniscectomy
CONSERVATIVE CARE & COMMON INJURIES
Kukkonen, J., Joukainen, A., Lehtinen, J., Mattila, K. T., Tuominen, E. K., Kauko, T., &Aarimaa, V. (2014). Treatment of non-traumatic rotator cu� tears. The
Bone & Joint Journal, 96-B(1), 75-81. doi: 10.1302/0301-620x.96b1.32168
Mafi, J. N., Mccarthy, E. P., Davis, R. B., & Landon, B. E. (2013). Worsening Trends in the Management and Treatment of Back Pain. JAMA Internal Medicine,
173(17), 1573. doi: 10.1001/jamainternmed.2013.8992
Surgery versus Physical Therapy for a Meniscal Tear and Osteoarthritis. (2013). New England Journal of
Medicine, 369(7), 683-683. doi: 10.1056/nejmx130035

OLD APPROACHAverage Cost: $2100-$2200
NEW APPROACHAverage Cost: $900-$1000
The initial meeting might nothappen for up to a month, andthen there is no set procedure
for treatment.
Immediately see physical therapist, whoinitiates an evidence-based conservative
program.
Initial meetingwith doctors.
PhysicalTherapy
Patient followsup with doctors.
Patient might undergodiagnostics, such as MRI
Patient mightsee a specialist
Patients with complicatedback pain are sent foradditional treatment
THE VIRGINIA MASON EXAMPLE FOR A PATHWAY FOR LOW BACK PAIN MANAGEMENT.
In partnership with Aetna, the VirginiaMason Medical Center cut low back paincare costs and the burden of low backcare by using physical therapy as theinitial intervention for patients.
THE CASE OF THE VIRGINIA MASON MEDICAL CENTER
• Patient wait times to see a provider dropped from 31 days to 1 day• MRI utilization plummeted from
42% to 6% of patients studied
• 94% of patients did not miss work
• 73% of patients utilized no prescription medications
• Total cost savings for the patient was
50%
RESULTS
McDonald, P. A., Mecklenburg, R. S., & Martin, L. A. (2015, July). The Employer-Led Health Care Revolution. Retrieved from https://hbr.org/2015/07/the-employer-led-health-care-revolution

BACK PAIN ACCOUNTS FOR 10% OFPRIMARY CARE PHYSICIAN VISITSAND $86 BILLION IN ANNUALHEALTHCARE SPENDING.
Mafi, J. N., Mccarthy, E.P., Davis, R. B., & Landon, B. E. (2013). Worsening Trends in the Management and Treatment of Back Pain. JAMA Internal Medicine, 173(17), 1573. doi: 10.1001/jamainternmed.2013.8992

PEOPLE WHO OPT FOR SURGERY FORTHE TREATMENT OF DEGENERATIVEDISK DISEASE DID NOT EXPERIENCEGREATER OUTCOMES IN PAIN ANDDISABILITY AS THOSE WHO OPTEDFOR PHYSICAL THERAPY.
Defining the Value of Spine Care. Rihn, Je�ry A. MD; Currier, Bradford L. MD; Phillips, Frank M. MD; Glassman, Steven D. MD; Albert, Todd J. MD. JAAOS - Journal of the American Academy of Orthopaedic Surgeons: July 2013 - Volume 21 - Issue 7 - p419-426 doi: 10.5435/JAAOS-21-07-419

THE INTEL EXAMPLE FOR A PATHWAY FOR LOW BACK PAIN MANAGEMENT
• Treatment costs of certain conditions fell by 24% - 49%• Patient satisfaction improved• More than 10,000 hours worth of waste in health care suppliers’ business processes was eliminated
RESULTSInitial ContactPatient with uncomplicatedlower back pain calls direct line to Health Care.
1.ScreeningRehab o�ce assistant uses ascreening tool to determinewhether the patient can gostraight to physical therapy. Ifso, patient is scheduled for anevaluation within 24 hours.
Physical TherapyPhysical therapist screenspatient for a second time forserious conditions, addressesfears (of cancer, permanentdisability, the need for surgery,and so on) , and beginstreatment: PT visits, once aweek (supplemented by homeexercises), for 3 weeks.
RecoveryPatient receives reassuranceimmediately and starts feelingbetter physically within a week.If patient does not improveas expected, an appointmentwith a specialist is arranged.
2.
3. 4.
In 2009, Intel faced soaring health carecosts — estimated to reach $1 billion by2012. The company tried variousmethods to reduce costs, such as: high-deductible/low premium plans, on-siteclinics, and employee wellness plans.However, these did not address the rootof the problem: the steadily rising costof care.
Their solution was to tackle the problemas it would a manufacturing challenge:by using lean improvement methods tovigorously manage the quality and costof its health care suppliers. Intel led ahealth care collaborative that focused onsix clinical processes for treating conditionssuch as diabetes and lower back pain.
THE CASE OF INTEL: Employer-led Healthcare Revolution
McDonald, P. A., Mecklenburg, R. S., & Martin, L. A. (2015, July). The Employer-Led Health Care Revolution. Retrieved from https://hbr.org/2015/07/the-employer-led-health-care-revolution

GOALS OF EVERFLEX
1. Decrease risk of excessive non-conservative medical management of common musculoskeletal conditions by encouraging early evidence based treatment plans
2. Improve productivity by decreasing down-time with an injury or prevent an injury from occurring
3. Improve access to care by addressing geographical constraints, financial concerns and inability to attend in-person sessions during work hours
WHAT IS EVERFLEX?
• Software based algorithm based on Clinical Practice Guidelines (CPG) of the Orthopaedic Section of the American Physical Therapy Association (APTA)
• Evidence based treatment patterns for various musculoskeletal conditions
• Injury Prevention and Injury Recovery Programs
• Screening process for early and prompt referral to physical therapist with video conference or in-person appointment
• High quality care and cost saving solution for
employees and employers

Clinical practice guidelines are defined by the Institute of
Medicine as systematically developed statements to assist
practitioner and patient decisions about appropriate health
care for specific clinical circumstances.
Physical therapy clinical practice guidelines were developed
using systematic reviews of the literature and provide the
reader with evidence suitable for evidence-based physical
therapist practice.
APTA CLINICAL PRACTICE GUIDELINESCURRENT ACADEMY OF ORTHOPAEDIC PHYSICAL THERAPY CPGs
• Neck Pain
• Shoulder Pain and Mobility Deficits
• Low Back Pain
• Hip Pain and Mobility Deficits
• Non Arthritic Hip Joint Pain
• Knee Stability & Movement Coordination Impairments: Knee Ligament Sprain
• Knee Pain and Mobility Impairments: Meniscal & Articular Cartilage Lessions
• Achilles Pain, Sti�ness, and Muscle Power Deficits; Midportion Achilles
• Ankle Stability and Movement Coordination Impairments
• Heel Pain- Plantar Fasciitis
is the first product to be reviewed & verified by the Academy of Orthopaedic
Physical Therapy.

CPG Citations
1. Neck PainPeter R. Blanpied, Anita R. Gross, James M. Elliott, Laurie Lee Devaney, Derek Clewley, David M. Walton, Cheryl Sparks, Eric K. Robertson. J Orthop Sports Phys Ther 2017;47(7):A1-A83. doi:10.2519/jospt.2017.0302
2. Shoulder Pain and Mobility DeficitsMartin J. Kelley, Michael A. Sha�er, John E. Kuhn, Lori A. Michener, Amee L. Seitz, Tim L. Uhl, Joseph J. Godges, Philip McClure. J Orthop Sports Phys Ther 2013;43(5):A1-A31, 351. doi:10.2519/jospt.2013.0302
3. Low Back PainAnthony Delitto, Steven Z. George, Linda Van Dillen, Julie M. Whitman, Gwendolyn Sowa, Paul Shekelle, Thomas R. Denninger, Joseph J. Godges. J Orthop Sports Phys Ther 2012;42(4):A1-A57. doi:10.2519/jospt.2012.42.4.A1
4. Hip Pain and Mobility DeficitsMichael T. Cibulka, Nancy J. Bloom, Keelan Enseki, Cameron McDonald, Judith Woehrle, Christine M. MacDonald. J Orthop Sports Phys Ther 2017;47(6):A1-A37. doi:10.2519/jospt.2017.0301
5. Non Arthritic Hip Joint PainKeelan Enseki, Marcie Harris-Hayes, Douglas M. White, Michael T. Cibulka, Judith Woehrle, Timothy L. Fagerson, John C. Clohisy, Roy D. Altman, Todd E. Davenport, Anthony Delitto, John DeWitt, Helene Fearon, Amanda Ferland, Timothy L. Flynn, Jennifer Kusnell, Joy MacDermid, RobRoy L. Martin, James W. Matheson, Philip McClure, John Meyer, Marc Philippon, Leslie Torburn. J Orthop Sports Phys Ther 2014;44(6):A1-A32. doi:10.2519/jospt.2014.0302
6. Knee Stability & Movement Coordination Impairments: Knee Ligament SprainDavid S. Logerstedt, David Scalzitti, May Arna Risberg, Lars Engebretsen, Kate E. Webster, Julian Feller, Lynn Snyder-Mackler, Michael J. Axe, Christine M. McDonough. J Orthop Sports Phys Ther. 2017;47(11):A1-A47. doi:10.2519/jospt.2017.0303
7. Knee Pain and Mobility Impairments: Meniscal & Articular Cartilage LessionsDavid S. Logerstedt, David A. Scalzitti, Kim L. Bennell, Rana S. Hinman, Holly Silvers-Granelli, Jay Ebert, Karen Hambly, James L. Cary, Lynn Snyder-Mackler, Michael J. Axe, Christine M. McDonough. J Orthop Sports Phys Ther 2018;48(2):A1-A50. doi:10.2519/jospt.2018.0301
8. Achilles Pain, Sti�ness, and Muscle Power Deficits; Midportion AchillesRobroy L. Martin, Ruth Chimenti, Tyler Cuddeford, Je� Houck, J.W. Matheson, Christine M. McDonough, Stephen Paulseth, Dane K. Wukich, Christopher R. Carcia. J Orthop Sports Phys Ther 2018;48(5):A1-A38. doi:10.2519/jospt.2018.0302
9. Ankle Stability and Movement Coordination ImpairmentsRobroy L. Martin, Todd E. Davenport, Stephen Paulseth, Dane K. Wukich, Joseph J. Godges. J Orthop Sports Phys Ther 2013;43(9):A1-A40. doi:10.2519/jospt.2013.0305
10. Heel Pain- Plantar FasciitisRobroy L. Martin, PT, PhD; Todd E. Davenport, DPT; Stephen F. Reischl, DPT; Thomas G. McPoil, PT, PhD; James W. Matheson, DPT; Dane K. Wukich, MD; Christine M. McDonough, PT, PhD. J Orthop Sports Phys Ther. 2014;44(11):A1-A23. doi:10.2519/jospt.2014.0
FOR MORE INFORMATION, VISITOR CONTACT US AT
(805) 250-5396
www.everflexhealth.com