confidential: for review only - bmj.com · confidential: for review only ... bmj journal: bmj date...
TRANSCRIPT
Confidential: For Review O
nly
Implementing shared decision making in routine NHS
settings - lessons from the MAGIC Programme
Journal: BMJ
Manuscript ID BMJ.2016.033197
Article Type: Analysis
BMJ Journal: BMJ
Date Submitted by the Author: 26-Apr-2016
Complete List of Authors: JOSEPH-WILLIAMS, NATALIE; Cardiff University, College of Biomedical Life Sciences Lloyd, Amy; Cardiff University, College of Biomedical Life Sciences, Centre for Trials Research Edwards, Adrian; Cardiff University, College of Biomedical Life Sciences,
Division of Population Medicine Stobbart, Lynne; Newcastle University, Institute of Health & Society Tomson, David; Collingwood Surgery Macphail, Sheila; The Newcastle Upon Tyne Hospitals NHS Foundation Trust Dodd, Carole; The Newcastle Upon Tyne Hospitals NHS Foundation Trust Brain, Katherine; Cardiff University, College of Biomedical Life Sciences, Division of Population Medicine Elwyn, Glyn; Dartmouth College, The Dartmouth Institute for Health Policy and Clinical Practice Thomson, Richard; Newcastle University, Institute of Health & Society
Keywords:
Shared Decision Making, Patient centred care, Implementation, Patient
involvement, Quality improvement, Patient participation, Physician-patient relations
https://mc.manuscriptcentral.com/bmj
BMJ
Confidential: For Review O
nly
V6.0 26.04.16
1
BMJ Analysis
Implementing shared decision making in routine NHS settings –
lessons from the MAGIC Programme
Implementing shared decision making is challenging, but possible, argue Natalie Joseph-Williams and
colleagues. A multi-level approach targeting organisations, clinicians, and patients is needed.
Natalie Joseph-Williams, Research Fellow 1
Amy Lloyd, Research Fellow 2
Adrian Edwards, Professor 1
Lynne Stobbart, Senior Research Associate3
David Tomson, Executive Partner and Freelance Consultant in Patient Centred Care4
Sheila Macphail, Consultant in Obstetrics and Fetal Medicine and Assistant Medical Director5
Carole Dodd, Programme Manager5
Kate Brain, Reader1
Glyn Elwyn, Professor6
Richard Thomson, Professor 3
1 Cardiff University, College of Biomedical and Life Sciences, Division of Population Medicine,
Cardiff, UK
2 Cardiff University, College of Biomedical and Life Sciences, Centre for Trials Research,
Cardiff, UK
3 Newcastle University, Institute of Health & Society, Newcastle upon Tyne, UK
4 Collingwood Surgery, North Shields, Tyne and Wear, UK
5 The Newcastle Upon Tyne Hospitals NHS Foundation Trust, Newcastle, UK
6 Dartmouth College, The Dartmouth Institute for Health Policy and Clinical Practice, New
Hampshire, USA
Corresponding author: Natalie Joseph-Williams
Current word count: 2084
Page 1 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
V6.0 26.04.16
2
Adoption of shared decision making (SDM) into routine practice has been remarkably slow, despite
forty years of research and considerable policy support. We need to move away from the traditional
research settings to learn from implementation work at the coalface, in collaboration with clinicians and
leaders responsible for routine healthcare. We need to identify what is and is not going to work in
reality. The MAGIC (Making Good Decisions in Collaboration) programme was commissioned by The
Health Foundation in 2010 to design, test, and identify the best ways to embed SDM into routine
primary and secondary care settings (see Box 1 for summary of MAGIC).[1 2] Here we draw upon our
overall learning from the three-year MAGIC programme, discuss the key challenges of implementing
SDM, and offer practical solutions to address them (See Table 1 for summary of solutions).
Key Challenge 1: “We do it already”
Attitudes are a key challenge facing any change programme. Introducing routine SDM and patient
choice requires both structural change, in terms of healthcare pathways and delivery, and culture and
attitudinal change amongst clinicians. Many clinicians feel that they already routinely involve patients
in decisions about their care, so often do not see how SDM differs from their usual practice. A minority
sees their role as ‘decision maker’ to act in the best interests of their patients. Clinicians’ long held
commitment to doing what they perceive to be the best for their patients is a key barrier to attitudinal
change. This is well intended, but fails to recognise that the individual patient’s values, opinions or
preferences might differ markedly from theirs.
An essential step in implementing SDM is to increase understanding of what it entails – that is,
‘building coherence’.[3 4] Clinical teams need support to review current practice, to build a shared
understanding of how SDM differs from their current practice, and to decide how they want to make
decisions with patients. Interactive skills training workshops using the SDM Model for Clinical
Practice[5] (Figure 1) were essential for building coherence, improving skills and promoting positive
attitudes (a slight variant of this model is also available).[6] Workshop feedback indicated that role-play
based training, with an emphasis on practical skills, worked better than theory-heavy presentations. We
increasingly included exercises that challenged embedded attitudes and promoted discussion around
them. The teams were generally already good at recognising options and discussing them with patients,
but risk communication and the task of ‘exploring what matters’ to patients, needed improvement. The
SDM skills training helped clinicians understand the key aspects of SDM and how it differed from
current ways of working. Some clinicians reported ‘light bulb’ moments, changing their view from ‘we
do this already’ to ‘we could do this better’.
Page 2 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
V6.0 26.04.16
3
Key Challenge 2: “We don’t have the right tools”
SDM is sometimes seen as giving patients decision aids (materials that help patients through the steps of
the decision making process). Many clinicians believe they cannot deliver SDM if they do not have a
‘tool’ to give their patients, or that a tool itself will enable SDM. One of the key learning points from the
MAGIC programme was that ‘skills trump tools, and attitudes trump skills’. It is therefore important to
build coherence of attitudes and understanding. Then, clinicians need to consider their approach to
communication skills to engage patients in decision making. Only then can timely access to evidenced-
based tools help to support the SDM process, but they are not an essential element. There will never be
decision support tools for every decision, nor will every patient find them acceptable or helpful. The
skills to have different types of conversations with patients are paramount, with or without an available
tool.
In the skills training workshops, role-play was particularly effective for showing that tools may support
the process, but do not replace SDM communication skills. Traditional outside-consultation tools, such
as websites, are costly and time consuming to develop and keep updated. Developing brief decision
support tools helped overcome this challenge.[7-11] Clinicians readily designed brief evidence-based
tools to use inside the consultation, such as Option Grids TM in the Cardiff sites[7] and Brief Decision
Aids in the Newcastle sites.[11] These provide short (1-3 pages) summaries of the treatment choices, the
likely outcomes, and the factors that patients might consider when making their decision. These brief
decision support tools assist with information sharing, providing risk and benefit data that are accessible
to both the clinician and patient together. Experience from MAGIC also suggested that in-consultation
tools were often better at facilitating discussion between patient and clinician than those used outside
the consultation. Some patients used the tool’s content to guide their own questions for the clinician and
it prompted them to ‘discuss what mattered to them’ – the nub of SDM. However, using such tools in
the consultation does not equate to SDM. The main danger is clinicians using brief decision aids to
enhance information transfer and their ‘talking at’ patients skills, rather than improving their ‘working
with’ patient skills – success depends more on skills and willingness of the patient and clinician to
contribute to the conversation, rather than use of decision aids.[12]
Key Challenge 3: “Patients don’t want shared decision making”
Clinicians often report that their patients ask ‘what would you do, doctor?’ and conclude that their
patients do not want to be involved in making healthcare decisions. The question is perfectly valid in the
context of SDM, and is one way of seeking the clinician’s expert opinion. It is different to the question
‘what should I do, doctor?’, which suggests a desire for a paternalistic approach. Indeed, it is worth
remembering that ‘shared’ in SDM recognises the value of two sources of expertise in the discussion.
Page 3 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
V6.0 26.04.16
4
Many patients feel unable, rather than unwilling, to share in decision making.[13 14] Some patients
think they will annoy clinicians by trying to be more involved,[15] and their desire to be a ‘good’
patient over-rides their desire for sharing decisions. Often this emerges from long standing experience
and expectations of a paternalistic approach and is more common in older people.[16 17] This can be
mistaken for lack of interest in engaging in decision making. Clinicians’ misconceptions about what
they think patients want must be addressed. They cannot make every patient be more involved, but more
can be done to make patients feel included and respected, and clinicians can often make more effort to
understand what is important to the patient. However, patients may also need support and preparation to
take part in a different type of consultation.
Patient activation and preparation are potentially valuable, and can increase the likelihood of patients
and clinicians being involved in mutually useful conversations. Patient activation campaigns focus on
changing patients’ attitudes about involvement in healthcare decisions, explaining what SDM involves,
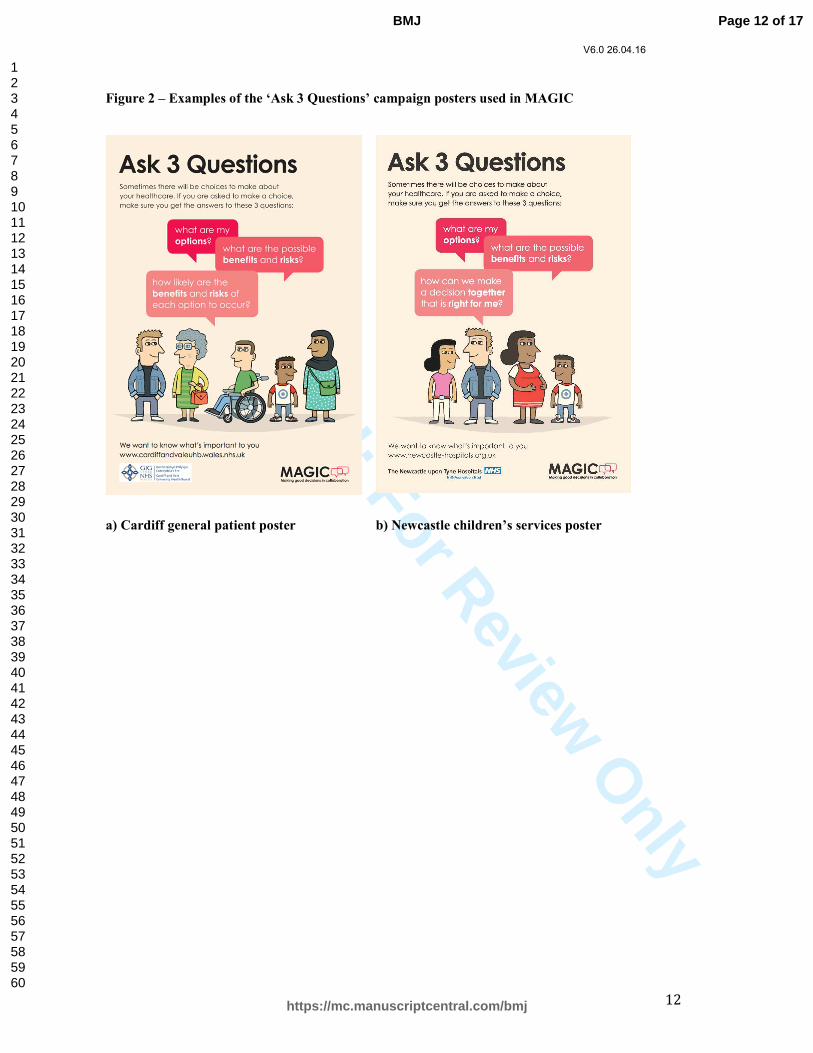
why it might help, and provide interventions such as question prompt lists. Some patients do not know
what SDM is, or what an SDM consultation is like; activation interventions such as the ‘Ask 3
Questions’ campaign used in the MAGIC programme can help patients know what to expect, and give
‘permission’ and encouragement to be involved (See Figure 2).[18-20]. These can be operationalised in
a variety of ways such as leaflets, posters, clinic letters and video. Interventions promoted from within
healthcare organisations are better received and convey that the organisation and clinicians support
SDM.
Successful implementation also needs wider patient and public involvement. In the MAGIC programme
we included both condition specific representatives for local interventions, and a wider user panel to
guide the broader implementation process. The lay panel was crucial in identifying areas for
improvements in the implementation work, providing users’ perspectives (i.e. identifying needs), and
aiding intervention development and testing.
Key Challenge 4: “How can we measure it?”
Clinicians and managers implementing SDM want to know what difference it makes to their patients,
and to clinical practice. In the MAGIC programme we found it difficult to identify or develop suitable
patient-reported measures to capture experience of SDM. Patient-reported measures are hampered by
ceiling effects, or social acceptability bias (wanting to give high ‘satisfaction ratings’), and patients may
also not fully understand and identify SDM when it occurs if they have not experienced it
previously.[21] However, the short three-item CollaboRATE measure (used in over 40 studies
worldwide) shows promise in addressing these issues.[22]
Page 4 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
V6.0 26.04.16
5
Tensions exist between desires for validated, reliable measures (measurement for research), and
measurement for quality improvement. Focusing on the latter helped embed SDM more readily with
some clinical teams. When measures directly informed practice and improved patient care, in real-time,
we witnessed greater motivation to improve and to sustain the improvement (e.g. Decision Quality
Measure in breast cancer, see Table 1).[23] Linking with local quality improvement expertise and
resources, where available, was valuable. For example, the 1000 Lives Plus national improvement
service for NHS Wales had supported QI skills development within the Cardiff site, which could be
utilised within the implementation of SDM.[24]
Key Challenge 5: “We have too many other demands and priorities”
Changing attitudes and behaviours involves effort at micro and macro levels. Clinical teams face many
competing demands and priorities, some of which are compulsory, some even incentivised (whether
financially or by targets). For example, there are tensions between the SDM approach and the Quality
and Outcomes Framework, where GPs are financially rewarded for behaviours that are evidence-based,
but not necessarily about what matters most to the patient. There are also increasing tensions between
SDM and clinical threshold guidelines or referral management schemes, which are widely applied
within commissioning in England. Similarly, for cancer treatment time targets current emphasis is on
time to treatment, but patients may prioritise time to make the decision.
Visible organisational buy-in and support are essential. This may be at Executive Board or middle
management level (or equivalent level in primary care). During the MAGIC programme, key
organisational leaders showed the clinicians that SDM was an important organisational priority to drive
improvement (see Table 1), and clinical leadership was key for driving implementation. SDM should be
framed as adaptation of existing clinical practice, not as a new and additional element of practice.
Framing interventions as healthcare organisation priorities that improve current practice, rather than
new additional tasks, also led to greater engagement. Clinicians then saw SDM as something the
organisation does, rather than another ‘initiative’ being ‘done to them’ and competing with other
demands. Teams sometimes needed support from the organisation to adapt clinical pathways to support
effective SDM; the SDM ‘tasks’ can also be distributed among different clinical team members e.g.
midwifes support decision making about mode of delivery, rather than a doctor. Many teams also have a
strong clinical identity, which can lead to insularity or, more positively, self-reliance. Shared learning
about ‘what works’ was essential and avoided ‘reinventing the wheel’.
Page 5 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
V6.0 26.04.16
6
A ‘shared decision making bundle’ – recommendations for implementation
We have discussed the key challenges faced during a SDM implementation programme in varied
clinical settings, across primary and secondary care, and in different healthcare organisations, including
commissioners in England. This summary is inevitably oversimplified, and cannot capture every
nuanced problem or barrier encountered during the programme. [14 25] We worked in complex settings,
with complex relationships (see Figure 3 for an outline of key factors influencing SDM
implementation).
We offer some solutions to these, from our experience. Many other factors also affect implementation
attempts, which are beyond the remit of a localised learning programme. In the real world, finance,
resources and time are all scarce. Although SDM is mentioned in key policy documents, such as the
NHS Constitution 2015 (see pages 4, 15),[26] it is not incentivised at national, regional or organisational
levels. These wider aspects need policy changes and the input of professional bodies. Furthermore, we
need to focus on cultural change among clinicians and patients, and this is a momentous challenge. A
receptive culture will only truly exist if clinicians view SDM as usual practice and as a fundamental
component of safe, effective and compassionate healthcare for patients, not as an optional style of
communication if we have time. It needs to be embedded in the medical and nursing curricula, and
inter-professional training programmes. Similarly, much health policy and professional practice has led
to feelings of powerlessness and passivity for many patients. Increasing patient agency and health
literacy is going to be equally important.[27]
Implementing SDM is challenging, but possible. It requires interventions targeted at organisations,
clinicians, and patients: a ‘shared decision making bundle’. No one intervention in isolation will succeed
alone. It requires the bundle of interventions working together at the different levels to achieve SDM
across the board.
Page 6 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
V6.0 26.04.16
7
Table 1 – Recommended solutions to key shared decision making implementation challenges*
Intervention /
approach
What it involved* What it helped with
Interactive
SDM skills
workshops
Two to three-hour session.
Based on SDM model for clinical practice.[5]
Interactive session using clinical scenarios and role play with actors or other
participants.
Focus on practical skills, less on theory of SDM.
When feasible, used existing training / meeting structures (e.g. MDT) and
processes (e.g. CPD); more likely to engage senior clinicians with this
approach.
Examples of the SDM skills workshops are available from -
http://personcentredcare.health.org.uk/resources/shared-decision-making-
skills-training-workshops
Challenging clinicians’ attitudes.
Differentiating SDM from current practice.
Developing shared understanding of the approach to decision
making.
Improving SDM micro-skills.
Overcoming the belief that SDM is only about tools.
Demonstrating the critical nature of understanding what is
important to the individual patient (values).
Development
of brief SDM
tools
Facilitating teams to identify key decision points suitable for SDM.
Mapping care pathways to agree on point of delivery.
Developing brief evidence-based in-consultation tools (1- 3 pages), e.g.
• Option Grids – available from The Option Grid Collaborative
website (http://optiongrid.org)
• Brief Decision Aids – available from the Patient website
(http://patient.info/decision-aids)
Developing tools that are locally relevant and fit with care pathway.
Patient representative involvement in design and user testing to refine tools.
Making reliable information available at the time of the
consultation for both patient and clinician.
Information sharing between clinician and patient about options.
Facilitating a SDM discussion between clinician and patient
(more than information transfer alone), by changing the dynamics
of the consultation.
Getting clinicians to support and engage with the SDM approach.
Increasing likelihood of implementation (when developed
locally).
Patient
activation &
preparation
Dedicated panel of patient and public representatives (general or clinical
team specific) to guide development and testing of interventions, and guide
implementation plans.
User panel helps to identify areas for improvement, identifying
user needs, and intervention design and testing.
Changing clinicians’ perceptions that patients do not want SDM.
Page 7 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
V6.0 26.04.16
8
Patient ‘activation’ – preparing patients to participate in SDM. This includes
raising awareness of the approach, explaining what it involves, and
providing tools/skills to help with engagement (e.g. ‘Ask 3 Questions’
campaign). A mix of elements e.g. posters and videos in waiting areas and
on web sites; flyers; launch event. Sent ahead of consultations with
appointment letter.
Examples of the Ask 3 Questions materials are available from:
http://personcentredcare.health.org.uk/resources/ask-3-questions-materials
Increasing patient awareness of SDM.
Promoting positive attitudes among patients about SDM
Preparing patients ahead of time to become more engaged in the
decision making process.
Measurement Measurement for improvement for driving change in clinical teams.
Clinically useful measures that have a direct impact on practice
e.g. Decision Quality Measure for breast cancer. Measures patients’ knowledge and
preferences. Breast care team use the tool to identify knowledge gaps and
demonstrate improvements in knowledge, and to elicit patients’ preferences (for
further discussion during SDM process).
Link to healthcare improvement programmes, when possible (expertise and
resources).
Utilise existing routine data collection systems, when available.
Engaging organisations and clinical teams.
Demonstrates improvement / change associated with SDM.
Belief that SDM is an organisational priority and a valued
activity.
Reminds clinical teams that they and the organisation is interested
in SDM.
Collaborative
& facilitated
approach
Dedicated clinical lead.
Regular contact.
Clinical team mapping care pathways and identifying areas for
improvement. Also assessing fit with current pathways and other objectives
/ priorities.
Regular shared learning opportunities (e.g. clinical lead meetings, learning
sets), including top-up learning sessions where clinicians could bring real
world challenges back to the SDM trainers.
Clinical leads help to drive the work forward in each clinical
team.
Understanding clinical teams’ priorities / demands and making
sure SDM fits in with these.
Getting clinicians to support and engage with the SDM approach.
Motivation to engage with and sustain implementation.
Organisation
buy-in / senior
level support
Visible organisational buy-in and executive / senior level support of SDM
For example
Getting clinicians to support and engage with the SDM approach.
Belief that SDM is an organisational priority and a valued
activity.
Page 8 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
V6.0 26.04.16
9
Walk-arounds (clinic visits) by Executive Board members
Internal Board reports identifying shared decision making as an
organisational priority
Grand Rounds presented by senior clinicians
Dedicated Executive Board member working with implementation team
“Board check list”
Framing interventions / approaches as healthcare organisations initiatives
(internally promoted).
Patients’ perceptions that the organisations and clinicians want
them to become more involved.
Structural
considerations
Supportive policy context i.e. making sure broader healthcare policies align
with the principle of SDM.
Encouragement and support from professional bodies of SDM approach.
Integration of patient-centred care / SDM into undergraduate medical /
nursing curriculum and continued inter-professional development.
Ensuring other systems / targets are compatible with SDM approach e.g.
Quality Outcomes Framework, criterion based systems of referral
management and guidance
Incentivisation at national, regional and organisational level.
Role of commissioning in England e.g. inclusion in CQUIN
Enabling clinicians and managers to see SDM as part of what
they already do – linking to other aspects of patient centred
practice.
Gradually moving SDM from ‘project’ to something that is part
of the organisation’s core function.
* A wide range of the MAGIC resources / interventions listed in this table can be found on The Health Foundation’s Person Centred Care Resource Centre:
http://personcentredcare.health.org.uk/ All materials are available open access.
Page 9 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
V6.0 26.04.16
10
Box 1 – A summary of the MAGIC programme commissioned by The Health Foundation
Cardiff
Sites
• Cardiff University (lead)
• Cardiff and Vale University Health Board
Clinical areas
• Four general practices
• Breast cancer (surgical options for early
stage breast cancer)
• Chronic kidney disease (treatment for end-
stage renal failure)
• Head and neck cancer (treatment options for
head and neck cancer)
• Paediatric ears, nose and throat (surgery for
recurrent tonsillitis)
Phase 1 (August 2010 – February 2012) Aim - design and test the best ways to implement SDM into routine clinical settings
Quality improvement methodology
Primary and secondary care settings
Multi-centre programme based in Cardiff and Newcastle (UK)
Newcastle
Sites
• Newcastle University (lead)
• The Newcastle upon Tyne Hospitals NHS
Foundation Trust
• Northumbria Healthcare NHS Foundation Trust
Clinical areas
• Four general practices
• Breast cancer (surgical options for early stage
breast cancer)
• Maternity (options relating to mode of delivery
after caesarean, place of birth, and screening for
Down’s syndrome)
• Urology (treatment options for prostate cancer)
Phase 2 (February 2012 – October 2013)
Aim – demonstrate that SDM can become part of routine clinical care (wider dissemination,
implementation and sustainability) and build practical and transferable knowledge about the conditions for
success.
Cardiff
Summary
• Work with up to 10 clinical teams
across the Cardiff & Vale University
Health Board to involve more patients
in shared decision making (spread from
Phase 1)
• Underpinned by a nine-step consultancy
model and the Model for
Improvement[1]: moving from
expression of interest, establishing team
readiness and priorities, action planning,
to implementation & sustainability
• Teams had access to support and
interventions/ approaches developed
during Phase 1: SDM skills, decision
support tools, patient participation,
quality improvement support
Newcastle
Summary
• Provide tools, materials and resources to enable
clinical implementation teams from MAGIC 1 to
continue their plans for sustainable change
• Engage with four new clinical teams (two each
from primary and secondary care)
• Engage with third sector organisations, providing
versions of skills training workshops to service
users and advocates
• Work closely with organisational strategic groups
and with emerging commissioning organisations
• Continue to support clinical teams that are not
part of the MAGIC programme per se, both those
who have already expressed an interest and begun
implementation of SDM and new teams that make
an approach
• Further develop a range of tools, materials and
processes to facilitate spread of SDM and to
demonstrate sustainable change.
Page 10 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
V6.0 26.04.16
11
Figure 1 – Shared Decision Making Model for Clinical Practice (from Elwyn et al 2012)[5]
Choice
Talk
Option
Talk
Decision
Talk
Decision support
Brief or extended
Initial preferences Informed preferences
Decision
D E L I B E R A T I O N
Page 11 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
V6.0 26.04.16
12
Figure 2 – Examples of the ‘Ask 3 Questions’ campaign posters used in MAGIC
a) Cardiff general patient poster b) Newcastle children’s services poster
Page 12 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review Only
V6.0 26.04.16
13
Figure 3 – Summary of key factors influencing SDM implementation
Page 13 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
V6.0 26.04.16
14
Contributors and sources:
This paper originated from the learning from the Making Good Decisions in Collaboration (MAGIC)
Programme, funded by The Health Foundation. NJW drafted the manuscript, and all authors worked collaboratively to contribute to the content, edit, and agree the final version. All authors were involved
in the MAGIC programme and contributed to the learning that is described throughout this manuscript.
NJW is a Research Fellow conducting patient centred care implementation research at the Division of
Population Medicine, Cardiff University. NJW was the Cardiff-based Programme Manager for MAGIC.
AL is a Research Fellow working on the design and implementation of interventions to improve clinical
practice. AL was the Cardiff-based SDM facilitator for MAGIC. AE is Professor of General Practice at
the Division of Population Medicine, Cardiff University, with research and teaching interests in
healthcare communication and quality improvement. LS is a Senior Research Associate and was the
Newcastle-based SDM facilitator for MAGIC. DT is a full time GP with long term interest in patient centred practice and training. He took a lead on the training programme in MAGIC. CD is an NHS
manager with broad experience in quality improvement implementation programmes. CD was the
Newcastle-based Programme Manager for MAGIC. SM was a Consultant Obstetrician and Fetal Medicine Specialist who facilitated the project with the Newcastle Upon Tynes Hospitals NHS
Foundation Trust, and took a lead in developing the training tools and delivering training to clinical
teams in secondary care. KB was PI in Cardiff for Phase 2 of MAGIC, and is a registered health psychologist with expertise in psychological aspects of cancer early diagnosis, prevention and
screening. GE was PI in Cardiff for Phase 1 of MAGIC and co-led the development of the programme.
GE oversaw implementation of SDM in Cardiff during Phase 1. RT was PI in Newcastle for Phases 1
and 2 of MAGIC, and co-led the development of the programme, and oversaw implementation in
Newcastle during Phases 1 and 2.
Competing Interests:
We have read and understood the BMJ Group policy on declaration of interests and declare that we have no competing interests.
Exclusive Licence:
The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all
authors, a worldwide licence to the Publishers and its licensees in perpetuity, in all forms, formats and
media (whether known now or created in the future), to i) publish, reproduce, distribute, display and
store the Contribution, ii) translate the Contribution into other languages, create adaptations, reprints,
include within collections and create summaries, extracts and/or, abstracts of the Contribution and
convert or allow conversion into any format including without limitation audio, iii) create any other
derivative work(s) based in whole or part on the on the Contribution, iv) to exploit all subsidiary rights
to exploit all subsidiary rights that currently exist or as may exist in the future in the Contribution, v) the
inclusion of electronic links from the Contribution to third party material where-ever it may be located;
Key Messages
• Skills trump tools, but attitudes trump skills - shared decision making is
about more than tools
• Preparation before enablement, in a supportive clinical team - successful implementation relies on a combination of interventions targeted at the
organisation, clinician, and patient level
• Organisational support and local ownership are vital for engagement
Page 14 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
V6.0 26.04.16
15
and, vi) licence any third party to do any or all of the above. All research articles will be made available
on an Open Access basis (with authors being asked to pay an open access fee). The terms of such Open
Access shall be governed by a Creative Commons licence—details as to which Creative Commons
licence will apply to the research article are set out in our worldwide licence referred to above.
Acknowledgements:
This paper originated from the MAGIC programme, funded by The Health Foundation. This programme involved collaboration between the following organisations: Cardiff and Vale University Health Board,
Cardiff University, the Newcastle upon Tyne Hospitals NHS Foundation Trust, and Newcastle
University. We are grateful to all of the MAGIC contributors, including the organisational
representatives, clinical teams, and patients for their contribution to the learning.
Page 15 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
V6.0 26.04.16
16
References
1. The Health Foundation. Implementing shared decision making: clinical teams' experiences of
implementing shared decision making as part of he MAGIC programme. London: The Health
Foundation, 2013
2. The Health Foundation. The MAGIC programme: Evaluation. London: The Health Foundation, 2013.
3. Lloyd A, Joseph-Williams N, Edwards A, Rix A, Elwyn G. Patchy 'coherence': using
normalization process theory to evaluate a multi-faceted shared decision making
implementation program (MAGIC). Implement Sci 2013;8(1):102
4. May C, Finch T. Implementing, embedding, and integrating practices: an outline of
Normalization Process Theory. Sociology 2009;43: 535-554
5. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice.
Journal of general internal medicine 2012;27(10):1361-7
6. Elwyn G, Tsulukidze M, Edwards A, Legare F, Newcombe R. Using a 'talk' model of shared decision making to propose an observation-based measure: Observer OPTION 5 Item. Patient
Educ Couns 2013;93(2):265-71
7. The Option Grid Collaborative. Option Grid. 2016. http://optiongrid.org/ 8. Elwyn G, Lloyd A, Joseph-Williams N, et al. Option Grids: Shared decision making made
easier. Patient Educ Couns 2012;90(2):207-12
9. Elwyn G, Pickles T, Edwards A, et al. Supporting shared decision making using an Option Grid
for osteoarthritis of the knee in an interface musculoskeletal clinic: A stepped wedge trial.
Patient Educ Couns 2016;99(4):571-7
10. Fay M, Grande SW, Donnelly K, Elwyn G. Using Option Grids: steps toward shared decision-
making for neonatal circumcision. Patient Educ Couns 2016;99(2):236-42
11. Patient. What are decision aids? (includes an online database of decision aids). 2016.
http://patient.info/decision-aids. 12. Hargraves I, Montori VM. Decision aids, empowerment, and shared decision making. BMJ
2014;349:g5811
13. Joseph-Williams N, Edwards A, Elwyn G. Power imbalance prevents shared decision making. BMJ 2014;348 g3178
14. Joseph-Williams N, Elwyn G, Edwards A. Knowledge is not power for patients: a systematic
review and thematic synthesis of patient-reported barriers and facilitators to shared decision making. Patient Educ Couns 2014;94(3):291-309
15. Frosch DL, Singer KJ, Timmermans S. Conducting implementation research in community-
based primary care: a qualitative study on integrating patient decision support interventions for
cancer screening into routine practice. Health Expect 2011;14 Suppl 1:73-84
16. Say R, Murtagh M, Thomson R. Patients' preference for involvement in medical decision
making: a narrative review. Patient Educ Couns 2006;60(2):102-14
17. Lifford KJ, Witt J, Burton M, et al. Understanding older women's decision making and coping
in the context of breast cancer treatment. BMC Med Inform Decis Mak 2015;15:45
18. Can consumers learn to ask three questions to improve shared decision-making?: A feasibility
study of the ASK (AskShareKnow) patient-clinician communication model interventionin a
primary health care setting International Shared Decision Making Conference: Pacientes @ the
Centre of Healthcare; 2013; Lima, Peru.
19. Shepherd HL, Barratt A, Trevena LJ, et al. Three questions that patients can ask to improve the
quality of information physicians give about treatment options: a cross-over trial. Patient Educ
Couns 2011;84(3):379-85
20. The Health Foundation. Person-centred care resource centre. 2016. http://personcentredcare.health.org.uk/.
21. Barr PJ, Elwyn G. Measurement challenges in shared decision making: putting the 'patient' in
patient-reported measures. Health Expect 2015; doi: 10.1111/hex.12380. [Epub ahead of print]
Page 16 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
V6.0 26.04.16
17
22. Barr PJ, Thompson R, Walsh T, Grande SW, Ozanne EM, Elwyn G. The psychometric
properties of CollaboRATE: a fast and frugal patient-reported measure of the shared decision-
making process. J Med Internet Res 2014;16(1):e2
23. Mcgarrigle H, Lloyd A, Joseph-Williams N, Elwyn G. Making Good Decisions in Collaboration
with patients with breast cancer: the role of Decision Quality Measures and in-consultation decision support tools. European Journal of Surgical Oncology 2012;38(5):441
24. 1000 Lives Plus National Improvement Programme. 2016.
http://www.1000livesplus.wales.nhs.uk/home. 25. Legare F, Ratte S, Gravel K, Graham ID. Barriers and facilitators to implementing shared
decision-making in clinical practice: update of a systematic review of health professionals'
perceptions. Patient Educ Couns 2008;73(3):526-35
26. Department of Health. The NHS Constitution. London: Department of Health, 2009.
27. Hernandez LM. Measures of Health Literacy: Workshop Summary. Roundtable on health
Literacy. National Academy of Sciences, 2009.
Page 17 of 17
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960