complications - integris health | integris
TRANSCRIPT

COMPLICATIONS Kacy Aderhold, MSN, APRN-CNS, CMSRN

ACUTE COMPLICATIONS
Hyperglycemia
Hypoglycemia
DKA
HHS

HYPERGLYCEMIA
Signs/Symptoms are caused by high glucose levels
and the body’s effort to get rid of the extra sugar:
• Higher BS than usual
• Increased urine output
• Increased thirst
• Increased hunger
• Dry skin and mouth
• Dehydration
• Fatigue
• Blurred vision
HYPERGLYCEMIA TREATMENT
Lifestyle Interventions
Insulin
Oral Agents
PATIENT EDUCATION

HYPOGLYCEMIA
Blood glucose < 70
Severe hypoglycemia < 40
Early recognition and treatment of hypoglycemia
can prevent deterioration to a more severe
episode with potential adverse outcomes!
(ADA, 2015)

HYPOGLYCEMIA SIGNS & SYMPTOMS
Adrenergic • Pallor
• Diaphoresis
• Tachycardia
• Shakiness
• Hunger
• Anxiety
• Irritability
• Headache
• Dizziness
Neuroglycopenic
• Confusion
• Slurred Speech
• Irrational behavior
• Extreme fatigue
• Disorientation
• Loss of consciousness
• Seizures
• Pupillary sluggishness
• Decreased response


RISK FACTORS FOR HYPOGLYCEMIA
Altered nutritional state
Heart failure, renal, or
liver disease
Malignancy
Infection
Sepsis
Sudden reduction in
corticosteroid dose
Altered ability of patient
to report symptoms
Reduction in oral intake
New NPO status
Inappropriate timing of
short- or rapid-acting
insulin
Reduction of IV
dextrose
Unexpected
interruption of TPN/TF

DR. PHIL CRYER’S THERMOMETER

HYPOGLYCEMIA MANAGEMENT STANDING ORDERS
Patient able to swallow safely and not NPO:
15/15 Rule!
Patient unable to swallow safely and/or NPO:
(100 – FSBS) x 0.3 = # mL of D50 IV
No IV Access:
Glucagon 1mg IM or Subcut

HYPOGLYCEMIA MANAGEMENT STANDING ORDERS
Examples of 15 grams of carbs:
• 4 oz. juice or regular pop
• 8 oz. milk (skim preferred)
• 4 pkgs sugar mixed with
water (good for fluid or
potassium restriction)
• REMEMBER: You must
recheck a FSBS 15
minutes after each
reading below 70mg/dL.
• Notify physician before the
next insulin dose or oral
anti-diabetic medication
dose if FSBS less than 70
• Don’t forget to Document!
If FSBS < 70 mg/dL, give 15 grams of carbs, wait 15 minutes and recheck
FSBS; Repeat if necessary until FSBS is > 70mg/dL
15/15 RULE FOR HYPOGLYCEMIA

HYPOGLYCEMIA MANAGEMENT STANDING ORDERS
If patient is hypoglycemic &
unable to swallow safely or NPO:
(100 – FSBS) x 0.3 = # mL of D50 IV
How much D50 would you give to a
patient with a blood glucose of 59?
12 mL of D50 IV

HYPOGLYCEMIA MANAGEMENT STANDING ORDERS
If patient is hypoglycemic and has no IV access:
Glucagon 1mg IM or Subcut

HOW DID THEY DO ON THEIR DOCUMENTATION?

DIABETIC KETOACIDOSIS (DKA) &
HYPEROSMOLAR HYPERGLYCEMIC STATE (HHS)
DKA & HHS are the most serious complications seen with hyperglycemia (Kaplow & Hardin, 2007)
Preventable complications
Similar presentation
Different time of onset, degree of dehydration, & severity of ketosis
DKA & HHS were the first listed diagnosis in 175,000 ED visits in 2011 (CDC, 2014)
In 2010, hyperglycemic crises caused 2,361 deaths in adults aged 20 years or older

DIABETIC KETOACIDOSIS
(Kitabchi & Razavi, 2009)
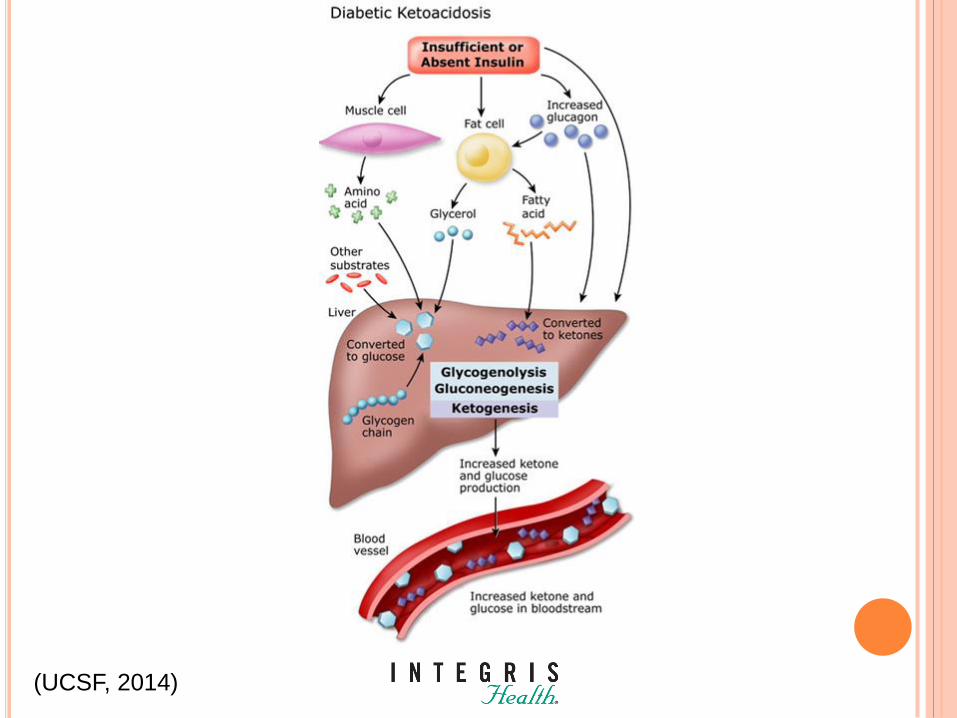
(UCSF, 2014)

DIABETIC KETOACIDOSIS
Most common in patients with Type 1 Diabetes
Patients with Type 2 Diabetes are at risk during
catabolic stress
Responsible for >500,000 hospital days/year
Estimated annual expense of $2.4 billion
Mortality in adult patients is <1%
Mortality is >5% in elderly patients & patients
with severe comorbidities
Mortality r/t underlying precipitating illness
(ADA, 2009)

DKA PRECIPITATING FACTORS
Infection
Discontinuation of or inadequate insulin therapy
Acute illness
Pancreatitis
MI
CVA
Alcohol or drug intoxication
Undiagnosed Type 1 Diabetes
(Kaplow & Hardin, 2007)
SYMPTOMS OF DKA
Polyuria
Excessive thirst
Weakness, fatigue
Nausea, vomiting
Stomach pain
Heavy, deep breathing
Fruity breath – the smell of ketoacids
Speech problems, confusion or unconsciousness
(Kaplow & Hardin, 2007)

HYPEROSMOLAR HYPERGLYCEMIC STATE
Severe hyperglycemia
Dehydration
Hyperosmolality
Absence of significance of ketoacidosis
(Kaplow & Hardin, 2007)

HYPEROSMOLAR HYPERGLYCEMIC STATE
Also known as Hyperosmolar Hyperglycemic
Non-Ketotic Syndrome (HHNS)
Most commonly in older adults with Type 2
Diabetes (Kaplow & Hardin, 2007)
Mortality 5-20% (ADA, 2009)

HHS PRECIPITATING FACTORS
Infection
Discontinuation of or
inadequate insulin therapy
Endocrine Disorders
Acromegaly
Thyrotoxicosis
Cushing’s Syndrome
Drugs
Undiagnosed Diabetes
Acute Illness
CVA
MI
Pancreatitis
PE
Intestinal obstruction
PD
Acute Renal Failure
Severe Burns
Subdural hematoma
Mesenteric thrombosis
Heat Stroke
Hypothermia
(Up To Date, 2014)
SYMPTOMS OF HHS
Polyuria
Polydipsia
Weight Loss
Neurological Symptoms
Focal neurologic signs (hemiparesis or hemianopsia)
Seizures
Mental obtundation
Coma
(ADA, 2009)

PATHOGENESIS OF DKA AND HHS
(ADA, 2009)

DIAGNOSTIC CRITERIA
BMP
Plasma glucose
BUN
Creatinine
Electrolytes
Anion Gap
Osmolality
Serum ketones
ABGs
CBC with differential
EKG
CXR
UA & Culture, urinary ketones
Sputum Culture
Blood Cultures
(ADA, 2009)

DKA & HHS DIFFERENTIAL DIAGNOSIS
(ADA, 2009)
DKA HHS
Mild (plasma
glucose
>250mg/dl)
Moderate
(plasma glucose
>250 mg/dl)
Severe (plasma
glucose
>250mg/dl)
Plasma Glucose
>600mg/dl
Arterial pH 7.25-7.30 7.00 to <7.24 <7.00 >7.30
Serum
Bicarbonate
15-18 10 to <15 <10 >18
Urine Ketone Positive Positive Positive Small
Serum Ketone Positive Positive Positive Small
Effective
Serum
Osmolality
Variable Variable Variable >320 mOsm/kg
Anion Gap >10 >12 >12 Variable
Mental Status Alert Alert/Drowsy Stupor/Coma Stupor/Coma

DKA MAIN TREATMENT PRINCIPLES
Continuous insulin & fluid replacement until
ketosis has resolved
Insulin Infusion MUST continue along with sufficient
glucose intake to prevent hypoglycemia
DO NOT stop insulin infusion until ketoacidosis and
dehydration resolve, patient is eating, and
intermediate or long acting insulin is administered
Identify precipitating factors & treat concurrent
illness as indicated.

TREATMENT OF DKA
Restore fluid volume
Initial NS bolus, then maintenance at 250mL/hr
When FSBS < 175mg/dL, add 5% dextrose
D51/2NS20K 150/hr if K+ <5 and urine output is > 0.5mL/kg/hr
D51/2NS 150/hr if K+ >5 or urine output is < 0.5mL/kg/hr
Subsequent fluids depend on hemodynamics, hydration status, electrolyte levels and urine output
Correct hyperglycemia
Initial IV bolus 10 units regular insulin
Continuous IV insulin infusion with regular insulin per protocol

TREATMENT OF DKA (CONT.)
Potassium
Insulin therapy, correction of acidosis, and
volume expansion decrease serum K+
If K+ < 5 and urine output < 0.5 mL/kg/hr,
potassium is added to maintenance fluid
Frequent patient monitoring
Electrolytes, BUN, venous pH, creatinine, urinary
output & blood glucose
(ADA, 2009)

CRITERIA FOR DKA RESOLUTION
Initiate Hyperglycemia Management Protocol when:
CO2 > 16
Anion gap < 16
Patient is ready to eat solid food
Fluid deficit is corrected
(ADA, 2009)

CASE STUDY
A 45 y/o male presents to the ER with s/s of DKA.
Patient has T1DM x 10 yrs. Patient’s labs and
assessment reveal moderate DKA and a critical
K+ of 6.0. The patient is treated with Kayexalate
to correct K+. The patient is started on fluids and
then an insulin infusion. Patient is admitted to
the ICU. 4 hours later the patient’s insulin
infusion is up to 28 units/hr. K+ is now 1.9 and
FSBS is 45.

Provider who will manage DM after discharge
Assess need for HH or outpatient DM education
Diagnosis
SMBG & home goals
Information on consistent eating patterns
When & how to take BG lowering medications
Sick day management
Proper use & disposal of needles & syringes
SURVIVAL SKILLS DISCHARGE EDUCATION
(ADA, 2015)

SICK DAY MANAGEMENT EDUCATION
Early contact with healthcare provider
Importance of insulin during illness and the
reasons never to discontinue without contacting
the healthcare team
Review of blood glucose goals and the use of
supplemental short or rapid-acting insulin
Having medications available at home to
suppress fever and treat infection
Initiation of an easily digestible diet containing
carbs and salt if nauseated
(ADA, 2015)
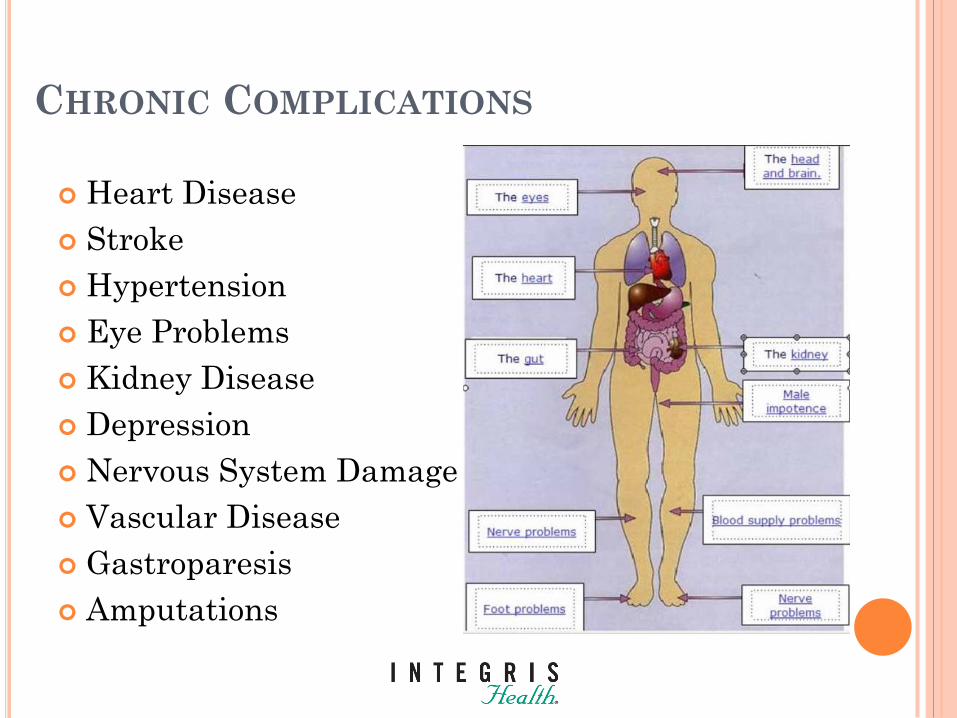
CHRONIC COMPLICATIONS
Heart Disease
Stroke
Hypertension
Eye Problems
Kidney Disease
Depression
Nervous System Damage
Vascular Disease
Gastroparesis
Amputations

CHRONIC COMPLICATIONS
In 2008, 23.6 million Americans had diabetes
In 2012, 29.1 million Americans have diabetes
“The rise in diabetes prevalence data results from
both the fact that more people are developing the
disease and the fact that people are living longer
with it, thanks to better management of
cardiovascular risk factors and fewer complications
such as renal failure and amputations.” (Tucker,
2011)

COST OF DIABETES
Estimated total national cost of diagnosed
diabetes is $245 billion.
$69 billion in indirect costs (disability, work
loss, premature mortality)
Average medical expenditure among people with
diabetes is 2.3 times higher than those without
One in five health care dollars is spent caring
for people with diabetes.
(CDC, 2014)
MACROVASCULAR COMPLICATIONS
MI, CVA, CAD, PAD
2 out of 3 people with diabetes die from heart
disease or stroke
Atherosclerosis process:
Accounts for ~80% of all diabetes-related mortality
Occurs at earlier age, advances more rapidly
DM alone accelerates the development of
atherosclerosis 200-400%

CEREBROVASCULAR DISEASE
Cerebral vascular disease mortality is 3-5
times higher in patients with DM

CARDIOVASCULAR DISEASE (CVD)
Every 1% increase in A1c increases CVD by 14%
MI is the #1 cause of death for people with DM
Patients with DM have a 30% higher risk for CVD
CVD death rates are 1.7 X higher among adults with DM
1.8 X higher MI hospitalization rates for patients with DM
1.5 X higher hospitalization rates for adult patients with DM
20-50% of patients with DM have asymptomatic, silent
ischemia

HYPERTENSION
• 71% of adults with diabetes aged 18 years or
older have a blood pressure > 140/90 (CDC, 2014)
• ADA Standards of Medical Care recommend
treating patients to a goal of <140/90 mmHg (ADA, 2015)
• Lower targets (such as <130/<80 mmHg) may be
appropriate for certain individuals, such as
younger patients (ADA, 2015).

PERIPHERAL ARTERY DISEASE (PAD)
• Blood vessels in feet and legs are narrowed or
blocked by fatty deposits.
• Blood circulation decreases, leading to slow healing
of wounds.
• PVD & neuropathy account for 50% of all non-
traumatic lower extremity amputations

MICROVASCULAR COMPLICATIONS
Retinopathy
Nephropathy
Neuropathy
Intensive insulin therapy improves the outcome
of microvascular disease!

DIABETIC RETINOPATHY
Diabetes is the leading cause of new cases of blindness
among adults in the U.S.
Small blood vessels in retina are damaged
Glaucoma and cataracts occur more frequently in
patients with DM
No early warning symptoms
(CDC, 2014)
DIABETIC RETINOPATHY PREVENTION
Blood pressure control
Blood glucose control
Lipid control
Early detection-
annual dilated eye
exam

KIDNEY DISEASE
DM is the leading cause of kidney failure.
49,677 people began tx for kidney failure due to DM in 2011
228,924 people with kidney failure due to DM were living on
chronic dialysis or with a kidney transplant in 2011.
Small blood vessels in the nephrons of kidneys are damaged
Hypertension accelerates progression of nephropathy
No early warning signs or symptoms
(CDC, 2011)

NERVOUS SYSTEM DAMAGE
60-70% of people with
diabetes have mild to
severe forms of
nervous system
damage.
Nerve damage can
result in pain in feet
or hands, slowed
digestion, sexual
dysfunction or other
nerve problems.
(CDC, 2011)

PERIPHERAL NEUROPATHY
Most common long-term complication of diabetes
Progressive microvascular damage
Described as numb, tingling, pins and needles, dead,
shooting, stabbing, knife-like, gnawing, electrical,
burning, hypersensitive
Damage is distal & symmetrical, feet affected 1st
Treatment:
The first step is stabilization of blood glucose
Anticonvulsants, SNRIs, Tricyclic antidepressants

AMPUTATIONS
Amputation rates 10X higher in patients with DM
In 2010, 73,000 non-traumatic lower-limb amputations
were performed in adults with DM
Increased rates in men, African Americans, Hispanics,
American Indians
Risk factors for patients with DM:
Loss of protective sensation related to neuropathy
Decreased circulation related to PVD & PAD
Impaired vision may cause patient to not notice wound
Increased risk for infection
Decreased wound healing
(CDC, 2011)

FOOT PROBLEMS
• Diabetes
increases risks
for foot problems
Foot Care Video
(Illumistream, 2007)
FOOT CARE Wash your feet daily with soap and warm water.
Dry your feet gently with soft towel.
If your skin is dry, apply lotion (but not between toes).
Examine tops, bottoms, and sides of feet and between toes. Use a mirror to
help see the bottoms and sides of feet. Or get help from a family member.
Check for sores, cuts, bruises, rashes, blisters, red spots, swelling, and
ingrown toenails.
Use your hands to feel for hot or cold spots, bumps, or dry skin.
If you have a foot injury, call your healthcare provider. Do not try to take care
of foot injuries yourself. Some over-the-counter foot remedies can harm your
skin, making injuries worse.
Trim your toenails straight across and file the edges. Rounded edges help
prevent ingrown toenails.
Choose socks that will not irritate your feet, such as seamless socks or those
with flat or soft seams.
Before you put on shoes, feel inside them to make sure there are no pebbles
or rough edges that might injure your feet. You may not be able to count on
the nerves in your feet to feel something wrong with your shoes or socks.
Protect your feet all the time by wearing shoes or slippers, even around the
house, pool, or beach.
(Illumistream, 2007)

GASTROPARESIS
Symptoms:
Frequent nausea
Vomiting undigested meals
Early satiety
Bloating
Erratic blood glucoses
Treatment:
Low fat, low fiber diet
Multiple, small meals- mostly liquid
metoclopramide, domperidone
Gastric pacemaker
Hemigastrectomy
Jejunostomy

DEPRESSION
People with diabetes are twice as likely to have
depression
Depression is associated with a 60% increased
risk of developing type 2 diabetes
(CDC, 2011)

Measure ADA Standard Goal
A1c <7%
Blood Pressure <140/90, lower targets may be
appropriate for some
Dilated Eye Exam At least once a year
Foot Exam Check feet every day
Foot exam with monofilament annually
Smoking STOP!!!
LDL (mg/dL) <100 mg/dL if no known CVD
<70 mg/dL if known CVD
Triglycerides (mg/dL) <150 mg/dL
HDL (mg/dL) >40 mg/dL in men
>50 mg/dL in women
GOALS TO PREVENT COMPLICATIONS

REFERENCES American Diabetes Association (2015). Standards of Care. Diabetes Care 38 (1), S1-
S99.
American Diabetes Association. (2009). Hyperglycemic crises in adult patients with
diabetes (consensus statement). Diabetes Care 32(7), 1335-1343.
Centers for Disease Control (2011) National Diabetes Fact Sheet, 2011. National
Center for Chronic Disease Prevention and Health Promotion.
http://www.cdc.gov/diabetes/pubs/factsheet11.htm
Illumistream (2007). Diabetes Foot Care for Diabetes #2. Clip Syndicate. Retrieved
on March 11, 2014 from
http://www.clipsyndicate.com/video/playlist/8317/409571?title=illumistream_at_clips
yndicate
Diabetes Education Online (2014). Diabetic ketoacidosis. Diabetes Teaching Center at
the University of California, San Francisco. Retrieved on February 25, 2014 from
http://dtc.ucsf.edu/living-with-diabetes/complications/diabetic-ketoacidosis/
Kaplow, R. & Hardin, S. (2007). Critical Care Nursing: Synergy for Optimal
Outcomes. MA: Jones & Bartlett.
Kitabchi, A.E. (2014). Clinical features and diagnosis of diabetic ketoacidosis and
hyperosmolar hyperglycemic state in adults. Up To Date. Retrieved on February 25,
2014 from http://www.uptodate.com/contents/clinical-features-and-diagnosis-of-
diabetic-ketoacidosis-and-hyperosmolar-hyperglycemic-state-in-adults
Tucker, M. (2011). Diabetes prevalence keeps climbing in the U.S. Clinical
Endocrinology News, 6 (2), 1.