comparison of a waxy maize and a potato starch-based balanced hydroxyethyl starch for priming in...
TRANSCRIPT

Starch for Priming in Patients Underg
Comparison of a Waxy Maize and a Potato Starch-Based Balanced Hydroxyethyloing Coronary Artery Bypass Grafting
Brijindera Singh Sethi, MD,* Sandeep Chauhan, MD,* Akshay Kumar Bisoi, MCh,† Poonam
Malhotra Kapoor, MD,* Usha Kiran, MD,* and Randhir Singh Rajput, MD*
Objective: Concerns have been raised about differences in
the safety profile of potato- versus waxy maize-derived
hydroxyethyl starch (HES). The objective of this study was
to compare 2 HES solutions derived from 2 different source
materials (potato versus waxy maize) for their dose-related
effects on hemostasis and organ function when used to
prime the cardiopulmonary bypass circuit (CPB).
Design: A prospective, randomized, controlled study.
Setting: Tertiary care center.
Participants: Eighty patients undergoing coronary artery
bypass grafting (CABG) on CPB.
Interventions: For priming the CPB circuit, the HESPRL
group received 1000 mL of potato-derived balanced 6% HES
130/0.42 along with 500 mL of Ringer’s lactate; the HESP
group received 1,500 mL of potato-derived balanced 6% HES
130/0.42; the HESMRL group received 1000 mL of waxy
maize-derived balanced 6% HES 130/0.4 along with 500 mL
of Ringer’s lactate, and the HESM group received 1500 mL of
waxy maize-derived balanced 6% HES 130/0.4.
Measurements and Main Results: There were no signifi-
cant differences in 24-hour mediastinal drainage, rate of re-
exploration, blood product usage, coagulation parameters,
Journal of Cardiothoracic and Vascular Anesthesia, Vol ], No ] (Month), 2
and measures of pulmonary, renal, and hepatic function
with respect to plant source of HES, when equivalent doses
were used. Sonoclot activated clotting time (SonACT) was
significantly higher and clot rate (CR) significantly lower at
end of surgery (T1) and 24 hours after surgery (T2) in the
HESP and HESM groups compared with the HESPRL and
HESMRL groups. Compared with baseline, CR and platelet
function were significantly lower at T1, PaO2/FIO2 ratio
decreased significantly at T1 and T2, and serum bilirubin
and transaminases increased significantly at T2 in all 4
groups.
Conclusions: There was no significant difference in cumu-
lative 24-hour mediastinal drainage when potato-derived
balanced 6% HES 130/0.42 or waxy maize-derived balanced
6% HES 130/0.4 was used to prime the CPB circuit in
patients undergoing CABG. In equal doses, both starches
exerted the same effect on blood coagulation and pulmo-
nary, renal, and hepatic function.
& 2013 Elsevier Inc. All rights reserved.
KEY WORDS: cardiopulmonary bypass, coagulation,hemodilution, hydroxyethyl starch, priming, outcome
From the *Department of Cardiac Anaesthesia; and †Department ofCardiothoracic and Vascular Surgery, All India Institute of MedicalSciences, Ansari Nagar, New Delhi, India.
Address reprint requests to Brijindera Singh Sethi, MD, Departmentof Cardiac Anaesthesia, All India Institute of Medical Sciences, AnsariNagar, New Delhi 110029 India. E-mail: [email protected]© 2013 Elsevier Inc. All rights reserved.1053-0770/2605-0031$36.00/0http://dx.doi.org/10.1053/j.jvca.2013.06.020
THE EVOLUTION OF CARDIOPULMONARY BYPASS(CPB) circuit priming solutions from fresh whole blood to
present-day asanguineous crystalloid or colloid solutions hasbeen riddled with controversy.1 The effects of CPB primingsolution on coagulation system and organ function are of vitalimportance in influencing postoperative outcomes after cardiacsurgery.2–4
The availability of a third-generation, balanced, low-molec-ular-weight, low molar substitution, rapidly degradable hydrox-yethyl starch (HES) preparation for priming has added a colloidversus colloid debate to the ongoing crystalloid versus colloiddebate.
The need to improve safety and pharmacologic propertieswhile maintaining the volume expansion characteristics hasled to the development of 2 new-generation HES solutionsoriginating from 2 different plant sources. A waxy maize-derived balanced 6% HES (130/0.4/9:1) and a potato-derivedbalanced 6% HES (130/0.42/6:1) have been developed recentlyand are used for volume expansion and for priming the CPBcircuit.5,6
The waxy maize- and potato starch-derived HES solutionsdiffer in their finer chemical structure, area under the plasmaconcentration curve, and apparent plasma clearance.7,8 The useof waxy maize starch is supported by a large evidence base;however, information supporting the use of potato-derived HESis limited.9 Extrapolation of clinical data obtained from studiescomparing one type of HES to the other would be highlyinappropriate.
Concerns have been raised about the differences in thesafety profile of potato-derived 6% HES 130/0.42 and waxymaize-derived 6% HES 130/0.4 with regard to blood coagu-lation10, renal dysfunction,11 and hepatic dysfunction.12 There
is a lack of clinical studies comparing the safety profile of the 2HES solutions from different plant origin when used as primingsolution for cardiac surgery on CPB. A recent editorial in aleading journal also lamented the lack of studies investigatingwhether the difference in molecular structure between potato-and maize-derived starch translates into differences in drugsafety when these colloids are used in perioperative medicine.13
In this randomized prospective study, the authors aimed totest the hypothesis that, in patients undergoing coronary arterybypass grafting (CABG), priming the CPB circuit with waxymaize-derived balanced 6% HES 130/0.4 resulted in lesspostoperative blood loss in comparison with potato-derivedbalanced 6% HES 130/0.42. The effects on blood coagulationand renal, hepatic, and pulmonary function were compared, andthe impact of 2 different doses of the study solutions wasexamined.
METHODS
After approval from the institute ethics committee and writteninformed consent from the patients, 80 consecutive patients undergoingelective CABG on CPB were recruited. Exclusion criteria were a
013: pp ]]]–]]] 1

SETHI ET AL2
history of previous cardiac surgery, severe congestive cardiac failure(ejection fraction o25%), known coagulation disorders, renal failure(serum creatinine 42 mg/dL, oliguria or anuria requiring dialysis),liver insufficiency (aspartate aminotransferase 440 U/L, alanine ami-notransferase 440 U/L), known hypersensitivity to HES, and intra-cranial bleeding.
A computerized randomization table was used to assign patients to1 of the 4 groups (n ¼ 20 in each group). The total prime volume was1,500 mL in all the groups. The HESPRL group received 1,000 mL ofpotato-derived balanced 6% HES 130/0.42 (Tetraspan; B Braun,Melsungen, Germany) along with 500 mL of Ringer’s lactate as CPBprime. The HESP group received 1,500 mL of potato-derived balanced6% HES 130/0.42 (Tetraspan) as CPB prime. The HESMRL groupreceived 1,000 mL of waxy maize-derived balanced 6% HES 130/0.4(Volulyte; Fresenius Kabi, Bad Homburg, Germany) along with500 mL of Ringer’s lactate as CPB prime. The HESM group received1,500 mL of waxy maize-derived balanced 6% HES 130/0.4 (Volulyte)as CPB prime.
The priming solutions were prepared by a perfusionist who was notinvolved in the study, and the anesthesiologist was not aware of therandomization results. Anesthetic and surgical management werestandardized in all groups. All the operations were performed by thesame surgical team to eliminate the variations in CPB time and surgicaltechnique as a cause of increased blood loss.
Anesthesia was induced with midazolam (0.05 mg/kg), thiopentone(4-5 mg/kg), fentanyl (3-5 mg/kg), and rocuronium (1 mg/kg) andmaintained with isoflurane in an air–oxygen mixture and intermittentdoses of midazolam, fentanyl, and vecuronium. All patients receivedRinger’s lactate solution via a peripheral line for maintenance andintraoperative volume replacement throughout the surgery. Mannitol20% (100 mL) and heparin (5,000 IU) were added to the CPB prime inall 4 groups. Antifibrinolytics were not administered in any of thepatients. Before establishing CPB, intravenous heparin (400 IU/Kg)was administered through a central line to achieve an activated clottingtime (ACT) 4480 seconds. CPB was performed using nonpulsatileflow at 2.5 L/min/m2, a nonheparin coated circuit and a membraneoxygenator (Affinity NT Oxygenation System, Medtronic Inc, Minne-apolis, MN). Mild hypothermia (321C-341C) and cold blood cardio-plegia (4:1 dilution) were used in all patients for myocardialpreservation. During CPB, phenylephrine or nitroglycerin was usedto maintain a perfusion pressure between 60 and 80 mmHg. All patientswere rewarmed to 361C (nasopharyngeal temperature) before weaningfrom CPB. After termination of CPB, the effects of heparin werereversed with protamine (1 mg per 100 U of heparin). An additionaldose of protamine, 0.2 mg/kg, was administered if ACT was more than140 seconds.
HES solutions were not used in the postoperative period, andintravascular volume was maintained with either Ringer’s lactateor blood products as required to maintain the central venous pressure(CVP) between 5-12 mmHg and urine output 40.5 mL/kg/min.Transfusion trigger for transfusion of packed red blood cells (PRBC)was a hemoglobin concentration of o8.0 g/dL during CPB and10 g/dL after weaning from CPB. Fresh frozen plasma (FFP) andplatelet concentrates (PC) were transfused for oozing from the surgicalsite or catheter site, increased chest tube drainage (4200 mL/hourfor 2 consecutive hours) and deranged coagulation profile (ACT 4140,clot rate o12 and platelet function o1.6) on SONOCLOT analysis(Sienco Inc, Arvada, CO). Re-exploration was considered whenthe chest tube drainage was 4200 mL/hour for 2 consecutive hourswith normal coagulation studies. The postoperative care was under-taken by a separate team of intensivists, unaware of the patient’sassigned group.
Consecutive clinical variables were measured in the 4 groups in thepreoperative period (T0), at the end of surgery (T1), and then 24 hours
after surgery (T2) in the intensive care unit (ICU). Hemoglobin,cumulative chest tube drainage in the first 24 hours after surgery, andSONOCLOT analysis were used to monitor coagulation. All SONO-CLOT measurements were taken by the same investigator, who wasunaware of the patient’s assigned group.
The SONOCLOT analyzer is designed to detect and quantifyviscoelastic changes in a whole-blood sample that occur throughouthemostasis.14 As determined in other SONOCLOT-based trials,15,16
SonACT, clot rate (CR) and platelet function (PF) were recorded at the3 study time points and compared. The SonACT, a glass bead-basedACT (normal 117-195 seconds), is the time until the beginning of fibrinformation and corresponds to the conventional ACT measurementsusing the Hemochron method.14 The CR (normal 7-23 clot signal units/minute) corresponds to the maximum slope of the SONOCLOTsignature during the fibrin polymerization and clot development. Thefunction of platelets is reported as PF and is derived from the timingand quality of clot retraction (0 represents no PF and 5 representsstrong PF).17
Renal function was monitored by measuring the urine output(hourly and 24-hour cumulative) and serum creatinine. The RIFLE(risk, injury, failure, loss, and end stage) classification18 for acutekidney injury (AKI) was used for assessment of renal function in thepostoperative period.
Serum bilirubin, aspartate aminotransferase (AST), and alanineaminotransferase (ALT) levels were measured at T0 and T2 to monitorliver function. Postoperative hyperbilirubinemia was defined as anincrease of serum bilirubin levels to 3 mg/dL.19 Threefold increase inserum transaminases from the preoperative level was consideredsignificant.
The duration of mechanical ventilation, ratio of partial pressure ofoxygen in arterial blood to the fraction of inspired oxygen (PaO2/FIO2),and the thoracic fluid content (TFC) using the Thoracic ElectricalBioimpedance (TEB)20,21 monitor (ICON; Osypka, Berlin, Germany)was used to compare the pulmonary function among the groups. Acuterespiratory distress syndrome (ARDS) was diagnosed based on theBerlin definition of ARDS.22
ICU stay, hospital stay, and in-hospital mortality were recorded assecondary measures of outcome. The patients were contacted bytelephone 60 days after the surgery to inquire about delayed adverseevents, especially renal failure requiring dialysis.
The primary outcome variable was cumulative chest tube drainagein 24 hours. Based on this pilot study, a standard deviation of 325 mLwas expected for 24-hour chest tube drainage. The authors calculatedthat with 80% power and 5% α error, a minimum sample size of 20patients per group was required to detect a 250-mL difference in chesttube drainage among the groups.
Data were analyzed using SPSS version 17.0 statistical software.Categoric data were compared using the Pearson χ2 test. Continuousdata comparison among the 4 groups was performed by applying one-way analysis of variance (ANOVA) or the Kruskal-Wallis test, asapplicable. Post hoc comparison with Bonferroni correction wasapplied to adjust the level of significance. Continuous variables withina group were compared using a paired t test. A p value of o0.05 wasconsidered statistically significant.
RESULTS
All 80 patients who were recruited completed the study. The4 groups were comparable with respect to age, sex, weight,body mass index (BMI), concomitant diseases, number andorigin of grafts, CPB, and aortic cross-clamp time (Table 1).
The cumulative 24-hour mediastinal drainage was higher inthe HESP (544 � 301 mL) and HESM (546 � 227 mL) groupscompared with the HESPRL (456 � 207 mL) and HESMRL
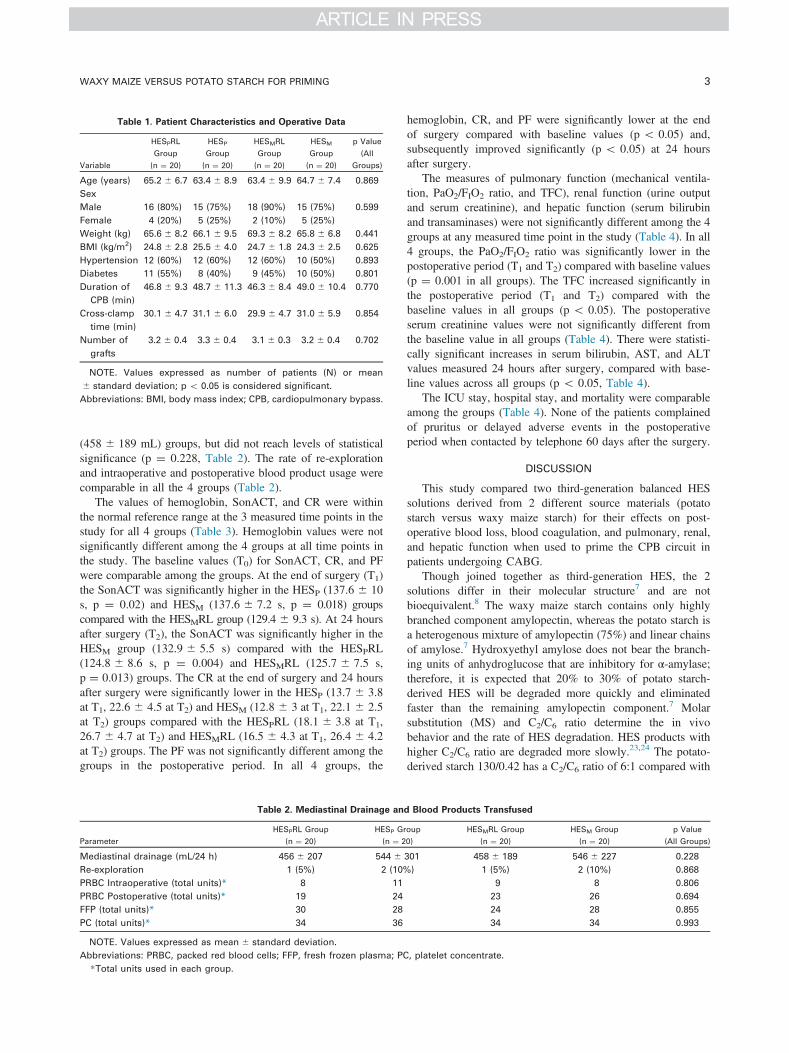
Table 1. Patient Characteristics and Operative Data
Variable
HESPRL
Group
(n ¼ 20)
HESP
Group
(n ¼ 20)
HESMRL
Group
(n ¼ 20)
HESM
Group
(n ¼ 20)
p Value
(All
Groups)
Age (years) 65.2 � 6.7 63.4 � 8.9 63.4 � 9.9 64.7 � 7.4 0.869
Sex
Male 16 (80%) 15 (75%) 18 (90%) 15 (75%) 0.599
Female 4 (20%) 5 (25%) 2 (10%) 5 (25%)
Weight (kg) 65.6 � 8.2 66.1 � 9.5 69.3 � 8.2 65.8 � 6.8 0.441
BMI (kg/m2) 24.8 � 2.8 25.5 � 4.0 24.7 � 1.8 24.3 � 2.5 0.625
Hypertension 12 (60%) 12 (60%) 12 (60%) 10 (50%) 0.893
Diabetes 11 (55%) 8 (40%) 9 (45%) 10 (50%) 0.801
Duration of
CPB (min)
46.8 � 9.3 48.7 � 11.3 46.3 � 8.4 49.0 � 10.4 0.770
Cross-clamp
time (min)
30.1 � 4.7 31.1 � 6.0 29.9 � 4.7 31.0 � 5.9 0.854
Number of
grafts
3.2 � 0.4 3.3 � 0.4 3.1 � 0.3 3.2 � 0.4 0.702
NOTE. Values expressed as number of patients (N) or mean
� standard deviation; p o 0.05 is considered significant.
Abbreviations: BMI, body mass index; CPB, cardiopulmonary bypass.
WAXY MAIZE VERSUS POTATO STARCH FOR PRIMING 3
(458 � 189 mL) groups, but did not reach levels of statisticalsignificance (p ¼ 0.228, Table 2). The rate of re-explorationand intraoperative and postoperative blood product usage werecomparable in all the 4 groups (Table 2).
The values of hemoglobin, SonACT, and CR were withinthe normal reference range at the 3 measured time points in thestudy for all 4 groups (Table 3). Hemoglobin values were notsignificantly different among the 4 groups at all time points inthe study. The baseline values (T0) for SonACT, CR, and PFwere comparable among the groups. At the end of surgery (T1)the SonACT was significantly higher in the HESP (137.6 � 10s, p ¼ 0.02) and HESM (137.6 � 7.2 s, p ¼ 0.018) groupscompared with the HESMRL group (129.4 � 9.3 s). At 24 hoursafter surgery (T2), the SonACT was significantly higher in theHESM group (132.9 � 5.5 s) compared with the HESPRL(124.8 � 8.6 s, p ¼ 0.004) and HESMRL (125.7 � 7.5 s,p ¼ 0.013) groups. The CR at the end of surgery and 24 hoursafter surgery were significantly lower in the HESP (13.7 � 3.8at T1, 22.6 � 4.5 at T2) and HESM (12.8 � 3 at T1, 22.1 � 2.5at T2) groups compared with the HESPRL (18.1 � 3.8 at T1,26.7 � 4.7 at T2) and HESMRL (16.5 � 4.3 at T1, 26.4 � 4.2at T2) groups. The PF was not significantly different among thegroups in the postoperative period. In all 4 groups, the
Table 2. Mediastinal Drainage an
Parameter
HESPRL Group
(n ¼ 20)
HESP G
(n ¼ 2
Mediastinal drainage (mL/24 h) 456 � 207 544 �
Re-exploration 1 (5%) 2 (10%
PRBC Intraoperative (total units)* 8 11
PRBC Postoperative (total units)* 19 24
FFP (total units)* 30 28
PC (total units)* 34 36
NOTE. Values expressed as mean � standard deviation.
Abbreviations: PRBC, packed red blood cells; FFP, fresh frozen plasma; PC
*Total units used in each group.
hemoglobin, CR, and PF were significantly lower at the endof surgery compared with baseline values (p o 0.05) and,subsequently improved significantly (p o 0.05) at 24 hoursafter surgery.
The measures of pulmonary function (mechanical ventila-tion, PaO2/FIO2 ratio, and TFC), renal function (urine outputand serum creatinine), and hepatic function (serum bilirubinand transaminases) were not significantly different among the 4groups at any measured time point in the study (Table 4). In all4 groups, the PaO2/FIO2 ratio was significantly lower in thepostoperative period (T1 and T2) compared with baseline values(p ¼ 0.001 in all groups). The TFC increased significantly inthe postoperative period (T1 and T2) compared with thebaseline values in all groups (p o 0.05). The postoperativeserum creatinine values were not significantly different fromthe baseline value in all groups (Table 4). There were statisti-cally significant increases in serum bilirubin, AST, and ALTvalues measured 24 hours after surgery, compared with base-line values across all groups (p o 0.05, Table 4).
The ICU stay, hospital stay, and mortality were comparableamong the groups (Table 4). None of the patients complainedof pruritus or delayed adverse events in the postoperativeperiod when contacted by telephone 60 days after the surgery.
DISCUSSION
This study compared two third-generation balanced HESsolutions derived from 2 different source materials (potatostarch versus waxy maize starch) for their effects on post-operative blood loss, blood coagulation, and pulmonary, renal,and hepatic function when used to prime the CPB circuit inpatients undergoing CABG.
Though joined together as third-generation HES, the 2solutions differ in their molecular structure7 and are notbioequivalent.8 The waxy maize starch contains only highlybranched component amylopectin, whereas the potato starch isa heterogenous mixture of amylopectin (75%) and linear chainsof amylose.7 Hydroxyethyl amylose does not bear the branch-ing units of anhydroglucose that are inhibitory for α-amylase;therefore, it is expected that 20% to 30% of potato starch-derived HES will be degraded more quickly and eliminatedfaster than the remaining amylopectin component.7 Molarsubstitution (MS) and C2/C6 ratio determine the in vivobehavior and the rate of HES degradation. HES products withhigher C2/C6 ratio are degraded more slowly.23,24 The potato-derived starch 130/0.42 has a C2/C6 ratio of 6:1 compared with
d Blood Products Transfused
roup
0)
HESMRL Group
(n ¼ 20)
HESM Group
(n ¼ 20)
p Value
(All Groups)
301 458 � 189 546 � 227 0.228
) 1 (5%) 2 (10%) 0.868
9 8 0.806
23 26 0.694
24 28 0.855
34 34 0.993
, platelet concentrate.
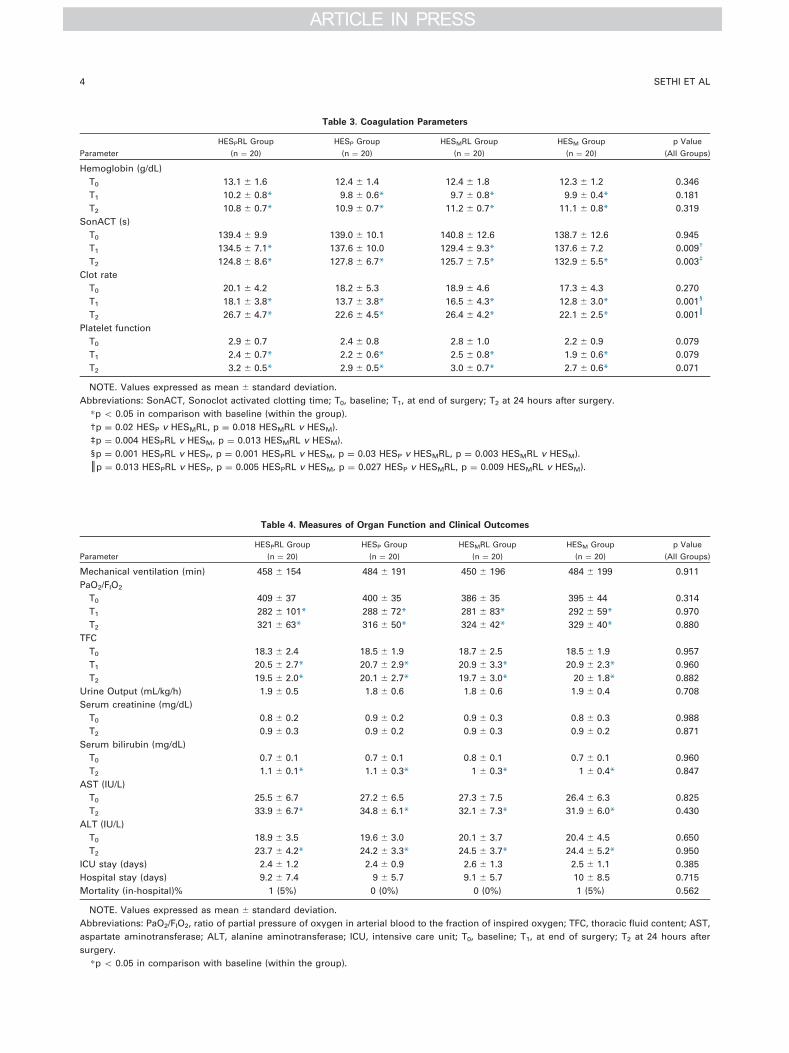
Table 3. Coagulation Parameters
Parameter
HESPRL Group
(n ¼ 20)
HESP Group
(n ¼ 20)
HESMRL Group
(n ¼ 20)
HESM Group
(n ¼ 20)
p Value
(All Groups)
Hemoglobin (g/dL)
T0 13.1 � 1.6 12.4 � 1.4 12.4 � 1.8 12.3 � 1.2 0.346
T1 10.2 � 0.8* 9.8 � 0.6* 9.7 � 0.8* 9.9 � 0.4* 0.181
T2 10.8 � 0.7* 10.9 � 0.7* 11.2 � 0.7* 11.1 � 0.8* 0.319
SonACT (s)
T0 139.4 � 9.9 139.0 � 10.1 140.8 � 12.6 138.7 � 12.6 0.945
T1 134.5 � 7.1* 137.6 � 10.0 129.4 � 9.3* 137.6 � 7.2 0.009†
T2 124.8 � 8.6* 127.8 � 6.7* 125.7 � 7.5* 132.9 � 5.5* 0.003‡
Clot rate
T0 20.1 � 4.2 18.2 � 5.3 18.9 � 4.6 17.3 � 4.3 0.270
T1 18.1 � 3.8* 13.7 � 3.8* 16.5 � 4.3* 12.8 � 3.0* 0.001§
T2 26.7 � 4.7* 22.6 � 4.5* 26.4 � 4.2* 22.1 � 2.5* 0.001║
Platelet function
T0 2.9 � 0.7 2.4 � 0.8 2.8 � 1.0 2.2 � 0.9 0.079
T1 2.4 � 0.7* 2.2 � 0.6* 2.5 � 0.8* 1.9 � 0.6* 0.079
T2 3.2 � 0.5* 2.9 � 0.5* 3.0 � 0.7* 2.7 � 0.6* 0.071
NOTE. Values expressed as mean � standard deviation.
Abbreviations: SonACT, Sonoclot activated clotting time; T0, baseline; T1, at end of surgery; T2 at 24 hours after surgery.
*p o 0.05 in comparison with baseline (within the group).
†p ¼ 0.02 HESP v HESMRL, p ¼ 0.018 HESMRL v HESM).
‡p ¼ 0.004 HESPRL v HESM, p ¼ 0.013 HESMRL v HESM).
§p ¼ 0.001 HESPRL v HESP, p ¼ 0.001 HESPRL v HESM, p ¼ 0.03 HESP v HESMRL, p ¼ 0.003 HESMRL v HESM).
║p ¼ 0.013 HESPRL v HESP, p ¼ 0.005 HESPRL v HESM, p ¼ 0.027 HESP v HESMRL, p ¼ 0.009 HESMRL v HESM).
Table 4. Measures of Organ Function and Clinical Outcomes
Parameter
HESPRL Group
(n ¼ 20)
HESP Group
(n ¼ 20)
HESMRL Group
(n ¼ 20)
HESM Group
(n ¼ 20)
p Value
(All Groups)
Mechanical ventilation (min) 458 � 154 484 � 191 450 � 196 484 � 199 0.911
PaO2/FIO2
T0 409 � 37 400 � 35 386 � 35 395 � 44 0.314
T1 282 � 101* 288 � 72* 281 � 83* 292 � 59* 0.970
T2 321 � 63* 316 � 50* 324 � 42* 329 � 40* 0.880
TFC
T0 18.3 � 2.4 18.5 � 1.9 18.7 � 2.5 18.5 � 1.9 0.957
T1 20.5 � 2.7* 20.7 � 2.9* 20.9 � 3.3* 20.9 � 2.3* 0.960
T2 19.5 � 2.0* 20.1 � 2.7* 19.7 � 3.0* 20 � 1.8* 0.882
Urine Output (mL/kg/h) 1.9 � 0.5 1.8 � 0.6 1.8 � 0.6 1.9 � 0.4 0.708
Serum creatinine (mg/dL)
T0 0.8 � 0.2 0.9 � 0.2 0.9 � 0.3 0.8 � 0.3 0.988
T2 0.9 � 0.3 0.9 � 0.2 0.9 � 0.3 0.9 � 0.2 0.871
Serum bilirubin (mg/dL)
T0 0.7 � 0.1 0.7 � 0.1 0.8 � 0.1 0.7 � 0.1 0.960
T2 1.1 � 0.1* 1.1 � 0.3* 1 � 0.3* 1 � 0.4* 0.847
AST (IU/L)
T0 25.5 � 6.7 27.2 � 6.5 27.3 � 7.5 26.4 � 6.3 0.825
T2 33.9 � 6.7* 34.8 � 6.1* 32.1 � 7.3* 31.9 � 6.0* 0.430
ALT (IU/L)
T0 18.9 � 3.5 19.6 � 3.0 20.1 � 3.7 20.4 � 4.5 0.650
T2 23.7 � 4.2* 24.2 � 3.3* 24.5 � 3.7* 24.4 � 5.2* 0.950
ICU stay (days) 2.4 � 1.2 2.4 � 0.9 2.6 � 1.3 2.5 � 1.1 0.385
Hospital stay (days) 9.2 � 7.4 9 � 5.7 9.1 � 5.7 10 � 8.5 0.715
Mortality (in-hospital)% 1 (5%) 0 (0%) 0 (0%) 1 (5%) 0.562
NOTE. Values expressed as mean � standard deviation.
Abbreviations: PaO2/FIO2, ratio of partial pressure of oxygen in arterial blood to the fraction of inspired oxygen; TFC, thoracic fluid content; AST,
aspartate aminotransferase; ALT, alanine aminotransferase; ICU, intensive care unit; T0, baseline; T1, at end of surgery; T2 at 24 hours after
surgery.
*p o 0.05 in comparison with baseline (within the group).
SETHI ET AL4

WAXY MAIZE VERSUS POTATO STARCH FOR PRIMING 5
9:1 for waxy maize-derived HES 130/0.4.9 In fact, Lehmannet al8 demonstrated a lower area under the concentration curveand a faster clearance for potato-derived HES 130/0.42. Thein vivo molecular weight (MW) and plasma concentrationdetermine the side effects on hemostasis.25 Thus, the differentpharmacokinetics of the 2 solutions may have potential effectson hemostasis.
The cumulative 24-hour mediastinal drainage, rate of re-exploration, and blood product usage were not significantlydifferent among the groups, suggesting equivalence of the 2HES solutions with regard to effects on hemostasis. This is animportant observation of the study considering the fact that,although the evidence for waxy maize-derived HES 130/0.4 isavailable,26,27 few clinical studies have evaluated the effect ofpotato-derived HES 130/0.42 on hemostasis in patients under-going cardiac surgery. Of the 3 studies12,28,29 that haveevaluated the effect of potato-derived HES 130/0.42, onlyone included patients undergoing cardiac surgery, and it waslater retracted.28 Four in vitro studies10,30-32 comparing theeffects of maize- or potato-derived HES on coagulation usingdifferent viscoelastic tests of coagulation reported conflictingresults. Furthermore, the findings of in vitro studies cannot betranslated to the clinical setting because of the absence ofcontribution by endothelial and vascular factors in the clottingprocess, as well as lack of metabolic degradation of the HESmolecules.
This study found no significant differences in coagulationparameters with respect to plant source of HES whenequivalent doses of the starch solutions (1,000 mL for theHESPRL and HESMRL groups and 1,500 mL for the HESPand HESM groups) were used to prime the CPB circuit. Thiswas in contrast to the study by Jamnicki et al,10 who suggestedthat potato starch-derived HES compromised in vitro bloodcoagulation more than the corn-derived HES. They attributedthis to the higher C2/C6 ratio of the potato-derived HES. Thepotato starch in this study, however, had a lower C2/C6 ratio.The findings were in accordance with 2 recent in vitrostudies.30,31
When higher doses (1,500 mL) of the study solutions wereused in the priming fluid (ie, the HESP and HESM groups),SonACT was significantly higher and CR significantly lower atT1 and T2 in comparison with the HESPRL and HESMRLgroups (1,000 mL). The dose dependency of HES-inducedcoagulopathy has been described previously.10,33 Interestingly,only the extent of change in coagulation parameters separatesthe HES-induced alteration in hemostasis from dilutionalcoagulopathy. HES compromises blood coagulation bydecreasing the plasma concentration of factor VIII and vonWillebrand factor.25 There are decreased expression andactivation of platelet surface glycoprotein IIb-IIIa receptor withimpaired platelet adhesion and aggregation.25 In addition, HESimpairs fibrin polymerization required for stable clot forma-tion.25 These effects explain the decreased CR (which indicatesfibrin polymer formation) and PF values found in this studyacross all groups at T1. In their in vitro study using thromboe-lastometry, Godier et al30 also found that irrespective of the rawmaterial of the HES, impairment of fibrin polymerizationappeared to be the leading determinant of HES-inducedcoagulopathy.
The other aspect of better SONOCLOT parameters in theHESPRL and HESMRL groups possibly may be related to theprocoagulant effect of Ringer’s lactate. This has been reportedpreviously at 33% hemodilution by Konrad et al15 in theirstudy to quantify the hemodilutional effects of medium-molecular-weight HES solutions and Ringer’s lactate onin vitro coagulation using SONOCLOT. Fries et al,34 in theirin vitro study using thromboelastography, reported that acombination of 6% HES 130/0.4 with Ringer’s lactate impairedcoagulation to a lesser degree than the HES solution adminis-tered alone.
On intragroup analysis, the SonACT, CR, and PF values atT2 were comparable to or even better than values obtained at T0
in all 4 groups. This could be the result of recovery offibrinogen levels and platelet function, blood componenttherapy, or the faster clearance of third-generation HESsolutions.35,36
Lehmann et al8 reported the equivalence of potato-derivedHES 130/0.42, waxy maize-derived HES 130/0.4, and penta-starch in terms of colloid osmotic and hemodilution effect.Previous studies also have shown that the degradation rate doesnot correlate with the degree and duration of the volumeeffect.37 The hemoglobin levels in this study were comparableamong the groups at all time points, indicating the equivalenceof hemodilution effect between the potato- and waxy maize-derived HES. The hemoglobin levels in the HESP and HESMgroups, which used higher doses of HES, were comparable tothe groups that used lower doses (HESPRL and HESMRL),because the total volume of the priming solution was madeequal by adding 500 mL of Ringer’s lactate to the 1,000 mL ofHES in the HESPRL and HESMRL groups.
The duration of mechanical ventilation and the changes inPaO2/FIO2 ratio and TFC were similar in all 4 groups, implying theequivalence of the pulmonary effects of the potato- and the waxymaize-derived HES. When compared with the baseline, there weresignificant decreases in the PaO2/FIO2 ratio at T1 and T2. Thesefindings probably were unrelated to the study drug and have beendescribed in other studies assessing pulmonary dysfunction afterCPB.38,39 Multiple factors contribute to the development ofhypoxemia in the post-CPB period, such as atelectasis, increasedintrapulmonary shunt, alteration in lung and chest wall mechanics,and changes in capillary bed and pulmonary parenchyma.40 Onepatient in the HESPRL group and one patient in the HESM groupdeveloped mild ARDS in the early postoperative period butrecovered promptly, with a maximum duration of ventilation of20 hours. The incidence of ARDS in this study (2.5%) was similarto that mentioned in the literature.41
CPB can lead to increased interstitial pulmonary edema andsubsequent abnormal gas exchange in the form of low PaO2/FIO2
ratio requiring prolonged mechanical ventilation.38 The type ofpriming solution can influence the extravascular lung wateraccumulation in the early post-CPB period.42 TFC measurednoninvasively by TEB reflects total (intravascular and extravas-cular) fluid volume contained in the chest cavity.21 Near-identicalchanges in the postoperative period indirectly demonstrated asimilar colloid osmotic effect of the 2 study solutions.
A recent clinical trial (6S) found that patients with severesepsis receiving fluid resuscitation with balanced 6% HES 130/0.42 had an increased risk of death at day 90 and were more

SETHI ET AL6
likely to require renal replacement therapy.11 Another recentsystematic review by Zarychanski et al,43 after exclusion of 7retracted trials, found HES to be associated with increased riskof mortality and AKI in critically ill patients requiring volumeresuscitation. In view of the evidence from these 2 studies, itmay not be prudent to use HES for volume replacement incritically ill patients. However the renal safety of third-generation starches in nonseptic surgical patients remainsunclear. This study found that HES 130/0.42 and HES 130/0.4were not different with respect to their effect on renal functionwhen used as priming solution in relatively low-risk patientsundergoing cardiac surgery. The 24-hour urine output andchanges in serum creatinine were not significantly different inthe 4 study groups. A total of 8 patients (2 in the HESPRLgroup, 2 in the HESP group, 3 in the HESMRL group, and 1 inthe HESM group) met the criteria for risk of AKI. Theincidence of 10% in this study is similar to that described inprevious studies in CABG patients.44,45 None of the 8 patientsrequired dialysis. Cardiopulmonary bypass-associated renaldysfunction may occur because of decreased renal perfusion,inflammatory response, embolic events, or nephrotoxin-likefree hemoglobin.45
In a recent meta-analysis of 17 randomized studies evaluat-ing the safety of waxy maize-derived HES 130/0.4 in surgicalpatients, Martin et al46 found no evidence of renal dysfunction.In a prospective multicenter observational postauthorizationsafety study (PASS) of children aged 12 years or younger,Sümpelmann et al6 found no evidence of renal dysfunctiondirectly related to HES 130/0.42.
Sander et al12 compared potato-derived 6% HES 130/0.42with 6% HES 200/0.5 in 60 patients undergoing majorgynecologic surgery. They reported mild-to-moderate hyper-bilirubinemia as a common adverse event in 36 patients (17 inpentastarch and 19 in tetrastarch group) with a questionablerelationship to the study drug. They suggested that postoper-ative hyperbilirubinemia may be induced by impaired excretionof bile, increased bilirubin supply from fragmented erythro-cytes, or concomitant medication such as antibiotics.
This study found no significant differences among the4 study groups with respect to serum bilirubin and trans-aminases, thus implying that potato-derived HES 130/0.42 andwaxy maize-derived HES 130/0.4 exert similar effects onhepatic function. The serum bilirubin, AST, and ALT increasedsignificantly but still remained within the reference range24 hours after surgery in all 4 groups. This finding probablywas unrelated to the study medication and was in agreementwith the findings of Ascione et al,47 who studied splanchnicorgan injury during CABG with or without CPB. These resultsare in contrast to those of Wang et al,19 who reported an overallincidence of postoperative hyperbilirubinemia to be 35% inpatients undergoing cardiac surgery. Kumle et al48 observed thatserious liver dysfunction was observed mainly with prolongedCPB times (470 minutes). These CPB times were relativelyshort, with a mean of less than 50 minutes, and no hyper-bilirubinemia was observed. However potato-derived starch iscontraindicated in patients with severe hepatic impairment.9
In this study, no patient in any group experienced pruritus inthe postoperative period through 60 days after surgery. The
pruritus arises from long-term storage of HES molecules andmay last for months after exposure. Kasper et al,26 in arandomized study of 120 patients undergoing CABG, con-cluded that high doses of 6% HES 130/0.4 and 6% HES 200/0.5did not contribute to pruritus.
LIMITATIONS
The authors cannot make any definitive statements regard-ing the power of the study to detect differences with respect tothe secondary outcome variables. Large comparative trialspowered for multiple safety relevant endpoints are neededbefore any recommendations can be made regarding practices.
The authors did not measure the traditional tests ofcoagulation, such as prothrombin time, activated partial throm-boplastin time, fibrinogen level, and platelet count. Tumanet al49 found that the sensitivity of SONOCLOT in predictingbleeding after CPB was 74%, with no false negatives and 33%false positives. This compared well with the predictive accu-racy of 33% using routine coagulation tests with 44% falsenegative and 73% false positive results. With respect to TEG,the SONOCLOT is superior in terms of practicality and speedof availability of results. Compared with SONOCLOT, there isa greater opportunity for variability in technique because ofdifferent operators during TEG.14 The TEG and SONOCLOTare comparable with respect to sensitivity and specificity, buttaken together, SONOCLOT and TEG were able to increasediagnostic accuracy significantly.50
The authors measured TFC with TEB. Previous attempts tovalidate the impedance-derived measurements with other refer-ence methods have produced conflicting results. In an extensivemeta-analysis, Fuller51 reviewed 75 studies comparing impe-dance cardiography cardiac output with that of Fick, thermo-dilution, dye-dilution, and radionuclear angiography, andconcluded that there was moderate agreement of the impedancemethod with other reference methods.
The total dose of colloids used in this study was not therecommended maximum daily dose of 50 mL/kg (as per themanufacturer’s package insert for both the starch solutions),because the authors wanted to observe the effects of a large doseadministered within a short time period. They did not use thestudy solution for volume replacement in the prebypass periodor the postoperative period, because they wanted to observe theeffects of HES solely as a priming solution for CPB. There wasalso a lack of control group in the form of Ringer’s lactate asprime, because the aim was to compare the effects of the 2 HESsolutions derived from different plant sources.
CONCLUSION
There was no significant difference in cumulative 24-hourmediastinal drainage whether potato-derived balanced 6% HES130/0.42 or waxy maize-derived balanced 6% HES 130/0.4was used to prime the CPB circuit in patients undergoingCABG. Despite the differences in physicochemical propertiesand plasma clearance, the 2 HES solutions in equal dosesexerted the same effect on blood coagulation and pulmonary,renal, and hepatic function.
WAXY MAIZE VERSUS POTATO STARCH FOR PRIMING 7
REFERENCES
1. Nussmeier NA, Searles BE: The next generation of colloids:Ready for “prime time”? Anesth Analg 109:1715-1717, 20092. Himpe D: Colloids versus crystalloids as priming solutions for
cardiopulmonary bypass: A meta-analysis of prospective, randomisedclinical trials. Acta Anaesthesiol Belg 54:207-216, 20033. Russell JA, Navickis RJ, Wilkes MM: Albumin versus crystalloid
for pump priming in cardiac surgery: Meta-analysis of controlled trials.J Cardiothorac Vasc Anesth 18:429-437, 20044. Eising GP, Niemeyer M, Gunther T, et al: Does a hyperoncotic
cardiopulmonary bypass prime affect extravascular lung water andcardiopulmonary function in patients undergoing coronary arterybypass surgery? Eur J Cardiothorac Surg 20:282-289, 20015. Base EM, Standl T, Lassnigg A, et al: Efficacy and safety of
hydroxyethyl starch 6% 130/0.4 in a balanced electrolyte solution(volulyte) during cardiac surgery. J Cardiothorac Vasc Anesth 25:407-414, 20116. Sümpelmann R, Kretz FJ, Luntzer R, et al: Hydroxyethyl starch
130/0.42/6:1 for perioperative plasma volume replacement in 1130children: Results of an European prospective multicenter observationalpostauthorization safety study (PASS). Paediatr Anaesth 22:371-378, 20127. Sommermeyer K, Cech F, Schossow R: Differences in chemical
structures between waxy maize- and potato-starch-based hydroxyethylstarch volume therapeutics. Transfus Altern Transfus Med 9:127-133, 20078. Lehmann G, Marx G, Förster H: Bioequivalence comparison
between hydroxyethyl starch 130/0.42/6:1 and hydroxyethyl starch130/0.4/9:1. Drugs RD 8:229-240, 20079. Westphal M, James MF, Kozek-Langenecker S, et al: Hydrox-
yethyl starches: Different products—different effects. Anesthesiology111:187-202, 200910. Jamnicki M, Zollinger A, Seifert B, et al: The effect of potato
starch derived and corn starch derived hydroxyethyl starch on in vitroblood coagulation. Anesthesia 53:638-644, 199811. Perner A, Haase N, Guttormsen AB, et al: Hydroxyethyl starch
130/0.42 versus Ringer’s acetate in severe sepsis. N Engl J Med 367:124-134, 201212. Sander O, Reinhart K, Meier-Helmann A: Equivalence of
hydroxyethyl starch HES 130/0.4 and HES 200/0.5 for perioperativevolume replacement in major gynaecological surgery. Acta Anaesthe-siol Scand 47:1151-1158, 200313. Bagchi A, Eikermann M: Mashed potatoes and maize: Are the
starches safe? Anesthesiology 118:244-247, 201314. Hett DA, Walker D, Pilkington SN, et al: Sonoclot analysis. Br J
Anaesth 75:771-776, 199515. Konrad CJ, Markl TJ, Schuepfer GK, et al: In vitro effects of
different medium molecular hydroxyethyl starch solutions and lactatedRinger’s solution on coagulation using SONOCLOT. Anesth Analg 21:274-279, 200016. Miyashita T, Kuro M: Evaluation of platelet function by sonoclot
analysis compared with other hemostatic variables in cardiac surgery.Anesth Analg 87:1228-1233, 199817. Ganter MT, Hofer CK: Coagulation monitoring: Current techni-
ques and clinical use of viscoelastic point-of-care coagulation devices.Anesth Analg 21:1366-1375, 200818. Bellomo R, Ronco C, Kellum JA, et al: Acute Dialysis Quality
Initiative workgroup (2004) Acute renal failure—definition, outcomemeasures, animal models, fluid therapy and information technologyneeds: The Second International Consensus Conference of the AcuteDialysis Quality Initiative (ADQI) Group. Crit Care 8:204-212, 200419. Wang MJ, Chao A, Huang CH, et al: Hyperbilirubinemia after
cardiac operation. Incidence, risk factors, and clinical significance.J Thorac Cardiovasc Surg 108:429-436, 1994
20. Rosenberg P, Yancy CW: Noninvasive assessment of hemody-namics: An emphasis on bioimpedance cardiography. Curr OpinCardiol 15:151-155, 200021. van de Water JM, Mount BE, Chandra KM, et al: TFC (thoracic
fluid content): A new parameter for assessment of changes in chestfluid volume. Am Surg 71:81-86, 200522. Ranieri VM, Rubenfeld GD, Thompson BT, et al: Acute respiratory
distress syndrome: The Berlin Definition. JAMA 307:2526-2533, 201223. Jung F, Koscielny J, Mrowietz C, et al: The effects of molecular
structure of hydroxyethyl starch on the elimination kinetics and fluidityof blood in human volunteers (in German). Arzneimittelforschung 43:99-105, 199324. Treib J, Haass A, Pindur G, et al: HES 200/0.5 is not HES 200/
0.5: Influence of the C2/C6 hydroxyethylation ratio of hydroxyethylstarch (HES) on hemorheology, coagulation and elimination kinetics.Thromb Haemost 74:1452-1456, 199525. Kozek-Langenecker SA: Effects of hydroxyethyl starch solutions
on hemostasis. Anesthesiology 103:654-660, 200526. Kasper SM, Meinert P, Kampe S, et al: Large-dose hydroxyethyl
starch 130/0.4 does not increase blood loss and transfusion require-ments in coronary artery bypass surgery compared with hydroxy-ethyl starch 200/0.5 at recommended doses. Anesthesiology 99:42-47, 200327. Kozek-Langenecker SA, Jungheinrich C, Sauermann W, et al:
The effects of hydroxyethyl starch 130/0.4 (6%) on blood loss and useof blood products in major surgery: A pooled analysis of randomizedclinical trials. Anesth Analg 107:382-390, 200828. Boldt J, Suttner S, Brosch C, et al: Influence on coagulation of a
potato-derived hydroxethylstarch (HES 130/0.42) and a maize-derivedhydroxethylstarch (HES 130/0.4) in patients undergoing cardiacsurgery. Br J Anaesth 102:191-197, 200929. Staikou C, Paraskeva A, Fassoulaki A: The impact of 30 ml/kg
hydroxyethyl starch 130/0.4 vs hydroxyethyl starch 130/0.42 oncoagulation in patients undergoing abdominal surgery. Indian J MedRes 136:445-450, 201230. Godier A, Durand M, Smadja D, et al: Maize- or potato-derived
hydroxyethyl starches: Is there any thromboelastometric difference?Acta Anaesthesiol Scand 21:1241-1247, 201031. Matsota P, Politou M, Kalimeris K, et al: Do different sub-
stitution patterns or plant origin in hydroxyethyl starches affect bloodcoagulation in vitro? Blood Coagul Fibrinolysis 21:448-451, 201032. Casutt M, Kristoffy A, Schuepfer G, et al: Effects on coagulation
of balanced (130/0.42) and non balanced (130/0.4) hydroxyethyl starchor gelatin compared with balanced Ringer’s solution: An in vitro studyusing two different viscoelastic coagulation tests ROTEM and SONO-CLOT. Br J Anaesth 105:273-281, 201033. Haynes GR, Havidich JE, Payne KJ: Why the food and drug
administration changed the warning label for hetastarch. Anesthesiol-ogy 101:560-561, 200434. Fries D, Innerhofer P, Klingler A, et al: The effect of the
combined administration of colloids and lactated Ringer’s solution onthe coagulation system: An in vitro study using thrombelastographcoagulation analysis (ROTEG). Anesth Analg 94:1280-1287, 200235. Woodman RC, Harker LA: Bleeding complications associated
with cardiopulmonary bypass. Blood 76:1680-1697, 199036. Waitzinger J, Bepperling F, Pabst G, et al: Pharmacokinetics and
tolerability of a new hydroxyethyl starch (HES) specification [HES(130/0.4)] after single-dose infusion of 6% or 10% solutions in healthyvolunteers. Clin Drug Investig 16:151-160, 199837. Jungheinrich C, Sauermann W, Bepperling F, et al: Volume efficacy
and reduced influence on measures of coagulation using hydroxyethyl starch130/0.4 (6%) with an optimised in vivo molecular weight in orthopedicsurgery: A randomised, double-blind study. Drugs RD 5:1-9, 2004

SETHI ET AL8
38. Apostolakis E, Filos KS, Koletsis E, et al: Lung DysfunctionFollowing Cardiopulmonary Bypass. J Card Surg 25:47-55, 201039. Weiss YG, Merin G, Koganov E, et al: Postcardiopulmonary
bypass hypoxemia: A prospective study on incidence, risk factors, andclinical significance. J Cardiothorac Vasc Anesth 14:506-513, 200040. Tenling A, Hachenberg T, Tyden H, et al: Atelectasis and gas
exchange after cardiac surgery. Anesthesiology 89:371-378, 199841. Milot J, Perron J, Lacasse Y, et al: Incidence and predictors of
ARDS after cardiac surgery. Chest 119:884-888, 200142. Hoeft A, Korb H, Mehlhorn U, et al: Priming of cardiopulmonary
bypass with human albumin or Ringer lactate: Effect on colloid osmoticpressure and extravascular lung water. Br J Anaesth 66:73-80, 199143. Zarychanski R, Abou-Setta AM, Turgeon AF, et al: Association
of hydroxyethyl starch administration with mortality and acute kidneyinjury in critically ill patients requiring volume resuscitation: Asystematic review and meta-analysis. JAMA 309:678-688, 201344. Tolpin DA, Collard CD, Vei-Vei L, et al: Subclinical changes in
serum creatinine predict mortality following coronary artery bypassgraft surgery. J Thorac Cardiovasc Surg 143:682-688, 2012
45. Rosner MH, Okusa MD: Acute kidney injury associated withcardiac surgery. Clin J Am Soc Nephrol 1:19-32, 200646. Martin C, Jacob M, Vicaut E, et al: Effect of waxy maize-derived
hydroxyethyl starch 130/0.4 on renal function in surgical patients.Anesthesiology 118:387-394, 201347. Ascione R, Talpahewa S, Rajakaruna C, et al: Splanchnic organ
injury during coronary surgery with or without cardiopulmonary bypass:A randomized, controlled trial. Ann Thorac Surg 81:97-103, 200648. Kumle B, Boldt J, Suttner S, et al: Influence of prolonged
cardiopulmonary bypass times on splanchnic perfusion and markers ofsplanchnic organ function. Ann Thorac Surg 75:1558-1564, 2003;Retraction in Ann Thorac Surg 92:412, 201149. Tuman KJ, Spiess BD, McCarthy RJ, et al: Comparison of
viscoelastic measures of coagulation after cardiopulmonary bypass.Anesth Analg 69:69-75, 198950. Mallet S, Cox D: Role of thromboelastography in bleeding
diathesis and regional anaesthesia. Lancet 338:765-766, 199151. Fuller HD: The validity of cardiac output measurement by thoracic
impedance: A meta-analysis. Clin Invest Med 15:103-112, 1992