companion nimals ct and mri in veterinary patients: an...
TRANSCRIPT

Companion animalS
546 In Practice November/December 2013 | Volume 35 | 546-563
doi:10.1136/inp.f6720
Julien Labruyère qualified from the University of Liège in 2001. He holds the European College of Veterinary Diagnostic Imaging diploma and is an RCVS specialist in veterinary diagnostic imaging. He his currently director and full-time teleradiology consultant at VetCT, his principal interests are ocular ultrasonography and cross sectional imaging techniques.
CT and MRI in veterinary patients: an update on recent advances
Julien Labruyère and Tobias Schwarz
Computed tomography (CT) and magnetic resonance imaging (MRI) are two diagnostic imaging procedures that have become commonplace in first-opinion practices. Both of these modalities are continually undergoing technological improvement and each has its advantages for different applications. This article provides an update on recent advances and compares the use of CT and MRI in different areas of the body.
In recent years, there has been a rapid increase in the availability of computed tomography (CT) and magnetic resonance imaging (MRI). Previously, these modalities were only available in universities or large referral insti-tutions. nowadays, first opinion practices are acquiring CT scanners and low field MRIs, and mobile imaging units make these advanced imaging modalities readily accessible to the veterinary profession.
Since their development, CT and MRI have under-gone continuous technological improvement and a large number of scientific papers describing features of diseas-es in animals have been published, contributing greatly to the advancements in clinical veterinary medicine.
CT and MRI scanning will remain complex and expensive procedures. Fundamental differences exist between both technologies. Veterinarians are often faced with a choice between CT or MRI for the optimal diagnostic workup of their patients. A clear understanding of the strengths and weaknesses of both modalities will allow them to select the optimal imaging modality.
The aim of this article is to review the key differ-ences between CT and MRI, discuss their most impor-tant indications in veterinary patients and present a summary of the most recent advances in these two cross-sectional imaging modalities.
Fig 1: The effect of windowing and levelling on CT image interpretation. As too much data are obtained on a CT scan the radiologist selects the window level (WL) centred on the density of the tissue of interest and a window width (WW) wide enough to include the densities of the tissues of interest. For example, window settings to observe the lung are different from those of the soft tissues and bones. The numerical values are given in Hounsfield units
Brain windowWL =35WW = 150
Lung windowWL =500WW = 1500
Bone windowWL = 500WW = 1500
Soft tissue windowWL = 50WW = 500
Tobias Schwarz qualified from the Humboldt University of Berlin in 1997. He is currently a senior lecturer in diagnostic imaging and diagnostic imaging service head at the University of Edinburgh. He is also the president of the European College of Veterinary Diagnostic Imaging.
CT and MRI.indd 546 08/11/2013 11:21
group.bmj.com on November 16, 2013 - Published by inpractice.bmj.comDownloaded from
Companion animalS
547In Practice November/December 2013 | Volume 35 | 546-563
How does CT work?
CT is a diagnostic imaging technique based on x-ray technology. The difference to conventional radiog-raphy is that x-rays are produced by a high-powered x-ray tube that rotates around a slice of the patient’s anatomy. The x-ray beam is attenuated by the patient’s anatomy to reach a panel of detectors, which trans-form the detected radiation into an electrical signal. The signal output is proportional to the density of the penetrated tissue. The computer generates a matrix image from the different projectional density values corresponding to the relative density of the different body parts. CT images are usually acquired in the transverse plane. Images in other planes (eg, sagittal, dorsal, oblique) can be reconstructed with specific software; however, the image resolution is inferior to the original transverse images, unless these were acquired with submillimeter slice width.
In honour of the inventor of CT, the attenuation val-ues are specified in Hounsfield units (HU) or CT num-bers. In theory, more than 4000 shades of grey could be represented on the monitor. However, the human eye is only able to differentiate 20 to 30 shades of grey. Therefore, it becomes necessary to adjust the image to an adequate range of CT numbers. This is known as windowing and levelling of the image (Fig 1).
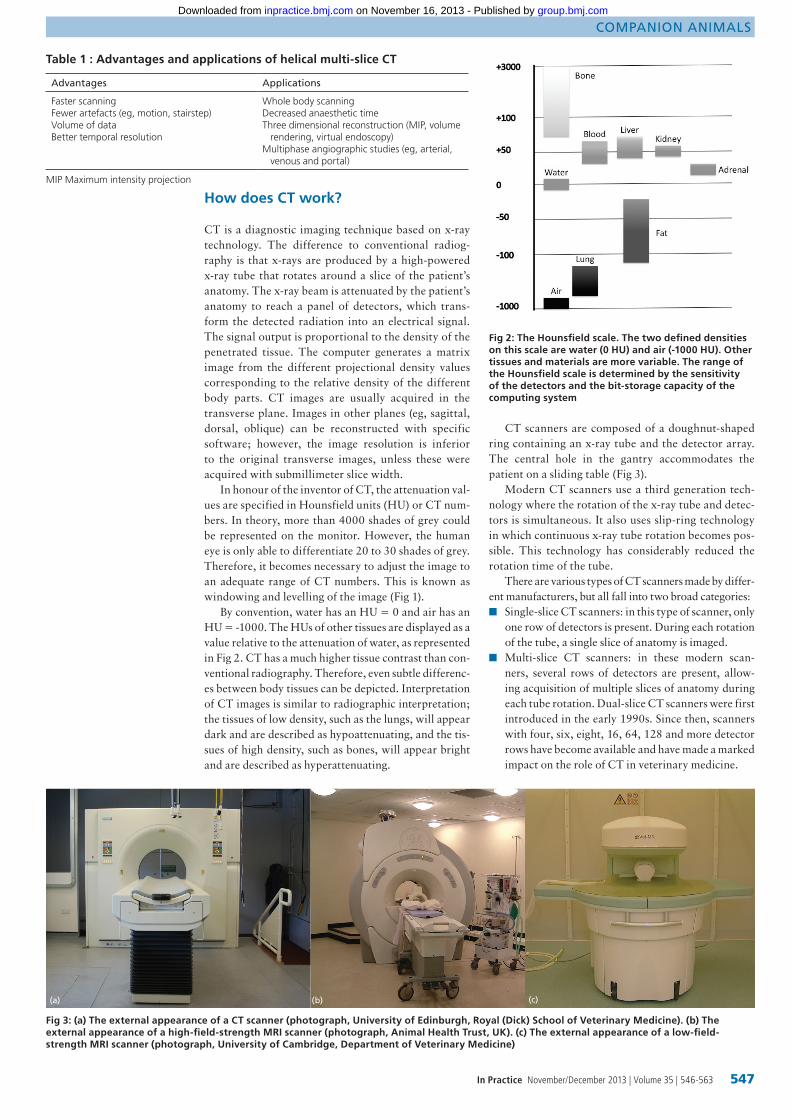
By convention, water has an HU = 0 and air has an HU = -1000. The HUs of other tissues are displayed as a value relative to the attenuation of water, as represented in Fig 2. CT has a much higher tissue contrast than con-ventional radiography. Therefore, even subtle differenc-es between body tissues can be depicted. Interpretation of CT images is similar to radiographic interpretation; the tissues of low density, such as the lungs, will appear dark and are described as hypoattenuating, and the tis-sues of high density, such as bones, will appear bright and are described as hyperattenuating.
CT scanners are composed of a doughnut-shaped ring containing an x-ray tube and the detector array. The central hole in the gantry accommodates the patient on a sliding table (Fig 3).
Modern CT scanners use a third generation tech-nology where the rotation of the x-ray tube and detec-tors is simultaneous. It also uses slip-ring technology in which continuous x-ray tube rotation becomes pos-sible. This technology has considerably reduced the rotation time of the tube.
There are various types of CT scanners made by differ-ent manufacturers, but all fall into two broad categories: ■■ Single-slice CT scanners: in this type of scanner, only
one row of detectors is present. During each rotation of the tube, a single slice of anatomy is imaged.
■■ Multi-slice CT scanners: in these modern scan-ners, several rows of detectors are present, allow-ing acquisition of multiple slices of anatomy during each tube rotation. Dual-slice CT scanners were first introduced in the early 1990s. Since then, scanners with four, six, eight, 16, 64, 128 and more detector rows have become available and have made a marked impact on the role of CT in veterinary medicine.
Advantages Applications
Faster scanningFewer artefacts (eg, motion, stairstep)Volume of dataBetter temporal resolution
Whole body scanningDecreased anaesthetic timeThree dimensional reconstruction (MIP, volume rendering, virtual endoscopy)Multiphase angiographic studies (eg, arterial, venous and portal)
Table 1 : Advantages and applications of helical multi-slice CT
Fig 2: The Hounsfield scale. The two defined densities on this scale are water (0 HU) and air (-1000 HU). Other tissues and materials are more variable. The range of the Hounsfield scale is determined by the sensitivity of the detectors and the bit-storage capacity of the computing system
Fig 3: (a) The external appearance of a CT scanner (photograph, University of Edinburgh, Royal (Dick) School of Veterinary Medicine). (b) The external appearance of a high-field-strength MRI scanner (photograph, Animal Health Trust, UK). (c) The external appearance of a low-field-strength MRI scanner (photograph, University of Cambridge, Department of Veterinary Medicine)
(a) (b) (c)
MIP Maximum intensity projection
CT and MRI.indd 547 08/11/2013 11:22
group.bmj.com on November 16, 2013 - Published by inpractice.bmj.comDownloaded from

Companion animalS
548 In Practice November/December 2013 | Volume 35 | 546-563
Each of these scanners can obtain the images in sequential (axial) or helical (spiral) mode. The sequen-tial mode allows image acquisition with an immobile table. The table will move in small increments after each tube rotation. This allows collection of a complete set of data. In single to eight-detector scanners, sequential scanning results in maximal image resolution. In heli-cal mode, continuous x-ray tube rotation is used along with simultaneous and continuous table movement through the gantry. This creates a helix of imaging data from the patient. The rapidity of image acquisition is greatly increased in helical mode, allowing examina-tion of large areas in only a few seconds. The helical mode has many advantages compared to the sequential mode (Table 1). Special software applications, such as multiplanar reconstructions and 3D reconstructions or virtual endoscopy (Figs 4, 5 and 6), are often of bet-ter quality, using data from helical scans. The image reconstruction of helically acquired data from multiple rows of detectors is very complex, but with 16 or more detector rows, the resulting image quality is often bet-ter than from sequentially acquired data. Multi-slice CT also allows acquisition with very thin slices (down to 0.5 mm) and facilitates highly detailed CT angiogra-phy images using iodinated contrast media. Intravenous contrast medium is used to increase vascular and soft tissue contrast, making lesions and vessels more visible. Therefore, a post-contrast CT series is performed in most patients. Exceptions are examinations where it is mainly bone that is of interest or if there are contraindi-cations for the use of iodinated contrast medium, such as dehydration, renal failure or known allergies.
Potential hazards from ionising radiation for moni-toring personnel mean that sedation or anaesthesia is necessary during the examination, enabling the per-sonnel to leave the CT room during the examination.
How does MRI work?
Based on the magnetic properties of protons, MRI can be seen as a map of hydrogen protons of the body. The patient needs to be in a strong magnetic field. The mag-netic moments of the hydrogen protons of the patient then align with the direction of the external magnetic field. With the help of radiofrequency (RF) transmitter coils, an additional magnetic field is then temporarily created. The RF pulse causes some protons to alter their alignment relative to the field. Once the RF pulse is turned off again, the altered protons return to their original equilibrium, a process called relaxation, accompanied by a release of energy in the form of an RF signal. The RF signal is cap-tured by the RF receiver coil, which is usually placed close to the body part of interest.
Fig 5: Three dimensional reconstruction CT image of a cat with a mediastinal mass (a). After drawing a region of interest, (b) the mass is represented as a blue volume within the thorax
Fig 6: Virtual CT endoscopy at the level of the carina with a view at both mainstem bronchi
Tissue/material T1 weighted MRI T2 weighted MRI
Air Black Black
Cortical bone Black Black
Fluid Dark Bright
Fat Very bright Very bright
Cerebrum White matter brighter than grey matter
Grey matter brighter than white matter
Table 2: Tissue characteristics on MRI images
(a)
(b)
Fig 4: Multiplanar reconstruction (MPR) is the computer technique that allows the images to be reformatted in any plane. (a) Sagittal, (b) transverse and (c) dorsal
(a)
(b) (c)
CT and MRI.indd 548 08/11/2013 11:22
group.bmj.com on November 16, 2013 - Published by inpractice.bmj.comDownloaded from

Companion animalS
551In Practice November/December 2013 | Volume 35 | 546-563
The speed of return to equilibrium is defined by two physical factors, the T1 and T2 relaxation times, which are tissue specific. This allows differen-tiation of different tissues on an MR image. Different combinations of RF pulses and magnetic fields can be used to create sequences of images with dif-ferent tissue contrast. The spin-echo T1 and T2 sequences are most com-monly used and their characteristics are displayed in Table 2. Additional MRI sequences can be applied to suppress selected tissues/material, such as fluid (FLAIR sequence) or fat (STIR sequence), in order to increase the visibility of adjacent structures. Intravenous injection of gadolinium-based contrast medium is used in most patients to increase the vascular and soft tissue contrast (Fig 7).
In contrast to CT, MR images can be acquired in any desired body plane (transverse, dorsal, sagittal, oblique) with maximal image resolution. This leads to an increase in total examination time. For exam-ple, a typical brain protocol will take between 30 and 45 minutes. Post processing reconstruction in other planes is also possible, but due to the bigger slice thick-ness of MR images (usually 2 mm or more), the image resolution is then markedly decreased.
An MRI scanner is composed of a main magnet, an RF transmitter coil and a receiver coil. Two main types of MRI scanners exist, which will be discussed now.
Low-field-strength MRIThese systems use a permanent magnet with a field strength of approximately 0.25 Tesla. The magnetic field is created between two horizontal discs allowing a relatively open access for the patient (Fig 3). This can
be advantageous for the scanning of equine patients or large body parts of other animals. Low field systems are relatively low in purchase price and maintenance as they have no specific requirements for electric sup-ply and cooling and only require inexpensive magnetic shielding. They also have a small footprint and the low magnetic field is a bonus from a safety perspec-tive. The image quality of current systems is good for most body parts, but it is not excellent. Because of the relatively small usable magnetic field, long body parts, such as the spine, need to be imaged in many small seg-ments for which the animal needs to be repositioned. This increases the total examination time.
High-field-strength MRIThese systems use superconducting magnets with a
Table 3: Key differences between CT and MRI
CT MRI
Ionising radiation No ionising radiations
Based on x-ray technology Relies on magnetic fields and radiofrequency pulses
X-ray beam attenuation as it passes through the body
Creates a map of hydrogen atoms in the body
Two main types of scanners: single-slice and multi-slice
Two main types of scanners: low- and high-field-strength
Image acquisition in transverse plane and reconstruction with near equivalent resolution in multi-slice scanners
Image acquisition in any plane
Thin slices (up to 0.5 mm) Thicker slices (usually minimal 2 mm)
Quick acquisition, usually seconds to few minutes
Slow acquisition, usually about 30 to 60 minutes
Great imaging detail for bones Great imaging detail for soft tissues
Equipment, setup and maintenance usually less expensive than MRI
Equipment, setup and maintenance usually more expansive than CT
Iodinated contrast media Gadolinium-based paramagnetic contrast media
CT MRI
Central nervous system CT is modality of choice if MRI unavailableHelpful when lesion is vascularisedComplementary to MRI in cases of trauma, fractures and bone malformations
Imaging modality of choiceExcellent tissue contrastSpecial sequences to identify particular pathology (eg, gradient echo, FLAIR, DWI)
Skull and splanchnocranium Excellent and rapidSuperior osseous details in generalEvaluation of the teeth
ExcellentShow additional meningeal enhancement in case of cribriform plate invasionSuperior assessment of cranial nerves, inner ear, adjacent brainstemSpecial sequences to identify nerve pathology ...(eg, STIR)
Thorax Imaging modality of choiceSuperior metastatic screening when compared to radiographs
MRI should be performed only if CT is not availableRespiratory and cardiac gating required
Abdomen and pelvis Excellent and rapidSuperior osseous details
Superior soft tissues contrast but requires additional expertise and experience
Musculoskeletal Excellent and rapidSuperior osseous details
Superior assessment of articular cartilage, synovial fluid, periarticular soft tissues, tendinous and ligamentous structuresSuperior assessment of bone marrow neoplastic infiltration
Angiography ExcellentBest results obtained with helical scanners and rapid injection pump
ExcellentBest results obtained with high-field-strength MRI scanners and special sequences
Table 4: Summary of the indications for CT and MRI according to the anatomical region
CT and MRI.indd 551 08/11/2013 11:25
group.bmj.com on November 16, 2013 - Published by inpractice.bmj.comDownloaded from

Companion animalS
552 In Practice November/December 2013 | Volume 35 | 546-563
typical field strength of one or 1.5 Tesla. Their exter-nal appearance is similar to CT scanners (Fig 3). A large cylindrical gantry composed of electromagnets supercooled with liquid helium creates the magnetic field. Superconducting magnets can achieve very high field strengths of up to nine Tesla. The long enclosed tubular space for the patient creates challenges for monitoring and can be a limitation for large animal MRI. For instance, with most high-field-strength MRI units, it is not possible to fit in the equine neck or sti-fle. High-field-strength MRI units are very expensive in purchase and maintenance, require ample space, expensive magnetic shielding and three phase power supply. However, the image quality is excellent for most body parts, longer body parts can be imaged without repositioning, and a wide range of functional imaging is possible. High-field-strength MRI scanners are more suited for advanced techniques, such as to MR angiography. Special sequences have also been developed to identify particular pathology, such as the
diffusion-weighted imaging (DWI) used in the charac-terisation of ischemic strokes.
Unlike CT, no ionising radiation hazards are associ-ated with MRI (Table 3). So far, no health risks from strong magnetic fields have been identified and the procedure is regarded as safe for patients and opera-tors. However, due to the strong magnetic field, any metallic device in the vicinity of the scanner can turn into a dangerous projectile. Vigilant monitoring of all personnel and patients for metal objects is therefore mandatory with high-field-strength MRI. This also means that anaesthetic and monitoring equipment must be non-ferrous and MR-compatible if positioned near the scanner. In most anatomical regions, CT and MRI are suitable cross sectional imaging techniques, should the choice exist. However, MRI is superior for inves-tigations of the central nervous system pathology and CT is the modality of choice in any thoracic imaging. Note that higher image quality will be obtained with high-field-strength MRI scanners. For a summary of the indications for CT and MRI in small animals, see Table 4.
Central nervous system
The use of cross sectional imaging in the investigation of brain diseases has revolutionised neurology. Due to its high tissue contrast capability, MRI has become the diagnostic imaging technique of choice to evaluate the brain parenchyma. However, CT is suitable to use in cases where MRI is not available. CT is also helpful when the lesion demonstrates contrast enhancement or involves osseous changes.
NeoplasiaMRI offers the possibility to describe precisely a lesion located in the brain parenchyma. The anatomical loca-tion, size, shape and extent can be clearly defined. By repeating various sequences over a lesion, it is also pos-sible to predict the nature and content according to the changes in contrast medium uptake. However, MRI and CT are non-specific with respect to the histology of most lesions. The two most common types of cen-tral nervous neoplasia encountered in dogs and cats are meningiomas and gliomas.
Meningiomas grow slowly, often taking years to reach the critical size to cause symptoms. They are well-defined masses originating from the meninges and will compress brain parenchyma. Meningiomas are highly vascularised and will demonstrate contrast enhancement on MRI and CT (Figs 8 and 9).
Gliomas originate from the brain parenchyma. These include astrocytomas and oligodendrogliomas. Their growth is often rapid and can exceed their vas-cular supply, resulting in central necrosis and poor contrast enhancement (Fig 8). In a recent study, no CT or MR features have been identified that can reliably distinguish between these two tumour types (Young and others, 2011).
Choroid plexus tumours arise from choroid plexus tissue of the ventricular system. Due to their origin, theses tumour systems tend to be located in or around the ventricular system. Because of the large concentra-tion of blood vessels, these tumours are highly vascu-
Fig 8: Transverse MRI images of the brain of a dog with seizures. The T2-weighted sequence (a) shows a broad-based mass (*) arising from the dura mater compressing the left frontal lobe of the brain. The underlying calvarial bone is decreased in signal intensity consistent with sclerotic hyperostosis (yellow arrows). A large amount of diffuse and hyperintense perilesional oedema is present in the vicinity of the mass (white arrows). The mass is markedly contrast-enhancing on the T1-weighted post-contrast sequence with a tail-like lateral margin. Dural tail sign (red arrow) (b). These features are indicative for a meningioma. (Images, Animal Health Trust)
(a) (b)
* *
Fig 7: Transverse MRI images of the brain of a dog with a histologically confirmed brain tumour (oligodendroglioma). The brightness of the tumour and the contrast to the neighbouring brain tissue varies between the T2-weighted image (a), FLAIR (b), T1-weighted image (c) and T1-weighted image post-contrast (d). The use of multiple MRI sequences helps to localise the lesion in the left frontal lobe and characterises its fluid-filled nature. (Images, Animal Health Trust)
(a) (b)
(c) (d)
CT and MRI.indd 552 08/11/2013 15:02
group.bmj.com on November 16, 2013 - Published by inpractice.bmj.comDownloaded from

Companion animalS
554 In Practice November/December 2013 | Volume 35 | 546-563
Fig 9: CT of a meningioma in a dog. On the initial CT scan (a) the mass can be seen as a strongly contrast enhancing pedunculated mass arising from the rostrodorsal calvarium causing adjacent hypoattenuating brain oedema and a deviation of the falx cerebri (away from the arrow). On a bone window (b) the hyperostotic nature of the underlying calvarium can be seen (arrows). The mass was removed surgically with incomplete margins (c). On a follow-up scan several weeks later (d), the reoccurrence of the mass with a dural tail sign (red arrows) and invasion into the frontal sinus can be seen
Fig 11: Transverse gradient echo MRI image of the brain of a dog with a pituitary macroadenoma. The hypointense (dark) areas in the mass in this particular sequence are indicative of haemorrhage (arrow). (Image, Animal Health Trust)
larised and will enhance on both modalities.Pituitary tumours are located at the base of the
cranium within the pituitary fossa. Small microadeno-mas are often not clearly appreciated on CT or MRI and necessitate the use of dynamic contrast studies. However, macroadenomas are very visible, contrast-enhancing lesions, which can show mass effect, peripheral oedema and haemorrhage (Figs 10 and 11).
Intracranial masses can be associated with periph-eral oedema because of their compressive effect on the brain tissue (Fig 8).
Vascular lesionsCerebrovascular accidents or ‘strokes’ are character-ised by an area of ischemia with or without haem-orrhage. Ischemic infarcts most commonly affect specific vascular territories. Haemorrhagic strokes can have a varied appearance, primarily based on the duration of the haemorrhage and alteration in blood haemoglobin. Diffusion-weighted MRI sequences allowing the mapping of water molecules can aid in the diagnosis of infarcts (Fig 12). Gradient echo MRI sequences are commonly used for the diagnosis of haemorrhage (Fig 11). In standard CT scans, only haemorrhagic infarcts can be diagnosed confidently. However, with additional software, it is possible to perform perfusion CT that allows diagnosis of ischemic infarcts.
InflammationInflammatory brain diseases can affect the brain parenchyma (encephalitis) or meninges (meningi-tis) and can be divided into infectious inflammatory and non-infectious inflammatory diseases. They produce highly suggestive changes on MRI, such as mass effect, contrast enhancement and perilesional oedema. Because of its high contrast resolution and the use of specific sequences, such as FLAIR, MRI is far superior for the evaluation of brain oedema and subtle periventricular lesions (Fig 13). In general, CT
(a) (b)
(c) (d)
Fig 10: Contrast-enhanced CT image of a pituitary tumour with laterally displaced pituitary and peripheral vessels (arrows). Displacement of the centrally located pituitary artery can be used to diagnose even microadenomas with dynamic CT or MRI
Fig 12: Dorsal MRI images of a canine brain (a). There is a well-defined T2 hyperintense cerebellar lesion (red arrow) adjacent to the vermis in the region supplied by the rostral cerebellar artery. The diffusion weighted sequence (b) provides supportive evidence for the diagnosis of infarction in this patient (white arrow). (Images, Animal Health Trust)
(a) (b)
CT and MRI.indd 554 08/11/2013 15:03
group.bmj.com on November 16, 2013 - Published by inpractice.bmj.comDownloaded from

Companion animalS
555In Practice November/December 2013 | Volume 35 | 546-563
is less sensitive for the detection and characterisation of parenchymal or meningeal inflammatory lesions.
TraumaCT is the modality of choice for the investigation of a head trauma. CT represents a practical option, as the scanning time will be much shorter than with MRI. With multi-slice CT scanners, sedation is usually suf-ficient to perform a subminute examination. The same applies to comatose patients. CT also offers superior osseous details compared to MRI, allowing clear dem-onstration of skull fractures (Fig 14).
Spinal diseasesThe use of CT alone for investigation of spinal cord disease in acutely paretic or plegic patients is supe-rior to conventional radiography and myelography; however, it is inferior to MRI. Extruded mineralised disc material will be readily visualised in non-contrast CT examinations. However, CT is less sensitive than MRI when the disc lesion is not mineralised. In these cases, CT myelography will often be necessary to identify small cord compressive lesions, but detailed assessment of the cord parenchyma on CT is limited. Presence of small intra-parenchymal lesions is much better recognised on MRI without the inherent risk of myelography (Figs 15 and 16).
Thorax
There is a very large variation in tissue density within the thorax, which extends from the air-filled bronchus (HU = –1000) to the bony ribs (HU = +1000), which can all be depicted by CT. In addi-tion, multi-slice CT technology allows acquisition of large body areas within seconds, which decreases the potential of respiratory motion artefacts. Ideally, the images are obtained during a period of apnoea. This is usually achieved by hyperventilating the patient immediately before scanning or by using remote ventilation and breath-holding techniques. CT is the modality of choice for the imaging of all thoracic structures including the pleura, mediastinum, bron-chi, pulmonary parenchyma and the thoracic wall,
Fig 13: Transverse MRI images of the brain of a chihuahua diagnosed with inflammatory encephalitis. The T2-weighted image (a) shows mild bilateral ventriculomegaly. A hyperintense lesion is clearly visible on the FLAIR sequence at the level of the right caudate nucleus (arrow) (b). The latter is unlikely to be visible on CT. (Images, Animal Health Trust)
(a) (b)
Fig 14: Transverse CT image of the nose of dog involved in a road traffic accident. CT provides excellent detail of the bone and shows multiple fractures and displacement of the hard palate (arrowheads)
Fig 15: T2-weighted sagittal plane MRI image of the vertebral column of a dog showing dorsal extradural compression of the spinal cord (arrow). The lesion is hyperintense on T2. Note the diffuse hyperintensity of the cord parenchyma at the level of compression suggestive of oedema or gliosis. Final diagnosis after surgery and histopathology was necrotising steatitis. (Image, Animal Health Trust)
Fig 16: Sagittally reconstructed CT myelography image of a dog with marked extradural compression of the spinal cord at multiple locations, most marked at T12/T13 (red arrow). The use of myelography allows delineation of the spinal cord compression. Note the presence of contrast medium partially filling the central canal of the spinal cord (yellow arrow). (Image, Ecole Nationale Vétérinaire de Maisons-Alfort)
T12
CT and MRI.indd 555 08/11/2013 15:03
group.bmj.com on November 16, 2013 - Published by inpractice.bmj.comDownloaded from

Companion animalS
558 In Practice November/December 2013 | Volume 35 | 546-563
except for the heart. CT also offers superior meta-static screening compared to radiography (Fig 17). In a recent study involving 18 dogs with histologically confirmed pulmonary metastatic neoplasia, only nine per cent of CT-detected pulmonary nodules were identified on thoracic radiography (Nemanic and others 2006). CT-lymphangiography allows identification of the thoracic duct in dogs and cats (Kim and others 2011).
Conversely, the low signal produced by the lungs on MRI together with respiratory and cardiac motion artefacts makes MRI less suitable for a rou-tine thoracic workup. However, if CT is not accessi-ble, MRI can be useful in the assessment of thoracic wall or mediastinal masses. Respiratory and cardiac gating techniques are required for MRI of the tho-rax. Cardiac MRI (Mai and others 2010) can also be performed, but necessitates special experience and extremely advanced MR scanners (Fig 18).
Skull and splanchnocranium
CT and MRI are equally useful in the investigation of the orbit, nasal cavities, sinuses and ears.
CT and MRI allow clear visualisation of the palpe-bral region, the anterior and posterior segments of the eye, the retrobulbar structures, and the zygomatic sali-vary glands. Abnormalities of the optic nerve, such as optic neuritis, are readily identified (Fig 19). Due to the large amount of fat in the orbital region, MRI fat-sup-pressed sequences, such as STIR, are particularly use-ful to demonstrate the extent of an orbital neoplasia.
For the nasal cavities, CT is particularly helpful for the evaluation of the nasal turbinates, maxillary and palatine bone destruction or periosteal new bone formations. Sinus pathologies can be equally assessed on CT and MRI. While both CT and MRI can detect changes involving the cribriform plate, rostral menin-geal enhancement is better demonstrated with MRI. This can be helpful to detect the early signs of intracra-nial involvement of nasal neoplasia. Volume-rendering reconstructions can demonstrate skull fractures and bone osteolysis in three dimensions (Fig 20). This tool is commonly used to communicate information to a client, a clinician, or for teaching purposes, but is rarely useful for diagnostic purposes. It is helpful for surgical and radiotherapy planning (Fig 20). CT offers exquisite bone details, which makes it ideal for evaluation of the teeth. CT and MRI features of sev-eral dental diseases have been reported, such as dental cysts, dental fractures, periapical abscesses, pulpitis and dental neoplasia (Fig 21). CT and MRI are both very helpful in the diagnostic workup of masticatory diseases, such as temporomandibular luxation, frac-tures, masticatory myositis and neoplasia (Fig 22).
CT and MRI are both able to detect fluid or a mass within the tympanic bulla and external ear canal. CT has greater ability to evaluate tympanic wall thicken-ing or erosions (Fig 23). MRI offers excellent tissue contrast for the para-aural soft tissues. Only MRI is capable of diagnosing true otitis interna by assess-ment of signal changes of the endolymph of the semi-circular canals and cochlea (Fig 24). Associated brain disease is better assessed by MRI, but might also be recognised on CT.
Extremities
The use of MRI in small animal musculoskeletal diseas-es is still in its early days compared to its use in humans and horses. The size of small animal joints is a limit-ing factor when the acquisition of images is performed with low-field-strength MRI. The MRI anatomy and standard patient positioning are still in the process of being described. Finally, while MRI is the gold stand-ard for investigation of early sport injuries in horses, athletic injuries are not a common presenting com-plaint in dogs and cats. To date, the shoulder and the stifle joints are the most commonly examined extremity parts with MRI. Reports on biceps and supraspinatus tendon pathology, neoplasia, cranial cruciate ligament discontinuity (Fig 25) and meniscal injuries have been published (Barrett and others 2009). MRI is also more sensitive for the detection of subtle bone marrow chang-es (Fig 26) compared to CT and could provide addition-al information concerning the cartilage. MRI is greatly utilised in the investigation of neoplasia, in particular for surgical planning. MRI is very well suited for the diagnosis of brachial plexus diseases.
CT is the modality of choice for the investigation of skeletal pathology, such as fractures, deformities and joint diseases. Multiplanar reconstructions are essential and 3D reconstructions are often helpful for surgical planning (Fig 27). CT has become the gold standard for imaging of elbow dysplasia, including osteochondrosis, medial coronoid disease (Fig 28) and joint incongruity. CT arthrography is increasingly used to outline the intracapsular anatomy of large joints, such as the stifle, elbow and shoulder. CT and arthroscopy have been shown to be complementary techniques, with CT identifying some lesions not seen on arthroscopy and vice versa.
Abdomen
CT offers excellent anatomical detail of the abdomen. Imaging protocols and specific pathological CT fea-tures have been established for most abdominal organs, including the liver, spleen, pancreas, gastrointestinal tract, adrenal glands, urinary tract and genital tract. If not clinically contraindicated, iodinated non-ionic
Fig 17: Transverse CT maximum intensity projection of the thorax of a dog. A 5 mm solitary pulmonary nodule is visible (arrow). This nodule was not visible on radiographs
CT and MRI.indd 558 08/11/2013 15:04
group.bmj.com on November 16, 2013 - Published by inpractice.bmj.comDownloaded from

Companion animalS
561In Practice November/December 2013 | Volume 35 | 546-563
contrast medium administration is recommended in order to fully delineate the organs and obtain infor-mation regarding their perfusion. CT is very helpful in the assessment of suspected neoplasia and regional lymph nodes with the addition of a thoracic metastatic scan (Fig 29). In obese large breed dogs, CT might be preferred to abdominal ultrasonography.
With multi-slice CT, it is also possible to obtain exquisite angiographic studies. Best results are obtained with help of a rapid injection pump. Abdominal CT angiography allows the diagnosis
of complex vascular diseases, such as arterioportal hepatic fistulae and portosystemic shunts (Fig 30).
Abdominal MRI is still in its infancy in veterinary medicine. Sophisticated high-field-strength MRI scanners with respiratory gating and motion reduc-tion software can produce excellent image quality. For the pelvic region, MRI offers superior soft tissue con-trast and the ability to assess the adjacent central nerv-ous system (CNS) structures more readily, whereas CT provides a better delineation of osseous changes. Special MR angiographic techniques can also be used to diagnose abdominal vascular disorders (Fig 31).
Fig 18: Bright-blood cardiac MRI in a normal dog. Representative images of Cine-bright blood loops in short and long axis. Various points through the cardiac cycle can be sampled, allowing dynamic assessment of the cardiac contractions similar to echocardiography. (Image, Wilfried Mai, University of Pennsylvania)
Fig 19: MRI of the brain dorsal plane, T2-weighted sequence, showing thickening of the left optic nerve consistent with optic neuritis (arrow). (Image, Animal Health Trust)
Fig 20: Three dimensional volume rendering of the skull of a dog diagnosed with highly destructive maxillary osteosarcoma. (Image, Fitzpatrick Referrals)
Fig 21: Transverse CT image of the rostral mandible of a French bulldog. The first right lower premolar (arrow) is surrounded by an expansile fluid filled cyst (C), consistent with a dentigerous cyst. Untreated, such cysts can eventually lead to a mandibular fracture
C
Fig 22: Transverse CT image of the temporomandibular joints of a cat that had fallen from a height. Notice the fractured mandibular condyle (white arrow) and mandibular fossa (red arrow)
CT and MRI.indd 561 08/11/2013 15:05
group.bmj.com on November 16, 2013 - Published by inpractice.bmj.comDownloaded from

Companion animalS
562 In Practice November/December 2013 | Volume 35 | 546-563
Fig 26: Dorsal plane STIR sequence MRI image of the mandible of a four-year-old basset hound. The destructive soft tissue mass involving the rostral aspect of the left mandible was diagnosed as a squamous cell carcinoma. Note the diffusely hyperintensity extending along the left ramus (arrows) consistent with neoplastic bone marrow invasion. (Image, Animal Health Trust)
Fig 27: Three dimensional volume rendered reconstruction CT image of the left and right forelimbs of a dog affected with bilateral angular limb deformity. Note the lateral radial luxation on the left limb
Fig 28: Transverse CT of the elbow of an eight-month- old bulldog. There is fragmentation of the medial coronoid process (arrow) of the ulna (U)
Fig 23: Transverse CT image at the level of the tympanic bullae of a dog showing marked thickening of the left ventral bulla wall (white arrow) suggesting chronic otitis media. There is an expansile lesion involving the right tympanic bulla consistent with a cholesteatoma (red arrow). Both tympanic bullae are filled with homogeneous non-enhancing material. (Image, Clerkenwell Animal Hospital)
Fig 24: Transverse plane MRI image, T2-weighted sequence of a normal dog at the level of the tympanic bullae. The cochleae of the inner ears are visible as T2 hyperintense signals (arrows), and have the shape of a duck. (Image, Animal Health Trust)
Fig 25: Sagittal plane proton-weighted MRI image of the stifle of a dog. The normally hypointense cranial cruciate ligament is no longer visible and is replaced by thick, hyperintense and heterogeneous material (arrows) consistent with incomplete cranial cruciate ligament rupture
CT and MRI.indd 562 08/11/2013 15:05
group.bmj.com on November 16, 2013 - Published by inpractice.bmj.comDownloaded from

Companion animalS
563In Practice November/December 2013 | Volume 35 | 546-563
Whole body imaging
Recently, whole body MRI protocols have been described for cancer staging in animals with a sufficient image quality to detect mass lesions, pulmonary infil-trate, lymphadenomegaly and lesions of the appendicu-lar skeleton (Kraft and others 2007). Some institutions are also performing whole body CT examinations for the same purpose. CT is certainly very useful in detect-ing previously undetected pulmonary metastatic dis-eases and bone lesions.
PET Scanning
Positron emission tomography (PET) is becoming increasingly available as an imaging modality in vet-erinary medicine (Hansen and others 2011). PET is a nuclear medicine imaging technique that detects gamma rays indirectly emitted by a positron-emitting tracer, the fluorodeoxyglucose (FDG). FDG is an ana-logue of glucose that will be metabolised by high-glu-cose-using cells, such as neoplastic cells. By combining PET informations with a CT or an MRI, it becomes possible to correlate metabolic and anatomic informa-tions on a same image. PET/CT or PET/MRI may even-tually become the gold standard of cancer staging in our canine and feline patients.
References BARRETT, E., BARR, F., OWEN, M. & BRADLEY, K. (2009) A retrospective study of the MRI findings in 18 dogs with stifle injuries. Journal of Small Animal Practice 50, 448-455HANSEN, A. E., McEVOY, F., ENGELHOLM, S. A., LAW, I. & KRISTENSEN, A. T. (2011) FDG PET/CT imaging in canine cancer patients. Veterinary Radiology & Ultrasound 52, 201-206KIM, M., LEE, H., LEE, N., CHOI, M., KIM, J., CHANG, D., CHOI, M. & YOON, J. (2011) Ultrasound-guided mesenteric lymph node iohexol injection for thoracic duct computed tomographic lymphography in cats. Veterinary Radiology & Ultrasound 52, 302-305 KRAFT, S., RANDALL, E., WILHELM, M. & LANA, S. (2007) Development of a whole body magnetic resonance imaging protocol in normal dogs and canine cancer patients. Veterinary Radiology & Ultrasound 48, 212-220MAI, W., WEISSE, C. & SLEEPER, M. M. (2010) Cardiac magnetic resonance imaging in normal dogs and two dogs with heart base tumor. Veterinary Radiology & Ultrasound 51, 428-435NEMANIC, S., LONDON, C. A. & WISNER, E. R. (2006) Comparison of thoracic radiographs and single breath-hold helical CT for detection of pulmonary nodules in dogs with metastatic neoplasia. Journal of Veterinary Internal Medicine 20, 508–515YOUNG, B. D., LEVINE, J. M., PORTER, B. F., CHEN-ALLEN, A. V., ROSSMEISL, J. H., PLATT, S. R., KENT, M., FOSGATE, G. T. & SCHATzBERG, S. J. (2011) Magnetic resonance imaging features of intracranial astrocytomas and oligodendrogliomas in dogs. Veterinary radiology & ultrasound 52, 132-141
Further readingALLEN, A. V., ROSSMEISL, J. H., PLATT, S. R., KENT, M., FOSGATE, G. T. & SCHATzBERG, S. J. (2011) Magnetic resonance imaging features of intracranial astrocytomas and oligodendrogliomas in dogs. Veterinary Radiology & Ultrasound 52, 132-141SCHWARz, T. & SAUNDERS, J. (2011) Veterinary Computed Tomography. Wiley-BlackwellWHATMOUGH, C. & LAMB, C. R. (2006) Computed tomography: principles and applications. Compendium on Continuing Education for the Practicing Veterinarian 28, 789-800
Fig 29: Transverse CT post-contrast image of a dog presented with an abdominal mass. The mass is ill-defined and shows a heterogeneous pattern of enhancement. The mass is adjacent to the descending duodenum (D) and displaces the right kidney (RK) dorsally. The mass also causes compression of vascular structures. A pancreatic carcinoma was confirmed. The spleen (S) was unremarkable
(D)
(S)
(RK)
(P)
(sh)(Ao)
(CVC)
Fig 30: CT angiography sagittal plane reconstruction, portal phase. There is a tortuous blood vessel extending from the portal vein (P) in a dorsal direction, joining the azygos vein along the thoracic vertebrae. The diagnosis was porto-azygos shunt (sh). Ao Aorta, CVC Caudal vena cava, P Portal vein
(Ao)
(CVC)
(P)
Fig 31: Contrast-enhanced MR angiography of the abdomen in a normal schnauzer dog. Ao Aorta, CVC Caudal vena cava, P Portal vein. (Image, Animal Health Trust)
CT and MRI.indd 563 08/11/2013 15:05
group.bmj.com on November 16, 2013 - Published by inpractice.bmj.comDownloaded from

doi: 10.1136/inp.f6720 2013 35: 546-563In Practice
Julien Labruyère and Tobias Schwarz on recent advancesCT and MRI in veterinary patients: an update
http://inpractice.bmj.com/content/35/10/546.full.htmlUpdated information and services can be found at:
These include:
References http://inpractice.bmj.com/content/35/10/546.full.html#ref-list-1
This article cites 9 articles
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on November 16, 2013 - Published by inpractice.bmj.comDownloaded from